CHURCHILL LIVINGSTONE An Imprint of Elsevier Science The Curtis Center Independence Square West Philadelphia, Pennsylvania 19106
OFFICE PRACTICE OF NEUROLOGY Copyright © 2003, Elsevier Science (USA). All rights reserved.
ISBN 0-443-06557-8
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Permissions may be sought directly from Elsevier’s Health Sciences Rights Department in Philadelphia, PA, USA: phone: (+1) 215 238 7869, fax: (+1) 215 238 2239, e-mail:
[email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com), by selecting ‘Customer Support’ and then ‘Obtaining Permissions.’ Distributed in the United Kingdom by Churchill Livingstone, Robert Stevenson House, 1-3 Baxter’s Place, Leith Walk, Edinburgh EH1 3AF, Scotland, and by associated companies, branches, and representatives throughout the world. Churchill Livingstone and the sailboat design are registered trademarks.
NOTICE Medicine is an ever-changing field. Standard safety precautions must be followed, but as new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary or appropriate. Readers are advised to check the most current product information provided by the manufacturer of each drug to be administered to verify the recommended dose, the method and duration of administration, and contraindications. It is the responsibility of the licensed prescriber, relying on experience and knowledge of the patient, to determine dosages and the best treatment for each individual patient. Neither the publisher nor the editors assumes any liability for any injury and/or damage to persons or property arising from this publication. Previous edition copyrighted 1996 Library of Congress Cataloging-in-Publication Data Office practice of neurology/edited by Martin A. Samuels, Steven Feske.—2nd ed. p. ; cm. Includes bibliographical references and index. ISBN 0-443-06557-8 1. Neurology. 2. Ambulatory medical care. I. Samuels, Martin A. II. Feske, Steven. [DNLM: 1. Nervous System Diseases—diagnosis. 2. Nervous System Diseases—therapy. 3. Ambulatory Care. WL 140 O32 2003] RC346 .O34 2003 616.8—dc21
Acquisitions Editor: Susan Pioli Developmental Editor: Melissa Dudlick Printed in the United States Last digit is the print number:
9
8
7
6
5
4
3
2
1
2002073673
In memory of Michael S. Pessin, M.D., esteemed friend and colleague. His outstanding clinical skills and research talents inspired many to follow a career in Stroke Neurology. His patients benefited from his vast knowledge, his dedication and his compassion.
Contributors
Robert J.Adams, MD Presidential Distinguished Chair Department of Neurology Medical College of Georgia Augusta, Georgia
JamesW. Albers, MD, PhD Professor of Neurology University of Michigan Medical School Department of Neurology University of Michigan Health System Ann Arbor, Michigan
Lloyd M. Alderson, MD, DSc Assistant Professor of Neurology Brown University School of Medicine Providence, Rhode Island
Michael P. Alexander, MD Associate Clinical Professor of Neurology Harvard Medical School; Department of Behavioral Neurology Beth Israel Deaconess Medical Center Boston Massachusetts
Anthony A. Amato, MD Associate Professor of Neurology Harvard Medical School; Vice Chairman Department of Neurology and Chief, Neuromuscular Division Brigham and Women’s Hospital Boston, Massachusetts
Sepideh Amin-Hanjani, MD Instructor Department of Surgery (Neurosurgery) Harvard Medical School Neurosurgical Service; Massachusetts General Hospital Boston, Massachusetts
Richard M. Armstrong, MD Bastrop, Texas
Gerald M. Aronoff, MD, FAADEP Chairman, Department of Pain Medicine Presbyterian HospitaVPresbyterian Orthopedic Hospital Charlotte, North Carolina
Ajay I70% >70% ~70%
PUN-
FUrrcnOn
MW
DEC~ N/DEC DEC
FEF2S-7,
DEC DEC DEC
Rv
FRC
INC DEC INC
DEC DEC INC
Abbreviations: DEC, decreased; N, normal; INC, increased; W,, forced expiratory volume in 1 second; VC, vital capacity; WC, forced vital capacity; MW, maximal voluntary ventilarnidrnaxirnal forced expiratory flow; RV, residual volume; FRC, functional residual capacity. tion; FEF,,-,, ’Some variability in these patterns is expected between individuals. bMay be decreased out of proportion to the W , .
manifest this obstructive pattern unless there is an associated pulmonary disease. Assessment of Respiratory Muscle Fdgue
Most lung volumes, including expiratory flows, are not affected by mild losses of respiratory muscle strength. One exception may be the maximal voluntary ventilation (MW), which is measured as the amount of air exchanged during 12 to 15 seconds of maximal effort with the reported value extrapolated to 1 minute. Because the maximum number of breaths one can take in 1 minute is about 35 to 40, the M W is usually about 35 to 40 times as great as the FEV,. Like the FEV,, the M W depends on the effort and pulmonary mechanics, but it is also a measure of endurance and is affected by respiratory muscle power and fatigue. Disorders that cause a decrease in FEV, also affect MW, but a reduction in M W out of proportion to a reduction in FEV, should raise suspicion that a neuromuscular disorder is affecting respiration if the patient has given a full effort. lnsplratory and Expiratory Pressures
When lung volumes are still normal in the early stages of neurogenic respiratory dysfunction, maximum inspiratory and expiratory forces may be reduced. These forces can be measured as pressures at the mouth by a manometer and also depend on effort, lung volume, mouth seal, age, and sex. The maximum expiratory pressure (PE,,) is normally 100 to 200 cm H,O, while the maximum inspiratory pressure (Pimm), also called the negative inspiratory force, usually is -70 cm H,O or more (i.e., more parallels diaphragm negative). In theory, because the PI,, function, it should be the more sensitive indicator of respiratory muscle weakness. In practice, PE,, may be more sensitive. In one study, it was abnormal in 87% of patients with respiratory dysfunction of neuromuscular origin. Many of these tests are best suited to the study of the lower motor neuron limb of the neurologic pathways of respiratory control. Clinical assessment of the upper motor neuron pathway is more difficult. The overall pattern of respiration can be evaluated by observing the rhythmicity of respiration or of the contractions of the diaphragm by EMG. Minute ventilation, the product of the tidal volume and the respiratory rate, also gives a measure of the overall integrity of breathing. The mouth occlusion pressure, the mouth pressure response to random occlusion of the airway during inspiration, is determined by an involuntary reaction and may also be decreased in lesions of central control. Central chemical drive can be assessed by CO, inhalation techniques and by the response to hypoxia. Once the presence of a neurogenic cause of respiratory
dysfunction has been confirmed using the measures of respiratory physiology just outlined, one’s knowledge of general and respiratory neuroanatomy can be directed toward determining the anatomic localization of the lesion. LOCALIZATION AND CAUSES OF NEUROGENIC RESPIRATORY DYSFUNCTION Upper Motor Neuron Disorders Upper motor neuron disorders that affect automatic respiration usually produce central (primary) alveolar hypoventilation. Although these patients exhibit resting hypoxemia and hypercapnia, they can normalize their blood gases with increased respiratory effort because of intact voluntary overdrive mechanisms. They are most vulnerable to hypoxia and hypercapnia when they are asleep, when voluntary mechanisms are inactive, and when the central automatic driving mechanisms are inadequate (Ondine’s curse). Lung volumes and inspiratory and expiratory pressures usually are not reduced. The most common site of a lesion that affects central respiratory control is the medulla oblongata. Usually, other brainstem signs accompany such a lesion. Imaging studies, especially magnetic resonance imaging, may be helpful in identifymg a structural abnormality. Upper cervical spinal cord lesions can also produce this syndrome. The following pathologic processes, discussed later in this book, may cause central alveolar hypoventilation. W W W W W
W
Tumor Encephalitis and polio Infarction or hemorrhage Trauma C 1 4 2 subluxation Demyelination Chiari malformations Degenerative diseases (e.g., Leigh’s disease) Association with Hirschsprung’s disease Drugs Idiopathic
A unique association occurs with Hirschsprung’s disease. In these rare patients, the combination of congenital brainstem and neural intestinal lesions raises the possibility that a developmental abnormality in serotonergic neurons in both the intestine and brainstem may lead to gut atonia and Ondine’s curse. In addition to structural lesions, drugs such as sedatives and narcotics can impair central respiratory control, especially in patients with underlying central nervous system or pulmonary disorders. Many brainstem lesions that cause coma can lead to central neurogenic hyperventilation (midbrain), apneustic (pontine), or
Principles of Ambulatoy Neurology and the Approach to Clinical Problems
142
ataxic (medullary) breathing. This subject has been reviewed by Plum and Posner (1982). More subtle dysfunction of the central sleep generator can cause central sleep apnea. High cervical spinal cord lesions (C4 and above), usually traumatic, produce a variety of respiratory abnormalities, from Ondine’s curse to persistent apnea, as a result of bilateral hemidiaphragm paralysis. Lower cervical and thoracic lesions may affectupper airway, paraspinal, intercostal, and abdominal muscle innervation and lead to decreased expiratory and inspiratory pressures and a restriction in lung and chest wall expansion. Hypoventilation and atelectasis may then become chronic problems. Pathologic processes above the brainstem may also affect respiration in more subtle fashion, but their mechanisms and clinical significance are not clear. The cerebral cortex, for example, innervates the contralateral hemidiaphragm. Thus, a cortical lesion, such as a stroke, may weaken the diaphragm, but such unilateral lesions do not appear to produce respiratory dysfunction. Cerebellar atrophy occasionally has been associated with a disordered rhythm of breathing. Disorders of the basal ganglia, especially Parkinson’s disease, may cause dyspnea. Respiratory muscle rigidity with associated shallow breathing, impaired laryngeal and respiratory muscle coordination, and airway obstruction are proposed causes. Other movement disorders, such as tardive dyskinesia, may occasionally interfere with the rhythm of respiration. Lower Motor Neuron Disorders
Lower motor neuron disorders (Table 13-2) account for the majority of neurologic diseases that affect respiration and ultimately result in alveolar hypoventilation. These disorders may cause diaphragmatic dysfunction and present with dyspnea, especially on exertion and when supine. Other signs of lower motor neuron disease, including limb and sometimes extraocular and oropharyngeal (bulbar) muscle weakness, often accompany the respiratory dysfunction. The degree of limb and bulbar weakness does not correlate well with the degree of respiratory muscle weakness. However, in some neuromuscular diseases, significant proximal limb weakness is more likely to accompany respiratory muscle weakness than is isolated distal limb weakness. Serious underlying diaphragm weakness is asymptomatic in many H TABU13-2. Peripheral Nervous System Disorders Associated
with Respiratory Dysfunction Anatomic Localization
Anterior horn cell
Disease
Amyotrophic lateral sclerosis Polio or postpolio syndrome Tetanusa Peripheral netve Cuillain-Barre syndrome Charcot-Marie-Tooth disease Critical illness polyneuropathy Neuromuscular junction Myasthenia gravis Botulism Lambert-Eaton myasthenic syndrome Muscle Dystrophies Inflammatory myopathies Acid maltase deficiency Mitochondria1rnyopathies Toxic myopathies Critical illness myopathy Hypokalernia and rhabdornyolysis HvDoDhosDhatemia ‘Predominantly affects spinal cord interneurons.
Principles of Diagnosis:Common Presenting Symptoms
patients predisposed by their underlying disease to have eventual respiratory decompensation; therefore, the physician should routinely assess the respiratory function in any patient presenting with one of the disorders in Table 13-2. CLINICAL AND LABORATORY ASSESSMENT IN PATIENTS WITH LOWER MOTOR NEURON RESPIRATORY DYSFUNCTION
When respiratory muscle weakness of lower motor neuron origin is identified, the physician should try to determine the precise anatomic localization (i-e.,anterior horn cell, motor root, peripheral nerve, neuromuscular junction, or muscle) and the cause of the neurologic lesion. The detailed neurologic history and examination help to localize the process unless it is isolated to respiratory muscles, a rare occurrence. A pertinent laboratory screen should then be undertaken. In addition to routine serologic studies, measurements of the level of serum creatine kinase and antibody titers to the acetylcholine receptor may be especially useful in suspected muscle diseases and myasthenia gravis. In the latter case, an edrophonium test may also be helpful (see Chapter 103). EMG helps to identify the level of the motor unit affected in patients with respiratory muscle weakness. In addition to routine nerve conduction studies and needle examination of the limbs and paraspinal muscles, repetitive nerve stimulation is done to assess the function of the neuromuscular junction. If myasthenia gravis is highly suspected and repetitive stimulation of a distal and proximal nerve is normal, single-fiber EMG, although nonspecific, increases the sensitivity of diagnosis of a generalized neuromuscular junction disorder to nearly 100% if two muscles are studied. Unfortunately, some patients are unable to cooperate with this demanding examination (see Chapter 103). Electrophysiologic evaluation of the phrenic nerves is now being performed more commonly in many centers and may be useful for anatomic localization of the lesion causing respiratory dysfunction, especially with lesions producing axonal loss. The phrenic nerves can be stimulated percutaneously at the posterior border of the sternocleidomastoidmuscles. Magnetic stimulation of the phrenic nerves is also being performed in some centers. EMG of the diaphragm can also be performed with minimal risk of pneumothorax. One technique has been reviewed by Bolton (1993). Evidence of denervation may be seen with anterior horn cell diseases, upper cervical root degeneration, or other lesions of the phrenic nerves producing axonal loss. Myotonic discharges may be recorded from the diaphragm and suggest a myotonic disorder, but typical motor unit potential changes of myopathy are difficult to separate from normal diaphragmatic motor unit potentials. Therefore, the EMG of the diaphragm does not specifically identify myopathy. Repetitive stimulation of the phrenic nerve for evaluation of neuromuscular junction transmission is technically difficult, but it may be useful in identifymg a neuromuscular junction defect as a cause of neurogenic respiratory failure. SPECIFIC LOWER MOTOR NEURON DISEASES Anterior Horn Cell Diseases
Amyotrophic lateral sclerosis is the most common disorder of the anterior horn cells (and upper motor neurons) that affects respiration, and it does so often. Such patients often have bulbar and limb weakness and fasciculations in addition to upper motor neuron signs. In the early stages of their illness, however, rare
Chapter 13
patients may have only subtle limb weakness or fasciculations, and exertional dyspnea or hypoventilation may be the presenting manifestation of their disease. Preferential phrenic nerveassociated motor neuron loss may cause such a presentation. Treatment is mainly supportive, and it may include riluzole. Long-term management of respiratory failure is based on ethical and medical factors. Some patients do well with intermittent noninvasive positive airway pressure ventilation via the nasal or oral route, and some benefit from continuous home mechanical ventilation via tracheostomy. (Amyotrophic lateral sclerosis is discussed in Chapter 86.)
Poliomyelitis Poliomyelitis, now rare in developed countries, was once a common cause of respiratory failure. Lower brainstem or cervical segment involvement leads to respiratory paralysis. Cerebrospinal fluid pleocytosis and an associated viral syndrome are important diagnostic clues. Rarely, patients with a remote history of polio develop hypoventilation as a component of the postpolio syndrome, especially if the VC falls below 50% of the predicted value. These patients usually have residual respiratory weakness caused by their initial bout with poliomyelitis. (Poliomyelitisis discussed in Chapter 69. Postpolio syndrome is discussed in Chapter 88.)
Tetanus Tetanus affects spinal cord inhibitory interneurons rather than anterior horn cells and may cause respiratory dysfunction by impairing diaphragm relaxation. Recognition of a recent wound and associated clinical features, such as muscle rigidity, are helpful in making the diagnosis. (Tetanus is discussed in Chapter 56.)
Peripheral Neuropathies Guillain-Barrk syndrome, an acute inflammatory demyelinating polyneuropathy, is the most common cause of acute neurogenic respiratory failure. Approximately 20% to 33% of patients with Guillain-Barrk syndrome need ventilatory assistance. Respiratory failure, if it occurs, usually does so in the first 2 weeks of the illness. Patients with respiratory failure also tend to have the greatest generalized weakness, but again, there is no reliable correlation between limb and respiratory muscle weakness. Fortunately, most recover with good supportive care, and plasma exchange and intravenous immunoglobulin shorten the duration of mechanical ventilation. (Guillain-Bard syndrome is discussed in Chapter 92.) Rarely, porphyria, vasculitis, heavy metals such as arsenic, paralytic shellfish poisons, and other toxins, including organophosphates, produce a neuropathic syndrome associated with respiratory failure. Intensive care unit patients may also develop phrenic nerve axonal loss and polyneuropathy in association with sepsis and multiorgan failure, called critical illness polyneuropathy. Some patients with the demyelinating form of Charcot-MarieTooth disease (hereditary motor and sensory neuropathy type I) may develop mild respiratory dysfunction, although this clinical observation has not been made frequently. These patients with Charcot-Marie-Tooth disease and those without respiratory symptoms have normal lung volumes but may have low inspiratory and expiratory pressures. Unilateral phrenic nerve injury or compression usually does not cause respiratory failure unless it is associated with a
Respiratory Dysfunction
143
pulmonary disorder or another cause of respiratory muscle weakness. Bilateral phrenic nerve injury, which may rarely occur intraoperatively, does cause respiratory failure.
NeuromuscularJunction Disorders Approximately 30% of patients with myasthenia gravis have respiratory muscle weakness, and 10% to 15% may develop respiratory failure as a major component of myasthenic crisis. Most of these patients have already been diagnosed with myasthenia gravis, but some present with respiratory distress as their initial complaint, often after a precipitating illness or after administration of drugs, such as neuromuscular junction blocking agents. An acetylcholinesteraseinhibitor overdose can also cause respiratory muscle weakness. (Myasthenia gravis is discussed in Chapter 103.) Botulism, a presynaptic neuromuscular junction disorder in which acetylcholine release is blocked by an ingested neurotoxin, may cause respiratory failure along with gastrointestinal symptoms, pupillary paralysis, and extraocular and bulbar weakness. (Botulism is discussed in Chapter 105.) Respiratory dysfunction occurs in about 6% of patients with another rare presynaptic disorder, Lambert-Eaton myasthenic syndrome. The respiratory dysfunction may develop spontaneously, or it may be precipitated by anesthesia. The diagnosis often is confused with myasthenia gravis, but the presence of lowamplitude motor responses that markedly increase in amplitude after a brief period of exercise should help to distinguish Lambert-Eaton myasthenic syndrome from myasthenia gravis. (Lambert-Eaton myasthenic syndrome is discussed in Chapter 104.) Tick paralysis is caused by the bite and persistent attachment of a tick, most commonly Derrnacentor andersoni, usually along the hairline of a child. It may cause respiratory and limb paralysis as a result of neuromuscular junction blockade. Complete removal of the tick cures this illness. Some snake, spider, and scorpion toxins also cause respiratory muscle paralysis. Drugs, such as magnesium in antacids, aminoglycosides, lithium, and acetylcholinesterase inhibitors may potentiate or cause defects in neuromuscular transmission. Myopathic Disorders Long-standing severe dystrophies, especially Duchenne’s muscular dystrophy, produce respiratory muscle weakness that causes a restrictive disorder, atelectasis, and hypoventilation. Superimposed scoliosis in many patients exacerbates the restrictive limitation. Thus, surgery for scoliosis often is performed early after boys with Duchenne’s muscular dystrophy become wheelchairbound and before pulmonary function deteriorates further. (Muscular dystrophies are discussed in Chapter 107.) Rare patients with myotonic dystrophy develop alveolar hypoventilation with a restrictive spirometric pattern, probably as a result of respiratory muscle weakness. Myotonic discharges may be identified by EMG of the diaphragm. Some patients with myotonic dystrophy may also develop hypersomnolence of central origin. (Myotonic dystrophy is discussed in Chapters 107 and 112.) Acid maltase deficiency is a rare glycogen storage disease that occurs in infantile, childhood, and adult forms. In the adult form, up to one third of the patients present with respiratory failure. Most patients also have proximal weakness, an elevation in creatine kinase levels, and increased insertional activity with
144
Principles of Ambulatory Neurologyand the Approach to Clinical Problems
Principles of Diagnosis: Common Presenting Symptoms ~
~~
complex repetitive discharges and even myotonic discharges in affected muscles, especially the paraspinals. Muscle pathology and biochemical studies reveal a vacuolar myopathy with low or absent acid maltase activity. (Acid maltase deficiency is discussed in Chapter 110.) Rarely patients with mitochondrial and severe congenital myopathies also develop respiratory failure. Acquired myopathies, especially the inflammatory disorders polymyositis and dermatomyositis, often are associated with respiratory muscle weakness of varying degrees, as identified by pulmonary function studies. Overt respiratory failure is less common. Respiratory muscle weakness may be the presenting feature in up to 4% of patients with polymyositis. (Inflammatory myopathies are discussed in Chapter 108.) Myopathies caused by toxins, such as alcohol, may also involve respiratory muscles. In particular, the combination of high-dose intravenous corticosteroids and neuromuscular blocking agents administered to some critically ill patients, especially those in status asthmaticus and after organ transplantation, can cause a myopathy (critical illness myopathy) that often affects respiratory muscles. Reversible loss of myosin thick filaments and muscle membrane inexcitability seem to cause the weakness in these patients. Hypophosphatemia can cause rapidly reversible respiratory weakness, probably on the basis of muscle dysfunction, but the anatomic localization of the abnormality is uncertain. Severe hypokalemia with or without rhabdomyolysis can cause limb and respiratory muscle weakness. Other electrolyte disturbances, such as hyponatremia, hyperkalemia, hypercalcemia, and hypermagnesemia, may also result in generalizedweakness without preferential diaphragm involvement.
MANAGEMENT OF NEUROGENIC RESPIRATORY DYSFUNCIION Treatments for the specific disorders mentioned in this chapter are discussed in later chapters that address these diseases. Here are some general guidelines for managing neurogenic respiratory failure. To handle this problem expertly, it is often helpful to enlist the assistance of colleagues in critical care and pulmonary medicine. Acute Management
This subject has been recently reviewed by Wijdicks and Bore1 (1998). As with all causes of respiratory distress, assessing airway, respiration, and vital signs is the first step. Patients must be individually evaluated regarding the need for acute intervention (e.g., hospitalization, intensive care unit management, endotracheal intubation) based on the clinician’s judgment and laboratory assessment. Evidence of intercurrent illnesses, especially pulmonary infections, should be sought. Electrolyte abnormalities and other metabolic disturbances can also worsen respiratory weakness. A chest radiograph, arterial blood gas measurement, and bedside FVC, PE,,,, or PI,, should be obtained on all patients. There is usually a correlation between the clinical state and inspiratory and expiratory pressures. A PE,, of less than 40 cm H,O may be associated with the inability to clear secretions, and a PI,, of less than -20 cm H 2 0 (absolute value) may indicate imminent progression to hypoventilation with hypercapnia. However, facial muscle weakness may lead to spuriously low readings. The inability of a patient to count to 20 in one breath is a useful bedside test suggesting that the VC is less than 18 mL/kg. With
A
Respiratory pathophysiology
Ventilatory management
Normal I
\
65 mUka
Poor cough-secretions accumulate Sigh mechanismcompromisedatelectasis; hypoxemia begins
/ /
/
30mUkg 25 mUkg
10 mUkg
Hypercapnia
/
\
Chest physical therapy Incentive spirometry to minimize ongoing atelectasis
lntubate electively for positive pressure ventilation; several high-volume breaths per minute
Sigh lost-atelectasis and shunting
Hypoventilation
\ \
5 mVkg
\
Positive pressure ventilation to aid Cop exchange and prevent fatigue (IMV) Full ventilation
\
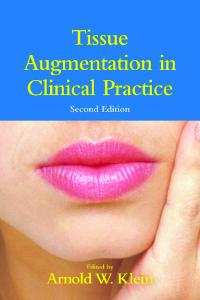
FIG. 13-5. Relationship between vital capacity, pathophysiology of lung function, and suggested therapy in respiratoly failure. (From Ropper AH: Neurological and Neurosurgical Intensive Care. 3rd Ed. Raven Press, New York, 1993, with permission.)
Chapter 14 W Autonomic Dysfunction
progression of diaphragm weakness to the point that the VC is less than 15 mL/kg, respiratory failure with hypoxemia and hypercapnia often occurs and may culminate in stupor and coma if untreated. With such a decline in the VC, paradoxic respirations may develop such that the abdomen moves inward instead of outward as the rib cage expands. If intercostal (expiratory) muscle weakness is also present, the rib cage may move inward instead of outward as the abdomen expands. Based on the VC and associated respiratory pathophysiology, Ropper (1993) has devised an approach to respiratory management that applies to all patients with neurogenic respiratory dysfunction (Fig. 13-5). In general, tracheal intubation is undertaken when mechanical ventilation is needed or when airway protection is desired to prevent aspiration. In patients with worsening neuromuscular respiratory muscle weakness, tracheal intubation usually should be performed before significant hypercapnia occurs. In addition, use of paralytic agents should be minimized. If anesthetics are used in patients with certain myopathies, such as myotonic dystrophy, one should be vigilant for the possible development of malignant hyperthermia. Chronic Management
Patients with chronic neurologic disorders that cause respiratory muscle weakness need good pulmonary toilet with postural drainage and chest physiotherapy. They may benefit from incentive inspiratory spirometry. Preventive care is also paramount. If they are bed-bound, patients should be turned frequently and have pressure points padded, and they should receive prophylaxis for venous thrombosis. Good nutrition and mobilization with physical and occupational therapy are important. Patients should receive influenza and pneumococcal vaccinations. Underlying pulmonary and neurologic diseases and intercurrent illnesses should be treated aggressively. Alveolar hypoventilation may be treated with supplemental oxygen, but positive-pressure mechanical ventilation via tracheostomy may be necessary to prevent hypercapnia. Some patients may need only intermittent ventilation. In lieu of tracheostomy, these patients who need only intermittent ventilation may benefit from intermittent positive-pressure ventilation delivered by nasal or oral mask, especially at night. This technique allows respiratory muscles to rest and improves ventilatory performance in some patients. Oxygen saturation, hypercapnia, and symptoms of hypoventilation may all improve. These patients may also benefit from negative-pressure (cuirass) ventilation. Finally, in some
14
145
patients with chronic central neurogenic hypoventilation, phrenic nerve pacing may be considered. ACKNOWLEDGMENTS
I appreciate the careful and thoughtful reviews of the manuscript by David Chad (Neurology Department, University of Massachusetts Medical Center) and Ronald Stiller (Pulmonary and Critical Care Medicine, University of Pittsburgh Medical Center).
SUGGESTED READINGS Bach JR, Alba AS: Management of chronic alveolar hypoventilation by nasal ventilation. Chest 97:53-57, 1990 Bolton CF: AAEM minimonograph #40: clinical neurophysiology of the respiratory system. Muscle Nerve 16809-818, 1993 Burki N: Measurements of ventilatory regulation. Clin Chest Med 10215-226, 1989 Demerits M, Beckers J, Rochette F, Bulcke J: Pulmonary function in moderate neuromuscular disease without respiratory complaints. Eur J Respir Dis 63:6247, 1982 Eichacker PQ, Spiro A, Sherman M et al: Respiratory muscle dysfunction in hereditary motor sensory neuropathy, type I. Arch Intern Med 148:1739-1740, 1988 Fostad H, Nilsson S: Intractable singultus: a diagnostic and therapeutic challenge. Br J Neurosurg 7:255-262, 1993 Griggs RC, Donohoe KM, Utell MJ et al: Evaluation of pulmonary function in neuromuscular disease. Arch Neurol 38:9-12, 1981 Haddad GG, Mazza NM, Defendini R et ak Congenital failure of autonomic control of ventilation, gastrointestinal motility and heart rate. Medicine (Baltimore) 57:517-524, 1978 Kelly BJ, Luce JM: The diagnosis and management of neuromuscular diseases causing respiratory failure. Chest 99:1485-1494, 1991 Plum F, Posner J B The Diagnosis of Stupor and Coma. 3rd Ed. FA Davis, Philadelphia, 1982 Pokey MI, LyaU RA, Moxham J, Leigh P N Respiratory aspects of neurological disease. J Neurol Neurosurg Psychiatry 665-15, 1999 Ropper AH: Neurologicaland Neurosurgical Intensive Care. 3rd Ed. Raven Press, New York, 1993 Vincken W, Elleker G, Cosio M G Detection of upper airway muscle involvement in neuromuscular disorders using the flow-volume loop. Chest 90:52-57, 1986 Vincken W, Elleker G, Cosio M G Determinants of respiratory muscle weakness in stable chronic neuromuscular disease. Am J Med 82:53-58, 1987 Wijdicks EFM, Bore1 CO: Respiratory management in acute neurologic illness. Neurology 5O:ll-20, 1998
Autonomic Dvsfunction Roy Freeman
The extensive afferent and efferent connections of the autonomic nervous system provide the anatomic basis for the diverse constellation of symptoms that accompany the autonomic degenerative diseases. This chapter covers the common diseases of the autonomic nervous system, the pathophysiology of dysautonomia, and the treatment of the features of autonomic dysfunction that are most frequently encountered by the practicing neurologist:
orthostatic hypotension, bladder dysfunction, and the disorders of gastrointestinal motility. DISEASES OF THE AUTONOMIC NERVOUS SYSTEM A wide variety of disorders may produce the signs and symptoms of autonomic dysfunction. Careful history taking and physical
Chapter 14 W Autonomic Dysfunction
progression of diaphragm weakness to the point that the VC is less than 15 mL/kg, respiratory failure with hypoxemia and hypercapnia often occurs and may culminate in stupor and coma if untreated. With such a decline in the VC, paradoxic respirations may develop such that the abdomen moves inward instead of outward as the rib cage expands. If intercostal (expiratory) muscle weakness is also present, the rib cage may move inward instead of outward as the abdomen expands. Based on the VC and associated respiratory pathophysiology, Ropper (1993) has devised an approach to respiratory management that applies to all patients with neurogenic respiratory dysfunction (Fig. 13-5). In general, tracheal intubation is undertaken when mechanical ventilation is needed or when airway protection is desired to prevent aspiration. In patients with worsening neuromuscular respiratory muscle weakness, tracheal intubation usually should be performed before significant hypercapnia occurs. In addition, use of paralytic agents should be minimized. If anesthetics are used in patients with certain myopathies, such as myotonic dystrophy, one should be vigilant for the possible development of malignant hyperthermia. Chronic Management
Patients with chronic neurologic disorders that cause respiratory muscle weakness need good pulmonary toilet with postural drainage and chest physiotherapy. They may benefit from incentive inspiratory spirometry. Preventive care is also paramount. If they are bed-bound, patients should be turned frequently and have pressure points padded, and they should receive prophylaxis for venous thrombosis. Good nutrition and mobilization with physical and occupational therapy are important. Patients should receive influenza and pneumococcal vaccinations. Underlying pulmonary and neurologic diseases and intercurrent illnesses should be treated aggressively. Alveolar hypoventilation may be treated with supplemental oxygen, but positive-pressure mechanical ventilation via tracheostomy may be necessary to prevent hypercapnia. Some patients may need only intermittent ventilation. In lieu of tracheostomy, these patients who need only intermittent ventilation may benefit from intermittent positive-pressure ventilation delivered by nasal or oral mask, especially at night. This technique allows respiratory muscles to rest and improves ventilatory performance in some patients. Oxygen saturation, hypercapnia, and symptoms of hypoventilation may all improve. These patients may also benefit from negative-pressure (cuirass) ventilation. Finally, in some
14
145
patients with chronic central neurogenic hypoventilation, phrenic nerve pacing may be considered. ACKNOWLEDGMENTS
I appreciate the careful and thoughtful reviews of the manuscript by David Chad (Neurology Department, University of Massachusetts Medical Center) and Ronald Stiller (Pulmonary and Critical Care Medicine, University of Pittsburgh Medical Center).
SUGGESTED READINGS Bach JR, Alba AS: Management of chronic alveolar hypoventilation by nasal ventilation. Chest 97:53-57, 1990 Bolton CF: AAEM minimonograph #40: clinical neurophysiology of the respiratory system. Muscle Nerve 16809-818, 1993 Burki N: Measurements of ventilatory regulation. Clin Chest Med 10215-226, 1989 Demerits M, Beckers J, Rochette F, Bulcke J: Pulmonary function in moderate neuromuscular disease without respiratory complaints. Eur J Respir Dis 63:6247, 1982 Eichacker PQ, Spiro A, Sherman M et al: Respiratory muscle dysfunction in hereditary motor sensory neuropathy, type I. Arch Intern Med 148:1739-1740, 1988 Fostad H, Nilsson S: Intractable singultus: a diagnostic and therapeutic challenge. Br J Neurosurg 7:255-262, 1993 Griggs RC, Donohoe KM, Utell MJ et al: Evaluation of pulmonary function in neuromuscular disease. Arch Neurol 38:9-12, 1981 Haddad GG, Mazza NM, Defendini R et ak Congenital failure of autonomic control of ventilation, gastrointestinal motility and heart rate. Medicine (Baltimore) 57:517-524, 1978 Kelly BJ, Luce JM: The diagnosis and management of neuromuscular diseases causing respiratory failure. Chest 99:1485-1494, 1991 Plum F, Posner J B The Diagnosis of Stupor and Coma. 3rd Ed. FA Davis, Philadelphia, 1982 Pokey MI, LyaU RA, Moxham J, Leigh P N Respiratory aspects of neurological disease. J Neurol Neurosurg Psychiatry 665-15, 1999 Ropper AH: Neurologicaland Neurosurgical Intensive Care. 3rd Ed. Raven Press, New York, 1993 Vincken W, Elleker G, Cosio M G Detection of upper airway muscle involvement in neuromuscular disorders using the flow-volume loop. Chest 90:52-57, 1986 Vincken W, Elleker G, Cosio M G Determinants of respiratory muscle weakness in stable chronic neuromuscular disease. Am J Med 82:53-58, 1987 Wijdicks EFM, Bore1 CO: Respiratory management in acute neurologic illness. Neurology 5O:ll-20, 1998
Autonomic Dvsfunction Roy Freeman
The extensive afferent and efferent connections of the autonomic nervous system provide the anatomic basis for the diverse constellation of symptoms that accompany the autonomic degenerative diseases. This chapter covers the common diseases of the autonomic nervous system, the pathophysiology of dysautonomia, and the treatment of the features of autonomic dysfunction that are most frequently encountered by the practicing neurologist:
orthostatic hypotension, bladder dysfunction, and the disorders of gastrointestinal motility. DISEASES OF THE AUTONOMIC NERVOUS SYSTEM A wide variety of disorders may produce the signs and symptoms of autonomic dysfunction. Careful history taking and physical
146
Principles of Ambulatory Neurology and the Approach to Clinical Problems
rn TABU 14-1. Autonomic Dysfunction with Central Nervous System Manifestations Multiple-system atrophy with autonomic failure (Shy-Drager syndrome) With cerebellar features (MSA-C, olivopontocerebellar atrophy) With extrapyramidal features (MSA-P, striatonigral degeneration) Parkinson’s disease Brain tumors (brainstem, cerebellum, diencephalon) Wernicke’s disease Multiple cerebral infarcts Syringomyelia and syringobulbia Hydrocephalus Multiple sclerosis Myelopathies Traumatic Inflammatory Pernicious anemia System degenerative Tabes dorsalis Progressive supranuclear palsy Huntington‘s disease Amyotrophic lateral sclerosis
examination with appropriate use of special investigations usually permit an accurate clinical diagnosis of these diseases. A useful practical approach is to classify the disorders associated with autonomic failure into diseases accompanied by predominantly central nervous system features, diseases accompanied by predominantly peripheral nervous system features, and diseases without neurologic features (Tables 14-1, 14-2, and 14-3).
Autonomic Dysfunction With Central Nervous System Features There are numerous disorders with autonomic manifestations and central necvous system signs. Of these diseases, multiple-system atrophy (MSA) with autonomic failure and idiopathic Parkinson’s disease most often produce clinically significant autonomic dysfunction. MSA is a degenerative disorder of the central nervous system that affects extrapyramidal (striatonigral degeneration), cerebellar (olivopontocerebellar atrophy), and autonomic neurons. Patients with MSA typically present with autonomic symptoms such as orthostatic hypotension, bowel and bladder dysfunction, anhidrosis, and impotence, together with motor dysfunction that can involve the extrapyramidal, cerebellar, and pyramidal systems. Impotence in men, urinary incontinence, and orthostatic hypotension are the most common symptoms of MSA. The symptoms of orthostatic hypotension usually lead patients to seek medical attention. In contradistinction to idiopathic Parkinson’s disease, MSA is more likely to have a symmetrical onset and is less responsive to levodopa and dopamine agonists. The resting Parkinsonian tremor is rarely present in MSA, whereas inspiratory stridor, vocal cord paralysis, and antecollis commonly occur. Initial rigidity and early motor fluctuations in response to therapy are also more common in patients with MSA. The median survival of MSA usually is less than 10 years, although exceptions occur. Pathologic studies have demonstrated cell loss and gliosis that include the striatonigral, olivopontocerebellar, and autonomic systems. An argyrophilic, filamentous, intracytoplasmic oligodendroglial inclusion is a specific histopathologic hallmark of MSA. These inclusions are also present in the nuclei of other glial cells and neurons. Several recent reports have indicated that these filamentous inclusions are immunoreactive for a-synuclein, suggesting that MSA and the
Principles of Diagnosis: Common Presenting Symptoms
rn TABLE14-2. Autonomic Dysfunction with Peripheral Nervous System Manifestations Diabetes Amyloidosis Cuillain-Barre syndrome Acute and subacute autonomic neuropathies Chronic inflammatory polyneuropathy Hereditary neuropathies Hereditary sensory and autonomic neuropathies Fabry‘s disease Navajo Indian neuropath Hereditary motor and sensory neuropathy Tangier disease Infectious diseases Chagas’s disease Human immunodeficiencyvirus neuropathy Botulism Diphtheria Leprosy Toxic neuropathies Vacor Vincristine Perhexiline maleate cis-Platinum Taxol Organic solvents Acrylamide Heavy metals Connective tissue diseases Sjogren‘s syndrome Systemic lupus erythematosus Rheumatoid arthritis Pernicious anemia Porphyria Uremia Alcoholic neuropathy Hepatic disease Paraneoplastic neuropathies Lambert-Eaton syndrome Dopamine P-hydroxylase deficiency Adie’s syndrome
rn TABLE14-3. Isolated Autonomic Dysfunction Pure autonomic failure Medications Antihypertensive agents Tricyclic agents Monoamine oxidase inhibitors Dopamine blocking agents Aging Endocrine diseases Adrenocortical deficiency Pheochromocytoma Surgical sympathectomy Mitral valve prolapse Hypovolemia Electrolyte disturbance Hyperbradykinism
Lewy body disorders, Parkinson’s disease, and Lewy body dementia have a common underling neuropathologic characteristic. The autonomic symptoms accompanying Parkinson’s disease usually are not as severe as those seen in patients with MSA. They characteristically occur late in the course of the illness and often are associated with levodopa and dopamine agonist therapy. Nevertheless, autonomic dysfunction often is the source of significant morbidity for the patient with Parkinson’s disease. There are many other disorders with autonomic dysfunction and central nervous system signs, but the autonomic symptoms usually are of secondary importance, and these disorders are unlikely to be confused with MSA or Parkinson’s disease (Table 14-1).
Chapter 14 H Autonomic Dysfunction
Autonomic Dysfunction with Peripheral Nervous System Features
Autonomic dysfunction occurs with most peripheral neuropathies, particularly those that predominantly involve the small or unmyelinated fibers. This review covers those peripheral neuropathies in which autonomic dysfunction is a clinically significant manifestation. A complete list of peripheral neuropathies with autonomic manifestations is found in Table 14-2. Diabetes Mellitus. Diabetes mellitus is the most common cause of autonomic neuropathy in the developed world. A constellation of signs and symptoms of cardiovascular, gastrointestinal, urogenital, thermoregulatory,sudomotor, and pupillomotor dysfunction occur. An increased resting heart rate is often observed in diabetic patients. With progression of the autonomic neuropathy, some patients display a fixed heart rate that responds only minimally to physiologic stimuli. The initial tachycardia is caused by a vagal cardiac neuropathy. The resting tachycardia may be followed by a decrease in heart rate and ultimately a fixed heart rate caused by progressive cardiac sympathetic nervous system dysfunction. Orthostatic hypotension occurs in diabetes as a consequence of efferent sympathetic vasomotor denervation, causing reduced vasoconstriction of the splanchnic and other peripheral vascular beds. There is an increased frequency of sudden death in patients with autonomic neuropathy. Proposed causes for sudden unexplained death in diabetics have included cardiorespiratory arrest caused by cardiac arrhythmias, silent cardiac ischemia, and sleep apnea. Bladder symptoms associated with autonomic neuropathy include hesitancy, poor stream, increased intervals between micturition, and a sense of inadequate bladder emptying. These symptoms may be followed by urinary retention and overflow incontinence. Detrusor muscle sensory abnormalities are the earliest bladder autonomic manifestation. These sensory abnormalities impair bladder sensation and increase the threshold for initiating the micturition reflex. A decrease in detrusor activity (detrusor areflexia) follows that leads to incomplete bladder emptying, an increased postvoid residual volume, decreased peak urinary flow rate, bladder overdistention, and ultimately urinary retention. Impotence is a common symptom in diabetic men. Reported incidence has ranged from 30% to 75% of diabetic men. Impotence may be the earliest symptom of diabetic autonomic neuropathy, although sensory, vascular, and psychogenic causes, alone or in varying combinations, also may be responsible for this symptom. Sympathetically mediated ejaculatory failure may precede the appearance of impotence, although impotence can occur with retained ability to ejaculate and experience orgasm. Autonomic dysfunction occurs throughout the gastrointestinal tract, producing several specific clinical syndromes. Diabetic gastroparesis may manifest as nausea, postprandial vomiting, bloating, belching, loss of appetite, and early satiety. Food residue is retained in the stomach because of impaired gastric peristalsis compounded by lower intestinal dysmotility. Gastroparesis often impairs the establishment of adequate glycemic control. Denervation of the vagus nerve may play a role in this disorder. Constipation is the most commonly reported gastrointestinal autonomic symptom and is found in up to 60% of diabetics. The pathophysiologyof diabetic constipation is poorly understood but may reflect loss of the postprandial gastrocolicreflex. Diarrhea and other lower gastrointestinal tract symptoms may also occur. Diabetic diarrhea is profuse and watery and typically occurs at
147
night. The diarrhea can last for hours or days and often alternates with constipation. Fecal incontinence, caused by anal sphincter incompetence or reduced rectal sensation, is another manifestation of diabetic autonomic neuropathy. The pathogenesis of diabetic diarrhea includes abnormalities in gastrointestinal motility, decreased gut transit time, reduced a2-adrenergic receptormediated fluid absorption, bacterial overgrowth, pancreatic insufficiency, coexistent celiac disease, and abnormalities in bile salt metabolism. Diabetic autonomic neuropathy initially results in a loss of thermoregulatory sweating in a stocking-glove distribution that can extend to the upper aspects of the limbs and anterior abdomen, conforming to the well-recognized length dependency of diabetic neuropathy. This process ultimately results in global anhidrosis that usually accompanies a profound generalized autonomic neuropathy. Hyperhidrosis also may accompany diabetic autonomic neuropathy. Excessive sweating may occur as a compensatory phenomenon involving proximal regions such as the head and trunk that are spared in a dying-back neuropathy. Gustatory sweating, an abnormal production of sweating that appears over the face, head, neck, shoulders, and chest after eating even nonspicy foods, is occasionally observed. Amyloid Neuropathy. Autonomic dysfunction often accompanies the polyneuropathy of both primary and familial amyloidosis. Autonomic dysfunction is not common in myelomaassociated amyloidosis. Patients with amyloid neuropathy typically present with distal sensory symptoms such as numbness, paresthesias, and dysesthesias, although the autonomic manifestations occasionally may be the presenting feature of amyloid neuropathy. On examination there are signs of a sensorimotor polyneuropathy that predominantly involves the small fibers that mediate pain and temperature sensation. Characteristic autonomic signs and symptoms include postural hypotension, diarrhea, constipation, fecal incontinence, disturbances in bladder function, pupillary abnormalities, and erectile failure. These autonomic manifestations are similar to those described for diabetic autonomic neuropathy. Sick sinus syndrome and AV conduction deficits often are present. Tests assessing cardiac vagal function often are abnormal. The variant transthyretin, in which methionine substitutes for valine at position 30, is the point mutation that is the most common cause of familial amyloid polyneuropathy in the United States. Other transthyretin mutations and mutations in apolipoprotein A-I and gelsolin also give rise to familial amyloid polyneuropathy. Primary amyloidosis (AL. amyloidosis) is characterized by the deposition of insoluble fibrillar proteins in the extracellular space of various tissues and organs. Peripheral neuropathy, which may be the presenting feature of the disease or an incidental finding, is present in up to 20% of patients with AL. Cardiovascular, gastrointestinal, and urogenital system autonomic dysfunction are common. Proposed mechanisms of injury include pressure exerted by amyloid deposits on peripheral nerves, dorsal nerve root ganglia, or autonomic ganglia and ischemic damage caused by amyloid infiltration of epineural and intraneural blood vessel walls. Acute and Subacute Autonomic Neuropathies. Autonomic manifestations usually accompany the Guillain-Bar& syndrome, although they are usually overshadowed by motor features of that disorder. However, autonomic manifestations may be the sole or predominant feature of an acute or subacute peripheral neuropathy. The hallmark of these autonomic neuropathies is the acute or subacute presentation of varying combinations of orthostatic
148
Principles of Ambulatory Neurology and the Approach to Clinical Problems W
hypotension, constipation, bladder atony, impotence, secretomotor paralysis, and blurring of vision associated with tonic pupils. Sensorimotor manifestations may accompany the autonomic manifestations but are not the predominant aspect of the presentation. The autonomic manifestations of this disorder may involve both the sympathetic and parasympathetic divisions of the autonomic nervous system (pandysautonomia) or the parasympathetic nervous system alone (cholinergic dysautonomia). Only 40% of patients recover fully to premorbid status. For an estimated 12%, symptoms persist to a significant degree. Full or partial recovery, when reported, occurs over the course of months to years. Autonomic testing in the recovery phase of illness in these patients often shows evidence of persisting subclinical autonomic dysfunction. Acute dysautonomia has been described in relation to the Epstein-Barr virus, streptococcal infection, and herpes simplex infection, in addition to other undiagnosed viral syndromes. Associations with malignancies and connective tissue diseases have been described in other cases. Immune-Mediated Autonomic Neuropathies. Autonomic dysfunction has been associated with the presence of specific autoantibodies. The subacute appearance of autonomic symptoms that include orthostatic hypotension, pupillomotor dysfunction, sudomotor dysfunction, constipation, urinary retention, impotence, and xerophthalmia has been associated with the presence of anti-Hu antibodies in patients with malignancies, especially small cell lung cancer. These antibodies also are found in patients with a paraneoplastic sensory neuronopathy and encephalomyelitis. In one large series, the autonomic nervous system was involved in 28% of patients with anti-Hu antibodies and was the predominant symptom in a third of these patients. Dysautonomia may be an isolated manifestation of a paraneoplastic disorder or part of a generalized paraneoplastic syndrome. For example, paraneoplastic constipation and intestinal pseudoobstruction have been associated with small cell carcinoma of the lung. Such patients have inflammatory infiltrates of the myenteric plexus of the stomach and antineuronal antibodies. Autonomic neuropathies have been documented in case reports in association with pancreatic carcinoma, Hodgkin’s disease, and testicular cancer. Dysautonomia is a common manifestation of the LambertEaton syndrome in patients with and without malignancies. Symptoms suggesting cholinergic dysfunction, such as dry mouth, erectile and ejaculatory failure, constipation, blurred vision, and impaired sweating, are most common. Autonomic tests, demonstrating unresponsive pupils that constrict to dilute pilocarpine, reduced sweating, and salivary and lacrimal secretomotor failure suggest that the abnormality is predominantly limited to the parasympathetic nervous system, although mild sympathetic nervous system abnormalities may be present. Autonomic tests have demonstrated both cholinergic and adrenergic abnormalities. Autonomic features associated with the Lambert-Eaton syndrome have been associated with seropositivity for P/Q-type Ca2+ channel antibodies. High levels of autoantibodies specific for nicotinic acetylcholine receptors in the autonomic ganglia also have been found in patients with idiopathic and paraneoplastic autonomic neuropathy. Characteristic clinical features in these patients included a subacute onset, gastrointestinal dysmotility, and abnormal pupillary responses to light and accommodation. A positive correlation between high levels of ganglionic receptor antibodies and the severity of autonomic dysfunction exists, suggesting that the antibodies may have a pathogenic role in these autonomic neuropathies.
Principles of Diagnosis: Common Presenting Symptoms
Hereditary Autonomic Neuropathies. The hereditary autonomic neuropathies are a heterogeneous group of disorders, some of which cause significant involvement of autonomic fibers. A list is provided in Table 14-2. The hereditary sensory and autonomic neuropathies (HSAN) are characterized by prominent sensory loss without motor involvement and by often striking dysautonomia. The autonomic manifestations are modest in autosomal dominant sensory neuropathy (HSAN type I) and autosomal recessive sensory neuropathy (HSAN type 11), with the possible exception of bladder dysfunction. These disorders are associated with severe sensory loss with acral injuries. Autonomic manifestations are prominent in HSAN type 111, or Riley-Day syndrome (familial dysautonomia, FD) . This autosomal recessive disorder is seen primarily in Ashkenazi Jewish children. The incidence of FD is 1 in 3700 live births among Ashkenazi Jews, and the carrier frequency is 1 in 32. The defective gene causing familial dysautonomia has been mapped to the long arm of chromosome 9 (9q31). The majority (99.5%) of patients with FD have a single noncoding mutation in the gene IKBKAE! The clinical features of this disease include insensitivity to pain and temperature but sparing visceral pain, absence of tears, hypoactive corneal and tendon reflexes, and absence of fungiform papillae. Poor suck and feeding, esophageal reflux with vomiting and aspiration, and a dyscoordinated swallow may be the first clinical manifestations. Later in the course of the illness, vibratory sensory loss and impaired appendicular coordination manifest. Autonomic disturbances may be prominent at any point in the disease course. Autonomic manifestations include episodic hyperhidrosis, vasomotor instability with defective temperature homeostasis, postural hypotension, hypertensive crises, and supersensitivity to cholinergic and adrenergic agents. Orthostatic hypotension often is present. Congenital insensitivity to pain with anhidrosis (anhidrotic sensory neuropathy) is a disorder with autosomal recessive inheritance (HSAN type IV). It manifests in the first months of life with insensitivity to pain, anhidrosis, episodes of unexplained fever, and retardation of motor development. Virtual absence of unmyelinated fibers has been noted in peripheral nerves. Deletion, splice, and missense mutations have been documented in the tyrosine kinase domain of the TRK A/NGF receptor gene in patients with this disorder. Fabry’s disease, or angiokeratoma corporis diffusum, is an X-linked, recessively inherited disorder that is associated with deficiency of the enzyme a-galactosidase A (ceramide trihexosidase). The enzyme deficiency results in the accumulation of ceramide trihexoside and other neutral glycosphingolipids in homozygotes. There is extensive lipid deposition in various tissues that include the skin, nervous system, vascular endothelium, kidney, cardiovascular system, and eye. The neurologic manifestations of this disorder are secondary to the deposition of glycolipid in autonomic and dorsal root ganglia, in perineurial cells, and in unmyelinated and myelinated axons. Young males with this disorder typically present with severe distal extremity paroxysmal pains and tenderness, a truncal reddish-purple macular papular rash, and angiectases of the skin, conjunctiva, nail bed, and oral mucosa. The autonomic manifestations include hypohidrosis or anhidrosis, reduced saliva and tear formation, impaired cutaneous flare response to scratch and histamine, and disordered intestinal motility. Patients’ gastrointestinal symptoms may be as severe as their sensory complaints. Pupillary constriction to dilute pilocarpine has been documented, suggesting denervation supersensitivity, although cardiovascular autonomic reflexes in one series were
Chapter 14
normal. The generalized presentation of the anhidrosis has suggested sweat gland dysfunction that may be caused by intracytoplasmic inclusions in the eccrine glands rather than autonomic neuropathy as a mechanism for the anhidrosis. Neuropathologic studies have demonstrated degeneration and loss of unmyelinated fibers. Fabry’s disease can be diagnosed by assaying the enzyme a-galactosidase A in leukocytes or skin fibroblasts. Infectious Diseases. The peripheral neuropathies associated with a number of infectious diseases have accompanying autonomic manifestations. Autonomic dysfunction may occur in patients with human immunodeficiency virus infection. The symptoms of dysautonomia have included orthostatic hypotension, syncope, presyncope, sweating disturbances, bladder and bowel dysfunction, and impotence. There is an increasing incidence of Chagas’s disease in the United States, and the autonomic manifestations of this disease should be considered in the differential diagnosis of dysautonomia. Chagas’s disease, which is caused by a parasitic infection by TTypanosoma auzi, is associated in the late stages of illness with severe cardiovascular and gastrointestinal dysautonomia. The pathogenesis of the autonomic dysfunction is unresolved and may be caused by direct neural injury during the acute illness or a persisting immune-mediated response. Reduced bowel motility, sialorrhea, megaesophagus, and megacolon are the most common gastrointestinal manifestations of this disease. Cardiovascular manifestations include impairment in the blood pressure response to standing, resting bradycardia, anhidrosis, conduction abnormalities, arrhythmias, cardiac failure, and cardiomegaly. Isolated Autonomic Nervous System Dysfunction Pure autonomic failure (PAF) is an idiopathic peripheral autonomic nervous system degeneration that, in contrast to ShyDrager syndrome, has no motor manifestations. There are also no signs or minimal signs of a somatic peripheral neuropathy. Because this disorder is slowly progressive and has a significantly better prognosis than Shy-Drager syndrome, it is important to differentiate between these two disorders. The autonomic features of Shy-Drager syndrome may precede the other neurologic signs by several years, preventing an early definitive diagnosis. Patients with PAF typically have a low resting plasma norepinephrine level caused by degeneration or dysfunction of the postganglionic sympathetic neuron. The plasma norepinephrine level, which in normal subjects increases by 100% to 200% when moving from the supine to the upright position, does not change significantlyin patients with PAF. However, there is a wide scatter of results within the group of patients with PAF that often makes it difficult to classify individual patients. Cardiovascular autonomic tests show impairment with a severity that is equivalent to that seen in patients with MSA. Lewy bodies have been observed in distal axons. Accumulation of a-synuclein in affected neurons has been documented in cases of pure autonomic failure. Other conditions with isolated autonomic manifestations are listed in Table 14-3.
SIGNS, SYMPTOMS, AND TREATMENT OF AUTONOMIC FAILURE Orthostatic Hypotension The assumption of the upright posture results in a complex sequence of physiologic reactions in response to the pooling of approximately 500 cc of blood in the lower extremities and splanchnic circulation. There is a decrease in venous return to the
Autonomic Dysfunction
149
heart, and the reduced ventricular filling results in diminished cardiac output and blood pressure. These hemodynamic changes provoke a baroreceptor-initiated compensatory reflex mediated via the central nervous system and effected by the peripheral efferent autonomic outflow. These compensatory mechanisms increase peripheral resistance, venous return, and cardiac output and thus limit the fall in blood pressure. The normal response to the assumption of the erect posture is a fall in systolic blood pressure (5 to 10 mm Hg), an increase in diastolic blood pressure (5 to 10 mm Hg), and an increase in the pulse rate (10 to 25 beats per minute). Should these mechanisms fail, the symptoms of cerebral hypoperfusion ensue. The hallmark of neurogenic orthostatic hypotension from both central and peripheral causes is the failure to release norepinephrine appropriately upon standing. Normally norepinephrine is released into the synaptic cleft in response to standing, resulting in a twofold to threefold increase in plasma norepinephrine. Treatment of Orthostatic Hypotension. Patient education is the cornerstone of the management of orthostatic hypotension. Patients with orthostatic hypotension should move from a supine to standing position in gradual stages, particularly in the morning, when orthostatic tolerance is lowest. Maneuvers such as straining, coughing, and raising the arms above the head should be avoided. The removal of potential reversible causes of orthostatic hypotension is the first and most important management step. Medications such as diuretics, antihypertensive agents, antianginal agents, and antidepressants are the most common offending agents. The excessive natriuresis and reduction in central blood volume can be attenuated or minimized by increasing sodium intake with high-sodium foods or salt tablets. Raising the head of the bed 10 to 20 degrees activates the renin-angiotensin-aldosterone system and decreases the nocturnal diuresis. Raising the head of the bed TAM 14-4. Pharmacologic Agents Used to Treat Orthostatic Hypotension Mineralocorticoids 9-a-fludrocortisone Syrnpathomimetic agents Ephedrine Pseudoephedrine Phenylephrine Methylphenidate Dextroamphetamine Tyramine (with monamine oxidase inhibition) Midodrine Clonidine Yohimbine DL- and 1-dihydroxyphenylserine Nonspecific pressor agents Ergot derivatives Caffeine Somatostatin analogues p-Adrenergic blocking agents Propranolol Pindolol Xamoterol Prenalterol Prostaglandin synthetase inhibitors lndomethacin flurbiprofen Ibuprofen Naproxen Dopamine blocking agents Metoclopramide Domperidone V1 and V2 receptor agonists Desmopressin acetate Lysine-vasopressin ErvthroDoietin
150
Principles of Ambulatory Neurology and the Approach to Clinical Problems rn Principles of Diagnosis:Common Presenting Symptoms
may also reduce the supine hypertension that is prevalent in these patients, either as a consequence of baroreceptor denervation or as a side effect of treatment. Severe supine hypertension often limits therapeutic intervention, although surprisingly, most patients tolerate sustained supine blood pressures without untoward effect. The use of custom-fitted elastic stockings permits the application of a graded pressure to the lower extremity and abdomen. These stockings minimize peripheral blood pooling in the lower extremities and splanchnic circulation. Unfortunately, nonpharmacologic measures help only the mildly afflicted, and pharmacologic intervention usually is needed. Numerous agents from diverse pharmacologic groups have been implemented in treating orthostatic hypotension (Table 14-4). The therapeutic goal is merely to ameliorate all symptoms while minimizing side effects. There is rarely the need to restore normotension. The most effective pharmacologic measures include mineralocorticoids, direct and indirect sympathomimetic agents, other pressors, prostaglandin synthesis inhibitors, and recently reported erythropoietin. 9-a-Fluorohydrocortisone (fludrocortisone acetate), a synthetic mineralocorticoid, is the medication of first choice for most patients with orthostatic hypotension. This agent has a long duration of action and may be taken once or twice daily. Fludrocortisone increases the blood volume and may enhance the sensitivity of blood vessels to circulating catecholamines. Treatment is initiated with a 0.1-mg tablet and can be increased to 1 mg daily, although little benefit is obtained by increasing beyond 0.5 mg. Unfortunately, treatment may be limited by supine hypertension caused by an increase in the peripheral vascular resistance. Other side effects include ankle edema, hypokalemia, and rarely congestive heart failure. Potassium supplementation usually is needed, particularly when higher dosages are used. Direct and indirect sympathomimetic agents have a long history of use in treating orthostatic hypotension. Commonly used a,-adrenoreceptor agonists include those with direct and indirect effects (ephedrine and pseudoephedrine), those with direct effects (midodrine), and those with only indirect effects (methylphenidate and dextroamphetamine sulphate). These agents, with the exception of midodrine, cross the blood-brain barrier, and central sympathomimetic side effects such as anxiety, tremulousness, tachycardia, and supine hypertension may occur. The peripheral a-agonist midodrine, which has received U.S. Food and Drug Administration approval for treating orthostatic hypotension, does not cross the blood-brain barrier, thereby avoiding the central sympathomimetic side effects. Potential side effects of this agent include pilomotor reactions and pruritus. Most patients respond to the interventions described earlier. A more complete list of medications used to treat orthostatic hypotension is presented in Table 14-4. Autonomic Dysfunction of the Urinary Bladder
The bladder wall is composed of three layers of interdigitating smooth muscle and serves as a receptacle for the storage and appropriate evacuation of urine. This smooth muscle (the detrusor muscle) forms the internal sphincter at the junction of the bladder neck and urethra. The bladder has parasympathetic, sympathetic, and somatic innervation. The parasympathetic nerves originate in the intermediolateral column of the second, third, and fourth sacral segments of the spinal cord and provide the major excitatory input to the urinary bladder. Activation of these muscarinic, cholinergic, postganglionic nerves produces detrusor muscle contraction.
TABLE 14-5. Classification of Bladder Dysfunction Detrusor hyperreflexia (or normoreflexia) Coordinated sphincters Striated sphincter dyssynergia Smooth muscle sphincter dyssynergia Nonrelaxing smooth muscle sphincter Detrusor areflexia Coordinated sphincter Nonrelaxing striated sphincter Denervated striated sphincter Nonrelaxingsmooth muscle sphincter
The sympathetic nerve supply to the bladder originates in the intermediolateral column of spinal segments T10-L2 and passes through the sympathetic ganglia to reach the hypogastric plexus via the splanchnic nerves. Postganglionic sympathetic neurons then innervate the dome of the bladder, producing inhibition via the P-adrenergic receptors of the detrusor muscle and excitation at the a-adrenergic receptors of the internal sphincter, bladder base, and urethra via the hypogastric nerves. The striated muscle of the external urethral sphincter is innervated by the pudendal nerves, which originate from the lateral anterior horn cells of the second, third, and fourth sacral segments, a region known as the sphincter motor nucleus or Onuf's nucleus. This sphincter is under voluntary control but undergoes reflex relaxation during micturition. Afferent fibers mediating bladder sensation and reflex bladder contraction are carried by sympathetic, parasympathetic, and somatic nerves to the spinal cord. The Treatment of Bladder Dysfunction. The innervation of the bladder provides the basis for understanding bladder autonomic dysfunction. There are several different schemas classifying voiding dysfunction. The classification of Krane and Siroky (1992; Table 14-5) incorporates a functional description of detrusor muscle and sphincter function and provides a logical basis for instituting therapy. Therapies directed at reducing bladder hyperreflexia and maintaining urinary continence may alternately decrease bladder contractility or increase bladder outlet resistance or use other means to bypass vesicular or sphincteric abnormalities. Therapies for bladder hypomotility, conversely, attempt to increase bladder contractility, decrease outlet resistance, or both. The nonpharmacologic interventions that include toileting regimens, Credk maneuver, intermittent catheterization, indwelling Foley catheterization, palliative or definitive surgical interventions, and biofeedback often are used in concert with medications. The patient's customized therapy is best pursued with the aid of urologic consultation. Individualized treatment regimens should be guided by the history, examination, urodynamic studies, and measurement of the postvoid residual volume. PHARMACOTHERAFY FOR BLADDER HYPERREFLEXIA. The pharmacotherapy for urinary incontinence caused by detrusor hyperreflexia attempts to decrease bladder contractility or increase outlet resistance. Atropine and associated antimuscarinic substances depress involuntary bladder contractions. The antimuscarinic agents oxybutynin (5 mg two to four times daily) and tolterodine (2 mg two times daily) are the agents most commonly used to treat bladder hyperreflexia. The antimuscarinic effects of tolterodine may be more specific to the bladder, and the anticholinergic side effects of this medication, particularly dry mouth, are reported to be less common than with oxybutynin. Extended-release formulations of these medications are available (oxybutynin 5 to 30 mg daily and tolterodine 4 mg daily). The medications that decrease bladder contractility may be used in conjunction with therapy increasing bladder outlet
Chapter 14
resistance. The bladder neck and proximal urethra are richly populated by a-adrenergic receptors, which, when stimulated, result in smooth muscle contraction. a-Adrenergic agonists are the principal agents used to increase bladder outlet resistance; ephedrine (25 to 50 mg four times per day), pseudoephedrine (30 to 60 mg four times per day), and others have been studied. Sympathomimetic side effects such as elevated blood pressure, anxiety, and insomnia may limit the dosage, and tachyphylaxis may develop. Sphincter characteristics during urodynamic studies may be helpful in guiding the use of these agents. Additional therapies are listed in Table 14-6. RIARMACOTHERAPY FOR BLADDER Hmmonm. Stimulation of muscarinic, postganglionic receptors results in enhanced bladder contractility. Bethanechol chloride is a parasympathomimetic drug with selective action at the urinary bladder. It is effective in chronic states of detrusor atony or hypotonicity, although it has also been used to facilitate reflex bladder contraction in patients with suprasacral cord injury. Typical oral dosages range from 25 to 100 mg four times daily. The cholinergic agonist carbachol chloride, which may have additional ganglion-stimulatingproperties, also may enhance bladder motility. These agents are of limited therapeutic benefit, and when the postvoiding residual volume is greater than 100 cc, clean intermittent self-catheterization should be considered. Autonomic Dysfunction of the GastrointestinalTrad
The autonomic control of the gastrointestinaltract is mediated by the extrinsic parasympathetic and sympathetic nervous systems and the intrinsic enteric nervous system. The parasympathetic input to the gut originates from the vagus and pelvic nerves from the second through fourth sacral segments. The postsynaptic cholinergic neurons provide excitatory input to the gastrointestinal tract. The sympathetic nervous system provides inhibitory input to the gastrointestinal tract. Extrinsic sympathetic efferents W
TABLE 14-6. Therapy of Bladder Hypermotility
Behavioral therapy Timed bladder emptying Biofeedback Catheterization and collecting devices Clean intermittent self-catheterization Urine collection devices Condom catheters indwelling catheters Incontinence briefs and pads Pharmacotherapy to inhibit bladder contractility Anticholinergic agents Smooth muscle relaxants Polysynaptic inhibitors Calcium channel antagonists P-Adrenergic agonists a-Adrenergic antagonists Prostaglandin synthetase inhibitors Tricyclic antidepressants Dimethyl sulfoxide Bromocriptine Pharrnacotherapy to increase outlet resistance PAdrenergic antagonists a-Adrenergic agonists Tricyclic antidepressants Estrogen Surgical therapy Denelvation procedures Augmentation cystoplasty Vesicourethral suspension Bladder outlet reconstruction Treatment of urinary tract infection Treatment of autonomic dysreflexia
Autonomic Dysfunction
151
TABLE 14-7. Pharmacotherapy of Bowel Hypomotility Bulk agents Bran Psyllium Methylcellulose Laxatives and cathartics Osmotic laxatives and cathartics Lactulose Sorbitol Magnesium salts Sodium phosphate Polyethylene glycol-saline solutions Glycerin suppositories Contact cathartics Diphenylmethane derivatives Phenolphthalein Bisacodyl tablets or suppositories Anthraquinone derivatives Senna Cascara Ricinoleic acid (castor oil) Stool softeners and lubricants Mineral oil Dulcosates Prokinetic agents Metoclopramide Domperidone Erythromycin Cholinomimetics Bethanechol Acetylcholinesterase inhibitors Opioid antagonists MisoDrostol
arise in the intermediolateral gray column synapse in the celiac, superior, and inferior mesenteric ganglia and ramify throughout the gastrointestinal tract in the distribution of their respective arterial trunks. The enteric nervous system is composed of a myenteric plexus located between the inner circular and outer longitudinal smooth muscle layers (Auerbach’s plexus) and a submucosal plexus (Meissner’s plexus). At least five types of intrinsic enteric neurons have been identified, and any individual neuron may contain multiple neuropeptides. Motor excitation is mediated by the cholinergic substance P neurons, and inhibition is mediated by the dynorphin vasoactive intestinal polypeptide neurons. Even in the absence of extrinsic autonomic nervous system influences, the enteric nervous system governs basic gut functions. Treating Bowel Hypomotility. An increase in dietary fiber (up to 25 @day), with water (10 oz four times per day) and exercise is the first line of therapy for most patients. The use of psyllium (up to 30 @day)or methylcellulose (up to 6g/day) with a concomitant increase in fluid intake further increases stool bulk. Some caution should be exercised with these agents; for example, high fiber may be disadvantageous in diabetic gastroparesis because of distention and cramping pain that can be associated with its use or because of the potential for bezoar formation. Stool softeners (e.g., docusate sodium 100 to 500 mg/day) or lubricants (e.g., mineral oil) together with an osmotic laxative (e.g., lactulose 15 to 60 mL/day) may be used if the aforementioned measures are ineffective. Glycerin suppositories or sodium phosphate enemas stimulate evacuation by promoting fluid retention in the rectum (Table 14-7). The contact cathartics such as the diphenylmethanederivatives (phenolphthalein and bisacodyl) and the anthraquinones (senna and cascara) should be used sparingly, although the use of these agents usually cannot be avoided in patients with constipation caused by autonomic failure. Extensive use of these agents may damage the myenteric plexus, producing cathartic bowel.
152
Principles of Ambulatory Neurology and the Approach to Clinical Problems W
Benzamide metoclopramide (5 to 20 mg orally, 30 minutes before meals and at bedtime) accelerates gastric emptying and has a central antiemetic action. In diabetics with concurrent gastroparesis and constipation, metoclopramide therapy may improve both symptoms, although its effect on colonic motility is less well defined, Tolerance to metoclopramide therapy has been described. Patients maintained in the long term on metoclopramide theoretically may be at risk for developing tardive dyskinesia and other dopamine antagonist-related side effects. Concurrent renal failure may increase risk of acute toxicity. Domperidone, a peripheral antidopaminergic agent, may provide symptomatic relief in patients with gastroparesis, although it is not clear that this medication improves objective measures of gastric emptying. Erythromycin and related macrolide compounds exhibit strong in vitro affinity for motilin receptors and have agonist properties that mimic the prokinetic action of exogenous motilin, a gastrointestinal polypeptide. Single intravenous doses of erythromycin shorten postprandial, gastric emptying time to normal levels in diabetics with gastroparesis. Oral erythromycin (250 mg three times per day) also improves gastric emptying, although not to the degree noted after a single parented administration. The somatostatin analogue octreotide may stimulate intestinal motor complexes, and this agent has been used to treat sclerodermatous pseudo-obstruction. However, somatostatin is known to impair motor responses to feeding, and treatment with octreotide in other conditions has been associated with hypomotility and bacterial overgrowth. Nausea and abdominal cramping pain occur with administration of the medication. Fat malabsorption and cholelithiasis have been described with chronic use. Rare patients who do not respond to medical therapy may need colonic surgery. Such patients should have documented slow colonic transit time and intact rectal sphincter function. Pharmacotherapy of Bowel Hypermotility. Before the diagnosis of neurogenic diarrhea, other causes must systematically be excluded. One theory regarding the pathogenesis of diabetic diarrhea holds that gastric and small bowel hypomotility may predispose to the proliferation of bacteria, which deconjugate bile salts and thus inhibit micelle formation. Steatorrhea and diarrhea thus result indirectly as a consequence of neurogenic hypomotility. A trial of tetracycline (500 to 1000 mg per day) therefore is conducted in most patients with unexplained chronic diarrhea, especially when steatorrhea is present. Treatment with prokinetic agents may also improve diarrhea. Should these measures fail, opioid agonists should be used. These agents decrease peristalsis and increase rectal sphincter tone. The synthetic opioids (diphenoxylate and loperamide) are preferable to alcohol solutions of opium. In the individual case, empiric management with tetracycline, opiates, prokinetic agents, psyllium, anticholinergics, and others often is needed. An alternative theory implicates a dysregulation of a*adrenoreceptor-mediated intestinal ion transport in diabetic diarrhea. Clonidine, a specific a,-adrenergic receptor agonist, may be used to treat diarrhea in dosages of up to 1.2 mg per day. The somatostatin analogue octreotide has been studied as a potential antidiarrheal agent in small numbers of patients with various conditions. As noted earlier, it may have a prokinetic action, but somatostatin has also been shown to inhibit stimulated water secretion in the gut. Fecal Incontinence. Studies of idiopathic fecal incontinence have found delayed conduction in pudendal nerves supplying the external sphincter and denervation changes in pelvic muscles. Impaired rectal sensation may be responsible for incontinence in
Principles of Diagnosis: Common Presenting Symptoms
such cases because detecting the presence of stool in the anal canal is essential to normal continence. Other authors have argued that the neuropathy is secondary to prolonged straining at stool and traction on pudendal nerves. Medical treatments generally attempt to rectify conditions that are either associated with or predispose to fecal incontinence. Use of high-fiber diets and bulking agents may be beneficial because a semiformed stool is more easily controlled than liquid feces. Fecal disimpaction is indicated in some cases. Daily tap water enemas aid in clearing residua in the rectum between evacuations and may allow functional continence. Antidiarrheal agents may benefit patients for whom incontinence and diarrhea coexist. Biofeedback based on the patient’s perception of a distensible balloon in the rectum and training to increase external sphincter pressure has met with success in some reports, although the response to biofeedback probably depends on the state of afferent pathways from the rectum. A majority of patients who undergo surgical sphincter repair may regain continence for solid stool, although the presence of pelvic floor neuropathy is associated with poorer outcome. Other surgical interventions, including colostomy, artificial anal sphincters, and creation of a reconstructed anal sphincter with muscle grafts, may be necessary in treatment-resistant cases.
SUGGESTED READINGS Anderson KE: The overactive bladder: pharmacologic basis of drug treatment. Urology 50:74-84, 1997 Arai K, Kato N, Kashiwado K, Hattori T Pure autonomic failure in association with human alpha-synucleinopathy. Neurosci Lett 296: 171-173, 2000 Axelrod FB: Hereditary sensory and autonomic neuropathies. Familial dysautonomia and other HSANs. Clin Auton Res 12(Suppl 1):12-14, 2000 Bannister R, Mathias CJ: Clinical features and investigations of the primary autonomic failure syndromes. In Bannister R, Mathias CJ (eds.): Autonomic Failure. Oxford University Press, Oxford, UK, 1992 Benarroch EE: New findings on the neuropathology of multiple system atrophy. Auton Neurosci 96:5942, 2002 Ben Shlomo Y,Wenning GK, Tison F, Quinn N P Survival of patients with pathologically proven multiple system atrophy: a meta-analysis. Neurology 48:384-393, 1997 Blaivas J G The neurophysiology of micturition: a clinical study of 550 patients. J Urol 127:958-963, 1982 Brunton L L Agents affecting gastrointestinal water flux and motility, digestants, and bile acids. In Gilman AG, Rall TW, Nies AS, Taylor P (eds.): The Pharmacological Basis of Therapeutics. Pergamon, New York, 1990 Cable WJ, Kolodny EH, Adams RD: Fabry disease: impaired autonomic function. Neurology 32:498-502, 1982 Camdessanche JP,Antoine JC,Honnorat J et ak Paraneoplastic peripheral neuropathyassociated with anti-Hu antibodies. A clinical and electrophysiological study of 20 patients. Brain 125:16&175, 2002 Camilleri M:Disorders of gastrointestinal motility in neurologic diseases. Mayo Clin Proc 652325446, 1990 Pemberton JH: Clinical Camilleri M, Thompson WG, Fleshman JW, management of intractable constipation. Ann Intern Med 121:520528, 1994 Dalmau J, Graus F, Rosenblum MK, Posner JB: Anti-Hu-associated paraneoplastic encephalomyelitislsensory neuronopathy. A clinical study of 71 patients. Medicine 71:59-72, 1992 Dyck PJ: Neuronal atrophy and degeneration predominantly affecting peripheral sensory and autonomic neurons. In Dyck PJ, Thomas PK, Griffin JWet al (eds.): Peripheral Neuropathy. Vol. 2. WB Saunders, Philadelphia, 1993
Chapter 14 H Autonomic Dysfunction
Falk RH, Comenzo RL, Skinner M: The systemic amyloidoses. N Engl J Med 3372398-909, 1997 Fedorak RN, Field M, Chang E B Treatment of diabetic diarrhea with clonidine. Ann Intern Med 102:197-199, 1985 Feldman M, Schiller LR Disorders of gastrointestinal motility associated with diabetes mellitus. Ann Intern Med 98:37&384, 1983 Fowler CJ: Investigation of the neurogenic bladder. J Neurol Neurosurg Psychiatry 605-13, 1996 Freeman R The peripheral nervous system and diabetes. In Weir G, Kahn R, King GL (eds.): Joslin’s Diabetes Mellitus. Lippincott Williams & Wilkins, Philadelphia, 2000 Freeman R Pure autonomic failure. In Robertson D, Biaggioni I (eds.): Disorders of the Autonomic Nervous System. Harwood Academic Publishers, Luxembourg, 1995 Freeman R Treatment of orthostatic hypotension: midodrine and other pressor drugs. In Robertson D, Low PA, Polinsky RJ (eds.): Primer on the Autonomic Nervous System. Academic Press, New York, 1996 Freeman R, Miyawaki E The treatment of autonomic dysfunction. [Review]. J Clin Neurophysiol 1061-82, 1993 Freeman R, Roberts MS, Friedman LS, Broadbridge C Autonomic function and human immunodeficiency virus infection. Neurology 40575-580, 1990 Furness JB: Types of neurons in the enteric nervous system. J Auton Nerv Syst 81~87-96,2000 Gilman S, Low PA, Quinn N et ak Consensus statement on the diagnosis of multiple system atrophy. J Auton Nerv Syst 74189-192, 1998 Goyal RK, Hirano I: The enteric nervous system. N Engl J Med 334:110&1115, 1996 Hague K, Lento P, Morgello S et ak The distribution of Lewy bodies in pure autonomic failure: autopsy findings and review of the literature [Review].Acta Neuropathol (Berl) 94:192-196, 1997 Hart RG, Kanter M C Acute autonomic neuropathy. Two cases and a clinical review. Arch Intern Med 150:2373-2376, 1990 Hilsted J, Low PA Diabetic autonomic neuropathy. In Low PA (ed.): Clinical Autonomic Disorders. Lippincott-Raven, Philadelphia, 1997 Hund E, Linke RP, Willig F, Grau A Transthyretin-associatedneuropathic amyloidosis.Pathogenesis and treatment. Neurology 5643 1435,2001 Indo Y, Tsuruta M, Hayashida Y et ak Mutations in the T W N G F receptor gene in patients with congenital insensitivity to pain with anhidrosis. Nat Genet 13:485-488, 1996 Iosa D, Dequattro V, De-Ping Lee D et ak Pathogenesis of cardiac neuro-myopathy in Chagas’ disease and the role of the autonomic nervous system. J Auton Nerv Syst 30S83-S88, 1990 Kaufmann H, Hague K, Per1 D: Accumulation of alpha-synuclein in autonomic nerves in pure autonomic failure. Neurology 56980-981, 200 1 Khurana RK: Paraneoplastic autonomic dysfunction. In Low PA (ed.): Clinical Autonomic Disorders. Lippincott-Raven, Philadelphia, 1993 Kunze WA, Furness JB: The enteric nervous system and regulation of intestinal motility. Annu Rev Physiol 61:117-142, 1999 Kyle RA, Dyck PJ: Amyloidosis and neuropathy. In Dyck PJ, Thomas PK, Griffin JW et al (eds.): Peripheral Neuropathy. WB Saunders, Philadelphia, 1993 Kyle RA, Gertz MA: Systemic amyloidosis. Crit Rev Oncol Hematol 1049-87, 1990 Lennon VA, Sas DF, Busk MF et ak Enteric neuronal autoantibodies in pseudoobstruction with small cell lung carcinoma. Gastroenterology 100:137-142, 1991 Locke GR 111, Pemberton JH, Phillips S F American Gastroenterological
153
Association medical position statement: guidelines on constipation. Gastroenterology 119:1761-1766, 2000 Madoff RD, Williams JG, Caushaj PF: Fecal incontinence. N Engl J Med 326~1002-1007, 1992 Mamdani MB, Walsh RL, Rubino FA et ak Autonomic dysfunction and Eaton-Lambert syndrome. J Auton Nerv Syst 12:315-320, 1985 Orthostatic hypotension, multiple system atrophy (the Shy-Drager syndrome) and pure autonomic failure. J Auton Nerv Syst 58:123-124, 1996 Papp MI, Lantos PL The distribution of oligodendroglial inclusions in multiple system atrophy and its relevance to clinical symptomatology. Brain 117:235-243, 1994 Saraiva MJM, Costa PP, Goodman DS: Biochemical marker in familial amyloidotic polyneuropathy, Portuguese type: family studies of transthyretin (prealbumin)-methionine-30 variant. J Clin Invest 76:217 12177, 1985 Schiller LR, Santa Ana CA, Schmulen AC et ak Pathogenesis of fecal incontinence in diabetes mellitus: evidence for internal-anal-sphincter dysfunction. N Engl J Med 307:166&1671, 1982 Spillantini MG, Crowther RA, Jakes R et al: Filamentous alpha-synuclein inclusions link multiple system atrophy with Parkinson’s disease and dementia with Lewy bodies. Neurosci Lett 251:205-208, 1998 Spillantini MG, Goedert M: The alpha-synucleinopathies: Parkinson’s disease, dementia with Lewy bodies, and multiple system atrophy. Ann N Y Acad Sci 920:1&27, 2000 Staskin DR Classification of voiding dysfunction. In Krane RJ, Siroky MB (eds.): Clinical Neuro-Urology. Little, Brown, Boston, 1992 Thomas PK Autonomic involvement in inherited neuropathies. Clin Auton Res 2:51-56, 1992 Tuck RR, McLeod J G Autonomic dysfunction in Guillain-BarrC syndrome. J Neurol Neurosurg Psychiatry 44983-990, 1981 Valdovinos MA, Camilleri M, Zimmerman BR Chronic diarrhea in diabetes mellitus: mechanisms and an approach to diagnosis and treatment. Mayo Clin Proc 68691-702, 1993 Vernino S, Low PA, Fealey RD et ak Autoantibodies to ganglionic acetylcholine receptors in autoimmune autonomic neuropathies. N Engl J Med 343:847-855,2000 Waterman SA Autonomic dysfunction in Lambert-Eaton myasthenic syndrome. Clin Auton Res 11:145-154, 2001 Wein AJ: Evaluation and treatment of urinary incontinence: practical uropharmacology. Urol C l i North Am 18:269-281, 1991 Wein AJ: Pharmacologic options for the overactive bladder. Urology 51:43-47, 1998 Wein AJ, Van Arsdalen K, Levin RM: Pharmacologic therapy. In Krane RJ, Siroky MB (eds.): Clinical Neuro-Urology.Little, Brown, Boston, 1992 Wenning GK, Ben Shlomo Y, Hughes A et al: What clinical features are most useful to distinguish definite multiple system atrophy from Parkinson’s disease? J Neurol Neurosurg Psychiatry 68434440, 2000 Wingate DL Autonomic dysfunction and the gut. In Bannister R, Mathias CJ (eds.): Autonomic Failure. Oxford University Press, Oxford, UK, 1992 Wood J D Physiology of the enteric nervous system. In Johnson LR, Christensen J, Jackson MJ et al (eds.): Physiology of the Gastrointestinal Tract. Raven Press, New York, 1987 Ziegler MG. Lake CR, Kopin IJ: The sympathetic-nervous-system defect in primary orthostatic hypotension. N Engl J Med 296:293-297, 1977 Zochodne DW: Autonomic involvement in Guillain-Barrk syndrome: a review. Muscle Nerve 121145-1155, 1994
154
15
Principlesof Ambulatory Neurology and the Approach to Clinical Problems W
Principlesof Diagnosis: Common PresentingSymptoms
Sexual Dysfunction Carlos Singer and Marca L. Sipski
Many neurologic disorders can affect sexual function. Sexual dysfunction may be a primary complaint or, more often, a problem secondary to the primary neurologic ones, which may go unaddressed by the patient and physician. Such disorders often necessitate cooperation between primary care physicians, urologists, gynecologists, endocrinologists, neurologists, and specialists in rehabilitation, sleep, and sexual disorders. The neurologist should understand the basic neuroanatomy and neurophysiology of the sexual response and the approach to diagnosis and therapy to serve as a consultant in managing the neurologic aspects of these disorders. This chapter presents an overview of this anatomy and physiology along with a review of the major categories of sexual dysfunction in men and women and an approach to evaluation and therapy. NEUROANATOMICAND NEUROPHYSIOLOCIC ISSUES
Sexual function can be controlled by psychogenic or reflexogenic mechanisms in both men and women. The psychogenic response is initiated by stimuli in the higher brain centers, resulting in sympathetic stimulation. The reflexogenic response is elicited by manual local stimulation of the genitalia via the sacral somatic innervation and elicits a parasympathetically mediated response. In men the center for reflexogenic erections is located in the S2-S4 sacral segments. Direct genital manipulation is transmitted to this center via the pudendal nerve (somatic nervous system). Its efferent erectogenic message is relayed by the parasympathetics via the pelvic nerves (nervi erigentes). At the level of terminals in the penile vasculature, an interaction with the noncholinergic nonadrenergic system (nitric oxide) occurs, resulting in dilation of the sinusoidal spaces of the penis, thereby initiating the erection. The penile engorgement compresses the draining veins, allowing maintenance of the erection. The thoracolumbar sympathetic center for erection responds to psychogenic stimuli and sends erectogenic messages via the hypogastric plexus and nerves that connect (and interact) with the parasympathetic system. A similar pattern has been determined in women. Based on studies of patients with spinal cord injuries (SCIs), it has been postulated that psychogenic lubrication occurs in response to signals from higher brain centers that travel down the lateral columns of the spinal cord near the pyramidal tracts and connect to and are facilitated by the thoracolumbar sympathetic pathways. Reflex lubrication would predictably be controlled by sacral parasympathetics. The preganglionic fibers of the parasympathetic branch involved in sexual response originate from the gray matter of the second, third, and fourth sacral segments of the spinal cord. These fibers enter the hypogastric plexus and synapse with the postganglionic fibers, which are distributed along the branches of the internal pudendal arteries. In men, seminal emission is the deposition of semen from the prostate, seminal vesicles, and distal vasa deferentia into the posterior urethra that precedes ejaculation. The afferent stimuli (genital stimulation and cerebral activity) follow the same pathways as in erectile function. The efferent signal then travels via the hypogastric sympathetic nerves. Ejaculation implies antegrade
propulsion of semen from the posterior urethra through the penile meatus. The afferent stimuli are the same as for seminal emission plus those resulting from the passage of semen into the posterior urethra. The efferent arm involves coordination between the somatic efferent nerves (S2-S4 via pudendal nerves) and efferent autonomic nerves (T12-L2 via hypogastric nerves). This allows rhythmic contractions of the striated pelvic floor musculature, compressing the urethra, and simultaneous closure of the bladder neck. The result is antegrade propulsion of the ejaculate. In women, smooth muscle contractions of the fallopian tubes, uterus, and periurethral glands during orgasm have been equated to emission in men and probably are mediated by the thoracolumbar sympathetics. Events paralleling ejaculation include contractions of striated muscles of the pelvic floor and perineal area and the anal sphincter mediated through the sacral parasympathetics in conjunction with somatic efferents. Recent data based on laboratory-based analyses of women with spinal cord injuries suggest that the ability to experience orgasm requires an intact sacral spinal reflex arc. MALE SEXUAL DYSFUNCTION
Male sexual dysfunction may present as an isolated complaint or as part of multiple somatic or psychological complaints. In some instances, it may be the manifestation of a disorder of the central or peripheral nervous system. In other instances the causes are outside the nervous system and involve one or more combinations of endocrinologic, drug-induced, urologic, vascular, and psychological mechanisms. Erectile Dysfunction Definitions and Clinical Aspects. Erectile dysfunction (ED), often called impotence, can be defined as the persistent inability to obtain or sustain an erection adequate for intromission, pelvic thrusting, and, in the absence of ejaculatory difficulties, ejaculation. ED may be primary or secondary depending on the respective absence or presence of a premorbid period of normal sexual function. Seven percent of otherwise intact men across the age spectrum have impotence. The figure increases to one third of men in their sixties, although two thirds of these impotent men still have preserved sexual drive. Clinical features that point to organic mechanisms, be they neurologic or non-neurologic, are a progressive onset first affecting maintenance of erections, gradually evolving into inability to achieve full erections. There is a gradual increase in the proportion of partial erections, a sense of decreased firmness, a tendency to rush through the sexual intercourse for fear of losing the erection, and an easy loss of firmness if minor distractions occur. Spontaneous morning erections progressively decrease in frequency and firmness. Sexual drive usually is preserved in the early stages of the condition. It tends to decrease much later, more commonly as a consequence of depression, itself a reaction to the dysfunction. If sexual drive is affected from the start, depression,
Chapter 15
endocrine dysfunction, and frontal lobe dysfunction should be ruled out. Psychogenic or drug-induced ED may start abruptly. Presence of decreased sexual drive at the outset suggests depression, but drug effectand hormonal imbalance should also be considered. In psychogenic ED, full erections may be possible with masturbation, sexual fantasy, or a different sexual partner. Morning erections may continue as frequent and as firm as before the onset of ED. The spouse’s participation during the interview may provide information indicating marital disharmony. Psychogenic impotence is further suggested by normal nocturnal penile tumescence (NPT) studies. Concurrent autonomic symptoms in the urinary, gastrointestinal, thermoregulatory, and cardiovascular spheres should be reviewed. If symptoms of autonomic failure are present, neuropathies or parkinsonism (multiple-system atrophy, Parkinson’s disease) should be considered. A detailed drug history may lead to medication adjustments, making it unnecessary to embark on a more costly diagnostic evaluation. Data on drugs that can cause sexual dysfunction are readily available, such as the yearly update provided in The Medical Letter. Alcohol and recreational drug use are also risk factors for ED. Concurrent atherosclerotic or peripheral vascular disease and heavy smoking may point to a vasculogenic mechanism. Diabetes is a common cause of ED through vascular and neuropathic mechanisms. Endocrinologic causes (hypothyroidism, hyperprolactinemia, hypoandrogenism) are likely to be associated with a decrease in sexual drive. Surgical procedures (e.g., prostate surgery, aortoiliac surgery, sympathectomy), pelvic radiation therapy, dialysis, and urologic structural abnormalities (e.g., hypogenitalism, Peyronie’s disease), predispose men to sexual dysfunction. The general and neurologic examination may provide additional clues to the cause. Distal sensory deficits to light touch, pin, temperature, or vibration and decreased or absent reflexes suggest neuropathy. The bulbocavernosus reflex may be decreased or absent in neuropathies. Mild cogwheel rigidity, unilateral slowness of finger tapping, decreased arm swing, or other early signs of parkinsonism should be sought. Orthostatic hypotension may suggest dysautonomia, as seen in peripheral neuropathies, Parkinson’s disease, or multiple-system atrophy. Saddle anesthesia, sensory level, spasticity, and other signs suggestive of myelopathies may also be detected in early stages, although they are likely to be symptomatic. Decreased or absent peripheral pulses may point to vasculogenic impotence. Peyronie’s disease and other urologic deformities will be apparent upon inspection. Diagnostic Evaluation of Erectile Dysfunction. The diagnostic evaluation of ED includes a determination of the contribution of organic and psychological mechanisms. After the history and physical examination, the presence of depression, spousal strain, and marital discord should be determined with a choice of available published scales. Examples include the Beck‘s Depression Inventory and the Locke-Wallace Marital Adjustment Test. NPT studies are the best method to determine organicity. These studies record erectile activity during rapid eye movement (REM) sleep by placement of mercury-filled strain gauges around the penis. The electrical resistance of the gauges increases as the mercury-filled tubing elongates and narrows. This change in impedance is transduced into voltage and recorded as a continuous tracing of circumference change. At the same time, sleep stages are also recorded. If adequate REM periods are generated during sleep, the concurrent presence or absence of firm erections can be docu-
Sexual Dysfunction
I55
mented reliably. A normal NPT study should identify most men with a predominantly psychogenic impotence, and the absence of firm erections strongly suggests organic ED. Snap-gauge bands, the stamp test, and portable take-home monitoring devices are alternative but less reliable methods because they cannot ascertain whether REM sleep has occurred, so false positives (absence of firm erections caused by absence of REM sleep) are likely. Even if the preliminary clinical and NPT evidence suggests psychogenicity, endocrine dysfunction should be evaluated with serum levels of prolactin, thyroid hormone, luteinizing hormone, follicle-stimulating hormone, total testosterone, and free testosterone. Given a prevalence of impotence of 60% in diabetic men, all impotent men should be checked for diabetes. This can be done by screening with a fasting blood glucose, or glycosylated hemoglobin, or more definitively ruling it out with a &hour glucose tolerance test. Once NPT studies confirm an organic contribution, the physician must decide on clinical grounds whether to investigate neurogenic mechanisms. The results of such tests may be of interest for the general understanding of the case but are not likely to determine a specific treatment. Bulbocavernosus reflex latency determination addresses the question of neuropathic contribution and may indirectly point to coexisting autonomic dysfunction of the penile organ. Abnormal pudendal evoked responses in the presence of normal bulbocavernosus reflex values suggest dysfunction in spinal cord, brainstem, or supratentorial sensory pathways. Biothesiometry, a measurement of penile vibration perception threshold, may be the only test to detect a sensory deficit as a mechanism of impotence. Electromyography of the sphincters may point to multiple-system atrophy if signs of reinnervation are discovered. (This last finding results from selective atrophy of Onuf‘s nucleus in the anterior horn of the sacral spinal cord. Neurons from Onuf‘s nucleus innervate the urethral and anal sphincters. The more superficial anal sphincter is more easily examined by needle electromyography.) Before referring to the sex therapist or the urologist, the primary care physician or consultant neurologist should be able to direct the initial portion of the diagnostic workup of erectile dysfunction. What follows falls in the hands of the urologist, but the well-informed clinician may remain actively involved as an additional source of guidance to the patient. The patterns of practice of urologists vary. Some limit themselves to intracavernous pharmacoactive agents used as diagnostic and therapeutic procedures and then move on to nonspecific treatment with suction erection devices or implants. Others may actively investigate vasculogenic mechanisms with the intent of undertaking a more specific surgical procedure if warranted. Hemodynamic penile studies, using duplex ultrasound scanning before and after intracavernosal injection of pharmacoactive agents, explore for presence of vascular insufficiency. The quality of response to intracavernous pharmacotherapy is also subject to analysis. A partial (less than firm) erection or a firm erection that can be sustained only for a short period of time (i.e., less than half an hour) suggests venous insufficiency, especially if hemodynamic studies are normal. A delay of more than 30 minutes in achieving a full erection suggests arteriogenic impotence. Similarly, if higher than standard dosages of pharmacoactive agents must be used to induce a firm erection or if a firm erection is unattainable, this also suggests arteriogenic impotence. Psychogenic and endocrinogenic ED respond to standard dosages of intracavernous agents. Neurogenic ED may necessitate slightly higher dosages, but not as high as the arteriogenic group.
156
Principles of Ambulatory Neurologyand the Approach to Clinical Problems H Principlesof Diagnosis: Common PresentingSymptoms
Suspected venous insufficiency can be confirmed by determining the flow necessary for an intracavernous infusion of saline to maintain a firm erection (cavernosometry). Radiopaque dye is then injected, with actual visualization of the venous leak (cavernosography). It is preferable to perform this study after penile injection of a pharmacoactive agent because this allows for a lessened fluid and contrast load and provides a more physiologic assessment of the venous occlusive mechanism. Pudendal angiography is indicated only if a patient with suspected arterial insufficiency is deemed to be a suitable candidate for reconstructive surgery. Invasive procedures involve significant discomfort and morbidity and should not be undertaken in a patient content with having his ED treated by less invasive or less specific means. Treatment of Erectile Dysfunction. The importance of the clinical history cannot be overemphasized. The clinician should first consider discontinuing or substituting medications, especially if their institution appears to have preceded the sexual dysfunction by a short time interval. A hormonal abnormality can be treated with specific measures best addressed by an endocrinologist. Depression, marital discord, a history suggestive of a psychogenic component, or a normal NPT study should prompt referral to a psychologist specialized in the field of sexual dysfunction. Neurogenic impotence and vasculogenic impotence can be treated with a variety of nonspecific therapeutic modalities. Use of oral sildenafd citrate has allowed successful treatment of ED regardless of cause. It is a highly selective and potent inhibitor of type 5 cGMP phosphodiesterase, enhancing erection by augmenting nitric oxide-mediated relaxation pathways, through increased cGMP accumulation in the corpus cavernosum. Onset of effect occurs within the first hour of intake, and it dissipates within 3 to 5 hours. Side effects include transient headache, flushing, dyspepsia, rhinitis, and visual disturbances such as changes in the perception of color or brightness. Concomitant use of nitrates is an absolute contraindication. The patient (or his partner) may choose to learn selfadministration of intracavernous vasoactive agents. They are more likely to be effective in patients with intact vascular mechanisms. The synthetic prostanoid prostaglandin E l (PGE1, alprostadil) is the most widely used agent. Mixtures of papaverine hydrochloride and phentolamine mesylate are equally effective. They have a lower incidence of pain but a much higher incidence of priapism and fibrotic nodules. In deciding to use intracavernous pharmacotherapy, the clinician should take into account the potential for hypotension, especially in patients with preexisting coronary artery disease. A formulation of alprostadil has also been approved for intraurethral administration. Suction erection devices are a nonpharmacologic, nonsurgical intervention with low incidence of side effects. A measure of manual strength and dexterity is necessary for their successful use. Prosthesis implants represent the option of last resort of neurogenic, arteriogenic, and venogenic erectile dysfunction. These devices come in semirigid and multicomponent inflatable varieties. The semirigid devices are low in cost and are easy to implant but have an aesthetically less desirable detumescent phase. The multicomponent inflatable prostheses are superior, providing greater mechanical reliability and patient satisfaction. However, reoperation may be necessary in case of certain complications such as postoperative infection, device erosion, or component failure. More specific surgical treatment modalities may be undertaken in carefully selected instances. Venogenic impotence can be treated with penile vein dissection and ligation. Arteriogenic impotence may be amenable to revascularization procedures.
Ejaculatory Disturbances Definitions, Concepts, and Clinical History EJAcumnoN. Premature ejaculation is the most comPREMATURE
mon male sexual dysfunction. Prevalence estimates range between 22% and 38%. Defining premature ejaculation has proven to be a daunting task. Some have suggested .basing the definition on existing normative data on the average time of intercourse (7 to 10 minutes). Others prefer to disregard this “stopwatch” approach because there is a lack of consensus as to what is a normal time period. Masters and Johnson define premature ejaculation as the inability to delay ejaculation long enough to allow the woman to reach orgasm in at least 50% of a couple’s sexual encounters. This definition assumes absence of orgasmic dysfunction in the woman. The DSM-IVR defines premature ejaculation as “persistent and recurrent ejaculation with minimal sexual stimulation before, on, or shortly after penetration and before the person wishes it. The clinician must take into account factors that affect the duration of the excitement phase such as age, novelty of the sexual partner or situation, and recent frequency of sexual activity.” Therefore, premature ejaculation may occur intravaginally or extravaginally. In addition, the DSM-IVR requires that the disturbance cause “marked distress or interpersonal difficulty” and that it not be due “exclusively to the direct effects of a substance (e.g., withdrawal from opioids).” Perhaps a more practical definition is the one that views premature ejaculation as a tendency to ejaculate at lower levels of sexual arousal. One possible mechanism is a lower rate of sexual intercourse as compared with control subjects, a notion with obvious therapeutic implications. EIACUUTORYINCOMPETENCE AND DRYEJAcumoN. Ejaculatory incompetence, also known as retarded ejaculation, implies an inability to ejaculate despite adequate erectile function with absence of both the orgasmic sensation and the ejaculate. It is currently viewed as psychogenic in the majority of cases. Organic factors such as spinal cord injury or disease, diabetes, or certain medications must be considered. This condition must be distinguished from “dry” ejaculation, in which there is an absence of ejaculate in the presence of an orgasmic sensation. This latter phenomenon suggests either defective seminal emission or retrograde ejaculation. Presence of semen or fructose in a postmasturbation urine sample points to the latter. Either dysfunction represents an organic sympathetic disturbance. Diagnostic Evaluation of Ejaculatory Disturbances. To date there are no specific neurophysiologic tests for evaluating ejaculatory dysfunction. For the neurologist or internist, the first task is to define (by virtue of the clinical history) the kind of ejaculatory dysfunction and the potential mechanisms (drugs, past surgeries, trauma). The physical examination may detect signs of neuropathy, myelopathy, or dysautonomia. It is not unusual for erectile dysfunction to be accompanied by the inability to ejaculate, in which case it is the former dysfunction that will necessitate the kind of diagnostic evaluation mentioned earlier. PREMATURE EJACULATION. Premature ejaculation is viewed primarily as a psychogenic problem. Numerous mechanisms have been invoked, including generalized or performance anxiety, unconscious negative feelings (hostility, fear) toward women, and unresolved marital problems. In addition to purely intrapsychic or relationship factors, a constitutionally faster ejaculatory reflex
Chapter 15 rn Sexual Dysfunction
(based on shorter latency of bulbocavernosus reflex) has also been invoked. This latter finding appears to apply to primary premature ejaculators (premature ejaculation from the beginning of their sexual lives) but cannot be used for diagnosis because of the overlap of results with controls. The physician should be aware of the rare instances in which organic dysfunction is associated with premature ejaculation. The index of suspicion for an organic cause increases in cases where the problem is preceded by a period of normal performance (secondary failure of ejaculatory control). Organic causes of premature ejaculation may include urologic conditions such as urethritis, prostatitis, and benign prostatic hypertrophy. Careful review of the literature reveals poor substantiation of the belief that these urologic conditions cause premature ejaculation. Better accepted causes of premature ejaculation are instances in which the sympathetic nervous system has been directly lesioned (abdominal aortic aneurysm surgery and pelvic fractures). Premature ejaculation has also been reported after withdrawal from antipsychotics or narcotics, with the use of desipramine, and with alcoholism. The postulated association with cardiovascular disease, arteriosclerosis, or venous leakage is also poorly substantiated. It has been stated that premature ejaculation may be caused by certain neurologic conditions such as multiple sclerosis, spinal cord tumors, polyneuritis, and alcoholic neuropathy. A closer review of some of the quoted sources fails to reveal with clarity the evidence on which these statements are based, particularly in the case of multiple sclerosis and spinal cord tumors. We still recommend that the clinician search for elements in the history or neurologic examination that raise the possibility of a true organic neurologic disorder underlying premature ejaculation. If clinically warranted, further neurologic investigation (i.e., magnetic resonance imaging, evoked responses, and cerebrospinal fluid analysis to rule out multiple sclerosis) may be necessary. Otherwise, there are no neurologic or non-neurologic paraclinical investigations specifically indicated for premature ejaculation, and referral to a sexologist or sex therapist is the next recommended step. ‘‘DRY‘.EJAcuwnoN. The patient with a complaint of “dry” ejaculation, which is the experience of the orgasmic sensation without the concomitant anterograde propulsion of ejaculate, warrants evaluation for an organic disturbance. To distinguish retrograde ejaculation from defective seminal emission, a postmasturbation urine sample is analyzed for the presence of spermatozoa or fructose. Certain drugs may induce either dry or retrograde ejaculation. Phenothiazines have long been known to affect ejaculation. Tricyclic antidepressants, monoamine oxidase inhibitors, lithium, and amphetamines are also capable of affecting ejaculation. Methyldopa, clonidine, and guanethidine are the most likely offenders of the antihypertensive agents by virtue of their interaction with sympathetic neurotransmission. There are also numerous urologic causes of retrograde ejaculation, which should be considered before invoking a neurogenic mechanism. The most common is transurethral resection of the prostate, but retropubic prostatectomy, bladder neck surgery, and trauma (i.e., pelvic fracture) are additional causes. A variety of congenital conditions causing bladder neck incompetence and conditions that mechanically obstruct the urethra are also worth noting. The neurologic mechanisms of ejaculatory and seminal dysfunction have in common a disruption of the sympathetic outflow. Erectile difficulties may or may not be concurrently present.
157
Surgeries most commonly associated with retrograde ejaculation or defective seminal emission include lumbar sympathectomy, retroperitoneal lymph node dissection, aortoiliac surgery, or colorectal surgery (e.g., abdominoperineal resection). Diabetes and other autonomic neuropathies also have to be considered. Of the myelopathies and myeloradiculoneuropathies,multiple sclerosis and spinal trauma are the most frequently mentioned. The possibility of ejaculatory dysfunction in the presence of relative preservation of erectile capacity has been well documented in spinal trauma victims. In some cases a clear cause cannot be found (idiopathic retrograde ejaculation). EJACULATORY INCOMPEENCE. There are no routine additional tests that can be ordered to investigate the disorder. The clinician should conduct a careful history and examination looking for possible coexisting or causative drug-induced or neurologic disorders. Subsequent laboratory or radiologic tests depend on their clinical findings. Once organic causes have been excluded, referral to a sex therapist will allow evaluation of psychogenic mechanisms. Treatment of Ejaculatory Disturbances. In cases of premature or incompetent ejaculation, referral to a sex therapist is recommended. Sex therapy techniques such as the “pausesqueeze” method have been suggested to treat premature ejaculation. Pharmacologic agents have also been used. They include topical anesthetics, neuroleptics, tricyclics, monoamine oxidase inhibitors, benzodiazepines, and a-blockers. Intracavernous pharmacotherapy with a papaverine and phentolamine mixture has also been reported successful in small series. A number of criticisms have been raised regarding these pharmacologic trials. Many of the trials are uncontrolled and involve small numbers of subjects. More recently, serotonin reuptake inhibitors taken a few hours before intercourse have been reported effective in placebocontrolled trials. Pharmacologic treatment can be considered in patients reluctant to accept or who have failed sex therapy. The other organic ejaculatory dysfunctions may respond to withdrawal of certain medications. The monthly medical publication The Medical Letter publishes a yearly update on the subject. The distinction between retrograde ejaculation and defective seminal emission is particularly relevant to couples seeking assistance for infertility. Vibratory stimulation, transrectal electrical stimulation, and intrathecal injections of neostigmine are techniques designed to obtain ejaculates for artificial insemination. FEMALE SEXUAL DYSFUNCTION DefSnlons and Clinical Aspects Recently a new international classification for female sexual dysfunctions was developed. Based on this classification, female sexual dysfunction is described in one of four categories: desire disorders (hypoactive sexual desire and sexual aversion disorder), sexual arousal disorder, orgasmic disorder, and sexual pain disorders (dyspareunia, vaginismus, and other sexual pain disorders). It follows that some neurologic disorders result in altered sexual response directly as a result of the neurologic disorder. However, to be considered a sexual dysfunction it must also be accompanied by significant personal distress, so not all alterations in sexual function occurring as a result of neurologic disorders would be considered sexual dysfunctions. In general, for women with neurologic disorders one must first obtain information about the woman’s premorbid sexual functioning and how her function was affected by the neurologic disorder. The woman should be questioned about the use of
158
Principles of Ambulatory Neurology and the Approach to Clinical Problems W
medications that can affect sexual function, surgical procedures, and the impact of her neurologic disorder on sensation and motor function. Partner issues should be reviewed, including the woman’s sexual preferences, her satisfaction with relationships, and whether her sexual dysfunction is situational. Additionally,the impact af associated psychological concerns and medical problems must be considered. Physical examination in women with spinal cord dysfunction should include particular attention to whether there is preservation of the ability to perceive pinprick and light touch sensation in the T11-L2 dermatomes because the combined ability to perceive these sensations has been related to the ability to achieve psychogenic genital vasocongestion. Furthermore, the presence of perianal sensation and an intact bulbocavernosus and anal wink reflex should be sought because women with complete lower motor neuron injuries affecting their sacral segments have been found to be significantlyless likely to achieve orgasm than women with all other patterns of spinal cord injury. In women with cerebral dysfunction, the loss of motor and sensory function in addition to the impact of other motor dysfunction on sexual activity should be considered. Moreover, the presence of speech and perceptual problems and their impact on sexual activity and the ability of the woman to engage in a sexual or other relationship should be considered. In women with neuropathy, the presence of autonomic neuropathy and the loss of motor or sensory function in the genital region and their impact on sexual response should be considered. Additionally, for all women a general physical and pelvic examination should be performed to assess estrogen status and circulatory function. DifferentialDiagnosis
There are no readily available tests for female sexual dysfunction. Instead, clinicians should direct their diagnostic workup to seek underlying neurologic or medical conditions and then apply their knowledge of the prevalence and mechanisms of sexual dysfunction in these disorders to provide counseling and assist other therapists. The differential diagnosis of sexual dysfunction in the woman with a neurologic disorder must take into account the impact of the neurologic disorder on sexual response. In addition, the impact of iatrogenic factors such as medications and surgery, concomitant medical and psychologic factors, preexisting sexual concerns, partner factors, and age-related factors must be considered. Once all these factors are taken into account, a sexual diagnosis can be entertained. Although the list is not exhaustive, the impact of various neurologic disorders on female sexual function is described later in this chapter. Because of the limited information that is available, these discussions are grouped based on common locations of neuropathology. Brain Disorders. Overall, the impact of various brain disorders on female sexual function is not well known. Various studies have reported a decrease in sexual satisfaction in women with traumatic brain injury and stroke. Additionally, decreased frequency of orgasm and decreased lubrication are noted with both groups. Parkinson’s disease has been reported to cause a decrease in libido and frequency of sexual activity in association with an increase in sexual complaints. Women with hypothalamic dysfunction have been reported to have menstrual irregularities, decreased desire, and lubrication and orgasm problems. Unfortunately, all studies have been self-reports, and many women suffering from brain dysfunction have concomitant issues, which
Principlesof Diagnosis: Common PresentingSymptoms
can affect their sexual function. These may include advanced age, diabetes mellitus, vascular dysfunction, use of medications, aphasia, and motor and sensory loss. Therefore, it remains uncertain whether specific patterns of brain dysfunctionwill result in specific alterations in female sexual response. Controlled laboratory-based analyses of the impact of specific locations of cerebral pathology on sexual response are needed. Spinal Disorders. A significant amount of research has addressed the impact of spinal cord dysfunction (SCD) on female sexual function. Women with spinal cord injuries (SCIs) report decreased sexual satisfaction and frequency of activity. Laboratory-based studies of women with SCIs have shown that the ability to perceive pinprick and light touch sensation in the T11-L2 dermatomes predicts the ability to achieve psychogenic lubrication. The sensory experience associated with orgasm has been shown to be similar in women with SCI and able-bodied women. A significantly lower ability to achieve orgasm as compared with able-bodied women (50% SCI, 100% able-bodied) was noted in the laboratory; moreover, greater latency to orgasm in women with SCI was reported as compared with able-bodied women. Women with complete lower motor neuron dysfunction affecting their sacral spinal segments have been found to be significantly less likely than women with all other levels and degrees of SCI to achieve orgasm. Although extensive studies have been performed in women with SCIs, minimal research has looked at the impact of other spinal disorders on female sexual response. However, because the end result of the neuropathology should be the same, it is recommended that the information available through the study of women with SCIs also be used when counseling women with spinal cord dysfunctions such as spina bifida and metastatic carcinoma. Multiple Sclerosis. Because multiple sclerosis can affect both the brain and spinal cord, it follows that its effect on sexual function depends on where the neuropathology exists in the individual patient. Studies have linked changes in lubrication and orgasm capacity with pelvic floor weakness and bladder and bowel dysfunction. Anorgasmia has been correlated with the total area of plaques observed in the brain on magnetic resonance imaging. Overall sexual dysfunction has been documented in nearly three quarters of women with multiple sclerosis, with complaints of decreased libido, anorgasmia, and decreased lubrication being common. Because sexual function entails a coordinated response from the autonomic nervous system, one would expect that women with autonomic neuropathies would experience sexual dysfunction. The most common group of women with neuropathy potentially experiencing sexual dysfunction is women with diabetes mellitus (DM). Women with DM have been studied via multiple self-report studies, and complaints of decreased desire, decreased lubrication and arousal, and orgasmic dysfunction have been recorded. Whether these sexual dysfunctions are associated with the presence of neuropathy has not been definitively documented. Moreover, only two studies have assessed the sexual response of women with DM in a laboratory, and these studies produced conflicting findings about whether the sexual responsiveness of women with DM differed from that of those without DM. Management
The first step in managing sexual dysfunction in women with neurologic disorders is to obtain a good history and physical
Chapter 16
examination and to determine whether there are any treatable sources of sexual dysfunction, such as the use of medications. Once these sources of dysfunction are eliminated, one should educate the woman as much as possible about the impact that her particular neurologic problem might have on her sexual function. Education of the partner, review of other emotional and partner issues, and referral for sexual counseling should be considered. No documented therapies have been approved to improve sexual function in women with neurologic disorders; however, one recent report found that women with SCIs reported greater levels of subjective sexual arousal with the use of sildenafil as compared with placebo. Therefore, off-label use of this medication can be tried, and future studies should consider the potential for other medications to improve female sexual function.
Hydrocephalusand Disorders of Cerebrospinal Fluid Flow
159
studied. No specific diagnostic test is readily available for female sexual dysfunction. Management currently depends on education and referral to a sexual counselor. Clinicians cognizant of sexual dysfunction medicine will be able to conduct the initial evaluation of these disorders and may be able to assist with counseling and referral to the appropriate professionals (sleep disorder specialist, endocrinologist, urologist, neurorehabilitationist, and sex therapist). By adopting a more active supervisory role, they ensure an adequate diagnostic evaluation and patient selection for the different treatment modalities. SUGGESTED READINGS Male Sexual Dysfunction
SUMMARY
Disorders of sexual performance in men include erectile and ejaculatory disturbances and should be distinguished from disorders in which a decrease in sexual desire is the principal rather than secondary mechanism. Clinical history is pivotal to characterize the dysfunction adequately and to search for the presence of risk factors or potential drug-induced conditions. Erectile dysfunction may be organic, psychogenic, or a combination of both. Nocturnal penile tumescence studies are crucial for reliable evaluation of these categories. Iatrogenic, endocrine, neurogenic, and vasculogenic mechanisms may underlie organic ejaculation dysfunction. There are no specific tests available to confirm the presence of the latter three mechanisms. Treatments may be specific or nonspecific to the cause. Ejaculatory disturbances include premature ejaculation and ejaculatory incompetence (primarily psychogenic) and dry ejaculation (exclusively organic). Dry ejaculation can be caused by defective seminal emission or retrograde ejaculation and can be distinguished by examination of a postmasturbation urine sample. Disorders of sexual performance in women include desire disorders, sexual arousal disorders, orgasmic disorders, and sexual pain disorders. Clinical history and examination are also pivotal in determining the underlying cause. The prototypical causes in the neurologic patient are represented by traumatic brain injury, spinal cord injury, and multiple sclerosis. Knowledge garnered as to prevalence and mechanisms in these conditions can then be used to try to understand the disorders that have been less well
16
Boller F, Frank E: Sexual Dysfunction in Neurological Disorders. Diagnosis, Management, and Rehabilitation. Raven Press, New York, 1982 Fowler CJ (ed): Neurology of Bladder, Bowel, and Sexual Dysfunction. Butterworth-Heinemann,Boston, 1999 Lechtenberg R, Old DA Sexual Dysfunction. Neurologic, Urologic and Gynecologic Aspects. Lea & Febiger, Malvern, PA, 1994 Schover LR, Jensen S B Sexuality and Chronic Illness. A Comprehensive Approach. Guilford Press, New York, 1988 Singer C, Weiner WJ: Sexual Dysfunction: A Neuro-Medical Approach. Futura, Armonk, NY, 1994
Female Sexual Dysfunction Basson R, Berman J, Burnett A et ak Report of the international development conference on female sexual dysfunction:definitions and classifications. J Urol 1632388, 2000 Korpelainen JT, Kauhanen JL,Kemola H et ak Sexual dysfunction in stroke patients. Acta Neurol Scand 98:400, 1998 Korpelainen JT,Nieminen P, Myllyla W: Sexual functioning among stroke patients and their spouses. Stroke 30715, 1999 Sipski ML, Alexander CJ (eds.): Maintaining Sexuality with Disability and Chronic Illness: A Practitioner’s Guide. Aspen Publishers, Gaithersburg, MD, 1997 Sipski ML, Alexander CJ,Rosen RC Sexual arousal and orgasm in women: effects of spinal cord injury. Ann Neurol4936-45, 2001 Sipski ML, Alexander CJ, Rosen RC, Hamer RM: Sildenafil effects on sexual and cardiovascular responses in women with spinal cord injury. Urology 55:812-815, 2000 Wermuth L, Stenager E Sexual problems in young patients with Parkinson’s disease. Acta Neurol Scand 91:453, 1995
Hydrocephalus and Disorders of Cerebrospinal Fluid Flow Sepideh Amin-Hanjani, William F. Pirl, Steven K. Feske, and Peter M. Black
Hydrocephalus is ventricular dilation caused by a disturbance in cerebrospinal fluid (CSF) circulation. This disturbance can occur anywhere in the CSF system. It is important to recognize hydrocephalus in the office practice of neurology and internal medicine because it can be associated with common complaints
such as headache, gait disturbance, and memory difficulty, and it can be treated successfully. Several terms are used to describe the anatomy of the particular hydrocephalic problem. Communicating hydrocephalus is characterized by continuity of the CSF in the ventricular system with the
Chapter 16
examination and to determine whether there are any treatable sources of sexual dysfunction, such as the use of medications. Once these sources of dysfunction are eliminated, one should educate the woman as much as possible about the impact that her particular neurologic problem might have on her sexual function. Education of the partner, review of other emotional and partner issues, and referral for sexual counseling should be considered. No documented therapies have been approved to improve sexual function in women with neurologic disorders; however, one recent report found that women with SCIs reported greater levels of subjective sexual arousal with the use of sildenafil as compared with placebo. Therefore, off-label use of this medication can be tried, and future studies should consider the potential for other medications to improve female sexual function.
Hydrocephalusand Disorders of Cerebrospinal Fluid Flow
159
studied. No specific diagnostic test is readily available for female sexual dysfunction. Management currently depends on education and referral to a sexual counselor. Clinicians cognizant of sexual dysfunction medicine will be able to conduct the initial evaluation of these disorders and may be able to assist with counseling and referral to the appropriate professionals (sleep disorder specialist, endocrinologist, urologist, neurorehabilitationist, and sex therapist). By adopting a more active supervisory role, they ensure an adequate diagnostic evaluation and patient selection for the different treatment modalities. SUGGESTED READINGS Male Sexual Dysfunction
SUMMARY
Disorders of sexual performance in men include erectile and ejaculatory disturbances and should be distinguished from disorders in which a decrease in sexual desire is the principal rather than secondary mechanism. Clinical history is pivotal to characterize the dysfunction adequately and to search for the presence of risk factors or potential drug-induced conditions. Erectile dysfunction may be organic, psychogenic, or a combination of both. Nocturnal penile tumescence studies are crucial for reliable evaluation of these categories. Iatrogenic, endocrine, neurogenic, and vasculogenic mechanisms may underlie organic ejaculation dysfunction. There are no specific tests available to confirm the presence of the latter three mechanisms. Treatments may be specific or nonspecific to the cause. Ejaculatory disturbances include premature ejaculation and ejaculatory incompetence (primarily psychogenic) and dry ejaculation (exclusively organic). Dry ejaculation can be caused by defective seminal emission or retrograde ejaculation and can be distinguished by examination of a postmasturbation urine sample. Disorders of sexual performance in women include desire disorders, sexual arousal disorders, orgasmic disorders, and sexual pain disorders. Clinical history and examination are also pivotal in determining the underlying cause. The prototypical causes in the neurologic patient are represented by traumatic brain injury, spinal cord injury, and multiple sclerosis. Knowledge garnered as to prevalence and mechanisms in these conditions can then be used to try to understand the disorders that have been less well
16
Boller F, Frank E: Sexual Dysfunction in Neurological Disorders. Diagnosis, Management, and Rehabilitation. Raven Press, New York, 1982 Fowler CJ (ed): Neurology of Bladder, Bowel, and Sexual Dysfunction. Butterworth-Heinemann,Boston, 1999 Lechtenberg R, Old DA Sexual Dysfunction. Neurologic, Urologic and Gynecologic Aspects. Lea & Febiger, Malvern, PA, 1994 Schover LR, Jensen S B Sexuality and Chronic Illness. A Comprehensive Approach. Guilford Press, New York, 1988 Singer C, Weiner WJ: Sexual Dysfunction: A Neuro-Medical Approach. Futura, Armonk, NY, 1994
Female Sexual Dysfunction Basson R, Berman J, Burnett A et ak Report of the international development conference on female sexual dysfunction:definitions and classifications. J Urol 1632388, 2000 Korpelainen JT, Kauhanen JL,Kemola H et ak Sexual dysfunction in stroke patients. Acta Neurol Scand 98:400, 1998 Korpelainen JT,Nieminen P, Myllyla W: Sexual functioning among stroke patients and their spouses. Stroke 30715, 1999 Sipski ML, Alexander CJ (eds.): Maintaining Sexuality with Disability and Chronic Illness: A Practitioner’s Guide. Aspen Publishers, Gaithersburg, MD, 1997 Sipski ML, Alexander CJ,Rosen RC Sexual arousal and orgasm in women: effects of spinal cord injury. Ann Neurol4936-45, 2001 Sipski ML, Alexander CJ, Rosen RC, Hamer RM: Sildenafil effects on sexual and cardiovascular responses in women with spinal cord injury. Urology 55:812-815, 2000 Wermuth L, Stenager E Sexual problems in young patients with Parkinson’s disease. Acta Neurol Scand 91:453, 1995
Hydrocephalus and Disorders of Cerebrospinal Fluid Flow Sepideh Amin-Hanjani, William F. Pirl, Steven K. Feske, and Peter M. Black
Hydrocephalus is ventricular dilation caused by a disturbance in cerebrospinal fluid (CSF) circulation. This disturbance can occur anywhere in the CSF system. It is important to recognize hydrocephalus in the office practice of neurology and internal medicine because it can be associated with common complaints
such as headache, gait disturbance, and memory difficulty, and it can be treated successfully. Several terms are used to describe the anatomy of the particular hydrocephalic problem. Communicating hydrocephalus is characterized by continuity of the CSF in the ventricular system with the
160
Principles of Ambulatory Neurology and the Approach to Clinical Problems
subarachnoid space of the brain and spinal cord. Noncommunicating hydrocephalus occurs when there is a blockage in the ventricular system or its outlets so that the ventricles and the subarachnoid space are not in continuity. It is important to recognize this distinction because a lumbar puncture is unsafe in the noncommunicating form. Hydrocephalus ex vacuo is not actually a form of hydrocephalus but rather is a state of increased ventricular size resulting from loss of adjacent parenchymal tissue mass. Although hydrocephalus has many different manifestations, it is instructive to group cases into two clinical syndromes: high-pressure hydrocephalus and normal-pressure hydrocephalus (NPH), with gradations between them. Another abnormality of CSF dynamics, called pseudotumor cerebri or benign intracranial hypertension, represents a syndrome of increased intracranial pressure (ICP) without associated ventriculomegaly. At the other end of the spectrum lie symptoms related to low CSF pressure, known as the syndrome of intracranial hypotension. This chapter describes the clinical presentations, diagnosis, and management of CSF flow abnormalities in adults. Similar principles apply in children. Pseudotumor cerebri is also discussed in Chapter 6.
HYDROCEPHALUS Clinical Presentation: High-pressure Hydrocephalus The onset of high-pressure hydrocephalus can be acute, over hours to days, or chronic, over weeks to months. High-pressure hydrocephalus can be life-threatening, causing obtundation, coma, and death. Its symptoms are related to increased ICP. Headache is the most common complaint. The headache, usually bifrontal, is most severe in the morning; it tends to be worse when the patient lies flat and to be relieved by sitting, and it can be exacerbated by coughing. It can progress to a generalized headache and may even wake the patient at night. Nausea and vomiting commonly occur in association with the headache and are also most severe in the morning. The nausea is not associated with head movements or any abdominal discomfort. The patient may also complain of visual changes, including decreased visual acuity, diplopia, and an inability to look up. “Graying-out” of vision may occur if a pressure wave causes serious optic nerve vascular compromise. The gait disorder typically is an unsteady, broad-based gait that may first appear as slow and uncertain and then develop into short, staggering steps. Changes in mental status can range from impairment of recent memory, to confusion, to a depression of the level of consciousness. Signs of frontal lobe disorder with slowness of response, inattentiveness, distractibility, inability to plan or sustain complex actions, and perseveration may be present. However, in contrast to primary cortical dementias, such as Alzheimer’s disease, there is no aphasia, agnosia, or apraxia. Physical examination may reveal papilledema from increased ICP, but this is not invariably present. Testing of extraocular movements may reveal a lateral rectus weakness caused by compression of abducens nerve fibers. This is a sign of generalized increased ICP; it is not a localizing sign even when it is unilateral. Paralysis of upward gaze and of accommodation results from pressure on the tectal plate. Truncal ataxia may be present. Almost all cases of high-pressure hydrocephalus in adults are caused by an obstruction of flow through the ventricular system or subarachnoid pathways. This results in increased mean pulsatile pressures in the ventricular system and a consequent increase in
Principles of Diagnosis: Common Presenting Symptoms
TABU 16-1. Some Causes of Adult Normal-Pressure Hydrocephalus Cause Subarachnoid hemorrhage Idiopathic Head injury Tumors Prior surgery Aqueduct stenosis Meningitis Others
Percentage
34 34 11 6 5 3 3 4
Modified from Kakman R Low pressure hydrocephalus. p. 29. In Wells CE (ed): Dementia. FA Davis, Philadelphia, 1977, with permission.
ventricular size. The ventricles continue to expand until the pressure can no longer be compensated, eventually leading to central herniation and death. An obstruction can occur anywhere along the CSF pathway. The causes are the same as those listed in Table 16-1 for NPH. Even with a specific cause, there may be no localizing signs to help the examiner discern the underlying cause. Subarachnoid hemorrhage is the most common cause of obstruction, with hydrocephalus occurring in as many as 67% of cases of subarachnoid hemorrhage. Because of this frequency, patients with a subarachnoid hemorrhage should be monitored for symptoms of hydrocephalus for up to 3 weeks after the event. Tumors causing obstruction of the ventricles or their outflow are another important cause of high-pressure hydrocephalus. In addition to intraventricular tumors, tumors may also obstruct the ventricular system extrinsically. Posterior compression of the third ventricle can result from a pineal tumor or inferior compression from a craniopharyngioma or pituitary adenoma. Similarly, the fourth ventricle can be compressed by posterior fossa tumors. Aqueduct stenosis, a congenital disorder that may present in adulthood, should also be seriously considered in the differential diagnosis. Clinical Presentation: Normal Pressure Hydrocephalus
NPH is characterized by enlargement of the ventricles and normal CSF pressure. It has a number of known causes, but the most common type is idiopathic NPH, which comprises about 50% of cases. It is best diagnosed by its clinical presentation: the classic triad of gait disturbance, disturbances in mentation (usually slowing of thought and action), and urinary incontinence. Symptoms of high-pressure hydrocephalus such as headache, nausea and vomiting, and visual changes are not seen. Gait Disorder. Gait disturbance is the most prominent symptom in NPH and is usually the earliest in onset. It has been described as unsteady or uneven, and patients often complain of falling. The gait is characterized by its wide base, slow speed, short steps, and vertical ataxia. (Patients place their feet on the ground with variable force.) Patients sometimes describe feelings of weakness in their legs, and they may actually be consuming more energy in walking than is normal. The problems with walking can progress to complete inability to walk and even inability to stand or sit because of unsteadiness. However, the gait disorder appears to be more of a frontal gait apraxia, which poses difficulties in organizing a smooth gait, rather than an actual ataxia. The same patients with NPH who are unable to walk demonstrate unimpaired functioning of the legs when lying on their back. There may also be some upper extremity involvement with tremor and deterioration of handwriting.
Chapter 16
Gait disorders are regularly encountered in older adults, and NPH accounts for only a small percentage of these cases. Some features of the disordered gait of NPH may help to distinguish it from other causes of gait disorder, although the distinction often may be difficult. Patients with Alzheimer’s disease may have a gait disorder, but compared to NPH, the gait tends to be shuffling and scuffing with increased double-support stride. It occurs late in Alzheimer’s disease, after cognitive deterioration. Cerebellar ataxia must also be considered in the differential diagnosis. In contrast to the vertical ataxia of NPH, in cerebellar ataxia, movements of the legs are more variable in the transverse and sagittal planes. Other features of cerebellar incoordination, such as dysmetria and terminal tremor, are not present in NPH. Parkinson’s disease is also characterized by a gait disorder and may be confused with NPH because both can display bradykinesia, increased tone, and dysarthria. However, the parkinsonian gait is described as hesitant with festination, en bloc turning, flexed posture, and lack of accessory movements such as arm swinging. In addition, cogwheel rigidity and masked facies are distinguishing features of Parkinson’s disease. Patients with Binswanger’s disease or multi-infarct dementia may also present with a frontal gait disorder that is indistinguishable from NPH, although patients with NPH tend to present at a later age and more often have gait disturbance at onset. Disturbance of Mentation. A variety of mental changes have been described in NPH, ranging from mild memory loss to severe dementia. Impairment of recent memory is the most common complaint. However, a more characteristic finding in NPH than memory loss is a general slowing of thought and action. A loss of initiative, spontaneity, and interest may progress to apathy and abulia. Responses and voluntary movements are slow and delayed. Some cognitive impairment may be present with verbal abilities unaffected, whereas nonverbal tasks such as copying, drawing, and arranging objects become difficult. Changes in mood, behavior, and personality may also be evident. This clinical picture represents a subcortical type of dementia, often encountered in older adults, which may be very difficult to distinguish from other subcortical dementias such as multi-infarct dementia, from depression, and, at times, from cortical dementias such as Alzheimer’s disease. Alzheimer’s disease can be distinguished by aphasia, agnosia, and apraxia, which are not components of the dementia of NPH. The changes in mentation seen in Alzheimer’s disease occur much earlier than the gait disturbance, which is usually a late symptom. In NPH, gait disorder usually precedes or occurs concurrently with changes in mentation. Major depression may present as a pseudodementia with memory loss and psychomotor retardation; however, neurovegetative symptoms and depressed mood should be present. Incontinence is generally not seen in depression. Binswanger’s disease and the multi-infarct state may cause a dementia very similar to that of NPH and pose a diagnostic difficulty that can be resolved only by other tests, such as magnetic resonance imaging (MRI). Incontinence. Urinary incontinence is the third part of the NPH triad, and although it is common in NPH, it is not seen with the same frequency as gait disorder and changes in mentation. It may occur as a late symptom. The incontinence ranges from a sense of urgency to a frontal lobe type of incontinence in which the appropriate awareness of the need to urinate is lost, leading to a loss of sphincter control. Fecal incontinence is rare. Urinary incontinence can also be seen in atrophic processes such as Alzheimer’s disease. Physical Examination. The physical examination reveals no focal signs unless there is a specific cause of NPH, such as tumor.
Hydrocephalusand Disorders of Cerebrospinal Fluid Flow
161
Papilledema is absent, and extraocular movements and upward gaze are intact. Tone may be normal, or a frontal, paratonic-type hypertonicity may be appreciated. Weakness is not present, but limb movement may be slow. Increased tendon reflexes may be observed, and a positive Babinski sign may be present in one or both feet. Sucking or grasping reflexes may appear in later stages. No sensory loss is seen. Cerebellar ataxia is not present. Patients may be unable to perform tandem walking, and they often have positive Romberg signs. Gait difficulties are as described earlier in this chapter. Etiology. NPH can be caused by anything that results in low-grade scarring or obstruction of the ventricular system or subarachnoid pathways. The causes are listed in Table 16-1. Subarachnoid hemorrhage is the most common cause of NPH with a known cause. Other causes include meningitis, partial obstruction of the CSF pathways by tumor, cranial radiation, and neurosurgery, particularly after a posterior fossa operation. NPH may follow trauma that causes a subarachnoid hemorrhage that subsequently obstructs the basal cisterns. Less commonly, it may follow an obstruction of a major venous sinus or the third ventricle and its outflow. Aqueduct stenosis more often leads to high-pressure hydrocephalus, but it may cause NPH as well. Idiopathic NPH, seen in a large number of cases, is more common in patients who are over 60. They are the most difficult group to treat. Pathogenesis. In the pathogenesis of NPH, Hakim and Adams (1965) have suggested that there is an initial rise in CSF pressure that leads to ventricular enlargement. This enlargement is maintained despite normal pressure because of the relationship of pressure and area described by LaPlace’s law (pressure = force/ area). The increased force on the ventricular wall is distributed at a lower pressure over the greater area of the enlarged ventricular wall. Even though the pressure appears normal most of the day, continuous ICP monitoring in some patients also shows periods of increased ICP waves at night. Investigation Studies
The purpose of ancillary testing in patients with hydrocephalus is twofold to establish a reliable diagnosis and to predict the utility of CSF diversion in treating the disorder. Once a patient has presented with a clinical picture suggestive of hydrocephalus, the initial diagnostic test of choice is computed tomography (CT) or MRI. An unenhanced scan visualizes the ventricular contours, and contrast enhancement may reveal otherwise indistinguishable underlying lesions. The cardinal features of hydrocephalus include enlargement of ventricles, with rounding of the ventricular contour; the presence of periventricular lucencies, especially around the frontal horns (although this finding on MRI is not specific); and normal-sized or diminished subarachnoid spaces. Enlargement of the subarachnoid spaces and prominent cortical sulci suggest atrophy with ex vacuo ventricular enlargement. There are advantages to MRI over CT. MRI is better than CT for identifying underlying lesions, such as small periaqueductal or posterior fossa tumors. MRI is also the modality best equipped to assess parenchymal disease seen with Binswanger’s disease or multi-infarct dementia, which may be difficult to distinguish from NPH on clinical grounds alone. Furthermore, sagittal imaging with MRI may help to distinguish hydrocephalus from atrophy by showing features that suggest hydrocephalus, such as thinning and bowing of the corpus callosum. However, periventricular hypointensity on TI-weighted MRI is less specific and can be seen
162
Principles of Ambulatory Neurology and the Approach to Clinical Problems H Principles of Diagnosis: Common Presenting Symptoms
in the setting of edema, ischemia, demyelination, and other disorders. In addition to anatomic determinations, MFU can show CSF flow patterns through the aqueduct of Sylvius. A variety of MRI techniques have been applied to establish flow and pulsatility patterns through the Sylvian aqueduct in patients with hydrocephalus. Recent reports suggest that these techniques may have value in differentiating the various types of hydrocephalus, although their reliabilityin predicting shunt responsiveness in NPH remains to be determined. Cisternography has been used in the past to evaluate CSF dynamics in patients with ventricular enlargement and suspected NPH. However, it appears to have little usefulness today. It is performed by intrathecal injection of a radioactive isotope (isotope cisternography) or contrast material and serial CT scanning (CT cisternography). The passage of the isotope or contrast into the ventricles and subarachnoid space is visualized. A normal pattern shows flow over the convexities and not into the ventricles. The typical pattern of NPH is ventricular entry and stasis without ascent over the convexities. Most patients show a mixed pattern. Recent reports indicate that cisternography provides no additional diagnostic accuracy over the combination of clinical and CT criteria. Determination of CSF pressure by lumbar puncture is an important component of diagnosis in some patients. Patients who do not have findings of high-pressure hydrocephalus and are suspected clinically to have NPH without an identifiable cause should undergo lumbar puncture. An opening pressure less than 180 mm H,O in this group of patients is consistent with a diagnosis of idiopathic NPH. The value of shunting in such patients may be further elucidated by a lumbar puncture with removal of approximately 50 mL fluid. Alternatively, serial lumbar punctures, which presumably create an ongoing dural leak acting as a temporary shunt, can be performed. Clinical improvement after large-volume lumbar puncture, especially of gait, predicts a good response to shunting. Temporary lumbar drainage has been suggested as a further maneuver for predicting shunt responsiveness. Continuous ICP monitoring can also help to identify patients with idiopathic NPH who are likely to benefit from CSF diversion. Monitoring can be performed using a frontal ventricular catheter, lumbar catheter, or epidural transducer, all of which allow prolonged pressure recording over at least 24 hours. Increased baseline CSF pressure or pressure waves (A or B waves) can be used as criteria for shunt responsiveness. B waves appear particularly useful. An adjunct to prolonged pressure recording is the use of infusion tests to assess resistance to CSF absorption. Lumbar infusion of normal saline has been shown to detect prolonged increases in ICP, indicating deficits in CSF absorptive capacity. A well-proven technique involves measuring CSF conductance by lumboventricular perfusion. Outflow resistance greater than 12.5 mL/minute/mm Hg has been correlated with improvement after shunting. The disadvantages of these testing modalities are their invasiveness and potential for equivocal measurements of CSF outflow resistance. They may offer prognostic information for shunting in a selected group of patients with idiopathic NPH in whom less invasive testing has been inconclusive. Recently the acetazolamide challenge test, looking at changes in cerebral blood flow and ICP in response to acetazolamide administration, has been advocated as a diagnostic test in patients with suspected NPH, but its reliability has yet to be determined.
There is some evidence that functional tests such as single photon emission computed tomography, which shows patterns of cerebral blood flow; positron emission tomography, which demonstrates brain metabolism; and magnetic resonance spectroscopy, which measures ratios of chemical markers in the brain, may help to differentiate NPH from other causes of dementia and may also be of some predictive value in determining shunt responsiveness. However, these tests are still under investigation and need further validation before they enter mainstream clinical practice. Electroencephalography and evoked responses have no utility in the diagnosis of hydrocephalus.
Decision Making and Management The optimal management of a patient with suspected hydrocephalus relies on the strength of the clinical diagnosis and the validity of ancillary tests aimed at prognostication. When making management decisions, it is useful to consider separately the clinical entities that result from high- and normal-pressurehydrocephalus. The patient with symptoms of increased ICP and ventriculomegaly, who is acutely deteriorating as indicated by a worsening level of consciousness or loss of vision, needs emergent neurosurgical consultation for placement of ventriculostomy. In less acute situations involving high-pressure hydrocephalus, CSF diversion by operative placement of a shunt is indicated. In cases of hydrocephalus secondary to an obstructive mass, however, primary management that includes removal of the mass may relieve the hydrocephalus. Operative removal is increasingly the treatment of choice, given recent improvements in microsurgical technique, although there may be a need for CSF diversion at a later date. Preoperative shunting carries the risk of upward tentorial herniation with large midline cerebellar masses, as well as the potential for spreading malignant cells to the peritoneum via the shunt. Another method of CSF diversion that has regained popularity in recent years is intracranial CSF diversion by means of endoscopic fenestration of the third ventricle. This procedure typically is performed in cases with lateral and third ventricles enlarged disproportionately to fourth ventricles. A fenestration is created in the floor of the third ventricle into the basal CSF cisterns, thus avoiding the need for permanent shunt placement. The definitive treatment for NPH is shunting, but poor responses in some groups and possible complications must be considered in the decision to proceed with shunt placement. Patients with the diagnosis of NPH as supported by the clinical syndrome and CT findings should undergo careful evaluation for an underlying cause. When a clear cause is present, such as recent subarachnoid hemorrhage, meningitis, evidence of aqueduct stenosis, or obstructive tumor, shunting is the treatment of choice and is associated with good outcome. As with high-pressure hydrocephalus caused by a mass, it is reasonable to remove an obstructive lesion as primary management for NPH. For cases of idiopathic NPH the decision is more complex. Numerous clinical findings and tests have been advocated as predictors of shunt responsiveness, some of which are discussed earlier in this chapter. Many studies have addressed this issue. The following parameters have consistently proven to be good prognosticators for shunt response: NPH of known cause Shorter duration of symptoms (although long duration is not a contraindication) Prominent gait disturbance
Chapter 16
Improvement after serial lumbar punctures or lumbar drainage Altered CSF dynamics as demonstrated by long-term monitoring or infusion testing, especially lumboventricular perfusion A CT scan showing periventricular lucency Studies of shunt responsiveness report response rates in the range of 30% to 80%. In our experience about two thirds of patients improve and perhaps 5% may worsen in some way with shunt placement. Differences in outcome may result from differential selection for shunting and analysis of outcomes. Standardized preshunting selection criteria may increase the likelihood of improvement. Of special interest are patients with ventricular enlargement who are free of symptoms related to hydrocephalus. The incidental finding of ventriculomegaly on imaging in such patients should prompt careful evaluation for subtle symptoms or signs of hydrocephalus. If the patient is truly asymptomatic, no further investigation or intervention is indicated; however, interval follow-up to assess the possible development of symptoms is warranted.
PSEUDOTUMOR CEREBRI (BENIGN INTRACRANIAL HYPERTENSION) Pseudotumor cerebri is a syndrome of increased ICP without ventriculomegalyor intracranial mass or inflammation. Although the cause is not known, several features seem to contribute to the mechanism of ICP elevation. Prior subarachnoid hemorrhage, central nervous system infection, and marked CSF protein elevation, as may be seen in inflammatory demyelinating radiculoneuropathies, may lead to a syndrome identical to idiopathic pseudotumor cerebri. This suggests that the functional lesion is an increased resistance to CSF flow at the level of the arachnoid granulations. Modeling of such a lesion suggests that it could cause ICP elevation without ventriculomegaly. Also, conditions that raise central venous pressure, such as obesity and chronic obstructive pulmonary disease with right-sided heart failure, may contribute to an identical state of intracranial hypertension. Raised intracranial venous pressure contributes a hydrostatic resistance to absorption of CSF at the level of the arachnoid granulations. It is probable that both lesions contribute to the decompensation of CSF homeostasis that culminates in symptomatic pseudotumor cerebri.
Clinical Presentation The most common patient is a young, obese woman. The major clinical symptoms are headache and visual symptoms that reflect the elevated ICP. The headache usually is dull and continuous and often nonspecific in quality, or it may have features suggestive of elevated ICP, such as worsening in the early morning, in the recumbent position, and with coughing or straining. Patients may complain of visual blurring, scotomas, or visual obscurations. The last are sudden, brief losses of vision in one or both eyes attributable to ICP elevations. Patients may also complain of double vision caused by an abducens paresis. It is thought that the abducens nerve is vulnerable to high ICP because of its long exposure to the subarachnoid space, Pulsatile tinnitus has also been reported as a symptom suggestive of pseudotumor cerebri. When ICP elevation is severe, nausea, vomiting, and depression of
Hydrocephalus and Disorders of Cerebrospinal Fluid Flow
163
TABLE 16-2. Causes of Pseudotumor Cerebri Increased venous pressure Sinus obstruction High-flow arteriovenous malformation lntracranial dural arteriovenous fistula Chronic obstructive pulmonary disease with cor pulmonale Obstructive sleep apnea Endocrine related Pregnancy, menarche, oral contraceptives Obesity Corticosteroid use or withdrawal Hypoparathyroidism Thyroid replacement Toxic or metabolic Hypervitaminosis A or hypovitaminosis A Drug related (e.g., nalidixic acid, tetracycline, lithium, growth hormone) Malnutrition or refeeding Idiopathic
the level of alertness may occur, as with intracranial hypertension from other causes. The common physical findings are diminished visual acuity, enlargement of the blind spots, and constriction of the visual fields. Almost all patients have papilledema with loss of spontaneous venous pulsations and blurring and elevation of the optic disc head. Pseudotumor cerebri with normal disks has been reported but is rare. Eye movements may be normal, or there may be unilateral or bilateral abducens paresis. Trochlear nerve paresis has been reported, but this is rare. The neurologic examination is otherwise typically normal. Much of the history-taking and examination is directed toward identifying or excluding potential underlying causes (Table 16-2). By far, the most common underlying contributor is obesity. However, idiopathic pseudotumor cerebri has been reported as a result of vitamin A toxicity and toxicity to tetracyclines, lithium, and more recently to recombinant human growth hormone. It has also been reported to occur after withdrawal of corticosteroid therapy. Therefore, all of these exposures should be sought in the history. Conditions that have resulted in blood products, inflammation, or protein elevation in the subarachnoid space may cause an identical clinical syndrome, so a history of such problems should be sought as well. Also, pregnancy may cause a patient to decompensate and come to medical attention, so women with child-bearing potential should be tested for pregnancy. Conditions that obstruct the cerebral venous drainage may cause an identical condition of elevated ICP. Cerebral venous thrombosis may present with isolated intracranial hypertension. Also, patients with intracranial dural arteriovenous fistulas or patients having had endovascular therapy affecting cerebral venous drainage may have intracranial hypertension. Therefore, given the availability of noninvasive and sensitive brain imaging with MRI, it is best to rule out such disorders with brain MRI and with magnetic resonance venogram sequences. Although small series have shown that the yield of such imaging will be low if done on patients with suspected idiopathic pseudotumor cerebri, there is no other noninvasive way to exclude such treatable lesions. Patients with inflammatory conditions, such as sarcoidosis, systemic lupus erythematosus, or Behget’s disease, can also present with isolated, and often recurrent, intracranial hypertension. CSF analysis is necessary to exclude such inflammatory disorders as well as infections and leptomeningeal infiltration with tumor. Medical conditions that might underlie intracranial hypertension include obesity, chronic obstructive lung disease with cor pulmonale, pickwickian syndrome, obstructive sleep apnea, and
164
Principles of Ambulatoy Neurology and the Approach to Clinical Problems W
possibly primary aldosteronism. These should be considered, especially when the presentation is atypical, such as in older patients, men, and nonobese patients. Also, cranial synostoses may predispose patients to intracranial hypertension.
Investigational Studies The diagnosis of pseudotumor cerebri is confirmed by radiologic imaging followed by lumbar puncture. Imaging of the brain by CT or MRI will show no mass lesions or other underlying cause of elevated ICP. The ventricles may be normal or small and slitlike. An “empty sella” is a common finding, and such patients may have normal pituitary function or only subtle abnormalities. MRI and magnetic resonance venography exclude cerebral venous sinus thrombosis. Lumbar puncture reveals elevated ICP, usually greater than 300 mm H20, and CSF that is characteristically normal in composition or shows only a low CSF protein level. There is no evidence of inflammation or protein elevation in truly idiopathic cases. Other investigations may be needed to address possible underlying conditions, as discussed earlier.
Principlesof Diagnosis: Common PresentingSymptoms
INTRACRANIAL HYPOTENSION
Clinical Presentation As with syndromes of elevated ICP, headache often is the presenting symptom of intracranial hypotension. Symptoms can develop after lumbar puncture, CSF shunts, spinal surgery or trauma, or invasive tumor eroding the skull base, but they often develop spontaneously with no apparent precipitating factor. The hallmark of intracranial hypotension is postural headache, worst when in the upright posture and completely relieved in the recumbent posture. When spontaneous, the cause is believed to be a dural tear, often in the cervical or thoracic spinal region, with resultant CSF leak from the subarachnoid space. The loss of CSF causes low ICP. The loss of the buoyant effect of the CSF causes traction on dural and vascular elements, especially in the upright position. The leak may not be evident and may be difficult to localize. The headache may be accompanied by nausea, vomiting, dizziness, and meningismus. Straining and coughing tend to exacerbate the headache. Other presentations include cranial nerve palsy, especially sixth nerve palsy. Visual symptoms can also be present in the form of photophobia or blurred vision.
Decision Making and Management The most important therapeutic goal is to preserve vision. Patients should have a periodic ophthalmologic examination with perimetry testing of the visual fields. And any deterioration should prompt more aggressive therapies to preserve vision. All obese patients should be encouraged to lose weight. A weight loss of several percent in many cases greatly lowers the ICP. Medical therapy may also include acetazolamide. There is some controversy about the mechanism and effectiveness of this agent. It decreases production of CSF and probably promotes absorption. Most patients tolerate it well; occasionally patients complain of distal paresthesias. Electrolytes should be followed, although significant metabolic acidosis is uncommon at the usual therapeutic dosages. Patients may begin with long-acting acetazolamide 500 mg twice daily. Dosages of 500 to 2000 mg, and occasionally more, may be effective. Most patients appear to respond well to acetazolamide even when efforts to lose weight are unsuccessful, as is often the case. Patients may respond to single or serial lumbar puncture and CSF drainage. This can be used as a temporizing therapy in patients with reversible causes or sometimes until spontaneous remission occurs. When medical therapy is inadequate, surgical therapy with optic nerve sheath fenestration or CSF drainage by lumboperitoneal or ventriculoperitoneal shunting may be necessary. Optic nerve sheath fenestration is preferred when visual loss is the issue because of its lower complication rate. However, when headaches are a major problem, it cannot be expected to relieve them. Pseudotumor cerebri in pregnancy raises some special issues. Pregnant women should not try to lose weight during the pregnancy, but weight gain should be carefully limited to 20 lb or less. Although not an established teratogen and probably safe during pregnancy, acetazolamide is best reserved until after the first trimester. If vision is stable, sometimes lumbar punctures can be used to temporize until delivery provides relief. However, when visual loss is progressive or when other effects of severe intracranial hypertension occur, then surgical decompression should be performed during pregnancy.
Investigational Studies In cases of suspected spontaneous intracranial hypotension, the diagnosis can be confirmed by lumbar puncture, which demonstrates a low ICP, generally less than 50 mm H20. CSF may be normal, but slight elevation of CSF protein and lymphocytic pleocytosis, consistent with relative flow stasis, may mimic CSF inflammatory and infectious disorders. Enhanced MRI typically reveals a diffuse dural enhancement, often accompanied by dural thickening, felt to represent engorgement of dural vasculature in the setting of reduced ICP. Additional findings can include subdural fluid collections and descent of the brain including downward displacement of the cerebellar tonsils. Radioisotope cisternography or contrast myelography can be used to detect sites of CSF leakage, often identified within the cervical or cervicothoracic regions.
Decision Making and Management In cases of iatrogenic intracranial hypotension occurring after dural puncture, the problem generally is self-limiting over the course of 2 to 4 days. Use of oral or intravenous hydration or caffeine has not consistently proven beneficial. Symptomatic headache relief can be achieved with the use of an abdominal binder to indirectly increase epidural venous pressure. The syndrome is most effectively treated with placement of an epidural blood patch, performed by inserting 10 to 20 mL of autologous blood into the epidural space in proximity to the level of the dural puncture. The procedure carries an initial success rate of greater than 90%. Spontaneous intracranial hypotension is a more elusive problem, but it can potentially be treated with a blood patch. This procedure has been successful both after localization of the dural leak and also blindly when no site of leakage can be identified. Surgical intervention to eliminate the source of the leak occasionally is warranted. Various other treatments have been advocated including complete bed rest for more than 2 weeks, continuous
Chapter 16
intrathecal or epidural saline infusions, and the conservative measures used to treat headaches after dural puncture. Shunts
Shunt Systems. Currently the commonly used systems for CSF diversion are ventriculoperitoneal,ventriculoatrial, ventriculopleural, and lumboperitoneal shunts. The most widely used is the ventriculoperitoneal shunt. The components of a typical CSF diversion system include the following: Proximal catheter: ventricular or lumbar catheter. A ventricular catheter is inserted into the right frontal horn via a right frontal or right parieto-occipital burr hole. A lumbar catheter for lumbar CSF diversion is an option in communicating hydrocephalus and carries the advantage of avoiding ventricular puncture and general anesthesia. However, lumbar shunts have a much greater tendency for obstruction and have generally fallen out of favor, except in conditions such as pseudotumor cerebri when the baseline ventricular size is small. Distal tubing. Silastic tubing is attached to the proximal catheter and tunneled subcutaneously to the distal site of drainage, that is, the peritoneal cavity (ventriculoperitoneal and lumboperitoneal shunts), the right atrium via the common facial vein (ventriculoatrial shunt), or the pleural cavity (ventriculopleural shunt). Valve. A valve is interposed between the proximal and distal shunt components, usually near the site of the ventricular catheter. It regulates the pressure and prevents retrograde flow of shunted CSF. Several valve designs exist, including spring-loaded, slit, or resistance valves, which vary by their mechanism of outflow regulation. These are fixed-pressure valves functioning at high, medium, or low settings. More recently, variable-pressure valves, which allow percutaneous adjustment of pressure settings, have become available. These valves allow the surgeon to fine-tune ICP in shunted patients without the need for reoperation. The ideal opening pressure of the valve for hydrocephalic patients is controversial. Ancillary components: ventricular reservoir and antisiphon device. Ventricular reservoirs are commonly placed proximal to the valve system in ventricular shunts and are generally palpable. They serve as an access for extracranial measurement of the ICP, CSF removal, and testing of the shunt system. When shunted patients are in an upright position, the ICP may become subatmospheric, leading to overdrainage. Antisiphon devices are designed to prevent intraventricular pressure from falling below atmospheric pressure at the level of the antisiphon device, thus preventing overdrainage.
Shunt-Related Complications. The most important shuntrelated complications are discussed in the following sections. OBSTRUCTION.Shunt obstruction can be insidious, intermittent, or sudden and presents with clinical deterioration indicative of shunt malfunction. The ventricular catheter may become obstructed by debris, coagulum, or contact with choroid plexus or brain secondary to decreased size of the ventricles. Proximal catheter obstruction is the most common cause of shunt
Hydrocephalus and Disorders of Cerebrospinal Fluid Flow
165
malfunction. The distal end may become blocked in ventriculoperitoneal shunts by omentum or peritoneal adhesions. Tapping a reservoir may confirm shunt obstruction and define where it is. Shunt blockage necessitates surgical exploration and revision. INFECTIO The N. rate of shunt infections in adults is less than 5%, which is lower than the rate in the pediatric population. Infection can manifest in several ways: wound infection at the site of shunt insertion, ventriculitis and meningitis, or secondary infection of the vascular system, including endocarditis (ventriculoatrial shunts) and peritoneal infection (ventriculoperitoneal shunts). However, most commonly, shunt infection presents insidiously as shunt malfunction, and typical findings of meningitis generally are not present. Most infections occur immediately after or within a few months of shunt insertion and generally are attributed to bacterial contamination during surgery. Shunt infection may also occur in the setting of systemic infection, such as pneumonia or urinary tract infection. The most common pathogens are Sraphylococcus epiderrnidis and, less often, Staphylococcus aureus, Pseudomonas aeruginosa, and Escherichia coli. The general approach to shunt infection is removal of the entire shunt system and external ventricular drainage until the infection has cleared after a full course of intravenous antibiotics. SUBDURAL COLLECTIONS.Collections of low-protein fluid, called subdural hygromas, may develop after placement of a shunt with low pressure. These probably represent effusions that develop in response to the excess space in the cranial vault unoccupied by brain matter. Subdural collections of blood or fluid generally are a result of overdrainage. Use of higher-pressure valves or variablepressure valves that allow graded ventricular decompression may decrease the incidence of this complication. For symptomatic collections, burr hole drainage is attempted initially. It may be necessary to temporarily clamp off the shunt so that the brain can expand and occlude the subdural space or to place a shunt catheter in the subdural collection. Subdural hematomas may form after the shunting of hydrocephalus as a result of tears in the cortical bridging veins when the brain matter has not yet adequately expanded to fully occupy the increased cranial space caused by fluid drainage. Even minor head trauma can increase the risk of subdural hematoma. Symptoms of overdrainage often mimic those of OVERDRAINACE. underdrainage; they include headache, nausea and vomiting, lethargy, diplopia, impaired upgaze, and visual impairment. However, unlike those of increased ICP, the symptoms of overdrainage typically are worse when the patient is upright and are relieved when lying down. Overdrainage can give rise to two distinct syndromes: the low ICP syndrome, which can be distinguished by positional measurement of ICP, and the slit ventricle syndrome, which is apparent on CT or MRI as reduction of the ventricles to subnormal size. The latter syndrome is more prominent in the pediatric population but may be seen in adults who were initially shunted at a young age. Encroachment of the ventricular walls onto the draining catheter leads to intermittent or complete CSF obstruction with accompanying signs and symptoms of suddenly increased ICP. For unclear reasons that may relate to decreased compliance of the system, the ventricles do not enlarge despite shunt obstruction. Both of these syndromes necessitate shunt revision with substitution of a new system, perhaps incorporating an antisiphon device or a valve with higher opening pressure. MECHANICAL FAILURE. Disconnection of shunt components or fracture of the Silastic tubing at stress points may occur, especially
166
Principles ofAmbulatoy Neurology and the Approach to Clinical Problems W
with head trauma. Palpation of the subcutaneous shunt tubing throughout its length may reveal a gap or bulge at the site of disconnection. A radiographic shunt series, comprising a selection of films showing anteroposterior and lateral views of the skull, chest, kidneys, ureter, and bladder and lateral views of the abdomen, depending on shunt type, can be helpful in determining the site of disconnection. Surgical exploration and revision are necessary in cases of mechanical failure. SHUNT Tm-SpEanc CoMmxnoNs. Ventricular shunts carry a small risk (approximately5%) of seizures;the incidence of seizures may be decreased with the use of an occipital rather than a frontal catheter. Prophylactic anticonvulsant medication is not indicated in routine management. Ventriculoatrial shunts carry the unique risk of thromboembolic episodes such as pulmonary embolism; with the shunt materials currently in use, these risks are small. Lumboperitoneal shunts often obstruct and have been associated with acquired tonsillar herniation. Evaluation of a Patient with Suspected Shunt Malfunction. Shunt malfunction must be suspected in patients presenting with headache, nausea and vomiting, lethargy, or visual changes. These patients should be evaluated for signs of increased ICP, including papilledema and abducens or upward gaze palsy. Alternatively, shunt malfunction may manifest as a recurrence of prior hydrocephalic symptoms, such as worsening of gait, memory, or incontinence. In fact, regression of clinical improvements at any time after shunt placement should raise the question of shunt malfunction. The clinical deterioration often is stereotyped in any one patient. Malfunction is most often a consequence of obstruction, infection, or malposition of the shunt system. On physical examination, palpation of the shunt tubing may reveal disconnection. Palpation and compression of the valve suggest blockage of the ventricular catheter if the valve can be compressed but refills very slowly, Blockage in the valve or distally is likely if the valve is incompressible. A normally working shunt should allow easy valve emptying and refill within 5 to 30 seconds. However, valve pumping is not considered to be a reliable indicator of shunt function, and some shunt systems have no palpable valve. A shunt series is of variable benefit because disconnection is an uncommon cause of shunt malfunction. It is indicated if there is clear suspicion of disconnection on examination. To determine the CSF pressure, lumbar puncture or tapping of the shunt reservoir can be performed. Lumbar puncture is preferable if it can be performed safely because shunt tapping carries a 1% risk of infection. A shunt tap should be considered an invasive procedure and necessitates meticulous attention to sterile technique. Neurosurgical consultation before the procedure is warranted. An attempt to withdraw CSF after puncture of the reservoir may help to localize the site of malfunction. Inability to withdraw suggests proximal obstruction at the level of the ventricular catheter. Easy withdrawal suggests distal obstruction. It is important to note that flushing of the system via shunt tap is unwise because it may further increase an already decompensating ICP. A shuntogram can be performed by injecting water-soluble iodine contrast dye into the reservoir, followed by serial radiographs over 30 minutes. The test is aimed at defining a site of obstruction and indicating the rate of dye clearance from the system. However, results often are inconclusive, and shuntograms are not commonly used. Ultimately, surgical exploration can identify the source of malfunction. It is important to exclude infection in any malfunction, so CSF should be analyzed at the time of lumbar puncture, shunt tap, or operative revision.
Principles of Diagnosis: Common Presenting Symptoms
SUGGESTED READINGS Adams RD, Victor M: Principles of Neurology. 5th Ed. McGraw-Hill, New York, 1993 Benzel EC, Pelletier AL., Levy PG Communicating hydrocephalus in adults: prediction of outcome after ventricular shunting procedures. Neurosurgery 26655, 1990 Black PM: Hydrocephalus and vasospasm following subarachnoid hemorrhage from ruptured intracranial aneurysm. Neurosurgery 18:12, 1986 Black PM, Hakim R, Olsen Bailey N The use of the Codman-Medos programmable Hakim valve in the management of patients with hydrocephalus: illustrative cases. Neurosurgery 3 4 1 110, 1994 Black PM, Ojemann RG, Tzouras A CSF shunts for dementia, incontinence and gait disturbances. Clin Neurosurg 32:632, 1985 Boon AJ, Tans JT, Delwel EJ et al: The Dutch normal-pressure hydrocephalus study. How to select patients for shunting: An analysis of four diagnostic criteria. Surg Neurol 53(3):201-207, 2000 Borgesen SE, Gjerris F The predictive value of conductance to outflow of CSF in normal pressure hydrocephalus. Brain 105:65, 1982 Brightball TC, Goodwin RS, Ford RG Magnetic resonance imaging of intracranial hypotension syndrome with pathophysiological correlation. Headache 40292-299, 2000 Corbett JJ, Digre K Idiopathic intracranial hypertension: an answer to, “the chicken or the egg?” Neurology 58:5-6, 2002 Crockard HA, Hanlon K, Duda EE, Mullan J F Hydrocephalus as a cause of dementia: evaluation by computerized tomography and intracranial pressure monitoring. J Neurol Neurosurg Psychiatry 40:736, 1977 Digre KB, Varner MW, Corbett JJ: Pseudotumor cerebri and pregnancy. Neurology 34721-729, 1984 Fisher C M Hydrocephalus as a cause of disturbancesof gait in the elderly. Neurology 32:1358, 1982 Friedman DI: Pseudotumor cerebri. Neurosurg Clin N Am 10609-621, 1999 Gallassi R, Morreale A, Montagna P et al: Binswanger’s disease and normal-pressure hydrocephalus: a clinical and neuropsychological comparison. Arch Neurol48:1156, 1991 Haan J, Thomeer RTWM: Predictive value of temporary external lumbar drainage in normal pressure hydrocephalus. Neurosurgery 22:388, 1988 Hakim R, Black PM: Correlation between lumboventricular perfusion and MRI-CSF flow studies in idiopathic normal pressure hydrocephalus. Surg Neurol4914-20, 1998 Hakim S, Adams RD: The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure: observations on cerebrospinal fluid hydrodynamics. J Neurol Sci 2:307, 1965 Hussey F, Schanzer B, Katzman R A simple constant-infusion manometric test for measurement of CSF absorption. 11. Clinical studies. Neurology 20:665, 1970 Jagust WJ, Friedland RP, Budinger TF: Positron emission tomographywith [ “F] fluorodeoxyglucosedifferentiates normal pressure hydrocephalus from Alzheimer-type dementia. J Neurol Neurosurg Psychiatry 4 8 1091, 1985 Kamiya K, Yamashita N, Nagai H, Mizawa I: Investigation of normal pressure hydrocephalus by 1231-IMPSPECT. Neurol Med Chir 31:503, 1991 Katayama S, Asari S, Ohmoto T Quantitative measurement of normal and hydrocephalic cerebrospinal fluid flow using phase contrast cine MR imaging. Acta Med Okayama 47:157, 1993 Katzman R Low pressure hydrocephalus. In Wells CD (ed.): Dementia. FA Davis, Philadelphia, 1977 Larsson A, Jensen C, Bilting M et al: Does the shunt opening pressure influence the effect of shunt surgery in normal pressure hydrocephalus? Acta Neurochir (Wien) 117:15, 1992 Larsson A, Wikkelso C, Bilting M, Stephensen H: Clinical parameters in 74 consecutive patients shunt operated for normal pressure hydrocephalus. Acta Neurol Scand 84475, 1991 Mascalchi M, Ciraolo L, Bucciolini M et al: Fast multiphase MR imaging
Chapter 17
of aqueductal CSF flow: 2. Study in patients with hydrocephalus.AJNR 11:597, 1990 McQuarrie IG, Saint-Louis L, Scherer PB: Treatment of normal pressure hydrocephalus with low versus medium pressure cerebrospinal fluid shunts. Neurosurgery 15:484, 1984 Miyake H, Ohta T, Kajimoto Y et ak Diamox challenge test to decide indications for cerebrospinal fluid shunting in normal pressure hydrocephalus. Acta Neurochir 141:1187-1193, 1999 Morgan MK, Johnston IH, Spittaler PJ: A ventricular infusion technique for the evaluation of treated and untreated hydrocephalus. Neurosurgery 29832, 1991 Nitz WR, Bradley WG, Watanabe AS et al: Flow dynamics of cerebrospinal fluid assessment with phase-contrast velocity MR imaging performed with retrospective cardiac gating. Radiology 183:395, 1992 OCarroll CP, Brant-ZawadzkiM: The syndrome of spontaneous intracranial hypotension. Cephalalgia 19:8&87, 1999 Puca A, Anile C, Maira G, Rossi G: Cerebrospinal fluid shunting for hydrocephalus in the adult: factors related to shunt revision. Neurosurgery 29322, 1991 Pudenz RH, Foltz E L Hydrocephalus: overdrainage by ventricular shunts: a review and recommendations. Surg Neurol35:200, 1991 Raftopoulos C, Chaskis C, Delecluse F et ak Morphological quantitative analysis of intracranial pressure waves in normal pressure hydrocephalus. Neurol Res 14389, 1992 Roman G C White matter lesions and normal-pressure hydrocephalus: Binswanger’s disease or Hakim syndrome?AJNR 12:40, 1991 Shiino A, Matsuda M, Morikawa S et ak Proton magnetic resonance spectroscopy with dementia. Surg Neurol39: 143, 1993 Sindou M, Guyotat-Pelissou, Chidiac A, Goutelle A Transcutaneous pressure adjustable valve for the treatment of hydrocephalus and
17
Traumatic Brain Injury
167
arachnoid cysts in adults: experience with 75 cases. Acta Neurochir (Wien) 121:135, 1993 Sorensen PS, Jansen EC, Gjerris F Motor disturbance in normal-pressure hydrocephalus: special reference to stance and gait. Arch Neurol 143:34, 1986 Sudarsky L, Ronthal M: Gait disorders among elderly patients: a survey study of fifty patients. Arch Neurol40740, 1983 Symon L, Dorsch NWC Use of long-term intracranial pressure measurement to assess hydrocephalic patients prior to shunt surgery. J Neurosurg 42:258, 1975 Tam& N, Nagashima T, Ehara K et ak Hydrocephalic oedema in normal-pressure hydrocephalus. Acta Neurochir 51(Suppl):348, 1990 Vanneste J, Augustin P, Davies GAG et ak Normal-pressure hydrocephalus: is cisternography still useful in selecting patients for a shunt? Arch Neurol 49:366, 1992 Vanneste J, Augustin P, Dirven C et ak Shunting normal-pressure hydrocephalus:do the benefits outweigh the risks? A multicenter study and literature review. Neurology 42:54, 1992 Waldemar G, Schmidt JF, Delecluse F et ak High resolution SPECT with 99MTc-d,l-HMPAO in normal pressure hydrocephalus before and after shunt operation. J Neurol Neurosurg Psychiatry 56:655, 1993 Welch K, Shillito JS, Strand R et ak Chiari I malformation: an acquired disorder? J Neurosurg 55:604, 1981 Wikkelso C, Anderson H, Bloomstrand C, Lindqvist G The diical effect of lumbar puncture in normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 45:64, 1982 Wood JH, Bartlet D, James AE, Udvarhelyi G B Normal-pressure hydrocephalus: diagnosis and patient selection for shunt surgery. Neurology 24517, 1974
Traumatic Brain Injury Michael P. Alexander
This chapter covers three aspects of traumatic brain injury (TBI) that may involve neurologists: the mild injury in the emergency room, the spectrum of problems of severe TBI, and the office management of mild TBI, including that of the patient who never recovers.
ACUTE MANAGEMENT OF munmnc BRAIN INJURY In the United Kingdom 10% of all emergency room visits are for TBI, mostly minor. Of the patients with minor TBI, most have no neurologic deterioration and do not need hospital care. Approximately 2% deteriorate and may need neurosurgical management. As summarized by Vollmer and coworkers (1991), “the major practical problem in [minor TBI] involves developing a management scheme that prevents delay in treatment of the small number of intracranial complications without causing excessive rates of hospitalization, inconvenience, and cost to the vast majority of patients.” In the mid-1980s in both the United Kingdom and the United States, multidisciplinary groups proposed management schemes. During the same decade, prospective studies from Scotland provided data sufficient to stratify overall risk for different segments of the minor TBI population. This stratification of risk has been supported by several additional investigations. The large prospective series carried out by Teasdale and colleagues (1990) in Glasgow illuminates the real locus of risk. A
Glasgow Coma Scale (GCS) score of 15 with no skull fracture carries a 1 in 6000 risk of deterioration. A GCS score of 15 with a skull fracture carries a risk of 1 in 32. A GCS score of 13 or 14 without skull fracture has a risk of 1 in 21, but with skull fracture the risk increases to 1 in 4. In the entire group, a skull fracture alone raises the risk of deterioration 400-fold. Studies from the United States also demonstrate the substantially lower risk of deterioration in the GCS 15 group (approximately 2% overall in several studies) compared with the GCS 13 or 14 group. Most investigators now do not consider a patient with a GCS score of 13 or 14, that is, with any impairment of consciousness in the emergency room, as a minor, low-risk case. The Glasgow Coma Scale is given in Table 17-1. In the United Kingdom, Shackford and colleagues (1992) identified several criteria as the indicators of increased risk, and it is recommended that any patient with even one criterion be admitted for observation and computed tomography (CT) scanning. These criteria are as follows: Confusion o r altered level of consciousness in the emergency room (i.e., GCS 13 to 14) Skull fracture Neurologic signs or severe headache or vomiting Difficult assessment (e.g., young age, intoxication) Other high-risk medical conditions (e.g., use of anticoagulants) N o reliable home observer
Chapter 17
of aqueductal CSF flow: 2. Study in patients with hydrocephalus.AJNR 11:597, 1990 McQuarrie IG, Saint-Louis L, Scherer PB: Treatment of normal pressure hydrocephalus with low versus medium pressure cerebrospinal fluid shunts. Neurosurgery 15:484, 1984 Miyake H, Ohta T, Kajimoto Y et ak Diamox challenge test to decide indications for cerebrospinal fluid shunting in normal pressure hydrocephalus. Acta Neurochir 141:1187-1193, 1999 Morgan MK, Johnston IH, Spittaler PJ: A ventricular infusion technique for the evaluation of treated and untreated hydrocephalus. Neurosurgery 29832, 1991 Nitz WR, Bradley WG, Watanabe AS et al: Flow dynamics of cerebrospinal fluid assessment with phase-contrast velocity MR imaging performed with retrospective cardiac gating. Radiology 183:395, 1992 OCarroll CP, Brant-ZawadzkiM: The syndrome of spontaneous intracranial hypotension. Cephalalgia 19:8&87, 1999 Puca A, Anile C, Maira G, Rossi G: Cerebrospinal fluid shunting for hydrocephalus in the adult: factors related to shunt revision. Neurosurgery 29322, 1991 Pudenz RH, Foltz E L Hydrocephalus: overdrainage by ventricular shunts: a review and recommendations. Surg Neurol35:200, 1991 Raftopoulos C, Chaskis C, Delecluse F et ak Morphological quantitative analysis of intracranial pressure waves in normal pressure hydrocephalus. Neurol Res 14389, 1992 Roman G C White matter lesions and normal-pressure hydrocephalus: Binswanger’s disease or Hakim syndrome?AJNR 12:40, 1991 Shiino A, Matsuda M, Morikawa S et ak Proton magnetic resonance spectroscopy with dementia. Surg Neurol39: 143, 1993 Sindou M, Guyotat-Pelissou, Chidiac A, Goutelle A Transcutaneous pressure adjustable valve for the treatment of hydrocephalus and
17
Traumatic Brain Injury
167
arachnoid cysts in adults: experience with 75 cases. Acta Neurochir (Wien) 121:135, 1993 Sorensen PS, Jansen EC, Gjerris F Motor disturbance in normal-pressure hydrocephalus: special reference to stance and gait. Arch Neurol 143:34, 1986 Sudarsky L, Ronthal M: Gait disorders among elderly patients: a survey study of fifty patients. Arch Neurol40740, 1983 Symon L, Dorsch NWC Use of long-term intracranial pressure measurement to assess hydrocephalic patients prior to shunt surgery. J Neurosurg 42:258, 1975 Tam& N, Nagashima T, Ehara K et ak Hydrocephalic oedema in normal-pressure hydrocephalus. Acta Neurochir 51(Suppl):348, 1990 Vanneste J, Augustin P, Davies GAG et ak Normal-pressure hydrocephalus: is cisternography still useful in selecting patients for a shunt? Arch Neurol 49:366, 1992 Vanneste J, Augustin P, Dirven C et ak Shunting normal-pressure hydrocephalus:do the benefits outweigh the risks? A multicenter study and literature review. Neurology 42:54, 1992 Waldemar G, Schmidt JF, Delecluse F et ak High resolution SPECT with 99MTc-d,l-HMPAO in normal pressure hydrocephalus before and after shunt operation. J Neurol Neurosurg Psychiatry 56:655, 1993 Welch K, Shillito JS, Strand R et ak Chiari I malformation: an acquired disorder? J Neurosurg 55:604, 1981 Wikkelso C, Anderson H, Bloomstrand C, Lindqvist G The diical effect of lumbar puncture in normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 45:64, 1982 Wood JH, Bartlet D, James AE, Udvarhelyi G B Normal-pressure hydrocephalus: diagnosis and patient selection for shunt surgery. Neurology 24517, 1974
Traumatic Brain Injury Michael P. Alexander
This chapter covers three aspects of traumatic brain injury (TBI) that may involve neurologists: the mild injury in the emergency room, the spectrum of problems of severe TBI, and the office management of mild TBI, including that of the patient who never recovers.
ACUTE MANAGEMENT OF munmnc BRAIN INJURY In the United Kingdom 10% of all emergency room visits are for TBI, mostly minor. Of the patients with minor TBI, most have no neurologic deterioration and do not need hospital care. Approximately 2% deteriorate and may need neurosurgical management. As summarized by Vollmer and coworkers (1991), “the major practical problem in [minor TBI] involves developing a management scheme that prevents delay in treatment of the small number of intracranial complications without causing excessive rates of hospitalization, inconvenience, and cost to the vast majority of patients.” In the mid-1980s in both the United Kingdom and the United States, multidisciplinary groups proposed management schemes. During the same decade, prospective studies from Scotland provided data sufficient to stratify overall risk for different segments of the minor TBI population. This stratification of risk has been supported by several additional investigations. The large prospective series carried out by Teasdale and colleagues (1990) in Glasgow illuminates the real locus of risk. A
Glasgow Coma Scale (GCS) score of 15 with no skull fracture carries a 1 in 6000 risk of deterioration. A GCS score of 15 with a skull fracture carries a risk of 1 in 32. A GCS score of 13 or 14 without skull fracture has a risk of 1 in 21, but with skull fracture the risk increases to 1 in 4. In the entire group, a skull fracture alone raises the risk of deterioration 400-fold. Studies from the United States also demonstrate the substantially lower risk of deterioration in the GCS 15 group (approximately 2% overall in several studies) compared with the GCS 13 or 14 group. Most investigators now do not consider a patient with a GCS score of 13 or 14, that is, with any impairment of consciousness in the emergency room, as a minor, low-risk case. The Glasgow Coma Scale is given in Table 17-1. In the United Kingdom, Shackford and colleagues (1992) identified several criteria as the indicators of increased risk, and it is recommended that any patient with even one criterion be admitted for observation and computed tomography (CT) scanning. These criteria are as follows: Confusion o r altered level of consciousness in the emergency room (i.e., GCS 13 to 14) Skull fracture Neurologic signs or severe headache or vomiting Difficult assessment (e.g., young age, intoxication) Other high-risk medical conditions (e.g., use of anticoagulants) N o reliable home observer
168
Principles ofAmbulatoy Neurology and the Approach to Clinical Problems W
W TABU 17-1. The Clasgow Coma Scale
Eye Opening None
To pain To speech Spontaneous
1 2
3 4
Not attributable to ocular swelling Pain stimulus is applied to chest or limbs Nonspecific response to speech or shout, does not imply the patient obeys command to open eyes Eyes are open, but this does not imply intact awareness
Motor Response
No response Extension
1 2
Abnormal flexion
3
Withdrawal
4
Localized pain
5
Obeys commands
6
Flaccid "Decerebrate." Adduction, internal rotation of shoulder, and pronation of the forearm "Decorticate." Abnormal flexion, adduction of the shoulder Normal flexor response; withdraws from pain stimulus with abduction of the shoulder Pain stimulus applied to supraocular region or fingertip causes limb to move so as to attempt to remove it Follows simple commands
Using the U.K. criteria, all 5 patients would have been admitted for observation or CT scanning: 4 for focal signs and 1 for intoxication. (Recall that all 310 were actually admitted.) Using the U.S. criteria, 4 would have had immediate CT scan (focal signs), and 1 would have been observed. It is impossible to predict how many others would have been observed. Servadei and associates (1993) reported 113 patients with GCS scores of 15 who were referred to a neurosurgical center because of a positive CT scan; 95% also had a skull fracture on radiograph. The 5 patients without fracture included 4 with ''small'' hemorrhages not necessitating surgery and 1 child who would have been observed or had a CT scan by both U.S. and U.K. criteria. This is a clinical management problem that every hospital with an emergency room probably should resolve through a quality improvement project. The current literature supports the following scheme (Fig. 17-1): Any patient with minor TBI with focal signs or GCS scores of 13 or 14 (i.e., altered mental state) in the emergency room should have a head CT scan. Patients with GCS 15 and no focal signs should be sent home if there was no loss of consciousness or amnesia, there are no worrisome medical issues, there is no intoxication, they are older than 14 years, and the home setting is secure. Patients with a GCS score of 15 and no focal signs but had unequivocal loss of consciousness and amnesia should have a CT or, if not available, plain skull radiography. If CT is negative, patients should be sent home. If skull radiographs are negative for fracture and if there are no medical issues, patients may be sent home. If plain films demonstrate a skull fracture, patients should be sent for CT or be kept for observation depending on relative costs, time of day, and local preferences.
Verbal Response
Self-explanatory Moaning and groaning but no recognizable words Intelligible speech (e.g., shouting or swear3 inappropriate ing) but no sustained or coherent conversation 4 Patient responds to questions in a converConfused sational manner, but the responses indicate varying degrees of disorientation and confusion 5 Normal orientation to time, place, and Oriented Derson Summed Glasgow Coma !kale Score = E + M + V (3 to 15). No response incomprehensible
1 2
In the United States, Masters and colleagues (1987) proposed a three-tiered strategy. For the mildest cases with no loss of consciousness, a normal neurologic examination, and no clinical signs of basilar skull fracture, discharge to home is appropriate. For patients with a history of loss of consciousness and amnesia but with normal examination results, extended observation and consideration of CT are recommended. For patients with GCS scores of 13 or 14 or with focal signs, immediate CT is indicated. There are problems with both sets of recommendations. The U.K. criteria generate a large number of admissions. The patients probably are not closely observed, given the low risk of clinical problems, and the high number of admissions are costly. Recent analysis suggests also that the criteria are too easily ignored, often just to avoid the paperwork of admissions in a low-risk group. The U.S. criteria probably underestimate the value of skull radiographs in narrowing the population at risk. The U.S. criteria for moderate cases ignore the large number of likely missed skull fractures with the markedly increased risk of possible deterioration. It has also been difficult to implement the use of these criteria. Recent studies clarify how these apparently different approaches, which entail observation, skull radiographs, and CT scans, result in fairly similar outcomes. Taheri and coworkers (1993) in the United States reported 310 consecutive admissions with a GCS score of 15; 5 (1.6%) patients deteriorated (i.e., needed neurosurgery). AU 5 patients who deteriorated were among the 10 patients with skull fracture. Of the 273 patients who had skull radiographs but no fracture, there were no delayed deteriorations.
Principles of Diagnosis: Common Presenting Symptoms
Shackford's group, in their major multicenter U.S. study, used a retrospective analysis of the role of CT in minor TBI assessment and came to similar conclusions, although the nature of the study limits its utility for prospective management decisions. A more important discovery was the frighteningly high number of admitted patients (30.2%) who had no documentation of any follow-up neurologic examination. CT scanning is the practice preference. In small hospitals without CT, local preferences should be spelled out as specific practice guidelines, and a quality improvement committee should follow compliance for risk management purposes. BEHAVIORAL NEUROLOGY OF SEVERE TRAUMATIC BRAIN INJURY
Patients with severe TBI usually are treated by neurosurgeons, often in the intensive care unit when they need respiratory assistance. There are only a few points to note regarding acute care: H
H
There is no definite role for prophylactic anticonvulsants beyond the first week after the injury. The value of dexamethasone is unknown. Even hyperventilation is of uncertain overall value, balancing reduced edema against vasoconstriction with possible ischemia, although it is always reasonable management. New classes of agents that may reduce or block cell death in the acute period are under study, and these may become available in the near future.
Chapter 17
ER GCS 13-14
ER GCS 15 FOCAL SIGNS
ER GCS 15 NO FOCAL SIGNS UNEQUIVOCAL LOC OR AMNESIA
ER NO NO NO
W
Traumatic Brain lnjuty
169
GCS 15 FOCAL SIGNS LOC AMNESIA
\ El
FRACTURE PRESENT
\N O
MEDICAL PROBLEMS AGE 14
F R AC T u R E
-1NTOXlCATlON
- NO TO ALL
POOR HOME SETTING
I
\ pKl
YES TO ANY
0 BSERVATION FIG. 17-1. Suggested emergency room (ER) management of mild TBI. Cr, computed tomography; CCS, Clasgow Coma Scale; LOC, loss of consciousness.
A specific diagnosis of the injury type is needed for the neurologic treatment of severe TBI survivors at a rehabilitation center. DiffuseAxonal Injury
Sudden acceleration-deceleration is the most important physical agent of TBI. Powerful inertial forces are generated. The microscopic structure of the brain leaves it most susceptible to inertial shear injury. Shearing disrupts axons and small blood vessels. Axonal disruptions lead to eventual cell death and, perhaps, to downstream neuronal injury from release of excitatory neurotransmitters. Small blood vessel injury can produce simple petechial hemorrhages, which are maximal in parasagittal white matter-increasing centripetally from the cortex to deep white matter-or focal or diffuse edema. This entire neuropathologic picture is called diffuse axonal injury, and clinical severity is directly related to the extent of neuronal and vascular damage. Recovery from diffuse axonal injury is highly correlated with several measures of injury severity, including GCS, duration of coma, and duration of post-traumatic amnesia. The clinical evolution of diffuse axonal injury beginning with coma follows characteristic stages: 1. Coma: no eye opening, no verbalization, no meaningful
response
have no motor impairments, severe cases may include a variety of motor deficits reflecting parasagittal, deep white matter lesions, superior cerebellar outflow and midbrain tegmental lesions, and, in the most severe cases, deeper brainstem lesions. As a rule, patients should receive inpatient rehabilitation until the transition from stage 5 to stage 6, from which point they can be treated at home. The transition from coma to functional competence depends on the severity of diffuse axonal injury. The mildest possible diffuse axonal injuries probably are “ding” injuries in sports. Careful assessment of a well-motivated patient with “ding” demonstrates recovery over 7 to 10 days. For injuries with brief loss of consciousness and 20 to 60 minutes of post-traumatic amnesia, the common concussion, the recovery period probably is 1% to 6 months. For more severe mild TBI with post-traumatic amnesia lasting longer than 60 to 90 minutes (GCS 13 or 14), recovery might take 4 to 12 months. As severity measures increase, recovery takes longer. These times are much longer than most neurologists realize. Recovery in this context refers to demonstrable cognitive and motor deficits. In many cases, recovery really means “resolution of all deficits.” In others, usually among more severe injuries, recovery means reaching a stable plateau of residual deficits. In all patients normal processes of adaptation, learning, and plasticity allow lifelong improvement of function. Only the most severe cases stall at stages 2 through 5.
2. Unresponsive wakefulness: eye opening (vegetative state) 3. Mute vigilance: watchful, irregular - direct responsiveness
F o a l Cerebral Contusions
Note that even at stage 7, there may be residual cognitive impairments. Although many patients with diffuse axonal injury
In addition to diffuse axonal injury, TBI can cause focal cerebral contusions. These may occur directly at a point of contact, but most are caused by inertial forces driving the basal frontal and temporal cortex into rough adjacent bony surfaces. Focal cerebral contusions are abrasions that originate in cortex, include disruption of vascular structures, and may cause physical disruption, ischemic injury, or hemorrhagic injury of adjacent white matter. , These abrasions may be seen anywhere, but the inferior and anterior temporal and orbital and polar frontal regions are most
I
4. Responsive confusional state: severe impairment in attention and memory, which may be quiet, agitated, or fluctuating 5. Oriented cognitive impairment: recovered day-to-day memory and usually independent basic self-care (physical limitations allowing) 6. Supervised functional independence 7. Independent functional competence
I
.
170
hinciples of Ambulatory Neurology and the Approach to Clinical Problems
common. Focal cerebral contusions have very poor correlation with the markers for severity of diffuse axonal injury, that is, the initial GCS score and loss of consciousness. In fact, patients with focal cerebral contusions may never, or only transiently, have been unconscious; that is, they may have had apparently minor TBI. Patients with multiple focal cerebral contusions, especially those with accompanying subdural hematomas, have a very high mortality rate. The clinical profile of focal cerebral contusions depends on location, number, and size. In the most common locations, behavioral problems predominate. Damage to orbital frontal cortex produces poor regulation of emotions with overreactivity, irritability, social disruptiveness, and lability. Damage to the polar frontal cortex produces impaired complex, motivated behaviors with shallow and distractible problem solving and disorganized complex social behaviors. Recovery depends on size, depth, and number of these contusions; they are often bilateral and symmetrical. The timing of recovery is similar to other focal destructive lesions, such as infarcts and hemorrhages. Recovery is potentially rapid for 2 to 4 months and then is flatter. It is important to note the similarity between the cognitive clinical profiles of late severe diffuse axonal injury and frontal focal cerebral contusions and also to note the markedly different probabilities of very late recovery between severe diffuse axonal injury (good) and focal cerebral contusions (poor). Hypoxic-Ischemic Injury
Although diffuse axonal injury and focal cerebral contusions are the defining injuries of TBI, hypoxic-ischemic injury is also, common in more severe cases and in certain cases of herniation, often from epidural hematomas. DiKuse hypoxic-ischemic injury is caused by a mixture of factors, including edema, increased intracranial pressure, local vascular damage, and systemic shock or chest or airway injury impairing ventilation; there may be no specific clinical markers beyond clinical suspicion. Diffuse hypoxic-ischemic injury has a dramatically worse prognosis for recovery for any given duration of loss of consciousness, falling to essentially zero when the loss of consciousness associated with this injury lasts for 7 days. Focal hypoxic-ischemic injury usually is caused by posterior cerebral artery entrapment lesions caused by herniation. Clinical consequences are the same as those predicted for more common posterior cerebral artery infarctions and depend on whether it is temporal or occipital and whether it is left, right, or bilateral. Recovery patterns mimic infarctions of more common origins. Mixed Pathologies Many patients have a mixture of pathologies, with GCS scores determined by severity of diffuse axonal injury or severity of early herniation. Duration of coma is determined by severity of diffuse axonal injury or hypoxic-ischemic injury. Post-traumatic amnesia is determined by severity of diffuse axonal injury, severity of diffuse hypoxic-ischemic injury, or location of focal cerebral contusions. Long-term outcome is determined by severity of diffuse axonal injury and diffuse hypoxic-ischemic injury and by location, size, and number of focal cerebral contusions and focal hypoxic-ischemic injury. The long-term prospects of patients over 40 years old are delayed and constrained. Patients with severe TBI seen months to years after injury and after acute rehabilitation may present because of seizures or some
Principles of Diagnosis: Common PresentingSymptoms
other neuromedical problem such as headaches or spasticity, because of behavioral or cognitive problems, or for advice about the next stages in rehabilitation. Competence in detailed mental status assessment and absolute clarity about the relative role of diffuse axonal injury and focal cerebral contusions in the clinical profile are necessary for behavioral and cognitive diagnoses because of their differing prognoses. If not previously performed, magnetic resonance imaging (MRI) is essential. It has advantages in revealing old focal cerebral contusions, particularly for demonstrating basal focal cerebral contusions without bone artifact, and for demonstrating residual signs of petechial hemorrhages from diffuse axonal injury (paramagnetic foci). Neuropsychological assessment is essential in characterizing cognitive limits and strengths. Treatment
Treatment issues that arise in the late assessment of patients with severe TBI are of two types: retraining or remediation and behavioral. The late rehabilitation recommendations are determined by three factors: the patient’s profile of deficits, the probable prognosis for improvement and learning as determined by the neuropathology, and financial, personal, and social resources. Rehabilitation of severe TBI is emotionally draining for patients and families. It is expensive and may take a long time and enormous patience. As noted earlier, the deficits usually are predominantly cognitive and behavioral. Neuropsychological and neuropsychiatric assessment are essential to proper characterization. Postacute rehabilitation of cognitive deficits takes several possible forms. There are programs that attempt to combine direct treatment of cognitive deficits with compensatory strategies for the patient, family, and workplace or school. The claims of direct treatment of attentional, memory, or other cognitive deficits are controversial for three reasons. First, it has been hard to demonstrate efficacy beyond natural recovery. Second, it has been difficult to demonstrate generalization of any recovered process for tasks beyond those trained. Third, the treatment tasks often lack common sense. If you want a patient to be able to work as a receptionist again, why have that patient do computer vigilance tasks? Why not do simplified “receptionist vigilance” tasks? Programs of direct treatment often are called cognitive rehabilitation, and they demand skepticism. The only class I study of this form of cognitive rehabilitation was unable to show any benefit, despite an adequate sample size, excellent compliance, careful follow-up, and psychosocial support. A second type of program emphasizes the compensation strategies and directly treats only tasks of functional relevance, such as budgeting, handling checks, riding public transportation, and filling out applications. These programs do not suffer from the three weaknesses of direct treatment programs, but they must be judged by how they match treatment goals with reasonable neurological prognoses and the patients’ real-life needs. These programs may also be called cognitive rehabilitation. The two types of programs differ in the claims that they make for treatment. Physicians should know the structure of the programs to which they refer patients. For some patients behavioral disorders are a primary obstacle to functional recovery. Behavioral management also depends on precise diagnosis. Only a taste of the diagnostic dilemmas can be presented here. For instance, does a patient with a unilateral frontal polar contusion have low motivation because of limitations
Chapter 17
in higher-order mental processes such as goal setting, setting mental representation of strategies to goals, or organizing complex activities? Or is the patient depressed? Or both? Does a patient with disinhibition and intrusive behavior have an attentional problem related to severe diffuse axonal injury, to orbitofrontal injury, to anxiety, or to a combination of these? Neuropsychiatric assessment may clarify these questions. Treatment may involve behavioral treatment, perhaps cognitively based, as in the second program type described above, or perhaps behaviorally based. Treatment may also be pharmacologic. There are two overriding lessons about drug treatment. First, there are no magic potions for the patient with TBI. For every patient with periodic agitation who responds to haloperidol, there is another who does not but who responds to benzodiazepines. There are concrete reasons not to use all known drugs in patients with TBI, such as motor side effects or worsened alertness. Claims for several generations of mood regulators in TBI, such as carbamazepine, propanolol, and valproic acid are only weakly supported. Second, when a clear psychiatric disorder is established, even if it is believed to be neurogenic, treatment should start with the same agents that have been efficacious in the purely psychiatric form of the disorder. Patients with severe diffuse axonal injury often can make good functional recovery even if their basic neurologic deficits and limitations do not change. Careful use of progressively more demanding rehabilitation programs leading to vocational and educational programs is always justified. Patients with substantial frontal focal cerebral contusions typically do not benefit greatly, but behavioral and compensatory strategies may improve their function within a particular setting if realistic goals are set.
BEHAVIORAL NEUROLOGY OF MINOR TRAUMATIC BRAIN INJURY
As reviewed earlier, minor TBI is defined by injury characteristics, not by outcome characteristics. Some patients with minor TBI have a bad functional outcome, and some with severe TBI have an excellent outcome; the outcome does not define the injury. As mentioned earlier, there is no reliable biologic marker for severity, although functional imaging or cognitive evoked potentials may yet provide such a marker. At present, minor TBI is defined by a melange of clinical measures: GCS at first examination, duration of loss of consciousness, and duration of post-traumatic amnesia. There are patients with minor TBI by those measures who have intracerebral hemorrhages, or “complicated minor TBI.” Complicated cases should be set aside from this discussion and considered as part of the spectrum of severe TBI. As outlined earlier, it is currently believed that diffuse axonal injury underlies all of these injuries, with minor TBI cases simply having less injury than severe ones. There may be crucial idiosyncratic differences in the location of diffuse axonal injury between cases that account for differences in outcome, but at present these potential differences cannot be detected clinically or with imaging. This uncertainty should induce humility in clinicians willing to write off deficits as psychogenic. Although it is customary to view GCS scores of 13 to 15 as minor, both in the emergency room and in outcome, there are probably differences between patients who have a GCS score of 15 and those who have GCS scores of 13 or 14. The mildest TBIs are the “ding” injuries and, perhaps, the pure inertial injuries from whiplash without loss of consciousness. In the modal mild TBI, there is brief loss of consciousness (less than 1 to 2 minutes),
Traumatic Brain Injury
171
post-traumatic amnesia, including much of the accident scene or even transport to the emergency room (20 to 60 minutes), and a GCS score of 15 in the emergency room. Retrograde amnesia often is remarkably brief if inquired about after post-traumatic amnesia has cleared. In more severe mild TBI, loss of consciousness may last up to 1 hour and post-traumatic amnesia up to 24 hours, and GCS scores may be 13 or 14 in the emergency room. These cases clearly shade into severe TBI with GCS scores of 11 to 12 and post-traumatic amnesia of 1 to 2 days. The more prolonged the injury measures, the more severe the injury. This discussion briefly covers four topics: the natural history of neurologic recovery; the other injuries associated with brain injury, such as head and neck, vestibular, and psychological injuries, that together produce the postconcussive syndrome; the natural history of postconcussive syndrome; and the persistent postconcussive syndrome. Neurologic Recovery The primary neurologic deficits of minor TBI are in attention and memory. It is arguable that other deficits, in complex mental operations often called executive functions and in behavioral regulation, are caused by these two primary deficits. Many patients also complain of sleep disorders. This may represent primary damage to sleep structures, or it may be caused by superimposed pain states, medications, enforced inactivity,or attentional deficits. Numerous studies have demonstrated that recovery of attention and memory takes a long time even in the mildest cases. “Ding” injuries seem to take 7 to 10 days to recover. The modal cases may take 1% to 6 months. Increasing age above 40 years may prolong these times. In the last few years there have been numerous reports on mild TBI in athletes. Boxing, soccer, football, and hockey have high rates of concussion. The major consequences in these patients probably result from the number of actual concussions, not the cumulative occurrence of nonconcussive head injuries. The time to recover from these mild “ding” injuries, even in wellconditioned, young, highly motivated athletes, is several days. During that time reaction times are prolonged, and the risk of additional injury is high. This is the rationale for restricting risk even in apparently unaffected or recovered subjects for at least a few days. Whether a second concussion shortly after the first can produce catastrophic brain injury (“second impact syndrome”),at least in adults, is controversial, but a second concussion before an earlier concussion has recovered greatly prolongs recovery time. In the later stages of recovery, deficits may be subtle, and well-designed tasks, such as information processing, choice reaction times, and stressed recall tasks, may be needed to demonstrate them. Some patients may even have effectively recovered and still show subtle deficits. The more subtle the deficits, the more they are affected by situational, psychological, comorbid medical, and premorbid personal factors. The same mild deficit in sustained attention may be much more symptomatic in a 46-year-old police officer with daily headaches and a sick spouse than in a 19-year-old part-time student who is otherwise asymptomatic and living with parents. There is no formula that maps neuropsychologicaldeficits (at least mild ones) directly onto functional status. There are no known treatments that accelerate recovery. Note that the times to recover are much longer than the “few days’ rest” often prescribed. The key management action is to arrange sufficient time for recovery, allowing for comorbid injuries, age, and employment status.
172
Principles of Ambulatoy Neurology and the Approach to Clinical Problems
Injuries Associated with PostconcussiveSyndrome
When heads hit windshields, more than the brain may be injured. The head may be injured, with lacerations, abrasions, fractures, and other injuries. The peripheral vestibular system may be disrupted. The neck may be strained. For that matter, systemic injuries may be severe enough to cause the minor TBI to be overlooked as care is directed to other life-threatening injuries. Finally, patients with mild TBI may have an experience that patients with severe TBI never have. They may remember the injury circumstances if not the actual point of injury. The psychological traumas-anxiety, fear, guilt-are accessible to many patients with mild TBI. Headache, cervical strain, and peripheral vestibular disorders are dealt with elsewhere in this text, but a few points relevant to TBI should be mentioned here. Patients with evidence of cervical soft tissue injury need early appropriate symptomatic treatment: limited immobilization, including cervical pillows, physical therapy, and analgesics. The emergence of headaches unrelated to simple local trauma is nearly universal after minor TBI. Most of these clear in days to weeks, and simple analgesics are sufficient. Acute peripheral vestibular injury can be treated with rest and vestibular suppressants, such as clonazepam, although sedation may be an unacceptable side effect in these patients, and the medications may slow adaptation and recovery. Patients with severe psychological trauma, including feelings of responsibility for a fatality, nightmares, or avoidance behaviors, should receive early counseling. Depression and anxiety have independent incidences of more than 40% in the first 6 months after concussion. The likely time course of recovery must be established early. Patients should understand the high probability of recovery, but they should receive assistance during this time. Natural History of Postconcussive Syndrome
The interaction of neurologic deficits, pain, vestibular injury, psychological trauma, other systemic injuries, and psychosocial disruptions, such as financial loss, temporary unemployment, and increased time at home, is the postconcussive syndrome. The most common symptoms are headache, poor memory, poor sleep, poor concentration, dizziness, anxiety, depression, and a variety of sensory sensitivities (e.g., photophobia, positional vertigo, hyperacusis). Most are multifactorial. Symptoms decline after the first few weeks to 40% to 50%, after a few months to 30%, and by 1 year to 15% to 20%. Treatment was discussed earlier in this chapter. The neurologic injury takes time to heal. Symptomatic treatment of other injuries is essential. Psychological counseling may be needed. A plan for gradual restitution of preinjury activities will prevent patients from returning too quickly and failing or from struggling in their routine activities and thus increasing psychological stress. Penistent Postconcussive Syndrome
Postconcussive syndrome is considered persistent when it is present for 1 year; in many patients, symptoms increase over time. Several studies have shown that symptoms in patients with persistent postconcussive syndrome undergo a shift from purely somatic initially to increasingly psychological vegetative symptoms. A number of factors are said to be associated with an increased risk of persistent postconcussive syndrome: female sex, ongoing litigation, low socioeconomic status, prior mild TBI,
Principles of Diagnosis: Common PresentingSymptoms
severity of initial neck pain, and preinjury emotional state. Note that differences in mildness from “dings” to a GCS score of 13 have not been implicated. However, no one factor is a very potent predictor. Dikmen and colleagues (1986) eloquently described the role of postinjury psychological factors in persistent postconcussive syndrome while observing that these factors have largely eluded prospective definition. Lishman (1988) provided an elegant description of how physiogenesis is transformed to psychogenesis. In recent years, some prospective analyses have yielded insights into persistent postconcussive syndrome. For example, these patients have more significant head and neck pain than their recovered counterparts. That chronic pain alone can produce symptoms of cognitive impairment is well known. Patients with persistent postconcussive syndrome are much more likely to have reached diagnostic criteria for specific psychiatric disorders by 6 months after the injury. Depression is most common. Global anxiety, at times with features of posttraumatic stress disorder, is also common. Memory of the injury scene may be a factor in the qualities of post-traumatic stress disorder. Peripheral vestibular disorder is a potent contributor to the anxiety that develops in a large number of patients with acute vestibular disease within 6 months of onset. Even frank phobic disorder can develop. That depression or anxiety can produce symptoms, and even signs, of cognitive dysfunction is also well known. Depressed patients with cognitive impairment even have a consistent pattern of frontal hypoperfusion in positron emission tomography studies. Much effort is spent trying to prove brain injury in these patients. Single photon emission computed tomography (SPECT) scans have little value. They have high negative predictive value (normal scan correlates with good outcome) but poor positive predictive value (abnormal scan has little correlation with outcome). Late SPECT abnormalities in symptomatic patients are similar to the SPECT “abnormalities” in depression. They neither prove or disprove brain injury, and they do not facilitate treatment. Finally, patients with persistent postconcussive syndrome have a larger number of chronic social problems than their recovered counterparts. As patients remain symptomatic, and perhaps even worsen, families become transformed. The families of patients with persistent postconcussive syndrome have a different belief structure: The patient is disabled; the doctors can’t or aren’t trying to find the cause; the family’s role is to take over and support the disabled patient. Arguments about injury characteristics, negative CT scans, and depression fall flat against this belief structure. Very few patients are frankly malingering. Treatment of persistent postconcussive syndrome often is unrewarding. Few approaches are open. First, symptomatic treatment should be offered where appropriate. This might include analgesia, vestibular suppressants, counseling, and physical therapy. Antidepressants can be used as headache treatments or sleeping aids. Antianxiety agents can be used as vestibular suppressants. Physical therapy for neck pain can be used to mobilize the patient into a schedule, a home program, and some fitness activities. Because these patients actually have trivial neurologic impairments, they are often ideal for cognitive rehabilitation programs designed for the patient with late severe TBI. Only programs of the second type described earlier are appropriate. Because of these patients’ good neurologic recovery, programs to reenter community activities and to practice interviews and time management can be quite successful. Treatment of basic
Chapter 18
psychiatric symptoms is an essential part of this plan. Depressed patients with TBI are no more swayed by cajoling and encouragement than functionally depressed patients. Treatment of these patients is quite difficult and entails simultaneous attention to somatic symptoms and to psychological processes. Two mistakes to avoid are attributing persistent postconcussive syndrome to malingering or to pending litigation without further neuropsychiatric assessment and endlessly pursuing symptomatic treatment of one somatic complaint without attempting to place the treatment in a broader medical, rehabilitative, and psychological context. SUGGESTED READINGS Alexander M P In the pursuit of proof of brain damage after whiplash injury. Neurology 51:336-340, 1998 Alexander M P Neuropsychiatric correlates of persistent postconcussive syndrome. J Head Trauma Rehabil 7:60, 1992 Bicik I, Radanov BP, Schafer N et al: PET with 18-fluorodeoxyglucoseand hexamethylpropyleneamine oxime SPECT in late whiplash syndrome. Neurology 51:345-350, 1998 Dikmen S, McLean A, Temkin N, Wyler A Neuropsychological and psychosocial consequences of minor head injury. J Neurol Neurosurg Psychiatry 491227, 1986 Eagger S, Luxon LM, Davies R4 et al: Psychiatric morbidity in patients with peripheral vestibular disorder: a clinical and neuro-otological study. J Neurol Neurosurg Psychiatry 55:383, 1992 Katz DI, Alexander M P Predicting outcome and course of recovery in patients admitted to rehabilitation. Arch Neurol 51:661, 1994 Kelly JP Sports related head injuries. J Head Trauma Rehab 13:1-65, 1998
SECTION
Laboratory Evaluation
173
Goel V, Grafman J: Role of the right prefrontal cortex in ill-structured planning. Cognit Neuropsychol 17:415-436,2000 Lishman WA Physiogenesis and psychogenesis in the “post-concussional syndrome.” Br J Psychiatry 153:460, 1988 Masters SJ, McClean PM, Arcarese 7.5 Skull x-ray examinations after head trauma: recommendationsby a multidisciplinary panel and validation study. N Engl J Med 31684, 1987 McAllister TW, Saykin AJ, Flashman LA et al. Brain activation during working memory 1 month after mild traumatic brain injury: a functional MRI study. Neurology 53:1300-1308, 1999 Mittenberg W, Tremont G, Zielinski R et al: Cognitive-behavioral prevention of postconcussion syndrome. Arch Clin Psychology 10: 139-145, 1996 Salazar AM, Warden DL, Schwab K et al: Cognitive rehabilitation for traumatic brain injury: a randomized trial. JAMA 283:3123-3124, 3075-3081,2000 Servadei F, Vergoni G, Nasi MT et al: Management of low-risk head injuries in an entire area: results of an 18 month survey. Surg Neurol 39:269, 1993 Shackford SR, Ward SI, Ross SE et al: The clinical utility of computed tomographic scanning and neurologic examination in the management of patients with minor head injuries. J Trauma 33:385, 1992 Shallice T, Burgess PW Deficits in strategy application following frontal lobe damage in man. Brain 114727-741, 1991 Taheri PA, Karamanoukian H, Gibbons K et al: Can patients with minor head injuries be safely discharged home? Arch Surg 128:289, 1993 Teasdale GM, Murray G, Anderson E et al: Risks of acute traumatic intracranial haematoma in children and adults: implications for managing head injuries. BMJ 300363, 1990 Vollmer DG, Dacey RG, Jane J A Craniocerebral trauma. p. 63. In Joynt R (ed): Clinical Neurology. Lea & Febiger, Philadelphia, 1991 Williams DH, Levin HS, Eisenberg HM: Mild head injury classification. Neurosurgery 27:422, 1990
3 PRINCIPLES OF DIAGNOSIS: SPECIAL TESTS
18
Laboratory Evaluation Steven K. Feske
The neurologic history and examination often allow the physician to make an anatomic or syndromic diagnosis. Additional studies, including laboratory tests, electrophysiology, neuroimaging, and biopsy can add precision to this diagnosis and often support an etiologic diagnosis. The chapters in this section describe the use of many ancillary tests that are helpful in neurologic diagnosis. The goal of these chapters is to provide a brief general description of the nature and interpretation of commonly used tests. More specific information about the indications and interpretations of certain tests can be found in the discussions of particular diseases.
This chapter addresses selected general laboratory tests significant in neurologic diagnosis. TESTS OF COAGULATION Stroke is the most common life-threateningneurologic disease and among the most common causes of death. The neurologist must understand the laboratory tests that contribute to the proper evaluation and management of vascular disease. The coagulation system is shown in Figure 18-1. The cascade of reactions following
Chapter 18
psychiatric symptoms is an essential part of this plan. Depressed patients with TBI are no more swayed by cajoling and encouragement than functionally depressed patients. Treatment of these patients is quite difficult and entails simultaneous attention to somatic symptoms and to psychological processes. Two mistakes to avoid are attributing persistent postconcussive syndrome to malingering or to pending litigation without further neuropsychiatric assessment and endlessly pursuing symptomatic treatment of one somatic complaint without attempting to place the treatment in a broader medical, rehabilitative, and psychological context. SUGGESTED READINGS Alexander M P In the pursuit of proof of brain damage after whiplash injury. Neurology 51:336-340, 1998 Alexander M P Neuropsychiatric correlates of persistent postconcussive syndrome. J Head Trauma Rehabil 7:60, 1992 Bicik I, Radanov BP, Schafer N et al: PET with 18-fluorodeoxyglucoseand hexamethylpropyleneamine oxime SPECT in late whiplash syndrome. Neurology 51:345-350, 1998 Dikmen S, McLean A, Temkin N, Wyler A Neuropsychological and psychosocial consequences of minor head injury. J Neurol Neurosurg Psychiatry 491227, 1986 Eagger S, Luxon LM, Davies R4 et al: Psychiatric morbidity in patients with peripheral vestibular disorder: a clinical and neuro-otological study. J Neurol Neurosurg Psychiatry 55:383, 1992 Katz DI, Alexander M P Predicting outcome and course of recovery in patients admitted to rehabilitation. Arch Neurol 51:661, 1994 Kelly JP Sports related head injuries. J Head Trauma Rehab 13:1-65, 1998
SECTION
Laboratory Evaluation
173
Goel V, Grafman J: Role of the right prefrontal cortex in ill-structured planning. Cognit Neuropsychol 17:415-436,2000 Lishman WA Physiogenesis and psychogenesis in the “post-concussional syndrome.” Br J Psychiatry 153:460, 1988 Masters SJ, McClean PM, Arcarese 7.5 Skull x-ray examinations after head trauma: recommendationsby a multidisciplinary panel and validation study. N Engl J Med 31684, 1987 McAllister TW, Saykin AJ, Flashman LA et al. Brain activation during working memory 1 month after mild traumatic brain injury: a functional MRI study. Neurology 53:1300-1308, 1999 Mittenberg W, Tremont G, Zielinski R et al: Cognitive-behavioral prevention of postconcussion syndrome. Arch Clin Psychology 10: 139-145, 1996 Salazar AM, Warden DL, Schwab K et al: Cognitive rehabilitation for traumatic brain injury: a randomized trial. JAMA 283:3123-3124, 3075-3081,2000 Servadei F, Vergoni G, Nasi MT et al: Management of low-risk head injuries in an entire area: results of an 18 month survey. Surg Neurol 39:269, 1993 Shackford SR, Ward SI, Ross SE et al: The clinical utility of computed tomographic scanning and neurologic examination in the management of patients with minor head injuries. J Trauma 33:385, 1992 Shallice T, Burgess PW Deficits in strategy application following frontal lobe damage in man. Brain 114727-741, 1991 Taheri PA, Karamanoukian H, Gibbons K et al: Can patients with minor head injuries be safely discharged home? Arch Surg 128:289, 1993 Teasdale GM, Murray G, Anderson E et al: Risks of acute traumatic intracranial haematoma in children and adults: implications for managing head injuries. BMJ 300363, 1990 Vollmer DG, Dacey RG, Jane J A Craniocerebral trauma. p. 63. In Joynt R (ed): Clinical Neurology. Lea & Febiger, Philadelphia, 1991 Williams DH, Levin HS, Eisenberg HM: Mild head injury classification. Neurosurgery 27:422, 1990
3 PRINCIPLES OF DIAGNOSIS: SPECIAL TESTS
18
Laboratory Evaluation Steven K. Feske
The neurologic history and examination often allow the physician to make an anatomic or syndromic diagnosis. Additional studies, including laboratory tests, electrophysiology, neuroimaging, and biopsy can add precision to this diagnosis and often support an etiologic diagnosis. The chapters in this section describe the use of many ancillary tests that are helpful in neurologic diagnosis. The goal of these chapters is to provide a brief general description of the nature and interpretation of commonly used tests. More specific information about the indications and interpretations of certain tests can be found in the discussions of particular diseases.
This chapter addresses selected general laboratory tests significant in neurologic diagnosis. TESTS OF COAGULATION Stroke is the most common life-threateningneurologic disease and among the most common causes of death. The neurologist must understand the laboratory tests that contribute to the proper evaluation and management of vascular disease. The coagulation system is shown in Figure 18-1. The cascade of reactions following
174
Principles of Ambulatoy Neurologyand the Approach to Clinical Problems
Principles of Diagnosis: Special Tests
Therefore, it depends on the normal function of factor VII of the extrinsic pathway and the common pathway downstream to it. The prothrombin time can be prolonged by any disease or medication affecting these factors. Warfarin inhibits synthesis of the vitamin K-dependent factors 11, VII, IX, and X. Three of these are necessary for proper function of the extrinsic and common pathways, and the prothrombin time is a sensitive assay of the intensity of anticoagulation by warfarin. Until recently, it was customary to report the prothrombin time as a ratio of the patient's value and a control value: PT,/PT,. Recommendations for the desirable intensity of anticoagulation were published as prothrombin time ratios. In recent years, it has been suggested that the prothrombin time value be reported as a standardized ratio, that is, the international normalized ratio (INR). This value normalizes differences based on the variable sensitivities of lots of reagent thromboplastin. The INR is defined as INR= (PT,/PT,)'S'
FIG. 18-1. The coagulation cascade, anticoagulant inhibitory systems,
and tests of coagulation function. The interactions of the four anticoagulant systems are shown in ovals: antithrombin 111 (AT Ill), protein C and S system (PCa/PS), tissue factor pathway inhibitor (TFPI), and plasmin. Some of the functional tests of coagulation are shown in rectangles: activated partial thrornboplastin time ( a m , prothrombin time (PT), thrombin time 0,Russell's viper venom test (RW), protamine sulfate test (PST), and D-dimer. FDP, fibrin degradation products; Fg, fibrinogen; 11, prothrombin; PL, cellular phospholipid surface; TF, tissue factor. (Modified from Nachman RT, Silverstein R: Hypercoagulable states. Ann Intern Med 120:520, 1994, with permission.)
from the activation of factor X constitutes the common pathway. The cascade of reactions beginning with the activation of factor XI1 and including the reactions of the common pathway constitutes the intrinsic pathway. Activation of factor X via factor VII and tissue factor and the resultant cascade of reactions through the common pathway constitute the extrinsic pathway. Normal coagulation depends on the interaction of the coagulant proteins that exist in blood as proenzymes and three anticoagulant systems-the protein C-protein S system, the antithrombin 111 system, and the tissue factor pathway inhibitor (TFPI) system-along with a fourth plasmin fibrinolytic system. Many functional and antigenic tests have been devised to assess the state of the coagulant systems. The sites of entry of the anticoagulant inhibitory systems and the fibrinolytic system and the sites of reagent activation or sampled products of many of the assays of coagulation are also shown in Figure 18-1; the descriptions of the tests of coagulation that follow refer to this figure.
Prothrombin lime The prothrombin time is the time in seconds that it takes plasma to clot after the addition of thromboplastin (tissue factor).
where PT, is the patient's prothrombin time in seconds, PT, is the mean of a series of control values, and IS1 is the international sensitivity index, a measure of the sensitivity (reactivity) of the thromboplastin used. The IS1 is calculated by the manufacturer of the thromboplastin or the laboratory and is a property of the particular lot of thromboplastin. A thromboplastin with a sensitivity equal to that of the World Health Organization standard has an IS1 of 1 and therefore yields an INR equal to the prothrombin time ratio. With less sensitive thromboplastins (higher ISI) the prothrombin time value for a given INR is lower, and the range of values is narrower; for more sensitive thromboplastins, the range of values for prothrombin time is wider, and subtler abnormalities of coagulation can be detected. An INR of 1.4 or less suggests hemodynamically adequate levels of coagulation factors. Recent recommendations for the desirable intensity of anticoagulation in various clinical situations are discussed in Chapter 25 and in Part 11.
Activated Partial Thromboplastin lime The activated partial thromboplastin time (aPTT), usually called simply PTT, is the time in seconds that it takes plasma to clot after the addition of a contact agent that fully activates factors XI1 and XI along with calcium and phospholipid. These reagents activate factors XI1 and XI, so the PTT depends on the normal function of these factors and the other factors of the intrinsic pathway. It can be prolonged by any disease or medication affecting these factors. It is more sensitive than the prothrombin time for detecting acquired circulating anticoagulants, often called lupus anticoagulants. It is also sensitive to the multiple-level effects of heparin and therefore is used as the functional assay of adequate heparinization. For most indications for which full heparinization is desirable, a PTT of 2 to 2.5 times the normal value is the therapeutic goal. Heparin therapy is discussed in Chapter 25.
AntbFactor Xa Activity Because they have low antithrombin activity, low-molecularweight heparins (LMWH) and heparinoids minimally affect the standard aPPT. For routine use, weight-adjusted dosing is adequate without monitoring. However, in patients with renal insufficiency, pregnancy, severe obesity, and other conditions that affect the pharmacokinetics of LMWH, monitoring should be done using anti-factor Xa activity. Using this assay, the goal
Chapter 18 H Laboratory Evaluation
175
therapeutic range should be about 0.3 to 0.7 U/mL; this corresponds to a heparin level by the protamine titration method of 0.2 to 0.4 U/mL and very roughly to an aPTT of 1.8 to 2.5 (up to 4.2) times control.
polymerase chain reaction testing. This heterozygouslesion occurs in about 2% to 15% of Caucasians of European descent.
It is widely accepted that hereditary and acquired dysfunction of these coagulation systems can cause thromboembolic disease, including strokes. Tests for the presence of hypercoagulability are now a part of the evaluation of stroke and other thrombotic events when the more common risk factors are absent. Abnormalities of two of the three anticoagulant systems, the protein C-protein S and antithrombin 111 systems, have been associated with thrombosis, although their association to arterial strokes is less clear. Decreased tissue factor pathway inhibitor activity may play a role in many thrombotic disorders; the clinical implications of reduced TFPI activity are now being actively studied. Also, abnormalities of fibrinogen and the plasmin fibrinolytic system can rarely cause clinical thrombosis.
A mutation of the prothrombin gene called prothrombin 20210A is associated with elevated plasma levels of prothrombin and venous thromboembolism. As for the factor V Leiden mutation, this lesion may clearly underlie cerebral venous sinus thrombosis. Data concerning an associated elevated risk of arterial strokes are conflicting. The mutation occurs in about 1% of Caucasians and 6% of Spaniards.
Protein C and Protein S Protein C is a vitamin K-dependent serine protease, that is, one of a family of proteolytic enzymes with serine in the active site. Protein S is its vitamin K-dependent cofactor. The protein C-protein S complex inactivates factors Va and VIIIa. This probably prevents thrombus formation at the capillary level. Decreased levels or dysfunctional molecules with low enzymatic activity can cause hereditary hypercoagulable states. Also, many conditions can cause acquired deficiencies. Assays for antigenic levels and enzymatic activity exist for both proteins. Protein S can be measured in the free (active) and bound states. Because they are vitamin K-dependent, these proteins are depleted by warfarin. It is best to wait 1 to 2 weeks after warfarin therapy has been discontinued to measure them. If warfarin therapy cannot be stopped, the ratio of protein C antigen to prothrombin antigen can estimate the effective level.
Prothrombin 2021OA
Fibrinogen Elevated fibrinogen has been identified in the Framingham study as a risk factor for stroke in men, although because no treatment has yet been recommended in its presence, it has not been useful to measure fibrinogen levels routinely. Dysfibrinogenemia,synthesis of an abnormal fibrinogen molecule, usually is associated with pathologic hemorrhage; however, thrombosis rarely occurs. Fibrinogen function can be assayed with tests of the final steps of the coagulation cascade, the thrombin time and the reptilase clotting time. The thrombin time is the time in seconds that it takes for plasma to clot after the addition of thrombin. This tests the generation of a fibrin clot from the existing fibrinogen. Reptilase hydrolyzes fibrinogen to promote clotting directly. Both of these clotting times are prolonged in the presence of an abnormal fibrinogen. An antigenic assay for the fibrinogen level is also available.
The Plasmin Fibdnolytic System Abnormal plasmin generation is a rare cause of hypercoagulability. These disorders can also be hereditary or acquired. Antigenic and functional assays are available in special circumstances; however, because these disorders are rare, screening is not routine.
Antithrombin 111
The Antiphospholipid Antibody Syndrome
Antithrombin 111 is a vitamin K-dependent serine protease inhibitor that irreversibly inactivatesfactors XIIa, XIa, IXa, Xa, and IIa (thrombin), all serine proteases. Heparins bind to antithrombin 111, enhancing its natural anticoagulant effects. As with proteins C and S, decreased activity can result from hereditary decreased synthesis with low levels of a normal molecule or synthesis of a dysfunctional molecule, or a deficiency state can be acquired from loss of hepatic synthetic function. Antigenic and functional activity assays are available.
The presence of circulating antibodies to negatively charged phospholipids has been associated with pathologic thrombosis. The mechanism of thrombogenesis is unknown but probably a result of a reaction of the antibody with phospholipid of the endothelial cell or platelet membrane. Several tests are available to look for the presence of such antibodies. So far, their optimal use and interpretation have not been clarified. These antibodies were originally identified in patients with systemic lupus erythematosus and named lupus anticoagulants because of their effect in prolonging phospholipid-dependent coagulation times. Binding to phospholipid inhibits the generation of the thrombin activator complex, which is produced by the interaction of factors Xa and Va and phospholipid (Fig. 18-1). This may prolong the PTT and, less commonly, the prothrombin time. This prolongation is not corrected by the addition of normal plasma in mixing studies when a circulating anticoagulant is present. However, these routine tests are not sensitive indicators of a lupus anticoagulant. Russell's viper venom test and the kaolin clotting time depend on the direct activation of factor X. These are more sensitive screening tests for a lupus anticoagulant. Using these tests to define the lupus anticoagulant, the false-negative rate of the PTT is 22% to 33%. Therefore, one of these two tests may be used to screen for lupus
Activated Protein C Resistance and Factor V Leiden The factor V Leiden mutation at the cleavage site for activated protein C results in resistance of factor V to inactivation by activated protein C, causing thrombophilia. This mutation is the most common hereditary risk factor for venous thrombosis. The increased risk includes cerebral venous thrombosis. Although reports suggest an increased risk of arterial stroke in young patients with this genetic lesion, an increased risk for arterial strokes has not been firmly established. Laboratory screening for this lesion is done using a coagulation assay for protein C resistance. The genetic lesion can be confirmed directly by
176
Principles of Ambulatoy Neurology and the Approach to Clinical Problems
anticoagulants. Russell’s viper venom test has been favored because it is simple, easy to perform, not influenced by inhibitors of factors VIII and IX (which can confound the interpretation of the kaolin clotting time), and does not necessitate a confirmatory test (as does the kaolin clotting time). (The kaolin clotting time corrects with the addition of phospholipid but not normal plasma.) In many laboratories, dilute aPTT assay and platelet neutralization tests for phospholipid dependence have replaced other tests as sensitive assays to detect a lupus anticoagulant. Although not as specific for the antiphospholipid antibody syndrome as the lupus anticoagulant, antigenic tests for the presence of antibodies to cardiolipin are more sensitive and reproducible, and they allow a quantitative assessment. Enzymelinked immunosorbent assays (ELISA) for immunoglobulin G (IgG), IgM, and IgA anticardiolipin antibodies are available. Specificity for clinical disease, such as thrombosis, fetal loss, and thrombocytopenia, correlates with higher titers and with the presence of anticardiolipin of the IgG class. Harris and colleagues (1987) have recommended cutoff values for interpreting the clinical significance of anticardiolipin antibodies (Table 18- 1). Most laboratories report this test as positive if values are at the lower end of the moderate positive range seen in Table 18-1. Harris and colleagues (1986) reported that predictive values for disease increase with increasing titers. It has been found that anticardiolipin antibodies bind to an epitope on the phospholipid-binding protein P2-glycoprotein I. Pathogenic antibodies depend on this P2-glycoprotein I binding in in vitro studies. This has led to an assay for P2-glycoprotein I. The presence of antibodies to P2-glycoprotein I also suggests clinical antiphospholipid antibody syndrome. Tests for other antiphospholipid antibodies are available, but their clinical relevance is less clear. The tests for lupus anticoagulant and antibodies to cardiolipin or phospholipid-binding protein are discordant. Depending on the method used to test for the lupus anticoagulant, it detects 50% to 94% of those with anticardiolipin by ELISA. A positive anticardiolipin test detects 70% to 80% of those with a lupus anticoagulant by a sensitive assay. Because of this discordance, it is recommended that, in the appropriate clinical setting, screening be done with both the ELISA for anticardiolipin subclasses and P2-glycoprotein I and a sensitive test for a lupus anticoagulant. A positive anticardiolipin value can then be quantitated to estimate the risk of thrombosis (Table 18-1).
Disseminated lntravascular Coagulation Disseminated intravascular coagulation (DIC) can be an acute and fulminant process, usually accompanied by hemorrhage or a subtle subacute or chronic process that can lead to hemorrhage or pathologic thrombosis. Therefore, screening tests for DIC some-
TABLE 18-1. The Clinical Significance of Anticardiolipin Titers Antibody Class
IgC WmL) IgM (Il/mL)
Normal 55
23
low Positive
Moderate Positive
High Positive
6-1 4 4-5
15-80 6-50
90 >50
Adapted from Harris EN et al: Evaluation of the anticardiolipin antibody test: report of an international workshop held 4 April 1986. Clin Exp lmmunol 68:215, 1987, with permission.
w
Principles of Diagnosis: Special Tests
times are an appropriate part of the evaluation of thromboembolic disease. A battery of tests is available to assay the several steps in this coagulopathy. Consumption of fibrinogen, thrombin, and coagulation factors higher up in the clotting cascade leads to a fall in the fibrinogen level and a prolongation of the clotting times: partial thromboplastin, prothrombin, and thrombin times. If the fibrinogen was high at the start, it may remain in the normal range. Consumption of platelets results in a fall in the platelet count and prolongation of the bleeding time. Intravascular fibrin deposition in the small vessels causes a microangiopathic hemolytic anemia, which is detected by a fall in the hemoglobin and hematocrit and schizocytes on a peripheral blood smear. If thrombosis and fibrinolysis are activated, fibrin monomer and fibrin degradation products are formed. Fibrin degradation products can be quantitated and usually are greater than 40 pg/mL in DIC. The serial dilution protamine sulfate test detects fibrin monomer and fibrin degradation products. Protamine sulfate causes the dissociation of soluble complexes of fibrin monomer and fibrin degradation products. Because these complexes prevent polymerization, this dissociation by protamine sulfate allows polymerization to proceed. A positive test means that fibrin monomer and fibrin degradation products are present and that fibrinogen and fibrinolysis have been activated. The protamine sulfate test is a sensitive but nonspecific test of DIC. The D-dimer is produced when plasmin induces lysis of crosslinked fibrin, so it serves as a marker of thrombus formation and lysis. The most common laboratory abnormalities in DIC, in decreasing order of frequency, are thrombocytopenia, D-dimer elevation, and elevation of PT, aPTT, and thrombin time and depletion of fibrinogen.
IMMUNOLOGIC MARKERS OF DISEASE Many neurologic diseases have an established or presumed autoimmune origin. These include many inflammatory medical diseases with neurologic complications, many neuropathies, myasthenia gravis, and many paraneoplastic syndromes. Many autoantibodies are useful in clinical diagnosis. Further discussions of most of the tests described in this section are found in later chapters discussing the diseases with which they are associated.
Autoantibodies in Rheumatic Disease Rheumatic disease enters into the differential diagnosis of several neurologic disorders, including neuropathies, sensory neuronopathy, myositis, aseptic meningitis, and stroke. Autoantibodies are never diagnostic; however, in the appropriate clinical context, they can support the diagnosis of an underlying rheumatic disease (Table 18-2). Rheumatoid Factors. The routinely used rheumatoid factor tests for the presence of IgM antibodies to certain immunoglobulins. This test is about 90% sensitive for typical rheumatoid arthritis. However, it is nonspecific and can be positive in many other rheumatic and nonrheumatic diseases, many of which cause neurologic disease, including systemic lupus erythematosus (SLE), dermatomyositis, Sjogren’s syndrome, sarcoidosis, and endocarditis. Ninety percent of patients with Sjogren’s syndrome have rheumatoid factors. Antinuclear Antibodies. More than 90% of patients with SLE have high titers of antinuclear antibodies (ANAs). These also are nonspecific. The pattern of nuclear immunofluorescent staining can add specificity. A peripheral staining pattern is specific for
Chapter 18
Laboratoly Evaluation
177
rn TABU 18-2. Some Autoantibodies in Immunologically Mediated Diseases with Neurologic Complications Antigen
Clinical Significance
Rheumatoid factors ANA Double-stranded DNA, peripheral pattern Single-stranded DNA, peripheral pattern Antihistone, homogeneous Sm, speckled RNP, speckled
Nonspecific, sensitive for RA and Sjogren’s syndrome Nonspecific Specific for SLE, active renal disease Nonspecific, very sensitive for SLE In SLE and drug-induced LE; if present alone, suggestive of drug-induced LE Specific for SLE, renal and CNS disease Nonspecific: PM with MCTD, SLE, Sjogren’s syndrome, scleroderma Jo- 1 PM with interstitial lung disease PM-Scl PM with scleroderma Ro (SSA) SLE, Sjogren‘s syndrome La (SSB) Primary Sjogren’s syndrome, if no other autoantibodies are present CANCA Vasculitis from Wegenet‘s granulomatosis or microscopic periarteritis pANCA GlomeruloneDhritis: . . also classic PAN and other vasculitides and rheumatic diseases Abbreviations: AN& antinuclear antibodies; c4NCA, antineutrophilic cytoplasmic antibodies, cytoplasmic pattern; CNS, central nervous system; LE, lupus erythematosus; MOD, mixed connective tissue disease; PAN, polyarteriiis nodosa; pANCq pen-nuclear pattern; PM, polymyositis; RA, rheumatoid arthritis; RNP, ribonudear protein; SLE, systemic lupus erythematosus. Adapted from Condemi JJ: Autoimmune diseases. JAMA 268:2883, 1992, with permission.
active SLE. Diffuse and speckled patterns are nonspecific. Antibodies to certain nuclear antigens are more specific for SLE. These include antibodies to double-stranded DNA and anti-Sm. Antibodies to the antigens Ro (also called SSA) and La (also called SSB) and single-strandedDNA are nonspecific;they are present in most patients with clinical SLE and a negative ANA screen. Antihistone antibodies also appear in lupus and, when found alone, suggest that it is drug induced. A positive ANA is found in about 70% of patients with Sjogren’s syndrome. The staining pattern usually is diffuse or speckled. Antibodies to the small nuclear ribonuclear proteins Ro and La are often seen as well, although they are nonspecific. The presence of isolated anti-La antibodies suggests primary Sjogren’s syndrome. Mixed connective tissue disease enters into the diagnosis of neuropathies, myositis, and aseptic meningitis. High titers of antibodies to ribanuclear protein (also called extractable nuclear antigens because they are soluble in aqueous buffers) are characteristic of this disease, although they too are nonspecific. Polymyositis can occur in association with various rheumatic diseases. Characteristic ANAs may accompany these different syndromes. As noted earlier, ribonuclear protein is found in polymyositis with mixed connective tissue disease. Autoantibodies to Jo-1 accompany polymyositis in interstitial lung disease. Autoantibodies to PM-Scl, a nucleolar antigen, accompany polymyositis in scleroderma. Autoantibodies in Systemic Vasculitis: Antineutrophilic Cytoplasmic Antibodies
Antineutrophilic cytoplasmic antibodies (ANCA) bind with enzymes within granules of polymorphonuclear leukocytes. Two patterns can be detected by immunofluorescent staining: a cytoplasmic pattern detected by ELISA and a perinuclear pattern detected by indirect immunofluorescence. The cytoplasmic pattern has a high sensitivity and specificity for two types of systemic vasculitis: Wegener’s granulomatosisand microscopic periarteritis. The perinuclear pattern is most commonly found in crescentic necrotizing glomerulonephritis, but it can be seen with low sensitivity and specificity in other inflammatory diseases, such as classic periarteritis nodosa and other systemic vasculitides, rheumatoid arthritis, SLE, inflammatory bowel disease, and chronic liver disease.
Autoantibodies in Myasthenia Gravis Acetylcholine Receptor Antibodies. Antibodies to the nicotinic acetylcholine (ACh) receptor are detected by Western blot analysis. They are found 75% to 95% of the time in patients with acquired generalized myasthenia gravis, with only rare false positives reported. The sensitivity is reduced to about 50% to 70% in myasthenia gravis limited to the ocular muscles. These antibodies have been implicated in the pathogenesis of myasthenia gravis to establish it convincingly as an autoimmune disease. In the appropriate clinical setting, a positive test can corroborate the diagnosis of adult and neonatal myasthenia gravis. However, the levels of these autoantibodies do not correlate with disease activity in populations, although there may be a correlation in a given case. These autoantibodies are also found in cases of drug-induced myasthenia. They are not present in congenital myasthenia. Antistriated Muscle Antibodies. In patients with myasthenia gravis, the presence of antibodies to striated muscle suggests that the patient harbors a thymoma. Autoadbodies En Paraneoplastic Syndromes
Several paraneoplastic neurologic syndromes have been associated with specific autoantibodies (Table 18-3). Although these autoantibodies have not been as clearly implicated in the pathogenesis of the neurologic syndrome as have ACh receptor antibodies in myasthenia gravis, when present they can help to direct the physician to the appropriate search for underlying tumors, and they can provide evidence that a given syndrome is a remote effect of cancer. Anti-Yo Antibodies. Anti-Yo antibodies react with an antigen found in the cytoplasm of cerebellar Purkinje cells. A subset of patients with paraneoplastic subacute cerebellar degeneration have these antibodies in the serum and cerebrospinal fluid (CSF). Almost all patients with subacute cerebellar degeneration and a high titer of anti-Yo antibodies have been women with ovarian, breast, or other gynecologic malignancies. Only rare cases of other malignancies have been reported, including lung cancer and lymphoma. Therefore, the presence of these antibodies should prompt a careful search for an underlying gynecologic malignancy. This should include exploratory pelvic surgery in patients with normal mammograms and no other indication of tumor. Tumor diagnosis may be delayed until long after the onset of the
178
Principles of Ambulatory Neurology and the Approach to Clinical Problems
Principles of Diagnosis:Special Tests
TAW 18-3. Autoantibodiesin Paraneoplastic Neurologic Syndromes Antibodv
Most Common Tumor Tmes
Clinical Syndrome ~
Anti-Yo Anti-Hu Anti-Ri Anti-CVZ Anti-Ma Anti-Ta Anti-CAR Anti-VCCC Anti-MAC
Subacute cerebellar degeneration Subacute sensory neuronopathy, limbic and brainstem encephalitis, subacute cerebellar degeneration Opsoclonus in adults, cerebellar dysfunction Encephalomyelitis, cerebellar degeneration, peripheral neuropathy, optic neuritis Brainstem and cerebellar dysfunction Limbic and brainstem encephalitis Retinal deneneration Lambert-Elaton myasthenic syndrome Paraproteinemia with indolent sensorimotor neuropathy
Ovarian, breast, other gynecologic cancers SCLC, neuroblastoma Breast cancer, gynecologic cancers, SCLC SCLC and other cancers Lung, breast, parotid, colon cancer Testicular cancer SCLC and other cancers SCLC MCUS
Abbreviations: CAR, cancer-associatedretinopathy; MAG, myelin-associatedglycoprotein; MGUS, monoclonal gammopathy of undetermined significance; SCLC, small cell lung cancer; VGCC voltagegated calcium channels.
neurologic syndrome. Patients with the syndrome of subacute cerebellar degeneration without anti-Yo antibodies are most likely to have lung cancer, especially small cell cancer, or Hodgkin’s disease. Rarely, other cancers, such as lymphomas, have been identified, or no tumor has been found. Anti-Hu Antibodies. Anti-Hu antibodies react with an antigen found in neuronal nuclei. Most patients with these antibodies in serum or CSF have been found to harbor a small cell cancer. Rarely other tumors have been found prostate carcinoma, neuroblastoma, and chondromyxosarcoma. Tumor diagnosis may be delayed, and rarely no tumor has been found. Several neurologic syndromes may accompany these antibodies. The major associated syndromes include subacute sensory neuronopathy; paraneoplastic encephalomyelitis, including limbic encephalitis, brainstem encephalitis, and myelitis; and cerebellar degeneration with loss of Purkinje cells (anti-Yo negative). The presence of these antibodies in the context of these neurologic syndromes should prompt a careful search for a small cell carcinoma or other, less common tumor. High titers of them in a patient with known small cell carcinoma support the paraneoplastic cause of the neurologic findings. Low titers are found in about 16% of all patients with small cell carcinoma. Anti-Ri Antibodies. Anti-Ri antibodies also react with a neuronal nuclear antigen. These antibodies are found in high titers in the serum and CSF of patients with paraneoplastic opsoclonus associated with breast cancer. They have not been found in childhood opsoclonus-myoclonuswith or without neuroblastoma or in breast cancer without opsoclonus. Their presence should stimulate a search for an underlying breast tumor or other malignancy. Anti-Ma/Ta Antibodies. The anti-Ma antibodies react with proteins expressed in neurons and spermatogenic cells of the testes. Both anti-Ma1 and anti-Ma2 (anti-Ta) antibodies may be found in the serum and CSF of patients with brainstem and cerebellar syndromes. The anti-Ma antibodies may occur in association with many tumor types, including lung, breast, parotid, and colon cancers. The anti-Ta (anti-Ma2) antibodies are associated with testicular cancer. Anti-CVZ Antibodies. Anti-CV2 antibodies react with oligodendroglial cytoplasmic antigens in the white matter of the central nervous system. They have also been shown to bind to peripheral nerve antigens. These antibodies have been found in patients with cerebellar degeneration, encephalomyelitis, sensorimotor neuropathy, optic neuritis, and other neurologic syndromes. The most common tumor type found in patients with the anti-CV2 antibody is small cell lung cancer, but a variety of other cancers has been associated with it.
Cancer-Associated Retinopathy Antibodies. The cancerassociated retinopathy antigen and possibly other ocular antigens are the targets of autoantibodies of cancer-associatedretinopathy. High titers of these antibodies have been associated with paraneoplastic retinal degeneration. This syndrome is rare. Most patients have had small cell lung cancer. Other associated cancers include those of the breast, prostate, colon, and cervix. Anti-Voltage-Gated Calcium Channels. Autoantibodies to voltage-gated calcium channels at nerve terminals have been found in some patients with small cell lung cancer, some of whom have had the Lambert-Eaton myasthenic syndrome. About 50% to 60% of patients with Lambert-Eaton myasthenic syndrome, whether with or without cancer, have been found to have such antibodies in their serum. This finding strongly suggests an autoimmune origin for this syndrome. Antibodies to Myelin-Associated Glycoprotein and Sulfated Glucuronyl Paragloboside. Several different syndromes of
neuroradiculopathy accompany monoclonal paraproteinemias. About one fourth to one half of the patients with an IgM monoclonal spike on serum protein electrophoresis have serum antibodies to myelin-associated glycoprotein (MAG), a glycoprotein that participates in myelin interactions with the axon, and antibodies to sulfated glucuronyl paragloboside (SGPG), contained in peripheral nerve axons. Usually these monoclonal IgM proteins have K-light chains; however, occasionally IgM-h immunoglobulins are found with similar anti-MAG and anti-SGPG activity. These patients typically have a demyelinating sensorimotor neuropathy with indolent progression and elevated CSF protein. Although it has not been shown that these antibodies are responsible for the neuropathy, treatment that lowers the M protein may be effective.
Autoantibodies in Other Diseases Anti-CM, Ganglioside Antibodies. Gangliosides are macromolecules made up of an oligosaccharide with at least one acid sugar associated with the lipid ceramide. They are widely distributed in the membranes of the central and peripheral nervous system tissues. Anti-GM, ganglioside antibodies have been found in the serum of some patients with a lower motor neuron syndrome that resembles amyotrophic lateral sclerosis (ALS). This syndrome is more common in males and is characterized by lower motor neuron dysfunction, typically without upper motor neuron signs, with less atrophy than in anterior horn cell disease, and with a more prolonged course, multifocal motor conduction block, and high titers of anti-GM,
Chapter 18
ganglioside antibodies. It has been called multifocal motor neuropathy with conduction block. An ELISA is available, and serum titers above 1:350 are considered specific for the syndrome. Typically they are much higher. Low titers, 1:300 or less, are nonspecific and may be found with central nervous system (CNS) damage from, for instance, multiple sclerosis and ALS. Multifocal motor neuropathy with conduction block has been successfully treated with cyclophosphamide. Because it cannot be distinguished reliably by the clinical examination from lower motor neuron forms of motor system disease, nerve conduction studies and assays of GM, ganglioside antibodies have been useful to define it. Successful treatment usually results in a fall in antibody titers, so the antibody test has also been used to follow the response to treatment. Other antiganglioside antibodies have been identified and associated with disease, such as the GQlb ganglioside associated with the Miller-Fisher variant of Guillain-Barre syndrome. Antibodies to Glutamic Acid Decarboxylase. Glutamic acid decarboxylase is the enzyme that catalyzes the formation of y-aminobutyric acid (GABA) from glutamic acid. GABA is a major inhibitory neurotransmitter in the CNS, and glutamic acid decarboxylase is present in high concentrations in the terminals of GABAergic neurons. Antibodies to glutamic acid decarboxylase have been found in the serum and CSF of about 60% of patients with the stiff man syndrome. They have also been found in some patients with insulin-dependent diabetes, a disease with a probable autoimmune mechanism that may co-occur with it. It has been hypothesized that an autoimmune attack on GABAergic neurons causes the stiff man syndrome. Although this hypothesis remains to be proven, these autoantibodies have been used along with clinical and electrophysiologicfindings as a possible marker for the syndrome.
TESTS OF INFECTION Bacterial cultures and viral isolation from CSF, blood, and other tissues and fluids are used to diagnose many infectious neurologic diseases. Titers of specific immunoglobulins can also be used to indicate past infection (IgG) or recent infection (IgM or a fourfold or higher rise of IgG titers from acute to convalescent specimens drawn 4 to 6 weeks apart). In many cases, however, the diagnosis is not easily made by culture, viral isolation, or antibody titers. This section discusses some of the other tests used to diagnose neurologic infections.
Antigen Detection Bacterial meningitis usually can be diagnosed by Gram stain and culture of CSF and blood. At times, especially when patients have already received antibiotics, all stains and cultures are negative. Latex agglutination has largely replaced counterimmunoelectrophoresis to identify the antigens of many of the more common organisms that cause meningitis. Tests are available for Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, group B streptococci, and Cryptococcus neoformans. These tests have sensitivitiesin the 80% to 100% range, although reports vary, and one study of the meningococcal latex agglutination test found it to be only 33% sensitive. The cryptococcal antigen is widely used for diagnosis and to follow the response to treatment. It is about 95% sensitive. False positives are rare.
Laboratory Evaluation
179
Polymerase Chain Reaction With the proper primers, a heat-resistant DNA polymerase, and a process of repeated heating and cooling to denature and rehybridize DNA, minute quantities of DNA can be amplified and detected in tissues. RNA can be similarly detected after synthesis of a complementary DNA (cDNA) using reverse transcriptase. This technique has been developed into sensitive and specific clinical tests for an increasing number of pathogens, including herpes simplex viruses, varicella-zoster virus, cytomegalovirus, EpsteinBarr virus, JC virus, Tomplasma gondii, Mycobacterium tuberculosis, Borrelia burgdorferi, and many others. Polymerase chain reaction for herpes simplex virus is very sensitive when specimens are collected early in the infection; however, the sensitivity falls off significantly in the days after presentation. Specificity for active CNS disease is good. Herpes simplex virus DNA is not found in the CSF of patients with latent herpes simplex virus infection but no CNS disease or non-herpes simplex virus neurologic disease.
Serology for Syphilis The Venereal Disease Research Laboratories (VDRL) test is a flocculation test that detects antibodies produced by treponemal infection. These antibodies, called reagins, are produced upon the invasion of host tissues. The rapid plasma reagin test is a refinement of the VDRL. It uses purified cardiolipin-lecithincholesterol antigen to detect the anticardiolipin antibodies produced by treponemal infection. It is more sensitive than the VDRL. The advantage of the VDRL is that it can be quantitated, and its titer reflects disease activity. After treatment, the titer usually falls, and the test becomes nonreactive over 6 to 12 months. Occasionally, a positive serum reaction of low titer (1:1, 1 2 , or slightly greater) persists after successful treatment. The VDRL can also be used to assay CSF. The CSF VDRL is very specific. Although false-positive tests can occur with contamination of the CSF with reactive blood or with CSF paraproteinemias and autoimmune disease, such false positives are rare. However, the sensitivityof the CSF VDRL is reported to be low. False-negative rates of up to 63% have been reported. Although this estimate may be too high, and false-negative rates as low as 6% have been reported, with current data it remains unreliable as a final criterion for diagnosing neurosyphilis. All positive nontreponemal tests should be confirmed by a serum treponemal test to eliminate false-positive serologies. Treponemal tests assay directly for antibodies to treponemal antigens. The two most commonly used tests are the fluorescent treponemal antibody absorption (FTA-ABS) and the microhemagglutination assay for Treponemapallidum (MHA-TP). These tests use antigens to nonpathogenic treponemes to "absorb" the nonspecific treponemal group antigens. With the serum free of these antigens, the tests detect the presence of specific serum antibodies by their reaction with T. pallidum. These tests are more sensitive and specific for syphilis than the nontreponemal tests. The reaction does not vary with treatment and once reactive will remain so indefinitely.To increase its positive predictive value, it is best used as a confirmatory test when the reagin test is reactive. Most authors do not recommend using the treponemal tests on CSF because they are so sensitive that the passive diffusion of tiny amounts of blood into the CSF causes a false-positive reaction. There is no clear consensus for the best approach to diagnosing neurosyphilis. Minimal findings probably should include a reac-
180
Plinciples of Ambulatoy Neurology and the Approach to Clinical Problems
tive serum treponemal test and an abnormal CSF (more than 5 WBC/mm3 or protein greater than 45 mg/dL). Yet with neither a positive CSF VDRL nor clinical disease consistent with neurosyphilis, the diagnosis must be questioned. Serologic Tests for Lyme Disease
Culture of B. burgdorferi is difficult and not useful for routine diagnosis of Lyme disease. Diagnosis therefore has depended on the presence of positive serologic tests in the appropriate clinical setting. Screening usually is done with ELISA for IgG, but the humoral response is delayed, so that the sensitivity is poor in the first few weeks of infection. Enzyme immunoassay (EIA) antibody capture assays are also available for Igh4 (and IgA), which may increase the sensitivity in early disease. Because of cross-reactivity with other antigens, the false-positive rate for these serologic tests is high in the presence of many other inflammatory diseases. Western blotting has been used to confirm the diagnosis of Lyme disease in indeterminate cases. Dressler and associates (1993) have proposed criteria for positive Western blots based on the presence of characteristic bands: two of the common IgM bands in early Lyme disease and five of the common IgG bands after the first few weeks. Their sensitivity and specificity data are shown in Table 18-4. Polymerase chain reaction for B. burgdorferi has been introduced as a test with high sensitivity and specificity; however, its use with the other diagnostic tests for Lyme disease has not yet been well defined. For all serologic tests and for polymerase chain reaction, it is important to remember that positive tests may persist long after successful treatment, and they alone are not indications of active infection. CEREBROSPINAL FLUID ANALYSIS
CSF analysis provides important information for diagnosis in many neurologic diseases. The lumbar puncture is safe and quickly and easily performed in most patients. The exceptions to this constitute the absolute or relative contraindications to lumbar puncture: patients with local infection at the puncture site, those with brain masses or masses involving the spinal cord above the puncture site, and those with bleeding diatheses or on anticoagulant therapy. When the physician cannot successfully reach the subarachnoid space using the usual technique, fluoroscopy can visually guide the insertion of the spinal needle. When CSF must be obtained above a spinal mass or infection, the neurosurgeon or neurologist can achieve this by lateral Cl-C2 puncture. In many cases of bleeding diatheses, an infusion of coagulation factors, such as fresh frozen plasma, cryoprecipitate, platelets, DDAVP, or
TABLE 18-4. Sensitivity and Specificity of Serologic Tests for Lyme Disease Sensitivity (46)
Specificity (%)
40 32
94 100
IgG ELSA
89
IgC Western blot
83
72 95
Early Lyme disease IgM ELSA IgM Western blot Lyme disease after first weeks
Positive enzyme-linked immunosorbent assay (ELISA) results include indeterminate cases (1 :200 to 1 :400). Adapted from Dressler F, Whalen JA, Reinhardt BN, Steere A C Western blotting in the serodiagnosisof Lyme disease. 1 Infect Dis 167:398, 1993, with permission.
Principles of Diagnosis: Special Tests
a specific factor can precede the procedure to allow sampling. In some cases, CSF is obtained upon the placement of an intracranial pressure monitor or ventricular catheter for monitoring or therapy. Normal CSF is clear and colorless. The normal pressure in the lumbar subarachnoid space with the patient relaxed in the decubitus position is 50 to 200 mm CSF (4 to 15 mm Hg). With normal CSF flow, the pressure decreases with inspiration and increases with expiration and jugular compression (Queckenstedt test). Pigments
The CSF can be colored by pigments that are the products of hemoglobin breakdown after its release from lysed erythrocytes (RBCs). Initially, oxyhemoglobin can be detected as a pink or orange pigment. Bilirubin stains the CSF yellow. It may not be detectable for up to 12 hours after the release of RBCs into the CSF. Eventually, methemoglobin may stain the fluid dark yellow or brown. The presence of such pigments is one cause of xanthochromia. Xanthochromia can be detected by visual inspection or, with greater sensitivity, by spectrophotometry. Clinically, xanthochromia is primarily of interest in distinguishing subarachnoid hemorrhage from blood introduced into the CSF by minor trauma during the lumbar puncture (traumatic tap). In a study of serial samples of CSF in patients with well-established diagnoses of subarachnoid hemorrhage, Vermeulen ( 1989) found that with spectrophotometric analysis, all of these patients had xanthochromia after 12 hours, which persisted for 2 weeks. Many, and perhaps most, patients will have xanthochromia before 12 hours have elapsed, but earlier samples have not been reported in systematic studies. Based on these data, the authors recommend that lumbar puncture be delayed for 12 hours after subarachnoid hemorrhage to avoid the scenario of the uninterpretable tap without xanthochromia. Although the spectrophotometric analysis of xanthochromia is very sensitive under these conditions of delay, it is less specific, and traumatic puncture can be accompanied by xanthochromia. The issue is important because other techniques traditionally used to differentiate these two diagnoses are known to be unreliable, as follows: Declining RBC counts. It is customary to establish the RBC count in an early and a late collection tube. If this results in a normal later tube, then it reliably indicates a traumatic tap. However, a fall to a significant but smaller number of RBCs is not reliable and can occur in subarachnoid hemorrhage. Clotting of CSF blood. Blood introduced by a traumatic tap may clot within minutes, unlike the defibrinogenated blood after subarachnoid hemorrhage. However, this test is reliable only when large numbers of RBCs are present. Crenation of RBCs. Crenation of normal RBCs occurs by an osmotic loss of water. Although the presence of crenated RBCs has been suggested as an indication of true subarachnoid hemorrhage, crenation can occur early, and this test is not reliable. Erythrophages. Erythrophages, which are macrophages that have engulfed RBCs, reliably attest to the presence of blood that has been in the CSF too long to be compatible with a traumatic tap unless an earlier lumbar puncture was performed introducing RBCs. However, cytology is needed to detect them, and they are rarely seen. Therefore, this test is too slow and insensitive to be of practical use.
Chapter 18
Although blood entering the CSF space activates the systemic hemostatic and fibrinolytic systems, and subarachnoid hemorrhage often causes elevation of the serum D-dimer, in clinical studies this test has not been adequately sensitive to screen for subarachnoid hemorrhage. Causes of xanthochromia other than pigments from blood in the CSF include the following:
Laboratory Evaluation
181
can vary greatly, so only rough guidelines can be suggested for differential diagnosis based on cell counts (Table 18-5).
Cytopathology Cytopathologic evaluation is useful to diagnose leptomeningeal or ependymal malignancy, usually carcinoma or lymphoma. This test is specific but insensitive. To optimize the sensitivity, a large volume of fluid should be sent to the cytopathology laboratory, and it should be processed immediately to avoid cell lysis or loss of characteristic morphologic features. In suspected cases, sometimes multiple samples must be analyzed before a diagnosis is confirmed. As noted earlier, because lymphomas usually produce monoclonal B cells, monoclonal antibody staining can help differentiate malignant from inflammatory lymphocytes when morphology does not.
Jaundice CSF protein greater than 150 mg/dL Certain drugs, such as rifampin Carotenoids in food faddists taking large dosages Melanin in meningeal melanomatosis Contamination with the cleansing iodine solution Cell Counts
CSF samples should be refrigerated and promptly analyzed to avoid systematic errors in cell counts. This is a real problem that must be circumvented in large hospitals where specimens are transported by messengers and often sit for long periods before analysis. Leukocytes (WBCs) begin to lyse within 1 hour of collection at room temperature. Most authors consider 5 or fewer mononuclear cells/mm3to be normal. In adults, more than 10 cells is clearly abnormal. In the case of a traumatic tap, the WBC differential count should be approximately proportional to the peripheral WBC differential count. A rough calculation allows for one WBC per 500 to 1500 RBCs; however, this calculation is very error-prone, and clinical judgment must enter into decision making. In normal CSF, almost all WBCs are mononuclear, mostly T lymphocytes. In inflammatory diseases, polymorphonuclear leukocyte and lymphocyte (again mainly T cells) numbers will rise. A predominance of polymorphonuclear cells suggests bacterial infection, early viral infection, or occasionally other infections, chemical meningitis, tumor, or infarction. Chronic infections, viral infections after the early phase, and noninfectious inflammatory disorders usually cause a rise in T lymphocytes. In leptomeningeal lymphoma, the lymphocytes typically are monoclonal B cells. Therefore, monoclonal antibody staining can help to differentiate lymphoma from inflammation. The numbers of cells
Glucose
Glucose enters the CSF by facilitated diffusion across endothelial cells mediated by a specific transporter. The CSF level depends on the serum level during the prior 4 hours or so and the rate of metabolism of glucose within the CSF. Therefore, a serum glucose level drawn within a few hours before the lumbar puncture should accompany any CSF sampling. When taken from the lumbar subarachnoid space, the normal CSF glucose is about 65% of the serum level. This ratio increases as sampling moves rostrally. When the serum glucose rises in diabetes mellitus, the CSF-toserum glucose ratio can fall to as low as 31%. In disease, the CSF glucose can be low as a result of increased metabolism by WBCs or increased glycolysis by the brain or as a result of decreased entry of glucose following from transporter inhibition. A low value always indicates some diffuse meningeal process. With a normal serum glucose, a CSF value of less than 50% of the serum value or less than 45 mg/dL usually indicates disease. Many infections, subarachnoid hemorrhage, chemical meningitis, noninfectious inflammatory diseases, and leptomeningeal malignancy can all lower the glucose level. Typically, the level is normal in viral infections, except herpes simplex virus, varicella-zoster virus, and mumps.
TAW 18-5. Cerebrospinal fluid Findings in Meningitis Origin
Cell bunts (cells/mmJ)
Glucose (mg/dL)
Rotein (mg/dL)
Normal Bacterial
55 >200cells (most >1000); PMN predominance Fewer; usually 5 to several hundred; lymph predominance loo
Gram stain; latex agglutination;culture
Normal
el00
Low Low
100-500 >loo
Increased Increased Lymphocytes; neoplastic . cells . RBCs; may have increased WBCs
2OO/mm3
1
Biopsy or treat empirically
I
Lumbar puncture
/ \ Diagnostic
I
Probable meningeal disease
Nondiagnostic
\
Treat likely diagnosis without lumbar puncture
Probable ADC I
Treat Treat FIG. 75-3. Approach to the diagnosis of patients with HIV infection and central nervous system symptoms. Hx, history; Px, physical examination.
500
Immune and Infectious Disease
Viral Infections
”HIBGIA”: Sometimes Useful in Diagnosis One principle sometimes helpful in diagnosis is called “HIBGIA” (“Had it before, got it again”). This refers to the fact that disease recurrence is common in patients with AIDS because of failure of acute therapy, failure of maintenance therapy, or failure to take maintenance therapy. By this principle, if a patient had a disease, particularly an infectious disease, and now has new neurologic complaints, then it is likely that the patient has recurrence of the disease. For example, if a patient was previously treated for syphilis and now has neurologic complaints, then neurosyphilis is a primary consideration as a diagnosis.
with every lumbar puncture to be able to evaluate a low CSF glucose level. Even when one or more of these abnormalities are present, it still may not be possible to reach a definite diagnosis.
An Approach to Clinical Diagnosis The diagnostic strategy shown in Figure 75-3 is suggested. The neuroimaging study itself, and not just the report of the study, should be reviewed by the clinician.
SUGGESTED READINGS Lumbar Puncture in Patients with AIDS The lumbar puncture can be hazardous in HIV-infected patients. Such patients may have parenchymal brain disease with mass effect and be asymptomatic or largely asymptomatic. For that reason, neuroimaging should be done first, before the lumbar puncture, in all HIV-infected patients. For patients with a large amount of mass effect, lumbar puncture is contraindicated. The CSF can be difficult to interpret in HIV-infected patients, and careful thought should be given to what information is needed from the lumbar puncture. An opening pressure should be obtained every time because many CNS diseases in patients with AIDS are complicated by elevated intracranial pressure. An elevated CSF white cell count (more than 5/mm3) is seen in 25% of HIV-infected patients undergoing a diagnostic lumbar puncture, an elevated CSF protein level (more than 50 mg/dL) in 50%, and hypoglycorrhachia in 10%. Because hypoglycorrhachia is so common, a concomitant blood glucose level should be obtained
76
Berger J R AIDS and the nervous system. pp. 743-762. In Aminoff M (ed): Neurology and General Medicine. 3rd ed. Churchill-Livingstone, Philadelphia, 2001 Gordon SM, Eaton ME, George R et al: The response of symptomatic neurosyphilis to high-dose intravenous penicillin G in patients with human immunodeficiency virus infection. N Engl J Med 331:14691473, 1994 Hollander H, McGuire D, Burack J H Diagnostic lumbar puncture in HIV-infected patients: analysis of 138 cases. Am J Med 96:223-228, 1994 Sidtis JJ, Gatsonis, Price RW et al: Zidovudine treatment of the AIDS dementia complex: results of a placebo-controlled trial. Ann Neurol 33:343-349, 1993 Simpson DM, Tagliati M: Neurologic manifestations of HIV infection (Review). Ann Intern Med 121:769-785, 1994 Worley JM, Price RW. Management of neurologic complications of HIV-1 infection and AIDS. pp. 193-217. In Sande MA, Volberding PA (eds): The Medical Management of AIDS. 3rd Ed. WB Saunders, Philadelphia, 1992
HIV Infection and Diseases of the Spinal Cord, Nerve Roots, Peripheral Nerves, and Muscle Bradley K. Evans
In patients with acquired immunodeficiency syndrome (AIDS), three common reasons for neurologic consultation are gait instability, painful feet, and urinary retention with inability to walk. These are usually caused by disease of the spinal cord (vacuolar myelopathy), peripheral nerves (distal sensory polyneuropathy), and nerve roots (cytomegalovirus [CMV] polyradiculitis), respectively. In addition to these common syndromes, human immunodeficiency virus (HIV)-infected patients can also develop other neuropathies and myopathies. VACUOLAR MYELOPATHY Vacuolar myelopathy is the most common cause of walking problems in HIV-infected patients. Patients tend to have a CD4 count less than 200/mm3, but the CD4 count may occasionally be as high as 500/mm3. Vacuolar myelopathy is a unique spinal cord syndrome, seen only in HIV-infected patients. Despite this strong
association with HIV infection, the exact pathophysiology is not known. There is no effective treatment. Over several months, walking deteriorates, and patients eventually need gait assistance and sometimes a wheelchair. Clinical Manifestations Symptoms begin with gait instability, which is slowly progressive over several weeks. The upper extremities are not affected. Some patients notice proximal weakness, but there is no urinary incontinence, except perhaps in the latest stages of the illness. Neurologic abnormalities are confined to the lower extremities and are symmetrical. The gait is wide-based and unsteady. Patients are unable to tandem walk, but they do not have a Romberg sign. Patients have proximal weakness, brisk reflexes, and bilateral Babinski toe signs. Sensation, including vibration sensation, is normal or nearly normal.
500
Immune and Infectious Disease
Viral Infections
”HIBGIA”: Sometimes Useful in Diagnosis One principle sometimes helpful in diagnosis is called “HIBGIA” (“Had it before, got it again”). This refers to the fact that disease recurrence is common in patients with AIDS because of failure of acute therapy, failure of maintenance therapy, or failure to take maintenance therapy. By this principle, if a patient had a disease, particularly an infectious disease, and now has new neurologic complaints, then it is likely that the patient has recurrence of the disease. For example, if a patient was previously treated for syphilis and now has neurologic complaints, then neurosyphilis is a primary consideration as a diagnosis.
with every lumbar puncture to be able to evaluate a low CSF glucose level. Even when one or more of these abnormalities are present, it still may not be possible to reach a definite diagnosis.
An Approach to Clinical Diagnosis The diagnostic strategy shown in Figure 75-3 is suggested. The neuroimaging study itself, and not just the report of the study, should be reviewed by the clinician.
SUGGESTED READINGS Lumbar Puncture in Patients with AIDS The lumbar puncture can be hazardous in HIV-infected patients. Such patients may have parenchymal brain disease with mass effect and be asymptomatic or largely asymptomatic. For that reason, neuroimaging should be done first, before the lumbar puncture, in all HIV-infected patients. For patients with a large amount of mass effect, lumbar puncture is contraindicated. The CSF can be difficult to interpret in HIV-infected patients, and careful thought should be given to what information is needed from the lumbar puncture. An opening pressure should be obtained every time because many CNS diseases in patients with AIDS are complicated by elevated intracranial pressure. An elevated CSF white cell count (more than 5/mm3) is seen in 25% of HIV-infected patients undergoing a diagnostic lumbar puncture, an elevated CSF protein level (more than 50 mg/dL) in 50%, and hypoglycorrhachia in 10%. Because hypoglycorrhachia is so common, a concomitant blood glucose level should be obtained
76
Berger J R AIDS and the nervous system. pp. 743-762. In Aminoff M (ed): Neurology and General Medicine. 3rd ed. Churchill-Livingstone, Philadelphia, 2001 Gordon SM, Eaton ME, George R et al: The response of symptomatic neurosyphilis to high-dose intravenous penicillin G in patients with human immunodeficiency virus infection. N Engl J Med 331:14691473, 1994 Hollander H, McGuire D, Burack J H Diagnostic lumbar puncture in HIV-infected patients: analysis of 138 cases. Am J Med 96:223-228, 1994 Sidtis JJ, Gatsonis, Price RW et al: Zidovudine treatment of the AIDS dementia complex: results of a placebo-controlled trial. Ann Neurol 33:343-349, 1993 Simpson DM, Tagliati M: Neurologic manifestations of HIV infection (Review). Ann Intern Med 121:769-785, 1994 Worley JM, Price RW. Management of neurologic complications of HIV-1 infection and AIDS. pp. 193-217. In Sande MA, Volberding PA (eds): The Medical Management of AIDS. 3rd Ed. WB Saunders, Philadelphia, 1992
HIV Infection and Diseases of the Spinal Cord, Nerve Roots, Peripheral Nerves, and Muscle Bradley K. Evans
In patients with acquired immunodeficiency syndrome (AIDS), three common reasons for neurologic consultation are gait instability, painful feet, and urinary retention with inability to walk. These are usually caused by disease of the spinal cord (vacuolar myelopathy), peripheral nerves (distal sensory polyneuropathy), and nerve roots (cytomegalovirus [CMV] polyradiculitis), respectively. In addition to these common syndromes, human immunodeficiency virus (HIV)-infected patients can also develop other neuropathies and myopathies. VACUOLAR MYELOPATHY Vacuolar myelopathy is the most common cause of walking problems in HIV-infected patients. Patients tend to have a CD4 count less than 200/mm3, but the CD4 count may occasionally be as high as 500/mm3. Vacuolar myelopathy is a unique spinal cord syndrome, seen only in HIV-infected patients. Despite this strong
association with HIV infection, the exact pathophysiology is not known. There is no effective treatment. Over several months, walking deteriorates, and patients eventually need gait assistance and sometimes a wheelchair. Clinical Manifestations Symptoms begin with gait instability, which is slowly progressive over several weeks. The upper extremities are not affected. Some patients notice proximal weakness, but there is no urinary incontinence, except perhaps in the latest stages of the illness. Neurologic abnormalities are confined to the lower extremities and are symmetrical. The gait is wide-based and unsteady. Patients are unable to tandem walk, but they do not have a Romberg sign. Patients have proximal weakness, brisk reflexes, and bilateral Babinski toe signs. Sensation, including vibration sensation, is normal or nearly normal.
Chapter 76
W
HIV Infectionand Diseases of the Spinal Cord, Nerve Roots, Peripheral Netves, and Muscle
Neuroimaging is unremarkable. The cerebrospinal fluid (CSF) may show mild pleocytosis, slightly elevated protein level, and, sometimes, a slight hypoglycorrhachia, but these CSF findings are nonspecific and usually are not helpful in the diagnosis. Diagnosis and Differential Diagnosis This clinical pattern is sufficiently distinctive to be virtually diagnostic, and any patient with these clinical findings should be suspected of being HIV infected. Somewhat similar clinical pictures can be seen in spinal cord compression, subacute combined degeneration, and cervical stenosis. Patients with spinal cord compression usually present more acutely with walking problems. They may have back pain and tenderness, urinary incontinence, or asymmetrical findings suggesting a partial Brown-Skquard syndrome. A patient with any one of these findings should undergo neuroimaging of the spinal canal. Lymphoma is the most common cause of spinal cord compression in patients with AIDS, and neuroimaging may also be indicated in patients with lymphoma who have typical findings of vacuolar myelopathy. HIV-infected patients have an increased risk of developing vitamin B,, deficiency. Macrocytosis and pancytopenia, typical clues to this diagnosis, may either be absent or wrongly attributed to HIV infection or its treatment. Because vitamin B,, deficiency is treatable, a serum vitamin B,, level should be done in all patients suspected of having vacuolar myelopathy. Although patients with subacute combined degeneration have a similar gait instability, they also have marked loss of vibration sensation and the Romberg sign, which are not seen in vacuolar myelopathy. Subacute combined degeneration and vacuolar myelopathy are very similar pathologically. Therefore, it seemed that vacuolar myelopathy might be the result of abnormal vitamin B,, metabolism in these patients (despite their normal serum vitamin B,, levels). Further study has shown that plasma and urinary homocysteine and methylmalonic acid values are normal in these patients and that cyanocobalamin, L-methionine, or a combination of the two is not an effective treatment for vacuolar myelopathy. Some HIV-infected patients who were already receiving adequate cyanocobalamin treatment for vitamin B,, deficiency have developed vacuolar myelopathy. The pathogenesis of vacuolar myelopathy therefore remains unknown. Cervical stenosis may also mimic vacuolar myelopathy. Patients with cervical stenosis tend to have distal, not proximal, lower extremity weakness. Neuroimaging tests establish the diagnosis of cervical stenosis. Because most patients with vacuolar myelopathy have proximal weakness, physicians may diagnostically consider a treatable myopathy or neuropathy. Sometimes, a patient has an elevated serum creatine kinase level or other evidence of a myopathy or has electrodiagnostic findings suggesting a concomitant neuropathy, but even in these patients, treatment of the myopathy or neuropathy usually does not improve walking. DISTAL SENSORY, SYMMETRICAL POLYNEUROPATHY Distal sensory, symmetrical polyneuropathy (DSP) is common in patients with AIDS, particularly in those with very low CD4 counts. DSP is an axonal, “dying-back” polyneuropathy, with pathologic changes not only in the distal peripheral nerve but also in the fasciculus gracilis in the cervical spinal cord. It is assumed
501
that HIV itself causes DSP, but how it does is not known. Why some patients with AIDS-about 30%-have DSP but others do not also is unknown. Clinical Manifestations Patients with DSP have dysesthesias in their feet. They may suffer pain, burning, coldness, aching, or just uncomfortable feelings, and walking is painful. They may present in a wheelchair with a primary complaint of “inability to walk.” There may be no neurologic abnormalities, or patients may have a “stocking” loss of light touch and pinprick sensations. Pain sensation remains intact. If there is sensory loss, it does not extend much above the ankles. Ankle jerks often are lost. Clinical abnormalities progress either very slowly or not at all. Patients developing signs of a more severe neuropathy (such as weakness in the lower extremities or any neurologic abnormality in the upper extremities) do not have DSP but another type of peripheral neuropathy. In DSP, electrodiagnostic tests, if they are done, are normal or show only mild distal denervation changes. Diagnosis and Differential Diagnosis Any mild peripheral neuropathy can cause complaints and neurologic findings similar to those of DSP. For instance, diabetes mellitus and alcoholism, the most common causes of peripheral neuropathies, often produce neuropathies in HIV-infected patients, too. Medications can cause a peripheral neuropathy, which, in its early stages, can mimic DSP. In HIV-infected patients, the most commonly implicated drugs are zalcitabine (dideoxycytosine or ddC) vincristine, and isoniazid. The neuropathy caused by ddC is not only dose related but also dependent on individual susceptibility. However, it is not possible to predict who will develop a neuropathy from ddC. Treatment consists of stopping the drug, but the neuropathy may continue to worsen (or “coast”) for up to 8 weeks after ddC is stopped. The neuropathy of vincristine is also related both to dosage and to individual susceptibility.For some of these patients, vincristine neuropathy may be extremely severe, resembling Guillain-Barrk syndrome. Isoniazid neuropathy can vary from a mild peripheral neuropathy to a fulminant syndrome of encephalopathy and diffuse weakness. Patients with a preexisting neuropathy who are malnourished and alcoholic are particularly susceptible. Pyridoxine (vitamin B6) 100 mg/day, given with isoniazid, helps prevent neuropathy and does not diminish isoniazid’s antimycobacterial actions. Preventive treatment with pyridoxine is important because for serious tuberculous infections there may be no practical alternative to isoniazid, even when a patient develops a neuropathy. Treatment In general, treatment of DSP is symptomatic; however, there is an ongoing clinical trial of nerve growth factor treatment to see whether this will directly improve the neuropathy. As far as symptomatic treatment for DSP is concerned, amitriptyline is most commonly prescribed, usually beginning at 25 mg at bedtime and increasing to 100 to 150 mg at bedtime. Its side effects are mental confusion, orthostatic hypotension, and urinary retention.
502
Immune and Infectious Disease
Viral Infections
Mexiletine, clonazepam, and capsaicin cream are useful alternatives to amitriptyline for some patients. Opiates are also effective. CYTOMECALOVIRUS POLYRADlCULlTlS This syndrome occurs exclusively in patients with AIDS, usually when the CD4 count is less than 50/mm3. In fact, many patients are being treated for a CMV infection elsewhere in the body at the time this illness begins. Clinical Manifestations The first complaint is either inability to walk or urinary retention. Symptoms progress over a few days to a couple of weeks, so patients may develop both problems. In addition to these primary complaints, about half of patients have superficial pain and dysesthesias in the pelvic girdle area. In the full-blown syndrome, patients have severe proximal weakness, loss of sensation in a bathing-trunk distribution, loss of knee jerks, and a large, flaccid urinary bladder. Diagnosis and Differential Diagnosis If diagnosed early, this is a treatable condition. Suspicion of CMV polyradiculitis should arise if the patient has an extremely low CD4 count, known CMV infection elsewhere in the body, rapid onset of proximal weakness, urinary retention, pain and dysesthesias of the proximal lower extremities, or any combination of these findings. The diagnostic test is a lumbar puncture. The CSF shows a polymorphonuclear pleocytosis (usually more than 100/mm3) and hypoglycorrhachia. About half of the time, CMV can be cultured from the CSF. Because neurosyphilis, human T-cell lymphotrophic virus type I, and lymphomatous meningitis can rarely cause a similar polyradiculitis, it is important to do diagnostic tests for these conditions. Other neurodiagnostic tests are only inconsistently helpful. Lumbar magnetic resonance imaging may or may not show contrast enhancement, suggesting inflammation of the meninges and nerve roots. Electromyogram may show denervation changes proximally, but it may not because of the acuteness of the illness.
Untreated, a patient with CMV polyradiculitis becomes bedridden, with urinary retention. With early treatment, urinary bladder function and ability to walk can return. Treatment is high-dose ganciclovir. Patients with negative CSF culture for CMV are just as likely to respond as are those with positive cultures. If the patient is already receiving high-dose ganciclovir, foscarnet is added. Whether glucocorticoids are beneficial is not known. INFLAMMATORY DEMYELINATINC POLYNEUROPATHIES The inflammatory demyelinating polyneuropathies include Guillain-Barre syndrome (or acute inflammatory demyelinating polyneuropathy) and chronic inflammatory demyelinating polyneuropathy (CIDP). These neuropathies tend to occur in the early or middle stages of the illness, often when the patient is not known to be HIV-infected. The neuropathy is identical to that of Guillain-Barre syndrome and CIDP occurring in patients who are
not HIV infected. In HIV-infected patients, the CSF may show a pleocytosis; CSF pleocytosis is unusual in patients who are not HIV infected and therefore is a valuable clue that the patient might have an HIV infection. Diagnosis of HIV infection in inflammatory demyelinating neuropathies requires specific HIV testing. The HIV antibody test may be falsely normal early in the infection, when inflammatory demyelinating neuropathies often occur. Either a p24 antigen test or repeat HIV antibody test in 2 to 6 months is needed for diagnosis in this situation. Whether or not the neuropathy is associated with HIV infection, treatment options are the same: glucocorticoids (for CIDP), plasmapheresis, and y-globulin. MONONEURITIS MULTIPLEX This is a poorly understood condition, which is rare. Patients notice localized pain or sensory loss and focal weakness. If symptoms begin in a single nerve distribution, the condition may initially be misdiagnosed as a compression neuropathy. Later, neurologic deficits indicate involvement of multiple individual nerves. Sometimes localization points to brachial or lumbar plexus lesions. Although this syndrome is vasculitic, the cause or causes are not known, but HIV, CMV, and hepatitis B virus have been implicated. Reportedly, mononeuritis multiplex early in the course of HIV infection may spontaneously remit, whereas mononeuritis multiplex in patients with low CD4 counts tends to progress. With progression, mononeuritis multiplex becomes symmetrical and clinically resembles a generalized polyneuropathy. There is no recognized treatment for mononeuritis multiplex in HIV-infected patients. Case reports suggest that ganciclovir may be effective for some patients with mononeuritis multiplex and low CD4 counts. MYOPATHIES In patients with AIDS, weakness is most commonly caused by malnutrition and concurrent illness. Proximal weakness is more commonly seen with vacuolar myelopathy than with myopathy. Although patients with vacuolar myelopathy and CMV polyradiculitis have proximal weakness, the upper extremities are spared, and there are other neurologic findings in the lower extremities that point to the correct diagnosis. In patients with a clinically important myopathy, the serum creatine kinase level is nearly always elevated. Therefore, this test is useful as a simple screening test for patients with AIDS and unexplained proximal weakness. Serum creatine kinase elevations occur in patients with AIDS who do not have a myopathy, so a high creatine kinase value alone, even in a patient with proximal weakness, is not diagnostic of a myopathy. In patients with AIDS and myopathy, electromyography shows brief, low-amplitude muscle potentials and helps confirm the diagnosis. There are three myopathic syndromes in HIV-infected patients: HIV wasting syndrome, inflammatory myopathy, and mitochondrial myopathy. Patients with the HIV wasting syndrome, which is common, have loss of gluteal mass (“saggy butt syndrome”). This may be caused by a myopathy, but it is usually unaccompanied by any weakness that the patient notices. Inflammatory myopathy can occur anytime during the course of HIV infection, but it is rare. Patients complain of proximal weakness involving the upper and lower extremities. There are no sensory abnormalities. Muscle stretch reflexes usually are dimin-
Chapter 77
ished in proportion to the weakness. The immune pathophysiology of this inflammatory myopathy is not known; HIV is not
found in muscle fibers. It is treated with glucocorticoids (e.g., prednisone 60 mg/day). HIV-infected patients may also have changes in their muscle biopsies consistent with a mitochondrial myopathy (ragged-red fibers). The mitochondrial changes presumably reflect direct muscle toxicity of zidovudine, which inhibits mitochondrial DNA polymerase in vitro. This myopathy is more common in patients who have taken high dosages (e.g., more than 1000 mg/day) of zidovudine for more than 6 months. Now that lower daily dosages of zidovudine are commonly used, this myopathy is rarely a clinical problem. The treatment is to decrease or eliminate zidovudine. On muscle biopsy, a patient with AIDS and a myopathy may have multiple abnormalities: inflammation, ragged-red fibers, and rod (or nemaline) bodies. The presence of all these changes makes it difficult to know what therapy to recommend. Either glucocorticoid treatment or decreasing zidovudine can be tried first.
77
HTLV-I Infection
SO5
SUGGESTED READINGS Berger J R AIDS and the nervous system. pp. 743-762. In Aminoff M (ed): Neurology and General Medicine. 3rd Ed. Churchill Livingstone, Philadelphia, 2001 Dalakas M, Illa I, Pezeshkpour GH et ak Mitochondrial myopathy caused by long-term zidovudine therapy. N Engl J Med 322:1098-1105, 1990 Simpson DM, Tagliati M: Neurologic manifestations of HIV infection. Ann Intern Med 121:769-785, 1994 So YT, Olney FUC Acute lumbosacral polyradiculopathy in acquired immunodeficiency syndrome: experience in 23 patients. Ann Neurol 3553-58, 1994 Worley JM, Price RW Management of neurologic complications of HIV-1 infection and AIDS. pp. 193-217. In Sande MA, Volberding PA (eds): The Medical Management of AIDS. 3rd Ed. WB Saunders, Philadelphia, 1992
HTLV-I Infection Robert R. McKendall
The discovery of human T-cell lymphotrophic virus type I (HTLV-I) and its linkage to an unusual leukemia and chronic myelopathy is an extraordinary story of modern-day medical scientific investigation. In 1980, Poeisz and his collaborators isolated a retrovirus from fresh lymphocytes of an American patient with cutaneous T-cell lymphoma. This was the first human retrovirus isolated, and it was called HTLV-I. A worldwide search for links between hematologic malignancies and human retroviruses ensued. In Martinique, neurologist Jean Claude Vernant noted a patient with tropical spastic paraparesis (TSP) who had serum antibodies to HTLV-I. He had a group of 25 patients with TSP tested for serum HTLV-I antibodies, and 78% were positive. This was the first link of TSP with HTLV-I. Independently, Mitsuhiro Osame observed multilobulated flower lymphocytes in the blood and cerebrospinal fluid (CSF) of some Japanese patients with spastic paraparesis. These cells were similar to the leukemic cells of adult T-cell lymphoma. Osame’s patients were shown to have serum and CSF antibodies to HTLV-I, and he reported on a new clinical entity, which he named HTLV-I-associated myelopathy (HAM). Soon, the DNA from HAM cell lines was shown to be identical to DNA from adult T-cell leukemia cell lines. Finally, based on seroepidemiologic, clinical,
pathologic, and viral isolation similarities, HAM and TSP were shown to be the same disease, caused by the retrovirus responsible for adult T-cell lymphoma (HTLV-I). In recent years, HTLV-I virus has been linked to uveitis and infective dermatitis of children. Other conditions less well proven but linked to the virus include interstitial cystitis, persistent prostatitis, polymyositis, arthropathy, and Sjogren’s syndrome. ______
EPIDEMIOLOGY Seroepidemiologic studies have expanded the known HTLV-I endemic areas far beyond the original descriptions in Japan and the Caribbean. Endemic regions exist in Central America, South America (Columbia, Venezuela, Peru, Bolivia, and Brazil), and Africa (Uganda, Ivory Coast, Tanzania, and Zaire). The virus remains rare in Europe and Australia. In North America, seropositive people have been found in Canada, the United States, and Mexico. The prevalence rate in U.S. volunteer blood donors is 0.025%. Most cases of HAM/TSP in the United States have occurred in immigrants, patients who had sexual partners from endemic areas, or blood transfusion recipients or in association with intravenous drug abuse. Endemic
Chapter 77
ished in proportion to the weakness. The immune pathophysiology of this inflammatory myopathy is not known; HIV is not
found in muscle fibers. It is treated with glucocorticoids (e.g., prednisone 60 mg/day). HIV-infected patients may also have changes in their muscle biopsies consistent with a mitochondrial myopathy (ragged-red fibers). The mitochondrial changes presumably reflect direct muscle toxicity of zidovudine, which inhibits mitochondrial DNA polymerase in vitro. This myopathy is more common in patients who have taken high dosages (e.g., more than 1000 mg/day) of zidovudine for more than 6 months. Now that lower daily dosages of zidovudine are commonly used, this myopathy is rarely a clinical problem. The treatment is to decrease or eliminate zidovudine. On muscle biopsy, a patient with AIDS and a myopathy may have multiple abnormalities: inflammation, ragged-red fibers, and rod (or nemaline) bodies. The presence of all these changes makes it difficult to know what therapy to recommend. Either glucocorticoid treatment or decreasing zidovudine can be tried first.
77
HTLV-I Infection
SO5
SUGGESTED READINGS Berger J R AIDS and the nervous system. pp. 743-762. In Aminoff M (ed): Neurology and General Medicine. 3rd Ed. Churchill Livingstone, Philadelphia, 2001 Dalakas M, Illa I, Pezeshkpour GH et ak Mitochondrial myopathy caused by long-term zidovudine therapy. N Engl J Med 322:1098-1105, 1990 Simpson DM, Tagliati M: Neurologic manifestations of HIV infection. Ann Intern Med 121:769-785, 1994 So YT, Olney FUC Acute lumbosacral polyradiculopathy in acquired immunodeficiency syndrome: experience in 23 patients. Ann Neurol 3553-58, 1994 Worley JM, Price RW Management of neurologic complications of HIV-1 infection and AIDS. pp. 193-217. In Sande MA, Volberding PA (eds): The Medical Management of AIDS. 3rd Ed. WB Saunders, Philadelphia, 1992
HTLV-I Infection Robert R. McKendall
The discovery of human T-cell lymphotrophic virus type I (HTLV-I) and its linkage to an unusual leukemia and chronic myelopathy is an extraordinary story of modern-day medical scientific investigation. In 1980, Poeisz and his collaborators isolated a retrovirus from fresh lymphocytes of an American patient with cutaneous T-cell lymphoma. This was the first human retrovirus isolated, and it was called HTLV-I. A worldwide search for links between hematologic malignancies and human retroviruses ensued. In Martinique, neurologist Jean Claude Vernant noted a patient with tropical spastic paraparesis (TSP) who had serum antibodies to HTLV-I. He had a group of 25 patients with TSP tested for serum HTLV-I antibodies, and 78% were positive. This was the first link of TSP with HTLV-I. Independently, Mitsuhiro Osame observed multilobulated flower lymphocytes in the blood and cerebrospinal fluid (CSF) of some Japanese patients with spastic paraparesis. These cells were similar to the leukemic cells of adult T-cell lymphoma. Osame’s patients were shown to have serum and CSF antibodies to HTLV-I, and he reported on a new clinical entity, which he named HTLV-I-associated myelopathy (HAM). Soon, the DNA from HAM cell lines was shown to be identical to DNA from adult T-cell leukemia cell lines. Finally, based on seroepidemiologic, clinical,
pathologic, and viral isolation similarities, HAM and TSP were shown to be the same disease, caused by the retrovirus responsible for adult T-cell lymphoma (HTLV-I). In recent years, HTLV-I virus has been linked to uveitis and infective dermatitis of children. Other conditions less well proven but linked to the virus include interstitial cystitis, persistent prostatitis, polymyositis, arthropathy, and Sjogren’s syndrome. ______
EPIDEMIOLOGY Seroepidemiologic studies have expanded the known HTLV-I endemic areas far beyond the original descriptions in Japan and the Caribbean. Endemic regions exist in Central America, South America (Columbia, Venezuela, Peru, Bolivia, and Brazil), and Africa (Uganda, Ivory Coast, Tanzania, and Zaire). The virus remains rare in Europe and Australia. In North America, seropositive people have been found in Canada, the United States, and Mexico. The prevalence rate in U.S. volunteer blood donors is 0.025%. Most cases of HAM/TSP in the United States have occurred in immigrants, patients who had sexual partners from endemic areas, or blood transfusion recipients or in association with intravenous drug abuse. Endemic
504
Immune and Infectious Disease
Nerves, and Muscle
infection in the United States has been well documented or is highly likely in Texas, North Carolina, Alabama, South Carolina, New York, Alaska, and Florida. Overall epidemiologic studies of HAM frequency and seropositivity rates have estimated that seropositive people have a 1% risk of developing adult T-cell lymphoma or HAM/TSP.
CLINICAL FEATURES Progressive leg weakness, spasticity, and urinary symptoms are the hallmarks of this disease. Back pain is less consistent. Patients often complain of difficulty walking rather than leg weakness; stiffness is the most common complaint. Foot dragging, falling, and difficulty running are other symptoms, and some impairment of ambulation is present in 60% to 80% of patients. Urinary retention, urgency, and incontinence are common, though not as primary presenting complaints. Impotence and constipation occur less often. Sensory disturbances are occasional and usually mild. Paresthesias occur in 25% to 33% of cases, and sensory cord levels are present in only 10% to 25% of cases. Cranial nerves usually are not impaired, although nystagmus and diplopia occur in 8%, and transient seventh nerve paralysis has been reported. Intention tremor, dysmetria, deafness, and retrobulbar neuropathy are other rare features. On neurologic examination, the findings reflect involvement primarily of the pyramidal tracts (motor), with lesser involvement of the posterior columns (proprioception). Weakness is primarily proximal, in the iliopsoas and gluteus medius. The legs are uniformly involved, and the arms are weak in up to 33% of patients. Hyperreflexia with or without clonus is present in 100% of patients, and upgoing Babinski signs are present in more than 90% of patients. A jaw jerk is present in 12% to 33% of patients in the larger series. The gait exhibits mild scissoring and an awkward stiffness. About 50% need a cane or other gait appliance. The diminished vibration sensation and proprioception in the feet and toes are mild. Involvement of touch and pain fibers is uncommon (6% to 10%). Brain magnetic resonance imaging (MRI), electroencephalography (EEG), and pathologic evaluation have shown that the disease clearly involves widespread areas of the nervous system; however, clinical symptoms of involvement outside the spinal cord are not often prominent. The onset and course are highly variable; most patients (75%) have an insidious course progressing over months to years. About 10% to 20% of cases progress to severe gait impairment over 1 to 3 months. Rarely, a more acute onset simulating a transverse myelopathy or even a vascular event has been observed. The disease usually begins with asymmetric leg weakness and stiffness. Over months, the other leg becomes involved. Mild paresthesias may develop, and the patient may begin to notice jumping or jerking of one or both legs caused by spasticity. Backache may then develop as the spasticity becomes more pronounced. Occasional urinary incontinence or difficulty starting the urine stream develops. When the patient notes interference with ambulation or athletic activities, medical attention is sought.
DIAGNOSIS Laboratory Studies Table 77- 1 summarizes the laboratory findings in HAM/TSP. The leukocyte count is normal, but blood smears may show flower lymphocytes, named for their multilobulated nuclei, which are morphologically similar to adult T-cell lymphoma cells. These cells are 1% of the leukocytes and must be searched for carefully. They
TABLE 77-1. Laboratory Features in Human
T-cell
Lymphotrophic Virus-Associated Myelopathy and Tropical Spastic Paraparesis Serum Flower lymphocytes Hypergammaglobulinemia (IgC and IgA) Oligoclonal bands Antibodies to gag, env, and tax viral proteins Venereal Disease Research Laboratories test positive Increased CD4+4B4+ (helper/inducer) T cells Normal CD4+2H2+(suppressor/inducer) T cells Elevation of circulating adhesion glycoprotein clCAM-1 Cerebrospinal fluid Glucose level normal Protein variably elevated Mononuclear pleocytosis Flower lymphocytes Oligoclonal bands Elevated IgG synthesis rate Anti-HTLV-I-specific antibodies by ELlSA and Western blot Elevated neopterin level Tumor necrosis factor-a detectable in mononuclear cells Elevated IL-1 Elevated IL-6 Elevated interferon-y Not all findings are present in all
patients
may also be present in the CSF, and they are pathognomonic of HTLV-I infection. Flower lymphocytes are CD4+ CD10+, indicating activated T-helper cells. Hypergammaglobulinemia (immunoglobulin [Ig] G and IgA) and serum oligoclonal bands may be important diagnostic clues. Most patients are seropositive for HTLV-I by enzyme-linked immunosorbent assay and Western blot. Interestingly, abnormal tests for syphilis and Lyme disease are common in both serum and CSF.
Cerebrospinal Fluid Abnormalities Routine CSF analysis may be normal or may show various abnormalities. The glucose level is uniformly normal. Protein is elevated in up to 40% of patients, ranging from 50 to 210 mg/dL. Cell counts are elevated in up to 57% of patients, the rise consisting of all mononuclear cells. Flower lymphocytes appear in 12% to 100% of cases. Elevated intrathecal production of IgG, as measured by oligoclonal IgG bands, IgG index, or CSF IgG synthesis rate, occurs in 21% to 85% of patients. The specificity of most of the antibody is unknown, but some of the IgG bands contain antibody to the viral gag protein p24.
Imaging The imaging study of choice for both spinal cord and brain evaluation is MRI. The spinal cord often shows atrophy and high-intensity T2-weighted lesions, which are diffuse in the cervical and thoracic cord (Fig. 77-1). The incidence of MRI abnormalities in the brain ranges from 25% to 80%. Lesions appear in subcortical, deep cerebral, and periventricular areas (Fig. 77-2). The periventricular lesions usually are contiguous with the lateral ventricles, often near the posterior horn, and usually appear as large confluent areas. The subcortical and deep lesions usually are small and multifocal.
Electroencephalographyand Evoked Potentials Diffuse EEG abnormalities occur in 64% of patients, and delays in visual, brainstem auditory, and somatosensory-evoked potentials
Chapter 77 W
HTLV-I Infection
SO5
have been described. However, these studies are nonspecific and not particularly useful diagnostically.
Differential Diagnosis A presumptive diagnosis of HTLV-I myelopathy entails a compatible clinical presentation of progressive or mildly relapsing and remitting myelopathy, a CSF with a low-grade inflammatory and immunoglobulin profile, MRI showing spinal cord atrophy or diffuse T2-weighted bright abnormalities, presence of Western blot-confirmed HTLV-I-specific antibodies in the serum or CSF, and exclusion of other causes, including cord compression, multiple sclerosis, vitamin B,, deficiency, human immunodeficiency virus infection, and Lyme disease. The presumptive diagnosis is strengthened by residence in a high-seroprevalence endemic area, by transfusion exposure, and by a history of intravenous drug abuse. Finding one of the associated systemic diseases commonly accompanying HTLV-I may also be helpful, including pulmonary alveolitis, arthritis not attributable to other causes, uveitis, persistent prostatitis, cystitis, infective dermatitis, and polymyositis. Pulmonary bronchoalveolitis may be detected as a persistent or fluctuating infiltrate on chest radiography. In addition to the findings listed earlier, a definitive diagnosis entails demonstration of virus or viral genes in CSF cells by isolation or polymerase chain reaction, evidence of intrathecal synthesis of specific HTLV-I antibody by comparison of Western blots run with serum and CSF at equal IgG concentrations, or presence of unexplained serum hypergammaglobulinemia or serum oligoclonal bands. Without at least one of the latter three findings, a diagnosis of HTLV-I myelopathy is only presumptive and is especially likely to be wrong in patients from areas of low seroprevalence. Multiple sclerosis would be more likely in those instances.
FIG. 77-1. Spinal cord MRI in a 64-year-old woman with myelopathy and HTLV-I virologically proved to be in cerebrospinal fluid cells. Transverse cut at T8 shows a small spinal cord in a spinal canal that appears large because of the loss in diameter of the spinal cord.
FIG. 77-2. Brain MRI abnormalities in a 53-yearsld black man with virologically proven HTLV-I-associated myelopathy and bilateral lower extremity weakness and urinary hesitation. Multiple areas of high signal intensity clustered in the left medial cerebrum on a T2-weighted scan.
PATHOGENESIS
The pathogenesis of HAM/TSP is incompletely understood. Only 0.25% to 7% of infected patients develop the disease. Several findings distinguish carriers from disease-affected patients and have been used as the basis for some of the therapeutic strategies discussed in this chapter. Afflicted patients have a proviral load in CD4+ cells that is 10 times higher than in carriers and have very high blood levels of CD8+ cytotoxic T lymphocytes (CTLs) that are virus specific. Most of these are directed against HTLV-I-tax gene products, p27x and p40x. In the active early phase of disease (2 to 5 years) the spinal cord shows an inflammatory pathology made up of CD4+ and CD8+ cells as well as B cells and macrophages. Later the inflammation decreases substantially and is made up mostly of CD8+ cells. Three hypotheses describe mechanisms that could contribute to central nervous system (CNS) demyelination and injury. First, infected CD4+ T cells migrate to the CNS and infect resident cells, which are then killed by tax-specific CD8+ CTLs. Second, infected CD4+ cells, which are known to become autoproliferative through virally induced interleukin-2 (IL-2) and IL-2R expression, undergo dramatic clonal expansion producing forbidden antiself clones or antiviral clones capable of cross-reacting through molecular mimicry with self CNS antigens after they migrate to the CNS. The third proposed mechanism is bystander damage, in which interferon-a (IFN-@-secreting HTLV-I-infected CD4+ T cells and their recognition by virusspecific CD8+ T cells in the CNS induce microglia to secrete TNF-a and other cytokines that may be toxic for myelin. Many therapeutic strategies have been directed at reducing proviral load, limiting clonal expansion of infected CD4+ T cells, or reducing the numbers of effector responses of anti-tax CTLs.
506
Immune and Infectious Disease a Other Infections and Mirnickers
PREVENTIONAND TREATMENT Prevention involves four major areas: blood transfusions, sexual transmission, breast feeding, and vaccine development. The rare instances of seronegativeHAM/TSP indicate that transmission by blood cannot be completely eliminated. Strong public health educational programs and marital counseling are needed to promote condom use and to warn seropositive mothers of the risk of transmission by breastfeeding.Vaccines would be cost-effective, at least in high-prevalence endemic areas, but currently no vaccines are in trials. Several treatment approaches are in development, but most have not been subjected to placebo-controlled, blinded trials, so the results must be interpreted cautiously. Oral prednisolone has been the most extensively tried treatment. It was reported to induce improvement over 6 months in the first Japanese reports, but improvement was not maintained after a 2-year follow-up period. There are other reports of continued improvement in a few patients treated with prednisone. Systemic natural human IFN-a was administered to 48 Japanese patients with HAM/TSP for 28 days in a double-blind trial randomized across three dosage levels. Patients treated with the highest dosage (3.0 MU) had statistically significant improvement in motor and urinary function compared with patients treated with 0.3 MU. In an open trial, 6.0 MU natural human IFN-a was administered to seven Japanese HAM patients for 22 weeks and resulted in sustained improvement in 5 (70%). In an open trial, pentoxifylline was associated with increased CSF levels of IL-4 and IL-10, which correlated with clinical improvement in 6 of 12 patients. An open trial with anti-IL-2R monoclonal antibody resulted in dramatic reduction of infected CD4 peripheral blood lymphocytes (PBLs) and viral load in nine patients, three of whom had improvement in their ambulation index. However this treatment also eliminates noninfected CD4 cells, which express IL-2R as a consequence of activation. Heparin has been used based on its ability to inhibit migration of activated T cells into the CNS and to inhibit induction of autoimmune diseases such as experimental allergic encephalomyelitis. Danazol, an anabolic steroid, has been used in two open trials, with modest success. Plasmapheresis has been used in small trials, usually with other immunologic therapies, and it should be tried in the patient who does not respond to steroids or IFN-a; however, the improvement seen with plasmapheresis may not be maintained.
HTLV-I reverse transcriptase is an essential enzyme for viral replication. Some reverse transcriptase-inhibiting drugs used to treat human immunodeficiency virus are also active against HTLV-I virus and were used with the rationale of reducing proviral burden. Results of treatment with zidovudine at dosages of 0.5 to 1 glday have been mixed and largely disappointing. However, lamivudine treatment in an open trial of five patients was shown to cause a 90% reduction of viral DNA in peripheral blood mononuclear cells (PBMC). In one patient, who had recent-onset disease, there was a fall in virus-specific CTLs and clinical improvement, which was not detailed. Supportive therapy of spasticity and urinary sphincter disturbances can be very helpful. Administration of baclofen, a-adrenergic medications, and anticholinergic medications is similar to that of myelopathies of other causes. The practitioner is well advised to cautiously interpret failed or unsustained responses seen in some trials. Small patient numbers, inadequate empirical dosing, too brief a duration of treatment, and inclusion of patients with burned-out late phase disease make it difficult to interpret these failures.
SUGGESTED READINGS Izumo S, Goto I, Itoyama Y et ak Interferon-a is effective in HTLV-Iassociated myelopathy: a multicenter, randomized, double-blind, controlled trial. Neurology 46:1016-1021, 1996 McKendall RR: HTLV-1 diseases. pp. 737-772. In McKendd RR,Stroop WG (eds): Handbook of Neurovirology. Marcel Dekker, New York, 1994 Nakagawa M, Izumo S, Ijichi S et ak HTLV-I-associated myelopathy: analysis of 213 patients based on clinical features and laboratory findings. J Neurovirol 1:50-61, 1995 Nakagawa M, Nakahara K, Maruyama Y et ak Therapeutic trials in 200 patients with HTLV-I-associated myelopathy/tropical spastic paraparesis. J Neurovirol 2:345-355, 1996 Roman GC Tropical spastic paraparesis and HTLV-1 myelitis. pp. 525542. In McKendall RR (ed): Handbook of Clinical Neurology. Vol56. Elsevier, Amsterdam, 1989 Roman GC, Vernant JC, Osame M (eds): HTLV-1 and the Nervous System. Alan R. Liss, New York, 1989 Taylor G P Pathogenesis and treatment of HTLV-I-associated myelopathy. Sex Transm Infect 74:316-322, 1998
SECTION
6
OTHER INFECTIONS AND MlMlCKERS
78
Chronic and Recurrent Noninfectious Meningitis Elizabeth A. Sekul, Ahmed Sadek, and Tetsuo Ashizawa
Chronic meningitis is defined as cerebrospinal fluid (CSF) pleocytosis for more than 4 weeks in association with clinical signs of meningitis such as headache, fever, and neck stiffness. Recurrent meningitis implies cellular clearing from the CSF between episodes. Chronic or recurrent lymphocytic meningitis can present a diagnostic challenge, particularly when it is the initial manifestation of multisystem disease. The underlying disease processes that can present with these meningitides are varied, but they can be classified into several categories. Infectious causes, particularly viral, fungal, rickettsial, tubercular, and syphilitic, probably are the most common cause and should be aggressively sought via direct culture, polymerase chain reaction (PCR) assays, antibody titers, and antigen presence (such as VDRL). Parameningeal foci of infection such as mastoiditis can also produce a picture of chronic CSF pleocytosis. Noninfectious causes of chronic or recurrent meningitis include a group of less common disorders (Table 78-1). Because the infectious causes are discussed elsewhere, the focus of this chapter is on the noninfectious causes of chronic and recurrent meningitis, including the vasculitides (which are also discussed in detail in other chapters).
MOLLARET'S MENINGITIS Mollaret's meningitis is a form of recurrent meningitis marked by episodic attacks of fever and myalgia, associated with the signs and symptoms of meningeal irritation. No other organ systems are involved. The attacks are self-limited, resolving without sequelae in 2 to 7 days. Other than the signs of meningeal irritation, the TAW 78-1. Noninfectious Causes of Chronic or Recurrent Meningitis Mollaret's meningitis BehGet's disease Vogt-Koyanagi-Harada syndrome Cranulomatous disease Sarcoidosis Wegenef s granulomatosis Lymphomatoid granulomatosis Primary angiitis of the central nervous system Other autoimmune vasculiides Systemic lupus erythematosus Sjogren's syndrome Systemic necrotizing vasculitides Drug-induced meningitis Meningeal carcinomatosis Spinal arachnoiditis Migraine
1
neurologic examination during the attacks usually is normal; however, seizures, facial nerve palsies, anisocoria, and positive Babinski signs have been reported. The disease duration averages from 3 to 5 years, with the longest reported duration being 28 years. The meningeal attacks are of variable intensity and frequency. Little has been published about ethnic or gender predilections of Mollaret's meningitis. It is generally believed that it commonly afflicts middle-aged subjects with no gender or racial preponderance. Although it is rare in children, patients as young as 1 year old have been reported. In Mollaret's meningitis, the CSF cell count ranges from 200 cells/mm3 to thousands of cells, which are predominantly lymphocytes, with few polymorphonuclear cells and distinguishing endothelial cells intermixed. This endothelial cell is the histologic hallmark of Mollaret's meningitis; however, they are not pathognomonic. They are mononuclear cells of the monocyte lineage with irregular and poorly differentiated nuclear and cytoplasmic membranes. They are present only during the first few days of the attack and then degenerate into lytic or ghostlike cells before they clear completely. The CSF protein is mildly elevated, and the glucose level is normal to slightly low. Oligoclonal bands may be present. The CSF returns to normal within 1 week of the attacks, and between attacks the CSF is normal. The laboratory findings outside the CSF are nonspecific, such as an elevated erythrocyte sedimentation rate or peripheral eosinophilia. The cause of Mollaret's meningitis is unknown, but it is felt to be autoimmune or allergic in nature. No microorganisms have been identified. However, in some cases herpes simplex type 2 DNA has been detected by PCR assay in the CSF during the acute illness, suggesting that this virus may play a major role in the pathogenesis. Because of the self-limited nature of this disease and lack of sequelae, treatment usually is symptomatic. Steroids may reduce the duration of the episode. Prophylactic therapy is controversial. Both prednisone and acyclovir have been reported to be effective prophylaxis. However, the unpredictability of the disease makes treatment efficacy in Mollaret's meningitis difficult to assess. BEH@"'S D I S m E
BehCet's disease is a multisystem disorder that causes aseptic chronic recurrent meningitis, sometimes as a presenting feature, and is also characterized by the classic triad of recurrent oral ulceration, genital ulcerations, and eye inflammation. The disease, though global, is much more common in Japan, the Middle East, and the Mediterranean countries, where its prevalence can reach 507
508
Immune and Infectious Disease
w
Other Infections and Mimickers
10 per ~00,000population. One study in the United States showed a prevalence of 0.3 per 100,000 population. Men are affected two to three times more often than women. Familial cases have been observed. This may be caused by an association with HLA-B5, particularly B51, which has been noted in the Mediterranean populations. However, this association is not as strong in the Western populations. The cause is unknown but probably is autoimmune in nature, mediated by a combination of factors involving immune dysregulation. Several reports suggest that the disease may be triggered by an infectious agent. Streptococcal and herpes infections have been the most widely studied, and results have been promising but not conclusive. Overall, no infectious agent has been reproducibly isolated in Behqet’s disease. The primary pathologic finding is a leukoblastic vasculitis, possibly directed at the vasa vasorum. In addition, musculocutaneous lesions show mononuclear infiltrates of the dermis and epidermis. In the central nervous system (CNS), inflammation, necrosis, gliosis, and variable degrees of demyelination can be seen. Hypercoagulability, probably caused by increased platelet aggregation, decreased prostacyclin synthesis, and decreased fibrinolytic activity also occurs in Behqet’s disease and increases morbidity. Because no combination of historical or laboratory findings is specific for Behqet’s disease, the diagnosis remains clinical. According to the clinical diagnostic criteria established in 1990 by the International Study Group for Behqet’s Disease, the diagnosis depends on the presence of oral ulcerations and two of the following: genital ulcerations, typical defined eye lesions, typical defined skin lesions, or a positive pathergy test. These oral lesions are aphthous or herpetiform ulcerations, which typically heal within several days without scarring and recur at least three times in one 12-month period. They may be very painful. The recurrent genital lesions consist of pustules or painful ulcerations that may scar. Ocular manifestations, which may lead to blindness within 5 years, include retinal vasculitis, hypopyon, and iritis, resulting from anterior uveitis, and in late-stage optic atrophy and secondary glaucoma. The recurrent skin lesions include erythema nodosum, nonpruritic pseudofolliculitis, and subcutaneous thrombophlebitis. A positive pathergy test is 90% specific but only approximately 60% sensitive for Behqet’s disease. BehCet’s disease is a protean disease affecting many systems, including neurologic, musculoskeletal, gastrointestinal, and cardiovascular. Arthritis is reported in 50% of patients and is typically nonmigrating, nonerosive, and oligoarticular, involving large joints. Gastrointestinal manifestations such as constipation, diarrhea, abdominal pain, and vomiting are common (50%). Cardiovascular disease is seen in approximately one third of patients. Thrombotic complications with venous occlusions more so than arterial occlusions can cause thrombotic complications. Arterial aneurysms, including aortic aneurysms, have been reported in conjunction with Behqet’s disease. Neurologic involvement occurs in up to 30% of patients, usually within 5 years of disease presentation; in 5%, it may be the initial presentation. The intermittency of the neurologic features is one of the most characteristic findings. Because of the frequency and severity of neurologic involvement, the term neuro-Beh&s disease was coined in the literature. The mortality rate associated with neuro-Behqet’s disease has been reported as high as 50% with most deaths occurring within 1 year of neurologic symptom onset. However, with improved treatment modalities, mortality rates as low as 13% have been reported. Any portion of the neuraxis may be involved, and neurologic complications can vary from one
relapse to the next. Three common patterns of central neurologic involvement are noted a brainstem syndrome affecting many cranial nerves, a meningoencephalitis syndrome, and an organic confusional state. Meningoencephalitis can occur in up to 12% as the presenting neurologic picture and can vary from uncomplicated aseptic meningitis to a fulminant and fatal meningoencephalomyelitis. Typically, fever, headache, meningismus, and CSF pleocytosis are present. Cerebral infarctions caused by meningeal vessel involvement may occur. The organic confusional state may lead to severe dementia, personality changes, or delirium. CSF pleocytosis may accompany the psychiatric symptoms; however, clinical findings of meningeal irritation usually are absent. In acute meningitis, cell count may exceed 500 cells/mm3, but in chronic manifestations, 60 cells or less usually are noted. Although these cells usually are lymphocytes, polymorphonuclear cells may be seen. The total protein level is normal or slightly elevated. The CSF glucose level in the active stages typically is normal. CSF immunoglobulin G (IgG) and IgA levels are increased with IgA oligoclonal bands but not IgG. The presence of these bands may be used to monitor disease activity. Serum laboratory findings in Behqet’s disease are nonspecific but suggestive of an inflammatory reaction. Cranial computed tomography (CT) and magnetic resonance imaging (MRI) may show signs of infarction or edema and are useful in distinguishing neuroBehqet’s from multiple sclerosis, which also may present with relapsing and remitting course, and from tumors and abscesses. Treatment of Behqet’s disease has been difficult to evaluate because of the relapsing nature of the disease. Both local and systemic treatment are advocated. Topical steroids for oral, genital, and ocular lesions are recommended. Oral ulcers may also respond to topical tetracycline. Corticosteroids remain the mainstay of systemic treatment and are used alone or in conjunction with other immunosuppressants, such as azathioprine or chlorambucil. Prednisone (20 to 100 mglday or 1mglkglday) may be needed to control the ocular and neurologic manifestations. Methylprednisolone 1000 mglday IV for 3 days with or without a prednisone taper has also been efficacious. Other drugs tried in BehCet’s disease include azathioprine, cyclophosphamide, cyclosporine, colchicines, thalidomide, levamisole, a-interferons, and dapsone. Colchicine (1 to 1.5 mg per day) is reported to be effective in treating mucocutaneous symptoms. Plasmapheresis in acute situations has been helpful in some patients. When vaso-occlusive disease occurs, steroids alone are not sufficient, and a combination of immunosuppressant agents and antiplatelet agents should be used.
VOCT-KOYANACI-HARADA SYNDROME Another uveomeningoencephalic syndrome that may be difficult to differentiate from Behqet’s disease is Vogt-Koyanagi-Harada syndrome (VKH). It is more common in pigmented races, particularly Hispanics and Asians. Its onset typically is later than that of Behqet’s disease, peaking in incidence in the fourth to fifth decade. Women are slightly more commonly affected than men. Unlike Behqet’s disease, in which the blood vessels are affected, the cause of VKH appears to be an autoimmune reaction to melanocytes. Melanocytes are located in the skin, uvea and retinal choroid, membranes of the inner ear, and leptomeninges, particularly at the base of the cerebrum, thus accounting for the particular limited pattern of involvement seen in this syndrome. MART-1, a self-antigen expressed on melanocytes and the retina, may be the target antigen. Other candidate antigen proteins
Chapter 78
include tyrosinase-related protein 1 and 2. Genetic predisposition with human leukocyte antigen (HLA) subtypes has been described. HLA-DR4 seems to be the most prevalent subtype in patients with VKH. However, some reports suggest that HLADRBl subtype correlates to the chronicity of the disease. In VKH, the ocular findings usually are more pronounced than the otologic or neurologic manifestations, although involvement of the latter is a rather constant feature. In the early active stage, the ophthalmologic involvement consists of bilateral uveitis and choroidal inflammation, which may result in retinal detachment. In the recovery stage, the retina has a characteristic sunset glow appearance caused by depigmentation. Later ocular findings consist of cataracts, glaucoma, and globe atrophy. In the early active phase, the meningeal involvement may lead to encephalopathy, seizure, myelopathy, or other focal signs. In some cases, the meningitis is subclinical. CSF lymphocytic pleocytosis ranges from less than 20 to 500 cells/mm3. Elevated CSF protein level, averaging 49 mg/dL in one series, occurs in approximately 50% of patients. Opening CSF pressure usually is normal. CSF immunoglobulins have been studied in only a few patients, with occasional elevations of CSF IgG noted. Melaninladen macrophages within the CSF may also occur early in the disease. Other manifestations of VKH include dysacousia with hearing loss and tinnitus, alopecia, poliosis (whitening of the eyebrows and lashes), and vitiligo. Unlike in Behget’s disease, the cutaneous involvement is not ulcerative but rather characterized by depigmentation. The treatment of VKH consists of systemic and local corticosteroid administration. Treatment generally is monitored by ophthalmologic parameters, and patients should be under the care of an ophthalmologist for this. Few studies using other immunosuppressants have been done; their efficacy remains to be proved.
SARCOIDOSIS The prevalence of sarcoidosis in the United States is 10 to 40 per 100,000. It is more common in women than in men and appears to be 10 to 20 times more common in blacks than in whites. The peak age of onset is 25 to 30 years of age, and it is rare below age 15 years. The cause of sarcoidosis is unknown. It is probably an antigen-driven disease because the response to the Kveim antigen has been universal. However, the antigen responsible remains unknown. An infectious cause has been studied extensively, particularly with Myobacterium as the likely candidate antigen, but results via cultures and PCR studies have not been conclusive. A recent report from Japan suggests that propionibacteria genome was detected in the sarcoid lymph nodes, but whether it is the cause has not been determined. Sarcoidosis is responsible for multiple neurologic presentations, including aseptic chronic or recurrent meningitis. Symptomatic neurosarcoidosis occurs in 4% to 14% of patients, usually within the first 2 years of disease onset, and may be the presenting feature. Spontaneous remissions occur in approximately two thirds of patients with neurologic involvement, whereas one third show a progressive course. The shorter the history and the younger the patient, the more likely is the resolution of symptoms. The most common CNS involvement in sarcoidosis is the granulomatous infiltration of the meninges, particularly at the base of the skull. This causes cranial nerve entrapments and subsequent palsies, most commonly of the facial nerve. Facial nerve palsies occur in approximately 50% of those who develop other CNS manifestations. Ocular involvement occurs in 30% of patients with neurosarcoidosis, ranging from
Chronic and Recurrent Noninfectious Meningitis
509
iriditis and uveitis to papilledema as a result of meningeal involvement of the casing of the optic nerve and subsequent swelling. Meningeal involvement can occur in all regions of the CNS and may lead to obstructive hydrocephalus caused by scarring. Involvement over the surface of the brain may act as seizure focus or, if generalized, may present with clinical meningitis. Rarely, space-occupying parenchymal lesions caused by granulomas may occur. Focal involvement of the arachnoid or dura of the spinal cord is unusual but can occur, presenting as transverse myelitis. Involvement of the hypothalamic-pituitary axis is not uncommon, and diabetes insipidus is the most common result. The peripheral nervous system is involved in up to 50% of patients, in a pattern varying from symmetricalpolyneuropathyto mononeuritis multiplex. In these patients, CSF pleocytosis tends to be slight, and the CSF protein is higher, as opposed to that in patients with CNS disease, but glucose level is normal. Myopathy clinically occurs in up to 50% of patients with sarcoid; however, granulomas often are found on muscle biopsy even in asymptomatic patients. The CSF findings in neurosarcoidosis show an elevated cell count, usually less than 100 mononuclear cells/mm3, and an increased protein level, up to 200 mg/dL. Approximately one half of the patients have elevated CSF IgG levels, derived mostly from serum. Rarely, oligoclonal bands are present. A low CSF glucose level may be present, especially when obvious meningeal involvement signs are found. Patients with isolated hypothalamic or pituitary involvement may have normal CSF. CSF angiotensinconverting enzyme (ACE) levels are elevated in approximately 50% of patients with neurosarcoidosis and only 8% of patients with systemic sarcoid. However, this is not specific because the CSF ACE level may also be elevated with tumors or bacterial meningitis. The diagnosis of sarcoidosis is based on the histologic findings of noncaseating granulomas containing large epithelial cells. There is no necrosis in the granulomas. Variable numbers of giant cells are present, of either the Langerhans or foreign body type. Clinically, sarcoidosis is suspected by hilar adenopathy on chest radiograph. Additional suspicion is aroused by demonstrated impairment of the delayed-type skin hypersensitivity response to appropriate antigenic stimulation. Other immunologic alterations include elevation of serum immunoglobulins, particularly IgG, and a positive response to the Kveim-Siltzbach antigen, derived from sarcoidosis-involved lymph node. In approximately 75% of patients with sarcoidosis, a nodule showing the histologic changes resembling sarcoidosis occurs when this antigen is injected intradermally. Approximately 90% of symptoms improve with steroid therapy, although treatment often must continue for months. Oral steroids usually are adequate, such as prednisone 60 to 80 mg/day, with slow switch to alternate-day therapy and then a gradual taper, monitoring for recurrent disease. Several reports suggest that cyclosporine (4 to 6 mg/kg/day) may be helpful in refractory neurosarcoidosis. Other immunosuppressive agents are of possible, unproven benefit.
WECENER‘S CRANULOMATOSIS Wegener’s granulomatosis is a systemic disease characterized by necrotizing granulomata and vasculitis affecting predominantly the medium and small vessels. Typical features of Wegener’s
510
Immune and Infectious Disease W
Other Infections and Mimickers
granulomatosis include granulomatous lesions of the upper and lower respiratory tract, focal segmental glomerulopathy, and necrotizing vasculitis. Approximately 90% of patients present with symptoms related to the upper or lower airway. The incidence of Wegener’s granulomatosis in the United States is approximately 1:30,000. Its peak incidence is in the fourth or fifth decade, with a mean age of 41 years. Its cause is also unknown. Neurologic involvement occurs in up to 30% of patients with Wegener’s granulomatosis and can include aseptic chronic meningitis similar to that seen in sarcoidosis, with granulomatosis in the basilar meninges. However, vascular involvement of the meninges can also occur. CSF may reveal lymphocytosis and elevated protein levels, particularly with meningeal involvement. Mononeuritis multiplex is a common neurologic complication occurring in approximately 15% of patients. Wegener’s granulomatosis can be recognized clinically by the presence of upper and lower respiratory tract lesions, although pathologic diagnosis (biopsy) is mandatory. Basic laboratory tests are unrevealing. Erythrocyte sedimentation rate may be elevated, particularly during periods of active disease. Recently a high specificity for antineutrophil cytoplasmic antibody (c-ANCA) positivity during active disease and Wegener’s granulomatosis has been noted. Recognition of Wegener’s disease is important because it is universally fatal if left untreated, with an average survival of 5 months. However, a remission rate of more than 90% has been reported with immunosuppressive treatment using cyclophosphamide. LYMPHOMATOIDCRANULOMATOSIS Another systemic granulomatosis very similar to Wegener’s granulomatosis is lymphomatoid granulomatosis. Again, the lungs are primarily involved, but unlike Wegener’s granulomatosis, the upper respiratory tract usually is spared. Neurologic manifestations occur in approximately 30% of cases. The most common CNS finding is necrotizing inflammatory masses in the brain parenchyma; however, the meninges often are involved, resulting in multiple cranial nerve palsies, encephalopathy, or radiculopathy with a picture of aseptic chronic meningitis. The cause of lymphomatoid granulomatosis is unknown. It appears to be a mixture of granulomatosis and lymphoproliferative disorders. It progresses to lymphoma in approximately 13% of patients. No consistent laboratory abnormalities are typical. However, in contrast to Wegener’s granulomatosis, leukopenia is very common. The CSF is abnormal in up to 50% of patients with findings similar to those of sarcoidosis and Wegener’s granulomatosis, except that mononuclear cells seen are chiefly reticular cells with some plasma cells and lymphocytes. These cells simulate those found in meningeal lymphoma and other diffuse meningeal neoplasms. Diagnosis is based on the clinical presentation and tissue histology. Treatment is with prednisone and cyclophosphamide.
affected slightly more often than women, and the illness may occur at any age. The disease is very unusual in children. The mortality rate may exceed 85%. PACNS may involve the entire neuraxis, but it predominantly affects the intracranial structures. It is usually asymmetrical in distribution and at times may be remarkably focal. It most commonly involves the small vessels of the leptomeninges; however, larger vessels are involved in up to one third of cases. Clinically, PACNS is subacute in onset. It presents with headache and mental status changes, which progress to confusion and disorientation followed by lethargy and focal signs. Focal or generalized seizures occur in approximately one fourth of patients. Cerebral edema may occur and often is massive. Among untreated people, 90% eventually develop focal CNS signs. The electroencephalogram is abnormal in 80% of patients, most often showing generalized or focal slowing. The erythrocyte sedimentation rate is elevated in approximately 70%, usually in the low range and rarely exceeding 100 mm/hour. Tests for autoantibodies such as antinuclear antibody are consistently negative. CSF abnormalities are seen in 80% of patients. An elevated opening pressure is frequent. The protein concentration is elevated in 80% of patients, with a mean of 160 mg/dL, and the CSF IgG level is elevated in some patients. CSF lymphocytic pleocytosis is noted in approximately two thirds of patients with up to 250 cell/mm3. Some erythrocytes (less than 1000/mm3) may also be seen in one third of patients. CT and MRI studies show patchy areas of ischemia and edema. Angiography is normal in many patients; however, the remaining patients show arterial beading, aneurysms, or arterial branch occlusions. Leptomeningeal biopsy is the most useful method to establish the diagnosis. Histologic findings include angiitis, segmental intimal proliferation, vascular narrowing, and intensive inflammatory infiltrates with granulomas consisting of lymphocytes, plasma cells, multinuclear cells, and fibrinoid necrosis. However, because of the focal nature of the disease, a negative biopsy does not preclude the diagnosis. The mean duration from onset of the symptoms to death is 6 months in untreated patients. Corticosteroids with another immunosuppressant, particularly cyclophosphamide, are the treatment of choice. OTHER AUTOIMMUNE VASCULITIDES Systemic Lupus Erythematosus Neurologic involvement can be documented in 25% to 75% of patients with systemic lupus erythematosus (SLE) at some point in their disease. Psychiatric symptoms or seizures are the most common complications and sometimes are accompanied by CSF lymphocytic pleocytosis. However, clinical aseptic meningitis is rare in SLE, especially as a presenting manifestation. Aseptic meningitis has also been reported in SLE in association with elevated serum antiphospholipid antibodies.
Sjogren’s Syndrome ISOLATED CENTRAL NERVOUS SYSTEM ANGllTlS The fourth noninfectious granulomatous disease that affects the meninges and can present as aseptic chronic meningitis is isolated or primary angiitis of the CNS (PACNS). It is a rare granulomatous vasculitis of unknown cause that is limited largely to the CNS. The incidence of isolated CNS vasculitis is low, but the exact incidence is unknown. It accounts for only a small fraction of dementias, encephalopathies, strokes, and myelopathies. Men are
Sjogren’s syndrome is characterized by keratoconjunctivitis sicca, xerostomia, and connective tissue disorder (usually rheumatoid arthritis). It is associated with anti-SSa and anti-SSb antibodies, which are autoantibodies to extractable components of nuclear cytoplasm. Peripheral nerve involvement is far more common than CNS involvement. However, CNS abnormalities occur in 20% of patients in some series and may mimic multiple sclerosis, with abnormal CSF findings and multiple lesions on MRI. A
Chapter 78
recurrent aseptic meningoencephalitis has also been noted. When present, CNS involvement is associated with cutaneous signs of vasculitis in more than 70% of patients, which in turn is highly correlated with anti-SSa antibodies. The CSF shows an elevated IgG index in nearly 100% of patients with Sjogren’s syndrome and CNS disease. Systemic Necrotizing Vasculiides
Polyarteritis nodosa, Churg-Straws syndrome, temporal arteritis, Takayasu’s arteritis, and drug abuse-associated vasculitis can also involve the meningeal blood vessels. Approximately 20% of patients with these diseases may have clinical or laboratory evidence of aseptic meningitis at some time during their illness. Aseptic meningitis has similarly been reported in other systemic vasculitidessuch as mixed connective tissue disease and Kawasaki’s d’isease. DRUG-INDUCED ASEPTIC MENINGITIS
Aseptic meningitis can also occur as a reaction to a wide variety of drugs taken systemically (Table 78-2). Whether this results from a direct toxic effect from diffusion of the drug across the bloodbrain barrier or from a hypersensitivity reaction of the cerebral blood vessels is unknown. Aseptic meningitis caused by nonsteroidal anti-inflammatory drugs occurs primarily in patients with connective tissue disorders, especially those with SLE and mixed connective tissue disease. Clinically, patients develop the classic signs of meningitis, usually including fever. In most cases, this reaction occurs within hours to 1 day of exposure and is reproducible upon reexposure to the offending agent. CSF studies in general show lymphocyte-predominant pleocytosis unless the fluid was collected early in the course, at which time polymorphonuclear cells may predominate. Eosinophils may also be present. The CSF protein level is mildly elevated, and glucose concentration is normal in most patients. Generally, the symptoms resolve without sequelae, and only supportive therapy is needed. On the first exposure, of course, a full evaluation for other causes of aseptic meningitis usually is warranted. Similar self-limiting aseptic meningitis may be seen in patients who receive a large intravenous dose of y-globulins. MENINGEAL CARCINOMATOSIS
Meningeal carcinomatosis commonly presents with headache, cranial nerve signs, back pain, focal weakness, or seizure. Unlike in most other chronic meningitides, nerve roots, including the cauda equina, often are involved with carcinomatous meningitis. This type of meningitis must be distinguished from the remote effects of cancer, toxicity of treatment, or infections. Malignant meningeal involvement can occur as a primary diffuse infiltration, from either CNS lymphoma or meningeal gliomatosis, or as an extension from a primary brain tumor such as a glioblastoma, astrocytoma, or medulloblastoma. However, a metastasis may also cause meningeal carcinomatosis, most commonly with breast cancer, lung cancer, melanoma, leukemia, and lymphoma. CSF pressure generally is elevated except in the early stages of the disease. The CSF protein level may be normal but usually is elevated. Cell counts typically are elevated but may be normal in up to one third of patients. Large-volume samples or multiple CSF samples may need to be examined cytologically before the malignant cells can be identified. However, the presence of
Chronic and Recurrent Noninfectious Meningitis
51 1
TABLE78-2. Drugs and Chemicals Associated with Aseptic Meningitis Antimicrobial drugs Sulfonamides Trirnethoprim Sulfasalazine Cephalosporin Ciprofloxacin lsoniazid Penicillin Antineoplastics (systemic use) Cytosine arabinoside Corticosteroids Methylprednisolone acetate Hydrocortisone sodium succinate Nonsteroidal anti-inflammatory drugs Diclofenac Ibuprofen Naproxen Sulindac Tolmetin Ketoprofen Salicylates Piroxicam lntrathecal drugs Antineoplastics Cytosine arabinoside Methotrexate Antimicrobials Baclofen Steroids Spinal anesthesia lntrathecal diagnostic agents Radiologic contrast media lophendylate Metrizarnide Radiolabeled albumin Miscellaneousdrugs hathioprine Carbamazepine Famotidine Intravenous immune globulin Murornonab CD-3 Phenazopyridine Pyrazinarnide Ranitidine Vaccines Polio Measles, mumps, and rubella Hepatitis B
malignant cells is not specific for direct meningeal involvement because they are often found in the CSF when brain tumors, particularly involving the ventricular wall or cortex, are present. Hypoglycorrhachia generally reflects diffuse meningeal involvement rather than localized disease. In some cases, cisternal puncture may have a higher yield when the basilar meninges are involved. Elevated CSF immunoglobulins and abnormal CSF IgG index and oligoclonal bands often are present. Tumor markers, such as vasopressin, carcinoembryonicantigen, adrenocorticotropin, lactic dehydrogenase, and P-glucuronidase may also be helpful. MRI or myelography may show thickened, nodular nerve roots or epidural tumors. Meningeal contrast enhancement on MRI or CT is sensitive but not specific for diffuse carcinomatosis. Treatment depends on the tumor type.
SPINAL ARACHNOlDmS Spinal arachnoiditis can be acute, subacute, or chronic. Chronic spinal arachnoiditis can cause chronic CSF lymphocytic pleocytosis and should be considered a variant of chronic meningitis. It
512
Immune and Infectious Disease
Other Infections and Mimickers
usually follows intrathecal injection of a foreign substance, such as contrast material, antibiotics, or anesthetic agents. However, prolapse of vertebral disc, spinal injury or surgery, and infections have been implicated. The presence of blood in the CSF increases the likelihood of developing arachnoiditis. The CSF pleocytosis generally is lymphocytic, but in acute cases following recent foreign substance administration, polynuclear cells may predominate, and a mild eosinophilia may develop. The CSF protein level is elevated to a variable degree. Chronic adhesive arachnoiditis is confirmed by MRI or myelography. Treatment is surgical but not always effective; the arachnoiditis may recur.
MIGRAINES Migraine headaches may be another cause of recurrent CSF lymphocytic pleocytosis. In general, CSF pleocytosis is uncommon in severe but uncomplicated migraines but can occur with elevated cell counts in the range of 15 to 100 cell/mm3. However, patients with complicated or hemiplegic migraines have a higher frequency of CSF abnormalities, with cell count up to 300 cells/mm3 and minor elevation in protein levels.
OTHER CAUSES Recurrent aseptic meningitis can also occur as a result of intermittent leakage of cystic contents from a craniopharyngioma, dermoid cyst, epidermoid cyst, teratoma, or malignant glioma. Cerebral MRI is helpful in establishing the cause of the meningitis in such cases. Patients with familial Mediterranean fever have also been reported to have recurrent aseptic meningitis. One in 2000 subjects who received mumps vaccination have developed aseptic meningitis in Japan and Germany.
means including PCR is necessary in most cases. CSF pleocytosis, protein levels, glucose levels, and immunoglobulin studies are mostly nonspecific. Recognition of systemic manifestations of the baseline diseases that cause aseptic meningitis therefore is often crucial. Various laboratory tests, such as viral titers and other serologic tests, arteriography, CT, MFU, and specific PCR studies may provide important clues for a correct diagnosis. Pathologic diagnosis is sometimes needed, particularly for the granulomatous diseases. Prognosis is variable, ranging from a self-limited benign course to a fatal outcome, depending on the cause. Treatment also depends on the underlying disease. Chronic or recurrent aseptic meningitis often becomes a challenge for physicians and necessitates thorough clinical investigations.
SUGGESTED READINGS Fishman RA: CSF findings in diseases of the nervous system. p. 253. In Fishman RA (ed): Cerebrospinal Fluid in Disease of the Nervous System. 2nd Ed. WB Saunders, Philadelphia, 1992 Frederics JAM, Bruyn G W Mollaret’s meningitis. p. 627. In McKendall RR (ed): Handbook of Clinical Neurology. 56th Ed. Elsevier, New York, 1989 International Study Group for Behget’s Disease: Criteria for diagnosis of Behget’s disease. Lancet 335:1078, 1990 Iomata H, Kato M: Vogt-Koyanagi-Harada disease. p. 611. In McKendall RR (ed):Handbook of Clinical Neurology. 56th Ed. Elsevier, New York, 1989
JainK K Drug-Induced Neurological Disorders. 2nd Ed. Hogrefe & Huber, Gottingen, 2000
Shannon KM, Goetz CG: Connective tissue disease and the central nervous system. p. 389. In Aminoff MJ (ed): Neurology in General Medicine. 2nd Ed. Churchill Livingstone, New York, 1995 Silberberg DH: Sarcoidosis of the nervous system. p. 701. In Aminoff MJ (ed): Neurology in General Medicine. 2nd Ed. Churchill Livingstone, New York, 1995
CONCLUSION
Stratigos AJ, Laskaris G, Stratigos J D Behqet’s disease. Semin Neurol
The causes of culture-negative chronic or recurrent meningitis are diverse, and the diagnosis often is difficult to make, particularly early in the disease process. Exclusion of infectious causes by other
Tucker T, Ellner JJ: Chronic meningitis. p. 188. In Tyler KL, Martin JB (eds): Infectious Disease of the Central Nervous System. FA Davis, Philadelphia, 1993
79
12:346, 1992
Prion Diseases Eugene Lai
The prion diseases are sometimes called transmissible spongiform encephalopathies or transmissible cerebral amyloidoses. They encompass several diseases affecting humans and animals; the human prion diseases include Creutzfeldt-Jakob disease (CJD), Gerstmann-Straussler-Scheinker(GSS)syndrome, kuru, and fatal familial insomnia (FFI; Table 79-1). The unique feature common to these disorders is the sharing of a similar pathogenesis that involves the aberrant metabolism of the prion protein. The term prion was introduced in 1982 by Stanley Prusiner to mean small, proteinaceous infectious particles that resist inactivation by procedures that modify nucleic acids. Recent advances in the molecular biology of prions revealed that a gene located at the short arm of human chromosome 20 codes for the prion protein. It codes for a normal host protein, but the function of the prion
protein has not yet been identified. In human prion diseases, an abnormal form of this protein, which becomes proteinase resistant, accumulates in the brain. These diseases may be sporadic, dominantly inherited, or acquired by transmission. The prion protein, which contains no nucleic acids (DNA or RNA), can produce disease after injection into animals, thus fulfilling its definition as an infectious agent composed purely of protein.
CREUTZFELDT-JAKOB DISEASE CJD is a rare central nervous system disorder characterized by a relentlessly progressive course and an invariably fatal outcome. It constitutes about 75% of all the human prion diseases. Sporadic, familial, and iatrogenic forms of CJD have been described.
512
Immune and Infectious Disease
Other Infections and Mimickers
usually follows intrathecal injection of a foreign substance, such as contrast material, antibiotics, or anesthetic agents. However, prolapse of vertebral disc, spinal injury or surgery, and infections have been implicated. The presence of blood in the CSF increases the likelihood of developing arachnoiditis. The CSF pleocytosis generally is lymphocytic, but in acute cases following recent foreign substance administration, polynuclear cells may predominate, and a mild eosinophilia may develop. The CSF protein level is elevated to a variable degree. Chronic adhesive arachnoiditis is confirmed by MRI or myelography. Treatment is surgical but not always effective; the arachnoiditis may recur.
MIGRAINES Migraine headaches may be another cause of recurrent CSF lymphocytic pleocytosis. In general, CSF pleocytosis is uncommon in severe but uncomplicated migraines but can occur with elevated cell counts in the range of 15 to 100 cell/mm3. However, patients with complicated or hemiplegic migraines have a higher frequency of CSF abnormalities, with cell count up to 300 cells/mm3 and minor elevation in protein levels.
OTHER CAUSES Recurrent aseptic meningitis can also occur as a result of intermittent leakage of cystic contents from a craniopharyngioma, dermoid cyst, epidermoid cyst, teratoma, or malignant glioma. Cerebral MRI is helpful in establishing the cause of the meningitis in such cases. Patients with familial Mediterranean fever have also been reported to have recurrent aseptic meningitis. One in 2000 subjects who received mumps vaccination have developed aseptic meningitis in Japan and Germany.
means including PCR is necessary in most cases. CSF pleocytosis, protein levels, glucose levels, and immunoglobulin studies are mostly nonspecific. Recognition of systemic manifestations of the baseline diseases that cause aseptic meningitis therefore is often crucial. Various laboratory tests, such as viral titers and other serologic tests, arteriography, CT, MFU, and specific PCR studies may provide important clues for a correct diagnosis. Pathologic diagnosis is sometimes needed, particularly for the granulomatous diseases. Prognosis is variable, ranging from a self-limited benign course to a fatal outcome, depending on the cause. Treatment also depends on the underlying disease. Chronic or recurrent aseptic meningitis often becomes a challenge for physicians and necessitates thorough clinical investigations.
SUGGESTED READINGS Fishman RA: CSF findings in diseases of the nervous system. p. 253. In Fishman RA (ed): Cerebrospinal Fluid in Disease of the Nervous System. 2nd Ed. WB Saunders, Philadelphia, 1992 Frederics JAM, Bruyn G W Mollaret’s meningitis. p. 627. In McKendall RR (ed): Handbook of Clinical Neurology. 56th Ed. Elsevier, New York, 1989 International Study Group for Behget’s Disease: Criteria for diagnosis of Behget’s disease. Lancet 335:1078, 1990 Iomata H, Kato M: Vogt-Koyanagi-Harada disease. p. 611. In McKendall RR (ed):Handbook of Clinical Neurology. 56th Ed. Elsevier, New York, 1989
JainK K Drug-Induced Neurological Disorders. 2nd Ed. Hogrefe & Huber, Gottingen, 2000
Shannon KM, Goetz CG: Connective tissue disease and the central nervous system. p. 389. In Aminoff MJ (ed): Neurology in General Medicine. 2nd Ed. Churchill Livingstone, New York, 1995 Silberberg DH: Sarcoidosis of the nervous system. p. 701. In Aminoff MJ (ed): Neurology in General Medicine. 2nd Ed. Churchill Livingstone, New York, 1995
CONCLUSION
Stratigos AJ, Laskaris G, Stratigos J D Behqet’s disease. Semin Neurol
The causes of culture-negative chronic or recurrent meningitis are diverse, and the diagnosis often is difficult to make, particularly early in the disease process. Exclusion of infectious causes by other
Tucker T, Ellner JJ: Chronic meningitis. p. 188. In Tyler KL, Martin JB (eds): Infectious Disease of the Central Nervous System. FA Davis, Philadelphia, 1993
79
12:346, 1992
Prion Diseases Eugene Lai
The prion diseases are sometimes called transmissible spongiform encephalopathies or transmissible cerebral amyloidoses. They encompass several diseases affecting humans and animals; the human prion diseases include Creutzfeldt-Jakob disease (CJD), Gerstmann-Straussler-Scheinker(GSS)syndrome, kuru, and fatal familial insomnia (FFI; Table 79-1). The unique feature common to these disorders is the sharing of a similar pathogenesis that involves the aberrant metabolism of the prion protein. The term prion was introduced in 1982 by Stanley Prusiner to mean small, proteinaceous infectious particles that resist inactivation by procedures that modify nucleic acids. Recent advances in the molecular biology of prions revealed that a gene located at the short arm of human chromosome 20 codes for the prion protein. It codes for a normal host protein, but the function of the prion
protein has not yet been identified. In human prion diseases, an abnormal form of this protein, which becomes proteinase resistant, accumulates in the brain. These diseases may be sporadic, dominantly inherited, or acquired by transmission. The prion protein, which contains no nucleic acids (DNA or RNA), can produce disease after injection into animals, thus fulfilling its definition as an infectious agent composed purely of protein.
CREUTZFELDT-JAKOB DISEASE CJD is a rare central nervous system disorder characterized by a relentlessly progressive course and an invariably fatal outcome. It constitutes about 75% of all the human prion diseases. Sporadic, familial, and iatrogenic forms of CJD have been described.
Chapter 79
TABU 79-1. The Human Prion Diseases Disease
Etiolonv
Creutzfeldt-Jakob Sporadic Familial Iatrogenic New variant Cerstmann-Straussler-Scheinker Kuru Fatal familial insomnia
Unknown Prion mutation Transmission Transmission Prion mutation Transmission Prion mutation
Prion Diseases
513
new variant CJD has been identified in Europe in the last 10 years. It has affected more than 80 people and is thought to be linked to the consumption of beef from cattle that contracted bovine spongiform encephalopathy (or mad cow disease). These patients have a number of distinctive features compared with those of classic CJD, including a young age at disease onset, a slower clinical course, the presence of early psychiatric and sensory symptoms, and the finding of widespread protein clumps or plaques on neuropathologic examination.
Diagnosis Clinical Features CJD usually occurs in late middle age, but its range can extend from 16 to 82 years. Both sexes are affected equally. The clinical manifestations encompass almost the entire nervous system and may be confusing in the early stages of the disease (Table 79-2). Approximately one third of patients present with mental deterioration that includes memory loss, behavioral abnormalities, and confusion; another third of patients have only physical complaints, most often cerebellar ataxia or visual disturbance; and the final third of patients present with a mixture of both mental and physical symptoms; More than one fourth of the patients report prodromal symptoms, consisting of fatigue, disturbance of sleep patterns or appetite, anxiety, or weight loss that may last for several weeks. As a rule, the disease progresses rapidly, and symptoms advance within weeks. Memory decline usually progresses to profound and global intellectual deficits, often with prominent grasp, glabellar, palmomental, and snout reflexes. Movement disorders, such as cerebellar ataxia, tremor, dysarthria, hypokinesia, rigidity, or choreoathetoid movements, may become pronounced. Myoclonus, often provoked by sensory stimuli, usually appears in midcourse of the disease. Pyramidal tract involvement is also common, as manifested by hyperreflexia, extensor plantar reflexes (Babinski signs), and clonus. Visual complaints include hallucinations, diplopia, dimming or blurring of vision, and visual distortions that may evolve into cortical blindness. The patient continues to deteriorate to mutism, complete helplessness, and a vegetative existence. The disease typically ends in death from respiratory or systemic infections, usually within 1 year of onset. Only 5% to 10% of patients may have clinical courses of more than 2 years.
The routine analysis of cerebrospinal fluid (CSF) usually is unremarkable, but an immunoassay for detecting the 14-3-3 protein in CSF is useful for confirming the diagnosis. However, a negative test does not rule out CJD. Though typically normal, a computed tomography scan of the head may show nonspecific cerebral atrophy. Magnetic resonance imaging (MRI) of the brain, especially using diffusion-weighted imaging (DWI) , may allow earlier and noninvasive diagnosis of CJD (Fig. 79-1). Areas of bright signal abnormalities on DWI correlate well with areas of the most severe and characteristic neuropathologic changes in CJD, typically in the basal gangha and deeper cortical layers. The electroencephalogram (EEG) is helpful diagnostically if it shows the characteristic abnormality. It is often normal early in the course of illness. In later stages, it may show generalized slow wave activity or background disorganization that progresses to a typical pattern of periodic (1 or 2 cycles/second) sharp waves against a slow background or, in some cases, to episodic burst suppression with high-voltage activity. A clinical triad of dementia, myoclonus, and the characteristic EEG pattern is highly indicative of CJD. The diagnosis can be confirmed by finding the typical light microscopy spongiform vacuolar changes in brain tissue during brain biopsy. Immunohistochemistry or Western blot analysis with antibodies against the prion protein further improves the specificity of the diagnosis. Differential diagnosis should include progressive neurodegenerative diseases such as Alzheimer’s disease, severe parkinsonism, and cerebellar degeneration. Acquired immunodeficiency syndrome, cerebrovascular disease, drug toxicities, central nervous system neoplasm or infection, acute exacerbation of multiple sclerosis, and acute psychosis should also be ruled out.
Pathology Epidemiology and Causes The disease occurs in adults throughout the world, with an annual incidence of 0.5 to 2.0 cases per 1 million population. Sporadic CJD constitutes most cases. Its exact cause is unknown but has been hypothesized to involve a somatic mutation of the prion gene that causes a spontaneous conformational conversion of the normal host prion protein to an abnormal form. A small proportion of the cases, varying from 5% to 15%, according to various reports, are familial and may arise from a germ line mutation in the prion protein gene. Familial CJD has been found to be prevalent among Libyan Jews. The disease is also transmissible, as demonstrated in cases of iatrogenic CJD. Human-tohuman transmission has occurred inadvertently during corneal and cadaveric dura mater transplantation and during the use of contaminated brain electrodes. A few cases have also resulted from treatment with growth hormone prepared from pooled human cadaveric pituitary glands. No transmission of the disease by casual contact or between family members has been reported. A
The pathological abnormalities in CJD are confined to the central nervous system. There is degeneration and disappearance of
TABLE 79-2. Clinical Characteristics of Creutzfeldt-Jakob
Disease (Percentage of Patients with Symptoms and Signs) SvmDtomr and Sims
Mental deterioration Memory loss Higher cortical functions Behavioral abnormalities Involuntary movements Myoclonus Cerebellar ataxia Pyramidal weakness or hyperreflexia Extrapyramidal rigidity Periodic EEC Visual or oculomotor disturbance
At Onset
69 48 16 29 4 1
33 2 0.5 0 19
Durinn Course 100 100
73 57 91
78 71 62 56 60 42
514
Immune and Infectious Disease w Other Infections and Mirnickers
specimens should be disposed of as biohazard waste after decontamination.
GERSTMANN-STRjiUSSLER-SCHEINKER SYNDROME GSS syndrome is a rare neurodegenerative disease that has an apparent autosomal dominant pattern of inheritance. There are approximately 30 known families with GSS in various parts of the world, including the Americas, Europe, and Japan. The clinical features are dominated by cerebellar ataxia, pyramidal signs, and dementia. The average age of onset is 40 years, and the average duration is about 5 years, with a range of 1 to 11 years. Its neuropathology is characterized by extensive multicentric prioncontaining amyloid plaques and spongiform change in the gray matter of the cortex. Mutations in the protein coding region of the prion protein gene that result in amino acid substitutions have been found in several kindreds.
KURU
Kuru is a disease of historic interest only. It is restricted to the Fore tribe of Papua New Guinea and is transmitted by ritual cannibalistic practices during the care of the dead. Patients present with progressive emotional lability, mental slowing, and movement disorders, such as ataxia, tremor, and rigidity, that progress to mutism and vegetative state. Death occurs within 1 year of symptom onset. Kuru has largely disappeared as a result of the cessation of the practice of cannibalism. FIGURE 79-1. Diffusion-weighted MRI of the brain showing bright signal in the basal ganglia characteristic of Creutzfeldt-Jakob disease.
FATAL FAMILIAL INSOMNIA
neurons and their processes together with widespread hypertrophy and proliferation of astrocytes. These changes result in microscopic vacuolation and spongy appearance of the gray matter, particularly the cerebral cortex, hence the term spongiforrn encephalopathy In 5% to 20% of cases, prion immunopositive amyloid plaques have been observed. The white matter usually is preserved, and inflammatory reactions are absent.
FFI is a progressive autosomal dominant disease with subacute onset that is characterized by untreatable insomnia, dysautonomia, motor disturbance, and severe selective atrophy of thalamic nuclei. Several Italian families have been studied, and FFI is also linked to a mutation in the prion protein gene.
SELECTED READINGS Management
No effective treatment is available, and the disease is uniformly fatal. In view of the transmissibility of the disease iatrogenically, certain precautions should be taken in the medical care and handling of materials from the patients. It should be noted that because of the low and limited infectivity of the responsible agent, affected patients present minimal risks to caretakers, and the handling of blood and tissue specimens is not dangerous if appropriate precautions are taken. Isolation of patient is not necessary. Casual skin contacts are allowed, and hand washing with ordinary soap afterwards is recommended. Gloves should be worn when handling blood, body fluids, and tissues, and accidental skin exposure to these samples should be washed with a 1:lO dilution of sodium hypochlorite (household bleach). Contaminated surgical and pathologic instruments can be cleaned by steam autoclaving at 132°C and 15-lb/in2 pressure for 1 hour or by immersing for 1 hour in 5% sodium hypochlorite. Laboratory
Brown P, Gibbs CJ, Rodgers-Johnson P et al: Human spongiform encephalopathy: the National Institute of Health series of 300 cases of experimentally transmitted disease. Ann Neurol 35:513-529, 1994 Hsich G, Kenney K. Gibbs CJ et a1 The 14-3-3 brain protein in cerebrospinal fluid as a marker for the transmissible spongiform encephalopathies. N Engl J Med 335:924-930, 1996 Lantos P L From slow virus to prion: a review of transmissible spongiform encephalopathies. Histopathology 20:1-1 1, 1992 Mittal S, Farmer P, Kalina P et al: Correlation of diffusion-weighted
magnetic resonance imaging with neuropathology in CreutzfeldtJakob disease. Arch Neurol 59:128-134, 2002 Poser S, Mollenhauer B, Kraubeta A et al: How to improve the clinical diagnosis of Creutzfeldt-Jakobdisease. Brain 122:2345-2351, 1999 Prusiner SB, Hsiao K K Human prion diseases. Ann Neurol 35:385-395, 1994
Webb RM, Leech RW, Brumback RA: Spongiform encephalopathies: the physician’s responsibility. South Med J 83:141-145, 1990 Weihl CC, Roos Rp: Creutzfeldt-Jakobdisease, new variant CreutzfeldtJakob disease, and bovine spongiform encephalopathy. Neurol Clin 17~835-859, 1999
Chapter 80
80
Rickettsial Infections of the Nervous System
515
Rickettsial Infections of the Nervous System J. Douglas Lee
Rickettsiae are obligate intracellular, small, gram-negative pleomorphic bacilli that normally cause infection in rodents and other mammals; humans are incidental hosts. The rickettsiae can be grouped as typhus, spotted fevers (Rocky Mountain spotted fever [RMSF]), Q fever, and Ehrlichia. Until recently, Bartonella (formerly Rochalimaea) was also included in this group. Typhus and RMSF, which cause central nervous system (CNS) involvement in almost all infected humans, and Q fever, which does so on occasion, are discussed here. Although these diseases are uncommon, they remain a diagnostic consideration in both rural and urban settings. Each year, 1000 cases of RMSF and somewhat fewer cases of typhus and Q fever are reported in the United States. These diseases undoubtedly are underreported because of a lack of consideration of the diagnosis. PATHOPHYSIOLOGY The organisms of typhus and the spotted fevers selectively infect vascular endothelial cells, producing microvasculitis with inflammation, vascular permeability, local hemorrhage, thrombosis, luminal obstruction, and microinfarction. This is more intense in RMSF than in typhus infections. Because systemic vessels are involved diffusely, a characteristic rash appears in most patients. The rash and the various CNS syndromes dominate the clinical picture; the word typhus is derived from the Greek word for “hazy” or “smoky,” referring to the delirium characteristic of the disease. In the CNS, perivascular glial nodules are almost always present and are considered pathognomonic of rickettsial infection. These are accumulations of enlarged endothelial cells, lymphocytes, and macrophages that contain the organisms, which appear 1 to 2 weeks after the illness. In contrast, the organism of Q fever, Coxiella burnetii, has no such predilection for endothelium, and vasculitis is not seen, so the frequency of CNS involvement (meningitis) is less and the clinical picture usually is characterized by fever with atypical pneumonia and abnormal liver enzyme levels but no rash. ~
CLINICAL PRESENTATION The presentation is related to the type of pathology involved. Patients with RMSF or typhus have an abrupt onset of fever, chills, headache, myalgia, and arthralgia. Restlessness, irritability, confusion, and lethargy are usual, often with photophobia and stiff neck. This picture of an acute severe meningitis may develop within hours and may precede the rash. Other neurologic signs are generally nonfocal but may include increased reflexes and Babinski signs, spasticity, and movement disorders, especially athetosis. Cranial nerve involvement can include facial weakness, gaze palsies, nystagmus, and dysphagia. Eye findings are common, including papilledema, retinal fasciculitis, and uveitis. In a small percentage of patients, transverse myelitis may develop, including paraplegia or quadriplegia and a neurogenic bladder. Seizures are common. Within 1 week, most patients have a petechial rash,
which on occasion becomes confluent. When the rash is accompanied by disseminated intravascular coagulation, it rarely may cause skin or extremity gangrene. Before antibiotic therapy, cases of full-blown encephalitis and delirium had an 80% mortality rate. Patients with Q fever most often have a febrile pneumonia but with few pulmonary symptoms. Headache and constitutional and gastrointestinal symptoms are common, but rash is not a feature. A small number of patients develop meningitis, with headache, nuchal rigidity, and confusion. Some also develop a chronic disease, such as hepatitis, endocarditis, or osteomyelitis. In endemic areas, seroprevalence in the population is high, and undiagnosed Q fever is common. LABORATORY ABNORMALKIES The leukocyte count usually is normal or low, with a left shift. Thrombocytopenia is common, as is mild prolongation of the prothrombin time. Disseminated intravascular coagulation is not commonly documented. In typhus and spotted fevers, as in multisystem vasculitides, abnormalities of the liver and muscle enzymes are common, with the degree of abnormality related to the level of overall illness. Hypoalbuminemia, hypocalcemia, and hyponatremia are also frequent. The cerebrospinal fluid in RMSF often shows a modest mononuclear pleocytosis with normal glucose and elevated protein levels; in typhus and Q fever, the cerebrospinal fluid usually is normal. Imaging results usually are normal. The electroencephalogram in most cases shows diffuse slowing. In Q fever, liver enzyme abnormalities are prominent, as are chest radiographic findings; muscle enzyme and fluid electrolyte abnormalities are less common. DIAGNOSIS The diagnosis of rickettsial infections is clinical, with confirmation by serology during convalescence. Proteus agglutinins (Well-Felix reaction) are commonly present but are nonspecific, insensitive, and delayed (up to 14 days after the onset of symptoms) and so should not be relied upon. Specific rickettsial antibodies may be detected after they develop later in the illness, and it is useful to freeze serum during the acute phase of the illness to allow testing of paired sera later. Some laboratories offer direct immunofluorescent staining to demonstrate the organism in tissue such as skin biopsies. The most important disease to differentiate in the febrile patient with rash is meningococcemia. Counterimmunoelectrophoresis and latex agglutination, in addition to routine cultures, may help make this differentiation. TREATMENT A tetracycline is the treatment for rickettsial infections in adults. Doxycycline 100 mg twice a day or tetracycline 500 mg four times a day is adequate. In children younger than 8 years old and those
516
Immune and Infectious Disease
w
Other Infections and Mimicken
TABLE80-1. Rickettsial Diseases of Humans: Differential Features sevew (treated mortality)
Disease
Organism
Ceonrarhv
Vector or Route
Reservoir
Rash’
RMSP
R. rickettsii
Western hemisphere
Dog tick
lick
Extremities to trunkd
Severe (4%-8Vo)
Epidemic typhus
R. prowazekii
Wood tick Louse feces
Severe (4%)‘
R. typhi
Flea
Human Flying squirrel Rodents
Trunk
Murine typhus
C. burnetii
Inhalation‘
Numerous mammals
Trunk to extremities None
Moderate (1%-4%)
Q fever
Eastern/SE U.S. Worldwide Eastern U.S.’ Worldwide Southern U.S. Worldwide
Moderate (uncommon)
“ash may be absent in any of these but is usually present. bMortality rate depends on preexisting disease and severity. It is likely that subclinical disease is common, and significant neurologic disease is a poor prognostic indicator. ‘Similar spotted fevers exist with different rickettsiae, vectors, and vertebrate hosts on various continents. dNinety percent of patients. eRare disease in United States. Hardy organisms inhaled from residua of infected placental tissue of wild or farm animals or domestic pets. ‘Brill-Zinsser disease or recrudescent typhus is seen in patients from endemic areas years after immigration. Disease is mild.
allergic to tetracycline, chloramphenicol 50 mg/kg/day in four equally divided doses is effective (maximum dosage 4 g/day). Drugs should be administered for 3 days after the patient becomes afebrile, usually about 7 to 10 days total. The fatality rate in typhus and RMSF remains close to 5%, with patients in the oldest age groups faring the worst.
SPECIFIC INFECTIONS The clinical diagnosis of specific rickettsia1 infections is based on the geographic area of exposure, potential vector exposure, and the distribution and spread of the rash (Table 80-1). Diseases with tick
81
vectors cluster in seasons and around activities allowing tick attachment. Diagnosis confirmation is by serology in most cases.
SUGGESTED READINGS Kirk JL, Fine DP, Sexton DJ, Muchmore H G Rocky Mountain spotted fever: a clinical review. Medicine 69:3545, 1990 Marrie TJ: Rikettsial infections of the central nervous system. Semin Neurol 12:213, 1992 Saah AJ, Marne TJ, Dumler JS, Walker DH: Rickettsial diseases, pp. 1719-1741. In Mandell G (ed): Principles and Practice of Infectious Diseases. 4th Ed. Churchill Livingstone, New York, 1992
Mycoplasma Infections Steven J. Spindel
The normal human oropharynx and genital tract are colonized by a class of bacteria that lack a cell wall, called Mollicutes, which includes the mycoplasmas and ureaplasmas. These are the smallest known free-living organisms. A few of these agents can cause diseases in humans and have central nervous system (CNS) manifestations, including Mycoplasma pneumoniae, Mycoplasma hominis, and Ureaplasma urealyticum. M. pneumoniae is a bacterial organism that is responsible for pharyngitis, bronchitis, and pneumonia in children and young adults. Nervous system disease has been well recognized in association with this organism, and neurologic manifestations are the most common extrapulmonary symptoms in patients with M. pneumoniae, especially in children.
outbreaks of respiratory infection have been observed to occur in 4- to 7-year cycles in crowded conditions such as schools, colleges, and military institutions. CNS manifestations occur in 7% to 10% of patients hospitalized with infection caused by M. pneumoniae. Neurologic involvement is reported mainly in the pediatric populations, probably because of the greater frequency of the organism in children and young adults. Similarly, the trend for nervous system disease is to manifest in younger patients, although it is an unusual pathogen of encephalitis in infants younger than 1 year old. Much like pulmonary disease, M. pneumoniae infections of the CNS show no gender preference and occur more often in the late summer and fall.
CLINICAL FEATURES EPIDEMIOLOGY M. pneumoniae-associated CNS disease was originally observed during epidemic outbreaks of “primary atypical pneumonia” in the 1940s, when the organism’s identity was not yet known. Transmission occurs via contaminated respiratory droplets, and the incubation period ranges from 16 to 32 days. Epidemic
Usually, M. pneumoniae causes an acute tracheobronchial pneumonia with fever, sore throat, and a severe cough, which may be difficult to distinguish, by clinical or radiographic criteria, from many other causes of pneumonia. The pulmonary disease generally runs its course in 2 to 4 weeks. M. pneumoniae can cause a primary infection of the CNS and
516
Immune and Infectious Disease
w
Other Infections and Mimicken
TABLE80-1. Rickettsial Diseases of Humans: Differential Features sevew (treated mortality)
Disease
Organism
Ceonrarhv
Vector or Route
Reservoir
Rash’
RMSP
R. rickettsii
Western hemisphere
Dog tick
lick
Extremities to trunkd
Severe (4%-8Vo)
Epidemic typhus
R. prowazekii
Wood tick Louse feces
Severe (4%)‘
R. typhi
Flea
Human Flying squirrel Rodents
Trunk
Murine typhus
C. burnetii
Inhalation‘
Numerous mammals
Trunk to extremities None
Moderate (1%-4%)
Q fever
Eastern/SE U.S. Worldwide Eastern U.S.’ Worldwide Southern U.S. Worldwide
Moderate (uncommon)
“ash may be absent in any of these but is usually present. bMortality rate depends on preexisting disease and severity. It is likely that subclinical disease is common, and significant neurologic disease is a poor prognostic indicator. ‘Similar spotted fevers exist with different rickettsiae, vectors, and vertebrate hosts on various continents. dNinety percent of patients. eRare disease in United States. Hardy organisms inhaled from residua of infected placental tissue of wild or farm animals or domestic pets. ‘Brill-Zinsser disease or recrudescent typhus is seen in patients from endemic areas years after immigration. Disease is mild.
allergic to tetracycline, chloramphenicol 50 mg/kg/day in four equally divided doses is effective (maximum dosage 4 g/day). Drugs should be administered for 3 days after the patient becomes afebrile, usually about 7 to 10 days total. The fatality rate in typhus and RMSF remains close to 5%, with patients in the oldest age groups faring the worst.
SPECIFIC INFECTIONS The clinical diagnosis of specific rickettsia1 infections is based on the geographic area of exposure, potential vector exposure, and the distribution and spread of the rash (Table 80-1). Diseases with tick
81
vectors cluster in seasons and around activities allowing tick attachment. Diagnosis confirmation is by serology in most cases.
SUGGESTED READINGS Kirk JL, Fine DP, Sexton DJ, Muchmore H G Rocky Mountain spotted fever: a clinical review. Medicine 69:3545, 1990 Marrie TJ: Rikettsial infections of the central nervous system. Semin Neurol 12:213, 1992 Saah AJ, Marne TJ, Dumler JS, Walker DH: Rickettsial diseases, pp. 1719-1741. In Mandell G (ed): Principles and Practice of Infectious Diseases. 4th Ed. Churchill Livingstone, New York, 1992
Mycoplasma Infections Steven J. Spindel
The normal human oropharynx and genital tract are colonized by a class of bacteria that lack a cell wall, called Mollicutes, which includes the mycoplasmas and ureaplasmas. These are the smallest known free-living organisms. A few of these agents can cause diseases in humans and have central nervous system (CNS) manifestations, including Mycoplasma pneumoniae, Mycoplasma hominis, and Ureaplasma urealyticum. M. pneumoniae is a bacterial organism that is responsible for pharyngitis, bronchitis, and pneumonia in children and young adults. Nervous system disease has been well recognized in association with this organism, and neurologic manifestations are the most common extrapulmonary symptoms in patients with M. pneumoniae, especially in children.
outbreaks of respiratory infection have been observed to occur in 4- to 7-year cycles in crowded conditions such as schools, colleges, and military institutions. CNS manifestations occur in 7% to 10% of patients hospitalized with infection caused by M. pneumoniae. Neurologic involvement is reported mainly in the pediatric populations, probably because of the greater frequency of the organism in children and young adults. Similarly, the trend for nervous system disease is to manifest in younger patients, although it is an unusual pathogen of encephalitis in infants younger than 1 year old. Much like pulmonary disease, M. pneumoniae infections of the CNS show no gender preference and occur more often in the late summer and fall.
CLINICAL FEATURES EPIDEMIOLOGY M. pneumoniae-associated CNS disease was originally observed during epidemic outbreaks of “primary atypical pneumonia” in the 1940s, when the organism’s identity was not yet known. Transmission occurs via contaminated respiratory droplets, and the incubation period ranges from 16 to 32 days. Epidemic
Usually, M. pneumoniae causes an acute tracheobronchial pneumonia with fever, sore throat, and a severe cough, which may be difficult to distinguish, by clinical or radiographic criteria, from many other causes of pneumonia. The pulmonary disease generally runs its course in 2 to 4 weeks. M. pneumoniae can cause a primary infection of the CNS and
Chapter 81
neurologic manifestations as a complication of pulmonary infection. The organism has been isolated from the cerebrospinal fluid (CSF), providing evidence that invasion of the CNS does occur and that M. pneumoniae can directly cause neurologic disease. Some investigatorsbelieve that other mechanisms are also at work because of the inability to detect the presence of M. pneumoniae in the CSF or brain tissue in several reported cases with CNS disease. An autoimmune process has been postulated whereby antibodies are produced against brain tissue in response to the infecting organism. Other theories include the production of a neurotoxin or a vasculitis affecting the CNS. Other Mycoplasma species have been shown in experimental animal models to produce CNS injury by these mechanisms, although they have not been demonstrated with M. pneumoniae. Postmortem examination of the brain occasionally reveals edema, hemorrhage, perivascular inflammatory infiltrates, microthrombi, and demyelination. Up to 20% of patients with neurologic symptoms have no associated pulmonary disease, a situation especially likely to occur in children. In patients who have antecedent respiratory symptoms, the average time to the onset of neurologic symptoms is 10 days (range 3 to 30 days). Symptoms then develop abruptly, often peaking in less than 24 hours (Table 81-1). Neurologic complications include the following: Encephalitis Meningitis Hydrocephalus Psychosis Myelitis Polyradiculitis Encephalitis and meningoencephalitis are the most common manifestation of CNS disease in M. pneumoniae infection. Encephalitis can be diffuse or focal and often affects the cerebellum (producing ataxia) and the pons (producing cranial nerve damage). Most patients have fever and meningeal symptoms, including headache, nausea, vomiting, and neck stiffness. Other clinical manifestations such as seizures, altered mental status, lethargy, ataxia, and focal neurologic defects (such as hemiparesis) are more commonly seen with encephalitis. Spinal cord involvement usually presents as transverse myelitis. Cranial nerve palsies also occur, and the facial nerve is most frequently affected. M. pneumoniae has also been associated with approximately 5% of patients with Guillain-Barrk syndrome. A significant number of patients also suffer damage in other organ systems (e.g., heart, liver, and bone marrow). TAW 81-1. Signs and Symptoms of Mycoplasma-Associated Encephalitis Signs and Symptoms Meningeal signs/symptoms Temp >39OC Convulsions Unconsciousness Somnolence Ataxia Ocular findings Respiratory symptoms Carditis
4b of Patients 78 53 46 35 42 20 15 38 6
Adapted from KoshkiniemiM: CNS manifestations associated with Mycoplama pneumoniae infections:summary of cases at the University of Helsinki and review. Clin Infect Dis 17(suppl. 1):552, 1993, with permission.
Mycoplasma Infections
517
Mortality and morbidity rates approach 10% and 23%, respectively, in some series. The time interval between respiratory symptoms and neurologic complications does not seem to affect the prognosis. Residual neurologic deficits occur more often after cases of encephalitis or polyradiculitis than after meningitis; in most published case series, meningitis results in very few or no neurologic complications or deaths. The neurologic sequelae of encephalitis include mental retardation, seizures, choreoathetosis, decreased visual acuity, and movement disorders.
DIAGNOSIS The CSF appears normal in up to 60% of cases. When pleocytosis is present, mononuclear cells predominate (55% to 75%). CSF glucose values are almost always normal, and the protein level is normal to high. The opening pressure may be normal or slightly elevated. Electroencephalographic abnormalities are noted in three-quarters of patients but usually reveal only diffuse, nonspecific slowing of limited diagnostic value. Brain imaging studies (such as computed tomography or magnetic resonance imaging) are normal or show mild diffuse edema. The primary diagnosis of M. pneumoniae-associated CNS disease often is made on clinical grounds and serologies. Serum complement fixation titers are the best available diagnostic test. A fourfold rise from acute to convalescent (obtained 7 to 21 days later) is diagnostic for M. pneumoniae. A single high titer of 1:32 or more also suggests the diagnosis. Titers begin to rise 1 week after the onset of infection and peak at 3 to 4 weeks. This test has good specificity (which rises with an increase in the titer), but the sensitivity is only approximately 50%. Complement fixation titers of the CSF are nonspecific because of cross-reactivity with antigens normally present in the CSF. Cold agglutinins for M. pneumoniae are positive in 30% to 50% of patients with pulmonary disease. A high titer of cold agglutinins, that is, more than 1 :128, can be very suggestive for M. pneumoniae. Bedside cold agglutinins are positive at titers of more than 1 :64, and, when present, this finding supports the diagnosis. However, a negative test does not exclude the presence of M. pneumoniae, and a low titer is nonspecific because other conditions can cause a weakly positive test (viruses, other causes of atypical pneumonias, collagen vascular disease, and myeloma). The peripheral leukocyte count may be normal or mildly elevated. Cultures for M. pneumoniae are slow growing, and the organism requires a special medium containing yeast and supplemental nutrients. These cultures are not routinely performed, and the physician with a clinical suspicion of M. pneumoniae should notify the microbiology laboratory so that these specific cultures can be done. There are also species-specific RNA probes available to demonstrate M. pneumoniae in sputum, pharyngeal swabs, and throat washings. Similar probes for M. pneumoniae in the CSF or brain tissue have not been well studied clinically. Other rapid techniques for diagnosing M. pneumoniae in clinical samples include enzyme immunoassays and indirect immunofluorescence, but these are not widely available. The polymerase chain reaction has detected M. pneumoniae in the CSF, but its diagnostic utility remains uncertain. The diagnosis of Mycoplasma can also be supported by the exclusion of other pathogens that can cause a similar clinical picture and CSF findings. The differential diagnosis includes viruses such as measles, mumps, varicella zoster, herpes simplex, adenovirus, other respiratory viruses, and enteroviruses.
518
Immune and Infectious Disease
Other Infections and Mimicken
TREATMENT
It is unclear whether the use of conventional antibiotic therapy for M. pneumoniae provides any benefit for CNS disease. Neurologic complications have been reported in patients receiving adequate antimicrobial therapy. Erythromycin and tetracycline for 2 to 3 weeks are the drugs of choice for M. pneumoniae infections. There are not enough data to support a longer duration of therapy for extrapulmonary symptoms. Other effective antibiotics include the new macrolides and the fluoroquinolones. Although these new agents do not penetrate into the CSF very well, the correlation between achieving adequate antimicrobial CSF levels and clinical outcome is uncertain. Note that tetracyclines and fluoroquinolones cannot be used in children, adolescents, or pregnant women. Additional therapies directed at CNS disease have included corticosteroids, anti-inflammatory medications, antidiuretics, and plasma exchange. There have been no prospective randomized trials of these modalities. OTHER MYCOPLASMAS AND UREAPLASMAS
M. hominis and U. urealyticum have been identified as causes of meningitis in neonates. In one series, M. hominis and LJ. urealyticum caused 2.8% and 1.5% of neonatal meningitis, respectively. These infections may occur more commonly in newborn infants born to women in lower socioeconomic groups and those with little or no prenatal care. The neonatal meningitis
caused by these organisms is as likely to occur in term infants as in premature infants. Infants become exposed to these organisms in the birth canal during delivery, and up to 30% subsequently become colonized. There are rare case reports of adults with ventriculoperitoneal shunt and ventriculostomy infections caused by M. hominis. There are no reports of U.urealyticum causing CNS disease in adults.
SUGGESTED READINGS Cassell GH, Cole BC: Mycoplasmas as agents of human disease. N Engl J Med 304:80, 1981 Clyde WA Jr: Clinical overview of typical Mycoplasma pneumoniae infections. Clin Infect Dis 17(Suppl. 1):S32, 1993 Couch RB: Mycoplasma pneumoniae (primary atypical pneumonia). p. 1446. In Mandell GL, Douglas RG, Jr., Bennett JE (eds): Principles and Practices of Infectious Diseases. 3rd Ed. Churchill Livingstone, New York, 1990 Koshkiniemi M: CNS manifestations associated with Mycoplasma pneumoniae infections: summary of cases at the University of Helsinki and review. Clin Infect Dis 17(Suppl. 1):S52, 1993 Maida E, Kristoferitsch W CSF findings in Mycoplasma pneumoniae infections with neurological complications. Acta Neurol Scand 65:524, 1982 Ponka A CNS manifestations associated with serologically verified Mycoplasma pneumoniae infection. Scand J Infect Dis 12175, 1980
SECTION 1
DISEASES OF THE SPINAL CORD
82
Clinical Approach to Disease of the Spinal Cord Mark H. Libenson
The spinal cord is structurally the simplest portion of the central nervous system, yet disorders of the spinal cord have the potential to challenge the clinician with a wide variety of clinical presentations representing a wide range of mechanisms of disease. Pathologic processes encountered in spinal cord disease include some with a slow onset of symptoms, such as metabolic or neurodegenerative diseases of the spinal cord, and some that present as catastrophic neurologic emergencies necessitating rapid diagnosis and treatment, such as spinal cord compression or trauma. The well-understood arrangement of tracts and cell columns in the spinal cord often allows precise neuroanatomic localization of signs and symptoms, yet this same orderly anatomic organization is notorious for producing falsely localizing signs that can lead the unwitting clinician astray.
GROSS ANATOMY OF THE SPINAL CORD The spinal cord (medulla spinalis) is the caudal continuation of the lower brainstem (medulla oblongata), beginning at the foramen magnum and tapering over its 45-cm adult length to end in the filum terminale, a narrow connective tissue band that anchors the spinal cord to the coccyx. Over most of its course, the diameter of the spinal cord is 1 cm or less, except for expansions in the cervical and lumbar spinal cord that reflect the increased number of entering and exiting neurons relating to the limbs. In cross-section, the spinal cord generally is somewhat oval in shape, wider in its transverse diameter, especially in its uppermost portions and at the cervical and lumbar enlargements. Below the level of T12 the substance of the cord tapers rapidly, forming the conically shaped conus medullaris (Fig. 82-1). Viewed by the naked eye, this critical communication link between the body and the brain is strikingly frail. The unprotected spinal cord is a fragile structure and undoubtedly would be a more frequent site of injury were it not surrounded by an elaborate system of osseous, ligamentous, and fluid defenses that allow the great flexibility of the spinal column while protecting the spinal cord itself from outside injury. The spinal cord is encircled by a series of bony vertebral rings, stabilized by a complex ligamentous system, sheathed in a tough connective tissue covering (the dura), and surrounded by a fluid cushion (the cerebrospinal fluid). Unlike the situation in the cranium, where the dura is closely adherent to the cerebral hemispheres and plays an additional role as the inner periosteal lining of the cranial bones, the dural covering of the spinal cord is situated away from the spinal cord, forming a permanent subdural space (Fig. 82-2). Examined in cross-section, a central, distinctive butterflyshaped gray matter core is seen surrounded by white matter tracts. 520
The central gray contains neuronal cell bodies; the white matter consists mostly of the ascending and descending myelinated tracts of the spinal cord. A small, ependyma-lined central canal runs the length of the cord, and nearly all neurons that cross from one side of the spinal cord to the other do so in the commissure that lies anterior to this canal. Reflecting the organization seen in the central nervous system as a whole, there is a general tendency in the spinal cord for motor structures to be located anteriorly and sensory structures posteriorly. Thus, the posterior gray matter of the spinal cord receives the dorsal (sensory) roots, and the anterior gray of the spinal cord contains the anterior horn cells (motor neuron cell bodies), which give rise to the anterior (motor) roots. The dorsal and anterior roots join together outside the cord to form each segment’s spinal nerve, which pierces the dura and exits through its corresponding intervertebral foramen. The location of the white matter tracts is an important exception to the anterior-posterior organizational rule; that is, the descending motor (corticospinal) tracts are located posterolaterally, and the sensory white matter tracts are located both anteriorly and posteriorly (dorsal and ventral spinothalamic tracts and dorsal columns) (Fig. 82-3). Each spinal nerve is named for its adjacent vertebral body. This leads to two problems in nomenclature. Because there is an additional pair of spinal nerve roots as compared with the number of vertebral bodies, the first seven spinal nerves are named for the first seven cervical vertebrae, each nerve exiting through the intervertebral foramen above its correspondingly named vertebral body. However, the spinal nerve exiting below the level of C7 is called the C8 spinal nerve (the extra spinal root), although no eighth cervical vertebra exists. Because of this extra nerve root, all subsequent roots exit below the vertebral body for which they are named, beginning with T1 (Fig. 82-4). The 8 cervical roots, 12 thoracic roots, 5 lumbar roots, 5 sacral roots, and 1 coccygeal root total 31 spinal nerve root pairs. All of these contain both motor and sensory roots with the exception of C1, which lacks a sensory component (explaining the absence of a C1 dermatome). The second problem in spinal root nomenclature arises from the positions of the spinal nerves with respect to their vertebral bodies. In the third embryonic month, the spinal segments are closely aligned to their corresponding vertebral segments, but after this point in fetal development, the bony spinal column’s downward growth outpaces that of the spinal cord. This differential growth gives rise to the appearance that the lower portion of the spinal cord has ascended in the spinal canal relative to the vertebral column. Indeed, because the adult spinal cord ends as the conus medullaris at approximately the L1 level, the lumbar and sacral roots must plunge downward below the termination of the
Chapter 82
Dorsal root of.
& cs 7
Ventral root of spinal nerve C1
Posterior intermedate sulcus
Dorsal root T I
Clinical Approach to Disease of the Spinal Cord
52 1
the medulla, both of which descend and join together at the level of the foramen magnum to form the anterior spinal artery, which accepts branches from segmental vessels of varying sizes as it descends the anterior surface of the spinal cord. The largest such segmental (or radicular) artery is the anterior radicular artery of Adamkiewicz, which serves the lumbar enlargement of the spinal cord. The anterior spinal artery irrigates the anterior two thirds of the cord. One or two smaller posterior spinal arteries also arise from the vertebral arteries and course down the dorsal aspect of the spinal cord, serving a wedge-shaped area constituting the posterior third of the cord.
FUNCTIONAL NEUROANATOMY OF THE SPINAL CORD A large number of ascending and descending tracts have been identified and mapped in the spinal cord; the three most important of these in terms of neuroanatomic localization of spinal cord lesions are the corticospinal tracts, spinothalamic tracts, and the dorsal columns. Motor Systems
w Dorsal root T6
k
Dorsal root L1
L!
'
Filum terminate 1- Coccygeal nerve
FIG. 82-1. Posterior view of the spinal cord showing attached dorsal root filaments and spinal ganglia. (From Carpenter MB: Core Text of Neuroanatomy. 3rd Ed. Williams & Wilkins, Baltimore, 1985, with permission.)
spinal cord to find their respective intervertebral foramina, forming the distinctive cauda equina (horse tail). As a consequence, a pathologic process at the level of the L4 vertebral body would be potentially in close proximity to both the L4 nerve root and the lower spinal roots that have arisen from the conus medullaris at the approximate level of L1 but exit the spinal canal caudal to the L4 vertebral body. The vascular supply to the spinal cord consists of a single, larger anterior spinal artery and two smaller posterior spinal arteries. The anterior spinal artery is formed from the union of a contributing branch from each vertebral artery at the level of
The corticospinal tract arises from neurons whose cell bodies are located in the motor areas of cerebral cortex, including the giant cortical motor neurons called Betz cells. The axons of these upper motor neurons reach the anterior horn cells of the spinal cord by descending through the internal capsule, the peduncles of the midbrain, and the belly of the pons. They continue caudally, forming a distinctive paired structure on the anterior surface of the medulla, the pyramids, from which the term pyramidal tract is derived. Without synapsing, nearly all of these pyramidal tract s o n s cross at the level of the medulla and the uppermost cervical spinal cord to form the decussation of the corticospinal tracts. Having crossed, the axons abandon their anterior location and move posteriorly to the posterolateral funiculi of the spinal cord. Most of these neurons are destined to synapse on the anterior horn cells located in the anterior gray of the spinal cord, the cell bodies of the lower motor neurons. These descending corticospinal tract fibers are laminated in the spinal cord in a clinically important arrangement, with fibers destined for the lower limbs traveling more superficially in the cord and fibers destined for upper limbs traveling more deeply in the cord (Fig. 82-3). A clinically less important anterior corticospinal tract descends in the anteromedial white matter of the cord. Because they have already crossed in the medulla, damage to these corticospinal tract neurons (upper motor neurons) in the spinal cord results in ipsilateral clinical findings such as spastic weakness, increased deep tendon reflexes, and a Babinski sign (Table 82-1). When there is damage to the anterior horn cells (lower motor neurons), ipsilateral clinical findings occur at the level of the affected segments, including flaccid weakness, muscle wasting, decreased deep tendon reflexes, and fasciculations (in addition to a distinctive group of electrophysiologic findings in peripheral nerve and muscle seen during nerve conduction velocity testing and electromyography, such as decreased compound muscle action potential amplitude, polyphasic motor units, fibrillation potentials, positive sharp waves, and decreased F waves and H reflexes, described more fully in Chapter 21). Thus, unilateral spinal cord lesions causes ipsilateral motor findings on neurologic examination, of the upper motor neuron type when the corticospinal tract is involved and of the lower motor neuron
522
Spinal Cord and PeripheralNcuromuxular Disease
Diseases of the Spinal Cord
FIG. 82-2. Anterior view of the spinal cord and its coverings. The pia mater is seen closely adherent to the spinal cord compared with the overlying arachnoidal and dural layers. Dorsal and ventral spinal rootlets are seen coalescing to form the spinal nerves. The dorsal root ganglia are seen just distal to this junction. (From Carpenter MB: Core Text of Neuroanatomy. 3rd Ed. Williams & Wilkins, Baltimore, 1985, with permission.)
FIG. 82-3. Cross-section of the cervical spinal cord showing white and gray matter areas, including the lamination of the corticospinal and lateral spinothalamic tracts. AHC, anterior horn cells; AS, anterior spinothalamic tract; D, dorsal spinocerebellartract; K,faxiculus cuneatus; FG, fasciculus gracilis; LL, portion of corticospinal tract serving lower limbs; SC, substantia gelatinosa; UL, portion of corticospinal tract serving upper limbs; V, ventral spinocerebellar tract; S (sacral), L (lumbar), T (thoracic), and C (cervical) mark portions of spinothalamic tract that carry sensory information from these areas. (Adapted from Watson C: Basic Human Neuroanatomy, An Introductory Atlas. 2nd Ed. Little, Brown, Boston, 1977, with permission.)
Chapter 82
Clinical Approach to Disease of the Spinal Cord
523
type when anterior horn cells or their exiting motor roots are involved.
Sensory Systems
\ .....-
ca*'
FIG. 82-4. Spinal cord root levels in relation to the vertebral bodies. Note the close association of vertebral and nerve root levels in the cervical cord compared to the lumbar cord. (From Haymaker W, Woodhall B: Peripheral Nerve Injuries. 2nd Ed. WB Saunders, Philadelphia, 1953, with permission.)
There are two major ascending systems that transmit conscious sensory information in the spinal cord the spinothalamic tracts and the dorsal columns. The first-order neurons of both of these afferent systems begin as sensory structures situated in end organs (e.g., sensory receptors in skin and stretch receptors in muscle). The cell bodies of the first-order neurons of these sensory pathways are located in the dorsal root ganglia of the spinal nerves. These gangha are seen as distinctive prominences on the dorsal nerve roots just proximal to the point where the anterior and dorsal branches join in the intervertebral foramen to form the peripheral spinal nerve. The spinothalamic tracts transmit pain and temperature sensation, commonly tested at the bedside in the form of pinprick and cold sensation. As the axons of these neurons enter the spinal cord, most rise one or two levels (in the dorsolateral tract of Lissauer) before entering the dorsal gray of the spinal cord, where they synapse (in the substantia gelatinosa) with the second-order neuron of the spinothalamic system. This second neuron crosses immediately in the anterior commissure of the spinal cord and ascends in the anterolateral funiculus as the lateral spinothalamic tract. (A small number of spinothalamic fibers may remain uncrossed and ascend in the less clinically important anterior spinothalamic tract.) As a result, when the anterolaterally located spinothalamic tract is damaged in the spinal cord, the patient experiences sensory symptoms in the contralateral half of the body. This is contrary to the case of injuries to the motor system described earlier, where the symptoms are ipsilateral. Again, there is a clinically important lamination of this tract where, as in the corticospinal tract, sensory neurons arising from the lower body travel more superficially in the tract and neurons arising from higher levels travel more deeply in the tract. The dorsal columns transmit vibratory and proprioceptive information, commonly tested at the bedside by placing a vibrating tuning fork on bone and by testing the patient's ability to detect changes in joint position on passive motion. These neurons enter the spinal cord via the dorsal root alongside pain and temperature neurons, but instead of making an immediate synapse in the dorsal horn, as do the latter type of neurons, these axons enter the ipsilateral dorsal column immediately and do not synapse until they reach the gracile or cuneate nuclei of the medulla. Because this long, single neuron does not cross the midline until it passes through the foramen magnum, a lesion
rn TAM 82-1. Effects of Damage to the Major Functional Anatomic Units of the Spinal Cord CorticospinalTrack (Upper Motor Neuron)
Anterior Horn Calls (Lower Motor Neuron)
Spinohbmic Tracts
Dorsal Columns
Modalii
Motor
Motor
Pain and temperature
Symptoms
Spastic paralysis, hyperreflexia
flaccid paralysis, decreased reflexes
Loss of pain and tempera-
Ipsilateral, below level of lesion
Ipsilateral, radicular dishibution accordingto levels involved
Contralateral, below level of lesion
Joint position sense and vibration Loss of proprioception, vibration sense, paresthesias, Romberg sign Ipsilateral, below level of lesion
Distribution of symptoms in relation to sDinal cord lesion
ture, sensation, numb ness, anesthesia
524
Spinal Cord and Peripheral Neuromuscular Disease W
Diseases of the Spinal Cord
involving one side of the dorsal columns of the spinal cord causes ipsilateral loss of vibration and joint position sense. Because the sensory modality of light touch is transmitted through both the spinothalamictracts and the dorsal columns, light touch sensation is not completely lost unless both the spinothalamic and dorsal column systems are affected. SPINAL CORD LOCALIZATION Determining the location of a lesion in the spinal cord begins by asking the question, “Is the lesion in the spinal cord?” In general, neurologic localization begins with the attempt to explain all of the patient’s findings by a single lesion before invoking multiple lesions to explain a particular pattern of findings. Although the concept may seem self-evident, it is worth repeating that isolated spinal cord lesions do not disturb cortical or brainstem functions. Therefore, findings such as aphasias, disturbances of vision or eye movement, swallowing, or consciousness are not consistent with a simple spinal cord localization; the presence of such findings leads to the search for the lesion above the level of the foramen magnum. Apparent exceptions to this rule include the presence of Horner’s syndrome (the first-order neuron of the sympathetic innervation of the pupil, eye, and upper face descends from the hypothalamus and brainstem ipsilaterally in the spinal cord as low
as Tl). A second such apparent exception is pain and temperature abnormalities in the face (some trigeminal neurons subserving pain and temperature enter the pons and descend into the upper cervical cord as low as the C2 to C4 levels before synapsing in the nucleus of the spinal tract of V and ascending to the contralateral thalamus). Table 82-2 lists selected spinal cord syndromes by anatomic site. Spinal cord localization is especially suggested when a patient presents with one of the hallmark spinal cord syndromes. Although patients in clinical practice rarely present with textbook descriptions of these distinctive syndromes, recognition of partial expressions or fragments of these classic syndromes often is the first step in correct diagnosis. Complete Spinal Cord Transdon Syndrome
Complete spinal cord transection may be caused by trauma; compression from tumor, hematoma, or abscess; or transverse myelitis (viral, postviral, or demyelinative), among other causes. Transection of the spinal cord results in interruption of the long motor and sensory tracts with concomitant complete loss of voluntary motor and conscious sensory function below the level of the transection (Fig. 82-5). Damage to sensory and motor roots at the level of the transection results in complete abolition of reflexes
TAUE82-2. Selected Spinal Cord Syndromes by Anatomic Location Extradural
Osteoarthritis Disc herniation Epidural abscess Bony and meningeal metastases Epidural hematoma Cervical spondylosis Rheumatoid arthritis Ankylosing spondylitis Other degenerative spine diseases Paget‘s disease Craniocervicaljunction abnormalities Mucopolysaccharidosis Klippel-Feil Achondroplasia Platybasia, or basilar invagination PoWs disease Atlantoaxial dislocation Foramen magnum tumor lntradural
Neurofibroma (schwannoma) Meningioma Leptomeningeal carcinoma Sarcomas Vascular tumors
Viral myelitis Autoimmune (postinfectious) myelitis Vascular (ischemic or infarct) Arteriovenous malformation lntramedullaryabscess Paraneoplastic myelitis Tumors (ependymoma, astrocytoma, oligodendroglioma, lipoma, epidermoid, dermoid, teratoma, hemangioma, hemangioblastoma, metastatic carcinoma) Electrical injuries Spinal arachnoiditis Balb’s concentric sclerosis Select Tracts or Cell Columns
Amyotrophic lateral sclerosis Primary lateral sclerosis HIV-associatedvacuolar myelopathy Adrenomyeloneuropathy or adrenoleukodystrophy Spinocerebellar degenerations Vitamin B, deficiency (subacute combined degeneration) Familial spastic paraparesis Werdnig-Hoffmann disease Kugelberg-Welander disease Tabes dorsalis Poliomyelitisinfection HTLV-1-associated tropical spastic paraparesis Lathyrism
Central Cord Syndrome
Syringomyelia Hematomyelia (trauma) lntramedullary tumors Demyelinating disease Infarcts
Malfonnative
Spinal dysraphism Spinal bifida Meningocele Myelocele Myelomeningocele Diastematomyelia Diplomyelia Caudal regression syndrome Hydromyelia Arnold-Chiari malformation type II Tethered cord
Diffuse, Focal, or Multifocal Spinal cord trauma Hematomyelia Multiple sclerosis Radiation myelitis Transverse myelitis Devic disease (neuromyelitis optica) Abbreviations: HIV, human immunodeficiency virus; HTLV-I, human T-cell leukemia virus type 1.
Chapter 82
FIG. 82-5. Complete transection of the spinal cord. The area shaded dark gray in the diagram denotes the area of lost motor and sensory function below a complete lesion of the midthoracic spinal cord.
at the level of the lesion. Minutes after a complete cord transection, there follows a period of spinal cord hypoexcitability called spinal shock, which may last days to weeks. During this period, there is complete absence of reflex and autonomic activity below the level of the injury, with flaccid paralysis. In some cases, spinal cord reflexes above the level of the transection also may be depressed. When the period of spinal shock passes, hyperreflexia with spastic paralysis below the level of the injury supervenes. Transection of the spinal cord at high cervical levels results in tetraplegia. Transection at the level of C2 results in sensory loss over the whole body and the occipital area (indeed, all dermatomal regions except the trigeminal nerve’s sensory distribution). Lesions at the level of C4 and below may leave enough preserved phrenic nerve function (C3, C4, and C5) to allow adequate diaphragmatic function after the period of acute injury. Lesions from C6 to T1 involve diminishing subgroups of the muscles innervated by the brachial plexus and allow increasing function of the arms and hands. Horner’s syndrome (ptosis, miosis, anhidrosis, and absence of facial flushing) may be seen in cervical cord transection above the level of T1 because of disruption of descending sympathetic fibers. Full diaphragmatic innervation compensates for loss of innervation of the intercostal muscles and other auxiliary respiratory muscles. Spinal cord transection below the level of T1 allows complete use of the upper extremities, including the hands. With lesions above T6, the abdominal reflexes are lost. With lesions at T10, the upper abdominal reflexes are preserved; with those at T12, all abdominal reflexes are present. With transection levels from L1 to S2, there is decreasing involvement of the lower extremities. With spinal cord levels below S2, innervation of the lower extremity muscles is preserved, but bowel and bladder function is affected, as described later in this chapter. During the initial stage of spinal shock after cord transection at any level, reflex emptying of the bladder may be lost, resulting in
W
Clinical Approach to Disease of the Spinal Cord
525
FIG. 82-6. Complete hemisection of the right side of the spinal cord: Brown-Sbquard syndrome. Dark gray area: area of loss of motor function (paralysis) and dorsal column function (ioint position and vibration sense). Light gray area: area of loss of spinothalamic tract function (pain and temperature sensation). Black area: area of loss of root function with lower motor neuron signs.
FIG. 82-7. Central spinal cord syndrome. Dark gray area: area of sensory loss in the classic cape-like distribution as might be seen in a low cenrical-high thoracic lesion of the spinal cord. Light gray area: additional area of sensory loss that may be seen with a laterally enlarging lesion at the same level. Depending on the shape of the lesion and areas of the spinal cord involved, other motor and sensory functions may be affected as well (not shown).
516
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of the Spinal Cord
urinary retention and bladder distention. In lesions that occur above the sacral level leaving the spinal bladder center in the conus medullaris and the roots of the pudendal nerve (S2, S3, and S4) intact, automatic, reflex emptying of the bladder returns days to weeks after the injury. There may be urinary urgency and spasticity of the bladder sphincter. In sacral lesions that interrupt the bladder center, the bladder becomes autonomous with feeble, inefficient, and uncoordinated contractions of the detrusor muscle. Combinations of these spastic and atonic bladder syndromes may occur in partial cord lesions at the sacral level. Similarly, bowel function ceases immediately after complete cord transection at any level, with loss of rectal tone and the anal “wink” reflex. Spontaneous bowel peristalsis returns within a few days as a rule, as do the anal and bulbocavernosus reflexes when the cord lesion lies above the sacral level. Constipation and sexual dysfunction are common. Later, in the hyperreflexic stage, anal tone may actually increase significantly. In lesions of the lumbosacral cord, however, the anus remains patulous.
A
Syndrome of Spinal Cord Hemisection: The BrownShuard Syndrome Hemisection of the spinal cord results in the distinctive syndrome of ipsilateral paralysis and contralateral pain and temperature loss below the level of the lesion, known as the Brown-Sequard syndrome. Although often not as prominent clinically, ipsilateral vibration and proprioceptive loss also occurs (on the same side as the motor symptoms). In the complete syndrome, the ipsilateral anterior horn cells and dorsal roots are also affected at the level of the transection (Fig. 82-6). Thus, a complete hemisection of the right side of the spinal cord results in paralysis with increased reflexes (after the acute phase) and loss of joint position and vibration sense on the right side below the level of the lesion and loss of pain and temperature sense on the left side. If the lesion happens to occur at the level of the lumbar or cervical plexuses, lower motor neuron involvement at that level may be more easily observed with loss of segmental reflexes and, later, wasting and other signs of denervation in the muscles of the affected root
B
FIG. 82-8. (A and 6) T1-weighted MRI scans of the cervical spine showing a herniation of the C6-C7 intervertebral disc in a 35-year-old man. (A) Midsagittal plane; the spinal cord appears gray and is surrounded by cerebrospinal fluid, which appears black. The vertebral bodies appear as a column of rectangles anterior to the cord and show a bright signal because of increased fat content in the marrow. The C6-C7 disc can be seen protruding posteriorly (arrow). (B) The same scanning sequence, but the plane of the scan is now just to the left of the midline. A larger portion of the disc can be seen herniating posteriorly and appearing to impinge on the spinal cord.
Chapter 82
C
Clinical Approach to Disease of the Spinal Cord
517
D
FIG. 82-8. Continued (C and 0) T2-weighted scans of cervical spine of the same patient The cerebrospinal fluid now appears white in this sequence, surrounding the darker spinal cord. (C) Scan in midsagittal plane showing the same disc obliterating the subarachnoid space anterior to the spinal cord. There is no abnormal (bright) signal in the spinal cord to suggest damage to the spinal cord itself. (0) TZ-weighted with scan plane again just left of the midline. The substance of this left-sided cervical disc herniation is better seen in this scan, extending posteriorly and to the left, impinging on the area traversed by the left C6 nerve root.
level's distribution. Likewise, with a right-sided spinal cord hemisection, an isolated area of complete sensory loss to both dorsal column and spinothalamic tract modalities is seen on the right in the dermatomes at or just below the level of the hemisection. This results from interruption of all sensory neurons entering the cord on the right side at the affected level. Spinal cord hemisection may be caused by partial expressions of the causes of complete cord transections.
Syndrome of Extrinsic Splnal Cord Compression (Cord-Root Syndrome) Lesions that compress the spinal cord from a location outside the dura produce symptoms in the most superficial fibers of the long pathways first. Because of the specific lamination of the corticospinal and spinothalamic tracts, as described earlier (lowerextremity fibers most superficial and upper-extremity fibers deepest), cervical compressive lesions may cause sensory and motor symptoms to appear first in the lower extremities. Symptoms may then appear to ascend as the compression becomes
more severe and more deeply situated fibers are successively affected. This anatomic arrangement is notorious for producing falsely localizing signs. For example, a distinct level of sensory loss may be discernible at the level of the umbilicus (T10) in the case of a compressive tumor at the foramen magnum. The unwary clinician obtaining a magnetic resonance imaging scan of the thoracic cord might be falsely reassured by a normal result because the level of the spinal cord where the lesion is located is not imaged. Therefore, the level of a sensory deficit found on examination produced by extrinsic, compressive cord lesions only marks the lowest possible level of the lesion; the actual lesion may lie anywhere between the level of sensory loss and the foramen magnum. In addition to affecting the long tracts of the spinal cord, extrinsic compressive lesions often disrupt motor and sensory roots at the level of the lesion. Identification of a root level can be a very helpful sign; the upper limits of a sensory (or motor) level found on examination only mark the lowest possible location of the lesion in the spinal cord for the reasons described earlier. When, in addition, a focus of back pain is present or distinct lower
528
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of the Spinal Cord
hemisection per se, may resemble the Brown-SCquard syndrome in presentation. Except in the case of early lesions, there is often some bilaterality to signs and symptoms with lateral compressive lesions of the cord, especially when the contralateral cord becomes compressed against the opposite side of the spinal canal. In cases of lateral compression rather than hemisection, the half of the spinal cord ipsilateral to the compressive lesion usually is more symptomatic than the contralateral half.
Central (Intramedullary)Spinal Cord Syndrome The initial signs and symptoms caused by smaller intramedullary lesions of the spinal cord often are related to dysfunction of the anterior commissure of the spinal cord, which contains crossing spinothalamic tract neurons (Fig. 82-7). This can result in a cape-like distribution of anesthesia at the level of the lesion in the case of cervical lesions. Additional symptoms caused by the lesion depend on the additional cord regions the lesion involves in the transverse plane. Lesions that include the anterior gray matter of the spinal cord may destroy the anterior horn cells, causing weakness and wasting of muscles (lower motor neuron signs) at the involved levels. Further enlargement of the area of the lesion may result in involvement of the spinothalamic tracts. Because spinothalamic tract fibers serving the sacral areas travel most superficially in the spinal cord (as described earlier), expanding intramedullary lesions cause increasing areas of anesthesia, but with a tendency to sacral sparing, as these fibers are most distant from the center of the cord (Fig. 82-3). Thus, an expanding cervical central cord lesion may begin by causing an area of cape-like anesthesia involving the arms but with progressively descending sensory involvement to the point that only the saddle area is spared. Larger lesions may similarly affect the descending corticospinal tracts. The most common causes of such lesions are syringomyelia, intrinsic cord tumors, and hematomyelia.
Syndromes of the Cauda Equlna and Conus Medullaris Because the cauda equina is composed of the lumbosacral roots as they descend into the thecal sac below the termination of the spinal cord, pathologic processes in this area may cause a patchy distribution of symptoms, depending on which nerve roots are involved. Pain often is a prominent symptom. Lesions of the conus medullaris may involve a similar array of nerve roots, but because this region of the cord contains important reflex centers, disorders of bowel, bladder, and sexual function are often most prominent.
Other Spinal Cord Syndromes FIG. 82-9. (A) T1-weighted MR images of the spinal cord in a
15-year-old girl with transverse myelitis. The cervical spinal cord is abnormally enlarged (arrows). She presented with limb weakness, sensory changes in the legs, and blurred vision in the right eye associated with optic papillitis. The combination oftransverse myelitis and optic myelitis found in this girl is also called neuromyelitis optica or Devic disease. (s) T2-weighted images of the spinal cord in the same patient. There is a blush of abnormally increased T2 signal in the affected area (arrows). motor neuron signs are found at a specific level, the level of the lesion may be pinpointed. Likewise, localized pain or tenderness over a vertebral spinous process may help localize a process associated with a destructive bony lesion. Lateral compressive lesions, though not causing a spinal cord
Anterior horn cell syndromes occur, sometimes with associated upper motor neuron involvement. The most important disorder seen in adults associated with this pattern is amyotrophic lateral sclerosis, in which there is a progression of both lower (anterior horn cell) and upper (corticospinal tract) motor neuron signs. Spinal muscular atrophy type I (Werdnig-Hoffmann disease) is a pure anterior horn cell degeneration presenting in infancy, although more slowly progressive forms are recognized. Infection with the poliomyelitis virus, now rare, shows a predilection for the anterior horn cells and produces asymmetrical lower motor neuron involvement and a cerebrospinal fluid pleocytosis after a febrile illness. Cervical and lumbar degenerative spine disease may result in stenosis of the spinal canal at those levels. This syndrome of spinal cord stenosis may mimic amyotrophic lateral sclerosis by causing both upper motor neuron signs from spinal cord
Chapter 82
compression and lower motor neuron signs at multiple levels caused by loss in height of the intervertebral foramina at multiple levels. Occlusion of the anterior spinal artery produces a distinctive anterior spinal artery syndrome with loss of spinothalamic and corticospinal tract function. Dorsal column functions are generally preserved because this posterior, wedge-shaped area of the spinal cord is irrigated by one or two posterior spinal arteries. Therefore, the patient is paralyzed to a varying degree below the level of the stroke with complete loss of pain and temperature sensation but with preservation of vibration and joint position sense. Other
Clinical Approach to Disease of the Spinal Cord
929
patterns of infarction of the cord as a result of vascular occlusions may also occur. Certain patterns of spinal cord involvement, though not anatomically confluent, are characteristic of specific disease processes. Tabes dorsalis occurs as a late complication of syphilitic infection. There is marked degeneration of the posterior columns, which produces an ataxia based on sensory loss. Loss of the posterior roots in the lumbosacral area is responsible for abnormal bowel, bladder, and sexual function caused by loss of sensory inputs and probably also explains the lancinating pains characteristic of that disorder. Subacute combined degeneration is the term
A
FIG. 82-10. MRI scan of the spine in an 1 1-year-old girl with a low thoracic spinal cord astrocytoma. (A) T1 sagittal image of the spinal cord showing a tumor mass in the low thoracic area (arrowhead). (B) T I gadolinium-enhancedimages of the same area showing an area of intense enhancement within the tumor (arrowhead). Illustration continued on following page
550
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of the Spinal Cord
D
C
FIG. 82-10. Continued (C) Axial T2-weighted image of normal-appearing spinal cord at the level of T8 (above the lesion) in the same patient. The spinal cord is dark, surrounded by brightly colored spinal fluid. (0) Axial T2-weighted image of the spinal cord at the level of T10 showing abnormal enlargement of the cord, relative obliteration of the cerebrospinal fluid space, and abnormally increased signal in the substance of the cord.
used for the myelopathy associated with vitamin B,, deficiency (often caused by failure to absorb this vitamin from the gut caused by lack of intrinsic factor in patients with pernicious anemia). Corticospinal, spinothalamic, and dorsal column tracts of the cord are all affected, with the posterior column findings often most prominent.
DIAGNOSTIC TESTING IN SPINAL CORD DISEASE Careful history-taking and a methodical neurologic examination will often strongly suggest a specific diagnosis; electrophysiologic and radiologic testing may confirm the diagnostic impression. Spine radiographs give an idea of the caliber of the spinal canal, the heights of the intervertebral foramina, or the presence of bony spurs or other bony lesions. Plain radiographs of the spine may also show evidence of spine instability, fracture, or dislocation in cases of trauma. Flexion and extension views of the cervical spine may demonstrate the atlantoaxial subluxation that is common in patients with Down’s syndrome. Plain radiographs may also show degenerative disease of the spine suggestive of disc or spondylitic disease. The appearance of lytic vertebral lesions may lead to a diagnosis of metastatic disease. Certain spinal cord malformations may be suspected when certain findings, such as spina bifida occulta, butterfly vertebrae or hemivertebrae, or a bony spur traversing the cord (diastematomyelia) are present. Lumbar puncture allows analysis of the cerebrospinal fluid and measurement of its pressure. Spinal fluid culture and serology may help pinpoint infectious causes of spinal cord disease, such as spinal abscess. The isolated finding of very high protein levels in the spinal fluid suggests spinal block, usually from tumor. More modest increases in spinal fluid protein are observed in cases of myelopathy that are associated with polyradiculopathy. Cytologic studies of spinal fluid may help make a specific diagnosis of
malignancy. Cell counts in spinal fluid may point toward infection or other inflammatory processes. Measurement of spinal fluid immunoglobulin G (IgG), myelin basic protein, and oligoclonal bands may help establish the diagnosis of multiple sclerosis. After lumbar puncture, myelography may be performed by injecting contrast material through a spinal needle. The contrast medium outlines the subarachnoid space and allows visualization of the spinal cord, nerve roots, or intradural lesions, which appear as shadows or defects in the column of injected contrast. Extradural compressive lesions appear as an indentation on the thecal sac. Computed tomographic scan of the spinal cord after injection of contrast into the thecal space, a so-called computed tomographic myelogram, may be performed after such an injection. Use of both plain and computed tomographic myelography has, for the most part, been supplanted by magnetic resonance imaging of the spinal cord, which has revolutionized the diagnosis of spinal cord disease. Magnetic resonance imaging shows better detail, distinguishes better between normal and abnormal tissues, and has significantly improved the imaging of both extrinsic and intrinsic spinal cord disease (Figs. 82-8, 82-9, and 82-10). Somatosensory evoked potentials can be used to study spinal cord function. A sensory stimulus, usually in the form of a mild electric shock, is applied to a limb, and the resulting evoked potential is measured at multiple levels as it travels rostrally through the nervous system, including over the spinal cord and sensory cerebral cortex. Asymmetry in amplitude or latency or absence of the evoked potential may allow inferences regarding the location, and sometimes the cause, of a spinal cord lesion. In general, somatosensory evoked potential testing reflects conduction through the fastest-conducting (largest) sensory neurons in the spinal cord, the dorsal column neurons. Nerve conduction velocity and electromyographic testing often can give both direct and indirect information about spinal cord function.
Chapter 83
SUGGESTED READINGS Adam RD, Victor M: Diseases of the spinal cord. In Principles of Neurology. 7th Ed. McGraw-Hill, New York, 2001 Brazis PW, Masdeu JC, Biller J: Localization in Clinical Neurology. 3rd Ed. Little, Brown, Boston, 1996 Carpenter MB: Core Text of Neuroanatomy. 3rd Ed. Williams & Wilkins,
Baltimore, 1985 deGroot J, Chusid JG: Correlative Neuroanatomy. 21st Ed. Appleton & Lange, East Norwalk, CT, 1991
83
Syringomyelia and Related Conditions
53 1
Gray H: Gray’s Anatomy. 23rd Ed. WH Lewis (ed). Lea & Febiger, Philadelphia, 1936 Hughes J T Disorders of the spine and spinal cord. In Adams JH, Duchen LW (eds): Greenfield’s Neuropathology. 5th Ed. Oxford University Press, New York, 1992 Ludwig G Clinical symptomatologyof spinal cord lesions. pp. 178-216. In Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology. Vol. 2. Wdey, New York, 1969 Williams PL, Warwick R Functional Neuroanatomy of Man. WB Saunders, Philadelphia, 1975
Syringomyelia and Related Conditions Patrick A. Roth and Alan R. Cohen
Syringomyelia is a term used to describe a fluid-filled cavity in the spinal cord. It may be associated with several distinct conditions or may occur as an isolated entity. Syringomyelia has fascinated clinicians for years because the symptoms often are a striking recapitulation of those predicted from a centrifugal distortion of the normal cross-sectional anatomy of the spinal cord. The diverse causes of this entity have generated a great deal of interest in its pathogenesis. The advent of magnetic resonance imaging (MRI) has revolutionized our understanding of this disease by improving diagnostic capabilities, providing precise anatomic information both preoperatively and postoperatively, and improving our understanding of the pathogenesis (Fig. 83-1). The natural history of syringomyelia has never been adequately characterized. It appears to be variable, and it is thus difficult to predict the rate or extent of progression in any individual case. Most studies that have looked at the natural history of syringomyelia are retrospective and involve either many different treatments for a population of patients or several sequential treatments for an individual patient so that a predicted tempo or extent of progression cannot be reliably extracted to provide a sense of risk in any given case. These complex retrospective studies also limit our ability to evaluate critically and compare the various treatment modalities used. Because a substantial portion of patients who are symptomatic develop progressive problems, most surgeons initiate some form of treatment in cases of symptomatic syringomyelia.
syringohydromyelia or hydrosyringomyelia to group the two entities into one category and thus avoid the distinction. We use the traditional term syringomyelia to include both of these theoretic anatomic variants because the distinction often is difficult to display pathologically and there is no clinical relevance in
HISTORY The earliest report of syringomyelia is that of ktienne in 1564. He compared the cavitation of the spinal cord with the ventricles of the brain. The term syringomyelia was derived by Ollivier $Angers in 1824 from the Greek words syrinx, “to become hollow,” and my&, “marrow.” In 1863, Virchow suggested the alternative term hydromyelia because he believed that the central canal was the source of the abnormal fluid within the canal. In 1875, Simon proposed that the term syringomyelia be used to describe a fluid collection within the substance of the cord separate from the central canal and that the term hydromyelia be used to describe a dilation of the central canal. Several authors continue to distinguish syringomyelia from hydromyelia by using the two terms separately; others use the term
FIG. 83-1. Syrinx of the cervical cord with a septation.
Chapter 83
SUGGESTED READINGS Adam RD, Victor M: Diseases of the spinal cord. In Principles of Neurology. 7th Ed. McGraw-Hill, New York, 2001 Brazis PW, Masdeu JC, Biller J: Localization in Clinical Neurology. 3rd Ed. Little, Brown, Boston, 1996 Carpenter MB: Core Text of Neuroanatomy. 3rd Ed. Williams & Wilkins,
Baltimore, 1985 deGroot J, Chusid JG: Correlative Neuroanatomy. 21st Ed. Appleton & Lange, East Norwalk, CT, 1991
83
Syringomyelia and Related Conditions
53 1
Gray H: Gray’s Anatomy. 23rd Ed. WH Lewis (ed). Lea & Febiger, Philadelphia, 1936 Hughes J T Disorders of the spine and spinal cord. In Adams JH, Duchen LW (eds): Greenfield’s Neuropathology. 5th Ed. Oxford University Press, New York, 1992 Ludwig G Clinical symptomatologyof spinal cord lesions. pp. 178-216. In Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology. Vol. 2. Wdey, New York, 1969 Williams PL, Warwick R Functional Neuroanatomy of Man. WB Saunders, Philadelphia, 1975
Syringomyelia and Related Conditions Patrick A. Roth and Alan R. Cohen
Syringomyelia is a term used to describe a fluid-filled cavity in the spinal cord. It may be associated with several distinct conditions or may occur as an isolated entity. Syringomyelia has fascinated clinicians for years because the symptoms often are a striking recapitulation of those predicted from a centrifugal distortion of the normal cross-sectional anatomy of the spinal cord. The diverse causes of this entity have generated a great deal of interest in its pathogenesis. The advent of magnetic resonance imaging (MRI) has revolutionized our understanding of this disease by improving diagnostic capabilities, providing precise anatomic information both preoperatively and postoperatively, and improving our understanding of the pathogenesis (Fig. 83-1). The natural history of syringomyelia has never been adequately characterized. It appears to be variable, and it is thus difficult to predict the rate or extent of progression in any individual case. Most studies that have looked at the natural history of syringomyelia are retrospective and involve either many different treatments for a population of patients or several sequential treatments for an individual patient so that a predicted tempo or extent of progression cannot be reliably extracted to provide a sense of risk in any given case. These complex retrospective studies also limit our ability to evaluate critically and compare the various treatment modalities used. Because a substantial portion of patients who are symptomatic develop progressive problems, most surgeons initiate some form of treatment in cases of symptomatic syringomyelia.
syringohydromyelia or hydrosyringomyelia to group the two entities into one category and thus avoid the distinction. We use the traditional term syringomyelia to include both of these theoretic anatomic variants because the distinction often is difficult to display pathologically and there is no clinical relevance in
HISTORY The earliest report of syringomyelia is that of ktienne in 1564. He compared the cavitation of the spinal cord with the ventricles of the brain. The term syringomyelia was derived by Ollivier $Angers in 1824 from the Greek words syrinx, “to become hollow,” and my&, “marrow.” In 1863, Virchow suggested the alternative term hydromyelia because he believed that the central canal was the source of the abnormal fluid within the canal. In 1875, Simon proposed that the term syringomyelia be used to describe a fluid collection within the substance of the cord separate from the central canal and that the term hydromyelia be used to describe a dilation of the central canal. Several authors continue to distinguish syringomyelia from hydromyelia by using the two terms separately; others use the term
FIG. 83-1. Syrinx of the cervical cord with a septation.
532
Spinal Cord and Peripheral Neuromuscular Disease I Diseases of the Spinal Cord
A
FIG. 85-2. (A) TI-weighted axial MRI of the spinal cord showing a syrinx that is symmetric and central in location. (6) T2-weighted axial MRI of the spinal cord showing a more eccentric and asymmetric syrinx.
separating the two entities on the basis of pathogenesis, natural history, or appropriate treatment modalities (Fig. 83-2).
PATHOGENESIS The development of theories of the pathogenesis of syringomyelia is fascinating. Gardner proposed a hydrodynamic theory for the pathogenesis of a syrinx. According to his theory, the formation of
a syrinx was the result of a communication between the fourth ventricle and the central canal of the spinal cord coupled with a relative obstruction in the outlets of the fourth ventricle, resulting in a water-hammer effect with cerebrospinal fluid (CSF) being propelled into the central canal with each systolic pulsation of the brain. Williams, alternatively, suggested that a syrinx was formed as a result of craniospinal pressure dissociation. He postulated that a normal Valsalva maneuver results in flow of CSF from the
Chapter 85
intraspinal compartment into the intracranial compartment, followed by a return flow back into the intraspinal compartment after the Valsalva. With an obstruction at the foramen magnum, there would be a relative impedance to this bidirectional flow, and alternative conduits would be used, such as flow between the central canal of the spinal cord and the fourth ventricle. The theories of Gardner and Williams are based on the existence of a communication between the fourth ventricle and the central canal of the spinal canal. However, recent evidence based on both autopsy and MRI studies suggests that most syrinxes do not communicate with the fourth ventricle. This has lent some support to different theories of pathogenesis. Ball and Dayan in 1972 suggested that the syrinx was the result of flow across the spinal cord from the spinal subarachnoid space through Virchow-Robin spaces. Similarly, Aboulker in 1979 postulated that the syrinx was the result of flow across the spinal cord from the spinal subarachnoid space through the dorsal nerve root entry zone of the spinal cord. Milhorat et al. in 1993 suggested that the syrinx might result from a block of the normal cephalad-directed flow of CSF in the central canal, originating in the spinal cord parenchymal extracellular space. They pointed out that the central canal of the thoracic and lumbar segments of the spinal cord normally is obliterated in adults and that this might explain the predominance of cervical or cervicothoracic syrinxes in adults and the holocord syrinxes more commonly seen in children.
Syringomyelia and Related Conditions
533
Chiari I hindbrain malformation (Fig. 83-4) are difficulty using the hands and gait disturbances. These symptoms generally have their onset in adolescence or early adulthood. Patients typically complain of weakness or loss of agility in their hands. Occasionally, patients describe their hand symptoms as numbness. The gait abnormalities often are perceived initially as weakness, stiffness, or fatigue. These symptoms often are asymmetric early. Pain is the next most common presenting symptom. It is most often suboccipital in location. Typically, patients describe intensification of the pain with coughing or sneezing. This is also the case with the Chiari I malformation without syrinx, however. Occasionally, the pain has a radicular component in addition. Infrequently, the pain radiates into the arms or scapulae with a nonradicular, poorly localized, boring character, referred to as funicular pain. Bowel and bladder dysfunction are not prominent complaints early in the disease. In some patients, atrophy is apparent, particularly in the hands; others develop noticeable scoliotic spine deformities, causing them to seek medical attention. Some patients seek medical attention for repeated unrecognized burns of their hands. On examination, many of these patients demonstrate atrophy of the upper extremities. This typically involves the hands most prominently. Over time, contractures can occur in the hand,
EPIDEMIOLOGY Many of the modern classification schemes have divided syringomyelia into a communicating and noncommunicating form. The communication is that of the syrinx with the basal cisterns and ventricular system. The term communicating may also imply that the syrinx is an extension of a collection of CSF that is not being adequately absorbed. In other words, communicating syringomyelias may be subsumed under the category of hydrocephalus. In other nomenclatures, the term hydrornyelia is used synonymously with communicating syringomyelia. Noncommunicating syringomyelias are much more common than communicating syringomyelias and typically include all of the common conditions associated with syringomyelia such as the Chiari I and Chiari I1 hindbrain malformations (which account for about one half of all syrinxes identified by MRI), intramedullary tumors, trauma, arachnoiditis, and compression of the spinal cord or brainstem by either extradural or intradural masses (Fig. 83-3). When no cause for the syrinx is discovered, the term idiopathic syringomyelia often is applied. MRI has helped identify many concurrent conditions in cases of syringomyelia and has thus resulted in a marked reduction in the perceived prevalence of idiopathic syrinxes. Syringomyelia is so commonly associated with these other related conditions that it is impractical to consider it as an isolated entity when describing its clinical presentations.
CLINICAL PRESENTATION Syringomyella Assodated with a Hindbrain Malfonnatlon The symptoms and signs associated with a syrinx are logically remembered if one bears in mind the cross-sectional anatomy of the spinal cord. Often juxtaposed on the symptoms and signs caused by the syrinx are the symptoms and signs caused by the associated hindbrain malformation. The most common presenting symptoms of a syrinx with the
FIG. 83-3. Contrast-enhanced sagittal MRI of the cervicomedullary junction showing a hemangioblastoma with an associated cervical syrinx.
534
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of the Spinal Cord
FIG. 83-4. Sagittal T1-weighted MRI of the cervical spinal cord showing tonsillar herniation characteristic of the Chiari I malformation. There is also an associated syrinx that does not communicate with the
fourth ventricle.
causing a main en griffe (French for “griffin-claw h a n d ) appearance. This term has an interesting derivation; a griffin is a mythological monster that has the body and hind legs of a lion and the head, wings, and claws of an eagle. Scoliosis, when present, typically is centered on the cervicothoracic junction and can precede other neurologic symptoms by years. The classic neurologic sign encountered is a suspended, capelike, dissociated sensory loss involving the thorax and upper extremities. The presence of this sign on examination strongly localizes the lesion to within the parenchyma of the spinal cord. This finding is the result of disruption of the crossing spinothalamic tracts in the central portion of the cord. Sensation above and below the level of the syrinx can be normal if only the crossing fibers are affected. This forms the basis for the deficit being suspended. In addition, if the process involves only the spinothalamic tract, pain and temperature alone, and not fine touch or proprioception, are affected. This forms the basis for the deficit being dissociated. As the syrinx enlarges, it next affects the anterior horn cells, first the more central anterior horn cells that supply the axial musculature and then the more peripheral anterior horn cells that affect the appendicular musculature. This is the presumed basis of the scoliosis (axial muscle weakness) and segmental atrophy and
weakness of the distal arm, respectively. Further progression of the syrinx involves the intermediolateral cell column of the cord (when the syrinx extends into the thorax). This manifests as Horner’s syndrome. Finally, the corticospinal tract and posterior columns are affected, resulting in spasticity and difficulty with fine touch and joint position sense. Interestingly, the motor and sensory disturbances associated with a syrinx nearly always begin asymmetrically, although they end up affecting both sides. More chronic findings on examination include painless ulcerations of the fingers, edematous hands, and Charcot joints. The presentation of syringomyelia with the Chiari I1 malformation often is more subtle. These patients come to medical attention at birth. There is almost always an associated myelomeningocele, which causes a variable amount of extremity and bowel and bladder dysfunction, depending on the level of the myelodysplasia. Hydrocephalus is also a very common finding, so most of these patients need a ventricular shunt early in life. Most syrinxes found with the Chiari I1 malformation are asymptomatic. Sometimes, the syrinx extends the entire length of the spinal cord, and yet signs attributable to the syrinx are difficult to elicit. The syrinx may appear along with other signs of shunt malfunction. The syrinx has even been reported to appear before ventricular dilation in cases of shunt malfunction. Patients with the Chiari I1 malformation may present with a variety of symptoms and signs attributable to brainstem dysfunction during the neonatal period. These babies feed poorly, with choking, vomiting, and aspiration. They can become stridorous or apneic. Radiographic investigation may reveal hydrocephalus, a syrinx, a tight posterior fossa, or a combination thereof. It can be difficult to sort out which of the findings is contributing to the problem or whether the presentation is the result of an intrinsically disordered brainstem. The most common cause of a symptomatic Chiari I1 malformation is a shunt malfunction. This possibility should be entertained even if the initial imaging of the brain does not reveal enlarged ventricles because the ventricles occasionally do not change early in the course because of decreased compliance or displacement of CSF into a syrinx or into a bulging myelomeningocele repair site. In rare cases, the syrinx extends cephalad into the brainstem and is thus referred to as syringobulbia. This typically occurs in the tegmentum, eccentrically to one side or the other. Patients may experience changes in their voice and dysphagia. On examination, atrophy and ipsilateral deviation of the tongue and ipsilateral pain and temperature sensation loss of the face may be found. In addition, nystagmus or Horner’s syndrome may be present. Often, the symptoms and signs can be difficult to separate from the associated Chiari malformation and direct brainstem compression.
Syrinx Associated with Spinal Cord Tumor Intramedullary cord tumors account for 2% to 4% of all central nervous system tumors. Syrinxes have been found with all of the commonly occurring intramedullary spinal cord tumors and are thought to occur in 25% to 50% of these tumors. Syrinxes are more likely to occur in conjunction with cervical spinal cord tumors than with thoracic or lumbar spinal cord tumors. Astrocytomas, ependymomas, and hemangioblastomas account for more than 90% of these tumors. The CSF protein level often is increased in the syrinxes associated with spinal cord tumors. The syrinx can extend cephalad or caudad to the tumor or both.
Chapter 83
Because the symptoms attributable to both the intramedullary tumor and syrinx are caused by disruption of the spinal cord, the clinical relevance of the syrinx, as distinct from that of the tumor, often is hard to assess. Often, the sensory level corresponds to the location of the tumor and not the syrinx even if the syrinx extends multiple segments above or below the tumor. The most common presenting symptom in adults is pain. It is a complaint in up to 90% of all adults with intramedullary tumors. The pain is described as a poorly localized ache in the midline corresponding to level of the tumor. Often, the pain radiates into an extremity in a nonradicular pattern and is characterized as a poorly localized deep ache. Syrinxes that occur in conjunction with spinal cord tumors may also affect the motor and sensory modalities. Motor problems often begin asymmetrically and are usually most profound in the hands when the tumors are located in the cervical spine. Difficulties with gait can also develop later. Examination often reveals proximal weakness and, occasionally, atrophy. Distally, there may be diminished fast finger motion and agility. Sensory disturbances also tend to start asymmetrically and distally. These disturbances may spread proximally and then cross to the other side. The classic finding of a suspended, dissociated sensory loss is uncommon but, when present, is highly suggestive of an intramedullary process. Surgical removal of the tumor often also eliminates the associated syrinx. The presence of a syrinx confers a better prognosis for complete surgical resection of the spinal cord tumor.
Syringomyelia and Related Conditions
535
venous thrombosis involving a spinal cord vascular malformation. Occasionally, sudden deterioration is superimposed on a more chronic condition. Clinically, these malformations have a very variable presentation. The myelopathy is less likely to be a central cord-like syndrome, and paraparesis or quadriparesis is more likely to be an early finding. Tethered spinal cord syndrome can present with a slowly progressive myelopathy much like the syrinx. Often, symptomatic tethered cords present with an orthopaedic deformity. This more often involves the thoracolumbar or lumbar spine or lower extremities, as opposed to the deformities typical of the syrinx, which primarily affect the cervical or cervicothoracic spine or upper extremities. The orthopedic abnormalities associated with the tethered cord can be varus, valgus, or cavus changes of the
Post-traumatic Syringomyelia Post-traumatic syringomyelia is a syndrome characterized by progressive deficits corresponding to a portion of the spinal cord remote from a previous injury. It usually manifests several years after the spinal cord injury. The incidence of post-traumatic syringomyelia is thought to be between 0.3% and 3.2% (Fig. 83-5). The most common presenting symptom is pain. The pain can occur in the torso or an extremity and may be related to movement of the head, when cervical in location, or to straining. Later findings include paresthesias, weakness, and hyperhydrosis. These symptoms typically are related to superiorly located segments of the spinal cord. Interestingly, the symptoms can skip segments of the cord. The paresthesias and motor findings usually start, and remain, asymmetric. Occasionally, the pain is replaced with hypalgesia. DIFFERENTIAL DIAGNOSIS The differential diagnosis of syrinx includes a large spectrum of pathologic processes. One must consider the inflammatory myelopathies that affect the spinal cord. These may be infectious or idiopathic. Normally, the clinical course is more fulminant, evolving over a period of days. Likewise, the demyelinating diseases usually evolve over a time course too short to be mistaken for the more chronically evolving syrinxes. Spinal arteriovenous malformations can present with a more chronic myelopathy. These malformations are most commonly dural malformations and are the result of a fistula or fistulas supplied by a radicular artery or arteries. The pathophysiology is thought to be a myelopathy from venous hypertension as the result of the fistula. On imaging studies, large serpiginous arterialized veins are seen in the subarachnoid space. The eponym FoixAlaiouanine has been used to describe a vascular disorder characterized by a necrotizing myelitis believed to be secondary to
FIG. 83-5. Sagittal T1-weighted MRI of the cervicothoracic spinal cord showing a syrinx and an atrophic spinal cord. Previously, this patient had sustained a " gunshot wound of the cervical spinal cord.
536
Spinal Cord and Peripheral Neuromuscular Disease
rn Diseases of the Spinal Cord
foot; recurrent dislocations of the hip; or rotational abnormalities of an extremity or extremities. An isolated presentation of scoliosis is not uncommon. Patients occasionally present with progressive isolated gait abnormalities such as spastic or wide-based gaits. Sometimes patients develop a peculiar change in posture, consisting of flexion of the knees and increased lumbar lordosis. In addition to orthopedic deformities, patients with tethered cords may present with spinal cord or, less commonly, root dysfunction. Again, this typically affects the lower extremities and can involve pain, weakness, sensory changes, and bowel or bladder dysfunction. The tethered cord often is associated with a host of lesions, including myelomeningocele, myelocystocele, lipomyelomeningocele, spinal lipoma, meningocele, split cord malformation (diastematomyelia), and a thickened fdum terminale. The presence of any of these conditions along with a low-lying conus medullaris should alert the clinician to the possibility of the tethered cord syndrome. Of interest is the myelomeningocele that is often associated with a syrinx and is nearly always associated with a low-lying conus in children. When these children present with progressive myelopathy or orthopedic abnormalities, it is sometimes difficult to decide whether the predisposing condition is the syrinx, the tethered cord, or both. Finally, lesions extrinsic to the spinal cord can mimic intramedullary processes. This is epitomized by the central cord injury, which typically results from a hyperextension injury, usually at C p C 5 or C5-C6, and leaves the patient with weakness predominantly affecting the hands bilaterally and relative sparing of the legs. Sensory disturbances are variable but, when present, can occur as a suspended, dissociated sensory loss, as in syrinxes. The central cord syndrome can also occur in a much more chronic form, presumably from repeated minor trauma to the cord from an extrinsic lesion, usually arthritic spurs. On MRI, there is often a bright spot on T2-weighted images. Experimental compression of the upper cervical spine in monkeys can produce pathologic changes in the central parts of the spinal cord in the area of C8 and TI. This is thought to be the result of venous stasis and has been proposed as the cause of the central cord syndrome form extrinsic compression. Finally, extrinsic lesions that occur at the foramen magnum can present similarly to the extrinsic lesions of the midcervical spine. Patients with anterior cervicomedullary compression can present with a disproportionate amount of hand weakness. Sensory changes often are minimal unless the compression is dorsal at the cervicomedullary junction. This selective hand involvement is thought to occur because the decussation of the corticospinal tract destined for the hand occurs slightly more superior and ventral to the decussation of fibers destined for the lower extremities and can thus be selectively disturbed. This entity has been described as a cruciate palsy, referring to the compression at the crossing of fibers. DIAGNOSTIC EVALUATION In cases of suspected syringomyelia,the study of choice is an MRI scan. MRI is the most sensitive study and the most informative. In cases of known Chiari malformation (type I or 11) and suspected syrinx, a cervical MRI either confirms or rules out the diagnosis in almost all cases. If the presence of a syrinx is confirmed, it is also necessary to look at ventricular size. If a syrinx is found on MRI and there is no associated hindbrain malformation, history of trauma, or extramedullary
spinal canal mass, it is important to administer contrast medium to search for a spinal cord tumor. If localization suggests that the syrinx is more caudal than the cervical spine, the MRI should extend down to the level of the conus to look for the many causes of tethered cord or to look for a vascular malformation. For patients who cannot undergo MRI, the myelogram followed by a computed tomography (CT) scan is sensitive and informative. The initial CT scan displays the syrinx as a dilated spinal cord and may also show stigmata of the Chiari malformations or an extramedullarymass in the spinal canal. A delayed CT of 6 to 12 hours may show contrast in the syrinx itself. TREATMENT Neurosurgeons have developed many techniques to treat syringomyelia in the past several years. These include posterior fossa bony decompression for the associated Chiari malformation with or without duraplasty, subpial tonsillar resection, lysis of adhesions, myelotomy, and plugging of the obex. In addition, simple percutaneous aspiration of the syrinx, terminal ventriculostomy (sectioning of the terminal ventricle or proximal fdum terminale), syrinx-to-subarachnoid shunts, syrinx-to-peritoneum shunts, and subarachnoid-to-peritoneum shunts have been used. The treatment to a large extent depends on the radiographic features of the syrinx. If there is hydrocephalus and the syrinx appears to communicatewith the fourth ventricle or basal cisterns, the procedure of choice is a shunt. In cases of spinal cord tumors, the treatment is removal of the tumor. In the other cases of syrinx, the most effective treatment is more controversial. When a syrinx is associated with a Chiari I malformation, most neurosurgeons perform some type of posterior fossa decompression. In addition to the bone removal, there is a wide variation in technique, as mentioned earlier. No studies substantiate the superiority of any one method over another. We choose not to plug the obex because of its potential danger and because of recent evidence suggesting a lack of communication of the syrinx and the fourth ventricle in most cases. In cases in which there is a concomitant ventral compression of the brainstem (e.g., basilar invagination), it has been suggested that the anterior disease be corrected first to avoid settling of the cerebellum through the enlarged foramen magnum and subsequent exacerbation of the ventral compression. Most neurosurgeons reserve shunting of the syrinx to the subarachnoid space or other body cavities for cases of syrinx without hindbrain abnormalities or cases with progression of symptoms and radiographic persistence of syrinx despite posterior fossa decompression. Some neurosurgeons use shunting of the syrinx as a first line of treatment. Regardless of which method is used, around 20% of patients continue to deteriorate despite treatment. In addition, there is a subset of patients who do not progress, even without treatment. The inability to separate these two groups prospectively or retrospectively makes an analysis of the different treatments difficult. There is some suggestion that age greater than 40 years at presentation and a long duration of preoperative symptoms each confer a poor prognosis for successful treatment. CONCLUSION Syringomyelia is an important part of the differential diagnosis for subacute spinal cord dysfunction. It is a subject with a rich history and an evolving theory of pathogenesis. A lack of insight into the
Chapter 84
natural history of the disease has hampered our ability to evaluate different treatment modalities. The advent of MlU is likely to revolutionize our understanding of syringomyelia and clarify both its natural history and the most appropriate treatments.
SUGGESTED READINGS Abouker J: La syringomyelia et les liquides intra-rachidiens. Neurochirurgie Suppl 25:l-144, 1979
84
Spondylosis and Disc Disease
537
Ball MY, Dayan AD: Pathogenesis of syringomyelia. Lancet 2:799-801, 1972 Gadner WJ: HYdrOdYnmiC mechanism of SyringomYelia. J New01 Neurosurg Psychiatry 28:247-259, 1965 Milhorat TH, Johnson WD, Miller JI et ak Surgical treatment of syringomyelia based on magnetic resonance imaging criteria. Neurosurgery 31:231-245, 1992 Milhorat TH, Miller 71, Johnson WD et ak Anatomical basis of syringomyelia occurring with hindbrain lesions. Neurosurgery 32:74& 754, 1993
Spondylosis and Disc Disease David S. Geckle and Mary Louise Hlavin
A careful clinical history and physical examination are critical for diagnosing, localizing, and treating degenerative spinal diseases, whether spondylosis or disc herniation. The combination of clinical symptoms and signs guides decision making regarding the need for diagnostic testing and appropriate therapy. Only a small fraction of patients with degenerative disease of the spine have a surgically significant disc herniation or spondylosis. History and physical examination remain the cornerstones to identifying these cases and optimizing diagnosis and treatment for patients with nonsurgical pathology. Neurologic diagnosis begins with a comprehensive history and a review of past medical problems. Chronic diseases (diabetes mellitus, arthritis, and collagen vascular diseases), prior spinal trauma or surgery, metabolic disturbances (acromegaly, hypoparathyroidism, and renal osteodystrophy), malignancy, intravenous drug abuse, and vascular disease are just a few of the factors that can predispose a patient to spinal disease. The presence or absence of such factors can aid in differentiating a benign disc or spondylotic disease from neuropathies, plexopathies, infection, metastasis, or other causes. LUMBAR DISEASE Lumbar spinal disease consists primarily of two entities: disc herniation and spinal stenosis. Herniations occur approximately equally among men and women; stenosis is more common among women than men. Approximately 95% of lumbar disc herniations occur at the LPL5 and L5-S1 levels where most of the flexion, extension, and lateral bending occur. Manual labor or prolonged periods of riding in motor vehicles predispose people to lumbar disc disease. Spinal stenosis, or narrowing of the lumbar spinal canal and foramina sufficient to result in compression of the neural structures, is caused by congenital or degenerative hyper-
trophy of vertebral facets and the ligamentum flavum. It may be focal or throughout the entire lumbar spine.
Clinlcal Features Low back pain is the most common manifestation of the herniated lumbar disc. Typically, the pain is a dull ache of gradual onset, which is worsened by exertion and relieved by rest. With acute herniations, it can often be a severe spasmodic pain of sudden onset exacerbated by any movement. Over time, the back pain usually progresses to sciatica, a progressive boring pain that radiates to the buttocks or down the posterolateral leg but may extend to the ankle or foot with lower disc herniations. This pain may be chronic or relapsing in nature and is often associated with sensory disturbances, typically paresthesias. The distribution of pain and sensory disturbances is useful in localizing the site of the lesion. Typical findings associated with lumbar root syndromes are summarized in Table 84-1. With far lateral disc herniations, the symptoms tend to be particularly severe. Lumbar stenosis generally presents with a slowly progressive course spanning several years. The patient typically complains of leg pain, often bilateral, that may be sharp and lancinating, dull and cramping, or burning in nature. It is usually triggered by walking, but standing or sitting for prolonged periods may exacerbate the condition. Generally, the pain is rapidly and dramatically relieved by lying down or sitting. Complaints of numbness, paresthesias, and leg heaviness or weakness during ambulation are common and may outweigh the pain component, although pain typically precedes their onset. Patients often report that they must walk in short stages, with frequent rest breaks. Although the symptoms of lumbar stenosis are caused by neural compromise, they are clinically similar to those of vascular insufficiency. Therefore, the term neurogenic cluudication often is
w TMLE 861. Common Lumbar Root Syndromes Root
Pain Location
Sensory Disturbance
Weakness
Reflex Change
L3
Anterior thigh, groin Anterior thigh Posterolateral thigh and calf, extending into great toe and dorsum foot Posterolateral thigh and calf, extending into lateral toes and heel
Anterior thigh Medial calf, medial foot Dorsum foot, great toe, lateral calf
lliopsoas (quadriceps) Quadriceps fibialis anterior, extensor hallicus longus Gastrocnemius, toe flexors
Patellar Patellar None
L4 L5
51
Lateral foot, posterior calf
Achilles
Chapter 84
natural history of the disease has hampered our ability to evaluate different treatment modalities. The advent of MlU is likely to revolutionize our understanding of syringomyelia and clarify both its natural history and the most appropriate treatments.
SUGGESTED READINGS Abouker J: La syringomyelia et les liquides intra-rachidiens. Neurochirurgie Suppl 25:l-144, 1979
84
Spondylosis and Disc Disease
537
Ball MY, Dayan AD: Pathogenesis of syringomyelia. Lancet 2:799-801, 1972 Gadner WJ: HYdrOdYnmiC mechanism of SyringomYelia. J New01 Neurosurg Psychiatry 28:247-259, 1965 Milhorat TH, Johnson WD, Miller JI et ak Surgical treatment of syringomyelia based on magnetic resonance imaging criteria. Neurosurgery 31:231-245, 1992 Milhorat TH, Miller 71, Johnson WD et ak Anatomical basis of syringomyelia occurring with hindbrain lesions. Neurosurgery 32:74& 754, 1993
Spondylosis and Disc Disease David S. Geckle and Mary Louise Hlavin
A careful clinical history and physical examination are critical for diagnosing, localizing, and treating degenerative spinal diseases, whether spondylosis or disc herniation. The combination of clinical symptoms and signs guides decision making regarding the need for diagnostic testing and appropriate therapy. Only a small fraction of patients with degenerative disease of the spine have a surgically significant disc herniation or spondylosis. History and physical examination remain the cornerstones to identifying these cases and optimizing diagnosis and treatment for patients with nonsurgical pathology. Neurologic diagnosis begins with a comprehensive history and a review of past medical problems. Chronic diseases (diabetes mellitus, arthritis, and collagen vascular diseases), prior spinal trauma or surgery, metabolic disturbances (acromegaly, hypoparathyroidism, and renal osteodystrophy), malignancy, intravenous drug abuse, and vascular disease are just a few of the factors that can predispose a patient to spinal disease. The presence or absence of such factors can aid in differentiating a benign disc or spondylotic disease from neuropathies, plexopathies, infection, metastasis, or other causes. LUMBAR DISEASE Lumbar spinal disease consists primarily of two entities: disc herniation and spinal stenosis. Herniations occur approximately equally among men and women; stenosis is more common among women than men. Approximately 95% of lumbar disc herniations occur at the LPL5 and L5-S1 levels where most of the flexion, extension, and lateral bending occur. Manual labor or prolonged periods of riding in motor vehicles predispose people to lumbar disc disease. Spinal stenosis, or narrowing of the lumbar spinal canal and foramina sufficient to result in compression of the neural structures, is caused by congenital or degenerative hyper-
trophy of vertebral facets and the ligamentum flavum. It may be focal or throughout the entire lumbar spine.
Clinlcal Features Low back pain is the most common manifestation of the herniated lumbar disc. Typically, the pain is a dull ache of gradual onset, which is worsened by exertion and relieved by rest. With acute herniations, it can often be a severe spasmodic pain of sudden onset exacerbated by any movement. Over time, the back pain usually progresses to sciatica, a progressive boring pain that radiates to the buttocks or down the posterolateral leg but may extend to the ankle or foot with lower disc herniations. This pain may be chronic or relapsing in nature and is often associated with sensory disturbances, typically paresthesias. The distribution of pain and sensory disturbances is useful in localizing the site of the lesion. Typical findings associated with lumbar root syndromes are summarized in Table 84-1. With far lateral disc herniations, the symptoms tend to be particularly severe. Lumbar stenosis generally presents with a slowly progressive course spanning several years. The patient typically complains of leg pain, often bilateral, that may be sharp and lancinating, dull and cramping, or burning in nature. It is usually triggered by walking, but standing or sitting for prolonged periods may exacerbate the condition. Generally, the pain is rapidly and dramatically relieved by lying down or sitting. Complaints of numbness, paresthesias, and leg heaviness or weakness during ambulation are common and may outweigh the pain component, although pain typically precedes their onset. Patients often report that they must walk in short stages, with frequent rest breaks. Although the symptoms of lumbar stenosis are caused by neural compromise, they are clinically similar to those of vascular insufficiency. Therefore, the term neurogenic cluudication often is
w TMLE 861. Common Lumbar Root Syndromes Root
Pain Location
Sensory Disturbance
Weakness
Reflex Change
L3
Anterior thigh, groin Anterior thigh Posterolateral thigh and calf, extending into great toe and dorsum foot Posterolateral thigh and calf, extending into lateral toes and heel
Anterior thigh Medial calf, medial foot Dorsum foot, great toe, lateral calf
lliopsoas (quadriceps) Quadriceps fibialis anterior, extensor hallicus longus Gastrocnemius, toe flexors
Patellar Patellar None
L4 L5
51
Lateral foot, posterior calf
Achilles
538
Spinal Cord and Peripheral Neuromuscular Disease
used. It is imperative to evaluate for the presence of true vascular claudication in these patients. One should always examine for the presence of diminished femoral or pedal pulses or trophic changes of vascular insufficiency. Because the two conditions may occur simultaneously, one must consider the diagnosis of lumbar stenosis when pain persists after successfulvascular reconstruction. Bladder dysfunction, though rarely the sole manifestation of a herniated disc, is typically but not always associated with conus or cauda equina compression. When associated with severe acute motor weakness, a massive central disc herniation is suggested. Sacral involvement leads to a cauda equina syndrome in 10% of patients with lumbar stenosis. It is important always to document a history of urinary retention or incontinence, impotence, and saddle sensory loss. Patients with a herniated lumbar disc tend to have slow, deliberate, limited movements. Often, they hold their lower back. Inspection of the spine in patients with disc herniation usually reveals a flattening of the normal lordotic curve and paravertebral muscle spasm. Approximately 50% of patients demonstrate a scoliosis to minimize traction on the affected nerve root, as seen in Figure 84-1. The seated patient tends to slide the hips forward to avoid the normal axial loading of the lower spine. The hip and knee of the symptomatic leg often are held in slight flexion to relieve tension on the affected root. Gait often is antalgic, with minimal weight bearing on the affected leg. With far lateral disc herniations, patients often are unable to walk and hold their leg in
A
Diseases of the Spinal Cord
extreme flexion, with pain on minimal movement. Patients with lumbar stenosis tend to assume a stooped posture because forward bending often relieves the pain. Lumbar extension, which may significantly narrow the neural foramina, often leads to acute bilateral sciatica in patients with lumbar stenosis. Percussion over the involved vertebrae often causes pain. Palpation along the sciatic nerve and into the sciatic notch, though generally causing pain, can rule out the presence of a peripheral nerve sheath tumor. With long-standing spinal disease, decreased muscle tone or bulk in the lower extremities may be seen. Circumferential measurements of thigh and calf can be used to verify this. Straight leg raising maneuvers usually do not exacerbate symptoms of lumbar stenosis but are useful in diagnosing disc disease. Lasegue’s sign, or the classic straight leg raising test, is positive in up to 95% of true disc herniation cases (Fig. 84-2). The bowstring sign, a straight leg raising until pain is elicited with subsequent flexion of the knee resulting in relief of pain, may be added for confirmation. A positive crossed straight leg raising test, or pain on raising the asymptomatic leg, is seen in approximately 30% of cases. This test produces pain as the involved root is dragged over a large or medially placed herniation (Fig. 84-3). Upper lumbar disc herniations produce pain with leg extension rather than flexion, providing the basis for the extensor sign or femoral nerve traction test. Tension on the upper nerve roots caused by this maneuver generally causes pain to the knee with L3 root impingement and below the knee with L4 root impingement.
B
FIG. 84-1. Scoliosis minimizes traction on the affected lumbar nerve root. (A) In laterally placed herniations, the patient leans away from the affected side. (B) In medially located herniations, the patient leans toward the symptomatic side. (From Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1:29, 1991, with permission.)
Chapter 84
539
stool. Because symptoms associated with lumbar stenosis may vary with exertion, it is important to perform motor testing both at rest and after activity. Deep tendon reflex changes are the most objective sign of disc disease. For good results, it is essential for the patient to be as relaxed as possible. Reinforcement maneuvers, such as isometric pulling of clasped hands, may be of use. Having the patient kneel on a chair is a useful trick in eliciting an ankle jerk. It is also important to recall that the deep tendon reflexes diminish with advancing age. Although diminution of the deep tendon reflexes is classically associated with disc herniation at a single level (Table 84-l), this pattern is not entirely reliable. For instance, a diminished patellar reflex is most often seen with a ruptured L3-L4 disc, but it can also be seen with a lesion at L2-L3. A decreased ankle jerk is most common with L5-S1 herniations; however, this finding may also be caused by compression of the S1 root by a large L&L5 disc. The neurologic examination often is normal in patients with spinal stenosis, although occasionally diminution of reflexes or distal sensory loss, suggesting multiple root compression, can be seen with advanced disease.
A
B
Spondylosis and Disc Disease
U FIG. 84-2. The classic straight leg raising test consists of two parts. (A) A straight leg raising followed by (B) a second lift with knee flexed. The
first should cause radiating pain (not merely tightness in the posterior thigh); the latter should not. (From Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1 :29, 1991, with permission.)
Patrick's sign, or the figure-four maneuver, may be useful in excluding hip disease, which can also result in pain referred to the low back (Fig. 84-4). Sensory examination is the most subjective part of the physical examination. Although generalizations about the patterns of sensory loss can be made, marked variations exist because of normal anatomic variation of dermatomal pattern, involvement of more than a single nerve root, or migration of a disc fragment. A far lateral disc herniation typically causes compression of the root one level higher than usually expected (Fig. 84-5). Table 84-1 reports the sensory changes most typically associated with lumbar root compression. Rectal sensory examination is critical because many patients are unaware of this deficit. Motor weakness, though the least frequently seen sign of disc herniation, provides another important adjuvant to lesion localization (Table 84-1). However, testing may be limited because exertion causes pain. Testing muscle groups that do not stretch irritated nerve roots can help to overcome this problem (Table 84-2). Given the inherent strength of the lower extremities, weakness on routine static testing may be difficult to perceive. Subtle weakness can be unmasked using active motor testing, that is, having the patient heel-and-toe walk, squat, or climb up onto a
FIG. 84-3. The crossed straight leg raising produces pain with a large medial disc but not one located laterally. (From Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1:29, 1991, with permission.)
Spinal Cord and Peripheral Neuromuscular Disease rn
540
Diseases of the Spinal Cord
\
../ FIG. 84-4. Patrick‘s sign is elicited by externally rotating the hip with both the hip and knee flexed. This should not cause pain in the patient with disc herniation but rather suggests hip pathology. (From Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1 :29, 1991, with permission.)
Diagnosis
FIG. 84-5. Far lateral disc herniations often compress the root above the disc space rather than that usually expected. (From Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1:29, 1991, with permission.)
I-
OUQS 41
84-2.
hout Root
Roots
Muscle CrOUD
u.LJ, L4 u,L5 u,L5
Thigh adductors Thigh abduction
L5, SI
Foot inversion Foot eversion
The value of plain spine radiographs in diagnosing lumbar disc disease remains controversial. Clearly, the plain spine film is the most effective method of evaluating alignment, an important consideration in preoperative planning for spondylotic disease. A narrowed disc space can indicate disc degeneration or protrusion; osteophyte formation suggests a more chronic process. Decrease of the anteroposterior and transverse diameters of the spinal canal, which is seen with severe developmental stenosis, often can be documented. In addition, plain films are invaluable in distinguishing disc disease from other conditions, which may present with similar symptoms, such as spondylolisthesis, spinal metastasis, fracture, infection, osteoarthritis, and vertebral hemangioma. Finally, radiographs can alert the surgeon to an occult spina bifida or spondylolysis preoperatively. Myelography provides an indirect means of evaluating disc herniation while simultaneously excluding other intradural pathology, such as tumors, arachnoiditis, and vascular malformations. It is important to visualize the thoracolumbar junction (TI0 to L1) to avoid missing a conus lesion or the occasional thoracic disc presenting with sciatica. In stenotic patients with a complete myelographicblock, flexion views may convert the block to partial, allowing visualization of the distal levels. When combined with postcontrast computed tomographic (CT) imaging, myelography provides the most accurate demonstration of bony anatomy. CT imaging is useful in evaluating the spine and surrounding structures. With the addition of intrathecal contrast, it can demarcate the thecal sac, cauda equina, and exiting nerve roots. CT is particularly helpful in assessing far lateral herniations and delineating bony anatomy. It is able to detect abnormalities of canal shape, lateral recess size, and neural foramina size, which are essential in evaluating spinal stenosis. Magnetic resonance imaging (MRI) allows simultaneous noninvasive imaging of the spine, intervertebral discs, thecal sac, conus, cauda equina, exiting nerve roots, and surrounding structures in multiple planes. It has emerged as the primary imaging technique in diagnosing spine disease. The addition of intravenous gadolinium has been shown to be accurate in distinguishing postoperative scarring from recurrent disc herniation.
Chapter 84
Although rarely indicated in straightforward cases of radiculopathy or stenosis, electromyography (EMG) may be a useful adjunct in complex cases. For maximal benefit, EMG should be performed 3 to 5 weeks after symptom onset to allow development of fibrillation potentials. Radiculopathy findings may disappear over time, so it is equally important not to wait too long. One must always correlate the EMG findings with the clinical setting. Do not allow positive EMG results to dictate surgical intervention when appropriate clinical symptoms and radiologic findings are not present. Treatment
Because more than 50% of patients with lumbar disc herniations respond to medical management, it is important to give nonsurgical therapy a trial in almost all patients. Clear indications for urgent surgical intervention include advanced neurologic deficit, cauda equina compression, sphincter dysfunction, neurologic deterioration with conservative management, and recurrent incapacitating episodes of pain. Persistent unacceptable disability from pain with nonoperative therapy is the most common indication for surgery. One must carefully weigh the psychosocial factors (litigation, secondary gain, depression, and so forth) involved in the patient’s disability before surgical intervention. Nonoperative therapy for disc herniation consists of bed rest with the use of selected analgesics, anti-inflammatory agents, and muscle relaxants to reduce symptoms caused by irritation and edema of the affected root. When symptoms have resolved, instruction in posture, back exercises, and moderation of daily activities (“low back school”) are important. Unless neurologic deterioration occurs, most physicians advocate at least 2 to 3 weeks of nonsurgical therapy. Occasionally, a brief course of oral steroids (such as a methylprednisolone dose pack) is useful in relieving symptoms of acute herniation. Although bed rest with lumbar flexion may provide temporary relief of painful radiculopathy, severe lumbar stenosis rarely responds to long-term nonsurgical management. In mild cases, flexion exercises and a lumbar corset or brace may result in relief by facilitating postural correction. Analgesics, anti-inflammatory agents, and muscle relaxants are useful in treating the radicular symptoms while awaiting surgical decompression. Definitive treatment for lumbar stenosis involves wide laminectomy with foraminotomies over the level of spinal compression. Discectomy is rarely indicated with adequate posterior decompression and may contribute to postoperative spinal instability. Inadequate decompression is a common cause of continued symptoms. Chronic cases of lumbar stenosis with advanced muscle atrophy or sphincter dysfunction are least likely to have full recovery. In patients with persistent postoperative mechanical low-back pain, spinal instability must be considered. In most cases, persistent nonradicular pain can be managed medically. In some, supplemental posterolateral spinal fusion may be needed. The decision to operate is based on the combination of clinical findings, the physician’s assessment, and the patient’s input, given all the options. The goal should be the most cost-effective and expeditious management to return each individual safely to full, productive activity.
CERVICAL DISEASE Benign cervical spine disease generally falls into one of two categories: radiculopathy or cervical myelopathic syndrome. How-
Spondyiosis and Disc Disease
541
ever, the pathogeneses of these differ somewhat and are essentially a result of two types of cervical disc anomalies: disc rupture (which results primarily but not exclusively in radiculopathy) and cervical arthrosis and spondylosis (which may result in radiculopathy, myelopathic syndrome, or both). The distinction between these two is essential because one is generally a self-limited condition and the other is progressive, and operative approaches to the two can differ significantly. Although there is no sex predilection to cervical disc disease, predominantly male patients are affected by spondylotic myelopathy. Cervical disc disease is less common than lumbar disease, accounting for only about one in seven spinal herniations. Like lumbar disc disease, most cervical herniations occur at one of two levels that bear the brunt of spinal motion and stress, either C5-C6 or C6-C7. Multiple simultaneous levels of involvement are rare in acute cervical disc herniation but are common with spondylitic disease. Approximately 5% of cervical disc herniations are recurrent. Spondylosis in the cervical spine typically is generated by bony marginal spurring stimulated by bulging discs and is usually located posteriorly or intraforaminally. In contrast, in the lumbar region, this lipping is almost exclusively anterolateral in location and rarely results in foraminal encroachment. Hypertrophy of the ligamentum flavum rarely causes symptoms in the cervical spine, although hypertrophy and ossification of the posterior longitudinal ligament (OPLL) is a well-defined problem. Patients with cervical spondylosis are twice as likely to have lumbar stenosis than the general population. Although generally not causative in and of itself, shallowness of the cervical canal predisposes patients to spondylotic myelopathy. Work-related stress, spasmodic torticollis, and congenital segmental defects such as Klippel-Fed undoubtedly play a role in generating cervical disease. The role of antecedent trauma is less clear. Clinical Features
Pain, paresthesias, and motor and sensory deficits are the hallmarks of cervical radiculopathy, although occasionally there may be a significant discrepancy between sensory and motor symptoms, resulting in either profound painless arm weakness with atrophy or severe incapacitating pain without other neurologic findings. The pain is typically proximal in distribution; the paresthesias are distal. Compression of the lower cervical roots produces very similar pain at the neck base, interscapular region, and shoulder and cannot be used to distinguish radiculopathies. However, cervical paraspinous or superior shoulder pain without radiation to the arm or scapular region should suggest C3-C4 disc herniation. A C6 radiculopathy sometimes causes chest pain, mimicking angina. Paresthesias generally are more accurate in localizing pathology, as summarized in Table 84-3. In addition to the more classic pins-and-needles paresthesia sensations, patients may complain of their hand or arm feeling “odd,” sometimes described as cool and other times just as “not their own.” Occasionally, a large centrally herniated disc results in acute quadriparesis with bowel or bladder dysfunction. Although the symptoms of bony spondylotic nerve root compression are similar to those of disc herniation, the course often is much more indolent. Although spastic paraparesis is the single most common presentation of cervical spondylotic myelopathy, it is distinctly unusual for symptoms to appear full blown or rapidly. Occasionally, however, symptoms can evolve rapidly after hyperextension. Early stages are typified by complaints of weakness and easy fatigability of the legs. The patient may note a
Spinal Cord and Peripheral Neuromuscular Disease
542
Diseases of the Spinal Cord
w TABU863. Common Cervical Root Syndromes Root
Pain location
Sensory Disturbance
Weakness
Reflex Change
C3,C4
Paraspinousmuscles, superior shoulder Neck, shoulder, anterior arm
Neck
Diaphragm, nuchal muscles, strap muscles Deltoid, supraspinatus, infraspinatus Biceps, brachioradialis (extensor carpi radialis, pronator teres) Triceps, latissimus doni, pectoralis major, supinator, pronator teres Intrinsic hand muscles, finger extensors Intrinsic hand muscles (Hornets syndrome)
None
c5
Shoulder Thumb, index finger, radial forearm
C7
Neck, shoulder, anterior upper arm, extending to antecubital fossa Neck, shoulder, dorsum of forearm
C8
Neck, shoulder, ulnodorsal forearm
T1
Neck shoulder, ulnar arm
Ring, little fingers, hypothenar eminence Ulnar forearm
C6
Middle finger
painless pseudoglove-like sensory loss, which prompts a futile investigation for carpal tunnel or peripheral neuropathy. Electriclike sensations with neck motion (Lhermitte’s phenomenon) are common, especially with neck extension. Neck or occipital pain and loss of temperature or pain sensation may be late symptoms. Patients with cervical radiculopathy typically hold their head rigid secondary to spasm. Extension of the head, like extension of the back in lumbar disease, often causes pain by compressing the exiting root against the facets. The Spurling maneuver, axial spine loading in conjunction with contralateral head rotation and extension, can be used to elicit pain much in the same manner as Lasegue’s sign. Flexion and extension may yield Lhermitte’s phenomenon in patients with myelopathy. As in the lumbar spine, motor and reflex changes are most specific for localizing pathology. These are summarized in Table 84-3. In the cervical region, in contrast to the lumbar region, roots are numbered by the vertebrae to which they are cephalad (e.g., the C6 root exits at the C5-C6 disc space level, just above the C6 pedicle and slightly superior to the disc space). Cervical roots exit laterally and ventrally and are held snugly against the disc while coursing toward the inferior pedicle while lumbar roots wrap more closely under the inferior pedicle. This is demonstrated in Figure 84-6. Subtle signs of C7 compression include weakness of the latissimus dorsi and pectoralis major. Latissimus function is evaluated by having the patient cough deeply while palpating these accessory muscles of respiration from behind. Unequal contractions indicate weakness. Pectoralis function is best tested using a pseudo-Froment’s sign or book test. Patients support a book between their palms with elbows extended, and the examiner then attempts to withdraw the book. Failure to maintain the humerus in adduction and involuntary elbow flexion indicates compensation for pectoralis weakness. Motor, sensory, and reflex changes are rare in early phases of spondylotic myelopathy. However, severe arthrosis results in obvious sensory losses, paraparesis, hyperreflexia, spasticity with scissoring of gait, and even upper extremity weakness. Long-term pathology may also be accompanied by anterior horn cell damage or exiting root injury (radiculopathy), resulting in a mixed picture of lower motor neuron findings (hyporeflexia, atrophy, and fasciculations) in the upper extremities combined with upper motor neuron findings in the lower extremities.
Biceps Biceps, brachioradialis Triceps None None
L3
A
I
L4
L5 FIG. 84-6. Comparison of (A) cervical and (B) lumbar root anatomy. The left half of each drawing depicts the bony anatomy; the right side demonstrates the intradural and foramina1 course of the nerve and their numbering. Note the closer application of the lumbar roots to the pedicle, which is found more laterally in the cervical region.
canal should equal the width of the body at its midportion and should be no more than 15% to 25% smaller than the body (Fig. 84-7). Absolute measurements of 14 mm or less indicate a narrow canal. Spurs and retrolisthesis may produce further impingement on canal size. However, it is important to remember that evidence of degenerative spine disease (disc space narrowing, osteophyte formation, and so forth) occurs in 25% to 50% of the population by age 50 and in 75% to 85% by age 65. These findings are most often incidental and asymptomatic. Oblique views may be used to assess neural foramina. Dynamic flexion and extension films are important to assess for anterolisthesis and retrolisthesis. MRI is rapidly supplanting CT myelography for assessing cervical spine disease. However, definition and evaluation of bony anatomy, including osteophyte encroachment on foramina and OPLL, can be inadequate with this imaging modality. CT scanning with intrathecal contrast may be needed for planning operative intervention, particularly with multilevel disease. It is important to remember that involvement at multiple levels can produce additive effects. Treatment
Diagnosis
Plain spine films can be important in evaluating cervical spine disease. Lateral views may demonstrate depth of canal, pedicle size, facets, and subluxation. As a general rule, the depth of the
As with lumbar radiculopathy, conservative therapy plays an important role in managing cervical radiculopathy. Cervical disc herniations usually are self-limited, and patients respond to nonoperative management, consisting of rest, local heat, modulation
Chapter 85
Vascular Disease of the Spinal Cord
543
In cases of severe pain or significant radicular weakness or sensory loss, urgent surgery is indicated. Acute cord compression from disc herniation, as manifested by rapidly progressive paresis, sensory level, or bowel or bladder involvement, also warrants emergency decompression. It is important to remember that long-standing compression with prolonged conservative treatment may lead to pain abatement with persistent weakness or numbness. Failure of return of strength or sensation is an indication for surgical intervention. In most cases cervical myelopathy is a progressive disease with little room for conservative management. Early diagnosis and surgery are key in preventing irreversible spinal cord injury, Cervical collars and nonsteroidal anti-inflammatory drugs may temporarily alleviate pain but do not address the underlying d'isease. Multiple surgical approaches exist for treating both cervical disc and spondylotic disease. These include anterior cervical discectomy with or without fusion, posterior laminectomy and foraminotomy, multiple anterior discectomies with fusion, anterior corpectomy with fusion, and multiple-level laminectomies. The ideal approach can be highly variable and individualized, both from patient to patient and from surgeon to surgeon.
FIG. 8 6 7 . Distance A represents canal width and should be no more than 15% to 25Vo smaller than 6,the vertebral body width.
or limitation of neck activity (through use of a cervical collar), traction, and pharmaceuticals, including anti-inflammatory agents, muscle relaxants, pain relievers, and occasionally steroids. It is imperative to ensure that there is no evidence of cord compromise before initiating traction to prevent cord injury. Head halter traction devices may be used, with initial weights starting at 5 lb and gradually increased as needed to no more than 5 lb per cervical level.
85
SELECTED READINGS Ehni B, Ehni G, Patterson RH Jr: Extradural spinal cord and nerve root compression from benign lesions of the cervical area. p. 2878. In Youmans JR (ed): Neurological Surgery. 3rd Ed. WB Saunders, Philadelphia, 1990 Garfin SR, Rydevik BL, Lipson SJet al: Spinal stenosis. p. 791. In Rothman RH, Simeone FA (eds):The Spine. 3rd Ed. WB Saunders, Philadelphia, 1992 Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1:29, 1991 Walton J, Gilliatt RW, Hutchunson M et al: Aids to the Examination of the Peripheral Nervous System. Bailliere Tindall, London, 1986
Vascular Disease of the St>inalCord Joseph H. Friedman
Vascular disorders of the spinal cord are rare, and most occur in the inpatient setting. Diagnosis may be difficult, and vascular causes of cord syndromes often are not considered. Spinal cord syndromes may be misdiagnosed as laboratory-negative multiple sclerosis or postencephalitic demyelination. Statistics on the incidence and prevalence of vascular cord syndromes are not very reliable as a result. Probably the most commonly recognized vascular disorder of the spinal cord is stroke associated with aortic surgery. However, stroke also occurs in other settings and, as in the brain, is either ischemic or hemorrhagic. Spinal cord vascular syndromes are more difficult to evaluate radiologically because of the small diameter and length of the cord, greater bone encasement, and the frequent problem of localization in which identical corticospinal signs can be caused by lesions anywhere in the thoracic cord. Table 85-1 lists vascular spinal cord syndromes. The spinal cord is supplied by the single midline anterior spinal
artery, which runs the length of the cord, and the two posterior spinal arteries (Fig. 85- 1). The posterior spinal arteries, unlike the anterior spinal artery, form a plexus, and often the artery becomes so small that it appears to be discontinuous. The vascular supply to the anterior and posterior spinal arteries varies with the level (Fig. 85-2). The cervical anterior and posterior spinal arteries are supplied by the vertebral arteries. At lower levels, there are variable numbers of segmental arteries that arise from the aorta and enter the cord via the nerve root sheaths. One vessel, the artery of Adamkiewicz, is larger than the others and supplies the lower thoracic and lumbar cord. This artery arises from the aorta and generally enters the spinal canal on the left side. The anterior spinal artery provides blood to about two thirds of the cord, including the anterior horns, the lateral spinothalamic tracts, and the corticospinal tracts, but not the posterior columns. The posterior spinal arteries supply the posterolateral portion of
Chapter 85
Vascular Disease of the Spinal Cord
543
In cases of severe pain or significant radicular weakness or sensory loss, urgent surgery is indicated. Acute cord compression from disc herniation, as manifested by rapidly progressive paresis, sensory level, or bowel or bladder involvement, also warrants emergency decompression. It is important to remember that long-standing compression with prolonged conservative treatment may lead to pain abatement with persistent weakness or numbness. Failure of return of strength or sensation is an indication for surgical intervention. In most cases cervical myelopathy is a progressive disease with little room for conservative management. Early diagnosis and surgery are key in preventing irreversible spinal cord injury, Cervical collars and nonsteroidal anti-inflammatory drugs may temporarily alleviate pain but do not address the underlying d'isease. Multiple surgical approaches exist for treating both cervical disc and spondylotic disease. These include anterior cervical discectomy with or without fusion, posterior laminectomy and foraminotomy, multiple anterior discectomies with fusion, anterior corpectomy with fusion, and multiple-level laminectomies. The ideal approach can be highly variable and individualized, both from patient to patient and from surgeon to surgeon.
FIG. 8 6 7 . Distance A represents canal width and should be no more than 15% to 25Vo smaller than 6,the vertebral body width.
or limitation of neck activity (through use of a cervical collar), traction, and pharmaceuticals, including anti-inflammatory agents, muscle relaxants, pain relievers, and occasionally steroids. It is imperative to ensure that there is no evidence of cord compromise before initiating traction to prevent cord injury. Head halter traction devices may be used, with initial weights starting at 5 lb and gradually increased as needed to no more than 5 lb per cervical level.
85
SELECTED READINGS Ehni B, Ehni G, Patterson RH Jr: Extradural spinal cord and nerve root compression from benign lesions of the cervical area. p. 2878. In Youmans JR (ed): Neurological Surgery. 3rd Ed. WB Saunders, Philadelphia, 1990 Garfin SR, Rydevik BL, Lipson SJet al: Spinal stenosis. p. 791. In Rothman RH, Simeone FA (eds):The Spine. 3rd Ed. WB Saunders, Philadelphia, 1992 Hlavin ML, Hardy RW Jr: Lumbar disc disease. Neurosurg Q 1:29, 1991 Walton J, Gilliatt RW, Hutchunson M et al: Aids to the Examination of the Peripheral Nervous System. Bailliere Tindall, London, 1986
Vascular Disease of the St>inalCord Joseph H. Friedman
Vascular disorders of the spinal cord are rare, and most occur in the inpatient setting. Diagnosis may be difficult, and vascular causes of cord syndromes often are not considered. Spinal cord syndromes may be misdiagnosed as laboratory-negative multiple sclerosis or postencephalitic demyelination. Statistics on the incidence and prevalence of vascular cord syndromes are not very reliable as a result. Probably the most commonly recognized vascular disorder of the spinal cord is stroke associated with aortic surgery. However, stroke also occurs in other settings and, as in the brain, is either ischemic or hemorrhagic. Spinal cord vascular syndromes are more difficult to evaluate radiologically because of the small diameter and length of the cord, greater bone encasement, and the frequent problem of localization in which identical corticospinal signs can be caused by lesions anywhere in the thoracic cord. Table 85-1 lists vascular spinal cord syndromes. The spinal cord is supplied by the single midline anterior spinal
artery, which runs the length of the cord, and the two posterior spinal arteries (Fig. 85- 1). The posterior spinal arteries, unlike the anterior spinal artery, form a plexus, and often the artery becomes so small that it appears to be discontinuous. The vascular supply to the anterior and posterior spinal arteries varies with the level (Fig. 85-2). The cervical anterior and posterior spinal arteries are supplied by the vertebral arteries. At lower levels, there are variable numbers of segmental arteries that arise from the aorta and enter the cord via the nerve root sheaths. One vessel, the artery of Adamkiewicz, is larger than the others and supplies the lower thoracic and lumbar cord. This artery arises from the aorta and generally enters the spinal canal on the left side. The anterior spinal artery provides blood to about two thirds of the cord, including the anterior horns, the lateral spinothalamic tracts, and the corticospinal tracts, but not the posterior columns. The posterior spinal arteries supply the posterolateral portion of
544
Diseases of the Spinal Cord
Spinal Cord and PeripheralNeuromuscular Disease
the cord, including the posterior columns on each side. The venous system draining the cord is composed of multiple small networks rather than particular large vessels with well-defined territories. The dura is supplied by dural branches of the intercostal or lumbar arteries that supply the cord. The pia is supplied by intramedullary spinal cord arteries. The subarachnoid space contains some vessels but fewer than the dura mater.
W
TABLE 85-1. Vascular Spinal Cord Syndromes
Acute Transient ischemic attack Infarct Subarachnoid hemorrhage Intramedullary hemorrhage Rapidly progressive Epidural hematoma Subdural hematoma Slowly progressive Arteriovenous malformation (dural or intradural)
B
STROKE A N D TRANSIENT ISCHEMIC ATTACK Clinical F e a t u r e s Ischemia of the spinal cord usually occurs in the distribution of the anterior spinal artery. Because the anterior portion is supplied by a single midline artery, in contrast to the paired posterolateral vessels and their plexus-type network that supply the dorsal portion, there is no collateral circulation in cases of hypoperfusion. Anterior cord ischemia typically causes the abrupt onset of radicular or diffuse back pain, flaccid weakness, sphincter dysfunction, and a sensory level for pain and temperature with preservation of the posterior column sensations of touch and position sense (Table 85-2). Obviously, the limbs involved and the sensory level depend on the level at which the ischemia occurs. Although the region of the cord most at risk because of poor collateral circulation is T5-T7, any region of the cord can become ischemic. Sulcal artery occlusion can produce a Brown-Skquard syndrome or other partial cord syndromes, whereas sustained hypotension or aortic dissection is more likely to produce a symmetric anterior cord syndrome.
J of, Post. Medullary Septum
L
t. Radicular A.
ha1 Branch
/ .Post. Ramus -Ant.
Ramus
V I F A n t . Radicular A. Ant. Medullary A. Ant. Spinal A.
Segmental A.
-Aorta
FIG. 85-1. Arterial supply to the spinal cord. (From Sliwa JA, MacLean IC: Ischemic myelopathy: a review of spinal vasculature and related clinical syndromes. Arch Phys Med Rehabil 73:365-372, 1992, with permission.)
Chapter 85 W Vascular Disease of the Spinal Cord
I
545
Etiology
t Basilar A. Ascending Cervical A. Deep Cervical A. ostocervical trunk hyrocervical trunk
Superior Intercostal A.
Ant. Medullary A.
Ilio-lumbar A. C o m m o n I l i a c A.
L a t e r a l S a c r a l A. with Sacral Segmental Arteries
FIG. 85-2. Origin of the segmental arteries. (From Sliwa JA, MacLean IC: Ischemic myelopathy: a review of spinal vasculature and related clinical syndromes. Arch Phys Med Rehabil 73:365-372, 1992, with permission.)
Posterior arterial and venous infarctions are very rare. Venous thrombosis can produce either bland or hemorrhagic infarction of the cord. Hemorrhagic infarcts tend to be sudden in onset, of rapid progression, and associated with back pain. Nonhemorrhagic infarcts are more insidious and indolent, developing over hours to days, without back pain. Embolic occlusion of veins is sudden in onset and often painful. Venous infarctions have a wider range of presentations than arterial occlusions because of the less well-defined vascular territories. Motor or sensory dysfunction or even central cord syndromes, such as dissociated sensory loss, can be seen, and the length of cord involved can be long. Posterior artery occlusions produce motor involvement in all cases, but of a variable degree. The sensory loss also is variable and may be limited to posterior column sensation. Bowel and bladder dysfunctions are common.
Aortic disease is the most likely cause of cord ischemia, but cardiac emboli, coagulopathies, and vasculitides are also potential causes. Syphilitic aortitis was the most common cause for cord stroke in the prepenicillin era, but atherosclerosis is thought to be the most common current cause. A rare cause of arterial emboli includes fibrocartilage. Atherosclerosis can cause spinal cord transient ischemic attacks (TIAs), infarcts, and slowly progressive syndromes. Aortic dissection may cause spinal cord ischemia and typically is associated with severe pain, probably from the vascular dissection itself independent of cord effects. Although cord infarcts may occur in a typical setting of atherosclerosis and peripheral vascular disease, it may occur in rare circumstances such as focal atherosclerosis after radiation treatment of a malignancy, aortic thrombosis, or a coagulopathy from an anticardiolipin antibody. A rare cause of cord stroke is sustained hypotension in a person who is maintained in an upright position, as may occur with a drug overdose in someone seated upright. Venous thrombosis may be idiopathic or associated with any thrombotic condition. Spinal cord TIAs may result from arterial narrowing, emboli, or transiently increased venous pressure. Steal phenomenon may also cause a TIA and occurs typically with an arteriovenous malformation (AVM) but has been observed with aortic coarctation. The differential diagnosis for transient cord dysfunction must include tumors, especially epidural metastases (Table 85-3). It is hypothesized that tumors cause transient neurologic dysfunction by a steal phenomenon, by arterial compression, or by increased venous pressure. Demyelinating diseases may also cause transient neurologic dysfunction and often are associated with pain, similar to that present with ischemia. If the episode is thought to be a TIA, then the proper evaluation depends on the clinical circumstances. Evaluation
The evaluation of a spinal cord stroke or TIA should include a two-dimensional echocardiogram and probably also a transesophaged echocardiogram (Table 85-4). Whether an aortic angiogram
TABLE85-2. Features of Spinal Cord Stroke Acute back and radicular pain Flaccid leg weakness (occasionally arm and leg) Loss of pain and temperature below lesion Preservation of touch and position senses Urinary retention
TAU -3.
DifferentialDiagnosis
Spinal cord transient ischemic attack Demyelinating disease Tumor Spinal stenosis or claudication Spinal cord stroke Tumor Epidural hematoma Subdural hematoma Syringomyelia Abscess, infection Demyelination Transverse myelitis Disc herniation Arteriovenous malformation
546
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of the Spinal Cord
TABLE 85-4. Evaluation of Ischemic Spinal Cord Syndromes
(Transient Ischemic Attack and Stroke) Magnetic resonance imaging of cord with and without gadolinium Coagulation studies Rapid plasma reagin test to exclude syphilis Routine and transesophageal echocardiograms Consider helical computed tomography of aorta Angiogram Vasculitis evaluation
or a spinal angiogram should be performed is determined by the clinical circumstances. Evaluations for syphilis, a coagulopathy, or a vasculitis must be considered. Magnetic resonance imaging (MRI) of the spinal cord, including a contrast examination, should be considered mandatory to exclude a tumor masquerading as ischemia. There are two main problems in diagnosing spinal TIA and stroke. First, because they are so uncommon, they are not considered on the differential diagnosis. The second problem is in confirming the diagnosis once suspected. As with cerebral TIAs, the diagnosis is made on history, risk factors, and exclusion of alternative diagnoses. Unlike cerebral strokes, cord infarcts can rarely be visualized on computed tomography (CT) and only uncommonly with MRI. Spinal angiography is available only at centers with specialized neurosurgical services, is potentially harmful, may not reveal an occlusion if the embolus has dislodged or fragmented after causing infarction, and, finally, probably will not alter therapy, making it a questionable proposition. Thus, spinal cord infarct often is a diagnosis of exclusion. Spinal angiography probably has a morbidity rate of about 5% as a result of the dye load and the small, atherosclerotic vessels involved. It should be performed in cases of suspected spinal AVMs or other conditions in which a definitive diagnosis would alter management in a tangible fashion. Aortic dissection is a life-threatening diagnosis and, if considered possible, should be excluded with a CT angiogram (helical CT). Venous infarcts may occur in the setting of severe systemic disorders or with AVMs.
Treatment
Treatment for cord ischemia presumably is identical to that of cerebral ischemia, but no data exist. The risk of reembolization should be reduced by using anticoagulants for cardiac emboli and aspirin when atherosclerosis is the presumed mechanism. Treatment of any other identified condition (e.g., vasculitis, hypercoagulable state) should be implemented. There are no data to support or counter the use of heparin in an acute infarct or shortly after a TIA. The increased risk of hemorrhage into such a small structure as the spinal cord precludes its use except for treating a known thrombotic or cardiac embolic disorder. When the cause of stroke is an aortic dissection, this should be addressed as soon as possible. Obviously, these patients are the most at risk from surgery or cautious waiting. The prognosis for cord stroke is unclear. As with strokes in the cerebral circulation, the prognosis is highly variable and unpredictable in any particular patient. In one series of eight cases, the patients who survived were all able to walk out of the hospital. However, a different series reported significantly worse results, with most patients making little improvement and remaining unable to walk. Almost all patients in the second study suffered chronic limb pain for several months.
HEMORRHAGES AND VASCULAR MALFORMATIONS Epidural Hematomas
Spontaneous hematomas into the epidural space occur more often than those into the subdural space because of their differences in vascularity. They both cause severe localized pain at the site of the hemorrhage, followed shortly by radicular pain. A few hours to a few days later, focal spinal cord deficits develop, which include paraparesis, quadriparesis, a sensory level deficit, and bladder dysfunction. Syndromes such as the Brown-SCquard syndrome may also occur. Most patients with spontaneous hematomas have a bleeding diathesis caused by excessive anticoagulation, liver failure, or use of antiarthritic drugs, which interfere with platelet function. The ictus may be triggered by sudden major changes in intraabdominal or intrathoracic pressure but may also be precipitated by mundane activities such as straining to defecate or calisthenics. Epidural hematoma is also a feared complication of lumbar puncture in patients with coagulopathies. One recent study suggests that this is quite unlikely, however. lntradural Hematomas
Subdural hematomas may localize to any level of the cord but tend to be rostral and dorsal. In contrast, epidural hematomas are mostly anterior. The neurologic clinical features are similar for subdural and epidural hematomas, making a clinical distinction difficult before imaging. Progression of deficits is the rule until the bleeding abnormality is corrected and the clot evacuated. The differential diagnosis is that of a rapidly progressive, painful cord syndrome. This includes sudden disc herniation, epidural cord compression from cancer, spinal cord ischemia, arterial dissection, epidural abscess, intraparenchymal tumor, and cyst. If the patient is evaluated when the pain is the only symptom, then an epidural or subdural hematoma should be considered only if a bleeding abnormality is known. Because deficits progress over hours in the presence of a coagulopathy and outcome depends on the severity and duration of the deficits, this must be considered a neurosurgical emergency. An immediate MRI scan is the diagnostic test of choice while the coagulopathy is being reversed, followed by an emergency surgical decompression. Dural Arteriovenous Malformation
Spinal AVMs are anatomically divided into intradural and nonintradural. Intradural AVMs can present with subarachnoid hemorrhage (SAH) or with progressive neurologic deficits. Dural AVMs tend to occur in patients in their fifth and sixth decade, whereas intradural AVMs occur in patients 10 to 25 years old. Dural AVMs occur near the nerve root sheath and, unlike most other spinal cord vascular syndromes, tend to be slowly progressive and may not be painful. Dural AVMs are more common in older men than in women. The symptoms vary, depending on location. The legs are the most affected. Sensory levels, paraparesis, bladder dysfunction, and radicular pain are common. Diagnosis is difficult because of problems of imaging sensitivity. A careful dorsal myelogram is more sensitive than a spinal MRI scan, but even so an AVM may be missed. Spinal angiography is the most sensitive test.
Chapter 85
The differential diagnosis of a progressive cord syndrome in older patients must include demyelinating diseases and tropical and familial spastic paraparesis. When the signs are primarily motor, then motor neuron disease or a peripheral neuropathy is considered. Depending on the rapidity of progression, a cord tumor must be excluded. A ruptured spinal AVM causes severe spinal and radicular pain at the site of rupture followed by the usual signs of an S A H , meningismus and obtundation. If the history of pain is not obtained, a distinction from the usual cause of SAH, namely a ruptured berry aneurysm, cannot be made. Spinal AVMs make up only a small fraction of the total of S A H but should be considered when the cerebral angiogram is unrevealing, especially if a history is obtainable and points to a focal spinal onset. Because these malformations may rebleed, identification and treatment are important. There appears to be a predilection for SAH from spinal AVMs to affect women, particularly in pregnancy. Both subdural and dural AVMs may induce slowly progressive cord syndromes and must be considered in cases of otherwise unexplained cord disease. Weakness and sensory changes in the legs are the most common presenting features, rather than pain, as is true of other vascular disorders of the spinal cord. Pain may be present, either early in the course or on a chronic basis, but has no particular features to distinguish it from the more common low back pain radicular syndromes. Bladder and sexual dysfunction may also occur. Spontaneous thrombosis of spinal cord veins draining in intradural AVM, a rare phenomenon, is known as the FoixAlajouanine syndrome. It may lead to slow or rapid spinal cord dysfunction. This has recently been described with intracranial dural AVMs draining into spinal veins but is typically seen with spinal intradural AVMs. AVMs of the body may be associated with cord AVMs, as in the Klippel-Trenaunay-Weber syndrome. In this syndrome a cutaneous angioma may be accompanied by a spinal cord AVM. Symptoms tend to occur in older patients, although the malformations are thought to be congenital. Because diagnosis may be difficult, it is possible that presentations at younger ages are thought to be caused by laboratory-negative multiple sclerosis,
Vascular Disease of the Spinal Cord
547
an entity that becomes increasingly rare with age, or to other, as yet poorly defined nonvascular entities.
SUGGESTED READINGS Byrne TN, Benzel EC, Waxman S G Disease of the Spine and Spinal Cord. Oxford University Press, New York, 2000 Caplan LR, McKee A C Case records of the Massachusetts General Hospital: a 65-year-old woman with an abrupt paralysis of the legs and impairment of bladder and bowel function. N Engl J Med 324:322332, 1991 DeToffol B, Cotty P, Gaymard B, Velut S: Progressive necrosis of the conus medullaris: magnetic resonance imaging and surgical findings. Neurosurgery 26:147-149, 1990 Howard SC, Gajjar A, Ribeirio RC et al: Safety of lumbar puncture for children with acute lymphoblastic leukemia and thrombocytopenia. JAMA 284~2222-2224, 2000 Katz JD, Ropper AH: Progressive necrotic myelopathy: clinical course 1-9 patients. Arch Neurol 57:355-361, 2000 Kim RC, Smith HR, Henbest ML, Choi BH: Nonhemorrhagic venous infarction of the spinal cord. Ann Neurol 15:379-385, 1984 Koenig E, Thron A, Scharder V, Dichgans J: Spinal arteriovenous malformations and fistulae: clinical neuroradiological and neurophysiological findings. J Neurol 236:26&266, 1989 Mattle H, Sieb JP, Rohner M, Mumenthaler M Nontraumatic spinal epidural and subdural hematomas. Neurology 37:1351-1356, 1987 Rosenblum B, Oldfield EH, Doppman JL, DiChira G Spinal arteriovenous malformations: a comparison of dural arteriovenous fistulas and intradural AVMs in 81 patients. J Neurosurg 67:795-802, 1987 Sandson TA, Friedman JH: Spinal cord infarction: report of 8 cases and review of the literature. Medicine 68:282-292, 1989 Satran R Spinal cord infarction. Curr Concepts Cerebrovasc Dis Stroke 22~13-17, 1987 Shephard RH: Spinal arteriovenous malformations and subarachnoid haemorrhage. Br J Neurosurg 65-12, 1992 Sliwa JA, MacLean I C Ischemic myelopathy: a review of spinal vasculature and related clinical syndromes. Arch Phys Med Rehabil 73:365-372, 1992 Wrobel CJ, Oldfield EH, DiChiro G et al: Myelopathy due to intracranial dural arteriovenous fistulas draining intrathecally into spinal medullary veins. Report of three cases. J Neurosurg 69:934-939, 1988
SECTION
2
MOTOR NEURON DISEASE
86
Amyotrophic Lateral Sclerosis Jeremy M. Shefner
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease of the motor system. A complete understanding of the pathogenesis of ALS remains elusive; however, in the last decade there have been dramatic advances. Glutamate-mediated neurotoxicity has been implicated in the degenerative process, as has decreased capacity to handle oxidative stress. For approximately 10% of patients, the disease is inherited in an autosomal dominant fashion. A mutation in the gene for cytosolic Cu/Zn superoxide dismutase (SOD1) is now known to be responsible for the disease in a minority of patients with inherited disease. This mutation causes disease in a small number of patients with ALS, but its discovery has triggered investigations into a wide range of therapeutic possibilities. The recent development of a mouse model of ALS based on the human SOD mutation allows rapid screening of potential new treatments, increasing the likelihood of developing effective new treatments. For years, ALS has represented a special challenge for neurologists, who were confronted with intellectually intact, often young patients for whom only symptomatic care was available. Although treatment options are still limited, it is now clear that the disease course can be modified, both by drugs that delay the progression of disease and by active treatment of pulmonary and nutritional factors. The availability of disease-modifymg agents makes the need for early diagnosis and treatment critical. This chapter focuses on the diagnosis and care of patients with ALS. Hypotheses about the cause of the disease and detailed discussion of potential therapeutic agents are deferred.
DEFINITION ALS is defined as a disease involving progressive upper and lower motor neuron deterioration at multiple levels of the neuraxis. At presentation, patients may have signs and symptoms related to just upper motor neuron or lower motor neuron disease, but the diagnosis can be made with certainty only if both types of abnormalities are present. The World Federation of Neurology has established criteria for the diagnosis of ALS; on purely clinical grounds, a diagnosis of ALS requires the presence of both upper and lower motor neuron signs in the bulbar musculature and concurrent upper and lower motor neuron involvement in two of the three spinal regions (cervical, thoracic, and lumbosacral). Lower motor neuron signs include weakness, muscle wasting, and fasciculations; upper motor neuron signs include increased deep 548
tendon reflexes, spasticity, pseudobulbar features, extensor plantar responses, and other abnormal stretch reflexes. When patients fulfill these criteria, the physician is left with little in the way of differential diagnosis, even in the absence of confirmatory diagnostic tests. Most commonly, however, patients present with fragments of this syndrome, and the clinician must make appropriate use of neurophysiologic and radiologic tests to eliminate other possible diseases. Common initial presentations are discussed later in this chapter; in time, most patients who present with partial syndromes show spread of abnormalities, so the diagnosis becomes more obvious. However, some patients present with some features of ALS but not others and demonstrate progression that does not seem consistent with the diagnosis of classic disease. A small subgroup of patients presents with a purely spastic disorder, involving increased tone in bulbar and spinal musculature, slow and clumsy movements, but little muscle wasting or weakness. This syndrome has been named primary lateral sclerosis and was described in the 1800s shortly after the original descriptions of ALS. Almost from its initial description, there was argument about whether primary lateral sclerosis was a separate disease or an atypical presentation of ALS. It is generally believed that, in most cases, patients presenting initially with pure upper motor neuron signs eventually develop classic ALS. However, a minority of such patients appear to have disease limited to the descending cortical pathways. These patients have a more benign clinical course, with expected survival greater than 15 years. Another subgroup of patients presents with purely lower motor neuron signs; in these patients, reflexes usually are absent or reduced. Often, the presenting complaint is limited to weakness in one limb; with time, weakness spreads to involve multiple extremities. Some of these patients develop signs of upper motor neuron dysfunction and thus are classified as having classic ALS. Others remain with only lower motor neuron signs, showing increasing weakness and atrophy in multiple areas of the neuraxis. Formerly, these patients were said to have progressive muscular atrophy and were distinguished from patients with ALS on the basis of their lack of upper motor neuron signs and their slow progression. With increasing electrophysiologic sophistication, however, many of these patients are now known to have a motor neuropathy rather than an anterior horn cell disease; these patients are discussed in Chapter 89. A final group of patients are those presenting with signs limited to the bulbar musculature. Usually, by the time these patients are
Chapter 86
seen, both upper and lower motor neuron signs are seen together; most often, speech is spastic, and fasciculations of the tongue are obvious. Historically, this presentation was called progressive bulbar palsy and was distinguished from classic ALS. However, it is now generally believed that these patients will develop classic disease, and their clinical course is indistinguishable from that of other patients with ALS.
EPIDEMIOLOGY ALS is a rare disease. Its incidence of 1.5 in 100,000 population is fairly constant worldwide, except for some specific foci of higher incidence that probably represent toxic exposure. In the United States, approximately 5000 patients are diagnosed with ALS every year. Average lifespan after diagnosis is 3 to 5 years, so that there are approximately 20,000 patients living with ALS in the United States. Men are more likely to contract the disease than women, with recent studies suggesting a male-to-female ratio of about 1.5, except in familial disease, where the ratio is 1:1. In general, ALS is a disease of middle to late life. Although cases have been documented of onset in the teenage years, most studies show the average age of onset ranging from 55 to 60 years. The incidence appears to rise steadily until approximately age 65 and then declines slowly. The incidence does not vary according to race, environment, or occupation. Approximately 10Y0 of patients report a family history of ALS, most often in an autosomal dominant pattern. In 1993, a point mutation in the gene for SODl was discovered. Subsequently, many other point mutations in the same gene have been identified. Although there is some variability in patients with identical mutations, it is clear that specific mutations are associated with more rapid or more slowly progressive disease. Other than rate of progression, however, patients with familial ALS from an identified mutation are indistinguishable from those with sporadic disease. The mechanism by which mutations in SODl produce disease is still unclear. However, recent studies have shown that mice with a normal complement of murine SODl who are genetically modified to overexpress the human mutant gene develop a motor neuron disease resembling ALS. This clearly implies that protein coded by the mutant gene exerts a toxic effect because these mice do not have an SODl deficiency. As mentioned earlier, in some areas in the world the incidence of ALS is much higher than in the United States. On Guam, a small peninsula in Japan, and parts of New Guinea, incidence rates are up to 100 times higher than elsewhere in the world. Many studies have attempted to determine why these areas have such high rates of U S ; the most likely cause seems to be a toxin in the food supply.
CLINICAL FEATURES Although patients with classic ALS involving both the extremities and the bulbar musculature present with a very characteristic clinical picture, most patients with early disease have focal signs and symptoms. The most common initial symptom is that of arm weakness; about one half of all patients with ALS present in this fashion. A wrist drop is a characteristic early sign, often noted concurrently with intrinsic hand muscle wasting. For unclear reasons, flexor compartment forearm muscles usually are affected later in the disease. Because of this asymmetry of forearm involvement,the hand often assumes a clawed posture. The disease usually spreads regionally, going from the distal to the proximal
Amyotrophic Lateral Sclerosis
519
arm; biceps and deltoid muscles usually are affected before the triceps. About one quarter of patients present with lower extremity symptoms, most commonly unilateral foot drop. As in the upper extremity, weakness tends to spread regionally, first to more proximal muscles in the same leg and then to the opposite leg before ascending to involve the arms. Most of the remaining patients present with symptoms of bulbar dysfunction or bulbar dysfunction in combination with other symptoms. Changes in the clarity of speech often are the first bulbar symptom, with difficulty swallowing also noted early. Patients notice that telephone communication is more difficult and often report that speech is more slurred late in the day. Swallowing liquids becomes difficult before solids; carbonated and alcoholic liquids are likely to be the least well tolerated, with thicker liquids tolerated better. Most of these signs and symptoms are related to lower motor neuron dysfunction; although upper motor neuron signs may be appreciated by the examining physician early in the course of ALS, they rarely are the cause of symptoms. Occasional patients present with initial complaints of limb stiffness and slowed movements, but such patients clearly are the exception. Even as the disease progresses and upper motor neuron signs become more apparent, lower motor neuron loss continues to be the most important factor affecting disability. Other less common presentations of ALS are isolated respiratory failure and diffuse fasciculations. Fasciculations are a common symptom in the general population and can precipitate a visit to a neurologist. In the absence of clear signs of motor neuron loss, however, fasciculations are almost never a harbinger of ALS. Physical examination of patients with isolated fasciculations usually is sufficient to provide reassurance. Electromyography (EMG) documents the presence of fasciculations but cannot distinguish between those that are benign and those that are associated with ALS. Muscle cramps are commonly reported by patients but almost always in association with significant upper motor neuron disease; they are not usually seen in otherwise normal limbs. A number of symptoms should make the physician doubt the diagnosis of ALS. Although end-gaze nystagmus and mild abnormalities of rapid eye movements can be seen, diplopia or vertigo are extremely uncommon. Vague sensory symptoms often are reported by patients, but objective sensory loss is rare and suggests alternative or concurrent disease processes. Often patients complain of a dysesthetic feeling; it is unclear whether this is a true sensory symptom or muscle soreness from overuse. Bowel or bladder incontinence is also said not to occur in ALS. However, constipation is a common complaint, perhaps related to loss of abdominal muscle tone. In addition, urinary urge incontinence often is reported, more often by women than by men. Urinary dysfunction is seen most often in two patient groups. Female patients who recall having temporary urgency incontinence after childbirth are likely to have recurrence of such symptoms. In addition, women (and occasionallymen) with a prominent upper motor neuron component to their disease may also report episodes of incontinence. In recent years, a number of carefully performed studies have yielded new information about how ALS progresses. Although patients report that periods of relative stability are interrupted by episodes of rapid deterioration, quantitative strength measurements have not confirmed these impressions. In several recent studies, patients were studied at regular intervals over a period of
550
Spinal Cord and PeripheralNeuromuscular Disease W
years using a battery of tests, including quantitative measurements of individual muscle strength and pulmonary function tests of vital capacity and inspiratory and expiratory force. It was found that if measurements from local body areas were combined to produce separate scores for arms, legs, bulbar, and pulmonary performance, strength declined linearly in any given area. The rate of decline varied within the same patient for different body areas, so that, for example, pulmonary function could decrease more rapidly than lower extremity strength. However, if a certain body area declined in strength slowly initially, the decline tended to remain slow throughout the course of the disease. The observation that ALS progresses in a predictable manner within local body regions for individual patients has a number of important implications. First, it allows physicians to give patients some way to evaluate how fast they are progressing and, to some extent, what the future holds. Obviously, this information is more reassuring to slowly progressing patients, but most patients appreciate realistic appraisals of their disease course. In addition, the ability to predict with some accuracy the course of an individual patient is important in designing therapeutic trials, offering the potential to decrease the size of control groups by reducing random variability of the population. Another important recent observation is that the deficits in ALS tend to progress in a regional manner. Thus, patients presenting with distal leg weakness are likely to experience proximal spread of weakness or symptoms in the contralateral leg before cranial nerve or pulmonary symptoms are noted. Along with the observation that different body regions progress at different rates, the phenomenon of regional spread suggests that local conditions in the central nervous system affect the course of the disease.
LABORATORY EVALUATION AND DIFFERENTIAL DIAGNOSIS Fully established classic ALS necessitates little in the way of laboratory support. However, in patients who present with focal complaints, a wide differential diagnosis must be considered. Compressive spinal and root disorders must be ruled out in patients without bulbar signs; concurrent cervical myelopathy with multiple root entrapments can produce a syndrome of combined upper and lower motor neuron dysfunction that is very difficult to distinguish from ALS. Clinically, the presence of sensory symptoms should help lead to the correct diagnosis, but radiologic study is crucial. Currently, magnetic resonance imaging of the spine is the diagnostic modality of choice. Often, it is necessary to image the entire spine before concluding that a compressive syndrome is not present. For patients who present with prominent upper motor neuron signs in the bulbar musculature or the extremities, such entities as multiple strokes, mass lesions, and multiple sclerosis must be considered. Magnetic resonance imaging of the head in such patients is indicated and usually is a sufficient tool to rule out these diseases. Historically, lumbar puncture has been performed frequently on patients with a probable diagnosis of ALS. Extremely high cerebrospinal fluid protein levels occasionally led to an unsuspected diagnosis of spinal cord compression, and the possibility of infection was frequently discussed. With improved radiologic modalities, however, the utility of lumbar puncture in patients
Motor Neuron Disease
with classic signs has declined, and it is not necessary to perform this test routinely. Blood tests do not play a major role in the diagnosis of classic ALS. However, some patients may present with only lower motor neuron signs, early age of onset, or other atypical features such as superimposed extrapyramidal or cerebellar signs. Such patients must undergo specific laboratory tests based on their particular presentation. In patients who present primarily with lower motor neuron signs, the differential diagnosis includes motor neuropathy, plexopathy, toxic exposure, metabolic dysfunction, infection, and muscle disease. The syndrome of multifocal motor neuropathy with conduction block can mimic ALS with primarily lower motor neuron involvement; diagnosis is established through careful nerve conduction studies and clinical examination. In addition, antibodies to gangliosides often are present in peripheral blood; gangliosides are an essential component of nerve membranes. Thus, blood should be sent routinely for ganglioside antibodies in patients with suspected ALS and predominant lower motor neuron signs. Details of this syndrome are discussed in Chapter 89. A screen for heavy metal intoxication often is performed but rarely contributes to the diagnosis in patients with lower motor neuron signs. Both lead and mercury intoxication has been reported to be associated with ALS-like syndromes; however, the more usual presentation of toxicity is a predominantly motor neuropathy with some sensory abnormalities but no upper motor neuron signs. Aluminum toxicity has been invoked as a possible cause of ALS in areas where the incidence of ALS is high, but evidence that it causes a significant neuropathy or ALS-like syndrome in the United States is lacking. In general, unless there is a history of prior exposure, blood and urinary screens for heavy metals are not likely to be contributory. One rare inherited metabolic disease can be mistaken for ALS. Hexosaminidase deficiency usually is a severe multisystem disease of childhood; however, occasionally it can present as late as age 40 years with a progressive disease that can closely mimic ALS. Hexosaminidase deficiency is inherited as an autosomal recessive trait, two genotypes of which have been associated with motor neuron syndromes. However, both types also involve other brain systems, often causing extrapyramidal or cerebellar signs, psychiatric disorders, and seizures. In general, screening for hexosaminidase deficiency is not warranted in patients with classic ALS presenting after age 40; however, in younger patients or in patients with atypical features, a blood test is available. Infections rarely are a source of confusion in the diagnosis of motor neuron diseases. However, a few possibilities should be kept in mind. Lyme disease, caused by the infectious agent Borreliu burgdorferi, commonly causes a neuropathy or radiculopathy as a secondary effect. Usually, this neuropathy has both sensory and motor features, but occasionally motor dysfunction is noted in isolation. In patients with a predominantly lower motor neuron syndrome who live in endemic areas, Lyme titers should be obtained; however, because the incidence of incidental positive titers is high in such patients, determination of antibody type should also be performed, and a lumbar puncture to determine whether there is central nervous system antibody production may be necessary. Human T-cell lymphotrophic virus type I (HTLV-I) is a neurotropic virus associated with a progressive spastic disorder sometimes associated with a neuropathy, making it very difficult to distinguish from ALS. If patients are from areas in which HTLV-I is endemic and have any atypical features such as back pain,
Chapter 66 W Amyotrophic Lateral Sclerosis
bladder dysfunction, or absent bulbar signs, blood and cerebrospinal fluid tests for antibodies to HTLV-I are available.
ELECCROPHYSlOLOClCFEATURES Electromyography EMG has proved to be an important tool both in establishing the diagnosis of ALS and in elucidating its pathophysiology. The abnormalities seen in ALS are similar to those seen in other forms of neurogenic disease. Evidence of ongoing denervation is derived from the presence of abnormal spontaneous activity such as fibrillation potentials. As a consequence of denervation, surviving motor axons reinnervate muscle fibers, producing characteristic abnormalities in motor unit morphology, as recorded by conventional concentric EMG electrodes and by newer techniques such as single-fiber and macro-EMG. Although the abnormalities seen in ALS resemble those present in other diseases of the anterior horn cell and motor axon, the distribution of abnormal findings and the pace of disease progression often are useful in distinguishing ALS from other diseases. Fibrillation potentials and positive sharp waves reflect activity of individual muscle fibers that have lost their synaptic contact with motor neurons. The frequency with which fibrillations are observed in ALS varies according to the amount of weakness or atrophy of the muscle being studied, the duration of the disease, and the location in the body. In addition, fibrillation potentials are more likely to be seen in certain muscle groups than in others. In the limbs, fibrillations are present more often in distal than in proximal muscles, with facial and tongue muscles being less likely than limb muscles to show fibrillations. Interestingly, fibrillations are noted in thoracic paraspinal muscles in most patients. Diagnostically, this is a useful finding because spondylosis of the thoracic spine is uncommon compared with cervical and lumbar spondylosis, and abnormalities noted in the thoracic region are thus less likely to reflect root compression. One of the most characteristic abnormalities seen in patients with ALS is the presence of fasciculations. Clinically, they are seen in most patients; electrophysiologically, they are noted almost without exception, even in sites where involuntary movements are not appreciated. However, it should be noted that clinical and electrophysiologicfasciculations may be entirely benign and that there is no way to distinguish between benign fasciculations and those that represent motor neuron disease. The changes seen in motor unit morphology in patients with ALS are qualitatively similar to those that occur as a consequence of any form of neurogenic atrophy. As anterior horn cells are lost, viable motor axons establish synaptic contact with muscle fibers that have been denervated. The electrical correlate of this process is an increase in amplitude and duration of the motor unit action potential. On average, motor unit amplitude is increased by about a factor of 4 over normal, with units in severely involved muscles having amplitudes of approximately 10 times normal and amplitudes from units in only slightly affected muscles increased somewhat less. The increase in size of individual motor unit potentials reflects reinnervation by viable motor axons after the death of other anterior horn cells. Thus, the number of functioning motor units in a given muscle should decrease with disease progression. A number of methods for estimating the number of motor units have been developed for distal muscles and have more recently
551
been extended to larger proximal muscles. In general, the number of motor units present in a given muscle is estimated by determining the maximum amplitude of the compound muscle action potential and then recording potentials from many single motor units. The total number of motor units is estimated by dividing the average amplitude of the single motor unit potentials into the amplitude of the compound motor action potential. Motor unit counting is a very useful way to measure disease progression objectively. By sequential performance of this test on individual patients over time, it has become clear that there is very substantial motor unit dropout before patients report loss of strength in a muscle and before the amplitude of the compound motor action potential has declined below normal. The most rapid dropout of motor units actually occurs very early in the disease, often before a muscle is symptomatically weak. In patients whose disease follows a chronic course, motor unit counts may remain stable for a long time period after dropping to approximately 10% to 20% of normal. Nerve Conduction Studies Although many patients with A L S report vague sensory symptoms, clinical sensory examination usually is normal. Therefore, it is not surprising that routine sensory nerve conduction studies are normal or nearly normal in most patients. However, just as very careful computerized tests of sensation have shown mild alterations in multimodal sensory function in patients with ALS, precise recordings of slower conducting sensory fibers have shown frequent mild abnormalities in the compound sensory action potential. This is consistent with autopsy studies, which have found up to 30% reductions in the number of dorsal root ganglion cells. In studies of motor function, conduction velocity in patients with ALS has been shown consistently to be normal or near normal until muscle atrophy becomes extreme. However, even when motor conduction velocity is normal, distal motor latency often is prolonged. Distal latencies that are prolonged out of proportion to proximal conduction velocity is a finding often associated with dying-back neuropathies in which the terminal axon is more affected than the cell body or proximal axon. Although ALS primarily causes a motor neuronopathy, recent morphologic studies suggest a component of dying-back axonopathy.
Dlagnostlc ElectrophysSologic CrHerSa ALS is primarily a clinical diagnosis. However, EMG and nerve conduction studies can be extremely important in establishing the diagnosis when insufficient clinical evidence is available. A number of criteria for electrophysiologic diagnosis have been suggested. As in many other diseases, the rigid application of criteria often is more a hindrance than a help; however, certain guidelines should be remembered. First, evidence of muscle denervation should be diffuse; that is, fibrillation potentials and large motor units should be present in multiple muscles of multiple extremities. Most published criteria require denervation to be present in three of four areas of the neuraxis, with the four areas being bulbar, cervical, thoracic, and lumbosacral. Second, there should be no evidence of motor conduction block. A formal discussion of conduction block is beyond the scope of this chapter, but conduction block implies that there is an area of axon through
552
Spinal Cord and Peripheral Neuromuscular Disease W
Motor Neuron Disease
which action potentials are not conducted, even though viable axon exists both proximal and distal to that area. Third, motor and sensory conduction velocity and compound sensory action potential amplitudes should be normal or nearly so from both arm and leg. If these conditions are fulfilled, the diagnosis of lower motor neuron disease can be considered confirmed. To make a diagnosis of ALS, however, clinical evidence of upper motor neuron disease must also be present.
TREATMENT Treatment of ALS has changed dramatically in the last decade. Although disease-modifymg treatment is still limited, care has evolved from a passive and supportive model to much more active intervention. Treatments include both accepted and experimental medications to alter disease course, as well as aggressive pulmonary support and nutritional supplementation. Movement toward an active treatment approach has been facilitated by publication in 1999 of a practice parameter for the care of patients with ALS that clearly spells out the levels of care that these patients need. Currently, only one drug has been clearly demonstrated to delay progression of ALS. Riluzole has been shown in two large, randomized, placebo-controlled trials to prolong survival in patients with ALS by approximately 10%. Its mechanism of action probably is reduction of glutamate-mediated toxicity, predominantly by inhibiting release, although a postsynaptic blockade also may occur. Other drugs that inhibit glutamate transmission are under investigation. Other possible avenues of treatment include reducing oxidative stress. Vitamin E has been shown to be effective in delaying disease onset in the mouse model of ALS discussed previously; for this reason, many patients take large doses of vitamin E. Recently, mitochondrial damage has been shown to be an early event in affected motor neurons; creatine, which has a protective effect on mitochondria, has also been beneficial in the ALS mouse. Clinical trials testing this agent are under way. Other therapeutic options currently being evaluated include cytochrome oxidase inhibitors and caspase inhibitors, both of which have shown promise in the ALS mouse. It is likely that an effective treatment will involve simultaneous treatment with a combination of agents, all acting on different aspects of the degenerative cascade. One avenue of treatment that has not proved useful is the administration of human growth factors. These agents have shown promise in multiple models of motor neuron disease (although not in the transgenic ALS mouse model). However, large therapeutic trials involving human ciliary neurotrophic factor, brain-derived neurotrophic factor, and insulin-derived growth factor have all been either negative or equivocal. Although only one agent has clearly demonstrated efficacy in altering the course of ALS, multiple other therapeutic options exist. Progressive pulmonary compromise is the cause of death in most patients with ALS and the source of significant disability. Noninvasive positive-pressure ventilation can improve patient comfort in many instances and may be life sustaining. However, availability of noninvasive ventilatory support does not obviate decisions regarding permanent assisted ventilation. Although a minority of patients with ALS ultimately choose tracheostomy and permanent ventilatory support, this option should be considered carefully. With appropriate family and financial resources, patients can remain at home while on a ventilator. Before such a course is
embarked upon, extensive education of both patient and caretaker is needed. Family members often do not fully comprehend the burden of such a course of action. However, with appropriate education, maintaining ventilated patients at home can provide an acceptable quality of life. In a recent study of 24 patients who elected home ventilation, 90% reported that they would make the same decision again; approximately 50% of the patients’ care givers said they would choose such an option for themselves should the need arise. Such care is very expensive; in the same study, the average cost of home ventilation for 1 year was about $150,000.
Aggressive nutritional support is also essential; not only does bulbar weakness have the potential to limit nutritional intake, but recent studies indicate that caloric needs of patients with ALS are actually greater. Initial treatment usually consists of dietary modification; ultimately, however, placement of a gastrostomy tube usually is necessary. The timing of this intervention is important; tube placement should occur before malnutrition has developed and before there is significant pulmonary compromise. The morbidity and mortality of gastrostomy tube placement are drastically increased in patients with impaired pulmonary status; the current standard of care dictates that tube placement be considered before a patient’s vital capacity falls below 50% of predicted. Ongoing evaluation of a patient’s ability to communicate is also a necessary part of the care of patients with ALS. Many patients develop dysarthria, leading to mutism at some point in their disease. Speech therapy has been of occasional benefit in such patients; in general, patients with primarily upper motor neuron bulbar symptoms do better with speech therapy than those with lower motor neuron weakness. A trial of speech therapy probably is warranted in all patients with worsening dysarthria. When vocal language can no longer be used, a number of options can be explored, ranging from computerized voice production devices for patients who have remaining upper extremity facility to systems that use eye movements. Early attention to this issue and detailed discussion with patients are crucial because it is much easier to make an appropriate decision about the best assistive device before communication is lost. Physical and occupational therapy and well-designed prosthetic devices can dramatically improve a patient’s functional status. Focal weakness can produce early gait problems, often caused by unilateral or bilateral foot drop. Ankle-foot orthoses can return many patients’ gait to almost normal. In patients with more significant lower extremity weakness, the involvement of a physical therapist with experience in neurologic disorders is essential. Although it may seem trivial, the right kind of cane or an appropriately modified walker can make a major difference in the life of a patient whose livelihood depends on the ability to ambulate. Similarly, disability from focal upper extremity weakness often can be treated with supports, braces, or modified instruments of daily living such as spoons or toothbrushes. A close association with a skilled occupational therapist gives patients assistance that neurologists by themselves cannot give. Spasticity is another symptom that can be treated with available agents. This is obviously more of a problem for patients with prominent upper motor neuron disease; although this is the case for the minority of ALS patients, for some it can be a significant problem. Baclofen is the most commonly used antispasticity drug for other neurologic disorders; however, its benefit is variable in patients with ALS. The major reason for this
Chapter 87
appears to be that dosages high enough to produce reductions in spastic tone also produce significant added weakness in this patient population. Tizanidine alone or in combination with baclofen may be more effective than baclofen alone in some patients. Benzodiazepines are occasionally useful but must be used very carefully in this group of patients already at risk for respiratory decompensation. Dantrolene, the other drug commonly used to treat spasticity, is almost always associated with unacceptable weakness in patients with ALS. An extremely important and overlooked component of the treatment of patients with ALS is attention to the patient’s emotional well-being. ALS is a devastating disease, producing progressive disability and dependence in the absence of intellectual deterioration. Depression in patients with ALS is nearly universal and is at least partially treatable. Patients and family members nearly always benefit from referral to local support groups and often from individual therapy. In addition, pharmacologic treatment often is useful. In the past, most commonly used antidepressant medications were associated with side effects such as fatigue and dry mouth that were particularly distressing to patients with ALS, but the recently developed selective serotonin reuptake inhibitors do not have these side effects and are much faster-acting than older antidepressants.
SUGGESTED READINGS Bed M F Mitochondrial dysfunction in neurodegenerative diseases.
W
Spinal Muscular Atrophy
SSJ
Cookson MR, Shaw PJ: Oxidative stress and motor neuron disease. Brain
Pathol 9:165-186, 1999 Ferrante RJ, Browne SE, Shinobu LA et al: Evidence of increased oxidative damage in both sporadic and familial amyotrophic lateral sclerosis. J Neurochem 69:2064-2074, 1997 Miller RG, Rosenberg JA, Gelinas DF et al: Practice parameter: the care of the patient with amyotrophic lateral sclerosis (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology: ALS Practice Parameters Task Force. Neurology 52:1311-1323, 1999 Moss AH, Casey P, Stocking CB et al: Home ventilation for amyotrophic lateral sclerosis patients: outcomes, costs, and patient, family, and physician attitudes. Neurology 43:438-443, 1993 Munsat T, Andres PL, Finison L et al: The natural history of motoneuron loss in amyotrophic lateral sclerosis. Neurology 3k409-413, 1988 Rosen DR, Siddique T,Patterson D et al: Mutations in Cu/Zn superoxide dismutase gene are associated with familial amyotrophic lateral sclerosis. Nature 362:5942, 1993 Rothstein JD, Martin LJ, K u n d RW Decreased glutamate transport by the brain and spinal cord in amyotrophic lateral sclerosis. N Engl J Med 3261464-1468, 1992
Shaw PJ, Eggett CJ: Molecular factors underlying selective vulnerability of motor neurons to neurodegeneration in amyotrophic lateral sclerosis. J Neurol 247(Suppl 1):117-27, 2000
Shefner J M Motor unit number estimation in human neurological diseases and animal models. Clin Neurophysiol 112:955-964,2001 Tyler HR, Shefner JM: Amyotrophic lateral sclerosis. pp. 169-216. In Vinken P, Bruyn G, Klawans H (eds):Handbook of Clinical Neurology. Vol. 59. Elsevier, New York, 1991
Biochem Biophys Acta 1366:211-223, 1998
87
Spinal Muscular Atrophy Kathryn J. Swoboda, Kathryn N. North, and Linda A. Specht
Spinal muscular atrophy (SMA) is a lower motor neuron disorder characterized by degeneration of the anterior horn cells in the spinal cord and bulbar motor nuclei. The clinical hallmarks of the disorder are symmetric muscle weakness and atrophy of limb muscles with variable bulbar involvement and tremor and supporting electrophysiologic and pathologic evidence of motor denervation. The most common form of the disorder is linked to chromosome 5q13 and inherited in an autosomal recessive fashion. About 96% of patients with a classic presentation have a homozygous deletion of the telomeric copy of the survival motor neuron gene on chromosome 5q. In the Western world, acute SMA is the most common genetic cause of infantile death and is the second most common serious neuromuscular disorder after Duchenne muscular dystrophy. Patients most often present in infancy and early childhood, and the disease is categorized into subtypes based on severity of weakness. Life expectancy is markedly reduced and varies greatly between and within types. Other disorders called SMA in the literature but not linked to 5q are clinically and molecularly heterogeneous. These include an X-linked infantile form of SMA, SMA with severe early diaphrag-
matic involvement (SMA with respiratory distress, or SMARDl), and X-linked spinobulbar muscular atrophy, or Kennedy’s disease. These non-5q-linked SMAs are mentioned briefly.
CLINICAL FEATURES Degeneration of the anterior horn cells in the spinal cord and lower brainstem results in a lower motor neuron pattern of weakness and muscle wasting in the limbs and tongue. The pattern of weakness in the limbs is symmetrical, more proximal than distal, and more severe in the lower limbs. A “piano-playing” tremor of the outstretched hands is prominent in many patients. The muscles of the trunk are involved with intercostal weakness, and bulbar involvement results in atrophy and fasciculation in the tongue. Deep tendon reflexes are decreased or absent, and plantar reflexes, if present, are downgoing. Typically, the diaphragm is spared until late in the disease (in severe forms), and there is no involvement of cardiac or smooth muscle. Clinical exclusion criteria for SMA include the presence of sensory disturbance, intellectual impairment, or sphincter disturbance. A subset of severely affected infants are born with proximal joint contradures
Chapter 87
appears to be that dosages high enough to produce reductions in spastic tone also produce significant added weakness in this patient population. Tizanidine alone or in combination with baclofen may be more effective than baclofen alone in some patients. Benzodiazepines are occasionally useful but must be used very carefully in this group of patients already at risk for respiratory decompensation. Dantrolene, the other drug commonly used to treat spasticity, is almost always associated with unacceptable weakness in patients with ALS. An extremely important and overlooked component of the treatment of patients with ALS is attention to the patient’s emotional well-being. ALS is a devastating disease, producing progressive disability and dependence in the absence of intellectual deterioration. Depression in patients with ALS is nearly universal and is at least partially treatable. Patients and family members nearly always benefit from referral to local support groups and often from individual therapy. In addition, pharmacologic treatment often is useful. In the past, most commonly used antidepressant medications were associated with side effects such as fatigue and dry mouth that were particularly distressing to patients with ALS, but the recently developed selective serotonin reuptake inhibitors do not have these side effects and are much faster-acting than older antidepressants.
SUGGESTED READINGS Bed M F Mitochondrial dysfunction in neurodegenerative diseases.
W
Spinal Muscular Atrophy
SSJ
Cookson MR, Shaw PJ: Oxidative stress and motor neuron disease. Brain
Pathol 9:165-186, 1999 Ferrante RJ, Browne SE, Shinobu LA et al: Evidence of increased oxidative damage in both sporadic and familial amyotrophic lateral sclerosis. J Neurochem 69:2064-2074, 1997 Miller RG, Rosenberg JA, Gelinas DF et al: Practice parameter: the care of the patient with amyotrophic lateral sclerosis (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology: ALS Practice Parameters Task Force. Neurology 52:1311-1323, 1999 Moss AH, Casey P, Stocking CB et al: Home ventilation for amyotrophic lateral sclerosis patients: outcomes, costs, and patient, family, and physician attitudes. Neurology 43:438-443, 1993 Munsat T, Andres PL, Finison L et al: The natural history of motoneuron loss in amyotrophic lateral sclerosis. Neurology 3k409-413, 1988 Rosen DR, Siddique T,Patterson D et al: Mutations in Cu/Zn superoxide dismutase gene are associated with familial amyotrophic lateral sclerosis. Nature 362:5942, 1993 Rothstein JD, Martin LJ, K u n d RW Decreased glutamate transport by the brain and spinal cord in amyotrophic lateral sclerosis. N Engl J Med 3261464-1468, 1992
Shaw PJ, Eggett CJ: Molecular factors underlying selective vulnerability of motor neurons to neurodegeneration in amyotrophic lateral sclerosis. J Neurol 247(Suppl 1):117-27, 2000
Shefner J M Motor unit number estimation in human neurological diseases and animal models. Clin Neurophysiol 112:955-964,2001 Tyler HR, Shefner JM: Amyotrophic lateral sclerosis. pp. 169-216. In Vinken P, Bruyn G, Klawans H (eds):Handbook of Clinical Neurology. Vol. 59. Elsevier, New York, 1991
Biochem Biophys Acta 1366:211-223, 1998
87
Spinal Muscular Atrophy Kathryn J. Swoboda, Kathryn N. North, and Linda A. Specht
Spinal muscular atrophy (SMA) is a lower motor neuron disorder characterized by degeneration of the anterior horn cells in the spinal cord and bulbar motor nuclei. The clinical hallmarks of the disorder are symmetric muscle weakness and atrophy of limb muscles with variable bulbar involvement and tremor and supporting electrophysiologic and pathologic evidence of motor denervation. The most common form of the disorder is linked to chromosome 5q13 and inherited in an autosomal recessive fashion. About 96% of patients with a classic presentation have a homozygous deletion of the telomeric copy of the survival motor neuron gene on chromosome 5q. In the Western world, acute SMA is the most common genetic cause of infantile death and is the second most common serious neuromuscular disorder after Duchenne muscular dystrophy. Patients most often present in infancy and early childhood, and the disease is categorized into subtypes based on severity of weakness. Life expectancy is markedly reduced and varies greatly between and within types. Other disorders called SMA in the literature but not linked to 5q are clinically and molecularly heterogeneous. These include an X-linked infantile form of SMA, SMA with severe early diaphrag-
matic involvement (SMA with respiratory distress, or SMARDl), and X-linked spinobulbar muscular atrophy, or Kennedy’s disease. These non-5q-linked SMAs are mentioned briefly.
CLINICAL FEATURES Degeneration of the anterior horn cells in the spinal cord and lower brainstem results in a lower motor neuron pattern of weakness and muscle wasting in the limbs and tongue. The pattern of weakness in the limbs is symmetrical, more proximal than distal, and more severe in the lower limbs. A “piano-playing” tremor of the outstretched hands is prominent in many patients. The muscles of the trunk are involved with intercostal weakness, and bulbar involvement results in atrophy and fasciculation in the tongue. Deep tendon reflexes are decreased or absent, and plantar reflexes, if present, are downgoing. Typically, the diaphragm is spared until late in the disease (in severe forms), and there is no involvement of cardiac or smooth muscle. Clinical exclusion criteria for SMA include the presence of sensory disturbance, intellectual impairment, or sphincter disturbance. A subset of severely affected infants are born with proximal joint contradures
554
Spinal cord and PeripheralNeuromuscular Disease
Motor Neuron Disease
and ventilator dependency and have documented sensory nerve involvement. Extraocular muscle weakness, marked facial weakness, ptosis, cardiac involvement, and loss of hearing or vision are not associated with 5q SMA (Table 87-1).
CLASSIFICATION AND SUBTYPES Classic Spinal Muscular Atrophy
Childhood-onset SMA usually is classified into three groups on the basis of age of onset and clinical severity (Table 87-2). The acute infantile form (Werdnig-Hoffmann, or type I) presents before 6 months of age. Many infants are normal to examination during the first few months of life, although some are noted to be hypotonic at birth or to have exhibited decreased fetal movements. Children with this form of the disorder never attain the ability to sit. Progression to generalized paralysis of the limbs and trunk is rapid, and bulbar involvement, with fasciculations and wasting of the tongue, is a useful diagnostic sign. Although the infant remains visually alert, feeding difficulties, respiratory failure with aspiration, and recurrent respiratory infections usually lead to death by 2 years of age. An intermediate form of SMA (type 11, or chronic WerdnigHoffmann disease) has its onset between 6 and 18 months of age. These children may be assessed as normal during the first 6 months of life and attain the ability to sit. Subsequent motor development is arrested, and they are unable to stand unassisted. Bulbar dysfunction is less marked, and tongue fasciculation is less common than in type I, but the peripheral tremor may be more marked. As in type I, survival is linked to respiratory function, and death usually is secondary to respiratory infection or progressive restrictive pulmonary disease. Prolonged survival into the third or fourth decade and beyond, with or without the need for artificial ventilation, may occur in this group of patients. The mildest form of childhood-onset SMA (KugelbergWelander, or type 111) usually presents between 18 months and 17 years of age with proximal symmetrical muscle weakness, predominantly affecting the legs. These patients usually, but not always, retain the ability to walk, although joint contractures and scoliosis may become evident. Bulbar function usually is preserved, and these patients survive into adulthood. As in type 11, tremor is common and may be the presenting feature. This form of SMA is H TABU87-1.
Diagnostic Criteria of Spinal Muscular Atrophy
Inclusion Criteria Symmetrical muscle weakness, proximal greater than distal Trunk muscles involved, with poor head and trunk control in severe cases Intercostal weakness but sparing of the diaphragm Evidence of denervation, either clinical (fasciculations or tremor) or laboratory (EMG or muscle biopsy) Exclusion Criteria Clinical Central nervous system dysfunction Arthrogryposis Abnormalities of other organ systems Sensory loss Severe facial or extraocular muscle weakness Hypertonia or hyperreflexia
Laboratory High creatine kinase Aminoaciduria Organic aciduria Hexosaminidase A or B deficiency Monoclonal gammopathy Biopsy evidence of lipid or glycogen storage disease or mitochondrial abnormality Abnormally slow nerve conduction velocitv ~~
(Adapted from Munsat TL Workshop report. International SMA Collaboration. Neuromuscul Disord 1 3 1 , 1990, with permission.)
TABLE 87-2. Classification of Spinal Muscular Atrophy TVDe
Onset
0 (arthrogryposis)
Prenatal
I (acute) I1 (intermediate) 111 (mild) IV (adult)
Missed Milestones
Ane at Death 0-6 months
48 months
Never breathe independently Never sit Never stand
>18 months Adulthood
-
Adult Adult
Birth-6 months
Usually IS%) than proximal CMAP amdkude. evaluate for abnormal temporal dispersion or partial condudi&n b l o c i a. Measure CMAP duration (distal and proximal) to identify abnormal dispersion. b. Evaluate CMAP amplitude and duration over short segments (few millimeters) to identify partial conduction block. c If capability exists, measure CMAP negative phase area (distal and proximal). Evaluate additional nerve if findings are equivocal. Definite abnormalities should result in a. Evaluation of contralateral extremity. b. Evaluation of specific suspected abnormality.
Needle Examination 1. Examine anterior tibialis, medial gastrocnemius, abductor hallucis, vas-
tus lateralis, biceps brachii, first dorsal interosseous (hand), and lumbar paraspinal muscles. 2. Any abnormality should be confirmed by examination of at least one contralateral muscle, lookina for symmetry. ’Muscles in parentheses indicate recording site for conduction studies. bAil F wave latency measurements are for distal stimulation sites. Record as absent if no response alter 15 stimulations. Abbrevioton: CMAP, compound muscle action potential. Modied from Aibers MI,Donofrio PD, McGonagle TK: Sequential electrodiagnostic abnormalities in acute inflammatory demyelinating polyradiculoneuropathy.Muscle Nerve 8:528-539, 1985, with permission.
580
Spinal Cord and Peripheral Neuromuscular Disease W
-JL-
Diseases of Peripheral Nerve
-n-
A
Dlstal to proxlmal: Amplltude -5% Duratlon + l o % Area 0%
Ak!+5mv Elbow
Dlstal to proxlmal: Amplltude -62% Duratlon +55% Area -30%
FIG. 92-1. Motor nerve conduction studies from a normal subject (/eft) and from a patient with an acquired inflammatory demyelinating polyneuropathy (right), demonstrating abnormal temporal dispersion or partial conduction block.
of findings reported reflect, in part, temporal changes associated with cumulative demyelination and axonal degeneration. The evaluation is similar to that of any polyneuropathy. The goal is to document the presence of a peripheral localization and to identify the predominant pathophysiology. This entails evaluation of sensory and motor nerves in the upper and lower extremities, including proximal stimulation of motor nerves and F wave studies. A representative protocol is shown in Table 92-1. The hallmark of all acquired demyelinating neuropathies is evidence suggestive of multifocal demyelination. Conduction velocity slowing greater than can be explained by axonal loss is consistent with demyelination, but abnormal dispersion of motor responses and unequivocal conduction block are the cardinal features of acquired demyelination (Fig. 92-1). The earliest abnormalities include absent F and H waves and decreased motor unit recruitment. Only during subsequent examinations does evidence of segmental conduction block and conduction slowing become apparent. Some patients with normal conduction velocities have prolonged distal latencies, whereas other patients have normal distal latencies and shorter conduction velocities. These different presentations reflect the site of major abnormality, and most patients presenting with only prolonged distal latencies subsequently develop partial conduction block, abnormal temporal dispersion, and reduced conduction velocities. The electrodiagnostic features of acquired demyelination are imprecise and depend on identification of findings that cannot be explained by axonal degeneration alone (Table 92-2). During the first two weeks of illness, about 50% of patients with AIDP fulfill strict criteria for demyelination, compared with almost 85% by the third week of illness. During these first few weeks, an unusual pattern of abnormal median but normal sural sensory responses occurs in almost 50% of patients with AIDP. The extreme pattern of an absent median but present sural response in the appropriate clinical setting occurs almost exclusively in AIDP and is unusual in other types of generalized neuropathy. A small percentage of patients with otherwise typical AIDP never fulfill criteria for demyelination. Some of these patients are thought to have an axonal form of AIDP. The needle electromyography (EMG) examination has a limited role in evaluating patients with AIDP. The occasional demonstration of myokymic discharges during the first few weeks of illness may be helpful in establishing the diagnosis, and ultimate demonstration of profuse fibrillation potentials may be helpful in defining the magnitude and extent of denervation in establishing prognosis.
TME 92-2. Electrodiagnostic Criteria Suggestive of Chronic Acquired Demyelination Evaluation should satisfy at least three of the following in motor nerves (exceptions explained in footnotes): Conduction velocity less than 75% of the lower limit of normal (two or more nerves)a Distal latency exceeding 130% of upper limit of normal (two or more nerves)” Evidence of unequivocal temporal dispersion (increase in negative component duration exceeding 15% for proximal versus distal stimulation) or a proximal to distal amplitude ratio less than 0.7 (one or more nerves)boc F wave latency exceeding 125% of upper limit of normal (one or more nerves).”.” Txcluding isolated ulnar or peroneal nerve abnormalities at the elbow or knee, respectively. bExcludingisolated median nerve abnormality at the wrist ‘Excluding the presence of anomalous innervation (e.g., median to ulnar nerve crossover). Modified from Alben JW,Donofrio PD, McConagle TK: Sequential electrodiagnostic abnormalities in acute demyelinating polyradiculoneuropathy.Muscle Nerve 1985, 8:528-539, with permission.
Other Laboratory Features Other than CSF and electrophysiologic evaluations, laboratory studies have limited use in AIDP. Abnormal white blood count and liver function tests are common, but these are nonspecific findings thought to reflect an antecedent illness. Occasionally, elevated antibody titers to viral antigens help identify a specific antecedent event, but these findings have no therapeutic implications. The most important role of laboratory studies is in identifymg a systemic problem mimicking AIDP. For example, any patient with acute neuropathy and abnormal liver function studies, profound sensory loss, and unexplained leukopenia should be evaluated for arsenic intoxication (24-hour urine heavy metal screen and fingernail or hair arsenic analyses). Porphyric neuropathy also should be considered in patients with suspected AIDP, particularly if there is limited electrophysiologic evidence of demyelination, a history of recurrent episodes, or the triad of abdominal pain, psychosis, and polyneuropathy. CSF pleocytosis, although compatible with AIDP, should suggest an alternative diagnosis such as HIV-associated neuropathy. There is an association of otherwise typical AIDP with systemic lupus erythematosus. Serologic evaluation for collagen vascular disease or vasculitis therefore is indicated in the appropriate clinical setting. Some patients with the Fisher’s syndrome have an IgG antibody to GQlb ganglioside. Surd nerve biopsy may identify
Chapter 92 W
an underlying vasculitis or other systemic illness, but biopsy generally is not indicated. Treatment
Patients with AIDP almost never receive their primary treatment in the outpatient setting, but the most important initial treatment decision of whether to admit the patient occurs in the office or emergency department. The diagnosis often is difficult to establish at onset, and the initial symptoms can be nonspecific, with many potential causes. Most neurologists recall patients who were thought to have early AIDP but who resolved without progression. Whether these patients had a mild form of AIDP is unknown. Regardless, the decision to follow such patients in the outpatient setting is not straightforward. Patients with mild sensory symptoms but no signs often are observed as outpatients, as are patients who have minor signs and who appear stable and are not clearly progressing. Factors that influence the decision to admit the patient to the hospital include the duration, magnitude, distribution, and progression of symptoms or signs, as well as the presence of coexisting medical or related problems that interfere with the ability to provide reliable outpatient observation. Patients with suspected AIDP who have respiratory symptoms or a weak cough must be admitted. The medical management of AIDP is beyond the scope of this chapter. However, a few comments about treatment are important even in an outpatient-based context. The advent of respiratory intensive care units dramatically reduced mortality in AIDP to its current rate of approximately 2% to 5%. Therefore, all patients must be observed for respiratory deterioration, and pulmonary therapy is important in limiting atelectasis. Frequent monitoring of the volitional cough and the forced vital capacity (FVC) is important, and the decision of whether to intubate depends on the extent and rate of respiratory deterioration. Intubation is indicated if the FVC falls below 15 mL/kg, but a rapid decline of FVC should result in elective intubation independent of the absolute measurement, as should aspiration with poor tracheal toilet, pulmonary infection with shunting, or early signs of respiratory fatigue. Arterial blood gases are poor indicators of impending respiratory failure, and increasing restlessness, tachycardia, tachypnea, and sleepiness often precede blood gas changes. A low Po, and lower than normal Pco, may indicate early atelectasis with shunting. Hypercapnia generally precedes hypoxia but is a late finding of respiratory failure and a dangerous criterion for elective intubation. Most deaths among patients with AIDP involve medical complications of respiratory paralysis, but about 50% are sudden and presumably reflect cardiac dysrhythmias or hypotension. Although dysautonomia is not directly related to the extent of weakness, catastrophic cardiac dysrhythmia or blood pressure lability is unusual in patients with mild functional impairment. Minor cardiac dysrhythmias occur in about 20% of hospitalized patients, but arrhythmias sufficiently severe to affect blood pressure or necessitate medication occur in about 5% of patients. Most commonly, these are second- or third-degree atrioventricular blocks, for which a temporary pacemaker insertion is needed. Autonomic instability resulting in hypotension or new hypertension occurs in 10% to 15% of patients with AIDP. Hypotension is best managed by the rapid infusion of fluid,and sympathomimetics usually are not needed. Most agree that hypertension should not be treated unless severe and persistent. Corticosteroids are of unproven efficacy in AIDP, and their use
Inflammatory Demyelinating Polyneuropathies
581
is controversial. The few controlled studies that evaluated their use either were inconclusive or concluded that prednisone slowed recovery. The demonstrated importance of humeral factors in AIDP suggested that therapeutic plasma exchange (PE) might alter the course of illness. Several multicenter randomized studies, including the North American study of plasmapheresis and acute Guillain-Barre syndrome, confirmed the clinical, statistical, and economic efficacy of PE in established AIDP when initiated within the first few weeks after onset. In the North American study, patients who received PE underwent a series of three to five 40- to 50-mLlkg exchanges in 7 to 14 days. PE was not effective for all patients. However, overall the time by which 50% of patients reached independent ambulation was shortened by about 1 month for patients who received PE compared with remaining patients. For respirator-dependent patients who received PE, the median time of respiratory support was 11 days shorter and the time to unassisted ambulation was more than 2 months shorter than in the control group, without a significant increase in the nature or frequency of complications. Relapse occurred in only 4 (1.6%) of 245 patients in the North American study, 2 in each study arm. As PE became the accepted standard treatment, with the initial PE initiated soon after the diagnosis of AIDP was established, some centers observed an unexpectedly high relapse rate shortly after the course of PE was completed. Although unproven, this was thought to reflect premature discontinuation of treatment, before the acute monophasic illness had run its course. Therefore, interval PE sometimes is continued through the fourth or fifth week of illness to reduce the likelihood of limited relapse (Table 92-3). Although this period of treatment seems logical based on the known temporal progression of untreated AIDP, controlled clinical trials have not supported the need for additional PE treatment. A randomized trial comparing intravenous immunoglobulin ( M g ) with PE suggested that M g is at least as effective as PE in AIDP. Many neurologists believe that M g is an appropriate alternative first-choice treatment of AIDP. For some patients, such as those with poor venous access who need central lines for PE, M g offers a particular advantage. Regardless of the timing or form of treatment, it is establishedthat treatment with either PE or M g does not convert AIDP to a more chronic or relapsing form of neuropathy.
rn TABLE92-3.Suggested Therapeutic Plasma Exchange Schedule in AIDPa Interval from onset of neurologic symptoms 4 weeks: no exchange unless progressing Interval from onset to completion of PE motor polyneuropathy Polyneuropathy Motor neuron disease
SD
Acidic glycolipids Cangliosides GM, and GD,b Chondroitin sulfate C Intermediate filaments Neurofilarnent Sulfatide
? SD, possible AD
Sensory polyneuropathy Polyneuropathy Polyneuropathy Sensorv polvneuropathv
AD SD AD AD
Abbreviations: AD, axonal degeneration; MAG, myelin-associatedglycoprotein;SD, segmental demyelination. Adapted from Steck AJ, Murray N, Dellagi K et al: Peripheral neuropathy associated with monoclonal IgM autoantibody. Ann Neurol45:711, 1988, with permission.
failure caused by amyloid cardiomyopathy, chronic diarrhea with wasting caused by amyloid infiltration of the gut wall, and autonomic neuropathy with prominent orthostatic hypotension. General laboratory studies reflect the medical syndromes, with proteinuria occurring in a high percentage, elevated erythrocyte sedimentation rate in about one half, and a mild increase in benign-appearing plasma cells in bone marrow in many. Up to 90% have an M-protein in serum or a monoclonal light chain in urine when thoroughly screened with serum and urine immunofixation. The patients lacking an M-protein, if the disease is not inherited, are called nonsecretory, although immunocytologic studies of their tissue disclose that the amyloid derives from single (monoclonal) light chains. Presumably, the serum concentration is too low in these patients to allow detection. The light chains are deposited in tissue, where they are digested by macrophages with the production of amyloid fibrils, which are then insoluble. The polyneuropathy has been well characterized. Sensory symptoms typically are most prominent and the earliest to appear. Almost all such patients present with numbness of the hands and legs, and complaints such as burning, aching, stabbing, and shooting pains are most common. In more than one half of patients, cutaneous sensations (light touch, pain, temperature) are more often and more severely affected than discriminative sensations (vibration and position sense). Occasional patients (about 20%) present with the typical symptoms of carpal tunnel syndrome before distal neuropathy symptoms appear, caused by amyloid infiltration of the flexor retinaculum of the wrist. Rare patients present with symptoms of autonomic dysfunction without symptoms of somatic sensory dysfunction. Symptoms and signs of weakness generally follow but usually are less prominent than the sensory findings. Exceptions are rare patients with amyloid infiltrative myopathy with proximal muscle weakness and patients with malignant plasma cell dyscrasias, such as myeloma, who may present with compressive radiculopathies that can mimic mononeuropathies or plexopathies. The findings tend to be symmetrical and predominant distally, with gradual proximal spread. Most patients soon complain of autonomic dysfunction with orthostatic lightheadedness and syncope, bowel and bladder disturbances, impotence, and sweating disturbances. Hypoactive pupils and orthostatic blood pressure drop with a fixed heart rate are the most easily detected autonomic signs at the bedside. Electrophysiologic studies (see Table 96-5) confirm the presence of a distal axonopathy that is maximal in the legs. Motor conduction velocities in the demyelinating range (less than 60% of the mean normal for that nerve) occur rarely, and then only in “unreliable” nerves, where the evoked compound muscle action potential is very low in amplitude. Sensory nerve action potentials usually are unobtainable. Often, there is evidence of disproportionate median nerve conduction slowing across the wrist because
TABLE 96-5. Major Electrodiagnostic Features of PN Associated with PCD Type of PN MGUS-lgM MGUS-lgC, MCUS-lgA OSM PSA
MM
Demyelinating
Axonal
+++ ++ +++ +
+ ++ + +++ ++
CTS
-
-
++ +
Pure Sensory
++ + + +
Other
+ + +++a
++b
aAutonomicinvolvement. bRoot involvementand polyradiculopathiessuperimposedon PN. Abbreviations: CTS, carpal tunnel syndrome superimposedon polyneuropathy;MGUS, monoclonal gammopathy of undetermined significance; MM, multiple myeloma; OSM, osteosclerotic myeloma; PCD, plasma cell dyscrasia; PN, polyneuropathy;PSA, primary systemic amyloidosis. From Kelly JJ Jr: Peripheral neuropathiesassociated with monoclonal proteins: a clinical review. Muscle Nerve 8:138, 1985, with permission.
Chapter 96 H TABU 96-6.
Medical Syndromes in Amyloid Polyneuropathy Flequencv (%l
Syndrome
Orthostatic hypotension Nephrotic syndrome Cardiac failure Malabsorption
42 23 23 16
From Kelly JJ Jr, Kyle RA, OBrien PC et al: The natural history of peripheral neuropathy in primary systemic amyloidosis. Ann Neurol 5:271, 1979, with permission.
W TABU96-7.
Results of Biopsy in Primary Amyloidosis with Neuropathy
Site
Rectum Kidney Liver Small intestine Bone marrow Sural nerve Other (skin. ninniva)
No. Patients 25 4 2 2 21 10 2
DysproteinemicPolyneuropathy
607
practical. There may be a role for frequent immunoabsorption treatment in the future. However, the nephropathy caused by light-chain deposition has been shown to at least partially reverse with a combination of melphalan and prednisone. Thus, these patients typically progress inexorably with increasing numbness and pain, autonomic failure, and weakness with added organ failure. Death usually occurs in 2 to 4 years from time of diagnosis and generally is caused by major organ failure, cardiac most commonly. Patients with pure neuropathies without significant organ failure survive longer.
MULTIPLE MYELOMA NEUROPATHY
Positive (%I
88 75 100 100 33 100 100
From Kelly JJ Jr, Kyle RA, O'Brien PC et al: The natural history of peripheral neuropathy in primary systemic amyloidosis. Ann Neurol 5:271, 1979, with permission.
of carpal tunnel syndrome, which can suggest the diagnosis. Needle EMG shows the changes expected of a distal axonopathy, with abundant signs of distal denervation and reinnervation. Cerebrospinal fluid usually is acellular and with only mild, nonspecific elevations of protein levels, generally in the range of 50 to 70 mg/dL. Diagnosis depends on the discovery of amyloid in tissue. Sural nerve biopsy is very useful in detecting amyloid in most cases, although sometimes it must be sought through multiple sections. Amorphous deposits of amyloid on Congo red or cresyl violet stains typically appear in the perivascular regions of the epineurium or occasionally in the endoneurium. However, amyloid is classically defined by its appearance under polarized light when the Congo red-stained deposits emit an apple-green birefringence. Electron microscopy can also be used to identify the characteristic fibrils. In some hands, immunofluorescent staining for monoclonal light-chain fragments is useful, but it is technically difficult. Because amyloid can be absent in any single tissue, even in sural nerve biopsy specimens despite neuropathy, I generally suggest biopsy of more than one tissue. Other useful tissues to biopsy (Table 96-7) include rectum, fat pad, and other affected organs such as kidney. Teased fiber studies show predominantly axonal degeneration. However, the cause of nerve fiber damage is not always readily apparent in all cases. In some instances, marked axonal denervation can be evident with minimal amyloid infiltration. This has led to many theories of the pathogenesis of the neuropathy, including vascular and pressure changes by the amyloid deposits. However, direct toxic effects of the amyloid fibrils on nerve fibers and dorsal root ganglion cells seem more likely. Treatment is problematic. The amyloid fibrils are insoluble once deposited in tissue. Thus, improvement is unlikely even if amyloid deposition is halted. In addition, the neuropathy has resisted all attempts to halt its progression, even with aggressive treatment with combinations of anti-inflammatory medications such as steroids, alkylating agents such as melphalan and cyclophosphamide,and other chemotherapeuticdrugs designed to slow production of the light chains. Prolonged plasmapheresis designed to lower the light-chain concentration in serum is not
Multiple myeloma is a malignant plasma cell dyscrasia with high serum and urinary concentrations of M-proteins, infiltration of bone marrow by malignant plasma cells, and multiple bony lesions caused by plasma cell infiltration. Most neurologic complications are caused by secondary effects of the tumor (hypercalcemia, infections) or by malignant infiltration of nerve roots or secondary compression of spinal cord or nerve roots caused by vertebral fractures. Polyneuropathies are uncommon. They occur in only a few percent of patients with multiple myeloma and are diverse in nature, similar to the polyneuropathies associated with other malignancies. The exception is osteosclerotic myeloma, discussed separately later in this chapter. Neuropathies associated with typical lytic multiple myeloma include distal sensorimotor axonopathy, a CIDP-like picture, and a sensory neuropathy resembling the carcinomatous sensory neuropathy. In addition, these patients may also develop plasma cell dyscrasia polyneuropathy caused by deposition of light-chain fragments in tissue. In one series, 20% of neuropathies associated with multiple myeloma were caused by plasma cell dyscrasia. Superimposed root involvement may mistakenly suggest a picture of mononeuritis multiplex, which we have not seen in our patients with amyloidosis with the exception of carpal tunnel syndromes. The root and cord compressive syndromes should be managed by conventional means, but like nonmalignant primary systemic amyloidosis, the amyloid neuropathy does not respond to chemotherapy.
OSTEOSCLEROTIC MYELOMA POLYNEUROPATHY AND RELATED SYNDROMES Osteosclerotic myeloma is a rare and more benign variant of multiple myeloma. Less than 3% of untreated patients with myeloma have sclerotic bony lesions. In addition, whereas polyneuropathy is rare with typical multiple myeloma, it is common with osteosclerotic myeloma, occurring in 50% or more of reported cases. Also, patients with osteosclerotic myeloma usually are not systemically ill and usually present because of the neuropathy or other remote effects of the malignancy rather than as a direct effect of the malignancy, as usually occurs in multiple myeloma. Anemia, hypercalcemia, and renal insufficiency are uncommon in osteosclerotic myeloma, bone marrows are rarely infiltrated with malignant plasma cells, and the serum M-protein concentrations are low. Finally, the course of osteosclerotic myeloma is indolent, and these patients have prolonged survivals even without treatment. Thus, there is something singular about the syndrome of osteosclerotic myeloma and its paraneoplastic accompaniments. The syndrome can be difficult to diagnose even by experienced physicians. The polyneuropathy accompanying osteosclerotic myeloma is
608
Spinal Cord and PeripheralNeuromu5cubr Disease
Diseases of Peripheral Nerve
distinctive and homogeneous. Deficits are mainly motor and slowly progressive, without sudden changes in severity or tempo of progression. Patients present with the onset of weakness, mostly in distal limbs initially, with gradual proximal spread accompanied by reflex loss. Sensory loss typically is less striking and tends to disproportionatelyaffect the larger sensory fibers, with greater loss of discriminative sensation than cutaneous sensation. Pain and autonomic dysfunction, with the exception of impotence (actually caused by endocrine dysfunction), is very uncommon. Nerves often are palpably thickened. The deficit usually is very symmetrical and the tempo of progression very slow, often over months to years. In keeping with the nature of the underlying disorder, general laboratory studies usually are uninformative. The best clue to the diagnosis is the presence of a serum M-protein, which is present in about 75% to 80% of patients. However, the M-protein may be very small and obscured by the normal serum protein components in the electrophoresis, emphasizing the importance of immunoelectrophoresis or immunofixation in all patients with idiopathic polyneuropathy. The M-protein is characteristicallyIgG or IgA (never IgM), h light chain (rarely K), and rarely present in the urine, in contrast to multiple myeloma. Neurodiagnostic studies are helpful but nonspecific. Nerve biopsy studies disclose a reduced concentration of myelinated fibers with changes of mixed demyelination and axonal degeneration. There may be mild foci of mononuclear cells in the epineurium surrounding blood vessels. These changes are nonspecific and characteristic of a number of neuropathies, including CIDP and diabetic polyneuropathy. The EMG (Table 96-5) reveals a mixed axonal and demyelinating picture that again is nonspecific but helpful in categorizing the neuropathy into the group with clear-cut demyelinating features and thus making it more likely to be diagnosable. Cerebrospinal fluid typically reveals a normal cell count but a very high protein concentration, generally higher than 100 mg/dL and sometimes as high as several hundred milligrams per deciliter. Because all these findings are nonspecific, the diagnosis often hinges on the discovery of the characteristic bony lesions and subsequent bone biopsy. The osteosclerotic lesions may be solitary or multiple. They tend to affect the axial skeleton and very proximal long bones but spare the distal long bones and skull. They may be pure sclerotic or mixed sclerotic and lytic. Radioactive bone scans, although more sensitive than radiographs as a rule in detecting bony metastases, are not as sensitive as radiographs in detecting osteosclerotic myeloma lesions, probably because of the indolent nature of plasmacytomas. Therefore, all patients with unexplained polyneuropathies that fit the clinical profile as described earlier should be screened with a radiographic skeletal survey. On occasion, these lesions are misinterpreted by radiologists who are unfamiliar with their appearance and significance. Three of our patients were believed to have benign osteosclerotic lesions (fibrous dysplasia in a rib in two and a vertebral hemangioma in one) with negative radionuclide bone scans. We insisted on biopsy because of the clinical picture, and the presence of a serum M-protein and plasmacytomas was revealed, leading to effective treatment. ThFrefore, if there is any question of the significance of a bony lesion in a patient with a suggestive clinical picture, the radiographs should be reviewed by the neurologist with the radiologist, and the lesion should be biopsied if doubt remains. Open biopsy generally is preferable to needle biopsy, in our experience. The diagnosis of this disorder is of more than academic interest because these patients may be helped by tumoricidal treatment. Patients with solitary lesions do best. Radiotherapy in tumoricidal
dosages to the lesion results in elimination of the M-protein from the serum and gradual recovery of the neuropathy over the ensuing months in most patients. However, these patients should continue to be followed because they tend to relapse with the development of new lesions months to years later. This is usually heralded by the return of the neuropathy and other symptoms and the reappearance of the serum M-protein. Patients with multiple lesions are more difficult to treat. Radiotherapy generally is not an option. In some cases, aggressive chemotherapy can help these patients, but in general the outcome is not as favorable as for solitary lesions. Treatment usually includes large dosages of steroids and alkylating agents. Treatments that usually are effective in autoimmune inflammatory neuropathies, such as steroids alone or azathioprine, usually are ineffective in these patients. The cause of the polyneuropathy is not known, but most theories of pathogenesis have focused on some secretory product of the tumor, most likely the M-protein itself and specifically some component of the Alight chain. However, there is little evidence that the M-protein plays a direct role in the neuropathy or the systemic symptoms. Other secretory products of these tumors have recently been implicated, including cytokines and vascular endothelial growth factor. The pathogenesis of nerve damage in this disorder and whether it is an axonopathy or a primary demyelinating disorder remain unresolved at this time. This disorder is also of interest because many of these patients develop a multiple-system syndrome that goes by a variety of names, including POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes), or Crow-Fukase syndrome. In addition to polyneuropathy, these patients have other features (Table 96-8) suggesting the presence of an underlying endocrinopathy or even malignancy. The reason for the endocrinopathy is unclear. Limited data suggest a disturbance of the hypothalamic-pituitary axis rather than primary end-organ failure, possibly caused by antibody activity against pituitary tissue. The organomegaly usually is nonspecific pathologically. Biopsy of affected lymph nodes generally discloses hyperplastic changes, sometimes resembling the pathologic findings in the syndrome of angiofollicular lymph node hyperplasia (Castleman’s disease), which is a benign localized or generalized hyperplastic lymph node syndrome of unknown cause. Of interest, patients with generalized angiofollicular lymph node hyperplasia without bony lesions may also have the manifestations of Crow-Fukase syndrome associated with serum M-proteins or polyclonal gammopathies. Thus, as discussed in the preceding paragraph, the main pathogenetic determinant of these syndromes probably is the presence of a serum product secreted by the tumor. The term POEMS syndrome for these cases is not entirely accurate and focuses attention on a small number of affected patients to the exclusion of others. For example, of the patients with osteosclerotic myeloma polyneuropathy, most have features other than neuropathy that are fragments of a multiple systemic disorder, but only a few would qualify for the POEMS diagnosis (Table 96-8). Thus, we prefer the term Crow-Fukase syndrome when referring to patients with polyneuropathy and multisystemic disorder, as suggested by Nakanishi et al.
MISCELLANEOUS SYNDROMES WaldensMm’s Macroglobulinemla It is sometimes difficult to separate Waldenstrom’s macroglobulinemia from I@-MGUS, and the latter may evolve into Waldenstrom’s macroglobulinemia over time. Thus, similar poly-
Chapter 96 W
609
Dysproteinemic Polyneuropathy
TAW 96-8. Non-neurologicAbnormalities in 16 Patients with Osteosclerotic Myeloma and Polyneuropathy PAtlEhl
Abnormality
1
2
3
4
5
6
7
8
NUMBER 9
10
11
Cynecomastia + Hepatomegaly + + + + Splenomegaly + + Hyperpigment + + + Edema + + + Lymphadenopathy + + Papilledema + + + Digit clubbing + + White nails Hypertrichosis + + Atrophic testes + Impotence + + + + Polycythemia + + + Leucocytosis + + + + + + Thrombocythemia 4Low plasma testosterone + + + High estrogen + + Low thyroxine + Hyperglycemia + From Kelly JJ Jr, Kyle RA, Miles JM et al: Osteoxlerotic myeloma and peripheral neuropathy. Neurology 33:202,1983, with permission.
neuropathy syndromes occur. The most common polyneuropathy probably is that associated with anti-MAG antibodies. This syndrome has the same features and clinical course as IgM-MGUS. Other patients may have either a CIDP-like picture, a distal ,aonal neuropathy, typical amyloid polyneuropathy, or even the sensory neuronopathy syndrome usually seen with small cell cancer of the lung.
Cryogiobuiinemia This disorder usually is divided into three types. In type 1, the M-protein itself is a cryoglobulin in the setting of a plasma cell disorder. In type 2, the cryoglobulin is a mixture of an M-protein of IgM type with rheumatoid factor activity against polyclonal immunoglobulins, usually occurring in the setting of a lymphoproliferative disorder. Type 3 occurs in the setting of a collagen vascular or other chronic inflammatory disease, and the cryoglobulin consists of polyclonal immunoglobulins. The polyneuropathy in all these syndromes is painful, symmetrical or asymmetrical, and sensorimotor and axonal in nature. Purpura occurs in distal limbs in a high percentage of patients, and the neuropathy generally is considered to be caused by a vasculopathy or vasculitis of skin and vasa nervorum. Lymphoma, Leukemia, and Cancer
These disorders can be associated with M-protein and polyneuropathy. In lymphoma with IgM M-protein, the IgM may have anti-MAG activity with the usual clinical and pathologic features. Other syndromes without clear antinerve activity in the M-protein fraction may respond to ablation of the malignancy. Still others have an unclear relation to the malignancy and show little response to tumoricidal treatment or to lowering of the M-protein concentration in serum. CONCLUSION
The field of plasma cell dyscrasiasand neuromuscular diseases has been a fruitful area for active research since the mid-1980s. It is
12
13
14
15
+ + +
+ +
+ -k
+ + + + + + +
16
+ -k
+ +
+ + + + +
+ +
very important to recognize patients with these diseases because treatment may lead to remission. Also, careful study of these patients may lead to a better understanding of the pathogenesis of polyneuropathies and possibly motor neuron disease. This may in turn lead to effective treatment for conditions for which there are now no effective treatments. Therefore, despite their infrequency, increased recognition of these disorders will continue to be a high priority for both peripheral nerve specialists and for general neurologists.
SUGGESTED READINGS Kelly JJ Jr: Peripheral neuropathies associatedwith monoclonal proteins: a clinical review. Muscle Nerve 8:138, 1985 Kelly JJ Jr, Adelman LS, Berkman E et ak Polyneuropathiesassociatedwith IgM monoclonal gammopathies. Arch Neurol45:1355, 1988 Kelly JJ Jr, Kyle RA, Latov N Polyneuropathies Associated with Plasma Cell Dyscrasias. Martinus-Nijhoff, Boston, 1987 Kelly JJ Jr, Kyle R4, Miles JM et ak Osteosclerotic myeloma and peripheral neuropathy. Neurology 33:202, 1983 Kelly JJ Jr, Kyle RA, Miles JM et al: The spectrum of peripheral neuropathy in myeloma. Neurology 31:24, 1981 Kelly JJ Jr, Kyle RA, OBrien PC et ak The natural history of peripheral neuropathy in primary systemic amyloidosis. Ann Neurol 5:271, 1979 Kelly JJ Jr, Kyle RA, OBrien PC et al: Prevalence of monoclonal protein in peripheral neuropathy. Neurology 31:1480, 1981 Kyle RA: Plasma cell dyscrasias. p. 1-35. In Spitell JA Jr (ed): Clinical Medicine. Harper & Row, Philadelphia, 1981 Latov NR, Hays AF', Sherman WH: Peripheral neuropathy and anti-MAG antibodies. Crit Rev Neurobiol 3:301, 1988 Latov N, Sherman WH, Nemni R et ak Plasma cell dyscrasia and peripheral neuropathy with a monoclonal antibody to peripheral nerve myelin. N Engl J Med 303:618, 1980 Nakanishi T, Sobue I, Toyokura Y et ak The Crow-Fukase syndrome: a study of 102 cases in Japan. Neurology 34:712, 1984 Steck AJ, Murray N, Dellagi K et al: Peripheral neuropathy associated with monoclonal IgM autoantibody. Ann Neurol 45:711, 1988 Suarez GA, Kelly JJ Jr: Polyneuropathy associated with monoclonal gammopathy of undetermined significance: further evidence that IgM-MGUS neuropathies are different than IgG-MGUS. Neurology 43:1377, 1993
610
97
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
NeuroDathies in Connective Tissue Diseases Richard K. Olney
Peripheral neuropathies of several types develop in the clinical context of known diffuse connective tissue diseases. Also, certain presentations of peripheral neuropathy raise the distinct concern that the neuropathy may be the initial manifestation of a previously unsuspected connective tissue disease. To facilitate the recognition of these latter neuropathies, the first section of this chapter reviews each type of neuropathy and comments on the known or possibly unsuspected connective tissue diseases that may be associated. To facilitate recognition of neuropathy in a patient with a known connective tissue disease, the second section reviews certain diffuse connective tissue diseases and comments on their associated neuropathies. ~~~
PERIPHERAL NEUROPATHIES ASSOCIATED WITH CONNECTIVE TISSUE DISEASES The peripheral neuropathies that are associated most closely with diffuse connective tissue diseases are as follows: Vasculitic neuropathy Distal symmetrical axonal polyneuropathy Trigeminal sensory neuropathy Sensory neuronopathy Entrapment or compression neuropathy Among these neuropathies, the diagnosis and initiation of treatment is most important to accomplish in a timely manner for vasculitic neuropathy because it is the most rapidly evolving and potentially fatal, so its diagnosis is particularly emphasized. Vasculitic Neuropathy
Vasculitic neuropathy is defined by the pathogenetic mechanism that produces injury to the nerve fibers: Inflammatory occlusion of blood vessels produces ischemic infarction of one or more nerves. The probability of vasculitic neuropathy usually is suspected clinically when it presents as a mononeuropathy multiplex in a patient with a known connective tissue disease. However, the possibility of vasculitic neuropathy is also important to consider in many other patients. This neuropathy may be the initial manifestation of connective tissue disease, particularly polyarteritis nodosa. Furthermore, vasculitic neuropathy often presents as a generalized polyneuropathy with little or no asymmetry rather than as a mononeuropathy multiplex. Thus, the possibility of vasculitic neuropathy must be considered in many patients with neuropathy of undefined cause, especially in those patients in whom symptoms and signs have developed with asymmetry or without following a length-dependent distribution (this distribution is typical for distal symmetrical axonal polyneuropathy and is discussed further under that heading) or in whom functionally significant deficits have developed rapidly (that is, over weeks or months). In other words, the possibility of vasculitic neuropathy must be considered in many patients with neuropathy of undefined cause if there are clinical features that are atypical for the more common distal symmetrical axonal polyneuropathy.
When vasculitis produces acute ischemia of a nerve, the patient usually experiences an immediate deep aching pain in a poorly localized but proximal distribution in the affected limb. Several hours to several days after this proximal deep aching pain, the patient develops a burning pain in the cutaneous distribution of the affected nerve. In patients with less acutely evolving vasculitic neuropathy, the proximal deep aching pain may be overshadowed by a more prominent distal burning pain that develops over days or several weeks. On neurologic examination, most patients have weakness and abnormal sensation for pain and temperature, whereas a minority of patients have impairment of vibration and position sense. This sensory loss and weakness typically develop over several hours to several days in the distribution of the affected nerve in the acutely evolving cases or over days to weeks in a more confluent distal distribution in the more slowly evolving cases. In patients who present with the more obvious mononeuropathy multiplex, some nerves are more predisposed to involvement than others. The peroneal nerve is the most commonly affected by vasculitis, and the ulnar nerve is the most commonly involved in the upper limb. The nerve infarctions typically are located at “watershed” zones of poor perfusion, which are at the midthigh level for the peroneal division of the sciatic nerve and at the mid-upper arm level for the ulnar nerve. If affected, the tibial and median nerves usually are also infarcted at these same levels. After eliciting the patient history and conducting the physical examination, the first step in the diagnostic workup is electrodiagnostic evaluation. The electromyographic (EMG) and nerve conduction studies assess the severity and pathophysiologic basis of the clinical symptoms and signs. In vasculitic neuropathy, acute axon loss is the predominant pathophysiology identified. Thus, EMG studies reveal reduced recruitment of motor unit potentials that parallels the clinical weakness, and fibrillation potentials are seen in affected muscles 1 to 4 weeks after onset of weakness. Nerve conduction studies document decreased amplitude of sensory nerve and compound muscle action potentials, with normal or mildly reduced conduction velocities. In patients with clinically obvious multifocal nerve involvement, a further purpose of these studies is to distinguish multifocal nerve infarction from multifocal entrapment. Whereas focally decreased conduction velocity or partial conduction block is seen at common entrapment sites with multifocal entrapment, signs of multifocal axonal degeneration distal to the midthigh or mid-upper arm levels are seen in vasculitic mononeuropathy multiplex. In patients without clinically obvious multifocal nerve involvement, a further purpose of these studies is to seek signs of multifocal or non-lengthdependent axonal degeneration that are not obvious clinically. With sensory or motor nerve conduction studies, these signs include finding a more than twofold difference in the amplitude between the right- and left-sided responses of the same nerve (i.e., bilateral asymmetry), a low-amplitude response for one but not another nerve within a limb, or a low-amplitude response for an upper limb nerve if amplitude is normal for at least one lower limb nerve (i.e., non-length-dependence). With needle EMG studies, non-length-dependent axonal degeneration is identified by finding acute partial denervation (reduced recruitment of motor unit
Chapter 97
potentials with or without fibrillation potentials) in some but not other proximal muscles that seem normal clinically. The second step in the diagnostic evaluation is obtaining laboratory tests and possibly a nerve or muscle biopsy. The connectivetissue diseases associated with vasculitic neuropathy are as follows: Polyarteritis nodosa (usually not previously diagnosed) Rheumatoid arthritis (usually an established diagnosis) Others infrequently (either unsuspected or known) Systemic lupus erythematosus Systemic sclerosis Sjogren’s syndrome Churg-Strauss syndrome Wegener’s granulomatosis The two most common causes are polyarteritis nodosa and rheumatoid arthritis with vasculitis. However, the extent of laboratory testing depends very much on the clinical context. The least extensive workup is indicated in a patient with a mononeuropathy multiplex, electrodiagnostic evidence suggestive of vasculitic neuropathy, a previously known diagnosis of rheumatoid arthritis, and the laboratory signs of a highly elevated erythrocyte sedimentation rate and rheumatoid titer. In such a patient, treatment may be initiated with reasonable confidence in the diagnosis of vasculitis, without performing a biopsy or other tests. The most extensive testing is indicated in a patient without a previously known connective tissue disease or in a case with a more confluent neuropathy in whom the possibility of vasculitis is less certain. In these patients, laboratory tests often include complete blood count with differential and platelet count, erythrocyte sedimentation rate, antineutrophil cytoplasmic antibody, antinuclear antibody, rheumatoid titer, complement levels, hepatitis B and C serologies, chemistry tests of renal and liver function, and urinalysis. If the clinical suspicion of vasculitic neuropathy is sufficiently high, biopsy of nerve or muscle is requested at the same time the preceding tests are ordered. This request often is made the same day as the clinical and electrodiagnostic evaluation, with the biopsy performed within 1 to 3 days as an emergency procedure. If the possibility of vasculitic neuropathy becomes reasonable only after some or all of the laboratory tests return (for example, in a more slowly evolving neuropathy that is partially or fully confluent) then biopsy of nerve or muscle is arranged as an urgent procedure when the possibility becomes reasonable. Treatment of vasculitic neuropathy usually is initiated with glucocorticoids, either oral 1 mg/kg/day prednisone or intravenous 1 g/day methylprednisolone for 3 days followed by oral prednisone. If the vasculitis is limited to peripheral nerve and muscle (which is as common as polyarteritis nodosa and rheumatoid vasculitis), treatment may consist of prednisone for 4 to 12 months, or 2 mg/kg/day azathioprine may be added and continued for 1 to 2 years. If the vasculitis is systemic and necrotizing, 2 mg/kg/day oral cyclophosphamide often is added and continued for 1 or more years. Recovery from the sensory and motor deficits is likely in survivors, with meaningful improvement in 28% at 3 months, 60% at 6 months, and 86% at 1 year. Distal SymmcMcal Axonal Polyneuropathy
This type of neuropathy develops in most types of diffuse connective tissue disease, which include the following:
W
Neuropathies in Connective Tissue Diseases
611
Rheumatoid arthritis (a mild one in a majority with known rheumatoid arthritis if carefully sought) Systemic lupus erythematosus (in 6% to 21%with known systemic lupus erythematosus) Systemic sclerosis (in 10% to 15% with known systemic sclerosis) Sjogren’s syndrome (in 10% to 15% with known primary disease) Giant cell arteritis (in 7% with known giant cell arteritis) The presenting complaints usually are sensory symptoms in the toes or feet. Paresthesias and symptoms of sensory loss are characteristic. The paresthesias often are described as tingling, but other adjectives referring to nonpainful extra sensations are not unusual. Symptoms of sensory loss include diminished awareness of pain (e.g., awareness of cut on foot only when blood seen), temperature (e.g., toes cannot sense when water in bathtub is hot), touch (e.g., noticed while clipping toenails), or position (e.g., difficulty getting toes in socks or stockings). Loss of position sense also may be noticed as imbalance. Partial sensory loss is occasionally described as feeling as if walking on sand or marbles. Pain in the toes or feet is a common symptom, too, but less characteristic if not associated with paresthesias or sensory loss. Sharp stabbing and lancinating pain, as well as more constant burning pain, usually is caused by neuropathy. Dull aching and pressurelike pain are nonspecific. With distal symmetrical axonal polyneuropathy, sensory symptoms begin in the toes or feet symmetrically and gradually spread proximally over time in a length-dependent manner. At the time when distal lower limb symptoms have spread up to the midcalf level, similar symptoms usually begin in the fingertips symmetrically. Often, near this point in time, weakness at the ankles becomes an additional complaint. Symptoms that are caused by ankle weakness include slapping of the feet with walking, tripping over steps or thick carpet, or having to step higher consciously to avoid tripping. To distinguish distal symmetrical axonal polyneuropathy from vasculitic neuropathy, the length dependency and symmetry of symptoms and signs are important concepts. In distal axonal polyneuropathy, nerve fibers that are the same distance from the nerve cell bodies (or the same distance from the spinal cord) should be affected to a similar degree. Thus, both feet should be symptomatic near the same point in time (roughlywithin a month of each other), and fingers should not be affected until the lower legs are affected. If symptoms begin in one or both hands before involvement between the ankle and knee, this strongly suggests either vasculitic neuropathy or a superimposed compression neuropathy. The neurologic signs of distal symmetrical axonal polyneuropathy parallel those of the symptoms but may be quantitatively different (either more or less severe than the complaints). The initial signs usually are a decreased threshold for vibration perception in the toes and at the ankle and depressed or absent ankle tendon reflexes. A decreased threshold for pain perception (pinprick) and temperature (warm usually is more useful than cold, as feet themselves are often cool) is often observed as well. Wasting of intrinsic foot muscles and weakness of toe movements occasionally are seen early in the course of distal symmetrical axonal polyneuropathy but usually are delayed until the upper edge of the stocking decrease in sensation is up to the midcalf level. A decreased threshold for perception of pain, temperature, or vibration is seen in the fingers at about the same time the lower limb sensory level has spread up to the midcalf level.
612
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral N e w
The first step in the diagnostic workup is electrodiagnostic evaluation to assess the severity and pathophysiologic basis for the clinical symptoms and signs. In distal symmetrical axonal polyneuropathy, signs of axon loss are seen most prominently in a distal and symmetrical distribution. Thus, EMG studies reveal reduced recruitment of motor unit potentials in distal more than proximal muscles and in intrinsic hand muscles no more severely than in muscles of anterior and posterior compartments of the lower leg. Reduced recruitment of motor unit potentials usually is accompanied by signs of chronic partial denervation with reinnervation (an increased incidence of long-duration, large-amplitude, or polyphasic motor unit action potentials) and, in more rapidly progressive cases, signs of acute denervation (reduced recruitment associated with fibrillation potentials). Nerve conduction studies document symmetrically decreased amplitude of sensory nerve and compound muscle action potentials, with normal or mildly reduced conduction velocities. If axon loss is not in a symmetrical and length-dependent distribution, then subsequent evaluation is refocused for a possible vasculitic neuropathy. The second step in the diagnostic evaluation is obtaining laboratory tests. In a patient with a known connective tissue disease, these usually include complete blood count with differential and platelet count, erythrocyte sedimentation rate, antibody titers that correlate with activity for that particular connective tissue disease, chemistry tests of renal and liver function, vitamin B,, level, thyroid function tests, serum protein electrophoresis, and urinalysis. The latter tests are obtained to evaluate the possibility of a cause for the polyneuropathythat is less directly related to the connective tissue disease. Distal symmetrical axonal polyneuropathy is rarely the first sign of an unsuspected connective tissue disease. The treatment of distal symmetrical axonal polyneuropathy often is symptomatic or rehabilitative. Symptomatic treatments usually are for pain and commonly include tricyclic antidepressants (usually amitriptyline, nortriptyline, or desipramine) or membrane-stabilizing drugs (usually gabapentin or carbamazepine). Rehabilitative treatments often include orthotic shoe inserts for activity-related pain or plastic ankle-foot orthoses for ankle weakness. Potentially curative treatment usually is limited to cases in which symptoms and signs turn out to be caused by a confluent vasculitic neuropathy.
Trigeminal Sensory Neumpathy Trigeminal sensory neuropathy is characterized by slowly progressive facial sensory symptoms, either unilaterally or bilaterally. The sensory symptoms often begin with a small unilateral patch of numbness that is around the mouth or on the cheek. This small patch typically expands gradually and unilaterally. The deficit typically is maximal over 6 to 24 months. Contralateral sensory symptoms do not develop in many patients but may develop in some, often after a delay of several years. Facial numbness often is associated with paresthesias or pain. The neurologic examination is abnormal for impaired perception of pain, temperature, or light touch in the symptomatic distribution. The corneal reflex is blunted or absent in many patients. The severity of sensory involvement can be documented objectively in a quantitative manner with blink reflex studies. An afferent delay (i.e., delayed ipsilateral R1 and bilateral R2) or an absent response is seen in about one half of patients. Trigeminal sensory neuropathy presents in two manners: Trigeminal neuropathy as initial or early manifestation of systemic sclerosis
Trigeminal neuropathy as a manifestation of a known connective tissue disease Sjogren’s syndrome Systemic lupus erythematosus Rheumatoid arthritis Dermatomyositis Undifferentiated connective tissue disease Based on the limited amount of pathologic data available, trigeminal sensory neuropathy appears to result from degeneration of peripheral myelinated axons caused by fibrosis or low-grade perivascular inflammation or vasculitis involving or distal to gasserian ganglion. Based on cases studied with magnetic resonance imaging, gadolinium enhancement of the cisternal preganglionic portion of the trigeminal nerve and of the gasserian ganglion that is often transient supports inflammation of or proximal to the ganglion. Even if this inflammation were caused by vasculitis, the development of systemic vasculitis is unusual. Furthermore, less than 10% of patients have even a subjective response to treatment with prednisone. Thus, trigeminal sensory neuropathy generally does not indicate the need to initiate prednisone or immunosuppressive therapy. However, trigeminal sensory neuropathy is important to recognize, because this often leads to the diagnosis and treatment of systemic sclerosis.
Sensory Neuronopathy Sensory neuronopathy is associated primarily with Sjogren’s syndrome. Most patients are middle-aged women who present with symptoms of sensory neuronopathy and are not known to have Sjogren’s syndrome. Although any limb may become symptomatic first, most patients present with symptoms in both legs and have gait ataxia. Other common chief complaints are clumsiness, incoordination, decreased awareness of limb position, or numbness. The onset often is insidious but may be acute or subacute. On neurologic examination, signs usually are most prominent in the lower limbs but can be most severe in one arm. Sensory impairment usually is greater for vibration and proprioception than for pain and temperature. Deep tendon reflexes usually are depressed or absent in affected limbs. Strength is normal but may seem mildly reduced because of the severity of incoordination. Romberg’s sign is positive if lower limbs are affected. Pseudoathetosis may be prominent if the upper limbs are involved. The first step in the diagnostic evaluation is electrodiagnostic testing. Sensory nerve action potentials typically are absent in affected limbs but, if recordable, have normal conduction velocities unless the amplitude is severely reduced. EMG and motor nerve conduction studies have normal results or mild abnormalities in such a limited distribution as to be of doubtful clinical significance. These results then confirm that the neuropathy is a sensory neuronopathy and that the differential diagnostic possibilities are limited to Sjogren’s syndrome, a paraneoplastic syndrome, a short list of toxic exposures, or unknown cause. If the patient has symptoms of dryness of the eyes or mouth, the second step in the diagnostic evaluation includes those directed at documenting Sjogren’s syndrome. Reduced lacrimation by Schirmer’s test, signs for keratoconjunctivitis sicca by the rose bengal test, evidence for Sjogren’s syndrome in minor salivary gland biopsy specimens, and elevated titers to antinuclear antibody or rheumatoid factor usually are present, whereas anti-Ro antibodies or arthritis is present in less than one third. Other testing may be performed to look for a primary or recurrent tumor
Chapter 97 W
and include anti-Hu (also known as antineuronal nuclear antibody, type 1) antibody. The pathogenesis of sensory neuronopathy in Sjogren’s syndrome is a dorsal root ganglionitis; dorsal root ganglia biopsy specimens have revealed lymphocytic infiltration with degeneration and loss of the neurons in the few patients who have undergone this procedure. Because of this pathogenetic mechanism, immunosuppressive treatment with cyclophosphamide or other drugs often is used, but the benefit of such therapy has not been established. About one half of patients stabilize and functionally improve during immunosuppression, but objective signs of improvement (as with larger sensory nerve action potentials) are not usually seen.
Entrapment or Compression Neuropathles An increased incidence of entrapment or compression neuropa-
thies is generally accepted in association with some connective tissue diseases. The association of the carpal tunnel syndrome and rheumatoid arthritis has been most thoroughly studied. During the course of rheumatoid arthritis, one quarter to one third of patients are likely to develop symptoms of carpal tunnel syndrome and have a positive Tine1 sign. One fifth to one quarter of patients with Sjogren’s syndrome or systemic sclerosis may also develop carpal tunnel syndrome. The predominant electrophysiologic abnormality in such cases is the prolongation of sensory or motor latency through the carpal tunnel. This electrodiagnosticfeature is useful in distinguishing entrapment or compression from vasculitic neuropathy. An increased incidence of ulnar neuropathy at the elbow and peroneal neuropathy at the fibular head has also been reported in rheumatoid arthritis. However, this seems to be based primarily on anecdotal reports rather than on prospective studies and therefore may represent a simple chance association rather than a predisposition.
Other Neuropathies Acute inflammatory demyelinating polyneuropathy, chronic inflammatory demyelinating polyneuropathy, and brachial neuritis have been described in patients with known systemic lupus erythematosus and, rarely, in patients later found to have systemic lupus erythematosus. These associations may represent the chance occurrence of two diseases or may possibly reflect an abnormal immunologic mechanism that predisposes to both diseases. The nature of the association is speculative at this point.
CONNECTIVE TISSUE DISEASES ASSOCIATED WITH PERIPHERAL NEUROPATHIES The diffuse connective tissue diseases that are commonly associated with peripheral neuropathies are as follows: Rheumatoid arthritis Systemic lupus erythematosus Systemic sclerosis Sjogren’s syndrome Vasculitides Polyarteritis nodosa Allergic granulomatosis (Churg-Strauss syndrome) Giant cell arteritis Wegener’s granulomatosis
Neuropathies in Connective Tissue Diseases
613
Rheumatoid Arthritis Rheumatoid arthritis is the most common connective tissue disease. It affects 1% to 2% of adults worldwide and more than 10% of the population that is above age 65 years. A definite diagnosis of rheumatoid arthritis requires the documentation of at least four of seven criteria in the 1987 revision. The neuropathies associated with rheumatoid arthritis are as follows: Vasculitic neuropathy in less than 10% Distal symmetrical axonal polyneuropathy in majority Trigeminal sensory neuropathy Entrapment or compression neuropathies, especially carpal tunnel syndrome Systemic necrotizing vasculitis complicatesrheumatoid arthritis in 8% to 25% of cases by the time of death, usually after arthritis has been present for an average of 14 years. However, on rare occasions systemic necrotizing vasculitis is the major presenting feature of rheumatoid arthritis. Weight loss, rheumatoid nodules, and cutaneous lesions usually are seen with systemic necrotizing vasculitis. Clinically apparent vasculitic neuropathy develops in about one half of patients with systemic necrotizing vasculitis. Although the majority of patients with rheumatoid arthritis develop a mild sensory distal axonal symmetrical polyneuropathy, clinically significant vasculitic neuropathy develops in less than 10%. With rheumatoid vasculitis, the erythrocyte sedimentation rate usually is elevated, and the rheumatoid factor typically has a high titer. The development of vasculitis in patients with rheumatoid arthritis results in a poor prognosis. Even with steroid and immunosuppressivetherapy, the 6-month survival rate is 80% and the 5-year rate is 60%, similar to that for polyarteritis nodosa. Although clinically significant vasculitic neuropathy develops in less than lo%, a majority of patients with rheumatoid arthritis have evidence of a mild sensory distal symmetrical axonal polyneuropathy when detailed clinical and electrodiagnostic examinations are performed. If nerve biopsies are performed on these patients, variable amounts of intimal thickening and less frequent perivascular mononuclear infiltration often are seen in endoneurial and epineurial vessels. Similar changes are common in peripheral nerves taken at autopsy from patients who had rheumatoid arthritis without clinically evident neuropathy. Thus, a low-grade vasculitis is one possible explanation for the mild sensory distal symmetrical axonal polyneuropathy, although there is no convincing evidence that immunosuppressive treatment is beneficial for it. Exposure to toxic medications and other undefined factors may also be important in the pathogenesis of the mild sensory distal symmetrical axonal polyneuropathy.
Systemic Lupus Erythematosus Systemic lupus erythematosus is a common connective tissue disease in young women. Its general prevalence in adults is about 1 in 2000, but its prevalence is 1 in 250 in black women under 65 years and 1 in 1000 in white women of comparable age. Women are five times more likely to be affected than men. Systemic lupus erythematosus is diagnosed by the cumulative occurrence of at least 4 of 11 multiple-system or laboratory criteria. Although central nervous system involvement fulfills 1 of these 11 criteria, peripheral neuropathy does not. The neuropathies associated with systemic lupus erythematosus are as follows: Vasculitic neuropathy (rarely) Distal symmetrical axonal polyneuropathy in 6% to 25%
614
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Newe
Trigeminal sensory neuropathy Other neuropathies (rarely) Acute inflammatory demyelinating polyneuropathy Chronic inflammatory demyelinating polyneuropathy Brachial neuritis About 6% to 25% of patients develop polyneuropathy, typically a distal symmetrical axonal polyneuropathy with predominantly sensory symptoms and subacute or chronic evolution. Most are not caused by low-grade vasculitis; however, vasculitic neuropathy and demyelinating polyneuropathy are well described in occasional patients. When the neuropathy is produced by a systemic necrotizing vasculitis, improvement usually results from treatment with plasmapheresis, steroids, and immunosuppressive drags. Steroids or other immunotherapies are not clearly beneficial in cases with distal symmetrical axonal polyneuropathy. Systemic Sclerosis
Systemic sclerosis usually presents initially with Raynaud’s phenomenon. Some patients rapidly develop diffuse cutaneous signs with symmetrical, widespread thickening of the skin and have early visceral involvement. Others have limited cutaneous signs with symmetrical, distal limb and facial thickening and late visceral involvement. These latter patients usually have CREST syndrome (calcinosis, Raynaud’s phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia). The association of systemic sclerosis with trigeminal sensory neuropathy has been recognized for a long time. Although systemic sclerosis was once though not to be associated with neuropathies in the limbs, recent observations suggest that 10%to 15% of patients may have a distal symmetrical axonal polyneuropathy.
Peripheral neuropathy is present in 10% to 15% of cases of primary Sjogren’s syndrome, usually a distal symmetrical one that begins with paresthesias in the feet. Although clinical symptoms and signs are limited to the sensory fibers initially, electrodiagnostic studies provide evidence of distal loss of sensory and motor axons in most patients. The erythrocyte sedimentation rate and the titer for rheumatoid factor are elevated in a majority of patients with neuropathy, and many have elevated titers for antinuclear antibody or Sjogren’s syndrome A (Ro) antibody. In patients with neuropathy, signs of cutaneous vasculitis are common, sensory loss may be asymmetrical, and biopsy of sural nerves often suggests vasculitis. Thus, a low-grade vasculitis may be the usual pathogenetic explanation for the mild distal, usually symmetrical axonal polyneuropathy in Sjogren’s syndrome. However, systemic necrotizing vasculitis is rare. Convincing evidence of a beneficial effect of steroid or immunosuppression is lacking for most patients with Sjogren’s syndrome and neuropathy unless vasculitis is present. Polyartedtis Nodosa
The neuropathies associated with systemic lupus erythematosus are as follows:
Polyarteritis nodosa is the most common type of systemic necrotizing vasculitis that produces vasculitic neuropathy, with involvement of small and medium-size arteries. It is usually seen in middle-aged or older adults, with male predominance. Peripheral neuropathy develops in about one half of patients. The neuropathy usually presents as a mononeuropathy multiplex or at least with asymmetry and is almost always caused by vasculitis. The vasculitic neuropathy is the major presenting symptom in more than one third of cases and clinically apparent at presentation in most of the remainder. In the one half who develop vasculitic neuropathy, it is usually present within the first year of polyarteritis. In patients with polyarteritis nodosa, symptoms and signs of systemic disease usually are present. Weight loss and fever are present in two thirds to three quarters of patients. Arthralgias and rash each occur in one half. Less common clinical features include hypertension and renal, cardiac, or gastrointestinal involvement. An elevated erythrocyte sedimentation rate occurs in all but 5%to 10%. Anemia, leukocytosis, or abnormal urinalysis is found in most patients. Hepatitis B surface antigen is positive in a significant minority and may be causally related to polyarteritis nodosa in those cases. The diagnosis entails the pathologic documentation of necrotizing vasculitis or the arteriographic demonstration of aneurysms at vessel bifurcations. Although arteriography of the renal, hepatic, or mesenteric vessels may support the diagnosis in many cases, similar abnormalities may be seen in Wegener’s granulomatosis, left atrial myxoma, and infective endocarditis. The highest sensitivity and specificity from invasive testing in patients who present with neuropathy are achieved with biopsy of an electrophysiologically abnormal cutaneous nerve or with a muscle biopsy. In 1990, the American College of Rheumatology proposed criteria for diagnosing and classifylng vasculitis caused by polyarteritis nodosa, whether presenting with or without neuropathy. In this study, an 82% sensitivity and a 87% specificity were achieved by satisfying 3 or more of the following 10 criteria:
Vasculitic neuropathy (rarely) Distal symmetrical axonal polyneuropathy in 10% to 15% Trigeminal sensory neuropathy Sensory neuronopathy
Weight loss (4 kg) Livedo reticularis Testicular pain or tenderness Myalgias
Sj6gren.s Syndrome Sjogren’s syndrome may develop as a primary connective tissue disease or may be secondary to another one, usually rheumatoid arthritis, systemic lupus erythematosus, or systemic sclerosis. Women are nine times more likely to affected than are men. Sjogren’s syndrome is characterized by dryness of the mouth (xerostomia) and the eyes (xerophthalmia). There are no universally agreed-upon criteria for its diagnosis. One recent proposal that is as well accepted as any requires four of the following six criteria for a definite diagnosis and three of six for a probable diagnosis: Specific symptoms of dry eyes Specific symptoms of dry mouth Evidence of keratoconjunctivitis with either a positive Schirmer’s test or a positive result on the rose bengal dye test Objective evidence of diminished salivary gland flow or salivary gland involvement An abnormal minor salivary gland biopsy The presence of autoantibodies (SS-A, SS-B, antinuclear antibody, or rheumatoid factor)
Chapter 97
Neuropathy Hypertension (diastolic > 90 mm Hg) Elevated blood urea nitrogen or creatinine Presence of hepatitis B surface antigen Characteristic arteriographic abnormality Pathologic evidence of necrotizing vasculitis Untreated patients with polyarteritis nodosa have a 6-month survival of 35% and a 5-year survival of 13%. Steroid therapy improves survival to 68% at 6 months and 50% at 5 years. The early use of cyclophosphamide allows up to a 94% 6-month survival. Either cyclophosphamide or other cytotoxic therapy permits up to an 80% 5-year survival. Although there is a trend for cyclophosphamide to improve survival, this difference has not proven to be statistically significant, so some authors do not recommend the routine addition of cyclophosphamide. Although adversely affected by visceral involvement, the prognosis does not seem to be influenced by the occurrence of vasculitic neuropathy. Allergic Granulomatosls (Churg-Strauss Syndrome)
The Churg-Straws syndrome, or allergic granulomatosis,has been considered a variant of polyarteritis nodosa by some. It may be diagnosed with 85% sensitivity and 99.7% specificity by the presence of four or more of the following six criteria: Asthma Peripheral eosinophilia Nonfixed pulmonary infiltrates Paranasal sinus abnormality Neuropathy A biopsy with a blood vessel that contains extravascular eosinophils. As with polyarteritis nodosa, vasculitic neuropathy is the only associated neuropathy. The prognosis and treatment of ChurgStrauss syndrome are essentially the same as those of polyarteritis nodosa. Giant Cell Meritis
Giant cell arteritis is perhaps the most common form of vasculitis, typically involving medium and large arteries that are branches of vessels originating from the aortic arch. Patients usually are older than 50 years, present with headache, and have an erythrocyte sedimentation rate elevated to 50 mm/hour or more. It is diagnosed most specifically by a temporal artery biopsy that
Neuropathies in Connective Tissue Diseases
61S
documents a necrotizing arteritis with giant cells. In contrast to the approximate 50% prevalence of neuropathy in polyarteritis nodosa or Churg-Strauss syndrome, neuropathy has been found in only 14% of patients with giant cell arteritis, with about one half being diffuse peripheral neuropathies. Although the mechanism is uncertain, an immune-mediated cause for the neuropathy is implied by the majority of patients having improvement in neuropathic deficits with steroid therapy. Even though a small number of patients have developed an acute mononeuropathy or multiple mononeuropathies that suggest vasculitis, nerve ischemia seems related to thrombosis of nutrient or larger vessels because the vessels involved with giant cell arteritis are larger than the epineurial arterioles that are affected in vasculitic neuropathy. Wegenefs Granulomatosls
Wegener’s granulomatosis is diagnosed by identifymg granulomatous vasculitis of small vessels in the upper and lower respiratory tracts and a segmental necrotizing glomerulonephritis. Peripheral neuropathy develops in 11% to 16% of patients, with the majority being vasculitic mononeuropathy multiplex. In the minority of these patients with distal symmetrical polyneuropathy, coincidental renal failure is common and offers an alternative explanation.
SUGGESTED READINGS Arnett FC, Edworthy S, Block DA et al: The 1987 revised ARA criteria for rheumatoid arthritis (abstracted). Arthritis Rheum 31(3):315-324, 1988 JennetteJC, Fa& RE Small-vesselvasculitis. N Engl J Med 337(21):15121523, 1997 Klippel JH: Primer on the Rheumatic Diseases. 11th Ed. Arthritis Foundation, Atlanta, 1997 Lightfoot RW, Michel BA, Bloch DA et al: The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum 33(8):108&1093, 1990 Masi AT, Hunder GG, Lie JTet al: The American College of Rheumatology 1990 criteria for the classificationof Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum 33(8):1094-1100, 1990 Moore PM: Neurology of the vasculitides and connective tissue diseases. 7 Neurol Neurosurg Psychiatry 65(1):lO-22, 1998 Olney RK: Neuropathies associated with connective tissue disease. Semin Neurol 18(1):63-72, 1998 Tan EM, a h e n AS, Fries JF et al: The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 25(11):1271-1277, 1982 Vitali C, Bombardieri S, Moutsopoulos HM et al: Preliminary criteria for the classification of Sjogren’s syndrome. Arthritis Rheum 36(3):340347, 1993
616
98
Spinal Cord and Peripheral Neuromuscular Disease H Diseases of PeripheralNerve
Toxic Peripheral Neuropathies Michael T. Pulley and Alan R. Berger
Peripheral neuropathies caused by toxin exposure are rare. The majority of cases are individual, sporadic intoxications, but outbreaks such as the Minamata Bay mercury disaster garner a disproportionate amount of attention. The sporadic occurrence of toxic peripheral neuropathies (TxPNs) makes diagnosis very difficult. Therefore, a high index of suspicion is needed to detect the unusual cases of suicidal or homicidal ingestion and rare small-scale occupational exposures. Establishing a relationship between occupational exposure to a toxin and a sporadic peripheral neuropathy often is challenging because of a vague exposure history. TxPNs often are identical clinically and electrophysiologically to those caused by metabolic abnormalities, nutritional deficiencies, or systemic illness. Testing for toxic substances is unhelpful either because the delay between exposure and examination allows the substance to be eliminated or because a reliable test of body burden is not available. Therefore, many naturally occurring peripheral neuropathies tend to be misdiagnosed as toxic in origin when an alternative cause is not obvious. The most common pathologic pattern of TxPNs is known as the central-peripheral distal axonopathy. Exposure to the toxin causes degeneration of the distal portions of peripheral sensory and motor axons as the initial damage. Continued exposure causes similar injury to the distal segments of corticospinal,spinocerebellar, and dorsal column axons. The damage to central tracts, which can result in spasticity, ataxia, and persistent sensory loss, may become apparent only after recovery of the peripheral sensory and motor axons. The lack of regeneration in central sensory and motor tracts results in persistent clinical deficits. CARDINAL TENETS OF NEUROTOXIC ILLNESS AFFECTING THE PERIPHERAL NERVOUS SYSTEM Recognition of TxPNs is based on understanding and applying basic tenets of neurotoxic disease rather than memorizing the characteristics of the many potential neurotoxins. The identification of a neurotoxic illness should satisfy, or at least not be inconsistent with, the following basic principles. Neurotoxins produce a consistent pattern of disease, dependent on the dosage and duration of exposure. People with neurotoxin exposure similar in duration and degree invariably manifest similar signs and symptoms as long as the toxin enters the circulation, and the agent, its metabolite, or its intermediate has similar access to the nervous system. If the exposure dosage or duration is different, the same toxin may produce strikingly different clinical syndromes, but a similar and consistent illness should result in patients with similar exposures. Individual susceptibility or idiosyncratic reactions do not occur if dosage and duration of exposure are similar. Therefore, a neuropathy is unlikely to be neurotoxic in nature if only one member of a group with similar exposure history develops a neuropathy. Similarly, neurotoxicity should be doubted when significantly different clinical manifestations occur in a group of people with identical chemical exposure. Symptoms of neurotoxic illness do not begin months to years after exposure but usually occur concurrent with or shortly after exposure. The two most common exceptions are the 2- to 6-week
delay after exposure to organophosphates and the occasional 2-month latency between cisplatin intoxication and neuropathic symptoms. Another cardinal feature of TxPNs is that the extent and severity of neuropathy usually are commensurate with the degree of toxin exposure. A single, brief, low-level exposure is unlikely to cause a devastating peripheral neuropathy. Although some lipid-stored agents (e.g., chlorinated hydrocarbons) may be detected in fat biopsies years after exposure, there is no evidence that this is associated with risk of future neurotoxicity. TxPNs usually stabilize and then gradually improve after removal of exposure to the neurotoxic agent. Some degree of recovery is the rule, except in the most severely affected patients. If there is no improvement or there is continued deterioration despite the cessation of exposure to a suspected neurotoxin, the neuropathy is unlikely to be neurotoxic in nature. In some cases, however, a toxic axonopathy may worsen transiently after cessation of exposure for several weeks (coasting) before recovery commences. The initial step in diagnosing a TxPN is a suspicion raised by a thorough occupational and environmental exposure history. Many patients do not suspect a relationship between their symptoms and chronic, low-level intoxication because most TxPNs are insidious in onset. The patient's personal hygiene, eating habits, and hobbies should be discussed. Does the patient wear protective devices at work and change clothes before coming home? Does the patient eat in the workplace and always wash hands before eating? Are others at work experiencing similar symptoms? Does transient removal from exposure, such as on weekends or holidays, improve symptoms? Does poor ventilation or inadequate drainage lead to an unacceptably high risk of toxin exposure? A visit to the workplace may be needed to answer these questions. Home visits may be needed to check hobby workshops, medicine cabinets, and food and water sources when domestic poisoning or substance abuse is suspected. Has there been recent pesticide application? Are there neighbors with similar illness? The neurologic examination is useful to demonstrate that deficits are in a pattern and of a severity consistent with neurotoxic illness. The clinical deficits resulting from a TxPN are symmetrical in distribution and distally predominate. Therefore, multifocal deficits suggest a diagnosis other than neurotoxic disease. Also, because TxPNs typically affect mixed nerve function, detecting purely small fiber sensory dysfunction makes neurotoxic disease unlikely. ORGANOPHOSPHATE
Background Organophosphorus (OP) compounds have numerous uses including insecticides, plastic modifiers, flame retardants, lubricants, petroleum additives, and antioxidants. Despite their widespread use, occupational group exposure is rare. The most common cause of OP intoxication is agricultural spraying. Although 150,000 to 300,000 cases of toxicity are reported annually, estimates are that only 2% of cases are reported to public health officials. Exposure to OP may result from working in the fields after spraying or from applying or preparing the pesticide. OP exposure may also result from intentional ingestion in suicide or homicide attempts.
Chapter 98
Dermal exposure is the most common route of OP intoxication, but absorption also occurs through the gastrointestinal (GI) and respiratory tracts. The mechanism of action of OP compounds is irreversible inhibition of the enzyme acetyl cholinesterase (AChE) by phosphorylation in nervous tissue and erythrocytes. AChE breaks down acetylcholinethat has been released from motor axons. Acetylcholine accumulation leads to excessive stimulation of nicotinic and muscarinic ACh receptors.
Three different clinical syndromes may occur with OP exposure. The primary determinants are the duration and extent of exposure, recent prior exposure, and the particular OP to which the person is exposed. Acute or Type I Syndrome. The type I OP syndrome begins less than 24 hours after exposure and therefore is known as the acute syndrome. The clinical manifestations result from activation of muscarinic cholinergic receptors. Thus, nausea and vomiting, diarrhea, salivation, sweating, micturition, and tachycardia or bradycardia are typical. Decreased alertness, cognitive impairment, fatigue, nervousness, and emotional lability are other potential symptoms of the type I syndrome. Convulsions and coma are seen in the most severe cases. Susceptibilityto the acute syndrome is increased by recent exposure to OP, which may have already diminished the amount of AChE. Because mental status abnormalities are common in the type I syndrome, differential diagnosis includes exposure to other toxins or recreational substance abuse. Intermediate or Type II Syndrome. The type I1 or intermediate OP syndrome appears 12 to 96 hours after exposure, whether or not the acute syndrome occurred. The intermediate syndrome may appear after apparent recovery from the acute syndrome. The symptoms result from overstimulation of nicotinic ACh receptors causing depolarizing neuromuscular blockade with resultant muscle weakness. Respiratory muscle weakness occurs first, followed by proximal muscle weakness, including that of the neck flexors. Although weakness of cranial nerve musculature may occur, including the extraocular muscles, distal extremity strength usually remains normal. Recovery begins 5 to 15 days after cessation of exposure and proceeds from the cranial muscles to the respiratory muscles and finally the proximal muscles and neck flexors. The differential diagnosis of the intermediate syndrome with prominent and often fulminant muscular weakness includes Guillain-Barrk syndrome, periodic paralysis, or a severe attack of myasthenia gravis. Organophosphate-Induced Delayed Polyneuropathy (OPIDP). A delayed central-peripheral axonopathy may develop
with exposure to some OPs. Ironically, the compounds that cause very mild cholinergic symptoms may cause more severe neuropathy. In contrast to most toxic neuropathies whose onsets coincide with toxin exposure, OPIDP usually begins 7 to 21 days after exposure. The OPIDP is independent of the presence of the type I or type I1 syndromes, is not related to AChE inhibition, and occurs more often with chronic, low-level exposure. Although the acute and intermediate syndromes occur more often, more long-term morbidity is associated with OPIDP. Initial manifestations include painful paresthesias in the feet and cramps in the calves. The most prominent manifestation is weakness. Distal lower extremities are affected early with foot drop, later progressing to involvement of the intrinsic hand muscles. Weakness is most severe within 2 weeks after onset. Sensory loss usually can be detected despite minimal
Toxic Peripheral Neuropathies
617
sensory symptoms. Gait ataxia often is present and often is disproportionate to the degree of sensory loss. The ankle jerks are absent, but the status of the other reflexes depends on the degree of central nervous system (CNS) impairment and may be pathologically brisk. Cranial nerve involvement and autonomic dysfunction are rare.
Differential Diagnosis The differential diagnosis of OPIDP includes other toxins that cause central-peripheral distal axonopathy. There is an extensive differential diagnosis when OPIDP is mild and presents as a simple distal axonopathy.
Diagnostic Testing The laboratory workup usually is unhelpful in cases of OP toxicity. Recent exposure causes reduction of AChE levels in erythrocytes. Because AChE regeneration occurs at the rate of 1% per day, levels may have returned to normal if there is a significant delay between exposure and testing. Weakness usually is seen when AChE levels are reduced to less than 20% of normal. AChE levels are not helpful in patients suspected of having OPIDP, except to document recent exposure, because the degree of exposure does not correlate with severity or even the presence of neuropathy. Cerebrospinal fluid (CSF) protein may be mildly elevated in cases of OPIDP, but there are no inflammatory cells. Electrophysiologictesting after OP exposure may demonstrate spontaneous repetitive motor action potentials (SRMAPs) in response to single motor nerve stimulation. SRMAPs are additional motor responses following the usual compound motor action potential and are a sensitive indicator of OP exposure. However, presence of S W s does not reflect the degree of intoxication, correlate with the degree of weakness, or predict its occurrence. Repetitive nerve stimulation usually demonstrates a decremental response after weakness has started. Rapid stimulation rates may be necessary to demonstrate decrement when weakness is mild. When OP exposure is severe, SRMAPs may be absent, and decrement is evident even with slow rates of stimulation. OPIDP causes abnormalities of nerve conduction studies consistent with a sensorimotor axonal neuropathy. Despite only mild clinical sensory loss, sensory nerve action potentials are reduced in amplitude or absent. Paradoxically, motor nerve conduction studies are normal or reveal minimal slowing of conduction velocity despite prominent motor symptoms. Electromyography (EMG) reveals evidence of active and chronic denervation in distal limb muscles in OPIDP but is normal in the type I and type 11 syndromes.
Therapy Preventing OP toxicity involves educating those at risk, wearing protective clothing, practicing good hygiene, and monitoring exposure levels. Removing contaminated clothing and washing the skin may prevent further absorption in an exposed person. Administering atropine during the acute syndrome has no effect on subsequent development of the intermediate syndrome or OPIDP. Neuropathy may be detected by electrophysiologictesting in the early stages before it becomes irreversible. Treatment of OP intoxication depends on the symptoms that develop. In acute OP poisoning intubation may be needed even if respiratory failure does not occur. Airway protection may be
618
Spinal cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
necessary because of vomiting or copious secretions in a patient with impaired arousal. Gastric lavage and administration of cathartics are indicated if ingestion is suspected. Atropine is effective in the type I syndrome, but it has a short duration of action and must be given repeatedly. There is evidence of increased risk of ventricular arrhythmias in patients given atropine in the setting of respiratory failure. Therefore, the patient must be adequately ventilated before atropine is administered. Because atropine is specific for muscarinic receptors, it has no effect on depolarizing neuromuscular blockade caused by overstimulation of nicotinic receptors in the type I1 syndrome. Early administration of pralidoxime may help accelerate reactivation of AChE. As long as adequate supportive measures are taken, the prognosis of the acute and intermediate syndromes is good. CNS damage caused by respiratory failure may be permanent. Although severe cases of OPIDP may cause residual foot drop, claw hand deformity, or atrophy, mild cases have a good prognosis. As with all causes of central-peripheral distal axonopathy, the degree of damage to distal dorsal column and corticospinal axons in OPIDP is critical in determining the eventual outcome. CNS damage may become apparent only after recovery from the peripheral neuropathy.
HEXACARBONS Background The hexacarbons n-hexane and methyl n-butyl ketone (MnBK) are clear, colorless, volatile liquids at room temperature. Both are metabolized to the toxic compound 2,s-hexanedione. Hexacarbons gain entry to the body via inhalation, dermal contact, and, rarely, ingestion. These compounds are used as solvents and are components of glues and lacquers. Neuropathy caused by hexacarbon exposure has been reported in several outbreaks including cabinet-finishing plants in the United States and the sandalmaking and shoemaking industries of Japan. Recreational glue sniffing resulting in high-level, acute exposure has become a significant contributor to the problem of hexacarbon neuropathy. Classification
High-level acute exposure causes CNS depression and narcosis that resolves without sequelae. However, glue sniffing involves repeated high-level exposure and leads to peripheral nerve damage and a subacute neuropathy. This neuropathy is predominantly motor and often involves the cranial nerves. The acute neuropathy caused by high-level hexacarbon exposure may be associated with autonomic dysfunction including vasomotor instability, impotence, and hyperhidrosis or anhidrosis. Chronic low-level exposure to hexacarbons causes a lengthdependent central-peripheral distal axonopathy that develops gradually. Like OPIDP, the central-peripheral axonopathy caused by hexacarbons first damages distal peripheral axons, then distal corticospinal, spinocerebellar, and dorsal column axons. Symptoms progress in a length-dependent fashion with involvement of both large- and small-fiber sensory modalities. The ankle reflexes usually are absent, but the other tendon reflexes may be preserved. In severe cases, weakness is the predominant neurologic manifestation and involves distal arm and leg muscles. Advanced cases have abdominal pain, weight loss, malaise, and leg cramps. Hexacarbon neuropathy is well known for the coasting phenomenon.
Differential Diagnosh Acute hexacarbon neuropathy, especially that associated with glue sniffing, may be mistaken for Guillain-Barrk syndrome, given the subacute presentation with prominent weakness and autonomic dysfunction. The central-peripheral distal axonopathy seen with chronic hexacarbon exposure is also seen with neuropathies from organophosphate, acrylamide, and carbon disulfide intoxication. DiagnosticTesting
A very characteristic morphologic feature of the peripheral nerves of those with hexacarbon toxicity involves the formation of giant axonal swellings. Such axonal swellings are also seen with exposure to carbon disulfide and acrylamide and in the genetic neuropathy giant axonal neuropathy. The axonal swellings are caused by accumulation of neurofilaments, primarily in paranodal regions because of disruption of axonal transport and crosslinking. The result is a distal-central dying-back neuropathy. 2,5-Hexanedione, the toxic metabolite, can be measured in the urine, and its presence may indicate excess hexacarbon exposure before the appearance of significant toxicity. An unusual electrophysiologic finding in hexacarbon neuropathy is prominent slowing of distal motor conduction velocities. Screening nerve conduction studies, performed on asymptomatic workers employed in factories where cases of solvent polyneuropathy have been detected, may show slowed conduction velocities. CSF protein may be elevated if the nerve roots are involved, but the spinal fluid is acellular. Therapy
There are no treatments specific for hexacarbon neuropathy, so prevention is the key. Helpful measures include use of protective clothing and gloves to decrease dermal contact, use of ventilators in areas with high concentrations, and measurement of ambient air levels to evaluate the risk of exposure. Removal from exposure will prevent progression, but coasting, as described earlier, is common. Severe neuropathies often result in residual sensory loss, muscle atrophy, and distal weakness. Patients with mild hexacarbon neuropathy typically recover completely. Damage of the distal portions of central pathways can cause long-tract weakness, spasticity, ataxia, or dorsal column dysfunction. This may become apparent only after resolution of the peripheral neuropathy.
CARBON DlSULFlDE Background Carbon disulfide (CS,) is a clear liquid that vaporizes at room temperature and is readily absorbed by inhalation. It is used to produce viscose rayon fibers and cellophane films. It is also a major metabolite in the breakdown of the drug disulfiram (Antabuse), which is used as a deterrent for alcohol abuse. Although CS, absorption typically occurs by dermal contact or inhalation, absorption from the GI tract can occur. Classification
High-level CS, exposure that is acute or subacute leads to CNS dysfunction. This may include confusion, memory impairment, hallucinations, and emotional lability. Chronic low-level exposure causes a combination of neuropathy and neuropsychological abnormalities. Subclinical neuropathy, detected only by electro-
Chapter 98
physiologic testing, may be the only manifestation with low-level intoxication. With increased exposure, a progressive sensorimotor distal polyneuropathy emerges. Sensory impairment occurs first with distal paresthesias and numbness. Weakness is not usually a complaint but may be detected by careful examination. Prolonged exposure may lead to headache, dizziness, memory impairment, and depression. Exposed patients may also display CNS dysfunction such as spasticity or hemiparesis in addition to extrapyramidal signs of bradykinesia, cogwheel rigidity, and tremor. Dlfferentlal Diagnosis
CS, causes a neuropathy that is very similar to that caused by hexacarbons, organophosphates, and acrylamide. Exposure history is the key in differentiatingthe responsible agent. Laboratory tests may also be helpful. Diagnostic Testing
CS, exposure can be documented by measurement of urinary levels of the metabolite 2-triothiazolidine-Parboxylic acid. Abnormalities of motor and sensory nerve conduction studies seen in CS, neuropathy include prolonged latencies and conduction velocity slowing. EMG of distal leg muscles reflects the axonal degeneration and chronic motor unit reinnervation, even though weakness is not a prominent clinical feature. The CSF is acellular with a normal protein level. Carbon disulfide neuropathy is associated with the formation of giant axonal swellings, identical to those seen in acrylamide and hexacarbon neuropathies. These axonal swellings are caused by crosslinking and accumulation of cytoskeletal proteins, including neurofilaments.
Toxic Peripheral Neuropathies
619
there may be progression to encephalopathy with seizures and truncal ataxia. This may be followed by a peripheral neuropathy. High-level acute exposure often leads to accompanying autonomic dysfunction with excessive sweating, vasomotor changes in fingers and toes, impairment of reflex heart rate, and blood pressure fluctuation. Chronic low-level exposure leads to neuropathy and dermatitis. Because acrylamide exposure is most often by dermal contact, a contact dermatitis typically is present before the clinical symptoms of neuropathy. CNS manifestations are rare in this setting. Chronic exposure is less likely to cause significant autonomic problems, but excessive sweating of the hands and feet is a common manifestation. Acrylamide exposure causes a central-peripheral distal axonopathy. Damage initially occurs in the distal portion of the longest peripheral axons, with subsequent damage to distal corticospinal, spinocerebellar, and dorsal column pathways. Initial findings include diffusely decreased reflexes and numbness in the distal lower extremities. Sensory loss involves large-fiber modalities of vibration and joint position sense rather than small-fiber function of pin and temperature sensation. Despite the dominance of sensory symptoms, physical examination may demonstrate weakness and cerebellar dysfunction. Differential Diagnosis
Other toxins described in this chapter also cause the centralperipheral distal axonopathy seen with acrylamide exposure. However, the symptom of excessive sweating in the hands and feet and accompanying contact dermatitis are unique to acrylamide. The giant axonal swellings seen in acrylamide toxicity are identical in morphology to those seen with hexacarbon or CS, exposure.
Therapy
Because therapeutic intervention is limited, prevention is essential. Respiratory exposure can be minimized by adequate ventilation, use of respirators, and regular air samplings. The compound pyridoxine is reactive with CS,, so it seems logical to treat with this compound to reduce toxicity. However, the available data do not indicate its effectiveness. The extent of recovery from CS, neuropathy is determined by the degree of peripheral nerve and CNS dysfunction present when exposure is terminated. Patients with mild cases usually recover filly, including most of the CNS abnormalities. In those with severe CS, neuropathy, more than one third have symptoms and signs of neuropathy 10 years later.
ACRYLAMIDE Background Acrylamide is a chemical component of agents used for grouting, and polyacrylamide is used as a flocculator in wastewater treatment plants. Acrylamide absorption takes place by inhalation, dermal contact, and rarely by ingestion. The monomer and its metabolite, glycinamide, are neurotoxic, whereas the polymer is innocuous. Classification
Acute acrylamide exposure that is low to moderate in intensity may cause anorexia, headache, malaise, and dizziness. The patient may not recognize his or her own behavioral changes, and the problem often is reported by observers. With high-level exposure
Diagnostic Testing
Acrylamide neuropathy is characterized electrophysiologically by reduced sensory potential amplitudes. Motor and sensory conduction velocities and motor potential amplitudes are normal. Electrophysiologic abnormalities have been documented in asymptomatic patients with acrylamide exposure. Sural nerve biopsy demonstrates reduced numbers of thickly myelinated large axons. Nerve biopsy may be helpful because acrylamide neuropathy is characterized by axonal swelling caused by disruption of axonal transport with resulting accumulation of neurofilaments in the paranodal region. However, these swellings are identical to those seen in carbon disulfide and hexacarbon neuropathies. Therapy
Prevention of acrylamide toxicity involves limiting exposure. This includes wearing protective clothing and gloves to limit dermal exposure, ensuring adequate ventilation, and using respirators in areas with high levels to prevent respiratory exposure. Gastric lavage may help reduce the level of intoxication if performed shortly after acute ingestion. Acrylamide neuropathy usually resolves completely in mild cases if further exposure is prevented. Residual loss of vibratory sensation may be apparent but asymptomatic. Residual spasticity, ataxia, profound sensory dysfunction, and memory problems may persist in more severe cases. These problems are more the result of damage to the distal portions of central sensory tracts than to peripheral nerve
6220
Spinal Cord and Peripheral Neuromuscular Disease w
Diseases of Peripheral Newe
dysfunction. As with some other toxic neuropathies, worsening of symptoms after termination of exposure can occur (coasting).
VACOR Background Vacor, or N-3-pyridylmethyl-N-p-nitrophenyl urea (PNU), is a chemical used as a rodenticide. It is structurally related to nicotinamide. Exposure to vacor usually occurs by accidental or intentional ingestion. Classification
Vacor causes a severe acute distal axonopathy after even a single exposure. There is also significant autonomic involvement. Within the first hour after high-level ingestion, acute weakness of the limbs and impairment of postural reflexes are seen. The weakness progresses rapidly to become severe generalized weakness including the cranial nerve-innervated muscles. There is also urinary retention. Vacor also damages the p cells of the pancreas leading to acute diabetes mellitus and diabetic ketoacidosis. Studies of vacor-induced neuropathy in animals demonstrate abnormalities of fast axonal transport in distal nerves with degeneration of nerve terminals. The morphology of the neuromuscular junction also is abnormal. Impairment of fast axonal transport may explain the rapid onset of weakness. The few autopsy studies reported have demonstrated wallerian-like degeneration in the peripheral nerves, roots, and dorsal root ganglia.
Exposure to TCE usually is accidental, although cases of intentional inhalation have been reported. Absorption takes place by inhalation, and TCE is very lipid soluble. Classification
High-level acute TCE exposure is the most common scenario. The most prominent manifestation of toxicity is trigeminal nerve dysfunction. Sensory loss involves all three trigeminal divisions, and weakness of mastication may be present. Facial, optic, oculomotor, and glossopharyngeal neuropathies have also been reported. CNS dysfunction with altered mental status and ataxia are additional manifestations of acute exposure to TCE. Although there are reports of relationship to a distal sensorimotor peripheral neuropathy, this is poorly substantiated. Chronic TCE exposure has been linked to cognitive dysfunction and peripheral neuropathy. DiagnosticTesting
TCE toxicity results in abnormalities of trigeminal somatosensory evoked potentials. Patients exposed to TCE may demonstrate abnormal electrophysiology before the onset of symptoms. TCE also has been reported to cause slowing of conduction velocity in facial, trigeminal (blink), and extremity nerves. Cell loss in the cranial nerve nuclei, axonal degeneration, and myelin degeneration has been reported in autopsy studies. Therapy
Differential Diagnosis
The short latency between exposure and onset of symptoms makes the differential diagnosis limited. Rapidly progressive GuillainBarre may be considered because that also causes autonomic failure. However, the acute diabetes caused by vacor is unique. Diagnostic Testing
The electrodiagnostic findings in vacor neuropathy have not been described. Given the loss of sensory and motor axons, the likely finding is of reduced sensory and motor potential amplitudes with abnormal EMG findings consistent with an axonopathy. Therapy
Although the precise biologic mechanism of vacor neuropathy is unclear, it can be prevented experimentally by administering nicotinamide. Residual endocrine and autonomic dysfunction are common in those who survive the acute ingestion. Motor weakness usually improves over several months. TRICHLOROETHYLENL Background
Trichloroethylene (TCE) is a solvent used in the dry cleaning and rubber production industries. It is also used as a degreasing agent, as a cleaner for photographic equipment and lenses, and in the extraction of fats and oils from vegetables. TCE previously was used as an anesthetic agent. The toxicity appears to be caused by dichloroacetylene (DCA), a metabolite, rather than TCE itself.
As with most toxins, removing the person from the exposure
source is the first step. Energetic deep breathing promotes elimination of this volatile compound. Gastric lavage should be performed in cases of ingestion. Mental status changes typically resolve rapidly, but residual facial numbness is common. Longterm follow-up has demonstrated residual facial sensory loss as long as 18 years later. ALLYL CHLORIDE Background
Ally1 chloride is a reactive halogenated hydrocarbon. Industrial chemical manufacturing uses include epoxy resins and glycerin. Absorption of allyl chloride usually is by inhalation. Classification
High-level chronic exposure to allyl chloride results in a distal symmetrical neuropathy. The presenting symptoms include distal numbness and weakness that appear gradually. Examination also reveals reduced ankle reflexes. Abnormal accumulations of neurofilaments have been demonstrated in animal studies. Ally1 chloride toxicity is another cause of central-peripheral distal axonopathy. Dlfferential Diagnosis
Other toxic neuropathies cause a similar pattern of neuropathy and cytoskeletal abnormalities, including carbon disulfide and hexacarbons. Obtaining the proper exposure history is the key.
Chapter 98
Diagnostic Testing
Toxic Peripheral Neuropathies
621
Abnormalities of nerve conduction studies include prolonged distal latencies, reduced conduction velocity, and reduced sensory and motor potential amplitudes. EMG demonstrates active and chronic denervation in distal muscles.
METHYL BROMIDE Background Methyl bromide is used in insecticides, fire extinguishers, and refrigerants. Absorption occurs by dermal contact or inhalation.
Therapy
Classification
Cessation of exposure usually results in good recovery.
Chronic, high-level exposure to methyl bromide causes multifocal neurologic dysfunction involving both the CNS and the peripheral nervous system. The pyramidal tracts, cerebellum, and mamillary bodies have been affected. High-level acute exposure may be fatal. Methyl bromide causes a distal sensorimotor polyneuropathy with onset after 3 to 7 months of exposure. Initial symptoms include paresthesias in the distal extremities followed by pain and ataxia. The optic nerves may be involved. Loss of color vision may be an early sign of toxic exposure to methyl bromide.
DIMETHYLAMlNOPROPRlONlTRlLE Background Dimethylaminoproprionitrile(DMAPN) was used as a catalyst in polymerization reactions in the production of polyurethane foams until it was discovered to be the causative agent in an outbreak of toxic axonopathy. No additional cases have been reported.
Differential Diagnosis Classification DMAPN causes a very unusual peripheral neuropathy. There are prominent urinary symptoms before the onset of sensory or motor complaints. The severity and onset of symptoms are determined by the degree of exposure. The initial symptoms include urinary hesitancy and abdominal pain. Reduced frequency of urination, decreased urinary stream, and incontinence follow. Eventually sexual dysfunction occurs with partial or complete impotence. Sensory symptoms develop in the feet at about the same time the sexual dysfunction begins. With continued exposure, sensory symptoms progress to the proximal legs and hands, and weakness develops in the distal legs. Sacral sensory loss to all modalities is common in DMAPN neuropathy. Although distal vibratory sensation is impaired, the deep tendon reflexes are surprisingly well preserved. Although the involvement of the small nerve fibers is suggested by the preservation of reflexes, autonomic features, and preferential loss of pain and temperature sensation, morphologic studies have not demonstrated this. Although bladder and sexual abnormalities are the rule, other autonomic functions are preserved. The cranial nerves are not affected.
Differential Diagnosis The differential diagnosis is primarily that of diabetic small fiber neuropathy or amyloid neuropathy.
Mercury is another toxin that has been reported to cause the combination of ataxia and other CNS dysfunction along with peripheral neuropathy.
Diagnostic Testing Electrophysiologic evaluation demonstrates a distal, motorpredominant axonopathy. Sural nerve biopsy reveals loss of large myelinated axons. Lumbar puncture reveals normal CSF.
Therapy The prognosis appears to be good in most cases. Recovery may be slow, taking 6 to 8 months in some cases.
ETHYLENE OXIDE Background Ethylene oxide (EtO) is a gas used to sterilize heat-sensitive medical equipment. EtO is also used in the production of antifreeze (ethylene glycol) and polyester fibers and polyethylene films. The primary route of exposure is via inhalation, although it can be absorbed by dermal contact or directly into the bloodstream if not allowed to evaporate completely from sterilized equipment.
Diagnostic Testing
Classificatlon
Urodynamic studies reveal bladder hypocontractility. Nerve conduction studies and EMG may be normal in mild cases of D W N neuropathy. Sensory potential amplitudes usually are reduced in the lower extremities. Motor conduction velocity may be abnormally slow in severe cases.
Acute exposure to EtO results in nausea, vomiting, headache, dizziness, and anorexia. There is also significant respiratory tract and mucous membrane irritation. EtO toxicity results in a distal sensorimotor axonopathy. The neuropathy may be seen after chronic low-level exposure or with subacute, high-level exposure. Symptoms include distal numbness and weakness, incoordination, and ataxia. Sensory loss is seen initially in the feet but begins to involve the hands with continued exposure. The weakness is also distal in onset. Deep tendon reflexes are diffusely reduced, and ankle jerks usually are absent. Chronic EtO exposure also causes CNS dysfunction. Manifestations include increased tone, dysarthria, and memory problems.
Therapy Removal from exposure is the only form of treatment. Young patients recover completely, but the prognosis is not as good in older patients. Residual bladder and sexual dysfunction are common in older adults.
622
Spinal Cord and Peripheral Neummuscular Disease rn Diseases of Peripheral Nerve
Diagnostic Testing
Electrophysiologic testing is consistent with a distal axonopathy. EMG reveals active and chronic denervation changes in distal muscles. Nerve conduction studies demonstrate low-amplitude sensory and motor potentials with normal conduction velocity or only mild slowing. Nerve conduction abnormalities may appear before the onset of symptoms in exposed patients. Sural nerve biopsy shows evidence of axon degeneration. Therapy
Removal from exposure is the only therapy. The prognosis usually is good for a gradual recovery from neuropathy once exposure is terminated. POLYCHLORINATED BIPHENYLS Background
Polychlorinated biphenyls (PCBs) have been used in electrical insulation and plasticizers. Although toxicity of PCBs has received a great deal of publicity, illnesses are more likely to be caused by impurities, not by “clean” PCBs. PCB use was banned in the 1970s, but contaminated products remain, and their disassembly may result in toxicity. PCB contamination of waterways and marine life is the most common source of exposure, but no cases of toxicity have been reported as a result of this type of exposure. Most cases of PCB toxicity reported recently have been in electrical workers removing PCB-contaminated transformers. However, an outbreak of neuropathy caused by PCB-contaminated cooking oil was reported in Taiwan. Because of their high lipid solubility, PCBs may remain in the tissues long after removal from exposure. Classification PCB exposure is associated with a distal, symmetrical sensorimotor peripheral neuropathy. Worsening of symptoms after termination of exposure has been described. It is believed that this is caused by deposition of PCBs in fat. Most patients who present with neuropathy have encephalopathy as well. Differential Diagnosis
The presentation of a subacute neuropathy with mental status changes is also seen with solvent (hexane, carbon disulfide) toxicity. Diagnostic Testing
LEAD Background
Neurologic dysfunction is a long-recognized consequence of lead exposure. Lead exposure was previously common because of widespread use of lead oxide in house paints, ceramic tableware, and toys. Tetraethyl lead was added to gasoline, and lead was used to solder metal food containers and drinking water pipes. Elimination of environmental sources of lead has dramatically decreased the incidence of lead toxicity. Exposure to lead also occurs in the industrial setting. Inorganic lead exposure has been reported in miners, solderers, cable makers, plumbers, automobile factory workers, pottery glazers, glass blowers, and workers in battery manufacturing, smelting, demolition, and automobile radiator repair. Lead exposure has also been reported to result from drinking “moonshine” whiskey, working in indoor gun firing ranges, and burning batteries for heat. Organic lead exposure results primarily from working with leaded gasoline products. Lead gains access to the tissues via ingestion, inhalation, or dermal contact.
Chronic, low-level lead exposure causes a peripheral neuropathy in adults and, rarely, in children. This neuropathy develops insidiously. Motor symptoms are prominent, and sensory signs are minimal or absent. The neuropathy causes weakness and atrophy of distal muscles, often initially involving the arms before the legs. Deep tendon reflexes are absent. Although focal deficits such as wrist and finger drop are common in early reports of lead neuropathy, it remains uncertain whether focal deficits were caused by unappreciated compression neuropathies superimposed on an underlying generalized neuropathy. Despite early concerns, it has not yet been conclusively shown that lead exposure results in amyotrophic lateral sclerosis or other progressive lower motor neuron degenerative syndromes. CNS dysfunction is a prominent component of lead toxicity. Children exposed to lead often present with an acute encephalopathy, developmental delay, loss of milestones, or long-term, mild cognitive impairment. Encephalopathy is occasionally seen in adults with acute high-level exposure and can progress to seizures, coma, or death. Ataxia, tremulousness, and choreiform movements may also indicate CNS involvement. Low-level chronic lead exposure may result in only mild cognitive or behavioral dysfunction. Lead toxicity leads to other organ system dysfunction that is usually present when the neuropathy becomes apparent. Typical effects include GI disturbance such as abdominal pain and constipation, a hypochromic microcytic anemia, and renal dysfunction. Nonspecific symptoms include weight loss and fatigue.
Electrophysiologic testing reveals slowing of conduction velocity in the sensory and motor nerves. PCB serum levels are available, but they do not correlate with the presence of neurologic symptoms and do not reflect the total body burden because PCBs are stored in fat.
The combination of a motor greater than sensory peripheral neuropathy, cognitive dysfunction, anemia, and GI symptoms suggests lead neuropathy but is also seen in porphyria.
Therapy
Dlagnostic Testing
Removal from exposure usually results in improvement. Persistent deficits are noted in most patients even several years later.
Lead levels are available in both urine and blood. Although blood lead levels are elevated after recent exposure, this is not a reflection
Differential Dlagnosis
Chapter 98
of the total body burden. Blood lead levels greater than 40 pg/lOO mL of whole blood are considered abnormal. Chelating agents increase the yield of urine lead measurement by drawing lead from the soft tissues and thereby facilitating its excretion. Twenty-fourhour urinary lead excretion of greater than 1 mg after chelation with calcium ethylenediaminetetraacetic acid (CaEDTA) is abnormal. The ratio of micrograms of lead excreted to milligrams of CaEDTA administered should not exceed 0.6. Peripheral blood smear shows a hypochromic, microcytic anemia. There may be basophilic stippling of erythrocytes. The electrophysiologic findings in lead neuropathy are somewhat controversial. Axonal and demyelinating abnormalities have been reported in nerve conduction studies. Sensory potential amplitudes are reduced, reflecting loss of sensory axons despite minimal or absent sensory symptoms and signs. Exposure to lead levels, previously felt to be safe, may lead to abnormal nerve conduction, and nerve conduction abnormalities may be present before the onset of symptoms. The degree of physiologic abnormalities correlates best with the degree of exposure. EMG reveals evidence of active denervation and chronic motor unit reinnervation, indicative of motor axon degeneration. Neuropsychological testing may reveal abnormalities of visuospatial functioning, memory, and attention.
W
Toxic Peripheral Neuropathies
623
weeks of high-level exposure. The initial manifestations are painful paresthesias, burning, tingling, and aching in the toes and feet. Early in the course of the neuropathy, reflexes are reduced or absent. Weakness follows a length-dependent pattern of evolution and in severe cases may involve the respiratory muscles. Dermatologic abnormalities and bone marrow suppression often are present along with neuropathy in cases of high-level exposure. Worsening of the neuropathy may continue for several weeks after removal from exposure (coasting). Low-level, chronic arsenic exposure causes dermatologic abnormalities before symptoms of the neuropathy. Careful neurologic examination or electrodiagnostic testing may reveal abnormalities even in the early stages before symptoms develop. Skin changes include hyperkeratosis, mucous membrane irritation, Mee’s lines (white transverse lines in the nails), and skin hyperpigmentation. Low-level chronic arsenic exposure is also associated with vague generalized symptoms such as anorexia, malaise, generalized weakness, and vomiting. Continued exposure leads to symptomatic neuropathy. Complaints usually involve burning and numbness in the feet and eventually the hands. There may be a mild sensory ataxia caused by impaired joint position sense. Weakness, if present, involves only the distal muscles.
Differential Diagnosis Therapy Prevention of further exposure is the initial step in treating lead toxicity. Lead excretion is facilitated by the chelating agents calcium EDTA, dimercaprol (British anti-Lewisite, BAL), succimer, and penicillamine. Improvement usually begins 2 weeks after initiation of chelation therapy. Although succimer and penicillamine are adequate for milder cases, combination therapy with both EDTA and BAL is necessary for more severe intoxication that includes encephalopathy. Those presenting with encephalopathy and seizures have a significant risk of death. The prognosis of lead neuropathy is good except in the most severe cases. ARSENIC Background The use of arsenic as a poison for suicide or homicide is well known. Typically, an acute, high-level ingestion occurs. However, arsenic toxicity can also be caused by chronic low-grade exposure. Toxicity caused by arsenic exposure has been reported in the occupational setting including smelting of lead and copper ore, mining, and manufacture of integrated circuits or microchips. Other sources of arsenic exposure include tainted illicit drugs, contaminated well water, and burning of preserved wood or arsenic-contaminated fossil fuels. Arsenic is absorbed from the GI tract, via dermal contact, and by inhalation (particulate arsenic and arsine gas).
Classification Acute high-level exposure to arsenic is associated with severe GI distress including vomiting, diarrhea, and abdominal pain. Prominent autonomic dysfunction with hypotension, tachycardia, vasomotor collapse, and possible death are also seen with sudden high-level exposure. High-level exposure may also cause CNS dysfunction. This can either be short-term, such as an organic psychosis, somnolence, or stupor, or more permanent in the form of cognitive and behavioral problems. Neuropathy begins within
The rapid development of distal paresthesias, areflexia, and mild weakness may be mistaken for Guillain-Barrk syndrome. However, the absence of physiologic evidence of demyelination, the associated GI symptoms, and normal spinal fluid protein allow differentiation. The associated dermatologic abnormalities, particularly in the chronic form, may also be seen with thallium exposure. Acrylamide neuropathy also is associated with skin changes, and excessive sweating in the hands and feet usually occurs. Diagnostic Testing
After exposure to arsenic, urinary levels remain elevated for weeks. A level greater than 25 pg in a 24-hour specimen is considered abnormal unless there been recent ingestion of seafood. Chronic or past exposure to arsenic is detected by testing of nails and hair. Blood arsenic levels are not reliable even in acute, high-level exposure because it is cleared from the blood in 2 to 4 hours. Electrophysiologicfindings in arsenic neuropathy are typical of a distal axonopathy. Nerve conduction studies demonstrate reduced sensory and motor potential amplitudes and mild slowing of motor conduction velocities. Needle EMG reveals some abnormal spontaneous activity and reduced motor unit recruitment.
Therapy Urinary arsenic levels can be monitored in asymptomatic patients to allow early detection of excessive exposure. As with all other toxic neuropathies, prevention is the key. Treatment in the intensive care setting is indicated because of the significant mortality rate associated with acute, high-level arsenic toxicity. Aggressive fluid and electrolyte resuscitation may be necessary with the vasomotor collapse. Arsenic elimination is aided by chelation therapy with penicillamine and BAL. Treatment should be initiated as early as possible after exposure and continued for several months. Although chelating agents often are helpful,
624
Spinal Cord and Peripheral NeuromurcularDisease W
Diseases of Peripheral Nerve
patients with severe cases may be left with significant residual dysfunction. Arsenic poisoning may also cause permanent CNS dysfunction.
THALLIUM Background The epidemiology of thallium toxicity has changed. In the past, high-level acute toxicity was most commonly caused by exposure to pesticides. Because these compounds have been eliminated from rat poisons and insecticides, occupational exposure is now more common. Although occasional reports of thallium poisoning from ingestion (either accidentally by children or intentionally by homicide or suicide) continue to surface, chronic low-level exposure is more common. Consumption of contaminated water or food may also lead to thallium toxicity. Thallium is absorbed through the GI tract, by inhalation, and through dermal contact.
DilagnostDc Testhg Sensitive methods are available that can detect microgram quantities of thallium. Levels can be measured in blood, urine, hair, and nails. The tissue that is most helpful depends on the timing of exposure relative to testing. Blood levels usually are helpful only acutely and do not reflect the total body burden. In cases where the baseline blood and urine thallium levels are normal, a challenge with potassium chloride causes an increase in urinary excretion. Hair and nails are the most sensitive indicators of chronic exposure or exposure that has since ceased. Nerve conduction studies reveal reduced sensory potential amplitudes caused by loss of large sensory fibers. There is usually mild conduction velocity slowing. Evidence of active denervation and chronic motor unit reinnervation is seen with EMG. Serial electrophysiologic testing can be used to monitor the severity of the peripheral neuropathy. The CSF protein is normal in cases of thallium neuropathy.
Therapy The presentation of thallium toxicity depends on the level and duration of exposure. Acute, high-level exposure leads to abdominal pain, diarrhea, and vomiting within hours. CNS manifestations include lethargy or coma. Thallium intoxication may also cause cardiac and respiratory failure. The neurologic or cardiopulmonary dysfunction may progress to death. Although alopecia is felt to be the classic sign of thallium intoxication, it is not specific for thallium and is not helpful in the acute setting. Alopecia is not invariably present and, when seen, appears 15 to 39 days after exposure. Thallium intoxication results in a distal, symmetrical polyneuropathy with symptoms developing in 2 to 5 days. Intense joint pains and burning paresthesias in the distal legs are the first complaints. Large and small sensory fibers are affected, and the neuropathy occasionallycan involve the hands or trunk. Although motor symptoms are unusual, careful examination often reveals mild, distal weakness. Subacute toxicity is seen with lower-level thallium exposure. Dermatologic manifestationsare prominent in this setting, including white striae of the nails (Mee’s lines), alopecia, and hyperkeratosis. The onset of neuropathy is delayed at least a week after exposure in subacute thallium toxicity. Pinprick sensation, light touch, and joint position sense are prominently affected. Gait difficulty early in the course is caused primarily by painful paresthesias in the feet. The tendon reflexes usually are preserved relative to the degree of sensory loss. Some distal weakness may be detected, but this is also mild. Autonomic nervous system dysfunction may lead to tachycardia or hypertension. Other reported neurologic manifestations with subacute thallium toxicity include cranial neuropathies, ataxia, and chorea. Chronic low-level thallium exposure is the least common scenario. This causes a neuropathy that is identical to that described earlier.
Differential Diagnosis Acute thallium neuropathy presenting with distal paresthesias and mild weakness may be confused with Guillain-Barr6 syndrome. However, weakness tends to be mild, and thallium intoxication causes prominent GI symptoms. Arsenic and thallium also cause GI symptoms, alopecia, and other dermatologic manifestations. They also result in painful neuropathy and autonomic dysfunction, making differentiation difficult.
Thallium toxicity can be prevented by avoiding exposure. Helpful measures include good personal hygiene, protective clothing, and enforcement of established workplace exposure levels. Thallium has an elimination half-life of 30 days. However, GI excretion may be enhanced by treatment with laxatives, Prussian blue, and activated charcoal. Administration of potassium chloride and forced diuresis promote renal excretion. Acute thallium intoxication often leads to permanent dysfunction. Residual CNS dysfunction can result from anoxic injury. There is usually a slow recovery from the acute neuropathy, but sensory deficits persist. Subacute thallium neuropathy has a more favorable prognosis for complete recovery. Full recovery from the neuropathy occurs within 6 months in most cases. Hair growth usually begins within 10 weeks of discontinuing exposure.
MERCURY Background Mercury intoxication became well known after large outbreaks. The Minamata Bay incident in Japan, caused by consumption of contaminated fish, is well documented. Another incident involved application of a fungicide containing organic mercury to grain in Iraq. Elemental mercury is a silver-colored liquid at room temperature. It is used in gauges such as barometers and thermometers. Inorganic mercurial salts and elemental mercury are present in dental amalgam, in the manufacture of chlorine, and in the natural gas industry. Organic mercurial compounds are used as industrial catalysts and as preservatives in latex paints. They are also found in disinfectants. Elemental mercury vapor is absorbed by inhalation. Organic mercury usually is absorbed through the GI tract. Mercury salts are absorbed through the skin and GI tract. Although studies have shown that those with mercury amalgam dental fillings inhale some mercury vapors, no clear relationship has been documented between dental fillings and any type of toxicity or disease process.
Although CNS dysfunction is the most prominent manifestation of mercury intoxication, there are some reports of peripheral
Chapter 98
nervous system effects. The form of mercury to which the patient is exposed determines the pattern of CNS dysfunction and the nature of systemic symptoms. Elemental mercury causes CNS toxicity without significant systemic illness because of its high lipid solubility. Micromercurialism is low-level elemental mercury toxicity. Symptoms are very nonspecific and include anorexia, tremor, fatigue, weight loss, and some GI dysfunction. Higher levels of elemental mercury exposure cause a severe tremor that may involve the head, face, and eyelids. Weakness and Babinski signs are also features of elemental mercury toxicity. Other symptoms include insomnia, hyperexcitability, and personality change. Exposure to mercury vapor leads to prominent neuropsychological dysfunction and irritation of the upper respiratory tract. Mercury salts also cause mental and psychiatric impairment. The expression “mad as a hatter” stems from the use of these salts in the felt of hatbands, causing behavioral and cognitive dysfunction. Mercury salts also cause renal failure and GI dysfunction. Organic mercurial toxicity is associated with sensory ataxia. This is caused by damage of sensory neurons in the dorsal root ganglion. Although the onset may be heralded by distal paresthesias, this is not caused by peripheral nerve damage. The paresthesias later progress to involve more proximal areas including the tongue. Organic mercurial compounds have varying effects depending on their structure. Complex organic mercury compounds are more likely to cause nephrotoxicity. Short-chain compounds such as methyl mercury cause tremor, hearing loss, constriction of visual fields, mental impairment, and dysarthria with prolonged exposure. A sensorimotor neuropathy has been described with exposure to all forms of mercury. The evidence for neuropathy caused by elemental mercury or mercuric salts is more substantial than that caused by organic mercurial exposure. Differential Diagnosis
Exposure to mercury vapor results in upper respiratory tract irritation and an acute neuropathy. The respiratory irritation may be mistaken for a viral infection and the ensuing acute neuropathy mistaken for Guillain-Barri syndrome. Diagnostic Testing
Laboratory studies that may be useful for investigating mercury intoxication include levels in the blood, urine, and tissues. Mercury blood levels are elevated in acute exposure. Long-term toxicity is assessed by mercury levels in hair samples or serial urine measurements after penicillamine administration. Neurophysiologic testing reveals an axonal neuropathy with predominant motor involvement. Peripheral neuropathy can be detected in those exposed to mercury while they are still asymptomatic.
Toxic Peripheral Neuropathies
625
Therapy
Prevention of mercury toxicity involves educating those at risk. Other measures inciude monitoring airborne levels and using protective devices. Mercury intoxication is treated primarily by removal from exposure. Chelating agents such as BAL and penicillamine increase urinary excretion of mercury. However, it is unclear whether this speeds the recovery process. The prognosis for a complete recovery is good in most cases of mercury intoxication. However, there may be residual neurologic dysfunction as long as 30 years later.
SELECTED READINGS Abou-Donia MB, Ibrahim SM, Corcoran JJ et ak Neurotoxicity of glycidamide, an acrylamide metabolite. J Toxicol Environ Health 39447-464, 1993 Albers JW, Kallenbach LR, Fine LJ et al: Neurological abnormalities associated with remote occupational elemental mercury exposure. Ann Neurol 24651459, 1988 Chu CC, Huang CC, Chen RS, Shih TS: Polyneuropathy induced by carbon disulfide in viscose rayon workers. Occup Environ Med 52:404-407, 1995 DeBleecker J: The intermediate syndrome in organophosphatepoisoning: an overview of experimental and clinical observations. Clin Toxicol 33:683486, 1995 Feldman RG: Occupational and Environmental Toxicology. LippincottRaven, Philadelphia, 1999 Gross JA, Haas ML, Swift T F Ethylene oxide neurotoxicity: report of four cases and review of literature. Neurology 29:97&983, 1979 Herskowitz A, Ishii N, Schaumburg H: n-Hexane neuropathy: a syndrome occurring as a result of industrial exposure. N Engl J Med 285:82-85, 1971 Heyman A, Pfeiffer JB,Taylor H M Peripheral neuropathy caused by arsenical intoxication: a study of 41 cases with observation on the effects of BAL (2,3-dimercapto-propanol).N Engl J Med 254401-409, 1956 Letz R, Gerr F, Cragle D et al: Residual neurologic deficits 30 years after occupational exposure to elemental mercury. Neurotoxicology 21(4): 459474,2000 Nordentoft T, Anderson EB, Morgensen PH: Initial sensorimotor and delayed autonomic neuropathy in acute thallium poisoning. Neurotoxicology 19:421-426, 1998 Schaumburg HH, Spencer PS: Clinical and experimental studies of distal axonopathy: a frequent form of nerve and brain damage produced by environmental chemical hazards. Ann NY Acad Sci 329:14, 1979 Schaumburg HH, Spencer PS: Recognizing neurotoxic disease. Neurology 37:276-278, 1987 Seppalainen AM, Tola S, Herberg S, Kock B Subclinical neuropathy at “safe” levels of lead exposure. Arch Environ Health 30180-183, 1975 Wadia RS, Sadagtopan C, Amin RB, Sardesai HV Neurological manifestations of organophosphorus insecticide poisoning. J Neurol Neurosurg Psychiatry 328414347, 1974
626
99
Spinal Cord and Peripheral Neuromuscular Disease rn Diseases of Peripheral Nerve
Drug-Induced Peripheral Neuropathies Janice E Wiesman and Robert G. Feldman
Peripheral neuropathy is a side effect of many medications, both prescription and over the counter (Table 99-1). When a patient presents with symptoms consistent with peripheral neuropathy, a detailed medication history is needed. Drug-induced neuropathy is more common in patients who are predisposed to neuropathy secondary to concomitant conditions such as diabetes mellitus, alcohol use, metabolic abnormalities (e.g., renal insufficiency), nutritional deficiencies, and chemical exposures. Typically, these neuropathies are axonal in nature and are dose dependent. Often, resolution is seen upon discontinuation of therapy. The mechanisms of drug-induced neuropathy include interference with microtubule formation and axonal flow, nutritional deficits, lipidosis, and impaired Schwann cell function (Table 99-2). This chapter provides a description of commonly encountered medications that are associated with peripheral neuropathy.
Peripheral neuropathy has been reported in up to 10% of patients undergoing long-term treatment. Central nervous system manifestations have also been reported. A reversible syndrome including ataxia, tremor, and occasional peripheral neuropathy was noted in 54% of patients in one study. Both peripheral and central nervous system symptoms typically resolve with discontinuation of the drug. Amiodarone’s toxic effect on nerves may be secondary to a drug-induced lipidosis. Amiodarone is an amphophilic drug that can bind to lipids and penetrate lysosomes in a manner similar to perhexiline and chloroquine. In contrast to the latter two, which produce a demyelinating neuropathy, the pathologic picture in amiodarone neuropathy is heterogeneous. Surd nerve biopsy has yielded a variable picture of the pathologic changes seen with amiodarone neuropathy. Primarily axonal, mixed axonal and
ALLOPURINOL Allopurinol is a xanthine oxidase inhibitor that reduces the production of uric acid. It is used to treat gout. Reports of neuropathy after long-term use are rare, and some authors question an association. Electrophysiologic evidence of both axonal and demyelinative components has been noted. Improvement occurs after withdrawal of the drug.
ALMlTRlNE Almitrine bismesylate is a selective pulmonary vasoconstrictor used to treat chronic obstructive pulmonary disease. A painful sensory neuropathy with numbness and paresthesia may develop months to years after the onset of treatment. It is often associated with weight loss, which itself may be a side effect of the drug. Recovery is typical after discontinuation but may be very slow. This has been attributed to the long half-life of the drug. Sural nerve biopsy shows axonal loss predominantly affecting large-diameter fibers; unmyelinated fibers are affected to a lesser degree. The cause of the neuropathy is thought to be toxic. High plasma concentrations have been reported in patients with neuropathy. The drug is metabolized by an oxidative reaction. In a group of patients with almitrine-induced polyneuropathy, all were found to be of the rapid metabolizer type. This is in contrast to patients with perhexiline-induced neuropathy, who are typically slow oxidizers. Hypoxia itself can cause a mild peripheral neuropathy, but almitrine neuropathy has been noted in patients without evidence of chronic hypoxia.
AMIODARONE Amiodarone is a class I11 antiarrhythmic agent that is associated with optic neuropathy (Table 99-3) and, less commonly, a sensorimotor or a predominantly motor peripheral neuropathy. Optic neuropathy is manifested by the insidious onset of slowly progressive bilateral, painless visual loss. This is in contrast to ischemic optic neuropathy, which tends to be acute, unilateral, and painful. Symptoms may be unilateral or bilateral and may include blurred vision, visual field abnormalities, and edema of the optic disk.
W TABLE 99-1.
Drug-Induced Neuropathies
Sensorv
Sensow-Motor
Motor
Alrnitrine Cytarabine Chloramphenicol Cisplatin Metronidazole Misonidazole Paclitaxel Pyridoxine Reverse transcriptase inhibitors Thalidornide
Arniodarone Aurothioglucose Colchicine Disulfiram Etharnbutol HMC-CoA reductase inhibitors Hydralazine lsoniazid Nitrofurantoin Perhexiline Phenytoin Surarnin Vinca alkaloids Zimeldine
Dapsone
W TABLE 99-2.
Pathology of Drug Induced Neuropathy
Axonal
Demyelinative
Mixed
Aurothioglucose Cisplatin Colchicine Cytarabine Dapsone Disulfirarn Etharnbutol HMC-CoA reductase inhibitors lsoniarid Metronidazole Nitrofurantoin Paclitaxel Perhexiline Reverse transcriptase inhibitors Vinca alkaloids
Zimeldine
Allopurinol Arniodarone Chloroquine Phenytoin Suramin
W TMLE 99-3.
Drugs Associated with Optic Neuropathy Arniodarone Chlorarnphenicol Disulfirarn Etharnbutol
Chapter 99
demyelinative and primarily demyelinativeneuropathies have been described. Lamellated lysosomal inclusion bodies are seen in Schwann cells, capillary endothelial cells, and muscle fibers. Similar lysosomal inclusions are also seen in perhexiline neuropathy, a demyelinative neuropathy. As predicted from the pathology, electromyography and nerve conduction studies have reported patients with axonal loss, patients with primarily demyelinative changes, and patients with a mixed neurophysiologic picture.
AUROTHIOCLUCOSE AND SODIUM AUROTHIOMALATE (GOLD) Aurothioglucose and sodium aurothiomalate are gold-containing compounds used to treat rheumatoid arthritis for more than 70 years. The mechanism of action is unknown. Dermatologic reactions are the most common side effect and are seen in approximately 15% of patients. Sensorimotor neuropathy is uncommon, with the incidence estimated at 0.5%. Symptoms may begin a few months after the start of treatment. Clinical manifestations include the typical paresthesias, numbness, and distal weakness but also include the unusual finding of myokymia. Neuropathy may present as an isolated symptom or in the company of immune-mediated signs such as rash and fever. Cerebrospinal fluid protein may be elevated. In an animal model, occurrence of neuropathy was found to be dose related. Recovery with cessation of therapy is the rule. Cranial neuropathies and encephalopathy have also been noted. Dimercaprol has been used to treat some complications of gold therapy but has not been useful in treating neuropathy. Sural nerve biopsy demonstrates either predominantly axonal degeneration involving all fiber types or predominantly segmental demyelination. It is not clear whether the demyelination is primary or secondary to axonal degeneration. Two mechanisms of action have been proposed: an autoimmune response or a direct toxic effect on the axon or cell body.
CHLORAMPHENICOL Chloramphenicolis an antibiotic used to treat a broad spectrum of bacterial infections including Salmonella typhi and ampicillinresistant Huernophilus influenzue. The risk of agranulocytosis and the availability of newer antibiotics have limited its use. Prolonged use of chloramphenicol has been associated with both optic neuropathy and a sensory neuropathy, with optic neuropathy being more common. Clinical manifestations of optic neuropathy may include loss of visual acuity, central scotoma, constriction of visual fields, and red-green dyschromatopsia. Funduscopic examination reveals peripapillary edema and hemorrhages around the optic nerve head. Neuropathy typically is seen after months of high-dose treatment. Chloramphenicol used in short courses is safer and less likely to induce neuropathy. Recovery typically is complete when the medication is discontinued, but residual deficits may be seen in some patients. Chloramphenicol inhibits mitochondrial protein synthesis. This toxic effect is attenuated by antioxidants, suggesting that the process is mediated, in part, by reactive oxygen species that may induce cell death. Interference with B vitamin-mediated processes has also been proposed as a possible mechanism of neurotoxicity. Impaired excretion of chloramphenicol caused by renal insufficiency may increase the risk for neurotoxic effects.
Drug-Induced Peripheral Neuropathies
627
CHLOROQUINE Chloroquine is used for both prophylaxis and treatment of malaria and in a variety of connective tissue and dermatologic diseases. It is an amphophilic substance, similar to amiodarone and perhexiline. Chloroquine is associated with the development of peripheral neuropathy. Clinical manifestations include loss of deep tendon reflexes; pain, paresthesias, and numbness typically are not present. Electrophysiologic abnormalities such as reduced motor unit number with increased motor unit size have been reported and attributed to axonal loss. Paradoxically, a report of sural nerve pathology described segmental demyelination and remyelination with lamellated, cytoplasmic inclusions in Schwann cells and perineurial and endoneurial cells. Axons were not affected. Generalized myopathy and cardiomyopathy are more familiar side effects of chloroquine. Myopathy presents with painless proximal muscle weakness. Electromyographic abnormalities are similar to those seen in polymyositis with small, easily recruited motor units and fibrillation potentials. Muscle pathology is significant for vacuolar degeneration of muscle fibers. The mechanism of neurotoxicity has not been fully elucidated, but inhibition of lysosomal enzyme activity probably is involved. The clinical manifestations resolve after the drug is discontinued.
CISPLATIN (PLATINUM) Cisplatin is a heavy metal complex containing platinum that is used to treat various solid tumors. It functions in a manner similar to alkylating agents, producing crosslinks in DNA. A predominantly large fiber, axonal, sensory neuropathy is common and may be severe with routine dosages. Neuropathy has been noted with standard dosing regimens and intra-arterial treatment. For systemic administration, an average total dosage of 500 mg/m’ has been reported as the threshold for development of neuropathy. Ototoxicity and neuropathy are dose-limiting side effects. Occasionally, neuropathy manifests after treatment is completed. Decreased vibration and joint position sense with lesser degrees of pain and temperature loss account for the typical clinical picture of difficulty with balance and sensory ataxia. Weakness occurs in severely affected patients. Even in patients with no symptoms, vibration threshold is elevated, and proprioception is diminished. Symptoms may improve after the drug is discontinued, but persistent abnormalities consistent with neuropathy are the rule. Electrophysiologic testing reveals decreased sensory amplitudes and mildly decreased conduction velocities consistent with axonal loss. Results of motor nerve conduction studies and electromyography may be normal. On nerve biopsy, degeneration of unmyelinated and myelinated fibers is seen along with secondary demyelination. Large fibers are preferentially affected. Damage to the posterior columns was seen at autopsy in a patient with severe neuropathy.
COLCHICINE Colchicine is an alkaloid agent obtained from the root of members of the genus Colchicum, a plant in the lily family. It is used to treat gout and primary biliary cirrhosis. Colchicinebinds to tubulin and blocks axonal transport in a way similar to that of the vinca alkaloids (Table 99-4).
628
Spinal Cord and PeripheralNeuromuscular Disease
Diseases of PeripheralNerve
TABLE 99-4. Drugs That Interfere with Axonal Transport Colchicine Doxorubicin Paclitaxel Vinca alkaloids
Vacuolar myopathy is more common than the mild, axonal sensorimotor neuropathy that is seen occasionally. Symptoms typically start in the hands with numbness and paresthesias and are later noted in the feet. This pattern of symptom onset is typical of that seen with agents that interfere with axonal transport. Distal muscle atrophy and weakness follow. Creatinine phosphokinase usually is elevated; this may be on the basis of myopathy or motor axon loss. Onset of myoneuropathic symptoms is usually subacute, but acute onset has been reported in cardiac transplant recipients treated with colchicine for cyclosporin-induced gout. Decreased clearance in the presence of renal insufficiency may be associated with the development of neurotoxicity. Resolution of clinical and electromyographic abnormalities is seen with discontinuation of the drug. Nerve conduction studies show a mildly decreased velocity in both sensory and motor nerves. Electromyography reveals features of myopathy as well as fibrillation potentials and positive waves, pointing to motor axon loss. Muscle biopsy does not show inflammation; rather, sarcoplasmic vacuolar degeneration is seen. This vacuolation is similar to that seen with vinca alkaloids. Fiber type grouping, secondary to axonal loss, is also seen. Sural nerve biopsy is consistent with an axonal neuropathy affecting large myelinated fibers most severely.
WTARABINE (AM-C) Cytosine arabinoside is used to treat hematologic malignancies. The mechanism of action is thought to be related to inhibition of DNA polymerase. Its most common toxicities are myelosuppression and gastrointestinal distress. Occasionally, an axonal, sensory neuropathy is precipitated by use of intravenous cytarabine. The neuropathy may be mild or severe and may be accompanied by pain in the lower extremities and “moving toes,” probably a manifestation of the sensory neuropathy. Recovery is incomplete after discontinuation of the drug. Other neurologic complications include myelopathy when administered intrathecally, a necrotizing leukoencephalopathy when combined with brain irradiation and seizures, or an acute cerebellar syndrome when given intravenously. There is a single case report of a man who developed a brachial plexopathy on two occasions within hours of being given intravenous, high-dose cytarabine.
DAPSONE Dapsone is a sulfone antibacterial agent used to treat leprosy, Crohn’s disease, and certain dermatologic conditions (i.e., dermatitis herpetiformis, pyoderma gangrenosum, and cystic acne). Hemolytic anemia and neuropathy have been reported in patients as adverse effects of dapsone treatment. A predominantly motor neuropathy, though uncommon, is the major neurologic complication of therapy. Symptoms may develop from months to years after treatment begins, but the usual time of onset is within 5 years. Distal muscle atrophy and weakness in the upper and lower extremities are noted. Paresthesias without
objective sensory loss may be present. Deep tendon reflexes usually are preserved but may be hypoactive. This constellation of symptoms and signs is seen in patients without leprosy and so distinguishes a medication effect from the peripheral neuropathy that may be associated with leprosy. Recovery occurs when the therapy is discontinued, which also points to a drug effect. Electrophysiologic and biopsy studies demonstrate axonal loss. Motor nerve conduction studies show a reduced or absent compound muscle action potential with a normal or slightly reduced conduction velocity. Sensory studies are normal. Electromyography shows a loss of motor units with fibrillation potentials and positive waves. Motor nerve biopsy shows axonal loss. Dapsone, like isoniazid, is metabolized by acetylation. N-Acetyltransferase polymorphisms may be of clinical consequence, increasing the susceptibility of slow acetylators to peripheral neuropathy and other toxic effects induced by dapsone.
DlSULFlRAM Disulfiram is a dithiocarbamate compound that is used as an aversive method to discourage alcohol consumption. It blocks alcohol metabolism, resulting in acetaldehyde accumulation, which produces a number of unpleasant symptoms including headache, gastrointestinal distress, and diaphoresis. A sensorimotor neuropathy has been reported to occur weeks to months after initiation of therapy. Paresthesias, decreased sensation to all modalities, and weakness are noted initially in the feet and later the hands. Distal deep tendon reflexes are absent or diminished. The subacute onset of symptoms in patients who are well nourished and their resolution on withdrawal of the drug point to a medication effect as opposed to a sequela of chronic alcohol use. The development of neuropathy appears to be dose dependent; neuropathy is rare with dosages of less than 250 mg/day. Recovery after discontinuation of therapy is the rule; however, a case of severe, fulminant, irreversible neuropathy has been reported in a woman who ingested ethanol with a large dose of disulfiram. Optic neuropathy and encephalopathy that may or may not be accompanied by neuropathy have been described. Surd nerve action potentials are absent or low in amplitude, whereas motor conduction studies show mildly to moderately reduced conduction velocity with reduced compound muscle action potential amplitude. Electromyography reveals abnormal spontaneous activity. Electrophysiologic parameters return to normal after treatment is stopped. Nerve biopsy is consistent with axonal pathology, with evidence of regeneration of fibers in a biopsy taken during the recovery phase. Disulfiram is metabolized to carbon disulfide, which is a known neurotoxin. Disulfiram affects Schwann cells and disrupts axonal transport. Electron microscopy discloses axons distended by accumulation of neurofilaments, similar to the changes seen in experimental carbon disulfide exposure.
DOXORUBICIN Doxorubicin is an anthracycline antibiotic used as a chemotherapeutic agent. Its mechanism of action is interference with protein synthesis by intercalation into nuclear DNA. It passes easily into the dorsal root ganglia and interferes with protein synthesis by sensory neurons. This disrupts both fast and slow anterograde axonal transport. Interference with transport and neuronal loss in both motor and sensory systems has been produced in experimen-
Chapter 99 H Drug-Induced Peripheral Neuropathies
tal animals. There have been no reports of clinical neuropathy in humans using doxorubicin, possibly because of dose-limiting toxicities on the heart, kidney, and hematopoietic system.
ETHAMBUTOL Ethambutol hydrochloride is an antimycobacterial agent used to treat tuberculosis. Optic neuropathy, probably on the basis of a derangement of mitochondrial metabolism, is the most common neurologic side effect. Symptoms include reduced visual acuity, central scotoma, dilated retinal veins, and fundal hemorrhage. It occurs at standard dosages and is typically reversible with discontinuation of treatment, but permanent visual loss has been described, particularly in patients older than 60 years. There may also be a higher risk in patients with renal insufficiency. Fibers subserving macular vision are preferentially affected. Concurrent treatment with isoniazid increases the risk of optic neuropathy, suggesting that disruption of B vitamin-mediated processes may also be involved. A sensorimotor peripheral neuropathy, involving both small and large fibers, is much less common. This usually improves with discontinuation of the drug. Motor nerve biopsy studies in an experimental rat model demonstrated axonal loss and regeneration. Pathology was noted in both proximal and distal nerve segments.
ANTI-HIV MEDICATIONS Nucleoside analogue reverse transcriptase inhibitors including didanosine (ddI), lamivudine (3TC), stavudine (d4T), zalcitabine (ddC), and zidovudine (ZDV, formerly AZT) are used to treat human immunodeficiency virus (HIV) infection. All but ZDV have been implicated as the cause of a predominantly sensory, axonal, painful peripheral neuropathy. Neuropathy is more common with ddI and ddC than with 3TC and d4T. Neuropathy often is the dose-limiting side effect. Because peripheral neuropathy is a complication of HIV infection, it is often difficult, but important, to determine whether neuropathy is caused by medication or is a result of HIV infection. Incidence, severity, and progression of peripheral neuropathy upon exposure to these medications is a function of the following factors: stage of immunosuppression (CD4 count), dosage of medication, duration of treatment, and preexisting risk factors for neuropathy. Patients with low CD4 cell counts are at greater risk to develop neuropathy with these medications. Zidovudine is known to cause a mitochondrial myopathy, and this may complicate the diagnosis of neuropathy. Symptoms include painful distal paresthesias and numbness starting in the lower extremities and spreading proximally, eventually including the upper extremities. On examination, abnormalities of temperature, light touch, vibratory sensation, and joint position sense are found. Ankle reflexes are absent. Discontinuation of the medications or a decrease in dosage typically leads to partial resolution of symptoms, whereas a neuropathy associated with the infection will continue to progress. When ddI or ddC are withdrawn, patients may experience a worsening of symptoms lasting a few weeks before symptoms begin to resolve. This has been called coasting. The agents differ in their propensity to cause neuropathy. With ddC monotherapy, 25% to 65% percent of patients develop neuropathy. With ddI monotherapy, the number is 12% to 34%; with d4T,
629
30% to 50%. Combining the drugs increases the incidence of neuropathy. Electrophysiologic testing demonstrates a sensory greater than motor, axonal neuropathy. In cell culture, neural cells exposed to ddI, ddC, and d4T demonstrated a dose-dependent inhibition of neurite regeneration. This was not seen with exposure to 3TC or ZDV. One mechanism of nerve damage is thought to be inhibition of mitochondrial DNA synthesis, but the existence of other mechanisms has also been proposed. In a rodent model, exposure to dd1 resulted in myelin splitting and intramyelin edema in sciatic nerve. There have been no reports of peripheral neuropathy caused by the use of protease inhibitors to treat HIV infection.
HMG-COA REDUCTASE INHIBITORS HMG-CoA reductase inhibitors are used to treat hypercholesterolemia and hyperlipidemia. This class of medication is typically associated with myopathy but there is a growing literature describing an association with neuropathy. This may occur in up to 10% of patients who are treated for more than 2 years. Symptoms improve with cessation of the drug and recur with re-exposure. Electrophysiological testing is consistent with an axonal, sensorimotor neuropathy. Surd nerve biopsy in one patient revealed axonal degeneration. The mechanism of damage is not known but may be related to a disturbance of axonal membrane function due to decreased cholesterol synthesis. Alternatively, these drugs may interfere with neuronal energy utilization through a known inhibition of ubiquinone, an enzyme in the mitochondrial respiratory chain.
HYDRAWINE Hydralazine is an antihypertensive agent that relaxes arteriolar smooth muscle. It is also used to treat congestive heart failure and preeclampsia. Rarely, it has been associated with a sensorimotor neuropathy. Manifestations include distal paresthesias and numbness along with mild distal weakness in some cases. As with isoniazid and phenelzine, the mechanism probably is related to vitamin B, depletion (Table 99-5). Hydralazine has been shown to inactivate pyridoxine and enhance its excretion. Administering pyridoxine during treatment may prevent neuropathy. The occurrence of neuropathy may be more likely in patients who are slow acetylators (Table 99-6). Complete recovery usually occurs after withdrawal of hydralazine.
TABLE 99-5. Drugs That Cause Vitamin B, Depletion Hydralazine lsoniazid PheneIzine
TABLE 99-6. Drugs with Greater Risk of Causing Neuropathy in Slow Acetylators Dapsone Hydralazine lsoniazid Perhexiline
630
Spinal Cord and peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
ISONIAZID Isoniazid is the hydrazide of isonicotinic acid. It is used to treat tuberculosis and HIV infection. Its therapeutic value results from its ability to block the synthesis of mycolic acids, which are components of the mycobacterial cell wall. A sensorimotor neuropathy may be seen soon after isoniazid therapy is initiated. Distal paresthesias and numbness are noted initially, followed by painful paresthesias and weakness if the drug is continued. The neuropathy resolves quickly if the medication is stopped at the first sign of symptoms. If the medication is continued and pain and weakness develop, recovery, though usually complete, occurs more slowly. Acute isoniazid overdose results in encephalopathy, seizures, and a subsequent peripheral neuropathy. Sural nerve biopsy demonstrates axonal degeneration of both myelinated and unmyelinated fibers. Motor nerve conduction studies show a prolongation of distal latency, reduced evoked response amplitude, and mildly decreased conduction velocity. Axonal degeneration occurs secondarily to a pyridoxinedeficient state created by the medication. Isoniazid inhibits the activity of pyridoxal phosphokinase. This results in decreased levels of pyridoxal phosphate, which normally serves as a coenzyme in decarboxylation and transamination of amino acids and metabolism of fatty acids. Isoniazid also combines with pyridoxine, resulting in increased excretion of the vitamin. Concurrent pyridoxine administration may prevent neuropathy. Isoniazid is metabolized by acetylation, and patients who are slow acetylators accumulate the drug and are at greater risk of neuropathy. Acetaldehyde, a metabolite of ethanol, has been shown to deplete vitamin B,; therefore, concurrent use of ethanol increases susceptibility to the neurotoxic effects of isoniazid. METRONIDAZOLE Metronidazole is used to treat anaerobic bacterial and protozoal infections as well as Crohn’s disease. It is a nitroimidazole compound, as is misonidazole. Common side effects include headache, gastrointestinal distress, and dry mouth. Neuropathy is unusual, usually occurring after prolonged exposure, and when it occurs it is sensory in nature. Both large- and small-fiber modalities are affected. Distal paresthesias and numbness begin in the feet and are later noted in the fingers. Distal tendon reflexes may be reduced or absent. Distal atrophy and weakness are not common. Symptoms improve upon discontinuation of the drug. In Crohn’s disease, neuropathy caused by metronidazole must be distinguished from the axonal neuropathy associated with the disease itself and from symptoms associated with vitamin B,, deficiency. Sensory nerve conduction studies show absent responses in the lower extremities and small-amplitude responses in the upper extremities. Motor nerve conduction studies typically are normal. Surd nerve biopsy studies support the electrophysiologic findings and reveal a primary axonopathy with loss of both myelinated and unmyelinated fibers. The mechanism of damage is not known. MISONIDAZOLE Misonidazole is a nitroimidazole compound that is used as a hypoxic cell radiosensitizer in treating malignant neoplasms. A painful sensory neuropathy often is the dose-limiting side effect. Electrophysiologic and histologic studies in humans are consistent with an axonal neuropathy with differential loss of large
fibers and secondary demyelination. In a small study looking at the protective effect of dexamethasone on the development of neuropathy, patients concurrently given dexamethasone had a lower incidence of neuropathy than those who received misonidazole alone. In neuron cell culture, misonidazole exposure resulted in changes in neurofilament proteins and loss of neurite projections. Electron microscopic study of biopsied nerve has shown axonal swelling with increase in neurofilaments. NITROFURANTOIN Nitrofurantoin is a wide-spectrum antibiotic used specifically for urinary tract infections. Sensorimotor neuropathy is uncommon. When it occurs, onset may be rapid, and the neuropathy may become severe and irreversible if the drug is not discontinued immediately. Patients typically complain of distal paresthesias and weakness beginning in the lower extremities and, if the medication is continued, progressing to the upper extremities. Examination may reveal diminished vibration sensation and reduced or absent deep tendon reflexes. Muscle atrophy may be seen in severe cases. Occasionally, a predominantly motor neuropathy occurs. Prognosis depends on the severity of the neuropathy. Of 92 patients on whom the results of follow-up examination were reported, 34 showed full clinical recovery, 45 showed improvement with residual sequelae, and 13 showed no improvement. Renal excretion is the primary route of elimination, so renal insufficiency may predispose to the development of neuropathy. In some patients it may be difficult to distinguish between the two causes. Because subacute neuropathy may exist in patients with uremia, use of nitrofurantoin should be avoided in the presence of renal failure. Older women using nitrofurantoin appear to be more susceptible than other groups to developing neuropathy. Despite these findings, a clear dose-response relationship has not been established. Electrophysiologic studies of patients with nitrofurantoininduced neuropathy revealed evidence of axonal loss and demyelination, including sensory nerve action potentials that are absent or reduced in amplitude, slowed motor nerve conduction velocities, and prolonged distal motor latencies. Electromyography may reveal fibrillation potentials and positive waves indicative of denervation of distal and proximal muscles as well as a decreased number of motor units in distal muscles. Mild abnormalities consistent with axonal loss have been demonstrated on electrophysiologic testing in asymptomatic patients using nitrofurantoin. Severe axonal degeneration has been reported with light and electron microscopic investigation. Autopsy examination of a severely affected patient showed degeneration of spinal roots and abnormalities of anterior horn and dorsal root ganglion cells. Nitrofurantoin may be directly toxic to neurons. It has been suggested that nitrofurantoin interferes with cellular energy metabolism. Although the mechanism of damage is not known, inhibition of acetyl-coenzyme A and disruption of pyruvate metabolism has been proposed. Toxic metabolites, such as semicarbazide, which has been shown to cause neuropathy in rats, have been proposed. PACLITAXEL Paclitaxel is a chemotherapeutic drug in the taxane family used to treat cancers of the breast and lung. It acts by binding to tubulin and interfering with mitosis.
Chapter 99 W
Paclitaxel causes a dose-dependent, predominantly sensory neuropathy that is not associated with axon length. Paresthesias typically begin in the hands and feet together. Loss of tendon reflexes, elevated vibratory threshold, and sensory ataxia follow. If treatment continues, small-fiber sensory modalities and motor function are impaired. Patients with diabetes, heavy alcohol use, and exposure to other chemotherapeutic agents that cause neuropathy are particularly susceptible to developing neuropathy with the use of paclitaxel. In some studies, 90% of patients receiving standard dosages noted symptoms. Symptoms can occur after a single standard dose. Sensory nerve conduction velocity and evoked response amplitudes are decreased. Motor nerve parameters may be normal. Histopathologically,axonal degeneration and secondary demyelination characterize the neuropathy. Large fibers are affected preferentially. In a rat model, degeneration of dorsal root ganglion cells was noted. The effect was thought to be that of a neuronopathy as opposed to a length-dependent axonal neuropathy. Paclitaxel binds to tubulin and interferes with microtubule dynamics by stabilizing tubules and preventing their depolymerization, thereby leading to mitotic arrest in dividing cells. Axonal degeneration in peripheral nerves is secondary to decreased axonal transport. This is similar to what is seen with colchicine and the vinca alkaloids. Studies of concurrent administration of glutamine or insulin-like growth factor for the prevention of neuropathy in patients treated with paclitaxel are under way.
PERHEXILINE Perhexiline maleate is an antianginal compound that, like amiodarone and chloroquine, is amphophilic and capable of penetration into lysosomes. The use of perhexiline for angina has been associated with the development of a sensorimotor neuropathy that typically occurs after a year of treatment in patients receiving a low dosage (200 mg/day) and earlier in those receiving a high dosage (400 mg/day). The neuropathy presents as distal pain and paresthesias progressing to weakness that affects both distal and proximal muscles. Autonomic symptoms and perioral dysesthesias have also been described. Patients with peripheral neuropathy also often have weight loss and liver dysfunction. Cerebrospinal fluid protein may be markedly elevated and associated with papilledema. Electrophysiologic testing reveals a striking reduction in nerve conduction velocity, consistent with demyelination. Although in most cases improvement occurs with treatment discontinuation, evidence of axonal loss portends a poor prognosis. Studies of human pathologic samples reveal lipid deposition in neurons of the dorsal root gangha and sympathetic ganglia. Nerve and muscle biopsy shows intracytoplasmic inclusions in Schwann cells, endothelial cells, and muscle fibers that are of lysosomal origin. Surd nerve biopsy demonstrates segmental demyelination with rare axonal degeneration. The effect on Schwann cells may result from inhibition of lysosomal enzyme activity. Perhexilinehas been used to produce an experimental model of peripheral neuropathy. Perhexiline is metabolized by enzymatic oxidation, and patients who develop neuropathy often have a reduced ability to oxidize the drug. Oxidation efficiency is genetically determined, and in an animal model, only rats with impaired oxidation developed peripheral neuropathy. This suggests that a genetic factor may predispose certain people to develop perhexiline-induced neuropathy.
Drug-Induced Peripheral Neuropathies
631
PHENEUINE Phenelzine sulfate is a derivative of hydralazine used to treat atypical depression and other psychiatric disorders. Its mechanism of action is inhibition of monoamine oxidase. There are rare reports of an associated, primarily sensory neuropathy. Electrophysiologic testing is consistent with axonal injury. Phenelzine reduces pyridoxine levels, similar to isoniazid and hydralazine, and that may be the mechanism of damage. However, this view has been challenged.
PHENYTOIN Phenytoin (diphenylhydantoin) is used to treat epilepsy and neuropathic pain. Peripheral neuropathy usually is mild and only discovered on clinical examination. Patients do not typically report symptoms. Diminished or absent deep tendon reflexes may be seen in the lower extremities. Deep tendon reflexes were absent in 18% of unselected patients who had been treated for more than 5 years. This rose to 50% in patients treated for 15 years. Mild sensory loss, particularly vibration sense, was noted in the lower extremities. Subtle symptoms of gait instability may be related to sensory ataxia caused by the neuropathy. There may be a relationship between duration of treatment, high plasma concentration of phenytoin, and low folate levels and the development of peripheral neuropathy. Rarely, an acute, severe neuropathy can develop that is reversible upon discontinuation of the medication. Nerve conduction studies demonstrate decreased evoked response amplitudes and mild slowing of conduction velocity, consistent with axonal injury. Sural nerve biopsy reveals loss of large, axons and secondary demyelination.
PROCARBAZINE Procarbazine is a hydrazine derivative used in Hodgkin’s disease, non-Hodgkin’s lymphoma, small cell carcinoma of the lung, and a variety of brain tumors. It inhibits DNA and RNA synthesis. Peripheral neuropathy has been noted in 10% to 20% of patients.
PYRIDOXINE Pyridoxine (vitamin B6)is an essential, water-soluble vitamin that is necessary for the function of a variety of enzymes. It is used to mitigate the increased excretion of pyridoxine by isoniazid, to treat pyridoxine-responsive epilepsy, and to treat mushroom poisoning by the false morel Gyrornitra esculenta. It is also used along with other medications that effectively decrease pyridoxine levels, such as cycloserine, hydralazine, and penicillamine. The recommended daily allowance is 2 mg; however, megadose treatment has been in vogue at various times to treat premenstrual symptoms, autism, and psychiatric illnesses and has been used by laypersons as a bodybuilding supplement. Over time, a daily dosage of 50 mg may cause a peripheral neuropathy. Dosages used to treat pyridoxine-dependent seizures have also been associated with neuropathy. A severe, primarily large-fiber, sensory neuropathy is characteristic, with sensory ataxia as the presenting symptom. Temperature and pain sensation are affected to a lesser extent than vibration and joint position sense. Weakness and paresthesia are not common. Symptoms typically subside when the drug is stopped but may persist for weeks before improvement is noted.
631
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
Predictably, recovery is more rapid and complete after exposure to lower dosages. Electrophysiologic testing characteristically demonstrates absent sensory responses with preserved or mildly slowed motor conduction velocity. Axonal degeneration of both small- and large-diameter fibers is seen on sural nerve biopsy. Experimental studies have demonstrated degeneration of dorsal root and gasserian ganglion cells accompanied by centrifugal axonal atrophy and degeneration of peripheral and central sensory axons, implying a primary sensory neuronopathy. Ventral roots were unaffected. There is evidence that prolonged, low-dose exposure results primarily in a small-fiber neuropathy with sparing of ganglion cells, whereas shorter exposure to high dosages leads to a sensory neuronopathy and large-fiber neuropathy.
discontinuation of the drug. Some authors recommend baseline electrophysiologic evaluation with follow-up studies at 6-month intervals to detect the earliest onset of neuropathy. Sural nerve biopsy performed 2 to 6 years after thalidomide discontinuation showed selective loss of large-diameter fibers. This is at odds with the clinical symptoms and signs and the normal nerve conduction velocities that are typically seen. Nerve conduction studies show a decreased or absent sensory response and decreased motor evoked potential amplitude with little or no decrease in conduction velocity. Recovery of sensory nerve conduction parameters may not parallel clinical recovery. This may result from the loss of dorsal root ganglion cells. Cerebrospinal fluid protein may be elevated. VlNCA ALKALOIDS
SURAMIN Suramin has been used as an antitrypanosomal agent since 1920 and recently has shown promise in treating neoplasms. A severe, dose-dependent sensorimotor neuropathy has been described. The neuropathy is of two types: a chronic, axonal form and a subacute, inflammatory, demyelinating form. Bulbar and respiratory muscle weakness and autonomic symptoms and signs have been described. Electrophysiologic testing may reveal either an axonal or demyelinating neuropathy. The demyelinating form is responsive to discontinuation of the drug and plasmapheresis. Sural nerve biopsy demonstrates axonal degeneration and myelin abnormalities. Cerebrospinal fluid protein may be elevated. The mechanism of suramin’s chemotherapeutic activity is not known. However, studies in cell culture point to a disruption of glycolipid transport or metabolism. Dorsal root ganglion cells exposed to suramin accumulate ceramide, which leads to cell death. Multilaminar inclusion bodies composed of GM1 ganglioside are seen in Schwann cells investing the dorsal root cells.
THALlDOMlDE Thalidomide was initially used in Europe as a hypnotic but rapidly fell out of favor after reports of birth defects in infants born to mothers using the drug to alleviate morning sickness. There has been renewed interest in this immunomodulatory agent for use in severe rheumatoid arthritis, Crohn’s disease, graft versus host reactions after bone marrow transplantation, erythema nodosum leprosum, and many dermatologic diseases, including discoid lupus and treatment of aphthous ulcers in patients with human immunodeficiency virus infection. The mechanisms of action are not precisely known. Thalidomide-induced peripheral neuropathy is dose dependent. The incidence is between 25% and 50% of patients, approximately half of whom were symptomatic and half of whom showed an asymptomatic decrease in the sensory action potential amplitude of 50%. Neuropathic symptoms appear in a lengthdependent manner. However, weakness, which develops late in the course, tends to affect the proximal lower extremities. Paresthesias and numbness are noted in the feet and spread proximally. Small-fiber modalities are affected to a greater degree than the large-fiber modalities of vibration and joint position sense. Cramping in the lower extremities is common. Tendon reflexes may persist. Symptoms may begin after the drug is stopped. Resolution of symptoms, either fully or partially, occurs in only 50% of patients. Improvement may not begin for 3 years after
Vinca alkaloids are derived from the periwinkle plant (Vincu roseu). Vinblastine, vincristine, and vindesine are used to treat hematologic and lymphomatous malignancies. Vincristine is a more active agent than vinblastine and vindesine and has a higher incidence of peripheral neuropathy. This may result from the longer elimination half-life of vincristine. Vincristine, used at therapeutic dosages, will cause neuropathy in almost all patients. Indeed, neuropathy is the dose-limiting factor. The syndrome described here is routinely observed with the use of vincristine. The other vinca alkaloids may produce loss of reflexes and paresthesias but do not usually result in a severe neuropathy. Symptoms may begin as early as 2 months after initiation of treatment. Typically, loss of ankle jerks is the first clinical manifestation noted, and in approximately half of patients it progresses to total areflexia. Most patients initially notice paresthesias first in the fingers and then in the feet. Small-fiber modalities are affected more commonly than large fibers, and proprioception is uncommonly affected. Weakness is a more serious problem than sensory loss and may develop rapidly. Motor manifestations include cramping, weakness, and muscle atrophy. Weakness is most often noted in the distal muscles of the lower extremities and, peculiarly, in the extensors of the fingers and wrists, out of proportion to weakness seen in other distal upper extremity muscles. A neuropathy associated with severe distal lower extremity pain and weakness has been associated with the addition of hematopoietic colony-stimulating factors to vincristine in the treatment of lymphoma. Patients with hereditary sensory and motor neuropathy, type la, may be particularly susceptible to vincristine neuropathy. Neuropathic symptoms and weakness usually improve when the dosage is decreased or the drug is discontinued. Mild distal loss of small-fiber modalities may persist after paresthesias have resolved. Reflexes may return, but ankle jerks typically remain absent. Some patients are able to continue the drug at a lower dosage without reappearance of symptoms. Vinca alkaloids inhibit mitosis by binding with tubulin and interfering with the assembly of microtubules. Microtubules are also necessary for fast axonal transport, and this inhibitory effect on axonal transport is the likely mechanism of axonal damage. This mechanism would also explain the appearance of symptoms in the upper extremities before the lower extremities; those axons are shorter and would display the effects more quickly than the longer axons in the lower extremities. As may be expected, sural nerve biopsy demonstrates axonal degeneration with minor segmental demyelination. Regenerating fibers are seen several months after the drug is discontinued. After
Chapter 100
large intravenous doses, neurofilamentous accumulations are seen in dorsal root ganglia cells and throughout the central nervous system, including anterior horn cells. Similar changes are seen in anterior horn cells with intrathecal dosing. Nerve conduction studies show decreased sensory evoked response amplitudes and compound muscle potential amplitudes with normal or mildly decreased conduction velocity, as would be expected in an axonal neuropathy. Electromyography demonstrates fibrillation potentials and a reduced number of motor units in distal muscles, consistent with axonal loss. ZlMELDlNE Zimeldine is a 5-hydroxytryptamine reuptake inhibitor used to treat depression. It was withdrawn from the market because of a number of adverse reactions including an acute inflammatory
Inherited Neuropathy
633
demyelinating neuropathy similar to Guillain-Barresyndrome. An autoimmune mechanism has been implicated. SUGGESTED READINGS Argov Z, Mastaglia F L Drug-induced peripheral neuropathies. BMJ 1:663-666, 1979 Clark DW Genetically determinedvariability in acetylation and oxidation. Therapeutic implications. Drugs 29(4):342-375, 1985 Le Quesne PM: Neuropathy due to drugs. pp. 1571-1581. In Dyck P, Thomas PK (eds): Peripheral Neuropathy. WB Saunders, Philadelphia, 1993 Macdonald D R Neurologic complications of chemotherapy. Neurol Clin 9(4):955-967, 1991 Simpson DM, Tagliati M: Nucleoside analogueassociated peripheral neuropathy in human immunodeficiency virus infection. J Acquir Immune Defic Syndr Hum Retrovirol 9(2):153-161, 1995
100 Inherited Neuropathy Guillermo A. Suarez The inherited neuropathies are a group of heterogeneous disorders. Some are related to known metabolic derangements (e.g., Fabry’s disease), whereas others have no known cause (Table 100-1). A useful way to classify this latter group is based on the inheritance pattern, populations of neurons affected, natural history, and electrophysiologic and histopathologic findings. In the last few years, the tremendous advances in our understanding of the genetics of these disorders through gene mapping by linkage
analysis and gene isolation by molecular genetics have provided new ways to classify these disorders. An attempt to classify these conditions with a reference point is to consider which population (system) of neurons is predominantly affected. Selective degeneration of lower motor neurons is classified as hereditary motor neuropathy or, simply, spinal muscular atrophy. Degeneration of motor and sensory neurons indicates hereditary motor and sensory neuropathies (HMSNs).
W TMLE 100-1. Inherited Neuropathies
Disorder
Genetic Transmission
Clinical Features
Electrophysiologicfindings
Pathologic Findings
AD
Distal leg weakness and sensory loss
Slow NCV, reduced or absent SNAPs
Hypertrophic neuropathy
AD
Onset later in life
Near-normal NCV, absent SNAPs
Reduction in large MF, axonal atrophy
CMT neuropathies Type 1
IA: 17 (~11.2-12); PMP22 gene I B 1 (lq22-23); Po gene
Type 1 I
I/ A: 1p36 11 B: 3q /I C*: unknown /ID: unknown Type 111
*vocal cord paralysis AD, sporadic, AR?
Onset in infancy; delayed motor skills
Very slow NCV
Demyelination, axonal atrophy
Type x Chr. X (q12-qZl ); connexin 32 gene
X-linked
Distal leg weakness and sensory loss
Moderate slow NCV
Hypertrophic neuropathy
Type IV
AR
Slow NCV
Loss of fibers with demyeli-
(Dejerine-Sottas disease) mutations on PMP22 and Po genes
nation and onion bulbs
IVA: 8q13-21.1 IV B: 11q23 Hereditary neuropathy with liability to pressure palsies Deletion of 17~11.2-12; PMP22 nene
AD
Recurrent mononeuropathies, mild distal polyneuropathy
Multiple mononeuropathies, peripheral neuropathy
Demyelination, thickening of myelin sheath (tomaculous)
Abbreviations: AD, autosomal dominant; AR, autosomal recessive; MF, myelinated fibers; NCV, nerve conduction velocity; PMP, peripheralmyelin protein; SNAPs, sensory nerve action potentials.
Chapter 100
large intravenous doses, neurofilamentous accumulations are seen in dorsal root ganglia cells and throughout the central nervous system, including anterior horn cells. Similar changes are seen in anterior horn cells with intrathecal dosing. Nerve conduction studies show decreased sensory evoked response amplitudes and compound muscle potential amplitudes with normal or mildly decreased conduction velocity, as would be expected in an axonal neuropathy. Electromyography demonstrates fibrillation potentials and a reduced number of motor units in distal muscles, consistent with axonal loss. ZlMELDlNE Zimeldine is a 5-hydroxytryptamine reuptake inhibitor used to treat depression. It was withdrawn from the market because of a number of adverse reactions including an acute inflammatory
Inherited Neuropathy
633
demyelinating neuropathy similar to Guillain-Barresyndrome. An autoimmune mechanism has been implicated. SUGGESTED READINGS Argov Z, Mastaglia F L Drug-induced peripheral neuropathies. BMJ 1:663-666, 1979 Clark DW Genetically determinedvariability in acetylation and oxidation. Therapeutic implications. Drugs 29(4):342-375, 1985 Le Quesne PM: Neuropathy due to drugs. pp. 1571-1581. In Dyck P, Thomas PK (eds): Peripheral Neuropathy. WB Saunders, Philadelphia, 1993 Macdonald D R Neurologic complications of chemotherapy. Neurol Clin 9(4):955-967, 1991 Simpson DM, Tagliati M: Nucleoside analogueassociated peripheral neuropathy in human immunodeficiency virus infection. J Acquir Immune Defic Syndr Hum Retrovirol 9(2):153-161, 1995
100 Inherited Neuropathy Guillermo A. Suarez The inherited neuropathies are a group of heterogeneous disorders. Some are related to known metabolic derangements (e.g., Fabry’s disease), whereas others have no known cause (Table 100-1). A useful way to classify this latter group is based on the inheritance pattern, populations of neurons affected, natural history, and electrophysiologic and histopathologic findings. In the last few years, the tremendous advances in our understanding of the genetics of these disorders through gene mapping by linkage
analysis and gene isolation by molecular genetics have provided new ways to classify these disorders. An attempt to classify these conditions with a reference point is to consider which population (system) of neurons is predominantly affected. Selective degeneration of lower motor neurons is classified as hereditary motor neuropathy or, simply, spinal muscular atrophy. Degeneration of motor and sensory neurons indicates hereditary motor and sensory neuropathies (HMSNs).
W TMLE 100-1. Inherited Neuropathies
Disorder
Genetic Transmission
Clinical Features
Electrophysiologicfindings
Pathologic Findings
AD
Distal leg weakness and sensory loss
Slow NCV, reduced or absent SNAPs
Hypertrophic neuropathy
AD
Onset later in life
Near-normal NCV, absent SNAPs
Reduction in large MF, axonal atrophy
CMT neuropathies Type 1
IA: 17 (~11.2-12); PMP22 gene I B 1 (lq22-23); Po gene
Type 1 I
I/ A: 1p36 11 B: 3q /I C*: unknown /ID: unknown Type 111
*vocal cord paralysis AD, sporadic, AR?
Onset in infancy; delayed motor skills
Very slow NCV
Demyelination, axonal atrophy
Type x Chr. X (q12-qZl ); connexin 32 gene
X-linked
Distal leg weakness and sensory loss
Moderate slow NCV
Hypertrophic neuropathy
Type IV
AR
Slow NCV
Loss of fibers with demyeli-
(Dejerine-Sottas disease) mutations on PMP22 and Po genes
nation and onion bulbs
IVA: 8q13-21.1 IV B: 11q23 Hereditary neuropathy with liability to pressure palsies Deletion of 17~11.2-12; PMP22 nene
AD
Recurrent mononeuropathies, mild distal polyneuropathy
Multiple mononeuropathies, peripheral neuropathy
Demyelination, thickening of myelin sheath (tomaculous)
Abbreviations: AD, autosomal dominant; AR, autosomal recessive; MF, myelinated fibers; NCV, nerve conduction velocity; PMP, peripheralmyelin protein; SNAPs, sensory nerve action potentials.
634
Spinal Cord and Peripheral NeuromuscularDisease W
Diseases of Peripheral Nerve
Degeneration of sensory and autonomic neurons is categorized as hereditary sensory and autonomic neuropathies (HSANs). Inherited neuropathies probably are the most common undiagnosed neuropathies. Dyck and colleagues reported that 42% of a series of 205 patients with undiagnosed neuropathies were found to have an inherited neuropathy when an appropriate kinship history was obtained (recording skeletal abnormalities such as high arches), and relatives were appropriately examined. It must be emphasized that a critical part of the examination is obtaining an appropriate family history by specifically asking whether the relatives have foot deformities, high arches, gait problems, muscle atrophy, trophic ulcers, or neuropathic symptoms.
HEREDITARY MOTOR AND SENSORY NEUROPATHY The classification of the inherited neuropathies and its nomenclature is constantly changing according to the new advances in the field. The group of HMSNs is also currently described as Charcot-Marie-Tooth (CMT) neuropathies. Originally, the term peroneal muscular atrophy or CMT disease was believed to be specific for one disorder. It is now known that this is not the case. Peroneal muscular atrophy occurs in several inherited neuromuscular disorders. Charcot and Marie emphasized the following features: pes cavus, progressive atrophy of distal leg muscles (legs resemble an inverted champagne bottle), tightness of Achilles tendons, hammertoes, and a steppage gait. Tooth emphasized that the disorder was inherited and concluded that it was caused by disease of the peripheral nerves. Landmark genetic, clinical, electrophysiologic, and pathologic studies of large kindreds by Dyck and Lambert allowed a separation in two main groups: the hypertrophic or demyelinating form, later called HMSN type I (CMT I), characterized by diffusely low motor nerve conduction velocities associated with nerve biopsy findings of axonal atrophy, demyelination, and onion bulb formations; and the neuronal form of CMT disease, subsequently named HMSN type I1 (CMT 11), characterized by normal or near-normal motor conduction velocity without hypertrophic neuropathy on nerve biopsy. The first group, hypertrophic type I, can be subdivided into patients with a classic phenotype as described by Charcot, Marie, and Tooth, and patients with recessively inherited or sporadic varieties, called HMSN type 111 (CMT III), or Dejerine-Sottas disease. This is usually a more severe demyelinating neuropathy, with onset in infancy or early childhood and with very low conduction velocities. The mode of inheritance generally is autosomal dominant in both CMT I and 11. However, in a minority of cases, the disorder is sporadic or affects siblings but not their parents. These cases have been attributed to possible autosomal recessive inheritance or most likely to a new mutation of a dominant gene, autosomal inheritance with nonpenetrance or reduced penetrance in the parents, or false paternity. X-linked inheritance has been established for the X-linked CMT neuropathy.
CMT I Genetic Transmission. The mode of inheritance of CMT I is heterogeneous and includes autosomal dominant transmission in the majority of families but also autosomal recessive and X-linked forms. There are several varieties:
CMT IA In most families with autosomal dominant inheritance, the CMT IA locus maps to a band (pl1.2-p12) on the
short arm of chromosome 17, which contains the peripheral myelin protein-22 (PMP22) gene. CMT IB: In a minority of patients, the CMT IB locus is on the long arm of chromosome l(lq22-q23), which harbors the myelin protein zero gene (P,). CMT IC: Families with autosomal dominant CMT and not linked to chromosome 1 or 17. CMT X Linkage analysis localized the locus to the proximal long arm of the X chromosome (Xq13.1). A gap junction protein, connexin 32, is the responsible gene that causes CMT X. CMT ID: A few families with autosomal dominant transmission have been linked to chromosome 10 (10q21) with mutations in the early growth response 2 gene (EGR2). Lupski and coworkers reported that a segment band of chromosome 17 (17pl 1.2-pl2) was duplicated in affected members of families with HMSN IA. The human peripheral myelin protein 22 gene (PMP22) is found in the region of the duplication. PMP22 encodes for the synthesis of a peripheral nervous system myeli protein. A few CMT IA kinships have found missense mutations of PMP22 in patients with CMT IA without the duplication. Most patients with genetically defined CMT IA have either a gene dose effect (duplication of 17pl 1.2-p12) or a mutation affecting the PMP22 gene on chromosome 17. Interestingly, the human PMP22 gene is deleted in patients with inherited tendency to pressure palsies, also known as hereditary neuropathy with liability to pressure palsies (HNPP) (discussed later in this chapter). Recently, two allelic mutations of the PMP22 gene have been found to produce a demyelinating neuropathy in mice. These observations strongly suggest that alterations in PMP22 expression, alone or in combination with yet unknown environmental factors, are responsible for this group of neuropathies. Clinical Features. Typically, only a small percentage of people with CMT I seek medical attention for neuromuscular symptoms; many actually have no symptoms. Patients have difficulty pinpointing the onset of neurologic problems, and presenting symptoms usually are difficulty in running, stumbling, slapping of the feet in walking, and muscle atrophy; they might not be aware of their problems until a relative or friend mentions that “their gait is funny.” Parents may report that children have weakness of ankles or running difficulty. Another common scenario is the incidental discovery of an indicator of neuropathy, such as an abnormal nerve conduction study (NCS): The electromyographer reports a more generalized nerve conduction abnormality, consistent with an inherited neuropathy, in patients who presented with low back pain, carpal tunnel syndrome, or other related disorders. The symptoms in HMSNs relate mainly to deficits, that is, weakness and atrophy of distal muscles. Sensory symptoms are those of a deficit-of-function “dead” feeling. Positive symptoms, such as prickling or “asleep numbness” and painful paresthesias, are not typical and should alert the physician to a possible acquired neuropathy. Autonomic symptoms usually are not reported by patients. Muscle cramps in the lower extremities, especially after exercise, are common. On clinical examination, the feet and legs are more affected than the hands. Inspection of the feet reveals pes cavus and hammertoes in approximately 70% of adult patients (Fig. 100-1). Kyphosis of the spine might be present in a small percentage of patients. Clinical enlargement of peripheral nerves or excessive
Chapter 100 W
FIG. 100-1. Typical pes caws and hammertoes of a patient with HMSN IA.
firmness is present in 25% of patients. The nerves between the axilla and the elbow should be assessed and palpated for enlarged nerves. Entrapment points, such as the ulnar nerve at the elbow, should be avoided because the nerve normally is thickened at that point. Muscle weakness and wasting affect muscles of the feet, peroneal, and anterior tibial muscles, usually in a symmetrical fashion. Later, in the upper limbs, a similar distal involvement occurs, first affecting intrinsic hand muscles. Deep tendon reflexes usually are diminished or absent in the lower and upper extremities, but there is significant variability in this sign. Classically, patients do not volunteer sensory symptoms, but sensory examination reveals distal impairment of sensation, usually affecting vibration and light touch in the feet and hands. Using quantitative sensory examination, an unequivocal abnormality of all sensory modalities is demonstrated. Occasionally, because of the sensory loss, high arches, atrophy of foot muscles, and calluses, ulcers develop over the metatarsal heads and over the tips of toes. In some patients, there is a prominent upper limb tremor with the typical features of an essential tremor, associated with the classic phenotype of CMT I. These cases have been labeled as Roussy-Levy syndrome, but there is no evidence that this is a distinct clinical or genetic disorder. There is significant variability in respect to severity of neuropathic deficits between individuals, even from the same kinship. There are asymptomatic cases, with slow nerve conduction values, and sometimes minimal changes on sural nerve biopsy. Laboratoy Features. The nerve conduction and electromyographic features are useful to separate CMT I from CMT 11. There is uniform slowing of motor conduction velocity in almost all nerves tested in patients with CMT I. There is good concordance of conduction velocity values within affected kindreds. Ulnar and median motor nerve conduction studies show the characteristic reduction in conduction velocity, but conduction studies in the
Inherited Neuropathy
635
lower extremities may not be very useful because of the more severe distal nerve fiber degeneration. Harding and Thomas proposed a criterion that a motor conduction velocity below 38 m/second be used as the cutoff value for CMT I. This is a useful criterion provided that the compound muscle action potential ( C W ) is at least 0.5 mV in the nerve where the conduction velocity is calculated, and the mean values of conduction velocity for the same nerve of all affected patients in the same kindred are used. If temporal dispersion of the CMAP or conduction block is found, an alternative diagnosis such as chronic inflammatory demyelinating polyneuropathy should be considered. Sensory nerves are also affected. Sensory nerve action potentials (SNAPS) are uniformly reduced or unrecordable using standard electrophysiologic techniques. Otherwise, routine laboratory studies, including cerebrospinal fluid (CSF) studies, provide normal results. DNA testing is commercially available and provides a good screening test for patients with suspected CMT neuropathies. Approximately 70% to 80% of patients with CMT IA test positive for the DNA duplication in chromosome 17~11.2-12. Pathologic Features. Pathologic studies (especially of sural nerves) show the typical features of a hypertrophic neuropathy, including onion bulb formation, made up of circumferentially directed Schwann cell processes, marked reduction in large myelinated fibers, increase in transverse fascicular area, and increased frequency of paranodal and segmental demyelination and remyelination. Extensive morphometric studies by Dyck and colleagues provide evidence of an axonal abnormality. There is clustering of demyelinating changes, increased frequency of demyelination and remyelination in distal segments, distal predominance of onion bulbs, and reduction in axon caliber relative to the number of myelin lamellae. These observations lend support to the hypothesis that axonal atrophy occurs first, and segmental demyelination may be secondary to it. This does not exclude a concomitant abnormality of Schwann cells. CMT IA and CMT IB
The inheritance pattern, clinical features, electrophysiologicfindings, course, and natural history of CMT IA and CMT IB overlap. Only molecular genetic techniques allow separation into these two groups. CMT IB is associated with mutations in the myelin protein zero gene (Po). CMT IA appears to be a less severe disorder than CMT IB. Treatment There is no specific treatment for CMT IA and IB. Clinical, genetic, and symptomatic counseling is important. Because of the high arches and foot deformities, proper foot care should be emphasized to avoid foot ulcers. Shoes should be comfortable,well made, and protective. The shoes and feet should inspected every day. Calluses must not be trimmed with a razor blade. If the patient develops a plantar ulcer, weight-bearing should be avoided until the ulcer has healed. Foot braces may be tried, but they are not necessary for every patient. If the brace does not improve gait, then it should not be worn. Foot surgery usually is reserved for patients who begin to develop valgus deformity of the ankle or severe degrees of pes cavus. The patient should understand that surgery is not going to cure the other manifestations of the disorder such as sensory loss and muscle weakness. Most affected patients are able to work full time, and there is no evidence that life expectancy is any different from that of the general population. Because of the distal weakness, training in an occupation that does not require fine motor skills may be recommended.
636
Spinal Cord and Peripheral Neuromuscular Disease rn Diseases of Peripheral Nerve
CMT II: Neuronal Form Genetic Transmission. CMT I1 is not as common as CMT I, and there is substantial genetic heterogeneity in this group. Linkage studies permit classification into four groups: CMT 2A, 2B, 2C, and 2D (Table 100-1). Clinical Features. The clinical features of patients with CMT I1 are similar to those with CMT I. However, there are some differences. Patients with CMT I1 usually are asymptomatic until later in life. Peripheral nerves usually are not clinically enlarged, and weakness of feet and leg muscles predominate; hands are less severely affected. Sensory loss is present in the distal extremities, and foot deformities (pes cavus) tend to be less marked. On the basis of the clinical phenotype, it is very difficult or impossible to separate CMT I1 from CMT I. laboratory Features. Motor nerve conduction velocities are near normal or normal in patients with CMT 11. The mean conduction velocity of ulnar nerves in the kindred studies was about 38 mlsecond. SNAPS are uniformly reduced or absent. Pathologic Findings. Sural nerve biopsies in patients with CMT I1 have shown reduction of large myelinated fibers, particularly distally, without significant demyelination on teased fibers. Small onion bulbs may be seen. CMT II with Diaphragm and Vocal Cord Weakness
A large kindred with autosomal dominant CMT I1 has been reported with a classic neuropathic phenotype, but in addition, 50% of the affected patients had vocal and diaphragm weakness. Death has been attributed to respiratory weakness, and intercurrent infections have been observed. Linkage studies have not localized this disorder to a known locus. CMT II:Autosomal Recessive
Ouvrier reported a more severe form of CMT I1 with onset in infancy or early childhood and recessive inheritance. The treatment of CMT I1 is similar to that of CMT I.
FIG. 100-3. Sural nerve biopsy of a patient with HMSN 111 (Dejerine-Sottas disease), transverse section embedded in epon and stained with methylene blue. Note prominent onion bulb formations and reduction in the number of myelinated fibers. (Courtesy of C. Ciannini, MD, Department of Pathology, Mayo Clinic, Rochester, MN.) CMT 111: Dejerine-Sottas Disease
CMT I11 is a rare hypertrophic neuropathy of infancy. Genetic studies have identified de novo mutations in the PMP22 gene and in the Pogene (an important structural protein of peripheral nerve myelin). The clinical features are those of a severe neuropathy with onset in early childhood. Motor development is delayed. Motor skills such as jumping and running are impaired. There is progressive muscular weakness affecting legs and arms. General areflexia, with prominent enlarged peripheral or cranial nerves, is typical (Fig. 100-2). There is definite sensory loss, and some patients have marked sensory ataxia. The course is progressive, with significant disability. Some patients are wheelchair-bound in early adulthood. Motor conduction velocity is markedly reduced, usually below 10 m/second. CSF protein levels often are elevated. Pathologic studies have shown enlargement of the transverse fascicular area, onion bulb formation (Fig. 100-3), segmental demyelination, reduction in the number of myelinated fibers, and axonal atrophy. Other cases reported as congenital hypomyelinated neuropathy probably represent a variant of CMT 111. The differential diagnosis includes acquired and inherited demyelinating neuropathies occurring in children. In patients labeled as having acquired neuropathy, the differential diagnosis must consider acute and chronic inflammatory demyelinating polyradiculoneuropathy; in those with inherited neuropathy, the differential diagnosis includes CMT I and 11, metachromatic leukodystrophy, Cockayne’s syndrome, HNPP, and other rare neuropathies. CMT IV
FIG. 100-2. Magnetic resonance imaging of the brain showing an enlarged and hypertrophied fifth cranial nerve in a patient with Dejerine-Sottas syndrome.
A rare form of CMT neuropathy with autosomal recessive transmission has been reported in families from Tunisia. One form has been mapped to chromosome 8 (8ql3-2 1) and designated CMT IVA. Another has been linked to chromosome 11 (1 lq23) and named CMT IVB. Other kinships have not linked to known loci, suggesting genetic heterogeneity. The phenotypic presentation is one of a severe demyelinating predominantly motor neuropathy with early onset in childhood. Patients have pes cavus and oiher ‘skeletal deformities and often need a wheelchair. The
Chapter I 0 0
EMG shows motor conduction values in the demyelinating range of 20 to 30 mhecond. The CSF protein content is normal, which helps to separate this neuropathy from the Dejerine-Sottas type or CMT 111.
X-Linked CMT Neuropathy (CMT X ) Genetic Transmission. Linkage studies localized CMT X to the long arm of chromosome Xq13. This region contains the connexin 32 gene, and mutations of this gene cause CMT X. Connexin 32 is an important gap junction protein localized around the nodes of Ranvier and Schmidt-Lanterman incisures. Clinical Features. The clinical features are similar to those of CMT I, with a neuropathy more severely affecting males and with onset in adolescence. Neuropathic deficits include distal muscle atrophy and weakness with foot drop and intrinsic hand muscle weakness with distal sensory loss. Deep tendon reflexes generally are hypoactive to absent. Pes cavus may be present in patients with this neuropathy. Laboratory Features. EMG studies have shown both axonal and demyelinating features with low-amplitude CMAPs and slowed conduction velocities. Sensory responses generally are of low amplitude or absent. Pathologic Findings. There is reduction of large myelinated fibers with evidence of demyelination and remyelination.
Refsum's Disease
The hypertrophic neuropathy associated with increased phytanic acid levels, or Refsums disease, is also called Refsum's neuropathy and used to be classified as HMSN type IV.The clinical features are distinctive and very different from the CMT profile and include retinitis pigmentosa, ataxia, skeletal malformations, and a predominantly sensory neuropathy. The main differential diagnosis is with the spinocerebellar degenerations, which often have an associated mild sensory neuropathy.
HMSN with Associated Features
There are families with the clinical phenotype of peroneal muscular atrophy, and they present with additional distinct features such as spastic paraparesis (HMSN V), optic atrophy (HMSN VI), retinitis pigmentosa (HMSN VII), deafness, and cardiomyopathy. In most family studies, the inheritance pattern was autosomal dominant.
1 Inherited Neuropathy
637
HEREDITARY SENSORY AND AUTONOMIC NEUROPATHIES The main feature of HSAN is the prominent involvement of sensory and autonomic fibers. The primary pathologic foci of this disorder are mainly small-diameter pain and thermal sensory neurons (axons) and autonomic neurons. There is significant clinical and genetic heterogeneity. It would be desirable to classify these disorders by the altered cellular or genetic mechanism, but for most HSANs, this is not known. For practical purposes, a classification based on the inheritance pattern, clinical features, and system of neurons predominantly affected is used (Table 100-2). The loss of pain sensation and sensory loss predisposes to the development of foot complications, including plantar ulcers, secondary infections such as cellulitis, and osteomyelitis, which may lead to osteolysis, eventually resulting in acral mutilations.
HSAN I
HSAN I is a genetically heterogeneous disorder, dominantly inherited in most cases. Linkage studies have mapped the genetic loci to chromosome 9q22. Neuropathic symptoms may begin in the second or fourth decade of life and slowly progress over time. Spontaneous neuropathic pain typically is burning, aching, or lancinating in quality, affects mainly the feet and legs, and is aggravated by heavy walking or weight-bearing. Sometimes pain is related to local events such as calluses or plantar ulcers. Neurologic signs include sensory loss predominantly involving pain and temperature sensation, but all modalities may be affected. The decreased sensation typically affects feet and legs in a symmetrical fashion. Deep tendon reflexes are absent at the ankles but present in the upper extremities. In some kindreds, a variable degree of motor involvement with peroneal muscular weakness may be seen. High arches of the feet with frequent corns and calluses of the soles of the feet may have gone unnoticed for years. Foot complications such as the typical plantar ulcer in the metatarsal head region or sole of the foot is a late manifestation of HSAN I. Plantar ulcers are not caused only by sensory loss; other risk factors play a critical role. These include excessive use and abuse of feet, neglect of foot care, excess weight, and neglect of foot injury. Men, particularly those involved in heavy physical activity, tend to develop ulcers more often than women. If foot ulcers are not recognized and treated promptly, a sequence of events occurs, leading to local infection, osteomyelitis, and loss of a foot or leg. Electrophysiologic studies reveal absence of SNAPs. The neuropathologic features are those of a chronic neuropathic
TAW 100-2. Hereditary Sensory and Autonomic Neuropathies Disorder
Genetic Transmission
Electrophysiologk Findings
Pathologic Findings
Painful feet, decreased pain Abnormal small nerve fiber Reduction of small MF and UF and temperature sensation function SNAPs generally absent Reduction of MF and UF AR Onset in early childhood, planType II tar ulcers, mutilation of digits and toes Reduced SNAPs, abnormal Marked reduction of UF AR Prominent autonomic manifesType 111: Familial dysautonomia small nerve fiber function tations, absence of fungichromosome 9 (9q3 1-q33) form papillae, and defective lacrimation Type IV AR Congenital insensitivity to pain, Normal SNAPs Reduction of small MF anhidrosis Abbreviations: AD, autosornal dominant; AR, autosornal recessive; MF, rnyelinated fibers; SNAPs, sensory nerve action potentials; UF, unrnyelinatedfibers.
Type I
AD
Clinical Features
638
Spinal Cord and Peripheral Neuromuscular Disease W
Diseases of Peripheral Nerve
process affecting small myelinated and unmyelinated fibers with axonal atrophy, myelin remodeling, and axonal degeneration. The differential diagnosis includes other varieties of HSAN (discussed later in this chapter). Three features are helpful to separate these conditions. The first is age of onset: HSAN I begins in the second or even later decades of life, but the other varieties (HSAN I1 to V) probably are congenital, with onset at birth. The second is progression of deficits: In HSAN I there is slow progression over the course of years, which is seldom the case in the other varieties. The third is pattern of involvement: HSAN I tends to affect the lower extremities, whereas in the other varieties the lower and upper extremities and trunk are generally affected. Spinocerebellar degeneration (i.e., Friedreich's ataxia) is separated from HSAN I by the following main features: sensory loss that predominantly affects proprioception and vibratory sensation, cerebellar ataxia, and minimal autonomic and small-fiber dysfunction. Familial forms of amyloidosis are separated clinically by the presence of sexual and sphincter dysfunction.
HSAN IV
Swanson originally described two affected siblings with insensitivity to pain, mild mental retardation, defective temperature control, and anhidrosis. Subsequent case reports have been documented. Pathologic findings include loss of unmyelinated fibers and lesser reduction of small myelinated fibers. This disorder is recessively inherited. HSAN V
Low and colleagues reported a 6-year-old child with congenital loss of pain sensation with normal muscle strength, reflexes, and normal light touch and vibratory sensation. SNAPS were normal, but sural nerve biopsy revealed marked loss of small myelinated fibers. Additional cases have also been reported. Treatment and Management
HSAN II
HSAN I1 is a rare recessively inherited condition with onset early in life. Unlike in HSAN I, all sensory modalities are involved, affecting not only the lower extremities but also hands, face, and trunk. Children with this disorder are at risk for ulcers of the feet, hand, lips, and tongue, and mutilation of fingers and toes may occur. Repeated paronychia, plantar ulcers, and stress foot fractures usually are present. Neurologic examination reveals sensory loss that affects all modalities of sensation involving legs and hands. Reflexes are diminished or absent throughout. There is distal anhidrosis with sphincter dysfunction and impotence in men. SNAPS are absent. Pathologic studies of sural nerves have shown marked reduction to absence of myelinated fibers with a reduction in unmyelinated fibers as well. Donaghy reported the association of retinitis pigmentosa, spastic paraplegia, and neurotrophic keratitis with sensory neuropathy. HSAN 111: Familial Dysautonomia
Initially described by Riley (Riley-Day syndrome), HSAN 111 is a rare autosomal recessive sensory neuropathy with autonomic manifestations that affects mainly Ashkenazi Jews, with an estimated gene frequency in North American Jews of less than 1 in 100,000. The genetic locus has been established by linkage analysis and is located on chromosome 9q31433. Recent studies have identified the IKB kinase complex-associated protein (IKAP) gene in this region, and mutations of this gene cause HSAN 111. The clinical manifestations usually are present at birth and consist of deficient lacrimation, poor sucking, episodic hyperthermia, frequent respiratory infections, vomiting, and failure to thrive. Emotional stimulation usually provokes autonomic crises with hypertension, profuse sweating, and excessive mottling of the skin. Constant clinical features helpful in the diagnosis are the absence of fungiform papillae on the tongue, defective lacrimation (alacrima), and corneal insensitivity. Hyporeflexia, decreased pain sensation, and kyphoscoliosis become apparent later in life, Electrophysiologic studies reveal reduction in SNAPS with preserved motor conduction velocities. Sural nerve biopsies demonstrate a marked reduction in the number of unmyelinated fibers. Postmortem examinations have shown marked reduction in the number of neurons in autonomic and spinal ganglia.
Emphasis on prevention of foot ulcers is the most important aspect of treatment for HSAN. Instructions along the lines described earlier for CMT should be provided. Patients should be instructed not to abuse their feet. Children should avoid jumping from heights, and certain sports such as parachuting or kicking sports should be deemphasized. Careful foot care with daily inspection of feet and shoes is of utmost importance. Patients should wear shoes even inside the house. Foot care with daily soaks, followed by petroleum jelly lotion, is in order. Calluses should not be trimmed; rather, they should be rubbed off after soaking. If a plantar ulcer develops, weight-bearing must cease until it is healed. Prompt debridement with antibiotic coverage usually is needed. In most cases, acromutilations are seen in patients who abused their feet and neglected the injuries for a long time until it was too late to salvage the foot or leg. ~
HEREDITARY NEUROPATHY WITH LIABILITY TO PRESSURE PALSIES (HNPP)
HNPP is an autosomal dominant neuropathy with susceptibility to pressure palsies. Genetic studies using linkage analysis have localized the abnormality to band 17pl1.2-pl2 on chromosome 17. In contrast to CMT IA,this segment is deleted in HNPP. The human PMP22 gene, which is normally found in this region, is deleted in HNPP and duplicated in CMT IA. There are reports of a few families without linkage to chromosome 17, suggesting genetic heterogeneity. Usually, the clinical manifestations start in the second or third decade of the patient's life. Onset of symptoms follows trivial trauma, compression, or sleeping on a limb. The resulting palsy, usually painless, persists for days or weeks instead of resolving in minutes or hours. Typically, a mononeuropathy with sensory loss and weakness develops in the appropriate anatomic distribution. The most commonly affected nerve trunks are the peroneal nerve at the fibular head, the radial nerve in the spiral groove of the humerus, and the ulnar nerve at the elbow. The history of minor compression or trauma is not always present. On examination, a mononeuropathy with the corresponding sensory loss and weakness in the distribution of the affected nerve is the rule. An important point, not always described in the literature, is that many patients have signs, albeit minor, of a distal, more generalized neuropathy. There is mild distal symmetrical sensory
Chapter 100
loss, and ankle reflexes are depressed or absent. In some patients, the telltale signs of an inherited neuropathy (high arches, hammertoes) are present. Nerve conduction studies are helpful to detect conduction slowing or block at one or more entrapment sites. Prolonged distal latencies out of proportion to the slowing of conduction velocities have been reported as a useful distinctive electrophysiologic feature. A more diffuse motor and sensory polyneuropathy affecting both clinically affected and unaffected nerves also is a helpful clue to the diagnosis. Pathologic studies, mainly of surd nerve biopsies, have shown segmental demyelination and remyelination with distinctive focal thickening of the myelin sheath, called “sausages” or “tomaculous” (Fig. 100-4). Uncompacted axonal myelin and reduplicated segments of myelin have been demonstrated by electron microscopy studies (Fig. 100-5). These observations suggest that a primary abnormality of myelin formation underlies this disorder, which may predispose myelinated fibers to be more susceptible to environmental factors, such as local trauma or compression. It should be emphasized that establishing heredity is critical in taking the clinical history in a patient who presents with pressure palsy. Family history is revealed only after detailed and often specific questioning. The presence or recurrence of pressure palsies with associated mild signs of a generalized neuropathy is a helpful clue to distinguish HNPP from individual cases of pressure palsy. To separate HNPP affecting the brachial plexus from sporadic brachial plexus neuropathy, the following features are helpful. In HNPP, the onset usually is painless, in contrast to the severe pain found at onset in brachial plexus neuropathy. The relationship to trauma and the presence of a generalized neuropathy are helpful
Inherited Neuropathy
639
clues to the diagnosis of HNPP. Other multiple mononeuropathies associated with diabetes, leprosy, sarcoidosis, Lyme disease, or necrotizing vasculitis are considered in the differential diagnosis of HNPP but usually do not present major diagnostic problems. Molecular DNA analysis can demonstrate the PMP22 deletion in HNPP and secure the diagnosis. Screening for PMP22 mutations is performed only in selected cases. There is no specific treatment for this condition. The major point in management is education for the prevention of nerve injury by avoiding pressure damage. Individual pressure palsies are treated by appropriate splinting and physical therapy. Recovery may be prolonged, but the prognosis for return of function is good.
FAMILIAL AMYLOID POLYNEUROPATHY Inherited amyloidoses are autosomal-dominant disorders characterized by deposition of amyloid in peripheral nerves and other tissues. The clinical phenotypes of hereditary amyloidosis often have in common peripheral neuropathy with prominent autonomic manifestations, which differ in age of onset, genetic defect, clinical patterns of neuropathy, and other tissue involvement. The first familial amyloid polyneuropathy (FAP) described was the previously named Portuguese variety, reported by Andrade in 1952; it is the most common type, and the amyloid is derived from a point mutation on the transthyretin (TTR) molecule, formerly known as prealbumin. The first mutation reported was the methionine for valine substitution at position 30. Since then, 80 point mutations of the TTR gene have been identified. The former classification of the FAP into four types was replaced by new understanding of the basic molecular genetic variations. Mutations of three proteins-TTR, apolipoprotein Al, and gelsolinare the basis of the current classification. m-Related FAP
A
B
C
FIG. 100-4. Sural nelve biopsy of a patient with hereditary neuropathy with liability to pressure palsies (HNPP). (A) Transverse section embedded in epon and stained with methylene blue. Note several profiles showing focal thickening of the myelin sheath “sausages“ or “tomaculous.“ (6 and C) Teased fiber preparation showing distinctive focal thickening of the myelin sheath ”sausages.” (Courtesy of C. Ciannini, MD, Department of Pathology, Mayo Clinic, Rochester, MN.)
TTR-related FAP was originally described by Andrade in northern Portugal and was formerly known as FAP type I. It is dominantly inherited and is the most common FAP and has also been described in Brazil, Japan, Sweden, and elsewhere. Onset of symptoms usually occurs in the third or fourth decade but may occur later in life. Neuropathic symptoms are pain and paresthesias affecting the feet and legs first, often associated with marked sensory loss, mainly affecting pain and temperature sensation. Initially, a syndrome that mimics lumbosacral syringomyelia develops in the patient, and other sensory modalities are affected later. Autonomic symptoms are prominent and sometimes dominate the clinical picture, especially postural dizziness and hypotension, distal anhidrosis, impotence, urinary retention, and dysfunction of gastrointestinal motility with alternating episodes of diarrhea and constipation. Pupillary abnormalities with escalloped margins are also present. The sensory abnormalities with loss of pain and temperature may predispose to the occurrence of foot ulcers or inadvertent burns. Neuropathic joint degeneration is a late complication. Sensory loss progresses to involve the upper extremities, usually affecting all sensory modalities in later stages. Muscle weakness and areflexia appear as the disease advances. Infiltration of other organs, such as kidneys, heart, and eyes, is typical in this disorder. Amyloid deposits may be found in the flexor retinaculum overlying the median nerve at the wrist and producing symptoms of a median neuropathy at the wrist (carpal tunnel syndrome).
Spinal Cord and Peripheral Neuromuscular Disease
640
Diseases of Peripheral Nerve
FIG. 100-5. Longitudinal section of large myelinated fiber from sural nerve of a patient with HNPP showing uncompacted inner lamellae of myelin characteristic of the disorder (bar = 1 pm). (From Yoshikawa H, Dyck PJ: Uncompacted inner myelin lamellae in inherited tendency to pressure palsy. J Neuropathol Exp Neurol 50:649, 1991, with permission.)
TMLE 100-3. Other Inherited Neuropathies Associated with Known Metabolic Defects Disorder
Genetic Transmission
Clinical Features
Metabolic Abnonnalitv
PathoIonic Findinns
MF loss, demyelination, and Infantile and adult forms; CNS Arylsulfatase A Schwann cell cytoplasm involvementwith mental retardation, blindness, metachromatic granules deafness, hypertonic tetraplegia; PNS involvement with weakness, areflexia, and slow NCV Onset at infancy; CNS white Segmental demyelination, inGalactosylceramidase AR Cloboid cell leukodystrophy clusion material within matter involvement with (Krabbe's disease) regression of motor skills, Schwann cell cytoplasm hypertonicity, seizures, and optic atrophy; PNS involvement with hyporeflexia and slow NCV Loss of MF and UF, Schwann Young males; spastic paraAbnormal P-oxidation of Adrenoleukodystrophy and X-linked adrenomyeloneuropathy paresis, peripheral neuropcell inclusions VLCFA athy, and signs of adrenal insufficiency X-linked Young males; painful smallSmall-fiber neuropathy; glycoa-Galactosidase Fabry's disease fiber neuropathy, anhidrolipid granules in vessels sis, skin angiokeratomas, kidney and vascular disease Three types: asymmetrical AR Tangier disease Clear vacuoles in Schwann Abnormal catabolism of highcell cytoplasm; demyelinadensity lipoproteins; very polyneuropathy with nortion, remyelination, and mal NCV; slowly progresslow plasma cholesterol ing symmetrical polyneuaxonal degeneration ropathy, mainly in the lower extremities; and polyneuropathy with a syringomyelia-like syndrome, orange tonsils Abetalipoproteinemia AR Large-fiber peripheral neuropAbsence of lipoproteins conReduction of MF athy, proprioceptiveloss, taining apolipoprotein B ataxia, pes cavus, atypical retinitis pigmentosa, acanthocvtosis Abnormalities in regulation of Porphyric neuropathy AD Porphyhc attacks painful criWallerian degeneration sis, progressive motor neuheme synthesis (AIP, VP, and HCP) rooathv, or enceohaiooathv Abbreveviotions: AD, autosomal dominant; AIP, acute intermittent porphyria; AR. autosomal recessive; CNS, central nervous system; HCP, hereditary coproporphyria; MF, myelinatedfibers; NCV, nerve conduction velocity; PNS, peripheral nervous system; UF, unrnyelinatedfibers; VLCFA, very long-chain fatty acids; VP, variegate porphyria.
Metachromatic leukodystrophy
AR
PLATE 100-1. Sural nerve biopsy of a patient with familial amyloidosis. Transverse section embedded in paraffin and stained with monoclonal antibodies to transthyretin (TTR). Note perivascular amyloid deposits showing a positive reaction with a monoclonal antibody to l l R .
Chapter 100
The disease runs a progressive course, and patients usually die of renal failure or cardiac complications 10 to 20 years after onset. Electrophysiologic studies in the early stages of the disease show an axonal predominantly distal sensory polyneuropathy with reduced or absent SNAPS and relative preservation of motor conduction velocity and CMAPs. Sural nerve biopsies reveal marked reduction in small myelinated and unmyelinated fibers, with widespread amyloid deposits throughout. Immunohistochemical studies of the amyloid deposits with monoclonal antibodies are helpful in providing evidence of hereditary amyloidosis. Inherited amyloidosis specifically reacts with antiserum against TTR (Plate 100-1). Amyloid deposits are also found in sensory and autonomic ganglia. The mechanism of nerve damage is unknown. Asymptomatic carriers of the mutant TTR gene can be detected by radioimmunoassay of serum. Because the liver mainly produces the abnormally mutated TTR, liver transplantation has been recommended to stop the production of the mutated TTR and modify the natural history of FAP. However, studies have shown limited benefits, mainly limiting the progression of neuropathic deficits in patients with mild neuropathy. Autonomic deficits have not improved, and patients with cardiac manifestations of amyloidosis tend to have a poor outcome after liver transplantation. Patient selection is important to minimize perioperative mortality, which is high in patients with advanced FAP. On balance, it appears that the potential benefits of liver transplantation should be carefully weighed against the risks, taking into account the duration and severity of FA!?. Apolipopmteh A1-Related FAP
The clinical manifestations of apolipoprotein A1 FAP are similar to those of TTR FAP except for early renal involvement and high incidence of duodenal ulcers. Autonomic involvement is not as florid as in TTR FAP. The amyloid of this form is not derived from TTR. The amyloid fibrils consist of a variant of apolipoprotein Al. Gelsolln FAP
Originally described in Finland and formerly know as FAF' IV (Meretoja), Gelsolin amyloidosis is characterized by ocular manifestations. Corneal opacity caused by amyloid infiltration, called lattice corneal dystrophy, is a cardinal clinical feature. A slowly progressive facial palsy with facial skin changes usually supervenes later. A mild generalized peripheral neuropathy without autonomic features may occur later.
Inherited Neuropathy
641
OTHER INHERITED NEUROPATHIES ASSOCIATED WITH KNOWN METABOLIC DEFECTS Other inherited neuropathies are summarized in Table 100-3.
SUGGESTED READINGS Adam D, Samuel D, Goulon-Goeau C et al: The course and prognostic factors of familial amyloid polyneuropathy after liver transplantation. Brain 123:1495, 2000 Ben Othmane K, Middleton LT, Loprest LJ et ak Localization of a gene (CMT2A) for autosomal dominant Charcot-Marie-Tooth disease type 2 to chromosome Ip and evidence of genetic heterogeneity. Genomics 17:370, 1993 Bergoffen J, Scherer SS, Wang S et ak Connexin mutations in X-linked Charcot-Marie-Tooth disease. Science 262:2039, 1993 Dyck PJ: Neuronal atrophy and degeneration predominantly affecting peripheral sensory and autonomic neurons. p. 1065. In Dyck PJ, Thomas PK, Griffin JW et al (eds): Peripheral Neuropathy. 3rd Ed. WB Saunders, Philadelphia, 1993 Dyck PJ, Chance P, Lebo R, Carney JA Hereditary motor and sensory neuropathies. p. 1094. In Dyck PJ, Thomas PK, Griffin JWet a1 (eds): Peripheral Neuropathy. 3rd Ed. WB Saunders, Philadelphia, 1993 Dyck PJ, Litchy WJ, Minnerath S et ak Hereditary motor and sensory neuropathy with diaphragm and vocal cord paresis. Ann Neurol 35:608, 1994 Dyck PJ, Thomas PK, Griffin JW et al (eds): Peripheral Neuropathy. 3rd Ed. WB Saunders, Philadelphia, 1993 Fischbeck KH, ar Rushdi N, Pericak Vance M et ak X-linked neuropathy: gene localization with DNA probes. Ann Neurol20:527, 1986 Hayasaka K, Himoro M, Sawaishi Y et ak De novo mutation of the myelin Po gene in Dejerine-Sottas disease (hereditary motor and sensory neuropathy type 111). Nat Genet 5:266, 1993 Keller MP, Chance PF: Inherited peripheral neuropathy. Semin Neurol 19:353, 1999 Lupski JR, de Oca Luna RM, Slaugenhaupt S et al: DNA duplication associated with Charcot-Marie-Tooth disease type 1A. Cell 66:219, 1991 Mendell J R Charcot-Marie-Tooth neuropathies and related disorders. Semin Neurol 18:41, 1998 Pareyson D Charcot-Marie-Tooth disease and related neuropathies: molecular basis for distinction and diagnosis. Muscle Nerve 22: 1498, 1999 Roa BB, Dyck PJ, Marks HG et al: Dejerine-Sottas syndrome associated with point mutation in the peripheral myelin protein 22 (PMP22) gene. Nat Genet 5:269, 1993
642
Spinal Cord and Peripheral NeuromuscularDisease
Diseases of Peripheral Nerve
10 1 Common Entrapment and Compression
Neuropathies of the Upper Extremity David M. Dawson
CARPAL TUNNEL SYNDROME Carpal tunnel syndrome is the result of compression of the median nerve within the carpal canal, a closed space bounded on the volar surface by the thick transverse carpal ligament. The normal cause of carpal tunnel syndrome is enlargement or hypertrophy of the nine flexor tendons that pass through this closed space. Both vascular effects on the median nerve and the effects of chronic recurring compression appear to play a role in the pathogenesis of the nerve disorder. Briefly stated, it appears that the demyelinative lesion of the nerve, which accounts for the focal nerve conduction slowing and probably for the neurologic symptoms, is a result of compression of the myelin sheaths, distortion of the nodes of Ranvier, and interruption of normal saltatory conduction. Some intermittent symptoms, such as nocturnal tingling, may be caused by interference with blood supply to the nerves because these symptoms are so easily reversible by change in wrist position. Carpal tunnel syndrome is important in two ways that are unique to this disorder. It was the first clinical physiologic correlation to be well described in the earliest days of clinical electromyographic testing in the 1960s, and it is the one entrapment neuropathy for which a major occupational role has been defined. For this latter reason, it is in the forefront of legal and compensation systems calculations, based on an industrywide effort to reduce the high incidence of this disorder in workers. In a review of medical records in Rochester, Minnesota, an incidence of 125 per 100,000 population was calculated in the late 1970s. In a recent survey in the Netherlands, 8% of the interviewees reported nighttime paresthesias of the hand, and of these about one third were found to have carpal tunnel syndrome, an incidence of 220 in 100,000. The prevalence of carpal tunnel syndrome in those who work with their hands is many times these baseline figures. The highest reported incidence thus far is 15%, in a group of meat cutters. The incidence of carpal tunnel syndrome is higher among electronic parts assemblers, musicians, dental hygienists, and of course those who use their hands in nonoccupational ways such as those who knit, do carpentry, or filet fish. In the nonoccupational group of patients with carpal tunnel syndrome, middle-aged women predominate, whereas of those who have an occupational basis for the condition, younger men are the peak population. Clinical Features
The clinical features of carpal tunnel syndrome are known to most practitioners. The most common and easily recognized clinical variant of the illness is slowly progressive nocturnal paresthesias, typically burning and unpleasant, located mostly in the hand. There may be some proximal radiation of the pain into the forearm and arm, rarely above the level of the shoulder. Many patients notice that some wrist positions exacerbate the symptoms, for example, when they drive with the wrist extended on the
steering wheel or when they hold a newspaper. In the earliest stages of the illness the symptoms are intermittent, and there are no neurologic findings on examination. As the condition progresses, symptoms become more persistent, and there may be decreased tactile sensation over the fingertips, typically over the index and middle fingers. Two-point discrimination over the fingertips is a reliable method of testing, as is light pinprick sensation over the dorsum of the fingers. Testing over the palmar surface of the fingers often is difficult, and it should be noted that the palm itself is spared because of the anatomy of the median nerve (i.e., the palmar cutaneous nerve arises proximal to the carpal tunnel). Other clinical variants of carpal tunnel syndrome are known. Some patients have pronounced autonomic disorder from the very beginning, such as sweating and dry skin or features that resemble Raynaud’s phenomenon. A few patients appear to have primary axonal damage from the beginning and present with dense sensory loss and atrophy of the thenar muscles. These patients may complain of weakness, which is most often caused by clumsiness and lack of discriminative ability of the sensory nerve fibers, but a few have weakness of thumb abduction and opposition. Not all patients with carpal tunnel syndrome present with slowly progressive illness; some present with acute loss of function, probably caused by vascular factors. The increased prevalence of carpal tunnel syndrome during pregnancy is well known, typically beginning in the sixth or seventh month and returning to baseline after delivery in more than 90% of women. A few women in whom this disorder develops during pregnancy do not recover sufficiently and have persistent problems. Occupational Considerations
Efforts have been made to define the exact occupational exposures that increase the incidence of carpal tunnel syndrome. These efforts have not been highly successful because there has been disagreement about the necessary features for the diagnosis, with some investigators using primarily neurophysiologic data, which have been unreliable in this setting for reasons that are discussed in this chapter. Highly repetitive wrist movement, vibrating tools, awkward wrist positions, and forceful movements of the hand seem to correlate with a high incidence of carpal tunnel syndrome. Workers whose occupation entails forceful repetitive movement of the hand have a higher incidence of carpal tunnel syndrome, at least ten times higher than that observed in workers who use the wrist without repetition and force. The matter remains under investigation. Some experts have not been able to find these correlations and believe that obesity, age, presence or absence of diabetes, and other nonergonomic factors are equally important. Nevertheless, major efforts are being made throughout the relevant industries to reduce the incidence of carpal tunnel
Chapter 101
Common Entrapmentand CompressionNeuropathiesof the Upper Extremity
syndrome and its major impact on the costs of productivity loss and medical care for affected workers. Electrophysiologic Features The electrophysiologic diagnosis of carpal tunnel syndrome depends on the demonstration of focal slowing of the median nerve at the wrist. This was first demonstrated by Simpson in 1956 and has been a mainstay of the investigation since that time. Distal motor studies across the wrist are easily performed but have a sensitivity of only about 50%. Prolongation of distal latency and conduction block between the palm and wrist are the two abnormalities commonly observed. When an inching technique is used across the palm, the exact area of neurophysiologic abnormality can be seen very clearly, and the sensitivity of the area is increased. The neurophysiologic disorder is localized within the palm, 2 to 4 cm distal to the wrist crease, which is at the distal edge of the volar carpal ligament. The most sensitive criterion for diagnosis of carpal tunnel syndrome is the demonstration of slowing of sensory or mixed nerve conduction at the wrist. Sometimes it is useful to test several digits to detect the abnormality. The use of an internal control, comparing a median conduction study with the analogous ulnar study, increases the electrophysiologicsensitivity to more than 90%. A comparison of the median mixed palmar latency with the ulnar mixed palmar latency across the wrist may prove useful. Likewise, a comparison of the median sensory latency of digit 4 to the ulnar sensory latency of digit 4 (digit 4 usually is dually innervated) is very sensitive in detecting subtle abnormalities of slowing. Comparison of the symptomatic and asymptomatic hands in the diagnosis of carpal tunnel syndrome often is not helpful because the asymptomatic hand is electrically affected in a high proportion of patients. Electromyographyis often used, primarily in the differential diagnosis. In patients with severe carpal tunnel syndrome and axonal loss, the abnormalities shown by electromyography should be seen in the opponens muscle and the abductor pollicis brevis. Approximately 95% of patients with clinically apparent carpal tunnel syndrome have definable neurophysiologic abnormalities. A few patients whose nerve conduction test appears to be normal respond to carpal tunnel release, which constitutes a false-negative result. Inevitably, there are also false positives, of which the most likely is the presence of abnormality in the asymptomatic hand, but there are also confounding false positives produced by other diseases, such as peripheral neuropathy, amyotrophic lateral sclerosis, and cervical spine disease. A well-planned individualized investigation usually can manage these difficulties.
DifferentialDiagnosis The most common differential diagnosis to be considered in a patient with apparent carpal tunnel syndrome is cervical radiculopathy-usually cervical root &which can often be recognized by the presence of neck pain, by pain that radiates to the arm in response to coughing or sneezing, and by a preponderance of pain proximally as opposed to distally (the opposite is true of carpal tunnel syndrome). When neurologic features are present, reflex loss, muscle atrophy, and sensory loss over the dorsum of the hand may be seen. Thoracic outlet syndrome (discussed later in this chapter) is most quickly recognized by showing that the symptoms occur with elevation and abduction of the arm or by showing that the
643
neurologic deficit spans the territories of C8 and T1 nerve roots rather than the median nerve. Proximal median nerve dysfunction is most easily recognized by testing for the function of the flexor pollicis longus, which produces flexion of the distal joint of the thumb, or for flexion or pronation of the wrist. Transient ischemic attacks, affecting the contralateral cerebral hemisphere, usually do not produce anything the patient would describe as pain.
Treatment Conservative management of carpal tunnel syndrome involves splinting the wrist in a slightlyextended position, reducing activity that might have caused the syndrome to develop, and injecting a steroid underneath the volar carpal ligament. The steroid injection can be performed by any practitioner if the median nerve is avoided and the steroid is injected several centimeters proximal to the wrist creases so that it can diffuse among the flexor tendons to reduce swelling and inflammation. The objective of conservative management is to reduce the tissue pressure within the carpal canal, which rises with wrist extension or flexion or as a consequence of inflammation of the flexor tendons. Patients who have progressive symptoms and have not responded to simple conservative measures (Fig. 101-1) should be referred to a surgeon for volar carpal tunnel release. Repeated steroid injections are to be avoided because they can lead to complications. Late-stage carpal tunnel syndrome with advanced atrophy, sensory loss, and few symptoms is not improved by surgery. The rare patients who have acute development of symptoms should be seen as an emergency and operated on promptly because they can have irreversible loss of function. The responses to treatment generally are satisfactory. Patients who use their hands for heavy labor will not be able to return to work for 3 to 4 months after surgery. Those who have a sedentary job can go back to work with a bulky dressing on the wrist within a week. Many patients have some postoperative pain, produced by local pressure on the wrist or use of the wrist, and this may last for several months. The long-term effects of carpal tunnel syndrome surgery are good, but 10% of patients are worse after surgery. ULNAR NEUROPATHY AT THE ELBOW Ulnar neuropathy at the elbow is second only to carpal tunnel syndrome in incidence of entrapment neuropathy of the upper extremity. The patient usually presents with tingling into the little finger, accompanied by some degree of weakness of the hand. With advancing disease, the motor symptoms predominate, and in the end a patient with ulnar neuropathy may lose much hand function, including digital control and grip. This is in contrast to carpal tunnel syndrome, in which the sensory symptoms and pain tend to predominate throughout. The causes of ulnar neuropathy at the elbow are varied. An effort should be made when examining patients to ascertain the cause of the problem, but it must be recognized that even after careful neurophysiologic investigation and a surgical procedure, the exact cause of nerve compression can be difficult to corroborate. Probably the most common cause of ulnar compression at the elbow, particularly in the milder cases and in those associated with repetitive elbow flexion, is cubital tunnel syndrome (Fig. 101-2). In this abnormality the ulnar nerve is compressed by the edge of the aponeurosis of the flexor carpi
644
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Newe
A
B
FIG. 101-1. Carpal tunnel syndrome. (A) A hemostat has been placed under the transverse carpal ligament. The patient's fingers are to the left, and the wrist is to the right. (13) The ligament has been incised, exposing the median nerve directly beneath it. (From Dawson D, Hallet M, Millender L Entrapment Neuropathies. p. 44. Little, Brown, Boston, 1983, with permission.)
ulnaris, located about 2 cm distal to the tip of the elbow when the elbow is flexed. Sometimes a Tine1 sign can be elicited at that exact point, or an inching technique with nerve conduction testing can show that as the point of compression. In some patients, chronic trauma to the nerve, especially when the ulnar groove is shallow, can lead to symptoms. Recurrent subluxation of the nerve, which then rides up over the medial epicondyle, can be associated with ulnar nerve disorder, but it should be recognized that subluxation also occurs in patients who have no symptoms. In previous decades, prior fracture of the olecranon or other damage to the elbow joint would lead to slow progressive scarring of the nerve (tardy ulnar palsy). This condition is not often observed today. Clinical Features
Although sensory complaints are very common in patients with ulnar nerve disorder at the elbow, the sensory loss usually is slight
and is located over the little finger and adjacent parts of the palm. Sometimes the split down the ring finger, showing that the medial side is innervated by the ulnar nerve, is a helpful diagnostic point. The motor loss in ulnar nerve compression is important to verify correctly. Some patients, such as musicians, who need careful digital control, may be more aware of the motor disability than the examination can show. Use of the long-finger flexors and extensors, innervated by radial and median muscles, can compensate for many movements of the digits but not all. Finger abduction, especially abduction of the fifth and index fingers, is easily tested. Adduction is testable as well, especially adduction of the ring finger for which long-finger flexors and extensors cannot substitute. If there is marked weakness of lumbricals and interosseous muscles, power grip may be reduced; the patient may be aware of this, and it can be measured and demonstrated. An important muscle to test in the presence of an ulnar nerve lesion is the long flexor for the fifth finger. This is innervated in the
Chapter 101
H Common Entrapmentand Compression Neuropathiesof the Upper Extremity
forearm by the ulnar nerve and is the only reliably testable muscle in the forearm that is so innervated. The flexor digitorum profundus for digit 5 controls flexion of the terminal phalanx, which can be compared with other flexors in that hand or with the comparable muscle on the other side. Once that muscle has been shown to be abnormal, the site of the lesion is much better defined because ulnar nerve compression at the wrist is thereby excluded. Occupational Considerations
There is no clear-cut occupational exposure that leads to ulnar nerve disorder. Compression of the ulnar nerve can occur in the postoperative period. It is not rare to discover a patient with new weakness and sensory loss in the hand after a period of anesthesia. The mechanism for this is not well known, but sometimes pronounced prolonged flexion of the elbow, extension on an armboard, or compression by an external sharp edge of the table can be confirmed. Musicians seem particularly susceptible to ulnar nerve compression, and it has been observed particularly in violinists and flutists, both of whom practice many hours per day with one arm or both in a flexed position.
Differential Diagnosis The differential diagnosis of ulnar nerve compression at the elbow differs from that of carpal tunnel syndrome. However, the two conditions may be easily confused or confounded because at least one half of the patients interviewed cannot reliably report which digits are affected by paresthesias. Thoracic outlet syndrome (discussedlater in this chapter) may occur in a form in which there is pronounced disorder of the C8 and T1 nerve roots. Usually this is associated with a fibrous band or other structural abnormality of the brachial plexus. Such patients may resemble those with ulnar
645
neuropathy but can be distinguished by the following facts: with C8-T1 root disorder, sensory loss is present over the medial side of the hand but extends upward over the territory of the medial antebrachial cutaneous nerve in the forearm. This does not occur with ulnar nerve palsies. Also, the muscle atrophy in neurogenic thoracic outlet syndrome includes all the muscles in the hand and may begin in the median territory, producing ulnar sensory loss and median weakness. Other problems with the brachial plexus must be considered on occasion, and metastatic carcinoma or stretch injuries of the plexus can resemble ulnar neuropathy as well. This is sometimes seen after cardiac surgery; in such patients the disorder appears to be related to the position of the arm during surgery, producing intrinsic muscle weakness and ulnar sensory loss, usually caused by brachial plexus stretch injury. Treatment
Treatment of ulnar neuropathies at the elbow is less satisfactory than that of carpal tunnel syndrome. Early mild cases may respond to a simple restriction of elbow flexion, using a bivalve cast or orthosis, which can be manufactured by an occupational therapist and worn during periods of rest or at night. Steroid injection therapy plays no role. Inflammatory medication may be helpful. With advancing motor or sensory loss or pain, a surgical approach is indicated. In some patients, especially those with mild early nerve compression, a simple release of the flexor carpi ulnaris aponeurosis, that is, a cubital tunnel release, may be sufficient. Beyond that point, surgeons can choose from several procedures. Some surgeons prefer an epicondylectomy, allowing the nerve to ride anteriorly into the bed of the removed epicondyle. Other surgeons prefer a transposition of the nerve in front of the epicondyle. The results of surgery are more commensurate with the degree of preoperative nerve disorder than they are with the
EPICONDYLE
APONEUROSIS
COLLATERAL LIGAMENT
FIG. 101-2. View of the medial side of the right arm, showing the course of the ulnar nerve past the medial epicondyle and entering the cubital tunnel under the edge of the aponeurosis of the flexor carpi ulnaris. (From Kincaid JC: The electrodiagnosis of ulnar neuropathy at the elbow. Muscle Nerve 1 1 :1005-1015, 1988, with permission.)
646
Spinal Cord and Peripheral Neuromuxulsr Disease
Diseases of Peripheral Nerve
choice of procedure. Generally speaking, the pain is relieved, and some return of function can be anticipated in most cases. The surgical issues and the relationship of the apparent cause of the neuropathy to the choice of procedure are well described by Campbell.
in the brachial plexus by nerve conduction testing are now believed to be erroneous. Likewise, somatosensory testing, using an electrode over the spinal cord, does not appear to contribute to a diagnosis.
RADIAL NERVE ENTRAPMENT Elecbophysiologk Features The techniques for neurophysiologic investigation resemble those for carpal tunnel syndrome. Generally, the search is for an area of focal slowing near the elbow. It is common to find an abnormality of the ulnar nerve, either by a reduction of the ulnar sensory action potential from the fifth finger or by general slowing and dispersion of the motor action potential. Sometimes these occur without a discernible focal slowing or conduction block at the elbow unless there is careful attention to technique. The neurophysiologic differential diagnosis is extensive. Neurogenic thoracic outlet syndrome must be excluded, primarily by showing that there is no focal slowing of the ulnar nerve and that some median nerve innervated muscles are also affected. In addition, the medial antebrachial sensory potential often is useful to study, being reduced or absent in neurogenic thoracic outlet syndrome. Again, comparison with the opposite ulnar nerve may not be an effective technique because the other side can be affected as well. The presence of generalized peripheral neuropathy can be ascertained by showing a reduction in another sensory action potential, such as the radial or the sural nerves. THORACIC OUTLET SYNDROME The diagnosis of thoracic outlet syndrome appears to carry a very high rate of error and does not have the neurologic or electrophysiologic support that exists for other entrapment neuropathies. There are a few patients who have the so-called true neurogenic thoracic outlet syndrome, commonly caused by a fibrous band traversing the brachial plexus. These patients present with weakness, pain, and numbness in the hand according to a very specific neurologic pattern. These patients are very rare, and even recognized experts in the field have seen no more than a handful of cases. The second type of thoracic outlet syndrome is much more common, although the limits of the syndrome are very poorly defined. Patients present with numbness, tingling, and pain in the hand, without demonstrable neurologic deficit. The symptoms often depend on arm or shoulder position. In some centers in the United States the patients are operated on, typicallywith a removal of the first rib through a transaxillary approach. Many patients operated on in this way have persistent or increased symptoms postoperatively, and most neurologists usually do not recommend first rib removal in these circumstances. It may be that the syndrome is produced by shoulder or arm position and is related to muscular spasm. Often it responds to physiotherapy over a period of several months, attesting to the reversible positional nature of the deficit. Electrophysiologic investigation of patients with neurogenic thoracic outlet syndrome demonstrates reduced sensory action potentials in the little finger and medial forearm and denervation changes in many of the intrinsic muscles of the hand (both ulnar and median) and sometimes in the muscles of 'the forearm that contain a C8 component. Patients with functional or reversible thoracic outlet syndrome have normal studies. Earlier reports that slowing can be demonstrated across the thoracic outlet syndrome
The radial nerve can be affected by a compression or entrapment neuropathy in its proximal portions in the forearm. This produces a clinical picture consisting of partial weakness of extensors of the fingers. Because the nerve most commonly compressed is the posterior interosseous branch of the radial nerve, the extensor carpi radialis is not affected, and the patient retains the ability to dorsiflex the wrist, typically with some deviation of the wrist toward the radial side. The other muscles extending the thumb and the fingers may be sequentially or partially affected, often starting on the ulnar side of the hand. This may produce an unusual appearance that, once seen, can be subsequently recognized but is often confusing at first. Entrapment of the posterior interosseous nerve typically does not produce a sensory loss because the superficial radial nerve leaves the parent nerve before the point of the constriction. The radial tunnel syndrome is another version of radial entrapment at the elbow, in which there is pain at the site where this constriction occurs, typically 5 to 10 cm distal to the elbow joint itself. Tenderness there or radiating pain produced by compression during examination may suggest that the radial nerve is affected. This may occur with only minimal weakness of the hand. The electrophysiologicinvestigation of radial tunnel syndrome or radial nerve compression depends on attempting to show slowing to distal radial innervated muscles or electromyographic changes limited to radically innervated muscles. The manner is somewhat controversial, and there appear to be patients who have the syndrome with barely detectable electrophysiologic abnormalities.
MEDIAN NERVE COMPRESSION IN THE FOREARM A number of syndromes have been described in which the median nerve is affected near the elbow, typically within the mass of the pronator muscle. For this reason these syndromes often are collectively called pronator syndrome. A blow on the arm at that point, anomaly of the muscle or of an arterial supply at that point, possibly hypertrophy of the pronator muscle, and compression by the arch of the flexor sublimis muscle have all been described. Because the entire median nerve is affected at that point, one would theoretically expect sensory loss throughout the median nerve territory in the palm and fingers and weakness of finger flexion, wrist flexion, some thumb abduction, and so on. In fact, these findings are quite rare; the pronator syndrome is a rarely authenticated diagnosis, and even when it is found, the deficits in the median nerve seem to be very incomplete or partial. A branch of the median nerve just distal to the pronator muscle is the anterior interosseous nerve. This is a nerve without a cutaneous sensory supply, supplying motor fibers to the flexors of the thumb and index finger. This rarely is involved in compressive lesions within the pronator muscle, and a subcategory of pronator syndrome consists only of anterior interosseous nerve palsy. However, a more prevalent version of anterior interosseous nerve deficit is not compressive at all. It is a subcategory of idiopathic brachial neuritis, also known as Parsonage-Turner syndrome, For
Chapter 102
Common Entrapmentand Compressive Neuropathiesof the Lower Extremity
some reason such patients very often have weakness of the deltoid, biceps, and serratus anterior and the muscles innervated by the anterior interosseous nerve. In summary, patients with a proximal median neuropathy in the region of the elbow should be viewed with skepticism. An anterior interosseous nerve palsy usually is caused by idiopathic brachial neuritis rather than by compression, and surgical exploration is not indicated. In the few patients in whom a pronator syndrome of some type exists, watchful waiting appears to be the best course in view of the vague nature of the syndrome in most instances and its unknown prognosis.
647
Dellon AL, Hament W, Gittelshon A: Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology 43~1673-1677, 1993
Kaplan SJ, Glickel SZ, Eaton RG Predictive factors in the nonsurgical treatment of carpal tunnel syndrome. J Hand Surg [Br] 15:106-108, 1990
Katz JN,Larson MG, Sabra A et al: The carpal tunnel syndrome: diagnostic utility of the history and physical examination findings. Ann Intern Med 112:321-327, 1990 Miller R G Ulnar neuropathy at the elbow. Muscle Nerve 14:97-101, 1991 Nathan PA, Myers LD, Keniston RC et al: Simple decompression of the ulnar nerve: an alternative to anterior transposition. J Hand Surg [Br] 17~251-254, 1992
SUGGESTED READINGS Campbell WW: Ulnar neuropathy at the elbow. pp. 123-175. In Dawson DM, Hallett M, Wilbourn AJ: Entrapment Neuropathies. 3rd Ed. Lippincott-Raven, Philadelphia, 1999 Dawson DM, Hallett M, Wilbourn AJ: Entrapment Neuropathies. 3rd Ed. Lippincott-Raven, Philadelphia, 1999 Dellon AL: Review of treatment results for ulnar nerve compression at the elbow. J Hand Surg [Am] 14688-699, 1989
Rosenbaum RB, Ochoa J L Carpal Tunnel Syndrome and Other Disorders of the Median Nerve. 2nd Ed. Butterworth-Heinemann,Boston, 2002 Silverstein BA, Fine LJ, Armstrong TJ: Occupational factors and carpal tunnel syndrome. Am J Ind Med 11:343-358, 1987 Stock SR: Workplace ergonomic factors and the development of musculoskeletal disorders of the neck and upper limbs: a meta-analysis. Am J Ind Med 1987-107, 1991 Szabo RM, Chidgey L K Stress carpal tunnel pressures in patients with carpal tunnel syndrome and normal patients. J Hand Surg [Am] 14:624, 1989
102 Common Entrapment and Compressive
Neuropathies of the Lower Extremity Bashar Katirji Although not as prevalent as their counterparts in the upper extremity, focal peripheral neuropathies of the lower extremity can be a diagnostic challenge because they are commonly confused with lumbosacral radiculopathies or plexopathies. This is particularly true in older adults, in whom lumbosacral radiculopathies, caused by lumbar spine disease, are common, and incorrect diagnoses may lead to unnecessary spinal surgery.
PERONEAL NEUROPATHY AT THE FIBULAR HEAD Anatomy
In the upper thigh, while sharing a common sheath with the tibial nerve (also called medial popliteal nerve), the common peroneal nerve (also called lateral popliteal nerve) innervates the short head of biceps femoris, the only hamstring muscle it innervates (Fig. 102-1). After separating from the tibial nerve in the upper popliteal fossa, the common peroneal nerve gives off the lateral cutaneous nerve of the calf, which innervates the skin over the upper third of the lateral aspect of the leg. It then winds around the fibular neck, lying in close contact with it, and passes through a tendinous tunnel between the edge of the peroneus longus muscle and the fibula, sometimes called the fibular tunnel. Near that point, the common peroneal nerve divides into superficial and deep branches. The superficial peroneal nerve innervates the peroneus longus and brevis and the skin of the lower two thirds of the lateral aspect of the leg and the dorsum of the foot. The deep peroneal is primarily motor; it innervates the ankle and toe extensors (tibialis anterior, extensor hallucis, extensor digitorum
longus and brevis) and peroneus tertius in addition to the skin of the web space between the first and second toes. Etiology Peroneal neuropathy at the fibular head is the most common compressive neuropathy in the lower extremity, although its exact incidence and prevalence are unknown. In most cases, it results from prolonged compression of the peroneal nerve between an external object and the fibular head. The common predisposing factors for acute compression at the fibular head are as follows: Recent surgery (such as anesthesia for coronary bypass or craniotomy) Weight loss (including anorexia nervosa) Recent prolonged hospitalization (including bed rest, coma) Habitual leg-crossing (usually combined with weight loss) Diabetes Peripheral polyneuropathy Others (prolonged squatting “strawberry pickers,” braces, casts) Intraoperative compression is the most common cause of acute peroneal neuropathy at the fibular neck. The second most common cause is trauma, including blunt or open trauma, as well as surgical nerve injury. Fracture of the fibula, knee dislocation, knee surgery, and arthroscopy, lacerations, and vehicular car accidents may result in peroneal nerve injuries. Stretch injuries of the peroneal nerve may occur after severe inversion sprains of the
Chapter 102
Common Entrapmentand Compressive Neuropathiesof the Lower Extremity
some reason such patients very often have weakness of the deltoid, biceps, and serratus anterior and the muscles innervated by the anterior interosseous nerve. In summary, patients with a proximal median neuropathy in the region of the elbow should be viewed with skepticism. An anterior interosseous nerve palsy usually is caused by idiopathic brachial neuritis rather than by compression, and surgical exploration is not indicated. In the few patients in whom a pronator syndrome of some type exists, watchful waiting appears to be the best course in view of the vague nature of the syndrome in most instances and its unknown prognosis.
647
Dellon AL, Hament W, Gittelshon A: Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology 43~1673-1677, 1993
Kaplan SJ, Glickel SZ, Eaton RG Predictive factors in the nonsurgical treatment of carpal tunnel syndrome. J Hand Surg [Br] 15:106-108, 1990
Katz JN,Larson MG, Sabra A et al: The carpal tunnel syndrome: diagnostic utility of the history and physical examination findings. Ann Intern Med 112:321-327, 1990 Miller R G Ulnar neuropathy at the elbow. Muscle Nerve 14:97-101, 1991 Nathan PA, Myers LD, Keniston RC et al: Simple decompression of the ulnar nerve: an alternative to anterior transposition. J Hand Surg [Br] 17~251-254, 1992
SUGGESTED READINGS Campbell WW: Ulnar neuropathy at the elbow. pp. 123-175. In Dawson DM, Hallett M, Wilbourn AJ: Entrapment Neuropathies. 3rd Ed. Lippincott-Raven, Philadelphia, 1999 Dawson DM, Hallett M, Wilbourn AJ: Entrapment Neuropathies. 3rd Ed. Lippincott-Raven, Philadelphia, 1999 Dellon AL: Review of treatment results for ulnar nerve compression at the elbow. J Hand Surg [Am] 14688-699, 1989
Rosenbaum RB, Ochoa J L Carpal Tunnel Syndrome and Other Disorders of the Median Nerve. 2nd Ed. Butterworth-Heinemann,Boston, 2002 Silverstein BA, Fine LJ, Armstrong TJ: Occupational factors and carpal tunnel syndrome. Am J Ind Med 11:343-358, 1987 Stock SR: Workplace ergonomic factors and the development of musculoskeletal disorders of the neck and upper limbs: a meta-analysis. Am J Ind Med 1987-107, 1991 Szabo RM, Chidgey L K Stress carpal tunnel pressures in patients with carpal tunnel syndrome and normal patients. J Hand Surg [Am] 14:624, 1989
102 Common Entrapment and Compressive
Neuropathies of the Lower Extremity Bashar Katirji Although not as prevalent as their counterparts in the upper extremity, focal peripheral neuropathies of the lower extremity can be a diagnostic challenge because they are commonly confused with lumbosacral radiculopathies or plexopathies. This is particularly true in older adults, in whom lumbosacral radiculopathies, caused by lumbar spine disease, are common, and incorrect diagnoses may lead to unnecessary spinal surgery.
PERONEAL NEUROPATHY AT THE FIBULAR HEAD Anatomy
In the upper thigh, while sharing a common sheath with the tibial nerve (also called medial popliteal nerve), the common peroneal nerve (also called lateral popliteal nerve) innervates the short head of biceps femoris, the only hamstring muscle it innervates (Fig. 102-1). After separating from the tibial nerve in the upper popliteal fossa, the common peroneal nerve gives off the lateral cutaneous nerve of the calf, which innervates the skin over the upper third of the lateral aspect of the leg. It then winds around the fibular neck, lying in close contact with it, and passes through a tendinous tunnel between the edge of the peroneus longus muscle and the fibula, sometimes called the fibular tunnel. Near that point, the common peroneal nerve divides into superficial and deep branches. The superficial peroneal nerve innervates the peroneus longus and brevis and the skin of the lower two thirds of the lateral aspect of the leg and the dorsum of the foot. The deep peroneal is primarily motor; it innervates the ankle and toe extensors (tibialis anterior, extensor hallucis, extensor digitorum
longus and brevis) and peroneus tertius in addition to the skin of the web space between the first and second toes. Etiology Peroneal neuropathy at the fibular head is the most common compressive neuropathy in the lower extremity, although its exact incidence and prevalence are unknown. In most cases, it results from prolonged compression of the peroneal nerve between an external object and the fibular head. The common predisposing factors for acute compression at the fibular head are as follows: Recent surgery (such as anesthesia for coronary bypass or craniotomy) Weight loss (including anorexia nervosa) Recent prolonged hospitalization (including bed rest, coma) Habitual leg-crossing (usually combined with weight loss) Diabetes Peripheral polyneuropathy Others (prolonged squatting “strawberry pickers,” braces, casts) Intraoperative compression is the most common cause of acute peroneal neuropathy at the fibular neck. The second most common cause is trauma, including blunt or open trauma, as well as surgical nerve injury. Fracture of the fibula, knee dislocation, knee surgery, and arthroscopy, lacerations, and vehicular car accidents may result in peroneal nerve injuries. Stretch injuries of the peroneal nerve may occur after severe inversion sprains of the
648
Spinal Cord and PeripheralNeuromuscularDisease W
Diseases of Peripheral Nerve
Cutaneous
distribution
A
F STINER
FIG. 102-1. Course and distribution of (A) the deep and (6) the superficial peroneal nerves. (From Haymaker W, Woodland
B: Peripheral Nerve Injuries. 2nd Ed. WB Saunders, Philadelphia, 1953, with permission.) ankle. Extrinsic masses (osteochondromas, ganglion cysts, lipomas, Baker cysts) or intrinsic nerve sheath tumors (schwannomas, neurofibromas, and neurogenic sarcomas) are more rare. True peroneal entrapment at the fibular tunnel usually is caused by an anomalous firm fibrous arch overlying the nerve but is extremely rare and occurs mainly in athletes, particularly runners. Clinical Features The onset of peroneal neuropathy is acute in intraoperative compression and trauma, although in patients with weight loss or in those hospitalized for a grave illness, the onset is more subacute and, at times, difficult to determine. When peroneal palsy is progressive, a mass lesion, nerve tumor, or, rarely, true entrapment should be suspected. In common peroneal neuropathies, the deep peroneal nerve often is more affected than the superficial nerve because of the topographic arrangement of the common peroneal nerve around the fibular neck. The exiting fascicles, forming the superficialbranch, are placed laterally, and the deep peroneal fibers are located medially in direct contact with the fibular bone. Selective deep peroneal neuropathy is less common, constituting about 5% of all peroneal lesions. Peroneal neuropathies in the thigh (i.e., sciatic nerve lesions affecting the common peroneal
nerve exclusively) are rare, accounting for less than 5% of all peroneal neuropathies. The disorder usually is unilateral but can be bilateral. Foot drop (i.e., severe weakness of ankle dorsiflexion) is the most common presentation of peroneal neuropathy. Foot drop can be complete or partial. The foot may drag behind, get trapped, or cause the patient to fall. Because of weak eversion and unopposed inversion, patients may sprain or fracture their ankles. Although numbness of the leg, usually involving the dorsum of the foot and lower lateral leg, is common, pain is rare. When present, it is deep and ill-defined, usually located around the knee. On examination, weakness is limited to ankle and toe dorsiflexion and to ankle eversion. Ankle inversion, toe flexion, and plantar flexion are normal. Pseudoweakness of ankle inversion is common when the foot drop is complete. To avoid pseudoweakness,the ankle should be dorsiflexed passively to 90 degrees before testing for ankle inversion. Hypesthesia to touch and pain is limited to the lower two thirds of the lateral leg and dorsum of the foot. Tinel's sign sometimes is elicited by percussing the peroneal nerve at the fibular neck. Knee and ankle reflexes and the hamstrings, glutei, and quadriceps muscles are normal. In deep peroneal neuropathy, the sensory manifestations are lacking (except occasionally in the first web space), and ankle eversion is normal.
Chapter 102 rn Common Entrapment and Compressive Neuropathies of the Lower Extremity
649
Common pemned n.--.--
B
FIG. 102-1. Continued Course and distribution of (A) the deep and (13) the superficial peroneal nerves. (From Haymaker W, Woodland B: Peripheral Nerve Injuries. 2nd Ed. WB Saunden, Philadelphia, 1953, with permission.)
Differential Diagnosis Foot drop may result from an upper or lower motor neuron lesion. The lower motor neuron lesions include common and deep peroneal neuropathy, sciatic neuropathy (especiallywhen affecting the common peroneal nerve predominantly or exclusively), lumbosacral plexopathy (particularly with lumbosacral trunk lesion), or L5 radiculopathy. Their clinical manifestations are shown in Table 102-1. Weakness of ankle inversion, toe or plantar flexion, or absent or depressed ankle jerk are key findings not consistent with peroneal nerve lesion. Radicular pain and positive straight leg test (Lasegue test) are common in L5 radiculopathy and may be present in plexopathy or sciatic neuropathy. In a large study of common peroneal neuropathy, physicians, including neurologists, clinically misdiagnosed 43% of patients as L5 radiculopathy or sciatic neuropathy. This was usually because of the difficulty in assessing ankle inversion and eversion in the presence of foot drop.
Electrodiagnosis Nerve conduction studies and needle electromyography (EMG) are essential for both diagnostic and prognostic purposes. Even when the clinical situation is clear, the electrodiagnostic studies help confirm the site of the lesion (fibular head, thigh, deep branch), estimate the extent of injury (based on the conduction
studies data) and its nature (demyelinating versus axonal versus mixed), and thereby predict the expected course of recovery (weeks or months). Nerve Conduction Studies. The peroneal motor and sensory conduction studies should be obtained bilaterally for comparison. In addition to the usual practice of recording the extensor digitorum brevis, it is essential to include the peroneal motor studies, recording the tibialis anterior, for two reasons. First, because the tibialis anterior is the principal ankle dorsiflexor, whether the disorder is demyelinating or axonal (and, thus, the prognosis) should be established using this most clinically relevant muscle. Second, the extensor digitorum brevis is not uncommonly atrophic (presumably caused by tight shoes), resulting in an erroneous conclusion that the lesion is axonal and severe. The findings on nerve conduction studies, shown in Figure 102-2, can be divided into six patterns: conduction block (complete and partial), axonal loss (complete and partial), mixed lesions (conduction block and axonal), and selective deep peroneal lesions. Focal slowing is present in a minority of patients, usually associated with conduction block. Low-amplitude or absent motor responses (consistent with pure axonal loss) are observed in 50% of cases, pure conduction block in 20%, and mixed lesions in 30%. Thus, significant axonal loss is present in at least 80% of the lesions, including cases associated with intraoperative compression. The superficial peroneal sensory amplitude is low to absent in axon loss common peroneal lesions. However, it is normal when
650
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
W Tmu 102-1. The Differential Diagnosis of Common Causes of Foot Drop
Peroneal Neuropathy at the Fibular Head
15 Radiculopathy
Lumbar Plexopathy (Lumbosacral Trunk)
Sciatic Neuropathy (Mainly Peroneal)
Disc herniation, spinal stenosis Weak Weak Normal Normal (unless 51) Poorly demarcated, predominantly big toe Common, radicular
Pelvic surgery. hematoma, prolonged labor Weak Weak Normal Normal (unless S1) Well demarcated to L5 dermatome Common, can be radicular
Hip surgery, injection injury, coma Normal or mildly weak Normal or mildly weak Normal or mildly weak Normal or depressed Peroneal and lateral cutaneous of calf Can be severe
Low in amplitude or conduction block across fibular head Low or absent"
Usually normal but can be low in amplitude
Low in amplitude
Low in amplitude
Normal
Low or absent
Low or absent
Abnormal Normal Normal Normal
Abnormal Abnormal Normal or abnormal Usually normal
Abnormal Abnormal Normal or abnormal Usually normal
Abnormal Normal or abnormal Normal Abnormal
Absent
May be absent
Absent
Absent
Differential Diagnosis
Common causes Ankle inversion Toe flexion Plantar flexion Ankle jerk Sensory loss distribution
Compression (weight loss, perioperative), trauma Normal Normal Normal Normal Peroneal only
Pain
Rare, deep
Electrodiagnosis
Peroneal motor study to EDB or Tib ant Superficial peroneal sensory study Peroneal musclesb Tibia1 L5 muscles' Other L5 musclesd Biceps femoris (short head) Paraspinal muscles fibrillations
"Can be normal in purely demyelinating lesions or lesion of the deep peroneal nerve only. bBelowthe knee: tibialis anterior, extensor digitorum longus, extensor digitorum brevis. extensor hallucis, and peronei. Tibialis posterior and flexor digitorum longus. dCluteusrnedius and tensor fascia lata. Abbreviations: EDB, extensor digitorum brevis; Tib Ant, tibialis anterior.
the lesion is purely demyelinating or limited to the deep peroneal branch. It is also normal in radiculopathy but usually low or absent in lumbosacral plexopathy, sciatic neuropathy, or peripheral polyneuropathy. Therefore, to exclude these possibilities, the tibial motor and sural sensory studies and H reflex study should be performed. Needle EMC. At least one superficial and two deep peroneal innervated muscles should be sampled. In all cases, fibrillation potentials are seen in the affected muscles when studied at least 3 weeks after the onset of foot drop. Sampling nonperoneal muscles such as the tibialis posterior, flexor digitorum longus, or gluteus medius is essential. As shown in Table 102-1, these are normal in peroneal lesions, but abnormal in L5 radiculopathy and lumbosacral plexopathy. In axonal peroneal neuropathies, nonlocalizable by nerve conduction studies, sampling the short head of biceps femoris is necessary to rule out a high (proximal) common peroneal lesion (sciatic neuropathy affecting the peroneal predominantly or exclusively). In these lesions, the short head of the biceps femoris is abnormal. More commonly, when the tibial component of the sciatic nerve is involved, the other hamstrings, gastrocnemius, and abductor hallucis are also affected, but the glutei are spared.
Prognosis
It is difficult to prognosticate based on clinical evaluation only. In general, as with other peripheral nerve injuries, partial lesions fare better than complete lesions because local sprouting reinnervates muscle fibers effectively. The prognosis depends on the pathologic nature of the lesion, as shown in Table 102-2. In a large study of peroneal neuropathy, most patients had prominent axonal loss: Purely axonal lesions without demyelination were present in half of the patients and significant axonal loss in 80%. In contrast to
common belief, this applies equally to the perioperative peroneal neuropathies, including the subgroup following anesthesia for coronary bypass surgery.
In acute compressive lesions, patients should be observed to allow improvement by remyelination or reinnervation. Conduction block lesions recover spontaneously in 2 to 3 months as long as further compression is prevented. Proper padding of beds, prevention of leg crossing, and arrest or reversal of weight loss should be initiated promptly. A kneepad is helpful in ambulating patients. Ankle bracing is important when the foot drop is profound to help in ambulation and prevent ankle contractures and sprains. Surgical intervention is appropriate in certain situations: When the nerve is lacerated and visibly discontinuous. This repair could be primary (at the time of laceration suturing) or secondary (if local infection is feared). When clinical or EMG evidence of reinnervation cannot established in the tibialis anterior 4 to 6 months after. Here, the nerve lesion probably is severe, at least of the third degree. In slowly progressive peroneal neuropathies, a nerve tumor, ganglion, cyst, or, rarely, true entrapment is suspected and the nerve explored after appropriate electrodiagnostic localization. Imaging studies, particularly magnetic resonance imaging, are particularly helpful in these special situations. ~~
SCIATIC NEUROPATHY AT THE HIP OR THIGH Anatomy The sciatic nerve originates from the L4, L5, S1, and S2 roots and leaves the pelvis via the sciatic notch, usually underneath the
Chapter 102
W
Common Entrapmentand Compressive Neuropathiesof the Lower Extremity
2KI
2
K
A
651
lopv&
A
2
K
h I -K O
....................................................... 6
J)
2KI
1x43 2KI
I
O
d
A
....................................................... 01
.......................................................
2 9
2g
D’
~ ~ , - - - f !
......................................................
:-A E
-C
IOrVJ
.......................................................
.y-&&
FIG. 102-2. Diagrams of the nerve conduction studies in peroneal mononeuropathies. (A) Normal; (6 and 6’) “pure” conduction block, partial and complete; (D and D’) ‘bure“axona/ loss, partid and complete; (C) mixed; (€1deep peroneal. RSP, recording site of the superficial peroneal sensoly response; RTA, peroneal motor response, recording tibialis anterior. Proximal latencies are not drawn to scale. (From Katirji MB, Wilbourn AJ: Common peroneal mononeuropathy: a clinical and electrophysiologic study of 116 lesions. Neurology 38:1726, 1988, with permission.)
rn T l w 102-1. Classification and Degrees of Peripheral Nerve Injury Sunderland
First Denree
Second Denree
Third Denne
Seddon Electrophysiology Pathology
Neurapraxia Conduction block Segmental demyelination
Axonotmesis Loss of axons Loss of axons with intact supporting structures
Neurotmesis Loss of axons Loss of axons with disrupted endoneurium
Excellent, recovery is usually complete in 2-3 months
Slow recovery, dependent on sprouting and reinnervation
Protractedand can fail because of misdirected axonal sprouts
Prognosis
Fourth Denree
Fifth Dearee
Neurotmesis
Neurotmesis Loss of axons Loss of axons with disruption of all supporting structures (discontinuous) Impossible without surgical repair
Loss of axons Loss of axons with
disrupted endoneurium and perineurium Unlikely without surgical repair
652
Spinal Cord and PeripheralNeuromuscular Disease W
Diseases of Peripheral Nerve
piriformis muscle, with significant individual variability. It is composed of a lateral division, named the common peroneal nerve or the lateral popliteal nerve, and a medial division named the tibial nerve or the medial popliteal nerve. Though enclosed in a common sheath, these two nerves are separate from the outset and do not exchange fascicles. In the thigh, the tibial component of the sciatic nerve innervates most hamstring muscles (semitendinosus, semimembranosus, and long head of biceps femoris) and supplies a branch to the adductor magnus, and the common peroneal component innervates the short head of biceps femoris only. Etiology Sciatic nerve injury may occur after hip surgery or trauma, after intramuscular gluteal injections, or in the setting of unattended coma (such as with drug overdose) or coma associated with poor positioning (such as in the intensive care unit). Clinical Features
Sciatic neuropathy presents with foot drop, dysesthesia, and sensory loss. On neurologic examination, weakness of ankle dorsiflexion (tibialis anterior) dominates the picture. However, careful examination often detects weakness of hamstrings (knee flexion), gastrocnemius (plantar flexion), or tibialis posterior (ankle inversion). The ankle jerk usually is asymmetrically depressed or absent. Sensory loss and dysesthesia of the sole and dorsum of the foot and lateral leg are common.
D-ferential Diagnosis Partial sciatic nerve lesions, which usually present with foot drop, may be difficult to differentiate from peroneal neuropathy, lumbosacral radiculopathy, and lumbosacral plexopathy (Table 102-1). Careful history and neurologic and electrodiagnostic evaluations often are necessary for accurate diagnosis.
Electrodiagnosls The electrodiagnostic findings in sciatic neuropathy parallel the clinical manifestations. In severe lesions, there is evidence of common peroneal and tibial neuropathies with denervation of the hamstring muscles. In mild to moderate lesions of the sciatic nerve, it is not uncommon for the studies to suggest that the lesion is an axon loss common peroneal neuropathy because the peroneal nerve often is affected more severely than the tibial nerve (Table 102-1). Helpful nerve conduction clues for the presence of a sciatic nerve lesion include an asymmetrically low or absent sural sensory nerve action potential, H reflex, or tibial motor amplitude recording abductor hallucis. Therefore, it is highly recommended that the contralateral H reflex and sural sensory and tibial motor nerve conduction studies be done in all patients with foot drop, especially when a sciatic nerve lesion is considered in the differential diagnosis. Prognosis
The prognosis of sciatic nerve lesions generally is guarded. Many patients continue with residual neurologic findings. Other patients are left with chronic foot pain and disabling manifestations of reflex sympathetic dystrophy (allodynia with skin, nail, and bone dystrophic changes).
Most symptomatic sciatic nerve lesions necessitate pain management. Tricyclic antidepressants and anticonvulsants are the drugs of choice. This, coupled with physical therapy and ankle foot orthosis for foot drop, often assist patients in ambulation. Surgical intervention (neurolysis or grafting) is indicated in severe lesions from which spontaneous recovery is deemed impossible.
FEMORAL NEUROPATHY IN THE PELVIS OR AT THE INGUINAL LIGAMENT Anatomy The femoral nerve (also called the anterior crural nerve) is formed by the combination of the posterior divisions of the ventral rami of L2, L3, and LA spinal roots (the anterior divisions of the same roots form the obturator nerve) (Fig. 102-3). It immediately gives branches to the psoas muscle before it enters its substance. Then, covered by a tight iliac fascia, the femoral nerve passes between the psoas and iliacus muscles, where it innervates the latter. After passing underneath the rigid inguinal ligament, the femoral nerve branches widely into its terminal motor branches (to the quadriceps and sartorius) and sensory branches (to the anterior thigh), including the saphenous sensory nerve, which innervates the medial half of the leg.
EtEology
The femoral nerve can be compressed at the inguinal region or in the retroperitoneal pelvic space. The most common causes of femoral neuropathy are as follows: 1. Compression in pelvis by
a. Retractor blade during pelvic surgery: abdominal hysterectomy, radical prostatectomy, renal transplantation b. Iliacus or psoas retroperitoneal hematoma: anticoagulation (systemic or subcutaneous abdominal heparin), hemophilia, coagulopathy, ruptured abdominal aneurysm, femoral artery catheterization c. Pelvic mass: tumor, abscess, cyst, aortic or iliac aneurysm 2. Compression in the inguinal region by a. Inguinal ligament during lithotomy position: vaginal delivery, laparoscopy, vaginal hysterectomy, urologic procedures b. Inguinal hematoma: femoral artery catheterization, such as for coronary angiography and total hip replacement c. Inguinal lymphadenopathy 3. Stretch injury: hyperextension, dancing, yoga 4. Others: radiation, laceration, misplaced injection By far the most commonly reported causes are those related to pelvic surgery, such as abdominal hysterectomy or radical prostatectomy. During these surgical procedures, the femoral nerve is compressed between the retractor’s blade and the pelvic wall. Most cases occur after the use of self-retracting blades rather than handheld blades. Compression at the inguinal ligament during prolonged lithotomy positioning for various procedures, including vaginal delivery, prostatectomy, and laparoscopy, is not uncommon and probably is underestimated. Acute hemorrhage in the retroperitoneal space within the iliacus muscle and, less commonly, the psoas muscle results in a compartmental syndrome and secondary severe femoral nerve damage. Although diabetes has been reported to cause selective femoral neuropathy, most cases
Chapter 102 W
Common Entrapmentand Compressive Neuropathiesof the Lower Extremity
653
Vastus lateralis------
kstus intermedius-
cutaneous n of thigh
terminal branch
I
Cutanecus distribution from anterlor aspect
Cutaneousdistnbubm from medlal bspect
FIG. 102-3. Course and distribution of the femoral nerve. (From Haymaker W, Woodland B: Peripheral Nerve Injuries. 2nd Ed. WB Saunders, Philadelphia, 1953, with permission.)
are actually caused by more extensive disease affecting the lumbar plexus and roots (diabetic radiculoplexopathy or amyotrophy).
Clinical Features Most femoral neuropathies present acutely with lower extremity weakness. Patients report buckling of the knee and frequent falls, particularly when they attempt to partially flex the knee. When the hip flexors are weak, patients cannot climb steps because they cannot clear the foot of the weak leg from the tread of stairs. Sensory symptoms over the anterior thigh and medial leg are common. Groin or thigh pain is mild (except with retroperitoneal
hematomas). The neurologic examination reveals weakness of the quadriceps muscle (knee extension) with absent or depressed knee jerk. However, thigh adduction is normal. The iliopsoas muscle (hip flexion) usually is weak when the lesion is pelvic. It should be noted that the quadriceps assists in flexing the hip; therefore, mild hip flexion weakness can be falsely attributed to the iliopsoas weakness. Hypesthesia over the anterior thigh and medial calf is common. The presentation of patients with acute iliacus or psoas hematoma is unique. Usually, they experience acute severe pain in the groin, thigh, and sometimes lower abdomen. They often keep the hip flexed to minimize pain because hip extension (such as on
654
Spinal Cord and peripheral Neummuxular Disease W
Diseases of Peripheral Nerve
reversed straight leg test) is extremely painful. In most cases, the neurologic deficit is limited to the femoral nerve, but extensive hematomas may result in damage to the lumbar plexus and even the entire lumbosacral plexus.
Differential Diagnosis Femoral neuropathy should be differentiated from L2, L3, and L4 radiculopathy and from lumbar plexopathy (Table 102-3). Weakness of the thigh adductors, innervated by the obturator nerve, excludes a selective femoral lesion. Positive reversed straight leg test is common in lumbar radiculopathy but may occur with plexopathy and femoral nerve lesion caused by retroperitoneal hematoma. In plexopathy or L4 radiculopathy, weakness of ankle dorsiflexion (tibialis anterior) is common. In patients with femoral neuropathy and severe pain, particularly in the setting of anticoagulation or coagulopathy, a retroperitoneal hematoma should be suspected and a pelvic computed tomography scan obtained urgently.
Eledrodiagnosis The role of electrodiagnosis is confirmative in typical cases but is very helpful when true clinical weakness is not clear because of pain associated with recent abdominal surgery or delivery. In addition, the nerve conduction studies play an important role in predicting prognosis. Nerve Conduction Studies. The femoral motor and saphenous sensory studies should be performed bilaterally for comparison. The saphenous sensory studies are technically difficult in older adults or if there is leg edema. Because the femoral motor response, recording rectus femoris, can be evoked only at one site (the groin), the pathophysiologic process and prognosis depend the size (amplitude or area) of the response. In addition, because most femoral lesions are acute, care should be taken in accounting for the time for wallerian degeneration. The drop in sensory amplitudes lags behind that of motor amplitudes: The former reach their nadir in 8 to 11 days, the latter in 4 to 5 days. Thus, beyond the period necessary for wallerian degeneration (i.e., after 10 to 11 days), the femoral motor amplitude is low or absent and the saphenous sensory response is absent in axonal lesions, but both remain normal in purely demyelinating lesions. Needle EMG. The quadriceps and iliacus muscles should be sampled in all patients with suspected femoral neuropathy. Fibrillation potentials and impaired recruitment are seen in affected muscles. The motor unit potentials are normal unless sprouting has occurred; in that case, they become large (increased in duration, high in amplitude, and polyphasic). If the iliacus is abnormal, the lesion is pelvic, that is, not at the inguinal ligament. The thigh adductors and tibialis anterior are normal in femoral lesions (Table 102-3).
Prognosis In general, femoral neuropathy carries a good prognosis, even when the lesion is caused by axonal loss. Sprouting and reinnervation are optimal because the target muscle (quadriceps) is both proximal and near the site of injury. Among all causes of femoral neuropathies, lesions caused by iliacus compartmental hematoma have the worse prognosis. Demyelinating lesions, such as those after lithotomy positioning, recover completely in 3 to 4 months. The femoral motor amplitude or area, recording rectus femoris, is essential in prognosticating these lesions.
Management To prevent compression at the inguinal ligament, prolonged lithotomy positioning with extreme hip flexion and external rotation should be avoided. Also, avoiding using retractors during pelvic and gynecologic operations practically eliminates the intraoperative femoral nerve injuries. Most cases of femoral neuropathy are treated conservatively. The management of retroperitoneal hematoma (observation versus evacuation) is controversial. Ideally, hematoma evacuation should occur as soon as it is detected and before signs of severe femoral nerve injury occur. Obviously, stopping anticoagulation or correcting coagulopathy is necessary. Physical therapy is recommended in all patients. A knee brace is indicated in patients with severe weakness of the quadriceps to prevent falls.
TARSAL TUNNEL SYNDROME
Anatomy After innervating the gastrocnemius, soleus, tibialis posterior, flexor digitorum profundus, and flexor hallucis longus in the calf, the tibial nerve passes through the tarsal tunnel at the medial aspect of the ankle and innervates the skin and muscles of the sole of the foot (Fig. 102-4). The roof of the tarsal tunnel is composed of a thin fascia, the flexor retinaculum, which connects the medial malleolus to the calcaneus. There, the tibial nerve is accompanied by the tibial artery and the flexor digitorum longus and flexor hallucis longus tendons. At or slightly distal to the tunnel, the nerve divides into its three terminal branches: the calcaneal branch, a purely sensory nerve that innervates the skin of the sole of the heel; the medial plantar nerve, which innervates the abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis in addition to the skin of the medial sole and, at least, the medial three toes; and the lateral plantar nerve, which innervates the abductor digiti quinti pedis, flexor digiti quinti pedis, adductor hallucis, and interossei in addition to the skin of the lateral sole and two lateral toes.
rn TABLE102-3. Differential Diagnosis of Femoral Neuropathy Thigh adducton Tibialis anterior (ankle dorsiflexion) Saphenous sensory nerve action potential ParasDinal fibrillations 'Abnormal in L4 radiculopathy only. bNormal in purely demyelinating lesions.
Femoral Neuropathy
Lumbar Plexopathy
lumbar Radiculopathy
Normal Normal Usually low or absentb Absent
Abnormal Abnormal Low or absent Absent
Abnormal Abnormal' Normal May be absent
Chapter 102 rn Common Entrapment and Compressive Neuropathies of the Lower Extremity
655
Etiology Tibia1 N e r v e
Flexor Retinaculum Branches Quadratus Plantae Muscle Lateral Plantar N e r v e
Medial Plantar Nerve Abductor HallucisMuscle FIG. 102-4. The tibial nerve at the ankle with its three terminal branches. (From Qck PJ, Thomas PK: Peripheral NeuroPathY. 3rd Ed.
WB Saunders, Philadelphia, 1993, with permission.)
Tarsal tunnel syndrome (TTS) is an uncommon disorder caused by compression of the tibial nerve or any of its three terminal branches under the flexor retinaculum. TTS is sometimes called medial tarsal tunnel syndrome to distinguish it from anterior tarsal tunnel syndrome, which is an entrapment of the terminal segment of the deep peroneal nerve under the extensor retinaculum in the dorsum of the foot. Many reported cases lack objective neurologic signs or electrophysiologic confirmation. Most well-documented cases are unilateral and idiopathic. Biomechanical causes, such as ill-fitting footwear or heel varus and valgus deformity may precipitate TTS, and runners, joggers, and dancers are at particularly high risk for developing this entrapment. TTS may also result from fibrosis caused by remote trauma to the ankle (sprain, fracture, or dislocation), tenosynovitis with or without rheumatoid arthritis, or mass lesion within the tunnel (varicose veins, ganglion, lipoma, schwannoma).
TAW 102-4. Other Entrapment and Compressive Neuropathies in the Lower Extremity NeNe
True Syndromes Lateral femoral cutaneous (meralgia paresthetica)
Ilioinguinal (inguinal neuralgia)
causes
Clinical Manifestations
Differential Diagnosis
Management
Entrapment at the inguinal ligament (idiopathic, pregnancy, obesity, diabetes, belt, beeper), pelvic mass, pelvic hematoma, or abdominal surgery Inguinal hernia repair, appendectomy, retroperitoneal mass or incision
Paresthesia and pain (deep and superficial) in lateral thigh; exam: well-demarcated sensory impairment of the lateral thigh; sensory conduction study technically difficult
L3 or L2 radiculopathy; femoral neuropathy
Burning pain in the lower abdomen, groin radiating to the scrotum and upper thigh, worse with walking; exam: sensory disturbance along inguinal ligament Painful paresthesias in upper thigh, scrotum, and medial groin; exam: sensory disturbance in scrotum and upper thigh, absence of cremasteric reflex Asymmetrical abdominal wall bulging and trivial sensory loss in suprapubic area Numbness in medial thigh with variable pain; exam: sensory loss in medial thigh; saphenous sensory conduction study useful
Cenitofemoral neuropathy (diagnostic nerve block might be needed), L1 or L2 radiculopathy, hip joint disease
Conservative because most resolve in months; local steroids sometimes helpful; decompression at the inguinal ligament rarely needed Analgesia and nerve blocks in postoperative cases; rarely, surgical exploration
Cenitofemoral
Appendectomy, inguinal hernia repair
lliohypogastric
Retroperitoneal mass or incision (nephrectomy)
Saphenous
Surgery for varicose veins or removal of saphenous vein for coronary artery graft. knee surgery, entrapment at Hunter's canal Hip surgery, pelvic fracture, obturator hernia, malignant pelvic neoplasm
Obturator
llioinguinal neuropathy (diagnostic nerve block might be needed), L1 or U radiculopathy, hip joint disease
Conservative
llioinguinal or genitofemoral neuropathy, L1 or L2 radiculopathy L4 radiculopathy, mild femoral neuropathy
Conservative
Leg weakness, pain, and paresthesias in thigh and inner leg; exam: weakness of thigh adductors
U and U radiculopathy,
Dependent on primary cause; surgical exploration rarely needed
Pain in the buttock and leg with ill-defined paresthesias; exquisite buttock tenderness near the sciatic notch; normal neurologic and electrodiagnostic examinations
Lumbosacral radiculopathy, particularly L5 and S1, hip joint disease, bursitis
Trivial; usually foot paresthesias and deep ankle pain; exam: atrophy of extensor digitorum brevis and hypesthesia in first web
Asymptomatic atrophy of extensor digitorum brevis, common or deep peroneal neuropathy at fibular head, L5 radiculopathv, arthritis
lumbar plexopathy, femoral neuropathy
Conservative; exploration of Hunter's canal rarely indicated
Disputed Syndromes
Piriformis syndrome
Anterior tarsal tunnel syndrome
Compression of the sciatic nerve at the pelvic outlet by the overlying piriformis muscle; history of trivial trauma to the buttock common; compressive bands or vessels common at surgery Compression of terminal segment of deep peroneal nerve by superficial fascia of ankle (tight shoes, fractures, sprains)
Conservative with physical therapy (prolonged stretching of piriformis muscle by flexion, adduction and internal rotation of the hip); surgical exploration rarely indicated Conservative with foot orthosis or local steroids
656
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Peripheral Nerve
Clinical Features
The most common symptom of TTS is burning pain and numbness of the foot and ankle, which may worsen after prolonged standing, walking, running, or jogging. Paresthesias in the sole without pain are less common, and subjective weakness and imbalance are extremely rare. The neurologic examination should document sensory impairment in the sole in the distribution of one or all of the terminal branches. The sensory loss spares the heel (innervated by the calcaneal branch) in 40% of patients. In 25% of patients with TTS, the sensory loss is only in the medial plantar nerve distribution, and in 10% it follows the lateral plantar nerve selectively. Tinel's sign, induced by percussion of the tibial nerve at the flexor retinaculum, is present in most patients. Muscle atrophy in one sole may be detected. Weakness is rare because the long toe flexors are intact. The ankle jerk and sensation of the dorsum of the foot are normal. Electrodiagnosis
Similar to the clinical presentation, the electrodiagnostic evaluation of the plantar nerves can be difficult for two reasons. First, sensory nerve action potentials, using surface stimulations and recordings, are technically difficult to elicit, especially in older adults with foot calluses or ankle edema. They are often absent in asymptomatic subjects. Second, needle examination of the muscles of the sole is painful and may show denervation changes in asymptomatic subjects, especially older adults. Nerve Conduction Studies. Both the motor and sensory studies should be attempted bilaterally for comparison. In addition to the routine tibial motor studies, recording abductor hallucis, the tibial motor study recording the abductor digiti quinti pedis should also be performed. The former evaluates the medial plantar nerve, and the latter evaluatesthe lateral plantar nerve. The amplitudes are low and latencies slow in less than half of the patients.
The orthodromic mixed plantar studies of the medial and lateral plantar nerves should be obtained by percutaneous (surface) stimulation of the medial and lateral plantar nerves on the sole of the foot while recording with surface electrodes over the tibial nerve posterior to the medial malleolus. These studies are the counterparts of the orthodromic median and ulnar palmar mixed studies performed to evaluate carpal tunnel syndrome. They are more sensitive than the motor studies but may be difficult to elicit in patients with foot calluses, ankle edema, or foot deformities, or even in normal adults over 45 years of age. Asymmetrical slowing or asymmetrically absent responses are diagnostic. Techniques for assessing solely the sensory fibers of the medial and lateral plantar nerves may be done but are technically difficult, must be averaged, and are not popular. Near-nerve needle recordings and stimulations have been advocated but are invasive and painful and may result in foot infection. Needle EMG. Sampling of the abductor hallucis and abductor digiti minimi pedis may show chronic neurogenic changes with or without fibrillations. Differential Diagnosis
The diagnosis of TTS is difficult because foot pain can be seen in a variety of orthopedic, rheumatologic, and neurologic conditions, including stress fracture, bursitis, arthritis, plantar fascitis, lumbosacral radiculopathy, peripheral polyneuropathy, and reflex sympathetic dystrophy. Accurate diagnosis is particularly difficult in patients with a prior history of trauma, and differentiating TTS from reflex sympathetic dystrophy can be challenging. Careful evaluation of the ankle and foot, including radiographs, bone scan, tomography, and EMG, often is necessary for correct diagnosis. Lesions of the medial or lateral plantar nerves at the tarsal tunnel may mimic selective lesions of these nerves within the sole of the foot, which may be caused also by trauma, bunion surgery, foot deformities (such as pes cavus), arthritis, or synovial cyst. A
llioinguinal Nerve T12
lliohypogastric Nerve Dorsal Nerve of Penis Perineal Nerves
Lateral Cutaneous Nerve of Thigh
Femoral & Genital Branches of Genito-femoral Nerve Obturator Nerve
Femoral Nerve
FIG. 102-5. Innervation of the skin of inguinal area and the upper thigh. (From Stewart JD: Focal Peripheral Neuropathies. 2nd Ed. Raven Press, New York, 1993, with permission.)
Chapter 102
Common Entrapment and Compressive Neuropathies of the Lower Extremity
careful history and a Tinel's sign distal to the tarsal tunnel are useful features. Electrodiagnostically, TTS should be differentiated from peripheral polyneuropathy and S l-S2 radiculopathies. The sural sensory or H reflex studies are abnormal in polyneuropathy, and the findings usually are symmetrical. In S1 radiculopathy, other muscles innervated by the S 1 root (such as the gastrocnemius) usually are affected, and the H reflex study usually is abnormal.
Prognosis Most patients improve without sequelae. Unfortunately, some patients, especially those associated with ankle trauma, may develop chronic pain and features of reflex sympathetic dystrophy.
Conservative treatment should be initiated in all patients first. Sources of pressure, such as ill-fitting shoes, should be identified and eliminated. Other conservative measures include minimizing ankle edema by elevation and special stockings, medial arch support o r bracing the foot with a light orthosis, antiinflammatory agents, or local injection with long-acting corticosteroids. Only a small proportion of patients need surgical decompression, and results vary. Good results can be achieved by selecting patients with documented entrapment in whom conservative treatment failed or patients with an identifiable mass. Less common compressive and entrapment neuropathies in the lower extremity are summarized in Table 102-4 and shown in Figure 102-5.
SUGGESTED READINGS Al Hakim M, Katirji MB Femoral mononeuropathy induced by the lithotomy position: a report of 5 cases and a review of the literature. Muscle Nerve 16891-895, 1993 Devi S, Lovelace RE, Duarte N: Proximal peroneal nerve conduction velocity: recording from anterior tibial and peroneus brevis muscle. Ann Neurol 2116-119, 1977
657
Goldman JA, Feldberg D, Dicker D et al: Femoral neuropathy subsequent to abdominal hysterectomy. A comparative study. Eur J Obstet Gynecol Reprod Biol 20:385-392, 1985 Katirji B: Peroneal neuropathy. Neurol Clin 17:567-591, 1999 Katirji MB, Lanska DJ: Femoral mononeuropathy after radical prostatectomy. Urology 36539-540, 1990 Katirji MB, Wilbourn AJ: Common peroneal mononeuropathy: a clinical and electrophysiologicstudy of 116 lesions. Neurology 38:1723-1728, 1988 Katiji MB, Wilbourn AJ: High sciatic lesions mimicking peroneal neuropathy at the fibular head. Neurol Sci 121:172-175, 1994 Kent KC, Moscussi M, Gallagher SG et ak Neuropathy after cardiac catheterization: incidence, clinical patterns and long term outcome. J Vasc Surg 19:1008-1012, 1994 Kim DH, Kline DG: Management and results of peroneal nerve lesions. Neurosurgery 39:312-319, 1996 Kim DH, Kline D G Surgical outcome for intra- and extrapelvic femoral nerve lesions. J Neurosurg 83:783-790, 1995 Kuntzer T, van Melle G, Regli F: Clinical and prognostic features in unilateral femoral neuropathies. Muscle Nerve 20:205-211, 1997 Kvist-Poulsen H, Bore1 J Iatrogenic femoral neuropathy subsequent to abdominal hysterectomy: incidence and prevention. Obstet Gynecol 60516-520, 1982 Oh SJ, Meyer RD: Entrapment neuropathies of the tibial (posterior tibial) nerve. Neurol Clin 17:593-615,1999 Oh SJ, Sarala PK, Kuba T, Elmore R S Tarsal tunnel syndrome: electrophysiologicalstudy. Ann Neurol 5:327-530, 1979 Parziale JR, Hudgins TH, Fishman LM: The piriformis syndrome. Am J Orthop 25:819-823, 1996 Pickett JB: Localizing peroneal nerve lesions to the knee by motor conduction studies. Arch Neurol 41:192-195, 1984 Radin E L Tarsal tunnel syndrome. Clin Orthop 181:167-170, 1983 SourkesM, Stewart J D Common peroneal neuropathy: a study of selective motor and sensory involvement. Neurology 41:1029-1033, 1991 Sunderland S The relative susceptibilityto injury of the medial and lateral popliteal divisions of the sciatic nerve. Br J Surg 41:300-302, 1953 Vargo MM, Robinson LR, Nicholas JJ, Rulin MC: Postpartum femoral neuropathy: relic of an earlier era? Arch Phys Med Rehabil71:591-596, 1990 Young MR, Norris Femoral neuropathy during anticoagulant therapy. Neurology 26:1173-1175, 1976 Yuen EC, Olney RK, So YT: Sciatic neuropathy: clinical and prognostic features in 73 patients. Neurology 441669-1674, 1994 Yuen EC, So YT, Olney RK: The electrophysiologic features of sciatic neuropathy in 100 patients. Muscle Nerve 18:414-420, 1995
SECTION
4
DISEASES OF NEUROMUSCULAR TRANSMISSION
103 Myasthenia Gravis David C. Preston The neuromuscular junction (NMJ) forms an electrochemical link transmitting the nerve action potential to muscle. A variety of disorders are known to impair the NMJ at the presynaptic or postsynaptic membrane. Among these disorders, myasthenia gravis (MG) is the most common, with an incidence of 2 to 10 cases in 100,000 people per year. Over the last 30 years, the autoimmune pathophysiology of MG has been well elucidated with the recognition of antibodies directed against the nicotinic acetylcholine receptor. Because this disorder is treatable and potentially curable, prompt recognition, especially early in the clinical course, is important. Mortality and morbidity, once not unusual in patients with MG, have been dramatically reduced in the modem era with early diagnosis and the use of immunosuppression, plasma exchange, and thymectomy.
CLINICAL FEATURES Patients with MG present with muscle weakness and fatigue. Because the disorder is limited to the NMJ, there is no abnormality of mental state, sensory function, or autonomic function. Myasthenic weakness characteristically affects the extraocular muscles, bulbar muscles, proximal limb muscles, or a combination of these. Eye findings are the most common, with ptosis and extraocular muscle weakness occurring in more than 50% of patients at the time of presentation and developing in more than 90% at some time during their illness. Often, extraocular weakness may begin asymmetrically,with one eye involved and the other spared. A very small amount of extraocular weakness is subjectively noticed by the patient as visual blurring or frank double vision. Myasthenic weakness has been known to mimic third, fourth, and sixth cranial nerve palsies as well as, rarely, an intranuclear ophthalmoplegia. Unlike third nerve palsies, however, MG never affects pupillary function. Fixed extraocular weakness tends to occur later. After extraocular weakness, bulbar muscle weakness is most common, with difficulty in chewing, swallowing, and speaking. Some patients experience severe fatigability and weakness of mastication and are unable to keep the jaw closed after chewing. Myasthenic speech is nasal (from weakness of the soft palate) and slurred (from weakness of the tongue, lips, and face) but without any difficulty with fluency. When limb weakness develops in patients with MG, the proximal musculature usually is affected, often in a symmetrical pattern. Patients complain of difficulty arising from chairs or going up and down stairs, reaching with their arms, or holding their head up. Rare patients present with a limb-girdle form of myasthenia gravis alone, without weakness of eye movement or bulbar muscles. 658
The hallmark of MG is pathologic fatigability, that is, progressive muscle weakness with use. Patients typically improve after rest or upon arising in the morning, with worsening as the day passes. Generalized fatigue is a common complaint in many neurologic and non-neurologic disorders. In MG and other disorders of the NMJ, fatigue is limited to muscular fatigue alone and often progresses to frank muscle weakness. Patients with MG do not generally experience a sense of mental fatigue, tiredness, or sleepiness. The clinical examination in a patient suspected of having MG is directed at assessing muscular strength and demonstrating pathologic fatigability. When trying to assess subtle weakness, it is often more useful to observe the patient walking and performing functional tasks, such as arising from a chair or the floor, rather than relying on manual muscle strength testing. Pathologic fatigability may be demonstrated by having the patient look up for several minutes (looking for ptosis or extraocular weakness) and count aloud to 100 (looking for nasal or slurred speech) or by repetitively testing the proximal limb or neck muscles. The remainder of the neurologic examination is normal. Reflexes are generally preserved or are reduced in proportion to the amount of muscle weakness. MG may develop at any age, although it is more common in younger and middle-aged adults; women slightly outnumber men among younger patients, but more men are afflicted among middle-aged and older patients. In patients with MG, there is a well-recognized association of abnormalities of the thymus gland. Thymic hyperplasia is found in as many as 70% of all cases, and thymoma is found in 11%. Although the role of the thymus is not completely understood in MG, it is probably important in initiating and maintaining the autoimmune response. Another interesting group of patients with MG is the 15% who have the ocular form of the disease, whose symptoms remain limited to the extraocular and eyelid muscles. When patients first present with fluctuating extraocular weakness, it is not possible to predict from either clinical or laboratory testing whether the disease will subsequently generalize or remain in the benign restricted ocular form. If a patient has had restricted ocular myasthenia for 1 to 2 years, there is a high likelihood that the myasthenia will never generalize and will remain limited to the extraocular muscles. This has some implications for treatment because patients with ocular MG do not develop crises or other severe complications of generalized MG. Autoimmune MG may be seen in two other groups. Transient neonatal MG is recognized in 21% of neonates born to mothers with MG. Maternal immunoglobulin G (IgG) antibodies directed
Chapter 103
against the acetylcholine receptor are passed through the placenta, resulting in the same clinical syndrome. The illness usually is mild and self-limited, disappearing over the first few months of life as the maternal antibodies are degraded. Finally, MG may be seen as a complication of penicillamine treatment. The clinical syndrome is similar except that many patients slowly improve once the penicillamine has been withdrawn.
DIAGNOSIS The diagnosis of MG usually is straightforward and based primarily on the recognition of the clinical pattern of the disease, followed by the appropriate laboratory, electrophysiologic, and radiologic evaluations (Table 103-1). Tensilon lest
The Tensilon test is a simple and quick method to evaluate the possibility of neuromuscular junction disease. Tensilon (edrophonium hydrochloride), a short-acting acetylcholinesterase inhibitor, is given intravenously, which may quickly reverse myasthenic weakness. It is most useful when there is an obvious objective clinical parameter to follow (e.g., degree of ptosis or extraocular muscle weakness). The clinician cannot rely on subjective improvement by the patient. When performing a Tendon test, a double-blinded study is preferable. Two 1-mL syringes are drawn up: one with 10 mg of Tendon and the other with saline. The syringes are coded with the physician performing the test unaware of which one contains the Tendon. One syringe is selected. A test dose of 2 mg is given and flushed with normal saline. If no response is seen within 1 minute, the additional 8 mg is given, followed by a saline flush. A response is looked for over the next 3 minutes. The procedure is then repeated with the second syringe. Side effects of Tendon are those of cholinergic excess (e.g., salivation, bradycardia, tearing). Atropine should be readily available if needed to counteract these side effects. Although Tendon is generally considered a safe test, care must be exercised in all patients, especially older patients with cardiac disease, because, infrequently, bradycardia may lead to syncope, and in exceptional cases asystole has been documented. Acetylcholine Receptor Antibodies
Acetylcholine receptor antibodies are detected in more than 85% of patients with generalized MG. Antibodies are much less common in patients with restricted ocular MG, occurring in only 50% of cases. Acetylcholine receptor antibodies are highly specific for MG, with few false-positive results. In general, myasthenic patients with circulating antibodies have a high incidence of
ed Tendon test (preferably double blinded with cardiac monitoring) Acetylcholine receptor antibodies Anti-nuclear antibodies (ANA) Thyroid function tests Routine nerve conduction studies and EMC followed by repetitive nerve stimulation of both distal and proximal nerves Single-fiber EMC if repetitive nerve stimulation is negative or equivocal Chest imaninn KT or MRI)
Myasthenia Gravis
659
thymic abnormalities. Autoantibodies against other tissues including thyroid and gastric tissues often are present also. Autoimmune thyroid disease is particularly common and eventually develops in 5% to 12% of patients. RepetlUve Nerve Stimulation
Repetitive nerve stimulation (RNS) is an effective way to fatigue the NMJ and cause acetylcholine depletion. These studies are abnormal in more than 60% of myasthenic patients. A decremental response on RNS is the electrical correlate of clinical muscle fatigue and weakness in myasthenic patients. In normal subjects, slow RNS (2 to 3 Hz) results in little or no decrement, but in cases of MG, a decrement of the compound muscle action potential of 10% or more is characteristically seen. Both distal and proximal nerves can be tested. Although RNS of distal nerves (e.g., the ulnar nerve) is technically easier to perform, the diagnostic yield increases with stimulation of proximal nerves (i.e., spinal accessory, musculocutaneous, or facial nerves), which is not unexpected because the proximal muscles often are much more involved clinically than the distal ones. Every patient undergoing RNS also should undergo routine nerve conduction studies and electromyography (EMG). Although RNS is a sensitive test for MG, a variety of other disorders (e.g., any severe denervating disease, such as amyotrophic lateral sclerosis, the myotonic disorders, severe myopathies, and the Lambert-Eaton myasthenic syndrome) can also cause a decremental response that will be missed unless a complete study is performed. Single-Fiber EMG
Normally, when a motor axon is depolarized, the action potential travels distally and excites all the muscle fibers within that motor unit at roughly the same time. The variation in the time interval between the firing of adjacent muscle fibers from the same motor unit (jitter) can be measured with single-fiber EMG (SF-EMG). Jitter typically is prolonged in disorders of the NMJ even without overt clinical weakness. In addition, SF-EMG may demonstrate blocking of muscle fibers (i.e., the endplate potential of one muscle fiber of a motor unit falls below threshold, and subsequently its muscle fiber action potential is not generated). The clinical correlate of blocking is muscle weakness. In patients who have difficulty cooperating with the examination, stimulated SF-EMG can be done. In stimulated SF-EMG, an additional needle electrode is inserted in the muscle near the endplate to stimulate axonal twigs while the SF-EMG needle electrode records muscle fiber action potentials. Often the extensor digitorum communis muscle is selected for study. If possible, it is always useful to study a clinically involved muscle. Indeed, a normal single-fiber examination in a clinically weak muscle effectively rules out the diagnosis of MG. SF-EMG is the most sensitive test to demonstrate impaired neuromuscular junction transmission (abnormal in 95% to 99% of patients with generalized MG). However, it must be emphasized that SF-EMG, although quite sensitive, is not specific, and it is typically abnormal in neuropathic and myopathic disease. Although it might be tempting to consider having any patient with fatigue undergo SF-EMG, the test is best reserved for patients in whom the diagnosis of MG is strongly suspected and other tests have been negative or equivocal. SF-EMG often is a technically demanding examination for the patient and the electromyographer.
660
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of NeurornuscularTransmission
Every patient with MG should undergo routine chest imaging with either computed tomography (CT) or magnetic resonance imaging (MRI) to look for evidence of thymic hyperplasia or thymoma. The presence of a thymoma is a clear indication for subsequent thymectomy. Early diagnosis of thymoma is important before invasion of the tumor beyond its capsule has occurred, with likely metastasis.
sion). In postsynaptic disorders such as MG, the number of quanta released by each stimulus is normal, but the effect of each quantum on its receptor is reduced. The net result is a lower endplate potential and a reduced safety factor of transmission at the NMJ. Thus, with slow repetitive stimulation in postsynaptic disorders, the endplate potential in some fibers may fall below threshold, with a resulting lack of a muscle fiber action potential. Clinically this manifests as signs and symptoms of weakness and fatigability, with a corresponding decrement during slow RNS.
ETIOLOGY
TREATMENT
The pathophysiology of MG is now well understood. MG is an autoimmune disease caused by sensitized T-helper cells and an IgG-directed attack on the nicotinic acetylcholine receptor of the NMJ. Thus, it is a disorder caused predominantly by antiacetylcholine receptor antibodies. A variety of experimental steps supports this hypothesis:
The treatment of patients with MG has improved substantially. Many options are available. Treatment consists of symptomatic agents (acetylcholinesterase inhibitors), immunosuppressives (steroids, azathioprine, cyclosporine), plasma exchange, intravenous immunoglobulin, and thymectomy.
Chest Imaging
Antibodies are present in the serum of most patients with MG. Antibodies can be passively transferred to animals, producing experimental myasthenia. Removal of antibodies allows recovery. Immunization of animals with an acetylcholine receptor produces antibodies and can provoke an autoimmune disease (experimental autoimmune MG), which closely resembles the naturally occurring disease. The mechanism of antibody damage to the receptor and motor endplate probably involves several steps. First, there is a complement-directed attack with destruction of the acetylcholine receptor and the junctional folds. Second, binding of the antibody to the receptor can cause stearic hindrance of acetylcholine binding at a neighboring site. Third, antibody binding can also result in increased removal of acetylcholine receptor from the membrane (modulation). Finally, rarely the antibody can bind to the acetylcholine receptor binding site itself and directly block acetylcholine binding. As mentioned earlier, there is a high incidence of thymic abnormalities in patients with MG. Fifty percent of patients with thymoma have MG. The role of the thymus in initiating and maintaining the autoimmune response in MG is unclear. However, it is notable that mammalian thymus expresses an acetylcholine receptor similar to that of embryonic muscle, and it is possible that this intrathymic acetylcholine receptor is the primary antigen-provoking antibody formation in the pathogenesis of MG. The abnormal and reduced numbers of acetylcholine receptors lead to impaired NMJ transmission. When a nerve action potential invades and depolarizes the presynaptic junction, voltagedependent calcium channels are activated, allowing an influx of calcium. The influx of calcium then results in release of acetylcholine from the presynaptic terminal. Acetylcholine is packed and released in discrete amounts known as quanta. Acetylcholine quanta then diffuse across the synaptic cleft and bind to acetylcholine receptors in the postsynaptic membrane, resulting in an endplate potential. Normally, the endplate potential is well above threshold and causes the generation of a muscle action potential. With slow repetitive stimulation (2 to 3 Hz), the number of quanta is greatly depleted during the first several seconds, and, subsequently, fewer are released. The corresponding endplate potential falls in amplitude but normally remains above threshold to ensure generation of a muscle action potential with each stimulation (i.e., the normal safety factor of NMJ transmis-
Acetylcholinesterase Inhibitors Symptomatic treatment consists primarily of giving acetylcholinesterase inhibitors such as pyridostigmine. These agents slow the degradation of acetylcholine in the synaptic cleft and effectively increase the amount of neurotransmitter available at the postsynaptic junction. Mestinon has a short half-life and must be dosed every 4 to 6 hours. The optimal dosage varies widely among patients. Patients typically are begun on half a tablet (30 mg) of pyridostigmine every 6 hours and slowly titrated to a higher dosage or more frequent dosing interval. There is no correct dosage. Some patients improve substantially on three to four tablets a day; others need far more. The major side effects are those of cholinergic excess, especially abdominal cramping and diarrhea, excessive perspiration, and salivation. Of course, excessive amounts can also cause weakness (cholinergic crisis). Most patients with MG respond well, at least initially, to these medications. Restricted ocular MG tends to be more refractory than generalized disease. For patients who have difficulty upon awakening in the morning, a slow-release form (Mestinon Timespan) is available as a 180-mg dose to be taken at bedtime.
Although acetylcholinesterase inhibitors are effective in most patients, the response generally is not completely satisfactory, and most patients have a better long-term response if the primary pathophysiology of the disease, the immune mechanism, is addressed. This consists of immunomodulating treatments such as steroids, other immunosuppressives, intravenous immunoglobulin, plasma exchange, and thymectomy. Steroids are the mainstay of therapy in MG. Improvement, including remission, usually can be obtained with oral steroids. The typical prednisone dosage is 1 mg/kg/day, taken as a single dose in the morning. Patients often are started on a low dosage (10 to 20 mg daily) while under close supervision or in the hospital because steroids, especially at high dosages, may cause transient worsening of myasthenia during the first 2 to 3 weeks. The dosage is slowly titrated up by 5 mg/day every 3 to 7 days until clinical benefit is obtained or a dosage of 1 mg/kg is reached. Improvement often begins in 1 or 2 months, with maximal improvement occurring at 6 to 12 months. After remission, patients can be switched to alternate-day steroids with the same total dosage and then slowly tapered. The chance of a successful taper is improved
Chapter 103
when the steroid dosage is tapered no faster than 5 mg/day/month. When the dosage reaches 40 to 50 mg every other day, tapering is best slowed to 2.5 mg/day/month. Often patients relapse several months after a successful taper and subsequent discontinuance. Many patients need a chronic low dose of steroids every other day to sustain a remission. The goal is to determine the lowest dosage of every-other-day therapy that will prevent a relapse. Unfortunately, when patients relapse, they often need a higher dosage of steroids, administered daily, to go back into remission, which must then be followed by another long, slow tapering process. Many patients, especially older adults, cannot tolerate the side effects of steroids (e.g., hypertension, weight gain, glucose intolerance, osteoporosis, cataracts, ulcers) and may need other types of immunosuppression. Azathioprine (AZA) has gained wide acceptance in myasthenia treatment and in many patients is the drug of choice. The concomitant use of AZA therapy commonly allows steroids to be tapered or discontinued. Clinical improvement is commonly delayed for 2 to 4 months but may not reach maximal benefit until after the first year or two. Patients typically are started on 50 mg daily as a single morning dose and slowly increased to 2 to 3 mglkglday over the next several weeks. Most patients tolerate M A without difficulty. However, adverse reactions may occur. The most common reactions are hematologic (anemia, leukopenia, thrombocytopenia), which necessitate close monitoring of blood counts during therapy (every 1 to 2 weeks initially). A typical hematologic endpoint is to let the white blood cell (WBC) count drop to 3500 to 4000/mm3 or the absolute lymphocyte count to drop to 5% to 10%. In addition, gastrointestinal disturbance, elevation of liver enzymes (two to 3 times normal), and susceptibility to serious infections may occur. Most of these complications can be dealt with by reducing the dosage (hematologic and liver enzyme abnormalities) or dividing the dosage with meals (gastrointestinal disturbance). Rarely, patients develop an acute, toxic hypersensitivity reaction to M A with fever, abdominal pain, and rash, which necessitates prompt and permanent discontinuance of the drug. Also of concern is the slightly increased risk of malignancy, especially lymphoma, which has been reported in nonmyasthenic patients treated with MA. Cyclosporin A (CSA), a drug that inhibits interleukin-2 and subsequently blocks cytotoxic lymphocytes and the proliferation of T-helper cells, is effective in preventing rejection in organ transplantation. This drug has also been found effective in several small studies of patients with MG. A typical induction dosage is 5 mg/kg, given as a divided dosage in the morning and evening. After remission, the dosage may be reduced gradually to a maintenance dosage of 2 to 3 mglkg. As with the other immunosuppressives, the goal is to determine the lowest dosage that prevents a clinical relapse. Trough CSA levels must be closely followed to maintain a level between 100 and 200 ng/mL. Blood pressure and renal function must be followed carefully. In regard to side effects, CSA is superior to other immunosuppressives in not suppressing the bone marrow. The major risks involve nephrotoxicity and hypertension. In addition, there are many potential drug interactions, most importantly the high likelihood of nephrotoxicity with the concurrent use of nonsteroidal antiinflammatory drugs. Prednisone, MA, and CSA are first-line therapies in MG treatment. The choice between the three is based primarily on the experience of the treating physician, with special emphasis on the side effect profile for the individual patient. Each of these agents has potential serious side effects. Obviously, they should never be used in any patient unless adequate compliance and follow-up are
Myasthenia Cravis
661
possible. The major errors in using these agents are in a dosage that is too low, a treatment duration that is too short, or nonaggressive treatment of side effects.
Plasma Exchange Removal of antibody allows clinical recovery in patients with MG. Often three to five large-volume plasma exchanges are needed to reduce the antibody level sufficiently. Plasma exchange is most appropriately performed when a patient has suddenly deteriorated and is in crisis or before major surgery such as thymectomy. It is in this situation, when rapid reversal of clinical weakness is necessary, that plasma exchange is most useful in minimizing further worsening or serious complications, such as intubation or pneumonia. However, as routine treatment for MG, plasma exchange is invasive and only temporary and is best reserved for the unusual patients who do not respond to other immunomodulating therapy.
IntravenousImmunoglobulin Intravenous immunoglobulin is used successfully in a variety of autoimmune diseases. Several reports have confirmed the efficacy of intravenous immunoglobulin in MG, including refractory patients for whom other traditional therapies have failed. Like plasma exchange, intravenous immunoglobulin is most useful when a patient with MG has suddenly deteriorated and rapid reversal of the weakness is important. It may also be useful in selected patients for whom plasma exchange is associated with side effects or difficulties with large volume intravenous access. As in other autoimmune conditions, patients initially are treated with dosages of 400 mg/kg/day for 5 days. Additional single doses are then given every 1 to 6 weeks, depending on the clinical response.
Thymectomy Most patients are successfully treated with the aforementioned approaches. The disease can be controlled in most patients, and it is now rare for patients to die of their illness. Myasthenia tends to be lifelong, and patients usually need prolonged therapy. Spontaneous remissions can occur, but relapses often occur again in the future. Immunosuppressives, especially prednisone, often are associated with potential long-term side effects. Although there has never been a prospective randomized trial, thymectomy is associated with a higher chance of complete remission or substantial improvement in MG patients. Patients with milder disease and relatively recent onset of symptoms (less than 3 years), without thymoma, are reported to respond best with thymectomy. Young patients with early myasthenia tend to do particularly well. Clinical improvement is commonly delayed 6 to 12 months after the operation and may continue for 5 years or more. In many centers, thymectomy often is not advised in patients older than 60 years because of other medical conditions that increase the risk of surgery (e.g., coronary artery disease) and the common observation that the thymus is atrophic in older adults. However, some studies have shown beneficial results in older adults. Therefore, each case must be individualized regarding the recommendation for surgery. The surgical technique (transcervical versus transsternal) has been debated by many clinicians. Most agree that, for thymectomy to be effective, the entire thymus gland must be removed, which usually necessitates a transsternal incision. In the modern era, the
662
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of NeuromuscularTransmission
morbidity and mortality associated with thymectomy have been reduced dramatically, making routine use of this therapy much more attractive. Unless the myasthenia is in complete pharmacologic remission before surgery, patients should routinely undergo several days of plasma exchange before thymectomy to reduce the likely worsening as a consequence of the stress of surgery and to promote early postoperative extubation. In addition, patients who relapse years after thymectomy or who never obtained a complete remission from their initial thymectomy may benefit from repeat thymectomy, even if imaging studies do not demonstrate residual thymus tissue. In one study, five of six patients with chronic refractory myasthenia improved with repeat thymectomy. Because 20% of normal subjects have some ectopic thymus tissue in the anterior mediastinum, some surgeons have advocated an extended cervicomediastinal thymectomy, removing all thymic, fat, and lymphatic tissue from the anterior mediastinum, superior mediastinum, diaphragm, and neck. In one of the largest surgical series of 202 patients with MG from Johns Hopkins University, extended cervicomediastinal thymectomy was associated with an odds ratio for improvement more than two times higher than that of the standard transsternal thymectomy. The other indication for thymectomy, of course, is the presence of a thymoma. The myasthenia of patients with thymoma tends to be more severe than that of other myasthenic patients, and a combination of surgery and aggressive medical therapy often is needed.
Restricted Ocular Myasthenia Patients with restricted ocular myasthenia represent a therapeutic challenge, responding to immunosuppressive therapy and thymectomy as well as patients with generalized MG. However, controversy remains regarding how aggressively to treat these patients. Patients with ocular myasthenia may be treated very differently in major centers. Some investigators argue that ocular myasthenia is not a serious illness, and the risks of immunosuppression or surgery cannot be justified. In these centers, patients with restricted ocular myasthenia are treated with acetylcholinesterase inhibitors and local ophthalmologic therapy, such as eyelid crutches or eye patches. On the other hand, many clinicians argue that when a patient first presents with myasthenia involving only the extraocular muscles, it is not possible to know whether the disease will progress to generalized myasthenia (indeed, most will) and that nearly all treatments are most effective if begun early in the illness. Many patients with restricted ocular myasthenia consider themselves nearly disabled from diplopia alone. These issues must be discussed with each patient before a path of aggressive or nonaggressive therapy is chosen.
However, 28% experienced exacerbations in the postpartum period. Because MG has no effect on smooth muscle, it does not interfere with uterine contractibility and has no effect on labor and delivery. However, during labor and delivery, magnesium as a treatment for toxemia is contraindicated because it can provoke a crisis. In a similar manner, if cesarean section is needed, spinal anesthesia is preferable to general anesthesia; curare and other neuromuscular junction blocking agents should not be used. In the pregnant patient with MG, treatment can be used as in nonpregnant MG patients, including acetylcholinesterase inhibitors, steroids, plasma exchange, and intravenous immunoglobulin. Immunosuppressive agents, including azathioprine and cyclosporine, are used with caution and best avoided if possible. Azathioprine crosses the placenta, with evidence of teratogenicity in animals. Based on reports of azathioprine and cyclosporine used in pregnancy in other conditions, the risk in humans appears low; however, the risk of using these drugs must be balanced in the individual patient, weighing the risk of relapse of a potentially life-threatening condition if a drug is withdrawn during pregnancy. Myasthenic Crisis Rarely, the initial presentation of MG may be a myasthenic crisis. Of course, crisis may also occur in patients with known myasthenia. Recognition and treatment of myasthenic crisis is one of the most important neuromuscular emergencies. In the 1960s, the mortality rate of myasthenic crisis was 50%. Now, with modern intensive care units, early diagnosis, and effective therapy, mortality from crisis is a rare event. Patients with moderate to severe MG may develop increasing bulbar and respiratory weakness. Often, this is the result of a concurrent infection or the addition of a new medicine. Several drugs are well known to exacerbate MG (Table 103-2). In response to worsening weakness, patients take more and more anticholinesterase medicines. Excessive anticholinesterase treatment can itself lead to increased weakness (cholinergic crisis). If the condition is not recognized early, the patient may succumb to primary respiratory collapse or aspirate from increasing bulbar weakness. Patients in crisis, whether cholinergic or myasthenic, must be treated aggressively. Any myasthenic patient who reports sudden worsening of symptoms must be evaluated immediately. Although the literature stresses the difference between myasthenic crisis and cholinergic crisis, it is often impossible to tell them apart. Miosis, fasciculations, diarrhea, sweating, abdominal cramping, excessive TABU105-2. Drugs Reported to Exacerbate Myasthenia Cravis
Myasthenia Cravis in Pregnancy Because MG often affects women of childbearing age, special issues are encountered with pregnant women with MG. The effect of pregnancy on MG is highly variable and unpredictable. There is no correlation between the underlying severity of the disease and the risk of exacerbation with pregnancy. However, times of greatest risk are the first trimester and postpartum periods. In patients in remission, the risk of an exacerbation during pregnancy is 17%. In patients with symptomatic MG, 39% improved, 42% had no change, and 6% deteriorated during pregnancy.
Arninoglycosides Clindarnycin Colistin Erythromycin Lithium Phenytoin Polymyxin B Procainamide Propranolol and other p-blockers Quinidine Quinine Tetracycline Veraoarnil and other Ca++ channel blockers
Chapter 104 1 Lambert-Eaton Myasthenic Syndrome
Tmu 103-3. Treatment of Myasthenic Crisis 1. Admit to intensive care unit. 2. Stop all anticholinesterases. 3. Rule out and treat concurrent infection. 4. Identify and correct any electrolyte abnormality. 5. Follow respiratory status closely and intubate if vital capacity is falling and reaches 15 m u k g (or higher if patient is at risk for aspiration). 6. Plasma exchange (5-6 timesA weeks).
salivation, and bradycardia all suggest cholinergic overdose. Many clinicians use a Tendon test to try to distinguish between the two. However, it is often difficult to assess improvement in a patient who is in severe distress. The treatment of myasthenic crisis is straightforward (Table 103-3). The major risk to life is respiratory failure. Patients should be watched carefully and intubated early to avoid later pulmonary complications. Anticholinesterases should be stopped. They can be restarted in a few days and probably can be used at lower dosages. Plasma exchange in myasthenic crisis is very useful in lowering antibody titers and rapidly reversing weakness. If a patient has not previously been on steroids or other immunosuppressants and no electrolyte imbalance or infection is discovered to explain the decompensation, then these probably will be needed to prevent further crisis. It is then reasonable to begin prednisone in the hospital while the patient is intubated and receiving plasma exchange.
SUGGESTED READINGS Achiron A, Bar& YH, Miron S et al: Immunoglobulin treatment in refractory myasthenia gravis. Muscle Nerve 23:551-555, 2000
663
Batocchi AP, Majolini L, Evoli A et al: Course and treatment of myasthenia gravis during pregnancy. Neurology 52(3):447452, 1999 Brooke MH: A clinician's view of neuromuscular diseases. Williams & Wilkins, Baltimore, 1986 Bulkley GB, Bass KN, Stephenson GR et al: Extended cervicomediastinal thymectomy in the integrated management of myasthenia gravis. Ann Surg 226:324-334, 1997 Drachman DB: Myasthenia gravis. N Engl J Med 390:1791-1810, 1994 Drachman DB: Present and future treatment of myasthenia gravis. N Engl J Med 316:743-745, 1987 Engel AG: Myasthenia gravis and myasthenic syndromes. Ann Neurol 16:519-534, 1984 Gronseth GS, Barohn RJ: Practice parameter: thymectomy for autoimmune gravis (an evidence-based review). Neurology 55:7-15, 2000 Hankins JR, Mayer RF, Satterfield JR et al: Thymectomy for myasthenia gravis: 14-year experience. Ann Surg 201:618-625, 1985 Howard J F Intravenous immunoglobulin for the treatment of acquired myasthenia gravis. Neurology 51:S30-S36, 1998 Lanska DJ: Indications for thymectomy in myasthenia gravis. Neurology 40:1828-1829, 1990 Miano MA, Bosley TM, HeimamPatterson TD et al: Factors influencing outcome of prednisone dose reduction in myasthenia gravis. Neurology 41~919-921,1991 Miller RG, Filler KA, Kiprov D, Roan R Repeat thymectomy in chronic refractory myasthenia gravis. Neurology 41:923-924, 1991 Palace J, Newsom-Davis J: A randomized double-blind study of prednis-
olone alone or with azathioprine in myasthenia gravis. Neurology 5 0 1778-1783, 1998 Papatestas AE, Genkins G, Kornfeld P et al: Effects of thymectomy in myasthenia gravis. Ann Surg 20679-88, 1987 Tindall RSA, Rollins JA, Phillips JT et al: Preliminary I'esults of a
double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravis. N Engl J Med 316719-724, 1987
104 Lambert-Eaton Myasthenic Syndrome H. Royden Jones, Jr. The Lambert-Eaton myasthenic syndrome (LEMS) is the most common neurologic paraneoplastic syndrome. Although very rare, LEMS is the prototype presynaptic neuromuscular transmission disorder in adults. Most patients with LEMS are symptomatic less than a year; however, diagnostic recognition rarely is delayed as much as 8 to 25 years after initial symptoms. Clinical manifestations of LEMS usually precede pulmonary or radiographic definition of small cell lung cancer (SCLC) by a number of months to years. In most instances when a cancer is not already identified at the time of the LEMS presentation, the likelihood of developing a SCLC or other malignancy becomes significantly less after 4 years. In that instance one then presumes that LEMS has a primary immunologic basis similar to myasthenia gravis. Commonly, LEMS is associated with cigarette addiction, especially among those who eventually develop SCLC. The incidence of LEMS in patients with SCLC is about 2% to 3%. This paraneoplastic disorder has an autoimmune basis. A significant association occurs in the paraneoplastic as well as the primary autoimmune variant, with the presence of HLA-B8 in both forms of LEMS, perhaps more so in patients without an associated
malignancy. LEMS also rarely occurs with other malignancies. These include other primary lung tumors such as atypical carcinoids or large cell neuroendocrine lung tumors. Additionally, and very rarely, certain lymphoproliferative disorders, as well as breast, colon, stomach, gallbladder, pancreas, prostate, bladder, and kidney cancers are associated with LEMS. However, a number of patients with LEMS (25% to 50%) never develop an underlying malignancy. Therefore, LEMS often has a nonparaneoplastic, primary, autoimmune pathophysiologic mechanism. There is a prominent association, perhaps 25%, between LEMS and other autoimmune processes. These include thyroiditis, pernicious anemia, vitiligo, Addison's disease, Sjogren's syndrome, type I diabetes mellitus, scleroderma, psoriasis, rheumatoid arthriTis, and celiac disease. LEMS occurs infrequently, perhaps at no more thanj5% the frequency of myasthenia gravis (MG), its autoimmune p+tsynaptic mirror image. This disorder most commonly presents ''after age 40. On the unusual occasion when LEMS presents in younger adults or, exceedingly rarely, even in children, it is almost always the primary nonparaneoplastic, autoimmune form of LEMS that
Chapter 104 1 Lambert-Eaton Myasthenic Syndrome
Tmu 103-3. Treatment of Myasthenic Crisis 1. Admit to intensive care unit. 2. Stop all anticholinesterases. 3. Rule out and treat concurrent infection. 4. Identify and correct any electrolyte abnormality. 5. Follow respiratory status closely and intubate if vital capacity is falling and reaches 15 m u k g (or higher if patient is at risk for aspiration). 6. Plasma exchange (5-6 timesA weeks).
salivation, and bradycardia all suggest cholinergic overdose. Many clinicians use a Tendon test to try to distinguish between the two. However, it is often difficult to assess improvement in a patient who is in severe distress. The treatment of myasthenic crisis is straightforward (Table 103-3). The major risk to life is respiratory failure. Patients should be watched carefully and intubated early to avoid later pulmonary complications. Anticholinesterases should be stopped. They can be restarted in a few days and probably can be used at lower dosages. Plasma exchange in myasthenic crisis is very useful in lowering antibody titers and rapidly reversing weakness. If a patient has not previously been on steroids or other immunosuppressants and no electrolyte imbalance or infection is discovered to explain the decompensation, then these probably will be needed to prevent further crisis. It is then reasonable to begin prednisone in the hospital while the patient is intubated and receiving plasma exchange.
SUGGESTED READINGS Achiron A, Bar& YH, Miron S et al: Immunoglobulin treatment in refractory myasthenia gravis. Muscle Nerve 23:551-555, 2000
663
Batocchi AP, Majolini L, Evoli A et al: Course and treatment of myasthenia gravis during pregnancy. Neurology 52(3):447452, 1999 Brooke MH: A clinician's view of neuromuscular diseases. Williams & Wilkins, Baltimore, 1986 Bulkley GB, Bass KN, Stephenson GR et al: Extended cervicomediastinal thymectomy in the integrated management of myasthenia gravis. Ann Surg 226:324-334, 1997 Drachman DB: Myasthenia gravis. N Engl J Med 390:1791-1810, 1994 Drachman DB: Present and future treatment of myasthenia gravis. N Engl J Med 316:743-745, 1987 Engel AG: Myasthenia gravis and myasthenic syndromes. Ann Neurol 16:519-534, 1984 Gronseth GS, Barohn RJ: Practice parameter: thymectomy for autoimmune gravis (an evidence-based review). Neurology 55:7-15, 2000 Hankins JR, Mayer RF, Satterfield JR et al: Thymectomy for myasthenia gravis: 14-year experience. Ann Surg 201:618-625, 1985 Howard J F Intravenous immunoglobulin for the treatment of acquired myasthenia gravis. Neurology 51:S30-S36, 1998 Lanska DJ: Indications for thymectomy in myasthenia gravis. Neurology 40:1828-1829, 1990 Miano MA, Bosley TM, HeimamPatterson TD et al: Factors influencing outcome of prednisone dose reduction in myasthenia gravis. Neurology 41~919-921,1991 Miller RG, Filler KA, Kiprov D, Roan R Repeat thymectomy in chronic refractory myasthenia gravis. Neurology 41:923-924, 1991 Palace J, Newsom-Davis J: A randomized double-blind study of prednis-
olone alone or with azathioprine in myasthenia gravis. Neurology 5 0 1778-1783, 1998 Papatestas AE, Genkins G, Kornfeld P et al: Effects of thymectomy in myasthenia gravis. Ann Surg 20679-88, 1987 Tindall RSA, Rollins JA, Phillips JT et al: Preliminary I'esults of a
double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravis. N Engl J Med 316719-724, 1987
104 Lambert-Eaton Myasthenic Syndrome H. Royden Jones, Jr. The Lambert-Eaton myasthenic syndrome (LEMS) is the most common neurologic paraneoplastic syndrome. Although very rare, LEMS is the prototype presynaptic neuromuscular transmission disorder in adults. Most patients with LEMS are symptomatic less than a year; however, diagnostic recognition rarely is delayed as much as 8 to 25 years after initial symptoms. Clinical manifestations of LEMS usually precede pulmonary or radiographic definition of small cell lung cancer (SCLC) by a number of months to years. In most instances when a cancer is not already identified at the time of the LEMS presentation, the likelihood of developing a SCLC or other malignancy becomes significantly less after 4 years. In that instance one then presumes that LEMS has a primary immunologic basis similar to myasthenia gravis. Commonly, LEMS is associated with cigarette addiction, especially among those who eventually develop SCLC. The incidence of LEMS in patients with SCLC is about 2% to 3%. This paraneoplastic disorder has an autoimmune basis. A significant association occurs in the paraneoplastic as well as the primary autoimmune variant, with the presence of HLA-B8 in both forms of LEMS, perhaps more so in patients without an associated
malignancy. LEMS also rarely occurs with other malignancies. These include other primary lung tumors such as atypical carcinoids or large cell neuroendocrine lung tumors. Additionally, and very rarely, certain lymphoproliferative disorders, as well as breast, colon, stomach, gallbladder, pancreas, prostate, bladder, and kidney cancers are associated with LEMS. However, a number of patients with LEMS (25% to 50%) never develop an underlying malignancy. Therefore, LEMS often has a nonparaneoplastic, primary, autoimmune pathophysiologic mechanism. There is a prominent association, perhaps 25%, between LEMS and other autoimmune processes. These include thyroiditis, pernicious anemia, vitiligo, Addison's disease, Sjogren's syndrome, type I diabetes mellitus, scleroderma, psoriasis, rheumatoid arthriTis, and celiac disease. LEMS occurs infrequently, perhaps at no more thanj5% the frequency of myasthenia gravis (MG), its autoimmune p+tsynaptic mirror image. This disorder most commonly presents ''after age 40. On the unusual occasion when LEMS presents in younger adults or, exceedingly rarely, even in children, it is almost always the primary nonparaneoplastic, autoimmune form of LEMS that
664
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Neuromuscular Transmission
is present. The youngest reported case initially had symptoms at age 1 year, but an appropriate diagnosis was not entertained until age 7. There is no particular sexual predominance, particularly with the almost equal percentage of women and men cigarette smokers. The neurophysiologic and immunologic characteristics of LEMS typify a presynaptic lesion of the neuromuscular junction. LEMS is indeed a mirror image of its much more common autoimmune cousin, the postsynaptic disorder MG. Repetitive motor nerve stimulation (RMNS) at 2 to 3 Hz may produce a decremental response in both LEMS and MG. The facilitation of the typical baseline low-amplitude compound muscle action potential (CMAP) to brief voluntary exercise is characteristic of LEMS and provides the basis for electromyographic diagnosis. Physiologic and immunologic investigations identified that the primary site of immunopathology involves the voltage-gated calcium channels (VGCC). An immunoglobulin G (IgG) antibody adheres to the peripheral cholinergic nerve terminals, blocking the calcium influx that normally occurs with nerve depolarization. This results in an inadequate release of acetylcholine quanta from motor and autonomic cholinergic nerve terminals. The VGCC present in the SCLC cells provides the presumed antigenic stimulus for antibody production in this paraneoplastic form of LEMS. The precise antigenic stimulus in the nonparaneoplastic varieties of LEMS remains to be identified. Presynaptic neurotransmitter release at the neuromuscular junction depends upon the presence of active P/Q type VGCCs through which calcium ions pass to facilitate the release of acetylcholine from the immediately available presynaptic quanta. This step is the essential process for acetylcholine to become available for postsynaptic binding at the neuromuscular junction. When autoantibodies adhere to the VGCC of the peripheral cholinergic nerve terminals, they block the calcium influx and eventually depolarization of the endplate. Muscular weakness is the primary clinical manifestation. The responsible IgG actually binds to the presynaptic neuromuscular junction. When an SCLC is present, one can find that this tumor expresses typical VGCC, providing the antigenic stimulus to produce VGCC antibodies. These antibodies have the ability to cross-react with various acetylcholine-releasing sites such as the neuromuscular junction, as well as various autonomic structures.
CLINICAL DIAGNOSIS A carefully derived history most often is the primary clinical clue leading to a LEMS diagnosis. Patients with LEMS characteristically present with a typical myopathic syndrome characterized by a predominantly proximal weakness. However, often the patient does not report other seemingly minor complaints, which are important clinical clues to the proper diagnosis. Such patients may believe that these seemingly minor concerns are not significant enough for her or him to mention to the physician. These characteristically include vague thigh numbness and stiffness or important symptoms and signs of dysautonomia, typically xerostomia and erectile dysfunction. On occasion, one may make a clinical diagnosis of LEMS very soon after meeting the patient. If the neurologist finds a patient who initially apologizes for sitting drinking a glass of water, primarily because of his or her very dry mouth, and who obviously has problems getting out of the chair to say “hello,” you may have all the clinical clues necessary to order the correct studies. This is especially true if the patient is a cigarette addict. This has
happened to me on a few occasions, especially with patients whose diagnosis had been “unclear” to prior examiners. The clinical presentation is similar whether LEMS is associated with the primary autoimmune form or the secondary paraneoplastic autoimmune type of disorder. However, the classic LEMS symptom constellation often is preempted by an interesting set of protean clinical manifestations. Twenty-three of 50 (46%) patients with LEMS seen at Queen Square (U.K.) and 18 of 23 (78%) seen at the Lahey Clinic had atypical symptoms including oculobulbar symptoms and signs that elsewhere led to a differential initial diagnosis. These were a chief complaint in 7 of 23 patients with LEMS. Diplopia occurred in 11, ptosis in 11, dysarthria in 10, and dysphagia in 8 patients. Therefore, early on, LEMS often mimics a number of more common neuromuscular disorders including MG, polymyositis, multiple sclerosis, occult malignancies, dysautonomias, or somatoform disorders, including hysteria. Occasionally, the clinical presentation of LEMS is preempted and therefore is confused by the earlier appearance of other SCLC-associated paraneoplastic disorders. These typically include a cerebellar ataxia or a primary sensory neuropathy. As with LEMS, each of these syndromes has a specific antibody identity; sometimes two and rarely all three clinical syndromes and their respective antibody markers are found in the same patient. LEMS muscle weakness classically mimics most myopathies with a proximal preponderance characterized by difficulties arising, walking, or climbing stairs. Although the proximal arm and neck muscles often are weak on examination, these are often not clinically significant to the patient and therefore are not initially reported to the physician. Fatigue is a prominent muscular symptom; it is often the initial LEMS manifestation. It is very important to note that in some patients, the initial neurologic examination is characterized by a seeming inconsistency or “give way” type of muscle weakness that may suggest that these patients do not have true weakness. In fact, 3 of the 22 patients with LEMS came to the Lahey Clinic with prior diagnoses of hysteria, malingering, or depression precisely because of a misinterpretation of their muscle testing results. These examination findings actually mirror the primary neuroimmunologic and corresponding neurophysiologic pathology. The facilitative component of their “give way” weakness represents the classic facilitative Ch&@ resnonse that typifies the electromyographic diagnostic LEMS facilitation findings with RMNS. When patients with suspected LEMS do not have detectable weakness, a subtle weakness may be better appreciated by watching the patient arise from a chair. On one occasion, clinically occult weakness in a patient of mine with a normal routine examination and a compelling history was precipitated by climbing stairs near my office. Bulbar symptoms often are thought to be less prominent than with MG. However, their presence far from excludes LEMS from diagnostic consideration. Eighteen of our 22 Lahey Clinic patients had some form of bulbar difficulty. This primarily included diplopia, ptosis, dysphagia, and dysarthria. A paradoxical lid elevation may occur with sustained upward gaze. This is secondary to LEMS facilitation, in contrast with MG, where this maneuver evokes increased ptosis. Muscle stiffness and tightness are also prominent LEMS symptoms in a few patients. Primary gait difficulty occasionally is the presenting symptom of LEMS. Unless this is a true gait ataxia secondary to concomitant paraneoplastic cerebellar degeneration or a primary sensory neuropathy, this pseudoataxia usually is secondary to subtle paraspinal and very proximal pelvic girdle weakness. In two of our patients, this clinical constellation previously led to an initial
Chapter 104
diagnosis of multiple sclerosis. Therefore, when one evaluates a patient with proximal limb weakness and a concomitant ataxia or neuropathy, this clinical setting is consistent with a LEMS diagnosis. Autonomic symptoms, including dryness of the mouth or erectile dysfunction in men, often give the astute clinician important clues that will lead to consideration of LEMS. However, the neurologist often needs to query the patient directly to gain this information. Other patients with LEMS sometimes report a feeling of vague numbness, especially prominent in the thighs. The combination of vague weakness, dry mouth, and paresthesias may mimic the common hyperventilation syndrome, a trap the unwary clinician must avoid. The muscle stretch reflexes typically are reported to be absent or depressed; however, these were normal in about 20% of our patients with LEMS. In the majority of the patients who have either sluggish muscle stretch reflexes or areflexia, we were able to demonstrate a characteristic postexercise facilitation. Similarly, this is also demonstrated with the muscle weakness. The second wind increase in strength is the clinical mirror image of the classic postexercise CMAP facilitation defined by electromyography (EMG). Occasionally sluggish pupillary light responses are found in patients with LEMS. This is another sign of autonomic dysfunction, also seen in botulism, another presynaptic neuromuscular transmission disorder. DIFFERENTIAL DIAGNOSIS Because the diagnosis of LEMS often is elusive during the initial stages of this disorder, especially with 18 of our 23 patients having a nonclassic clinical presentation, one must be always alert to this diagnostic possibility. The differential diagnosis includes a broad spectrum of neurologic disorders. Before our initial evaluation, the preceding diagnoses included MG in six patients, a myopathy in five, psychiatric issues in three, cerebellar degeneration or multiple sclerosis in two, a peripheral neuropathy in one, and orthostatic hypotension in another; one patient was presumed to have an occult malignancy, which proved to be true when the LEMS was diagnosed. The other four patients were diagnosed with LEMS subsequent to SCLC surgery. Two of these four developed postoperative respiratory depression, and in the remaining two patients typical LEMS symptoms developed a number of months to a year and a half after their surgery and during chemotherapy. One major clinical difference between MG and LEMS relates to the fact that in most instances MG has a preponderance of bulbar symptoms early in its course. The more generalized weakness, as well as the occasional respiratory compromise in MG, follows a period of predominant cranial nerve dysfunction. However, in our experience cranial nerve symptoms are quite common with LEMS. They are often mild, sometimes transient and usually are not the presenting symptom. Recently, however, we have had the opportunity to evaluate a patient with “antibody-negative myasthenia gravis” presenting with ptosis and diplopia. Much to our surprise, she indeed was antibody positive, but to only the VGCC antibody. Subsequently, she has developed increasing fatigue with some response to 3,4-diaminopyridine (3,4-DAP). Another difference between MG and LEMS is the prominence of autonomic symptoms found in LEMS. Uncommonly, LEMS and MG may occur in the same patient. This is confirmed by the concomitant presence of both VGCC and acetylcholine receptor antibodies in the same patient. Other rare presynaptic neuromuscular transmission disorders (e.g., botulism and magnesium intoxication)
Lambert-Eaton Myasthenic Syndrome
665
present acutely; in contrast, patients with LEMS rarely have a sudden clinical onset. Inflammatory myopathies, namely polymyositis (PM) and dermatomyositis (DM), typically have predominant proximal and neck weakness. This distribution is also common in LEMS. However, these patients with inflammatory myositis do not have subtle facilitation of strength immediately after the initial testing of each muscle. Usually the muscle stretch reflexes are preserved with both PM and DM. These patients also lack the typical autonomic and vague sensory symptoms classically seen with LEMS. Muscle tightness, stiffness, and pain are present in more than a third of our patients with LEMS. Therefore, metabolic myopathies such as McArdle’s disease rarely need to be considered, particularly in younger adults. In contrast, patients with LEMS do not have myoglobinuria. Both the inflammatory myopathies and some of the metabolic myopathies have elevated levels of serum creatine kinase (CK). This is also very uncommon with LEMS. If present, the CK elevation is very modest, in contrast to the usual marked elevation in DM and PM. Chronic inflammatory demyelinating polyneuropathy, with its insidious onset of proximal weakness and absent or reduced muscle stretch reflexes, also enters the LEMS differential diagnosis. No clinical evidence of facilitation of muscle strength or these reflexes is found in these patients. Distal paresthesias very occasionally may be the presenting symptom of LEMS. This is particular so when there is a conjoint autoimmune paraneoplastic sensory polyneuropathy. These patients have both positive VGCC antibodies associated with the anti-Hu antibodies that are the signature of a paraneoplastic sensory neuropathy. Multiple sclerosis also enters into the LEMS differentid diagnosis. Occasionally a patient with LEMS presenting with an ataxic gait initially is thought to have multiple sclerosis. At other times the clinician may note clues suggesting the presence of a paraneoplastic process, with one affecting primarily the cerebellum. Some patients with this clinical presentation have had repeatedly normal central nervous system imaging procedures. In some instances, it was not until proximal muscle weakness, per se became apparent, particularly affecting the paraspinal muscles and leading to an unstable gait, or concomitant signs of dysautonomia developed that a possible LEMS diagnosis was considered. The other possibility to consider in this setting, when differentiating the patient with multiple sclerosis or primary cerebellar degeneration, is a coexistent paraneoplastic autoimmune anticerebellar neuronal mechanism. LEMS also must be considered in any patient who is considered depressed, hysterical, or possibly malingering, especially those who present with vague weakness, paresthesias, or erectile dysfunction. At times, clinically defining the characteristic associated symptoms or observing for subtle signs of neurophysiologic facilitation with testing of proximal muscle strength or muscle stretch reflexes may provide important initial clues to a LEMS diagnosis. When these are present, the clinician can alert the electromyographer to test carefully for LEMS. DIAGNOSTIC STUDIES Tensilon Testing The clinical presentation of some patients with LEMS has many similarities to MG. Therefore, some patients with LEMS undergo Tensilon (edrophonium hydrochloride) testing. However, it is important to emphasize that a Tensilon test is actually a nonspecific evaluation of neuromuscular junction function. One
666
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Neurornuscular Transmission
study found that the Tendon test was “subjectivelyor objectively” positive in 14 of 21 patients with LEMS. Therefore, the response to this simple test cannot be used to differentiate MG from LEMS.
Electromyography Skillfully performed EMG still is the best clinically available, immediately useful study for diagnosing LEMS. Before performing the various RMNS studies, it is necessary to perform standard motor and sensory nerve conduction studies and needle EMG to exclude a number of other motor unit disorders. Typically, in LEMS, motor nerve stimulation demonstrates very markedly diminished CMAP amplitudes. These are often no more than 10% of normal size. One must be aware with early LEMS that the CMAPs may be normal, as noted in 2 of 50 patients in a major review of this subject by Newsom-Davis. In this instance, a repeat study 6 to 12 weeks later may demonstrate a drop in CMAP amplitude with a facilitation back to baseline after 10 seconds of voluntary exercise. Sensory nerve action potentials are normal except when there is a concomitant primary sensory neuropathy. In this instance, the sensory nerve action potentials are absent or of very low amplitude. The neurophysiologic diagnosis of LEMS depends primarily on the CMAP facilitation after a brief period of exercise. Usually at rest, most patients with LEMS demonstrating a significant neuromuscular transmission deficit with RMNS. This averaged a 27% decrement with 2 to 3 Hz stimulation. In contrast to MG, wherein documentation of a decrement may entail testing multiple
EXERCISE
3* Loter
nerves, particularly proximal or bulbar, the neuromuscular transmission disorders in patients with LEMS usually are present in all motor nerves tested. The crucial differentiation between a presynaptic and postsynaptic NMTD is the finding that brief voluntary exercise prompts a marked CMAP facilitation in patients with LEMS but not those with MG. High-frequency 20 to 50 Hz RMNS traditionally also results in a 100% or greater CMAP facilitation but this format is painful and sometimes prone to movement artifact. Therefore, testing for postexercise facilitation is preferred. To make an electromyographic diagnosis of LEMS, it is necessary to obtain postexercise facilitation greater than loo%, that is, at least twice the baseline. Usually patients with LEMS have 200% to 1000% CMAP facilitation (Fig. 104-1). It is very important for the electromyographer to have the patient exercise for only 10, absolutely no more than 15 seconds to achieve maximal postexercise facilitation to prevent its being masked by a longer period of exercise. A previous and improperly performed EMG contributed to the failure to detect a postexercise facilitation in three of our patients who were exercised too long (i.e., 30 to 60 seconds) at another EMG laboratory. The shorter period of exercise proved to be critical to our diagnosis of LEMS. Clinical examination and RMNS in 29 patients with SCLC and no symptoms of LEMS did not detect any subclinical cases. Conventional needle EMG in patients with LEMS demonstrates an increased number of low-amplitude, short-duration motor unit potentials, as seen with other myopathies. Their amplitude may enlarge with sustained contraction.
2 ’ Loter
10 ’ Later
“L 30
seconds
M. G.
10 seconds
Br. Ca.
10 seconds
A
Smv.
T
FIG. 104-1. Effects of exercise on the compound muscle action potential (CMAP) of the hypothenar muscles evoked by maximal stimulation of the ulnar nerve at the wrist. The response of the rested muscle as recorded on the left is compared with responses at 3 seconds, 2 minutes, and 10 minutes after the end of a maximal voluntary contraction of this muscle for 10 to 15 seconds. Each record consists of superimposed CMAPs evoked at a rate of 3 Hz. Br. Ca, patient with LEMS and small cell lung cancer; M.C., patient with generalized myasthenia gravis; N, normal patient. The important finding in LEMS is the low-amplitude CMAP and the marked facilitation after brief voluntary exercise with an associated neuromuscular transmission defect. (From Rooke ED, Eaton LM, Lambert EH, Hodgson CH: Myasthenia and malignant intrathoracic tumor. Med Clin North Am 44:972, 1960 with permission.)
Chapter 104 H Lambert-Eaton Myasthenic Syndrome
Antibody Studies VGCC antibody testing is the final determinant of the accuracy of LEMS. This laboratory modality provides the definitive means to confirm the clinical and electromyographic impression of LEMS in both the paraneoplastic and the primary autoimmune forms of this disorder These P/Q type antibodies were present in 92% of 72 clinically definite LEMS patients studied by the Oxford group of Newsom, Davis, Vincent et al. They also demonstrated the presence of these P/Q VGCC antibodies in 3 of 90 SCLC patients (3.3%) who had no neurologic symptoms. Thus, a positive VGCC antibody test per se does not diagnose LEMS. One absolutely needs the typical clinical and electromyographic findings to support this diagnosis.
Chest Radiographs, Computed Tomography, and Magnetk Resonance Imaging Interestingly, just 5 of our 23 patients with LEMS had abnormal chest radiographs before their LEMS diagnosis: four with SCLC and the other with a lymphoma. When the electromyographic findings were typical for LEMS, a subsequent chest radiograph demonstrated perihilar masses in two others who then had a positive SCLC biopsy. By contrast, in the other patients, the post EMG chest radiograph was either normal or nondiagnostic. A computed tomography (CT) scan of the lung is indicated whenever a diagnosis of LEMS is made and the initial chest radiograph is normal. This is a more sensitive modality. It immediately led to an SCLC diagnosis in four of our seven newly diagnosed patients with LEMS. However, when the CT scan is negative, pulmonary cytologic studies, including sputum analysis and bronchial washings, are occasionally of value for the diagnosis of occult lung tumors in some LEMS cases. Repeat chest CT scan and magnetic resonance imaging (MRI) in patients with LEMS without documented SCLC, particularly middle-aged smokers, must be performed intermittently-possibly every 3 to 6 months-for at least 4 years after the initial LEMS diagnosis.
THERAPY Two primary forms of therapeutic modalities are available for patients with LEMS. One group is used to provide symptomatic neuromuscular transmission improvement. In the other instance, a set of options is available primarily to modify the autoimmune process. Historically, guanidine was the first symptomatic therapy used effectively for patients with LEMS. This drug enhances acetylcholine release from motor nerve terminals. Unfortunately, it is generally contraindicated because of its inherent renal and hematologic toxicity. Today it is used only in the rare instances when all other therapies have failed and the patient is very symptomatic. Another drug, 3,4-diaminopyridine (3,4-DAP), also promotes acetylcholine release from the presynaptic portion of the neuromuscular junction. It prolongs the VGCC open time. Currently it is available for LEMS treatment primarily in Europe. After a recent very positive major two-arm parallel treatment study at Duke, the U.S. Food and Drug Administration still declined to grant approval for routine 3,4-DAP use. However, they now permit its use with local institutional review board approval and concomitant submission of a protocol to the Food and Drug Administration for compassionate use. This medication provided significant clinical and neurophysiologic improvement in 25 of 26 patients
667
with LEMS. It is as effective in patients with SCLC as in those with idiopathic autoimmune LEMS. In a 2000 study by Sanders et al., patients received 20 mg three times daily. When starting a patient de novo, the initial dosage usually is 5 mg three times daily (15 mg/day). Gradually one may work up to a maximum of 80 mg/day. Neurologists who use 3,4-DAP are urged to be cautious with large dosages because central nervous system irritability, usually manifested by seizures, is a major side effect. The anticholinesterase medication pyridostigmine also improves neuromuscular transmission. In contrast to MG, pyridostigmine is not always as effective for LEMS. However, anticholinesterases potentiate the effects of 3,4-DAP. When 3,4-DAP becomes more widely available, it has the potential if combined with pyridostigmine to be the first line of LEMS therapy. There is an important caveat in that pyridostigmine and 3,4-DAP provide only symptomatic therapy and do not address the autoimmune mechanisms responsible for both paraneoplastic and primary autoimmune LEMS. Of the various forms of chronic immunomodulation, prednisone is often the traditional drug of choice. However, in patients with SCLC or those at high risk for SCLC in whom a tumor has yet to be identified, initiation of immunosuppressive therapy theoretically may lessen the body’s immune response to the patient’s tumor. No data are available to confirm that hypothesis. I initiate an immunosuppressive medication only after a patient’s symptoms are disabling and she or he cannot effectivelybe returned to performing activities of daily living. In general, a dosage of 40 to 100 mg/day is given until improvement begins, which may take a few months. Next, one changes to an alternate-day dosage schedule, decreasing the low-day dosage by 10 to 20 mg every 10 to 15 days until a schedule of alternating 40 and 10 to 80 and 20 mg/day is achieved. Then the high-day dosage is gradually decreased to a maintenance level of alternating 10 and 0 to 30 and 15 mglday. Other clinicians suggest starting with the alternateday schedule of prednisone at a dosage of 1.0 to 1.5 mg/kg every other day. Azathioprine, starting with 50 mg daily and gradually increasing to 2.0 to 2.5 mg/kg daily, often combined with prednisone, may enhance the effectiveness of the treatment. However, azathioprine has a delayed onset of clinical effectiveness. Therefore it is not a good initial therapeutic modality. Intravenous immunoglobulin therapy for LEMS, with or without SCLC, may produce significant improvement with 1 g/kg on two consecutive days. Patients often note a return of strength beginning 2 to 3 days after infusion; the improvement may peak at 2 to 3 weeks and persist for a total of 4 to 6 weeks. Relapses may be controlled by repeat courses. This may become the primary LEMS immunotherapy, however a greater experience is needed to best assess MO’s therapeutic potential and relative risk benefit. Finally, plasmapheresis is another form of immunotherapy that is useful for patients with LEMS and significant weakness. This course of treatment may have a peak effect lasting just 2 weeks. When this temporary improvement is lost, another series of treatments may be needed within 6 weeks of the initial therapy. Its effectiveness often is less than when used for myasthenia gravis. Chemotherapy has been the primary treatment modality in seven of our patients with SCLC. In all seven instances, the tumor was not identified until after the LEMS diagnosis. One patient also had a pneumonectomy. The chemotherapy was very effective,with resolution of both clinical and neurophysiologic evidence of the LEMS and no sign of the lung tumor for 6 years. He then developed SCLC in the opposite lung and died a few months later.
668
Spinal Cord and peripheral Neuromuxular Disease
Diseases of NeuromuscularTransmission
Another patient’s illness was stable for 1 year. One patient treated primarily with chemotherapy died within just a few months, and the other three patients with SCLC and LEMS who were similarly treated were lost to follow-up. Finally, a middle-aged man with LEMS was initially treated with prednisone. Chemotherapy was added when chest CT finally became positive 1 year after diagnosis. He died 6 months later. With the recent access to 3,4-DAP, we have treated two patients with a combination of this and chemotherapy. A larger study will be necessary to assess the value of this combined therapy.
Medications Contraindicated in Patients with LEMS Certain common medications may exacerbate LEMS symptoms. Cardiac drugs, including P-adrenergic and calcium channel blocking agents along with antiarrhythmic agents such as procainamide and quinidine also must be used cautiously in LEMS. The aminoglycoside antibiotics, quinine, and magnesium citrate cathartics may also potentiate the LEMS neuromuscular transmission defect by increasing weakness. Lithium, a cation, caused a significant exacerbation in one of our patients who was previously given a diagnosis of depression as a n explanation of her classic LEMS symptoms. Anesthesiologists need to be aware of a LEMS diagnosis because it is important that they select medications that will not prolong postoperative respiratory depression. O n rare occasions, this may be the initial manifestation of LEMS.
PROGNOSIS AND FOLLOW-UP In J. H. ONeill and colleagues’ seminal study, 18 of 23 patients with LEMS and SCLC died within 32 months of tumor diagnosis. They had a median survival of 8.5 months. There were 5 survivors; 3 had remission of LEMS with no detectable tumor from 2.9 to 4.2 years. In contrast, the prognosis in patients with primary autoimmune LEMS without SCLC was excellent in 21 patients, with a median follow-up of 6.9 years.
CONCLUSION The clinical manifestations of LEMS mimic a number of neurologic syndromes. These include MG, polymyositis, multiple sclerosis, and somatoform disorders. Evidence of muscle weakness may not always be present early on; one has to take care to not attribute reports of recent-onset fatigue or muscle tightness to psychological mechanisms such as depression or hysteria. Bulbar symptoms suggesting MG or brainstem stroke may also be present. Some patients with LEMS have a positive Tensilon test, but the acetylcholine receptor antibodies usually are negative. Other patients with LEMS have concurrent paraneoplastic syndromes, particularly cerebellar ataxia or a primary sensory polyneuropathy. A complete EMG, including a search for a neuromuscular transmission disorder and, most importantly, postexercise facilitation within 10 to 15 seconds of maximal voluntary exercise, is essential for the appropriate clinical diagnosis. The finding of positive VGCC in the clinical setting of LEMS confirms the diagnosis. The treatment of choice is 3,4-DAP, if available; however, at times prednisone, intravenous immunoglobulin, and rarely plasmapheresis may also be helpful. An SCLC is found in 50% of patients with LEMS; these patients generally have a poor prognosis, in contrast to those with the more benign idiopathic primary autoimmune form.
SUGGESTED READINGS Bird SJ: Clinical and electrophysiologic improvement in Lambert-Eaton syndrome with intravenous immunoglobulin therapy. Neurology 42:1422-1423, 1992 Blumenfeld AM, Recht LD, Chad DA et al: Coexistence of Lambert-Eaton myasthenic syndrome and subacute cerebellar degeneration: differential: effects of treatment. Neurology 41:1682-1685, 1991 Breen LA, Gutmann L, Brick JF, Riggs J R Paradoxical lid elevation with sustained upgaze: a sign of Lambert-Eaton syndrome. Muscle Nerve 14863-866, 1991 Brown JC, Johns RJ: Diagnostic difficulty encountered in the myasthenic syndrome sometimes associated with carcinoma. J Neurol Neurosurg Psychiatry 37: 1214-1224, 1974 Dalakas MC: Intravenous immunoglobulin in the treatment of autoimmune neuromuscular diseases: present status and practical therapeutic guidelines. Muscle Nerve 22( 11):1479-1497, 1999 Gutmann L, Phillips LH, Gutmann L Trends in the association of Lambert-Eaton myasthenic syndrome with carcinoma. Neurology 42~848-850,1992 Howard JF, Sanders DB, Massey J M The electrodiagnosis of myasthenia gravis and the Lambert-Eaton syndrome. Neurol Clin North Am 12~305-330, 1994 Kleopa KA,Teener JW, Scherer S S et al: Chronic multiple paraneoplastic syndromes. Muscle Nerve 23: 1767-1772, 2000 Lambert EH, Eaton LM, Rooke ED: Defect of neuromuscular conduction associated with malignant neoplasms. Am J Physiol 187:612413, 1956 Lang B, Waterman S , Pinto A et al: The role of auto-antibodies in Lambert-Eaton myasthenic syndrome. Ann NY Acad Sci May 13; 841:596-605, 1998 Lennon VA, Kryzer TJ, Griesmann GE et al: Calcium-channel antibodies in the Lambert-Eaton syndrome and other paraneoplastic syndromes. N Engl J Med 332(22):1467-1474, 1995 Lundh H, Nilsson 0, Rosen I Current therapy of the Lambert-Eaton myasthenic syndrome. Prog Brain Res 84163-170, 1990 Lundh H, Nilsson 0, Rosen I, Johansson S: Practical aspects of 3,4-diaminopyridine treatment of Lambert-Eaton myasthenic syndrome. Acta Neurol Scand 88136-140, 1993 Maddison P, Lang B, Mills K, Newsom-Davis J Long term outcome in Lambert-Eaton myasthenic syndrome without lung cancer. J Neurol Neurosurg Psychiatry 70:212-217, 2001 McEvoy K: Diagnosis and treatment of Lambert-Eaton myasthenic syndrome. Neurol Clin North Am 12:387-399, 1994 Motomura M, Hamasaki S, Nakane S et al: Apheresis treatment in Lambert-Eaton myasthenic syndrome. Ther Apheresis 4:287-290,2000 Newsom-Davis J: Paraneoplastic neurological disorders. J R Coll Physicians Lond 33:225-227, 1999 Newsom-Davis J, Leys K, Vincent A et al: Immunological evidence for the co-existence of the Lambert-Eaton myasthenic syndrome and myasthenia gravis in two patients. J Neurol Neurosurg Psychiatry 54:452453, 1991 Oh SJ, Kim DS, Head TC, Claussen G C Low-dose guanidine and pyridostigmine: relatively safe and effective long-term symptomatic therapy in Lambert-Eaton myasthenic syndrome. Muscle Nerve 20(9):1146-1152, 1997 ONeil JH, Murray NMF, Newsom-Davis J: The Lambert Eaton myasthenic syndrome: a review of 50 cases. Brain 111:577-596, 1988 O’Suilleabhain P, Low PA, Lennon VA Autonomic dysfunction in the Lambert-Eaton myasthenic syndrome serologic and clinical correlates. Neurology 50538-93, 1998 Rooke ED, Eaton LM, Lambert EH, Hodgson CH: Myasthenia and malignant intrathoracic tumor. Med Clin North Am 44977-988, 1960 Sanders DB, Howard J F High dose intravenous immunoglobulin treatment in Larnbert-Eaton myasthenic syndrome. The New York Academy of Sciences. Myasthenia Gravis and Related Disorders: Experimental and Clinical Aspects; PIII-44. Washington, DC, April 12-15, 1992
Chapter 105
W
Sanders DB, Massey JM, Sanders LL, Edwards LJ: A randomized trial of 3,4-diaminopyridinein Lambert-Eaton myasthenic syndrome.Neurology 54603407,2000 Streib E Adverse effects of magnesium salt cathartics in a patient with the myasthenic syndrome (Lambert-Eaton syndrome).Ann Neurol2: 175176, 1977 Tim RW, Massey JM, Sanders D B Lambert-Eaton myasthenic syndrome (LEMS). Clinical and electrodiagnostic features and response
Toxic and Metabolic Disorders of the Neuromuscular Junction
669
to therapy in 59 patients. Ann N Y Acad Sci 13(841):823-826, 1998 Ueno S, Hara Y: Lambert-Eaton myasthenic syndrome without calcium channel antibody: adverse effect of calcium antagonist diltiazem. J Neurol Neurosurg Psychiatry 55:409410, 1992 Voltz R, Carpentier AF, Rosenfeld MR et al: P/Q-type voltage-gated calcium channel antibodies in paraneoplastic disorders of the central nervous system. Muscle Nerve 22:119-122, 1999
105 Toxic and Metabolic Disorders of the
Neuromuscular Junction rn
Jackson Pickett There are many toxic and metabolic disorders of neuromuscular transmission. This chapter focuses on some of the more common disorders seen in the United States.
Proximal limb muscles Distal limb muscles Diaphragm
BOTULISM
Local toxin production in the gut may explain why constipation often is the first symptom. Cranial muscle weakness leads to difficulties with feeding and breathing. Breathing difficulties are
There are five types of botulism (Table 105-1); all are rare. AU forms of botulism have similar signs and symptoms but vary in the source of the toxin. The toxin acts by binding to autonomic and motor nerve terminals. After being taken up by nerve terminals, the toxin reduces the number of quanta of acetylcholine released by a nerve stimulus. Recovery from the toxin involves sprouting of nerve terminals, which form new synapses. This process can take months.
Infant Botulism Clinical Features. The most common form of botulism is infant botulism. More than 90% of affected infants are less than 6 months of age; the remaining 10% are under 1 year of age. The sexes are equally affected. The spectrum of infant botulism (Table 105-2) varies from sudden infant death syndrome to an otherwise healthy infant who has a change in stool character. Most of the reported cases have been severe enough to necessitate hospital admission. Epidemiologic studies have identified many factors in the development of infant botulism (Table 105-3). It is assumed that infants consume spores that germinate in the gut, forming organisms that produce toxin. In most cases the source of the spores is not found. The signs and symptoms of infant botulism severe enough to necessitate hospitalization are shown in Table 105-4. Initial symptoms include constipation, poor feeding, weak cry, and a loss of head control. These symptoms last from 5 hours to 1 week before admission. When fully developed, the disorder causes weakness of cranial and limb muscles and abnormalities of the autonomic, mainly parasympathetic, nervous system. Symptoms and signs usually peak in 1 to 2 weeks. Recovery starts after 3 to 5 weeks and often takes 1 to 4 months. The sequence of muscular involvement in infant botulism is as follows:
Autonomic nervous system Cranial muscles
W TABU 105-1. Median Number of Cases of Botulism
Reported in the United States Each Year
No. of Casesflear
TVpe
Infant botulism 71 Foodborne botulism 24 Adult infectious botulism 2 Wound botulism 3 Inadvertent caused by toxin treatment Not known Data from Shapiro RL Hatheway C, Swerdlow DL: Botulism in the United States: a clinical and epidemiologic review. Ann Intern Med 129:221, 1998.
W TABLE 105-2. Spectrum of Infant Botulism
Asymptomatic carriers of organism in stool Mild cases Constipation Feeding difficulties Mild weakness Failure to thrive Moderate to severe cases Hospitalized patients Sudden infant death syndrome
W TABLE 105-3. Possible Factors in the Development of Infant
Botulism Source of spores Geographic location: 50% of the US. cases found in California, Pennsylvania, and Utah Nature of soil Parents who work in soil Honey or corn syrup consumption Susceptibility of host Age: 1 week to 1 year Infants 2 months of age: less than one bowel movement per day for 2 months, breastfeeding,and ingestion of corn syrup Switch from milk to solid foods
Chapter 105
W
Sanders DB, Massey JM, Sanders LL, Edwards LJ: A randomized trial of 3,4-diaminopyridinein Lambert-Eaton myasthenic syndrome.Neurology 54603407,2000 Streib E Adverse effects of magnesium salt cathartics in a patient with the myasthenic syndrome (Lambert-Eaton syndrome).Ann Neurol2: 175176, 1977 Tim RW, Massey JM, Sanders D B Lambert-Eaton myasthenic syndrome (LEMS). Clinical and electrodiagnostic features and response
Toxic and Metabolic Disorders of the Neuromuscular Junction
669
to therapy in 59 patients. Ann N Y Acad Sci 13(841):823-826, 1998 Ueno S, Hara Y: Lambert-Eaton myasthenic syndrome without calcium channel antibody: adverse effect of calcium antagonist diltiazem. J Neurol Neurosurg Psychiatry 55:409410, 1992 Voltz R, Carpentier AF, Rosenfeld MR et al: P/Q-type voltage-gated calcium channel antibodies in paraneoplastic disorders of the central nervous system. Muscle Nerve 22:119-122, 1999
105 Toxic and Metabolic Disorders of the
Neuromuscular Junction rn
Jackson Pickett There are many toxic and metabolic disorders of neuromuscular transmission. This chapter focuses on some of the more common disorders seen in the United States.
Proximal limb muscles Distal limb muscles Diaphragm
BOTULISM
Local toxin production in the gut may explain why constipation often is the first symptom. Cranial muscle weakness leads to difficulties with feeding and breathing. Breathing difficulties are
There are five types of botulism (Table 105-1); all are rare. AU forms of botulism have similar signs and symptoms but vary in the source of the toxin. The toxin acts by binding to autonomic and motor nerve terminals. After being taken up by nerve terminals, the toxin reduces the number of quanta of acetylcholine released by a nerve stimulus. Recovery from the toxin involves sprouting of nerve terminals, which form new synapses. This process can take months.
Infant Botulism Clinical Features. The most common form of botulism is infant botulism. More than 90% of affected infants are less than 6 months of age; the remaining 10% are under 1 year of age. The sexes are equally affected. The spectrum of infant botulism (Table 105-2) varies from sudden infant death syndrome to an otherwise healthy infant who has a change in stool character. Most of the reported cases have been severe enough to necessitate hospital admission. Epidemiologic studies have identified many factors in the development of infant botulism (Table 105-3). It is assumed that infants consume spores that germinate in the gut, forming organisms that produce toxin. In most cases the source of the spores is not found. The signs and symptoms of infant botulism severe enough to necessitate hospitalization are shown in Table 105-4. Initial symptoms include constipation, poor feeding, weak cry, and a loss of head control. These symptoms last from 5 hours to 1 week before admission. When fully developed, the disorder causes weakness of cranial and limb muscles and abnormalities of the autonomic, mainly parasympathetic, nervous system. Symptoms and signs usually peak in 1 to 2 weeks. Recovery starts after 3 to 5 weeks and often takes 1 to 4 months. The sequence of muscular involvement in infant botulism is as follows:
Autonomic nervous system Cranial muscles
W TABU 105-1. Median Number of Cases of Botulism
Reported in the United States Each Year
No. of Casesflear
TVpe
Infant botulism 71 Foodborne botulism 24 Adult infectious botulism 2 Wound botulism 3 Inadvertent caused by toxin treatment Not known Data from Shapiro RL Hatheway C, Swerdlow DL: Botulism in the United States: a clinical and epidemiologic review. Ann Intern Med 129:221, 1998.
W TABLE 105-2. Spectrum of Infant Botulism
Asymptomatic carriers of organism in stool Mild cases Constipation Feeding difficulties Mild weakness Failure to thrive Moderate to severe cases Hospitalized patients Sudden infant death syndrome
W TABLE 105-3. Possible Factors in the Development of Infant
Botulism Source of spores Geographic location: 50% of the US. cases found in California, Pennsylvania, and Utah Nature of soil Parents who work in soil Honey or corn syrup consumption Susceptibility of host Age: 1 week to 1 year Infants 2 months of age: less than one bowel movement per day for 2 months, breastfeeding,and ingestion of corn syrup Switch from milk to solid foods
610
Spinal Cord and Peripheral NeuromuscularDisease
Diselases of Neuromuscular Transmission
TABU 105-4. Signs and Symptoms of Infant Botulism Site
Sign or Symptom
Autonomic nervous system
Constipation Sluggish pupils Flushed appearance Decreased tearing or salivation Bradycardia or tachycardia Hypotension or hypertension Urinary retention Poor feeding Reduced gag or suck reflex Facial weakness or ptosis Assisted ventilation Poor cry Weakness Reduced stretch reflexes Decreased activity
Cranial nerves
Somatic nerves
TABU 105-5. Differential Diagnosis of Infant Botulism infections Sepsis Meningitis Encephalitis Metabolic Abnormalities of cations and glucose Disorders of amino acid metabolism Hypothyroidism Metabolic encephalopathy Reye's syndrome Subacute necrotizingencephalomyelitis (Leigh's disease) Toxins Alcohols Anticholinergics Heavy metals Narcotics Organophosphates Neuromuscular Congenital myasthenia gravis Congenital myopathy Diphtheritic neuropathy Cuillain-Barre syndrome Infantile spinal muscular atrophy (Werdnig-Hoffman disease) Muscular dystrophy Poliomyelitis Tick paralysis
first caused by weakness of the bulbar muscles, leading to airway obstruction, and later by weakness of the respiratory muscles. Proximal limb and neck muscles often are weaker than distal muscles; the diaphragm is involved late in the course of the disease. A symmetrical descending paralysis is typical. Diagnosis. The combination of an infant who develops constipation, then feeding and respiratory difficulties, and later weakness of the neck and limbs, should suggest the diagnosis of infant botulism. Disorders to consider in the differential diagnosis are listed in Table 105-5. This differential can be reduced by screening for treatable infectious, metabolic, and toxic disorders; performing an electromyogram (EMG) and nerve conduction studies; searching for a tick; and sending blood and stool to be analyzed for botulinal toxin and organism. The usual results of the EMG and nerve conduction studies are shown in Table 105-6. The nerve conduction studies typically reveal small compound muscle action potentials (CMAPs). A decrement in the CMAP with slow repetitive nerve stimulation (i.e., 2 to 3 Hz) often occurs, implying a neuromuscular junction disorder. However, an increment in CMAP amplitude with rapid repetitive stimulation (i.e., 30 to 50 Hz) is characteristic and highly suggestive of a presynaptic
neuromuscular junction, such as botulism, where the number of quanta released by a nerve stimulus is markedly reduced. An increment lasting many minutes may be seen. Small and short motor unit potentials may be seen on needle EMG, localizing the disorder to the distal nerve terminals, neuromuscular junctions, or muscle fibers. In selected cases, single-fiber electromyography (SF-EMG) can be used to diagnose neuromuscular junction disorders, including botulism. SF-EMG measures the variability (i.e., jitter) in the onset of one muscle fiber action potential compared to another muscle fiber action potential of the same motor unit. In neuromuscular junction disorders, jitter increases. Conventional SF-EMG relies on cooperation of the patient in voluntarily maintaining contraction of the muscle being studied; such is not feasible when studying infants. In these cases, stimulated SF-EMG may be used to measure jitter. Stimulated SF-EMG also shows increased jitter. However, in presynaptic disorders, such as botulism, increased jitter improves as the frequency of stimulation increases, comparable to the increment in the CMAP seen with rapid repetitive stimulation. The diagnosis of infant botulism depends on the demonstration of the organism or toxin in the stool and the absence of toxin in any food. Toxin can be found in the serum in up to 12% of cases. In the United States, the type A toxin is most common in the West and type B in the East. Two types of toxin may be present in rare cases. The organism usually is Clostridium botulinum, but Clostridium butyricum (type E toxin) and Clostridium baratii (type F toxin) have been reported. To identify the toxin, mice are injected with serum or a stool extract, with and without antitoxin, and observed for death caused by paralysis. Both toxin and organism can be excreted in the stool for months, even as the infant recovers. Infants can improve before the toxin in the stool peaks. Treatment. The treatment of infant botulism in the hospital often involves intubation and mechanical ventilation, tube feedings, and Credk's maneuver to empty the bladder (Table 105-7). The hospital course varies from a few days to 6 months; about 5% of infants relapse. It is important to anticipate respiratory problems. A respiratory arrest occurs in about 30% of infants. All infants with difficulty coughing, gagging, or swallowing should be observed for apnea. Antitoxin has not been used because no toxin is detected in the serum in about 90% of cases, and serious allergic reactions have occurred when horse serum antitoxin has been given. The use of a human-derived antitoxin may soon clarify whether antitoxin is effective. For information on obtaining human botulinum immune globulin, contact the California Department of Health Services at 510-540-2646. If antibiotics are
rn TABLE105-6. Electrodiagnostic Studies in Infant Botulism studv
Result ~
Conduction studies Motor conduction velocities and latencies Normal Compound muscle action potential amplitude Low Sensory conduction studies Normal Rapid repetitive stimulation (>lo Hz) Increment 92% Decrement 47% Electromyography Positive sharp wave and fibrillation potentials 541 92% Small and short motor unit ootentials ._ . Data from Cornblath DR, Sladky JT,Surnner Al: Clinical electrophpiology of infantile botulism Muscle Nerve 6:448, 1983
Chapter 105 rn Toxic and Metabolic Disorders of the Neurornuscular Junction
TMU 105-7. Treatment of Infant Botulism Support respiratory system Monitor for apnea Prevent airway obstruction May need respirator for months Maintain nutrition May need tube feeding if unable to cough, gag, suck, or swallow Feed upright Urinary retention Crede's maneuver Treat urinary infections Of uncertain value Antibiotics Drugs to increase strength Human-derived antitoxin Laxatives and enemas
T m 105-8. Complications Seen in Infant Botulism Treatment All patients Apnea Autonomic instability C. difficile-associated diarrhea Pneumonia Sepsis Urinary tract infection lntubated patients Plugged endotracheal tube Postextubation stridor Recurrent atelectasis Subglottic stenosis Syndrome of inappropriate secretion of antidiuretic hormone Tracheal granuloma Tracheitis Tracheomalacia Unintended extubation
needed, drugs that inhibit neuromuscular transmission, such as aminoglycosides, should be avoided. With a mean hospital stay of 1 month and 80% of hospitalized infants on a respirator, treatment complications are expected (Table 105-8).Most involve the respiratory system or are caused by infections. Despite these problems in management and the presence of severe paralysis, only 2% to 3% of infants die, and the rest recover completely.
Foodborne Botulism Clinical Features. Foodborne botulism differs from infant botulism in that a source of toxin is present, and more than one half of the cases occur in outbreaks. Type A toxin is the most common (Table 105-9), and western states report more cases of botulism. The usual source of types A and B toxin is home-canned food, baked potatoes in aluminum foil, garlic in oil, sauteed onions kept under butter sauce, and cheese sauce; marine life is the typical source of type E toxin. Most patients with botulism are older than 10 years, and the median age is 30 to 40 years. The toxin does not cross the placenta, so the fetus of a mother with botulism is not at risk. The sexes are equally involved. The incubation period can vary from 2 hours to 8 days but usually is 12 to 36 hours. Typical initial signs and symptoms are blurred vision, diplopia, ptosis, dysarthria, dysphagia, and generalized weakness (Table 105-10).As with infant botulism, paralysis in foodborne botulism descends and usually is symmetrical, although 20% of the cases can be asymmetrical. Proximal muscles are weaker than distal, and
671
arms are more involved than legs. Autonomic involvement includes blurred vision, orthostatic hypotension, urinary retention, constipation, dry mouth, and dilated, fixed pupils. In addition to weakness and autonomic dysfunction, there may be evidence of acute gastroenteritis with nausea, vomiting, abdominal pain, and diarrhea. The deficits peak in 4 to 5 days, and most improvement occurs in months, although 2 years later some patients still report dyspnea, fatigue, dry mouth, constipation, or impotence. Diagnosis. A symmetrical descending paralysis with a mixture of autonomic, especially parasympathetic, dysfunction should suggest the diagnosis of botulism. The diagnosis is supported by other cases with a common food source for the toxin. The diagnosis of botulism is confirmed by detecting the toxin in serum or stool, or the organism in the stool, or by demonstrating the toxin in the suspected food. Because the mouse assay is slow, electromyography may give more rapid support for the diagnosis. The changes in foodborne botulism are similar to those in infant botulism (Table 105-11). Milder cases may show a greater increment, and findings may vary with the limb studied. The differential diagnosis of foodborne botulism includes Guillain-Barrk syndrome Tick paralysis Shellfish poisoning Myasthenia gravis Lambert-Eaton syndrome Guillain-Barrk syndrome is an ascending, mainly motor polyneuropathy. It can be distinguished from botulism by the presence of sensory abnormalities, ascending weakness, and a high cerebro-
TABU105-9. Types of Distribution of Foodborne Botulism Toxin Tvpe
Percentage of Cases
A
50% 25% 25%
B C
GeographicSites
West of Mississippi East of Mississippi Alaska and Great Lakes
~~
Data from Shapiro RL, Hatheway C, Swerdlow DL: Botulism in the United States: a clinical and epidemiologic review. Ann intern Med 129:221, 1998.
TMU 105-10. Signs and Symptoms of Foodborne Botulism Symptoms Abdominal cramps or pain Blurred vision Constipation Diarrhea Diplopia Dizziness Dysphagia Dysphonia Nausea or vomiting Photophobia Sore throat Urinary retention or incontinence Weakness Signs Abnormal eye movement Ataxia Dilated and fixed pupils Dry mouth Nystagmus Postural hypotension Weakness
672
Spinal Cord and peripheral Neuromuscular Disease W
Diseases of Neuromuscular Transmission
The differential diagnosis of wound botulism includes
rn TMLE 105-11. Electrodiagnostic Studies in Foodborne Botulism study
Result
Conduction studies Motor conduction velocities and latencies Normal Compound muscle action potential amplitude Low in 85% Sensory conduction studies Normal Repetitive stimulation 62% Increment with rapid stimulation Decrement with slow stimulation 8% Electromyography Small and short motor unit potentials increased jitter and blocking with single-fiber electromyography Data from Cherington M: Clinical spectrum of botulism: a review. Muscle Nerve 21 : 701,1998.
spinal fluid protein. A search for a tick is reasonable. Shellfish poisoning develops over minutes, and usually sensory symptoms and signs are present. Myasthenia gravis and Lambert-Eaton syndrome usually develop more slowly than botulism. Treatment. The key to successful treatment of a patient with severe botulism is respiratory support. Respiratory failure may develop insidiously. Patients with a vital capacity of less than 30% of predicted value usually need to be intubated. Antitoxin is often given, but its efficacy is uncertain, and allergic reactions to horse serum can occur in 10% of patients. A human-derived antiserum should produce fewer allergic reactions. If gastrointestinal function permits, toxin can be removed with ipecac, gastric lavage, or enemas. Guanidine and 4-aminopyridine can improve strength in some patients but do not reverse respiratory paralysis. With current management, only about 5% to 10% of patients die, although infectious complications are common. Wound Botulism Clinical Features. Wound botulism favors young men in-
volved in outdoor activities during the spring, summer, and fall. Usually the wound is obvious, with a compound fracture or crush injury. In recent years, wound botulism has increased and now is associated with drug injections, often resulting in skin abscesses, and intranasal cocaine administration, causing sinusitis. The symptoms and signs of wound botulism are similar to those of foodborne botulism, although the onset is slower with a median incubation period of a week. Patients with wound botulism lack the nausea, vomiting, and diarrhea often seen with foodborne botulism but may have fever and sensory abnormalities caused by the wound or its infection. About two thirds of patients with wound botulism need a respirator, and 10% to 15% die. Diagnosis. The combination of a wound and a descending paralysis should suggest the diagnosis of wound botulism. Circulating toxin in the serum is found in only about 46% of patients, and the organism can be grown from the wound in 50% to 60% of cases. About three fourths of the cases in which the toxin type is identified are caused by type A, with the remainder caused by type B. The most sensitive test for wound botulism is repetitive nerve stimulation. An increment with rapid repetitive stimulation usually is present and localizes the disorder to the presynaptic neuromuscular junction. In the future, enzyme-linked immunosorbent assays and polymerase chain reactions may aid in the diagnosis.
Tetanus Rabies Myonecrosis Acute cranial polyneuritis Tetanus differs from wound botulism by the presence of trismus and spasms of facial and somatic muscles. Rabies has a much longer incubation period, 30 to 70 days after an animal bite, extreme excitability, hydrophobia, and a cerebrospinal fluid pleocytosis. Myonecrosis spares the cranial nerves. Acute cranial polyneuritis has less autonomic involvement, can have abnormal conduction studies or an elevated cerebrospinal fluid protein level, and lacks an increment with repetitive stimulation. Treatment. Treatment focuses on supportive measures and local wound care. About two thirds of wounds appear to be clean, although cultures often reveal the organism. Antibiotics and antitoxin often are used, but their efficacy is unknown. Adult Infectious Botulism Clinical Features. Occasional cases of botulism in patients over the age of 1 year occur in which no wound or food is the source of the toxin. These cases probably have the same mechanism as infant botulism, in which the organism produces toxin in the gut. Production of the toxin in the gut, or autointoxication, is favored by gastrointestinal disease or surgery, gastric achlorhydria, or antibiotic treatment. Autointoxication should be suspected when the patient has consumed food that contains C. botulinum but not its toxin and a long incubation period is present.
DRUGS Drugs can impair neuromuscular transmission by unmasking or worsening an existing neuromuscular junction disorder, causing a neuromuscular junction disorder in a previously normal patient, or inducing the immune system to cause a syndrome resembling myasthenia gravis. The following drugs can induce an immunemediated syndrome resembling myasthenia gravis: Chloroquine D-Penicillamine Pyrithioxin Tiopronin Trimethadione The resemblance to myasthenia gravis with some of these drugs is close and includes a decrement with slow repetitive stimulation, increased jitter with single-fiber electromyography, and antibodies to the acetylcholine receptor. Most drugs aggravate, produce, or unmask a neuromuscular junction disorder by their direct effect (Table 105-12). An accurate history of drugs taken by the patient is needed for diagnosing drug-induced neuromuscular junction disorders. Renal or liver failure often accentuates the effects of drugs. The diagnosis can be confirmed by withdrawing the drug and observing the return of the patient to his or her previous state. Recovery from neuromuscular junction blocking agents can be prolonged and take several months.
Chapter 105 H Toxic and Metabolic Disorders of the Neuromuscular Junction
rn TABLE105-12. Drugs That Can Impair Neuromuscular Transmission by Their Direct Effect Antibiotics Aminoglycosides Amikacin Dihydrostreptomycin Centamicin Kanamycin Neomycin Netilmicin Streptomycin Tobramycin Fluoroquinolones Ciprofloxacin Monobasic amino acids Clindamycin Lincomycin Penicillin Ampicillin Polypeptides Colistimethate Colistin Polymyxin B and E Sulfonamides Tetracyclines Oxytetracycline Rolitetracycline Anticonvulsants Barbiturates Mephenytoin Phenytoin Trimethadione Botulinum toxin Cardiovascular drugs P-Blockers Nadolol Oxprenolol Pindolol Practolol Propranolol Bretvlium
Calcium channel blockers Verapamil Lidocaine Procainamide Quinidine Trimethaphan Hormones Adrenocorticotropic hormone Corticosteroids Estrogen Progesterone Thyroid hormone Neuromuscular blocking drugs Ophthalmic drugs Betaxolol Echothiophate Timolol Psychotropic drugs Lithium Monamine oxidase inhibitors Phenelzine Phenothiazines Chlorpromazine Promazine Rheumatologic drugs Penicillamine Chloroquine Miscellaneous drugs Aprotinin Azathioprine Diuretics D,L-Carnitine Emetine Methoxyflurane Sodium lactate infusion Trihexyphenidyl Radiographic contrast agents
HYPERMACNESEMIA Hypermagnesemia usually occurs in patients with renal failure who are given antacids or laxatives containing magnesium or treated for eclampsia with magnesium. The signs and symptoms of hypermagnesemia are as follows: Amnesia Ataxia Cardiac arrest Cutaneous flushing Dry mouth Hypotension Loss of stretch reflexes Nausea and vomiting Nystagmus Pupillary dilation Respiratory arrest Slurred speech Urinary retention Weakness These findings should suggest the diagnosis, and magnesium levels will confirm this impression. Electrodiagnostic studies reveal small
673
CMAps, which increase in amplitude after brief exercise or rapid
repetitive stimulation. These abnormalities reflect a reduction in the release of acetylcholine at neuromuscular junctions. Hypermagnesemia treatment involves reduced magnesium intake, intravenous calcium, or hemodialysis, depending on the severity of the findings. Respiratory support may be needed.
ORGANOPHOSPHATE INTOXICATION Exposure to organophosphate compounds usually is accidental but can be caused by a suicide attempt or terrorist attack. They cause acute symptoms and signs (Table 105-13) by irreversibly inhibiting acetylcholinesterase. This leads to an accumulation of
TABLE 105-13. Acute Signs and Symptoms Seen with Organophosphate Compounds Muscarinic Abdominal pain Aching of eyes Airway obstruction Anorexia Blurred vision Bradycardia Bronchial contraction and secretion Conjunctival hyperemia Coughing Cyanosis Diarrhea Hypotension Involuntary defecation and micturition Lacrimation Laryngeal spasms Nasal hyperemia Nausea and vomiting Pulmonary edema Pupillary constriction Runny nose Salivation Sweating Urinary frequency Nicotinic (including autonomic ganglia) Areflexia Fasciculations Fatigability Hypertension Muscle cramps Ophthalmoparesis Pallor Respiratoryfailure Tachycardia Proximal > distal weakness Central nelvous system Anxiety Apathy Ataxia Cheyne-Stokes respiration Coma Confusion Decreased concentration and memory Depression Emotional lability Excessive dreaming Failure of central respiratory drive Insomnia Nightmares Restlessness Seizures Slurred speech Tension Tremor Withdrawal
674
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Neuromuscular Transmission
acetylcholine at peripheral muscarinic and nicotinic synapses and at central nervous system synapses. The acute cholinergic crisis consists of miosis, fasciculations of the eyelids, face, and calves, and excess secretion. Acute symptoms start in 5 minutes to 1 day and usually peak in 0.5 hour to 6 hours and last 1 to 5 days. Diagnosis is aided by a history of exposure, signs such as miosis and fasciculation, improvement with atropine and pralidoxime, and a reduction of cholinesterase activity in the serum or red blood cells. The cholinergic crisis can be followed by a myasthenialike state, which lasts for 2 to 7 days. Weeks after the exposure, a delayed neuropathy can develop. Laboratory tests may aid in the diagnosis. Serum and red blood cell cholinesterase activity is inhibited early and for prolonged periods after exposure. For this reason cholinesterase levels do not correlate with clinical severity. After a single stimulus to a motor nerve, the initial CMAP is followed by repetitive potentials. These repetitive potentials reflect an accumulation of acetylcholine at neuromuscular junctions, which depolarizes motor nerve terminals. Depolarized motor nerve terminals backfire and activate other muscle fibers via an axon reflex. Repetitive potentials not only are seen in organophosphate intoxication but also can occur in congenital myasthenic syndromes caused by a deficiency of acetylcholinesterase and prolonged open time of sodium channels and with other drugs that inhibit acetylcholinesterase reversibly. Repetitive potentials are the earliest and most common change seen with electrodiagnostic studies. Slow repetitive stimulation studies may reveal a decrement. The decrement is caused by a combination of collision of the orthodromic action potentials with the backfiring action potentials from earlier stimuli and desensitization of acetylcholine receptors caused by a buildup of acetylcholine. A decrement with repetitive stimulation predicts the need for respiratory support. The treatment of acute organophosphate intoxication involves supporting respiratory function, giving atropine and pralidoxime to reverse the inhibition of acetylcholinesterase, and terminating exposure. SNAKE BITES
A wide variety of snakes can inflict a bite that is potentially neurotoxic, including the following: Australian elapids Cobras Coral snakes Kraits Mambas North American rattlesnakes Old world vipers Sea snakes South American rattlesnakes Snake venom is a complex mixture, and it is unusual for neurotoxic features to dominate. In the United States, bites by the eastern coral snake and the Mojave rattlesnake can result in cranial and somatic muscular paralysis. Most snake bites involve young men bitten in summer. Typical neurotoxic symptoms and signs include paresthesias, ptosis, diplopia, weakness, and difficulty with breathing. Usually the diagnosis is obvious, although 15% of patients may lack fang marks, and neurotoxic symptoms can be delayed for up to a day. Treatment includes antivenom, support of
respiration, and treatment of other complications caused by the venom. SPIDER BITES
The black widow spider generates most neurotoxic spider bites. A typical case involves the female spider biting a child or young man on an extremity in the late summer or early fall. The bite may be painless or feel like a pinprick. Later, a cramping pain develops and muscle contractions ensue, often causing a rigid abdomen, trismus, and paroxysms of pain. The symptoms and signs seen after a black widow spider bite are shown in Table 105-14. Usually symptoms peak in a few hours, although in occasional cases symptoms peak in the second day. Most symptoms resolve in 1 to 2 days. Patients can feel weak or lethargic for up to 1 month. The diagnosis is based on knowing that the patient was bitten by a spider and identifying the type of spider. This is usually easy to do, although occasional patients may be bitten during sleep, and 20% of patients do not show evidence of a bite. The usual treatment consists of calcium gluconate, opioids, and benzodiazepines to relieve pain. An antivenom is available and effective but is derived from horse serum. Serious allergic reactions to the horse serum occur in about 3% of patients. For this reason, the antitoxin is most likely to be given to children, older adults, pregnant women, and patients with cardiovascular disease. SCORPION STINGS
Most scorpion stings are painful but otherwise spare the nervous system. In the United States, the chief neurotoxic scorpion is Centruroides exilicauda, which resides mainly in the Southwest, and its sting leaves no visible mark. Signs and symptoms of a Centrumides sting include the following: Local pain and paresthesia Pain and paresthesia remote to sting bite
TABLE 105-1 4. Signs and Symptoms of Black Widow Spider Bite Common Pain Muscle cramping and rigidity Abdominal rigidity Sweating Anorexia, nausea, and vomiting Hyperesthesia of skin Headache Restlessness Occasional Arrhythmias Bradycardia or tachycardia Bronchorrhea Cyanosis Delirium Fear of death Hypertension Increase or decrease in temperature Opisthotonos Piloeredion Priapism and ejaculation Psychosis Salivation Seizures Shock Trismus Urinarv retention
Chapter 105
Autonomic abnormalities Jerking or shaking of limbs or trunk Blurred vision Wandering eye movements Hypersalivation Trouble swallowing Tongue fasciculations Compromise of upper airway Slurred speech Patients with a severe sting should be hospitalized, sedated, given supportive care, and considered for antivenom therapy.
BEE AND WASP STINGS The main danger of bee and wasp stings is an allergic reaction to their venom. In rare cases, myasthenia gravis has developed after a wasp sting.
TICK PARALYSIS Tick paralysis is an uncommon disorder seen in the Pacific Northwest, Rocky Mountains, and southern United States. The tick season begins in March and ends in August, with a peak in May and June. The most common ticks in the United States are Derrnacentor andersoni and Dermacentor variabilis. Tick paralysis usually is caused by a gravid female tick that has fed for 4 to 7 days. About 80% of patients are children, and two thirds of the children are girls because they are more likely to have long hair, where the tick hides. About 20% of cases are in adults, and 80% of these are men. The disease starts with a day-long prodrome of irritability, lassitude, or generalized weakness. Over the next day or two a symmetrical flaccid paralysis develops in the legs and ascends to the arms and then the neck, pharyngeal, and respiratory muscles. Weakness can be proximal more than distal. Areflexia and paresthesia are common, but objective sensory loss is unusual. Early on and in mild cases, ataxia may be more prominent than weakness. From 10% to 12% of patients, almost always children, die. Most laboratory tests are normal. Nerve conduction studies reveal involvement of motor and sensory nerves, with mild slowing of conduction velocity, a reduced amplitude of the evoked response, and prolonged distal latencies. The diagnosis of tick paralysis is suggested when a young girl develops an ascending areflexic paralysis in the spring or summer. These abnormalities resemble Guillain-Barrk syndrome. The correct diagnosis hinges on finding and removing a tick, found on the head or neck in 60% to 70% of the cases. The tick should be removed by steady traction. Once the tick is completely removed, improvement usually is rapid, but paralysis can progress for up to 2 days after tick removal.
Toxic and Metabolic Disorders of the Neuromuscular Junction
675
PLANTS CONTAINING NICOTINE A number of plants contain pyridine and piperidine alkaloids,
including nicotine, that can cause the following signs and symptoms: Nicotinic Weakness Fasciculations Paralysis Tachycardia Coma Seizures Hypertension Muscarinic Salivation Lacrimation Urination Gastrointestinal cramping Vomiting Miosis Bronchospasm Bradycardia Diaphoresis
Severe plant poisonings are unusual and are treated with activated charcoal if the ingestion is recent, atropine to block muscarinic symptoms, anticonvulsants for seizures, and ventilatory support if needed. Patients must be monitored for rhabdomyolysis and renal failure.
SUGGESTED READINGS Barrons RW Drug-induced neuromuscular blockade and myasthenia gravis. Pharmacotherapy 17:1220, 1997 Bond G R Snake, spider, and scorpion envenomations in North America. Pediatr Rev 20:147, 1999 Cherington M Clinical spectrum of botulism. Muscle Nerve 21:701, 1998 Cornblath DR, Sladky JT, Sumner AJ: Clinical electrophysiology of infantile botulism. Muscle Nerve 6448, 1983 Felz MW, Smith CD, Swift TR A six-year-old girl with tick paralysis. N Engl J Med 34290,2000 Furbee B, Wermuth M: Life-threatening plant poisonings. Crit Care Clin 13:849, 1997 Maselli RA, Bakshi N Botulism. Muscle Nerve 23:1137, 2000 Midura, T F Update: infant botulism. Clin Microbiol Rev 9:1, 1996 Shapiro RL, Hatheway C , Swerdlow DL Botulism in the United States: a clinical and epidemiologic review. Ann Intern Med 129:221, 1998. Walker FG, Bilden EF, Gibly RL: Envenomations. Crit Care Clin 15:353, 1999
SECTION
5
DISEASES OF MUSCLE
106 Amroach to Patients with Muscle Disorders Anthony A. Amato Evaluating patients with neuromuscular disorders can be challenging. As in other neurologic diseases, the key to arriving at the correct diagnosis is carefully localizing the lesion. Weakness can be the result of central lesions (brain or spinal cord processes, e.g., brainstem infarct, central pontine myelinolysis, transverse myelopathy), anterior horn cell disease (e.g., amyotrophic lateral sclerosis [ALS], poliomyelitis), peripheral neuropathy (e.g., Guillain-BarrC syndrome [GBS]), neuromuscular junction defects (botulism, Lambert-Eaton myasthenic syndrome, myasthenia gravis), or myopathic disorders. The most important aspect of assessing patients with neuromuscular disorders is taking a thorough history of the patient’s symptoms, disease progression, and past medical and family history and performing a detailed neurologic examination. Based on the findings on the history and physical examination, the clinician should order specific laboratory tests, electrophysiologic tests, and muscle or nerve biopsies rather than using a shotgun approach to diagnosis. It is usually not difficult to distinguish generalized weakness secondary to cerebral or brainstem insults from other causes of muscle weakness because in these central disorders weakness is accompanied by impaired consciousness. However, myelopathies can be more troublesome. Compressive lesions of the spinal cord and nerve roots can result in a combination of upper and lower motor neuron abnormalities that can mimic ALS and vice versa. Acute transverse myelitis may result in rapid quadriparesis, in which the deep tendon reflexes are initially absent from a “shocked cord.” Such cases may be confused initially with GBS. Although transverse myelitis and GBS usually are associated with sensory loss, a true sensory level is not evident in GBS but should be evident in myelopathies. Motor and sensory symptoms and signs are helpful in distinguishing peripheral neuropathies from anterior horn cell disorders, myopathies, and neuromuscular junction disorders. However, some types of peripheral neuropathy are predominantly or purely motor and therefore can be difficult to distinguish from these other disease processes. Most neuropathies are associated with distal greater than proximal weakness. However, significant proximal weakness can be seen in certain peripheral neuropathies (e.g., GBS, chronic inflammatory demyelinating polyradiculoneuropathy). Furthermore, although usually associated with proximal weakness, certain myopathies and rarely even neuromuscular junction disorders can manifest with primarily distal weakness. ALS is the result of degeneration of upper and lower motor neurons. The degeneration of lower motor neurons leads to 676
muscle weakness, atrophy, and fasciculations that typically begin focally. Upper motor neuron involvement manifests as spasticity and pathologically brisk deep tendon reflexes. Although most patients over time develop both upper and lower motor neuron deficits, some patients continue to have pure lower motor neuron abnormalities, and others have only upper motor neuron signs. Some of the hereditary spinal muscular atrophies present with generalized symmetrical proximal greater than distal weakness and can be difficult to distinguish from myopathic disorders. The key in distinguishing neuromuscular junction defects from myopathies is the fluctuation in symptoms and signs in the former. Patients with myasthenia gravis usually fatigue with repetitive activity, whereas patients with Lambert-Eaton syndrome can actually improve with continued physical exertion. Neuromuscular junction disorders have a predilection to affect the extraocular muscles, which are less commonly affected in myopathies. The following discussion on approaching patients with neuromuscular complaints emphasizes myopathic and neuromuscular junction disorders. The workup of patients with peripheral nerve disorders is discussed in Chapter 90.
MEDICAL HISTORY While obtaining the medical history, the clinician should attempt to define onset and course of the illness and the distribution of symptoms. Disorders presenting in infancy (Table 106-1) are different from those that manifest later in childhood or early adult life (Table 106-2)or in late adulthood (Table 106-3).Importantly, the rate of progressiou must be assessed as some disorders progress acutely over days or weeks (Table 106-4),whereas others evolve more slowly over months (Table 106-5).Furthermore, the course of the disease may be monophasic, relapsing, or chronic and progressive. The patients’ presenting symptoms depend on the muscle groups that are predominantly affected. Proximal leg weakness usually manifests initially as progressive difficulty climbing stairs and arising from a chair, commode, or the floor. Affected patients often use their arms to help pull themselves up the stairs with a hand rail or push themselves up from a sitting position. Patients with weakness of the anterior compartment of the distal leg develop foot drop, and they complain of frequent tripping or stubbing of the toes. When the distal legs are affected, patients have difficulty standing on their toes. Shoulder girdle weakness affects the patient’s ability to lift his or her arms overhead (e.g., as in brushing one’s hair or lifting
Chapter 106 W Tmu 106-1. Differential Diagnosis of the
Floppy Infant
Central nervous system disorders (most common cause) Anterior horn cell Spinal muscular atrophy type 1 and 2 Peripheral neuropathy Congenital hypomyelinatingor arnyelinating neuropathy Charcot-Marie-Tooth (CMT) 111 (Dejerine-Sottas) CMT I and CMT II (rare) Giant axonal neuropathy Neuromuscular junction Infantile botulism Infantile myasthenia gravis Congenital myasthenia Myopathy Congenital myopathies (all of them can present in infancy) Muscular dystrophies Congenital muscular dystrophies Dystrophinopathy or sarcoglycanopathy (rare) Congenital myotonic dystrophy Metabolic myopathies Glycogen storage defects Acid maltase deficiency Debrancher deficiency Branching enzyme deficiency Myophosphorylase deficiency (rare) Disorders of lipid metabolism Carnitine deficiency Fatty acid-Acyl-CoA dehydrogenase deficiencies Mitochondrial myopathies Benign and fatal infantile myopathy Leigh’s syndrome Endocrine myopathies (e.g., hypothyroidism)
objects). Patients with hand weakness complain of difficulty in grasping or gripping objects. They describe problems opening jar tops and turning doorknobs. Patients with neck weakness may have difficulty lifting their head off a pillow. Furthermore, sudden braking or accelerating in a car can cause the head to jerk back and forth. Involvement of cranial muscles may result in ptosis, diplopia, dysarthria, or difficulty chewing and swallowing. The examiner should inquire about extreme fluctuations in strength during the day or associated with physical activities. Fluctuations in strength are more typical of neuromuscular junction disorders. Ask patients whether they have noticed any muscle atrophy or enlargement of their muscles. Specific neuromuscular conditions are associated with fasciculations, myalgias, cramps, stiffness or myotonia, periodic paralysis, and myoglobinuria. The clinician should ask about sensory symptoms. Patients may complain of feeling “numb,” but this word has different meanings for different people. The examiner should specifically ask the patient about the presence or absence of sensory loss, tingling, prickly, electrical, stabbing, burning, and dull aching pain. Fatigue is a very nonspecific symptom, and the majority of patients referred to my neuromuscular clinic for evaluation of fapgue do not have a primary neuromuscular disorder. Although many patients complain of “feeling weak all over,” their neuromuscular examination typically is normal or limited by give-way. Clearly, patients with neuromuscular disorders experience fatigue. However, patients with neuromuscular disorders usually have objective muscle weakness on examination. Evaluation of muscle pain is another common reason for referral to neuromuscular clinics. Most neuromuscular disorders, including myopathies, are not associated with severe muscle pain or tenderness. Some patients with muscular dystrophy or inflammatory myopathy describe mild to moderate, nontender, deep,
Approach to Patients with Muscle Disorders
677
aching discomfort in the muscles that is seldom severe enough to warrant analgesics (Table 106-6). However, severe myalgias and tenderness can accompany fasciitis, myositis related to infections, and rhabdomyolysis or myoglobinuria caused by various metabolic myopathies, electrolyte disturbances, and toxins. Patients with psychosomatic iUness often complain of severe generalized muscle pain and tenderness unrelieved by analgesic medications. They usually also describe generalized weakness or fatigue. Despite these severe symptoms, there is no objective evidence of a neuromuscular disease on clinical examination, laboratory testing, electrophysiologic studies, or muscle biopsy. The medical history of patients is important because certain illnesses are associated with specific neuromuscular disorders. For example, inflammatory myopathies may be seen in patients with connective tissue disease, concurrent autoimmune disorders may be present in patients with myasthenia gravis (MG), LambertEaton myasthenic syndrome (LEMS) is associated with small cell lung cancer and other autoimmune disorders, and neuropathies are common in patients with systemic diseases (e.g., diabetes mellitus, human immunodeficiency virus infection, cancer). The
W TABLE 1
Weakness Presenting in Childhood or Early Adulthood
Anterior horn cell Spinal muscular atrophy type 3 Poliomyelitis Amyotrophic lateral sclerosis (rare) Peripheral neuropathy Acute or chronic inflammatorydemyelinating polyneuropathy Hereditary neuropathies Neuromuscular junction Botulism Myasthenia gravis Congenital myasthenia Lambert-Eaton syndrome Myopathy Congenital myopathies Central core Multicore Centronuclear Nernaline Myofibrillar Muscular dystrophies Dystrophinopathy (Duchenne or Becker) Limb girdle muscular dystrophies Congenital muscular dystrophy (partial merosin deficiency) Myotonic dystrophy Other dystrophies (e.g., FSHD, EDMD) Metabolic myopathies Glycogen storage defects Acid maltase deficiency Debrancher and branching enzyme deficiency Disorders of lipid metabolism Carnitine deficiency Fatty acid-Acyl-CoA dehydrogenase deficiencies Mitochondrial myopathies Periodic paralysis Electrolyte imbalance Hyperkalemia Hypokalemia Hypophosphatemia Hypercalcemia Endocrine myopathies Toxic myopathies Inflammatory rnyopathies Dermatomyositis Polymyositis (after age 20 years) Infectious rnyositis Abbreviations: EDMD, Emety Dreifuss muscular dymophy; FSHD, facioxapulohumerai muscular dystrophy.
678
Spinal Cord and Peripheral NeuromuscularDisease I Diseases of Muscle
TABU106-3. Weakness Presenting in Middle t o Late Adulthood Anterior horn cell Spinal muscular atrophy type 3 Kennedvs disease poliomyelitis Amyotrophic lateral sclerosis Peripheral neuropathy Hereditary neuropathies Acute or chronic inflammatory demyelinating polyneuropathy Drug-induced or toxic neuropathies Diabetic neuropathy Amyloid Vasculiis Neuromuscular junction Botulism Myasthenia gravis Lambert-Eaton syndrome Myopathy Congenital myopathies Myofibrillar myopathy (other types are uncommon) Muscular dystrophies Dystrophinopathy (Becker) Limb girdle muscular dystrophies Oculopharyngeal dystrophy Bent spine or dropped head syndrome Metabolic myopathies Glycogen storage defects Acid maltase deficiency Debrancher deficiency Disorders of lipid metabolism (rare) Mitochondria1myopathies Periodic paralysis Familial hypo-KPP manifest within the first three decades Familial hyper-KPP usually manifests in the first decade Electrolyte imbalance Hyperkalemia Hypokalemia Hypophosphatemia Hypercakemia Endocrine myopathies Toxic myopathies Myopathy associated with systemic disease (e.g., cancer), poor nutrition, disuse Amyloid myopathy Inflammatory myopathies Inclusion body myositis (most common inflammatory myopathy after age 50 years) Dermatomyositis Polymyositis (after age 20 years) Infectious myositis Abbreviations: hyper-KPP, hyperkalemic periodic paralysis; hypo-KPP, hypokalemic periodic paralysis.
review of systems should assess symptoms associated with specific disorders (e.g., arthralgias to assess for underlying connective tissue disease). It is essential to obtain an accurate family history. When a hereditary disorder is suspected, try to examine other affected family members. Some patients may claim a family history of a particular disorder, but when affected family members are examined a different disease may be diagnosed. For example, I have seen patients who stated that muscular dystrophy runs in their family. However, on examination of these affected family members, their disease turned out to be spinal muscular atrophy. In addition, some family members who are asymptomatic may be found to have subtle signs of disease on a thorough examination, leading to the correct diagnosis of a hereditary neuromuscular disorder. The clinician must inquire about current and recent medications, alcohol, tobacco, drug abuse, and previous exposures to environmental toxins to rule out a toxic neuropathy or myopathy.
The severity of the neuromuscular disorder depends on the type of toxin and the dosage and duration of the exposure.
PHYSICAL EXAMINATION After the medical history, a complete neurologic examination should be performed. Most importantly, ascertaining the pattern of involvement will help narrow the differential diagnosis. Most rn TABU 106-4. Neuromuscular Disorders Presenting with Acute or Subacute Proximal Weakness Anterior horn cell Poliomyelitis Peripheral neuropathy Guillain-Barre syndrome Porphyria Diphtheria Tick paralysis Toxic neuropathies Diabetic amyotrophy Vasculitis Carcinomatous infiltration (e.g., leukemia, lymphoma) Paraneoplastic neuropathy Neuromuscular junction Botulism Lambert-Eaton syndrome Myasthenia gravis Myopathy Periodic paralysis Electrolyte imbalance Endocrinopathies Inflammatory myopathies Dermatomyositis Polymyositis Infectious myositis (Note: Inclusion body myositis does not present acutely) Toxic myopathies Metabolic myopathies Glycogen and lipid disorders in association with myoglobinuria
W
TABU106-5. Differential Diagnosis of Chronic Progressive Proximal Weakness
Anterior horn cell Amyotrophic lateral sclerosis Spinal muscular atrophy type 3 Kennedy's disease Peripheral neuropathy Chronic inflammatory demyelinating polyneuropathy Multifocal motor neuropathy Toxic neuropathies Neuropathy associated with systemic disorders Connective tissue disease (e.g., vasculitis) Diabetes mellitus Amyloidosis Paraneoplastic Carcinomatous infiltration (e.g., leukemia, lymphoma) Neuromuscular junction Lambert-Eaton syndrome Myasthenia gravis Myopathy Muscular dystrophies Congenital myopathies Periodic paralysis Electrolyte imbalance Endocrinopathies Inflammatory myopathies Dermatomyositis Polymyositis Infectious myositis Toxic myopathies Metabolic myopathies (some glycogen and lipid storage disorders, mitochondrial myopathies)
Chapter 106
TABLE106-6. Disorders Associated with Muscle Pain Mild forms of muscular dystrophy (e.g., Becker muscular dystrophy, limb girdle muscular dystrophy) Metabolic Myopathies Glycogen storage diseases (e.g., phosphorylase, phosphofructokinase deficiencies) Myoadenylate deaminase deficiency Mitochondrial cytopathies Hypothyroid myopathy Toxic myopathies (e.g., cholesterol-loweringagents, cyclosporine, chloroquine) Inflammatory myopathy Idiopathic (dermatomyositis, polymyositis, overlap myositis) Infectious myositis (including human immunodeficiency virus infection) Fasciitis Eosinophilic myalgia syndrome Polymyalgia rheumatica Fibromyalgia
TABU 106-7. Disorders with Proximal Weakness Anterior horn cell Poliomyelitis Amyotrophic lateral sclerosis Spinal muscular atrophy Kennedqs disease Peripheral neuropathy Cuillain-Barre syndrome Chronic inflammatory demyelinatingpolyneuropathy Porphyria Diphtheria Tick paralysis Diabetic amyotrophy Polyradiculopathy secondary to carcinomatous infiltration (e.g., leukemia, lymphoma), infection (Lyme disease, human immunodeficiency virus, cytomegalovirus), sarcoidosis Neuromuscular junction Botulism Lambed-Eaton syndrome Myasthenia gravis Congenital myasthenia Myopathy Limb girdle muscular dystrophies Congenital myopathies Periodic paralysis Electrolyte imbalance Endocrinopathies Inflammatory myopathies Dermatomyositis polymyositis Inclusion body myositis infectious myositis Toxic myopathies Metabolic myopathies (various glycogen and lipid storage disorders and mitochondria1myopathies)
Approach to Patients with Muscle Disorders
679
muscle wasting, and frontal balding. A characteristic rash typically is present in patients with dermatomyositis. Therefore, specific neuromuscular disorders can be diagnosed or at least strongly suspected just by observing the patient while taking his or her medical history. For a proper and thorough examination, the patient must undress except for undergarments and a gown. Watch the patient arise from the seat and walk. Watch the patient stand and walk from the side as well as from the front and back. On side viewing, the clinician can detect excessive lumbar lordosis, hyperextension of the knee (genu recurvaturn), and ankle contractures in patients
TABLE 106-8. Differential Diagnosis of Distal Weakness Cervical disease Multilevel radiculopathy (C7, CB, T1) Lower trunk brachial plexopathy Syringomyelia Tumor of the cord Lumbosacral disease Tumor of the conus medullaris Polyradiculopathy (L4, L5, S1, S2) Lumbosacral plexopathy Motor neuron disorders Distal spinal muscular atrophy Amyotrophic lateral sclerosis Neuromuscular junction Myasthenia gravis (rare) Congenital myasthenia gravis (e.g., slow ion channel defect) Peripheral neuropathies Charcot-Marie-Tooth disease and related hereditary neuropathies Multifocal demyelinating motor or sensorimotor neuropathies Vasculitis Toxic or metabolic neuropathies Intrinsic muscle disorders Distal myopathies or dystrophies Facioscapulohumeral muscular dystrophy Scapuloperoneal syndromes Emery-Dreifuss muscular dystrophy Oculopharyngodistal muscular dystrophy Myotonic dystrophy Acid maltase deficiency Debrancher enzyme deficiency Phosphorylase b kinase deficiency Myofibrillar myopathy Central core disease Centronuclear myopathy Nemaline myopathy Inclusion body myositis Focal myositis
w TAW 106-9. Neuromuscular Causes of F'tosis or Ophthalmoplegia
myopathies preferentially affect the proximal more than distal muscles, and the converse is true in most types of peripheral neuropathy. However, proximal weakness can be seen in disorders other than myopathies (Table 106-7). Furthermore, distal muscles can be weaker than the proximal muscles in certain myopathies and other neuromuscular disorders besides peripheral neuropathies (Table 106-8). A few neuromuscular disorders have a predilection for involving the extraocular muscles (Table 106-9). The physical examination begins while the clinician is obtaining the history of the present illness. Extraocular, facial, jaw, pharyngeal, tongue, and neck weakness may be apparent by just observing the patient during history taking. Ptosis, ophthalmoparesis, or dysarthria may be evident while one is talking to the patient, leading to consideration of myasthenia gravis. Patients with myotonic dystrophy often have facial weakness, temporalis
Peripheral neuropathy Guillain-Barre syndrome Miller-Fisher syndrome Neuromuscular junction Botulism Lambert-Eaton myasthenic syndrome Myasthenia gravis Congenital myasthenia Myopathy Mitochondrial myopathies Kearns-Sayre syndrome Progressive external ophthalmoplegia Oculopharyngeal and oculopharyngodistal muscular dystrophy Myotonic dystrophy (ptosis only) Congenital myopathy Myotubular Nemaline (ptosis only) Hyperthyroidism or Graves's disease (ophthalmoplegia without ptosis)
680
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Muscle
with proximal muscle weakness. An excessive lordosis and a wide-based, waddling gait often accompany hip girdle weakness. Patients with quadriceps weakness hyperextend the knee (known as genu recurvatum or back-kneeing) to provide stability to the knee while standing and walking. Exaggerated lumbar lordosis and genu recurvatum may also lead to toe walking. A steppage gait is evident in patients with foot drop caused by weakness of the anterior compartment of the distal lower extremity. Instead of striking the ground first with the heel of the foot, the patient lands flat-footed or strikes the ground with the toes first. To avoid tripping, the patient lifts the knee higher than normal so that the foot clears the ground during the swing phase of ambulation. Also, watch the patient walk on his or her heels and toes to help assess distal lower extremity strength. Weakness of the shoulder girdle may result in winging of the scapula, drooping of the shoulders, and inward rotation of the arms. In addition, the clavicles may become displaced horizontally, and there can be diagonal or horizontal displacement of the anterior axillary lines. One may also observe that internal rotation of the arms leads to the palm of the hands facing to the back (dorsum of hand facing forward) rather than the palms facing the body. Inspect the muscles of the face, trunk, and extremities for atrophy, hypertrophy, or fasciculations. Palpate the muscles for tenderness and check the tone. In addition, muscles can be percussed in the upper and lower extremity as well as the face, including the tongue, to look for myotonia. Action myotonia is assessed for by having the patient make a grip for a brief period and then try to relax. Patients with myotonia have delayed relaxation. Myotonia generally improves with repetition, whereas paramyotonia worsens with repetitive activity. Paramyotonia occurs in patients with paramyotonia congenita and is best demonstrated by having patients repeatedly open and close their eyes; eventually patients have difficulty completely opening their eyes. Percussion of muscles can elicit other abnormalities. In so-called rippling-muscle disease, a wave of muscle contractions emanating from the site of percussion is seen. Patients with hypothyroidism may have mounding of the percussed muscle (myoedema). I use the Medical Research Council (MRC) scale for uniformity in grading manual muscle strength. The MRC scale is as follows: grade 0, no visible contraction; grade 1, trace contraction; grade 2, full movement across the joint with gravity eliminated; grade 3, full movement across the joint against gravity; grade 4, full movement against gravity plus some resistance; grade 5, normal strength. A modification of this scale usually is used by adding plus (e.g., 4+) or minus signs (e.g., 3-) next to the numbers for a finer distinction or degrees of muscle weakness between the larger grades. I routinely grade the strength of the orbicularis oculi, jaw, and tongue; neck flexion and extension; shoulder abduction, flexion, and extension; elbow flexion and extension; wrist flexion and extension; finger and thumb flexion, extension, and abduction; hip flexion, extension, and abduction; knee flexion and extension; ankle dorsiflexion; plantar flexion, inversion, and evasion; and toe flexion and extension. Because the MRC scores reflect movement against gravity, these muscle groups must be tested against gravity. Therefore, neck flexion should be assessed with the patient supine; neck extension, hip extension, and knee flexion with the patient prone; and hip abduction with the patient on his or her side. It is essential to place the patient in these various positions to accurately assess muscle strength. Muscle function is also evaluated by observing the patient arise
from the floor or a chair or climb steps. Have the patient hop on one foot at a time to detect subtle weakness. Recording the time necessary to accomplish specific tasks (e.g., climbing ten steps or walking 30 feet) is helpful, especially in monitoring the patient. In patients with myasthenia gravis, measure the distance of the interpalpebral fissures and record the time it takes for ptosis to appear after sustained upgaze. Muscle tone is graded as normal, decreased, or increased. Corticospinal tract lesions lead to increased tone or spasticity. Myopathies, neuromuscular junction disorders, and neuropathies are associated with normal or decreased tone. Deep tendon or muscle stretch reflexes are graded as 0, absent; 1+, decreased (requiring reinforcement maneuvers to obtain); 2+, normal; 3+, brisk (spread to other muscle groups); 4+, pathologically brisk (clonus). Hyperreflexia is seen in patients with upper motor neuron lesions, and hyporeflexia is decreased in patients with lower motor neuron disease and peripheral neuropathy. Reflexes are normal in patients with myasthenia gravis but are usually diminished in patients with Lambert-Eaton syndrome. Deep tendon reflexes may be normal or diminished in myopathies. Plantar responses usually are assessed by stroking the sole of the foot and looking for pathologic dorsiflexion or extension of the big toe (a positive Babinski sign). The pathologic extension of the big toe can also be demonstrated by stroking the lateral aspect of the foot (Chaddock’s sign), after rubbing the anterior aspect of the shin (Oppenheimer’s sign), or after a prick of the extensor aspect of the toe (Bing’s sign). Plantar responses are extensor in patients with corticospinal tract involvement. However, in patients with significant weakness of the toes, a plantar response may be unobtainable and therefore not interpretable. Test sensory perception to various modalities (temperature, pain, touch, vibration, and proprioception). Temperature and pain are conveyed by small-diameter nerve fibers, whereas deep touch, vibration, and proprioception are conveyed mainly by large-diameter sensory nerves. Some neuropathies predominantly affect small-diameter nerve fibers, whereas other neuropathies have a predilection for larger fibers. The sensory examination is normal in patients with pure motor neuron disease, myopathy, or MG unless the patient has a concurrent neuropathy. Patients with LEMS may experience mild sensory symptoms. Muscle weakness in infants usually is characterized by an overall decrease in muscle tone (floppy infant). It is important to examine the parents of floppy infants for clues to the infant’s neuromuscular disorder (e.g., myasthenia gravis, myotonic dystrophy). Infants are more difficult to examine than older children and adults. The examiner should observe the infant lying supine for any spontaneous muscle movement. Infants can be positioned prone to see whether they are capable of extending their head. An inability to do so suggests weakness of the neck extensor muscles. Assess neck flexion strength by pulling the child from the supine to sitting position while looking for head lag. The infant should be held prone in the examiner’s hands to see whether the head and extremities droop (so-called ragdoll appearance). The vigor of crying heard during the examination helps assess bulbar strength in the infant. The site of the lesion (upper motor neuron, anterior horn cell, peripheral nerve, neuromuscular junction, or muscle) usually is apparent after a detailed medical history and physical examination are obtained. In the patient in whom the site is still unclear, further testing is needed. Electromyograms (EMGs) and nerve conduction studies (NCSs) are useful in localizing the lesion to the anterior horn cell, peripheral nerve, neuromuscular junction, or muscle.
Chapter 106
Features on EMG or NCS may also help identify the specific disorder (e.g., MG, LEMS, Charcot-Marie-Tooth disease type 1). Finally, rather than a shotgun approach to ordering additional laboratory tests, specific tests are requested depending on the localization of the disease process. It is essential to diagnose neuromuscular disorders early and correctly, particularly for treatable diseases (e.g., inflammatory neuropathies and myopathies, MG, LEMS). Even in chronic disorders in which progression cannot be halted (e.g., muscular dystrophy, ALS), diagnosis is important because therapies (e.g., physical, occupational, and speech therapy) are available to improve quality of life. Furthermore, correct diagnosis is essential for genetic counseling. The remainder of this chapter outlines the specific tests that are ordered when evaluating a patient suspected of having a neuromuscular junction disorder or myopathy.
ELECTRODIACNOSTICEXAMINATION In general, I routinely perform at least two motor and sensory NCSs in an arm and a leg when evaluating patients for a neuromuscular disorder. In addition, it is important to do an EMG of proximal and distal muscles as well as thoracic paraspinal muscles. If a neuromuscular junction process is considered, I perform repetitive nerve conduction studies and, if this is not informative, single-fiber EMG. Nerve Conduction Studies
Motor and sensory NCSs are invaluable in assessing patients with neuromuscular disorders, particularly in looking for evidence of a peripheral neuropathy. Sensory NCSs are normal in motor neuron disease, myopathies, and neuromuscular junction diseases. Motor NCSs demonstrate normal amplitudes, distal latencies, and conduction velocities in myasthenia gravis. In LEMS, the amplitudes of the compound muscle action potentials (CMAPs) usually
L.
Approach to Patients with Muscle Disorders
681
are low. After the muscle is exercised for 10 to 15 seconds, the CMAP amplitude typically is 200% higher than the baseline value in patients with LEMS. Motor NCSs usually are normal in patients with myopathies. However, in very weak muscles, particularly in patients with distal myopathies, the CMAP amplitudes can be diminished. Repetitive Nerve Stimulation
Repetitive stimulation studies are used to diagnose neuromuscular junction disorders (i.e., botulism, LEMS, congenital myasthenia, and MG). The technique is easier to perform on distal muscles (e.g., abductor digiti minimi) because these muscles can be stabilized and stimulation is generally less painful. However, the sensitivity of the test is less in the distal muscles in patients with myasthenia gravis. More proximal muscles (e.g., trapezius, quadriceps, and face) are more likely to demonstrate decrement, but repetitive stimulation at these sites is technically more difficult secondary to diminished ability to stabilize the muscle groups, and the procedure usually is more painful at these sites. As noted earlier, patients with myasthenia gravis have normal baseline CMAP amplitudes. However, on slow rates (2 to 3 Hz) of repetitive stimulation, a decrementing response (more than 10%) may be observed (Fig. 106-1). Ten seconds of exercise may correct this decrement (postexercise facilitation). If decrement is not seen at rest, it is important to exercise the muscle for 1 minute and then perform repetitive stimulation once a minute for 5 minutes to look for the decrement (postexercise exhaustion). In botulism and LEMS, the baseline motor amplitudes are low. Decrements may be seen after low rates of repetitive stimulation. An incrementing response may be seen after fast rates of repetitive stimulation (20 to 50 Hz; Fig. 106-2). This is a very painful procedure and is rarely necessary because 10 seconds of exercise usually can reproduce a significant increase in amplitude from baseline as noted earlier.
A b d Pol
Br
R u p NPanp Ware4 NPdur PPanp (I) ( X c h g ) C7sb) (Xchg) ( Z c h g ) E.O 0.0 0.8 1 0.0 2
3 4
5
-34.8 -52.8
-59.3 -62.5
-36.2 -53.5 -60.6 -64.8
8.0 -3.8
-36.6 -54.0
-3.8 -3.8
-61.5 -65.1
FIG. 106-1. Myasthenia gravis. Repetitive nerve stimulation at 3 Hz of the median nerve recording from the abductor pollicis brevis demonstrates a significant decrement (more than 1go/,) supportive of a neuromuscular junction defect.
682
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Muscle
FOOT SWITCH:
STIM,M#DE:
POT
NO.
1
5 10 20
30 90 50 60 I
AMP. OECR 2
P-P AMP mU
1.59 1.68 2.27 3.90 5.22 6.26
AREA
mums 2.6i 2.70
0 -9 -97 -153 -239 -306 0
OUFL OUFL I
READY 1 STIMULATE /m 1 SINGLE
3.80 6.20 7.82 9.li OUFL OUFL
0 I
I
I
I
1
FIG. 106-2. Lambert-Eaton myasthenic syndrome. Repetitive nerve stimulation of the ulnar nerve recording from the adductor digiti minimi at 30 Hz reveals a low-amplitude (1.54 mv) wave followed by an incrementing response to more than 300% of the baseline amplitude.
Needle Electromyography The routine needle EMG is performed with particular attention paid to motor unit action potential (MUAP) duration, morphology, amplitude, and recruitment. It is also important to assess for the presence of abnormal insertional and spontaneous activity. A thorough examination of multiple muscles is necessary, especially in mild or moderately severe disease states. By assessing these various components, the electromyographer usually can determine whether the lesion is neuropathic or myopathic. Special techniques such as quantitative EMG may be needed in difficult or borderline cases. Single-fiber EMG is useful in diagnosing patients with myasthenia gravis in whom repetitive stimulation, a Tendon test, and autoantibody testing are uninformative. Single-fiber EMG measures the “jitter” between two single muscle fibers belonging to the same motor unit. Jitter is increased in myasthenia gravis. However, increased jitter is not specific for myasthenia gravis because it can be seen in any pathologic process involving remodeling of the neuromuscular junction (e.g., reinnervation in motor neuron disease, neuropathies, necrotizing myopathies).
LABORATORY EVALUATION Myasthenia CravSs Approximately 40% of patients with myasthenia gravis have thymic hyperplasia, and 10% have a thymoma. Therefore, a chest computed tomography (CT) scan should be obtained in all patients with myasthenia gravis. The presence of a thymoma is an absolute indication for thymectomy. It is controversial whether or not to thymectomize patients with nonthymomatous generalized myasthenia gravis. Most experts in the field would not thymectomize purely ocular myasthenia unless there was evidence of a thymoma. Acetylcholine receptor antibodies are detectable in 70% to 80% of patients with ocular myasthenia gravis and up to 90% of
patients with more severe generalized myasthenia. Antistriatal muscle antibodies are present in approximately 30% of adults with myasthenia gravis, roughly 80% of whom have thymomas. However, one can have a thymoma without antistriatal antibodies. Therefore, the lack of these antibodies does not obviate a chest CT scan. I also order antinuclear antibodies and a thyroid function test because of the increased frequency of other autoimmune diseases and hyperthyroidism in patients with myasthenia gravis. Lambert-Eaton Myasthenic Syndrome LEMS can occur as paraneoplastic complication (approximately two thirds of cases) or as a primary autoimmune disorder without an underlying cancer. Small cell cancer of the lung is responsible for 90% of the malignancies associated with paraneoplastic LEMS. The majority of patients with cancer are more than 40 years old, and symptoms of LEMS usually precede detection of the malignancy by several months or years. I order chest CT scans, mammograms, and pelvic CT scans on patients with LEMS. I also recommend a gastrointestinal evaluation if the patient has signs or symptoms of gastrointestinal involvement. Antibodies directed against the voltage-gated muscle calcium channel (Lambert-Eaton syndrome) are present in 90% of patients with paraneoplastic and primary autoimmune LEMS. There is a higher frequency of other autoantibodies and autoimmune diseases (e.g., systemic lupus erythematosus, rheumatoid arthritis, primary biliary cirrhosis, inflammatory bowel disease) in the primary form of LEMS.
Botulism is caused by the exotoxin of Clostridium botulinum. Infantile botulism is contracted by ingestion of bacterial spores (e.g., usually from contaminated honey), which subsequently colonize the gut and release the toxin. Wound botulism can occur after colonization of deep wounds, as occurs in compound
Chapter 106
fractures, or subcutaneous injection sites in drug addicts. Botulism can also arise from food poisoning resulting from the direct ingestion of the toxin from improperly canned and cooked foods. The toxin can be assayed in the serum and stool in suspected cases. Polymerase chain reaction (PCR) can also be used to identify the organism in biological specimens and food. Myopathies The single most useful blood test in a patient evaluated for weakness is a serum creatine kinase (CK) level. The upper limit of normal in the ambulatory population for serum CK depends on the person’s sex and race and is typically higher than most established laboratory normative data. For instance, the upper limit of normal for serum in black men is just over 500 IU/L; in black women, white men, and Hispanics the CK can be more than 300 IU/L; and in white women the upper limit of normal is more than 200 IU/L. Importantly, mild elevations in serum CK can be seen in neurogenic process such as motor neuron disease or other rapidly denervating process in which large amounts of muscle are damaged. However, the serum CK is rarely elevated above 1000 IU/L in these conditions. In addition, it is important to note that not all patients with myopathies have elevated serum CK levels. Furthermore, the serum CK levels do not necessarily correlate with the severity of the underlying myopathy. Other enzymes that are routinely screened for on routine laboratory tests (e.g., aspartate aminotransferase [AST], alanine aminotransferase [ALT], lactate dehydrogenase [ LDH], and aldolase) may also be elevated in myopathies and in liver disease. To distinguish elevation of these enzymes caused by liver disease from a myopathic process, a serum CK that is specific for muscle disease and gamma-glutamyltransferase (GGT) that is specific for liver disease should be obtained. In this regard, treatment of inflammatory myopathies with certain immunosuppressive agents (i.e., azathioprine and methotrexate) is hepatotoxic. Therefore, while following the liver functions tests of such patients on treatment, it is essential to check to GGT and CK levels, not just the AST, ALT, or LDH, because these later enzymes may become elevated from an exacerbation of the underlying myositis rather than from liver damage. I also order routine electrolytes in patients suspected of having a myopathy. Hyperkalemia and hypokalemia can be caused by a number of conditions and can result in generalized weakness. Likewise, hypercalcemiaand hypocalcemia may lead to generalized weakness. Thyroid function tests are obtained because both hyperthyroidism and hypothyroidism are associated with myopathies. In patients suspected of having an inflammatory myopathy, an erythrocyte sedimentation rate and antinuclear antibody test are ordered to assess for an underlying connective tissue disease. A serum protein electrophoresis or immunofixation looking for a monoclonal gammopathy should be ordered to help diagnose primary amyloidosis. With the explosion in our understanding of molecular genetics, there is an ever-expanding list of hereditary myopathies that can be diagnosed by way of DNA testing. In male patients with a limb girdle pattern of weakness, I start out by ordering DNA testing for dystrophin mutations on whole blood. Approximately two thirds of dystrophinopathies have mutations detectable by routine PCR and Southern blot analysis of whole blood DNA. Therefore, a negative mutation analysis for dystrophin does not rule out a dystrophinopathy. If this test is negative, I proceed with a muscle biopsy. The tissue can be immunostained for deficiencies in
Approach to Patients with Muscle Disorders
683
dystrophin, sarcoglycan, merosin, dysferlin, and caveolin-3, and a Western blot can be performed to look for calpain deficiencies. The diagnoses of myotonic dystrophy, facioscapulohumeral muscular dystrophy, oculopharyngeal dystrophy, and EmeryDreifuss muscular dystrophy usually are clinically obvious but can be confirmed by DNA testing of whole blood. DNA testing is also available for the most common mutations associated with hyperkalemic and hypokalemic periodic paralysis. Certain mitochondrial myopathies can also be confirmed by way of mutational analysis of mitochondrial DNA (mtDNA) in leukocytes (e.g., myoclonic epilepsy with ragged red fiber myopathy; mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke; and neuropathy, ataxia, retinitis pigmentosa syndrome), but in others, DNA analysis of muscle tissue is needed (many of the mtDNA depletion and deletion syndromes). PHARMACOLOGICTESTING The edrophonium (i.e., Tendon) test is useful in diagnosing myasthenia gravis. Edrophonium is an anticholinesterase and results in a transient increase in acetylcholine in the neuromuscular junction and theoretically improves strength. Anticholinergic side effects of edrophonium include bradycardia, nausea, vomiting, increased tearing, and lacrimation. Clinicians should monitor the pulse and blood pressure of patients and be prepared to administer atropine to counteract the anticholinergic effects of edrophonium. To perform the edrophonium test, I place a butterfly needle in an antecubital vein, keeping the catheter open with saline. A 2-mg (0.2-mL) test dose of edrophonium is administered because some patients are extremely sensitive to even low dosages. If there is no improvement after 30 seconds, the remaining 8 mg is administered in small increments (2 mg every 15 seconds). If the patient has an objective improvement or severe side effect, the rest of the injection may be halted. It is most important to assess an objective sign of weakness, not the patient’s subjective response. It is important to evaluate objective measures of improvement. In this regard, the degree of ptosis or improvement in extraocular motility is the most useful sign to follow. The edrophonium test should not be considered positive if the patient states that he or she feels stronger if there is no objective improvement. Unfortunately, the test is not always positive in patients with myasthenia gravis. Furthermore, a modest response to edrophonium may be seen in other disorders such as LEMS, combined or overlap MG and LEMS, U S , congenital myasthenic syndromes, botulism, and GBS. MUSCLE BIOPSIES Many patients with a myopathy should undergo a muscle biopsy for accurate diagnosis. The clinical examination, laboratory workup, and electrophysiologic studies may indicate that the patient has a myopathy but not the specific type of muscle disorder. However, muscle biopsies are not indicated to evaluate patients complaining of muscle pain, weakness, or fatigue without objective signs of a myopathy (e.g., elevated serum CK levels, abnormal EMG, objective weakness on manual muscle testing). Muscle biopsies may be performed through an open (minor surgical procedure) or closed (needle or punch) procedure. Some authorities prefer open muscle biopsy because several large samples can be obtained and processed for routine and electron microscopy, metabolic analysis, and protein analysis (Western blot). Others recommend needle muscle biopsies in which the
684
Spinal Cord and Peripheral Neuromuscular Disease W
Diseases of Muscle
individual sample sizes are small but many more areas of potentially affected muscle tissue can be assessed via smaller incisions. I prefer open biopsy, especially in multifocal processes, such as in inflammatory myopathies and in myopathic disorders for which electron microscopy is needed to confirm a diagnosis. The muscle selected for biopsy should be mildly weak, preferably MRC grade 4.If the muscle is too weak (e.g., MRC grade 3 or less), the tissue typically has end-stage damage, and it is often impossible to distinguish certain myopathic disorders from severe neurogenic atrophy. In patients with little weakness on examination, electromyography can be helpful in selecting the muscle to biopsy. However, it is important to biopsy the contralateral muscle to avoid artifact from needle electromyography. The easiest muscle to biopsy is the biceps brachii, if it is affected. Alternative muscles are the deltoid or quadriceps. The gastrocnemius muscle should be avoided because there can be neurogenic changes related to an asymptomatic radiculopathy, which may make diagnosis of a myopathy difficult. The muscle specimen is routinely analyzed by light and electron microscopy. In addition, biochemical assays for various enzyme deficiencies (e.g., glycogen and lipid storage diseases), Western blot for specific protein abnormalities (e.g., dystrophin), and DNA analysis for genetic mutations (e.g., mitochondria1 myopathies) can be performed on the biopsy specimen. Amyloid deposition can be detected with Congo red or crystal violet staining. Various immune staining techniques are used to diagnose specific muscular dystrophies (e.g., dystrophin staining for Duchenne and Becker muscular dystrophy, merosin staining for congenital muscular dystrophy, sarcoglycan stains for limb girdle muscular dystrophies, emerin stain for Emery-Dreifuss muscular dystrophy). Immune staining is also useful in the early diagnosis and in understanding the pathogenesis of the different inflammatory myopathies and vasculitis (e.g., stains for complement, membrane attack complex, immunoglobulins, human leukocyte antigens, and cell markers). Electron microscopy is used for detailed evaluation of the ultrastructural components of muscle fibers.
SUGGESTED READINGS Amato AA, Barohn RJ: Idiopathic inflammatory myopathies. Neurol Clin 15:615-648, 1997
Barohn RJ: Approach to peripheral neuropathy and neuronopathy. Semin Neurol 18:7-18, 1998 Barohn RJ, Amato AA, Griggs RC Overview of distal myopathies: from the clinical to the molecular. Neuromuscul Disord 8:309-316, 1998
Brooke MH: Clinical evaluation of patients with neuromuscular disease. pp. 1-31. In Schapira AHV, Griggs RC (eds): Muscle Diseases. Butterworth-Heinemann, Boston, 1999 Cherington M: Clinical spectrum of botulism. Muscle Nerve 21:701-710, 1998
Cohn RD, Campbell K P Molecular basis of muscular dystrophies. Muscle Nerve 23:1456-1471, 2000 Drachman DB Myasthenia gravis. N Engl J Med 330:1797-1810, 1994 Dumitru D: Electrodiagnostic Medicine. Hanley & Belfus, Philadelphia, 1995
Griggs RC, Mendell JR, Miller RG: Evaluation and Treatment of Myopathies. FA Davis, Philadelphia, 1995 Gronseth GS, Barohn RJ: Practice parameter: thymectomy of autoimmune myasthenia gravis (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 507-15, 2000 Howard J F Adverse drug effects on neuromuscular transmission. Semin Neurol 10:89-102, 1990 Lennon VA Serologic profile of myasthenia gravis and distinction from the Lambert-Eaton myasthenic syndrome. Neurology 48(Suppl 5): S23-S27, 1997
Maselli RA: Pathophysiology of myasthenia gravis and Lambert-Eaton syndrome. Neurol Clin 12:285-303, 1994 McEvoy KM: Diagnosis and treatment of Lambert-Eaton myasthenic syndrome. Neurol Clin 12:387-399, 1994 Mitchell P, Bebbington M Myasthenia gravis in pregnancy. Obstet Gynecol 80:178-181, 1992 Morel E, Eymard B, Vernet-der Garabedian B et al: Neonatal myasthenia gravis: a new clinical and immunologic appraisal on 30 cases. Neurology 38138-142, 1988 Nations SP, Wolfe GI, Amato AA et al: Distal myasthenia gravis. Neurology 52:632-634, 1999
Pascuzzi RM, Kim YI: Lambert-Eaton syndrome. Semin Neurol 1035-41, 1990
Plauche W C Myasthenia gravis in mothers and their newborns. Clin Obstet Gynecol 3482-99, 1991 Sanders DB, Massey JM, Sanders LL, Edwards LJ: A randomized trial of 3,4-diaminopyridinein Lambert-Eaton myasthenic syndrome. Neurology 54603-607, 2000
Tim RW, Massey JM, Sanders DB: Lambert-Eaton syndrome: electrodiagnostic findings and response to treatment. Neurology 54:2 176-2178, 2000
107 Muscular Dystrophies Basil T. Darras
Muscular dystrophies are genetically determined primary diseases of muscle, characterized pathologically by muscle fiber degeneration. The main symptom and sign of muscular dystrophies is weakness, which is usually progressive. Pathologic, clinical, and genetic criteria have been used as the basis for their classification. Table 107-1 lists the principal forms of muscular dystrophy and their mode of inheritance.
DUCHENNE AND BECKER MUSCULAR DYSTROPHIES (DYSTROPHINOPATHIES) Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD) are progressive myopathies, inherited as X-linked recessive traits. DMD is the most severe form of muscular dystrophy, with an incidence of about 1 in 3300 live male
684
Spinal Cord and Peripheral Neuromuscular Disease W
Diseases of Muscle
individual sample sizes are small but many more areas of potentially affected muscle tissue can be assessed via smaller incisions. I prefer open biopsy, especially in multifocal processes, such as in inflammatory myopathies and in myopathic disorders for which electron microscopy is needed to confirm a diagnosis. The muscle selected for biopsy should be mildly weak, preferably MRC grade 4.If the muscle is too weak (e.g., MRC grade 3 or less), the tissue typically has end-stage damage, and it is often impossible to distinguish certain myopathic disorders from severe neurogenic atrophy. In patients with little weakness on examination, electromyography can be helpful in selecting the muscle to biopsy. However, it is important to biopsy the contralateral muscle to avoid artifact from needle electromyography. The easiest muscle to biopsy is the biceps brachii, if it is affected. Alternative muscles are the deltoid or quadriceps. The gastrocnemius muscle should be avoided because there can be neurogenic changes related to an asymptomatic radiculopathy, which may make diagnosis of a myopathy difficult. The muscle specimen is routinely analyzed by light and electron microscopy. In addition, biochemical assays for various enzyme deficiencies (e.g., glycogen and lipid storage diseases), Western blot for specific protein abnormalities (e.g., dystrophin), and DNA analysis for genetic mutations (e.g., mitochondria1 myopathies) can be performed on the biopsy specimen. Amyloid deposition can be detected with Congo red or crystal violet staining. Various immune staining techniques are used to diagnose specific muscular dystrophies (e.g., dystrophin staining for Duchenne and Becker muscular dystrophy, merosin staining for congenital muscular dystrophy, sarcoglycan stains for limb girdle muscular dystrophies, emerin stain for Emery-Dreifuss muscular dystrophy). Immune staining is also useful in the early diagnosis and in understanding the pathogenesis of the different inflammatory myopathies and vasculitis (e.g., stains for complement, membrane attack complex, immunoglobulins, human leukocyte antigens, and cell markers). Electron microscopy is used for detailed evaluation of the ultrastructural components of muscle fibers.
SUGGESTED READINGS Amato AA, Barohn RJ: Idiopathic inflammatory myopathies. Neurol Clin 15:615-648, 1997
Barohn RJ: Approach to peripheral neuropathy and neuronopathy. Semin Neurol 18:7-18, 1998 Barohn RJ, Amato AA, Griggs RC Overview of distal myopathies: from the clinical to the molecular. Neuromuscul Disord 8:309-316, 1998
Brooke MH: Clinical evaluation of patients with neuromuscular disease. pp. 1-31. In Schapira AHV, Griggs RC (eds): Muscle Diseases. Butterworth-Heinemann, Boston, 1999 Cherington M: Clinical spectrum of botulism. Muscle Nerve 21:701-710, 1998
Cohn RD, Campbell K P Molecular basis of muscular dystrophies. Muscle Nerve 23:1456-1471, 2000 Drachman DB Myasthenia gravis. N Engl J Med 330:1797-1810, 1994 Dumitru D: Electrodiagnostic Medicine. Hanley & Belfus, Philadelphia, 1995
Griggs RC, Mendell JR, Miller RG: Evaluation and Treatment of Myopathies. FA Davis, Philadelphia, 1995 Gronseth GS, Barohn RJ: Practice parameter: thymectomy of autoimmune myasthenia gravis (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 507-15, 2000 Howard J F Adverse drug effects on neuromuscular transmission. Semin Neurol 10:89-102, 1990 Lennon VA Serologic profile of myasthenia gravis and distinction from the Lambert-Eaton myasthenic syndrome. Neurology 48(Suppl 5): S23-S27, 1997
Maselli RA: Pathophysiology of myasthenia gravis and Lambert-Eaton syndrome. Neurol Clin 12:285-303, 1994 McEvoy KM: Diagnosis and treatment of Lambert-Eaton myasthenic syndrome. Neurol Clin 12:387-399, 1994 Mitchell P, Bebbington M Myasthenia gravis in pregnancy. Obstet Gynecol 80:178-181, 1992 Morel E, Eymard B, Vernet-der Garabedian B et al: Neonatal myasthenia gravis: a new clinical and immunologic appraisal on 30 cases. Neurology 38138-142, 1988 Nations SP, Wolfe GI, Amato AA et al: Distal myasthenia gravis. Neurology 52:632-634, 1999
Pascuzzi RM, Kim YI: Lambert-Eaton syndrome. Semin Neurol 1035-41, 1990
Plauche W C Myasthenia gravis in mothers and their newborns. Clin Obstet Gynecol 3482-99, 1991 Sanders DB, Massey JM, Sanders LL, Edwards LJ: A randomized trial of 3,4-diaminopyridinein Lambert-Eaton myasthenic syndrome. Neurology 54603-607, 2000
Tim RW, Massey JM, Sanders DB: Lambert-Eaton syndrome: electrodiagnostic findings and response to treatment. Neurology 54:2 176-2178, 2000
107 Muscular Dystrophies Basil T. Darras
Muscular dystrophies are genetically determined primary diseases of muscle, characterized pathologically by muscle fiber degeneration. The main symptom and sign of muscular dystrophies is weakness, which is usually progressive. Pathologic, clinical, and genetic criteria have been used as the basis for their classification. Table 107-1 lists the principal forms of muscular dystrophy and their mode of inheritance.
DUCHENNE AND BECKER MUSCULAR DYSTROPHIES (DYSTROPHINOPATHIES) Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD) are progressive myopathies, inherited as X-linked recessive traits. DMD is the most severe form of muscular dystrophy, with an incidence of about 1 in 3300 live male
Chapter 107
TISU 107-1. Muscular Dystrophies Form of Dvstrophv
Inheritance
Duchenne Becker Emery-Dreifuss Limb-girdle 2A, 2B. 2C, 2D,. . . Congenital Distal Facioscapulohumeral Limb-girdle lA, lB, l C , lD,. . . Emery-Dreifuss Oculopharyngeal Myotonic Proximal myotonic myopathy Distal
X-linked recessive Autosomal recessive Autosomal dominant
births and a prevalence rate in the total population of about 3 per 100,000. BMD has a similar presentation but a milder clinical course. The incidence of BMD is about 1 in 30,000 male births. In addition, there is an intermediate group of patients with either mild DMD or severe BMD, who are also known as outliers. It is now well known that all three types of muscular dystrophy are allelic, resulting from dystrophin deficiency caused by mutations of a single gene, called the dystrophin gene. Other dystrophinopathies, occurring at a lower incidence, include the following:
Muscular Dystrophies
685
running, jumping, going up steps, and similar activities; an unusual waddling gait, lumbar lordosis, and calf enlargement usually are observed. Muscular weakness selectively affects proximal limb muscles before distal and the lower extremities before the upper. Early on, the patient may complain of leg pains. Jumping and running are almost impossible in most cases, and, in arising from the floor, affected boys use hand support to push themselves to an upright position (Gower’s sign). Neck flexor weakness occurs at all stages of the disease and distinguishes boys with DMD from patients with milder presentations; at least early on, patients with BMD and an intermediate phenotype, or outliers, appear to have preserved neck flexor strength. Cardiac muscle is also affected. Most children with DMD often have varying degrees of nonprogressive impairment of cognitive function, although an occasional child may have average or above-average intelligence. Physical examination shows pseudohypertrophy of the calf muscles (Fig. 107-1) and, in some instances, quadriceps and other muscles, lumbar lordosis, waddling gait, shortening of the Achilles tendons (Fig. 107-2), and hyporeflexia or areflexia. The shortening of the Achilles tendons and equinovarus deformity are related to imbalance between plantar flexors, invertors, and the tibialis anterior muscles; the former muscles remain very strong until late in the course of the disease, while the latter ones weaken gradually. Cranial nerve innervated muscles and sphincters remain essen-
X-linked dilated cardiomyopathy (XLDCM) Isolated quadriceps myopathy Muscle cramps with myoglobinuria Asymptomatic elevation of muscle enzymes Manifesting DMD or BMD carrier females
Clinical Aspects Great heterogeneity in the clinical features and course of the various dystrophinopathies has been observed, creating a spectrum ranging from very mild to very severe presentations. The severe end of the spectrum includes DMD, BMD, and the outliers or intermediate phenotype when skeletal muscle is primarily affected and XLDCM when the heart is the organ primarily affected. Isolated quadriceps myopathy, muscle cramps with myoglobinuria, and asymptomatic elevation of muscle enzymes represent the mild end of the dystrophinopathy spectrum in males. DMD or BMD carrier females can be asymptomatic or can manifest mild to severe symptoms. The main distinction between DMD and BMD is made by the age of wheelchair dependency, which is less than 13 years in DMD and beyond 16 years in BMD. Patients who become wheelchairbound between 13 years and 16 years are classified as outliers or as exhibiting an intermediate phenotype. The mild end of the BMD spectrum has been extended by several investigators to include patients with an increase in serum concentration of creatine kinase (CK) and abnormal dystrophin on muscle biopsy, but with subclinical skeletal muscle involvement. The distinction between BMD and XLDCM is hard to make in these atypical patients when they develop severe cardiomyopathy. Duchenne Muscular Dystrophy. In children with DMD, although there is histologic and laboratory evidence of myopathy from birth, the onset of weakness usually occurs between 2 and 3 years of age; in some cases, it may be delayed and become apparent after the age of 3 years. The child usually has difficulty with
FIG. 107-1. Pseudohypertrophy of the calf muscles in a patient with Duchenne muscular dystrophy. (Courtesy of Theodore Munsat, MD, New England Medical Center, Boston.)
686
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Muscle
FIG. 107-2. A family of five brothers, all with Duchenne muscular dystrophy. Note the calf pseudohypertrophy, scapular winging, and the associated lumbar lordosis, which, combined with the forward pelvic tilt and heel cord tightening, lead to toe-walking or even standing, as seen in the oldest boy. (Courtesy of Danilo A Duenas, MD, Miami Children's Hospital, Miami.)
tially unaffected. Neck flexors are weaker than extensors, biceps and triceps usually are weaker than deltoids, wrist flexors are less involved that extensors, and the quadriceps are involved more than hamstrings. Between 3 and 6 years of age there may be some evidence of improvement, which is gradually followed by relentless deterioration, leading to wheelchair confinement by the age of approximately 13 years. Wheelchair-bound children tend to develop contractures and scoliosis with deterioration of pulmonary function. As a result of evolving cardiomyopathy, 90% of patients with DMD exhibit abnormalities in their electrocardiogram (ECG) (increased R/S amplitude ratio in lead V1, deep Q waves in left [V5, V6] precordial leads). Intra-atrial and atrioventricular and ventricular conduction disturbances also occur. The incidence of cardiomyopathy increases gradually in teenage years, with about one third of patients being affected by age 14 years, one half by age 18 years, and all patients after age 18 years. Echocardiography showed diminished contractility of the myocardium. The majority of patients with DMD remain free of cardiovascular symptoms until late in the disease course, probably because of their inability to exercise, which may mask cardiac symptoms. In the late stages of the disease, congestive heart failure and arrhythmias may develop, especially during intercurrent infections. Intestinal hypomotility, also known as intestinal pseudo-obstruction, is an important and sometimes life-threatening complication in patients with DMD. It seems to be related to smooth muscle degeneration. Most die in their late teens or twenties from respiratory insufficiency or cardiac failure secondary to progressive cardiomyopathy. In some cases, the immediate cause of death is not apparent. Assisted ventilation can prolong a patient's life
expectancy, but the patient will depend on others for activities of daily living. Becker Muscular Dystrophy. In Becker dystrophy the age of onset of symptoms usually is later, between 5 and 15 years or sometimes even in the third or fourth decade or later, and the degree of clinical involvement is milder; cardiac disease and mental retardation are not as common or as severe as in the Duchenne variety. Also, contractures are not as likely to develop in BMD. In addition, in Becker and intermediate types of muscular dystrophy there is relative preservation of neck flexor muscle strength. Patients with BMD typically remain ambulatory beyond the age of 16 years and into adult life; they usually survive beyond 30 years. Mean age at death is in the mid-40s. Nevertheless, the BMD spectrum includes men with onset of symptoms after the age of 40 years who remain ambulatory even into their 60s. The degree of clinical involvement is milder, but the pattern of muscle wasting is similar to the one noted in DMD. Pelvic girdle and thigh muscles are involved first, and calf muscle pseudohypertrophy occurs early in most but not all patients. Tibialis anterior and peroneal muscle groups are less affected. Shoulder girdle weakness develops later after the onset of proximal lower extremity weakness. In a series of 67 patients, lower extremity weakness was noted first at the mean age of 11 years and upper extremity weakness at the mean age of 31 years. Calf muscles, forearm, and hand intrinsics remain strong until the late stage of the disease. Calf pain during or after exercise was reported as a presenting symptom in 25% and as a complaint at some point during the course of the disease in 91% of all patients. Only 2 of the 67 patients presented with myoglobinuria. Thus, muscle pain is very common in patients with BMD, but myoglobinuria occurs
Chapter 107
infrequently. In patients with BMD, facial muscles usually are preserved. Creatine kinase (CK) values usually are highly elevated in Becker dystrophy and therefore cannot be used to differentiate between the two types of dystrophy. Furthermore, the distinction between Becker dystrophy and limb-girdle muscular dystrophy (LGMD) often is hard to make in cases with a negative family history of BMD. However, the calf muscle pseudohypertrophy usually is not as striking in LGMD as it is in DMD and BMD. Manifesting DMD and BMD Carrier Females. Carriers usually are free of symptoms but may have mildly elevated serum CK and usually mild calf hypertrophy. In approximately 8% of the cases, however, they can present with mild myopathy of the limb-girdle type or even DMD or BMD. Cardiac involvement usually is subclinical; however, a recent cross-sectional study demonstrated that 8% of definite DMD carriers had dilated cardiomyopathy, compared with none in BMD carriers. Only 38% of the studied population of carriers had a completely normal heart investigation. The remaining had subclinical ECG or echocardiography abnormalities. Some carriers can even manifest severe cardiac symptoms.
Genetics Dystrophin Gene. The DMD/BMD gene, now known as dystrophin gene, was isolated recently; it is the largest gene yet
Muscular Dystrophies
687
identified in humans, spanning approximately 2.3 Mb at Xp21. The protein product dystrophin has a total molecular weight of 427 kDa and is recognized on Western blots of human skeletal muscle proteins using antidystrophin antibodies. With the use of immunocytochemistry, dystrophin has been localized to the cytoplasmic face of the plasma membrane of muscle fibers. It has also been shown that dystrophin is part of a large, tightly associated glycoprotein complex containing many other proteins (Fig. 107-3). It is believed that in normal cells, the dystrophin stabilizes the glycoprotein complex and protects it from degradation; in the absence of dystrophin, the complex becomes unstable. There is almost always secondary reduction in the amount of proteins of the glycoprotein complex in the muscle tissue of patients with DMD. The loss of associated membrane proteins as a result of dystrophin deficiency may initiate the degenerative changes seen in muscular dystrophy. Dystrophin Gene Mutations. Of the DMD/BMD mutations identified so far, most are deletions, detected with the dystrophin cDNA in approximately 65% of patients with DMD and 85% of patients with BMD. Partial gene duplications have also been reported in a small percentage of patients (about 5%). In the remaining 30% to 35% of patients without detectable deletions or duplications, the molecular lesions represent point mutations or splicing errors. Furthermore, some patients with Duchenne- or Becker-like phenotypes but without a clear-cut X-linked pattern of inheritance have been shown to harbor defects in other genes,
FIG. 107-3. The dystrophin-associated protein complex. Arrows indicate the protein components mutated in various muscular dystrophies. The laminin 1x2-chain gene is mutated in a subtype of congenital muscular dystrophy without structural brain anomalies and the sarcoglycan proteins in patients with sarcoglycanopathies (autosomal recessive LGMDs). BMD, Becker muscular dystrophy; CMD, congenital muscular dystrophy; DMD, Duchenne muscular dystrophy; LGMD, limb-girdle muscular dystrophy. (Courtesy of Dr. Bonnemann and Dr. Kunkel, Children's Hospital, Boston.)
688
Spinal Cord and Peripheral Neuromuxular Disease
rn Diseases of Muscle
some of which encode the dystrophin-associated glycoproteins (e.g., sarcoglycans). Published studies have failed to reveal any apparent correlation between the size of dystrophin gene deletions and the severity and progression of the DMD/BMD phenotype. The molecular basis of DMD and BMD seems to be related to the disruption or preservation of the amino acid reading frame by the deletion mutations. The latter either disrupt or preserve the reading frame in most cases of Duchenne or Becker muscular dystrophy, respectively. Dystrophin. Dystrophin can be detected easily on immunoblots of 100 pg of total muscle protein derived from a small portion of a muscle biopsy by using antidystrophin antibodies. The quantity and quality of dystrophin can be evaluated either visually or by using densitometry. If the 427-kDa dystrophin protein is normal in size and amount, the diagnosis of DMD or BMD can almost be excluded. More than 99% of DMD patients display complete or almost complete absence of dystrophin in skeletal muscle biopsy specimens. Most patients with BMD (about 85%) have dystrophin of abnormal molecular weight, either smaller (80%) or larger (5%), in gene deletion or gene duplication cases, respectively, which often is low in quantity. However, about 15% of patients with BMD have normal-sized protein of low quantity. The test is very specific because patients with neuromuscular diseases other than DMD or BMD have normal dystrophin. Dystrophin immunoblotting can be used to predict the severity of the evolving muscular dystrophy phenotype. It seems that what determines the severity of the disease is the quantity of the dystrophin molecule rather than its size. Patients with DMD have less than 5% of the normal quantity of dystrophin. Patients with dystrophin levels between 5% and 10% of normal, regardless of protein size, seem to develop an intermediate phenotype (mild DMD or severe BMD). Patients with mild to moderate Becker phenotype usually have levels above 20% (Table 107-2). Diagnosis
Until a few years ago, the diagnosis of DMD or BMD was based on myopathic symptoms and signs, highly elevated serum CK values, myopathic changes on electromyography (EMG) and muscle biopsy, and sometimes a positive family history. The cloning of the gene defective in DMD and BMD and the characterization of its protein product, dystrophin, have provided molecular diagnostic tools for accurate diagnosis of this disorder. Serum Muscle Enzymes. Before the age of 5 years, the serum CK levels usually are 10 to 200 times the upper limit of normal, or even higher. Thus, CK values of 10,000 to 50,000 IU/L are not unusual in DMD and BMD. In a child with DMD, during the first 3 years of life, the serum CK concentration is always more than 10
rn TABU 107-2. Quantity and Size of Dystrophin in Dystrophinopathies Clinical Phenotype
Duchenne
Dystrophin Protein Sizea
Normal or abnormal size Intermediate or seNormal or abnormal vere Becker size Mild or moderate Normal size Becker Abnormal size 'Size and quantity measured by Western blot analysis.
Dystrophin Quantity.
0%-5% 5%-20%
20%-50% 20%- 100%
times the upper limit of normal; if it is less than that, the diagnosis should be questioned. CK levels in DMD are elevated even during the first year of life, when the child is asymptomatic, and they peak between the ages of 2 and 3 years. However, the CK concentration tends to decline gradually with advancing age, at a rate of about 20% per year; the decline is related to the progressive elimination of dystrophic muscle fibers, which are the source of the elevated serum CK levels. Serum CK concentration can be markedly elevated in Becker dystrophy, as in DMD, and therefore cannot be used as a way to differentiate between the two types of dystrophy. At age 20, in a series of 52 patients with BMD, the mean serum CK concentration was elevated 35-fold; however, the highest elevation is observed in the first 10 years of life and, as in DMD, it declines with advancing age and disease progression. Electromyography. EMG shows myopathic changes, usually short-duration, low-amplitude polyphasic rapidly recruited potentials, particularly in proximal muscles. Needle examination may also show increased insertional activity with fibrillation potentials. Early on, the nerve conduction studies, including repetitive nerve stimulation, are normal. With disease progression, the compound muscle action potentials decrease in amplitude, the insertional activity diminishes, motor unit potentials become very small with decreased recruitment, and the fibrillation potentials disappear. At the end, the muscle becomes electrically silent. However, it should be noted that patients with classic DMD or BMD do not need electrodiagnostic studies for diagnostic purposes, but in sporadic cases of BMD or symptomatic carrier females with modest creatine phosphokinase (CPK) elevation (less than 1000 IU/L) and proximal muscle weakness, EMG may have to be considered to exclude a neuropathic process (e.g., spinal muscular atrophy [SMAI 1. Muscle Biopsy. The muscle biopsy demonstrates degeneration, regeneration, isolated opaque hypertrophic fibers, and significant replacement of muscle by fat and connective tissue. The degenerating necrotic fibers are recognized on trichrome staining by their green-blue color (instead of the normal deep blue staining) and their glassy or homogenous cytoplasm. Increased variability in muscle fiber size is also observed, with larger than normal fibers in younger patients followed, with progression of the disease, by the appearance of numerous muscle fibers of a smaller-than-normal size. Regenerating fibers are clusters of small fibers with basophilic cytoplasm and vesicular nuclei. Hypercontracted fibers are called opaque or large dark fibers. Their origin is unclear, but they could be produced at the time of the muscle biopsy and be an artifact of tissue removal, perhaps enhanced by the fragility of the plasma membrane. Central nuclei are present in 2% to 4% of the fibers. Type 1 fiber predominance is seen in most patients. Inflammatory cell infiltrates are seen in the perimysium, endomysium, and perivascular spaces and consist mostly of mononuclear cells, especially macrophages. Another striking characteristic is the development of endomysial and perimysial fibrosis with disease progression; in the late stage of the disease only a few muscle fibers remain, separated by large zones of connective tissue and fat. The differences in the microscopic appearance of muscle in DMD and BMD correlate well with the severity of the disease, with fewer necrotic, hypercontracted, and regenerating fibers seen in milder phenotypes. Dystrophin Immunostaining. In muscle biopsies derived from patients with DMD, there is no detectable staining with antidystrophin antibodies, but in patients with BMD, either normal or partial staining of the sarcolemma is observed. In patients with other neuromuscular diseases, there is homogene-
Chapter 107 W
Muscular Dystrophies
689
C
F
I
M
N
FIG. 107-4. lmmunostaining of frozen sections of skeletal muscle biopsies. (D-N) Antidystrophin antibodies using indirect immunofluorescence. (A-C) Hematoxylin and eosin-stained sections corresponding to 0,E, and F, respectively. There is complete absence of immunofluorescence at the sarcolemma in a muscle section from a patient with Duchenne muscular dystrophy (DMD) (C, 0,compared with the homogeneous staining of the plasma membrane in normal muscle (4, 0) and in muscle biopsies from patients with Emery-Dreifuss muscular dystrophy (G), Fukuyama type of congenital muscular dystrophy (H), limb-girdle muscular dystrophy (0,facioscapulohumeral muscular dystrophy (I), myotonic dystrophy (K), and Kugelberg-Welander type of spinal muscular atrophy (L). In a frozen section of muscle from a patient with Becker muscular dystrophy (B), partial staining of the sarcolemma is observed (€). Note the mosaic pattern of immunostaining in muscle biopsies from a symptomatic (M) and an asymptomatic (N) DMD carrier. (Modified from Arahata K et al: Nature 333:861, 1988; Arahata K et al: N Engl J Med 320:138, 1989; Darras BT: J Pediatr 1 17:1, 1990; M courtesy of E. Bonilla, MD, Columbia University, New York)
ous staining of the plasma membrane (Fig. 107-4).The test appears useful in identifymg sporadic cases of symptomatic females with high CK or clinical weakness, or asymptomatic female DMD carriers in families without a male proband or in families with no detectable deletion or duplication and uninformative linkage analysis results. Symptomatic and asymptomatic DMD carriers with elevated CK values may exhibit a characteristic mosaic pattern of dystrophin immunostaining (Fig. 107-4). However, a negative (normal) result does not exclude carrier status because of the possibility of nonrandom X chromosome inactivation, and also the possible selective loss of dystrophinnegative fibers. The dystrophin immunostaining and X chromosome inactivation tests are not commercially available at this point, but they can be performed in selected clinical or research laboratories.
Algorithm for the Diagnosis of DMD and BMD The precise diagnostic approach in a male child or adult with markedly elevated CK values and evidence of myopathy on physical examination is shown in Figure 107-5. Sporadic Cases. In sporadic cases (i.e., family history negative for DMD and BMD), the clinical presentation can be clear, highly suggestive of DMD or BMD, or not, depending on the clinical features and the age of the child. In both cases, the first step in molecular diagnosis is DNA testing for a dystrophin gene mutation, by multiplex polymerase chair reaction (PCR) or Southern blot assay (Fig. 107-5).If a deletion or duplication is found by PCR or Southern blot assay, its reading frame status allows prediction of the phenotype (DMD or BMD) in most instances. Because of the rare occurrence of exceptions to the
Spinal Cord and Peripheral Neuromuscular Disease rn Diseases of Muscle
690
Male child or adult Highly elevated CK levels or clinical myopathy
Clinical expression clear and negative family history (sporadic case)
Clinical expression not clear and negative family history
Positive family history based on clinical diagnosis only (familial case)
I
DNA deletion test using multiplex PCR assay and/or Southern blot assay
I
I
DNA deletion test using multiplex PCR assay and/or Southern blot assay
I I
No deletiin detected
Deletion or duplication
In-frame
Out-of-frame
Muscle biopsy (optional) Deficient
Western blot assay immunostains
I‘ Family testing via linkagehaplotype
deletion analysis Decreased amount andor altered size
Western blot assay for dystrophin for prognostic confirmation (optional)
muscular
dystrophy
FIG. 107-5. Algorithm for the laboratory diagnosis of sporadic and familial cases of DMD and BMD and for family testing (carrier detection and prenatal or presymptomatic diagnosis). (Modified from Darras BT: Duchenne/Becker muscular dystrophy. Scientific American Medicine, Vol. 3 [Neurology] pp. 1-9, Scientific American, 1993.)
“in-frame/out-of-frame” rule, the clinician has the option of a muscle biopsy, which can be performed to assess the quantity and size of dystrophin and thereby more precisely predict the severity of the disease. Familial Cases. In cases with a positive family history of typical DMD or BMD (i.e., familial cases), molecular diagnosis may not be necessary if the clinical diagnosis has been confirmed in another affected family member by analysis of the dystrophin protein or DNA. In such familial cases, the clinical course in the older affected relative adequately, although not always, predicts the severity of the evolving muscular dystrophy phenotype in other family members. However, it should be remembered that extragenic factors may modify the clinical progression of DMD and BMD, even among members of the same family with the same mutation. If the diagnosis is DMD or BMD has been made clinically in other family members but has not been confirmed previously by analysis of dystrophin or DNA, the PCR-based DNA deletion test should be attempted first because it is less invasive than a muscle biopsy. If a mutation is found, muscle biopsy becomes unnecessary because, as explained earlier, except for rare exceptions the clinical
course is most likely to be the same as in other affected family members (Fig. 107-5). Females with Dystrophinopathy. Female patients can have an early-onset, progressive muscular dystrophy and therefore be symptomatic if they have 45X, 46XY, or Turner mosaic karyotypes; apparently balanced X/autosome translocations with breakpoints in Xp21, within the dystrophin gene, and preferential inactivation of the normal X and a normal karyotype but nonrandom X chromosome inactivation leading to diminished expression of the normal dystrophin allele. Therefore, chromosomal analysis is indicated in all symptomatic females, especially the ones with highly elevated serum CK .levels, following the exclusion of other neuromuscular diseases (e.g., polymyositis, SMA) by EMG or muscle biopsy. Further study with a dystrophin assay or a DNA deletion test may be diagnostic in a symptomatic female, especially in cases with 45X, 46XY, or Turner mosaic karyotypes. Treatment
Therapeutic interventions in DMD and BMD are aimed at maintaining function, preventing contractures, and providing
Chapter 107 W
psychological support. Passive stretching exercises to prevent contractures of the iliotibial band, the Achilles tendons, and flexors of the hip are the mainstays of physical therapy. Lightweight plastic ankle-foot orthoses (AFOs) should be applied if the foot remains in plantar flexion during sleep. Standing or walking can be maintained by using long-leg braces. Surgery can be performed to release contractures of the hip flexors, iliotibial bands, and Achilles tendons. Standing and ambulation seem to prevent scoliosis. After age 12, pulmonary function studies, ECG, and chest radiographs should be performed yearly to monitor the pulmonary and cardiac functions. Overnight mouth intermittent positive pressure can be used to treat symptomatic nocturnal hypoventilation, and respiratory assistance may be used during periods of respiratory infection. Clinical studies provide evidence that prednisone improves the strength and function of patients with DMD. This improvement begins within 10 days, with a single dose of 0.75 mg/kg/day of prednisone for maximal improvement, and reaches a plateau after 3 months. Observed side effects include weight gain, hypertension, behavioral changes, growth retardation, and cataracts. Prednisone may be recommended for selected ambulatory patients over age 5 and continued if the side effects are not severe. Immunosuppression with azathioprine does not have a beneficial effect. Cyclosporin has been reported to improve clinical function in children with DMD who received the medication for 8 weeks. However, because of the rare reports of cyclosporininduced myopathy in patients receiving the medication for other reasons, the use of cyclosporin in DMD remains controversial. Oxandrolone, an anabolic (androgenic) steroid, has been shown in a pilot study to be beneficial in DMD, but a randomized, prospective trial did not show a significant benefit; although there was a difference in strength on some measures, the efficacy was not of a magnitude to justify its use. Aminoglycoside treatment of cultured cells can suppress stop codons in vitro and also in the ma'x mouse. Myoblast transfer has been attempted recently in humans, but the results, so far, have not been encouraging. Stem cell transplantation, aminoglycoside therapy, and other experimental gene therapies are under evaluation. EMERY-DREIFUSS MUSCULAR DYSTROPHY
Emery-Dreifuss muscular dystrophy (EDMD) is an X-linked recessive (chromosome Xq28), autosomal dominant, or autosomal recessive condition (chromosome 1q21) with onset in late childhood or adult life. Mutations in the emerin (Xq28) and lamin A/C genes (lq21) are responsible for the EDMD form of muscular dystrophy. The muscle weakness and wasting in EDMD have a humeroperoneal distribution, often starting in the arms, with weakness of both the biceps and triceps and relative preservation of the deltoid muscles. Later on, distal leg weakness with atrophy of the peroneal muscles is noted. In some cases mild facial weakness may be observed as well. The myopathy tends to be slowly progressive. Contractures at the elbows are noted early, often associated with toe-walking as the first manifestations of the disease. Contractures of the posterior aspect of the neck, lower spine, and Achilles tendons also occur. Cardiac involvement is common and consists of a cardiomyopathy, with atrioventricular (AV) block and often atrial paralysis. The ECG may show varying degrees of AV block, small T waves, and atrial arrhythmias. The cardiomyopathy may lead to sudden death in approximately 50% of the affected patients, usually early in adult life.
Muscular Dystrophies
691
Laboratory studies show modest elevation of CK, which is rarely above a few hundred units per liter. Although the EMG usually displays myopathic features, it may also reveal evidence of denervation. The muscle biopsy usually shows mild myopathic changes with internal nuclei, variation in fiber size, focal connective tissue proliferation, and occasional necrotic fibers. In the X-linked variety of EDMD, DNA testing for emerin gene mutations is now available. Recently, DNA testing for the lamin A/C gene mutations has become commercially available also. Therefore, at this point, the value of muscle biopsy in EDMD is limited if the mutation analysis is positive for an emerin or lamin A/C mutation; however, a muscle biopsy can provide further evidence for the diagnosis of X-linked EDMD by demonstrating via immunohistochemistry absence of nuclear immunostaining for emerin. Furthermore, a muscle biopsy may confirm the myopathic nature of the process in atypical, sporadic cases or in rare cases without detectable mutations. The differential diagnosis includes the rigid spine syndrome, which, in addition to the elbow and ankle contractures, usually is associated with very limited flexion of the spine and mild and slowly progressive myopathy. However, cardiomyopathy has not been observed. Because the cardiac involvement in EDMD is potentially fatal, the cardiac status of the patient should be investigated even if he or she is asymptomatic. Installation of a cardiac pacemaker may be life-saving in patients with evidence of AV block. Holter monitoring should be considered in patients with normal electrocardiograms.
MYOTONIC DYSTROPHY Clinical Aspects
Myotonic dystrophy (DM) is the most common form of muscular dystrophy among Caucasians, with a prevalence estimated at 3 to 5 per 100,000 population and an incidence of 1 in 8000. DM is a multisystem disorder, transmitted by autosomal dominant inheritance, with variable penetrance. In the classic form, DM has its onset in adolescence or adulthood, but a neonatal form also occurs. The main clinical features of DM are myotonia (delayed muscle relaxation after contraction), weakness, and wasting affecting facial muscles and distal limb muscles, frontal balding (in males), cataracts, cardiomyopathy with conduction defects, multiple endocrinopathies, and low intelligence or dementia. The face is long, with wasting of the masseter and temporal muscles; there is also variable ptosis and facial diplegia (Fig. 107-6). The neck is thin because of wasting of the sternocleidomastoids. There may be associated dysarthria, swallowing difficulties, and mild external ophthalmoplegia. Myotonia can be an early symptom, demonstrated by percussion of muscles, usually of the thenar eminence, and by the difficulty of releasing the grasp. Later in the course of the disease, the progressive muscle weakness and wasting become the predominant features, leading to severe distal weakness in the hands and feet. Endocrinopathies include hyperinsulinism, rarely diabetes, adrenal atrophy, infertility in women, testicular atrophy, and growth hormone secretion disturbances. Smooth and cardiac muscle involvement usually are expressed by disturbed gastrointestinal mobility and cardiac conduction defects. The congenital form of the disease occurs in children born to mothers with myotonic dystrophy and presents with profound hypotonia at birth, associated with facial diplegia, feeding and respiratory difficulties, and skeletal deformities, such as clubfeet.
692
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Muscle
FIG. 107-6. Congenital myotonic dystrophy. Note the facial diplegia, ptosis, temporal and masseter muscle wasting, and characteristic appearance of the mouth (like an inverted V). (Courtesy of N. Paul Rosman, MD, New England Medical Center, Boston.)
Later, during childhood, delayed developmental progression is noted. A genetically distinct form of DM with remarkable clinical similarity to classic DM but no chromosome 19 CTG repeat expansion has been mapped to chromosome 3q (DM2). Until recently, the diagnosis of myotonic dystrophy was based on clinical features, family history, EMG, and muscle biopsy findings. EMG demonstrates myopathic potentials and myotonia. Muscle histology may reveal internal nuclei, type I fiber atrophy, and ring fibers. However, the diagnosis could not be confirmed easily in many cases, especially mildly affected ones. The recent identification of the myotonic dystrophy mutation has provided molecular diagnostic tests for almost 100% accurate diagnosis of this disorder in both symptomatic and asymptomatic patients. Genetic Diagnosis
The DM locus was mapped by linkage analysis to chromosome 19q13.3; this genetic localization finally led to the recent identification of the genetic defect in DM, which is thought to be an amplified trinucleotide CTG repeat, located in the 3’ untranslated region of a gene, which putatively encodes a serine-threonine protein kinase (myotonin-protein kinase [DMK]). Although this CTG repeat is polymorphic, it is stable in normal subjects. In contrast, the CTG repeat in DM chromosomes is unstable and can become significantly enlarged. In normal subjects, the two alleles contain 5 to 50 copies of the CTG repeat. However, normal subjects with 38 to 49 copies of the repeat are classified in a borderline category because of the small possibility of expansion of the CTG repeat in their offspring or family members. Mildly affected patients or asymptomatic premutation carriers have 50 to 99 CTG repeats, whereas severely affected subjects have 100 to 2000 or more copies (full mutation) (Table 107-3). To date, a large
number of affected patients have been assessed by both Southern blot and PCR, and an increase in CTG copy number has been documented in more than 99% of subjects. Amplification of the CTG repeat has been proposed to be the molecular mechanism for genetic anticipation, which is the increasing severity of the disease phenotype in successive generations; in DM families, the CTG copy number increases during successive generations. A positive correlation has been observed between increased number of CTG repeats and earlier age of disease onset. Conversely, in a few families, reduction in size of the trinucleotide repeat mutation has been observed during transmission, with a decrease in disease severity. However, it is not possible to predict the age of onset of the disease in a particular patient on the basis of the CTG copy number. For a given number of repeats (greater than loo), a wide range in disease severity may be observed. Nonetheless, infants with severe congenital DM, as well as their mothers, are shown to have on average a greater amplification of the CTG repeat. The greater the CTG repeat expansion in the mother, the higher the probability of a DM offspring being affected with the congenital form of the illness. Unfortunately, these new developments do not explain the exclusive maternal inheritance in cases of congenital DM. Genomic imprinting and the presence of a maternal intrauterine factor have been proposed as two possible mechanisms. The amplification is detectable by Southern blotting, in most cases using DNA extracted from peripheral blood leucocytes. However, this type of analysis may fail to detect expansions where the CTG copy number is less than 150; in some of these patients, who usually are mildly affected, analysis by PCR is important. Conversely, some very large expansions may fail to amplify by PCR. Therefore, both techniques must be used in the molecular diagnosis of DM. Treatment
DM treatment is symptomatic. As patients develop distal weakness, braces for foot drop usually are helpful. The myotonia often responds to medications that stabilize membranes, such as phenytoin, gabapentin, carbamazepine, quinidine, procainamide, mexiletine, and acetazolamide. Theoretically, however, procainamide and quinine prolong the conduction intervals, which are already abnormally prolonged in many patients with DM. Mexiletine is a far better option than phenytoin, carbamazepine, gabapentin, quinine, and procainamide, and it is usually effective in a dosage ranging from 75 to 200 mg two to three times daily. Its main side effects are gastrointestinal, which improve when the drug is taken with food. Tocainide is as effective as mexiletine, but it may suppress the bone marrow. However, because these patients are troubled primarily by the weakness and less by the myotonia, they may benefit more from mechanical devices such as ankle supports than from membrane stabilizers. PROXIMAL MYOTONIC MYOPATHY
In the last 10 years, a subgroup of families with myotonia, weakness, and cataracts but with other features atypical for DM were identified because they had no abnormal expansion of the CTG repeat in the DM gene on chromosome 19. The description of these families and their lack of linkage to the classic DM locus led to the recognition of proximal myotonic myopathy (PROMM) as a clinically and genetically distinct condition. The core features of PROMM are autosomal dominant
Chapter 107 W
Muscular Dystrophies
693
TABLE107-3. CTC Repeat Expansion in Myotonic Dystrophy Category
Normal
Borderline Normal
Permutation Carriers
Full Mutation
Number of repeats Clinical DhenoWDe
5-37 Normal
38-49 Normal
50-99 Mildlv svmDtomatic or no svmDtoms
More than 100 Svmptornatic
inheritance in at least two generations, absence of CTG repeat expansion on chromosome 19, predominantly proximal weakness, cataracts identified by slit lamp examination, and electromyographic myotonia. Additional supportive features include myalgias and painful muscle cramps, fluctuating weakness and stiffness, calf pseudohypertrophy, diabetes mellitus or insulin resistance, hypothyroidism, cataracts, cardiac conduction defects, deafness, and gastrointestinal symptoms. Hypersomnia and significant cognitive delay or brain atrophy on magnetic resonance imaging are not features of PROMM. Also, a congenital form of PROMM does not occur; most patients have onset of symptoms in their 30s or 40s. Furthermore, the occurrence of genetic anticipation has not been documented. The diagnosis is primarily clinical and supported by the absence of CTG expansion or genetic linkage to the DM gene on chromosome 19. CK levels usually are elevated 2- to 10-fold, but normal levels may be seen in a number of patients. In addition to classic DM, the differential diagnosis includes other myotonic disorders, inflammatory myopathies, neuromuscular transmission defects, and mitochondrial disease. Because of the less severe involvement of cardiac and respiratory muscle function, the prognosis usually is better in patients with PROMM. No specific therapy exists for PROMM, but careful monitoring of cardiac status is indicated. LIMB-GIRDLE MUSCULAR DYSTROPHIES LGMD was first described by Erb in 1884. The term limb-girdle dystrophy embraces a number of conditions with heterogenous causes; a European Neuromuscular Center (ENMC) meeting in 1995 defined LGMD as a muscular dystrophy with predominantly proximal distribution of weakness that, early in the course of the disease, spares distal muscles as well as facial and extraocular muscles. Most cases are inherited in an autosomal recessive fashion and, as is to be expected, are sporadic. However, families with an autosomal dominant pattern of inheritance have been described as well. The age of onset of LGMD varies from early childhood to adulthood, but typically the onset is not congenital. In some cases, weakness may be noted early, leading to significant disability during childhood; in other cases the weakness may not be apparent until early in adult life. With the exception of a few cases with rapid progression, the course usually is slowly progressive. The weakness affect the shoulder girdle (scapulohumeral type) or the pelvic girdle (pelvifemoral type). Most childhood-onset cases have a pelvifemoral distribution of weakness. In many adult patients, the disease involves both shoulder and pelvic girdles with gradually increasing proximal limb weakness leading to restriction of mobility and eventually to wheelchair confinement. Neck flexor and extensor muscles may be involved concomitantly. Facial weakness usually is mild and, in some cases, totally absent. Even in mild cases, there is preferential weakness and atrophy of the biceps muscle. Low back pain may be a prominent symptom in patients with LGMD. Intellect usually is normal, and cardiac or other systemic involvement is not as common as in dystrophinopathies.
TABU1074. Limb-Girdle Muscular Dystrophies Type
Gene Location
Protein
LCMD-1A LCMD-1 B LCMD-1 C LCMD-1D LCMD-1E LCMD-2A LCMD-2B LCMD-2C LCMD-2D LCMD-2E LCMD-2F LCMD-2C LCMD-2H LCMD-21
5q22-q31 lqll-q21 3p25 6q23 7q 15ql5-q21 2p13 13q12 17q12-q21 4q12 5q33-q34 17qll-ql2 9q31-q34.1 19q13.3
Myotilin Lamin A/C Caveolin-3 ? ? Calpain-3 Dysferlin YSarcoglycan a-Sarcoglycan p-Sarcoglycan GSarcoglycan Telethonin
? ?
Inheritance
AD AD AD AD AD AR AR AR AR AR AR AR AR AR
Abbreviations:AD, autosomal dominant; AR, autosomal recessive; LGMD, limb-girdle
muscular dystrophy.
The discovery of the genetically distinct subtypes of LGMD has led to nomenclature designating autosomal dominant LGMD as LGMD- lA, lB, lC, and so forth and autosomal recessive LGMD as LGMD-2A, 2B, 2C, and so forth. The current status of this classification is shown in Table 107-4. Mutations within the same gene may result in different phenotypes, sometimes not consistent with the strict definition of LGMD; for example, LGMD-2B and Miyoshi distal myopathy are caused by dysferlin gene mutations, whereas mutations in the gene encoding lamin A/C may result in the phenotypes of autosomal dominant Emery-Dreifuss muscular dystrophy, LGMD-lB, or cardiomyopathy with conduction system disease. Sarcoglycanopathies are early-onset autosomal recessive LGMDs caused by mutations in a-,p-, y-, and 6-sarcoglycans, which are members of the dystrophin-associated glycoprotein complex (Fig. 107-3). The pattern of weakness in sarcoglycanopathies is reminiscent of DMD and BMD, including the calf hypertrophy, but cognitive function is preserved. In calpain deficiency (calpainopathy) the pattern is more atrophic, with significant involvement of the periscapular muscles, biceps, gluteus maximus, adductors, and hamstrings. The early weakness and atrophy of the gastrocnemius with inability to walk on the toes and high CK are very supportive of dysferlinopathy, and an early foot drop may indicate a telethoninopathy. Cardiac involvement is common in LGMD-1B (laminopathy) and LGMD-1D and unusual in LGMD- 1A (myotilinopathy), LGMD- 1C (caveolinopathy), and LGMD-1E. Cardiomyopathy may occur in a subset of patients with sarcoglycanopathy. CK is usually modestly elevated but can be very high in sarcoglycanopathies, dysferlinopathy, and caveolinopathy. EMG shows myopathic changes with small polyphasic potentials; a muscle biopsy reveals dystrophic changes with degeneration and regeneration of muscle fibers, fiber splitting, internal nuclei, fibrosis, moth-eaten, and whorled fibers. Most autosomal recessive LGMDs have earlier onset, rapid progression, and high CK values. If the CK is more than 1000 IUlL in a patient with a myopathic LGMD-like phenotype, thereby making other nonmyopathic motor unit disorders (e.g., SMA) less
694
Spinal Cord and Peripheral Neuromuscular Disease
likely, one should proceed to a dystrophin DNA test; given that this test is positive in 65% to 80% but not all DMD and BMD cases, a dystrophinopathy is not excluded by a negative result. The next appropriate diagnostic procedure is a muscle biopsy; immunohistochemistry with antibodies against a - , p-, y-, and 6-sarcoglycans, dystrophin, dystroglycans, and merosin may offer a means for a specific biopsy diagnosis (e.g., a-sarcoglycanopathy) but not always. If the biopsy suggests a myopathic process but DNA testing and immunohistochemistry for all of the above-mentioned proteins is normal, myotilin, calpain-3 (LGMD-2A), dysferlin (LGMD-2B), and telethonin (LGMD-2G) testing may need to be pursued in selected research laboratories. The patients with autosomal dominant LGMD usually have a later age at onset and a more ingravescent clinical progression. The CK values in these patients may not be as grossly elevated. However, in LGMD- 1C, related to caveolin mutations, CK values are elevated 4- to 25-fold, and the clinical onset of this form of LGMD may begin in childhood; if clinically suspected, DNA testing for caveolin mutations is currently available only in research laboratories. Some sporadic dominant cases, and even autosomal recessive ones with modest CK elevation, may be clinically indistinguishable from SMA type 111, the KugelbergWelander form of SMA. Because SMA type I11 may also have a modest CK elevation (less than 1000 IU/L), in this setting an EMG is particularly useful for differentiating a neurogenic from a myopathic process and thus deciding to proceed with DNA testing for possible SMA or a muscle biopsy for a potential myopathy. Treatment is supportive and is aimed at preventing contractures because substantial disability may result from them. Therefore, a passive stretching physical therapy program must be instituted early. Later in the course of the disease, cardiorespiratory monitoring is indicated.
Diseases of Muscle
FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY
Facioscapulohumeral (FSH) dystrophy was first described by Duchenne (1872) and, subsequently, by Landouzy and Dejerine (1884). The classic form of FSH dystrophy is inherited in an autosomal dominant fashion and has been mapped to chromosome 4q35. Although FSH dystrophy usually is slowly progressive, it can be extremely variable in its severity and even the age of onset. The infantile variety of FSH dystrophy has a very early onset (usually within the first few years of life) and is rapidly progressive, with wheelchair confinement by the age of 9 or 10 years in most cases. There is profound facial weakness, inability to close the eyes in sleep, and inability to smile and to show any evidence of facial expression. The weakness rapidly involves the shoulder and hip girdles with lumbar lordosis, pronounced forward pelvic tilt, and hyperextension of the knees and the head upon walking. Marked weakness of the wrist extensors may result in a wrist drop. The infantile variety of FSH dystrophy often is sporadic. In the classic form of FSH dystrophy, the onset usually is in the second or third decade and the progression is slow, with almost normal lifespan. The facial muscles are involved initially with inability to close the eyes tightly, smile, or whistle; a pouting appearance of the lips, smooth face, and mild dimpling in the areas lateral to the angles of the mouth are characteristic (Fig. 107-7A and B ) . However, the facial weakness can be mild early on and may remain mild for many years. The muscles of the shoulders and upper arms are also involved with marked atrophy of the biceps and triceps, but relative preservation of the deltoid muscles (Fig. 107-7C). There is significant scapular winging (Fig. 107-8) and characteristic appearance of the shoulders with bulging of the trapezii muscles (Fig. 107-7A), riding of the scapulae upward and over the lateral parts of the thorax, and forward jutting of the medial ends of the clavicles when the arms are
CD
ICB
FIG. 107-7. Facioscapulohumeral muscular dystrophy. (A) Horizontal and widened appearance of the mouth, with vertical dimpling on either side of the mouth; the rest of the face is unlined. (B) Pouting appearance of the lips, when viewed from the side. (C) Atrophy of the arm caused by wasting of the biceps and triceps. The deltoid and muscles of the forearm are preserved ("Popeye" arm). (0)Hypertrophy of the extensor digitorum brevis muscle, in spite of marked foot drop, seen as bulging on the lateral aspect of the foot. (Adapted from Book M: A Clinician's View of Neuromuscular Disease. Williams & Wilkins, Baltimore, 1986, with permission.)
Chapter 107
rn Muscular Dystrophies
695
weakness may show some improvement by surgical fixation of the scapulae. Because loss of scapular fixation may recur after surgery, it would be advisable to recommend surgery on one side and, if successful, to consider fixation of the other side later. Wrist and ankle supports may be useful also. Despite the pronounced inflammatory response in muscle biopsies, therapy with corticosteroids is not advocated.
OCULOPHARYNGEAL MUSCULAR DYSTROPHY
FIG. 107-8. Facioscapulohumeral muscular dystrophy. Profound scapular winging with rising of the scapulae upward and laterally. (Courtesy of N. Paul Rosman, MD, New England Medical Center, Boston.)
abducted. Distal muscles of the upper extremities usually are spared, but a foot drop may occur (scapuloperoneal variety). Inspection of the extensor digitorum brevis (EDB) muscle is helpful in diagnosing FSH because it is usually hypertrophic in FSH (Fig. 107-70); atrophy of the EDB muscle is common in peripheral motor neuropathies. In a number of cases, the disease progresses rapidly in middle age, leading to significant disability. Exudative telangiectasia of the retina with an associated sensorineural hearing loss (Coats’s syndrome) has been described to occur in some cases of FSH dystrophy. The EMG displays myopathic features; the muscle biopsy shows variability in fiber size, with a lot of large hypertrophic fibers, a few angulated atrophic fibers, and often a significant inflammatory response. Histologic differentiation from polymyositis is based on the fact that hypertrophy of the muscle fibers is not seen in the latter. CK is only mildly elevated and is rarely elevated in patients presymptomatically. A commercial DNA test is now available for FSH muscular dystrophy; most patients with classic FSH for whom detailed molecular studies have been done carry a chromosomal rearrangement within the subtelomere of chromosome 4q (4635). A tandem array of 3.3-kb repeated DNA elements (D4Z4) is deleted in patients with FSH. In the general population, the number of repeat units varies from 10 to more than 100; in patients with FSH, an allele of 1 to 10 residual units is observed because of the deletion of an integral number of these units. This new diagnostic test is positive in 95% to 98% of typical FSH cases. Nonetheless, the exact gene defect is not known yet, so the sensitivity of the genetic test for atypical cases remains uncertain. In typical cases, we see no value in performing a muscle biopsy. Treatment of FSH is primarily supportive. The eyes must be checked for evidence of telangiectasia, which is usually treatable with photocoagulation of the abnormal vessels. Because the deltoid muscles usually are preserved, patients with significant
Oculopharyngeal muscular dystrophy (OPMD) is a rare myopathy characterized by ocular and pharyngeal muscle involvement. It presents with ptosis, dysarthria, and dysphagia, but it can also be associated with proximal and distal extremity weakness. The onset usually is in middle age, with usually asymmetrical involvement of the levator palpebrae muscles first and progressive extraocular weakness. It is a slowly progressive myopathy, and although ptosis can occlude vision, severe dysphagia can sometimes lead to weight loss and death if not treated. OPMD is distinguished from FSH muscular dystrophy by the fact that the extraocular weakness in OPMD is far more severe; it is also distinguished by the distribution of weakness. OPMD can also be confused with myotonic dystrophy, but myotonia is absent in OPMD; ocular muscle involvement is rarely severe in early myotonic dystrophy. The differentiation from a mitochondrial myopathy might pose a problem. However, the associated features of retinitis pigmentosa, ataxia, elevated cerebrospinal fluid protein, cardiac conduction defects, and developmental delay often seen in mitochondrial myopathies help in the differentiation. Muscle biopsy shows variation of fiber size and rimmed vacuoles. CK levels may be elevated. In a small number of patients, cricopharyngeal myotomy has been attempted with improvement of the dysphagia. OPMD is an autosomal dominant myopathy with complete penetrance and a high incidence in the Canadian province of Quebec, where it is estimated at 1 in 8000 people. The frequency of OPMD in France is lower, at 1 in 200,000 people. It appears that a single founder chromosome is responsible for OPMD in the French Canadian population. OPMD has been linked to chromosome 14ql1, and a GCG repeat expansion has been shown in the PABP2 gene (poly-A binding protein 2). Ninety-eight percent of control French Canadian chromosomes had 6 GCG repeats, and 2% had 7 repeats. In OPMD, the expanded alleles range from 8 to 13 repeats. The OPMD repeat is short, with small and stable expansions. The PABP2 protein has been localized to the nucleus, where it seems to be involved in mRNA polyadenylation.
DISTAL MUSCULAR DYSTROPHY Distal myopathies are a heterogeneous group of myopathies characterized by weakness starting distally but gradually progressing to proximal muscles as well. Almost all forms of distal myopathy can present as early as the second decade, but the onset is usually between 40 and 60 years. Their current clinical and genetic classification is shown in Table 107-5.
CONGENITAL MUSCULAR DYSTROPHY This term has been applied to infants who are hypotonic and weak at birth and in whom muscle biopsies show changes consistent with muscular dystrophy. Arthrogryposis is commonly seen in the newborn period. The Fukuyama type of congenital muscular
696
Spinal Cord and Peripheral Neuromuscular Disease
Diseases of Muscle
TABLE107-5. Distal Muscular Dystrophies Tvpe
Inheritance
Initial Weakness
CK
Biopsy
Locus/Cene
Miyoshi: early adult onset type II (LGMD 28')
Autosomal recessive or sporadic
Legs: posterior compartment
Increased 10-1 50x normal
2p13 dysferlin
Nonaka: early adult onset pe I familial IBM ) Laing: early adult onset type 111
Autosomal recessive or sporadic
Legs: anterior compartment
Autosomal dominant Autosomal dominant
Moderate myopathic changes, no vacuoles Myopathic; vacuoles in some cases Vacuolar myopathy
14q
Welander: late adult tVpe I Markesbery-Griggs/ Udd: late adult onset type II
Legs: anterior compartment Neck flexors Hands: fingers and wrist extensors Legs: anterior compartment
Slightly to moderately elevated, usually OH-
+ OH + Fe3+
The discovery of the neurotoxin MPTP ( 1-methyl-4-phenyl1,2,3,6-tetrahydropyidine) has also shed light on the pathogenesis of PD in addition to providing a useful animal model for research studies. MPTP selectively destroys the substantia nigra, producing parkinsonism in humans and animals. This toxin is converted to MPP+ (1-methyl-4-phenylpyridiniumion) by MAO-B and exerts its effect via this active metabolite. MPP+ is taken up by mitochondria and inhibits both complex I and a-ketoglutarate dehydrogenase. Complex I inhibition results in increased free radical generation from the respiratory chain and therefore can contribute further to oxidative damage. In addition, MPP+ may also generate free radicals directly. The role of a complex I defect in the pathogenesis of PD is further supported by the observation in postmortem studies of a 30% to 40% decrease in complex I activity and immunostaining in the SNc of patients with PD. In addition, reduced complex I activity has been reported in platelets and muscle of patients with PD. Mitochondria1 dysfunction induced by MPP+ has also been shown to play a role in apoptosis, the proposed major cause of cell death in PD. PROPOSED NEUROPROTECTIVE AGENTS Monoamine Oxidase Inhibitors Because of the role of MA0 in both the oxidation of dopamine to hydrogen peroxide and the conversion of MPTP to MPP+, neuroprotective strategies have focused much attention on inhibitors of this enzyme. The main agent studied has been the selective h4AO-B inhibitor selegiline. It has a half-life of 2 hours but its metabolites, L-amphetamine and L-methamphetamine, have halflives of 17.7 and 29.5 hours, respectively. Inhibition of MAO-B by drugs such as selegiline prevents the formation of MPP+ and the development of experimental parkinsonism in animal models. In vivo studies have shown that selegiline can protect against free radical formation induced by dopamine turnover, MPP+, and a variety of other toxins. In addition, selegiline has been found to have potential neuroprotectiveproperties that are separate from its MAO-B inhibitory effect. Selegiline administration has been shown to increase levels of a variety of protective antioxidant molecules including superoxide dismutase, catalase, GSH, and glutathione peroxidase. Selegiline has been also shown to augment the release of trophic factors and antiapoptotic molecules such as bcl-2. Initial evidence reported by Knoll in rodents and a retrospective study by Birkmayer in patients with PD suggested that selegiline therapy may result in longer survival and less disability. This prompted several prospective, double-blind, placebocontrolled studies. The largest study, DATATOP, investigated both selegiline and a-tocopherol (vitamin E) in 800 untreated patients with PD. In this study, a symptomatic benefit confounded the results of a potential neuroprotective effect. However, subgroup analysis suggested that a symptomatic benefit was not enough to explain the delayed progression, and there may have also been a neuroprotective component that delayed the need for levodopa in the selegiline-treated group. After the initial 2-year double-blind DATATOP trial was
completed, open-label extension studies offered selegiline treatment to all patients regardless of whether they had reached the endpoint of needing levodopa therapy. These extension phases did not support a neuroprotective effect of selegiline treatment. In 1993, a second randomization was undertaken in the DATATOP patients who had needed levodopa. Independentlyof their original assignment, subjects were randomized to continue selegiline or to switch to placebo. Preliminary analyses suggest that selegiline increases the risk of dyskinesias but decreases the risk of motor fluctuations and freezing. There has been some controversy over the possibility of increased mortality in patients treated with selegiline. The Parkinson’s Disease Research Group of the United Kingdom (PDRG-UK) reported the results of an open-label prospective trial of 520 patients with PD treated with either levodopa and selegiline or levodopa alone. After an average of 5.6 years of treatment, those treated with selegiline and levodopa had 60% higher mortality than those treated with levodopa alone. However, a similar increase in mortality has not been seen in other studies. A meta-analysis evaluated mortality in five prospective, long-term, double-blind, randomized, controlled studies of patients with early PD treated with selegiline and levodopa, and no difference in mortality was detected. The higher mortality in the PDRG-UK study is hard to explain but may have been related to greater disease severity, the high dropout rate (50% did not complete the study on their original treatment assignment), or poor study design, which used an intention-to-treat analysis (which placed responsibility for death on the original treatment group despite later changes in treatment) rather than an on-treatment analysis. More recently, three other double-blind, placebo-controlled studies have demonstrated that treatment with selegiline delayed the need for either levodopa or other dopaminergic agents, slowed the onset of motor fluctuations, and decreased the need for an increase in levodopa dosage. Therefore, selegiline treatment can be useful as monotherapy to spare levodopa use or in combination therapy with levodopa to reduce the needed levodopa dosage and potentially slow disease progression. In both instances, the recommended dosage is 5 mg twice a day, with the last dose given at noon because later dosing can cause insomnia. Dosages higher than 10 mg/day can cause a hypertensive crisis when foods rich in tyramine are ingested. Side effects of nausea, dizziness, and confusion are uncommon when selegiline is used as monotherapy, but cognitive dysfunction and psychosis are more liely to occur when used with levodopa and in older adults.
Antioxidant Therapy Based on the oxidative stress hypothesis, there has been interest in the use of antioxidants for neuroprotection in PD. Proposed antioxidants include vitamin E, vitamin C, GSH, N-acetylcysteine (a precursor of GSH), coenzyme Q-10, reduced NADH, and selenium (a cofactor of glutathione peroxidase). In DATATOP, subjects were treated with 2000 IU of vitamin E daily. No significant benefit was demonstrated in this treatment arm. The question of brain bioavailability of oral vitamin E was assessed by measuring CSF levels. This demonstrated a 74% higher level of vitamin E in subjects than in controls. At present, there is insufficient evidence that antioxidants provide any neuroprotective effect for patients with PD. More extensive clinical trials are necessary to support their general use in early PD treatment.
Chapter 115
SYMPTOMATIC TREATMENT Several medications are available that have been shown to alleviate the symptoms of PD. The extensive list includes levodopa, dopamine agonists (bromocriptine, pergolide, cabergoline, pramipexole, and ropinirole), selegiline, amantadine, catechol-0methyltransferase (COMT) inhibitors used with levodopa, and anticholinergic agents. It is widely accepted that levodopa, the immediate metabolic precursor of dopamine, is the most effective medication for treating parkinsonian signs and symptoms. Given alone, more than 95% of levodopa is converted to dopamine in the periphery by dopa decarboxylase, with minimal active drug crossing the blood-brain barrier. But when it is given as Sinemet (levodopa plus carbidopa, a peripheral dopa decarboxylase inhibitor), the central nervous system effect of levodopa is potentiated and peripheral side effects of nausea and vomiting decrease. However, over time (5 years on average), the majority of patients treated with levodopa develop response fluctuations that present as wearing-off of the effect after shorter periods of time, delayed ons, dosage failures, and sudden, unpredictable offs. In addition, many patients develop levodopa-induced dyskinesias, which can often be disabling and sometimes painful. Because of these troublesome motor fluctuationswith levodopa therapy, adjunctive therapy with dopamine agonists has been used in attempt to smooth out motor responses. In addition to the concern about motor fluctuations and dyskinesias, it is unknown whether levodopa is neurotoxic, contributing to the progression of nigral cell degeneration. This hypothesis of levodopa toxicity is based on observations that the metabolism of levodopa and dopamine produces free radicals, which could cause nigral cell death. Because of these concerns, the early treatment of PD has been subject to fierce debate and controversy, with some advocating early levodopa treatment and others in support of delaying levodopa treatment in hopes of avoiding these motor complications and potential toxicity of levodopa. Many who support use of levodopa early in the disease course argue that the motor complications are not secondary to levodopa treatment but are simply a manifestation of disease severity. The reason for this disagreement lies in the incomplete evidence of the potential role of levodopa in hastening disease progression in PD. There is both in vitro and in vivo evidence of potential neuronal death produced by levodopa, but there are also studies that show that high dosages of levodopa are safe in normal animals and humans. It has been suggested that levodopa may be toxic only to the already degenerated nigral neurons in PD or in chemically lesioned animals. However, a recent study in 6-hydroxydopamine(OHDA) lesioned rats showed no evidence of neuronal death as a consequence of levodopa therapy. Because of this concern about levodopa toxicity, some clinicians advocate using dopamine agonists as monotherapy for initial treatment of PD to delay the need for levodopa and thereby potentially delay the onset of motor complications. In addition, it has also been proposed that dopamine agonists may be potentially neuroprotective and therefore should be considered early in the treatment of PD.
Dopamine Agonlsts Dopamine agonists are pharmacologic agents that mimic the action of dopamine by directly stimulating dopamine receptors in
Initial Therapy of Parkinson's Disease
14s
the striatum. They are considered to be the most effective symptomatic treatment after levodopa. There are five types of dopamine receptors (D1-D5), and dopamine agonists bind nonselectively to these receptors to varying degrees. Dopamine agonists can be divided into the ergot and nonergot agonists. Ergot Agonists: Bromocriptine, Pergolide, Cabergoline. The first dopamine agonists used to treat PD were the ergot derivatives bromocriptine and pergolide. Bromocriptine has been generally recommended for use as adjunctive treatment with levodopa to control motor fluctuations and therefore is used mainly in more advanced disease. Most studies found that the bromocriptine dosage must be built up to 30 mg/day or more. Several trials have investigated the use of bromocriptine monotherapy in the initial treatment of PD. Early studies generally showed decreased incidence of motor complications but found the benefit of bromocriptine monotherapy to be short-lived (usually less than 1 year), often necessitating the early addition of levodopa. The PDRG-UK compared bromocriptine monotherapy with levodopa therapy in early Parkinson's disease. This study confirmed that bromocriptine was less effective than levodopa, but the incidence of dyskinesias and on-off fluctuations was significantly lower in the bromocriptine-treated group. Montastruc and others performed a 5-year open-label, controlled study comparing bromocriptine to which levodopa was later added with levodopa alone in untreated patients with PD. Their results showed that adding levodopa after 3 years of bromocriptine monotherapy delayed the occurrence of motor fluctuations and dyskinesias compared with levodopa alone, without any significant difference in UPDRS motor scores. Several studies have looked at the use of bromocriptine in combination with levodopa as a strategy to delay the onset of motor complications. These have shown conflicting results, with some showing equal efficacy of combination therapy with lower incidence of motor complications and others showing no improvement in motor fluctuationswith Combination therapy and better efficacy with levodopa alone. Whether used alone or in combination, the initial dosage is half of a 2.5-mg tablet twice daily with meals, increasing by 2.5 mg/day every few days. The most common side effects are nausea, sedation, postural hypotension, hallucinations, and confusion. Dopamine agonist monotherapy and combination therapy with levodopa has also been evaluated with other agonists. In a 3-month double-blind, placebo-controlled study, pergolide, a D1/D2 agonist, was found to be safe and effective as monotherapy in the early treatment of PD. In a long-term study of pergolide in combination with levodopa, 48% (151 of 314) of patients treated with both pergolide and levodopa had continued benefit after 3 years, and 40% maintained improvement after 4 years. Twentynine percent of de novo patients (18 of 62) had continued benefit on pergolide monotherapy for up to 3 years. The incidence of both wearing off and dyskinesias was highest in the patients initially treated with levodopa and lowest in the patients treated with pergolide alone. A double-blind randomized study has compared initial treatment with pergolide versus levodopa in early PD (PELMOPET). One-year interim analysis was significant for a delay in motor complications in pergolide-treated patients, but this difference did not persist after 3 years. In addition, there was a trend toward better efficacy in the levodopa-treated group. Adverse effects were more common in the pergolide group. Fluorodopa positron emission tomography scans did not show any significant difference in PD progression between groups. The initial dosage is 0.05 mglday for the first 2 to 3 days, followed by
746
Movement Disorders
Parkinson's Disease and ParkinsonianSyndromes
an increase by 0.10 or 0.15 mg/day every third day over the next 12 days. The dosage can then be increased by 0.25 mg/day every third day, aiming for a therapeutic dosage of 0.75 mg to 3 mg/day in divided doses three times per day. Some patients experience initial worsening before benefit, and first-dose hypotension can also occur. Most common side effects include dyskinesias, dizziness, hallucinations, nausea, somnolence, insomnia, constipation, diarrhea, and dyspepsia. Cabergoline, a long-acting dopamine agonist (not approved for PD treatment in the United States), was studied in a 3- to 5-year double-blind, randomized trial comparing initial therapy of PD with cabergoline alone or in combination with levodopa versus levodopa alone. The development of motor complications was significantlyless in the cabergoline-treated group than in subjects only receiving levodopa. Thirty-five percent of patients remained on cabergoline monotherapy after 3 years. There was a trend toward more improvement in UPDRS motor scores in the levodopa-treated group. However, there was no significant difference in UPDRS activities of daily living (ADL) scores between the two treatment groups, and in patients who did not need open-label levodopa therapy, the extent of improvement in motor disability was also similar between groups. Nonergot Dopamine Agonists: Pramipexole and Ropinirole. Pramipexole is a D2/D3 dopamine agonist that has been studied extensively as monotherapy in early PD and found to be very effective. In a 6-month double-blind, randomized study by Shannon et al of 335 patients with early PD, pramipexole significantly reduced the severity of parkinsonian symptoms compared with placebo. Mean daily dosage was 3.8 mg/day, and adverse events included nausea, constipation, and insomnia. In a 10-week study conducted by the Parkinson Study Group, 264 patients were randomized to five different dosages of pramipexole and were found to have significantly better UPDRS scores than those given placebo. These two short-term double-blind studies were continued in two long-term open-label trials, which found pramipexole to be effective and well tolerated in early PD for 3 years or more. The likelihood of remaining on pramipexole without requirement of levodopa after 4 years was 38% to 41%. Pramipexole monotherapy was also compared with levodopa therapy in a 2-year multicenter, double-blind, randomized controlled study of 301 patients with early PD (CALM-PD study). Open-label levodopa was permitted after the 10-week escalation phase. Fifty-three percent of patients in the pramipexole group needed supplemental levodopa, and 35% of levodopa-treated patients needed supplemental levodopa. Pramipexole treatment resulted in significantlylower occurrence of motor complications (28%) compared with treatment with levodopa alone (51%). However, there was a greater improvement in total UPDRS scores in the levodopa-treatedgroup. The majority of motor fluctuations occurred after the use of supplemental levodopa. Adverse events were more common in the pramipexole-treated group, specifically with somnolence, hallucinations, and peripheral edema. The P-CIT striatal single photon emission computed tomography uptake demonstrated a 35% reduction in dopamine transporter loss over 4 years in the pramipexole group. The recommended starting dosage is 0.125 mg three times daily and should be increased weekly by 0.125 or 0.25 mglday, aiming for a therapeutic dosage of 1.5 to 4.5 mg/day. There is some suggestion that the total daily dosage of 1.5 mg is sufficient for a therapeutic response. Ropinirole, a D2/D3 dopamine agonist, has been evaluated in several studies as monotherapy in early PD. Sethi and others studied ropinirole monotherapy in 147 patients with early PD in a
double-blind, placebo-controlled trial. The primary outcome measure was the number of patients who completed the study without the need to start levodopa. Significantly fewer ropiniroletreated patients needed levodopa compared with controls. However, 37% of ropinirole-treated patients withdrew because of adverse effects, compared with 16% of placebo-treated patients. The most common adverse effects were somnolence, dizziness, and arthralgias. A 3-year double-blind, randomized controlled trial compared ropinirole monotherapy with bromocriptine in 355 patients with early PD. Ropinirole was found to be more effective than bromocriptine as determined by UPDRS ADL and motor scores and as evidenced by fewer patients (33.9%) in the ropinirole-treated group needing levodopa than in the bromocriptine-treated group (41.9%). A 5-year double-blind, randomized controlled trial compared ropinirole with levodopa treatment in early PD, with the primary endpoint evaluating the occurrence of dyskinesias. Sixty-six percent of ropinirole-treated patients needed. levodopa supplementation, compared with 36% of patients randomized to levodopa therapy. The incidence of dyskinesias was significantlylower in the ropinirole-treated group, regardless of levodopa supplementation. In addition, disabling dyskinesias occurred in only 8% of the ropinirole group, compared with 23% in the levodopa group. The occurrence of wearing off was also lower in the ropinirole group (23%) than in the levodopa group (34%). However, the difference in UPDRS motor scores from baseline was significantlybetter, and the occurrenceof freezing was lower in the levodopa group. The incidence of somnolence and hallucinations was higher in the ropiniroletreated group. Studies using "F-DOPA positron emission tomography demonstrated better preservation of imaging markers in the ropinirole group. Recommended starting dosage is 0.25 mg three times daily, and the dosage should be increased weekly, aiming for a therapeutic dosage of 12 to 16 mg per day. Side effects are similar to those of other dopamine agonists and include nausea, dizziness, postural hypotension, dyskinesias, edema, somnolence, confusion, and hallucinations. Therefore, dopamine agonists can be effective as monotherapy in the initial treatment of PD, but most patients need levodopa supplementation after a variable time period, ranging from months to years. This variability is likely to be related to the heterogeneity of patients with PD, with some having a more benign course and others a more progressive course. Dopamine agonists in combination with levodopa appear to result in a lower incidence of motor complications than levodopa alone. This effect may occur simply because they allow a lower dosage of levodopa to be used. When deciding which dopamine agonist to use for symptomatic therapy, there are two main factors to consider: efficacy and side effect profile (Table 115-1).With the exception of bromocriptine, controlled studies have not compared one agonist with the other. One study has shown that bromocriptine is less effective than ropinirole. However, the remaining agonists (pergolide, pramipexole, and ropinirole) are generally believed to be equal in efficacy. Although the nonergot agonists are less likely to cause ergot-related side effects such as St. Anthony's fire and pulmonary or retroperitoneal fibrosis, all the agonists are generally equivalent in their side effect profile. The most common side effects are nausea, dyskinesias, leg edema, hallucinations, confusion, and somnolence. However, recently a previously unreported form of somnolence was reported in which patients suddenly fell asleep without any warning of drowsiness. These sleep attacks resulted in motor vehicle accidents involving patients treated with pramipex-
Chapter 115 H Initial Therapy of Parkinson's Disease
rn TABU115-1. Side Effects with Dopamine Agonists Common Side Effects
Uncommon Side Effects
Brornocriptine
Nausea
Pergolide Ca bergoline
Hallucinations Somnolence
Red, inflamed skin (St. Anthony's fire) Erythromelalgia Pleural thickening and effusions Retroperitonealfibrosis
Ergot Agonists
Confusion Dyskinesias Leg edema Constipation Postural hypotension Nonergot Agonists Prarnipexole Same as above Ropinirole
747
glaucoma, constipation, memory impairment, confusion, hallucinations, and urinary retention. The risk of side effects is greater in older adults. The starting dosage of trihexyphenidyl is 1 mg at mealtimes, and is increased by 2 mg/day for 3 to 5 days to 6 mglday three times a day. Benztropine is begun with 0.5 to 1 mg at bedtime, and the dosage can be increased gradually to 4 to 6 mglday as needed, divided two or four times a day. Procyclidine is initiated with 2 mg three times a day, after meals, and increased to 5 mg three or four times a day.
Levodopa Sleep attacks
ole and ropinirole who fell asleep at the wheel. Since that initial report, these sleep attacks have also been reported with levodopa and other dopamine agonists, but only pramipexole and ropinirole have a package insert warning about this potential risk of falling asleep without perceived warning. Therefore, when prescribing either one of these agonists, it is important to advise people about this potential risk, especially if they drive. Despite the general equivalence of the three major dopamine agonists, if one is not effective or poorly tolerated, it is worth trying another agonist. When switching from one agonist to another, one can switch directly to another agonist using the estimated dosage equivalents without needing to taper off one or gradually increasing the other. The dosage equivalent of pergolide and pramipexole is estimated to be 1:1, and 1 mg of pergolide or pramipexole is equivalent to 3 or 4 mg of ropinirole.
Amantadine Amantadine is an antiviral agent found to have an antiparkinsonian effect with several proposed mechanisms of action. These include the release of dopamine from central neurons, delay of dopamine uptake by neural cells, blockade of N-methyl D-aspartate (NMDA) receptors, and anticholinergic effects. As monotherapy or in combination with other antiparkinsonian medications, it is given at a dosage of 100 mg two or three times a day. Side effects include hallucinations, confusion, leg edema, and livedo reticularis. In mild symptoms of early PD, amantadine reportedly results in 20% to 40% global improvement in two thirds of patients when given as monotherapy. It seems to have minimal effect on tremor, and there is no evidence of tolerance development. Amantadine has also been found to be beneficial at decreasing levodopa-induced dyskinesias, so it can also be useful as combination therapy with levodopa.
Anticholinergics: Trihexyphenidyl, Benztmpine, and Procyclidine Anticholinergic agents are generally effective for treating tremor and have little effect on rigidity and bradykinesia. However, the response of tremor is variable, and more severe tremors usually are not responsive. Therefore, anticholinergics are effective mainly in treating mild tremors of early PD. The use of these drugs often is limited by side effects, which include dry mouth, narrow-angle
Although the use of levodopa in early PD remains a controversial issue, there is general agreement about the early use of levodopa in treating older adults (over 65 years), who are at higher risk of having cognitive side effects of confusion or hallucinations from dopamine agonists, amantadine, or anticholinergics. In addition, the motor complications of levodopa are less likely to occur in older adults. There are two main formulations of levodopa: immediate-release Sinemet (carbidopdlevodopa) and controlledrelease Sinemet (Sinemet CR). Immediate-release Sinemet has a faster onset but shorter duration of action. Sinemet CR has a delayed onset but a longer duration of action. It has been hypothesized that Sinemet CR, which provides a more steady plasma levodopa concentration, would decrease the incidence of motor fluctuations. A 5-year randomized multicenter study comparing treatment with immediate-release and controlledrelease Sinemet in 618 early levodopa-naive patients with PD did not reveal a significant difference in the occurrence of motor fluctuations or dyskinesias. However, the patients who completed the study (61%) may have had a more benign form of PD because they had a lower prevalence of motor fluctuations and dyskinesias than expected and were still on low dosages of levodopa after 5 years. This lower disease severity may have been a confounding factor because the occurrence of motor fluctuations may be an expression of disease severity. In this study, Sinemet CR provided a significant improvement in ADL measures compared with standard Sinemet. This may have been secondary to the slightly higher dosages of Sinemet CR (bioavailable dosage of 510 mg/day versus 426 mg/day) but also suggests that one may be able to use higher dosages of Sinemet CR without producing a higher incidence of motor fluctuations or dyskinesias. The improvement in ADL scores with Sinemet CR may have also been secondary to a lower severity of off periods and dyskinesias, which was not specifically measured in this study. Other clinical trials have demonstrated improvement in PD after conversion from standard Sinemet to CR, but some patients needed supplementation with standard Sinemet to maintain an optimal response. Therefore, it is not clear which form of levodopa is more effective in early PD treatment, and they may be more effective in combination. Immediate-release Sinemet may be more useful when the patient needs a faster onset of action, such as the first dose of the day, and Sinemet CR may be more useful when a longer duration of action is needed, such as at bedtime. The available dosages of Sinemet are 25/100, 10/100, and 25/250 mg. The starting dosage of Sinemet is 25/100 (25 refers to the carbidopa dosage and 100 refers to the levodopa dosage), one half tablet daily or twice daily with meals, increasing by one half tablet every 4 to 7 days. When replacing regular Sinemet with Sinemet CR, one must take into account that the bioavailability of Sinemet CR is only approximately 80% of that of standard Sinemet, so it may be necessary to increase the dosage by 25%. The
718
Movement Disorders W
Parkinson’s Disease and Parkinsonian Syndromes
TABLE115-2. Management of Levodopa Side Effects Side Effect
Management
Nausea
Take Sinemet with food Carbidopa Domperidone Quetiapine Clozapine (weekly CBCs needed) Increase salt intake in diet Increase fluid intake Compression stockings fludrocortisone Midodrine Lower levodopa dosage Add amantadine
Psychosis Orthostatic hypotension
Dyskinesias
available strengths of Sinemet CR are 50/200 (scored) and 25/100 (nonscored). All preparations are now available in generic form for lower cost. Sinemet CR should not be chewed, or its controlled-release properties will be lost. The most common side effects are nausea, vomiting, lightheadedness, orthostatic hypotension, psychosis including visual hallucinations or paranoid ideation, and dyskinesias. Extra carbidopa 25 mg three times a day or domperidone 10 mg two or three times a day (available in Canada and Europe) can be used to alleviate nausea. Atypical antipsychotics such as quetiapine or clozapine can be used to treat psychosis without worsening parkinsonism. Additional salt, fludrocortisone, or midodrine (an a-adrenergic agent) can be used for orthostatic hypotension. The recommended dosage of fludrocortisone is 0.1 mg/day, gradually increasing to 0.4 mg/day as needed. The starting dosage of midodrine is 2.5 mg twice daily at breakfast and lunch and increasing by 2.5 mg daily, up to a maximum dosage of 10 mg three times a day (Table 115-2).
NONPHARMACOLOGICTREATMENT Besides medical therapy, other essential interventions can significantly improve the symptoms of PD and should be undertaken early in the disease course. Of utmost importance in maintaining a high level of functioning is regular exercise and physical therapy. Patients should be encouraged to continue participating in exercises they enjoy such as walking, swimming, bicycling, hiking, golfing, and tennis. Other activities such as ballroom or square dancing can also help to maintain physical capabilities. Physical therapy that focuses on stretching exercises is very beneficial in diminishing muscle stiffness and rigidity, and gait training can be helpful for balance problems. For patients with speech difficulties, speech therapy can improve hypophonia. Occupational therapy focuses on improving ADLs, specific adaptations for continuation of employment, and exercises that can enhance fine motor coordination. Adaptations of the home environment may also be necessary, such as grab bars in the bathroom, specialized utensils, and easy-hold cups. Dietary considerations are also important. Constipation is a common problem in PD. Therefore, interventions such as increased dietary fiber and good hydration may facilitate regular bowel habits. For those with symptomatic orthostatic hypotension, compression stockings and increased salt intake can be helpful. Swallowing problems should be addressed by a speech therapy evaluation, swallowingstudy, and, if necessary, a change in the consistency of solids or liquids to avoid aspiration.
Seborrheic dermatitis has been associated with PD and can be managed by neutral or bland acne soap, ketoconazole shampoo, or shampoos, lotions, or creams containing selenium or pyrithione zinc. Psychotherapy may be beneficial for patients who have depression, anxiety, or difficulty coping with their illness. Counseling for family members and caregivers may be useful.
CONCLUSION There are many options to consider in the initial management of PD. When symptoms are still very mild and not very disabling, selegiline can be considered for its mild symptomatic benefit and potentially neuroprotective effect. Amantadine and anticholinergics can also be considered in patients whose symptoms are mild or in those with tremor. When more effective dopaminergic agents are needed to alleviate symptoms, one needs to decide whether to treat early with levodopa or to use a levodopa-sparing strategy and treat with dopamine agonist monotherapy. Because levodopa is generally more effective, if symptoms are very disabling, levodopa is likely to be a better choice. However, for younger patients who are at greater risk of developing complications from levodopa therapy, dopamine agonists are the treatment of choice. Levodopa therapy should be recommended as initial treatment in older adults to avoid the higher incidence of cognitive side effects from agonists. Pergolide and the newer nonergot agonists, pramipexole and ropinirole, show little difference in efficacy and tolerability. Nonpharmacologic therapies such as exercise, physical, occupational, and speech therapy, and a high-fiber diet may be offered early in the disease to maintain an optimum level of functioning and well-being.
SUGGESTED READINGS Barone P, Bravi D, Bermegjo-Pareja F et al: Pergolide monotherapy in the treatment of early PD: a randomized, controlled study. Neurology 53:573-579, 1999 Fahn S: Is levodopa toxic? Neurology 47(Suppl 3):S184-195, 1996 Koller WC, Hutton JT, Tolosa E et ak Immediate-release and controlledrelease carbidopa/levodopa in PD: a 5-year randomized multicenter study. Neurology 53:1012-1019, 1999 Korczyn AD, Brunt ER, Larsen JP et ak A 3-year randomized trial of ropinirole and bromocriptine in early Parkinson’s disease. Neurology 533364370, 1999 The Parkinson Study Group: Effects of tocopherol and deprenyl on the progression of disability in early Parkinson’s disease. N Engl J Med 328:176-183,1993 The Parkinson Study Group: Pramipexole vs. levodopa as initial treatment for Parkinson disease: a randomized controlled trial. JAMA 284(15): 1931-1938, 2000 Prasad KN, Cole WC, Kumar B: Multiple antioxidants in the prevention and treatment of Parkinson’s disease. J Am Coll Nutr 18(5):413-423, 1999 Rascol 0,Brooks DJ, Korczyn AD et ak A five-year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with ropinirole or levodopa. N Engl J Med 3421484-1491, 2000 Shoulson I and the Parkinson Study Group: DATATOP a decade of neuroprotective inquiry. Ann Neurol44(Suppl 1):S16&166, 1998 Waters CH:Therapeutics of Parkinson’s disease. pp. 79-91. In LeWitt P, Oertel W (eds): Parkinson’s Disease: The Treatment Options. Martin Dunitz Ltd, London, 1999 Weiner WJ: The initial treatment of Parkinson’s disease should begin with levodopa. Mov Disord 14(5):71&724, 1999
Chapter 116 rn Improving Responses to Levodopa
749
1 16 Improving Responses to Levodopa Peter Le Wilt MD
Parkinson’s disease (PD) is unique among neurodegenerative disorders in the near-complete relief of signs and disabilities that can be achieved with dopaminergic therapy. This difference has been shown most dramatically by use of the natural amino acid precursor of dopamine, levodopa (L-dihydroxyphenylalanine,or L-DOPA).Restoring striatal dopaminergic neurotransmission by levodopa (LD) administration is efficacious even when the dropout of substantia nigra neurons is extensive. Benefits of LD can be observed in almost all parkinsonian signs and symptoms. In the first few years of therapy (sometimes called the honeymoon period), LD dosages in the range of 200 to 600 mg/day generally offer highly satisfactory control of parkinsonism without the need for adjunctive medications. The aspects of PD that tend to be most disabling, such as slowness of movement and decreased dexterity, have the greatest likelihood for improvement with LD. Other clinical features such as resting tremor sometimes cannot be controlled to the same extent. However, LD’s overall effectiveness in idiopathic PD usually is dramatic and rapid in onset. Its benefit generally exceeds those of other available medications, including dopaminergic agonists possessing even greater potency at activating striatal dopaminergic receptors. For these reasons, LD has served as the standard against which all other antiparkinsonian therapy is judged. A trial of LD often is used to confirm the diagnosis of PD, even though other neurodegenerative disorders with parkinsonism sometimes show improvementswith this drug. When LD was first developed more than three decades ago, treatment with this drug seemed to provide a cure. The marked improvements usually achieved at the start of therapy for most patients with PD tend to continue indefinitely. The limits to maintaining the same degree of benefit from LD therapy include the progression of the underlying disorder, which can lead to impaired posture and balance unresponsive to LD. Several types of adverse reactions can be prominent at the start of LD therapy. These side effects, including sedation, nausea, and postural hypotension, can limit how rapidly the drug can be introduced, although tolerance generally develops over several weeks. Antinausea medication with trimethobenzamide can be helpful and does not exacerbate parkinsonism as other medications of this class do. The most effective antinausea medication, domperidone, is not available in the United States. Postural hypotension often responds to one or more strategies for counteracting the drop of blood pressure upon standing. These include increasing intake of salt or fluid (or both), indomethacin, dihydroergotamine, fludrocortisone, or midodrine. Often the need for such treatments diminishes with time after tolerance to LD has developed. The main shortcoming of chronic LD therapy for many patients is a gradual decline in the previously consistent benefit derived from this drug. Gaps in sustained control of parkinsonian signs, characterized by the reemergence of parkinsonian features at regular intervals between doses, occur for at least half of all patients after 2 or more years of therapy. Another side effect commonly developing during chronic LD use is involuntary movement (dyskinesia and sometimes dystonia). The potential for
these problems was unsuspected when LD first became available. One of the few voices raising concern was that of Professor Oleh Hornykiewicz, who commented as far back as 1970 that “while LD was the most natural substance for treating the striatal dopamine deficiency syndrome, it was far from perfect as a drug.” Sometimes these imperfections in clinical control can be evident even within a few months after the start of LD. The dual problems of wearing-off during each LD dosing cycle and LD-induced involuntary movements can develop in the same person. These problems can develop even in patients for whom the drug, at its best, continues to provide full relief of PD years after its initiation. Because motor fluctuations and dyskinesias are such common occurrences by 3 years after the start of LD, it is unclear why they do not occur for all patients. It is not known why some LD-treated patients with PD continue to have consistent, uncomplicated responses to this drug. Pulsatile stimulation of dopaminergic receptors has been suspected to be a causative factor in motor fluctuations and dyskinesias. However, there are several alternative explanations, and the mechanisms for these problems are still the subject of active research. In any case, once these idiosyncratic response patterns have developed, they tend to be irreversible. Even with attempts to minimize LD intake, dyskinesias can persist as regular peak effect responses. Although wearing-off responses often are associated with the same degree of improvement from each dose of LD over a shortened period of benefit, some patients lose the extent of antiparkinsonian improvement they once may have achieved with this drug. After several years of LD therapy, adverse effects in the psychic realm such as hallucination, paranoid and delusional thoughts, and other psychotic ideation can emerge, especially in the older patient with coexistent cognitive decline. With all the problems associated with chronic LD therapy, some researchers have been concerned that this drug might impart direct toxicity. In vivo studies have not supported this speculation. Although some long-term trials indicate that fewer adverse outcomes may be associated with the initial use of dopaminergic agonists, there is no evidence of a detrimental side to LD therapy with respect to the underlying disorder. Pharmacologic research has explored many options for dealing with the limitations of LD therapy. With respect to motor fluctuations and dyskinesias, there are several ways to extend the action of LD and to tailor its responses to more desirable outcomes. This chapter discusses several issues of practical importance for managing their common complications of chronic PD therapy. The topics listed in Table 116-1 are discussed in detail in this chapter.
MAXIMAL USE OF ALTERNATIVES TO LEVODOPA Although LD is the gold standard of antiparkinsonian therapy, other drugs also can relieve mild disabilities such as tremor, decreased arm swing, and various manifestations of slowed movement. Amantadine and anticholinergics have a place in PD therapeutics as alternatives or supplements to LD therapy. One option for some mildly affected patients is to delay starting LD.
750
Movement Disorders W
Parkinson’s Disease and Parkinsonian Syndromes
TABLE 116-1. Checklist for Monitoring Levodopa Therapy Have alternatives to levodopa (LD) been used? Are the timing and quantities of LD dosing optimal for achieving maximal benefit? Are patients likely to benefit from strategies to extend effects from each LD dose? Have there been adverse effects that call for a change in the regimen? Have new patterns of drug response developed, warranting the addition of dopaminergic agonists? Is the patient a candidate for neurosurgical interventions offering improvements beyond medication benefits? Does declining benefit from LD suggest a neurologic diagnosis different from Parkinson’s disease? Has the medication regimen been assessed for cost-effectiveness? Are supportive services for patients and their families being used to their maximum?
Whether long-term exposure to LD therapy might accelerate disease progression has been controversial for many years. While this view is not supported by clinical studies or experimental animal models of parkinsonism, chronic LD use is a risk factor for the development of dyskinesias. Although it is inappropriate to delay offering LD to a patient with significant disability, many clinicians delay the start of LD for minimally symptomatic patients. Amantadine and anticholinergics add to the number of medications taken and carry their own possible side effects, but these drugs can be effective and may reduce long-term LD exposure. For parkinsonian features of slowed movements, decreased dexterity, and similar problems, treatment with dopaminergic agonists may be appropriate. These drugs include bromocriptine, pergolide, pramipexole, and ropinirole. Dopaminergic agonists duplicate many of the benefits provided by LD therapy. Although they are more expensive, entail longer buildup schedules, and can have more side effects, these drugs may offer better long-term outcomes than LD. Several studies have been conducted comparing monotherapy regimens of dopaminergic agonists with LD. In each instance, the maximal benefits for symptom relief were somewhat less with the dopaminergic agonists. However, there was a lower incidence of dyskinesias and motor fluctuations, suggesting that these alternatives to LD might lower risks for problems commonly developing after sustained LD use. These studies have also shown that LD combined with a dopaminergic agonist from the start or shortly afterward may also confer a better outcome than LD alone. Recent findings from long-term studies of ropinirole and pramipexole as initial therapy suggested that these drugs also might possess neuroprotective actions. As compared with the use of carbidopa or LD, treatment with either of these dopaminergic agonists was associated with less loss of striatal dopaminergic innervation. Although these intriguing findings are not proof of a clinically significant neuroprotective action, the results of both the pramipexole and ropinirole studies provide an argument for using these (or possibly other dopaminergic agonists) instead of LD therapy. Several laboratory studies provide clues of how these drugs might delay the progression of PD. For patients presenting the earliest stages of PD, a common sign (and a feature that can be indicative of worsening parkinsonism) is just a resting tremor. The impact of tremor on comfort, self-image, or even livelihood should not be underestimated, even though this feature usually is not a source of much disability. Often, the use of anticholinergic drugs or amantadine can provide more relief of tremor than LD or other dopaminergic drugs. Unfortunately, in some instances tremor does not respond to conventional antiparkinsonian medications. There are a few addi-
tional pharmacologic options. One is clozapine, an atypical neuroleptic that has a unique (and as yet uncharacterized) mode of action at reducing parkinsonian tremor. Only small dosages (e.g., 12.5 to 25 mg/day) of clozapine are needed. Clozapine use necessitates regular monitoring of the white blood cell count but can be quite safe in the small dosages generally effective against tremor. Botulinum toxin selective denervation of affected forearm muscles has been tried but generally is ineffective against tremor. Another pharmacologic approach is medication effective for treating essential tremor, P-adrenergic-blocking drugs and primidone. Though primarily effective for postural or action tremors, these drugs occasionally help control resting tremors in patients with PD. Neurosurgical interventions to treat tremor from parkinsonism and other causes can be highly effective and are established therapies. Like thalamotomy, high-frequency electric pulsing (deep brain stimulation, DBS) of the thalamus and the subthalamic nucleus from implanted electrodes can provide tremor control even in patients with unresponsiveness to all antiparkinsonian medications. The clinical results from DBS are better in general than from electrolytic lesioning techniques. Both lesioning and DBS procedures achieve permanent results. These surgical procedures are now carried out at many highly experienced centers throughout the United States. In addition to tremor, DBS of the subthalamic nucleus can provide dramatic improvements of gait disorders, start hesitation, rigidity, and other parkinsonian features.
OPTIMIZING TIMING AND AMOUNTS OF LD THERAPY LD therapy entails periodic monitoring and dosage adjustment. The features of parkinsonism can change over time, as can the patterns of drug response. For many patients, the most obvious change is development of a regular onset and decline in the antiparkinsonian effects from each dose of LD. This variability in clinical effect closely follows the timing of rise and fall in plasma LD concentrations. Analysis of the relationships between the drug’s pharmacokinetics and clinical actions suggests that the central nervous system response to the drug is subject to a short delay (approximately 5 to 15 minutes) as compared with peripheral LD pharmacokinetics. The loss of a long-duration benefit from each dose of LD seems to imply that, initially, the striatum is able to store and slowly release dopamine for long periods of time. Eventually, this storage capacity is lost. When a patient develops wearing-off responses, there are new challenges and several options for achieving consistent response to LD. Although a specific mechanism for these phenomena has not been elucidated, neuroimaging of the brain with respect to LD uptake has been informative. Patients with PD and typical wearing-off fluctuation patterns have been studied by administration of ‘%uorodopa in trace amounts for positron emission tomography studies. After intravenous injection of this labeled LD analogue, the rise in striatal activity of the parent tracer (or its metabolites) in subjects with PD was briefer for patients with LD wearing-off responses than for controls. Similar results came fiom experiments in rodents investigating the timing of LD metabolism in a lesioned nigrostriatal system. These studies have provided in vivo correlates of clinical observations showing shortened dopaminergic stimulation derived from each oral dose of LD. Based on these observations, strategies to increase constancy of LD delivery to the brain have been devised. Because LD pharmacokinetics and clinical response are closely correlated, modification of the dosing schedule is a logical start for improving outcomes. Verification of a wearing-off response pattern is a first step. Although a home diary of “on” and “off
Chapter 116
timing with respect to LD doses may be useful, most patients are aware if they experience a rise and fall of antiparkinsonian effect following each dose of medication. With immediate-release preparations of LD (combined with carbidopa), the rise and fall of plasma LD concentrations typically follows an elimination half-life cycle of 2.5 to 3.5 hours. Pharmacokinetic-pharmacodynamic studies have shown that LD’s half-life correlates well to its duration of antiparkinsonian effect. The factors imparting the greatest source of variability in plasma LD concentrations are associated with its absorption. LD enters the bloodstream via a facilitated large neutral amino acid uptake mechanism located in the duodenum and jejunum. LD uptake is subject to competition by other dietary amino acids and other gastrointestinal (GI) factors such as transit time and duodenal pH. Only a small fraction of ingested LD reaches the brain. Typically, patients treated with LD need 300 to 800 mg/day for optimal effect. Generally it is taken as 100 to 150 mg LD per dose and at intervals of 3 to 6 hours. The patient experiencing wearing-off responses may be helped by a change to interdose intervals of 2 to 3 hours. The amount of LD per dose can be reduced as shorter interdose intervals are adopted. A decrease to less than %hour intervals does not provide any greater consistency of LD benefits. Usually, the failure of significant improvement from dosing with LD as close together as 2 hours indicates another type of motor fluctuation that might warrant management by means other than extension of LD effect. For patients with a great deal of sensitivity to each dose of LD, it may be necessary to divide carbidopa and LD pills into small fragments to minimize the amount absorbed at any one time. Even though the small tablet (100 mg) is scored only for breaking in half, most patients can create 25-mg dosing increments for titration to optimal effect. Preparing the oral dose of carbidopa and LD in a liquid suspension offers another way to ingest precisely measured fractions of this drug. Neither LD nor carbidopa dissolves in water, and so the suspension must be agitated (by swirling) to permit accurate measurement of LD content by liquid volumes. Careful use of LD in liquid suspension can permit dosing with precise amounts of the drug, especially with quantities between the limited dosage increments possible with whole or half tablets. Patients can prepare a suspension by
751
Improving Responses to Levodopa
adding one 25/100 carbidopalLD tablet for each 50 mL of water to achieve a 2-mg/mL LD concentration. By adding 100 mg ascorbic acid (vitamin C) to each 500 mL of the suspension, patients can prevent LD oxidation (which is evident from a blackening of the solution with a flocculent precipitate). The timing of LD intake can be a critical determinant of optimal drug effect. Like their physicians, patients should become familiar with the pharmacokinetic profile of immediate-release LD (Fig. 116-1). Also illustrated is the delayed rise and fall of LD derived from the sustained-release preparation (Sinemet CR and generic versions). The bioavailability of LD from the sustainedrelease preparations is approximately 70% that of the immediaterelease formulations. Although measurement of plasma LD concentration is not practical for management decisions in the usual clinical setting, the timing of absorption and wearing-off can be inferred from these usual pharmacokinetic patterns. In actuality, the profiles of plasma LD concentration can differ markedly from dose to dose. This variability can be the consequence of factors such as GI transit time and the timing of meals. Most patients find that taking the drug without food gives the best chance of absorbing each dose of LD. Therefore, ingesting this medication at least one half hour before meals or an hour afterward is advisable. If patients develop nausea or other types of GI distress from LD taken without food, these problems generally can be alleviated with a few crackers or a slice of bread. LD absorption can also be subject to interference by protein intake in meals. As described earlier, the entrance of LD into the bloodstream is controlled by an active process of large neutral amino acid uptake. Some reports have given the impression that competition for LD uptake by dietary protein-derived amino acids is a common cause of motor fluctuations. However, most clinical experience indicates that irregularity in LD absorption is only rarely related to the protein content in the diet. It is possible to test for sensitivity to protein by experimenting with meals containing either high- or low-protein content. A patient can evaluate how well parkinsonism is controlled by LD during days when a high-protein lunch was consumed, in comparison to outcomes on days during which lunch contained little or no protein. If the high protein intake interferes with the antiparkinsonian effect, a patient can make dietary alterations to improve the quality of LD 1200
900 C
.-0 4-
mL *
FIG. 116-1. Typical plasma concentrations of levodopa over time following oral dosing with: (a) two tablets of immediate-release carbidopa/levodopa 25/100 mg (solid line); (b) one tablet of sustained-release carbidopa/levodopa 50/200 mg (Sinemet CR 50/200; dotted line); and (c) the effect of a 200 mg tablet of the catechol-0-methyltransferase inhibitor entacapone (Comtan) on two tablets of immediate-release carbidopa/levodopa 25/100 mg (broken line).
C
g~
sp m
600
8
3
0
-I
300
L
I
ing
2
6
4
Hours
8
752
Movement Disorders W
Parkinson’s Disease and Parkinsonian Syndromes
responses. In this rare situation, a patient can plan for a uniform protein intake for each meal and redistribute daily protein intake predominantly to a meal at the end of the day. There are other reasons for delayed or incomplete LD absorption. Gastric retention of ingested LD can be a limiting factor of absorption and subsequent delivery to the central nervous system. Variations in the stomach‘s release of the drug can add an hour or more to the usual delay of 15 to 30 minutes between pill ingestion and the onset of clinical effect. Delayed uptake has been described to occur after lunch (the “siesta stomach syndrome) or in other situations when ingested LD fails to act. STRATEGIES TO EXTEND EFFECTS OF EACH LD DOSE Sustained-Release LD Preparations When variation in clinical benefits develops with the use of immediate-releaseLD, one option is a switch to a sustained-release preparation. These formulations were designed to provide extra duration of antiparkinsonian effect and a more gradual decline in plasma LD concentration. Two sustained-release products were developed in the 1980s after much experimentation with alternative preparations. Madopar CR (formerly Madopar HBS) is a capsule transformed into a gelatinous diffusion body that floats on the fluid contents of the stomach. Madopar CR, which contains 100 mg LD and 25 mg benserazide, is not available in the United States. Another LD preparation designed for delayed release of its contents has been marketed in the United States and elsewhere as Sinemet CR. This product is also available as a generic equivalent. Sinemet CR is a scored tablet with a mixture of 50 mg carbidopa and 200 mg LD embedded in a polymeric matrix. It is also prepared in a tablet containing 25 mg carbidopa and 100 mg LD. Both Madopar CR and Sinemet CR have delays of hour or more after ingestion to reach peak LD concentration. The extension of LD effect is, on average, up to 2 hours longer than that of immediate-release LD preparations. Sinemet CR and Madopar CR have shown effectiveness at decreasing end-of-dose and other types of motor fluctuations in some patients. Comparisons between the two products suggest that their pharmacokinetic profiles are similar. However, many clinicians comparing the utility of Sinemet CR with Madopar CR have found Sinemet CR to achieve a much more reliable extension of LD’s effect. Less of the LD content is absorbed from both the Sinemet CR and the Madopar CR preparations (only about 70%, on average), as compared with immediate-release forms. Patients switching from an immediate-release to a sustainedrelease LD formulation can achieve an increase in duration and improved consistency of effect. Sometimes, the switch to the sustained-releaseproduct leads to a simplified medication schedule or improved medication compliance in a setting such as a nursing home. Unfortunately, there is ample evidence that sustained-release preparations do not always result in more consistent LD plasma concentrations. Many patients have experienced more variability in clinical effect from Sinemet CR than from immediate-release LD taken regularly at intervals of 2 to 3 hours. For patients experiencing LD response fluctuations, sustainedrelease carbidopa and LD can be combined with immediaterelease forms to optimize intake of this drug at each dosing interval. For the first dose of the day, the immediate-release preparation can be used. Many patients receiving sustained-release LD need booster doses of immediate-release LD (25/100 mg) to
achieve small increments of increased LD effect. Breaking in half the carbidopa and LD CR 50/200 tablet does not eliminate its sustained-release properties, although the exposed pill surface somewhat hastens LD absorption. A patient in need of more rapid medication effects might chew a fraction of the tablet to offset its delayed release properties. The main application for sustained-release preparations is to lessen the abruptness of wearing-off responses. Although this is sometimes successful, the peak effect of LD may be too much for some patients because the sustained-release formulation contains either 100 or 200 mg of LD per dose. This can be associated with a higher occurrence of dyskinesias. The more gradual rise in plasma LD concentration may also be associated with a less abrupt onset of peak effect dyskinesia or dystonia (which typically occurs 30 to 60 minutes after a dose of LD). The greater period of drug effect with sustained-release LD can be useful for patients with frequent awakening during the night because of dystonic cramping, tremor, or difficulty in attaining a comfortable sleeping position. Although sustained-release LDS more gradual rise and fall in drug concentration might seem to be beneficial for all patterns of motor fluctuation, some patients are not helped. This has been recognized with the diphasic (dyskinesia-improvementdyskinesia pattern) of LD response. Trials of Sinemet CR have shown exacerbation in the duration of dyskinesias experienced by such patients. Patients with increased occurrence of dyskinesias or other LD-related side effects may need to reduce the amount of controlled-release preparation in their afternoon doses because of plasma accumulation of LD. Catechol-0-MethyltransferaseInhibition
Other approaches to extend the duration of LDS effect have been sought in peripherally acting inhibitors of catechol-0methyltransferase (COMT). Two drugs have been developed for this purpose: tolcapone and entacapone. COMT activity is present throughout the body, including red blood cells, liver, kidney, and gut. A large fraction of orally ingested LD is converted by COMT to 3-O-methyldopa, an inactive metabolite that cannot revert to the synthesis of dopamine. Bloodstream concentrations of 3-0methyldopa generally exceed those of LD with conventional antiparkinsonian therapy. Inhibition of COMT with tolcapone or entacapone results in decreased LD clearance, resulting in more sustained plasma concentrations. The prolongation of LD’s elimination half-life does not generally result in an increase of peak LD concentrations in the first hour after its intake (Fig. 116-1). Both COMT inhibitors are excluded from the brain in conventional dosages, so they do not retard the degradation of dopamine by this enzyme in the brain. The peripheral clearance of LD can be reduced by approximately one third with the use of tolcapone or entacapone. This can result in a much more gradual decline in plasma LD concentrations, resulting in longer duration of effect and less abrupt wearing-off of LD actions in patients experiencing this type of fluctuation. Its benefits are in part caused by an increase of the fraction of an LD dose entering the brain, an effect that can be duplicated in part by increased LD dosing. Possibly the most important clinical value for COMT inhibition is an overall reduction in variability of plasma LD concentrations, resulting in more consistency of LD effect in a disorder for which clinical control by medications can become increasingly unpredictable. Both tolcapone and entacapone are highly selective inhibitors of COMT whose sole action in PD is by enhancement of LD effect.
Chapter 116
Tolcapone is recommended for use at either 100 or 200 mgldose at 6-hour intervals, based on a longer duration of action than entacapone. Entacapone, available only in a 200-mg tablet, is recommended for administration with each dose of LD (either immediate or sustained release). However, the duration of entacapone effect as a COMT inhibitor permits it to be administered as far apart as 4-hour intervals for maximal effect. Tolcapone has been associated with a few instances of fatal liver damage, leading to its withdrawal from marketing in Europe and elsewhere. The mechanism (or even proof) of a direct connection between the drug and this idiosyncratic outcome has not been established, however. Although most people treated with this COMT inhibitor did not show any evidence of hepatotoxicity, tolcapone’s availability in the United States is limited to patients for whom other comparable therapy fails. Because entacapone acts in identical fashion to tolcapone, there is currently little use of tolcapone (although the latter probably is more potent as a peripherally acting COMT inhibitor and has a longer duration of effect). COMT inhibition can be regarded as an all-or-none event that can be of value in patients whose parkinsonian control has become highly dependent on moment-to-moment concentrations of plasma LD. Increases of daily “on” time by approximately 1 hour have been reported in patients with typical wearing-off responses. Tolcapone and entacapone do not tend to improve other types of motor fluctuations such as start hesitation or unpredictable “off states. For the patient willing to take LD at intervals as close as 2 hours, COMT inhibition generally does not offer any additional advantage. However, given the variability of plasma LD concentrations often experienced with the use of sustained-release LD preparations, COMT inhibitors can offer an improvement (and the more expensive sustained-release LD preparation can be eliminated). The start of COMT inhibitors can be without a titrated introduction. However, the immediate effect can be an increase of LD delivery to the brain, so patients experiencing dyskinesias or other peak effect LD actions should reduce their LD intake. A trial as short as 1 week can establish whether a new regimen of COMT inhibition is of value. The clinical effects of these drugs are gone within 1 day of their discontinuation because both tolcapone and entacapone are reversible inhibitors of the enzyme. Apart from an increase of dopaminergic side effects such as dyskinesias, the main adverse reactions of tolcapone and entacapone are the rare occurrences of GI bloating and diarrhea, both of which can develop after several weeks of therapy and cease once the drugs are stopped. Current regulations for the use of tolcapone include biweekly testing for elevations in liver-derived enzymes and a detailed informed consent process emphasizing the rare possibility of potentially fatal hepatotoxicity.
Monoamine Oxldase-B Inhibition Another approach for lessening wearing-off responses involves inhibition of central nervous system monoamine oxidase (MAO). This enzyme is the initiating step in the major pathway of dopamine catabolism. MA0 has been differentiated into two forms on the basis of substrate specificity. In PD therapeutics, drugs with a broad-spectrum inhibition of MA0 (which are used to treat’depression) pose a problem because MAO-A inhibition would permit hypertensive reactions to result from dietary tyramine. Selective MAO-B inhibition potentiates the antiparkinsonian effects of dopamine without risk of adverse reactions from tyramine. A selective and irreversible inhibitor of MAO-B,
Improving Responses to Levodopa
753
selegiline (also known as deprenyl), has been used to augment LD’s effects. Selegiline can be used safely at dosages of 10 mglday in chronic therapy for PD. By blocking the breakdown of dopamine derived from each dose of LD, selegiline augments the duration of its clinical action. In postmortem studies, conventional selegiline treatment produced more than 90% inhibition of striatal MAO-B. A lo-mglday dosage of selegiline has been widely adopted in using the drug for adjunctive therapy, although it is likely that chronic treatment with a much lower dosage would also achieve full MAO-B inhibition. Studies using regimens of up to 40 mglday revealed no additional antiparkinsonian actions over results achieved from 10 mglday. Another important consideration in using selegiline is that after discontinuation of the drug, its effects as an MAO-B inhibitor linger for several weeks. Selegiline does not alter the absorption or peripheral metabolism of LD. Additional properties of selegiline besides MAO-B inhibition are unlikely to contribute to its pharmacologic profile in augmenting dopamine’s action. The metabolites of selegiline may cause some of the adverse effects some patients experience from this drug. A conventional daily dosage of selegiline is converted to small quantities of L-amphetamine and L-methamphetamine. It is unliiely that these metabolites have any effect on parkinsonism. Administered with LD, selegilineaugments both the magnitude and the duration of LD’s effects. This can occur even with sustained-release LD preparations. Extensive clinical experience with selegiline supports the use of selegiline as a means for potentiating LD’s clinical effects. Most studies have shown the increased duration of effect to be no more than 30 to 45 minutes per dose of immediate-release LD. For some patients, selegiline therapy can lessen the problem of wearing-off decline in LD’s action. However, not all patients experiencing wearing-off will respond. Other types of motor fluctuations such as start hesitancy or sudden “off’ states ‘do not improve with selegiline, nor is selegiliie useful in treating patients with involuntary movements because it can exacerbate this problem. Dysphoric reaction, vivid dreams, hallucinations, and sleep disturbance are other possible dose-related side effects. Adjunctive therapy with selegiline can be beneficial for patients who are undermedicated with LD. Sometimes, the same types of improvement with selegiline could also be achieved by an increased dosage or closer spacing of the LD intake. For patients already receiving LD at a maximally tolerated dosage, addition of selegiline calls for a reduction in LD intake by 20% or more to avoid peak dose side effects. Based on its action as an irreversible inhibitor of MAO-B, it seems that the actions of selegiline should be lasting, although some studies have shown that even when there is benefit, it can decline after several months. As an MAO-B inhibitor, selegiline should be regarded as having an all-or-none effect on LDS actions. A brief trial can demonstrate its value for enhancing LDS benefits. No dietary restrictions are needed with the use of selegiline at a daily dosage of 5 to 10 mglday. When daily intake exceeds 30 mglday, however, the drug loses its selectivity for MAO-B and could produce hypertensive reactions if the patient ingests tyramine. A few serious adverse drug interactions have been described to result from coadministration with selegiline. With meperidine (also known as pethidine outside the United States), a toxic adverse reaction resembling opiate overdosage has been described. Other compounds with opiate properties might also produce similar adverse reactions with selegiline. An idiosyncratic adverse reaction between antidepressant medications (particularlythe selective serotonin reuptake
754
Movement Disorders
rn Parkinson's Disease and Parkinsonian Syndromes
blockers) and selegiline has been reported, resembling the idiosyncratic reaction described with meperidine. Enteral LD Infusion
Although the pharmacokinetic profiles of sustained-release LD preparations can improve the constancy of LD's effect, irregularities in gastric emptying can still govern the absorption of the drug. Domperidone does not always increase gastric emptying for the purpose of enhancing LD's uptake. Even if the stomach regularly delivers the drug to the upper GI tract, some irregularity in its uptake is inevitable because of the influences of meals, GI motility, and other factors. For some patients, the therapeutic window for LD can be so narrow that the only means for adequate control is through an invariant plasma blood concentration. Intravenous LD infusions, adjusted to an optimal drug delivery rate for symptomatic relief, have shown that antiparkinsonian control can be improved by constant plasma LD concentrations. Similarly, methods for direct enteral infusion of LD suspensions have been shown to improve on the dose-by-dose variability associated with the drug taken in tablet form. A permanent route of enteral access can be installed with minimal discomfort, sometimes on an outpatient surgical basis. This method of per-gastric duodenal or jejunal infusion makes use of a small-bore feeding tube inserted through the abdominal wall and connected to a portable pump. This procedure has few complications apart from the infusion tubes curving back into the stomach or knotting. An alternative means of enteral infusion is insertion of an infusion tube by jejunostomy. Although fewer tube reinsertion procedures may be needed with jejunostomy, it entails an abdominal operation, in contrast to the outpatient radiologic procedure for placing a per-gastric feeding tube. For patients unable to improve their clinical state by adjusting their oral intake of LD or adjunctive medications, continuous enteral infusion can offer great benefits. This physical means for bypassing the pylorus also provides an opportunity for a rate-controlled delivery of the drug to its primary absorptive sites in the duodenum and jejunum. Patients using enteral infusion are not constrained to the dosing regimens limited to the quantities of LD in available formulations. The infusion permits precise adjustment to either the optimal rate of delivery or the bolus dose needed for desired effects. The portable pumps currently available permit the LD delivery needed to achieve either stable or readily altered plasma concentrations of LD. The infusion rate can be adjusted in extremely small increments of drug delivery as titration proceeds in search of optimal effect. With continuous enteral LD infusion, the clinical effect from each rate change becomes evident within 5 minutes. Constant infusion avoids the occurrence of peak concentrations and the consequent surge of dopaminergic effect that are associated with use of conventional LD preparations. Consequently, dyskinesias can be diminished or eliminated. Although the constant infusions can result in increased daily needs for LD in some instances, the net effect can be a marked improvement in the control of motor fluctuations. PArCLRNS OF DRUG RESPONSE WARRANTING CHANGE IN TREATMENT REGIMEN
With chronic therapy of parkinsonism, changes in clinical control of symptoms over time may herald new targets for treatment. Involuntary movements, dystonic postures, painful spasms, and sudden freezing may develop as inevitable consequences despite
regular doses of LD. Attempts to alter LD intake may be unsuccessful at modulating these problems, which often respond to dopaminergic agonists (Table 116-2). Therapy with bromocriptine, pergolide, ropinirole, or pramipexole can bring about more on time and fewer freezing episodes.Although these drugs differ in their structures, dopamine receptor subtype stimulation profiles, and pharmacokinetics,their net antiparkinsonian effect is similar. Not all patients improve from or can tolerate dopaminergic agonists. If introduced gradually over up to 2 months, these drugs produce tolerance to their acute side effects such as nausea, vomiting, and hypotension. Dose-limiting side effects can include sedation, vivid dreams, and hallucinations. Sometimes one agonist is much more effective or better tolerated than another, and so a switch between these drugs often is warranted in patients achieving suboptimal control. In addition to helping with unpredictable and sudden off states, the dopaminergic agonists present another solution for managing the wearing-off in LD effect. Because of their longer plasma half-lives, the addition of a dopaminergic agonist can help to lessen the tendency for an abrupt loss of clinical effect in LD-treated patients. Another situation in which dopaminergic agonists can improve antiparkinsonian control is for peak effect dyskinesias. Patients whose disabling involuntary movements emerge at the height of LD's antiparkinsonian actions sometimes can be helped by a decrease in the LD dosage and the addition of a dopaminergic agonist. Other problems related to advanced PD could also be responsive to dopaminergic agonists. The tendency to fall as a result of retropulsion usually is not helped, but gait hesitancy, causing imbalance, can be improved by adding a dopaminergic agonist to an LD regimen. Dopaminergic agonists can be useful for early morning dystonia, a problem in which the feet are subject to painful spasms related to the gradual loss of dopaminergic effect over the course of the night. The extended duration of effect from dopaminergic agonists, like that of sustained-release LD, can avert this problem when these medications are taken at bedtime. Apart from this indication, antiparkinsonian medications are not generally advisable for use during
W
TABLE 116-2. Situations Warranting the Use of Dopaminergic Agonists
When there is inadequate benefit in control of parkinsonism from a daytime levodopa (LD) regimen greater than 800 muday With the occurrence of start hesitation or unpredictable "off" states such as freezing episodes As substitute for LD when intolerable dyskinesias occur With the occurrence of early morning dystonia (typically unilateral dystonic foot cramping) With peak effect and end-of-dose dystonic reactions associated with LD therapy (or preceding its start) As an alternative treatment for patients with the diphasic (dyskinesiaimprovement-dyskinesia)pattern of LD response For enhancing the consistency of antiparkinsonian control in a patient experiencing dose-by-dose fluctuations in L D s effects, even if other extension strategies have failed For controlling parkinsonian features minimally responsive to LD treatment (such as resting tremor or imbalance) or when little overall benefit from LD has occurred Rarely, when LD therapy is not well tolerated (because of nausea, hallucinations, sleep disturbance, or dyskinesias and despite the increased potency of the dopaminergic agonists) As initial monotherapy (or in combination with LD) to avoid long-term adverse outcomes of LD therapy (motor fluctuations, dyskinesias) and, possibly, for a neuroprotective action against Parkinson's disease progression
Chapter 116 rn ImprovingResponsesto Levodopa
sleeping hours because they can cause vivid dreams and sometimes enhance nocturnal myoclonus. In the past decade, there has been little formal investigation of drug holidays, the notion that abrupt discontinuation of LD and other antiparkinsonian medications might lessen LD-induced adverse effects. Although there has been limited support for the concept in terms of outcomes for several weeks after a drug holiday, the abrupt stopping of antiparkinsonian medications can be uncomfortable and dangerous. Drug withdrawal has been associated with a neuroleptic malignant syndromelike response, aspiration pneumonia, and deep vein thrombosis from marked rigidity and immobility. It is possible that the claimed benefits of drug holidays in the past were actually the consequence of reduced intake of LD, especially if the daily dosage was excessive previously. ADVERSE EFFECTS THAT CALL FOR A CHANGE IN THE TREATMENT REGIMEN The following problems may be indications for changes in medications.
755
clozapine and quetiapine can be highly effective for improving these problems without exacerbating parkinsonism. Olanzapine and risperidone are also effective but can increase parkinsonian features.
Forgetfulnessand Other Cognitive Decline Sometimes an accompaniment of too much dopaminergic therapy, decreased memory function and confusion can also develop in patients receiving anticholinergic medication. Even if this problem is not recognized initially, forgetfulness always calls for reducing and stopping anticholinergic agents, and this should be carried out from time to time to assess both benefits and possible contributions to impaired cognitive abilities. Surprisingly, anticholinergic therapy also is very well tolerated by some older adults. A trial of cholinesterase inhibitors, including donepezil, rivastigmine, or galantamine (Reminyl) for several weeks can be used to assess the potential for one of these drugs to improve cognitive impairments without exacerbating parkinsonism.
Postural Hypotension Peak Effect Dyskinesias or Dystonla Dyskinesias can be quite benign, sometimes unnoticed by patients. If they are troublesome, several measures can be taken. The total LD intake or the amount per dose may need to be decreased. Sometimes dyskinesias and dystonia are more prominent in the afternoon and evening because of cumulative effects of LD taken earlier in the day. If so, dosage reduction later in the day is appropriate. An increase in the intensity of peak effect involuntary movements can result from previous addition of selegiline or a dopaminergic agonist. If so, these adjunctive medications can be decreased or eliminated if they provide no additional benefit. Dyskinesias sometimes can be blocked with amantadine (100 to 300 mg/day). Other pharmacologic approaches include the use of neuroleptic medications in small dosages, such as 2.5 to 5 mg molindone, a selective D, dopamine receptor blocker. Other drugs that can be used in small dosages for this purpose include risperidone and pimozide. With small neuroleptic dosages, it may be possible to lessen involuntary movements without much interference with LD’s antiparkinsonian actions. Another approach to lessen LD-induced dyskinesias has been the use of clozapine. A recent study found that this atypical neuroleptic substantially reduced the amount of time patients spent in a dyskinetic state. Whereas other neuroleptics would antagonize the control of bradykinesia, clozapine does not. Quetiapine also has shown usefulness at lessening adverse effects of LD therapy, such as dyskinesias, but without exacerbating parkinsonism.
Vivid Dreams, Hallucinations, and Psychotic Thinking All forms of dopaminergic therapy, anticholinergics, and amantadine can cause these problems, sometimes in a dose-related manner. A reduction in the amounts of these drugs taken at the end of day can improve quality of sleep by lessening the extent of disruptive dreams or myoclonic jerks. Occasional benign hallucinations or illusions that are not believed (i.e., they are not associated with delusional thinking) may be easily tolerated by some patients. Although these problems can presage the eventual development of more psychotic overtones, some patients may regard benign hallucinations as an acceptable tradeoff for the benefits of the medications. Unlike other neuroleptic drugs,
Often asymptomatic,postural hypotension is seen in patients with PD who are receiving dopaminergic therapy. The extent of postural blood pressure drop can be alarming even if the patient is experiencing no lightheadedness. It may be that, with chronic orthostatic change in blood pressure, the recordings made in the arm cease to represent core blood pressure to the brain. Symptomatic hypotension may be a cause for reduction in the regimen of antiparkinsonian drugs. However, a trial of alternative medications can be undertaken to counter the blood pressure drop. These include salt and water loading, fludrocortisone, midodrine, and indomethacin. Slight elevation of the head of the bed can lessen the diuresis of salt retained during the day. In addition, the more chronic stimulation of the renin-angiotensin system may help to counter any tendency for orthostatic hypotension. RESPONSES TO MEDICATIONS SUGGESTING AN ALTERNATIVE DIAGNOSIS When an LD regimen of 750 mg/day (with carbidopa) has been unable to improve parkinsonism, the problem might be an incorrect diagnosis. Several other neurodegenerative disorders (including progressive supranuclear palsy and the variant forms of multiple system atrophy, including Shy-Drager syndrome and olivopontocerebellar degeneration) have prominent parkinsonism but minimal or no effect from a trial of LD. Because these disorders may be difficult to distinguish from typical PD (especially in their early stages), the failure of response to LD may be the first clue for an alternative diagnosis. Rarely, cases of acquired parkinsonism (such as brainstem or striatal lesions, certain toxic exposures, or increased intracranial pressure) show a response to LD. It is also important to recognize that even in typical PD, features such as resting tremor, micrographia, or imbalance may fail to respond to LD or other medications. COST-EFFECTIVENESS PD medications are expensive burdens for patients and health care systems. Drugs should be reevaluated from time to time to determine whether they are a good value. As mentioned earlier,
756
Movement Disorders
Parkinson’s Disease and Parkinsonian Syndromes
there are several alternative ways to alleviate certain problems in PD therapeutics. For example, although controlled-release LD preparations can offer convenience and more sustained antiparkinsonian effects, their higher cost may lead patients to choose conventional and less expensive immediate-release carbidopa and LD, to be taken more frequently. Dopaminergic ergots can help prevent the wearing-off of LD’s effect (as can selegiline or COMT inhibitors), but sustained-release LD preparations or frequent doses of LD may be more cost-effective for solving this particular problem. Some patients may want to undergo a trial of reducing medication intake to weigh the benefits and costs of therapy. In this way, patients can derive a sense of how much change in disability is achieved from each increment in medication. The question of whether chronic regimens of medications are continuing to help is particularly appropriate for reassessing amantadine. This drug can lose effectiveness over time. Although some patients have continued benefit from 300 mg/day, others achieve the same results with 100 or 200 mg/day. A trial of reducing the dosage of amantadine (over the course of 2 weeks).canbe used to reassess its current value. The same questions can be asked of other adjunctive medications. COMT inhibitors, dopaminergic agonists, and sustainedrelease LD preparations may be helpful against the wearing-off of effect. Sometimes, combination regimen medications have evolved that duplicate each other at targeting the wearing-off problem. Trials of reducing medication intake might reveal the minimum of these drugs needed for adequate symptomatic control. Because patients sometimes do not know whether starting a new medication has actually led to any benefit, a trial reduction might help to clarify this issue. Generic equivalents for Sinemet (carbidopa and LD) and bromocriptine have recently become available in addition to amantadine and LD. These preparations offer substantial savings to patients and are not known to differ in clinical actions from the brand name products.
services. Some patients feel that particular exercise programs have had a major impact on their well-being. Although the best form of exercise varies on the basis of age, level of physical conditioning, and gait or balance disturbance, most patients can benefit from a variety of exercise programs. Patients often need reassurance that the temporary exacerbation of tremor after exercise does not exacerbate the underlying disorder. Depression in patients with PD can be disguised by motor aspects of the disorder (which can also create the image of the disorder by psychomotor retardation and a depressed facial expression). The speech difficulties common in PD can lead to social withdrawal. Encouragement of outlets for communication in support groups, in family discussions, or with mental health professionals is important. Several forms of speech therapy are available, including a program called the Lee Silverman Voice Training Technique. Many patients with PD, like others with physical disability in the golden years of retirement, are extremely frustrated and frightened by the impact of the disorder on their lives. To the extent that unrealistic perceptions of PD govern their thoughts, reassurance of the current status of this disorder is often important. Practitioners should acquaint themselves with studies in which the natural history of PD has been explored because benign outcomes of this disease are well known, and the rate of disability in others can be realistically described. Many patients with PD are alarmed about the possible impact of the disorder on their mind. Although some patients do develop dementia or other types of impairment, many patients have retained full mental capacities even after 10 or more years with the disorder. Patients may need frank assessments of their condition from time to time, not just optimistic reassurance from their physician. Finally, patients can draw a great deal of optimism from the active realm of research into the causes and treatments of PD. For some patients, involvement in clinical trials has helped them to cope with this disorder. Several therapies for extending or augmenting LD effect are currently under development.
SUPPORTIVE SERVICES FOR PATIENTS AND FAMILIES A wide range of information sources and services are available for patients and their families. Several national and statewide PD support organizations provide newsletters, fact sheets, advisory services, and support group meetings. A number of well-written and accurate books describe the experience of living with parkinsonism. Some communities have geriatric services that can be used to great advantageby patients with parkinsonism and their families. Rehabilitation approaches to parkinsonism include gait training, equipping the home for impaired ambulation and balance, and increasing endurance in the face of disabling bradykinesia and other aspects of impaired motor control. Learning tricks to overcome freezing and using walkers or canes to enhance independent ambulation are all reasonable goals for rehabilitation
SUGGESTED READINGS Agid Y, Ahlskog E, Albanese A et ak Levodopa in the treatment of Parkinson’s disease: a consensus meeting. Mov Disord 1491 1-913, 1999 Factor SA, Weiner WJ (eds): Parkinson’s disease: diagnosis and clinical management. Demos, New York, 2002 Goetz CG, Koller WC, Poewe W et ak Management of Parkinson’sdisease: an evidence-based review. Mov Disord 17(Suppl 4):S1-166, 2002 LeWitt PA, Oertel WH (eds): Parkinson’sDisease:The Treatment Options. Martin Dunitz Publishers, London, 1999 Nutt JG, Holford NHG The response to levodopa in Parkinson’s disease: imposing pharmacological law and order. Ann Neurol 39:561-573, 1996 Riley DE, Lang AE: The spectrum of levodopa-related fluctuations in Parkinson’s disease. Neurology 43:1459-1464, 1993
Chapter 117
Surgical Treatment of Parkinson’s Disease
757
1 17 Surgical Treatment of Parkinson’s Disease Drew S. Kern and Rajeev Kumar Surgical treatment for Parkinson’s disease (PD) became popular in the 1950s with the realization that thalamic lesions greatly relieved tremor. However, with the introduction of levodopa in the late 1960s the number of surgeries performed greatly diminished. In the past decade, there has been a reemergence of surgical treatment for PD for several reasons. First, patients have become disabled despite maximal drug therapy from levodopa-induced motor complications including dyskinesias. Second, there is an increased understanding of basal ganglia circuitry and the pathophysiology of PD. This is partially the result of studies using rodent and 1 -methyl+phenyl- 1,2,3,6-tetrahydropyridine (MPTP) nonhuman primate models of PD. Finally, significant advancements in neuroimaging (especially magnetic resonance imaging) and intraoperative electrophysiologic recordings have increased surgical targeting accuracy. The classic model of basal ganglia organization (Fig. 117-1) involves a direct and indirect pathway modulating input received from the cerebral cortex. Dopamine released in the striatum via projections from the substantia nigra pars compacta (SNc) binds to D, and D, receptors. D, receptors are excitatory and stimulate striatal neurons of the direct pathway; conversely, D, receptors are inhibitory, and D, stimulation inhibits striatal neurons of the indirect pathway. Striatal neurons of both pathways use the neurotransmitter y-aminobutyric acid (GABA) but differ in neuropeptide cotransmitters. Stimulation of the direct pathway results in inhibition of the globus pallidus pars interna (GPi) and the substantia nigra pars reticulata (SNr). Stimulation of the indirect pathway reduces inhibitory output from the striatum to the globus pallidus pars externa (GPe), which then inhibits the subthalamic nucleus (STN). The STN contains the only glutamatergic excitatory outputs in the basal ganglia and projects primarily to the GPi and SNr but also sends widespread
FIG. 117-1. Simplified schematic diagram detailing the major afferent and efferent projections of the basal ganglia in healthy normal subjects and in Parkinson’s disease. Thickness of arrows represents relative degree of excitation or inhibition. Black arrows, inhibitory projections; gray arrows, excitatory projections. CPe, globus pallidus pars extema; CPi, globus pallidus pars interna; SNc, substantia nigra pars compacta; SNr, substantia nigra pars reticulata; STN, subthalamic nucleus.
projections to the GPe, pedunculopontine nucleus, striatum, and SNc. The main inhibitory outputs of the basal ganglia are the GPi and SNr, which send inhibitory projections to the brainstem, and the ventral lateral (VL) and ventral anterior (VA) nuclei of the thalamus. Therefore, in normal movement there is activation of the direct pathway and inhibition of the indirect pathway, resulting in VL and VA facilitation of appropriate movement selection via projections to motor cortical association areas including the supplementary motor area. PD is characterized primarily by loss of dopaminergic neurons in the SNc. Therefore, according to the model, the direct pathway is underactive and the indirect pathway is overactive, and there is reduced thalamic facilitation of normal movement. Therefore, surgical treatments that decrease basal ganglia inhibition of the thalamus may alleviate parkinsonism. As a result, neurosurgeons have targeted the hyperactive GPi and STN. The ventralis intermedius (Vim) nucleus of the thalamus receives predominantly cerebellar afferents and is thought to be an important part of the multiple oscillating loops responsible for the generation of tremor. Surgical intervention at this site may interrupt its rhythmic firing and improve tremor. This model of basal ganglia circuitry has several anatomic and functional inadequacies. Studies using retrograde tracers have identified extensive branching of striatal axons to multiple projection sites, unlike the model that suggests few specific projection sites. Furthermore, there are many inputs from regions other than the basal ganglia received by the STN that have not been addressed. These structures can profoundly influence function and include the cerebral cortex, the centromedian nucleus and parafascicular nucleus of the thalamus, and the pedunculopontine nucleus. Supporting evidence for this observation comes from rat models that report only a 20% increase in STN
758
Movement Disorders W Parkinson’s Disease and Parkinsonian Syndromes
neuronal firing after GPe lesioning. The model also predicts that lesions of the GPi should amplify levodopa-induced dyskinesias, but in clinical practice they are relieved. Although understanding of basal ganglia function has improved in the past decade, there are clear gaps in our knowledge that are being critically investigated.
PATIENT SELECTION Selecting appropriate patients for surgery typically involves a team consisting of a movement disorder neurologist, a functional neurosurgeon, and a neuropsychologist. The role of the neurologist is to ensure that the diagnosis is correct and that all nonsurgical treatments have been used. Confirmation of PD as the diagnosis, as opposed to an atypical parkinsonian syndrome (such as multiple-system atrophy or progressive supranuclear palsy), is extremely important. The neurosurgeon evaluates the patient’s general health with respect to the risks of surgery and frankly discusses with the patient the potential complications of surgery including intracerebral hemorrhage, which could result in serious neurologic disability or death. The neuropsychologist performs an in-depth cognitive examination to determine whether there are any signs of dementia and interviews the patient and caregiver to determine whether there are behavioral abnormalities such as anxiety, depression, or other psychiatric symptoms. There are no well-established criteria for surgery that predict both efficacy and adverse effects; however, some basic guidelines adopted by many surgical teams exist. In general, appropriate candidates for surgery lack significant cognitive impairment or unstable medical problems and have substantial disability in performance of activities of daily living (ADL) caused by marked motor fluctuations and levodopa-induced dyskinesias despite optimal medical therapy. Patients who are cognitively impaired or have excessive anxiety are poor candidates for surgery because of their inability to provide useful intraoperative feedback, difficulty with postoperative management (specifically in programming deep brain stimulation), and increased risk of worsening their preexisting cognitive deficits. Other contraindications include severe uncontrolled hypertension, cancer, or cardiac, renal, hepatic, or pulmonary diseases. Patients must have emotional support available from family or other caregivers. Postoperatively, there may be a difficult adjustment period associated with the new role of the patient being less dependent on others because of marked improvement of parkinsonian disability. Caregivers must
W TABLE117-1.
also help patients attend multiple deep brain stimulation (DBS) programming visits (often after overnight drug withdrawal). Table 117-1 lists the major criteria and predictors to be considered when selecting patients for surgery. The degree of improvement obtained with a supramaximal dosage of levodopa after overnight withdrawal of antiparkinson medication is highly predictive of the response to STN DBS and probably also to pallidal interventions. With the exception of tremor, signs that are not improved with levodopa fail to improve with surgery and include cognitive and psychiatric problems, on-period freezing, and levodopa-refractory dysarthria, dysphagia, and postural instability. Furthermore, the levodopa test reinforces for the patient and family realistic expectations of the results of surgery. Determining the appropriate timing of surgery can be difficult because surgery for PD is elective and is undertaken to improve patient’s quality of life. The patient and the physician should frankly compare the potential for significant improvement and potential adverse effects of more aggressive drug therapy compared with surgery. Many factors must be considered in this decision, including the patient’s personal, professional, and social situation. Regardless, surgery should not be unnecessarily delayed until the patient loses his or her job or there is a significant decrease in independence and loss of quality of life.
ABLATION AND DEEP BRAIN STIMULATION The two most widely used surgical techniques are ablation and DBS. Both procedures produce similar results despite fundamental methodologic differences. There are three major surgical sites for intervention: the Vim nucleus of the thalamus, the GPi, and the STN. The initial surgical method for both ablation and DBS is similar and involves neuroimaging (computed tomography or magnetic resonance imaging) with a stereotactic headframe in place and then physiologic confirmation of the target site using intraoperative stimulation or recording techniques. Thereafter, either a radiofrequency lesion (ablation) or a permanently implantable electrode (for DBS) is placed at the target site. Systematic complications of stereotactic surgery include a 1% to 2% probability of symptomatic hemorrhage per side operated, resulting in permanent neurologic deficit or death. The equipment for DBS includes a quadripolar electrode implanted into the brain and held stationary by fixation to the skull. The electrode lead is connected to a cable that runs under
Selection Criteria for Surgery in Parkinson‘s Disease
Inclusion Criteria
Exclusion Criteria
Significant impairment of ADLs and quality of life caused by motor fluctuations and levodopainduced dyskinesias despite maximal drug therapy Physically healthy with potentially a long life expectancy after surgical treatment Physical and mental stamina to provide feedback during a lengthy operation Understand risks of surgery Preoperativeand postoperative emotional S U D D O ~ ~
Significant cognitive impairment Uncontrolled cardiac, renal, hepatic, or pulmonary disease, cancer, or hypertension Significant psychiatric illness including anxiety, mood disorders, and severe depression Marked cerebral atrophy or extensive white matter T2 signal changes
Predictive Factors for Good Outcome Shorter duration of disease Younger patients Very high degree of improvement of parkinsonism with levodopa
Predictive Factors for Poor Outcome Unrealistic expectations, such as a belief of being cured Presence of levodopa-refractory features of parkinsonism (with the exception of tremor)
Chapter 117
FIG. 117-2. DBS hardware as implanted in a patient.
the scalp and skin of the neck and connects to a pulse generator placed subclavicularly (Fig. 1 17-2). Stimulation settings are adjusted by means of a transducer placed on the skin overlying the pulse generator. The following stimulation parameters are adjustable: frequency (100 to 185 Hz is most effective), pulse width (typically 60 to 120 pV), voltage (usually 1.0 to 3.6 V), and stimulating contacts (monopolar or bipolar stimulation). The clinical effects of DBS result from a combination of the microlesion caused by electrode implantation alone (minor effect that often gradually disappears as perielectrode edema resolves postoperatively) and stimulation (major effect). The mechanism of DBS is unknown, but similarity to the clinical effects of ablation suggests that DBS may be inhibitory. It has been suggested that DBS may activate local inhibitory interneurons. Another possibility is that of neuronal jamming, whereby activation of fibers transfers nonphysiologic and incomprehensible messages to downstream target nuclei, which are then disregarded. DBS has many advantages over ablation. Electrode implantation causes fewer permanent neurologic complications because less brain tissue is destroyed than in ablation because radiofrequency lesions may be inadvertently expanded or misplaced to involve important structures adjacent to the intended target. In addition, autopsy studies suggest that long-term continuous
W
Surgical Treatment of Parkinson's Disease
759
stimulation does not cause significant anatomic damage to adjacent brain tissue. The effects of DBS are reversible, with symptoms returning to preoperative levels when stimulation is stopped. The hardware can also be removed at any time if indicated. In contrast, the effects of ablation are irreversible and not adjustable without additional surgery, which may occasionally be needed to expand an inadequate lesion. With DBS, stimulation parameters can be fmely adjusted to maximize beneficial results and minimize adverse effects caused by current spread to adjacent structures. Finally, the electrodes can be surgically repositioned if they are initially suboptimally situated. Ablation also has advantages over DBS. Ablation and electrode implantation are performed with the patient awake; however, DBS entails additional surgery performed under general anesthesia to implant the pulse generator and connector wire. Furthermore, the pulse generator must be surgically replaced every 3 to 7 years because of battery drainage. Several visits typically are necessary after electrode implantation to adjust the stimulation parameters, especially for patients undergoing GPi or STN DBS, whereas minimal follow-up is needed after ablation. With DBS, approximately 25% of patients experience hardware complications within 2 to 3 years postoperatively. The most notable complications involve mechanical hardware breakage and skin erosion over the hardware (which may be associated with cutaneous infection). These problems usually involve the peripheral components and necessitate replacement of damaged or infected hardware and sometimes treatment with antibiotics. In patients with severe postural instability and frequent falls, ablative surgery may be a better choice because falls may damage or displace DBS hardware. DBS is also a very expensive procedure, with the hardware alone costing approximately $20,000. Therefore, in many areas of the world, lesioning procedures are the only affordable surgical option. THALAMlC SURGERY
Lesions of the Vim (thalamotomy) and thalamic DBS are effective in markedly reducing or eliminating severe tremor and may diminish rigidity and levodopa-induced dyskinesias contralateral to the surgical side, but they do not improve other features of PD such as bradykinesia and gait disorders (Table 117-2). Reports of improvement in bradykinesia probably are artifactual and reflect reduction of tremor that interferes with evaluation of bradykinesia. Unilateral ablation and DBS predominantly improve contralateral tremor. Tremor is also slightly reduced ipsilaterally with thalamic DBS. Therefore, patients with severe bilateral tremor
TMLE 117-1. Effects of Unilateral and Bilateral Ablation and DBS of Vim Nucleus, CPi, and STN in Patients with Parkinson's Disease BILATERAL
UNILATERAL
Vim Motor UPDRS off Motor UPDRS on ADL UPDRS off ADL UPDRS on Dyskinesiason Medication dosage
10%-30% -10% No change No change No change No change
GPi
-30% No change -30% -30%
-75% No change
Vim
STN
25%-50% 0%-39% -30% -30% No change
-
No change No change
GPi
30%-50% -25% 30%-40% 3 w 0 % 80%-100%
No change
sm -50% -25% 30%-50% 20%-30% 60%-1ooorb 50%-100%
Percentages representaverage reduction in standardized rating scale scores, symptoms, and drug dosage comparedwith baseline measurementsfor combined unilateral or bilateral surgery (ablation or DBS). Dashes indicate no reported data. All percentagesrepresent average reductionsat 6-12 months postoperatively."ow'represents assessments scored after overnight drug withdrawal, and "on" indicatesscores with drug treatment Abbreviobbns: ADL activitiesof daily living; DBS, deep brain stimulation; CPi, globus pallidus pars interna; STN, subthalamic nucleus; Vim, ventralis intermedius.
160
Movement Disorders
w
Parkinson’s Disease and Parkinsonian Syndromes
benefit most from bilateral procedures. Bilateral thalamotomy is associated with a high incidence of severe dysarthria and adverse cognitive effects, whereas these complications are avoided with bilateral thalamic DBS or unilateral thalamic DBS performed contralateral to a previous thalamotomy. Mild paresthesias usually affecting the contralateralhand or face occur in most patients with unilateral or bilateral thalamic DBS. Mild dysarthria and dysequilibrium are more common with bilateral than with unilateral thalamic DBS and occur in 10% to 30% of patients. All of these side effects usually are easily managed by stimulation adjustments and are outweighed by marked bilateral tremor reduction. Thalamic DBS more effectively reduces rest than action tremor and distal limb greater than proximal limb or axial tremor. Certain skills that may be impaired by tremor in PD such as handwriting are improved, but ADL scores are not substantially improved because the greatest sources of disability in PD are bradykinesia and gait disorders. Head and voice tremor is also markedly relieved after bilateral thalamic DBS but is improved much less with only unilateral thalamic DBS. Long-term data indicate sustained reduction of tremor beyond 1 year, although stimulation intensity often may need to be increased with disease progression. Left thalamic DBS may slightly reduce lexical verbal fluency, but otherwise thalamic DBS has not been reported to significantly impair cognition. Schuurman et al (2000) recently reported a randomized, controlled trial comparing unilateral thalamotomy and unilateral thalamic DBS in patients with PD, essential tremor, and multiple sclerosis. Efficacy in controlling contralateral limb tremor was similar as measured 6 months postoperatively;however, thalamotomy was associated with a higher rate of complications, which reduced the overall functional improvement in patients treated with this therapy. In the thalamotomy group, 11 of 23 patients experienced complications, compared with only 2 of 21 patients who received thalamic DBS. Dysarthria was common with both thalamotomy and thalamic DBS, whereas cognitive deterioration, hypesthesia, gait or balance disturbances, and arm ataxia were unique to thalamotomy. Adverse effects in the DBS group were minimized by the adjustability of stimulation. Historical reports suggest that approximately 60% to 80% of patients who receive unilateral thalamotomy experience transient side effects lasting up to 1 week, including facial or arm paresis, arm ataxia, confusion, dysarthria, gait disturbances, or memory impairment. Furthermore, 20% to 45% of thalamotomy patients have persistent adverse effects lasting at least 6 months after surgery. We have observed that many patients who initially underwent thalamotomy or thalamic DBS for treatment of tremor have subsequentlyneeded GPi or STN surgery to treat other symptoms, such as bradykinesia, gait disorder, and levodopa-induced dyskinesias, which have become more pronounced with progression of PD. Furthermore, STN DBS seems to reduce tremor as effectively as thalamic surgery. Therefore, thalamic procedures can no longer be recommended as a treatment for patients with PD, and we advocate GPi or STN surgery as the initial surgical procedure in patients with severe medication-refractory tremordominant PD. PALLIDAL AND SUBTHALAMIC SURGERY STN and GPi surgery improve all cardinal features of PD, including tremor, bradykinesia, rigidity, and levodopa-induced dyskinesias; however, there are significant differences with respect to clinical and adverse effects.
The preferred site for GPi lesioning (pallidotomy) is the posterior and ventral portion of the GPi (sensorimotor portion), which contains cells that fire in relation to movement. Gross et al (1999) have reported a relationship between ablation site in this region and improvement of various features of parkinsonism: Centrally located lesions maximally improve bradykinesia, postural instability, and gait; anteromedial lesions improve rigidity and contralateral levodopa-induced dyskinesias most; and posterolateral lesions have the greatest effect on tremor. Furthermore, anteromedial lesions may impair cognition and memory, whereas posterolateral lesions lead to improvement on neuropsychological measures. Therefore, most investigatorsbelieve that it is important to completely lesion the sensorimotor portion of the GPi (posterior, ventral, and lateral) while avoiding nonmotor associative regions (anteromedially)and other adjacent structures that if lesioned result in cognitive and motor complications. Unilateral pallidotomy improves off-drug parkinsonian motor signs approximately 30% (50% contralaterally) and largely abolishes contralateral levodopa-induced dyskinesias. Although contralateral improvements may be sustained up to 5 years, ipsilateral and axial improvement in parkinsonism is lost by 1 year postoperatively, and improvement in ipsilateral dyskinesias is lost between 1 and 2 years after surgery. As a result, off-drug ADL scores are improved by 30% for up to 2 years. Unfortunately, patients tend to return to levels of dependence comparable to baseline between 2 and 5 years postoperatively. Unilateral pallidotomy reduces motor fluctuations and time spent in the off state for up to 2 years. On-period motor scores are not significantly improved, and antiparkinson medication usually cannot be reduced after unilateral pallidotomy. Nevertheless, on-period ADL scores are improved, probably by reduction of levodopa-induced dyskinesias (Table 117-2). Adverse effects related to unilateral pallidotomy that generally subside within the first 2 weeks postoperatively include dysarthria, impaired balance, and confusion. Transient contralateral facial weakness and bulbar dysfunction are also common and may persist in 2% to 3% of patients. Visual field deficits, specifically homonymous superior, central, and inferior quadrantanopias contralateral lesions that are extended into the optic tract, are present in small percentage of patients. Right hemisphere lesions are associated with impairment in visual learning, including difficulty drawing complex shapes; however, these adverse effects generally resolve by 6 months postoperatively. In comparison, left pallidotomy may mildly impair verbal learning (specifically verbal memory, working memory, initial encoding, and delayed free recall) with measurable deficits persistent beyond 12 months postoperatively. In rare instances, behavioral changes that range from loss of social interaction to impulsivity and poor judgment can also persist after surgery. Bilateral pallidotomy compared with unilateral pallidotomy results in 10% to 25% greater improvement of off-period parkinsonism and almost complete elimination of all levodopainduced dyskinesias. Although bilateral pallidotomy may be performed without complications, several case reports suggest that bilateral pallidotomy often may be accompanied by dysarthria and dysphagia, possibly because of inadvertent lesioning of the corticobulbar tracts. Furthermore, severe global cognitive decline and a disabling dysexecutive and obsessive-compulsive disorderlike psychiatric syndrome have been reported, possibly caused by the lesions encroaching on nonmotor anteromedial portions of the pallidum. Therefore, bilateral pallidotomy cannot be routinely
Chapter 11 7
recommended as a treatment for PD. Useful alternatives include unilateral pallidotomy with contralateral GPi DBS or bilateral STN or GPi DBS because DBS yields similar results with fewer persistent complications. Only a few small case series have been reported detailing the effects of STN lesioning (subthalamotomy). Historically, STN lesioning was thought to be associated with a high risk of hemiballism. However, recent studies indicate that this complication rarely occurs in PD because it is likely that the parkinsonian state protects against the development of hemiballism. Compared with unilateral pallidotomy, unilateral subthalamotomy results in greater reduction of motor UPDRS scores in both on and off states. In addition, the need for antiparkinson medication is reduced. These improvements are sustained for at least 2 years. Bilateral subthalamotomy may result in greater improvement than unilateral subthalamotomy. Preliminary data indicate a 57% improvement in motor UPDRS scores and 50% to 100% reduction of drug therapy. Although transient dyskinesias are common, no permanent dyskinesias has been reported. There are few data on the adverse effects of this procedure, but left-sided lesions may be more apt to impair verbal memory than right-sided lesions. The reported overall clinical effects of unilateral GPi and STN DBS are extremely similar to those reported with lesioning of the anatomic sites (Table 117-2). Unilateral S T N DBS should be undertaken with some caution because the need to reduce antiparkinson medication may lead to a lopsided effect, with the ipsilateral side of the body being undertreated. Nevertheless, in very asymmetrical tremor-dominant patients, we have been able to successfully apply this intervention without complications. Bilateral GPi and STN DBS demonstrate similar overall motor effects. Off-period motor and ADL UPDRS scores and levodopainduced dyskinesias are markedly improved, there may be slight improvement in on-period UPDRS motor scores, on-period ADL scores are modestly improved, and motor fluctuations are dramatically reduced. Most reports suggest that the benefits of bilateral STN DBS are maintained for at least 2 years. There are few data on the long-term effects of bilateral GPi DBS; however, some case series suggest a significant deterioration after 1 or 2 years. Some patients have subsequently undergone bilateral STN DBS with marked and sustained improvements 6 months postoperatively (Table 117-2). Although both STN and GPi DBS reduce dyskinesias, the mechanism of improvement differs. STN stimulation has a pronounced antiparkinsonian effect and may induce dyskinesias or reduce the threshold for levodopa-induced dyskinesias. As a result, antiparkinson medication must be reduced to reduce dyskinesia. On average, patients are able to reduce drug therapy by 50%, and 10% to 20% of patients are able to stop all drug therapy for at least 1 year with elimination of all motor fluctuations. Stimulation of the globus pallidus has location-specific effects. Stimulation of the ventral GPi suppresses levodopa-induced dyskinesias and improves rigidity but blocks the beneficial effects of levodopa on bradykinesia and gait. Stimulation of the dorsal globus pallidus (probably GPe) improves bradykinesia and rigidity but may induce dyskinesias. Therefore, stimulation in the middle of the pallidum is the optimal location because this allows one to obtain improvement in parkinsonism and direct dyskinesia suppression. However, as with pallidotomy, antiparkinson drug therapy usually is not altered. Although there has been no large randomized study comparing GPI with STN DBS, some data suggest that STN DBS may be superior. As mentioned earlier, STN DBS allows marked reduction
Surgical Treatment of Parkinson's Disease
761
or discontinuation of antiparkinson medication, which is largely unchanged with GPi DBS. Furthermore, STN stimulation uses less battery power because of lower stimulation parameters probably because the STN is a smaller target than the pallidum. This results in fewer surgeries to replace the battery and, as a result, less cost. The STN may be an easier surgical target because it is more clearly identified by magnetic resonance imaging. Despite these advantages, STN DBS necessitates more frequent follow-up visits with complex postoperative management of medication and other problems, including stimulation-induced dyskinesias, mood changes, stimulation-induced dysarthria, and sialorrhea. The majority of adverse effects of bilateral GPi and STN DBS are transient, occurring as the optimal stimulation parameters are adjusted. Stimulation-induced adverse effects with GPi DBS include paresthesias and tonic motor contraction caused by internal capsule stimulation and nausea and phosphenes with stimulation of the optic tract. Bilateral GPi DBS has been reported to be cognitively well tolerated, although lexical fluency may be reduced. STN stimulation induces dyskinesias in most patients with optimally placed electrodes and pretarsal blepharospasm (often necessitating treatment with botulinum toxin injection) in 10% to 20% of patients. Involuntary laughter, mania, and hypersexuality have been rarely reported, possibly caused by stimulation of nonmotor limbic portion of the STN. In addition, severe acute depression may be induced with inadvertent stimulation of the SNr, inferior to the STN. Levodopa has significant psychotropic effects in many patents with PD, and its withdrawal may occasionally result in abulia, anhedonia, or depression or unmask restless legs syndrome. In younger cognitively intact patients, STN DBS is extremely well tolerated, slightly impairs lexical fluency, and may actually improve working memory. However, in older patients (especially those with borderline cognitive function), a variety of cognitive processes reliant on intact frontostriatal circuitry may be significantlyimpaired in the worst cases, lending to a mental state comparable to progressive supranuclear palsy. HUMAN FETAL TRANSPLANTATION There have been several clinical studies involving human fetal transplantation in the past decade. Transplanted fetal mesencephalic tissue can produce large amounts of dopamine, establish connections and integrate into the denervated host striatum, and improve parkinsonism. Of historical interest only is autogenous adrenal medullary cell transplantation; however, poor benefit and high morbidity and mortality led to the abandonment of this treatment in the 1980s. Results of the various open label unilateral and bilateral transplantation studies are difficult to interpret because of methodologic differences between studies including amount of fetal tissue implanted (1 to 4 fetuses per side), age of fetus (5 to 17 weeks postconception), use (or nonuse) of immunosuppressive drug therapy, and graft site (putamen, caudate, or both). With unilateral transplantation, contralateral motor symptoms in the off state improve by 10% to 50%, and time spent in the on state without dyskinesias increases by 0% to 65%; however, ipsilateral symptoms are not reduced. Bilateral transplantation can safely be performed and reduces total UPDRS scores (motor and ADL) 18% to 50%, and the need for drug therapy may be reduced. Long-term evaluations of transplantation indicate sustained survival of grafted neurons assessed by PET scans and autopsies. Furthermore, improvement of off-period parkinsonism may be sustained
762
Movement Disorders
w Parkinson’s Disease and Parkinson-likeSyndromes
for 10 years after bilateral or unilateral transplantation. The greatest risks of transplantation are intracerebral hemorrhage and infection caused by immunosuppression therapy. Additional complications that have been reported include depression, panic disorders, transient confusion, and hallucinations. Freed et al (2001) recently reported a double-blind sham surgery study of bilateral putaminal implantation. At l-year postoperatively there was no significant difference in UPDRS scores between those receiving real and sham surgery. However, motor and ADL UPDRS scores improved in patients younger than 60 years old receiving transplantation, although tremor and freezing of gait was not improved. Between 1 and 2 years postoperatively, further improvements in off-period parkinsonism in this patient cohort have been noted in patients of all ages. As in STN DBS, these improvements have correlated with the degree of preoperative levodopa responsiveness; however, the reliability and magnitude of the improvement have not been as great as those seen with STN DBS. Freed et al (2001) also reported off-state or “runaway” dyskinesias in several of their bilaterally transplanted patients with the best improvement of parkinsonism. Another group using different transplantation methods has also recently reported this worrisome complication, although this group found no correlation between the improvement in parkinsonism and the development of off-phase dyskinesias. Off-period dyskinesias originally were attributed to excessive growth of grafted dopaminergic neurons; however, a recent study indicates that fluorodopa uptake does not correlate with off-period dyskinesias. The mechanism of off-period dyskinesias is unknown and warrants further study. In several patients dyskinesias have been troublesome enough to necessitate specific antidyskinetic drug therapy or pallidal surgery. Typically, transplantation of 3 to 4 fetuses per putamen (or 6 to 8 donors per patient) are necessary to obtain adequate symptomatic relief despite recent developments in drug technology (such as lazaroid tirilazad) that increase the survival rate of transplanted dopaminergic neurons. The ethical issues surrounding this treatment, the large amount of fetal tissue needed to treat one patient with PD, and the difficulty in obtaining donor tissue make it unlikely that this treatment will ever become widespread. Nevertheless, this experience has paved the way for transplantation of dopaminergic neurons obtained from other, more readily available sources. DWELOPMENT OF NOVEL SURGICAL APPROACHES A number of novel surgical interventions are being investigated as treatments for PD. Retinal pigment epithelial cells produce DOPA as an intermediate during eumelanin production. One eye may provide enough dopaminergic cells for transplantation to treat hundreds of patients, and this source is readily obtainable from cadavers. A pilot study of 6 patients who underwent unilateral transplantation demonstrates 30% to 48% improvement in off-period parkinsonism 12 months postoperatively. Stem cells are pluripotent cells that may be obtained from blastocyst-stage embryos and even from adults (with bone marrow stromal cells being the most promising candidate). Once obtained, these cells may be replicated in culture and then driven to differentiate into a
dopaminergic phenotype by application of different growth factors. Large numbers of cells may then be obtained for transplantation. Recent work has demonstrated survival, integration into the host, and reversal of a rodent model of parkinsonism after transplantation. The use of neurotrophic factors has also been explored in PD. Glial cell line-derived neurotrophic factor (GDNF) promotes the sprouting of dopaminergic terminals, increases dopamine production from existing neurons, and prevents nigrostriatal tract degeneration. Although intracerebroventricular injection of GDNF in rodent and nonhuman primate models of PD demonstrates sprouting of neurons and improvement in motor symptoms, a phase 1 and 2 human clinical trial resulted in a high incidence of adverse effects and no clinical improvement. However, a small open label pilot study of direct intrastriatal GDNF infusion has reported remarkable benefits without the adverse effects seen in the intracerebroventricular injection study. Multiple vector systems derived from viruses or liposomes can deliver genes that express trophic factors, such as GDNF. Direct injection of a lentiviral vector to deliver GDNF in a nonhuman primate model of PD has been demonstrated to result in long-term GDNF gene expression and marked improvement of parkinsonism. If successful in human PD and if a system whereby GDNF production could be regulated is developed, this therapy may be superior to most other surgical interventions currently under study. In the past decade, there have been rapid advances in our understanding of the pathogenesis of PD. It is likely that current surgical treatments of PD will be replaced in the next decade by new restorative therapies. Furthermore, as the roles of the various genetic and environmental contributions to PD pathogenesis are identified, it is likely that curative or preventive therapy using genetic engineering techniques will be developed. SUGGESTED READINGS Alvarez L, Macias R, Guridi J et al: Dorsal subthalamotomy for Parkinson’s disease. Mov Disord 16:72-78, 2001 Deep-Brain Stimulation for Parkinson’s Disease Study Group: Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med 345:956963,2001 Fine J, Duff J, Chen R et al: Long-term follow-up of unilateral pallidotomy in advanced Parkinson’s disease. N Engl J Med 342:1708-1714, 2000 Freed CR, Greene PE, Breeze RE et al: Transplantation of embryonic dopamine neurons for severe Parkinson’s disease. N Engl J Med 334710-719,2001 Gross RE, Lombardi WJ, Lang AE et ak Relationship of lesion location to clinical outcome following microelectrode-guided pallidotomy for Parkinson’s disease. Brain 122:405-416, 1999 Kordower JH, Emborg ME, Bloch J et ak Neurodegeneration prevented by lentiviral vector delivery of GDNF in primate models of Parkinson’s disease. Science 290767-773, 2000 Kumar R, Lozano AM, Kim YJ et ak Double-blind evaluation of subthalamic nucleus deep brain stimulation in advanced Parkinson’s disease. Neurology 51:850-855, 1998 Parent A, Cicchetti F: The current model of basal ganglia organization under scrutiny. Mov Disord 13:199-202, 1998 Schuurman PR, Bosch DA, Bossuyt PMM et al: A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. N Engl J Med 342:461-468, 2000
Chapter 118
Mental Changes in Parkinson’s Disease
763
118 Mental Changes in Parkinson’s Disease Joseph H. Friedman
A number of behavioral abnormalities occur in Parkinson’s disease (PD) that contribute significantly to morbidity and greatly complicate its management. Although it is clear that these conditions are more common in patients with PD, it is not clear whether they are intrinsic to the pathologic process itself or are a response to living with an incurable, progressive, disabling condition. Dementia is more common in patients with PD than in age-matched controls. It usually occurs after several years of the illness and correlates with disease severity; ultimately it affects about 30% of patients. Other common mental changes include the following:
Depression occurs in about 50% of patients with PD and is medication responsive. Fatigue is a major problem in 30% of patients with PD, correlating better with depression than disease severity and often predating diagnosis. Sleep disorders are very common, manifested mainly as difficultystaying asleep and falling back to sleep once awake, leading to daytime somnolence and sleep fragmentation. Vivid dreams and yelling in sleep are very common. REM behavior disorder is a rare disorder in the general population but not uncommon in PD in both treated and untreated patients and may predate onset of the motor signs of PD. Visual hallucinosis occurs in 20% to 30% of drug-treated patients. Psychosis occurs in 5% to 10% of drug-treated patients.
DEMENTIA Patients with PD are subject to the same dementing illnesses as other people. Dementia of the Alzheimer’s type, vascular dementia, and other conditions presumably develop at the same rate as in an age-matched population without PD. Although there is speculation that Alzheimer’s disease and PD may have a clinical and pathologic relationship, presumably they are somewhat different phenomenologically. Patients with PD develop a dementia that is thought to be part of their primary PD pathology. Mild dementia can be difficult to recognize in PD because of the confounding effects of motor dysfunction and medication. The DSM-IV criteria defining dementia are difficult to apply strictly to PD. There is no specific “Parkinson’s dementia.” Pathologically, there is a large overlap among PD with dementia, Alzheimer’s disease, and diffuse Lewy body disease. Similarly, there is a large overlap among the clinical aspects of all of the dementias. Although one can statistically discriminate discrete populations having a “subcortical” dementia, characterized by deficits in memory, ordering, verbal fluency, problem solving, and visual perception tasks, from those with a “cortical” or Alzheimer’s-type dementia, with memory problems, aphasia, agnosia, or apraxia,
individual cases often are more difficult to categorize because patients often have both cortical and subcortical problems. It is possible that the subcortical type of dementia in PD is more slowly progressive than dementia of the Alzheimer’s type, but this is unknown. Cholinesterase inhibitors enhance memory in patients with dementia of Alzheimer’s type but have not been adequately tested in the dementias of PD. Theoretically, the cholinergic drugs may worsen the cholinergic-dopaminergic imbalance in PD, leading to worsening motoric dysfunction, and should therefore be used cautiously in patients with PD. Worsened motor function should reverse upon drug discontinuation, however, so this is not a risky undertaking.
DEPRESSION The incidence of depression is also higher in PD than in the general population. Whether this is intrinsic to the disease or reactive is debated. Most studies have demonstrated a higher rate of depression in PD than in age-matched controls, but one often-cited study found no difference in prevalence between patients with PD and a cohort matched for disability with rheumatoid arthritis. Some data suggest that the quality of depression in PD is somewhat different from that in idiopathic depression, with fewer suicide attempts and fewer feelings of guilt and failure but with more irritability and pessimism about the future. Regardless of the epidemiology or theoretical aspects of depression, each patient must be approached individually. Recognizing depression may be difficult. Because interpreting the affect of most patients with PD is problematic, it takes experience or long-term knowledge of the patient to use facial expression,speech changes, and interactive style as a guide. Occasional patients complain that others think that they are depressed or angry when they are not, because of the masked facial expression. Loss of motivation, feelings of sadness, loss of appetite, loss of libido, and anhedonia are the symptoms most important to evaluate. Fatigue, sleep disturbances, declining social interactions, and weight loss, which suggest depression in patients without PD, are so common in nondepressed patients with PD that although they are more common in depressed patients with PD, they are not good guides to the diagnosis of depression. Depression also must be distinguished from apathy, which is often present with dementia and probably is untreatable. Apathy may be seen in PD without dementia but is not common. A person with advanced PD may be unable to do much for enjoyment and may be resigned rather than apathetic or depressed. Complicating the diagnosis of depression is the possibility that the patient will deny feeling depressed even when depression is present. Information from family members can be very helpful in making the diagnosis. Treating depression in PD is made difficult by the frailty of the patients and the common problem of drug intolerance, especially
764
Movement Disorders W
Parkinson’s Disease and Parkinson-like Syndromes
in patients already taking several psychoactive medications. There have been at least five double-blinded placebo-controlled trials of different antidepressantsin PD, all finding the drugs to be effective in ameliorating depression and some noting concomitant improvement in parkinsonism. There are no studies comparing one antidepressant to another. It appears that antidepressants are as effective in treating depression in PD as in the population without PD. Therefore, the choice of drug should depend on the individual patient and the physician’s degree of comfort with the various medications. Coexisting problems that may help guide an antidepressant drug choice include drooling, prostatism, urinary urgency, insomnia, daytime somnolence, confusion, dementia, cardiac rhythm abnormalities, and orthostatic hypotension. Tricyclics are useful for a patient who may benefit from an anticholinergic agent, especially if insomnia is present. A patient who drools and has tremor or a spastic bladder may experience improvement in affect from the antidepressant actions of a tricyclic such as amitriptyline or imipramine and physical improvement from the anticholinergic side effects. A patient with insomnia and anxiety may respond better to a sedating drug such as trazodone, nefazodone, or mirtazapine. The new serotonin reuptake blockers are thought to be activating and may help patients with excessive somnolence and inertia during the day. They also have few side effects and are well tolerated in general. They should be given in the morning, unlike the other antidepressants, which are usually given at night to avoid inducing or exacerbating insomnia. The serotonin reuptake inhibitors can cause restlessness or akathisia and on rare occasion may induce or worsen parkinsonism. Therefore, some PD experts do not use these drugs as first line antidepressants. Members of the Parkinson Study Group were evenly split on this question. The selective serotonin reuptake inhibitor antidepressants may interact with selegiline, the monoamine oxidase-B (MAO-B) inhibitor, to cause a “serotonin syndrome.” This is undoubtedly rare. There is some confusion regarding selegiline and depression, with some believing it has antidepressant properties. This occurs only at dosages high enough to make the drug a nonselective MAO-A and MAO-B inhibitor and therefore a drug with the same potential for hypertensive crises as phenelzine and tranylcypromine. Electroconvulsive therapy is another option for treating depression in PD and probably is underused. Electroconvulsive therapy is generally recommended for patients who are either refractory to antidepressant medications or who cannot tolerate them. Electroconvulsive therapy has a beneficial effect on the motor aspect of PD independent of its effect on mood. The motoric benefit usually lasts days to weeks but can last longer. About 75% of electroconvulsive therapy-treated patients with PD improve motorically, and a higher percentage improve psychiatrically. After electroconvulsive therapy for depression, oral antidepressants are still needed, but at lower dosages to maintain a patient in remission than to achieve remission. There is scant data on maintenance electroconvulsivetherapy in PD. ANXIETY, OBSESSIVE-COMPULSIVE TRAITS, AND FATIGUE Anxiety and obsessive-compulsive personality traits may be more common in PD. These conditions do not correlate with disease severity. Data are sparse. Shulman et al. have described the syndrome of “inner tremor,” when patients feel tremulous but are
not. This feeling correlated with anxiety and was unrelated to visible tremor or PD severity. Anxiety may respond to the selective serotonin reuptake inhibitor antidepressants and to the usual anxiolytics. Fatigue is another common problem that does not correlate with disease severity. It is a complicated symptom that includes sleepinessas well as physical, emotional, and mental fatigue. About 50% of patients with PD at all levels of disease severity describe it as one of their three worst symptoms. DRUG-RELATED MENTAL EFFECTS The mental side effects of the antiparkinsonian drugs are legion. Sleepiness, mania, hypersexuality, confusion, personality changes, visual hallucinosis, vivid dreams, psychosis, and even depression itself have been reported as drug effects. These problems occur in a large percentage of patients. Older patients, especially demented ones, are more likely than others to experience mental side effects. The anticholinergic drugs, such as trihexyphenidyl and benztropine, are so likely to cause mental side effects, particularly memory loss, confusion, and hallucinations, that they should be used extremely cautiously in older adults and almost never in demented patients. Sleep Disorders
Levodopa and the dopamine agonists often cause various sleep abnormalities. The most common are vivid dreams and sedation. Patients report dreams so realistic that only their content reveals to the patient that the phenomena experienced were dreams and not reality. In the case of the confused patient, the dream often is mistaken for reality. In patients who are slightly demented, the vivid dream sometimes is interpreted as real when the content is believable (for example, that a car accident had occurred during the night on the street in front of the house). More confusing to the patient is waking up in the middle of a dream, thinking it is real, and waking the spouse. It is important to distinguish dream phenomena from confusion because the former usually can be treated simply with an explanation and reassurance, whereas the latter requires a reduction in PD medications. Patients with PD often yell, laugh, curse, or scream in their sleep. This is almost always a problem for the spouse or the rest of the household and not for the patient because it causes awakening only uncommonly. Equally problematic are the almost as common jerking, hitting, and kicking that occur during sleep, again without awakening the patient. A less common phenomenon is FEM behavior disorder, in which patients sometimes are not hypotonic during E M sleep and act out their dreams, leading to falls and family complaints about nocturnal confusion. This occurs when the dream involves the patient defending himself or his spouse from attack. Often the patient is actually hitting the spouse. This syndrome may predate the onset of the motor signs of PD. Therefore, it is important to take a complete history about altered behavior because episodic behavioral alterations may turn out to be benign drug effects on sleep rather than the beginning of a dementing or psychotic process. Nightmares are infrequent and may be drug induced. They are more common in people with a premorbid history of them. Unfortunately, levodopa may exacerbate nightmares by making them more vivid and better remembered in addition to causing the sufferer to cry and yell during sleep.
Chapter 118
Visual HalludnosSs
Visual hallucinosis occurs in about 20% to 30% of drug-treated patients followed over the long term. It is the experience of seeing real-appearing images in the presence of a clear sensorium. At first, the images are perceived as real, but after the first few attempts to touch them cause them to disappear, the patient learns to distinguish the hallucination from reality and usually is not much bothered by it. Hallucinations tend to be people, often children or small adults. They are strangers in most cases but may be relatives, friends, or deceased acquaintances and are silent even when ostensibly conversing, closing doors, or performing other tasks that should make noise. The visions are free of emotional content, very different from the situation in primary psychoses, such as schizophrenia, in which the hallucinations (almost always voices) say demeaning or nasty things or behave in ways to excite or engage the person. In levodopa-induced hallucinosis, the visions may appear at any time of day but are more common in the evening and tend not to upset the patient. Light does not abort their appearance, nor does darkness increase them. They often occur when the person is alone or engaged in a routine social activity, such as watching television with a spouse, and appear only rarely when the patient is involved in absorbing activities such as entertaining guests, playing with grandchildren, or visiting a doctor’s office. The hallucinated people most commonly watch the patients, showing no emotion themselves. A visual hallucination must be distinguished from a visual illusion, which is a misperception, with something seen as other than what it is. These usually occur in shadowy or dark areas and tend to take on a menacing aura. Patients also experience a feeling of another person being near them and report looking up or turning around to see who it is. Visual illusions are not seen clearly, whereas visual hallucinations are seen as clearly as or even more clearly than real objects. Occasionally, objects rather than people are hallucinated, but friendly animals such as dogs, horses, and cats may be perceived as well as insects. The hallucinations may persist for seconds, minutes, or hours but tend to last minutes and to recur. They usually disappear when “touched and usually ignore attempts to engage them in conversation (they do not usually move their lips, attempt sign language, or write on paper pads). The same person or group usually visits the patient repeatedly. When the patient is demented or psychotic, the hallucinations are perceived as real and may cause serious behavioral disturbances, especially if they are threatening. Auditory, tactile, or olfactory hallucinations are much less common but may occur in psychosis typically in people already suffering visual hallucinations. Treatment usually entails a reduction in drug dosage, but for some patients the loss of motor function that ensues is more difficultto tolerate than the hallucinosis, and some patients choose not to reduce their dosage. Psychosis Psychosis, a major mental disturbance in which reality is significantly misperceived, causing a marked decline in psychosocial functioning, occurs in 5% to 10% of patients treated over the long term. It is more common in older adults and demented patients but occurs in previously mentally intact patients with PD with no prior psychiatric history. On formal neurologic examination, they score perfectly on the mini-mental status examination unless there is an attention deficit.
Mental Changes in Parkinson‘s Disease
765
The psychosis induced by levodopa and the dopaminergic drugs tends to be stereotypic. Visual hallucinations occur along with paranoid delusions. Most common is the delusion that the spouse is having a sexual affair. In the case of single patients, a common delusion is that their savings are being looted by the children or the caretaker is plotting to place them in a nursing home. Unfortunately, the appearance of psychosis makes management at home more difficult and is the single most important predictor of nursing home placement in patients with PD. Some patients believe they are about to die, that they are dead already, that loved ones have just died, and so forth. In fact, psychosis appears to be associated with an increased mortality. Phenomena that are rare in primary psychoses, such as Capgras’s syndrome, the syndrome of reduplication in which the caretaker or some other significant person or even object has been replaced by a replica that looks and behaves like the original, may occur. Unlike schizophrenia, dopaminergic psychosis has only “positive” phenomena. There is no loosening of associations, anhedonia, poverty of thought, loss of ego boundaries, or blunting of affect. A delirious or encephalopathic state may also occur, in which attention span is diminished and disorientation occurs. Usually psychosis develops insidiously, although it may appear suddenly after a new medication is begun or an old one increased. However, psychosis onset in a patient on a stable medication schedule is common, and the early features often are overlooked if not asked about at routine evaluations. For example, it is common for psychosis to be present for months before being brought to the physician’s attention. Until recently, management of psychosis was almost impossible. One could reduce medication, attempt a drug holiday, or start a neuroleptic antipsychotic when a dosage reduction was not sufficient. Since the commercial release of clozapine, the situation has changed dramatically. Management of psychosis is now fairly straightforward in most cases. It is important to keep in mind that neurologically impaired patients often suffer adverse mental and motor effects when affected by an intercurrent nonneurologic process. Therefore, it is important to exclude medical problems such as infection, renal failure, thyroid dysfunction, or a new, nonneurologic medication as the underlying problem. However, this is usually not the case, and structural lesions are not worth looking for without a clear indication, such as a new focal sign or head trauma. Electroencephalography is nearly useless in this situation. Once the physician is satisfied that the problem is a druginduced psychosis, then any drugs that can be eliminated should be. Anticholinergic drugs have the highest mental adverse effect profile of the anti-PD medications and should be stopped at the onset of psychosis. Other anti-PD medications should then be tapered and discontinued, if possible, without jeopardizing motor function. The general approach is to reduce and then discontinue a single drug rather than reducing several drugs, with the aim of reducing polypharmacy as much as possible. There appears to be better tolerance for a single drug at a high dosage than for multiple drugs at low to moderate dosages, although no data exist to support this widely held tenet. If a recent medication change precipitated the psychosis, then it should be reversed; otherwise, the order of drug discontinuation should be as follows: anticholinergics, selegiline, amantadine, dopamine agonist, catechol-0-methyltransferase (COMT) inhibitor, and then levodopa. Once the lower limit of motor function has been reached, quetiapine or clozapine should
766
Movement Disorders
rn
Parkinson’s Disease and Parkinson-like Syndromes
be started if psychosis has not improved. These are atypical antipsychotics, which cause no parkinsonian side effects. Numerous studies now attest to their efficacy and tolerability when used properly, although only clozapine has two double-blind placebo controlled trials to support its use. Only if the patient cannot be treated at home is hospitalization justified. Clozapine should be initiated at 6.25 mg/day and quetiapine at 12.5 mg/day given at bedtime. The usual effective daily dosage is in the 6.25- to 50-mg range for clozapine and 25 to 100 mg/day for quetiapine. This is in contrast to the dosages used in schizophrenia, which are 300 to 900 mg daily. In general, the dosage is increased depending on response and adverse effects. Unlike schizophrenics, psychotic patients with PD may respond within 1 or 2 days. It seems that once the dosage is sufficient to allow the patient to sleep through the night, the psychosis remits. Therefore, it is suggested that the dosage be increased until the patient sleeps through the night. If this does not improve the psychosis, the dosage must be increased. Most patients do best if the dosage is given only at bedtime to reduce the daytime sedative side effects and to help keep the patient and caregiver sleeping through the night. It should be noted that not all atypical antipsychotic drugs are equal when it comes to PD. Risperidone worsens motor function in most patients. Olanzapine worsens motor function in about 40% to 50% of patients. Newer agents are under development. How long patients need to remain on the antipsychotic is unknown. Most patients, once on an atypical antipsychotic, can have their anti-PD medications increased without problem. If psychosis recurs when anti-PD drugs are increased, then the antipsychotic dosage is increased.
SUGGESTED READINGS Cummings JL: Depression and Parkinson’s disease: a review. Am J Psychiatry 149:443-454, 1992 Faber R, Trimble MR Electroconvulsive therapy in Parkinson’s disease and other movement disorders. Mov Disord 6:293-303, 1991 Fenelon G, Mahieux F, Huon R, Ziegler M Hallucinations in Parkinson’s disease: prevalence, phenomenology and risk factors. Brain 123:733745, 2000
French Clozapine Study Group: Clozapine in drug-induced psychosis in Parkinson’s disease. Lancet 91692041-2042, 1999 Friedman JH, Factor S A Atypical antipsychotics in the treatment of drug-induced psychosis in Parkinson’s disease. Mov Disord 15(2):201211, 2000
Friedman JH, Friedman H: Fatigue in Parkinson’s disease. Neurology 43:20 16-20 18, 1993
Hughes AJ, Daniel SE, Blankson S, Lees AJ: The clinicopathologic study of 100 cases of Parkinson’s disease. Arch Neurol50:140-148, 1993 Parkinson Study Group: Low dose clozapine for the treatment of drug-induced psychosis in Parkinson’s disease. N Engl J Med 340:757763, 1999
Per1 DP, Olanow CW, Calne D: Alzheimer’s disease and Parkinson’s disease: distinct entities or extremes of a spectrum of neurodegeneration? Ann Neurol44(Suppl 1):S19-S31, 1998 Poewe W, Luginger E Depression in Parkinson’s disease: impediments to recognition and treatment options. Neurology 52(Suppl 3):52-56, 1999
Richard IH, Kurlan R A survey of antidepressant drug use in Parkinson’s disease. Neurology 99:1168-1170, 1997 Starkstein SE, Mayberg HS, Prezioi TJ, Robinson RG A prospective longitudinal study of depression, cognitive decline, and physical impairments in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 55:377-382, 1992 Stein MB, Heuser U, Juncos JL, Uhde Tw: Anxiety disorders in patients with Parkinson’s disease. Am J Psychiatry 147:217-220, 1990
1 19 Multiple-System Atrophy: Striatonigral
Degeneration and Shy-Drager Syndrome Paula Ravin The term multiple-system atrophy (MSA) generally refers to a broad class of parkinsonian syndromes with features not normally seen in idiopathic Parkinson’s disease. It has been noted in numerous neuropathologic studies that MSA is found in 8% to 10% of patients diagnosed with idiopathic Parkinson’s disease and, in some, is clinically indistinguishable. However, the postmortem examination of such patients reveals variable degrees of neurodegenerative changes in cerebellar, striatal, nigral, and subcortical structures such as the thalamus, nucleus accumbens, septal nuclei, hypothalamus, locus ceruleus, and a variety of parasympathetic nuclei (dorsal vagal nucleus, Edinger-Westphal nucleus, Onuf nucleus of the sacral cord, and so on), hence the term multiplesystem, although atrophy is not the only anatomic change. A
number of reports give evidence of focal gliosis, neuronal loss, glial cytoplasmic inclusions, depletion of specific neurotransmitters (y-aminobutyric acid, dopamine, norepinephrine, glutamate), and functional changes in metabolism of glucose or dopamine binding characteristics on positron emission tomography. Oppenheimer and Graham coined the term multiple-system atrophy in a paper in 1969 broadly categorizing patients into three subclasses: Shy-Drager syndrome, striatonigral degeneration, and olivopontocerebellar atrophies, the latter of which is further subdivided into familial and sporadic forms. The syndrome of Steele-Richardson-Olszewski or progressive supranuclear palsy is not included because it represents a distinctive clinical picture of supranuclear downgaze palsy, axial dystonia, cognitive impair-
766
Movement Disorders
rn
Parkinson’s Disease and Parkinson-like Syndromes
be started if psychosis has not improved. These are atypical antipsychotics, which cause no parkinsonian side effects. Numerous studies now attest to their efficacy and tolerability when used properly, although only clozapine has two double-blind placebo controlled trials to support its use. Only if the patient cannot be treated at home is hospitalization justified. Clozapine should be initiated at 6.25 mg/day and quetiapine at 12.5 mg/day given at bedtime. The usual effective daily dosage is in the 6.25- to 50-mg range for clozapine and 25 to 100 mg/day for quetiapine. This is in contrast to the dosages used in schizophrenia, which are 300 to 900 mg daily. In general, the dosage is increased depending on response and adverse effects. Unlike schizophrenics, psychotic patients with PD may respond within 1 or 2 days. It seems that once the dosage is sufficient to allow the patient to sleep through the night, the psychosis remits. Therefore, it is suggested that the dosage be increased until the patient sleeps through the night. If this does not improve the psychosis, the dosage must be increased. Most patients do best if the dosage is given only at bedtime to reduce the daytime sedative side effects and to help keep the patient and caregiver sleeping through the night. It should be noted that not all atypical antipsychotic drugs are equal when it comes to PD. Risperidone worsens motor function in most patients. Olanzapine worsens motor function in about 40% to 50% of patients. Newer agents are under development. How long patients need to remain on the antipsychotic is unknown. Most patients, once on an atypical antipsychotic, can have their anti-PD medications increased without problem. If psychosis recurs when anti-PD drugs are increased, then the antipsychotic dosage is increased.
SUGGESTED READINGS Cummings JL: Depression and Parkinson’s disease: a review. Am J Psychiatry 149:443-454, 1992 Faber R, Trimble MR Electroconvulsive therapy in Parkinson’s disease and other movement disorders. Mov Disord 6:293-303, 1991 Fenelon G, Mahieux F, Huon R, Ziegler M Hallucinations in Parkinson’s disease: prevalence, phenomenology and risk factors. Brain 123:733745, 2000
French Clozapine Study Group: Clozapine in drug-induced psychosis in Parkinson’s disease. Lancet 91692041-2042, 1999 Friedman JH, Factor S A Atypical antipsychotics in the treatment of drug-induced psychosis in Parkinson’s disease. Mov Disord 15(2):201211, 2000
Friedman JH, Friedman H: Fatigue in Parkinson’s disease. Neurology 43:20 16-20 18, 1993
Hughes AJ, Daniel SE, Blankson S, Lees AJ: The clinicopathologic study of 100 cases of Parkinson’s disease. Arch Neurol50:140-148, 1993 Parkinson Study Group: Low dose clozapine for the treatment of drug-induced psychosis in Parkinson’s disease. N Engl J Med 340:757763, 1999
Per1 DP, Olanow CW, Calne D: Alzheimer’s disease and Parkinson’s disease: distinct entities or extremes of a spectrum of neurodegeneration? Ann Neurol44(Suppl 1):S19-S31, 1998 Poewe W, Luginger E Depression in Parkinson’s disease: impediments to recognition and treatment options. Neurology 52(Suppl 3):52-56, 1999
Richard IH, Kurlan R A survey of antidepressant drug use in Parkinson’s disease. Neurology 99:1168-1170, 1997 Starkstein SE, Mayberg HS, Prezioi TJ, Robinson RG A prospective longitudinal study of depression, cognitive decline, and physical impairments in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 55:377-382, 1992 Stein MB, Heuser U, Juncos JL, Uhde Tw: Anxiety disorders in patients with Parkinson’s disease. Am J Psychiatry 147:217-220, 1990
1 19 Multiple-System Atrophy: Striatonigral
Degeneration and Shy-Drager Syndrome Paula Ravin The term multiple-system atrophy (MSA) generally refers to a broad class of parkinsonian syndromes with features not normally seen in idiopathic Parkinson’s disease. It has been noted in numerous neuropathologic studies that MSA is found in 8% to 10% of patients diagnosed with idiopathic Parkinson’s disease and, in some, is clinically indistinguishable. However, the postmortem examination of such patients reveals variable degrees of neurodegenerative changes in cerebellar, striatal, nigral, and subcortical structures such as the thalamus, nucleus accumbens, septal nuclei, hypothalamus, locus ceruleus, and a variety of parasympathetic nuclei (dorsal vagal nucleus, Edinger-Westphal nucleus, Onuf nucleus of the sacral cord, and so on), hence the term multiplesystem, although atrophy is not the only anatomic change. A
number of reports give evidence of focal gliosis, neuronal loss, glial cytoplasmic inclusions, depletion of specific neurotransmitters (y-aminobutyric acid, dopamine, norepinephrine, glutamate), and functional changes in metabolism of glucose or dopamine binding characteristics on positron emission tomography. Oppenheimer and Graham coined the term multiple-system atrophy in a paper in 1969 broadly categorizing patients into three subclasses: Shy-Drager syndrome, striatonigral degeneration, and olivopontocerebellar atrophies, the latter of which is further subdivided into familial and sporadic forms. The syndrome of Steele-Richardson-Olszewski or progressive supranuclear palsy is not included because it represents a distinctive clinical picture of supranuclear downgaze palsy, axial dystonia, cognitive impair-
Chapter 119 w
Multiple-System Atrophy: Striatonigral Degenerationand Shy-Drager Syndrome
ment, and mild parkinsonism and has discrete pathologic changes associated with the diagnosis. CLINICAL DIAGNOSIS
Correct identification of MSA presents a challenge even to experts in movement disorders. The relevance of distinguishing these disorders early on pertains to prognosis, predicted responses to medication, possibility of a genetic association that can be identified (and may soon be tested with marker gene), and referring patients to research centers with special interest in MSA. The typical signs and symptoms of Parkinson’s disease are not always found in MSA early on or may be insignificant clinically compared with other features. Classic resting tremor, for example, is found in 30% of idiopathic Parkinson’s disease initially but only about 5% or so of MSA cases, with sustension or intention tremor seen in another 40% of idiopathic Parkinson’s disease initially and 1OYo of MSA cases. Rigidity with akinesia or bradykinesia is common to both disorders, but postural instability often is seen early in MSA, whereas it is usually found in more advanced or late-onset idiopathic Parkinson’s disease and does not evolve as rapidly. Recent articles attempting to distinguish idiopathic Parkinson’s disease and MSA retrospectively on clinical grounds have suggested certain other distinguishing features or red flags to look for in making an initial differential diagnosis and refining it over the first 2 to 3 years of observation. To start with, the mean age at onset of MSA (all subtypes) is 53, with progression of disability to death in an average of 7 to 10 years, as opposed to idiopathic Parkinson’s disease, with a mean age at onset of 60 and progression over 10 to 20 years. The malelfemale ratio of MSA appears to be 1.8:l.O in familial olivopontocerebellar atrophy, 2.0:1.0 in Shy-Drager syndrome, and unclear in striatonigral degeneration, in which cumulative data suggest a slight male predominance, as in idiopathic Parkinson’s disease ( 1.2:1.O). In a review of the literature on MSA through 1994, Quinn and Wenning noted that 80% of cases were “parkinsonian type,” and 20% were “cerebellartype.” The presence of truncal or limb ataxia, dysarthria, scanning speech, a positive Romberg test, and lateral nystagmus with square wave jerks along with rigidity and bradykinesia points to the olivopontocerebellar atrophies. Autonomic dysfunction usually is seen before dopaminergic therapy in all patients with MSA. It is most prominent in Shy-Drager syndrome, where incapacitating orthostatic hypotension results in patients being wheelchair-bound in 5 to 7 years. More subtle signs such as persistent impotence in males, heat intolerance, sudden fluctuations in blood pressure with “hot flashes,” and loss of sweating in the palms, axilla, and groin can precede the parkinsonian features of MSA by up to 10 years. The majority of patients with striatonigral MSA have asymmetrical rigidity and dystonia, with pyramidal signs emerging before dopaminergic therapy. Early motor fluctuations (occurring before 5 years) with levodopa therapy are seen particularly in striatonigral patients with older onset than the early-onset Parkinson’s disease patients with motor fluctuations. The initial improvement in parkinsonian features from moderate levodopa therapy (300 to 500 mg daily) is not as robust in MSA as in Parkinson’s disease either. Patients with Shy-Drager syndrome may experience improvement in bradykinesia and rigidity with levodopa but cannot tolerate dosage increases over several years because of exacerbation of symptomatic orthostatic hypotension. Loss of responsivity to levodopa after 5 to 7 years is common in
767
MSA. In some cases of olivopontocerebellar atrophy (OPCA) a poor response to dopamine agonists also indicates widespread loss of dopamine receptor sites. Neurogenic bladder features are found in both MSA and Parkinson’s disease, but urinary retention, bladder dyssynergia, and frank bladder or bowel incontinence are seen much earlier in MSA. Another sign of autonomic failure that seems to be unique to MSA is the “cold hands sign” reported by Klein et al. They documented a baseline skin temperature significantly lower in patients with MSA than in those with Parkinson’s disease or controls before and after cooling. The appearance of dusky or violaceous hands with blanching and delayed circulatory return, especially on the side of earliest symptoms, may be a red flag in MSA. At a consensus conference on MSA in 1998, a consortium of movement disorder specialists worldwide defined three diagnostic categories of MSA based on the clinical domains of autonomic dysfunction,parkinsonism, cerebellar dysfunction, and corticospinal tract dysfunction. “PossibleMSA” is represented by one clinical domain and two features from other domains, “probable MSA” is autonomic dysfunction plus poorly levodopa-responsive parkinsonism or cerebellar dysfunction, and “definite MSA” is pathologically confirmed by the presence of high-density ghal cytoplasmic inclusions and degeneration of the nigrostriatal or olivopontocerebellar tracts. Exclusion criteria include symptomatic onset before age 30, positive family history, hallucinations unrelated to medication, focal cortical signs (alien limb, aphasia, parietal lobe dysfunction), and other systemic illness reproducing these signs. The presence of DSM-defined dementia, supranuclear palsy, or slowing of vertical saccades would also be outside the realm of MSA. The consortium recommended using only two subcategories for MSA-parkinsonian type (MSA-p) and cerebellar type (MSA-c)-to emphasize the consistent neuropathology linking the syndromes of Shy-Drager, striatonigral degeneration, and olivopontocerebellar degeneration because clinical parameters alone are not reliably discriminative.Table 119-1 summarizes the variety of symptoms and signs that may be useful in making an early clinical diagnosis of MSA most accurately. Cognitive dysfunction can occur in MSA but often is evidenced only by subtle tests of frontal lobe function in MSA-p. Cognitive change is occasionally observed in MSA-c, as it is with some of the dominant hereditary ataxias. Changes in mood and affect with irritability, lability, and depression are commonly noted in SCA-2, for example. These patients have deficits in executive function on neuropsychological testing with progression of their illness (see Chapter 124 on progressive ataxia). DIAGNOSTIC TESTS A variety of structural, functional, and physiologic tests have been proposed to increase the sensitivity and specificity of MSA diagnosis. Reports of urodynamic and detrusor or anorectal sphincter electromyography being diagnostic are controversial because of technical difficulties in performing and interpreting such studies. Magnetic resonance imaging of the brain has been refined to highlight the signal intensity differences in the striatum and cerebello-brainstem structures in MSA and Parkinson’s disease, including phosphorus magnetic resonance spectroscopy, gradient echo sequencing, and magnetic resonance imaging volumetric measurements. A high correlation between image details and clinical diagnoses has been claimed but not confirmed by pathologic diagnoses to date. P-CIT single photon emission
768
Movement Disorders
rn Parkinson's Disease and Parkinson-like Syndromes
TABLE119-1. Signs and Symptoms of MSA MSA PD
SND
SD
OPCA
PSP
Age of onset
60f7
53f7
52f6
70f6
Duration of disease
10-20
7-10
5-10
28 f 4 (FOPCA) 49 f 6 (SOPCA) 10-25 (FOPCA)
Rigidity Bradykinesia Orthostasis Neurogenic bladder Response to levodopa Dyskinesia, dystonia Tremor Rapid progression Cognitive dysfunction
*
+ +
+ +
* ++I-
U
+ (young onset) * + ("subcortical")
+ * + +
U
+ +
+ ("subcortical")
6-15 (SOPCA) f f f f f f
+
-H
f
f
++t (FOPCA)
+ (SOPCA)
6-10
+ ++ + -
U
+++
Abbreviations: FOPCA,familial olivopontocerebellaratrophy; MSA, multiplesystem atrophy; OPC& olivopontocerebellaratrophy; PD, Parkinson's disease; PSP, progressivesupranuclear palsy; SD, Shy-Drager syndrome; SND, striatonigral degeneration; SOPCA, sporadic olivopontocerebellaratrophy; -, absent; +, mild; +,moderate; +I+, marked.
computed tomography, Altropane single photon emission computed tomography, and fluorodopa positron emission tomography brain scans also recognize qualitative and quantitative differences between Parkinson's disease and MSA but with substantial overlap of the clinical spectrum. NEUROPATHOLOGIC FEATURES As noted earlier in this chapter, the definitive diagnosis of MSA is most accurately determined by the postmortem pathology. Histologically, the putamen shows marked loss of nerve cells, with associated gliosis in the posterior and lateral portions. The anteromedial putamen and head of the caudate may evidence lesser changes in some cases, as seen in Huntington's disease. Melanin pigment or siderin granules are left behind from the degenerated putamen neurons and may also accumulate in the globus pallidus and substantia nigra-pars reticulata (not the pars compacta). Varying degrees of neuron loss are found in pontine nuclei, the inferior olives, Purkinje cells of the cerebellar hemispheres, and the intermediolateral columns of the thoracic and lumbar spinal segments or Onuf nucleus in the sacral cord. Lewy bodies have long been considered the sine qua non for the diagnosis of idiopathic Parkinson's disease. They are identified as intracytoplasmic eosinophilic inclusions 5 to 25 pm in diameter, with a dense core and smudgy halo antigenically similar to neurofilament. In MSA, they may be slightly higher common than in normal aging controls but not to the extent seen in idiopathic Parkinson's disease. The distribution of Lewy bodies in both MSA and idiopathic Parkinson's disease is generally the same, whereas the degree of gliosis, nigral cell degeneration, and pigmented deposits (melanin, lipofuscin, or siderin) is much greater in all the brainstem nuclei involved in MSA. Glial cytoplasmic inclusions in MSA contain alpha synuclein, a synaptic protein that is also found in Lewy bodies. The familial olivopontocerebellar atrophies tend to have an even more widespread neuron loss and reactive changes (gliosis and demyelination, axonal thinning, or gross atrophy) involving all the same areas affected by sporadic olivopontocerebellar atrophy. In addition, there is often a neuronal wipeout in the dentate nuclei, locus ceruleus, corticospinal tracts, Clarke columns and spinocerebellar tracts, posterior column, and anterior gray
horns. These extensive lesions explain the diversity and severity of clinical signs found in most cases of familial olivopontocerebellar atrophy, whereas spontaneous olivopontocerebellar atrophies are fairly stereotypic in appearance. The observation of extremely dense deposits of lipofuscin in all areas of neuron loss seen in a patient with familial olivopontocerebellar atrophy and glutamate dehydrogenase deficiency has been a confounding factor in characterizing the neuropathologic features of olivopontocerebellar atrophies uniformly. It seems that there are a variety of look-alikes in this subdivision of MSAs that may differ in their primary metabolic defects but lead ultimately to a characteristic pattern of cellular loss. THERAPEUTIC STRATEGIES
The therapy for MSA depends on which systems degeneration presents the most troublesome symptoms because parkinsonian features usually are not the predominant ones. Also, as noted earlier, response to dopaminergic drugs is poorly sustained and may include worsening of orthostatic hypotension. Dyskinesias often occur with levodopa therapy after an average of 2.5 years of replacement with low to moderate dosages and can be seen simultaneously with axial rigidity, resting tremor, bradykinesia, and bulbar dysfunction (dysphagia and dysarthria). A slight response to levodopa may be evident only in up to 40% of patients with MSA, and clinical deterioration occurs after withdrawal of dopaminergics (e.g., for a drug holiday) with failure of an enhanced response to levodopa after reintroduction a few weeks later. Vague feelings of unsteadiness and overt falls early in the course of disease are common to all forms of MSA and may be aggravated by treatment with neuroleptic drugs given for presumed vestibulopathy, bringing out the parkinsonian aspects of these disorders instead. If postural changes in systolic pressure of more than 20 mm Hg are found without dopaminergic therapy, further assessment of the autonomic nervous system can help define appropriate choices of drug therapy. Testing of the baroreceptor arc includes measuring Valsalva ratio, performing the cold pressor test, and observing changes in blood pressure and electrocardiogram rhythm with hypoventilation and slow, steady breathing. These are simple physiologic tests of the integration of both the
Chapter 1 19
Multiple-SystemAtrophy: Striatonigral Degenerationand Shy-Drager Syndrome
afferent and efferent limbs of the arc and vagal tone. More sophisticated testing of catecholamine responses and pharmacologic rechallenge tests are best performed in a dedicated laboratory setting where the exact conditions of the tests and their responses can be measured and interpreted accurately. Mild orthostatic hypotension can be remedied with a combination of support hose or Jobst stockings (if tolerated) and volume expansion by adding salt to the diet. Often low-dose fludrocortisone (0.1 mg/day to 0.2 mg three times daily) is helpful if not contraindicated by a history of congestive heart failure. Indomethacin at 25 to 50 mg three times daily or ibuprofen at 400 to 800 mg three times daily can indirectly result in higher mean arterial pressures. Midodrine, a selective a-agonist, can be used safely in patients with coronary disease, but adequate volume expansion is needed to increase sympathetic tone and upright blood pressure. Supine hypertension, irritability, scalp tingling, and short duration of effect (less than 4 hours) are the main drawbacks of this drug. Patients should be advised to avoid standing abruptly after prolonged sitting and to try to stay well hydrated and avoid overexposure to hot and humid environments. They should minimize vasovagal responses by avoiding large meals, excessive alcohol, and straining at bowel movements. Sleepingin an elevated position (head of bed up 30 degrees) in reverse Trendelenburgcan ameliorate early morning hypotension by increasing the renin secretion overnight. Cardiac pacing and implantable devices for noradrenergic replacement therapy (an autonomic pacing system) are still under investigation and show promise for the more refractory condition of primary autonomic failure without central nervous system involvement. When dopaminergic therapy is no longer tolerated for the extrapyramidal symptoms, amantadine or anticholinergicsmay be beneficial in controlling tremor, rigidity, and bradykinesia at dosages comparable to those used in idiopathic Parkinson’s disease. A coincidental benefit is mild urinary retention as a side effect of these drugs in the face of urgency and incontinence seen in mild to moderate MSA. However, acute or severe urinary retention may ensue if the patient with MSA also has detrusor dyssynergia. The neurogenic bladder problems of MSA can include incomplete voiding, leading to recurrent infections caused by urinary stasis, or involuntary urethral sphincter relaxation with incontinence of small or large volumes. On rare occasions this is accompanied by the same phenomenon in the anal sphincter, causing double incontinence in advanced MSA. Treatment includes standard precautions such as urinary acidification and episodic to chronic antibiotic treatment plus a postvoid Cred6 maneuver and toileting schedules. Judicial limitations of fluid intake at night and protective garments or condom catheters can improve urinary hygiene as well. Chronic constipation may parallel the course of the bladder disturbance and is addressed with bulk agents, stool softeners, increased daytime fluid intake, and laxatives or enemas when all else fails. Osmotic laxatives such as lactulose syrup or polyethylene glycol for patients with diabetes can be used judiciously to promote bowel motility when recurrent impaction or painful cramps occur with other agents. The gait disorder of MSA typically is multifactorial and should be evaluated by experienced physical,and occupational therapists. Loss of postural reflexes is the most dangerous component and is not remediable with medication. Teaching safety awareness and use of assistive devices for ambulation are key to maintaining patient independence. Other factors such as extrapyramidal tone,
769
postural hypotension, and limb ataxia may be diminished by adding amantadine (50 to 100 mg three times a day) to anticholinergic therapy at least for the first 1 or 2 years after diagnosis, but often not beyond that. Finally, speech and swallowing disturbances in MSA are refractory to pharmacologic therapy but must be evaluated to reduce the risk of aspiration and fatal choking. Vocal pacing, respiratory exercises, and language boards can help patients communicate effectively when speech quality is grossly impaired. Standard aspiration precautions combined with an H, blocker or proton pump inhibitor may also delay serious problems with pneumonia or reactive airway disease. CONCLUSIONS
Multiple system atrophy is an apt term for a class of diseases that have in common parkinsonism and the following atypical features: Extrapyramidal signs like those of idiopathic Parkinson’s disease but less responsive to dopaminergic therapy initially or within 2.5 years of using moderate dosages of levodopa Additional symptoms and signs of pathology in the cerebellum, pyramidal tract, autonomic nervous system, and numerous brainstem nuclei Frequent development of spontaneous or dopa-induced dystonia and dyskinesia, also within a few years of presentation Earlier mean age of onset and more rapid progression to disability than idiopathic Parkinson’s disease Characteristic pathologic changes on postmortem examination, with neuron loss and gliosis but without prominent Lewy bodies Current research in MSA relates to early diagnostic discrimination between idiopathic Parkinson’s disease and the striatonigral degeneration variant by performing positron emission tomography or single photon emission computed tomography scanning with selective markers, identifjmg a common metabolic derangement that may cause systemic breakdown, and gathering enough epidemiologic data to identify a possible genetic precursor or environmental exposure contributing to these diseases. Whereas MSA is far less common than idiopathic Parkinson’s disease, its atypical features often lead families and physicians to pursue further studies. The opportunity for better understanding of all parkinsonian disorders therefore lies in identifying patients with MSA, offering them specialized care, and ultimately encouraging their participation in research studies. SUGGESTED READINGS Gilman S, Low P, Quinn N et al: Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci 163394-98, 1999 Hughes AJ,Colosimo C, Kleedorfer B et al: The dopaminergicresponse in multiple system atrophy. J Neurol Neurosurg Psychiatry 55:100@1013, 1992 Klein C, Brown R, Wenning G et al: The “cold hands sign” in multiple system atrophy. Mov Disord 12(4):514-518, 1997 Penny J B Multiple system atrophy and non-familial olivopontocerebellar atrophy are the same disease. Ann Neurol 37:553-554, 1995 Polinsky RJ: Multiple system atrophy: clinical aspects, pathophysiology and treatment. pp. 487498. In Jankovic J (ed): Neurologic Clinics. Vol. 2. WB Saunders, Philadelphia, 1984 Quinn N, Wenning G Multiple system atrophy. In Battistin et a l (eds): Advances in Neurology. Vol. 69. Lippincott-Raven, Philadelphia, 1996
710
Movement Disorders W
Parkinson’s Disease and Parkinson-like Syndromes
120 Progressive Supranuclear Palsy Douglas G. Cole and Nutan Sharma
Steele, Richardson, and Olzewski described progressive supranuclear palsy in 1964, and the disorder has since become a well-established clinicopathologic entity. Its dominant clinical feature is parkinsonism. Although rare, it may be the most common clinicopathologically defined atypical parkinsonian disorder. CLINICAL FEATURES Patients generally present in their fifties and sixties, less often in their forties, seventies, or eighties. The presentation may include imbalance, loss of manual dexterity, visual disturbances, dysarthria, dysphagia, altered intellectual function, personality changes, or insomnia. All features are not invariably present in every patient, but most evolve eventually during the course of the illness. Postural instability and visual disturbances are characteristic and often early symptoms of progressive supranuclear palsy. Some patients begin to fall suddenly and without apparent explanation (paroxysmal disequilibrium). Most develop a tendency to fall backward, but they may fall in any direction. Some describe difficulty walking on an incline or on uneven surfaces, maintaining balance when lifting a heavy object, or arising from a chair or getting out of a car. Visual difficulties reflect primarily impaired voluntary control of eye movements. Patients may describe difficulty navigating when walking down stairs or problems reading a book or trying to find food on a plate. They often complain of blurred vision and occasionally of diplopia. They may describe difficulty in opening or closing their eyes. Some say that they simply cannot see. Establishing the presence of early imbalance or visuomotor impairment in the history of a patient with parkinsonism strongly favors the diagnosis of progressive supranuclear palsy; sustained absence of either of these symptoms makes its diagnosis unlikely. Speech and swallowing commonly deteriorate. Choking develops insidiously but then becomes a major source of morbidity. Most patients develop cognitive impairment (i.e., a modest loss of cognitive function compared with their baseline). Fewer are thought to develop dementia (i.e., a more profound and widespread decline of memory and other cognitive functions that alone is sufficient to compromise social and vocational abilities). Depression and personality changes are common. As in many parkinsonian disorders, sleep disturbances also are common. Examination of patients with progressive supranuclear palsy reveals symmetrical, axially predominant parkinsonism, abnormal eye movements, gait instability, and pseudobulbar palsy. Axially predominant parkinsonism is characterized by rigidity and hypokinesia that is most prominent in the muscles of the neck and trunk. On casual observation, the examiner may note that the patient moves his or her head abnormally slowly or en bloc with the trunk. Passive motion of the neck, especially to flexion and extension, reveals rigidity. The magnitude of this rigidity may vary, but neck tone is rarely normal, even in the early stages of progressive supranuclear palsy. When severe, it can be associated with retrocollis and dystonic extension of the entire trunk.
1
Patients with progressive supranuclear palsy lose facial expressiveness. Some patients develop rigidity of the limbs, but others have normal limb tone despite severe axial rigidity. Loss of manual dexterity is common. Fine movements of the fingers and hands become slow and uncoordinated. This loss of precise motor control may occasionally be exacerbated by apraxia, but prominent apraxia is uncommon. Abnormal eye movements are a critical feature of progressive supranuclear palsy. The most typical abnormality is impaired voluntary gaze. The examiner may suspect a defect in eye movements when calling the patient’s name in the waiting room: Instead of turning the eyes briskly toward the sound of his or her name, the patient slowly turns the head or even the whole body. On more formal examination, one can observe that when the patient holds his or her head still and tries to follow a moving object with the eyes or to move the eyes in a particular direction without a visual target, the eye movements are incomplete, absent, slow, or fractionated. When the patient fixes the eyes on a stationary object while allowing the examiner to move his or her head, however, the eyes display a full range of motion (intact oculocephalic reflex or “doll’s head response”).The ability to converge the eyes is lost. Typically, gaze remains conjugate. Usually, the voluntary eye movement most prominently affected in progressive supranuclear palsy is downgaze. Although impaired voluntary downgaze strongly suggests the diagnosis of progressive supranuclear palsy in the correct context, it is not pathognomic for the disease. For example, impaired downgaze and parkinsonism can be seen in central nervous system Whipple’s disease, which, though exceedingly rare, is eminently treatable. Furthermore, some patients with progressive supranuclear palsy display more involvement of horizontal or upgaze than downgaze. In this regard, one should note that decreased range of voluntary upgaze is common in older adults. This eye movement finding alone is rarely sufficient for suspecting that a patient has progressive supranuclear palsy. The severity of eye movement abnormalities in progressive supranuclear palsy is variable. When dramatic, supranuclear gaze palsy is easy to appreciate. When subtle, it may be detectable only through close observation. For example, some patients may have only slowing of the fast phase of opticokinetic nystagmus. The presence of square wave jerks and inability to suppress the vestibulo-ocular reflex can bolster suspicion of progressive supranuclear palsy. Other patterns of eye movement abnormalities occasionally develop in patients with this disease. Several patients have been described with an internuclear ophthalmoplegia. Other patients lose all eye movements, including reflex eye movements. Rare patients retain normal eye movements throughout the course of the disease. Exceptional cases notwithstanding, the importance of a careful visuomotor examination in any patient with parkinsonism cannot be overemphasized. The combination of prominent impairment of
Chapter 120
voluntary eye movements and parkinsonism suggests progressive supranuclear palsy until proven otherwise. In this disease, visual function can also be compromised by abnormal opening and closing of the eyes. Many patients with the disease have retracted upper eyelids, which gives them a characteristic staring expression. Decreased blink frequency, common in many parkinsonian disorders, makes patients susceptible to corneal injury. Alternatively, some patients with progressive supranuclear palsy fmd that they are unable to open their eyes voluntarily. This so-called apraxia of eyelid opening, when severe, can produce functional blindness. However, visual acuity is not primarily affected in progressive supranuclear palsy. Patients with the disease typically have difficulty arising from a chair, and when they try to sit down, they often begin to topple backward uncontrollably. When standing, they may hold the trunk erect. They stand and walk with a normal base, bilateral symmetrical diminution of armswing, and en bloc turning. Their steps may be shuffling or festinating. The ability to walk in tandem or hop or stand on either foot is lost. Some patients display retropulsion when pulled from behind. Others fall spontaneously. Eventually, patients become unable to walk. Dysarthria and dysphagia in progressive supranuclear palsy reflect pseudobulbar palsy. Speech is slurred and quiet. Some patients develop difficulty initiating speech or irregular, halting speech or festinating speech. They may eventually become anarthric. Drooling is prominent. The gag reflex may be hyperactive or hypoactive. Aspiration is common. Primitive reflexes and frontal release signs, such as the glabellar response, root response, snout reflex, grasping, and palmomental response, are common. Utilization behavior, echolalia, palilalia, or perseveration can be dramatic. Emotional incontinence can evolve. Evidence of intellectual deterioration with the disease includes generalized cognitive slowing, inattentiveness, and memory loss. In some patients, the magnitude of intellectual decline equals that of the loss of voluntary motor control, and true dementia ensues. In others, however, intellectual decline remains mild for years, despite disabling loss of motor function. Because motor dysfunction can progressively compromise a patient’s ability to communicate, establishing the intellectual status of a patient with progressive supranuclear palsy often entails careful and patient questioning. However, one should not assume that a patient with the disease is demented on the basis of physical debility. Rest tremor is rare in progressive supranuclear palsy. Absence of such a tremor on history or examination is an important clue to the diagnosis. Strength, primary sensation, and cerebellar function are preserved. Occasional patients develop mild hyperreflexia or an extensor plantar response, but pyramidal tract dysfunction is not a prominent feature of the illness.
Progressive Supranuclear Palsy
77 1
fies Parkinson’s disease. The symmetrical distribution of parkinsonism in progressive supranuclear palsy contrasts with the asymmetrical parkinsonism usually found in Parkinson’s disease. Retrocollis, erect posture, and dystonic extension of the trunk are uncommon in patients with Parkinson’s disease; mild anteroflexion of the neck and hunched posture are more typical. Rest tremor is almost always present at some point during the course of illness in patients with Parkinson’s disease. Finally, patients with Parkinson’s disease usually experience sustained and dramatic benefits from levodopa. This is not the case for patients with progressive supranuclear palsy. Other atypical parkinsonian disorders that respond poorly to levodopa may resemble progressive supranuclear palsy. Corticobasal ganghonic degeneration produces asymmetrical parkinsonism associated with severe apraxia and parietal sensory deficits. Multiple-system atrophies, such as striatonigral degeneration, Shy-Drager syndrome, and the olivopontocerebellar atrophies, produce varied patterns of deficits reflecting involvement of the corticospinal system, the cerebellar system, the autonomic nervous system, and the peripheral nerves. Some of these disorders are hereditary. Normal pressure hydrocephalus is a poorly understood syndrome in which patients can develop gait ataxia followed by urinary incontinence and dementia. This syndrome should rarely, if ever, be confused with progressive supranuclear palsy. However, it is important to keep this diagnosis in mind for any patient who presents with impaired gait because occasional patients with early stages of normal pressure hydrocephalus improve after drainage of cerebrospinal fluid. Clues to the diagnosis of normal pressure hydrocephalus include the temporal evolution of symptoms (which is critical), the presence of hydrocephalus on imaging, normal cerebrospinal fluid pressure, and the absence of any atypical features. Multiple cerebral infarctions can produce pseudobulbar palsy, but we have not seen infarctions alone mimic the entire syndrome of progressive supranuclear palsy. A history of stepwise decline is a clue to the presence of vascular disease. Spongiform encephalopathies sometimes enter into the differential diagnosis but tend to produce evidence of cortical dysfunction, such as myoclonus, and tend to progress rapidly. The clinical pictures of Alzheimer’s disease and Pick’s disease may overlap with that of progressive supranuclear palsy. Usually, the relative prominence of dementia compared with motor involvement indicates the correct diagnosis, but sometimes the scenario can confound even the most experienced observer. Wilson’s disease and central nervous system Whipple’s disease are rare but important to consider because they are treatable. Uncommon hereditary disorders, such as adult-onset Niemann-Pick disease and Joseph‘s disease, can mimic progressive supranuclear palsy on rare occasions.
DIFFERENTIAL DIAGNOSIS The major diagnostic considerations in a patient who may have progressive supranuclear palsy are other parkinsonian neurodegenerative disorders, most importantly Parkinson’s disease. It has been estimated that about 5% of patients diagnosed with Parkinson’s disease actually have progressive supranuclear palsy. Several clues are especially helpful in differentiating the two disorders. In contrast to progressive supranuclear palsy, imbalance and impaired vision are rare in the initial stages of Parkinson’s disease. The eye movement defects so typical of the former are not seen in the latter. Whereas axial parkinsonism is the rule in progressive supranuclear palsy, appendicular predominance typi-
DIAGNOSIS The diagnosis of progressive supranuclear palsy rests on recognition of the characteristic syndrome. In a typical case, a single imaging study of the brain, ideally a magnetic resonance scan, is appropriate to screen for coexistent disorders such as cerebral infarctions. This study may reveal prominent atrophy of the midbrain, with enlargement of the third ventricle, but these are not reliable findings. Patients who may have disorders with a biochemical signature, such as Wilson’s disease, should be evaluated accordingly.
772
Movement Disorders rn Parkinson’sDisease and Parkinson-like Syndromes
In some patients, a firm diagnosis cannot be made at the time of presentation. Rarely, characteristic abnormalities on positron emission tomography (PET) or single photon emission computed tomography (SPECT) can support a suspected diagnosis of progressive supranuclear palsy. Generally, however, the most important step is to follow patients over time. Usually, the diagnosis of progressive supranuclear palsy becomes apparent. BIOLOGIC BASIS Progressive supranuclear palsy is a tau-opathy. Tau proteins are phosphorylated, microtubule-associated proteins that are abundant in the central nervous system. Human tau proteins are encoded by a single gene consisting of 16 exons on chromosome 17q21. The tau isoforms found in the brain are generated by alternative mRNA splicing of 11 of these exons. In the adult human brain there are six tau isoforms that differ in the presence of either three or four microtubule-binding domains. In the brain with progressive supranuclear palsy, there is selective enrichment of tau isoforms that contain four microtubule-binding domains. Although the pathogenesis of progressive supranuclear palsy is unknown, there is increasing evidence of a genetic influence. One polymorphism in the tau gene, a dinucleotide repeat in the intron between exons 9 and 10, is associated with progressive supranuclear palsy at a greater-than-chance frequency. However, the role that a particular tau polymorphism may play in the pathogenesis of progressive supranuclear palsy remains to be elucidated. The brains of patients with progressive supranuclear palsy demonstrate tau pathology. Specifically, tau-immunopositive tufted astrocytes within the putamen and tau-immunopositive oligodendroglia within the white matter are seen. There is also an abundance of straight neurofibrillary tangles and neurophil threads consisting of hyperphosphorylated tau protein. In addition, there are neuronal loss, gliosis, and globose neurofibrillary tangles. Neuronal loss and gliosis are severe in the substantia nigra, subthalamic nucleus, globus pallidus (especially the internal portion), and superior colliculus. In some cases, neuronal loss is so severe in these areas that little remains but a skein of glia. Neuronal loss is slightly less prominent in the pretectum, locus ceruleus, periaqueductal gray matter, and substantia innominata. The brains of many patients show additional involvement of the motor nuclei in the brainstem (particularly the ocular motor nuclei), striatum, thalamus, dentate nucleus of the cerebellum, and basal forebrain. The distribution of globose neurofibrillary tangles largely parallels that of neuronal loss, but no efforts have been made to establish a quantitative correlation between the two findings. Subtle pathologic changes may be found in the cortex, especially in the frontal regions. The dopamine system is markedly abnormal. PET and postmortem studies have shown that dopamine in the striatum is profoundly depleted. Dopamine is preserved in the cortex, however, indicating sparing of the mesocortical dopamine projections. PET and postmortem autoradiographic studies indicate that pharmacologically defined D2 dopamine receptors are decreased in the striatum, but striatal D1 dopamine receptors are preserved. This situation contrasts with that found in Parkinson’s disease, in which striatal dopamine loss is associated with normal or elevated numbers of striatal D2 receptors. Consistent abnormalities have not been found in acetylcholine, serotonin, or norepinephrine levels. However, these neurotransmitters have been studied in only a few patients.
PET and SPECT have demonstrated decreased metabolic activity of the cortex, especially the frontal cortex, as well as the basal ganglia, thalamus, and pons. The observed metabolic abnormalities of the frontal cortex contrast with the relative lack of pathology seen by light microscopic analysis. Degeneration of the striatonigral axis probably contributes to parkinsonism in progressive supranuclear palsy but may not fully explain motor impairment. Changes in ‘8F-6-fluorodopa uptake measured with PET, an index of the integrity of nigrostriatal dopaminergic nerve terminals, do not correlate with the Hoehn and Yahr scale score, an index of parkinsonian disability. Loss of voluntary eye movements indicates compromise of the supranuclear brain structures, such as the superior colliculi and the frontal lobes, which regulate eye movements. Preservation of reflex eye movements indicates sparing of the neuromuscular apparatus directly responsible for eye movements (i.e., the ocular motor nuclei and their associated nerves and muscle). Internuclear ophthalmoplegia suggests involvement of the medial longitudinal fasciculus. Loss of reflex eye movements indicates that pathology has extended to the ocular motor nuclei themselves. Pseudobulbar palsy arises from bilateral degeneration of extrapyramidal structures. Recent evidence indicates that oxidative damage and mitochondrial dysfunction may play a role in the pathogenesis of progressive supranuclear palsy. Elevated levels of two markers of lipid peroxidation, malondialdehyde and 4-hydroxynonenal, have been found in the midbrain, subthalamic nucleus, and superior frontal cortex of brains from patients with progressive supranuclear palsy. Mitochondria from patients with progressive supranuclear palsy have been shown to have specific defects in complex I activity. One possible mechanism for the development of progressive supranuclear palsy is that subclinical defects in mitochondrial metabolism may produce pathologic consequences with the accumulation of age-dependent oxidative damage.
TREATMENT Efforts to treat progressive supranuclear palsy have sought to exploit the strategy of neurotransmitter replacement that has been successful in treating Parkinson’s disease. Some patients derive modest benefit from levodopa, but this benefit is rarely as dramatic as for patients with Parkinson’s disease, and it wanes rapidly. Nevertheless, when it is used judiciously, there is little risk to a trial of levodopa. The patient’s unsatisfactory response to levodopa over time often provides an important clue to the diagnosis of progressive supranuclear palsy. Three factors are likely to account for the failure of dopamine replacement in progressive supranuclear palsy: Loss of striatal D2 dopamine receptors may compromise the benefits of dopamine, the output of the basal ganglia is funneled through the internal globus pallidus (because the internal globus pallidus degenerates in progressive supranuclear palsy, any benefits of restoring striatal activity probably would be limited because striatal signals could not be transmitted to the rest of the brain), and widespread degeneration of subcortical structures besides the basal ganglia decreases the likelihood that simply normalizing basal ganglia function would restore normal brain function. Other approaches to treatment have included the use of direct dopamine receptor agonists, cholinergic agents, serotonin agonists or antagonists, and tricyclic antidepressants. These trials have been disappointing. The a’-adrenergic antagonist idazoxan was shown in a double-blind, placebo-controlled crossover study to amelio-
Chapter 121
rate imbalance and manual dexterity in a small number of patients, but the magnitude of improvement was small. The use of idazoxan is also hampered by side effects and limited availability. Treatment is otherwise palliative. Insomnia responds well to low dosages of trazodone. Focal areas of dystonia or painful rigidity can be treated with injections of botulinum toxin. Precautions to prevent falls and aspiration are important.
COURSE The syndrome of progressive supranuclear palsy worsens inexorably. Typical life expectancy from time of onset is about 5 years, although the range varies from 1 year to more than 2 decades. Patients are at risk for bone fractures and brain trauma from falls, sepsis, wound infections, and aspiration pneumonia. They eventually become unable to walk, speak, or swallow and often develop a fixed posture of dystonia in extension. Death is caused by intercurrent illness or inanition. It is important to provide patients and families with accurate information regarding the course and complications of progressive supranuclear palsy to help them make realistic plans for treating the secondary complications of the disorder when they occur.
UNRESOLVED ISSUES Careful observation since the 1960s has firmly established progressive supranuclear palsy as a clinicopathologic entity. Nevertheless, many issues regarding the disease are unresolved. For example, the nature and true extent of dementia in those with the disease must still be determined. The status of the cholinergic, noradrenergic, serotonergic, and amino acid neurotransmitter systems must be clarified. Understanding the potential involvement of neurotransmitter systems must incorporate new information provided by molecular biologic identification of multiple, previously unrecognized receptor subtypes. The significance of both tau-immunopositive neurofibrillary tangles and tauimmunopositive aggregates within astrocytes and oligodendroglia must be determined. In addition, the role of different tau polymorphisms in increasing the risk of developing progressive supranuclear palsy warrants further study. Beyond these phenomenologic issues are several more perplexing enigmas. Current understanding of the pathophysiology of basal ganglia disorders suggests that loss of dopamine results in parkinsonism by allowing overactivity of the inhibitory input from
W
Diffuse L e v Body Disease
773
the internal globus pallidus to the thalamus. Experimental and human studies suggest that destruction of the subthalamic nucleus or internal globus pallidus can restore normal thalamic activity and thereby ameliorate parkinsonism. Parkinsonism in progressive supranuclear palsy, a disorder in which there is concurrent degeneration of the substantia nigra, subthalamic nucleus, and internal globus pallidus, is not consistent with this scheme. This apparent paradox remains to be reconciled. However, it suggests that pallidotomy, which may be useful to treat intractable Parkinson’s disease, will not help patients with progressive supranuclear palsy. Furthermore, the pathophysiology of dementia in progressive supranuclear palsy, when it occurs, is obscure. Some suggest that degeneration of subcortical structures alone can cause dementia by deafferentating the cortex. Others believe that dementia occurs only when the brain is subject to a second, independent process, such as Alzheimer’s-type degeneration or infarction. A thud possibility is that the subtle cortical pathology in progressive supranuclear palsy observed by some indicates functionally significant pathology sufficient to impair cognition. Most importantly, the cause of neuronal degeneration in the disease is unknown. In short, the recognition and characterization of progressive supranuclear palsy have raised more questions than they have answered. Efforts to treat, and ultimately reverse, the effects of the disease will require answers to these questions. No experimental model of the disease exists. For the time being, at least, new insights into the disease will come from clinically based investigation. Patients should be informed about available research studies and encouraged to participate in them when appropriate.
SUGGESTED READINGS Agid Y, Javoy-Agid F, Ruberg M et al: Progressive supranuclear palsy: anatornoclinicaland biochemical considerations. pp. 191-206. In Yahr MD, Bergmann KJ (eds): Advances in Neurology. Vol. 45. Raven, New
York, 1986 Albers DS, Augood SJ: New insights into progressive supranuclear palsy. Trends Neurosci 24:347-352, 2001 Hughes AJ, Daniel SE, Kilford L, Lees AJ: Accuracy of cliiical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55181-184, 1992 Steele J C Progressive supranuclear palsy. Brain 95:693-705, 1972 Steele JC, Richardson JC, Olszewski J: Progressivesupranuclearpalsy. Arch Neurol 10:333-358, 1964
121 Diffuse L e w Bodv Disease 4
4
Daniel Z. Press Diffuse Lewy body disease (DLBD) is a recently defined but common neurodegenerative disorder that lies on the interface of movement disorders and dementia. The hallmarks of DLBD are cognitive decline, parkinsonism, visual hallucinations, and a fluctuating course. The clinical and pathologic features of DLBD place it between idiopathic Parkinson’s disease (PD) and Alzheimer’s disease (AD), overlapping both. Patients with DLBD can
present with typical PD; the diagnosis of DLBD becomes clear with the development of memory problems and visual hallucinations. Patients with DLBD can present primarily with cognitive symptoms suggesting AD, only early parkinsonism and visual hallucinations distinguish DLBD from AD. The prevalence of DLBD has not been clearly determined. Estimates range from 10% to 25% of all dementias, making it the second most common cause
Chapter 121
rate imbalance and manual dexterity in a small number of patients, but the magnitude of improvement was small. The use of idazoxan is also hampered by side effects and limited availability. Treatment is otherwise palliative. Insomnia responds well to low dosages of trazodone. Focal areas of dystonia or painful rigidity can be treated with injections of botulinum toxin. Precautions to prevent falls and aspiration are important.
COURSE The syndrome of progressive supranuclear palsy worsens inexorably. Typical life expectancy from time of onset is about 5 years, although the range varies from 1 year to more than 2 decades. Patients are at risk for bone fractures and brain trauma from falls, sepsis, wound infections, and aspiration pneumonia. They eventually become unable to walk, speak, or swallow and often develop a fixed posture of dystonia in extension. Death is caused by intercurrent illness or inanition. It is important to provide patients and families with accurate information regarding the course and complications of progressive supranuclear palsy to help them make realistic plans for treating the secondary complications of the disorder when they occur.
UNRESOLVED ISSUES Careful observation since the 1960s has firmly established progressive supranuclear palsy as a clinicopathologic entity. Nevertheless, many issues regarding the disease are unresolved. For example, the nature and true extent of dementia in those with the disease must still be determined. The status of the cholinergic, noradrenergic, serotonergic, and amino acid neurotransmitter systems must be clarified. Understanding the potential involvement of neurotransmitter systems must incorporate new information provided by molecular biologic identification of multiple, previously unrecognized receptor subtypes. The significance of both tau-immunopositive neurofibrillary tangles and tauimmunopositive aggregates within astrocytes and oligodendroglia must be determined. In addition, the role of different tau polymorphisms in increasing the risk of developing progressive supranuclear palsy warrants further study. Beyond these phenomenologic issues are several more perplexing enigmas. Current understanding of the pathophysiology of basal ganglia disorders suggests that loss of dopamine results in parkinsonism by allowing overactivity of the inhibitory input from
W
Diffuse L e v Body Disease
773
the internal globus pallidus to the thalamus. Experimental and human studies suggest that destruction of the subthalamic nucleus or internal globus pallidus can restore normal thalamic activity and thereby ameliorate parkinsonism. Parkinsonism in progressive supranuclear palsy, a disorder in which there is concurrent degeneration of the substantia nigra, subthalamic nucleus, and internal globus pallidus, is not consistent with this scheme. This apparent paradox remains to be reconciled. However, it suggests that pallidotomy, which may be useful to treat intractable Parkinson’s disease, will not help patients with progressive supranuclear palsy. Furthermore, the pathophysiology of dementia in progressive supranuclear palsy, when it occurs, is obscure. Some suggest that degeneration of subcortical structures alone can cause dementia by deafferentating the cortex. Others believe that dementia occurs only when the brain is subject to a second, independent process, such as Alzheimer’s-type degeneration or infarction. A thud possibility is that the subtle cortical pathology in progressive supranuclear palsy observed by some indicates functionally significant pathology sufficient to impair cognition. Most importantly, the cause of neuronal degeneration in the disease is unknown. In short, the recognition and characterization of progressive supranuclear palsy have raised more questions than they have answered. Efforts to treat, and ultimately reverse, the effects of the disease will require answers to these questions. No experimental model of the disease exists. For the time being, at least, new insights into the disease will come from clinically based investigation. Patients should be informed about available research studies and encouraged to participate in them when appropriate.
SUGGESTED READINGS Agid Y, Javoy-Agid F, Ruberg M et al: Progressive supranuclear palsy: anatornoclinicaland biochemical considerations. pp. 191-206. In Yahr MD, Bergmann KJ (eds): Advances in Neurology. Vol. 45. Raven, New
York, 1986 Albers DS, Augood SJ: New insights into progressive supranuclear palsy. Trends Neurosci 24:347-352, 2001 Hughes AJ, Daniel SE, Kilford L, Lees AJ: Accuracy of cliiical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55181-184, 1992 Steele J C Progressive supranuclear palsy. Brain 95:693-705, 1972 Steele JC, Richardson JC, Olszewski J: Progressivesupranuclearpalsy. Arch Neurol 10:333-358, 1964
121 Diffuse L e w Bodv Disease 4
4
Daniel Z. Press Diffuse Lewy body disease (DLBD) is a recently defined but common neurodegenerative disorder that lies on the interface of movement disorders and dementia. The hallmarks of DLBD are cognitive decline, parkinsonism, visual hallucinations, and a fluctuating course. The clinical and pathologic features of DLBD place it between idiopathic Parkinson’s disease (PD) and Alzheimer’s disease (AD), overlapping both. Patients with DLBD can
present with typical PD; the diagnosis of DLBD becomes clear with the development of memory problems and visual hallucinations. Patients with DLBD can present primarily with cognitive symptoms suggesting AD, only early parkinsonism and visual hallucinations distinguish DLBD from AD. The prevalence of DLBD has not been clearly determined. Estimates range from 10% to 25% of all dementias, making it the second most common cause
774
Movement Disorders
Parkinson’s Disease and Parkinson-like Syndromes
rn TME 121-1. Consensus Criteria for the Clinical Diagnosis of Probable and Possible DLBD The central feature of DLBD is progressive cognitive decline affecting normal social or occupational function. Prominent or persistent memory impairment may not be present at onset but generally develops with progression. Prominent deficits generally include attention, visuospatial function, and frontal-subcortical skills (working memory, executive function, slowed processing). Two of the following core features are necessary for a diagnosis of probable DLBD, and one is necessary for possible DLBD: Fluctuating cognition with marked variations in attention and alertness Recurrentvisual hallucinations Spontaneous motor features of parkinsonism Features supportive of the diagnosis are Repeated falls Syncope Transient loss of consciousness Neuroleptic sensitivity Systematized delusions Hallucinations in other modalities A diagnosis of DLB is less likely in the presence of Stroke, with evidence of focal neurologic signs or ischemic lesion on imaging Evidence on examination of a different illness or brain disorder sufficient to account for the clinical picture Adapted from McKeith IG, Calasko D, Kosaka K et al: Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB internationalworkshop. Neurology 47:1113-1124, 1996.
of dementia in older adults, following only Alzheimer’s disease. Diagnostic criteria for DLBD with good specificity have been established (Table 121-l),but the sensitivity of the criteria are not as good. Thus, DLBD often is misdiagnosed as AD. Despite these difficulties, many patients present in a characteristic manner, and in these cases the clinician can be fairly confident in the diagnosis and consider specific treatments.
To complicate nosologic and pathologic matters further, the majority of cases of DLBD have some degree of concomitant Alzheimer’s changes. Amyloid plaques are more common than neurofibrillary tangles. The extent of AD changes is variable, and a subgroup of cases exist without any plaques or tangles, confirming that “pure” DLBD is sufficient to cause dementia. Various names have been proposed to express the frequent overlap of AD and DLBD, including “Lewy body variant AD” and the less specific “dementia with Lewy bodies”, which encompasses any dementing illness associated with Lewy bodies. One way of sorting these mixed disorders is to view DLBD as existing along two spectra, one being the degree of Alzheimer’s changes and the other the degree of cortical and subcortical Lewy bodies (Fig. 121-1). Although these distinctions are useful in theory, distinguishing between the groups antemortem is not yet possible. DIAGNOSIS The criteria for diagnosis are solely clinical. Progressive cognitive decline is necessary, but additional features must be present: fluctuations in cognition and alertness, recurrent formed visual hallucinations, or motor features of parkinsonism (Table 121-1). DLBD is also strongly associated with REM sleep behavior disorder (RBD), and RBD supports the diagnosis of DLBD. There are no serologic markers for the disorder. The ApoE4 genotype is more common in both DLBD and AD but is not sufficiently common to be clinically useful for diagnosis. The clinical criteria are as follows.
Progressive Cognitive Decline The cognitive profile of DLBD is similar to that of AD. Both diseases impair memory, naming, visuospatial function, and
PATHOPHYSIOLOGY The role of Lewy bodies in the pathophysiology of both DLBD and PD remains a mystery. Lewy bodies are intracytoplasmic, spherical eosinophilic neuronal inclusions that are the neuropathologic signature of idiopathic PD. They contain a number of proteins, including ubiquitin and a-synuclein. Lewy bodies typically are found in subcortical nuclei such as the substantia nigra, where they are easily visualized with routine stains. In contrast, cortical Lewy bodies are difficult to visualize on routine studies. Specialized stains for their constituent proteins have aided greatly in their identification and in the development of pathologic criteria for diagnosing DLBD. In DLBD, Lewy bodies are particularly common in limbic regions such as the cingulate, entorhinal cortex and amygdala. In the nonlimbic cortex, the temporal lobe usually is more affected than the frontal and parietal lobes. With careful pathologic review, nearly all cases with cortical Lewy bodies have some Lewy bodies in subcortical regions and vice versa. Lewy body disorders vary along two dimensions: parkinsonism and dementia. In PD subcortical Lewy bodies predominate, and the clinical feature is a movement disorder. In DLBD cortical Lewy bodies predominate, and the clinical presentation is of dementia. The severity of the dementia in DLBD correlates with the number of cortical Lewy bodies seen pathologically. Some patients with PD clinically and without dementia also have large numbers of cortical Lewy bodies postmortem. Although the general correlation of cortical Lewy bodies with dementia is strong, cortical Lewy bodies are not pathognomonic of dementia.
Subcortical
Cortical
Lewy Body Distribution FIG. 121-1. A schematic overview categorizing the overlap between lewy body disorders and Alzheimer‘s disease based on the severity of the Alzheimer‘s pathology and the distribution of the Lewy bodies. Dementia with Lewy bodies is the inclusive term. PD = Parkinson’s disease; AD = Alzheimer‘s disease; DLB = Dementia with Lewy bodies; and DLBD = Lewy Body Disease.
Chapter 121 W
T a m 121-2. Differential Diagnosis of Parkinsonism and Dementia
Diffuse Lewy body disease Alzheimefs disease Frontotemporaldementia Normal pressure hydrocephalus Vascular dementia Progressive supranuclear palsy Corticobasalganglionicdegeneration Multiple system atrophy Dementia pugilistica Wilson’s disease
executive or frontal lobe function. There are some potentially useful clinical distinctions between the disorders. Patients with DLBD often have unusually severe visuospatial deficits and disproportionate cognitive slowing on timed tasks. Their memory usually fails at the retrieval stage (they may recognize items that they could not recall) as compared to the failure of storage in AD (the information is lost completely). The rate of progression of dementia in DLBD generally is slightly faster than AD, but there is a great deal of overlap.
Parkinsonism Estimates of the rate of parkinsonian signs in DLBD range from 45% to loo%, probably because of differences in ascertainment and definition. When parkinsonian signs are present in DLBD, they closely mirror those of idiopathic Parkinson’s disease. Rigidity and bradykinesia are present in approximately 90% of both groups. Rest tremor is less common in DLBD but still present in 55%, as compared to 85% of patients with PD. The parkinsonian symptoms of DLBD usually are mild. They are levodopa responsive but generally do not warrant treatment. Parkinsonism can be seen in other neurodegenerative disorders including AD, frontotemporal dementia, and vascular dementia (Table 121-2). The presence of tremor and the treatment responsiveness favor the diagnosis of DLBD from the other non-PD parkinsonian syndromes.
Visual Hallucfnatlons Approximately 80% of patients with DLBD have visual hallucinations. Visual hallucinations are very rare in AD in the absence of ocular causes, and their presence is highly suggestive of DLBD. The hallucinations often are of people or animals and resemble those seen as a side effect of excessive dopaminergic stimulation in patients with PD. Some degree of insight into their nature generally is present, but this recedes over the course of the disease. The hallucinations are not typically threatening and may upset the caregiver more than the patient. Hallucinations occasionally are associated with paranoid delusions or delusional beliefs that loved ones have been replaced (Capgras’s syndrome).
Fluctuations in Cognition and Alertness Unlike with AD, patients with DLBD often show marked variations in cognitive performance and level of alertness that can be discerned by caregivers. Fluctuations can occur rapidly, over a minutes to hours, or very gradually over weeks to months. The depth of the fluctuations can range from episodes of simple daytime sleepiness or mild impairments in concentration to
Diffuse Lewy Body Disease
77s
episodes of wakeful unresponsiveness, or “going blank.” The short-term fluctuations in cognition and in level of arousal recently have been shown to correlate closely with rapid changes (over seconds) in the electroencephalogram background frequency. These fluctuations probably are caused by damage to brainstem alerting and arousal systems.
Sleep Disorders In REM sleep behavior disorder (RBD), the normal atonia of REM sleep does not occur, allowing movements, often vigorous, during REM periods, as if acting out dreams. The best clinical assessment for RBD is to ask a patient’s bed partner if there are abnormal, even violent movements during sleep. RBD is a frequent precursor of PD, with one study finding that 38% of patients develop a parkinsonian disorder. RBD often is associated with dementia, and 90% of patients with both diagnoses meet clinical criteria for DLBD. In the few cases that have come to autopsy, the diagnosisof DLBD has been confirmed pathologically.
Neuroimadng Routine neuroimaging with magnetic resonance imaging or computed tomography is not clinically definitive in separating DLBD from AD or PD, but it is essential to diagnose vascular dementia and normal pressure hydrocephalus, both of which have parkinsonian features and dementia. Distinguishing DLBD from AD is more of a challenge. An absence of medial temporal lobe atrophy on structural magnetic resonance imaging suggests DLBD rather than AD, but if medial temporal lobe atrophy is present, either diagnosis is possible. Functional studies of nigrostriatal dopamine function with ‘8F-fluorodopapositron emission tomography scanning may separate DLBD from AD, but this technique has not been validated and is generally not clinically available.
TREATMENT There is no treatment to slow the progression of the neurodegeneration in DLBD. A large subset of patients with DLBD have concomitant Alzheimer’s changes, predominantly amyloid plaques. One study has shown that large dosages of vitamin E (a-tocopherol), 1000 IU twice daily, may slow the progression of AD and are very well tolerated. Although vitamin E has not been specifically tested in DLBD, it is a reasonable agent to prescribe. In the future, agents that either specifically prevent a-synuclein deposition in Lewy bodies or prevent amyloid deposition in plaques would be worthwhile agents to investigate. Symptomatic treatment options are available, but the side effects often worsen some feature of the disease. The parkinsonism in DLBD responds to dopaminergic agents. Levodopa is less likely than dopamine agonists to worsen hallucinations. Anticholinergics should be avoided because of the likelihood of markedly worsening the cognitive symptoms. Levodopa should be used only when motor symptoms are functionally limiting, and it should then be used at the lowest effective dosage (generally 150 to 300 mg levodopa divided into three daily doses). If hallucinations worsen during treatment, there are two options: lower or discontinue the medicine or introduce a low dosage of an atypical neuroleptic. Visual hallucinations occur in DLBD even without the provocation of levodopa. Whether provoked or spontaneous, visual hallucinations often can be managed without medication. They
776
Movement Disorders
Parkinson's Disease and Parkinson-like Syndromes
often occur in patients with impaired vision, so efforts to maximize visual acuity, such as keeping rooms well lit and treating any primary visual problems, are helpful. If the hallucinations are not disturbing to the patient, then educating the family in how to adapt to them may be sufficient. If the hallucinations are disturbing or debilitating to the patient or the family, then a trial of an atypical neuroleptic is warranted. Very low dosages of clozapine (6.25 to 37.5 mg) have been demonstrated to treat hallucinations in PD without exacerbating the parkinsonism. Concerns over agranulocytosis,excessive sedation, and lowering of seizure threshold makes this agent less practical clinically. Low dosages of quetiapine or olanzapine may be more practical, although neither has been well investigated. Risperidone often is considered to be an atypical neuroleptic but clearly worsens parkinsonism in patients with dementia and should be avoided. Typical neuroleptics can induce profound, even fatal worsening of the parkinsonism and should be avoided in any patient in whom DLBD is a diagnostic consideration. Another useful treatment is cholinesterase inhibitors. The cholinergic deficit in DLBD often is even more severe than that of AD. Open-label trials and one multicenter, double-blind, placebocontrolled study confirm that cholinesterase inhibitors can both improve the cognitive symptoms and ameliorate many of the psychiatric symptoms without worsening the parkinsonism. The three agents currently available are donepezil, rivastigmine, and galantamine. They appear to be equally effective. Side effects of both result primarily from their cholinomimetic properties (nausea, vomiting, headaches, and excessively vivid dreams). Because confusion, hallucinations, sleep disturbance, and delusions may appear early and repeatedly in the course of DLBD, home care of patients with DLBD often is very difficult for caregivers. The symptoms of DLBD often lead to nursing home placement, regardless of the underlying diagnosis. Efforts to support families through the course of the disease are crucial. The assistance of well-trained social workers should be sought early in the course of the disease. Preparation will allow a much smoother transfer if nursing home care becomes necessary.
PROGNOSIS
diagnosis is predicated on specific features including parkinsonism, dementia, visual hallucinations, and fluctuating levels of attention. Symptomatic treatment is available, but side effects generally limit the benefit. Cholinesterase inhibitors are an exception and can improve both the dementia and the psychiatric symptoms. DLBD probably represents more than just the manifestations of the pathologic overlap of two common disorders, PD and AD. Clarification will include a better understanding of the pathophysiology of cortical Lewy bodies and the ability to clinically discern the degree of AD changes and Lewy body changes in patients antemortem.
ACKNOWLEDGMENT This work was supported by NIH grant NS10980. Special thanks to Michael P. Alexander, MD, for editorial review.
SELECTED READINGS Barber R, Gholkar A, Scheltens P et ak Medial temporal lobe atrophy on MRI in dementia with Lewy bodies. Neurology 52:1153-1158, 1999 Boeve BF, Silber MH, Ferman TJ et ak REM sleep behavior disorder and degenerative dementia: an association likely reflecting Lewy body disease. Neurology 51:363-370, 1998 Hu XS, Okamura N, Arai H et al: "F-Fluorodopa PET study of striatal dopamine uptake in the diagnosis of dementia with Lewy bodies. Neurology 55:1575-1577, 2000 Lennox G: Dementia with Lewy bodies. pp. 67-79. In Growdon J, Rossor M (eds): The Dementias. Vol. 19. Butterworth-Heinemann, Boston, 1998
Louis ED, Klatka LA, Liu Y, Fahn S: Comparison of extrapyramidal features in 31 pathologically confirmed cases of diffuse Lewy body disease and 34 pathologically confirmed cases of Parkinson's disease. Neurology 48:37&380, 1997 Luis CA, Barker WW, Gajaraj K et ak Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 14:526-533, 1999 McKeith IG, Galasko D, Kosaka K et ak Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB international workshop. Neurology 47~1113-1124, 1996
The rate of progression of DLBD is somewhat quicker than that of PD or AD. The mean survival from diagnosis for DLBD generally is between 6 and 9 years, as compared to 8 to 11 years for PD and AD.
McKeith IG, Grace JB, Walker Z et al: Rivastigmine in the treatment of dementia with Lewy bodies: preliminary findings from an open trial. Int J Geriatr Psychiatry 15:387-392, 2000 McKeith IG, Perry EK, Perry RH: Report of the second dementia with Lewy body international workshop: diagnosis and treatment. Neurol-
SUMMARY
Salmon DP, Galasko D, Hansen LA et al: Neuropsychological deficits associated with diffuse Lewy body disease. Brain Cogn 31:14&165,
O ~ Y53:902-905,
Many of the manifestations of DLBD reflect the underlying pathology of both cortical Lewy bodies and frequent Alzheimer's changes. A number of fundamental questions about the pathophysiology and the nosology remain. The accurate clinical
1999
1996
Walker MP, Ayre GA, Cummings JL et ak Quantifying fluctuation in dementia with Lewy bodies, Alzheimer's disease, and vascular dementia. Neurology 541616-1625, 2000
Chapter 122 W
Corticobasal Degeneration
777
122 Corticobasal Degeneration Lewis R. Sudarsky
HISTORY This disease was first described by Rebeiz, Kolodny, and Richardson in 1968. The original report featured clinical and neuropathologic findings in three patients; all three presented with an asymmetrical akinetic-rigid syndrome, involuntary movements, and signs of cortical dysfunction. Because of the distinctive,poorly staining ballooned neurons seen at postmortem, the entity was called corticodentatonigral degeneration with neuronal achromasia. This descriptive term has evolved into corticobasal degeneration (CBD), now an accepted designation for the syndrome and pathology detailed in this chapter. Corticobasal degeneration is most often seen in a Parkinson’s practice or movement disorder clinic; it is substantially less common than progressive supranuclear palsy (PSP) or multiplesystem atrophy. Typical patients present with a movement disorder and are observed to have cortical signs. There is usually no family history of this or any related neurodegenerative disease. We now appreciate that classic CBD is part of a broader clinical spectrum. Patients who present in this fashion with a motor control disorder have neuropathologic features in common with patients who present with frontal dementia (see Chapter 138) or restricted cognitive impairment (e.g., primary progressive aphasia). CBD may be more difficult to recognize when cognitive change is the salient presenting feature.
PATHOLOGY AND RELATlONSHlP TO PICK‘S DISEASE Postmortem examination of the brain reveals cortical atrophy with ventricular enlargement. Most of the atrophy is frontoparietal, particularly affecting the perirolandic cortex. There is also a degree of gross atrophy and evidence of neuronal degeneration in the basal ganglia and thalamus. Involvement of the forebrain is characteristically asymmetrical. In the brainstem, there is loss of pigmented cells from the substantia nigra. Microscopic examination of the cortex and basal ganglia reveals neuronal loss and gliosis. There are ballooned neurons, which stain poorly with standard neuropathologic techniques. These are similar to the ballooned neurons observed in Pick’s disease, although there are no Pick bodies in CBD. Other findings include globose neurofibrillary tangles, neuronal inclusions, and astrocytic plaques that immunostain densely for tau protein. A four-repeat isoform of tau protein is deposited in the brain in CBD, as is the case in PSP. These cytoskeletal markers suggest a relationship between CBD, PSP, Pick‘s disease, and other neurodegenerative diseases characterized by tau protein pathology and aggregation (tauopathies).
CLINICAL PRESENTATION CBD typically presents in the sixth, seventh, or eighth decade of life. Onset is gradual and insidious, as with any neurodegenerative disease. A majority of patients (64% in series of Rinne et al.) begin with sensorimotor disability in one arm or hand. Some present with imbalance and difficulty walking. The disorder is distinctly
asymmetrical, and asymmetry can often be appreciated on imaging studies. Enough of the typical features are present within a year to allow recognition and diagnosis. Patients exhibit a combination of motor features and cortical signs (Table 122-1). The most typical cases begin as an asymmetrical, bradykinetic or rigid disorder, a hemi-Parkinsonian syndrome without rest tremor. The disability in the involved hand often is out of proportion to the amount of bradykinesia. Response to levodopa usually is partial and not sustained. Over time patients identify the affected limb as awkward and useless and preferentiallyuse the other side. With progression, the patient may exhibit a dystonic hand; alien limb phenomena develop in 50% of patients over the first 2 years. Hand dystonia may be severe, with clawing of one or two fingers into the palm, producing skin maceration. In the series of Rinne et al., 28% of patients presented with a gait disorder: stiffness and disequilibrium, shuffling, and sometimes an awkward dystonic gait. These patients progressed to exhibit imbalance and postural instability, sometimes unexplained backwards falls. Those whose illness began in the lower limbs often had falls within a year. Other motor features characterize CBD in the first 3 years, including myoclonus, dysarthria, and an oculomotor disorder. Myoclonus may be observed in the more involved limb as a component of the rigidity and dystonia or bilaterally in the upper limbs, with action producing a “jerky action tremor.” This myoclonus often is stimulus sensitive. Dysarthria often is present within a year of onset, sometimes earlier if patients exhibit pronounced oral or buccal apraxia. The oculomotor features are not specific; slow saccades often are observed. Head thrusts or eye blinks may be needed to initiate gaze to the side. Some patients develop apraxia of lid opening. In addition to motor features, patients with CBD exhibit signs of cortical dysfunction. These also are most typically asymmetrical and focal, rather than global, although 7 of 36 patients (19%) in the series of Rinne et al. had some generalized cognitive impairment. Cortical sensory loss often is an early feature, and some patients have sensory complaints at presentation. Examination may reveal tactile extinction, astereognosis, or agraphesthesia in the presenting limb. Many patients with otherwise typical
rn TAME122-1. Early Clinical Features of Corticobasal Degeneration Insidious onset, age 50-80 (mean age 60) Motor features &ymmetrical, akinetic-rigid disorder Imbalance or postural instability Upper limb dystonia Myoclonus, “jerky action tremor oculomotor disorder: slow saccades, head thrusts to initiate gaze Cortical signs ldeomotor apraxia Cortical sensory loss Alien limb Dhenomena
778
Movement Disorders H Parkinson’s Disease and Parkinsonian Syndromes
Parkinson’s disease have sensory complaints, but sensory loss sets this illness apart, Apraxia in CBD is also evident principally in the most affected limb and must be distinguished from clumsy execution caused by primary motor deficit. Ideomotor apraxia (using the terminology of Heilman) usually is observed and is correlated with regional involvement of cerebral cortex (the parietal lobe and supplemental motor area). Alien limb movements develop in 50% of patients over the first 2 years, and these movements make CBD distinctive among neurodegenerative disorders. The limb, usually the more severely affected arm and hand, will wander in a semipurposeful fashion. It will often grope for and grasp objects, sometimes manipulating objects involuntarily. It may actively interfere with the use of the other arm. Patients describe their limb as “having a mind of its own” but generally do regard it as part of their own body, in contrast to the alien limb of patients with ischemic neurologic deficits involving the parietal lobe. Imaging studies (computed tomography, magnetic resonance imaging) usually reveal asymmetrical cerebral volume loss, most dramatic in the perirolandic cortex. Single photon emission computed tomography and positron emission tomography studies show reduced metabolism in frontal and parietal regions, thalamus, and basal ganglia. Markers of dopaminergic function such as 18F-DOPAuptake and ‘231-P-CITdemonstrate a loss of nigrostriatal dopamine neurons in patients with CBD. Physiologic studies also show abnormalities in patients with more advanced disease. Electroencephalogram shows asymmetrical slowing, and action myoclonus may be recorded using surface electromyography. DIFFERENTIAL DIAGNOSIS
At the initial presentation, CBD can easily be mistaken for Parkinson’s disease, which is substantially more common. The diagnosis should be considered in a patient with unilateral Parkinsonism unresponsive to levodopa, especially if there are elements of apraxia in the affected limb. Once all the findings have unfolded, CBD is a distinctive syndrome and is usually recognized easily by clinicians who have encountered it previously. In a clinicopathologic study from the National Institutes of Health, the sensitivity was low (35%) but the specificity near perfect when cases were reviewed based on findings at the first visit. In a group of patients with neurodegenerative disorders, the best predictive correlation with the diagnosis of CBD was for patients with limb dystonia, apraxia, myoclonus, and asymmetry. The clinical picture begins to blur after 3 or 4 years, and the appearance of late-stage patients is less distinctive. A variety of neurodegenerative diseases can cause abnormalities of cortical function and Parkinsonism. A differential diagnosis composed from this list includes PSP, frontotemporal dementia with Parkinsonism, multiple-system atrophy, diffuse Lewy body disease, Parkinson’s with dementia, and Alzheimer’s with extrapyramidal features. Making a pathologic diagnosis based on clinical features at this stage is not always easy. Again, marked asymmetry, early apraxia, and sensory loss favor a diagnosis of CBD. NATURAL HISTORY AND TREATMENT
The course of neurodegeneration in CBD is progressive, and the illness is substantially more aggressive than Parkinson’s disease. As a rule, there are bilateral signs with a degree of generalized rigidity in 3 to 5 years. Loss of ambulation usually occurs within this time frame, earlier if the illness begins in the lower limbs. In the
study of Wennig et al., mean duration of illness to death was 7.9 years. In the series of Rinne et al., follow-up examination at 5 years found that the disability had spread to an arm and leg in 80% and four limbs in 73%. The presenting limb invariably was dystonic and fixed. Dysarthria and dysphagia are a substantial problem as the illness progresses. Ninety percent of patients exhibit oculomotor problems, including difficulty with gaze initiation, at 5 years. Therapeutic options are not very satisfactory. Most of the treatment is symptomatic and supportive because there is no disease-modifymg therapy. There is dwindling response to dopaminergic medications after the first year. Clonazepam is used to control myoclonus with some benefit. Baclofen sometimes is used to treat rigidity. Physical therapy is used to maintain mobility, and assistive devices can help with ambulation unless postural instability is advanced or apraxia makes use of a walker problematic. When dysphagia progresses and begins to produce aspiration, patients must decide whether to pursue a feeding gastrostomy. OVERLAP WITH PSP AND OTHER NEURODEGENERATIVE DISEASES
At a more advanced stage, with generalized rigidity, postural instability, and elements of supranuclear gaze palsy, the syndrome of CBD overlaps with PSP. Some patients who appear to have CBD at presentation develop a more symmetrical, akinetic-rigid disorder with severe oculomotor difficulty. A number of these overlap patients have the pathology of PSP at postmortem. (Patients with CBD typically exhibit more apraxia than patients with PSP, which may be a useful distinguishing feature.) In a recent study at the Mayo Clinic, 13 patients identified during life with CBD were retrospectively reviewed after postmortem examination. Pathology was that of CBD in seven but was that of another neurodegenerative disease in six. This experience suggests that the clinical syndrome of CBD, however distinctive, may not be a homogenous morbid entity. We need a better understanding of the neurobiology of the disease and identification of biological markers to help with diagnosis within this family of neurodegenerative disorders. It is hoped that new insights about the neurobiology of the tauopathies will lead to a novel therapeutic strategy for this and related diseases. SUGGESTED READINGS
Bergeron C, Pollanen S , Weyer L et al: Unusual clinical presentations of cortico-basal ganglionic degeneration. Ann Neurol 40:893-900, 1996 Boeve BF, Maraganore DM, Parisi JE et ak Pathologic heterogeneity in clinically diagnosed corticobasal degeneration. Neurology 53:795-800, 1999
Gibb WRG, Luthert PJ, Marsden CD: Corticobasal degeneration. Brain 112~1171-1192, 1989
Litvan I, Agid Y, Goetz C et ak Accuracy of the clinical diagnosis of corticobasal degeneration: a clinico-pathologic study. Neurology 48: 119-125, 1997
Rebeiz JJ, Kolodny EH, Richardson E P Corticodentatonigral degeneration with neuronal achromasia. Arch Neurol 18:20-33, 1968 Riley DE, Lang AE, Lewis A et ak Cortical-basal ganglionic degeneration. Neurology 401203-1212, 1990 Rinne 70, Lee MS, Thompson PD, Marsden CD: Corticobasal degeneration: a clinical study of 36 cases. Brain 117: 1183-1 196, 1994 Wennig GK, Litvan I, Jankovic J et al: Natural history and suMval of 14 patients with corticobasal degeneration confirmed at autopsy. J Neurol
Neurosurg Psychiatry 64184-189,
1998
Chapter 123
Secondaly Parkinsonism
779
123 Secondary Parkinsonism Jeffrey D. Macklis
In addition to idiopathic Parkinson’s disease, a wide variety of more common and more rare disorders can present with similar symptoms of parkinsonism, mimicking the clinical presentation of Parkinson’s disease to varying degrees. Depending on the age of the patient, relevant concurrent illness, clinical circumstances, time course, and specifics of the neurologic examination, investigating these possibilities may include only clinical awareness or in-depth laboratory and neuroimaging evaluation. This chapter briefly reviews some of the more relevant causes of secondary parkinsonism, roughly in the order of decreasing prevalence in most practice settings. The complex of parkinsonian symptoms, including cogwheel rigidity, bradykinesia, rest tremor, and postural instability, can result in part from dysfunction at a variety of levels in the nigrostriatal system, most commonly resulting in functional dopamine deficiency. Therefore, disruption of this system by drugs or infarction in the striatum, imbalance of dopaminergic versus cholinergic striatal innervation, or toxic or viral injury to nigral neurons themselves can cause symptoms that alone can be difficult to differentiate from the idiopathic nigral neuron degeneration of Parkinson’s disease. In general, neurodiagnostic studies are most helpful in ruling out various secondary parkinsonian syndromes and other distinct diseases. In the current climate of health care cost containment, it is not warranted and not feasible to investigate all possibilities in all patients; this chapter may provide a framework in which to choose how extensive a diagnostic evaluation to pursue and in which direction to proceed.
DRUG-INDUCED PARKINSONISM Almost as common as idiopathic Parkinson’s disease is parkinsonism resulting from prescribed medication. Historically, this has resulted most commonly from the antipsychotic and antiemetic phenothiazines (chlorpromazine and related compounds), butyrophenones (haloperidol and related compounds), and metoclopramide. More recently, the introduction of the newer classes of atypical antipsychotics such as clozapine, respiridol, and olanzapine have reduced the incidence of such syndromes somewhat because these agents are thought much less likely to induce secondary parkinsonism. However, though seemingly much less common with these agents, secondary parkinsonian syndromes still arise as a result of these drugs. Extremely rarely, and typically only at very high dosages, secondary parkinsonism can result from the antihypertensives reserpine and methyldopa. Although case reports of parkinsonism from piperazine derivative calcium channel blockers and the antiarrhythmic amiodarone exist, the significance is uncertain, and these agents are rare in most clinical settings. The standard neuroleptic compounds exert their action at least partially via dopaminergic blockade within the striatum, and reserpine and methyldopa act via dopamine depletion. Druginduced parkinsonism can occur at all ages and usually is readily treated by dosage adjustment or withdrawal. Diagnosis is by careful elicitation of medication history and by diagnostic or therapeutic dosage reduction. It may not be possible
to eliminate all parkinsonian features while maintaining successful antipsychotic treatment, but diagnosis sometimes can help with choices among alternative antipsychotic or sedative medications. Although the atypical antipsychotic medications have a much lower incidence of parkinsonian side effects, clozapine necessitates complex monitoring for the risk of neutropenia, so respiridol and olanzapine have become preferred agents in this class. Although the occurrence of parkinsonian side effects in a population is not clearly dose dependent, on an individual basis the effects of all of these compounds are dose dependent and fully reversible. Resolution of symptoms takes days to weeks after discontinuation and should leave no residual symptoms or signs (although rarely months to years must pass until full resolution). Of course, idiopathic Parkinson’s disease may exist as an underlying illness and may be worsened by pharmacotherapy with these agents, in which case small dosages may cause pronounced symptoms.
VASCULAR PARKINSONISM Vascular infarction or compromise in the striatum or subcortical white matter can mimic some aspects of idiopathic Parkinson’s disease. Most often, this takes the form of small vessel disease, resulting in multiple lacunar infarctions. Because the average age of onset for Parkinson’s disease (approximately60) falls within the range common for stroke, the clinical circumstances,presentation, and constellation of clinical signs are central to correct diagnosis. In addition, it is not uncommon for small vessel disease and multiple appropriately placed lacunae to coexist with idiopathic Parkinson’s disease. Although the diagnosis of the primary cause of parkinsonism in these mixed cases can be imperfect and highly dependent on the relative progression of pyramidal and extrapyramidal signs over time, diagnosis can be aided by observing the response to dopaminergic medication. However, more commonly, the clinical onset and signs are more easily differentiated between idiopathic Parkinson’s disease and parkinsonism resulting from multiple infarctions. This diagnosis initially was used to suggest a cause for Parkinson’s disease in the late nineteenth century. It continued through periods of favor and disfavor over the next century and now is used more generically to describe secondary parkinsonism resulting from vascular disease. Although controversial in the past, this broader use provides a framework in which to view an important and common part of the differential diagnosis of secondary parkinsonism. Attention to diagnosing vascular disease and managing underlying risk factors can be important in avoiding complications of occult hypertension and cardiovascular disease in addition to avoiding largely ineffective dopaminergic therapy with potentially important cardiovascular side effects. Vascular parkinsonism most commonly occurs in patients with multiple risk factors for small vessel disease, especially hypertension and prior history of stroke. Lacunar infarctions in the striatum and subcortical white matter (or less often the brainstem or cerebellum) can occur in relative clinical silence in a diffuse
780
Movement Disorders
Parkinson’s Disease and Parkinsonian Syndromes
bilateral distribution or with a clearly ictal onset. Therefore, the presentation typically is either subacute and symmetrical (unlike the typically asymmetrical presentation for idiopathic Parkinson’s disease) or acute and unilateral. Stepwise progression can occur, but such a clear history is uncommon given the often subtle initial symptoms of these small infarctions. Rest parkinsonian tremor, festination, and seborrhea are uncommon, whereas associated pyramidal signs and superimposed gegenhalten rigidity often are present. Dementia, pseudobulbar palsy, and cerebellar signs can also be present, depending on the distribution of vascular infarction. Diagnosis can be aided by neuroimaging, especially by magnetic resonance imaging to look for an appropriate distribution of lacunar infarctions or small vessel disease. The most common imaging findings are multiple infarcts in the caudate, putamen, or globus pallidus. Response to levodopa often is not as successful as in Parkinson’s disease because the lack of dopamine processing by nigral neurons typically is not the limiting disorder. Often, as with other subtle stroke symptoms and signs, gradual resolution can occur in the absence of specific therapy. Alternatively, vascular parkinsonism can progress along with findings of more diffuse cerebrovascular disease. Sinemet or direct dopaminergic agonists can be somewhat effective at alleviatingsymptoms in some cases. However, reducing the risk factors for stroke, especially hypertension, and initiating antiplatelet therapy are the most effective interventions to slow progression. Cognitive changes resulting from diffuse Binswanger’s encephalopathy can exacerbate cognitive changes from dopaminergic medication and complicate treatment.
STRUCTURAL PARKINSONISM Although usually easy to differentiate from idiopathic Parkinson’s disease, a variety of structural lesions can cause a subset of parkinsonian features, including gait abnormalities and bradykinesia. Usually, other historical or clinical features are present to aid in differential diagnosis. Basal ganglionic or midbrain mass lesions, normal-pressure or obstructive hydrocephalus, and chronic subdural hematoma can all lead to such variable presentations. Gait abnormalities usually are the presenting symptom, and atypical tremor and rigidity are common. Parkinsonian rest tremor is rarely present, pyramidal signs are the rule, and symptoms suggestive of individual diagnoses often are present and helpful. For example, headache or seizure with a mass or subdural hematoma, cognitive dysfunction and incontinence with normal-pressurehydrocephalus, and subacute progression all raise suspicion for one of these disorders. Neuroimaging often can rule out or confirm one of these clinically suspected disorders. The disorder is thought to involve either direct striatal compression and compromise, periventricular white matter compromise, or direct midbrain injury with nigral dysfunction, depending on the location of the mass lesion or the type and extent of the hydrocephalus. This is one of the few situations in which imaging is indicated in parkinsonian syndromes; in combination with vascular parkinsonism, these disorders present with atypical signs for parkinsonism and often lateralized pyramidal tract findings, pointing the way for neuroimaging. Response to dopaminergic therapy is variable, with some thought that good response indicates midbrain compromise from the mass or hydrocephalus, and poor response reflects primary striatal compromise. In cases of normal pressure hydrocephalus, mass, or subdural hematoma, appropriate further neurodiagnos-
tics and possible surgical intervention are warranted. In many cases, dopaminergic therapy can be used symptomatically before or after primary therapy.
TOXIC PARKINSONISM Although l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine(MPTP) emerged in the 1980s and 1990s as the most important recent and most scientifically illuminating toxic cause of secondary parkinsonism, a variety of industrial and agricultural toxins, often occupation related, can cause parkinsonism. Many of these toxins are mitochondrial poisons that interfere with electron transport. Others cause diffuse neurotoxicity with a marked effect on the basal ganglia. Careful elicitation of occupational and chemical exposure history is crucial to diagnosis because laboratory confirmation is possible only in a few situations. Although modern industrial standards and safeguards have drastically reduced the toxin levels in modern U.S. work settings, older workers, immigrants from developing countries, and patients with subtle syndromes may still need diagnosis of these toxin exposures. The best-known industrial toxin that can cause parkinsonism is manganese, which can be found in mine ore or, potentially, in vapors from unventilated welding. Such industrially related parkinsonism was much more common in the nineteenth and early twentieth century (“manganese madness”) and now is quite uncommon in this country. Manganese absorption occurs via the respiratory and gastrointestinal tracts and reaches high brain levels. Initial dementia and behavioral changes are the cardinal features, including agitation, psychosis, and aggression, following a time course from months to many years, depending on the exposure level. These changes classically make the transition over time to a more subdued affect and parkinsonian features. Patients can present with dystonia in addition to quite typical but symmetrical parkinsonian findings, with the exception of rare rest tremor. Diagnosis is by careful elicitation of the patient history; confirmation by serum or cerebrospinal fluid levels is available but rarely needed. Eliminating the manganese exposure can reduce or stabilize symptoms and signs over a period of months. A more modern toxin that produces a pathologic and clinical syndrome nearly identical to idiopathic Parkinson’s disease is the synthetic narcotic contaminant MPTP, which caused a localized epidemic of toxic parkinsonism among intravenous drug abusers using the synthetic heroin analog l-methyl-4-phenyl-4propionoxypiperidine (MPPP) near San Jose, California, in the early 1980s. Monoamine oxidase-B (MAO-B) converts MPTP to 1-methyl-4-phenyl-pyridiniumion (MPP), a mitochondrial electron transport poison responsible for the specific degeneration of dopaminergic substantia nigra neurons in this disorder. This neurotoxicology was one of the early indications for using selegiline as an MAO-B inhibitor in Parkinson’s disease. Although a few industrial exposure cases have been suggested, they are not seen in most practices. The clinical presentation, apart from the typically much younger age at onset of these patients, can mimic Parkinson’s disease remarkably, although rest tremor can be absent or less striking than other clinical signs. Diagnosis is by patient history, although circumstantial support via toxic screen may be helpful. In experimental settings, positron emission tomography has demonstrated striatal dopamine reduction strikingly similar to that in Parkinson’s disease. Response to standard dopaminergic therapy has been beneficial, although the severity of many cases and the frequency of “freezing” as a limiting symptom have made treatment less satisfactory in many patients. In limited experimen-
Chapter 123
tal trials of fetal nigral neuron transplantation, good therapeutic response has been obtained, thought to be especially long-lasting in MPTP cases because this is a static insult without ongoing degenerative disease. A number of organic solvents, most notably carbon disulfide (used in rayon and cellophane production) and, less often, methanol, have been associated with secondary parkinsonism. Exposure to carbon disulfide and other industrial solvents is largely via the respiratory tract, although cutaneous absorption is also possible. Methanol exposure usually is via illicit ingestion. The clinical presentation, progression, and complex of symptoms and signs are very similar to those for manganese intoxication noted earlier. Although they were largely a problem of the nineteenth and early twentieth centuries in the United States, lax industrial safeguards in less developed countries make these organic toxins relevant in some patient populations. Neuropathologically,necrosis in both the substantia nigra and globus pallidus could account for the parkinsonian findings appearing in combination with diffuse encephalopathy and peripheral neuropathy with carbon disuliide, and methanol results in putamen degeneration. Carbon monoxide intoxication can also result in parkinsonian features, along with the diffuse encephalopathic, ataxic, and often dystonic findings that result from injury to the globus pallidus, hippocampus, cerebellar Purkinje cells, and deep cortical regions. Rarely would such a presentation be confused with idiopathic Parkinson’s disease. Similarly, a variety of organic toxins including cytosine arabinoside (AraC), pyridines, amines, nitrides, sulfatides, and excitatory amino acid analogues have been reported to cause parkinsonian features in rare cases. Some agricultural pesticides and herbicides, including paraquat, diquat, and other mitochondrial poisons, have been associated with toxic parkinsonism. Response of most of these toxic syndromes to standard dopaminergic therapy is variable but typically unsatisfactory. Recently, experimental evidence has been found of direct association of a parkinsonian syndrome in rodents with one mitochondrial toxin, rotenone. Such animal models allow both insights into the pathophysiology of nigral neuron degeneration and directed trials of preventive antioxidant therapies. Although it is unclear whether such toxin-induced parkinsonism has broad implications for understanding the causes and subtleties of the more common idiopathic Parkinson’s disease, reproducible animal models of functional loss resulting from nigral neuron death are very useful in pharmacologic prophylaxis and both pharmacologic and surgical therapeutics. In addition, these findings of nigral neuron degeneration in rodents further support the importance of similar environmental, occupational, and industrial exposure in these small but important categories of human parkinsonian disease.
POST-TRAUMATIC PARKINSONISM Both significant, isolated head trauma and more chronically acquired pugilistic parkinsonism from career-long boxing can result in partially parkinsonian syndromes. The disorder in the acute cases is thought to involve a combination of rotation shearing axonal injury and the hemorrhagic petechial microvascular disease associated with such rotation forces. Because the midbrain can be the site of maximal rotation in these cases, even injuries resulting in only subtle changes elsewhere can result in clinical parkinsonism. Alternatively, the parkinsonian symptoms and signs can be a small part of a complex of multifocal central nervous system injury that becomes clearly delineated only after
Secondary Parkinsonism
78 1
partial recovery from the acute post-traumatic hospital course. In boxers with a history of repetitive head blows associated with less dramatic rotation injuries, the same mechanism is thought to underlie the clinical syndrome. Although mild concussive injuries are common in all boxers, professionals without head protection and with more numerous episodes of loss of consciousness are thought to accumulate the most clinically marked parkinsonism. In the former isolated injury cases, a history of serious head trauma with concussion or coma is the rule, and parkinsonism typically is accompanied by cognitive changes, pyramidal or cerebellar signs, and often localizing midbrain signs on examination. Unlike in many other secondary parkinsonian syndromes, rest tremor is common. Pugilistic parkinsonism is centrally related to occupation as a boxer or history of repeated low-level head injury. Dementia and parkinsonism, including rest tremor, are the central features, although ataxia and superimposed pyramidal signs from the same disorder or from unrelated prior subdural hematoma are not uncommon. Neuroimaging typically shows diffuse cerebral atrophy and can reveal diffuse, bilateral basal ganglia calcifications from microhemorrhage, subtle midbrain white matter changes on magnetic resonance imaging, or no additional definitive findings. Imaging is also indicated to rule out chronic subdural hematoma as an atypical cause of secondary parkinsonism. Other neurodiagnostic studies, including electroencephalographyand neuropsychological testing, are indicated depending on the clinical setting, but other studies are rarely helpful. Response to standard dopaminergic therapy can be beneficial, although patients usually do not improve much because of the broader underlying disorder. Because of the spectrum of neurologic symptoms in addition to parkinsonism, treatment is symptomatic and individualized. Often, not much can be done therapeutically beyond providing appropriate social support and community services.
ENCEPHALITIC PARKINSONISM Although encephalic parkinsonism was quite prevalent after the epidemic of Economo’s encephalitis (or encephalitis lethargica) from approximately 1915 to approximately 1935, few survivors remain, and no more recent equivalent encephalitic epidemic has been associated with such parkinsonian features. Other viral encephalitides and syphilitic encephalitis have been associated with secondary parkinsonism in a much more limited number of cases. The parkinsonian symptoms and signs could develop over a wide period after the acute illness, from almost immediately to more than 10 years later. The parkinsonian findings usually lacked typical rest tremor. Dystonia, tics, and diffuse cognitive changes were common as well, along with other neurologic findings that varied between patient populations studied. Pathologically, dopaminergic nigral neurons were strikingly reduced in number, without Lewy body formation, along with more diffuse neuronal injury and gliosis responsible for other elements of the syndrome. Although patients initially responded well to levodopa therapy when it was introduced in the 1960s, they were found to be extremely sensitive to toxic side effects with small dosages and especially prone to dyskinetic and cognitive complications. ~~
METABOLIC DISEASES WITH PARKINSONIAN FEATURES A few well-recognized metabolic disorders can include parkinso-
nian features among their broader and more defining clinical
782
Movement Disorders
Non-Parkinsonian Movement Disorder
symptoms and signs. Although it is beyond the scope of this chapter to describe each of these disease states in detail, it is useful to keep these disorders in mind in the broadest differentiation of atypical parkinsonism in correctly aged and appropriate patients. Because the parkinsonism associated with these disorders is not isolated even at the onset, confusion with idiopathic Parkinson’s disease is unlikely in most cases. Specific elements of the family or personal histories can direct appropriate use of diagnostic testing in individual circumstances. Wilson’s disease, a copper metabolism disorder with autosomal recessive inheritance and reduced ceruloplasmin levels resulting in hepatic and central nervous system copper deposition, can present with prominent basal ganglionic or cerebellar symptoms and signs. Parkinsonism is rarely found in isolation; dystonia, dysarthria, and nonrest tremor are common initial symptoms. Onset typically occurs in the teens and twenties, but patients in early school age through their fifties have been described. Because onset can occur much earlier than that of most idiopathic Parkinson’s disease, this diagnosis should be considered in especially young patients with parkinsonian findings. Diagnosis is by family history, slit lamp examination for Kayser-Fleischer rings, and assay of abnormal copper metabolism with decreased serum ceruloplasmin in 95% of cases, and increased urinary copper excretion. Hepatic biopsy for increased copper deposition is definitive in combination with other findings. Treatment is centrally via limitation of copper intake and absorption and via chelation therapy. Dopaminergic symptomatic therapy could confound observation of the clinical response to therapy and is rarely useful. Other rare disorders can present with parkinsonian features among more diffuse neurologic findings. Acquired hepatocerebral degeneration can display a clinical picture similar to that of Wilson’s disease, with mixed extrapyramidal findings, infrequent rest tremor, and prominent cognitive changes. Prominent degeneration in the globus pallidus, caudate, and putamen typically is seen. Both hypoparathyroidism and pseudohypoparathyroidism can result in bilateral basal ganglia calcification and symmetrical parkinsonian features, including rest tremor, rigidity, and gait disturbance, along with dystonia and chorea. Parkinsonism is not found in isolation, with paresthesias, tetanic contractures, and seizures being the most common accompanying features. Hallervorden-Spatz disease, an autosomal recessive illness with iron deposition and degeneration of the globus pallidus, substantia nigra, and red nucleus, typically presents in childhood or
adolescence and progresses over 1 or 2 decades. Parkinsonian features are mixed with prominent pyramidal and cognitive changes. Symptomatic dopaminergic therapy has been attempted with variable, limited results. Both pancreatic encephalopathy and central pontine myelinolysis can result in basal ganglionic lesions and have been described with parkinsonian features during the course of the illness. Attention to such rare associations may allow early diagnosis in some of these atypical parkinsonian disorders.
CONCLUSION Although idiopathic Parkinson’s disease often is straightforwardto diagnose in its classic age range of onset, clinical features, progression, and response to dopaminergic therapy, a broader differential diagnosis should be considered when atypical features are present or when parkinsonism occurs in younger patients. A range of secondary parkinsonian syndromes exist, some of which are fully or partially reversible with appropriate diagnosis and management. Because of the protean nature of many parkinsonian syndromes, the history often is more helpful in specific diagnosis than the neurologic examination; specialized neurodiagnostic studies can be used to support or confirm a suspected diagnosis, but a broad laboratory screen is rarely indicated. Although most of the secondary parkinsonian syndromes are rare, they represent an important class of disorders of the nigrostriatal system that have illuminated the basis of Parkinson’s disease and its potential therapies.
SUGGESTED READINGS Adams JH, Duchen LW. Greenfield‘s Neuropathology. 5th Ed. Oxford University Press, New York, 1992 Adams RD, Victor M: Principles of Neurology. 5th Ed. McGraw-Hill, New York, 1993 Betarbet R, Sherer TB, MacKenzie G et d.Chronic systemic pesticide exposure reproduces features of Parkinson’s disease. Nat Neurosci 3(12):1301-1306, 2000
Langston JW, Ballard P, Tetrud JW, Irwin I: Chronic Parkinsonism in humans due to a product of meperidine-analog synthesis. Science 25;219(4587):979-980, 1983
Rowland LD Merritt’s Textbook of Neurology. 8th Ed. Lea & Febiger,
Philadelphia, 1989 Stern MB, Koller W C Parkinsonian Syndromes.Marcel Dekker, New York, 1993
SECTION
2 NON-PARKINSONIAN MOVEMENT DISORDERS
124 Spinocerebellar Ataxias H
Christopher M. Gomez
The spinocerebellar ataxias (SCAs) are a complex group of disorders, characterized by progressive gait Unsteadiness, hand incoordination, and dysarthria caused by degeneration of the cerebellum or its spinal pathways. The disorders that make up this heterogeneous syndrome progress slowly over years to decades and thus are distinguished from viral, postviral, paraneoplastic, and immune disorders that more typically cause acute, subacute, or relapsing-remitting ataxia. Because of the heterogeneity of this syndrome and the difficulties with case ascertainment, the prevalence of this heterogeneous group of disorders is difficult to estimate. Most specialists agree that one half to two thirds of patients visiting ataxia clinics have a demonstrable hereditary form of the disease. Epidemiologic studies in Europe, Japan, and northern Africa have estimated the prevalence of all forms of ataxia to be 4.5 to 15 in 100,000, and of hereditary ataxia in several studies to be 4.8 to 6.4 per 100,000. Since the late 1800s and until the modern genetic revolution, neurologists used purely clinical observations, such as differences in age of onset, rate of progression, hereditary pattern, and associated clinical features to attempt to understand and classify the different SCA subtypes. These classifications culminated with that of A. E. Harding and continue to serve as a framework on which to begin diagnostic workups and expand clinical definitions in the modern genetic era. In the past 10 years there has been an explosion in progress in understanding the genetics of hereditary ataxia. The mutational basis for at least 9 forms of recessively inherited ataxia and at least 13 forms of dominantly inherited SCA has been established. The existence of an additional 6 forms of dominantly inherited SCA has been suggested by genetic linkage studies. Numerous insights from these genetic discoveries have greatly aided in interpreting clinical data and initiating investigation into the pathogenesis of ataxia. Despite remarkable advances in the genetics of ataxia, there are few definitive treatments for patients with progressive ataxia. This is particularly the case for approximately one third of patients with ataxia who have an apparently nonhereditary condition that has been called sporadic SCA. For this heterogeneous group of patients treatment is limited to symptomatic approaches and diagnosis and management of complications.
RECESSMLY INHERITED AND X-LINKED ATAXlAS About one half of patients with a hereditary ataxia have a recessively inherited condition (Table 124-1). The two most common and important of forms of recessively inherited ataxia are ataxia telangiectasia (AT) and Friedreich’s ataxia (FRDA). How-
ever, recent advances in the genetics of hereditary ataxia have enabled the recognition of several rarer forms of recessively inherited and X-linked ataxia, which may have similar ages of onset or clinical presentation to those of AT and FRDA (Table 124-1). Because some, such as hereditary ataxia with vitamin E deficiency, may have definitive treatments, their distinction is important. Ataxia Telangiectasia
AT is the most common form of infantile-onset cerebellar ataxia, with a prevalence estimated at 1 to 2.5 per 100,000. In the classic form of AT, progressive gait unsteadiness begins in the second year of life, soon after the patient begins to walk. Slurring of speech and hand incoordination follow soon afterward. There may be a history of mild mental delay. Peculiar head thrusting movements with voluntary gaze sometimes are seen, arising from a characteristic gaze apraxia. Rarely, milder forms may have age of onset of cerebellar symptoms as late as 9 years of age or may present with the gaze apraxia and resting tremor along with the systemic signs. AT is a systemic condition in which the underlying cellular abnormality is related to defective DNA repair. Patients with AT have immunologic incompetence, higher risk of malignancy, and progeric features. Patients often have a history of recurrent sinopulmonary and cutaneous infections, such as impetigo, before the onset of neurologic abnormalities. Chronic sinusitis and bronchiectasis often are present. Patients with AT also have a higher frequency of lymphoreticular malignancy and germ cell tumors in childhood and adenocarcinoma and other solid tumors as adults. First-degree relatives, obligate carriers of the recessively inherited mutation, also have a higher incidence of adenocarcinoma. There is often a delay in development of secondary sex characteristics and a delayed or irregular menstrual cycle, indicating the presence of hypogonadism. Small ocular and cutaneous telangiectasias, initially most evident on the conjunctiva and pinnae, may not be present during the first few years after onset of ataxia but spread to skin creases, oral mucosa, knees, and elbows. Premature graying of hair, senile keratoses, and atrophic skin, present in older children, indicate an accelerated aging process. Patients often are of short stature because of growth retardation. The mental status examination may suggest slowed cognitive function. Cranial nerve examination reveals a marked impairment of voluntary gaze. Patients have extremely slow or absent saccadic eye movements. When asked to look to one side they thrust their head toward the target, and the eyes follow with a slow eye movement, more resembling a pursuit 783
Abetalipoproteinemia
(IOSCA)
Infantile-onset spinocerebellar ataxia
Late-onset Friedreich’s ataxia (LOFA)
Friedreich’s ataxia with retained reflexes (FARR)
Friedreich’s ataxia
progression, no dysarthria, hyperreflexia, mild or no cerebellar ataxia B. Episodes of vertigo A. Ophthalmoplegia, deafness, sensory axonal neuropathy, athetosis, epilepsy areflexia, athetosis, optic atrophy A. Late milestones, nyctalopia, blindness, retinitis pigmentosa, nystagmus, proprioceptive loss, areflexia B. Babinski, generalized weakness
A. Late onset, slow
sition sense, saccadic intrusions, Babinski B. Optic atrophy, deafness A. Hyperreflexia, Babinski, reduced vibratory sense B. Spasticity, atrophy
A. Areflexia, absent po-
1-20
1-2
25-68
13-45
2-25
1-9
A Ocular apraxia, cho-
Ataxia telangiectasia
reoathetosis, nystagmus B. Areflexia, peripheral neuropathy, mental retardation
Age
Neurologic Findings.
Disorder
TABLE124-1. Recessive Ataxia
Microsomal triglyceride transfer protein (MTP) gene/ 4q22-24; ApoB gene/2p24
1Oq23-q24
Frataxin-l/X25/FRDAl
Frataxin-1/X25/FRDA1
Frataxin-1/X25/FRDA1
ATM phosphoinositol 3-kinase
Protein/Cene/Locus
Truncating mutations, deletions, missense mutations, Q1450X. R2495X
CAA < 500
CAA 408 ? 252, C130V
missense and truncations, M 1 I, I154F. W173C, L106X,A> C lnt3
CAA 719 f 184, most
>70 distinct missense, deletion, nonsense, frame shift, splicingtruncation mutations
Mutations and Alleles
Mutations in ATM; increased X-ray sensitivity, a-fetoprotein levels; chromosoma1 breakage (translocations); reduced imrnunoglobulin levels Genetic screen for GAA repeats in FRDA gene > 120; sequence analysis for point mutations No malignancy, telangiectasias, normal immunity
Steatorrhea, scoliosis, occasional liver cirrhosis
Reduced apolipoprotein B, acanthocytes, reduced vitamins A, E, absent MTP in intestinal biopsy
Genetic linkage to IOSCA locus Hypergonadotropic hypogonadism in females
No cardiomyopathy
Genetic screen for CAA repeats in FRDA gene > 120; sequence analysis for point mutations Genetic screen for CAA repeats in FRDA gene > 120; sequence analysis for point mutations
FARR LOFA
Diagnosis Variants
Scoliosis, pes cavus, milder cardiomyopathy
Immunodeficiency, recurrent infections, neoplasia (leukemia, lymphoma, germ cell tumors, breast), telangiectasias, short stature Cardiomyopathy, scoliosis, pes cavus, diabetes
Non-CNS
2
s
%
2
sB
21
?
5.
5
P
?
0
A. Seizures, delayed milestones, mental retardation, muscle weakness, pyramidal signs B. Lactic acidosis
CoQlO deficiency
HEXA gene 15q23-q24 HEXB 5q13
3-1 7
Scoliosis, camptodactyly, achalasia, gastrointestinal dysmotility Skeletal muscle, recurrent myoglobinuria, ragged red fibers
?
Birth-1 6 yr
None
None
Cardiomyopathy, dermal xanthomas, tendon xanthomas
1q31-32/AXPCl
Truncation mutations
Start codon, deletions, insertion, missense, truncationframeshift mutations 86 HEXA and 23 HEX6 and mutations, e.g., HEXB R505Q C269S 1207V A505Q (a G-to-A transition) within intron 12
2-1 4
3-20
a-Tocopherol transfer protein (ITPA)/ 8ql3.1-13.3
3-62
'Neurologic findings in addition to cerebellar dysarthria, hand and gait incoordination. A, usual; 6, common.
Posterior column and retinitis pigmentosa
Autosomal recessive spastic ataxia of CharlevoixSaguenay
A. Motor neuron disease, pyramidal tract 6. Dementia, myoclonus, optic atrophy, supranuclear gaze paresis, psychosis, dystonia A. Nystagmus, spasticity, axonal peripheral neuropathy, Babinski, ankle areflexia, deep sensory 6. Lower limb amyotroqhy. A. Retinitis pigmentosa, proprioceptive loss, intact pain, areflexia, dysarthria
flexia, Babinski 6. Dystonia, retinopathy
A. Leg weakness, are-
Hexosaminidase A and B deficiency
Ataxia with isolated vitamin E deficiency (AVED) Tay-Sachs; Sandhoff's
Ataxia with pigmentary retinopathy, with normal vitamins A, E, Frataxin-1, phytanic acid Reduced CoQlO in skeletal muscle
Reduced vitamin E with normal vitamins A, D, K; normal fat absorption and lipid profile Reduced hexosaminidase activity using natural, sulfated substrate, membrane-bound lamellar cytoplasmic inclusions in rectal ganglia Juvenile onset, spastic ataxia with nystagmus, normal cardias, neg. fratest
786
Movement Disorders
Non-Parkinsonian Movement Disorders
than a saccade. Some patients have nystagmus. There is severe trunk and gait unsteadiness. Upper limbs are uncoordinated, with inaccurate grasp of objects and intention tremor, Speech is slowed and dysarthric. Facies appear impassive. There may be choreoathetoid movements of the limbs and titubation of the head. Deep tendon reflexes are depressed or absent. Plantar responses, initially flexor, may become extensor with time. Sensation is initially normal, but vibratory sense may be lost with disease progression. Romberg sign is notably absent. With progressive ataxia, patients usually are wheelchair-bound in childhood. The neuropathy is progressive, and reduced muscle power and neurogenic atrophy develop in the late stages of the disease. Survival beyond the third decade is rare. Death may result from continued neurologic deterioration, aspiration and pneumonia, malignancy, or, rarely, infections. Infections are common in AT because of severe immunologic incompetence. There are deficiencies in cell-mediated and humoral immunity in these patients. Lymphoid organs are poorly developed, and there is serum deficiency in immunoglobulins, particularly immunoglobulin A. Serum a-fetoprotein, normally a tumor marker, often is elevated. Magnetic resonance imaging (MRI) demonstrates marked atrophy of the cerebellum, particularly the vermis, with an enlarged fourth ventricle and cisterna magna. The brainstem is spared. There are occasional white matter T2 signal intensities. Cerebrospinal fluid examination may show a slight increase in protein. The electroencephalogram shows nonspecific abnormalities. Nerve conduction studies show small or absent sensory nerve action potentials and slight slowing of motor nerve conduction velocity. Electromyography reveals evidence of denervation late in the disease. Pathologic studies have demonstrated more uniform findings than in the clinical presentation. There is striking loss of Purkinje cells and variable loss of granule cells in the cerebellar cortex. Inferior olivary neurons and dentate neurons are also depleted. In distinction from FRDA, the spinal cord is largely intact, but there is some loss of myelin in the dorsal columns and loss of neurons in the sensory and autonomic ganglia and motor neurons. Sural nerve biopsies may show loss of large myelinated fibers and lipid deposits. There is no specific treatment for AT. Prevention and treatment of infections and early diagnosis and treatment of malignancies have the most significant impact on long-term survival. Because of the marked radiosensitivity of nonmalignant tissues in AT, tumors should not be treated with radiotherapy. From the neurologic standpoint patients are managed with supportive and preventive measures. Dysphagia and aspiration should be minimized. Physical therapy and rest combine to allow patients to cope with increasing disability. Although AT is an autosomal recessive condition, and carriers have no neurologic phenotype, they do have a higher incidence of malignancies. The gene responsible for AT was identified in 1993 by classic positional cloning methods. The AT gene spans 150 kb, consists of 66 exons, and encodes a 350-kDa protein, ATM (ataxia telangiectasia mutated). The ATM protein is localized mainly in the nucleus and has homology to a phosphatidylinositol3-kinase. AT variants of several types have been recognized. Some of them have a later onset and milder and slower progression of neurologic abnormalities. Some patients have a significantly longer lifespan. Some have no obvious neurologic abnormalities and only the immunologic, cutaneous, and malignancy abnormalities.
The basic cellular defect that underlies the neurologic, neoplastic, and immunologic abnormalities of AT appears to be related to defective DNA repair. Chromosomal translocations, especially with chromosomes 7 and 14, can be identified in peripheral blood lymphocytes and increase with age and during culture in vitro. Cells in culture have increased sensitivity to ultraviolet, gamma, and X irradiation. At least 70 different AT gene mutations have been found in patients with AT. The majority of these are frame-shift or nonsense mutations and are predicted to cause a truncated protein. Missense, splicing, and in-frame deletion mutations are less common. Except in cases of consanguinity, most patients are actually compound heterozygotes rather than true homozygotes. Patients from certain ethnic groups (e.g. Amish, Mennonite, Costa Rican, Polish, British, Italian, Turkish, Iranian, Israeli) have a high prevalence of specific ATM mutations, which may sometimes aid in choice of which mutations to look for to make a molecular diagnosis. Mutations predicting early protein truncation lead to more severe AT phenotype. The pathogenic mechanism by which the deficiency of ATM leads to the many facets of the disease is yet to be elucidated on clinical grounds. Infantile onset ataxia with typical cutaneous signs, ocular motor apraxia, and retained dorsal column sensation can establish the diagnosis. Reduced serum immunoglobulins and raised a-fetoprotein or increased numbers of chromosomal rearrangements or accumulation during culture strongly suggest the diagnosis. There is no commercially available screen for detecting ATM mutations. The differential diagnosis includes other sporadic, recessively, or dominantly inherited forms of progressive ataxia with onset in this age range. The distinct syndrome of congenital nonprogressive ataxia may be initially suspected until progression is noted. In the absence of signs of AT or chromosomal rearrangements, as may occur early in the disease, the other conditions usually can be excluded on clinical grounds and with laboratory studies (Table 124-1). Friedreich’s Ataxia
FRDA, which represents about one half of all cases of hereditary ataxia, has a prevalence of 2 to 4 per 100,000 and is the most common form of hereditary ataxia. The classic form has an age of onset between 2 and 25 years, and about 25% have an atypical presentation with milder phenotype and onset after 25 years. As with AT, genetic advances have partially explained the phenotypic variability and have allowed recognition of striking clinical variants. Typically, gait unsteadiness begins in childhood, often simultaneous with spinal scoliosis. Gait ataxia progresses steadily, but worsening of both ataxia and scoliosis may seem greater during rapid growth in puberty. Dysarthria and hand incoordination usually develop in the next few years. Gait unsteadiness is particularly poor in darkness because of prominent involvement of posterior columns. Optic nerve atrophy occurs in approximately 25% and sensorineural hearing loss in 10% of patients with FRDA. Loss of sensory nerve action potentials, measured in nerve conduction studies, occurs early in the disease. Progression of the ataxia in the classic form is fairly uniform, and patients are wheelchair bound 12 years after onset. Death may occur from the mid-thirties to the sixth and seventh decades, particularly with the milder variants. Death often is related to cardiomyopathy, diabetes, or aspiration pneumonia.
Chapter 124
Several significant nonneurologic complications occur in FRDA. Spinal scoliosis or kyphoscoliosis is present in more than 90% of patients and may appear before the onset of imbalance. Intervention with bracing or surgical placement of stabilizing rods may be necessary to avoid deformities that reduce mobility and pulmonary function. Ten to twenty percent of patients with FRDA develop diabetes mellitus, an average of 15 years after onset of ataxic symptoms. Cardiac disease is a prominent feature of FRDA, present in nearly all patients with the typical form. The principal change is a progressive hypertrophic cardiomyopathy. Some patients experience exertional dyspnea, although because the neurologic impairment in FRDA reduces activity, the reduced cardiac output rarely leads to exercise intolerance. Palpitations are also common. The electrocardiogram typically shows T wave inversions or evidence of left ventricular hypertrophy. Some patients develop arrhythmias, particularly supraventricular and atrial fibrillation with advanced disease. The principal change in the heart is fibrosis and thickening of the myocardium, which may lead to either concentric hypertrophy or asymmetrical septal hypertrophy with outflow obstruction. In advanced stages there may be a dilated cardiomyopathy. Histologically, there is interstitial fibrosis, with infiltration of inflammatory cells and deposition of fatty deposits and iron deposits. On examination, typically, kyphoscoliosis is present. With wheelchair-bound patients, lower extremities often have pes cavus deformity and cyanotic venous stasis changes. Mental status is intact. Pallor of the optic disks occasionally is present. Eye movements demonstrate a characteristic pattern consisting of frequent spontaneous or pursuit-evoked large-amplitude saccadic intrusions (square wave jerks). Visual pursuit is saccadic, and there may be dysmetric saccades but rarely nystagmus. Depending on the stage, spinocerebellar dysfunction and incoordination of voluntary movements, including dysarthria, hand incoordination, and gait unsteadiness may be mild to severe. Motor examination often shows reduced tone in the upper extremities. There may be mild muscle atrophy, particularly of the lower extremities. Lower extremities may be quite spastic, particularly in the retained reflexes variant (described later in this chapter). Choreoathetoid movements may be present. Deep tendon reflexes may be detectable early in the disease, at some joints, but soon disappear. Plantar responses usually are extensor. Position sensation is absent in the lower extremities, but pain and temperature sensation are intact. Pathologically, FRDA is characterized by severe atrophy of the spinal cord, greatest in severity in the cervical cord. There is demyelination of the dorsal columns and pyramidal tracts and cell loss in Clark‘s columns, dorsal root ganglia, and anterior horns. In the dorsal roots and peripheral nerves there is loss of the large myelinated fibers that process from the periphery in a dying-back process. There is also patchy cell loss and gliosis in the cerebellum and medulla. The elucidation of the genetic basis for FRDA has allowed recognition of several clinical variants of FRDA that would be excluded from the diagnosis of FRDA on clinical grounds. Patients with the syndrome of juvenile-onset SCA with retained deep tendon reflexes, once recognized only as a distinct clinical entity, have been recognized within FRDA families. Patients with this syndrome, which has been called Friedreich’s ataxia with retained reflexes, have a lower incidence of decreased position sense loss, pes cavus, and less severe cardiomyopathy than areflexic “typical” patients with FRDA. Other patients have spastic paraparesis or
H
SpinocerebeiiarAtaxias
787
generalized chorea, some may have severe optic neuropathy, and some may have no evidence of dysarthria. Some patients (15%) experience onset of ataxic symptoms significantly beyond 25 years and as late as 60 years. This condition has been called late-onset Friedreich‘s ataxia. They have a lower occurrence of skeletal deformities and cardiomyopathy as well as a longer mean interval to wheelchair confinement. The recognition of these patients is important for management and for potential treatment with rational therapies. There is no definitive treatment for FRDA, and management chiefly involves supportive care and avoidance of complications. As in all patients with ataxia, physical therapy and rest allow patients to cope with increasing disability. Dysphagia and aspiration should be minimized. Spasticity may be managed with baclofen. Progressive scoliosis unresponsive to bracing should be treated with surgical stabilization of the spine by placement of Harrington rods. Cardiac disease and diabetes should be managed symptomatically. Recent studies have suggested that administration of the cofactor coenzyme Q l O (CoQlO) may significantly improve cardiomyopathy, possibly through its action as a free radical scavenger. The gene and mutational basis for FRDA were elucidated in 1996. The gene affected, X25, consists of seven alternatively spliced exons, the principal product of which encodes a 210-amino acid protein, frataxin. Frataxin, which is highly conserved in evolution, localizes to the inner mitochondrial membrane. The principal mutation of X25 consists of an expansion of an unstable repeat of the trinucleotide GAA, normally present in the first intron, resulting in reduced levels of frataxin mRNA. The GAA trinucleotide repeat present in the normal X25 gene exhibits length polymorphism, with normal alleles ranging from 7 to 38 repeats. An interruption of a (GAGGAA)n sequence is present in most normal alleles over 27 repeats. Disease is associated with 66 to more than 1700 repeats, and 98% of all FRDA alleles contain more than 600 repeats. Certain alleles, both premutation alleles and disease-associated alleles, are unstable during meiosis, prone to either contraction or expansion. Premutation alleles are those that have lost the (GAGGA4)n interruption and are prone to expansion to become either larger premutation alleles or disease-associated alleles. Missense or nonsense mutations in the X25 coding region represent rarer alleles. These are normally found through nucleotide sequence analysis of the X25 gene in patients with ataxia bearing a single pathologic GAA repeat, who are thus compound heterozygotes (4%). There is a statistically significant correlation between the size of the shorter of the two GAA repeats and clinical features in FRDA, including age of onset, presence of leg muscle weakness or wasting, duration until wheelchair use, and prevalence of cardiomyopathy, pes cavus, and scoliosis. For example, the GAA repeat size accounts for 50% to 75% of the variance in age of onset. Nevertheless, phenotypic variability between siblings with identical repeat number or even between monozygotic twins with FRDA demonstrates that factors such as somatic heterogeneity of the GAA expansion or environmental factors modify disease phenotype. The diagnosis of FRDA is based on clinical grounds and on genetic testing for the GAA repeat expansion in the X25 gene. The differential diagnosis includes all childhood-onset SCAs but particularly those with overlapping signs such as autosomal recessive spastic ataxia of Charlevoix-Saguenay, posterior column ataxia with retinitis pigmentosa, abetalipoproteinemia, ataxia with vitamin E deficiency, and infantile-onset SCA. These conditions present with combinations of ataxia, proprioceptive loss, spastic-
788
Movement Disorders
Non-Parkinsonian Movement Disorders
ity, and diminished reflexes between ages 1 and 20 as with FRDA, and, except for infantile-onset SCA, can be confirmed by a blood or genetic test. An ataxic variant of Charcot-Marie-Tooth neuropathy type 1 has a similar presentation. Recent dramatic advances in the genetics of FRDA have provided important insights into the pathogenesis of FRDA. Frataxin appears to play a role in iron transport in mitochondria. Single-cell yeast genetically deficient of their frataxin homologue develop damaged mitochondria that accumulate excess iron. In a similar fashion, iron deposits can be detected in cardiac muscle from patients with FRDA. Accumulated cellular iron leads to overproduction of oxygen free radicals, which are believed to be responsible for significant subcellular toxicity caused by oxidative damage. Patients with FRDA have elevated serum and urinary levels of oxidatively damaged DNA and lipids. There is recent promising evidence that a synthetic analogue of CoQlO can reduce the levels of these oxidized metabolites and improve cardiac function. Ataxia with Isolated Vitamin E Deficiency Ataxia with vitamin E deficiency (AVED), or familial isolated vitamin E deficiency, is a rare form of autosomal recessive progressive ataxia with features similar to those of FRDA. Although it arises most commonly before 20 years of age, the age at onset ranges from 3 to 62 years. Patients develop progressive gait unsteadiness and dysarthria that progresses to wheelchair confinement at a more variable (3 to 37 years) pace than that of FRDA. Examination usually reveals dysarthria, hand incoordination, gait unsteadiness, areflexia, and vibratory and proprioceptive sense loss. More than one half of patients have extensor plantar responses. Diffuse muscle weakness most prominent distally may be present in 42% of patients. Retinopathy (9%) and dystonia or bradykinesia (13%) are found in minority of patients. Cardiomyopathy is also found in about 19% of patients. Skin may show xanthelasmata or tendon xanthomas. Electrophysiologic studies reveal mildly delayed nerve conduction, decreased amplitudes of sensory action potentials, and sensory delay in the posterior columns. Pathologically peripheral nerve examination demonstrates a dying-back process. There is severe dying-back degeneration of the posterior columns, massive accumulation of lipofuscin in neurons including dorsal root ganglion cells, and mild loss of Purkinje cells. The diagnosis of AVED is made by determination of serum vitamin E (a-tocopherol) levels, which are severely reduced or absent. In distinction from Bassen-Kornzweig disease and other causes of fat malabsorption, other fat-soluble vitamins are not reduced, and patients have no steatorrhea and have normal levels of abetalipoprotein. The condition is caused by defective a-MTP, which was established by conventional linkage analysis, followed by demonstration of mutations in the MTP gene. The a-MTP is a cytosolic liver protein that is presumed to function in the intracellular transport of a-tocopherol. At least 13 different mutations have been found in this gene, approximately half of which are missense and the remainder protein truncating. Twenty to fifty percent of patients are compound heterozygotes, which may help explain the clinical variability. Reduced levels of a-tocopherol may lead to impaired scavenging of oxygen free radicals, leading to oxidative damage of cellular proteins, lipids, and nucleic acids. Treatment consists of supplementation with oral vitamin E at a dosage of 800 mg twice daily, along with supportive care.
Maternally Transmitted Ataxias Mitochondrial disorders resulting from a variety of mutations of the mitochondrial genome give rise to a complex array of neurologic disorders (Table 124-2). This complexity results from the varied types of genes affected in the mitochondrial genome and the occurrence of both mutant and wild type mitochondria in the same cell, a state called heteroplasmy. Progressive ataxia may be a prominent feature in patients bearing either of two well-recognized mutations of the mitochondrial genome. The mutation T8993G causes a missense mutation, L156R, in the MTATP6 gene, resulting in an amino acid change from a highly conserved leucine to arginine in mitochondrial H(+)-ATPase. This point mutation can lead to two different neurologic pictures. In the case of extreme heteroplasmy, infants with cognitive impairment infantile spasms suffer from necrotizing encephalomyopathy, which has been called maternally inherited Leigh‘s disease (MILS). When a greater proportion of the normal mitochondria are present, patients develop a condition called neurogenic muscle weakness, ataxia, and retinitis pigmentosa with subacute, optic atrophy (NARP). Each family member may have a neurologic picture between the two extremes of MILS and NARP, depending on the proportion of mutant mitochondria, having a variable combination of developmental delay, retinitis pigmentosa, dementia, seizures, ataxia, proximal neurogenic muscle weakness, and sensory neuropathy, in a pedigree pattern consistent with maternal transmission. Similarly, the mutation T8993C leads to a L156P mutation and a similar neurologic spectrum. Similarly, patients with the mitochondrial DNA mutations A8344G or A8344C, affecting the tRNA lysine, may have infantileonset spastic quadriparesis, myoclonic epilepsy with ragged red fibers and stroke, chronic progressive external ophthalmoplegia, or ataxia with deafness, myopathy, and neuropathy along with axial lipomas (Ekbom’s syndrome). The diagnosis of mitochondrial disorders is difficult to establish. Because of heteroplasmy, the number of mutant mitochondrial genomes may be low, making the mutation difficult to detect. DNA analysis of mitochondrial DNA from muscle may be of higher yield. There is no definitive treatment for mitochondrial disorders. Treatment options may differ depending on the effect of the mutation. Treatment considerations include CoQ10, vitamins A, E, B,, and B,, C, thiamine, and riboflavin.
AUTOSOMAL DOMINANT SCA The autosomal dominant SCAs are a genetically heterogeneous group of neurodegenerative disorders characterized by progressive motor incoordination, often in association with other progressive neurologic deficits. Patients with these conditions typically have an affected parent or can trace the condition in family members in earlier generations. Most affected patients have a similar onset of slowly progressive gait ataxia, dysarthria, and hand incoordination, rarely preceded for several years by symptoms of diplopia or vertigo. Patients may first notice trouble walking down stairs, on uneven terrain, or in the dark, running, or performing other activities requiring greater balance. These subtle changes may be accompanied by occasional slurring of speech. Eventually imbalance and dysarthria are more obvious, and problems with upper limb incoordination and dysphagia develop. Symptoms may be more easily recognized when there are other affected family members.
A. Motor delay, ataxia, and dysarthria in males B. Spasticity
A. Neurogenic muscle weakness, ataxia, and retinitis pigmentosa, optic atrophy B. Migraines
Photomyoclonic epilepsy, deafness
X-linked ataxia with sideroblastic anemia
Neurogenic muscle weakness, ataxia, and retinitis pigmentosa with subacute, optic atrophy (NARP)
Myoclonus epilepsy and ragged red fibers (MERRF)/ Ekbom’s
Infancy-42
2-52
Infancy
Age
tRNA-Lys gene, tRNALeu gene, mitochondrial DNA
Mitochondrial ATPase 6 gene
Mitochondrial iron transporter gene (ABC7)
Protein/Cene/Locus
*Neurologic findings in addition to cerebellar dysacthria, hand and gait incoordination. A, usual; B, frequent
Neurologic Findings.
Disorder
rn TAW 124-2. X-Linked and Maternally Transmitted Ataxia
A83446 mitochondrial tRNA-Lys, A32436 mitochondrial tRNALeu
T 89936, in mitochondrial ATPase 6 gene L156R; T8993C, L156P
1400M missense
Mutations and Alleles
Short stature, cardiomyopathy, ragged red fibers, axial lipornas, diabetes mellitus, hypertension, skeletal deformities
Mild asymptomatic anemia or microcytic anemia
Non-CNS
Maternally inherited Leigh’s, extreme heteroplasmy, necrotizingencephalomyopathy, cognitive impairment, infantile spasms Progressive external ophthalmoplegia, migraine; dementia, lactic acidosis, spastic quadriparesis; arrested mental and motor development
Variants
Increased CSF lactate, sequence analysis of mitochondrial DNA
CBC (Pappenheimer bodies), FEP, bone marrow biopsy (ring sideroblasts) Increased CSF lactate, hypocitrullinemia, sequence analysis of mitochondrial DNA
Diagnosis
e bJ
d
3
i
790
Movement Disorders rn Non-Parkinsonian Movement Disorders
In the past 8 years, the existence of at least 13 genetically and clinically distinct types of autosomal dominant SCA has been confirmed. These rapid developments resulted primarily from improved technology for genetic research, the advances of the human genome project, and the fact that several SCAs are caused by a similar, novel mutational mechanism, the unstable polynucleotide repeat. The characterization of this mutational mechanism has provided important insights into disease pathogenesis and has helped explain certain aspects of clinical presentation. Table 124-3 summarizes the clinical and genetic aspects of the autosomal dominant SCAs. In an effort to improve the classification of these diseases, a nomenclature has been established by the Human Genome Organization. Each form of autosomal dominant spinocerebellar degeneration that is assigned to a unique chromosomal locus by genetic linkage studies is designated by the symbol SCA, followed by a number. SCA1, the first disorder of this type, was isolated in 1994, and the locus for SCA16 was identified in 2001. In five of these the chromosomal locus is known, but the gene has not yet been isolated. In the remaining eight, the responsible mutation is an expansion of an unstable repeated nucleotide sequence in one of several unrelated genes. These genes happen to contain, within their sequence, trinucleotide or pentanucleotide repeats that are polymorphic over a small size range and repeat number. Five of the responsible genes encode a tract of glutamine residues that is expanded in the diseaseassociated alleles, and in the other three, the expanded repeat occurs in a noncoding region. In some cases, particularly with large repeat sizes, the entire neurologic picture appears to vary even within the same family, for example from a purely ataxic syndrome to one of dystonia and rigidity in SCA3. Progressive cerebellar dysfunction leads to great overlap in the clinical and pathologic features of the SCAs. In the earliest stages of disease and in the mildest forms, when extracerebellar signs are not prominent, the SCAs are all similar. As the disease progresses, certain neurologic features may appear that are unique or prevalent in some SCA types. This is often best demonstrated upon examination of other family members in different stages of the disease. SCAlSCA4 and SCA7 generally are more severe conditions, with more extensive involvement of brainstem and motor pathways, often giving rise to shorter lifespan than other forms of autosomal dominant ataxia that have been called pure cerebellar ataxia. The latter conditions, including SCA5, SCA6, SCA8, SCA10, SCA11, SCA13, SCA16, particularly when some associated features such as seizures in SCAlO are not noted, have strong clinical overlap. The worldwide distribution of the genetically diagnosable SCAs is not uniform. Some SCA types extremely common in one world region have not been detected in others. This variability may result from the prevalence within certain ethnic populations or other genetic isolates of premutations (large normal alleles) that more readily give rise to pathologic alleles. Autosomal Dominant Ataxias Caused by Trinucleotide Repeats and Clutamine Tracts
Five of the eight autosomal dominant ataxias whose genes have been identified are caused by an expansion of the trinucleotide repeat CAG within five distinct genes. These repeats encode expanded tracts of glutamine in five distinct and unrelated proteins. This newly discovered mutational mechanism also underlies three additional neurodegenerative disorders-Huntington disease, dentato-rubro-pallido-luysianatrophy, and X-linked
spinobulbar muscular atrophy-indicating its importance in neurologic disease. The genes responsible for these disorders normally contain a repeated sequence that encodes a tract of glutamine residues. The CAG trinucleotide repeat appears to be particularly prone to changes in the repeat number, leading, even in normal genes, to heritable, in-frame expansions and contractions of the polyglutamine tract. For these proteins, variability in the size of the polyglutamine tract over a small range appears to have no clinically significant consequences. However, there is a threshold, different for each disorder, beyond which expansion of the polyglutamine tract leads to neurologic disease. The expanded polyglutamine tract adversely affects protein folding or protein-protein interactions, rendering the mutant protein toxic to some neuronal types. Purkinje cells appear to be particularly vulnerable in this process. In most cases, the toxicity of the mutant protein appears to be unrelated to the original function of the wild type protein but is instead attributed to a newly acquired property that is harmful to nerve cells. The genetic change has been called a toxic gain of function. The cellular basis for this toxicity has not been clarified but appears in many cases to require transport of the mutant protein to the nucleus. The pathologic CAG repeat alleles are prone to expansion (or contraction) during gametogenesis, particularly in the case of SCA1, SCA2, SCA3, and SCA7. A clear inverse correlation exists between age of onset and the length of the CAG repeat allele in SCA1-SCA3, SCA6, and SCA7, implying that longer polyglutamine tracts, encoded by larger CAG repeats, generate more toxic proteins. When children inherit a larger CAG repeat allele from one of their parents than is borne by the affected parent, they usually develop symptoms at an earlier age than did their parent, a phenomenon known as anticipation. The degree of anticipation differs for each SCA type and appears to depend on the stability of the repeat. Anticipation is uncommon in SCA6 and more often seen in SCA1, SCA3, and SCA7. Anticipation in a family may be so dramatic that a child may be diagnosed with what is believed to be a sporadic neurodegenerative disease years before his or her parent or grandparent who has the gene expansion becomes symptomatic. Spinocerebellar Ataxia Type 1
Among patients with SCA, the proportion with SCAl ranges from 3% in Japan (0% in Korea and Portugal) to 40% in Russia and South Africa and is found in about 6% of US.patients with SCA. SCAl typically emerges in the third or fourth decade, but severe forms of childhood- or juvenile-onset SCAl have been documented that are known to be caused by the more severely expanded alleles. The initial symptom is gait unsteadiness, but increasing dysarthria and dysphagia soon follow. The rate of progression in adult-onset SCAl may vary widely, with confinement to wheelchair between 3 and 17 years after onset and death 10 to 30 years after onset. Death often is related to respiratory failure caused by bulbar involvement. Patients with juvenile-onset disease (whose symptoms appear before age 13) have still more severe disease, having more widespread central nervous system involvement and being fatal before age 16. On examination patients typically have hypermetric saccades, nystagmus, brisk deep tendon reflexes, and Babinski signs along with cerebellar signs early stages of disease. Ophthalmoparesis in the form of slowing saccadic velocity, restricted horizontal versions, or upgaze palsy may develop, and nystagmus disappears
Axial myoclonus Pure ataxia, prominent nystagmus, head tremor Episodes of ataxia, +/- vertigo, nausea, migraine headache, confusion; SCA6-like progressive ataxia Dementia, psychosis, myoclonus, postural abnormalities, seizures
Prominent nystagmus, hyperreflexia Action tremor, paucity of movements, hyperreflexia, Babinski's Moderate MR
16-65
Any age
12-42 20-66
1-45
8-55
15-43
10-49
Prion/prp/ 2Opter-pl2
a l A subunit of P/Q type voltage-gated calcium channel/ CACNAlA/19pl3
SCA13/ 19pl3.3-13.4 SCA14/19ql3.4-ter SCA16/8q22.1-24.1
Protein phosphatase 2A(PPP2R2B/ 5q3 1-5q33
SCAl1/15q14-21.3
E46L/SCA10/22ql3
SCA8/13q21
15-66
1-50
a l A subunit of P/Q type voltage-gated calcium channel/ CACNAlA/19pl3 Ataxin-7/SCA7/ 3p21.1-pl2
129V. 129M
Several sequence polyrnorphisms
Episodic weakness
Subacute dementia; fatal insomnia
P102L, P1 OSL, A117V,Y145X, V1 SOV, E200K, M232R
NA NA
NA
Hypotonia, cerebral atrophy, PDA, CHF
Infantile spasms, microcephaly, hypotonia, pigmentary retinopathy, PDA, anemia Severe rigidity
Variants
Splice site, missense mutations
NA NA
NA
NA NA NA
CAC 66-93
NA
AllCT 800-4500
CTA/CTC 101-345
CAG 41-306
CAG 19-33
NA
NA
CAC 56-86
CAC 34-750
CAG 35-83
Mutations and Alleles
CAC 6-29
NA
AllCT 10-29
CTA/CTC 19-80. >350
CAG 7-16
CAG 4-1 8
NA
SCA5/11 q
10-68
19-7 1
NA
CAC 12-43
16q24-ter
Ataxin-3/SCA3/ 14q21
CAC 15-31
26-72
5-65
Normal Alleles
CAC 6-39
Neurologic findings in addition to cerebellar dysarthria, hand and gait incoordination. CHF, congestive heart failure; GI-2, episodic ataxia type 2; FHM, familial herniplegic migraine; NA, not available; PDA, patent dudus arteriosus.
UD/GSS Prion ataxia
EA-UFHM
SCAI 6
SCA14
SCAI 3
SCAI 2
SCAl1
SCAlO
SCAB
sCA7
SCA6
SCA5
sCA4
S W
Diplopia, facial myokymia, dystonia, rigidity, sensory neuropathy Sensory neuropathy, areflexia or pure Slow progression, pure ataxia, minima1 nystagmus, early dysarthria Slow progression, prominent nystagmus, episodic vertigo Macular retinopathy, early color loss and blindness, spasticity, slow saccades Usually pure ataxia, some bizarre eye movements, some cognitive impairment Seizures
Ataxin-Z/SCAZ/ 12q23-24.1
SCA2
16-3 1
Protein/Cene/Locus
Ataxin-l/SCAl/6~23
15-63
Lingual, limb, amyotrophy, early hyper LOSS of saccades, dementia, patchy areflexia
Anticipation
Age
Neurologic Findings.
Disorder
SCAl
TABU 124-5. Dominant Ataxia
No commercial genetic test; linkage to CACNAlA/ 19~13;detection of CACNAlA mutation EEC, CSF 14-1-3-3 protein, brain biOPSY
NA NA
NA
CAG repeats >65 in SCAI 2 gene
AllCT repeats >800 in SCAI 0 gene
CTA/CCC repeats at the SCA8 locus 101-345
CAC repeats >40 in SCA7 gene
the CACNAlA gene
CAC repeats >19 in
SCA3 gene
CAC repeats >55 in
SCAI gene CAC repeats >33 in SCA2 gene
CAC repeats >38 in
Diagnosis
792
Movement Disorders
Non-Parkinsonian Movement Disorders
as the disease progresses. Numerous neurologic signs may be present with advancing disease. There may be mild cognitive impairment, signs of optic nerve atrophy, fasciculations or frank atrophy in the tongue or perioral muscles, diminished voluntary cough, chorea or dystonia, hypotonia, fasciculations or atrophy of the limb muscle, decreased or absent deep tendon reflexes, and loss of proprioception or vibration sense. Computed tomography (CT) and MRI brain scans in SCAl reveal cerebellar and pontine atrophy. In neuropathologic studies there is neuronal cell loss of Purkinje cells, dentate nucleus, the inferior olive, and mild cell loss in cranial nerve nuclei 111, IV, IX, X, and XII. The axons of degenerating Purkinje cells have eosinophilic spheres or “torpedoes.” There is demyelination of several white matter tracts, including the restiform body and brachium conjunctivum, the dorsal and ventral spinocerebellar tracts, and, to a lesser degree, the posterior columns. The differential diagnosis includes all autosomal dominant SCAs. Patients with cerebellar ataxia with prominent fasciculations and atrophy of the tongue should be suspected of having SCA1. SCAl is caused by an expansion in CAG repeat in the SCAl gene on 6p23 that leads to an elongated tract of glutamine residues within the protein ataxin-1. Ataxin-1 is a nuclear protein of unknown function. The altered folding of ataxin-1 caused by the expanded polyQ tract is detrimental to several types of neurons, especially in the cerebellar Purkinje cells and brainstem motor neurons. In transgenic mice expressing this gene, toxicity entails transport of the protein to the nucleus, where it is sequestered into ubiquitinated aggregates that may be a cellular pathway for turnover of abnormal proteins. Similar intranuclear ubiquitinated aggregates are seen in brains in SCA3, SCA7, Huntington’s disease, and DRPLA. The diagnosis of SCAl is established by the demonstration of expansion in one CAG repeat allele in the SCAl locus greater than 38 repeats in a patient with ataxia.
There is marked loss of inferior olivary neurons in the brainstem and marked loss in the substantia nigral neurons. In the spinal cord, marked demyelination in the posterior columns and to a lesser degree in the spinocerebellar tracts is seen. Motor neurons and neurons in Clarke’s column are reduced in size and number, and there is thinning of myelin in anterior and posterior roots. In some cases the cerebral cortex is thinned, and the white matter is atrophic and gliotic, particularly in the frontal and temporal lobes. The differential diagnosis includes all other autosomal dominant cerebellar ataxias. The saccadic abnormalities in SCA2 resemble those of AT, normally an infantile onset, recessively inherited ataxia. They are also seen in SCA7, a condition associated with visual impairment. The combination of extremely slow or absent saccades with segmental or complete areflexia but normal color vision in one or more family members with autosomal dominant ataxia strongly suggests the diagnosis of SCA2. SCA2 is caused by an expansion in CAG repeat in the SCA2 gene on 12q23-24.1 that leads to an elongated tract of glutamine residues within a novel protein, ataxin-2. Like that of the affected proteins in SCA1, SCA3, and SCA7, the function of ataxin-2 is also unknown, but unlike the other known ataxia-associated proteins in SCAl, SCA3, and SCA7, ataxin-2 is predominantly a cytoplasmic protein. Transgenic mice overexpressing mutant ataxia-2 become ataxic, but there is no Purkinje cell loss. Unlike ataxin-1, toxicity of ataxin-2 does not entail transport into the nucleus. The diagnosis of SCM is established by the demonstration of an expansion in one CAG repeat allele in the SCA2 locus greater than or equal to 34 repeats in a patient with ataxia.
SpinocerebellarAtaxia Type 2
SCA3, or Machado-Joseph disease, is the most common recognized form of SCA in most populations. The proportion of patients with SCA3 ranges from 7% in India (0% in South Africa and Italy) to 74% in Portugal, and it is found in about 21% of U.S. patients with SCA. The age of onset of SCA3 usually is the second to the fourth decade. There are also reports of rare childhoodonset variants with severe disease, as well as variants with rigidity. Initial symptoms usually are unsteadiness or stiffness of gait, clumsiness, and slurred speech, but a significant proportion of patients develop diplopia before any gait difficulty. Typically the disease is slowly progressive, leading to the need for assistive devices including a wheelchair 10 to 15 years after onset. Death results from pulmonary complications and cachexia 6 to 29 years after onset. Neurologic examination depends on the stage of the disease. There are variants of SCA3, caused in part by larger expanded alleles. Patients with the more cerebellar form of the disease may show ataxic gait and limb movements, gaze-evoked nystagmus, saccadic visual pursuits, and dysarthria. In more advanced disease other neurologic findings appear, including restricted upgaze, disconjugate eye movements, often a staring appearance to the eyes, or total ophthalmoplegia, temporal and facial atrophy, characteristic action-induced perioral twitches, lingual atrophy and fasciculations, dysphagia, and reduced cough, loss of distal sensation, and hyperreflexia combined with distal areflexia. Some family members may manifest a substantially different neurologic picture, with prominent parkinsonism or dystonia combined with rigidity or peripheral neuropathy.
The proportion of patients with SCA2 ranges from 4% in Portugal (0% in Russia) to 47% in Italy and is 15% for U.S. patients with SCA. The mean age of onset of SCA2 is in the fourth decade but progression is more rapid when onset occurs before age 20. A form of infantile-onset SCA2 has been recognized, associated with extreme expansions of SCAZ alleles, in which children have infantile spasms, severe hypotonia, pigmentary retinopathy, dysphagia, and failure to thrive and usually die before 2 years of age. In adult-onset SCA2 confinement to wheelchair may occur 10 to 20 years after onset, and death may occur 10 to 30 years after onset. Death may be caused by respiratory or autonomic failure. SCAZ is characterized by slowly progressive ataxia, sometimes with leg stiffness or painful leg muscle cramps at night. Mild dementia has been reported, which appears to be predominantly an impairment of executive functions. Examination may reveal very mild dysarthria; slowed, hypometric, or absent saccades; supranuclear ophthalmoplegia; fasciculations in the face and tongue; dystonia and chorea; and segmental or total loss of reflexes. As with SCA1, MFU brain scans reveal cerebellar and pontine atrophy. In neuropathologic studies of the cerebellum, findings are similar to those of SCA1. Purkinje cells are severely reduced in number. In the remaining Purkinje cells, dendritic branching is reduced, and torpedo-like formations are present in axons. Granule cells also are reduced in number, whereas Golgi and basket cell neurons and deep cerebellar neurons are well preserved.
Spinocerebellar Ataxia Type 3, or Machado-Joseph Disease
Chapter 124 rn Spinocerebeliar Ataxias
Brain imaging reveals pontocerebellar atrophy in most cases, but the cerebellar cortex sometimes is remarkably preserved in cases of the dystonic form of the disease. Nerve conduction studies often reveal reduced amplitude of sensory and motor nerve action potentials and evidence of denervation. Neuropathologic studies demonstrate that cerebellar Purkinje cells and inferior olivary neurons are more spared than the other dominantly inherited ataxias. Typically there is prominent loss of pontine neurons, neurons of the substantia nigra, anterior horn cells, and Clarke’s column in the spinal cord, as well as neurons in many cranial motor nuclei. The vestibular nucleus often is prominently involved. The differential diagnosis includes all other autosomal dominant cerebellar ataxias. The presence of cerebellar ataxia in one family member and dystonic-rigid condition in another firstdegree relative strongly suggests a diagnosis of SCA3. As with SCA1, the CAG repeat expansion in SCA3 occurs in a novel gene on 14q21 that leads to an elongated tract of glutamine residues within a novel, nucleocytoplasmic protein, ataxin-3. Mutant ataxin-3 proteins form intranuclear ubiquitinated aggregates in neurons in SCA3 brain. The diagnosis of SCA3 is established by the demonstration of an expansion in one CAG repeat allele in the SCA3 locus greater than 55 repeats in a patient with ataxia. SpinocerebellarAtaxia Type 6 and I t s Allellc Disorders
The proportion of patients with SCA6 ranges from 2% in Italy (0% in China, Portugal, and Brazil) to 31% in Japan, and it is found in about 15% of U.S. patients with SCA. The age of onset ranges from 19 to 71 years, with a mean age of onset in the fifth decade. Age of onset may vary between siblings with the same mutation by as much as 12 years. Initial symptoms are gait unsteadiness, stumbling, and imbalance in about 90% of cases. The remainder of patients present with dysarthria. Symptoms progress slowly, and eventually all patients have gait ataxia, upper limb incoordination, intention tremor, and dysarthria. Patients with SCA6 occasionally manifest episodic ataxia or episodic vertigo. Diplopia occurs in about 50% of patients. Others experience visual disturbances related to difficulty fixating on moving objects. Dysphagia and choking are common. Lifespan is not shortened. Neurologic examination in SCA6 reveals frequent gaze-evoked horizontal and vertical nystagmus. All patients develop dysarthria, hand incoordination, and gait ataxia. Hyperreflexia and extensor plantar responses occur in up to half of patients. Patients with SCA6 do not have sensory complaints, restless legs, stiffness, migraine, primary visual disturbances, or muscle atrophy. MRI brain scans in SCA6 show essentially pure cerebellar atrophy. Nerve conduction studies are not revealing. Neuropathologic studies show striking loss of cerebellar Purkinje cells with preservation of other neuronal regions. The differential diagnosis includes all other autosomal dominant cerebellar ataxias. Of the other SCAs, SCA6 most closely resembles SCA5, SCA8, and SCAll and the Japanese kindreds linked to the SCA4 locus, although nystagmus may be prominent in only some of these conditions. The presence of slowly progressive ataxia with prominent gaze-evoked horizontal and vertical nystagmus and a straightforward autosomal dominant inheritance pattern strongly suggests SCA6. Episodic ataxia type 2 (EA-2) is a dominantly inherited condition characterized by bouts of ataxia, dysarthria, vertigo, and
793
nausea, sometimes accompanied by migraine-like headache, confusion, and muscle weakness, lasting minutes to hours. Emotional stress, fatigue, exercise, and certain foods often precipitate spells. In addition to the ataxia there may be severe nystagmus during attacks. Between bouts of ataxia there may be gaze-evoked nystagmus and a milder degree of ataxia that increases over the years, coming to resemble that of SCA6. The condition is inherited in a autosomal dominant pattern. MRI often shows cerebellar atrophy, as in SCA6. This condition is to be distinguished from episodic ataxia type 1 (caused by mutations in a potassium channel), in which bouts of ataxia last seconds to minutes and completely resolve. The bouts of ataxia, particularly in EA-2, are prevented by administration of acetazolamide (500 to 1000 mg/day) or valproate (500 to 1500 mg/day), although it is not known whether the progression of the ataxia is slowed. Familial hemiplegic migraine (FHM) is a dominantly inherited condition of intermittent migraines in which at least some of the family members have transient hemiparesis or hemibody numbness as aura of migraine accompaniment. These patients may sometimes note some unsteadiness during attacks and with time may also have interictal ataxia and cerebellar atrophy on MRI. Standard migraine therapies, especially valproate, are successful in managing the migraines, but it is likely that progressive ataxia continues. SCA6 is caused by an expansion in a CAG repeat in the gene CACNAlA on 19~13.1,previously recognized to encode the a l A subunit, the main pore-forming subunit for the P/Q type voltage-gated calcium channel. The CAG repeat is in the extreme 3’ region, encoding a polyglutamine tract in the C terminus. These channels are highly expressed in cerebellar Purkinje cells. There is some evidence that this change in structure of the C terminus alters the function of the P/Q type channels, causing them to open more readily and remain open longer and favoring overload of Purkinje cells with calcium. The diagnosis of SCA6 is established by the demonstration of an expansion in one CAG repeat allele in the SCA6 locus greater than 19 repeats in a patient with ataxia. EA-2 and FHM are allelic disorders of the SCA6 that are associated with several CACNAlA point mutations, predicting truncation or amino acid substitution of the ala subunit. The diagnoses of FHM and EA-2 are difficult to establish because genetic testing is not available for the various mutations. Spinocerebellar Ataxla Type 7
SCA7 is a rare form of SCA in all populations. The proportion of patients with SCA7 ranges from 0.5% in Germany and Russia (0% in Portugal, Korea, India, and China) to 16% in some regions in Spain, and it is found in about 4.5% of U.S. patients with SCA. The age of onset of the symptoms ranges widely, from infancy to the fifth or sixth decade. As with SCA1, SCA2, and SCA3, the very early-onset forms are much more severe and rapidly progressive. SCA7 is characterized by abnormalities in color vision and central visual acuity, because of a macular pigmentary degeneration, and in adults visual symptoms often precede the cerebellar symptoms or are detectable upon development of imbalance. Typical cerebellar signs of gait unsteadiness, incoordination, and dysarthria develop soon afterward and progress to a bedridden state. Rate of progression depends on age of onset. In the infantile-onset form there is rapidly progressive cerebellar and brainstem degeneration, and visual loss may be difficult to ascertain before death. Otherwise, retinal degeneration is progressive and leads to blindness. When visual symptoms appear at or before adolescence,
794
Movement Disorders W
Non-Parkinsonian Movement Disorders
blindness can occur within a few years. Ataxia progresses to wheelchair confinement in 5 to 10 years. On examination, initial visual findings may be subtle and detectable only using tests of color vision. Funduscopy may show subtle granular changes in the macula. With more advanced disease, central visual acuity may diminish to the 20/200 range, color discrimination is lost, and there are more prominent pigmentary macular changes. With onset of near total blindness the pigmentary retinopathy is advanced but still has a macular pattern. Saccades are markedly slowed or entirely absent. In blind patients this is evident using the patient’s hand as a psychic target or by electronystagmography. Hyperreflexia and spasticity are evident early in the disease, as are extensor plantar responses. Patients have an ataxic gait and dysarthric speech with some component of spasticity. MRI imaging in SCA7 has shown cerebellar atrophy without brainstem involvement. Electroretinograms initially show a decrease in the photopic (cone) response, followed by a decrease in the scotopic (rod) response. The retinal degenerative component distinguishes this hereditary ataxia from other forms of SCA. In cases of extreme expansion of the SCA2 gene, pigmentary retinal degeneration can also develop. Recessive ataxias such as posterior column and retinitis pigmentosa, abetalipoproteinemia and AVED, mitochondrial encephalopathies such as NARF’, and Leber’s hereditary optic neuropathy can present with ataxia and, in some cases, with a concomitant visual degeneration. Aside from the retinal involvement, there is clinical and pathologic overlap between SCA7 and other SCAs. Although the loss of saccades is similar to that of SCA2, the hyperreflexia and spasticity in the same patient may distinguish this condition from SCA2, where reflexes are diminished. Infantile- and childhood-onset SCA7 may be confused with lipid storage diseases, such as ceroid lipofuscinoses, except the hereditary pattern is autosomal dominant. These conditions can be distinguished by DNA or other laboratory tests. Like SCAl and SCA3, SCA7 is caused by a CAG repeat expansion a novel gene on 3p21.1 and leads to an elongated tract of glutamine residues within a novel protein, ataxin-7. Mutant ataxin-7 proteins also form intranuclear ubiquitinated aggregates in neurons in SCA7 brain. The diagnosis of SCA7 is established by the demonstration of an expansion in one CAG repeat allele in the SCA7 locus greater than 36 repeats in a patient with ataxia. Autosomal Dominant Ataxias Caused by Noncoding Nucleotide Repeats
Three types of autosomal dominant SCA are caused by trinucleotide or pentanucleotide repeat expansions in noncoding regions of genes. As in the polyglutamine disorders, the repeated sequences are polymorphic in the normal genes; that is, they have a range of normal allele sizes. Disease results when these repeats become expanded to a pathologic size range. The molecular and cellular basis for the dominant pathologic effect of changes in gene structure that do not alter protein sequence and for the progressive cerebellar degeneration and ataxia is unknown. Spinocerebellar Ataxia Type 8
SCA8 originally was described in association with a single large kindred of individuals with adult-onset SCA having a dominant inheritance pattern with incomplete penetrance. In the original study there was clear distinction between normal and pathologic
alleles in a single family. However, there were numerous intermediate alleles of uncertain significance in multiple small families and in sporadic cases. Subsequent studies have reinforced the concept that such alleles should not be considered pathogenic and that the diagnosis of SCA should be confined to a narrower range of pathologic alleles (Table 124-3). Patients with pathologic alleles have a characteristic presentation. Symptoms first appear between ages 18 and 65, with a mean of 39 years. Initial symptoms consist of gait ataxia, dysarthria, and dysphagia. Findings on examination include spastic and ataxic dysarthria, gaze-evoked nystagmus, limb and gait ataxia, limb spasticity, and diminished vibratory sensation. Progression generally is fairly slow, but severely affected family members become confined to wheelchair by the fourth or fifth decade. MRI and CT brain scans show cerebellar atrophy. There are no pathologic studies to date. SCA8 is associated with an expansion of a polymorphic CTA/CTG repeat in the 3’ untranslated region of a gene located at 13q21. The gene, called kelch-related protein because of homology to the Drosophila protein, kelch, consists of either three or four exons. The length of the repeat present in the general population is 16 to 37 repeats in 99% of alleles. The repeat length that is likely to result in disease ranges from 107 to 127 CTG repeats. The diagnosis of SCA8 is suggested by the demonstration of expansion in one CTG repeat allele in the SCA8 locus greater than 106 repeats and less than approximately 300 repeats in a patient with ataxia. Spinocerebellar Ataxia Type 10
SCAlO is a form of autosomal dominant cerebellar ataxia that was recently described in several kindreds of Mexican origin. The age of onset ranges from 10 to 49 years. Initial symptoms of the disease are gait unsteadiness, clumsiness, and dysarthria. In a significant number of patients generalized motor seizures develop within a few years after onset of the ataxia. Some patients have low IQ. Findings on examination include nystagmus, dysarthria, gait and limb ataxia, and nystagmus, with normal reflexes and motor function. Seizures respond to anticonvulsants. MRI brain scans demonstrate cerebellar atrophy. There have been no pathologic studies to date. SCAlO is caused by expansion of a pentanucleotide (ATTCT) repeat in intron 9 of a novel gene on chromosome 22q13 of unknown function. Normal ATTCT repeats range from 10 to 22 ATTCT units. The expansions of the ATTCT repeat, which have not been accurately sized, are massive, up to 22.5 kb longer than the normal alleles. The SCAlO gene consists of 12 exons that span 173 kb of genomic DNA. The open reading frame encodes a 475-amino acid protein that is 82% identical to the mouse ortholog. The diagnosis of SCAlO is established by the demonstration of expansion in one ATTCT repeat allele in the SCAlO locus greater than 800 repeats in a patient with ataxia. Patients with intermediate expansions of 30 to 799 repeats would also be candidates for a possible diagnosis of SCA10, and a more detailed examination of the kindred would be appropriate. Spinocerebellar Ataxia Type 12
SCA12 has been described in two families, one American and one East Indian. If the common presenting symptom of action tremor is referenced, the age of onset is broad, ranging from 8 to 55 years, with a mean of 34 years. The initial symptom is tremor in nearly all cases. The clinical features are variable, especially the degree of cerebellar dysfunction. Findings on examination include occa-
Chapter 124
sional cognitive impairment, gaze-evoked nystagmus, action, postural, or kinetic tremor of the head or arms, bradykinetic limb movement, paucity of spontaneous movement, rare focal dystonia, mild to moderate gait and limb ataxia, and mild dysarthria, hyperreflexia, and Babinski signs. CT scanning and MRI show cerebellar and cerebral atrophy. The electroencephalogram and electromyogram with nerve conduction studies are normal. SCA12 is caused by expansions of a CAG repeat tract that lies 133 nucleotides upstream of the reported transcription start site of the PPP2FUB gene at 5q31333. This gene encodes a brain-specific regulatory subunit of the protein phosphatase PP2A. Normal CAG repeat alleles have 7 to 28 repeats. Pathologic alleles have 55 to 78 CAG repeats. The diagnosis of SCAl2 is established by the demonstration of expansion in one CAG repeat allele in the SCA12 locus greater than 55 repeats in a patient with ataxia. Intermediate expansions of 29 to 54 repeats are also candidates for disease alleles, but more detailed examination of the kindred is needed.
Autosomal Dominant Ataxias with a Defined Genetic Locus Genetic linkage studies have confirmed the existence of at least five other forms of autosomal dominant ataxia and have localized the responsible genes to intervals of 3 and 10 cM. Newly diagnosed patients with dominant SCA and negative gene tests may represent new kindreds with these less well-characterized ataxias. The differential diagnosis includes all other autosomal dominant cerebellar ataxias. The genes for each of these dominant ataxias are tightly linked to small chromosomal regions between defined microsatellitemarkers (Table 124-3). Until the genes are identified, the diagnosis of these disorders can only be suspected by demonstration of genetic linkage using these markers. The designations for SCA9 and SCA15 have been reserved. Clinical features for these subtypes have not yet been reported.
Spinocerebellar Ataxia v p e4 SCA4 was originally described in a single large Utah family whose disease was mapped genetically to a locus of 16q22.1. The age at onset of disease ranges from 19 to 59 years (mean 39 years), but it usually appears in the fourth or fifth decade. Patients initially develop gait unsteadiness, followed by difficulty with fine motor tasks and often dysarthria. The condition is slowly progressive over decades, typically leading to wheelchair dependence. Patients often admit to sensory loss or paresthesias. However, there is wide variability in the severity of disease among family members, and some patients develop foot deformities and severe bulbar symptoms. Examination shows prominent distal sensory loss for multiple modalities, at times encompassing the entire limbs, and partial or complete areflexia. Loss of ankle jerks is an early finding. Sensory nerve amplitudes are diminished or absent. Recently, six Japanese families with autosomal dominant cerebellar ataxia were identified whose disease was genetically linked to the same chromosomal region, 16q22.1. In these the age of onset ranged from 45 to 72 years (mean 55.9 years), with gait ataxia and dysarthria as initial symptoms. Findings on examination were gait and limb ataxia and horizontal gaze nystagmus. Sensation was normal in all subjects except for one 85-year-old patient. Tendon reflexes were mostly normal, except that some subjects (16.6%) had slightly decreased ankle jerks. In further contrast to the Utah patients, sensory and motor nerve conduction
SpinocerebellarAtaxias
795
studies were normal in these patients. MRI of the brain in both groups shows cerebellar atrophy without obvious brainstem involvement. The gene for SCA4 has been genetically mapped to 16q22.1. Isolation of the SCA4 gene will be necessary to confirm that these two conditions are allelic disorders.
Spinocerebellar Ataxia Types 5,11, and 16 SCA5 was originally described in an American family of AngloSaxon origin descending from the grandparents of President Abraham Lincoln. The genetic locus was assigned to chromosome 11. Subsequently, a second SCA family of French origin was identified with a similar clinical presentation in which the responsible gene is located in the same region. Initial symptoms consist of slowly progressive gait unsteadiness and dysarthria. The age of onset was 10 to 68 years, usually in the third decade. The ataxia is very slowly progressive, and some patients remain ambulatory for more than 10 years. Examination shows evidence of a pancerebellar syndrome with intact or increased reflexes, normal plantar reflexes, and normal sensory examination. Facial myokymia is a prominent feature among the French kindred. Nystagmus is less prominent than in SCA6 or SCA8. MRI shows a marked global cerebellar atrophy with sparing of the brainstem. The gene for SCA5 has been genetically mapped to 1l p l l - q l l . SCAl1, which has been described in one British family, has a similar age of onset (15 to 43 years, mean 25 years) and clinical picture to those of SCA5, consisting of a slowly progressive cerebellar syndrome without clinical evidence of involvement of other brainstem pyramidal or extrapyramidal regions. Nearly all patients are ambulatory, with a mean disease duration of 24 years. SCAll does not appear to shorten lifespan. All people in the kindred continue to be ambulatory, with a mean disease duration of 23.9 f 13.4 years. Examination demonstrates dysarthria, limb and gait incoordination, nystagmus, and mild hyperreflexia with normal plantar reflexes. Brain imaging shows isolated cerebellar atrophy. The gene for SCAll has been genetically mapped to a 7.6-cM interval 15qlPq21.3. SCA16 has been described in one Japanese kindred. Patients in this family develop slowly progressive gait unsteadiness and dysarthria beginning between ages 20 and 66. Examination reveals cerebellar signs including truncal and limb ataxia, scanning dysarthria, and horizontal gaze-evoked nystagmus and impaired visual pursuit. MRI scans show pure cerebellar atrophy. The gene for SCA16 has been genetically mapped to a 37.6-cM interval 8q22.1424.1.
Spinocerebellar Ataxia Types 13 and 14 SCA13 and SCA14 were described in two kindreds whose disease maps genetically to two adjacent loci on chromosome 19. SCA13 was described in a single four-generation French kindred with autosomal dominant cerebellar ataxia. The disease in this family has onset in childhood, often in the first year of life. Initial symptoms are clumsiness and dysarthria, along with evidence of cognitive slowing. Examination demonstrates cerebellar signs, nystagmus, and pyramidal signs in some. Neuropsychiatric testing reveals moderate mental retardation (IQ, 62 to 76), and mild developmental delay in motor acquisition. MR brain imaging shows moderate cerebellar and pontine atrophy. The gene for SCA13 has been genetically mapped to an 8-cM interval chromosome 19q13.3.
796
Movement Disorders H Non-Parkinsonian Movement Disorders
SCA14, described in a single four-generation Japanese kindred, has a distinct clinical picture from that of SCA13. The age of onset ranges from 3 to 42 years. Initial symptoms are gait ataxia in many cases. However, in several patients with an earlier onset initial signs include an irregular tremulousness of the neck and axial musculature, described as intermittent axial myoclonus, followed soon afterward by mild ataxia. Disease progression usually is slow. Other findings on examination included gaze-evoked nystagmus, saccadic visual pursuits, upper and lower limb ataxia, dysarthria, and reduced Achilles reflexes. Neuroimaging studies reveal cerebellar atrophy. The gene for SCA14 has been genetically mapped to a 10.2-cM interval 19q13.4-qter, surprisingly near the region defined for SCA13.
SPORADIC ATAXIA About half of patients with SCA do not appear to suffer from a form of familial SCA (Table 124-4). Nevertheless, some of these patients may actually have an unsuspected form of hereditary ataxia. Five to eight percent of patients with sporadic ataxia are found to have GAA expansions in the frataxin-1 gene and have a variant of FRDA. An additional 2% to 11% of patients with
TMU 124-4. Approach for Patients with Ataxia and No Known Family History Routine studies Metabolic panel (diabetes, liver disease, renal disease) CBC differential (pernicious anemia, sideroblastic anemia) TFT (hypothyroidism) VDRL (syphilis) Lyme serology (Lyme disease) Erythrocyte sedimentation rate Vitamin E, vitamin B,, vitamin B,2, nicotinamide Brain and spine MRI (cerebellar atrophy, demyelinating disease, posterior fossa mass) Alcohol history Immune ataxias Serum antibodies to voltage-gated calcium channels, glutamic acid decarboxylase, glutamate receptors, and the Purkinje cell autoantibodies anti-Yo, anti-Ri, anti-Ti, and anti-Hu Serum antigliadin antibodies Cryptic hereditary ataxias Dominant SCAl-SCA3, SCAC-SCAB, SCAlO gene tests for dominant ataxias (commercially available) SCAI 2, SCAI 5 (research) Mutations in PRP gene P102L, P1OSL, A1 17V, Y 145X, V1 SOV, E200K, M232R (Gerstmann-Straussler disease) Recessive Frataxin-1 (GAA)n repeat gene test, FRDA genetic screen for frataxin mutations Quantitative immunoglobulins, a-fetoprotein, chromosome breakage study, X-ray sensitivity, ATM mutations (research); blood studies to exclude ataxia telangiectasia Vitamin E level, lipoprotein electrophoresis (AVED/ abetalipoproteinemia) Hexosaminidase A assay with sulfated substrate (atypical hexosaminidase A deficiency) Muscle biopsy for CoQlO (muscle CoQlO deficiency) Sacsin mutations (research) (ARSACS) Very long chain fatty acids (Refsum’s disease) X-linked CBC, differential for sideroblasts @-linked sideroblastic anemia with ataxia) Very long chain fatty acids (adrenomyeloneuropathy) Mitochondria1 Fasting and 2-hour postprandial plasma glucose, pyruvate, and lactate CSF lactate Mitochondria DNA mutations 18993, A8244 Prion-associated ataxias CSF 14-1-3-3 orotein (sooradic or hereditaw orion-associated ataxia9
apparently sporadic ataxia have a form of SCA for which a genetic test is available, such as SCA1. In the case of recessive conditions, for which a single occurrence of the disease is not unusual, the diagnosis of FRDA may not be suspected on clinical grounds because of some atypical features. These patients are important to identify, particularly because of the unique complications for which they are at risk and because they are candidates for emerging therapies for FRDA. In the case of autosomal dominant conditions, the diagnosis may not be suspected because the affected parent is unknown, dies before disease onset, has a milder condition or later age of onset than the patient, or bears only a premutation, or for other reasons the disease has reduced penetrance. These patients are important to recognize for similar reasons as well as for potential issues of family genetic counseling. Finally, other cases may represent mitochondrial disorders that are difficult to diagnose. Therefore, in the absence of a family history, genetic screening for the available genetic ataxias is appropriate if no other cause is demonstrable because up to 20% may be hereditary. If patients with unsuspected hereditary ataxia are discounted, about one third of patients with progressive ataxia have a truly sporadic form of the disease. These patients do not have a clinically recognizable, recessively inherited form, such as AT or FRDA, and have no family history of ataxia or neurologic disease that could have been an undiagnosed case of ataxia. Genetic testing is negative for the current genetically characterized forms, such as SCA1-SCA3, SCA6-SCA8, and FRDA. These conditions, called sporadic SCA, are the most challenging group of ataxias from a diagnostic, prognostic, and management standpoint. On one hand, the emphasis on genetic testing has caused frustration among these patients and physicians because of a lack of a definitive genetic diagnosis. Although the genetic advances have yet to impact the treatment of ataxia, patients with the diagnosis of sporadic ataxia will not have the benefit of genetic counseling or of an accumulating experience on the natural history and prognosis of the disease. On the other hand, the insights gained from genetic studies of SCA, particularly of SCA8, have shown that variable penetrance can obscure the presence of a hereditary condition. Thus, there remains the lingering concern that a given patient with sporadic ataxia may have an unrecognized hereditary ataxia. Patients with sporadic ataxia usually have one of two clinical presentations. Onset of sporadic ataxia typically occurs in the sixth decade but may occur over a wide age range. Approximately two thirds of these patients develop a condition characterized by cerebellar ataxia alone (i.e., with little or no involvement of other regions of the nervous system). These patients have a more slowly progressive form, may remain ambulatory for well beyond 5 years, and do not have a shortened lifespan. Neurologic examination, which may resemble that of patients with SCA6, reveals essentially cerebellar signs of dysarthria, truncal ataxia, and hand incoordination, often with nystagmus and brisk deep tendon reflexes. Occasionally vibratory sense is reduced and ankle reflexes are absent. The remaining approximately one third of patients with sporadic ataxia develop a form of multiple-system atrophy, characterized by ataxia associated with a combination of dementia, ophthalmoplegia, bulbar findings, tremor, bradykinesia or rigidity, autonomic dysfunction, or other neurologic abnormalities. These patients often have a more aggressive course leading to confinement to wheelchair by 5 years and in which frequent aspiration, reduced respiratory drive, or urinary retention leads to premature death by respiratory failure or sepsis. Neurologic examination, which resembles that of patients with SCAl, SCA2,
Chapter 124
or SCA3, may reveal slowed saccades and restricted ocular versions or nystagmus, spastic dysarthria, dysphonia, bradykinesia, resting or postural tremor, rigidity, spasticity, extensor plantar responses, and, rarely, amyotrophy. Brain imaging in sporadic ataxia shows cerebellar atrophy in nearly all cases at the time of presentation. Those with the ataxic form of multiple-system atrophy may simultaneously have generalized cerebral atrophy or may develop prominent atrophy of the pons, particularly the basis pontis with time. Conditions that may present as a form of sporadic SCA include Creutzfeldt-Jakob disease (CJD),subacute cerebellar degeneration, hypothyroidism, vitamin deficiency, chronic ethanol abuse, or a mitochondrial disorder. Sporadic ataxia has been associated with several different autoantibodies, although this finding is more typical of subacute cerebellar degeneration. Nevertheless, the majority of patients with sporadic ataxia have a truly idiopathic condition. After excluding a role for medical causes of ataxia in a given patient, such as diabetic polyneuropathy, hypothyroidism, or vitamin deficiency, consideration should be given to rare, but potentially identifiable conditions. Included among these are ataxia associated with antibodies and ataxic variants of prion disease.
W
Spinocerebellar Ataxias
797
the disorder is transmissible through certain treatments such as corneal transplants. Although ataxia often is a prominent feature of CJD, such patients usually have multiple other neurologic findings (pyramidal or extrapyramidal signs, myoclonus, akinetic mutism) and typical electroencephalographic changes (periodic sharp waves) that allow recognition of this condition. T2- or diffusion-weighted MR images in these cases may demonstrate multiple scattered cortical and deep gray matter hyperintensities. There may be generalized cortical atrophy but usually no cerebellar atrophy. There is also an ataxic variant of the disease more common among iatrogenic CJD and the autosomal dominant forms (Gerstman-Straussler-Schenkerdisease). In the ataxic variant other neurologic findings are present, but ataxia is the most prominent feature. Cerebellar atrophy has been documented in some of these patients. The electroencephalogram may not show the typical changes. The finding of an increase in the neuronal proteins, 14-3-3 protein and neuron-specific enolase, in cerebrospinal fluid supports the diagnosis but is a nonspecific finding. Hereditary CJD is associated with certain alleles of the prion protein gene (PrP), particularly with variations at codons 102,117, 129 (methionine or valine), and 178. The various forms of CJD progress more rapidly than the SCAs and are uniformly fatal. No treatments exist €or these conditions.
Antibody-AssociatedAtaxias
Ataxia associated with autoantibodies is more commonly manifested in the syndrome of subacute cerebellar degeneration associated with malignancy (see Chapter 178). However, in the early stages the presentations of these conditions may be similar. Autoantibodies to several antigens found in cerebellar Purkinje cells have been found in sera of patients with ataxia. Antibodies to voltage-gated calcium channels, glutamic acid decarboxylase (GAD), and glutamate receptors, as well as the Purkinje cell autoantibodies called anti-Yo, anti-Ri, and anti-Ti are associated with ataxia, usually in association with malignancies such as small lung carcinoma, adenocarcinoma of the breast or ovary, or Hodgkin’s disease. Rarely, these antibodies, particularly in the case of anti-GAD, may be found in sera of patients with progressive ataxia. The presentation of ataxia in association with these antibodies in an otherwise healthy patient should prompt an extensive workup for occult malignancy. Except in the case of anti-GAD antibodies and anti-VGCC antibodies, there is no evidence demonstrating that autoantibodies have a role in the pathogenesis of ataxia. Some of these antibodies may be markers of another autoimmune process or merely an indicator of cerebellar damage. Plasmapheresis has not had any convincing benefit in these conditions. Antibodies to gliadin (the protein in gluten), as found in celiac sprue, have been detected in sera of patients with ataxia. Patients with ataxia may have a history of gastrointestinal symptoms or may have simply an abnormal jejunal biopsy. The ataxia is said to be unrelated to vitamin malabsorption. These patients are important to recognize because there is some evidence that ataxia may improve with dietary restriction of gluten. No distinguishing clinical features are found in the antibody-associated ataxias. Prion-AssociatedAtaxia
CJD and its variants are spongiform encephalopathies caused by accumulation of proteinaceous particles called prions, typically manifesting as rapidly progressive dementia (see Chapter 79). There are both autosomal dominant and sporadic variants, and
MANAGEMENT OF PROGRESSIVE ATAXIA There are no definitive therapies that delay or halt the progression of the disease. The focus in care for these patients is on optimizing their ability to compensate for and cope with a chronic progressive neurologic condition and on managing symptoms and complications. This is accomplished through the proper referrals for physical and occupational therapy and by encouraging exercise and psychological counseling. Canes and walkers help prevent patients from falling. Early use of a cane may avoid psychological stigma and may prevent confusion with alcohol intoxication. Modification of the home with such conveniences as grab bars, raised toilet seats, and ramps to accommodate motorized chairs often is helpful. Prophylactic eye care, including use of sunglasses and limitation of ultraviolet exposure, should be encouraged to limit extraneous damage to the retina in the case of SCA7. Speech therapy and communication devices such as writing pads and computer-based devices may benefit those with dysarthria. Weighted eating utensils and dressing hooks help maintain a sense of independence. Weight control is important because obesity can exacerbate difficulties with ambulation and mobility. When dysphagia becomes troublesome, video esophagrams can identify maneuvers and the consistencies of food least likely to trigger aspiration. Tremor-controlling drugs do not work well for cerebellar tremors, but these patients may also develop postural or resting tremors that are amenable to conventional symptomatic therapy. Drugs used in Parkinson’s disease, such as amantadine and levodopa, may be of benefit when extrapyramidal signs such as bradykinesia and rigidity are present. Spasticity responds to baclofen. Drooling may be managed by anticholinergic medications aided by a suction apparatus. Seizures, for example in SCA10, respond to anticonvulsants. Axial myoclonus, as occurs in SCA13, responds to diazepam or valproate. Vertigo and oscillopsia may respond to vestibular suppressant medications, such as antihistamines or Lioresal. Vitamin supplements are recommended, particularly if caloric intake is reduced. Because of toxic effects may be additive, patients should avoid alcohol.
798
Movement Disorders
Non-Parkinsonian Movement Disorders
SUGGESTED READINGS Allikmets R, Raskind WH, Hutchinson A et al: Mutation of a putative mitochondrial iron transporter gene (ABC7) in X-linked sideroblastic anemia and ataxia (XLSA/A). Hum Mol Genet 8(5):743-749, 1999
Delatycki MB, Williamson R, Forrest SM: Friedreich ataxia: an overview. J Med Genet 37( 1):l-8, 2000 De Vivo D C The expanding clinical spectrum of mitochondrial diseases. Brain Dev lS(1):l-22, 1993 Federico A, Palmeri S, Malandrini A et al: The clinical aspects of adult hexosaminidase deficiencies. Dev Neurosci 13(4-5):280-287, 1991
Geneclinics: Hereditary Ataxia Overview http://www.geneclinics.org/profiles/ataxias/details.htm~ Gomez CM: Inherited ataxia. In Johnson RT (ed): Current Therapy and Neurologic Disease. WB Saunders, Philadelphia, 2001 Handbook of ataxia disorders. In Klockgether T (ed): Neurological Disease and Therapy. Vol. 50. Marcel Dekker, New York, 2000 Harding AE: The hereditary ataxias and related disorders. In Clinical Neurology and Neurosurgery Monographs. Vol. 6. Churchill Livingstone, New York, 1984 Higgins JJ,Morton DH, Loveless JM: Posterior column ataxia with retinitis pigmentosa (AXPC1) maps to chromosome lq3 1 4 3 2 . Neurology 52( 1):146-150, 1999
Klockgether T, Wullner U,Spauschus A, Evert B: The molecular biology of the autosomal-dominant cerebellar ataxias. Mov Disord 15(4):604612, 2000
Musumeci 0, Naini A, Slonim AE et al: Familial cerebellar ataxia with muscle coenzyme QlO deficiency. Neurology 56(7):849-855, 2001 Online Mendelian Inheritance in Man http://www.ncbi.nlm.nih.gov/Omim/ Ouahchi K, Arita M, Kayden H et ak Ataxia with isolated vitamin E deficiency is caused by mutations in the alpha-tocopherol transfer protein. Nat Genet 9(2):141-145, 1995 Poser S, Zerr I, Schroeter A et al: Clinical and differential diagnosis of Creutzfeldt-Jakobdisease. Arch Virol Suppl 16:153-159, 2000 Puccio H, Koenig M: Recent advances in the molecular pathogenesis of Friedreich ataxia. Hum Mol Genet 9(6):887-892, 2000 Richter A, Morgan K, Bouchard JP et al: Clinical and molecular genetic studies on autosomal recessive spastic ataxia of Charlevoix-Saguenay (ARSACS). Adv Neurol61:97-103, 1993 Sharp D, Blinderman L, Combs KA et al: Cloning and gene defects in microsomal triglyceride transfer protein associated with abetalipoproteinaemia. Nature 365:65-69, 1993 Spacey SD, Gatti RA, Bebb G The molecular basis and clinical management of ataxia telangiectasia. Can J Neurol Sci 27(3):184-191, 2000
Tan E, Ashizawa T Genetic testing in spinocerebellar ataxias: defining a clinical role. Arch Neurol 58(2):191-195, 2001
125 Tremors Frisso Potts Tremor is an involuntary, rhythmic oscillation of a body part produced by synchronized contraction of antagonist muscles. These oscillations tend to have a consistent frequency and can be made to appear and disappear by postural adjustments of the body part. These characteristics, discussed later in this chapter, allow us to differentiate tremors from other kinds of movement disorders.
DIAGNOSIS The easiest way to classify tremors clinically is as follows: Tremor at rest: Parkinson’s disease Tremor during voluntary activity (action tremors): Physiologic tremor Enhanced physiologic tremor Essential or familial tremor Neuropathic tremor Writing tremor Orthostatic tremor Cerebellar tremor Tremors at rest are most obvious when the affected body part is in repose and are abolished or much diminished during voluntary movement. The opposite is true of action tremors. The clinical examination of the tremulous patient usually starts with visual inspection while the patient sits on a straight-backed, armless chair, forearms resting supinated at the thighs and hands
allowed to rest between the slightly abducted knees. This position will bring out most tremors at rest. In some cases, it may be necessary to ask the patient to perform complex silent calculations or cause other types of mild mental stress (e.g., asking the patient who the fifth vice-president of the United States was) to distract the patient and bring out the tremor. This is especially true if the patient has become adept at hiding the tremor. As a general rule, the less attention the patient pays to a resting tremor, the more likely it is to occur. Asking the patient to hold his o r her arms outstretched with fingers spread will activate most action tremors. In some cases, it may be necessary to ask the patient to perform a precise maneuver such as holding a pencil point close to but not touching a small target. Other provocative maneuvers are discussed further later in this chapter. Clinical observation may be further refined by electrophysiologic studies, such as electromyography, that record the frequency and amplitude of the tremor and the pattern of underlying muscle activity. These tremor tests are painless and easily performed, and they increase diagnostic accuracy, especially in cases of mixed tremor types or tremors that fail to respond to treatment. Figure 125-1 demonstrates the patterns seen in some commonly encountered tremors.
TREMOR AT REST Rest tremor is seen exclusively in Parkinson’s disease and in drugor toxin-induced parkinsonism. Most often, the tremor involves the muscles of the forearm, giving the characteristic pill-rolling appearance. The tremor may also be seen in other parts of the
798
Movement Disorders
Non-Parkinsonian Movement Disorders
SUGGESTED READINGS Allikmets R, Raskind WH, Hutchinson A et al: Mutation of a putative mitochondrial iron transporter gene (ABC7) in X-linked sideroblastic anemia and ataxia (XLSA/A). Hum Mol Genet 8(5):743-749, 1999
Delatycki MB, Williamson R, Forrest SM: Friedreich ataxia: an overview. J Med Genet 37( 1):l-8, 2000 De Vivo D C The expanding clinical spectrum of mitochondrial diseases. Brain Dev lS(1):l-22, 1993 Federico A, Palmeri S, Malandrini A et al: The clinical aspects of adult hexosaminidase deficiencies. Dev Neurosci 13(4-5):280-287, 1991
Geneclinics: Hereditary Ataxia Overview http://www.geneclinics.org/profiles/ataxias/details.htm~ Gomez CM: Inherited ataxia. In Johnson RT (ed): Current Therapy and Neurologic Disease. WB Saunders, Philadelphia, 2001 Handbook of ataxia disorders. In Klockgether T (ed): Neurological Disease and Therapy. Vol. 50. Marcel Dekker, New York, 2000 Harding AE: The hereditary ataxias and related disorders. In Clinical Neurology and Neurosurgery Monographs. Vol. 6. Churchill Livingstone, New York, 1984 Higgins JJ,Morton DH, Loveless JM: Posterior column ataxia with retinitis pigmentosa (AXPC1) maps to chromosome lq3 1 4 3 2 . Neurology 52( 1):146-150, 1999
Klockgether T, Wullner U,Spauschus A, Evert B: The molecular biology of the autosomal-dominant cerebellar ataxias. Mov Disord 15(4):604612, 2000
Musumeci 0, Naini A, Slonim AE et al: Familial cerebellar ataxia with muscle coenzyme QlO deficiency. Neurology 56(7):849-855, 2001 Online Mendelian Inheritance in Man http://www.ncbi.nlm.nih.gov/Omim/ Ouahchi K, Arita M, Kayden H et ak Ataxia with isolated vitamin E deficiency is caused by mutations in the alpha-tocopherol transfer protein. Nat Genet 9(2):141-145, 1995 Poser S, Zerr I, Schroeter A et al: Clinical and differential diagnosis of Creutzfeldt-Jakobdisease. Arch Virol Suppl 16:153-159, 2000 Puccio H, Koenig M: Recent advances in the molecular pathogenesis of Friedreich ataxia. Hum Mol Genet 9(6):887-892, 2000 Richter A, Morgan K, Bouchard JP et al: Clinical and molecular genetic studies on autosomal recessive spastic ataxia of Charlevoix-Saguenay (ARSACS). Adv Neurol61:97-103, 1993 Sharp D, Blinderman L, Combs KA et al: Cloning and gene defects in microsomal triglyceride transfer protein associated with abetalipoproteinaemia. Nature 365:65-69, 1993 Spacey SD, Gatti RA, Bebb G The molecular basis and clinical management of ataxia telangiectasia. Can J Neurol Sci 27(3):184-191, 2000
Tan E, Ashizawa T Genetic testing in spinocerebellar ataxias: defining a clinical role. Arch Neurol 58(2):191-195, 2001
125 Tremors Frisso Potts Tremor is an involuntary, rhythmic oscillation of a body part produced by synchronized contraction of antagonist muscles. These oscillations tend to have a consistent frequency and can be made to appear and disappear by postural adjustments of the body part. These characteristics, discussed later in this chapter, allow us to differentiate tremors from other kinds of movement disorders.
DIAGNOSIS The easiest way to classify tremors clinically is as follows: Tremor at rest: Parkinson’s disease Tremor during voluntary activity (action tremors): Physiologic tremor Enhanced physiologic tremor Essential or familial tremor Neuropathic tremor Writing tremor Orthostatic tremor Cerebellar tremor Tremors at rest are most obvious when the affected body part is in repose and are abolished or much diminished during voluntary movement. The opposite is true of action tremors. The clinical examination of the tremulous patient usually starts with visual inspection while the patient sits on a straight-backed, armless chair, forearms resting supinated at the thighs and hands
allowed to rest between the slightly abducted knees. This position will bring out most tremors at rest. In some cases, it may be necessary to ask the patient to perform complex silent calculations or cause other types of mild mental stress (e.g., asking the patient who the fifth vice-president of the United States was) to distract the patient and bring out the tremor. This is especially true if the patient has become adept at hiding the tremor. As a general rule, the less attention the patient pays to a resting tremor, the more likely it is to occur. Asking the patient to hold his o r her arms outstretched with fingers spread will activate most action tremors. In some cases, it may be necessary to ask the patient to perform a precise maneuver such as holding a pencil point close to but not touching a small target. Other provocative maneuvers are discussed further later in this chapter. Clinical observation may be further refined by electrophysiologic studies, such as electromyography, that record the frequency and amplitude of the tremor and the pattern of underlying muscle activity. These tremor tests are painless and easily performed, and they increase diagnostic accuracy, especially in cases of mixed tremor types or tremors that fail to respond to treatment. Figure 125-1 demonstrates the patterns seen in some commonly encountered tremors.
TREMOR AT REST Rest tremor is seen exclusively in Parkinson’s disease and in drugor toxin-induced parkinsonism. Most often, the tremor involves the muscles of the forearm, giving the characteristic pill-rolling appearance. The tremor may also be seen in other parts of the
Chapter 125
FIG. 125-1. Tremor recordings in (A) physiologic tremor, (6) Parkinson’s disease, and (C) essential tremor. Surface electromyographic tracings are from wrist extensors (WE) and from wrist flexors (WF). The accelerometric tracing from the index finger is at the bottom of each tracing. Note diminution of tremor as subject goes from rest to reaching for an object (6).Time base is 1 second.
Tremors
799
-
wJ--
WE WF
body, although it is unusual for this to happen without some involvement of the upper extremities. Voluntary movement abolishes or markedly decreases the amplitude of the tremor. Thus, it rarely affects the patient’s writing or interferes severely with activities of daily living. However, there are patients in whom the severity of the tremor makes it more than a cosmetic nuisance. As many as 20% of patients with resting tremor of Parkinson’s disease may have a superimposed action tremor, A tremor recording in Parkinson’s disease demonstrates alternating electromyographic (EMG) bursts in antagonist muscles at a frequency of 3 to 7 Hz (Fig. 125-1).The tremor appears to be generated by rhythmic activity of the lower motor neuron caused by descending rhythmic discharges from the hemispheres and uninfluenced by segmental stretch reflexes because dorsal rhizotomy does not affect the tremor. The recording has the appearance of voluntary flexion-extension, pronation-supination movements of the hand; with little effort, a normal subject may generate a tremor recording indistinguishable from that of an affected individual. The supranuclear origin of the tremor is also supported by the presence of rhythmic neuronal bursts in the contralateral sensorimotor cortex and ventrolateral thalamus in monkeys with l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine(MPTP)-induced parkinsonism. Similar activity has been recorded from the thalamus of patients with Parkinson’s disease. These bursts are not affected by deafferentation and can be eliminated by lesions of the appropriate thalamic nuclei with consequent resolution of the tremor. The tremor usually improves with dopaminergic treatment for Parkinson’s disease. Occasionally, the decrease in rigidity brought about by these drugs uncovers or enhances the resting tremor. For these cases, and for those who fail to respond to dopaminergic treatment, concomitant therapy with anticholinergic agents should be tried. A daily dosage of 1 to 6 mglday of benztropine mesylate or 2 to 12 mg trihexyphenidyl hydrochloride may be useful. The medication should be given in three or four divided doses, and the least amount needed for beneficial effect used. When pharmacotherapy fails, severe cases of tremor at rest may be approached surgically. Stereotactic thalamotomy of the ventral intermediate nucleus and chronic electrical stimulation of this site without thalamotomy have shown encouraging results. Lately, stereotactic pallidotomy and cerebellar stimulation have gained increased acceptance.
ACTION TREMORS
Not every investigator agrees with the use of the term action tremor. There are those who prefer the term postural tremor, whereas others prefer to divide these tremors into kinetic (those occurring during movement) and static (those occurring while the limb is held in a fixed position). Further categorization introduces the term tusk-specific tremor, referring to tremors that occur only during a specific movement or task. I have chosen not to burden the reader with multiple subdivisions and I discuss each action tremor under this fairly broad term. Tremors, in general, are very sensitive to changes in metabolic or emotional states. Anxiety tends to increase the amplitude of tremors, especially of action tremors, and it may be the precipitating cause in some cases. Many medications, including the following, are known to produce or enhance action tremor: Corticosteroids Methylxanthines Lithium Heavy metals Thyroid hormone Glutamates Catecholamines Neuroleptics Tricyclics Nicotine Bromides Valproic acid Physiologic Tremor
Physiologic tremor is the most ubiquitous of the tremors discussed earlier. AU people have it to a greater or lesser extent. It can be easily demonstrated by having a subject hold out an arm with fingers outstretched. The tremor usually is so slight that it cannot be seen on the fingers, but if a piece of paper is laid across the hand, the oscillations are amplified and become obvious. The genesis of this tremor probably is the combination of such disparate elements as individual motor unit recruitment rates and the intrinsic elastic properties of joints and other bony and
800
Movement Disorders rn Non-Parkinsonian Movement Disorders
connective tissue components. Mechanical perturbations caused by circulatory pulse waves may also contribute to the tremor. No treatment is required. Enhanced Physiologic Tremor
Enhanced physiologic tremor is easily seen in the outstretched fingers; it is of much larger amplitude than physiologic tremor and it can be disabling. Although it does not affect gross movements such as tracking an object, it affects writing and other precise tasks. This tremor may be seen and heard because it may affect the speech apparatus. Tremor recording shows a regular rhythm at about 10 Hz, and the surface EMG activity shows alternating bursts in antagonist muscles. The tremor is associated with muscle fatigue and may be induced in normal subjects by the administration of epinephrine or its congeners. Expectedly, it is the tremor of fear and anxiety, notably of stage fright. This tremor may also be a result of metabolic derangements. It is the tremor of hyperthyroidism, Cushing’s disease, and withdrawal from alcohol and minor sedatives. Therefore, it is important to look for underlying conditions causing a hyperadrenergic state. This is especially true if the tremor is continuous rather than intermittent, as would be the case in anxiety. The drugs listed earlier in this chapter may produce or enhance this tremor. The catecholamines’ effect is mediated by peripheral P-adrenergic receptors. That the locus of action of these drugs is outside the central nervous system has been demonstrated by intra-arterial infusion experiments. Conversely, blockade of these drugs with propranolol diminishes or abolishes the tremor. It appears that these receptors are instrumental in producing synchronous a-motor neuron discharges by enhancing the stretch reflex arc. What is not known is the exact location of the receptors and how they go about modulating neural activity. Removing underlying causes (environmental or metabolic) is the best management. When this is not possible, single doses of 20 to 40 mg propranolol provide relief for several hours. This is especially useful in the prophylactic treatment of performing artists. If there is concern over the potential bronchoconstrictive or hypoglycemic effect of propranolol’s P,-blockade, pure PIblockers (metoprolol) may be used. These are not as effective, and higher dosages may be needed. Essential Tremor
Also known as familial, rubral, or static tremor, essential tremor is most often seen affecting the upper extremities while a patient carries out precise tasks. It may involve other body parts, however, and gives the voice a quavering sound when it affects pharyngeal and laryngeal muscles. It is most common in older age groups and is responsible for most cases of so-called senile tremor. Although 60% of patients with essential tremor have a family history, sporadic cases abound. Transmission appears to be autosomal dominant, but the gene locus has not been found. An important diagnostic point is that this tremor rarely, if ever, affects a body part without affecting the upper extremities first. The literature is replete with cases of isolated essential tremor involving neck muscles, a single digit, or a foot. In most of these cases, closer examination would find a focal dystonia presenting as tremor. In general, patients with essential tremor have no other neurologic symptoms or signs. However, this tremor often coexists with acquired dystonias, such as writer’s cramp and torticollis. As many as 20% of patients with Parkinson’s disease have a
superimposed essential tremor. This does not necessarily mean that patients who develop essential tremor are at a higher risk than the general population for developing Parkinson’s disease. The frequency of the tremor ranges from 5 to 10 Hz, faster in younger patients and decreasing with age, even in the same person. Surface EMG recordings demonstrate synchronous bursts in antagonist muscles (Fig. 125-1). In cases of dystonia presenting as tremor (the nodding head of torticollis is a classic example) or in cases of dystonia and tremor coexisting, the EMG pattern would nicely tease out the complex interaction between the participating muscles. This tremor probably is suprasegmental in origin because manipulation of segmental reflex arcs has little effect on its amplitude or rhythm. Positron emission tomography studies using radioactive water or carbon- 15-labeled carbon dioxide suggest that abnormal activation of the cerebellum and red nucleus may play a role in its genesis. At present, its pathophysiology is unknown. A remarkable feature of this tremor is its response to alcoholic beverages. Within minutes of ingesting 0.5 to 1 ounce of ethanol, patients experience a decrease in tremor amplitude that may last for several hours. As the effect dissipates, a transient worsening may occur. Well-controlled studies have confirmed this effect and have shown that its action is within the central nervous system because intra-arterial injection of ethanol has no effect on the tremor. P-Blockers also have a beneficial effect on the tremor, but unlike ethanol, a single intravenous or oral dose has no effect; they may not be effective unless administered for several days. As a general rule, nonselective P-blockers are more effective than selective P,- or P,-blockers. Lipophilic P-blockers are more effective than nonlipophilic ones because of their greater penetration of the blood-brain barrier. Some patients may respond to as little as 30 mg/day propranolol in divided doses; others may need ten times that much. The same warnings about P-blockers discussed earlier for enhanced physiologic tremor apply here. Because of P-blockers’ side effects, primidone is fast becoming the drug of choice. Again, the dosage must be individually adjusted. As little as 5 mg/day is useful for some, whereas others need nearly toxic dosages. For optimal response with either drug, start at a very low dosage with weekly increments to tolerance. Some patients respond to P-blockers and some to primidone. Combination therapy is rarely useful. Gabapentin has been beneficial for some patients. Dosages as low as 600 mg per day may be effective, but usually higher dosages are needed. Its low incidence of side effects makes it an attractive alternative. Those who do not respond to these drugs may benefit from methazolamide in dosages of 100 to 300 mg/day or nicardipine in dosages of 30 to 60 mg/day. Judicious use of botulinum toxin injection (as described later in this chapter) may be the treatment of choice for patients whose tremor does not respond to these agents. When pharmacotherapy fails, a patient may find relief from surgical ablation of the ventralis lateralis or ventral intermediate thalamic nucleus. Chronic stereotactic stimulation of the ventral intermediate nucleus or chronic cerebellar stimulation may also be useful in those who do not respond to drug therapy. Neuropathic Tremor
Neuropathic tremor is seen in a variety of acquired neuropathies. It is important to differentiate it from the essential tremor associated with hereditary sensorimotor neuropathy type I. The acquired neuropathies most likely to produce a tremor are chronic
Chapter 125 H Tremors
801
relapsing demyelinating polyneuropathy and immunoglobulin M (1gM)-associated paraproteinemic neuropathy. Causality is suggested by the fact that in a single patient, changes in the amplitude of the tremor vary directly with changes in the severity of the neuropathy. The tremor is generally irregular at a rate of 6 to 8 Hz. The EMG from antagonist muscles demonstrates bursts of varying amplitude and duration without a consistent pattern. The presence of the tremor is not related to the degree of weakness or sensory loss. Slowing in motor conduction velocity often is seen in neuropathic tremor, but the degree of slowing is not related to severity. The pathophysiology of these tremors is unclear, and there probably are multiple mechanisms involved in their genesis. One of these may be desynchronization of afferent volleys from muscle spindles and Golgi tendon organs. The demyelinative features of the neuropathy probably play an important role because in primarily axonal neuropathies (e.g., associated with alcohol, diabetes), tremor is absent or barely noticeable, whereas the tremor may appear during recovery from Guillain-Barre syndrome. Some patients may respond to propranolol or Mysoline, but therapy is best directed at the neuropathy.
minutes after assuming the standing posture and is abolished by walking. It involves mainly the lower extremity and trunk muscles, although some weight-bearing tasks in the upper extremities may produce tremor in susceptible people. Most patients suffering from this tremor have no other neurologic complaint, but there are reports of an association with essential tremor and painful cramp syndromes. One case associated with aqueductal stenosis and another with chronic relapsing demyelinating polyneuropathy have been reported. The upright posture itself is not responsible for the tremor; rather, it appears that the isometric muscle activity needed for weight-bearing is the trigger. Surface EMG recording shows synchronous bursts in antagonist muscles occurring at rates as high as 30 Hz in some patients and as low as 7 Hz in others. Some authors have proposed that the tremor is caused by impaired feedback from muscle spindles. However, its physiologic and pharmacologic underpinnings remain unknown. Primidone in the dosages cited earlier or clonazepam in daily dosages of 4 to 6 mg may improve some patients.
Writing Tremor
Also known as cerebellar outflow tremor, cerebellar tremor is seen in late cortical atrophy of the cerebellum and in lesions of the cerebellar outflow tract, such as occur in multiple sclerosis. It is different from the appendicular dysmetria and ataxia associated with hemispheric cerebellar lesions. The tremor is manifested as regular oscillations of the trunk or limbs while maintaining a posture. The axial and proximal limb muscles demonstrate an alternating pattern of EMG bursts at about 3 Hz. The tremor also affects goal-directed movement because as a limb approaches a target, the more distal muscles start to show the alternating bursts, and the tremor increases in amplitude. Patients show less tremor if they keep their eyes open and observe the limb during the task, a phenomenon called visual stabilization. The mechanism for the tremor is unknown; it appears to be unrelated to abnormalities of stretch reflex or proprioceptive input. Pharmacotherapy has yielded disappointing results. There has been some success using high dosages (600 to 1200 mg/day) of isoniazid hydrochloride. However, at these levels, liver toxicity is common. Carbamazepine has also been helpful for some patients. As in many other devastating tremors, stereotactic ablation of the ventral intermediate thalamic nucleus may be useful.
Any action tremor may affect penmanship, but some patients demonstrate a tremor predominantly during writing. The tremor is most often unilateral and shows no familial tendency. It may occur as an isolated symptom or accompany other tremors or focal dystonias. It has been dubbed primary writing tremor, but it seems that it is the pronated, slightly extended position of the wrist rather than the act of writing itself that produces the tremor. This tremor may also be triggered by eliciting stretch reflexes from muscles responsible for forearm pronation. Tremor recordings vary from patient to patient. In some patients, bursts of EMG activity at a rate of 4 to 6 Hz can be recorded from antagonist muscles. The pattern may be synchronous or alternating, and the bursts in a single recording may vary in amplitude and duration. In some cases, a single muscle shows tonic activity and its antagonist a pattern of bursts. All this suggests that this tremor has more in common with acquired dystonias, or the so-called occupational cramps, than with the tremors mentioned earlier. As is generally true of dystonias, its pathophysiology is unknown. Systemic therapy for this tremor relies mainly on the use of anticholinergic drugs in dosages described earlier under “Tremor at Rest.” Atropine and scopolamine in the usual cardiac dosages have been tried but have not produced encouraging results. P-Blockers, alcohol, levodopa, and neuroleptics are not useful. Biofeedback and other forms of therapeutic self-hypnosis have been used with varying success. These treatments are quickly giving way to intramuscular botulinum toxin injection. Upon identifymg the muscles most active in the tremor, minute amounts of the toxin are injected to produce selective weakness or paralysis of the offending muscles. The number of injections necessary depends as much on the severity of the tremor as on the skill of the administering physician. Orthostatic Tremor
Although the true incidence of orthostatic tremor is not known, it is much less common than other types of action tremor. It is seen primarily in older patients and occurs during the act of standing. The tremor appears after a latent period of several seconds or
Cerebellar Tremor
SUGGESTED READINGS Cardoso FEC, Jankovic J: Hereditary motor-sensory neuropathy and movement disorders. Muscle Nerve 16:904-910, 1993 Deep-Brain Stimulation for Parkinson’s Disease Study Group: Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med 345:956-963,2001 Elble RJ, Moody C, Higgins C: Primary writing tremor: a form of focal dystonia? Mov Disord 5:118-126, 1990 Fitzgerald PM, Jankovic J: Orthostatic tremor: an association with essential tremor. Mov Disord 6:60-64, 1991 Goetz CG, Horn SS: Treatment of tremor and dystonia. Neurol Clin 19:129-144, 2001 Hark GM, Lindberg M, Bergenheim AT Impact of thalamic deep brain stimulation on disability and health-related quality of life in patients with essential tremor. J Neurol Neurosurg Psychiatry 72:47-52, 2001 Louis E D Essential tremor. N Engl J Med 345:887-891, 2001 Matsumoto J, Morrow D, Kaufman K et ak Surgical therapy for tremor in multiple sclerosis: an evaluation of outcome measures. Neurology 57:1876-1882, 2001
802
Movement Disorders rn Non-Parkinsonian Movement Disorders
Munchau A, Schrag A, Chuang C et ak Arm tremor in cervical dystonia differs from essential tremor and can be classified by onset age and spread of symptoms. Brain 124:1765-1776, 2001 Walker FO, McCormick GM, Hunt VP: Isometric features of orthostatic tremor. Muscle Nerve 13:918-922, 1990
Wills AJ, Jenkins LH, Thompson PD et al: Red nuclear and cerebellar but no olivary activation associated with essential tremor: a positron emission tomography study. Ann Neurol 36636442, 1994 Zesiewicz TA, Hauser RA: Phenomenology and treatment of tremor disorders. Neurol Clin 19:651-680, 2001
126 Huntington’s Disease Walter 1. Koroshetz Huntington’sdisease is an autosomal dominant neurodegenerative disease that leads to marked atrophy of basal ganglia structures, the caudate, and putamen, as well as less marked atrophy of other brain nuclei. It is thought to be the most common inherited adult neurodegenerative disease, affecting 1 in 15,000 in the United States. The average age of onset is approximately 38 years old; much younger-onset cases and onset in older adults also occurs less commonly. The hallmark of the illness is an involuntary movement disorder, chorea. Some patients have little or no chorea and instead appear slow and rigid (i.e., with parkinsonian characteristics). The illness leads to death, with an average duration of symptoms of about 20 years. The gene that causes the disease has been identified. The Huntington mutation is an expanded trinucleotide (CAG), repeat that causes an excessively long polyglutamine stretch located in a novel protein called huntingh’n. How the mutation leads to the onset of a disorder of motor, emotional, and cognitive control in people who have matured normally until middle age is still a mystery. The gene discovery has made genetic diagnosis common, both in neurologically normal patients (presymptomatic testing) and in neurologically or psychiatrically impaired patients (diagnostic testing). Transgenic animal models of the disease provide researchers with powerful new tools to search for effective treatments. It is hoped that research will soon uncover the cause of the slow neuronal loss, which is stimulated by the mutation and underlies the tragic illness. CLINICAL MANlFESTATlONS
Huntington’s disease is characterized by progressive impairment of a patient’s cognitive, emotional, and motor control, which is accompanied by neuronal death in the central nervous system, primarily in the caudate and putamen of the basal ganglia. Primary sensory pathways do not appear to be affected. Cerebellar function is affected only in an atypical Huntington’s disease variant, with signs usually beginning in childhood. The psychological effects of the disease are magnified by the fact that it is autosomal dominantly inherited and that affected patients usually have witnessed the entire course of the disease in their parent by the time they begin to show signs. Older siblings may also be severely disabled or have already died. Because it is an autosomal dominant disorder, a thorough family history is essential to make the clinical diagnosis. Care is needed to avoid errors of incorrectly attributing any neurologic or psychiatric symptom to Huntington’s disease in the presence of a family history. A negative family history that is taken as absolute, without investigation, can also lead to errors in not diagnosing Huntington’s disease in an affected patient.
The disease progresses slowly and often in a pattern consisting of three phases. Early on, affected patients have difficulty maintaining their premorbid level of function at work, school, or home. Emotional disorders may be prominent, there is disability caused by poor motor control, and chorea is usually present. In this stage, patients can maintain their own activities of daily living. Toward the end of stage 1 the person loses the ability to remain employed or drive an automobile and becomes reliant on family or society for some level of support. In stage 2, dysarthria affects communication, and dysphagia may occur. Disordered motor control may lead to falls, chorea may be prominent, and mentation is dulled. Such patients must be supervised to avoid self-injury, prevent poor financial decisions, and even maintain adequate nutrition, housing, and cleanliness. In stage 3, dystonia and rigidity may set in, choreoathetosis may be continuous, and the person eventually becomes bedridden and unable to speak or swallow. The course of the disease progresses fairly linearly down the Boston Independence and Physical Disability Scales (Table 126-1). The Total Functional Capacity Score, which is presented in Table 126-2, is more sensitive to progression of the disease in stages 1 and 2. Presenting Signs and Symptoms
Patients with Huntington’s disease present with a variety of clinical syndromes. Most commonly, a person at risk for this disease begins to fall behind in performance at work or home in the fourth or fifth decade of life. Slowness in executing tasks, inflexibility, forgetfulness, poor judgment, and increased irritability may impair their usual level of ability. The patient may present with a history of recent change in the degree of difficulty of his or her job or recent job loss. Family members often report that a change in personality has occurred in the 3 to 5 years before clinical symptoms. Increased numbers of motor vehicle accidents may occur. Increased irritability is common; occasionally florid psychiatric disorders predominate for years before the motor signs of Huntington’s disease appear. Symptoms of a motor disorder in early-stage Huntington’s disease are not specific but are very suspicious if definite slow worsening occurs in a person with a known affected parent. The spouse may report that the affected person began to have sudden jerking movements during sleep over the past few years. These must be distinguished from the sleep-onset myoclonus that occurs in a normal person but is often incorrectly assumed to be a sign of Huntington’s disease in at-risk people. Clumsiness of fine finger movements is detected by some people (i.e., typists, musicians, and carpenters). A deterioration in baseline handwriting skills is common. Unexplained falls, dropping of objects, and a change in
802
Movement Disorders rn Non-Parkinsonian Movement Disorders
Munchau A, Schrag A, Chuang C et ak Arm tremor in cervical dystonia differs from essential tremor and can be classified by onset age and spread of symptoms. Brain 124:1765-1776, 2001 Walker FO, McCormick GM, Hunt VP: Isometric features of orthostatic tremor. Muscle Nerve 13:918-922, 1990
Wills AJ, Jenkins LH, Thompson PD et al: Red nuclear and cerebellar but no olivary activation associated with essential tremor: a positron emission tomography study. Ann Neurol 36636442, 1994 Zesiewicz TA, Hauser RA: Phenomenology and treatment of tremor disorders. Neurol Clin 19:651-680, 2001
126 Huntington’s Disease Walter 1. Koroshetz Huntington’sdisease is an autosomal dominant neurodegenerative disease that leads to marked atrophy of basal ganglia structures, the caudate, and putamen, as well as less marked atrophy of other brain nuclei. It is thought to be the most common inherited adult neurodegenerative disease, affecting 1 in 15,000 in the United States. The average age of onset is approximately 38 years old; much younger-onset cases and onset in older adults also occurs less commonly. The hallmark of the illness is an involuntary movement disorder, chorea. Some patients have little or no chorea and instead appear slow and rigid (i.e., with parkinsonian characteristics). The illness leads to death, with an average duration of symptoms of about 20 years. The gene that causes the disease has been identified. The Huntington mutation is an expanded trinucleotide (CAG), repeat that causes an excessively long polyglutamine stretch located in a novel protein called huntingh’n. How the mutation leads to the onset of a disorder of motor, emotional, and cognitive control in people who have matured normally until middle age is still a mystery. The gene discovery has made genetic diagnosis common, both in neurologically normal patients (presymptomatic testing) and in neurologically or psychiatrically impaired patients (diagnostic testing). Transgenic animal models of the disease provide researchers with powerful new tools to search for effective treatments. It is hoped that research will soon uncover the cause of the slow neuronal loss, which is stimulated by the mutation and underlies the tragic illness. CLINICAL MANlFESTATlONS
Huntington’s disease is characterized by progressive impairment of a patient’s cognitive, emotional, and motor control, which is accompanied by neuronal death in the central nervous system, primarily in the caudate and putamen of the basal ganglia. Primary sensory pathways do not appear to be affected. Cerebellar function is affected only in an atypical Huntington’s disease variant, with signs usually beginning in childhood. The psychological effects of the disease are magnified by the fact that it is autosomal dominantly inherited and that affected patients usually have witnessed the entire course of the disease in their parent by the time they begin to show signs. Older siblings may also be severely disabled or have already died. Because it is an autosomal dominant disorder, a thorough family history is essential to make the clinical diagnosis. Care is needed to avoid errors of incorrectly attributing any neurologic or psychiatric symptom to Huntington’s disease in the presence of a family history. A negative family history that is taken as absolute, without investigation, can also lead to errors in not diagnosing Huntington’s disease in an affected patient.
The disease progresses slowly and often in a pattern consisting of three phases. Early on, affected patients have difficulty maintaining their premorbid level of function at work, school, or home. Emotional disorders may be prominent, there is disability caused by poor motor control, and chorea is usually present. In this stage, patients can maintain their own activities of daily living. Toward the end of stage 1 the person loses the ability to remain employed or drive an automobile and becomes reliant on family or society for some level of support. In stage 2, dysarthria affects communication, and dysphagia may occur. Disordered motor control may lead to falls, chorea may be prominent, and mentation is dulled. Such patients must be supervised to avoid self-injury, prevent poor financial decisions, and even maintain adequate nutrition, housing, and cleanliness. In stage 3, dystonia and rigidity may set in, choreoathetosis may be continuous, and the person eventually becomes bedridden and unable to speak or swallow. The course of the disease progresses fairly linearly down the Boston Independence and Physical Disability Scales (Table 126-1). The Total Functional Capacity Score, which is presented in Table 126-2, is more sensitive to progression of the disease in stages 1 and 2. Presenting Signs and Symptoms
Patients with Huntington’s disease present with a variety of clinical syndromes. Most commonly, a person at risk for this disease begins to fall behind in performance at work or home in the fourth or fifth decade of life. Slowness in executing tasks, inflexibility, forgetfulness, poor judgment, and increased irritability may impair their usual level of ability. The patient may present with a history of recent change in the degree of difficulty of his or her job or recent job loss. Family members often report that a change in personality has occurred in the 3 to 5 years before clinical symptoms. Increased numbers of motor vehicle accidents may occur. Increased irritability is common; occasionally florid psychiatric disorders predominate for years before the motor signs of Huntington’s disease appear. Symptoms of a motor disorder in early-stage Huntington’s disease are not specific but are very suspicious if definite slow worsening occurs in a person with a known affected parent. The spouse may report that the affected person began to have sudden jerking movements during sleep over the past few years. These must be distinguished from the sleep-onset myoclonus that occurs in a normal person but is often incorrectly assumed to be a sign of Huntington’s disease in at-risk people. Clumsiness of fine finger movements is detected by some people (i.e., typists, musicians, and carpenters). A deterioration in baseline handwriting skills is common. Unexplained falls, dropping of objects, and a change in
Chapter 126 w
TMLE126-1. Boston Independence and Physical Disability Scales Boston Independence Scale
Boston Physical Disabilii Scale
100: No special care needed 090: No physical care needed if
100: Normal, no disease evident 090: Onset: minimal signs, slight
difficult tasks are involved
facial or extremity movement disorder 080: Normal daily activity with effort, gait disturbance, stumbling, slurred speech
080: Predisease level of employ-
ment changes or ends; cannot perform household chores to predisease level; may need help with finances 070: Self-care maintained for bathing, limited household duties (cooking and use of knives), driving terminates; unable to manage finances 060: Needs minor assistance for dressing, toileting, bathing; food must be cut for patient 050: 24-hour supenision appro-
priate; assistance needed for bathing, eating, toileting 040: Chronic care f a c i l i needed;
limited self-feeding, liquefied diet 030:Patient provides minimal assistance in own feeding, bathing, toileting 020: No speech, must be fed 010: Tube fed, total bed care
070: Limited activity, occasional
falls, oven chorea, less speech with dysarthria, occasional dysphagia 060: Can be left alone for short
period of time, several falls, can walk up to 1 block outside of home 050: Needs assistance in walking, limited ambulation at home, difficulty communicatingand swallowing 040:Limited a b i l i t o walk assisted; single-word utterances 030:Confined to wheelchair, unintelligible speech, frequent choking 020: Completely bedridden, anarthria 010: Fuced posture necessitating total care, gastrostomy, cathe terization
the usual pattern of walking or speaking are other common symptoms that may herald the onset of clinical Huntington’s disease. Because the mutation is inherited and patients are clearly normal during childhood and throughout early adulthood and only slowly develop the clinical syndrome in early to middle adulthood, there can be no true “onset” of illness. Huntington’s disease is inexorably progressive, although patients accumulate disability at various rates. Diagnosis usually is made when chorea without other cause becomes evident. However, studies of at-risk people and newly diagnosed patients reveal that even before chorea occurs, certain “soft signs” may appear. The speed of saccadic eye movements is slowed, and there may be an abnormal delay before the production of a saccadic eye movement to a command. Repetitive fine finger movements, repetitive tongue movements, or repetitive lingual pronunciations may be slow and clumsy. Patients may have difficulty learning a sequence of motor acts (Luria three-step test). Restless movements may occur that resemble normal repositioning movements but at increased frequency. Stereotyped “habit” movements may be more apparent, or small-amplitude flicks of the fingers may be seen while the patient holds hands outstretched or walks. Neuropsychological evaluation may reveal deficits in memory or in the ability to respond to changing instructions (changing sets). Clinical depression is common in the years just preceding or encompassing the time of clinical diagnosis. The suicide rate in this time period is markedly increased.
Huntington’s Disease
803
Chorea The combination of fluid or jerky, writhing, torsional movements in all extremities resembles a form of primitive dance, and the word chorea is from the Greek word meaning “to dance.” In the early stages of the illness, the movements often are quick flicks of the fingers or muscles about the mouth or ankles. One common variant in which the fingers are quickly extended resembles the motion of flicking the ashes off a cigarette. The movements in the face may resemble winking or quick, wry smiling movements. As indicated earlier, there is often an increased frequency and constancy of movements that are seen commonly in normal people and associated with restlessness. A small proportion of affected people never demonstrate chorea. In most affected patients, chorea is unsightly but not truly disabling. It can affect function in that patients may spill liquids, hit extremities against sharp or hot objects, or drop objects during a choreic movement. However, in some chorea becomes so pronounced (largeamplitude continuous writhing movements) that it interferes with all normal motor activity. Chorea is inhibited by neuroleptic agents and enhanced by dopamine agonists. Treatment with high or even moderate dosages of neuroleptic drugs is problematic because it may worsen the voluntary movement disorder in a dose-dependent fashion. As the disease progresses, the involuntary movements change in form. In some patients, the movements increase in amplitude and frequency so that the person is in constant motion while awake. The person may walk with grotesque contortions of both axial and appendicular musculature. As the illness progresses, some patients demonstrate a slowing of writhing movements to choreoathetosis. In the late stages of the illness, the predominant disorder is dystonia, a fixed, abnormal, usually twisted posture. Progression to rigidity and dystonia can be iatrogenically produced by treating chorea overaggressively with neuroleptic drugs.
Disordered Motor Control Major disability comes from the disordered voluntary motor disorder in Huntington’s disease. This aspect of the disease
TABLE 126-2. Total Functional Capacity Scale (Shoulson inventory) Occupation 0 =unable 1 =marginal work only 2 = reduced capacity for usual job 3 =normal Finances 0 = unable 1 =major assistance 2 =slight assistance 3 =normal Domestic chores 0 = unable 1 =impaired 2 = normal Activities of daily living 0 =total care 1 =gross tasks only 2 =minimal impairment 3 = normal Care level 0 =full-time skilled nursing 1 =home or chronic care 2 = home
004
Movement Disorders W
Non-Parkinsonian Movement Disorders
progresses until there is almost no ability to make goal-directed purposeful movements to the extent that swallowing, speaking, and even sitting are no longer possible. Huntington’s disease contains much of the bradykinesia found in Parkinson’s disease without the same rigidity or tremor but instead with overlying chorea. This is not surprising because both diseases cause a dysfunctional striatum. In the motor control sphere, the old teaching that Parkinson’s and Huntington’s diseases cause opposite nervous system effects is incorrect. In the early stages, the voluntary motor disorder is characterized by slowness and incoordination. There is usually trouble in making rhythmic movements or fast, repetitive, fine movements with the tongue or fingers. When patients are asked to tap the index finger to the thumb or tap the tongue to the top lip repetitively, the movements are made more slowly than normal, and there are occasional deviations from the desired pattern. Patients have a peculiar inability to regularly time fast tapping movements with the hand. A test that demands changing the motor program is very difficult. To test these patients, they are asked to tap out a sequence of three motor acts (tap thigh alternately with a fist, then the side of the hand, and then the palm of the hand, then repeat the sequence). A similar disability is seen when the patient is asked to tap the front and back surface of the dominant hand on the palm of the nondominant hand alternately (dysdiadochokinesia). A change in the pattern of speech occurs, and some family members consider this to be the first sign of the disease. An alteration in pronunciation and in the normal phrasing and timing of speech is likely to be what is noticed early. On examination, repetitive lingual sounds are pronounced poorly (i.e., “la, la, la, la, la”), whereas repetitive buccal sounds are performed better (i.e., “me, me, me, me, me”). Swallowing movements are also affected by the motor control disorder in Huntington’s disease. Swallowing difficulty often begins with trouble swallowing dry foods such as crackers, cookies, or dry cereals. Patients are unable to strip such food pieces from the pharynx and may inhale them instead. Next, thin liquids such as water and soda are trouble; this can sometimes be remedied by the use of a straw to deliver the fluid straight to the back of the mouth because the tongue coordination necessary to do so may not be present. Thicker liquids are easier to propel into the hypopharynx, and a custard consistency usually is the easiest to swallow, even in the later stages of the illness. Gait and posture are severely affected by the disease as it progresses. Gait may become wide based, but more characteristically the steps are irregular in both timing and placement of the feet. Because of the combination of gait disorder and slurred speech, patients are not uncommonly misdiagnosed as inebriated by law enforcement officials. Postural instability occurs over time, and affected patients cannot balance on one foot or walk tandem in a straight line. In the early or middle stage of the disease, they may exhibit retropulsion when given a light shove backward. Falling becomes a serious issue in the middle and later stages of the illness. A number of patients with Huntington’s disease sustain subdural hematomas or orthopedic injuries during falls. As the disease progresses into the later stages, all lose the ability to walk and even to maintain balance for the standing or upright sitting position. There is an apraxia, which affects functional movement in patients with Huntington’s disease. Occasionally a patient is misperceived as lazy or depressed because he or she is seen as not performing even the most simple tasks about the house. On examination, the patient may be unable to mimic the most basic hand postures, and it is clear that he or she cannot learn or
produce the movement necessary for activities of daily living. Because of slowness, incoordination, apraxia, and chorea, patients in the middle stage of Huntington’s disease lose the ability to write, use keys, button clothing, tie shoelaces, wash dishes, feed themselves without spilling food, and so forth. In the later stages, affected patients are totally dependent on others for feeding, clothing, and bathing because of the total lack of voluntary control of movement. Death caused by Huntington’s disease usually is triggered by aspiration pneumonia caused by pharyngeal dysfunction. Speech patterns change early in the illness, with slurring and poor modulation of volume and tone. As the illness progresses, dysarthria becomes more severe, and, in the later stages, speech becomes unintelligible. Patients with end-stage Huntington’s disease can do little more than moan or produce incoordinated vowel sounds. Swallowing dysfunction also occurs throughout the course of the illness. Choking spells usually do not occur until the later stages, although some patients have had occasional coughing or choking with swallowing in the early stages. As the disease progresses, the texture of food must be altered to allow effective swallowing. More time must be allotted to meals. Because swallowing usually is slower than other movements, it is important to come up with strategies to ensure that the mouth is emptied before more food is taken in. Thickening liquids and softening and moistening solid foods (pureed) usually is necessary as the disease progresses. Patients in later stages of Huntington’s disease need to be fed patiently by others. Pharyngeal dysfunction eventually becomes so severe that nutritional needs cannot be met orally in the late stage of the illness. Aspiration of oral contents occurs as a final event, leading to pneumonia. Reflexes usually are hyperactive; there may be clonus at the ankle. Tone is increased in the late stages of the illness coincident with dystonia, and tone is increased in the bradykinetic and rigid juvenile cases. In early-stage Huntington’s disease, the tone in an extremity can be normal until the examiner attempts to produce passive movement or the patient produces active movement in another extremity. The tone generally is greatly increased by these stimuli. Despite severe dementia, frontal lobe signs usually are not seen (grasp, suck, and rooting reflex). Vertical eye movements can be limited in end-stage disease. With middle- to late-stage disease, horizontal eye movements are linked to unsuppressible head turn or blinks. No deficits in pupillary reflexes, heating, visual acuity, visual fields, or primary sensation are apparent in Huntington’s disease. Muscular wasting is seen, but the cause is not clear. Cerebellar signs such as dysmetria and nystagmus are not usually seen. Autonomic abnormalities are not usually noted until later in this disease. Patients in its end stage become incontinent, usually associated with dementia. Some patients with Huntington’s disease have experienced unusual episodic sweating. In the late stages, we have seen occasional patients with recurrent high fevers, elevated creatine phosphokinase levels, and diaphoresis. A source of infection should be looked for in such cases but may not always be uncovered.
Psychiatric Disorders Depression is extremely common in patients with Huntington’s disease, and it may become apparent before the neurologic signs enable the clinical diagnosis. The suicide risk is increased in at-risk and affected patients. Depressed mood usually responds to antidepressants, but the response often is a partial one. Depression
Chapter 126
may occur in the context of a mixed psychiatric disorder, or there may be cycling of mania and depression. An unusual feature of some patients with Huntington’s disease is an overwhelming apathetic disorder, usually with a less pronounced dysthymic disorder. Patients often are poor at generating spontaneous, constructive activity. It is not uncommon for patients with Huntington’s disease to become extremely sedentary and spend most of the day in the house, either in bed or watching television. Some seem drawn to stay in bed and strongly oppose attempts to mobilize. With structure and guidance, a much more productive level of activity can be sustained longer into the illness. Distinguishing apathy from depression is difficult and often reduces to behavior resistant or responsive to antidepressants. A disorder of emotional control is common in patients with Huntington’s disease. This is often manifested by an increased level of irritability, with or without an underlying anxiety disorder. Angry outbursts in the home can be extremely disruptive and are one of the main causes for institutionalization of patients with Huntington’s disease. These outbursts often occur suddenly and without warning. They are usually short-lived (minutes), but their repercussions for other family members may be longer lasting, especially if they are associated with physical violence. The patient with Huntington’s disease may be contrite when confronted with the history but unable to alter the pattern of behavior. The trigger for emotional outbursts is not uncommonly a demand for assistance that is not met immediately or a request by the patient with Huntington’s disease that is not considered reasonable by a caregiver or family member. Occasionally, emotional dyscontrol is a manifestation of delusional thought or severe depression. We have seen some patients in whom episodes of emotional dyscontrol coincide with intense feelings of hunger occurring before a scheduled meal. Cigarette smoking also appears to be exceedingly common in people with Huntington’s disease, and the urge to smoke often is magnified to the extreme. Episodes of anger often occur in the context of some obstruction to smoking. In some very severe cases, hitting out or an angry outburst appears almost reflexive and triggered by most interactions. More commonly it is related to obstruction of the affected patient’s obsessive, perseverative behavior. One must inquire into the safety of children or older adults living in the home with a patient who suffers from emotional dyscontrol. A true psychotic disorder with hallucinations can occur, but it is rare as part of Huntington’s disease. Paranoia, delusional thought, bizarre behavior, and anxiety disorders occur more commonly in combination with disordered emotional control. Obsessive-compulsive behavior is very common in patients with Huntington’s disease. Patients may become fixated on a specific activity, such as smoking, watching television, visiting a specific place, warding off a specific person, continuing to drive, exercising, or returning to a broken home. Inflexibility and the inability to put off gratification combined with this perseverative thought can create major management trouble in the home or institution. Fear of being alone or removed from the family, fear of bathing, fear of leaving the house, fear of heights, and fear of choking are not uncommon and may complicate patient care.
Cognithre Disorders In Huntington’s disease, there is early memory impairment. This progresses over time and is accompanied by impaired attention, distractibility, and inflexibility. Previous mental tasks may take much longer and may be accompanied by more frequent errors.
Huntington‘s Disease
801
Reasoning ability, simple arithmetic processes, temporal ordering, and abstract thought all become severely impaired. Patients do most poorly on tests that entail a change in strategy. They have trouble with tasks that entail visual spatial integration of input, which may contribute to their driving disability. They have difficulty in generating and executing plans necessary to accomplish even simple goals at work or in the home. The dementia of Huntington’s disease is a subcortical dementia. Unlike Alzheimer’s disease, the memory disorder does not progress to amnesia. It appears that new memories can be made and old memories recalled, but this occurs less often as the disease progresses. There is eventually a poverty of thought; only a small proportion of events can be recalled. Perseveration and impersistence are prominent as the disease progresses. Patients with Huntington’s disease have severe impairment of motor skill learning. We have found a special inability for such patients to learn sequence information. In end-stage disease, either very limited and primitive communication or no apparent communication with the patient is possible. There is not a true aphasia, although speech production can diminish to the point that only a rare vocalization occurs. This can progress to mutism and lack of ability to follow even the simplest command. The condition most resembles severe abulia because early on coaxing is needed to obtain responses, and responses can occur in a specific context.
Sleep Disorders Patients may complain of inability to sleep or daytime drowsiness. Sleep studies often demonstrate abnormal sleep architecture, with frequent awakenings associated with motor jerks. Some patients improve with the use of clonazepam at bedtime. Amitriptyline at bedtime may also be helpful. Nutritionaland Metabolic Disorders
Many physicians caring for patients with Huntington’s disease suspect that there is a hypermetabolic disorder. Weight loss is common and can be extreme and rapid. Institutionalized patients who are sedentary except for their chorea and dystonia can need a huge caloric intake (3000 to 4000 cal/day) to maintain their body weight. It is our impression that patients do worse clinically as their weight decreases and sometimes improve as they gain weight. In our study of factors associated with slow progression of illness, with the exception of age at onset, weight at the time of diagnosis was the most statistically significantly associated variable. No particular food group is known to be of special benefit. Highcalorie nutritional supplements often are necessary to maintain body weight. Clinical Variants
In most cases, symptoms and signs of Huntington’s disease occur as outlined earlier, with soft signs and chorea first becoming manifest around age 40. The disease progresses over 20 years. The Boston Independence and Physical Disability Scales (Table 126-1) provide a means to chart the progression of the disease in an almost linear fashion from onset to end-stage disease. However, some patients deviate significantlyfrom the more common clinical course. Juvenile cases of Huntington’s disease occur uncommonly, and they are usually inherited from an affected father or from a mother who was also affected as a juvenile. The genetic cause of this
806
Movement Disorders
w Non-Parkinsonian Movement Disorders
paternal sex effect is discussed later in this chapter. Juvenile disease often presents as an akinetic or rigid syndrome without chorea. The saccadic eye movement velocity usually is very slow. Myoclonic tremor is common. Seizures may occur. Patients with juvenile Huntington’s disease often present with failing grades and a deterioration in their coordination. Their disease tends to progress more rapidly, and our data suggest that the rate of progression is closely associated with onset age. People without signs of Huntington’s disease until their seventh or eighth decade usually have a very slow progression of disability. They often present with chorea without dementia and often are misdiagnosed as suffering from senile chorea. Unfortunately, the transmission of the HD gene is associated with “anticipation” when transmitted through the father. The children of a father with late-onset Huntington’s disease can develop signs of the illness much earlier than their parents; this difference usually is associated with inheritance of a larger CAG repeat length in the child. This results from the instability of the mutation in spermatogenesis, where tremendous variation of CAG repeat length occurs (Duayao et al. 1993). In some patients, severe, disabling psychiatric disorders may cause disability years to decades before physical signs of the disease become evident.
nucleus. There is a fine structure to the caudate and putamen neural architecture, which also exhibits region-specific changes as the disease progresses. The pathologic features of Huntington’s disease have been mimicked to some degree by animal model studies using toxins. Intrastriatal injection of chemicals that activate the N-methyl+aspartate type of glutamate receptor in the brain cause degeneration of spiny neurons in animals and selective sparing of the diaphorase-staining aspiny neurons. More interestingly, chemicals that block mitochondrial function also lead to the pattern of neuronal death seen in the brain of a patient with Huntington’s disease. In addition, selective striatal damage is seen when these chemicals are administered systemically. There is also a described clinical syndrome in humans who have accidentally ingested one such mitochondrial inhibitor, 3-nitropropionic acid, which is characterized by striatal damage and dystonia. These observations have led to speculation that a mismatch between the energy demand caused by glutamate neurotransmission and the energy supply, as determined by mitochondrial function, leads to neuronal death, preferentially in the striatum and especially in spiny neurons. In further support of this theory, it has been found that the brain lactic acid levels are increased by excessive glutamate neurotransmission and by mitochondrial failure. Most importantly, brain lactate levels have been found to be elevated in patients with Huntington’s disease.
NEUROIMAGING FEATURES There is progressive atrophy of the caudate and putamen in patients with Huntington’s disease. Pathologic and morphometric imaging studies have shown that the degree of caudate atrophy is proportional to the affected person’s CAG repeat length divided by age (Penney and Rosas). The caudate nucleus normally protrudes into the ventricle so that atrophy is easily observed as an increase in the width of the lateral ventricle. There is loss of the usual convexity of the lateral wall of the ventricle, caused by caudate atrophy, leading to the so-called boxcar ventricular shape on computed tomography. Generalized brain atrophy is commonly seen along with caudate atrophy in the later stages of the illness. In patients with late onset, the caudate atrophy often is considered proportional to the cortical atrophy, and the diagnosis is not apparent by imaging alone. In juvenile Huntington’s disease, there may be an increased T2-weighted signal in the caudate on magnetic resonance imaging.
PATHOLOGIC FEATURES AND CLUES TO PATHOGENESIS The brain weight in end-stage Huntington’s disease is greatly reduced, but the cerebellar weight often is normal. The caudate in end-stage disease is severely atrophic and may consist only of a tissue paper-thin layer of glial cells with occasional neurons intermixed. The progression of the clinical signs of the disease appears to correlate with the pathologic grading of the degree of caudate atrophy. Interestingly, from a neurobiologic viewpoint, the neuronal death that occurs in Huntington’s disease is cell-type specific. In the atrophic caudate, interneurons that stain for nicotinamide adenine dinucleotide phosphate diaphorase and somatostatin are preferentially spared. The spiny neurons, which receive glutamatergic afferents from cortex and dopaminergic afferents from nigra and send GABAergic efferents to the pallidum are preferentially affected. There is also a gradient of cell death that occurs. The wave of cell death as the disease progresses seems to march from dorsal to ventral and medial to lateral in the caudate
MOLECULAR GENETICS The gene mutation that causes Huntington’s disease was identified in 1993. With the use of polymorphic DNA markers and linkage analysis in multiple large pedigrees, the gene was localized to the short arm of chromosome 4 in 1983. It was the first case of location of a disease gene based on DNA analysis of affected families, so-called reverse genetics. The HD mutation is an expansion of a trinucleotide repeat (CAG),, which codes for a polyglutamine stretch of amino acids in a novel protein. In unaffected people, the HD gene can contain up to 33 (CAG) repeats; the average number of repeats in this gene in the normal population is approximately 22. In people with Huntington’s disease, there are more than 38 (CAG) repeats in the HD gene that was inherited from an affected parent. People with Huntington’s disease usually also have a normal HD gene allele with fewer than 33 (CAG) repeats. The discovery of the gene mutation led to the explanation of a number of puzzling issues in the genetics of Huntington’s disease. Patients with juvenile Huntington’s disease were found to have inherited exceedingly long (CAG), repeats. Whereas most patients with Huntington’s disease have an allele with 40 to 55 (CAG) repeats, patients with the juvenile form have more than 60 and as many as 80 (CAG) repeats in their HD gene. As discussed earlier, patients with juvenile Huntington’s disease usually inherited the disease from an affected father. It was found that the length of the expanded (CAG), repeat could further expand in father-to-child transmissions. Indeed, the (CAG), length was fairly constant in all tissues except in the sperm, where it was found to be unstable. Sperm from affected men contained a wide variety of (CAG), repeat numbers. It is thought that fertilization by a sperm with a very high (CAG), repeat length in the HD gene gives rise to an offspring with juvenile Huntington’s disease. With the exception of the juvenile cases [(CAG), greater than 601, the actual (CAG), repeat length in patients with Huntington’s disease has little or no predictive value.
Chapter 126
Are there new HD mutations? We and others have followed individuals and families in whom a person with a clinical syndrome identical to Huntington’s disease was found in the absence of a family history of affected parents. We wondered whether these cases represented new mutations or manifestations of another disease. After the discovery of the HD mutation, we found that the suspected people did have the HD gene. More interestingly,family members who were elderly and not affected by Huntington’s disease had (CAG), repeats in the intermediate range (33 to 38), more than those found in the general population but less than those found in people with the disease. The appearance of “de novo” cases was explained by expansion of an HD allele in the intermediate (CAG), zone into the HD gene range (more than 38) during transmission from father to child. NEUROBIOLOGY OF THE HUNTINGTON’S DISEASE PROTEIN It is expected that a great deal will be learned about the pathogenesis of Huntington’s disease from studies of the H D mutation. It is hoped that the development of transgenic mouse strains containing the HD mutation will provide a faithful model of the disease to develop strategies aimed at preventing the progression of neuronal death. Homozygous knockout of the H D gene is fatal in a transgenic mouse model. Transgenic mouse models with expanded CAG in the huntinghn gene develop progressive neurologic and neuropathologic changes that vary with the specifics of the model. Indeed, even a fly model has been developed in which expanded CAG repeats in the huntingtin gene are associated with degeneration of the light-gathering apparatus, the rhabdomere. A uniform feature of the mouse models has been the finding of cellular and nuclear inclusions composed of the mutant huntingtin protein. This finding in the mouse led investigators to search for and find identical inclusions in humans with HD. Similar inclusions have been found in other CAG repeat disorders. Their role in neurodegeneration (i.e., whether they represent a cause or effect) is not known. A variety of molecular abnormalities have been isolated in the mouse models, including activation of caspase enzymes involved in programmed cell death, activation of the proteolytic enzyme calpain, and decreased production of the neurotrophin brainderived neurotrophic factor (BDNF). A major discovery has been the finding of altered gene transcription caused by mutant huntingh’n’s expanded polyglutamine repeat. This alteration seems to preferentially affect the genes regulated by a specific transcription factor, the SP-1 transcription factor. The expanded polyglutamine repeat in the huntingtin protein leads to a gain of some destructive function. This probably occurs because the abnormally long polyglutamine stretch in huntinghn binds to and alters the function of a normal protein or proteins. If a central molecular disorder can be identified, then agents may be designed to ameliorate the action of the mutant hunh’ngtin. Highthroughput screens, which check hundreds of thousands of compounds for their ability to alter one specific action or another of the mutant huntingth, are already up and running. Promising compounds will be identified that can then be tested in mouse models of Huntington’s disease for their ability to ameliorate neurologic deterioration and death. A number of assumptions still underlie any one strategy’s ability to bring a successful agent to patients, but the general method seems promising with persistent effort.
Huntington’s Disease
807
The HD gene messenger RNA and protein are not confined to nervous tissue but have been found in all tissues. HD gene message and protein are also found in all brain regions, in brain tissue from people affected with the illness, and in brain tissue from normal subjects. There does not seem to be a differential localization of the messenger RNA or the protein to the striatum. This suggests that it may be possible to follow the molecular pathology of the mutant huntingtin protein in a nonneural tissue such as skin or white blood cells. GENETIC TESTING Presymptomatic testing for Huntington’s disease became available with the use of linkage analysis in appropriate families in 1983. The discovery of the gene mutation has simplified the genetic diagnosis, and it is now available in a variety of clinical laboratories. Because of the absence of a treatment that could prevent or slow down progression of the illness, there is no health benefit to early diagnosis. Many people want to know their gene status to plan their careers, families, and finances. However, because of the tragic nature of the illness and the occurrence in loved ones, many people live in constant fear of inheriting the illness. The emotional stress of living at risk can motivate people to seek presymptomatic testing. A favorable outcome can be a great relief, but there is generally a 50% chance that the result will be unfavorable. The stress of living with the knowledge that one has the HD gene can be much more severe than that of living with a 50% risk. During genetic counseling, many patients (30% to 50%) realize that the stress of living at risk is preferable to the stress of learning about an unfavorable gene status and drop out of testing. For this reason, it is recommended that presymptomatic testing be performed with careful counseling and with some delay between the request for testing and the actual DNA analysis. This allows the person at risk to weigh carefully the potential personal effects of knowing that they will surely inherit the disease that had previously disabled their parent, siblings, or other relatives. Because of the high prevalence of depression in the years preceding diagnosis, it is also considered wise to screen patients coming for genetic testing for depressive disorder and especially suicidality because the stress of an unfavorable test result in the context of a uncontrolled depressive disorder may be tragic. TREATMENT No treatment is known to slow the progression of the neuronal degeneration in Huntington’s disease. Medical treatment is tailored to specific issues that arise and affect the patient’s functional level. A number of experimental therapies have been tried in affected individuals. CARE-HD Study
In a National Institute of Neurologic Disease and Stroke (N1NDS)funded, randomized, double-blind study the Huntington’s Disease Study Group (HDSG) evaluated the ability of two agents, remacemide and coenzyme QlO (CoQlO), to slow progression of Huntington’s disease. Remacemide was chosen because it was an investigational N-methyl D-aspartate receptor blocker available in an oral form. CoQlO was chosen because it is a chemical active in mitochondrial electron transport and a free radical scavenger. CoQlO in dosages of 360 mg/day was shown to partially reverse the elevated brain lactate observed in patients with Huntington’s
808
Movement Disorders H Non-Parkinsonian Movement Disorders
disease by magnetic resonance spectroscopy. Since the Coenzyme Qlo and Remacemide in Huntington’s Disease (CARE-HD) study design and execution, both CoQ 10 and remacemide were found to extend survival in transgenic HD mice. The CAFE-HD study was carried out using a 2 x 2 factorial design with one quarter of the mild to moderately affected patients in the placebo group, one quarter in the CoQlO alone group, one quarter in the remacemide alone group, and one quarter receiving both agents. Three functional scales were used to evaluate the study population of 325 affected patients over a 30-month period along with a variety of neuropsychological and motor tests. Remacemide had a minimal affect on reducing chorea scales, but loss of function occurred at the identical rate in those taking remacemide and those not on remacemide. In those treated with 600 mglday of CoQ10, deterioration also began at the identical rate as seen in those not on CoQ10. However, after 6 to 12 months there was a trend toward slowing of progression of disease in the CoQlO treated group on all three of the functional scales. This decrease of 15% to 20% in decline over 30 months did not reach statistical significance on the primary endpoint of the study, the total functional capacity scale (TFC; P = .15). Slowing of progression was statistically significant on the functional assessment scale ( P = .05), and the P value was .06 on the independence scale. No significant side effects of coQl0 were noted. Some have interpreted this as a negative study for both remacemide and coQ10. Others have been more convinced that the coQ10-treated group progressed identically with the noncoQl0 group over the first two or three evaluation periods, and then the groups began to diverge in their rate or decline, as might be expected with a neuroprotective agent (Fig. 126-1). The consistency of the differences seen on all three functional scales makes noise from the measurement devices an unlikely explanation of the difference. However, it remains possible that noise in the randomization could account for the difference, with more slow progressors assigned to the coQlO group by chance. Officially the HDSG interpreted this as the first study to show a trend toward benefit of a particular treatment in Huntington’s disease. There has been very little enthusiasm to pursue this 15% to 20% slowing of decline caused by coQl0 with another study. Instead the consensus has been to test another treatment coming from the transgenic animal studies that might show a greater benefit. The availability of transgenic mouse and even fly models of Huntington’s disease offers the opportunity for investigators to test a large number of compounds for their ability to delay neurologic deterioration or death. Treatment with unsaturated fatty acids, minocycline to inhibit caspase, creatine supplementation to improve cellular energy stores, n-butyric acid to inhibit histone deacetylase, and cystearnine inhibition of transglutaminase are other strategies in small clinical trials or under consideration.
Depression Depressive symptoms are common in patients with Huntington’s disease. They may be tied to despair arising from situational issues such as declining function in the workplace, inadequate supports in the home, financial difficulties, and social isolation. Psychological counseling and guidance in managing the disability that comes with this disease can cause remarkable change. Maintenance of structured activities for the affected patient, either at home, through local Huntington’s disease societies, in long-term care institutions, or in day care programs often is very helpful in helping the affected person to maintain a sense of self-worth.
CHANGE IN TOTAL FUNCTIONAL CAPACITY SCALE IN CARE-HD
A 0-0.5 -1 -1.5 -2 -2.5 -
-1
I
I
I
I
I
I
I
I
3
7
11
15
19
23
27
31
Months
DECLINE IN FUNCTIONAL ASSESSMENT SCALE IN CARE-HD
0-0.5 -1 -1.5 -2 -2.5 -3 -3.5 -4 -4.5
’
I
I
I
I
I
I
I
I
I
-1
3
7
11
15
19
23
27
31
Months FIG. 126-1. (A) Change in total functional capacity scale in CARE-HD. (B) Decline in functional assessment scale in CARE-HD.
Antidepressant medications can be of great help in those with a serious mood disorder. Tricyclic antidepressants (amitriptyline, imipramine, and nortriptyline) and serotonergic agents (fluoxetine or sertraline) have been used most commonly. Initially, low dosages are prescribed and changes in dosage made at 3-week intervals until depression responds or toxicity develops. Amitriptyline before bedtime is also useful in some patients for their sleep disorder. Unlike patients with Alzheimer’s or Parkinson’s disease, patients with Huntington’s disease do not have increased sensitivity to the anticholinergic side effects of the tricyclics. Fluoxetine can suppress appetite, so weight should be carefully monitored. The tricyclics may also be useful because they tend to stimulate appetite. Occasional patients respond poorly to all attempts to treat their severe depression. In many cases, a partial improvement occurs, but some chronic dysthymic disorder persists for decades. In occasional patients with severe incapacitating depression, monoamine oxidase inhibitors or electroshock therapy has been successful. Depressed patients with Huntington’s disease may also suffer from emotional dyscontrol disorders. Suicide is not rare, and patients should be questioned about suicidal intent. In patients with a history of suicidal thought or with impulsive behavior, care should be taken to limit the amount of antidepressant and other
Chapter 126
medications prescribed at one time. When appropriate, a family member or caretaker should administer the medications.
Chorea does decrease in frequency, speed, and amplitude with dopamine blocking agents but often at the price of increased incoordination, dystonia, and bradykinesia. In many cases, chorea is overmedicated with neuroleptic drugs, to the patient’s disadvantage. It is therefore important to determine whether treatment is leading to a functional improvement, as opposed to a cosmetic improvement, in chorea at the cost of decreasing motor function. In general, haloperidol dosages greater than 5 mg/day are met with worsening motor function, although exceptions are common. In some patients, benzodiazepines such as clonazepam are helpful. Emdonal Dyscontrol Management of the emotional outbursts is perhaps the most difficult and important task for the caregiver. Sudden verbal or physical abuse of self or others is the most common reason for institutionalization of patients with Huntington’s disease. Patients should first be evaluated for those events in the environments that trigger the outbursts. Common-sense but creative changes such as adjustments in the time of feeding if outbursts are triggered by hunger, a relaxation strategy when anxiety occurs, and setting schedules and safe havens for smoking, can be very helpful. In some, there is an underlying depression or mania, and treatment with antidepressants, carbamazepine, valproate, or lithium is helpful. In some, there is a chronic sleep disorder, and irritability is related to sleep deprivation and improves with more restful sleep. Clonazepam, carbamazepine, and valproate may be helpful in limiting the level of irritability that underlies the emotional dyscontrol. Some patients are inappropriately fixated on specific concerns or demands. These are often the most difficult to manage; a trial of antidepressants that are useful in treating obsessive-compulsive disorder (fluoxetine or clomipramine) can be of some help. In some instances, a delusional thought disorder underlies the outbursts, and this may not always be apparent because of the patient’s communicative disability. Neuroleptic agents such as haloperidol and thioridazine (more sedating) are effective in some instances, but their psychiatric benefits are balanced by their tendency to cause increased bradykinesia and rigidity. The motor control side effects of the neuroleptic medications tend to increase as the disease progresses. Quetiapine and clozapine are the most useful agents because they are potent antipsychotic agents with minimal extrapyramidal side effects. Quetiapine can be especially helpful in managing the emotional dyscontrol of Huntington’s d’isease. In difficult-to-control patients, often a combination of medications is used. In addition to antidepressants and atypical neuroleptics, valproate or carbamazepine should be tried in an attempt to level mood; high-dose propranolol and lithium can be effective in some severe dyscontrol disorders. Motor Control Disorder
No medical treatment is known to have a major effect on this very disabling aspect of the disease. Emphasis should be placed maintaining safe ambulation and swallowing as long as possible. Physical therapy and conditioning exercises can improve a patient’s safety and function. Some patients are thrown off balance
Huntington‘s Disease
809
by their chorea, and a very small dosage of haloperidol may decrease the rate of falling. However, haloperidol worsens the postural stability, so it also increases the rate of falling in some. In some rare patients with a parkinsonian variant of Huntington’s disease, a small dosage of a dopamine agonist is helpful. Alterations in diet are necessary to prevent aspiration, with a soft, thick, moist substance being the most easily swallowed.
CONCLUSION With discovery of the gene mutation and development of transgenic animal models of the disease, there is new hope that scientific and clinical research will offer promising therapies based on new knowledge about the pathogenesis and effects of the gene mutation in Huntington’s disease. At present, the families and patients afflicted by Huntington’s disease often live a life that is very different from that of the average American. There is a great need for understanding and knowledgeable physicians, social workers, genetic counselors, physical therapists, and other care providers to help affected patients maintain their self-worth and dignity throughout neurodegeneration. SUGGESTED READINGS
Bittenbender JB, Quadvasel F A Rigid and akinetic forms of Huntington’s chorea. Arch Neurol 7:275, 1962 Duayao M, Ambrose C, Myers R et al: Trinucleotide repeat length instability and age of onset in Huntington’s disease. Nat Genet 4387-392, 1993 Dunah AW, Jeong H, Griffin A et al: Spl and TAFII130 transcriptional activity disrupted in early Huntington’s disease. Science 296(5576): 2238-2243, 2002 Ferrante RJ, Andreassen OA, Dedeoglu A et ak Therapeutic effects of coenzyme QlO and remacemide in transgenic mouse models of Huntington’s disease. J Neurosci 22(5):1592-1599, 2002 Gervais FG, Singaraja R, Xanthoudakis S et al: Recruitment and activation of caspase-8 by the huntinghn-interacting protein Hip-1 and a novel partner Hippi. Nat Cell Biol 4(2):95-105, 2002 Gusella JF, Wexler NS, Conneally PM et ak A polymorphic DNA marker genetically linked to HD. Nature 306234, 1983 Haydon MR Huntington’s Chorea. Springer-Verlag, New York, 1981 Hersch S, JonesR, Koroshetz W, Quaid K The neurogenetics genie: testing for the Huntington’s disease mutation. Neurology 44:69-73, 1994 Huntington G On chorea. Med Surg Rep 26317-321, 1872 Huntington’s Disease Collaborative Research Group: A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell 72:971-983, 1993 Huntington’s Study Group: A randomized, placebo-controlled trial of Coenzyme Qloand Remacemide in Huntington’s Disease (CARE-HD). Neurology 57:397404, 2001 Myers RH, MacDonald M, Koroshetz W et ak De novo expansion of a (CAG), repeat in sporadic Huntington’s disease. Nat Genet 5:168-173, 1993
Myers RH, Vonsattel JP, Stevens TJ et ak Clinical and neuropathologic assessment of severity in HD. Neurology 38:341-347, 1988 Nasir J, Floresco S , OKusky JR et ak Targeted disruption of the Huntington’s disease gene results in embryonic lethality and behavioural and morphological changes in heterozygotes. Cell 81:811, 1995 Rosas H, Koroshetz WJ: Huntington’s disease. In Choi DW, Marcoux F (eds): Handbook of Experimental Pharmacology: CNS Protection. Springer Verlag, Heidelberg, 2002 Rosenblatt A, Ranen NG, Nance MA, Paulsen JS: A Physician’s Guide to the Management of Huntington’s Disease. 2nd Ed. Huntington’s Disease Society of America, New York, 1999 Young AB, Shoulson I, Penney JB et al: Huntington’s disease in Venezuela: neurological features and functional decline. Neurology 36244-249, 1986
810
Movement Disorders
Non-Parkinsonian Movement Disorders
127 Tardive Dyskinesia and Other Drug-Related
Movement Disorders Edison Miyawaki
TD is a clinically diverse syndrome in which choreatic, athetoid, dystonic, or other abnormal involuntary movements manifest late in the course of neuroleptic treatment. Research definitions cite a minimum of 3 months’ exposure to a neuroleptic, persistence of involuntary movements 1 month after stopping the offending drug, and exclusion of other identifiable causes. In clinical practice, however, dyskinesias may appear after a shorter time on the medications and may persist even after very brief exposure. Reports from the preneuroleptic era (e.g., Kraeplin in 1919 or Leonhard in the 1930s) described various strange, adventitious movements in psychotic patients. These presumably sporadic dyskinesias, as well as cases of senile chorea in people without psychiatric illness, have raised questions about the direct causeand-effect relationship between neuroleptics and tardive syndromes. Over time, however, it has become clear that TD is a distinct, if heterogeneous, clinical syndrome.
in and out of the mouth. Not all facial movements during neuroleptic treatment represent TD: Perioral tremor (rabbit syndrome) is understood as a sign of drug-induced parkinsonism, and orofacial dyskinesias may be seen in older, edentulous patients without history of neuroleptic use. Involuntary movements of the proximal limbs and trunk in TD are also common and may be of such large amplitude and high velocity as to suggest ballismus. Some cases reach bizarre proportions, as in “copulatory” pelvic thrusting. Distal movements also occur, including “air guitar” fingers, foot tapping, and extension of the great toe. Choreoathetosis is the term applied to many of these manifestations, but there is an additional, monotonously repetitive quality in TD that is characteristic. Terms such as tardive stereotypy and rhythmic chorea have been applied as a consequence. As with other movement disorders, the involuntary movements in TD worsen with emotional stress, diminish with sedation, and disappear with sleep. Dystonia may accompany stereotypic or choreoathetoid movements in TD. In some cases, the sustained abnormal postures of the limbs, head, neck, or trunk may be the dominating feature, and some have thought that tardive dystonia is a separate syndrome with predilection for younger age groups. Mean age of onset is 40 according to the literature, but all ages are at risk. Older patients may be predisposed to focal dystonias, particularly of the head and neck. Torticollis, retrocollis, oromandibular dystonia, and truncal dystonia are characteristic. Striking lateroflexion and backward twisting of the trunk on the waist (called Pisa syndrome) has been observed both acutely and in tardive fashion. The dystonias often are the most debilitating aspects in TD: Morbidity results from problems in gait, dystonia-induced rib fractures, eating-induced dystonias, opisthotonic posture (severe arching of the back and retrocollis), and other disabilities. Additional tardive syndromes have been described. Akathisia, a restlessness partially relieved by volitional activity, is a well-known acute effect of neuroleptics, but it has also been observed as a late effect. Recurrent oculogyric crises can occur after discontinuation of long-term neuroleptic treatment. Various reports of respiratory dyskinesia underscore the idea that any muscle group under voluntary control can be affected in TD: Periodic tachypnea, other irregular respirations, grunting, and dysphagia have all been described. Rarely, tremor can be a tardive phenomenon. Although typically seen in drug-induced parkinsonism, tremor can worsen upon withdrawal of the offending drug and may respond to dopamine-depleting agents. Tardive myoclonus has also been reported.
Phenomenology
Natural History and Epidemiology
The most common signs involve orofacial and lingual movements. Onset is insidious, and early features are restless tongue movements, patterned facial movements resembling tics, and increased eyeblink frequency (blepharospasm). Later signs include “vacuous” chewing movements, lip smacking, and tongue movements
TD is a variable disease, but a wealth of data suggest that its natural history can be affected by prudent neuroleptic management. TD can remit when neuroleptics are discontinued promptly upon diagnosis, or TD can attenuate with reductions in neuroleptic dosage, often a more feasible alternative in the clinical setting.
A number of major drug-related movement disorders are associated with the use of the so-called typical antipsychotics. The major mechanism of action of these traditional neuroleptics (drugs that produce effects on the nervous system) is dopamine receptor antagonism. Through the 1990s, however, atypical antipsychotics were prescribed increasingly in neurology and psychiatry. These newer neuroleptics have two aspects that make them atypical: They are mixed dopamine and serotonin receptor antagonists, and they result in fewer acute and late extrapyramidal effects. The 1990s also saw the ascendency of serotonin reuptake inhibitors for treating depression and other disorders, and reports have surfaced about various movement disorders associated with their use. The atypical antipsychotics and serotonergic antidepressants are changing the landscape of the major drug-related movement disorders. New cases of tardive dyskinesia and other traditional, neuroleptic-induced syndromes may have become less common, but they have not disappeared, and other interests have emerged. Also in the 1990s, a large body of work addressed basal ganglia pathways whose dysregulation may be responsible for a variety of drug-associated phenomena. Attention has focused particularly on levodopa-induced dyskinesia in Parkinson’s disease, but the implications are wide ranging. This chapter addresses classic drug-induced syndromes and incorporates a number of nonneuroleptic toxicities into that discussion; it ends an overview of basal ganglia pathophysiology as it relates to drug effects.
TARDIVE DYSKINESIA (TD)
Chapter 127
In long-term studies, the likelihood of clinical improvement in TD correlates with duration of time off drug or, alternatively, the length of follow-up. Studies examining outcome after more than 5 years show the greatest numbers with clinical improvement. Despite these optimistic views, some cases of TD persist indefinitely and can worsen over time. In the 1980s, it was generally agreed that prevalence of TD was on the order of 20% among psychiatric patients. Gardos and Cole estimated that the risk of developing TD for a schizophrenic patient treated with neuroleptics for 1 continuous year was approximately 5%. Kane et al. have quoted a cumulative incidence of 20% after 4 years of treatment (roughly 5% per year, in agreement with Gardos and Cole). More recently, attention has shifted to questions about the likelihood of developing TD during treatment with one of four FDA-approved atypical antipsychotics: clozapine, risperidone, olanzapine, and quetiapine. Kane followed 28 patients who had received clozapine for at least 1 year. Two patients, both of whom had previously taken typical neuroleptics, appeared to develop mild TD on clozapine. A prospective study of 122 risperidone- and haloperidol-treated older adults (61 in each group) concluded that the risk of TD was significantly less on risperidone; life table analysis was used based on a %month period of observation. In a large, double-blind, prospective study comparing 1 year of olanzapine treatment with haloperidol treatment, TD risk in the olanzapine group was one tenth that of the haloperidol group, and it was estimated that the annual risk of TD during olanzapine treatment was less than 1%. A case report of TD during quetiapine treatment has been published, but systematic data are not available at this time. In sum, TD can still occur during treatment with atypical antipsychotics,but the likelihood appears significantlyless than has been reported for typical antipsychotics.
Risk Factors The literature regarding predispositions to TD has addressed patient and drug treatment variables. Reports have been various and often contradictory. Authorities seem to concur that age (greater than 60 years), female gender, diagnosis of an affective disorder, and a history of prior neuroleptic-induced movement disorder are major patient-related risk factors. Older patients are more likely to develop severe and persisting forms of TD. Prevalence data find higher rates among women than men (27% versus 21%). Older women exhibit the highest rates for both TD and spontaneous dyskinesia. Among the affective disorders, recurrent depression in particular seems to confer high risk, perhaps because of the intermittent nature of mixed antidepressant and antipsychotic treatments. Patients who experience prior adverse neuroleptic reactions are at greater risk for TD, but experts are mixed about the type of reaction-acute dystonic reactions or drug-induced parkinsonism-that confers the greatest risk. Among treatment-related variables, a number of potential factors have been examined, including drug type, dosage, and concomitant medications. Perhaps the only point of consensus is that no specific type of typical neuroleptic (phenothiazine,thiothixene, or butyrophenone) is more likely than the other to cause TD. Higher dosage and longer duration of treatment have long been thought to increase risk, but evidence to confirm either suspicion has been curiously wanting. Another widely held notion is that concomitant use of anticholinergics during neuroleptic treatment increases the likelihood of TD. Although anticholinergics can worsen existing dyskinesia, their use in psychiatric patients before
Tardive Dyskinesia and Other Drug-Related Movement Disorders
81 1
the development of TD may not be a significant risk factor. Anticholinergics are useful in treating acute and tardive dystonias, and the varying anticholinergic properties of typical neuroleptics do not appear to increase or decrease the likelihood of TD. Dmerential Diagnosis
TD must be distinguished from other neuroleptic-induced movement disorders and from other drug-associated dyskinesias. Parkinsonism, dystonia, or akathisia can coexist with TD in one quarter to one third of cases. Dyskinesias similar to those seen in TD have been reported in association with a number of commonly used drugs (Table 127-1); movements generally remit with discontinuation of the non-neuroleptic drug in question. In general, TD distinguishes itself from other drug-induced syndromes because signs may persist after discontinuation of the neuroleptic. Sporadic dyskinesias described in schizophrenia may also persist, but they are often less rhythmic and more variable and complex. Adventitious orofacial movements associated with de-
w TMLE 127-1. Drugs Associated with Hyperkinetic Movements (Other Than Typical Neuroleptics) Drugs not commonly recognized as dopamine antagonists Prochlorperazine Metoclopramide Amoxapine (7-hydroxy metabolite) a-Methyl-p-tyrosine Drugs associated with dyskinesia in idiopathic Parkinson’s disease Levodopa or carbidopa Dopamine agonists (bromocriptine, pergolide, pramipexole, ropinerole, amantidine) Drugs associated with chorea, stereotypy, or dyskinesia during acute use or withdrawal Alcohol Amphetamines (and other stimulants) Anticholinergics (including atropine) Anticonvulsants (carbamazepine, ethosuximide, methsuximide, phenytoin, topiramate, valproate) Antihistamines Baclofen Benzodiazepines(triazolam in particular) Buspirone Caffeine Calcium channel blockers (cinnarizine, flunarizine, verapamil) Chloroquine-basedantimalarials Clebopride Cyclosporine Diazoxide Digoxin Fentanvl Flecainide H,-specific blockers: cimetidine, ranitidine lsoniazid Methadone Methyldopa Mianserin Pentamidine Reserpine Steroids (anabolic and oral contraceptives) Theophylline Other drugs, other movements Cefiazidime, other P-lactam antibiotics (asterixis) Morphine and meperidine (myoclonus) Monoamine oxidase inhibitors (tremor, myoclonus) Lithium (tremor, myoclonus) Drugs and treatments that may aggravate an existing tardive state Tricyclic antidepressants Lithium Cannabis Electroconvulsivetherapy
812
Movement Disorders H Non-Parkinsonian Movement Disorders
mentia and edentulism also mimic TD. Neuroleptic withdrawal may itself result in dyskinesias that can take days, weeks, or months to resolve. TD and these so-called withdrawal dyskinesias may have a common pathophysiologic mechanism. TD shares clinical features with many basal ganglia diseases. Meige’s syndrome is an idiopathic focal dystonia characterized by blepharospasm and oromandibular dystonia that typically begins in middle age and may not be distinguishable from orofacial TD. Idiopathic torsion dystonia, young-onset parkinsonism, and doparesponsive dystonia, all diseases with a predilection for the young, may mimic tardive dystonia. Facial tics and grimacing characterize Tourette’s syndrome, although childhood onset and the characteristic fluctuating course in Tourette’s help differentiate it from TD. Many idiopathic disorders are progressive and are not associated with prior neuroleptic exposure, in contrast to the static or slowly resolving course of TD. Other differential diagnostic considerations include medical disorders associated with choreoathetosis: hyperthyroidism, hypoparathyroidism, hyperglycemia, Syndenham’s chorea, chorea associated with lupus, the antiphospholipid antibody syndrome, chorea gravidarum, Henoch-Schonlein purpura, and neuroacanthocytosis. Rare cases of brain tumors or other space-occupying lesions have manifested as dyskinesias. Stereotyped mannerisms are common in mental retardation, autism, pervasive developmental disorders, viral encephalitis, and various storage and metabolic diseases (e.g., ceroid lipofuscinosis, phenylketonuria). A peculiar stereotypy (hand- and self-clasping) characterizes Rett’s syndrome, an autistic disorder of girls recently linked to mutations of a methyl-CpG binding protein gene (MECP2) located on the X chromosome. Other basal ganglia disorders have prominent neuropsychiatric features and movements that may be confused with TD. As a general rule, the presence of neurologic signs other than dyskinesia or dystonia (e.g., pyramidal signs, ataxia, prominent dementia) suggests an alternative diagnosis. Huntington’s disease, an autosomal-dominant dementia linked to chromosome 4, can present with either early dyskinesia or subtle personality change, but it is relentlessly progressive. Unlike in Huntington’s disease, pure chorea is an unusual sign in TD. Wilson’s disease is an autosomal recessive disorder linked to chromosome 13; consanguinity is common in the family history. Onset of symptoms can occur in childhood, adolescence, or early adulthood. Two major forms have been described: Rigidity is the hallmark of a dystonic form, whereas tremor, dysarthria, clumsiness, and gait instability characterize a pseudosclerotic form. Both are progressive, and both involve evidence of abnormal copper deposition (in Descement’s membrane at the corneal limbus, in liver, and in the lentiform nucleus). Hemochromatosis and alcoholic cirrhosis with portosystemic shunting have been associated with a non-Wilsonian hepatolenticular degeneration with similar motoric features. Hallervorden-Spatz disease is an autosoma1 recessive disorder with onset in childhood. Progressive spasticity, dystonia, choreoathetosis, and dementia accompany pathologic deposition of iron in the globus pallidus and brainstem. Treatment
Prevention is the answer to any iatrogenic problem, so the indications for neuroleptics should be clear, the need for ongoing treatment should be reassessed regularly, and minimum effective dosages should be used. Beyond dosage reduction or neuroleptic
discontinuation as a general, first-line strategy, different TD syndromes warrant different treatment approaches. Options in Tardive Dystonia. Anticholinergics (e.g., trihexyphenidyl) have been used traditionally as a first-line agent, but high dosages often are needed, and side effects often are limiting. Benzodiazepines (e.g., clonazepam) are also useful alone or in combination with anticholinergics. Again, high dosages may be necessary, with attendant concerns about dependency and sedation. Baclofen may be of some benefit. Tetrabenazine, a dopaminedepleting agent, is not commonly available in the United States, but it has been used quite successfilly in movement disorder clinics. Tetrabenazine is a modest dopamine receptor antagonist and therefore runs the theoretical risk of perpetuating TD as it treats it. Reserpine is a commonly available alternative to tetrabenazine. Orthostatic hypotension and depression are major side effects for both drugs. The notion that anticholinergics can exacerbate coexisting choreoathetosis is open to question, but if a dystonia improves on an anticholinergic, it should be slowly withdrawn and reintroduced only if dystonias reappear. In general, it is wise to limit polypharmacy whenever possible. Particularly in the case of the TDs, however, response can be lackluster; multiple agents at one time or serial empirical trials often are necessary. Three options exist in recalcitrant cases. Some have advocated use of atypical antipsychotics early in TD treatment. To date, the greatest experience has been with clozapine, but the risk of agranulocytosis and blood-monitoring considerations have led most clinicians to reserve its use until other trials have failed. Botulinum toxin, a widely accepted treatment for focal and segmental dystonias, is an effective treatment in tardive dystonia, but not all dystonias are amenable because of the size or numbers of muscles involved. Surgeries, particularly lesions of the thalamus or globus pallidus, have been explored in case reports. Options in Choreoathetoid TD. Because TD appears to be less common with the atypical antipsychotics, many patients on typical antipsychotics have been switched to one of the four approved atypicals with the idea that TD might also be managed to some degree. When such a strategy is adopted, use of clozapine should be reserved for the last, for reasons cited earlier. Increasingly, the atypicals are being used as first-line agents to treat psychotic conditions, but the risk of TD still exists. Therefore, other treatment options still must be entertained. Oxidative stress has been an interest in TD as elsewhere in neurology: Vitamin E, at dosages of 1600 IU/day, is advocated, but its efficacy is unclear. Agents that augment y-aminobutyric acid (GABA) neurotransmission are popular, including not only the benzodiazepines (particularly clonazepam and diazepam) but also valproic acid, and, uncommonly, y-vinyl GABA. Baclofen, a third GABA-ergic agent, has been used at high dosages, but it sedates and has itself been associated with chorea in a case report. As in tardive dystonia, tetrabenazine and reserpine have been used in difficult cases. High dosages may be needed, and benefits often are delayed for weeks to months. Use of electroconvulsive therapy in TD is controversial: In some reports, it has worsened rather than improved adventitious movements. The benefits of pallidal or thalamic surgeries are theoretically viable but untested. Options in Tardive Akathisia. In acute akathisia, anticholinergics have little effect, except in cases in which there is coexisting parkinsonism. In tardive akathisia, anticholinergics are not useful. P-Blockers may be an option, but in general tetrabenazine and reserpine seem most effective. There has been little reported on tardive akathisia with use of the atypical antipsychotics.
Chapter 127
ACUTE DYSTONIC REACTIONS As in TD, clinical phenomenology in the acute dystonic reactions is diverse. Oculogyric crises, blepharospasm, trismus, oromandibular dystonia, abnormal tongue positions (e.g., the bon-bon sign, when the tongue fixes to the inside of the cheek), myoclonic contractions of the face, neck, and extremities, and glossopharyngeal contractions (which may present with stridor) may all manifest in combination or in isolation. Spasmodic torticollis or retrocollis is common, and, in children, dramatic truncal presentations (opisthotonus, tortipelvis) may occur. Acute dystonic reactions occur early in the course of treatment with typical neuroleptics, usually within the first 5 days, but serotonin-specific drugs (including the selective agonists buspirone and sumatriptan) may also precipitate such reactions. Acute dystonic reactions occur in perhaps 2% of patients who receive typical neuroleptics, but African American and Asian American men may be at greater risk. High-potency neuroleptics such as haloperidol and fluphenazine are more likely to result in acute dystonia than lower-potency agents such as chlorpromazine and thioridazine. Patients treated with depot injections may present with multiple episodes, often within 72 hours of administration. Neuroleptic use in any medical or psychiatric context may result in acute dystonic reactions. Anticholinergics (e.g., parenteral diphenhydramine or benzotropine) abort the acute dystonias; benzodiazepines are a second-line option. Prophylactic use of anticholinergics may be indicated in psychiatric settings because of the formidable compliance problems that can result from an acute reaction.
AKATHlSlA Akathisia (from Greek, “not sitting”) is a disorder in which various excessive movements (forced marching, rocking in place, even moaning) are associated with an inwardly felt discomfort, variously described as a pulling or drawing feeling in the legs or a profound anxiety. Movements can be voluntarily suppressed, but only for a time. Haskovec (1901) first described the phenomenon in hysteria; later authors observed it in Parkinson’s disease, encephalitis lethargica, and postencephalitic parkinsonism. Many now believe that akathisia is a form of drug-induced parkinsonism. Akathisia shares features with restless legs syndrome, but in the latter, symptoms tend to manifest only‘when recumbent and typically in the evening, and other features are absent, including myoclonus, periodic movements of sleep, and dystonic postures in the legs and feet. Pseudoakathisia is motor restlessness without associated subjective distress. Acute akathisia should be suspected in any patient with subjective and objective restlessness after first neuroleptic exposure, change to a higher-potency agent, or an increase in dosage of a standing neuroleptic. Worsening “psychotic” agitation in the context of escalating neuroleptic dosage may be a clue to neuroleptic-induced akathisia. “Cyclic” akathisia has been described in patients who receive regular depot neuroleptic injections. Akathisia has also been associated with the serotoninselective reuptake inhibitors, particularly fluoxetine and paroxetine. Pharmacologic treatments have had inconsistent results. Traditionally, anticholinergics have been a mainstay, but their efficacy in akathisia is less convincing than in neuroleptic-induced dystonia or in drug-induced parkinsonism. When akathisia is accompanied by parkinsonism, anticholinergics are a reasonable first-line agent.
Tardive Dyskinesia and Other Drug-Related Movement Disorders
813
Lipophilic P-adrenergic drugs (e.g., propranolol) may be the most effective treatment, and benzodiazepines can relieve subjective distress.
DRUG-INDUCED PARKINSONISM (DIP) Any or all of the cardinal signs of idiopathic Parkinson’s disease-resting tremor, bradykinesia, rigidity, and postural instability-may be produced by neuroleptics and by a variety of other drugs, as reviewed in Table 127-2. Unlike in TD, differences in neuroleptic type influence the likelihood of developing DIP Higher-potency agents (e.g., haloperidol, fluphenazine, and thiothixene) present greater risk than lower-potency agents (e.g., chlorpromazine). Although the atypical neuroleptics are associated with less DIP, risperidone in particular may result in DIP in dose-dependent fashion, with greater risk at more than 6 mg per day; older adults may be vulnerable at significantly lower dosages. Ninety percent of cases develop within the first 72 days of treatment, according to an old but often-cited survey. Many manifest DIP in the first 3 weeks. Prevalence figures vary widely, from 10% to more than 65%, perhaps reflecting the underdiagnosis of DIP in some settings, such as among institutionalized older adults. However, there is agreement that older patients on high-potency agents are at particular risk. Bradykinesia or akinesia may be the only manifestation; rigidity and reduced armswing are early and frequent findings. Mutism, drooling, and dysphagia may be prominent. Tremor is less common in DIP than in idiopathic Parkinson’s disease, but when present it is often asymmetrical and may be of resting, postural, or action varieties. Perioral tremor should be considered a focal manifestation of DIP. DIP has been reported during neuroleptic withdrawal, and persisting parkinsonism has been described for as long as 18 months in small numbers of patients. In an older adult population, 25% of patients with DIP developed signs of idiopathic Parkinson’s disease within 41 months of drug discontinuation. These observations have prompted speculation that DIP can manifest in those who are vulnerable to the development of idiopathic Parkinson’s disease and other related disorders. Individual sensitivity to neuroleptics has been invoked to explain the absence of a clear dosage-response relationship in DIP. Two clinicopathologic cases have been reported in which DIP resolved after neuroleptic discontinuation, but nigral degeneration, Lewy
R ’IrA.rr 12T-Z Drugs Assodated with Parkinsonism Typical antipsychotics Drugs not commonly recognized as dopamine antagonists (see Table 127-1) Risperidone, especially a t more than 6 mg per day Lithium Valproic acid Selective serotonin reuptake inhibitors (SSRls): fluoxetine, paroxetine, fluvoxamine SSRls in combination with Cimetidine Selegiline Other monoamine oxidase inhibitors Chronic cocaine Alcohol withdrawal Cisapride Lovastatin Amiodarone Diltiazem Other calcium channel blockers, flunarazine, and cinnarizine (these agents chemicallv resemble the neuroleotic trifluoDerazine)
814
Movement Disorders w
Non-Parkinsonian Movement Disorders
bodies, and neurochemical evidence for loss of striatal dopamine were documented at autopsy. DIP should be managed with reduction in neuroleptic dosage, change to a lower-potency agent, or discontinuation of an offending drug. When such interventions are ineffective, the anticholinergics trihexyphenidyl and benztropine often are used. Amantidine may also be effective. Clinicians have traditionally understood a reciprocity between dopamine and acetylcholine in the basal ganglia, as supported by the use of anticholinergics in DIP and in idiopathic Parkinson’s disease, or in light of cases in which parkinsonism has emerged during treatment with cholinesterase inhibitors such as physostigmine or tacrine. However, it appears that dopamine receptor blockade differs qualitativelyfrom depletion states, and anticholinergics may be preferentially beneficial only in DIP. Levodopa reverses parkinsonism in animals and humans exposed to reserpine, a dopamine-depleting drug, but dosages of levodopa to as high as 1 gram have not been effective in treating DIP. Some 28 reports have been published regarding motoric effects of the selective serotonin reuptake inhibitors (SSRIs), specifically fluoxetine, paroxetine, and fluvoxamine. DIP, akathisia, and dystonic reactions have been described. Signs develop within days or weeks of treatment. Concomitant neuroleptic use in some cases led to an early theory that drug interactions or SSRI-mediated effects on drug metabolism were responsible, but alternative mechanisms have been studied to account for an isolated SSRI effect, including serotonergic modulation of dopamine neurotransmission. Rigidity, tremor in some cases, and shuffling gait all reverse with discontinuation of the SSRI.
NEUROLEPTlC MALIGNANT SYNDROME (NMS) NMS is an uncommon complication of neuroleptic therapy, thought to occur in less than 1% of patients. Both the typical and atypical neuroleptics have been implicated. Hyperthermia (more than 37OC) and muscle rigidity are cardinal features, which appear after first drug exposure or after an increase in dosage. Associated phenomena include a confusional state, autonomic instability (tachycardia, blood pressure fluctuations, sweating, tachypnea), elevations in creatine phosphokinase, leukocytosis, and metabolic acidosis. Various combinations of these signs may occur. Acute withdrawal of levodopa or dopamine agonists in Parkinson’s disease may induce an NMS-like condition. Lithium may act synergistically with neuroleptics to induce NMS in some cases. Infection, dehydration, and use of high-potency neuroleptics are other predisposing factors. All ages are at risk; men and women are affected equally. Mortality, estimated at 10% to 25%, typically results from pulmonary embolism associated with deep vein thrombosis, renal failure, cardiovascular collapse, or pneumonia. Differential diagnosis includes meningoencephalitis, systemic infection, heat stroke, traumatic or other rhabdomyolysis, anticholinergic or lithium toxicity, strychnine poisoning, tetanus, generalized dystonia (various causes), and the serotonin syndrome. Two additional entities, lethal catatonia and malignant hyperthermia, merit separate comment. Lethal catatonia is a condition that was first described before the use of neuroleptics. It is associated with psychotic agitation and, in its most severe forms, akinesia, rigidity, fixed abnormal postures, and mutism. Profoundly catatonic patients may manifest fever and dysautonomia. Some have argued that lethal catatonia is clinically equivalent to NMS except for the neuroleptic exposure (analogy may be drawn to hyperkinetic movement disorders similar to TD seen in
unmedicated psychotic patients). Malignant hyperthermia (MH) is a hereditary disorder in which patients exposed to inhaled anesthetics or succinylcholine develop a severe akinetic rigidity that does not respond to pancuronium or associated muscle relaxants. MH may occur in the absence of a family history, especially in patients with known preexisting muscular dystrophies or myopathy. In patients at risk for MH, biopsied muscle fibers exhibit exaggerated contractility upon exposure to halothane and caffeine. Similar muscle changes can occur in NMS, but they have been inconsistently observed, and the mechanism for such abnormalities may differ in NMS (e.g., neuroleptics may affect calcium levels at sarcoplasmic reticulum). Anesthetics do not predispose to NMS, and patients with MH are not at greater risk for NMS. Muscle relaxants such as pancuronium have been used safely in very severe forms of NMS. Dopaminergic blockade, perhaps at the level of hypothalamus, has been the most popularly espoused mechanism for NMS. Henderson and Wooten postulated the hypothalamic effect in 1981, based on a case in which a parkinsonian patient with a history of a psychotic disorder and chronic haloperidol therapy developed NMS upon withdrawal of dopamine agonists. Traditional neuroleptics may affect temperature regulation to some degree in all patients. The reasons why certain patients progress to NMS are obscure, but in an interesting prospective study of 26 episodes in 25 patients over 9 years, reduced serum iron levels (less than 10 kmol/L) were consistently observed at the time of diagnosis, often with normalization after the NMS resolved. Reduced serum iron may change central dopamine receptor sensitivity and thereby predispose to NMS, but other factors probably play a role. Treatment in NMS is largely supportive. Neuroleptic, anticholinergic, and lithium salts should be discontinued. Fluid status must be monitored closely. Concurrent infection must be excluded or treated aggressively. Low-dose heparin lessens the risk of deep venous thrombosis. Bromocriptine, dantrolene sodium, and levodopa may each have a role in refractory cases, but their efficacy is unclear. Their routine use is not universally accepted. In some patients, reinstituting neuroleptic treatment after a bout of NMS is necessary. Even when the same neuroleptic or one of similar potency is reintroduced, risk of recurrence is estimated at 50%. Why the risks are not higher is unclear. Neuroleptic rechallenge should be delayed for at least 2 weeks after a bout of NMS to minimize risk, and use of lower-potency agents is preferable.
SEROTONIN SYNDROME Perhaps the earliest case of what has come to be known as the serotonin syndrome dates to 1955, when a recurrent, then fatal encephalopathyoccurred in a patient who received repeated doses of meperidine while being treated with iproniazid, a monoamine oxidase inhibitor. In addition to being a narcotic, meperidine also inhibits serotonin reuptake. In the 1990s, treatment with SSRIs, particularly in combination with the monoamine oxidase inhibitors, resulted in diverse clinical toxicities. The term serotonin syndrome was popularized at that time, and its common manifestations include encephalopathy, dysautonomia, fever, rigidity, myoclonus, and hyperreflexia. Unlike in NMS, elevations in creatine phosphokinase and leukocyte count are uncommon but can occur. Exposure to drugs that enhance serotonergicaction is a sine qua non, but that list is long (Table 127-3) and includes drugs with multiple neurotransmitter actions (e.g., tertiary amine
Chapter 127 W
Tardve Dyskinesia and Other Drug-Related Movement Disorders
TABU 127-3. Some Drugs That Enhance Serotonergic Neurotransmission
Amitriptyline Buspirone Clomipramine Cocaine Dextromethorphan Fenfluramine Fluoxetine Fluvoxamine lmipramine lsocarboxazid Levodopa Lithium Lysergic acid diethylamide Methylenedioxymethamphetamine Meperidine Paroxetine Phenelzine Selegiline Sertraline Tranylcypromine Trazodone Venlafaxine
tricyclic antidepressants) and drugs not commonly known to have major serotonergic effects. Lithium is an example of the latter, although its toxicities are familiar to the clinician: Lithium produces tremor at therapeutic dosages, and at toxic levels it causes encephalopathy with rigidity and myoclonus. The spectrum of signs seen in lithium toxicity could also be the spectrum of the serotonin syndrome. In both cases, toxicity can be benign or severe but not necessarily dose dependent in the case of the serotonin syndrome. The mental status ranges from subtle encephalopathy to frank coma. Generalized seizures occur in a minority of cases. Motor dysfunction is a major aspect of the disorder, particularly myoclonus, hyperreflexia, rigidity (which may be limited to the legs), and ataxia. Reflex and tone abnormalities are generally bilateral; bilateral extensor toes manifest in a minority of patients. An internal ophthalmoplegia is not uncommon: Dilated, unreactive pupils may be seen in an estimated 25% of cases. Other autonomic features are similar to those seen in NMS, including prominent diaphoresis, fever, pulse and blood pressure fluctuations, and tachypnea. Although some authors cite a relationship between the serotonin syndrome and the carcinoid syndrome, others have found that skin flushing, nausea, diarrhea, and abdominal pain are rare. The syndrome carries a good prognosis if the offending drug is discontinued or if overdose is treated aggressively. In severe cases, seizures, coma, hyperthermia, disseminated intravascular coagulation, and metabolic acidosis may occur. Cyproheptadine, a serotonin antagonist with affinity for 5-HT,, and 5HT, receptors, has been used as antidote in some case reports, but treatment is largely supportive.
PATHOPHYSIOLOGY IN THE DRUG-INDUCED MOVEMENT DISORDERS Dopamine plays a complex modulatory role on pathways that influence movement in general. In a prevailing model, paucity of movement and excessive, involuntary movement result from imbalance between so-called direct and indirect connections between the striatum, particularly the caudate and putamen, and the motor thalamus. The relationship between the two pathways
815
has been characterized as a push-pull relationship in which the direct pathway facilitates normal movement, and the indirect pathway inhibits unwanted movement. Both are influenced by dopamine projections arising from midbrain structures, including the substantia nigra pars compacta and the ventral tegmental area. Dopamine’s actions at the striatum differ on the basis of distinct receptor types expressed on striatal neurons. Normally, dopamine excites neurons of the direct pathway that express D1-type receptors, whereas dopamine inhibits neurons of the indirect pathway that express D2-type receptors. Some have questioned the neatness of the D1 direct-D2 indirect division because many striatal neurons coexpress both types, but dopamine clearly has receptor-dependent effects on pathways that operate in parallel in both normal and disease states. Postsynaptic dopamine receptor supersensitivity has been implicated in the pathogenesis of TD, but the hypothesis is problematic in at least two important respects: It does not fully explain the time course of TD, and it does not explain why TD happens only in a minority of cases. Acute dopamine blockade reliably results in receptor supersensitivity in a short time frame (perhaps days), not the longer time frame over which some, but not all, patients develop motor complications. Upon discontinuation of dopamine receptor blockade, supersensitivity reliably disappears (perhaps over months), yet some dyskinesias may persist for longer periods of time. Thus, major reservations exist about a supersensitivity hypothesis, especially if one assumes that receptor changes must be directly responsible for the development of a toxicity. But a perturbation of a diffusely projecting neurotransmitter system such as dopamine may have more complicated effects in which supersensitivity still plays a role. All neuroleptics that block D2 receptors are associated with an increased risk for both DIP and TD. To account for the time course of motor complications and for the lack of universality of those complications, however, other potentially adaptive receptormediated effects must be involved. These alternative effects may involve other classic neurotransmitter systems (serotonergic, GABAergic, and cholinergic) or cotransmitter expression (e.g., substance P and dynorphin associated with direct pathway projections or enkephalin and neurotensin associated with indirect pathway projections). A new perspective on dopamine’s modulatory effects is emerging in which a specific drug perturbation can have ramified effects, which in turn suggest ongoing plastic or adaptive change in response to that exposure. In idiopathic Parkinson’s disease, dopamine denervation results in imbalanced activities of direct and indirect pathways, but a variety of non-dopamine changes have also been reported. One notable, recent set of observationsin Parkinson’s disease points to enhanced glutamatergic activity of projection neurons arising from cerebral cortex and terminating on medium spiny striatal neurons, associated with presynaptic D2 receptor supersensitivity. Enhanced excitatory neurotransmission has also been implicated in the pathogenesis of TD. In the setting of chronic levodopa treatment associated with dyskinesia in Parkinson’s disease, changes in gene expression, as measured by the induction of so-called immediate-early genes, are observed in specific patterns throughout the striatum. These studies have been conducted primarily in animal models, but they are instructive in a larger sense. The patterns of induction may relate to specific kinds of treatment (e.g., drugs with mixed D1 and D2 effects versus D1- or D2-specific effects), but, more importantly, induction of these genes may alter aspects of neuronal function over long periods of time, with variable effects on the balance of
816
Movement Disorders
Non-Parkinsonian Movement Disorders
pathways in the basal ganglia. The effects of immediate-early gene expression may include system changes (e.g., persisting druginduced changes in the patterns of neuronal discharge in basal ganglia structures). This ongoing area of work represents an extension of synaptic models of drug effects that have dominated thinking in psychopharmacology over the past quarter century.
SUGGESTED READINGS Baldassano CF, Truman CJ, Nierenberg A et a1 Akathisia: a review and case report following paroxetine treatment. Compr Psychiatry 37(2):122124, 1996
Beasley CM, Dellva MA, Tamura RN et ak Randomized double-blind comparison of the incidence of tardive dyskinesia in patients with
schizophrenia during long-term treatment with olanzapine or haloperidol. Br J Psychiatry 174(1):23-30, 1999 Caley C F Extrapyramidal reactions and the selective serotonin-reuptake inhibitors. Ann Pharmacother 31(12):1481-1489, 1997 Casey DE: Neuroleptic-induced acute extrapyramidal syndromes and tardive dyskinesia. Psychiatr Clin North Am 16(3):589-610, 1993 Diederich NJ, Goetz CG: Drug-induced movement disorders. Neurol Clin North Am 16(1):125-139, 1998 Friedman JH: Drug-induced parkinsonism. pp. 41-83. In Lang AE, Weiner WJ (eds): Drug-Induced Movement Disorders. Futura, Mount Kisco, NY, 1992
Gardos G, Cole J O Overview: public health issues in tardive dyskinesia. Am J Psychiatry 137(7):776-781, 1980 Graybiel AM, Canales J J, Capper-Loup C Levodopa-induced dyskinesias and dopamine-dependent stereotypies: a new hypothesis. Trends Neurosci 23(Suppl):S71-77, 2000 Hasan S, Buckley P Novel antipsychotics and the neuroleptic malignant syndrome: a review and critique. Am J Psychiatry 155(8):1113-1116, 1998 Henderson VW, Wooten G F Neuroleptic malignant syndrome: a pathogenetic role for dopamine receptor blockage? Neurology 31(2):132137, 1981 Jeste DV, Lacro JP, Bailey A et ak Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr SOC47(6):716-719, 1999 Kane JM: Tardive dyskinesia: epidemiological and clinical presentation. pp. 1485-1495. In Bloom FE, Kupfer J (eds): Psychopharmacology: The Fourth Generation of Progress. Raven Press, New York, 1995 Kane JM, Woerner MG, Pollack S et ak Does clozapine cause tardive dyskinesia? J Clin Psychiatry 54(9):327-330, 1993 Leo RJ: Movement disorders associated with serotonin reuptake inhibitors. J Clin Psychiatry 57(10):449-454, 1996 Miyawaki E, Meah Y, Koller W C Serotonin, dopamine, and motor effects in Parkinson’s disease. Clin Neuropharmacol 20(4):300-3 10, 1997 Simpson GM: The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 61(Suppl4):3944, 2000 Sternbach H: The serotonin syndrome. Am J Psychiatry 148(6):705-713, 1991
128 Primary and Secondary Generalized Dystonias Joseph Jankovic Dystonia is a neurologic syndrome dominated by involuntary, sustained (tonic), or spasmodic (rapid or clonic), patterned, and repetitive muscle contractions, often causing twisting and other abnormal movements or postures. The most common forms of dystonia include blepharospasm, an involuntary closure of eyelids caused by forceful contractions of the orbicularis oculi; oromandibular dystonia, manifested by jaw closure (trismus, bruxism) or jaw opening; cervical dystonia, manifested by torticollis, retrocollis, anterocollis, and other twisting movements of the neck; and writer’s cramp. Because of its variable presentation and fluctuating intensity, dystonia is still often wrongly attributed to psychological causes. Traditional descriptions of dystonia emphasize that the muscle contractions are sustained; therefore, rapid movements often are not recognized as dystonic. These rapid movements resemble myoclonus, which is a jerklike movement produced by brief muscular contractions (positive myoclonus) or inhibitions (negative myoclonus). Some patients have both dystonia and myoclonus (dystonia-myoclonus syndrome). The latter disorder often improves with alcohol intake. One of the most characteristic features of dystonia, which helps differentiate it from the other hyperkinetic movement disorders, is that dystonic movements, whether slow or rapid, are repetitive and patterned (involving the same group of muscles). This is in contrast to chorea, which consists of brief movements that flow randomly from one body part to another. Tics are abrupt movements (or sounds) that are usually more intermittent and coordinated than dystonia or myoclonus, more easily suppressible, and often preceded by
premonitory symptoms such as an urge or a tension that is temporarily relieved by the execution of the tic. Some tics are more sustained and are called dystonic tics. Although dystonic movements usually are continual, the timing and intensity of the movements can be influenced by various factors, including emotion, fatigue, relaxation, motor activity, sensory tricks, and sleep. Rarely, dystonia can fluctuate so much that it might be absent in the morning and become pronounced and disabling in the afternoons and evenings. This diurnal dystonia usually occurs in children and young adults, may be associated with parkinsonian features in the patients and their relatives, and usually improves dramatically with levodopa. Not all patients with dopa-responsive dystonia have diurnal variations, and many patients with dopa-responsive dystonia are initially misdiagnosed as having cerebral palsy. Another type of noncontinual dystonia is the paroxysmal dystonias. These are characterized by an abrupt onset or an exacerbation of dystonic movements lasting seconds to hours. They may be induced by a sudden movement (kinesigenic dystonia) or may occur spontaneously (nonkinesigenic dystonia). Paroxysmal dystonia may be sporadic or inherited, but head trauma, certain metabolic disorders, and other causes can produce paroxysmal dystonia. An example of secondary paroxysmal dystonia is the oculogyric crisis, characterized by sudden, intermittent conjugate eye deviations, sometimes seen in patients with postencephalitic parkinsonism, Tourette’s syndrome, and druginduced dystonia.
816
Movement Disorders
Non-Parkinsonian Movement Disorders
pathways in the basal ganglia. The effects of immediate-early gene expression may include system changes (e.g., persisting druginduced changes in the patterns of neuronal discharge in basal ganglia structures). This ongoing area of work represents an extension of synaptic models of drug effects that have dominated thinking in psychopharmacology over the past quarter century.
SUGGESTED READINGS Baldassano CF, Truman CJ, Nierenberg A et a1 Akathisia: a review and case report following paroxetine treatment. Compr Psychiatry 37(2):122124, 1996
Beasley CM, Dellva MA, Tamura RN et ak Randomized double-blind comparison of the incidence of tardive dyskinesia in patients with
schizophrenia during long-term treatment with olanzapine or haloperidol. Br J Psychiatry 174(1):23-30, 1999 Caley C F Extrapyramidal reactions and the selective serotonin-reuptake inhibitors. Ann Pharmacother 31(12):1481-1489, 1997 Casey DE: Neuroleptic-induced acute extrapyramidal syndromes and tardive dyskinesia. Psychiatr Clin North Am 16(3):589-610, 1993 Diederich NJ, Goetz CG: Drug-induced movement disorders. Neurol Clin North Am 16(1):125-139, 1998 Friedman JH: Drug-induced parkinsonism. pp. 41-83. In Lang AE, Weiner WJ (eds): Drug-Induced Movement Disorders. Futura, Mount Kisco, NY, 1992
Gardos G, Cole J O Overview: public health issues in tardive dyskinesia. Am J Psychiatry 137(7):776-781, 1980 Graybiel AM, Canales J J, Capper-Loup C Levodopa-induced dyskinesias and dopamine-dependent stereotypies: a new hypothesis. Trends Neurosci 23(Suppl):S71-77, 2000 Hasan S, Buckley P Novel antipsychotics and the neuroleptic malignant syndrome: a review and critique. Am J Psychiatry 155(8):1113-1116, 1998 Henderson VW, Wooten G F Neuroleptic malignant syndrome: a pathogenetic role for dopamine receptor blockage? Neurology 31(2):132137, 1981 Jeste DV, Lacro JP, Bailey A et ak Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr SOC47(6):716-719, 1999 Kane JM: Tardive dyskinesia: epidemiological and clinical presentation. pp. 1485-1495. In Bloom FE, Kupfer J (eds): Psychopharmacology: The Fourth Generation of Progress. Raven Press, New York, 1995 Kane JM, Woerner MG, Pollack S et ak Does clozapine cause tardive dyskinesia? J Clin Psychiatry 54(9):327-330, 1993 Leo RJ: Movement disorders associated with serotonin reuptake inhibitors. J Clin Psychiatry 57(10):449-454, 1996 Miyawaki E, Meah Y, Koller W C Serotonin, dopamine, and motor effects in Parkinson’s disease. Clin Neuropharmacol 20(4):300-3 10, 1997 Simpson GM: The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 61(Suppl4):3944, 2000 Sternbach H: The serotonin syndrome. Am J Psychiatry 148(6):705-713, 1991
128 Primary and Secondary Generalized Dystonias Joseph Jankovic Dystonia is a neurologic syndrome dominated by involuntary, sustained (tonic), or spasmodic (rapid or clonic), patterned, and repetitive muscle contractions, often causing twisting and other abnormal movements or postures. The most common forms of dystonia include blepharospasm, an involuntary closure of eyelids caused by forceful contractions of the orbicularis oculi; oromandibular dystonia, manifested by jaw closure (trismus, bruxism) or jaw opening; cervical dystonia, manifested by torticollis, retrocollis, anterocollis, and other twisting movements of the neck; and writer’s cramp. Because of its variable presentation and fluctuating intensity, dystonia is still often wrongly attributed to psychological causes. Traditional descriptions of dystonia emphasize that the muscle contractions are sustained; therefore, rapid movements often are not recognized as dystonic. These rapid movements resemble myoclonus, which is a jerklike movement produced by brief muscular contractions (positive myoclonus) or inhibitions (negative myoclonus). Some patients have both dystonia and myoclonus (dystonia-myoclonus syndrome). The latter disorder often improves with alcohol intake. One of the most characteristic features of dystonia, which helps differentiate it from the other hyperkinetic movement disorders, is that dystonic movements, whether slow or rapid, are repetitive and patterned (involving the same group of muscles). This is in contrast to chorea, which consists of brief movements that flow randomly from one body part to another. Tics are abrupt movements (or sounds) that are usually more intermittent and coordinated than dystonia or myoclonus, more easily suppressible, and often preceded by
premonitory symptoms such as an urge or a tension that is temporarily relieved by the execution of the tic. Some tics are more sustained and are called dystonic tics. Although dystonic movements usually are continual, the timing and intensity of the movements can be influenced by various factors, including emotion, fatigue, relaxation, motor activity, sensory tricks, and sleep. Rarely, dystonia can fluctuate so much that it might be absent in the morning and become pronounced and disabling in the afternoons and evenings. This diurnal dystonia usually occurs in children and young adults, may be associated with parkinsonian features in the patients and their relatives, and usually improves dramatically with levodopa. Not all patients with dopa-responsive dystonia have diurnal variations, and many patients with dopa-responsive dystonia are initially misdiagnosed as having cerebral palsy. Another type of noncontinual dystonia is the paroxysmal dystonias. These are characterized by an abrupt onset or an exacerbation of dystonic movements lasting seconds to hours. They may be induced by a sudden movement (kinesigenic dystonia) or may occur spontaneously (nonkinesigenic dystonia). Paroxysmal dystonia may be sporadic or inherited, but head trauma, certain metabolic disorders, and other causes can produce paroxysmal dystonia. An example of secondary paroxysmal dystonia is the oculogyric crisis, characterized by sudden, intermittent conjugate eye deviations, sometimes seen in patients with postencephalitic parkinsonism, Tourette’s syndrome, and druginduced dystonia.
Chapter 128
The severity of dystonia varies from a barely noticeable and often unrecognized symptom to disabling muscle contractions rendering the patient unable to ambulate or fully participate in activities of daily living. In several of my patients, the dystonic muscle contractions were so severe they produced muscle breakdown and myoglobinuria. Primary (idiopathic) dystonia often starts as a task-specific dystonia (e.g., writer’s cramp). With increasing severity, however, the dystonic movements may occur in other, less specific activities and at rest and may eventually overflow to adjacent or other muscles. If left untreated, dystonia may evolve into fixed postures and contractures. Secondary dystonia usually is present at rest, even at onset. Dystonia often is associated with either dystonic or essential tremor. Dystonic tremor is actually a rhythmic dystonia, most evident when the patient voluntarily attempts to move in the direction opposite to the force of dystonia. Thus, a patient with torticollis to the right, when attempting to maintain primary head position, may develop lateral irregular tremor that disappears when the patient allows the head to turn to the right (in the direction of the torticollis). In contrast, patients with coexistent essential tremor continue to have the oscillatory movement regardless of the direction of the force of the dystonia. Although the two types of tremor usually can be identified clinically, the differentiation may be aided by the use of electromyography. It is not yet clear whether the postural tremor associated with dystonia, such as the hand flexion-extension tremor seen in 25% of patients with cervical dystonia, is a form of essential tremor or whether it is an expression of some dystonia-related physiologic abnormality. A pathogenic relationshipbetween dystonia and essential tremor is suggested by the frequent occurrence of essential postural tremor in family members of patients with dystonia. In some patients, head and trunk tremor (2- to 5-Hz frequency) may precede the onset of dystonia and may be the initial manifestation or forme fiuste of dystonia (dystonic tremor). Certain task-specific tremors (e.g., primary writing tremor) may actually represent forms of focal dystonia. Some patients with primary writing tremor voluntarily contract their forearm muscles in an attempt to control the hand tremor. This compensatory muscle contraction is sometimes wrongly attributed to dystonia. Besides essential tremor and myoclonus, dystonia occasionally is also associated with other movement disorders, including parkinsonism. The epidemiology of dystonia has not been studied by appropriate methods, but it has been estimated that there are at least 100,000 people with dystonia in the United States. If dystonic writer’s cramp were included, the true prevalence would be much greater because most patients with dystonic writer’s cramp do not seek medical attention.
CLASSIFICATION There are many ways to classify dystonia, but it is convenient to categorize dystonia according to its age at onset, cause, and anatomic distribution.
Age at Onset Age at onset is one of the most predictable determinants of future course and prognosis. Dystonia may start at any age and may be categorized as either infantile (less than 2 years), childhood (2 to 12 years), juvenile (13 to 20 years), or adult onset (older than 20 years). Childhood-onset dystonia, particularly common among Ashkenazi Jews, often is characterized by caudal-rostral progres-
Primary and Secondary Generalized Dystonias
817
sion, with legs being more involved early in the course. Whereas childhood-onset dystonia usually becomes generalized, adultonset dystonia usually remains focal or segmental. A typical presentation of childhood-onset dystonia is inversion of one foot while running or a writer’s cramp; the best examples of adultonset dystonia are blepharospasm and torticollis. Causes Dystonia either occurs alone, without any other neurologic deficits (called primary torsion dystonia), or may be a symptom of an underlying disorder (so-called secondary dystonia). Primary torsion dystonia can be either sporadic (idiopathic) or inherited, and it is not associated with any cognitive, pyramidal, cerebellar, or sensory abnormalities. The most important advance in our knowledge about genetic dystonia has been the identification of a 3-base-pair (GAG) deletion in the q32-34 region of chromosome 9 of families with autosomal dominant primary dystonia (DYT1 dystonia). In about one third of those carrying this mutation in the DYTl or TORRlA gene, dystonia is expressed clinically (30% to 40% penetrance). The onset usually is in childhood, typically presenting with distal, action dystonia that gradually progresses to a generalized disorder. DNA testing for the DYTl dystonia has demonstrated that many cases thought to be sporadic are actually inherited. This is particularly true among dystonic patients of Ashkenazi Jewish origin, in whom DYTl dystonia accounts for 90% of all cases of dystonia. The TORlA gene encodes torsinA. Although the function of torsinA is still not fully understood and its role in the pathogenesis of primary dystonia is still unknown, the protein is known to be a member of the AAA+ superfamily of chaperone proteins predominantly expressed in dopaminergic neurons. Other gene loci or mutations causing dystonia include a locus on 7q2 1-23 responsible for myoclonic dystonia, mutations in the GTP-cyclohydrolase 1 (GCH1) gene on chromosome 14q causing dopa-responsive dystonia, and a gene marker on chromosome 19q13 responsible for the rapid-onset dystonia-parkinsonism syndrome. Not all dystonias are of genetic origin; some are sporadic and others are secondary to some specific causes (Table 128-1). Of the secondary dystonias, Wilson’s disease is particularly important to recognize because early treatment of this autosomal recessive disease, caused by mutations in the gene on long arm of chromosome 13 encoding copper transporting P-type ATPase, can result in a complete or nearly complete abolishment of neurologic and liver problems. Almost any metabolic or structural lesion of the brain, particularly if it involves the putamen, other basal ganglia, and rostral brainstem structures, can produce dystonia. Besides Wilson’s disease, another important cause of secondary dystonia is drug-induced dystonia. The dopamine receptorblocking drugs (neuroleptics,such as the major tranquilizers, and gastrointestinal drugs, such as metoclopramide) can cause not only an acute transient dystonic reaction but also a persistent dystonic disorder (tardive dystonia). Besides central causes, which presumably account for most dystonias, peripherally induced dystonia caused by an injury to a nerve or a nerve root, often associated with reflex sympathetic dystrophy, is being increasingly recognized as an important cause of focal and segmental dystonia. About 40% of all patients with dystonia have been previously misdiagnosed as having a psychogenic illness. In actuality, however, less than 5% of all dystonias seen in a movement disorder clinic are of psychogenic origin, and the frequency is even lower in
818
Movement Disorders
rn Non-Parkinsonian Movement Disorders
TABU 118-1. Etiologic Classification of Dystonia 1. Primary dystonia A. Sporadic
B. lnheriied (all autosomal dominant) Classic (Oppenheim's) dystonia (DMl, 9q34) Childhood- and adult-onset cranial-cervical-limb dvstonia (DM6.8p21-22) Adult-onset cervical and other focal dystonia (OW, 18p) 11. Dystonia-plus syndromes A Sporadic Parkinson's disease Progressive supranuclear palsy Multiple system atrophy Corticobasal degeneration B. lnheriied 1. Autosomal dominant Dopa-responsive dystonia (DRD) (OMS, CTP cyclohydrolase I 14q22.1) Dystonia-myoclonus (1 1q23) Dystonia-ataxia (SCA 3 and SCA 6) 2. Autosomal recessive Dopa-responsive dystonia caused by tyrosine hydroxylase deficiency (1 1p l 1.5) Biopterin-deficientdiseases Aromatic amino acid decarboxylase deficiency (dopamine agonistresponsive dystonia) 111. Heredodegenerative diseases (typically not pure dystonia) A X-linked recessive Lubag (X-linked dystonia-parkinsonism, DM3, Xql2-Xq2 1) Pelizaeus-Merzbacher disease Lesch-Nyhan syndrome Dystonia-deafness(Xq22) Deafness, dystonia, retardation, blindness B. Autosomal dominant Rapid-onset dystonia-parkinsonism (RDP) Juvenile Parkinsonism-Dystonia Huntington's disease (IT1 5,4p 16.3) Spinocerebellar degenerations (SCA3, SCAC) Dentato-rubral-pallidoluysian atrophy (DRPLA) Hereditary spastic paraplegia with dystonia Thalamo-olivary degeneration with Wernicke's encephalopathy C. Autosomal recessive Wilson's disease (Cu-ATPase, 1 3q14.3) Neurodegenerationwith brain iron accumulation type 1 (NBIA 1) (Hallervorden-Soak disease. 20012.3-01 3) Hkoprebetalipopioteinernia,acanihocyt&is, ietinitis pigmentosa, and oallidal degeneration (HARP svndrome) Ataxia telangiectaga Associated with metabolic disorders 1. Amino acid disorders Clutaric acidemia Methylmalonic acidemia Homocystinuria Hartnup's disease Tyrosinosis 2. Lipid disorders Metachromatic leukodystrophy Ceroid lipofuscinosis Niemann-Pick type C (dystonic lipidosis, "sea blue" histiocytosis) Cangliosidoses, CM 1, CM2 variants Hexosaminidase A and B deficiency 3. Other metabolic disorders Biopterin-deficient diseases Triosephosphate isomerase deficiency Aromatic amino acid decarboxylase deficiency (dopamine agonistresponsive dystonia) Biotin-responsive basal ganglia disease D. Mitochondria1 Leigh's disease Leber's disease ~
~
~
~
~
E. Unknown inheritance Neuroacanthocytosis ReWs syndrome lntraneuronal inclusion disease Infantile bilateral striatal necrosis Familial basal ganglia calcifications Hereditary spastic paraplegia with dystonia Deletion of 18q With a known, specific cause Perinatal cerebral injury and kernicterus: athetoid cerebral palsy, delayed-onset dystonia Infection: Viral encephalitis, encephalitis lethargica, Reye's syndrome, subacute sclerosing panencephaliiis, Jakob-Creutzfeldt disease, HIV infection Other: tuberculosis, syphilis, acute infectious torticollis Drugs: levodopa and dopamine agonists, dopamine receptorblocking drugs, fenfluramine, anticonvulsants, flecainide, ergots, certain calcium channel blockers Toxins: MN, CO, CS2, cyanide, methanol, disulfiram, 3-nitroproprionic acid, wasp sting Metabolic: hypoparathyroidism Paraneoplastic brainstem encephalitis Vitamin E deficiency Primary antiphospholipid syndrome (PAPS) Cerebral vascular or ischemic injury Sjogren's syndrome Multiple sclerosis Central pontine myelinolysis Brainstem lesions Spinal cord lesions Syringomyelia Brain tumor Arteriovenous malformation Head trauma and brain surgery (thalamotomy) Lumbar stenosis Peripheral trauma (with causalgia) Electrical iniurv IV. Other hyperkinetk jndromes associated with dystonia A. Tic disorders with dystonic tics B. Paroxysmal dyskinkias Paroxysmal kinesigenic dyskinesia (PKD) (1 6pll.2-q12.1) Paroxvsmal nonkinesinenic dvskinesia (PNKD) (2a33-35) ParoGmal exertion-iiduced'dyskinesia (PEDj (1 6pl2-ql2) Paroxysmal hypnogenic dyskinesia (PHD) (20q13.2-13.3) V. Psychogenic VI. Pseudodystonia Atlanto-axial subluxation Syringomyelia Arnold-Chiari malformation Trochlear nerve palsy Vestibular torticollis Posterior fossa mass Soft tissue neck mass Congenital postural torticollis Congenital Klippel-Feil syndrome Isaac's syndrome Sandiffer's syndrome Satoyoshi's syndrome Stiff person syndrome Ventral hernia
Chapter 128
general neurologic practice. The differentiation between psychogenic and neurologic dystonia is one of the most formidable challenges facing the clinical neurologist. Because primary dystonia is not associated with any laboratory abnormalities, the diagnosis of psychogenic dystonia must be based on positive criteria; it is not sufficient to merely exclude other causes. Certain clues usually provide evidence of a psychogenic cause. These include false weakness, false sensory symptoms, multiple somatizations, self-inflicted injuries, bizarre movements or pseudoseizures, obvious psychiatric illness, and other features that are incongruous with typical dystonia. Relief of dystonia with psychotherapy, powerful suggestion, placebo, or physiotherapy excludes a neurologic cause because complete and permanent remissions are rare in organic forms of dystonia. Improvement under hypnosis or with amobarbital is not particularly helpful because both can ameliorate even neurologic dystonia. On the other hand, acute exacerbation and relief of the dystonia by a powerful suggestion coupled with intravenous or oral placebo provides important support for the diagnosis of psychogenic dystonia.
Dystonia is classified according to its anatomic distribution as focal, segmental, multifocal, generalized, and unilateral (hemidystonia). Cranial Dystonia. Craniocervical structures are most often affected in adult-onset dystonia. Blepharospasm, an involuntary bilateral eye closure produced by spasmodic contractions of the entire (pretarsal, preseptal, and periorbital) orbicularis oculi muscles, often is accompanied by dystonic movements of the eyebrows and of the paranasal, facial, masticatory, labial, lingual, oral, pharyngeal, laryngeal, and cervical muscles. Blepharospasm often is exacerbated by exposure to bright light, wind, and air pollution, as well as by activity and stress. In most patients with blepharospasm, the onset often is heralded by increased frequency of blinking associated with a sandlike feeling of irritation in the eyes. Blepharospasm usually starts with clonic contractions of the eyelids, gradually progressing to more sustained and forceful eye closure. Eventually, patients have difficulty reading, watching television, driving, and performing other daily activities that depend on normal vision. If left untreated, up to 15% become functionally blind. Various maneuvers such as wearing dark glasses, pulling on an upper eyelid, pinching the neck, talking, humming, or singing can transiently relieve the involuntary eye closure in some patients. Afflicted women outnumber men 3 to 1 and, in most, symptoms commence by 50 years of age. Oromandibular Dystonia. Oromandibular dystonia consists of involuntary spasms of jaw, mouth, and tongue muscles producing jaw closure and trismus (jaw clenching) and bruxism (tooth grinding), often causing secondary dental wear and temporomandibular joint syndrome. In addition, involuntary tongue movements, jaw opening, or jaw deviation may cause difficultieswith chewing, speaking, and swallowing. Oromandibular dystonia should be differentiated from hemifacial or hemimasticatory spasm, tardive dyskinesia, tetany, tetanus, and mechanical disorder of the temporomandibular joint. Focal cranial and oromandibular dystonias are also discussed in Chapter 129. Cervical Dystonia. Cervical dystonia is the most common form of focal dystonia encountered in movement disorder clinics. Although torticollis, lateral rotation of the head, is the most common abnormal posture, the majority of patients have a
Primary and Secondav Generalized Dystonias
819
combination of torticollis, laterocollis, retrocollis, and anterocollis. In addition to cervical involvement, at least one third of all patients with cervical dystonia have scoliosis, suggestingadditional involvement of the thoracic muscles. Local pain accompanies cervical dystonia in more than one third of all patients. The pain can be caused by intense muscular spasms or by associated cervical spondylotic radiculomyelopathy. Cervical dystonia often is exacerbated during periods of stress or fatigue and usually is relieved by relaxation and various sensory maneuvers. Up to 20% of patients achieve spontaneous remission, but the dystonia usually recurs after several months. In most patients, cervical dystonia is a lifelong disorder, and in about 20% of patients, it progresses to a segmental or generalized dystonia. As in other forms of dystonia, the abnormal muscle contractions that produce head deviation can be temporarily controlled by a variety of sensory tricks, such as touching the chin, face, or back of the head. Although this observation suggests that cervical dystonia can be influenced by altering the proprioceptive input, the exact mechanism of the counterpressure, sensory trick, or geste antagoniste phenomenon is not known. Focal cervical dystonia is discussed in more detail in Chapter 129. Laryngeal Dystonia (Spasmodic Dysphonia). The career of a teacher, a trial attorney, or a professional singer can be prematurely ended with the development of spasmodic dysphonia. Despite growing evidence in support of neurologic origin, the symptoms are still too often attributed to psychogenic causes. Dystonia of the larynx may cause excessive and uncontrolled closing of the vocal folds (adductor spasmodic dysphonia), producing effortfid and strained voice interrupted by frequent breaks in phonation. The abductor form of spasmodic dysphonia is much less common, and it consists of prolonged vocal fold openings, producing breathy and whispering voice and phonatory pauses extending into vowels. The adductor spasmodic dysphonia is caused by hyperadductions of the thyroarytenoid vocalis complex, and the abductor form of spasmodic dysphonia is caused by contractions of the posterior cricoarytenoid muscle. Whereas nearly all cases of adductor spasmodic dysphonia are thought to represent a form of focal dystonia (see also Chapter 129), many cases of abductor dysphonia are thought to be of psychogenic origin. Many patients with spasmodic dysphonia also have voice tremor, and in some cases isolated voice tremor precedes the onset of spasmodic dysphonia by several years. Limb Dystonia. Idiopathic limb dystonia usually starts as an action dystonia. In contrast, secondary dystonia, caused either by central (brain) or peripheral (nerve or root) injury or lesion, often is present at rest, even at the onset. The task-specific focal dystonias seen in many occupational cramps (e.g., graphospasm or writer’s cramp) are the most common example of idiopathic arm dystonia. The task- or position-specific dystonias often occur with writing, typing, and feeding, during certain sport-related activities, and while playing musical instruments. Like other forms of dystonia, hand and arm dystonias often are associated with either dystonic or essential tremor. For example, some patients with writer’s cramp may display involuntary supination of the hand away from the desk, and when the patient volitionally pronates the hand in the act of writing, a twisting, jerking movement may appear. Such dystonic tremor occurs only during a specific action, and the tremor may not be evident when arms are outstretched in front of the body or when placed in any other position. However, about one third of patients with focal, task-specific dystonia experience a coexistent postural, essential tremor manifested by a flexion-extension oscillation of the hand
820
Movement Disorderr 1 Non-Parkinsonian Movement Disorders
during posture holding. When dystonia affects the foot in an adult, the possibility of Parkinson’s disease or a parkinsonian syndrome as the cause of the foot dystonia should be considered. Besides the striatal foot, some patients with Parkinson’s disease have a striatal hand deformity, often confused with rheumatoid arthritis. In children, the foot can twist into an equinovarus posture when the patient is running or walking, or the leg might kick during walking. The foot and leg dystonia may evolve into a fixed dystonic posture, commonly causing plantar flexion, extension at the knee, and flexion-adduction at the hip. Trunk Dystonia. Trunk dystonia can result in scoliosis, lordosis, kyphosis, tortipelvis, and opisthotonic posturing. At onset, abnormal movements of the trunk may be seen during walking or running, but in the advanced stages of the disease, the trunk deformities become fixed and present even when the patient is sitting or lying. Many patients with trunk dystonia have a bizarre gait resembling the gaits of various animals, hence the terms dromedary-, monkey-, and ducklike gait. Various sensory tricks, such as placing the hands in the pockets, behind the neck or back, or on the hip, might enable the patient to walk almost normally. Also, running, walking backward, or dancing might improve the truncal dystonia and dystonic gait. Hemidystonia. In contrast to other types of dystonias, which are usually idiopathic, about 85% of patients with hemidystonia have computed tomography or magnetic resonance imaging evidence of contralateral basal ganglia lesion or a history of hemiparesis. Besides ischemic or hemorrhagic strokes, other causes of hemidystonia include perinatal or other head trauma, thalamotomy, encephalitis, neurodegenerative disorders, arteriovenous malformation, and porencephalic cyst. Whereas a long delay of several years between injury and onset is typical for dystonia related to perinatal injury, the latency between the acute lesion and subsequent onset of dystonia often is less than 6 months in adult patients. ANATOMY, BIOCHEMISTRY, AND PATHOPHYSIOLOGY Although in most patients with dystonia no specific abnormality can be identified by neuroimaging or autopsy studies, there is convincing evidence supporting a central origin (basal ganglia, brainstem, or both) for this movement disorder. Some brains of patients with atypical dystonia have been found to have a mosaic pattern of striatal gliosis. Studies of patients with secondary dystonia have identified lesions involving the basal ganglia, particularly the putamen, and the rostral brainstem. The involvement of basal ganglia in dystonia is also supported by the finding of reduced glucose metabolism, as demonstrated by position emission tomography scans, in the basal ganglia, the frontal projection field of the mediodorsal thalamic nucleus, and the frontal cortex of patients with idiopathic torsion dystonia. No consistent abnormalities have been demonstrated in the few brains of patients with dystonia examined at autopsy. Neurophysiologic studies in patients with dystonia show prolonged firing of electromyelographic activity with cocontraction of antagonist muscles, repetitive and slow spasms of 1 to 2 seconds each and separated by equal periods of relative electromyelographic silence (previously called myorhythmia), postural 6- to 10-Hz frequency tremor, reduced reciprocal inhibition, and abnormal H reflex and blink reflex recovery cycle. These findings have been interpreted as indicating enhanced excitatory drive to the rostral brainstem or reduced spinal and brainstem inhibition.
TREATMENT Despite the paucity of knowledge about the cause and pathogenesis of most dystonic disorders, the symptomatic treatment of dystonia has markedly improved, largely as a result of the introduction of botulinum toxin. This therapeutic intervention is discussed in Chapter 129. Before contemplating symptomatic therapy, potentially curable causes of dystonia, such as certain drug-induced dystonias or Wilson’s disease, should be considered. Physical therapy, including well-fitted braces, may be helpful to some dystonic patients but are usually unsatisfactory when used alone. Although there is little scientific rationale for the drugs used to treat dystonia, about one third of patients benefit from some pharmacologic therapy (Table 128-2). The selection of a particular choice of therapy is guided largely by personal clinical experience and empiric trials. The first treatment of choice usually is determined by its low potential for adverse effects and by the anatomic distribution of dystonia. Although less than 10% of all children with dystonia have dopa-responsive dystonia, all patients with childhood-onset dystonia should be first treated with levodopa and carbidopa (Sinemet). Anticholinergic medications such as trihexyphenidyl have been found to be most effective for generalized dystonia. This therapy generally is well tolerated when the dosage is increased slowly. It is generally recommended to start with a 2-mg preparation, one half tablet at bedtime, and advancing up to 12 mg/day over the next 4 weeks. Some patients
H TABLE 128-2. Treatment of Dystonia
Focal Dyrtonias
Blepharospasm Botulinum toxin injections Clonazepam, lorazepam Trihexyphenidyl Orbicularis oculi myectomy Oromandibular dystonia Botulinum toxin injections Trihexyphenidyl Baclofen Spasmodic dysphonia Botulinum toxin injections Voice and supportive therapy Cervical Botulinum toxin injections Trihexyphenidyl Diazepam, lorazepam, clonazepam Tetrabenazine Cyclobenzaprine Carbamazepine Baclofen (oral) Peripheral surgical denervation Task-specific dystonias (e.g., writer‘s cramp) Benztropine, trihexyphenidyl Botulinum toxin injections Occupational therapy Segmental and Generalized Dystonias
Levodopa (in children and young adults) Trihexyphenidyl, benztropine Diazepam, lorazepam, clonazepam Baclofen (oral, intrathecal) Carbamazepine Tetrabenazine (with lithium) Triple therapy: tetrabenazine, fluphenazine, trihexyphenidyl lntrathecal baclofen infusion (axial dystonia) Peripheral denenration Thalamotomy and globus pallidus deep brain stimulation
Chapter 129
need 60 to 100 mg/day but may experience dosage-related drowsiness, confusion, memory difficulty, and hallucinations. Pyridostigmine, a peripherally acting anticholinesterase, and eye drops of pilocarpine (a muscarinic agonist) often ameliorate at least some of the peripheral side effects such as dry mouth, urinary retention, and blurred vision. Many patients need a combination of several medications and treatments. Benzodiazepines (clonazepam or lorazepam) may provide additional benefit for patients whose response to anticholinergic drugs is unsatisfactory. Baclofen may be helpful for oromandibular dystonia but is only minimally effective for generalized dystonia. In selected cases of severe axial and generalized dystonia, however, continuous intrathecal infusions of baclofen may be useful. Dopamine receptor-blocking drugs or neuroleptics (e.g., fluphenazine) have been used to treat dystonia, often in conjunction with anticholinergics. However, the use of dopamine receptor-blocking drugs to treat dystonia should be discouraged because of the potential for development of tardive dyskinesia. This risk may be minimized by coadministering reserpine or tetrabenazine. Tetrabenazine, a presynaptic dopamine-depleting drug, has been useful in some patients with dystonia, but its availability in the United States is limited. Attacks of kinesigenic paroxysmal dystonia may be controlled with anticonvulsants (e.g., carbamazepine, phenytoin), but the nonkinesigenic forms of paroxysmal dystonia are less responsive to pharmacologic therapy, although clonazepam and acetazolamide may be beneficial. Surgical approaches, such as local denervation, muscle excision, and stereotactic procedures such as thalamotomy or globus pallidus deep brain stimulation, play an increasingly important role, particularly in treating generalized dystonia.
Focal Dystonia: Treatment with Botulinurn Toxin
821
Bandman 0, Valente EM, Holmans P et ak Dopa-responsive dystonia: a clinical and molecular genetic study. Ann Neurol 44:649456, 1998
Bressman SB, Sabatti C, Raymond D et al: The DYTl phenotype and guidelines for diagnostic testing. Neurology 54:1746-1 752, 2000 Duffey P, Butler AG, Hawthorne MR, Barnes H: The epidemiology of primary dystonia in the north of England. pp. 121-125. In Fahn S, Marsden CD, DeLong DR (eds): Dystonia 3, Adv Neurol, Vol. 78, pp. 12 1-126. Lippincott-Raven, Philadelphia, 1998 Fahn S, Bressman S, Marsden CD: Classification of dystonia. Adv Neurol 78~1-10, 1998
Hallett M: Physiology of dystonia. Adv Neurol 78:ll-18, 1998 Hewett 1, Gonzalez-Agosti C, Slater D et al. Mutant torsin A, responsible for early-onset torsion dystonia, forms membrane inclusions in cultured neural cells. Hum Mol Genet 9:1404-1414, 2000 Jankovic J: Can peripheral trauma induce dystonia and other movement disorders? Yes! Mov Disord 16:7-12, 2001 Jankovic J: Dystonia: medical therapy and botulinum toxin in dystonia. pp. 169-184. In Fahn S , Marsden CD, DeLong DR (eds): Dystonia 3, Adv Neurol, Vol. 78, pp. 169-184. Lippincott-Raven, Philadelphia, 1998
Jankovic J: Re-emergence of surgery for dystonia. Editorial commentary. J Neurol Neurosurg Psychiatry 65:434, 1998 Jankovic J, Brin M: Botulinum toxin: historical perspective and potential new indications. Muscle Nerve 2O(Suppl 6):S129-S145, 1997 Nemeth A The genetics of primary dystonias and related disorders. Brain 125:695-721, 2002
Nygaard TG, Raymond D, Chen C et al: Localization of a gene for myoclonus-dystonia to chromosome 7q2 1-23. Ann Neurol 46794798, 1999
Swoboda KJ, Soong BW, McKenna C et al: Paroxysmal kinesigenic dyskinesia and infantile convulsions. Clinical and linkage studies. Neurology 553224230, 2000 Vitek JL, Chockkan V, Zhang J-Y et al: Neuronal activity in the basal ganglia in patients with generalized dystonia and hemiballism. Ann Neurol46:22-35, 1999
SUGGESTED READINGS Adityanjee, Yeken AA, Jampala VC, Mathews T: The current status of tardive dystonia. Biol Psychiatry 45:715-730, 1999
Warner TT, Jarman P The molecular genetics of dystonias. J Neurol Neurosurg Psychiatry 64:427429, 1998
129 Focal Dvstonia: Treatment with Botulinum Toxin Daniel Tarsy By contrast with generalized dystonia, which usually begins in childhood (see Chapter 128), adult-onset idiopathic dystonia usually remains localized to one body part without progression or spread to neighboring body regions. Whereas childhood-onset dystonia usually begins in the lower extremities, most adult dystonias begin in muscles of the face, neck, or upper extremities, where they remain focal. Occasionally, dystonia may spread to adjacent body parts to become segmental. Focal dystonias are listed in Table 129-1 with their more common names. Adult-onset focal dystonias are considered to be focal manifestations of idiopathic torsion dystonia. The involuntary movements and abnormal postures of focal dystonia also occur in generalized dystonia, and focal dystonias in adults sometimes spread to adjacent body regions to produce segmental dystonia. Examples of
segmental dystonia include the association of blepharospasm with oromandibular dystonia (Meige’s syndrome) and spasmodic torticollis with dystonic writer’s cramp. Adult-onset focal dystonia is far more common than childhood generalized dystonia. The reported prevalence of idiopathic adult-onset dystonia is 295 in 1,000,000, compared with 34 in 1,000,000 for generalized dystonia, but is undoubtedly underestimated in current studies. Recent prevalence estimates have indicated at least 250,000 cases of idiopathic dystonia in the United States. Because in many cases focal dystonia is incorrectly attributed to psychological causes, underdiagnosis is common, and long delays in diagnosis and appropriate treatment result. Dystonia is a syndrome of sustained muscle contractions that cause repetitive torsional movements and abnormal postures.
Chapter 129
need 60 to 100 mg/day but may experience dosage-related drowsiness, confusion, memory difficulty, and hallucinations. Pyridostigmine, a peripherally acting anticholinesterase, and eye drops of pilocarpine (a muscarinic agonist) often ameliorate at least some of the peripheral side effects such as dry mouth, urinary retention, and blurred vision. Many patients need a combination of several medications and treatments. Benzodiazepines (clonazepam or lorazepam) may provide additional benefit for patients whose response to anticholinergic drugs is unsatisfactory. Baclofen may be helpful for oromandibular dystonia but is only minimally effective for generalized dystonia. In selected cases of severe axial and generalized dystonia, however, continuous intrathecal infusions of baclofen may be useful. Dopamine receptor-blocking drugs or neuroleptics (e.g., fluphenazine) have been used to treat dystonia, often in conjunction with anticholinergics. However, the use of dopamine receptor-blocking drugs to treat dystonia should be discouraged because of the potential for development of tardive dyskinesia. This risk may be minimized by coadministering reserpine or tetrabenazine. Tetrabenazine, a presynaptic dopamine-depleting drug, has been useful in some patients with dystonia, but its availability in the United States is limited. Attacks of kinesigenic paroxysmal dystonia may be controlled with anticonvulsants (e.g., carbamazepine, phenytoin), but the nonkinesigenic forms of paroxysmal dystonia are less responsive to pharmacologic therapy, although clonazepam and acetazolamide may be beneficial. Surgical approaches, such as local denervation, muscle excision, and stereotactic procedures such as thalamotomy or globus pallidus deep brain stimulation, play an increasingly important role, particularly in treating generalized dystonia.
Focal Dystonia: Treatment with Botulinurn Toxin
821
Bandman 0, Valente EM, Holmans P et ak Dopa-responsive dystonia: a clinical and molecular genetic study. Ann Neurol 44:649456, 1998
Bressman SB, Sabatti C, Raymond D et al: The DYTl phenotype and guidelines for diagnostic testing. Neurology 54:1746-1 752, 2000 Duffey P, Butler AG, Hawthorne MR, Barnes H: The epidemiology of primary dystonia in the north of England. pp. 121-125. In Fahn S, Marsden CD, DeLong DR (eds): Dystonia 3, Adv Neurol, Vol. 78, pp. 12 1-126. Lippincott-Raven, Philadelphia, 1998 Fahn S, Bressman S, Marsden CD: Classification of dystonia. Adv Neurol 78~1-10, 1998
Hallett M: Physiology of dystonia. Adv Neurol 78:ll-18, 1998 Hewett 1, Gonzalez-Agosti C, Slater D et al. Mutant torsin A, responsible for early-onset torsion dystonia, forms membrane inclusions in cultured neural cells. Hum Mol Genet 9:1404-1414, 2000 Jankovic J: Can peripheral trauma induce dystonia and other movement disorders? Yes! Mov Disord 16:7-12, 2001 Jankovic J: Dystonia: medical therapy and botulinum toxin in dystonia. pp. 169-184. In Fahn S , Marsden CD, DeLong DR (eds): Dystonia 3, Adv Neurol, Vol. 78, pp. 169-184. Lippincott-Raven, Philadelphia, 1998
Jankovic J: Re-emergence of surgery for dystonia. Editorial commentary. J Neurol Neurosurg Psychiatry 65:434, 1998 Jankovic J, Brin M: Botulinum toxin: historical perspective and potential new indications. Muscle Nerve 2O(Suppl 6):S129-S145, 1997 Nemeth A The genetics of primary dystonias and related disorders. Brain 125:695-721, 2002
Nygaard TG, Raymond D, Chen C et al: Localization of a gene for myoclonus-dystonia to chromosome 7q2 1-23. Ann Neurol 46794798, 1999
Swoboda KJ, Soong BW, McKenna C et al: Paroxysmal kinesigenic dyskinesia and infantile convulsions. Clinical and linkage studies. Neurology 553224230, 2000 Vitek JL, Chockkan V, Zhang J-Y et al: Neuronal activity in the basal ganglia in patients with generalized dystonia and hemiballism. Ann Neurol46:22-35, 1999
SUGGESTED READINGS Adityanjee, Yeken AA, Jampala VC, Mathews T: The current status of tardive dystonia. Biol Psychiatry 45:715-730, 1999
Warner TT, Jarman P The molecular genetics of dystonias. J Neurol Neurosurg Psychiatry 64:427429, 1998
129 Focal Dvstonia: Treatment with Botulinum Toxin Daniel Tarsy By contrast with generalized dystonia, which usually begins in childhood (see Chapter 128), adult-onset idiopathic dystonia usually remains localized to one body part without progression or spread to neighboring body regions. Whereas childhood-onset dystonia usually begins in the lower extremities, most adult dystonias begin in muscles of the face, neck, or upper extremities, where they remain focal. Occasionally, dystonia may spread to adjacent body parts to become segmental. Focal dystonias are listed in Table 129-1 with their more common names. Adult-onset focal dystonias are considered to be focal manifestations of idiopathic torsion dystonia. The involuntary movements and abnormal postures of focal dystonia also occur in generalized dystonia, and focal dystonias in adults sometimes spread to adjacent body regions to produce segmental dystonia. Examples of
segmental dystonia include the association of blepharospasm with oromandibular dystonia (Meige’s syndrome) and spasmodic torticollis with dystonic writer’s cramp. Adult-onset focal dystonia is far more common than childhood generalized dystonia. The reported prevalence of idiopathic adult-onset dystonia is 295 in 1,000,000, compared with 34 in 1,000,000 for generalized dystonia, but is undoubtedly underestimated in current studies. Recent prevalence estimates have indicated at least 250,000 cases of idiopathic dystonia in the United States. Because in many cases focal dystonia is incorrectly attributed to psychological causes, underdiagnosis is common, and long delays in diagnosis and appropriate treatment result. Dystonia is a syndrome of sustained muscle contractions that cause repetitive torsional movements and abnormal postures.
822
Movement Disorders W
Non-ParkinsonianMovement Disorders
rn TABLE129-1. Focal Dystonias
CRANIAL DYSTONIA
Dvstonia
Common Names
Cranial dystonia
Blepharospasm Oromandibular dystonia Jaw opening Jaw closing Spasmodic dysphonia Adductor dysphonia Abductor dysphonia Pharyngeal dystonia Lingual dystonia Spasmodic torticollis Writer‘s cramp Occupational cramps Inversion foot dystonia
Cervical dystonia Arm dystonia Leg dystonia
Dystonic movements may either be slow and sustained (tonic) or rapid (clonic), are typically repetitive, and are patterned, by contrast with choreic movements, which are more random and unpredictable, and myoclonus, which is rapid, rhythmic, and unassociated with alterations in posture. In some cases, rapid dystonic movements are difficult to distinguish from myoclonic jerks; therefore, the term myoclonic dystonia has been introduced. Some of these result from voluntary attempts to resist an abnormal posture, such as the patient with torticollis whose head pulls slowly to the right and jerks intermittently to the left. Essential tremor may coexist with focal dystonia to produce an associated tremor of the head and upper extremities. Dystonic movements in primary dystonia are characteristicallymade worse during voluntary movements. Action dystonia refers to involuntary movements that occur only during voluntary use of a group of muscles and are absent at rest. Some are task specific, such as writer’s and other occupational cramp disorders; vocal cord, jaw, or tongue spasms activated by speech; pharyngeal contractions during swallowing; and foot dystonia while walking. As the dystonia progresses, it appears more spontaneously and may be precipitated by movements in other body parts. In severe cases, the dystonia may progress to a permanent fixed posture with or without contractures. Dystonia usually increases with fatigue or stress and improves or is abolished with relaxation and sleep. Some patients acquire sensory tricks or compensatory postures that partially suppress the dystonic movements and postures but complicate the appearance of the movement disorder. Botulinum toxin has radically changed the management of adult-onset focal dystonia; its use in cranial and cervical dystonia is the subject of this chapter. In many cases, botulinum toxin has become the treatment of choice. Botulinum toxin works by inhibiting calcium-dependent acetylcholine release at the neuromuscular junction and has been especially effective in treating oculomotor disorders, blepharospasm, spasmodic dysphonia, and spasmodic torticollis. Botulinum toxin is the treatment of choice in blepharospasm and produces benefit in 70% to 80% of patients. Oromandibular dystonia of the jaw-closing and jaw-opening types benefits from botulinum toxin, but injection requires special attention to anatomic details and, in the case of pterygoid and digastric injections for jaw-opening dystonia, carries the risk of dysphagia. Botulinum toxin is used in spasmodic torticollis after preliminary trials with medication but is increasingly being used as a first-line treatment in this situation as well. Botulinum toxin is also the treatment of choice for spasmodic dysphonia, a condition in which medications and speech therapy are ineffective.
Cranial dystonia is a combination of dystonic movements of the eyelids, face, and jaw that is also known as Meige’s syndrome. Onset usually is between ages 40 and 60 and is more common in women than men. Blepharospasm is the most common manifestation of cranial dystonia and produces involuntary forced closure of the eyelids and increased eyeblink frequency. Differential diagnosis includes secondary forms of blepharospasm caused by neuroleptic drugs, Parkinson’s disease, progressive supranuclear palsy, Wilson’s disease, and lesions of the brainstem. Local irritative disorders of the eyes and eyelids would be expected to cause transient rather than chronic blepharospasm. Blepharospasm is bilateral but sometimes asymmetrical in distribution. Unilateral blepharospasm usually is caused by hemifacial spasm, which is not a dystonia but an irritative disorder of the facial nerve that causes myoclonic facial muscle contractions limited to one side of the face. The contractions of the orbicularis oculi in blepharospasm may be brief, causing repetitive blinking, or persistent, causing prolonged, forced closure of the eyes. Some patients manifest apraxia of eyelid opening, resulting in difficulty opening the eyes in the absence of orbicularis oculi spasm. Driving, bright lights, watching television, and reading are common aggravating factors. During examination, patients often display more prominent blepharospasm while relating their history than while quietly listening or being examined. Sensory tricks used to suppress blepharospasm are limited but may include jaw or neck movements, coughing, chewing gum, or placing a finger or hand near or on the upper lids. Eyebrow lifting and ticlike movements of the lower face and mouth may occur, representing attempts to control the blepharospasm; these movements do not necessarily warrant a diagnosis of Meige’s syndrome. Pharmacologic treatment usually is unsatisfactory but has included anticholinergic drugs, benzodiazepines, baclofen, and tetrabenazine. Surgical interventions such as myectomy and selective facial nerve section have been used with limited success and often produce cosmetically unacceptable facial muscle weakness. Botulinum toxin is the treatment of choice in patients unresponsive to medication and results in significant improvement in a majority of patients in terms of both eyeblink frequency and intensity of blepharospasm. Botulinum toxin is injected in dosages of 2.5 U subcutaneousiyinto the medial and lateral upper eyelid and lateral lower eyelid and intramuscularly into the lateral canthus. The pretarsal portion of the upper lids should be injected in patients with eyelid opening “apraxia.” Diffusion into the middle portion of the upper eyelid must be avoided to prevent levator palpebra weakness. Therapeutic effect usually is evident within several days and lasts approximately 3 months. Unwanted effects include ptosis, ecchymosis, diplopia, ectropion, blurred vision, and dry eyes. Excessive weakness may prevent normal eye closure during sleep and should be managed with appropriate ophthalmic lubrication. Oromandibular dystonia is the second most common manifestation of cranial dystonia. It may occur alone but is often associated with other cranial dystonias such as blepharospasm, lingual or pharyngeal dystonia, or spasmodic dysphonia. Differential diagnosis includes tardive dystonia, edentulous jaw movements, and bruxism. Jaw muscles may be involved asymmetrically or even unilaterally and produce involuntary jaw opening, jaw closing, or jaw deviation. Associated movements of the lower face are common and may include contractions of the platysma, pursing movements of the lips, tongue protrusion, and spasmodic
Chapter 129 H Focal Dystonia: Treatment with Botulinum Toxin
contractions of the mouth and pharynx. Blepharospasm, oromandibular dystonia, and spasmodic movements of the face and neck typically occur synchronously in repetitive and sometimes rhythmic fashion. In early stages, they may be triggered by speaking or chewing; later, they are precipitated by other facial movements; eventually, they become continuous. Oromandibular dystonia produces major disability, including pain, speech impairment, difficulty eating, and trauma to oral and dental structures. Pharmacologic therapy usually is ineffective but, similar to blepharospasm, has included anticholinergic drugs, benzodiazepines, baclofen, and tetrabenazine given alone or in combination. Botulinum toxin has been used with some success in oromandibular dystonia, but administration requires more detailed anatomic knowledge and is more prone to complication caused by spread of toxin than treatment of blepharospasm. Combined management by an otolaryngologist and speech pathologist is strongly recommended. Jaw-closing oromandibular dystonia is technically easier to treat and less often associated with dysphagia. Injections are made into masseter and medial pterygoids and, if necessary, temporalis muscles. Jaw-opening dystonia requires injection into lateral pterygoids and anterior digastrics. Pterygoid injections must be done under electromyographic guidance and usually can be done extraorally by someone experienced in the anatomy of this region. Other muscles usually can be located by palpation but are also best injected under electromyographic guidance. Dosages of botulinum toxin vary widely, and treatment should begin with small dosages titrated according to response over several treatment sessions. Typical dosages for masseter are 25 to 75 U; temporalis, 15 to 75 U; pterygoids, 5 to 50 U; and anterior digastrics, 2.5 to 30 U. Two to three injections are administered per muscle in small volumes per injection to reduce potential for regional spread. Dysphagia is the most common adverse effect and is more common after injection of jaw-opening than jaw-closing muscles. Nasal dysarthria, weakness of chewing, and local pain are other occasional adverse effects. SPASMODIC DYSPHONIA Spasmodic dysphonia, also called laryngeal dystonia, is an action dystonia in which there is involuntary adduction or abduction of the vocal cords activated by speech, resulting in abnormal voice production. Adductor dysphonia accounts for approximately 90% of cases of laryngeal dystonia and consists of involuntary approximation of the vocal cords caused by contraction or tensing of the thyroarytenoid (vocalis) muscles during speech. This results in a characteristic voice disorder in which patients speak in an effortful, strained, and staccato pattern with frequent short breaks in vocalization. In abductor dysphonia, involuntary separation of the vocal cords caused by contraction of the posterior cricoarytenoid muscles produces a characteristic breathy or whispered voice pattern with loss of volume. Some patients with adductor dysphonia compensate for adduction by whispering, whereas in a few patients, adductor and abductor dysphonia coexist, with one predominating over the other in most cases. Spasmodic dysphonia often is misdiagnosed as psychogenic in origin, but there is no evidence to support this view, and patients with spasmodic dysphonia usually can be distinguished from patients with truly psychogenic voice disorders by appropriate otolaryngologicexamination and voice evaluation techniques. Differential diagnosis includes voice tremor as a manifestation of essential tremor, extrapyramidal disorders affecting voice production, structural abnormalities of the vocal cords, and
823
chronic inflammatory vocal cord conditions. Pharmacologic treatment is entirely unhelpful in this disorder and, by contrast with other focal dystonias, is not worth undertaking before the use of botulinum toxin. Vocal therapy techniques may be worthwhile in some cases, especially when there seems to be a nondystonic contribution to the voice disorder. Recurrent laryngeal nerve section can produce relief of symptoms, but adverse effects are common, and follow-up studies have shown a high relapse rate. Surgical techniques designed to relax or tighten the vocal cords are currently under investigation but are too new to assess. Before using botulinum toxin, patients should undergo neurologic, otolaryngologic, and voice evaluation. Fiberoptic laryngoscopy to exclude anatomic abnormalities and to confirm hyperadduction or hyperabduction is desirable. Voice recording and videostrobolaryngoscopy sometimes are indicated to exclude other voice disorders that may be difficult to differentiate from spasmodic dysphonia. Early treatment of spasmodic dysphonia with botulinum toxin used injections of 15 to 30 U into a single vocal cord. However, currently bilateral injections usually are given in a dosage range of 1.5 to 7.5 U per cord. After administration of appropriate local anesthesia, the cricothyroid membrane is penetrated with a 27-gauge electromyographicinjection needle, with the patient in a supine position. The needle is directed 30 degrees laterally and superiorly into the vocal cord. The vocal cord is identified electromyographically by increased spontaneous activity or activation with phonation, and botulinum toxin is injected into one or two sites on each side. In some centers, botulinum toxin has been injected by an indirect laryngoscopic approach, which has the advantage of not requiring electromyographicguidance. An initial dosage of 2.5 to 5.0 U bilaterally is recommended, with the understanding that there is a wide variability in response. Some patients experience insufficient therapeutic effect and need an additional injection, whereas others may experience excessive effect, manifested by a period of breathy or aphonic speech lasting for as long as several weeks. When benefit occurs, it usually appears within several days. The most common adverse effect is breathy speech or aphonia, which dictates future dosage adjustments. Dysphagia is uncommon and usually is limited to subjective difficulty drinking liquids without aspiration. Once the appropriate dosage is determined for individual patients, it should be expected that nearly all patients will experience significant improvement in speech. Duration of benefit is highly variable and ranges between 6 weeks and 6 months, with an average duration of 3 to 4 months. Abductor dysphonia is treated by posterior cricoarytenoid (PCA) or cricothyroid injection. Injection of PCA is more difficult than with thyro-arytenoid injection and requires positioning of the electromyographicallyguided needle posterior to the lamina of the thyroid cartilage. Only one posterior cricoarytenoid muscle is injected at a time because of the risk of bilateral abductor paralysis. Overall success with this method is less than for adductor dysphonia and sometimes requires careful bilateral injections, cricothyroid muscle injection, or thyroplastic procedures.
CERVICAL DYSTONIA Cervical dystonia, also known as spasmodic torticollis, is the most common focal dystonia that comes to medical attention. Secondary forms may result from a variety of orthopedic, neurologic, and infectious disturbances of the craniocervical junction, but most of these occur in children or young adults, are related to
824
Movement Disorders W
Non-Parkinsonian Movement Disorders
obvious underlying causes, and do not produce the characteristic features of idiopathic cervical dystonia as it presents in adults. Like other focal dystonias, cervical dystonia was once believed to be psychogenic in origin, but psychological studies and general clinical experience do not support this view. Onset usually is between ages 30 and 50, and women are affected slightly more often than men. Symptoms usually begin with mild neck stiffness or subtle postural deviations of the head. A small number of patients report neck pain at onset, although with the exception of post-traumatic cases, onset usually is unrelated to immediate antecedent trauma. As the disorder progresses, pain and discomfort become prominent in 75% of patients and usually are localized to the posterior paracervical region and shoulder. Pain is much more prominent than in other focal dystonias and probably is of musculoskeletal or radicular origin. Pain typically is located in the posterior cervical region ipsilateral to the direction of head rotation or head tilt and almost never occurs in the affected sternomastoid muscle. Symptoms of cervical spondylosis and radiculopathy may complicate the clinical picture after several years of persistent cervical dystonia. Several abnormal head postures occur, consisting of various combinations of rotation (torticollis), lateral tilt (laterocollis), hyperextension of the head (retrocollis), and forward flexion (antecollis). Torticollis and laterocollis are the most common postures, whereas pure retrocollis and antecollis are less common in idiopathic cervical dystonia. Retrocollis is particularly common as a manifestation of tardive dystonia caused by neuroleptic drugs. Most patients display a combination of these postures, with the most common head position consisting of rotation of the head to one side with upward deviation of the chin and lateral tilt of the head to the opposite side. Symptoms often increase with fatigue and tend to be worse late in the day. Patients use a variety of sensory tricks, which are usually more effective early rather than later in the course. These begin with a light touch on the chin, but in more severe cases, a hand on the back or side of the neck or head is needed for relief. Head support while lying down usually reduces torticollis, but some patients experience an exacerbation of symptoms when in a reclining position. Some patients gain relief with use of a high-backed chair or recliner and drive with the assistance of a head rest. Fixed deformities, such as sternomastoid hypertrophy and elevation or anterior displacement of one shoulder, may appear with time. Most patients exhibit tonic deviation of the head, but in some cases clonic jerks are prominent. In many cases, these are caused by the patient’s effort to suppress the abnormal posture. Head tremor is common and is caused by dystonic tremor or associated essential tremor. The clinical course usually is one of slow progression over the first several months to years. followed by a static course. Spontaneous but usually temporary remissions have been reported in 5% to 10% of patients and usually occur within 5 years of onset. Most patients with cervical dystonia do not benefit from oral medications. Ordinary muscle relaxants typically are ineffective and have usually been tried before neurologic referral. The drugs of choice for treating cervical dystonia are anticholinergic drugs such as trihexyphenidyl, with which there has been the greatest experience. As many as 20% of patients respond to low or moderate dosages of 4 to 10 mg. Although the percentage of responders is low, the response may be good enough to obviate botulinum toxin treatment. Unfortunately, adverse effects are common even at low dosages and include nausea, dry mouth, drowsiness, visual disturbance, forgetfulness, urinary retention, and glaucoma. Some patients manifest mild choreiform dyskine-
sias that clear after discontinuation of treatment. Sensitivityto side effects in adults usually precludes high-dose anticholinergic treatment. Benzodiazepines such as diazepam, lorazepam, or clonazepam often are helpful for symptomatic pain management but carry the risk of dependency and susceptibility to withdrawal symptoms after chronic use. Baclofen and carbamazepine are of little or no benefit, whereas dopamine receptor antagonists such as haloperidol are contraindicated for chronic use because of risk of tardive dyskinesia. Nonpharmacologic therapies used to treat cervical dystonia have included hypnosis, biofeedback, relaxation techniques, psychotherapy, acupuncture, and braces, but in the majority of cases these are unhelpful. Physical therapy plays a limited role in treating cervical dystonia but is useful as an adjunct to maximize range of motion and for pain management in patients who have partially benefited from other treatments. Currently, patients with cervical dystonia are diagnosed earlier and seek treatment sooner than patients treated in the early years of botulinum toxin therapy. It is important to understand the ways in which cervical dystonia is disturbing because all symptoms or signs are not equally benefited. Involuntary movements and pain are the two major manifestations. Involuntary movements are disturbing because of the jerking head movements, the cosmetic effect produced by postural deformities, difficulties in carrying out routine activities of daily living such as working, driving, reading, and watching television, subjective gait disturbance, fatigue related to constant efforts to suppress the involuntary movements, and head tremor. Chronic pain, social withdrawal, and reactive depression are common consequences. It is worthwhile to review these areas of disability in detail both before and after treatment so that expectations before treatment and gains after treatment can be more readily identified. It is important to understand the anatomy of neck muscles and the way in which abnormal postures relate to contractions of specific cervical muscles (Table 129-2). The need for electromyography to assist botulinum toxin injection of cervical muscles is controversial and depends largely on the skills of the treating physician. Observed abnormal head postures usually can be correlated with a predictable pattern of muscle involvement. Careful observation and analysis of the patient’s posture, involun-
H TABLE 129-2.
Action of Commonly Injected Cervical Muscles
Muscle
Action ~~
~
Sternomastoid
Contralateral rotation lpsilateral tilt Anterior flexion
Trapezius
Shoulder elevation lpsilateral tilt Neck extension
Splenius capitis
lpsilateral rotation lpsilateral tilt Neck extension
Levator scapulae
Shoulder elevation lpsilateral tilt
Scalenus group
lpsilateral tilt Head flexion
Deep postvertebrals (semispinalis, longissimus capitis)
lpsilateral tilt Head extension
Chapter 129 W
tary movements, and voluntary movements, together with palpation of often hypertrophied muscles, usually allows appropriate selection of muscles for injection. Rotational torticollis is produced by the combined effect of sternomastoid contraction rotating the head contralaterally and contraction of ipsilateral posterior cervical muscles-splenius capitis, longissimus capitis, and oblique capitis inferior-rotating the head ipsilaterally. Although some authors include trapezius as a head rotator, it primarily tilts the head ipsilaterally, is extremely thin in the paracervical region, and in most cases does not require injection. Splenius capitis is a much thicker muscle and, in patients with cervical dystonia, often is hypertrophied and easily palpable in the posterior cervical triangle behind and below the mastoid, where it emerges from under the trapezius. In most cases, injection of ipsilateral splenius and contralateral sternomastoid is sufficient, and electromyographyis unnecessary. Because the semispinalis is a posterior cervical muscle that sometimes rotates the head contralaterally, it may be worth injecting this muscle with electromyographic guidance on the side contralateral to head rotation in cases resistant to routine patterns of injection. The oblique capitis inferior is a small and much deeper muscle that cannot be identified without electromyography and may also require injection in some cases. Laterocollis is produced by contraction of the ipsilateral sternomastoid (clavicular more than sternal head), levator scapulae, scalenus muscles, splenius, and trapezius. In this case, electromyographyis useful in estimating the degree to which each muscle contributes to head tilt. In most cases, weakening of ipsilateral sternomastoid, levator scapulae, and splenius is sufficient. Injections into the scalenus group usually are avoided because they are deep, more likely to be associated with dysphagia, and lie in close anatomic relationship to the brachial plexus and lung. Retrocollis probably is the easiest form of cervical dystonia to treat and requires injections into splenius capitis, trapezius, and sometimes deeper posterior cervical muscles such as semispinalis. Side effects are rare and limited to occasional excessive neck extensor weakness. Antecollis often is resistant to treatment with botulinum toxin. Although sternomastoid muscles, scalenes, and platysma contribute to anterior head flexion and are easily injected, the more important prevertebral head flexors, longus colli and longus capitis are more powerful muscles that require special expertise and fluoroscopic and electromyographic monitoring for injection. If electromyography indicates a significant contribution by sternomastoid and scalenes, bilateral injection of these muscles may be considered but is associated with a higher incidence of dysphagia. Typical initial injections into the sternomastoid are 50 to 70 U; splenius capitis, 80 to 100 U; trapezius, 60 to 80 U; levator scapulae, 30 to 50 U; scalenus muscles, 20 to 40 U; and deeper posterior cervical muscles, 80 to 100 U. Women, patients with smaller neck muscles, or patients with previous surgical denervation, and patients given bilateral injections should receive lower dosages to reduce the incidence of dysphagia and excessive neck muscle weakness. Botulinum toxin has been demonstrated to be safe and effective in a number of open and controlled trials. Although subjective improvement sometimes seems to exceed objective measures of benefit, published studies have uniformly shown significant improvement for both abnormal head posture and pain in 60% to 80% of patients. Initial response to treatment should be documented carefully to justify follow-up treatments. The degree of
Focal Dystonia: Treatment with Botulinum Toxin
825
torticollis observed in the examining room may not adequately represent the amount of improvement. Although in many cases improvement in head posture is apparent, family members sometimes are better observers than the patient, who is often less aware of head position. Pain relief, increased range of motion, reduced dystonic tremor, reduction in the need to voluntarily suppress abnormal postures, and resultant improvements in mood are useful indicators of treatment response. The cause of primary resistance is uncertain, but 20% to 25% of patients do not respond to treatment. Patients treated early may respond more favorably than patients with chronic cervical dystonia, possibly because of muscle contractures and fixed postures. A change in the pattern of muscle activity whereby uninjected, deeper posterior cervical muscles develop increased spasm may account for other treatment failures. The use of botulinum toxin in cervical dystonia is remarkably safe. Immediate side effects are limited to occasional small subcutaneous hematomas and rare pneumothorax. When possible, patients should discontinue aspirin for several days before injections. Patients anticoagulated with warfarin with prothrombin times in therapeutic range can be safely injected. Occasional brief pain may occur if the needle encounters the greater occipital nerve in the suboccipital region or the brachial plexus during scalene injection. Later-appearing adverse effects include dysphagia, neck weakness, and new patterns of cervical pain. Dysphagia is uncommon if dosages in sternomastoid muscles are kept below 60 U. Higher injections closer to the mastoid and into the posterior aspect of this muscle also minimize this side effect. When it occurs, dysphagia appears 5 to 6 days after injection and lasts for 2 to 4 weeks. Dysphagia is primarily for solid foods and is easily managed with soft solids or thick liquids and modification of swallowing techniques such as turning the head toward the weak side. Aspiration is possible but is rare in botulinum-induced dysphagia. A modified barium swallow with fluoroscopy may demonstrate unilateral pharyngeal weakness but is not necessary for routine management in most cases. Excessive weakness in neck muscles is uncommon, but patients may experience difficulty elevating the head from a bent position or turning in bed because of excessive posterior cervical muscle weakness. Occasionally, patients experience increased pain at the injection sites or a new distribution of cervical or shoulder pain within the first several weeks of injection. This usually occurs in patients with pretreatment cervical pain and may be caused by new patterns of muscle use and ligamentous stretch. Generalized fatigue, myalgia, and weakness are uncommon and in controlled studies have not exceeded similar effects after placebo. Although single-fiber electromyographic studies may show evidence of neuromuscular blockade in muscles distant from the injection site and minor abnormalities of autonomic cardiovascular reflexes have been demonstrated, clinical manifestations of these laboratory observations have not been apparent. BOTULINUM TOXIN Clostridium botulinum produces seven antigenically distinctive toxins that are all potent paralytic agents. These are designated as A, B, C, D, E, F, and G. These toxins are polypeptides with a molecular mass of 150,000 Da. When the single-chain toxin is cleaved, it yields a dichain molecule in which a heavy chain of about 100,000 Da is linked by a disulfide bond to a light chain of approximately 50,000 Da. In this form, botulinum toxin is capable of producing neuromuscular junction blockade. Botulinum toxin
826
Movement Disorders W
Non-ParkinsonianMovement Disorders
produces weakness by blocking acetylcholine release. The steps involved in this process include binding to the preterminal membrane, internalizing the toxin, and blocking neurotransmitter release. The heavy chain of the toxin is responsible for binding to the presynaptic nerve terminal, whereas the light chain is responsible for blocking acetylcholine release. Botulinum toxin A has been shown to exert its effect by cleaving the synaptic protein SNAP-25, which is a constituent of the synaptic vesicle membrane. As a result of this cleavage, the presynaptic vesicle loses its ability to fuse with the nerve terminal membrane to initiate exocytosis. In animal studies, botulinum toxin has been shown to reach the central nervous system, where it binds to brain synaptosomes. However, the toxin’s clinical effect in botulism or local muscle paralysis after injection is not believed to be caused by central nervous system mechanisms. After injection into a muscle, the toxin diffuses several centimeters from the injection site. Because the radius of spread appears to be determined by the dosage and volume injected, injections of smaller dosages and volumes may reduce spread to adjacent muscles, thereby reducing incidence of unwanted weakness in adjacent muscles. Clinical studies comparing efficacy of multiple and single injections have produced inconsistent results, and it is currently recommended that two to four injections be given into each treated muscle. Long-term effects of intramuscular botulinum toxin have been studied widely in animals but only occasionally in humans. In experimental animals, botulinum toxin causes denervation atrophy, whereas in human studies of orbicularis oculi muscles, atrophy and fibrosis persist up to 4 months after exposure to botulinum toxin. Botulinum toxin produces sprouting of motor axon terminals in both animal and human studies. Some of these sprouts end blindly, whereas others appear to terminate on muscle motor endplates. It is unlikely that axonal sprouting is responsible for recovery of muscular strength after botulinum toxin injection, most histologic studies show incomplete sprouting unlikely to represent functionally effective reinnervation. The dosage of botulinum toxin capable of producing significant systemic toxicity in humans is not known. In monkeys, the median lethal dosage for botulinum toxin A is estimated at 40 U/kg. This would amount to approximately 3000 units in a 75-kg man. The lethal oral dosage is also not known with certainty but has been estimated to be in the vicinity of lo4 to lo6 times the parenteral dosage. In recent years, the appearance of secondary resistance has emerged as an increasing problem in botulinum toxin clinics. It is presumed that many if not all of these cases are caused by the appearance of blocking antibodies to botulinum toxin A. Interestingly, experience with botulism food poisoning has failed to show antibodies to botulinum toxin in surviving patients. Unfortunately, there is no assay for botulinum toxin entirely dependable antibodies. An in vivo mouse neutralization assay is available, and enzyme-linked immunosorbent assay has also been used to detect botulinum antibodies but has not been correlated with the presence of secondary resistance. In several studies, the frequency of detectable botulinum antibodies has been in the range of 3% to 5%, with evidence that increased dosage and reduced interval between injections are related to the presence of antibodies. Botulinum toxin B is now available for treatment of patients who have developed antibodies to Botulinum toxin A. Botulinum toxin should be administered by a physician well acquainted with the diagnosis and treatment of disorders characterized by excessive and inappropriate muscle spasm. It is
important to carefully review the anatomy relevant for the body part being injected. Although not necessary in every case, electromyography often is helpful in using botulinum toxin for cranial and cervical dystonias. Since its introduction into clinical practice, significant adverse effects have been extremely rare. Despite its extreme potency, it is a remarkably safe drug increasingly used to treat spasmodic muscles in a wide variety of body locations. Although there is no information regarding potential adverse effects in pregnancy, it is recommended that botulinum toxin not be used in pregnant or lactating women. Primary muscle disorders such as myasthenia gravis, LambertEaton syndrome, motor neuron disease, and primary myopathies are relative contraindications to the use of botulinum toxin. However, because the amount of toxin that reaches the systemic circulation after local intramuscular injection is minute, this may not necessarily constitute an absolute contraindication in a dystonia for which no other treatment is available.
SUGGESTED READINGS American Academy of Neurology Therapeutics and Technology Assess-
ment Subcommittee: Assessment: the clinical usefulness of botulinum toxin-A in treating neurologic disorders. Neurology 40:1332, 1990 Blasia J, Chapman ER, Link E et al: Botulinum neurotoxin A selectively cleaves the synaptic protein SNAP-25. Nature 365:160, 1993 Blitzer A Botulinum toxin injection for the treatment of oromandibular dystonia. Ann Otol Rhinol Laryngol98:93, 1989 Blitzer A, Brin M F Laryngeal dystonia: a series with botulinum toxin therapy. Ann Otol Rhinol Laryngol 100:85, 1991 Blitzer A, Brin MF, Stuart C et al: Abductor laryngeal dystonia: a series treated with botulinum toxin. Laryngoscope 102:163, 1992 Comella CL, Buchman AS, Tanner CM et al: Botulinum toxin injection for spasmodic torticollis: increased magnitude of benefit with electromyographic assistance. Neurology 42:878, 1992 Conference Report: Clinical use of botulinum toxin. NIH Consensus Development Conference Statement. Arch Neurol 48:1294, 1991 Dutton JJ,Buckley E G Botulinum toxin in the management of blepharospasm. Arch Neurol43:380, 1986 Gifianda P, Vita G, Nicolosi C et al: Botulinum toxin therapy: distant effects on neuromuscular transmission and autonomic nervous system. J Neurol Neurosurg Psychiatry 55:844, 1992 Greene P, Kang U, Fahn S et al: Double-blind, placebo-controlled trial of botulinum toxin injections for the treatment of spasmodic torticollis. Neurology 401213, 1990
JankovicJ, Brin M F Therapeutic uses of botulinum toxin. N Engl J Med 3241186, 1991 Jankovic J, Schwartz KS: Longitudinal experience with botulinum toxin injections for treatment of blepharospasm and cervical dystonia. Neurology 43:834, 1993 Ludlow CL The treatment of speech and voice disorders with botulinum toxin. JAMA 264:2671, 1990 Marsden CD: The focal dystonias. Clin Neuropharmacol9(Suppl2):S49, 1986 Marsden CD: The problem of adult-onset idiopathic torsion dystonia and other isolated dyskinesias in adult life. Adv Neurol 14259, 1976 Schantz EJ, Johnson EA Properties and use of botulinum toxin and other microbial neurotoxins in medicines. Microbiol Rev 56:80, 1992 Sloop RR, Cose BA, Escutin RO: Human response to botulinum toxin injection: type B compared with type A. Neurology 49:189-194, 1997 Zuber M, Sebald M, Bathien N et al: Botulinum antibodies in dystonic patients treated with type A botulinum toxin: frequency and significance. Neurology 43:1715, 1993
Chapter 130
Task-Specific Focal Dystonia
827
130 Task-Specific Focal Dystonia Michael E. Charness
Dystonia is a movement disorder characterized by involuntary, sustained contraction of muscles, resulting in tremor, repetitive movements, or abnormal postures. Focal dystonia affects a single body region, such as the face (Meige’s syndrome), neck (torticollis), or upper extremity (writer’s cramp or musician’s cramp). Task-specific focal dystonia (TSFD) or occupational cramp is a disorder of involuntary movements elicited by the performance of skilled, stereotyped, repetitive movements. Simple cramp is the occurrence of TSFD only during a specific skilled task. Dystonic cramp is the occurrence of TSFD during a variety of related tasks, such as typing, writing, and playing the piano. In some patients, there is progression from simple cramp to dystonic cramp.
EPIDEMIOLOGY Writer’s cramp occurs in approximately 300 patients per million, as determined by analysis of a Mayo Clinic database. A European study estimated a prevalence for writer’s cramp of 14 per million. The true prevalence of musician’s cramp is unknown; however, TSFD is diagnosed in approximately 10% to 15% of patients presenting to performing arts clinics. Several series have confirmed that TSFD is more common among men than among women.
CLINICAL FEATURES The onset of TSFD usually is insidious. Patients with writer’s cramp often describe a clear deterioration in their handwriting without recollection of the precise onset. Similarly, many musicians with TSFD recollect a moment when their playing became particularly troublesome but also recall having some difficulty playing months to years earlier. In musicians, the onset of TSFD precedes the diagnosis by an average of 5 years. TSFD tends to worsen and then stabilize without involving other body segments. About 5% of patients develop TSFD of the contralateral limb. Only rarely is there spontaneous remission, and in many instances TSFD significantly limits or ends the careers of professional musicians. Writer’s cramp is typically painless. Attempts to write produce tightness in the upper extremity, slowness of movements, and a marked degradation of penmanship. In most patients, writing produces involuntary contraction of the flexors of the thumb, index finger, and wrist. Grip may be so forceful that the pencil breaks. Dystonic muscle contraction sometimes leads to tremor. Straining to write for prolonged periods of time sometimes causes muscle tightness and pain in the hand, forearm, arm, neck, and shoulders. In some patients, there is involuntary extension of the index finger or the thumb, causing the pencil to drop. Involuntary movements usually are evident within the first few seconds of writing. In this respect, TSFD differs clearly from the muscle pain, tightness, and occasional cramping that occur commonly after prolonged writing. Patients commonly alter their customary style for gripping the pencil, sometimes with significant improvement. Whereas cursive writing on a horizontal surface may be extraor-
dinarily difficult, cursive writing on a vertical surface, such as a blackboard, may be nearly normal. Many patients with writer’s cramp can type normally. Conversely, many patients with typinginduced cramp can write normally. For high-level musicians, the motor aspects of performance are automatic, and their major focus is on musical interpretation. Often, the first symptom of TSFD in musicians is the uncustomary effort needed to play their instruments. This heightened effort may create the perception that performance has declined, even before the problem is apparent to professional colleagues, critics, or an audience. Over time, patients also note involuntary muscle contraction, tightness in their upper extremities, and a greater deterioration in performance, which then becomes apparent to others. Dystonic movements may occur selectively during certain sequences of finger movement, such as ascending scales but not during descending scales. In other instances, extended hand positions provoke dystonia, causing difficulty playing chords or octaves but not scale passages.
DIAGNOSIS TSFD is diagnosed clinically, based on the history and physical examination. The history is often so characteristic that the diagnosis becomes clear, even before the patient is examined. Brain imaging studies are normal in most patients with TSFD. For patients with TSFD and an otherwise normal physical examination, brain imaging can be omitted. There are no clinically useful electrodiagnostic, biochemical, or genetic tests for confirming the diagnosis. TSFD sometimes occurs early in the setting of Parkinson’s disease or in Wilson’s disease. In patients with writer’s cramp, the involuntary movements are not always evident because the fingers and thumb are fixed around the writing instrument. One often appreciates increased tension in the hand and forearm that commences with writing. More striking is the slow, laborious production of illegible handwriting, sometimes associated with tremor. In mild cases, it is helpful to compare handwriting samples from before and after the onset of symptoms. In musicians, TSFD can be heard as well as seen. There may be a marked degradation of performance, leaving a concert artist sounding like a beginner. In milder cases, the level of performance must be evaluated in relation to the patient’s previous level of accomplishment, based on an occupational history or old recordings. Because the hands are not wrapped around a writing instrument, involuntary movements often are more apparent than in writer’s cramp. Many different patterns of abnormal movement can be appreciated, including flexion of the little and ring fingers, extension of the digits, or flexion of the index finger and thumb (Fig. 130-1). Often there is associated flexion or extension of nearby digits, which patients recognize as compensatory. In selecting muscles for injection with botulinum toxin, it is important to distinguish the primary abnormal movements from the compensatory movements.
828
Movement Disorders
Non-Parkinsonian Movement Disorders
FIG. 150-1. Different patterns of dystonia in three pianists. Top left: flexion of the right little and ring fingers at the PIP joints. Bottom left: extension of the right index finger at the MCP and PIP joints. Bottom right: flexion of the right index finger at the PIP joint and thumb at the IP joint. (From Charness ME, Ross MH, Shefner JM: Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve 19:431-437, 1996, with permission.)
Wind players may develop a TSFD affecting the embouchure, manifesting as lip tremor, tongue protrusion, jaw closure, and elevation or depression of a corner of the mouth. Air leaks may be visible between the lips on one side of the mouthpiece, and there is marked degradation in the quality and articulation of notes. Some patients with task-specific jaw closure develop difficultywith speech or eating. It is essential to observe the affected task in TSFD because physical examination is otherwise normal in most patients. When a piano is not available, tapping on a tabletop can sometimes reproduce dystonic movements. There may be tightness and tenderness of muscles in the shoulder girdle and neck, the result of sustained playing or writing with excessive muscle contraction. There are sometimes signs of nerve entrapment, which may antedate the dystonia or may develop as a result of the sustained abnormal postures and increased muscle tone. In a minority of patients, dystonic movements or tremor are apparent in the outstretched hands. Some patients have a task-specific disorder characterized by tremor rather than sustained muscle contraction. In patients with primary writing tremor, there is little or no tremor of the outstretched hands, but writing produces a high-amplitude 5- to 7-Hz tremor. A similar disorder is observed in musicians, who exhibit tremor while playing their instrument but manifest little tremor otherwise.
PATHOPHYSIOLOGY The hallmark of TSFD is prolonged bursting of co-contraction in agonist and antagonist muscles during the performance of a skilled task. Electromyographic recordings also reveal reduced activation of selective muscles and loss of fine control. Some physiologic abnormalities are apparent in the absence of movement. There is reduced reciprocal inhibition of the H reflex, decreased spinal inhibition, increased cortical excitation, and reduced intracortical inhibition. Frank distortions in the cortical representations of the digits have been identified by brain mapping in patients with TSFD. The distance between the cortical sensory representations of digit pairs is smaller in musicians with TSFD than in nondystonic musicians or in normal controls. There is also fusion of the cortical sensory representation of the digits and inversion of the position of the thumb and little finger representations. These findings are consistent with observations in monkeys that alterations of sensory input can lead to a reorganization of the sensory cortex. Indeed, patients with TSFD show a defect in the discrimination of temporally and spatially related sensory input to the hand. The organization of the motor cortex is also altered in patients with TSFD. TSFD arises primarily in musicians with high levels of skill and develops rarely during the acquisition of the skill. Therefore, TSFD may emerge through a perversion of the plastic neural responses
Chapter 130
that are associated with the learning and rehearsal of highly skilled movements. The rapid, repetitive hand movements involved in executing skilled movement may independently contribute to the development of TSFD by producing peripheral nerve or soft tissue injury, activating sensory pathways that influence motor programs, or changing the local balance of cortical inhibition and excitation. Physiologic studies of patients with TSFD provide evidence for alterations in the planning of movement, the anatomic organization of sensorimotor function, and the integration of sensory information that guides motor processes. Some of these abnormalities are bilateral, even in the presence of unilateral symptoms, and therefore may precede the development of TSFD. Learning an advanced skill is common to all musicians; therefore, additional factors must account for the development of TSFD in a minority. TSFD occurs with increased frequency among first-degree relatives of patients with Oppenheim’s dystonia (DYTl). One reported family had multiple affected members with writer’s cramp and mutations in the DYTl gene. A study of 18 consecutive musicians with TSFD did not reveal any with mutations in the DYTl gene. A majority of musicians develop TSFD in the setting of nerve entrapment, soft tissue injury, learning of a second musical instrument, stress, or alterations in musical technique. These conditions may independently alter sensorimotor representation within the nervous system. Many musicians with dystonic flexion of the little and ring fingers have an ipsilateral ulnar neuropathy. In some, the severity of the dystonia and the ulnar neuropathy fluctuate in parallel. Interestingly, patients with ulnar neuropathy and no TSFD show the same pattern of co-contraction in agonist and antagonist muscles as patients with TSFD. Although patients with isolated ulnar neuropathy have reduced reciprocal inhibition of the H reflex and decreased spinal inhibition, they do not exhibit the increased cortical excitation observed in patients with TSFD. What triggers the transition from ulnar neuropathy to TSFD is unknown. ~~
TREATMENT Treating TSFD is difficult, and success is inversely proportional to the need for neuromuscular perfection. Only a few world-class musicians with TSFD have regained top concert form. A larger number of musicians with TSFD have improved sufficiently to enlarge their repertoire and increase their range of playing and teaching opportunities. Treatment of embouchure dystonia in wind players has been particularly frustrating, with few successes. Small improvements in TSFD result in larger functional gains for writers than for musicians; therefore, treatment of writer’s cramp often is more successful than treatment of musician’s cramp. The ubiquity of computers and the decreased need for writing in many jobs has also decreased the burden of writer’s cramp and the need for treatment. Voice-activated input software provides an occupational alternative for patients with typist’s cramp. Rest alone is rarely helpful in TSFD. Musicians have returned to playing after as long as 5 years of rest without any improvement in their TSFD. One drummer did recover completely after 25 years of rest, but this is hardly a viable option for most patients. Approximately 10% of patients benefit from anticholinergic medications; however, these are poorly tolerated and rarely used for long periods of time. A small proportion of my patients have found gabapentin to be mildly helpful. Hypnotherapy, biofeed-
Task-Specific Focal Dystonia
829
back, and occupational therapy are modestly successful in some patients. Changes in hand position, ergonomics, and instrument redesign can be beneficial. Fat pens and writing devices are clearly helpful for some patients with writer’s cramp. The use of gloves, splints, or elastic bands fastened around a finger sometimes produces improvement, perhaps by altering sensory feedback, but benefits rarely endure. Instrument redesign has enabled some musicians to continue performing. One musician redesigned his flute to largely eliminate a focal dystonia that was triggered by placing the left index finger on the instrument. Plastic “figure-8” rings can limit involuntary flexion of individual digits and are useful adjuncts in selected patients. Several highly motivated musicians have experienced substantial improvement in TSFD after motor retraining. These retraining programs involve the complete avoidance of dystonic playing and the slow rehearsal of nondystonic playing, often with the assistance of visual imagery. Improvement occurs over months to a few years, during which time patients are unable to engage in professional performance. Many patients with writer’s cramp learn to write with the nondominant hand. Between 10% and 25% of these patients develop dystonia in the nondominant writing hand. Constraint-induced movement therapy involves applying splints that limit movement to one digit at a time. Patients are encouraged to practice their instruments while splinted in an attempt to reverse the fusion of sensorimotor maps and regain independence of finger movement. Enthusiasm for this approach has not survived early reports of success. Limb immobilization and sensory discrimination training have also been used to correct the abnormal sensory maps of patients with TSFD. Several uncontrolled trials in small series of patients have yielded promising results, but these findings need to be replicated. Injection of subparalyzing dosages of lidocaine can improve TSFD for several days, perhaps by reducing the Ia afferent input from muscle spindles, which contributes to TSFD. This approach is not practical for most patients. Slow repetitive transcranial magnetic stimulation of the motor cortex transiently improves writer’s cramp, but a practical clinical application has not yet been described. Some patients with ulnar neuropathy and dystonic flexion of the little and ring fingers have experienced improvement in their dystonia after treatment of their ulnar neuropathy. Surgical correction of an ulnar neuropathy is a reasonable consideration when TSFD and ipsilateral ulnar neuropathy do not respond to conservative measures. The selective weakening of dystonic muscles with botulinum toxin produces transient improvement in a majority of patients with TSFD. However, when followed for several years, a majority of patients discontinue treatment because of insufficient response, expense, or poor access to a qualified provider. The goal of treatment is to produce sufficient weakness to prevent dystonic contraction without also compromising the task. Patients with dystonic contraction of a small number of easily identified muscles are better candidates for injection than those with complex patterns of dystonia. There is clearly less latitude for excessive weakness in musicians than in writers because musical performance is readily degraded by mild weakness. Even the targeted level of weakness may compromise musical performance. Botulinum toxin injection does not address several physiologic abnormalities in TSFD, including the failure of certain muscles to contract and the spread of contraction to multiple adjacent muscles. Nonetheless, in carefully selected patients, the improve-
830
Movement Disorders
Non-ParkinsonianMovement Disorders
ment from botulinum toxin injection can sometimes be striking, even if not complete. For upper extremity dystonia, botulinum toxin is injected through a hollow electromyographic needle after anatomic and physiologic localization of the target muscle. Weakness develops over a few days to a week. It is helpful to assess patients 2 weeks after the first injection to evaluate the therapeutic response and the pattern and magnitude of weakness. An injection may be unsuccessful because it produces too much or too little weakness in the targeted muscles. Spread of toxin to adjacent, nontargeted muscles occurs in a majority of cases and may also compromise the therapeutic response. Botulinum toxin reduces the release of acetylcholine at the neuromuscular junction, leading to chemodenervation of the target muscle. The resulting weakness, whether beneficial or excessive, is always reversible within 1 to 6 months; therefore, injections must be repeated several times annually. Injection of botulinum toxin also causes a functional reorganization of the motor cortex, suggesting an additional mechanism of action. In a minority of patients with TSFD, repeated injection of botulinum toxin leads to the development of neutralizing antibodies, with progressive blunting of the therapeutic response.
By1 NN, McKenzie A Treatment effectiveness for patients with a history of repetitive hand use and focal hand dystonia: a planned, prospective follow-up study. J Hand Ther 13:289-301,2000 Candia V, Elbert T, Altenmuller E et ak Constraint-induced movement therapy for focal hand dystonia in musicians. Lancet 353:42, 1999 Charness ME, Ross MH, Shefner JM: Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve 19:431437, 1996 Elbert T, Candia V, Altenmuller E et ak Alteration of digital representations in somatosensory cortex in focal hand dystonia. Neuroreport 9~3571-3575, 1998 Friedman JR, Klein C, Leung J et ak The GAG deletion of the DYTl gene is infrequent in musicians with focal dystonia. Neurology 55:14171418, 2000 Frucht SJ, Fahn S, Greene PE et al The natural history of embouchure dystonia. Mov Disord 16:899-906,2001 Marsden CD, Sheehy MP Writer’s cramp. Trends Neurosci 13:14&153, 1990 Newmark J, Hochberg FH: Isolated painless manual incoordination in 57 musicians. J Neurol Neurosurg Psychiatry 50:291-295, 1987 Priori A, Pesenti A, Cappellari A et ak Limb immobilization for the treatment of focal occupational dystonia. Neurology 57:405-409, 2001 Ross MH, Charness ME, Sudarsky L, Logigian E L Treatment of occupational cramp with botulinum toxin: diffusion of toxin to adjacent noninjected muscles. Muscle Nerve 20593-598, 1997
SUGGESTED READINGS Bain PG, Findley LJ, Britton TC et ak Primary writing tremor. Brain 118:1461-1472, 1995
13 1 Tics and Tourette’s Syndrome Frederick 1. Marshall and Roger Kurlan
In 1885, Georges Gilles de la Tourette began cataloging and organizing movement disorders at the suggestion of his mentor, Jean Charcot. Having earlier translated Beard’s article on the peculiar “Jumping Frenchmen of Maine,” the 28-year-old Tourette struck out to find evidence of their progenitors on the wards of the Salpetriere in Paris. Instead, he came on a small group of patients who suffered from multiple motor and vocal tics. Of the nine patients described in his original article, five suffered from scatologic outbursts, a symptom that provoked them to selfimposed social isolation and prompted generations of physicians, including Charcot himself, to presume a psychiatric cause for the disorder. The syndrome of Gilles de la Tourette, now properly called Tourette’s syndrome, has captured the imagination of clinicians ever since. It was not until the 1960s, however, that Tourette’s syndrome emerged from its status as a rare curiosity. With the introduction of haloperidol treatment and the demonstration that chronic motor and vocal tics could be suppressed medically, the disorder became the concern of neurologists as well as psychiatrists. More than any other advance, the success of neuroleptic treatment placed Tourette’s disorder firmly in the center of an emerging understanding of the links between brain and behavior.
DEFINITION, PHENOMENOLOGY, AND NATURAL HISTORY
Despite compelling evidence of its hereditary nature and of the genetic link with a spectrum of other neurobehavioral disorders such as obsessive-compulsive disorder and attention deficit hyperactivity disorder (ADHD), there remains no disease-specific biologic marker for Tourette’s disorder. Therefore, the diagnosis of Tourette’s disorder rests on recognition of its characteristic signs and symptoms. The Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria include the presence of both multiple motor tics and one or more vocal tics at some time during the illness (not necessarily concurrently); duration longer than 1 year, during which time there is no tic-free interval longer than 3 months; onset before age 18; marked distress or significant impairment in social, occupational, or other important areas of functioning; and absence of possible confounding agents or conditions (e.g., stimulants, Huntington’s disease, postviral encephalitis). The remaining primary tic disorders include chronic tic disorder and transient tic disorder. The former differs from Tourette’s syndrome in that either motor or vocal tics (but not
830
Movement Disorders
Non-ParkinsonianMovement Disorders
ment from botulinum toxin injection can sometimes be striking, even if not complete. For upper extremity dystonia, botulinum toxin is injected through a hollow electromyographic needle after anatomic and physiologic localization of the target muscle. Weakness develops over a few days to a week. It is helpful to assess patients 2 weeks after the first injection to evaluate the therapeutic response and the pattern and magnitude of weakness. An injection may be unsuccessful because it produces too much or too little weakness in the targeted muscles. Spread of toxin to adjacent, nontargeted muscles occurs in a majority of cases and may also compromise the therapeutic response. Botulinum toxin reduces the release of acetylcholine at the neuromuscular junction, leading to chemodenervation of the target muscle. The resulting weakness, whether beneficial or excessive, is always reversible within 1 to 6 months; therefore, injections must be repeated several times annually. Injection of botulinum toxin also causes a functional reorganization of the motor cortex, suggesting an additional mechanism of action. In a minority of patients with TSFD, repeated injection of botulinum toxin leads to the development of neutralizing antibodies, with progressive blunting of the therapeutic response.
By1 NN, McKenzie A Treatment effectiveness for patients with a history of repetitive hand use and focal hand dystonia: a planned, prospective follow-up study. J Hand Ther 13:289-301,2000 Candia V, Elbert T, Altenmuller E et ak Constraint-induced movement therapy for focal hand dystonia in musicians. Lancet 353:42, 1999 Charness ME, Ross MH, Shefner JM: Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve 19:431437, 1996 Elbert T, Candia V, Altenmuller E et ak Alteration of digital representations in somatosensory cortex in focal hand dystonia. Neuroreport 9~3571-3575, 1998 Friedman JR, Klein C, Leung J et ak The GAG deletion of the DYTl gene is infrequent in musicians with focal dystonia. Neurology 55:14171418, 2000 Frucht SJ, Fahn S, Greene PE et al The natural history of embouchure dystonia. Mov Disord 16:899-906,2001 Marsden CD, Sheehy MP Writer’s cramp. Trends Neurosci 13:14&153, 1990 Newmark J, Hochberg FH: Isolated painless manual incoordination in 57 musicians. J Neurol Neurosurg Psychiatry 50:291-295, 1987 Priori A, Pesenti A, Cappellari A et ak Limb immobilization for the treatment of focal occupational dystonia. Neurology 57:405-409, 2001 Ross MH, Charness ME, Sudarsky L, Logigian E L Treatment of occupational cramp with botulinum toxin: diffusion of toxin to adjacent noninjected muscles. Muscle Nerve 20593-598, 1997
SUGGESTED READINGS Bain PG, Findley LJ, Britton TC et ak Primary writing tremor. Brain 118:1461-1472, 1995
13 1 Tics and Tourette’s Syndrome Frederick 1. Marshall and Roger Kurlan
In 1885, Georges Gilles de la Tourette began cataloging and organizing movement disorders at the suggestion of his mentor, Jean Charcot. Having earlier translated Beard’s article on the peculiar “Jumping Frenchmen of Maine,” the 28-year-old Tourette struck out to find evidence of their progenitors on the wards of the Salpetriere in Paris. Instead, he came on a small group of patients who suffered from multiple motor and vocal tics. Of the nine patients described in his original article, five suffered from scatologic outbursts, a symptom that provoked them to selfimposed social isolation and prompted generations of physicians, including Charcot himself, to presume a psychiatric cause for the disorder. The syndrome of Gilles de la Tourette, now properly called Tourette’s syndrome, has captured the imagination of clinicians ever since. It was not until the 1960s, however, that Tourette’s syndrome emerged from its status as a rare curiosity. With the introduction of haloperidol treatment and the demonstration that chronic motor and vocal tics could be suppressed medically, the disorder became the concern of neurologists as well as psychiatrists. More than any other advance, the success of neuroleptic treatment placed Tourette’s disorder firmly in the center of an emerging understanding of the links between brain and behavior.
DEFINITION, PHENOMENOLOGY, AND NATURAL HISTORY
Despite compelling evidence of its hereditary nature and of the genetic link with a spectrum of other neurobehavioral disorders such as obsessive-compulsive disorder and attention deficit hyperactivity disorder (ADHD), there remains no disease-specific biologic marker for Tourette’s disorder. Therefore, the diagnosis of Tourette’s disorder rests on recognition of its characteristic signs and symptoms. The Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria include the presence of both multiple motor tics and one or more vocal tics at some time during the illness (not necessarily concurrently); duration longer than 1 year, during which time there is no tic-free interval longer than 3 months; onset before age 18; marked distress or significant impairment in social, occupational, or other important areas of functioning; and absence of possible confounding agents or conditions (e.g., stimulants, Huntington’s disease, postviral encephalitis). The remaining primary tic disorders include chronic tic disorder and transient tic disorder. The former differs from Tourette’s syndrome in that either motor or vocal tics (but not
Chapter 131 H Tics and Tourette‘s Syndrome
both) must be present for more than 1 year. Transient tic disorder differs from both chronic tic disorder and Tourette’s syndrome in that symptoms must be of less than 1 year’s duration. It is now widely suspected that these disorders exist on a continuum of severity; the underlying genetic defect in Tourette’s syndrome expresses itself in milder form as chronic or transient tic disorder. There are also a number of secondary causes of tics. Tics may occur in hereditary neurologic disorders such as Huntington’s disease, the neurocutaneous syndromes, dystonia musculorum deformans, and neuroacanthocytosis. Perinatal encephalopathy, stroke, head trauma, carbon monoxide poisoning, and central nervous system infections (e.g., encephalitis lethargica, Sydenham’s chorea) have all been reported as causes of tics. Drugs that have been implicated include anticonvulsants (carbamazepine, phenobarbital, and phenytoin), cocaine, psychostimulants, and levodopa. The antipsychotics themselves may cause tardive tics. Among the hyperkinetic movement disorders, tics may be differentiated on several grounds. In addition to being abrupt in onset and duration, they are characterized by a tendency to spontaneously fluctuate, to be multifocal and migratory, and to be at least temporarily suppressible. Often, the patient may describe premonitory symptoms of a sensory nature, such as a “tickle” or “urge:’ which are then relieved by the movement itself. Tics tend to increase during times of stress. To the extent that they are suppressed for any length of time, however, tics generally reemerge in force once the patient relaxes. The physical and emotional burden of suppressing tics often is overwhelming, and patients describe a feeling of exhaustion attendant on efforts to keep their tics from emerging. Most patients say their tics tend to become less severe during intense concentration on or distraction by some other activity. Tics may be subdivided into simple and complex types and motor and vocal forms. Simple motor tics are defined as abrupt contractions of a single muscle group, such as eye blinking, head jerking, or wrist flicking. By contrast, complex motor tics involve the coordinated contractions of a series of muscle groups. The resultant movements may take on an almost purposeful appearance, as exemplified by touching or stroking behaviors, dancelike movements, or copropraxia (obscene gestures). Vocal tics may be thought of as a particular variety of motor tic involving contractions of the laryngeal, pharyngeal, respiratory, or oronasal musculature. Simple vocal tics are inarticulate noises that do not convey meaning. Examples include snorting, grunting, barking, and clicking. Complex vocal tics generally are words or fragments of words. Despite the emphasis placed upon coprolalia (obscene speech) as a symptom of Tourette’s syndrome, less than 20% of patients ever suffer from this symptom. Although it is perhaps the most socially stigmatizing manifestation of Tourette’s syndrome, most patients may be reassured that the symptom, if it occurs, tends to be transitory. Many patients with Tourette’s syndrome demonstrate a tendency to repeat their own words (palilalia) or the last words that they hear (echolalia). Similarly, they may mimic or copy the gestures and movements of others (echopraxia). These behaviors may be manifestations of the underlying tic disorder or may blend into the realm of obsessive-compulsive disorder. One important means of differentiating complex tics from compulsions is to question the patient about the meaning, if any, he or she ascribes to the behavior. Whereas tics are not associated with any preformed ritualistic set of notions about their significance, compulsions invariably are. For example, compulsive acts often are performed according to specific rules, such as repeating acts a
831
certain number of times or in a particular order. Complex motor tics, on the other hand, do not have such ritualistic qualities. Tourette’s syndrome and the related primary tic disorders generally have their onset in the childhood years. As many as 20% of school-aged children develop some sort of transitory tic. These are often ignored by the family and other care providers or are attributed to the passing mannerisms of a “childish” nature. Estimates of the lifetime risk of full-blown Tourette’s syndrome vary widely, but a likely assessment would be 30 to 100 cases per 100,000 people. There is a 3:l ratio of males to females with the syndrome. It occurs in all races and socioeconomic classes. The clinical picture is uniform across cultural groups, save for a decreased incidence of coprolalia among Japanese. The most likely location for the initial tic to present is the face and eyes, with decreasing incidence of tics occurring in a rostral-caudal fashion throughout the remainder of the body. Approximately 12% to 37% of people with Tourette’s syndrome present with simple vocal tics (eg., throat clearing) as the initial symptom, with far fewer presenting with complex vocal tics. A number of studies have established the long-term prognosis of the disorder. When tics alone are considered, the general consensus is that approximately one third of patients will enjoy complete remission by late adolescence or early adulthood. Another one third will have a significant decrease in both the amount and severity of their tics. The final one third of patients will remain symptomatic throughout early adulthood and middle age. Little is known about Tourette’s syndrome in older adults. The most famous of Tourette’s original patients, the Marquise de Dampierre, is said to have lived out her life in seclusion, dying at age 86. However, collective experience indicates that tics and obsessive-compulsive disorder tend to diminish with advanced age.
RELATED DISORDERS The genetic association between Tourette’s syndrome and obsessive-compulsive disorder is now widely accepted. Approximately 50% of patients with Tourette’s syndrome suffer from symptoms of obsessive-compulsive disorder. Typical compulsions relate to ritualistic cleaning and grooming behaviors (e.g., hand washing, showering, teeth brushing), ordering and arranging objects, checking and rechecking objects in the environment (e.g., locks, switches, electrical outlets, stoves), counting, hoarding, and repeating certain actions (e.g., walking though a doorway, touching a piece of furniture). Common obsessions include fear of contamination, fear of thinking evil or sinful thoughts contrary to one’s religion, fear of losing potentially vital objects or loved ones, recurring thoughts of doing harm to self or others, and recurring sexual thoughts and images that are ego-dystonic. Evidence for the hypothesis that obsessive-compulsive disorder is an alternative expression of the genetic trait for Tourette’s syndrome comes from family studies demonstrating an increased incidence of obsessive-compulsive disorder among first-degree relatives of Tourette’s syndrome probands. Segregation analyses of Tourette’s syndrome families implicate a major gene inheritance pattern with variable expression of Tourette’s, obsessivecompulsive, and chronic tic disorders. There appears to be a gender-specific penetrance of these traits, with males showing almost complete penetrance when considering Tourette’s and chronic tic disorders alone. Females, on the other hand, show a lower penetrance for Tourette’s and chronic tic disorders alone,
832
Movement Disorders H Non-Parkinsonian Movement Disorders
increasing to about 70% when obsessive-compulsive disorder is added. Between 20% and 60% of children with Tourette’s syndrome have symptoms compatible with a diagnosis of ADHD, including decreased attention span, poor impulse control, difficulty concentrating, and hyperactivity. Indeed, the symptoms of ADHD often predate the onset of tics, prompting treatment with stimulant medications that may trigger or worsen the underlying tic disorder. The association between ADHD and Tourette’s syndrome is generally less well documented than that between obsessivecompulsive disorder and Tourette’s syndrome. Some family studies demonstrate that ADHD segregates separately from Tourette’s syndrome; in any event, an etiologic relationship is difficult to establish with certainty. In addition to ADHD and obsessive-compulsive disorder, patients with Tourette’s syndrome often suffer from other comorbid behavioral difficulties, including depression, anxiety, and conduct disorder. Personality characteristics such as irritability, argumentativeness, and impulsivity all may occur, either as a part of the disorder itself or as a reaction to it.
TREATMENT Tourette’s syndrome is multifaceted, necessitating an individualized assessment and treatment plan for each patient. In general, one or another aspect of the disorder emerges as most troublesome. One patient may find that the tics are disabling, whereas another may be incapacitated by obsessive fears. Once identified, the patient’s primary problem may be specifically targeted. It is important to bear in mind that most patients with Tourette’s syndrome have only mild to moderate symptoms. Such patients typically are well adapted to their social, educational, and family environments and may ideally avoid medication altogether. If interventions are to be made, they are often most useful in the context of a restructured environment. This is particularly true in the case of school, where patients may benefit from such simple measures as supportive counseling, self-paced learning, one-onone tutorials, and small group teaching. We regard the home as a place of refuge where it is not necessary for the patient to expend energy in the taxing effort to suppress tics. Family and individual supportive counseling may be of benefit here as well. Treatment with medications should be reserved for patients with disabling symptoms, as defined with regard to maladaptations in home, work, or school environments. A large variety of agents are available for the treatment of tics, obsessive-compulsive symptoms, attention deficit, hyperactivity, and other related behavioral disorders (Table 131- 1). Agents must be selected on the basis of target symptoms and potential side effects. Dosages should be titrated slowly, seeking the least amount of drug that is both effective and tolerable. Haloperidol was introduced as a highly effective tic-suppressing agent in the late 1960s. Before its introduction, clinicians tended to view Tourette’s syndrome as a psychological disorder. The remarkable response rate (75% to 80%) forced a new understanding of the syndrome in terms of a derangement in brain dopaminergic systems. With the more recent clarification of the link between obsessive-compulsive disorder and Tourette’s syndrome, this formulation has expanded to include serotonergic models as well. The major action of the neuroleptics in tic suppression is thought to rest on their blockade of dopamine D2 receptors. The antipsychoticagent clozapine, with its predominant
TABU 151-1. PharmacologicTreatments of Tourette’s Syndrome Problem
Anent
Tics
Clonidine, guanfacine Atypical antipsychotics Neuroleptics Tetrabenazine, reserpine Other drugs Botulinum toxin injections (for dystonic tics) Selective serotonin reuptake inhibitors Clonidine, guanfacine, rnethylphenidate
Obsessive-compulsive symptoms Attention deficit hyperactivity disorder
action at the D4 receptor, has not been effective in patients with Tourette’s syndrome previously responsive to haloperidol. Although haloperidol is an effective medication for Tourette’s syndrome, it is important to avoid the reflexive use of this agent. We favor starting at a very low dosage, 0.25 mg nightly, and working up slowly by 0.25 to 0.5 mg every 4 to 7 days until symptoms are relieved or side effects appear. Most patients respond at dosages of 5 mg/day or less. We prefer not to exceed 15 mg/day. In an effort to avoid the worst effectsof sedation, we aim for a single bedtime dosing schedule. Motor side effects of haloperidol include acute dystonic reactions, drug-induced parkinsonism, akathisia, and tardive dyskinesia. In addition, patients may develop disabling drowsiness, depression, increased appetite with attendant weight gain, and school and social phobias. Pimozide is the only neuroleptic currently marketed specifically to treat Tourette’s syndrome. It has been shown to be as effective as haloperidol for suppressing tics. The motor side effect profile is similar to that of the other neuroleptics, including haloperidol, fluphenazine, and trifluoperazine. Like the latter agents, however, pimozide may be less sedating than haloperidol. Any of these neuroleptics can be used satisfactorily to suppress tics. The most serious potential side effect of pimozide is prolongation of the Q-T interval. There are rare reports of sudden death at dosages greater than 60 mg/day (which is much higher than the dosages typically used to treat tics). An electrocardiogram should be obtained before starting this medication, and it should be monitored during the period of dosage adjustment. Patients may begin treatment at 1.0 mg (one half tablet) nightly. Medication should be slowly titrated to achieve the minimum effective dosage. Maximum recommended dosage for pimozide is 0.2 mg/kg/day, generally not greater than 10 mg/day. A newer class of antipsychotic drugs has become available that have more variable actions at dopamine receptor subtypes and generallyappear to have a lower risk of extrapyramidal side effects. Because of their more favorable side effect profile, these atypical antipsychotics often are used before the classic neuroleptic antipsychotics for tic control. The following atypical agents appear to be effective tic suppressants: risperidone (0.25 to 10 mg/day), olanzapine (2.5 to 15 mg/day), and ziprasidone (20 to 160 mg/day). The Q-T interval on the electrocardiogram should be monitored during treatment with ziprasidone. A number of nonantipsychotic tic-suppressing agents have gained adherents among clinicians treating patients with Tourette’s syndrome. In general, these agents are less reliably effective than the neuroleptics, but their side effect profiles are favorable, so they are often used as first-line agents.
Chapter 131
The centrally acting antiadrenergic agent clonidine has been used extensively for tic suppression, and a recent double-blind study has confirmed its efficacy. The comorbid occurrence of behavioral difficulties often prompts consideration of clonidine therapy because this agent is also effective for treating ADHD. Side effects include drowsiness, orthostatic symptoms, headache, and irritability. Acute withdrawal may lead to rebound hypertension, agitation, and tachycardia. Effects of treatment may take up to 3 months to manifest. Clonidine is started in dosages of 0.05 mg (one half a tablet)/day and gradually increased until thrice-daily dosing is achieved. Dosages generally do not exceed 0.5 mg/day total. A transdermal delivery system, Catapres-TTS (Boehringer Ingelheim, Ridgefield, CT), allows dosing once a week and is useful in children who find it difficult to swallow pills. The patches come in sizes of 3.5, 7.0, and 10.5 cm2 (corresponding to 0.1, 0.2, and 0.3 mg/day). Another drug with pharmacologic effects similar to clonidine is guanfacine, and it has the advantages of single daily (bedtime) dosing and causing less sedation. The dosage range is 0.5 to 4 mg/day. Other agents that have been reported to have a role in tic management include clonazepam, reserpine, tetrabenazine, and the calcium channel blockers. Case reports of carbamazepine, lithium, corticosteroids, estrogens, and clomiphene have been conflicting. Trials of the opiate antagonist naloxone have not confirmed earlier reports of success with this agent. Local intramuscular injections of botulinum toxin can be used to treat patients with painful dystonic (consisting of muscle tightening or twisting) tics. Treatment of obsessions and compulsions associated with Tourette’s syndrome has rested primarily on the use of serotonin reuptake inhibitors. A variety of such drugs are available, including clomipramine, fluoxetine, sertraline, fluvoxamine, paroxetine, and citalopram. Treatment of ADHD has been dominated by the use of stimulants. The most common medication prescribed is methylphenidate, which has been shown superior to dextroamphetamine and pemoline in comparative studies. Side effects include agitation, insomnia, headaches, anorexia, weight loss, and lowered seizure threshold. Although psychological dependence can occur with long-term use of high-dose methylphenidate, it has not been reported in children treated for ADHD. This agent is contraindicated in patients with glaucoma. The typical dosage range for methylphenidate is 0.1 to 0.3 mg/kg two or three times a day. New long-acting forms of methylphenidate are available (Concerta, Metadate CD) that allow single morning dosing. A recent double-blind, placebo-controlled study does not support earlier concerns that methylphenidate worsens tics. In fact, in this study tics actually lessen over time after the introduction of methylphenidate. Whether other forms of stimulants can worsen tics has not been assessed.
Tics and Tourette’s Syndrome
833
Attractive alternatives to stimulant medications are clonidine and guanfacine, which appear to be effective against both tics and ADHD. We often use these drugs as first-line agents for youngsters with Tourette’s syndrome whose school performance is impaired by hyperactivity and attention problems. As noted earlier, patients with Tourette’s syndrome often suffer from poor interpersonal relationships on the basis of behavior disturbances. These may range from simple character traits such as defensiveness and argumentativeness to full-blown personality disorders. The underlying link between these problems and Tourette’s syndrome is difficult to establish with certainty. Whether they are specific to Tourette’s syndrome or merely a result of the emotional, social, and personal difficulties associated with living with the disease is not well understood. In any case, these behavior disturbances have proven extremely difficult to treat with medications. Rather, a coordinated approach, involving supportive counseling, family therapy, and school and community interventions, appears most useful. As always, it remains important to maintain a low threshold of suspicion for depression, which can be difficult to assess in children.
SUMMARY Tourette’s syndrome represents one end of the spectrum of primary tic disorders. Recognition of the clinical heterogeneity of the syndrome has been a major advance in recent years and has enabled a more rational approach to therapy based on targeting dominant symptoms. With knowledge that Tourette’s syndrome is inherited has come hope that the underlying genetic defect will soon be unraveled.
SUGGESTED READINGS Bruun RD, Budman CL The natural history of Tourette’s syndrome. Adv Neurol 58:1, 1992 Cohen DJ, JankovicJ, Goetz CG (eds): Tourette syndrome. Adv Neurol 85,2001 JankovicJ: Diagnosis and classificationof tics and Tourette syndrome.Adv Neurol 58:7, 1992 Kurlan R (ed): Handbook of Tourette’s Syndrome and Related Tic and Behavioral Disorders. Marcel Dekker, New York, 1993 Kurlan R Tourette’ssyndrome: current concepts. Neurology 39:1625, 1989 Leckman JF, Cohen DJ (eds): Tourette’s Syndrome. Tics, Obsessions, Compulsions. Wiley, New York, 1999 Shapiro AK, Shapiro ES, Young JG,Feinberg TE (eds): Gilles de la Tourette Syndrome. 2nd Ed. Raven Press, New York, 1988 Tourette Syndrome ClassificationStudy Group: Definitions and classification of tic disorders. Arch Neurol 50:1013, 1993 The Tourette’s Syndrome Study Group: Treatment of ADHD in children with tics. Neurology 58:527, 2002
034
Movement Disorders W
Non-Parkinsonian Movement Disorders
132 Mvoclonus 4
fiona Molloy and Mark Hallett Myoclonus is not a diagnostic term but rather a descriptive one. It refers to a neurologic symptom or sign and is nonspecific with regard to neuroanatomic source, pathogenesis, or underlying cause. Myoclonic movements are involuntary and manifest as brief, unexpected shocklike jerks of an area of the body. Myoclonus can arise from any level of the central nervous system (CNS) including the cortex, basal ganglia, brainstem, and spinal cord. Myoclonic movements may consist of a simple jolt of a muscle group or may be sufficiently forceful to make a whole limb move vigorously. Myoclonus may occur in isolation, in the absence of other neurologic or systemic manifestations, and as a normal phenomenon such as in the hiccup. Although myoclonic movements usually are not associated with a loss of consciousness, myoclonus may occur in conjunction with epilepsy and in such situations can be considered a fragment of a seizure. Both a quick, forceful muscular contraction (“positive” myoclonus) or, less commonly, a sudden lapse of muscular tone (“negative”myoclonus or asterixis) may be experienced, or both may be present. Negative myoclonus may be one sign of CNS electrophysiologic instability accompanying toxic metabolic encephalopathy; myoclonus also often occurs after cardiorespiratoryarrest (postanoxic myoclonus). The diagnosis of myoclonus has important clinical, prognostic, and therapeutic implications. DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS Differential diagnosis and treatment of myoclonus often pose a challenge to the neurologist. When myoclonus is suspected, a comprehensivehistory and physical examination should be carried out. Clinical history should carefullydetermine onset,t’imecourse, drug or toxin exposure, history of seizures, past or current medical problems, mental status changes, and family history. The neurologic examination should include movement distribution, temporal profile, and activation characteristics. Distribution can be focal, multifocal, segmental, or generalized. The temporal profile may be continuous or intermittent, rhythmic or irregular. If intermittent, myoclonus can occur sporadically or in trains. The activation of myoclonus may be at rest (spontaneous), induced by various stimuli (reflex myoclonus), induced by voluntary movement (action myoclonus), or the result of a combination of these factors. All activation characteristics should be noted as absent or present. The frequency and regularity of the myoclonic movements can vary from once a month, as in early morning myoclonic seizures, to continuous jerking over months, as in epilepsia partialis continua. Suspected myoclonic movements may be enhanced by certain maneuvers. For example, action myoclonus is enhanced by moving the body part, facial myoclonus by closing the eyes or showing the teeth, and upper extremity myoclonus by either postural movement or most prominently by kinetic movements such as finger-nose-finger maneuver. Somatosensory stimuli such as stretching the fingers or tapping on any part of the affected limb may elicit reflex myoclonus.
Myoclonus can mimic many other abnormal movements such as tics, chorea, tremor, dystonia, or disorders of the peripheral nervous system such as fasciculations. Although tics may be as brief in duration as myoclonic movements, there are several distinguishing features; for example, tics usually are stereotyped movements resulting from the need to move. These movements may be partially suppressed by the patient and are thought to be triggered by “psychic tension” that dissipates after the movement has been made. The involuntary movements of chorea may produce muscle jerking, but the characteristic slower movements and irregular flow from one part of the body to another often help differentiate chorea from myoclonus. Tremor is the most common differential for rhythmic myoclonus; however, tremor’s characteristic sinusoidal rhythmicity helps distinguish it from a myoclonic movement. Disorders arising in the peripheral nervous system that can be confused with myoclonus include fasciculations, myokymia, and hemifacial spasm; however, electrophysiologicstudies can be particularly helpful with the diagnosis in such situations because they show characteristic findings with needle electromyography. Myoclonus may exist concurrently with other involuntary movement disorders in the same patients. For instance, some families with essential tremor and myoclonus have been described, myoclonus and dystonia are combined in inherited myoclonic dystonia, and both action and reflex myoclonic jerks may be present in patients with Huntington’s chorea.
CLASSIFICATION Numerous systems have been used to classify myoclonus. Three of the most succinct and commonly used approaches rely on classifying the condition according to clinical characteristics, etiologic factors, and physiologic mechanisms. Clinical Characteristics
Myoclonic movements may be classified according to a wide range of clinical characteristics, including location, rhythm, relationship to movement, and precipitating or eliciting stimuli. The whole body, or most of it, may be affected in a single jerk (generalized myoclonus). Many different parts of the body may be affected, not necessarily at the same time (multifocalmyoclonus), or myoclonus may be confined to one particular region of the body (focal or segmental myoclonus). Myoclonic jerks may occur repetitively (as in palatal myoclonus) or irregularly and unpredictably (as in propriospinal myoclonus). Myoclonus may be evident at rest, on maintaining a posture, or on movement (action myoclonus). Jerks may be triggered by external stimuli (reflexmyoclonus), which can be visual, auditory, or somatesthetic (touch, pinprick, muscle stretch). Asterixis is the most common form of negative myoclonus and can be demonstrated by asking the patient to extend the arms and wrists in a sustained posture. When asterixis is present, wrist extension is suddenly inhibited and the hands flap. Negative myoclonus can also involve muscle groups in the lower extremi-
Chapter 132
ties, giving rise to the classic bouncy gait that can lead to frequent falls. Electrophysiologically, asterixis consists of silent electromyographic (EMG) discharges, usually lasting 50 to 200 msec, resulting in a brief loss of antigravitational activity and postural control. Negative myoclonus can have a physiology similar to cortical myoclonus with electrophysiologic correlates and may be induced by sensory stimulation. Asterixis is particularly significant because the phenomenon often is associated with a toxic or metabolic encephalopathy. Negative myoclonus tends to be treatment resistant. EUologic Factors
For the therapeutic purposes, it is important to establish the cause of myoclonus to determine a reversible or partly treatable cause. Myoclonus can be associated with many neurologic disorders and is seen with structural or metabolic lesions of the spinal cord, brainstem, and cerebellum and occasionally in normal individuals. Physiologic Classifkation
An underlying cause is not always evident. Therefore, in many clinical situations, physiologic classification of myoclonus can be more advantageous. This approach guides symptomatic treatment by determining the site and mechanism of origin of the symptoms, precipitating factors, and pathways of spread. Different myoclonic disorders, with markedly varying causes, genetic susceptibilities, and prognostic implications may fall into the same physiologic group, sharing homogeneous electrophysiologic properties that usually point to common physiologic abnormalities. The physiologic classification of myoclonus divides the condition broadly into two main groups: epileptic (cortical origin) and nonepileptic (subcortical origin, including structures such as basal ganglia, brainstem, and spinal cord) types. Epileptic myoclonic movements originate in the sensorimotor cortex and are propagated via the corticospinal tract. Epileptic myoclonus may manifest as isolated muscle jerks or repetitive focal myoclonic jerks, as in epilepsia partialis continua, or may be one of multiple seizure types within an epileptic syndrome. Photic cortical myoclonus originates in a hyperexcitable motor cortex and is driven by a normal-appearing occipital response. Seizures may well occur together with epileptic myoclonus, and the disorder often is idiopathic. Most myoclonic jerks of cortical origin are accentuated by action and sensory stimulation. Physiologic characteristicsof epileptic myoclonus include EMG burst length of 10 to 50 msec, agonists and antagonists usually firing synchronously, and an electroencephalogram (EEG) correlate. Based on neurophysiologiccharacteristics, epileptic myoclonus is further classified into three subtypes: cortical reflex myoclonus, reticular reflex myoclonus, and primary generalized epileptic myoclonus. Like other types of myoclonus, cortical reflex myoclonus is not disease specific. Cortical reflex myodonus manifests as brief muscle jerks, representing a fragment of focal or partial epilepsy, and can be provoked by sensory stimulation. Myoclonusrelated activity may not be recognized on conventional EEG. Jerk-lockedEEG or back-averaging (averaging the EEGs backward in time with respect to the myoclonus) is a helpful electrophysiologic technique to localize myoclonus of cortical origin. The EEG shows a focal positive-negative event over the sensorimotor cortex contralateral to the jerk, preceding both spontaneous and reflexinduced myoclonic jerks. Giant somatosensory evoked potentials (SEPs) are common in cortical myoclonus. Stimuli generating
rn
Myoclonus
855
giant SEPs often provoke a subsequent EMG burst of myoclonic activity (the C-reflex) at a latency compatible with conduction through fast corticomotoneuron pathways from the motor cortex to muscle. After a cortical potential, activation propagates in a rostrocaudal direction so that contraction of facial muscles (masseter [fifthcranial nerve] before the orbicularis oculi [seventh cranial nerve]) is followed by contraction of the muscles in the neck, arms, trunks, and legs in descending order. Reticular reflex myoclonus arises in the reticular formation and represents a type of generalized epileptiform activity. The jerky movements usually are generalized, favoring proximal more than distal and flexor more than extensor muscle groups. Voluntary action and sensory stimulation tend to increase the jerking. Electrophysiologic characteristics of this disorder are as follows: EMG bursts occur, lasting 10 to 30 msec and triggered by sensory stimulation or by action; the EEG correlates, when present, are not time-locked to the muscle activation; and the EMG activity begins in the neck muscles and travels up the brainstem and down the spinal cord. Postanoxic myoclonus has been extensively studied neurophysiologically and can feature both cortical and reticular reflex myoclonus. Clinically, there are both multifocal and generalized jerks, and physiologic studies should reveal features of both disorders. Primary generalized epileptic myoclonus is a fragment of primary generalized epilepsy. There are two well-described clinical presentations: focal jerks often involving only the fingers, called minipolymyoclonus; and generalized synchronous whole-body jerks not unlike those seen with reticular reflex myoclonus. The EEG correlate is a slow, bilateral, frontocentrally predominant negativity similar to the wave of a primary generalized paroxysm.
SPECIAL ENTITIES Epileptic Myoclonus Epileptic myoclonus refers to epilepsies characterized exclusively or predominantly by brief myoclonic, atonic, or tonic seizures. Epileptic myoclonus can be positive or negative in type. Disorders classified within this group include infantile spasms, LennoxGastaut syndrome, cryptogenic myoclonic epilepsy, myoclonus associated with petit mal, and juvenile myoclonic epilepsy of adolescence. Of these conditions, juvenile myoclonic epilepsy is the most common epileptic syndrome presenting with myoclonus, usually in adolescence. The main symptom is myoclonic jerks, usually without loss of consciousness, predominantly in the morning after awakening from sleep. Generalized tonic-clonic seizures also tend to occur in the morning. Linkage studies suggest that a gene on chromosome 6 is involved in juvenile myoclonic epilepsy, at least in some families. Progressive Myoclonus Epilepsy
Progressive myoclonus epilepsy (PME) is a group of neurodegenerative diseases characterized by progressive encephalopathy, myoclonus (spontaneous, action, and stimulus sensitive),generalized tonic-clonic and other seizures, dementia, and ataxia. The differential diagnosis of PME includes several rare childhoodonset metabolic conditions, including sialidosis (cherry red spot myoclonus syndrome), mitochondrial encephalopathy (such as myoclonic epilepsy and ragged red fibers), Lafora body disease, Unverricht-Lundborg disease, and neuronal ceroid lipofuscinosis (Batten’s disease). Myoclonic movements associated with PME are most pronounced on movement.
as6
Movement Disorders W
Non-Parkinsonian Movement Disorders
Progressive myoclonic ataxia (Ramsay-Hunt syndrome) sometimes is distinguished from PME by mild or absent seizures and minimal or nonexistent dementia; myoclonus and ataxia are the major problems. The myoclonus associated with this disorder often is stimulus sensitive.
diarrhea, fever, and sweating. This syndrome has been reported after treatment with tryptophan, monoamine oxidase inhibitors, selective serotonin reuptake inhibitors, and tricyclic antidepressants, alone or in combination. Basal Ganglia Disease
The myoclonus observed in Creutzfeldt-Jakob disease, a clinical hallmark of the encephalopathy, can occur at rest or be exacerbated by action or a stimulus. EEG reveals a characteristic pattern of periodic sharp wave complexes in the majority of patients. Myoclonus is also seen in patients with the AIDS dementia complex. Patients with Alzheimer’s disease may exhibit myoclonus, which typically occurs late in the illness and can present as stimulus-induced multifocal distal jerking. Myoclonus is also a feature of some childhood retardation syndromes, including Rett syndrome and Angelman syndrome. In both disorders, the myoclonus is cortical in origin. Metabolic Encephalopathies Including Endocrine Disorders
Disorders such as hepatic failure, renal failure, hyponatremia, hypoglycemia, and nonketotic hyperglycemia can give rise to myoclonus. Treatment should be directed to the underlying condition. For example, myoclonus in patients with chronic renal failure on hemodialysis can be caused by aluminum toxicity and can be treated successfully with chelation therapy with desferrosamine mesylate. A progressive neurologic disorder including ataxia and myoclonus has been reported with coeliac disease. The neurologic syndrome is dominated by action and stimulus sensitive myoclonus of cortical origin, often associated with ataxia and infrequent seizures. The condition may progress despite strict adherence to diet, and no treatment is known. The opsoclonus-myoclonus syndrome (dancing eyes-dancing feet syndrome) can have a variety of symptomatic causes, of which idiopathic and paraneoplastic are the most common. There are clinical and etiologic differences between adult and pediatric presentations. About half of the pediatric cases have an underlying neuroblastoma. In adults, opsoclonus and myoclonus may occur in brainstem encephalitis, whether inflammatory or paraneoplastic. Whipple’s disease may also be associated with a similar clinical picture. An autoimmune origin seems likely because there is a distinctive pattern of serum immunoglobulin M (IgM) and IgG binding to neural tissues and antigens. Symptoms respond to steroids or adrenocorticotropic hormone. Multifocal action myoclonus is the most common form of myoclonus associated with this syndrome. Toxic Encephalopathies Including Drug Side Effects A wide variety of drugs and toxins may provoke multifocal and
generalized myoclonus, as may organ failure. Among drugs, antidepressants (particularly the selective serotonin reuptake inhibitors), anesthetics, anticonvulsants (particularly at toxic levels), withdrawal of benzodiazepines and propranolol, lithium, monoamine oxidase inhibitors, and levodopa can all cause myoclonus. Among toxins, bismuth, heavy metals, glue, and gasoline sniffing can cause myoclonus. Myoclonus is prominent in the serotonin syndrome together with confusion, agitation,
Myoclonus is a rare clinical feature of Parkinson’s disease. Myoclonic movements are more common in multiple-system atrophy in which the involuntary movements are cortical in origin with enlarged SEPs, and the distribution is asymmetrical or focal. Myoclonic jerks, both action and stimulus sensitive, are prominent, characteristic features of corticobasal degeneration. The myoclonus is of cortical origin and stimulus sensitive with a short latency that may be helpful in differential diagnosis. Myoclonus may also be a feature of Huntington’s disease, Wilson’s disease, and, less commonly, Hallervorden-Spatz disease. Hereditary dentatorubral-pallidoluysianatrophy is transmitted as an autosoma1 dominant trait and manifests with myoclonus, epilepsy, cerebellar ataxia, choreoathetosis, and dementia. The myoclonus associated with this disorder often is stimulus sensitive. Postanoxic Myoclonus
Postanoxic myoclonus, originally described by Lance and Adams in 1963, occurs in patients after cerebral anoxic insult. The acute posthypoxic period may be dominated by generalized myoclonus. Generalized myoclonic status epilepticus in the first few days after the insult carries a very grave prognosis, and these patients often die. If patients recover, the characteristics of the myoclonus are altered, and generalized jerks are replaced with spontaneous, action-induced and stimulus-sensitive myoclonus restricted to the limbs. In addition to action myoclonus, Lance and Adams described cerebellar ataxia, postural lapses, gait disturbance, and generalized seizures. Long-term follow-up studies have shown that myoclonus, neurologic abnormalities, and disability improve over time. Gait disturbance (bouncy gait) caused by postural lapses in the trunk and lower extremities is the most disabling feature and most resistant to treatment. Electrophysiologic studies have shown cortical reflex myoclonus in most cases, but exaggerated startle response or reticular reflex myoclonus may also occur. The site of the responsible lesion in the brain is not clear, but there does appear to be a disorder of serotonin metabolism, a speculation supported by both the therapeutic response to 5-hydroxytryptophan and by the normalization of decreased cerebrospinal fluid levels of 5-hydroxyindoleacetic acid following successful therapy. Focal CNS Damage
The cause of focal cortical myoclonus can be almost any type of focal cortical lesion; tumors, angiomas, and encephalitis should be suspected. Curiously, particularly in patients with epilepsia partialis continua, the cortex can appear normal histologically. Surgical excision of the excitable tissue has cured the myoclonus in several patients, and this approach should be considered. Nonepileptic Myoclonus
Nonepileptic myoclonus implies that the neuronal discharge originates subcortically in structures between the cortex and spinal cord. Electrophysiologic studies help to differentiate between
Chapter 132 W
epileptic myoclonus and nonepileptic myoclonus. In nonepileptic myoclonus, EMG bursts are longer (40 to 300 msec), and the antagonist muscle activity is synchronous or asynchronous. Because of its subcorticalnature, there is no EEG correlate, and the SEPs, even during active jerking, do not show large-amplitude responses. Some myoclonic jerks represent a normal physiologic phenomenon, such as sleep jerks (hypnic jerks) and hiccup. Essential myoclonus manifests as a nonprogressive multifocal myoclonus. With a few possible exceptions, other neurologic deficits are absent. The condition may be inherited as an autosomal dominant trait, presenting in the first or second decade with a benign course, although most cases are sporadic. The distribution of muscles affected may be focal, segmental, generalized, or multifocal. Myoclonic movements associated with this condition often are induced or aggravated by action but may also occur spontaneously. In some patients, the physiologic abnormality is that of action-induced ballistic EMG bursts with inappropriate overflow into other muscles. In some families described with essential myoclonus, there are manifestations of dystonia; some individuals have both, others have either myoclonus or dystonia. The myoclonus in such families may respond to alcohol and is therefore called alcohol-sensitive myoclonic dystonia. In other families, both essential myoclonus and essential tremor are found together and independently. Exaggerated startle syndrome (hyperekplexia) is characterized by an abnormal exaggerated motor response or jump in response to an unexpected sensory stimulus (auditory, somatesthetic, or visual). The startle can vary from a blink with contortion of the face to an actual jump resulting in a fall to the ground. There is no associated loss of consciousness. An exaggerated startle syndrome may be caused by local brainstem pathology (anoxia, inflammatory lesions including sarcoidosis and multiple sclerosis, and hemorrhage) and also can occur as an inherited condition (hereditary hyperekplexia) transmitted as an autosomal dominant trait. Hyperekplexia must be distinguished from startle-evoked epileptic seizures, a condition associated with congenital focal cerebral lesions. In response to startle, there is a tonic spasm of the contralateral side followed by a complex partial seizure. Nocturnal myoclonus encompasses a variety of myoclonic conditions that can occur during drowsiness or sleep. Physiologic forms include the hypnic jerk, and pathologic forms include isolated periodic movements in sleep, restless legs syndrome with periodic movements in sleep, and excessive fragmentary myoclonus in NREM sleep. Periodic movements in sleep are commonly present in the sleep disorder laboratory, and the diagnosis is facilitated by the characteristic EMG pattern. The EMG bursts are of the tonic type, lasting 500 to 2000 msec, occurring every 10 to 30 seconds, and are most prominent in the tibialis anterior muscles. These movements tend to occur in NREM sleep but can also appear in drowsiness when the patient is conscious of the movement. Segmental myoclonus may arise in the spinal cord or brainstem. Simple spinal segmental myoclonus usually is a secondary phenomenon; the underlying cause should be determined and treated appropriately. Lesions of the spinal cord that may lead to muscle jerks include infection, degenerative disease, tumor, cervical myelopathy, and demyelinating disease. Such movements may also follow spinal anesthesia or the introduction of contrast media into the cerebrospinal fluid. Movements consist of focal, repetitive rhythmic jerks confined to one or more adjacent spinal segments. Spinal myoclonus usually is unaffected by sleep. Another type of spinal myoclonus is propriospinal myoclonus,
Myoclonus
837
which also arises in the spinal cord and involves many spinal segments linked by long propriospinal pathways. The cause is not always clear, although a focal spinal cord lesion occasionally is found. Clinically the disorder is characterized by nonrhythmic repetitive axial jerks, which usually start in the abdominal muscles and spread up and down the trunk. The jerks can be spontaneous or stimulus induced. Diagnosis is confirmed using EMG studies, which classically show the myoclonus originating in the midthoracic region and spreading slowly (about 5 mhecond) in both a rostra1 and caudal direction. Palatal myoclonus, also commonly called palatal tremor, manifests as rhythmic palatal movements. Palatal myoclonus comprises two separate disorders: essential palatal tremor, where an ear click is a prominent feature, and symptomatic palatal tremor, which is associated with cerebellar disturbances. The ear click described in essential palatal tremor is caused by rhythmic contractions of the tensor veli palatini (innervated by trigeminal nerve). The pathophysiology of essential palatal tremor is unknown, and investigations including magnetic resonance imaging of the brain typically are normal. In symptomatic palatal tremor, a focal brainstem lesion may be identified (usually vascular, traumatic, encephalitic, neoplastic, or demyelinating). The underlying pathology interrupts the pathway between the red nucleus, inferior olive, and dentate nucleus. The resulting denervation of the contralateral inferior olive leads to its hypertrophy, which can be visualized on magnetic resonance imaging. In this case, the palatal movement is caused by contractions of the levator veli palatini (innervated by the nucleus ambiguus). Myoclonus may also be psychogenic in origin. Certain features that help establish the psychogenic nature include clinical symptoms and signs inconsistent with “organic” myoclonus, evidence of underlying psychopathology (particularly marked anxiety), and the presence of an incongruous sensory deficit or inconsistent weakness. Physiologic investigation may reveal the presence of a Bereitschaftspotential before EMG bursts on jerk-locked backaveraging of the EEG, which is associated with a voluntary movement. More than 50% of patients have been reported to improve after gaining insight into the psychogenic mechanisms of their movement disorder. TREATMENT
Myoclonus can be a disabling condition, and treatment is largely empirical because few well-controlled double-blind studies of antimyoclonic agents have been performed, and clinical ratings of the effectiveness of treatment have been mostly descriptive. Once the likely cause and neuroanatomic origin of a patient’s myoclonus are established, therapy should be initiated. Resolution of an underlying encephalopathy or withdrawal of an offending drug or toxin may result in partial or total resolution of the myoclonus. In cases where a reversible cause cannot be identified, pharmacologic intervention is the treatment of choice. Many of the drugs used to treat cortical myoclonus have anticonvulsant properties (Table 132-1) and usually act by enhancing y-aminobutyric acid inhibitory activity. Clinical response may be more robust when two or three drugs are combined. One practical approach to treating cortical myoclonus is to initiate therapy with sodium valproate and, if there is no response, to add clonazepam. If symptom relief is not adequate, piracetam may then be added. Although piracetam has antimyoclonic activity (particularly useful in cortical myoclonus) and is well tolerated at dosages up to 24 @day,its mechanism of action is
838
Movement Disorders rn Non-Parkinsonian Movement Disorders
TABU132-1. Approach to the Drug Treatment of Myoclonus Treatment
Dosage Range (mg/day)
Cortical Myoclonus Clonazepam Valproate Piracetam Primidone Acetazolamide Lisuride (photic myoclonus) L-5-Hydroxytryptophan
0.5-20 1200-2000 1200-1 6,000 500-750 up to 200 1-2 up to 3000*
Reticular Myoclonus Clonazepam Valproate
0.5-20 750-2000
Segmental Spinal Myoclonus Clonazepam Trihexyphenidyl Tetrabenazine
0.5-20 u p to 35 50-200
Essential Myoclonus Benztropine Sumatriptan Phenytoin
4-9 Up to 6 mg (subcutaneously) 250-325
Nocturnal Myoclonus Clonazepam LevodoDa Pergolide
0.5-20 UD to 300 0.'125-0.25
*In combination with a peripheral aromatic amino acid decarboxylase inhibitor (such as carbidopa 100 to 300 muday). Not available in the United States; its usefulness is limited by poor tolerabilii.
unclear. Piracetam is one of the most widely used antimyoclonic agents in Europe. However, this drug is not available in the United States. Primidone and acetazolamide may also be effective as adjunctive therapies in severely affected cases. Not all antiepileptic medications are antimyoclonic, and some, such as phenytoin or carbamazepine, may even exacerbate myoclonus, as described in PME resulting from Unverricht-Lundborg disease. Efficacy of newer anticonvulsants such as vigabatrin, gabapentin, and lamotrigine remains to be established. However, both vigabatrin and gabapentin may paradoxically worsen some types of myoclonus. The extent of symptomatic control achieved in patients with epileptic myoclonus usually is striking at the beginning of treatment, but long-term responses can vary. Both the antioxidant N-acetylcysteine and alcohol have been reported to display potent antimyoclonic activity in Unverricht-Lundborg disease. Negative myoclonus often is resistant to drug therapy, and, as a result, disabling postural lapses in antigravity leg muscles usually are prominent, resulting in the typical bouncy unsteady stance and gait, often with falls. Reticular, spinal, and other segmental myoclonus usually responds best to clonazepam. Adjunctive treatment may include baclofen, serotonin reuptake inhibitors, and 5-hydroxytryptophan (a serotonin precursor) either alone or with a peripheral decarboxylase inhibitor. The risk of a potentially lethal eosinophiliamyalgia syndrome greatly limits the use of 5-hydroxytryptophan. Essential myoclonus sometimes improves with alcohol, a P-blocker such as propranolol, or an anticholinergic agent such as trihexyphenidyl. Dopamine depleters such as tetrabenazine may also have an adjuvant role. Treatment with alcohol should be
avoided because of the potential for abuse, and patients may experience a rebound of symptoms upon cessation of drinking. The ear click in essential palatal myoclonus is the symptom necessitating therapy. Several drugs such as clonazepam, tryptophan, carbamazepine, trihexyphenidyl, flunarizine, and sumatriptan may be useful. Botulinum toxin injections to the tensor velum palatini may successfully treat the ear click, although excess weakness of the soft palate may result. This technique should be used only by skilled physicians who have undergone specialist training in this procedure. The goal of treatment for restless leg syndrome is to reduce the symptoms and improve the quality of sleep. Clonazepam and temazepam have been shown to be effective in treating periodic movements of sleep. Opiates, direct dopamine agonists, and levodopa have also been shown to be worthwhile. An evening dose of a dopamine agonist such as pergolide is first-line treatment in patients with nocturnal myoclonus and restless legs syndrome. Clonazepam and valproic acid should be the first line of therapy in patients with posthypoxic myoclonus. If symptoms do not improve with these agents, 5-hydroxytryptophan may tried, although its side effect profile limits its practical use. Piracetam is particularly helpful for patients with documented cortical myoclonus. Adrenocorticotropic hormone is indicated for treating infantile myoclonic epilepsies, and corticosteroids and immunoglobulins are indicated for treating opsoclonus-myoclonus.
SUGGESTED READINGS Berkovic SF, Andermann F, Carpenter S,Wolfe LD: Progressive myoclonic epilepsies: specific causes and diagnosis. N Engl J Med 315:29&305, 1986 Brown P, Thompson PD, Rothwell JC et ak Axial myoclonus of propriospinal origin. Brain 114197-214, 1991 Deuschl G, Tor0 C, Valls-Sol6 J et al: Symptomatic and essential palatal tremor. 1. Clinical, physiological, and MRI analysis. Brain 117:775788, 1994 Earley CJ, Yaffee JB, Allen Rp: Randomized, double-blind, placebocontrolled trial of pergolide in restless legs syndrome. Neurology 51:1599-1602, 1998 Hallett M: Myoclonus and myoclonic syndromes. pp. 2717-2723. In Engel J Jr, Pedley TA (eds): Epilepsy: A Comprehensive Textbook. Vol. 3. Philadelphia, Lippincott-Raven, 1997 Koskiniemi M, Van Vleymen B, Hakamies L et ak Piracetam relieves symptoms in progressive myoclonus epilepsy: a multicentre, randomised, double blind, crossover study comparing the efficacy and safety of three dosages of oral piracetam with placebo. J Neurol Neurosurg Psychiatry 64344-348, 1998 Lance JW, Adams RD: The syndrome of intention or action myoclonus as a sequel to hypoxic encephalopathy. Brain 8 6 1 11-136, 1963 Obeso JA, Artieda J, Rothwell JC et al: The treatment of severe action myoclonus. Brain 112:765-777, 1989 Obeso JA, Rothwell JC, Marsden C D The spectrum of cortical myoclonus: from focal reflex jerks to spontaneous motor epilepsy. Brain 108:193224, 1985 Shibasaki H: Electrophysiological studies of myoclonus. Muscle Nerve 23~321-335, 2000 Werhahn KJ, Brown P, Thompson PD, Marsden CD: The clinical features and prognosis of chronic posthypoxic myoclonus. Mov Disord 12:216-220, 1997
839
Chapter 133 H Movement Disorders in Sleep and Restless Legs Syndrome (Ekbom’s Syndrome)
133 Movement Disorders in Sleep and Restless Legs Syndrome (Ekbom’s Syndrome) H
Bruce Ehrenberg
Thomas Willis, in 1685, was the first to describe patients troubled by restless leg movements, and he noted that they often had insomnia. Ekbom published a series of articles about restless legs syndrome (RLS) in the 1940s. Symonds described abnormal twitches during sleep-“nocturnal myoc1onus”-which he distinguished from “common nocturnal jerks.” The latter are now called sleep onset myoclonus, hypnic jerks, or sleep starts and are considered normal, as are the twitches of various skeletal muscles without synchrony, periodicity, or symmetry usually seen during rapid eye movement (REM) sleep. Symonds’s patients with nocturnal myoclonus all had insomnia, and at least one patient had periodic arousals at 1-minute intervals, consistent with the modern definition of periodic limb movements disorder of sleep (PLMD; this term has replaced nocturnal myodonus). The current definition allows for the fact that patients present with hypersomnia, although cause-effect ties are unproven. Lugaresi et al. were first to polygraphically record periodic leg movements in sleep from patients with PLMD. They recorded similar nocturnal phenomena from patients with RLS, thus indicating that these two disorders may be physiologically linked. His group also studied the sleep manifestations of various other forms of pathologic myoclonus and found that spinal myoclonus and facial spasms often persist during sleep, cortically mediated epileptic myoclonus (rhythmic jerks of epilepsia partialis continua, repeated partial motor seizures of Jacksonian epilepsy, and spasm of subacute sclerosing leucoencephalitis) gradually decreases with onset of sleep, and movements of extrapyramidal origin (choreoathetosis,hemiballismus) or subcortical and brainstem origin (palatal myoclonus, opsoclonus) reliably disappear in sleep. Nevertheless, nocturnally these disorders must be carefully differentiated from PLMD, as should the myoclonic manifestations of Alzheimer’s and Creutzfeldt-Jakob disease. Likewise, the fasciculationsof amyotrophic lateral sclerosis and other diseases of the anterior horn cell or lower motor neuron, which are mediated at the spinal cord level and do not disappear in sleep. The REM behavior disorder is a nocturnal syndrome with movements ranging from fragmentary myoclonus to gross body movements during REM sleep, often involving widespread motion of limbs in an acting-out fashion, as though the patient were physically involved in a dream; this may be seen in an idiopathic form or with degenerative disorders such as olivopontocerebellar degeneration or more often as an early premonitory indication of idiopathic Parkinson’s disease and may be related to a loss of the generalized motor inhibition normally found in human REM sleep. The tremor of Parkinson’s disease diminishes or stops during sleep. However, periodic leg movements of sleep (PLMS) are common in Parkinson’s patients, and this was originally thought to be a direct effect of levodopa treatment. However, the PLMs are active through the night, and considering the short half-life of the levodopa used in the early studies, it is likely that most of the observed movements occurred after the dopaminergic effects had worn off. Indeed, levodopa is now a useful treatment for the leg
TABU133-1. Movement Disorders and Sleep TvDe of Movement
Tremor (essential or Parkinson’s) Choreoathetosis(including Huntington’s) Hemiballismus Spinal myoclonus Palatal myoclonus and epileptic myoclonus Opsoclonus Epilepsia partialis continua Other sleep-related epilepsy Spasms of subacute sclerosing panencephalitis Torsion dystonias Paroxysmal nocturnal dystonia Rapid eye movement behavior disorder Periodic limb movements disorder Restless legs syndrome Sleepwalking (somnambulism) Sleep bruxism (teeth-grinding) Fragmentary non-REM myoclonus Benign neonatal sleep myoclonus Sleep starts Rhythmic movement disorder [head-bannind
NREM
REM
Awake
-
+ +
f
-
+ + + + +
* f
f
+
Rare ?
f
f
-
+
-
+
f
+
+ -
Rare Rare f + (normal) Rare Rare
movements of RLS and PLMD. Similarly, dopaminergic blockers such as chlorpromazine or haloperidol are known to cause worsening of RLS (and probably of PLMD as well). The question as to whether there is an increased prevalence of PLMD or RLS in Parkinson’s disease is unresolved, in part because there is a high baseline prevalence of these disorders in the relevant age group. Sleep bruxism (nocturnal teeth-grinding) and fragmentary myoclonus of non-REM (NREM) sleep are two other movement disorders found in sleep that share some common features with RLS and PLMD and may be distant cousins physiologically. Table 133- 1 summarizes the relationship of several movement disorders to the major phases of waking and sleep. DEFINITIONS AND METHODS Clinical Features Periodic Limb Movements Disorder of Sleep. PLMD is defined by clinical hypersomnolence plus the characteristic repetitive episodes of stereotyped limb movements (PLMS refers to the same type of movements in a patient who may or may not be hypersomnolent). Although the arms can be involved, most patients have only leg movements, usually consisting of big toe extension, sometimes combined with partial flexions of the ankle, knee, and hip (it has been noted that there may also be fanning of the smaller toes, thus mimicking the Babinski and “triple flexion” responses; however, this is not a common presentation). Unlike most other movement disorders, which are abolished during sleep,
a40
Movement Disorders W
Non-Parkinsonian Movement Disorders
PLMS activity appears with the onset of sleep. The movements usually are associated with sleep disturbances ranging from full awakenings to minimal electroencephalographic (EEG) arousals, and the percentage of movements associated with any such sleep disruption can vary from 0% to 100% but usually is about 35%. Patients are unaware of all but the most prominent movements and arousals, and the movement activity can vary greatly from night to night, making it difficult to diagnose PLMD by patient history alone. Bed partner reports of leg kicking can be helpful, and if periodic movements are carefully timed, the diagnosis may be made. The movements generally have a duration of 0.5 to 5 seconds (most patients average 2 seconds) and a repetition interval of 5 to 90 seconds (most patients repeat at 20- to 40-second intervals). The limbs are immobile between episodes. The amplitude of the movements can be crudely measured on the polysomnogram (PSG) by comparing the electromyogram (EMG) in the anterior tibialis muscles during voluntary contractions while awake with the EMG bursts in the same muscles during sleep. However, because volitional muscle activation varies, there is no reliable way to calibrate the EMG output for all patients; some patients may have repeated arousals in association with very small EMG bursts that are difficult to distinguish from background noise. Perhaps these recording problems account for cases in which the apparent movements are too few in number to explain a particular patient’s daytime sleepiness. Indeed, the PSGs (all-night sleep electroencephalograms) of some hypersomniacs without leg movements show numerous arousal and subarousal EEG patterns with the same periodicities seen when leg movements are present, thus implying that the movements are only an epiphenomenon of a fundamental central nervous system (CNS) disturbance during sleep; some clinicians believe that these nonmovement arousals (sometimes called a-intrusions) are equal in impact to the disturbance of sleep seen in full-blown PLMD. Conversely, there are patients with PLMS who have very large numbers of leg movements but few or no EEG arousals. These patients may have less prominent daytime fatigue, but some may develop degenerative arthritis. Some patients have very violent kicks and may injure their bed partners or themselves. (Two patients with PLMS in our clinic developed knee injuries while asleep, eventually needing surgery.) The distribution of leg movements over the various sleep stages can vary; some patients have the largest amounts of leg movement activity in stages 3 to 4,but most have the maximum activity in stage 2. One study showed the relationship between U S and PLMS in nine members of one family; the leg movements were recorded in wakefulness and sleep and showed a periodicity similar to that seen in PLMS, with the intermovement intervals gradually increasing as the patients became drowsy and entered stage 2 sleep; the authors concluded that RLS and PLMS are two clinical manifestations of the same CNS dysfunction. When PSG recordings are scored, the sleep stages are delineated first so that leg movements can be assessed according to the sleep stage in which they occur (including brief periods of wakefulness). Leg movements associated with the end of an apnea or hypopnea are thought to be hypoxia-induced and are counted separately because they may be abolished by treatments for sleep apnea. It is useful to note the number of times a leg movement is followed by a full awakening, usually defined as the appearance or an occipital alpha rhythm (8 to 12 Hz) for at least 60 seconds; an incomplete awakening, alpha rhythm for 15 to 60 seconds; or an arousal, which can be defined as the appearance of occipital alpha activity
for 3 to 15 seconds. (Occasionally, there are large amounts of generalized 7- to 11-Hz activity during NREM sleep-the so-called alpha-delta pattern-in patients with the fibrositis-fibromyalgia syndrome, although these patients can have alpha-delta without PLMS.) Furthermore, it may be difficult to differentiate some normal features of NREM sleep from subtle arousal patterns: prolonged “spindle-beta’’ (12 to 18 Hz) accelerations, bursts of delta (1 to 3 Hz) activity, and K complexes. Also note that the more recently described cyclic alternating pattern (CAP), described by Terzano et al, accounts for much of the above periodic sleep-related EEG activity, whether associated with physical movement or not. Subtle arousals can be surmised when a physiologic event such as a leg movement is closely associated with a vertex V wave or K complex, EEG phenomena that are known to occur normally when externally applied stimuli disturb sleep. Carskadon et al. found that PLMS is common in “normal” older adults, and even though their subjects complained of neither nocturnal insomnia nor daytime sleepiness, there was a substantial amount of daytime sleepiness on objective testing (Multiple Sleep Latency Test); Coleman remarked that this indicates that a sleep-wake complaint is very subjective. Indeed, patients with PLMD may present with either insomnia (sleep maintenance type) or hypersomnia. (It should be noted that sleep maintenance insomnia usually is associated with a physiologic sleep disorder, whereas sleep onset insomnia is most often associated with a psychological or psychiatric condition.) This looks like a paradox, but working diagnoses usually are based on presenting complaints, even though objective (PSG or Multiple Sleep Latency Test) findings may not fully explain the patient’s symptoms. Indeed, the line distinguishing insomniacs from hypersomniacs is blurred on close examination: Both groups have poor-quality sleep of which they are aware to various degrees, and the primary difference is the ability of patients with insomnia to maintain alertness (appropriately in the daytime but too well at night), whereas the patients with hypersomnia have similarly poor-quality sleep at night and much more difficulty staying awake in the daytime. Restless Legs Syndrome. The diagnosis of restless leg syndrome ( U S ) was formerly based on the obligatory presence of disagreeable sensations usually before sleep onset, as well as the presence of observable leg movements. New NIH criteria* remove the latter requirement and focus the major effort on uncovering whether there is an urge to move the legs (which, by implication, adds back the possibility of an observer witnessing overt movements). In either case, the old or the new approaches place a heavy burden on patient and physician in requiring precise descriptions of the core symptoms, thus placing a hurdle in the path of the diagnosis of this common debilitating disorder. However, the increasing availability of multilingual questionnaires and validated forms to be used by patients and clinicians as diagnostic and severity-assessment instruments should begin to alleviate this problem. *NIH Criteria (Allen RP, et al): 1. An urge to move the legs, usually accompanied or caused by uncomfortable and unpleasant sensations in the legs. (Sometimes the urge to move is present without the uncomfortable sensations and sometimes the arms or other body parts are involved in addition to the legs.) 2. The urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity such as lying or sitting. 3. The urge to move or unpleasant sensations are partially or totally relieved by movement, such as walking or stretching, at least as long as the activity continues. 4. The urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night. (When symptoms are very severe, the worsening at night may not be noticeable but must have been previously present.)
Chapter 133
Movement Disorders in Sleep and Restless Legs Syndrome (Ekbom’s Syndrome)
The sensations usually are deep-seated, bilateral and limited to the lower legs but can involve the thighs and rarely may be unilateral or involve the arms or other parts of the body. Sometimes, the words used-itching, tingling-suggest the dysesthesias of peripheral neuropathy, whereas at other times the patient describes severe pains in the legs, suggesting sciatica, diabetic nerve infarction, or radiculopathy caused by root encroachment. [AUof these are potential causes of secondary RLS, which sometimes can be alleviated by removal of the underlying cause-such as a renal transplant in a patient with uremic-induced RLS-but usually the RLS is best treated by one of the “standard treatments” (see TREATMENT section below). Indeed, before a diagnosis of primary RLS can be made-and although it is likely that some patients, especially those with the common diabetic or uremic neuropathies, could have both primary RLS and a neuropathy at the same time-for most purposes (and particularly genetic studies) it is necessary to be fairly certain that none of the “secondary” causes are present)]. The disorder can begin at any age and may wax and wane over the years, even remit entirely for lengthy periods. In primary RLS, which are mostly familial cases, there may be earlier onset in each successive generation (so-called “anticipation”). The inheritance pattern may be autosomal dominant, but the variable penetrance can make cases from small families appear to be sporadic until a detailed family history is obtained (including data on nocturnal movements). There is a tendency for exacerbation in times of stress, and many women with U S may have their initial bout during the latter half of (usually their first) pregnancy. The restlessness or discomfort begins toward evening and increases further with sitting or lying down, making television or movie watching difficult. The symptoms are nearly always relieved by walking or pacing or by exercise of any kind, including stretching, cycling, swimming, and running. However, when the patient sits back down, the symptoms tend to return quickly unless the exercise has been extensive. Montplaisir et al. have developed simple laboratory methods to diagnose RLS using only surface EMG electrodes applied to the anterior tibialis muscles during a 30-minute evening recording. This test was called the suggested immobilization test (SIT) because patients were asked to sit on a stretcher or bed with eyes open and try to remain motionless. This method yielded positive results (periodic EMG bursts on the recordings) in about 67% of patients if recorded on two consecutive nights. To increase the sensitivity of testing, the forced immobilization test (FIT) was developed. This test is similar to the SIT except that patients sit on the stretcher with their legs tied down in the extended position. Three quarters or more of patients with RLS also have PLMS in sleep, as demonstrated by PSG. However, patients with RLS have been shown to exhibit periodic leg movements while awake if they are closely observed after being asked to avoid voluntary leg movements, such as during a SIT or FIT. The periodicity often is briefer in the awake state (typically 15 seconds apart) than during sleep (usually 20- to 40-second intervals, as previously described for PLMS). Montplaisir et al. showed that the average intermovement interval in familial RLS or PLMS with insomnia lengthens from 24 seconds in stage 1 sleep to 35 seconds upon entering stage 2 of sleep. Patients with severe RLS or PLMS may not be able to sleep at all through most of the night, but those who are able to sleep usually can enter stage 2 within 30 to 60 minutes, and although there may be abundant periodic leg movements, their sleep usually is no worse than the average patient with PLMS
841
alone, and there is a tendency for the patient with RLS to have fewer leg movements toward morning. Some of the severely afflicted patients are phase-delayed; that is, they stay awake for several hours, then fall asleep when the leg movements have completed the presumptive circadian cycle. These patients may then sleep later into the morning to catch up on the number of hours they need, whereas still others are unable to obtain even 4 to 5 hours total sleep per night, often because they must arise for work. Indeed, without the societal influence requiring a job for survival (most of those jobs starting early in the morning), patients with advanced RLS and delayed sleep phase syndrome (the need to stay up late due to the leg movements and the resultant need to sleep late the next morning to get sufficient total sleep) would probably be able to gain enough sleep to function normally if environmental factors were arranged to allow them to do so. As with PLMD, patients with RLS may complain of either insomnia or excessive daytime sleepiness. The patients with RLS and excessive daytime sleepiness often are older, but young adults with it may need more therapeutic effort because employability may be an issue. Excessive daytime sleepiness was studied by Coleman et al. in a small group of older patients with PLMD; the number of arousals per hour of sleep correlated with the subsequent day’s degree of sleepiness as measured on the Multiple Sleep Latency Test. Another study showed differences in the sleep disruption patterns of insomniac and hypersomniac patients with PLMD; the sleepy patients had longer histories of poor sleep (average 22.4 versus 14.3 years) with more total arousals that were short in duration and concentrated in clusters. More recently, reduced hypocretin 2 (orexin) levels have been found in the CSF of RLS patients. This substance, secreted in the lateral posterior hypothalamus, is one of the most alerting neurotransmitters ever discovered and is the same substance found reduced (with much lower levels) in narcolepsy. (Narcolepsy patients have one of the highest incidences of PLMS, after RLS.) The cause of this finding is unknown. Coleman et al. looked at the final diagnosis among patients with sleep disorders whose PSGs showed PLMS; in one early study of 441 sleep clinic patients, they found more than 40 (total) periodic movements in 19% of insomniacs, 15% of patients with sleep apnea, 10% of narcoleptics, 12% of patients with other hypersomnias, and 9% of patients with other disorders, including parasomnias and sleep-wake schedule disorders. This seemed to indicate either that PLMS is a nonspecific finding among patients with a variety of sleep complaints, or that PLMS may be a contributing factor in many different sleep disorders. The latter concept is still today supported by the fact that some patients with daytime hypersomnolence have “only” PLMS as a sleep-disturbing factor on their PSGs (although increasing recognition of other PSG/EEG phenomena, such as Terzano’s “CAP” activity mentioned earlier, may yet account for much of this). In addition, several studies show an increased incidence of PLMS in narcolepsy, but other studies dispute the importance of the finding or show no increase. However, no matter how sleepy, patients with an ICSD diagnosis of PLMD do not have the EM-onset sleep tendency that is diagnostic of narcolepsy. Secondary RLS (but not necessarily PLMD or PLMS alone) are associated with iron deficiency anemia (whether due to heme loss, malabsorption, or chronic diseases causing low erythropoietin, especially uremia), neuropathies such as diabetes, amyloid or uremia, and normal pregnancy.
842
Movement Disorders W
Non-Parkinsonian Movement Disorders
Fibromyalgia or fibrositis syndrome has been related to PLMS and alpha-delta sleep. The latter involves the appearance of large amounts of a activity during deep NREM sleep (stages 3 and 4, often called 6 sleep) and can be found in patients with other disorders, including hypersomnolence, eating disorders, and schizo-affective disorders. Some patients with fibrositis may initially respond to small doses of chlorpromazine or amitriptyline, but antipsychotics in such patients can cause severe akathisia and PLMS, and tricyclics may worsen both daytime sleepiness and PLMS. A small study of patients with atypical depression found that each had PLMS. Other disorders in which PLMS or RLS may play a part include attention deficit hyperactivity disorder (pediatric and adult forms), migraine, toxemia of pregnancy, epilepsy, premenstrual syndrome, and pseudodementia. Treatment of the sleep problem in each of these disorders may be helpful, but larger, controlled studies are needed to confirm these findings.
EPIDEMIOLOGY PLMS and RLS together may affect 5 to 15% of the population, but the incidence of PLMS increases with age and is most prevalent in older adults (see Coleman et a1 1983). A survey of healthy seniors over age 60 found PLMS in 57%, although one half had fewer than five movements per hour. In other studies, PLMS and RLS incidences of 37% to 53% have been found among sleep disorder patients over 60 years of age, and 18% in one study had PLMS or RLS as their primary diagnosis, whereas longitudinal follow-up showed an increasing prevalence of nocturnal movements with aging. More recently, large scale studies have begun to uncover evidence that, after sleep apnea, RLS/PLMD/PLMS may contribute additionally to the morbidity/mortality burdens stemming from hypertension and cerebro-cardiovascular disease. On the other end of the age spectrum, children as young as 1 year have been noted to have PLMS, but they usually have a strong family history of RLS. Among patients of all ages, 3% to 26% of insomniacs and 1% to 12% of hypersomnolent patients can be diagnosed with PLMD or RLS. Given the high prevalence among older adults, the rate of sleep complaints seems low compared with that of younger age groups. Perhaps many seniors accept the prevailing geriatric stereotype of slowed function or lowered expectations of sleep quality. Increasing efforts are being made to communicate to the primary care provider the high level of variability and subtlety in RLS symptoms in the hope that the contributed component to the costly and severe comorbidity rates may be reduced.
CAUSES Montplaisir et al. noted an elevation of dopamine metabolites in the CNS and suggested that dopamine receptors may be reduced in sensitivity in these disorders. His genetics group’s more recent announcement (Rouleaux et al) of a link to chromosome 12q in a series of large Quebec families may close this loop because the gene that codes for neurotensin, an agent that alters sensitivity at dopamine receptors, is located near the linkage locus (as is the putative analog of the important Drosophila circadian gene “timeless”) although no mutations have been discovered. The outstanding recent advancement in understanding the pathophysiology of RLS and PLMS comes from Allen and Earley at Johns Hopkins, where the role of iron metabolism has been largely elucidated. They have shown that cerebrospinal fluid and post-
mortem substantia nigra tissue transferrin levels are high and ferritin levels are low in most patients, suggesting a failure of Fe++ transport into the central nervous system. Because iron acts as an important cofactor for tyrosine hydroxylase, the enzymatic ratelimiting step in dopamine synthesis, it stands to reason that any impairment in its availability centrally can lead to deficient production of dopamine. This would also explain why erythropoietin alleviates RLS in patients on renal dialysis (who can have both iron deficiency and neuropathy as exacerbating factors for their RLS). As mentioned earlier, PLMS is almost invariably present in cases of familial RLS, although it is now becoming more and more doubtful that the two entities are driven by identical mechanisms despite the striking similarity of their periodicity and clinicoanatomical localization. Askenasy et al. thought that PLMS and RLS in patients with Parkinson’s disease result from basal ganglia dysfunction, but this conclusion was based on improvement from levodopa. Wechsler et al. showed that patients with PLMS have hyperexcitable blink reflexes, somatosensory evoked responses, long-latency motor responses, and H reflexes, indicating possible pontine dysfunction. However, PLMS may still be either the cause-through sleep deprivation-or the result of such hyperexcitability. Referring to Smith’s work on the Babinski-lie appearance of the lower extremities during the movements of PLMS, Walters and Hening questioned whether there is pyramidal tract dysfunction in PLMS, causing a release of central inhibitory activity. The antigravity muscles of the legs (gastrocnemii, quadriceps, glutei) can overpower the opposing muscles, causing contractures in immobilized patients when a stroke or spinal cord lesion blocks upper motor neuron outflow. There may be an inherent imbalance between opposing muscle groups requiring the smaller, weaker still muscles to undergo greater amounts of exercise, and this need may be genetically greater in patients with PLMS or RLS, such that internal mechanisms supervene whenever daytime activity levels have been insufficient. Exercise in normal subjects has been shown to improve stage 3 and 4 sleep which may suppress PLMS by inhibiting the central drive for PLMS, thereby also reducing the symptoms of RLS. In two women accustomed to 5 hours of strenuous exercise daily, abrupt reduction of such effort (one due to injury, the other due to pregnancy-related “cultural norms”) caused marked PLMS and sleep disruption leading to daytime hypersomnolence within a week. By extension, it is possible that in older adults the deterioration in stages 3 and 4 sleep and the great prevalence of PLMS are both caused by age-related reductions in exercise levels. This does not account for the occasional case of severe PLMS found in young adults or children, but such earlyonset cases probably result from genetic factors. Coleman et al. noted that patients with PLMS may have altered circadian rhythms and postulated that this might be an underlying causative factor in PLMS. RLS symptoms also show a marked circadian pattern, with most patients having maximum restlessness during the evening and first part of the night. It has been suggested that these disorders may be caused by dysfunction of the circadian rhythm pacemaker in the suprachiasmatic nucleus. The suprachiasmatic nucleus is well supplied with y-aminobutyric acid (GABA) receptors, perhaps explaining the response to benzodiazepines, and also valproate, which is thought to enhance activity at these receptors. Another intriguing aspect of the circadian hypothesis is the known association of the daily temperature curve with the sleep-wake cycle; because many patients with RLS (and
Chapter 133 W
Movement Disorders in Sleep and Restless Legs Syndrome (Ekbom’s Syndrome)
PLMS?) note cold feet, this suggests altered thermoregulation in the hypothalamus, perhaps in turn caused by suprachiasmatic nucleus dysfunction. Some argue that instead of causing poor sleep, PLMs may be a normal phenomenon. Bixler et al. found a 6% incidence of PLMs (with a PSG showing at least 3 clusters of 30 or more consecutive leg movements) in a normal population (mean age, 40 years). However, their subjects had arousals with only 10% of the leg movements. This may explain why there were no sleep complaints; patients with insomnia or hypersomnolence usually have arousals in association with more than 30% of the leg movements.
TREATMENT Only since the early 1980s have effective pharmacologic treatments for PLM and RLS emerged. Initially only drugs that acted at the GABA receptor (including the benzodiazepines, baclofen and, more recently, valproate), the benzodiazepines having been the most commonly used treatment for RLS until the discovery of dopaminergic therapy in the mid- 1980s. As sleep-inducing medications in the treatment of insomnia, benzodiazepines in general, and more recently clonazepam in particular, have seen widespread use among psychiatrists treating various affective disorders, including depression. Indeed, because PLMD and RLS cause 15% of insomnia, there may well be many undiagnosed patients with PLMD or RLS who are fortuitously receiving this treatment. However, hypersomnolent patients with PLMD may have great difficultywith the sedative effects of benzodiazepines, even at very small dosages. The other major problem with benzodiazepines is the gradual development of tolerance to the beneficial effects. This can be a vexing problem when attempts are subsequently made to withdraw the medication because the underlying insomnia will be severely exacerbated. Other withdrawal effects include tremors, headaches, nausea, and seizures (all partly brought out by the sleep disruption and the “denervation hypersensitivity” of the GABA receptor). This could account for patients who are addicted and cannot tolerate being weaned. Indeed, patients with PLMD and RLS (and other patients with chronic severe sleep disturbances) may gravitate toward benzodiazepines when obtainable (or to alcohol as an alternative) and then develop addiction after initially obtaining relief. Because there is no clear mechanism of action for benzodiazepines other than sedative and hypnotic effects and no evidence that the leg movements are significantly reduced, the search has continued for more effective, less problematic therapies. Baclofen was found effective in one study, but interestingly, it did not decrease the leg movements and seemed to improve sleep by decreasing the number of arousals associated with the leg movements. One problem with this drug is its short half-life. Another class of agents that affects GABA receptors but has not been formally studied in PLMD is the barbiturates, including phenobarbital, among the most widely prescribed sleep agents for decades. Ekbom found phenobarbital helpful only in milder cases, mainly as a sedative, and again, the problems of tolerance and abuse are well recognized with this class of drugs. Valproate is a medication whose mechanism of action is not fully understood, but studies have suggested that its anticonvulsant property involves enhancement of GABA receptor activity. This medication is not known to produce addiction, and tolerance to its antiepileptic effects has not been seen. Valproate has been used as
845
a sleep-inducing agent in Europe. Valproate in low to moderate dosages at bedtime improves nocturnal sleep and daytime alertness in 40% of patients with PLMD. Patients with PLMS and hypersomnolence may be extremely sensitive to the usually mild sedative effects of valproate, so small dosages given only at bedtime, aiming for a low serum level in the morning, may work best. Patients who return with high levels may complain of excessive morning fatigue, headaches, and moodiness, probably related to a “hangover.” However, in some patients after a few weeks it may be appropriate to increase the dosage to maintain the beneficial effect. Caution concerning the weight gain potential is advised, especially with higher doses of valproate. The most effective medications for RLS and PLMD are the dopaminergic agents levodopa, pergolide, pramipexole, and ropinirole. The slow-release form of levodopa or carbidopa has been beneficial for patients with RLS and also in intractable cases of PLMD. Studies by Coleman et al. originally speculated that levodopa might be an exacerbating factor for PLMS, but work by Montplaisir et al. demonstrated that the effects of the short-acting form last only 2 hours, after which there is rebound, causing exacerbation of the PLMD. Therefore, regular levodopa or carbidopa may work for patients whose symptoms occur only at bedtime but is suboptimal for patients with RLS or PLMD whose worst sleep occurs in the latter half of the night, when bouts of leg movement activity increase in intensity in the lighter stages of NFEM sleep. For these patients, one slow-release 50/200-mg tablet at bedtime is a major improvement in therapy because this form lasts 4 to 6 hours, especially if its effects are prolonged by entacapone (a catechol-o-methyl transferase inhibitor), allowing most patients to experience a better night’s sleep. This long-acting combination form is also a boon to patients with RLS and diurnal leg symptoms that begin early in the day. Indeed, many patients experience their first morning RLS symptoms only after initiating an evening dose of levodopa, as a rebound phenomenon (so-called augmentation). Rebound is more severe with higher daily dosages of levodopa and can be counteracted by using the long-acting form in evenly divided 24-hour dosing schedules and adding medications with alternative mechanisms of action to the regimen to reduce the total daily levodopa intake. The current drugs of first choice for treating RLS are pramipexole and ropinirole, often in dosages far below those that are effective for Parkinson’s disease, the only current indication for these two dopamine agonists (each with D3- as well as D2receptor-activating abilities). These two agents appear to be the best-tolerated of all available agents, although reports of patients falling asleep suddenly while driving have caused concern. Most of these patients may have been taking large parkinsonian dosages and may have been sleep deprived, but it is advisable to warn patients about this possibility when prescribing one of them for the first time. Another long-acting dopaminergic agent is pergolide, in starting dosages of 0.05 to 0.1 mg, usually given at bedtime. Bupropion is touted as a dopaminergic-serotonergic antidepressant and in daily dosages of 75 to 150 mg may be helpful when levodopa or carbidopa is not tolerated. In any case, for depressed patients with RLS, it is a good alternative to tricyclic and selective serotonin reuptake inhibitor antidepressants because members of both of these classes may exacerbate RLS or PLMD. (Of the other antidepressants, only trazodone and monoamine oxidase inhibitors are tolerable to patients with US.) Pemoline, methylphenidate, and D-amphetamine have long
844
Movement Disorders 1 Non-Parkinsonian Movement Disorders
been used as daytime stimulants in patients with hypersomnolence, and each may act as dopaminergic agonist. Although some patients who take stimulants report improved nocturnal sleep quality, it is not known how many of these patients have PLMD or RLS; in any case, most patients develop insomnia if the stimulant dosages are high enough. Patients with narcolepsy have a 10% to 75% incidence of PLMS (increasing with advancing age). Valproate, levodopa, or 6-hydroxybutyrate produces better-quality nocturnal sleep, leading to a decrease in daytime sleepiness, potentially allowing reductions in stimulant dosage. Opiates (including propoxyphene) can be very helpful in PLMD and RLS; codeine was used in one study, and despite the potential for tolerance and abuse, the authors state that their patients tended to follow the prescribed regimens. Compared with valproate, levodopa, or benzodiazepines, the opiates have a longer and better record of safety in pregnancy and may be especially useful when PLMD or RLS become severe early in the first trimester. Adrenergic blockers have limited use in patients with sleep disorders. An occasional patient with PLMD may respond to an a-adrenergic blocker such as phenoxybenzamine. Studies have shown a moderate but not necessarily long-lasting response to the P-blocker propranolol in RLS, akathisia, and narcolepsy. Clonidine, an a,-adrenergic agonist, has been used in RLS. Serotonergic agents such as L-tryptophan and 5hydroxytryptophan have been used with rare success in RLS but have not been found useful in PLMD. Other therapies useful in treating RLS that have not been clearly shown to work for patients with PLMD include iron and folate (both helpful in RLS even in the absence of a deficiency), vitamin E, vasodilators, and aldehydes, but none of these is currently in widespread general use, although clearly any patient with RLS and anemia should be evaluated and treated appropriately. Indeed, it is becoming clear that RLS may well be associated with a central deficiency of iron in nearly all cases. Aside from valproate, another anticonvulsant that has been tried in PLMD and RLS is phenytoin. Carbamazepine has been shown to work in mild RLS but is not in widespread use. Patients with PLMD or RLS sometimes are awakened by leg cramps, but most patients with recurrent nocturnal cramps do not have PLMD. Nevertheless, quinine, long used for nocturnal cramps, is sometimes used to treat patients with PLMD, but there is no evidence to support its use for either RLS or PLMD. Other drugs that can bring out or exacerbate RLS or PLMD include lithium, caffeine, terbutaline, and nifedipine (all calcium channel blockers are suspect; they can cause parkinsonism and akathisia, probably by reducing dopaminergic neurotransmission). As mentioned earlier, antipsychotic neuroleptic drugs commonly cause akathisia, which is similar to RLS but has a
different circadian pattern and can be associated with a sleep disturbance that may also be similar to that of PLMD. In treating PLMD, it must always be kept in mind that subtle forms of sleep apnea may cause the clinical appearance of periodic leg movements on PSG without obvious changes in respiration or oxyhemoglobin saturation. Therefore, in cases where the PLMD seems intractable to all medications, a trial of nasal (continuous positive airway pressure) or a dental device (a “snore guard”) may be warranted if snoring has been a concomitant.
SUGGESTED READINGS Allen RP, Hening WA, Montplaisir J, Picchietti D, Trenkwalder C, Walters A and members of the IRLSSG. Restless Legs Syndrome: Diagnosis criteria, special considerations, and epidemiology. Report from the diagnosis and epidemiology workshop at NIH, summer, 2002 The Atlas Task Force of the American Sleep Disorders Association. EEG arousals: scoring rules and examples. Sleep 16:174-184, 1992 The Atlas Task Force of the American Sleep Disorders Association: Recording and scoring leg movements. Sleep 16749-759, 1993 Bucher SF, Seelos KC, Oertel WH, Reiser M, Trenkwalder C. Cerebral generators involved in the pathogenesis of the restless legs syndrome. Ann Neurol41:639-645, 1997 Coleman RM, Bliwise DL, Sajben N et ak Epidemiology of periodic movements of sleep, pp. 217-229. In Guilleminault C, Lugaresi E (eds): SleeplWake Disorders: Natural History, Epidemiology,and Long-Term Evolution. Raven Press, New York, 1983 Diagnostic Classification Steering Committee, Thorpy MJ, Chairman:
International Classification of Sleep Disorders: Diagnostic and Coding Manual. pp. 69-71, 29 1-293. American Sleep Disorders Association, Rochester, MN, 1990 Ehrenberg B L Sleep Pathologies associated with nocturnal movements, pp. 582-593. In: Joseph AB, Young RR (eds): Movement Disorders in Neurology and Neuropsychiatry, 2/e. Blackwell Scientific, Boston, 1999
Ekbom KA: Restless leg syndrome. Neurology 102368-873, 1960 Montplaisir J, Godbout R, Pelletier G, Wames H: Restless legs syndrome and periodic limb movements during sleep, pp. 589-597. In Kryger MH, Roth T, Dement WC (eds): Principles and Practice of Sleep Medicine. WB Saunders, Philadelphia, 1994 Rechtschaffen A, Kales A, eds. A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. U.S. Department of Health, Education, and Welfare, Public Health ServiceNational Institutes of Health, National Institute of Neurological Diseases and Blindness, Neurological Information Network, Bethesda, MD, 1968
Terzano MG, Parrino L, Sherieri A, Chervin R, Chokroverty S, Guilleminault C, Hirshkowitz M, Mahowald M, Moldofsky H, Rosa A, Thomas R, Walters A. Consensus Report: Atlas, Rules, and Recording Techniques for the Scoring of Cyclic Alternating Pattern (CAP) in Human Sleep. Sleep Medicine 2:537-555, 2001 Walters A, Hening W Clinical presentation and neuropharmacology of restless legs syndrome: a review. Clin Neuropharmacol 10:225-237, 1987
Chapter 134
Stiff-Man Syndrome
845
134 Stiff-Man Syndrome Kathleen McEvoy
Stiff-man syndrome is a rare motor function disorder characterized by involuntary stiffness of axial muscles and superimposed painful muscle spasms. The cause is unknown, but there are clinical and laboratory associations with autoimmune diseases, and it is becoming increasingly apparent that stiff-man syndrome may form a spectrum of diseases with some types of encephalomyelitis. In addition, some cases of the syndrome may be paraneoplastic. Whether these atypical cases of stiff-man syndrome are varying manifestations of the same pathologic entity or phenotypically similar but pathophysiologically distinct from typical stiff-man syndrome remains to be defined. Stiff-man syndrome is also known as Woltman-Moersch syndrome, acknowledging the neurologists who first recognized and described this condition in the 1950s. They published a report of 14 patients with progressive and fluctuating rigidity and spasms seen over a 35-year period at the Mayo Clinic. In the years after this report, numerous other patients were recognized throughout the world. By 1990, about 100 patients had been reported in the literature.
EPIDEMIOLOGY AND THE AT-RISK POPULATlON Stiff-man syndrome is clearly rare, but its true prevalence cannot be known because of poor ascertainment. Diagnosis can be made only if it is suspected, and physician recognition of this rare and unusual disorder is very low, especially in the primary care setting. Misdiagnosis as a psychiatric disorder is common. Because stiff-man syndrome can be a devastating and sometimes lifethreatening condition when untreated, its recognition is critical. The index of suspicion for diagnosis of stiff-man syndrome should be elevated in certain patient populations, particularly those with a personal or family history of organ-specific autoimmune diseases or organ-specific autoantibodies. Women may be more likely to develop the syndrome. The age of onset of symptoms usually is in the fifth decade of life but ranges from the third through at least the seventh decade, with cases in children rarely reported. No antibody-positive cases have been reported in children.
SYNDROME RECOGNITION Clinical Manifestations Typical stiff-man syndrome is well characterized by the diagnostic criteria laid out by Lorish et al. (1989): a prodrome of stiffness and rigidity in axial muscles; slow progression of stiffness to include proximal limb muscles, making volitional movement and ambulation difficult; a fixed deformity of the spine; superimposed episodic spasms precipitated by sudden movement, jarring, noise, and emotional upsets; normal findings on motor and sensory examinations; normal intellect; and typical electromyographic findings of continuous muscle activity abolished by intravenous diazepam or a positive therapeutic response to oral diazepam. Although these criteria remain valid for diagnosing typical
stiff-man syndrome, reflex asymmetry and enhancement are common, and extensor plantar responses may be seen in otherwise typical patients. Symmetry of stiffness is the rule, to which there are exceptions. The spinal deformity is a most helpful feature in recognizing stiff-man syndrome and distinguishing it from common back pain. Symptoms usually develop over a period of months, beginning in the low back muscles, producing pain and stiffness, and also deformity of the spine, with exaggerated lumbar lordosis. Paraspinal muscle spasm is pronounced, and lumbar range of motion is severely limited. Lordosis usually is maintained even with forward bending, which is done almost completely at the hips. Abdominal muscles often are rigid. Many patients describe abdominal protuberance, which is really caused by the spinal deformity. After months or years, paraspinal hypertrophy develops and may be striking. Whereas the muscular activity generally is noted to abate during sleep, the spinal deformity may become fixed and persistent. In some patients, the muscular hyperactivity and spinal deformity are more rostral, producing cervical tightness and hunching of the shoulders. In most patients, disease is predominant at one level so that either the lumbar or cervical level is symptomatic. Stiffness and rigidity may extend to the anterior neck muscles, but trismus is not seen in typical stiff-man syndrome, and would suggest the possibility of tetanus as the cause of muscle stiffness. Stiffness and simultaneous contraction of agonists and antagonists may spread to the proximal extremities. In lumbar patients, this produces a characteristic stiffness of gait not unlike that of Frankenstein’s monster. Ambulation is slow and difficult and may be punctuated by freezing episodes. Falls are common. Postural reflexes are overridden by stiffness, so the patient falls like a tin soldier, and the risk of fracture is high. Fear of falling exacerbates the gait disorder because emotional stimuli potentiate the abnormal muscle stiffness. Most patients experience increased stiffness in social situations or in public places. Stressful situations and exposure to cold temperatures also aggravate stiffness and spasms. Not surprisingly, any activity requiring truncal flexibility is performed slowly and awkwardly, if at all. This includes arising from chairs, getting out of bed, tying shoes, and arising from a fall. Mobility and ability to perform activities of daily living may be severely limited. This and the aggravation of symptoms in public places or social situations render many patients essentially housebound. Painful muscle spasms are a universal feature of stiff-man syndrome, and they are generally more amenable to treatment than the underlying stiffness and rigidity. Their absence in an untreated patient renders the diagnosis suspect. The spasms occur primarily in axial muscles but may spread to involve the limbs as well. They may arise spontaneously but usually are induced by movement, startle, or emotional stimuli. Common examples include an unexpected tap on the shoulder, the sound of a doorbell or telephone, or excessive activity producing back pain. These
846
Movement Disorders rn
Non-Parkinsonian Movement Disorders
spasms may be strong enough to break bones and to bend the pins used for repair. Autoimmune Associations
The autoimmune pathogenesis of stiff-man syndrome is strongly supported by the presence of antibodies to glutamic acid decarboxylase (anti-GADS) or anti-islet cell antibodies (antiICAs) in most patients, the common presence of other organspecific autoimmune diseases or autoantibodies in stiff-man syndrome patients and first-degree relatives, and the response to immunosuppressive therapy. The target of autoimmune attack within the central nervous system is not known with certainty, nor is it known whether the antibodies detected are pathogenic or merely markers of disease. Passive transfer of the syndrome to animals via patient serum has not yet been demonstrated, and there is no animal model of the disease. Anti-GAD antibodies have been detected in significant numbers of patients reported to have stiff-man syndrome in several series. Anti-ICAs are nearly identical to anti-GADS, with differences only in the N-terminal epitopes, and are adequate as a screening test for the diagnosis. This antibody is present in low titer in many patients early in the course of development of type I diabetes mellitus. Anti-ICAs are present in high titer in the majority of patients diagnosed with typical stiff-man syndrome in recent years at the Mayo Clinic, independent of the presence of diabetes. Titers have not fallen with time and are present in patients with long-standing stiff-man syndrome. This antibody is very rare in people with neither diabetes nor stiff-man syndrome but may occasionally be detected in intermediate titers in patients with multiple autoimmune endocrinopathies. Recent reports describe a new antibody in patients with breast cancer and stiff-man syndrome. Most patients with autoimmune stiff-man syndrome harbor other autoantibodies, most commonly antithyroid antibodies. Many have other autoimmune diseases, as do their first-degree relatives. Type I diabetes is present in approximately 30% of patients. Most patients have antimicrosomal thyroid antibodies, and some have had clinical autoimmune thyroid disease, either Hashimoto’s or Graves’s. Other autoimmune endocrinopathies and organ-specific autoimmune diseases from the thyrogastric cluster of autoimmunity may be seen, including pernicious anemia, vitiligo, premature ovarian failure, premature gray hair, autoimmune adrenal failure, and myasthenia gravis. The presence of anti-GAD or anti-ICA, other autoantibodies, or other autoimmune diseases in the patient or family help to support the diagnosis of stiff-man syndrome in a patient with the appropriate clinical presentation but are not necessary for the diagnosis. An association with epilepsy has been postulated but is not supported by the literature. Stiff-man syndrome often is misdiagnosed as a psychiatric disorder. Until recent years, there was doubt in the medical community as to the existence of the syndrome. In fact, many patients with it do have coexisting psychiatric conditions, generally anxiety or affective disorders, and some overuse alcohol and other medications, in part to control their disease. The combination of the unusual nature of the symptoms, the limited findings on neurologic examination despite significant disabilities in function and gait, the lack of findings on routine laboratory testing, the exacerbation by emotional stimuli, the frequency of accompanying anxiety or affective disorder, and
probably also the relative frequency of the disease in women all contribute to the common error of attributing symptoms solely to psychiatric disease. Even the efficacy of treatment with benzodiazepines may be taken to support this error in diagnosis.
Other Laboratoy Testing
The diagnosis of stiff-man syndrome is made on clinical grounds based on the patient history and examination results. The clinical index of suspicion is raised in patients with known tendencies to autoimmune disorders. The presence of anti-GADS or anti-ICAs strongly supports the diagnosis in patients with appropriate signs and symptoms. Other laboratory testing may provide specific support for the diagnosis of stiff-man syndrome but largely rules out other diseases. Electrophysiologic testing in stiff-man syndrome includes routine electromyography (nerve conduction studies and needle electrode examination), as well as specialized surface electrode studies documenting the pattern of muscle activity in axial and limb muscles and the response to stimuli. Nerve conduction study results generally are normal, including long loop reflexes. Routine electromyographic testing shows continuous activation of normalappearing motor unit potentials in affected muscles despite attempts to relax. Surface electrode demonstration of widespread continuous muscle activity in axial muscles is important as a tool to document that inability to relax is not caused simply by discomfort from the recording needle. Additional studies may be done to document simultaneous activation of agonists and antagonists in limbs and exaggerated response to startle stimuli in many patients. Brain and spinal imaging typically is normal, as is spinal fluid examination. Occasional patients show inflammatory cerebrospinal fluid (CSF) changes, including mild pleocytosis, elevated immunoglobulin G index, or oligoclonal bands. These changes may be more likely in atypical patients, such as those with cerebellar signs, and may represent an inflammatory phase in the development of stiff-man syndrome or, in some cases, true encephalomyelitis.In such patients, as in those with inflammatory changes on magnetic resonance imaging, it is particularly important to exclude demyelinating disease.
ATYPICAL SYNDROME FORMS Atypical forms of stiff-man syndrome may be seen. Some patients have findings that are otherwise typical of the syndrome except for the presence of mild brainstem or cerebellar signs such as ophthalmoparesis, nystagmus, or dysmetria. Jerking stiff-man syndrome, or stiff-man syndrome with prominent myoclonic jerks, has been described. The presence of significant sensory disturbance or significant primary sphincter dysfunction suggests an alternative diagnosis, such as demyelinating disease, other causes of myelopathy, or central nervous system disease. Symptoms of stiff-man syndrome usually develop over a period of months. More rapid onset-a period of 6 to 8 weeks or less-suggests encephalomyelitis as the underlying cause. In these cases, other neurologic manifestations are commonly present, especially brainstem or cerebellar signs. Anti-GAD antibodies have been detected in patients with pathologically proven encephalomyelitis with rigidity.
Chapter 134
Encephalomyelis with Rigidity The pathogenic mechanisms of typical stiff-man syndrome are not known with certainty. Some forms of encephalomyelitis may produce progressive stiffness and rigidity. Since the original description of the syndrome, several cases have been reported with clinical features highly suggestive of stiff-man syndrome but with additional focal neurologic signs atypical for the diagnosis, including cerebellar signs, oculomotor disturbances, facial or bulbar weakness, extensor plantar responses, vertigo, or epilepsy. Autopsies have shown inflammatory infiltrates in the gray matter of the spinal cord and brainstem, with perivascular lymphocytic infiltration and microglial proliferation. These cases were called progressive encephalomyelitis with rigidity. Anti-ICA and antiGAD antibodies have been detected in several nondiabetic patients with confirmed encephalomyelitiswith rigidity. In a patient with symptoms of stiff-man syndrome, the possibility of underlying encephalomyelitis is suggested by any of the following: onset of symptoms over less than 6 to 8 weeks, the presence of fever or clouding of consciousness, inflammatory CSF changes, or focal neurologic signs.
Paraneoplastic Stiff Man Syndrome Most stiff-man syndrome is not paraneoplastic. Thorough evaluations and long follow-up reveal no evidence of cancer in most patients. In a few cases, the syndrome has been associated with carcinoma; however, most well-documented cases have features suggestive of underlying encephalomyelitis, as outlined earlier. Antibodies against a separate antigen and a distinct clinical picture, with predominantly proximal lower extremity rather than axial involvement, have been described in patients with stiff-man syndrome associated with breast cancer.
DIAGNOSIS The overlap between the clinical entities of typical stiff-man syndrome, progressive encephalomyelitis with rigidity, and paraneoplastic stiff-man syndrome suggests that stiff-man syndrome, as originally described by Moersch and Woltman, may be part of a spectrum of disease, with the syndrome perhaps resulting from a more confined form of spinal encephalomyelitis. Occasional focal neurologic signs and CSF changes might then be expected even with typical stiff-man syndrome, and additional focal signs, a more hlminant onset, and more inflammatory CSF would be the rule in more extensive cases of encephalomyelitis. Paraneoplastic inflammation might produce still a different distribution of involvement. Alternatively, stiff-man syndrome and progressive encephalomyelitis with rigidity may be different diseases with similar signs and symptoms. The diagnosis of typical stiff-man syndrome remains primarily clinical, using the diagnostic criteria as previously outlined, with support from serologic and electrophysiologic tests. Further testing, including magnetic resonance imaging and spinal fluid examination, may be necessary to exclude other neurologic disease. The time course of the slow progression should be longer than 8 weeks. A clinical classification of stiff-man syndromes might be extended beyond typical stiff-man syndrome to include cases of atypical stiff-man syndrome that have focal neurologic signs and cases that are atypical in that they have focal neurologic
Stiff-Man Syndrome
847
signs and also either rapid onset and progression of symptoms or myoclonus. A differentialdiagnosis should include multiple sclerosis, other causes of myelopathy, extrapyramidalsyndrome including Parkinson’s disease, bilateral frontal lobe dysfunction (e.g., caused by hydrocephalus, vascular disease, trauma, or malignancy), degenerative disorders producing spasticity, tetanus, other causes of primary muscle stiffness or continuous muscle fiber activity such as Isaac’s syndrome, and other orthopaedic or rheumatologic causes of reduced spinal range of motion.
MANAGEMENT For nearly a decade after stiff-man syndrome was first described, there was no known effective treatment for this disorder. In 1963, Howard discovered the efficacy of diazepam, and benzodiazepines have remained a mainstay of treatment. As in other autoimmune disorders, although pharmacologic manipulations may be directed at the physiologic defect (e.g., benzodiazepines for stiff-man syndrome, anticholinesterase drugs for myasthenia gravis), immunosuppressive therapy may be necessary for optimal management. In recent years, immunosuppression has proven effective in some cases; however, despite a combined approach to treatment with both directly neuroactive drugs and immunosuppressive agents, symptomatic control sometimes is marginal. Patient education and supportive care are essential.
Phannacologic Manipulation of Spinal Mechanisms of Stiffness Diazepam was the first drug shown to be effective in stiff-man syndrome, and it has been the most widely used. Its efficacy is unquestionable. The exact mechanism by which it relieves stiffness and spasms in stiff-man syndrome is not known, but it is believed to act at the spinal level via the y-aminobutyric acid receptor system to reduce abnormal motor activity. Whereas modest antianxiety dosages of diazepam are of some benefit and often have been administered even before diagnosis, patients with stiff-man syndrome often need and tolerate very large dosages. Many patients take 40 to 60 mg/day, a few take more than 100 mg/day, and dosages greater than 300 mg/day have been reported. A reasonable starting dosage is 5 mg three times a day, but rapid escalation may be needed. Equivalent dosages of other benzodiazepines are also effective. Sedation may occur transiently but usually is not a dose-limiting side effect. Mood and personality changes are common and often limit the dosage. Abuse and dependence on these and other agents may develop in stiff-man syndrome, despite claims to the contrary. Care should be taken to ensure that the drugs are being used to treat symptoms of stiff-man syndrome rather than anxiety per se. Baclofen is also efficacious in stiff-man syndrome. As with benzodiazepines, very large dosages may be needed, sometimes more than 100 mg/day. An initial dosage of 5 mg twice or three times a day may be increased every few days as tolerated. Because strength is normal in stiff-man syndrome, there is no unmasking of underlying muscle weakness, as may be seen in multiple sclerosis or other forms of spasticity. Dosage therefore is limited by other side effects, mainly sedation. Intrathecal administration allows high spinal levels with much lower brain levels and therefore is an attractive consideration in this syndrome. Initial
a48
Movement Disorders
rn Non-Parkinsonian Movement Disorders
experience with intrathecal baclofen is promising. Although the pump implantation and drug titration entail risk, expense, and effort, the benefits may be significant. Sodium valproate in anticonvulsant dosages and vigabatrin may also provide at least modest benefit. Alcoholic beverages relieve symptoms, but medicinal use is not recommended, especially because affective disorders and substance abuse are common in stiff-man syndrome. Pharmacologic manipulation of spinal mechanisms of stiffness often provides less than satisfactory control of stiff-man syndrome, at least with oral administration. Spasms may be eliminated, but relieved stiffness and improved mobility often are possible only with high dosages and significant medication side effects. Intrathecal baclofen may circumvent this, but it is expensive, invasive, somewhat cumbersome, and not generally available. Immunosuppression therefore is often indicated.
Immunosuppressionand Related Therapies Corticosteroids and azathioprine are clearly effective in reducing disease activity in stiff-man syndrome. Isolated reports of response to corticosteroids antedate the discovery of antibodies in stiff-man syndrome and even the suspicion that the syndrome was autoimmune. The possibility of a direct effect on mechanisms of stiffness has been raised. The comparable efficacy of other immunoactive treatments suggests that any direct effect of steroids on syndrome-related stiffness must be small. Prednisone may be administered in a regimen similar to that used in myasthenia gravis. Initial dosages of 60 mg/day generally take effect within a few weeks. A switch or rapid taper to alternate-day therapy and then a slow taper of the dosage usually is well tolerated. Experience thus far is too limited to predict the lowest tolerated dosage, especially because many patients are concurrently treated with azathioprine. Unlike myasthenia gravis, in which immunosuppression often obviates for anticholinesterase medications, stiff-man syndrome seldom responds so well to immunosuppression that diazepam can be withdrawn. Some side effects of corticosteroid treatment are of particular concern in stiff-man syndrome. Diabetes mellitus is present in about 30% of these patients; this complicates corticosteroid treatment but is not an absolute contraindication. Steroid-induced osteoporosis may increase the risk of fractures caused by falls. If intrathecal baclofen is to be used, the higher infection risk with any immunosuppression is of concern. Azathioprine appears to be an effective steroid-sparing agent in stiff-man syndrome and may allow steroids to be tapered completely. Again following the pattern of treatment of myasthenia, an initial dosage of 50 mg once per day may be increased over 1 month to 2 to 2.5 mg/kg/day in three divided doses. Liver enzymes and a complete blood count must be checked weekly for the first month and monthly thereafter. A normal level of thiopurine methyltransferase activity in patients’ red blood cells ensures that they are not among the 1 in 300 who are severely deficient in this enzyme, which participates in azathioprine metabolism. However, a normal level of thiopurine methyltransferase does not rule out the possibility of severe leukopenia or hepatic dysfunction. Hepatic intolerance usually occurs early, within the first week. The white blood cell count may drop at any time. High steroid dosages may falsely elevate the white blood cell count early in the course of azathioprine treatment. As steroids are tapered, the leukopenia becomes apparent. About 5% of people are intolerant
of azathioprine because of a febrile serum sickness type of response. Others note gastrointestinal upset, which may respond to dividing the daily dosage into six rather than three doses. The long-term risk of promoting the development of neoplasms with azathioprine appears to be very small and is almost certainly less than the overall risks of prolonged steroid treatment. Plasma exchange is effective in some cases and has rescued some severely affected patients from crises. Other patients do not improve with plasma exchange but may still respond well to steroids and azathioprine. Experience with intravenous immunoglobulin G in stiff-man syndrome is limited but promising. Nonpharmacologic treatments may significantly augment the effects of pharmacotherapy in stiff-man syndrome. Physiatric intervention may provide symptomatic relief of muscle discomfort and stiffness, as may aids and instruction in mobility and gait safety. Stretching exercises benefit some patients. Behavioral medicine and biofeedback may also be helpful in managing the psychological factors that can aggravate symptoms. Good patient education allows patients and their families to understand the organic nature of the syndrome and the role of stress and psychological factors. As in other rare disorders, patients very much appreciate the chance to speak with others suffering from the same disorder. In addition to managing stiff-man syndrome itself and watching for side effects and complications of treatment, treating physicians must be vigilant for development of associated conditions, such as diabetes and multiple endocrine failure.
SUMMARY The diagnosis of stiff-man syndrome has been primarily clinical, supported by electrophysiologic findings. Clinical criteria for diagnosis therefore have necessarily been strict and exclusive to ensure accurate diagnosis of the specific syndrome. A number of neurologic and musculoskeletal disorders can resemble the syndrome in some aspects. Differentiation from demyelinating disease is essential. Diazepam and other drugs that act on the y-aminobutyric acid receptor system are effective in stiff-man syndrome. Anti-GADS and anti-ICAs have been found in many patients with stiff-man syndrome, lending support to the autoimmune hypothesis. Immunosuppression with corticosteroids or azathioprine ameliorates symptoms in most patients. Plasma exchange sometimes is helpful. With the advent of improved neuroimaging to exclude demyelinating or structural disease, and with serologic testing to support the diagnosis of stiff-man syndrome in questionable cases, we are now able to reapproach the issue of defining the diagnosis of stiff-man syndrome and may consider a wider spectrum of clinical manifestations and causes, including primary autoimmune stiff-man syndrome, stiff-man syndrome associated with encephalomyelitis, paraneoplastic stiff-man syndrome, and atypical clinical manifestations.
SUGGESTED READINGS Auger RG: AAEM mini-monograph diseases associatedwith excess motor unit activity. Muscle Nerv (in press) Lorish TR, Thorsteinsson G, Howard FM: Stiff-man syndrome updated. Mayo Clin Proc 64:629, 1989 McEvoy KM: Stiff-man syndrome. Semin Neurol 11:3, 1991
SECTION
1
BEHAVIORAL NEUROLOGY
135 Examining Mental State Sandra Weintraub The purpose of the mental state examination in neurology is to detect and characterize cognitive and behavioral abnormalities resulting from brain disease. Although several standardized mental state tests are available, there is no single all-purpose test. Existing tests do not sample the full range of cognitive and behavioral domains, and there are no standard measures of such symptoms as prosopagnosia, semantic processing deficits, and impaired judgment. Another limitation of available mental state screening tests is that they are too easy for most people of normal intelligence with a high school education but too difficult for those with limited education. This is especially problematic for the early detection of dementia associated with aging. For these reasons, it is important that the mental state examination be guided by principles of neurobehavioral organization and that the clinician possess a flexible array of instruments and procedures at several levels of difficulty to test the nature of presenting symptoms. In this chapter, a theoretical approach to neurobehavioral organization is outlined. This perspective structures the examination of mental state, its interpretation, and synthesis of findings. Domains of mental function are defined, and selected procedures to test their integrity are described. General principles that apply to the examination of all types of neurobehavioral disorders, including those caused by neurodegenerative diseases of the brain, are discussed.
NEUROCOGNlllVEAND BEHAVIORAL ORGANIZATION The backbone of the mental state examination consists of a limited number of cognitive and behavioral domains defined by studies in human psychology and brain science: arousal, mood, motivation, attention, language, perception, reasoning, executive functions, and comportment. Each of these domains encompasses distinct types of mental processes, and each has been well characterized with respect to its neuroanatomic substrates. Identifying the domain of the primary clinical symptoms, therefore, serves to identify the neuroanatomy of the disorder, while the symptom history, the patient’s past history, and the remainder of the neurologic examination identify its nature (i.e., vascular, neoplastic, neurodegenerative, infectious, or toxic or metabolic). For example, primary amnesia detected on examination only predicts damage to limbic networks. A subacute onset and symptoms of malaise suggest encephalitis as a possible cause; insidious onset and gradual progression suggest a neurodegenerative disease with affinity for limbic regions, such as Alzheimer’s; acute onset and a cardiac history are more consistent with cerebrovascular accident. 850
To interpret the examination of mental state, it is necessary to subscribe to a model of how behavior and cognition are organized in the brain. One such model, proposed by Mesulam, offers a practical framework to guide the examination and interpretation of the findings. According to this model, mental domains can be divided into two large classes. “State-dependent’’ domains are mediated by diffusely projecting neuroanatomic networks of the type that constitute the major neurotransmitter projection pathways. This anatomic arrangement supports neural activity that rapidly modulates the general information processing state, or tone, of the brain. Arousal and many aspects of attention, mood, and motivation are supported by this type of anatomic organization. In contrast, “channel-dependent” domains are supported by large-scale neuroanatomic networks consisting of distinct groups of distributed cortical epicenters and their monosynaptic, reciprocal cortico-cortical connections. Each of these networks also incorporates connections with distinct subcortical components in the thalamus and striatum. Language, visual and auditory perception, explicit memory, and highly integrative functions such as comportment, judgment, reasoning, and executive functions are mediated by this second type of anatomic organization. This proposed system of neurobehavioral organization leads to the first important practical principle governing anatomic localization of mental state abnormalities: primary deficits in channeldependent domains predict damage to discrete anatomic networks in the brain; primary deficits in state-dependent domains are not similarly localizable. Identifying the primary domain of impairment can be challenging because there are no pure tests of each domain. For example, even a seemingly simple test such as mental calculation is multifactorial from the perspective of the component operations and neural machinery enlisted in the actual performance of this task. Concentration, auditory language comprehension, working memory, arithmetic knowledge, and speech production are all components of performance, and each represents a different domain of mental functioning. A patient’s inability to carry out mental calculation could result from failure in any one of these components. The interpretation of failure (and subsequent predictions of the anatomic locus of disease) would be very different if the responsible deficit were aphasia rather than a problem with working memory and attention, or with numerical reasoning. Therefore, if the clinician wants to know whether a patient can do mathematical computation, it might be best to test this more directly with paper-and-pencil calculations, eliminating many of the confounding variables.
Chapter 135
STRUCTURE AND INTERPRETATIONOF THE EXAMINATION OF MENTAL STATE
The major neurocognitive and behavioral domains that structure the examination of mental state are depicted in Figure 135-1. Each domain is assessed with different tests. Although these domains are not hierarchically organized in the brain, it is heuristically useful to sequence the examination in a hierarchical manner and to apply this sequence to the interpretation of findings. Deficits provide two kinds of information. First, if primary, they are of localizing value. Secondly, a deficit in one domain can impede performance in others, leading to “secondary deficits.” For example, a primary anomia can interfere with accurate word retrieval on tests of verbal learning, despite normal retentive memory. These facts lead to a second important general principle in the examination of mental state: primary deficits in one domain can interfere with performance on tests in other domains not themselves directly affected by the primary disease process. An application of this principle follows. If a patient fails tests of attention and tests of all other domains, there are two possible interpretations: the deficit in attention, a state-dependent function, is primary and the only true deficit, interfering with performance of all other tests and yielding the appearance of more widespread deficits; or the deficits in each domain are all truly primary. If the first alternative is correct, then discrete network localization is not possible, and the remainder of the workup is to
FIG. 135-1. A framework for the examination of mental state, based on major domains of mental functioning. Even though tests of mental state are intended to target a single domain, performance may rely on other domains as well. Deeper shades of gray indicate that performance at each level depends on several layers of mental processing. For example, performance of verbal and nonverbal learning and memory tests requires normal language, visual perception, and drawing skills, and the levels of arousal, attention, and motivation must be sufficient to support task completion. Therefore, failure to recall a list of words can be interpreted as evidence of primary amnesia only if the other domains enlisted in performance are functioning normally. This framework can be used to analyze each task with respect to its component domains and also to interpret the pattern of task failure at the conclusion of the examination.
W
ExaminingMental State
85 1
search for factors that interfere with the projection networks (e.g., toxic or metabolic or white matter disease); if the second is true, then the search turns to diseases that cause multifocal cortical or subcortical damage. To decide between the alternatives, it is necessary to test each domain in a manner that controls for the attentional deficit. For example, to demonstrate normal retentive memory in the inattentive patient, it is necessary to reduce the attentional load by either repeatedly drilling information before testing recall or by limiting the amount of information to be initially learned (e.g., three words instead of five). PRINCIPLES OF TEST SELECCION
There are many instruments, procedures, and clinical maneuvers that can be used to evaluate mental state. Most seasoned clinicians use a routine set of procedures for which they have internalized standards over many years of experience that allow them to judge the presence and severity of observed deficits. The specific tests that are used in the mental state examination are not as important as the principles that direct their use and interpretation. Two general principles apply to test selection: Each test should contain as few component processes as possible so that it is easier to interpret the source of failure. As in the example given earlier, written calculation is a more direct test of acalculia than mental calculation because the latter could also be disturbed by impaired working memory or diminished arousal. However, written calculation itself becomes an undesirable test of this function in a patient with dysgraphia. The examiner must have a thorough understanding of the processes engaged by any given test. Each task used in the mental state examination should be analyzed with reference to the domains it actually enlists (outlined in Fig. 135-1) to understand the possible sources of failure. Tests should be appropriate for the patient’s level of education, cultural background, and level of life accomplishment. Patients differ with respect to the premorbid level of skill each brings to the examination. Intellectual capacity, education, socioeconomic background, and cultural factors each can influence performance independently, in the absence of brain disease. Therefore, for each domain tested, the clinician should come prepared with tasks at several levels of difficulty: easy, intermediate, and hard. For example, to test persistence without introducing other variables, serial sevens may be appropriate for a patient with a college education, and counting backwards or forwards by ones or even tapping a finger for a minute, would be more appropriate for a patient with a fourth grade education.
Some strategies for bedside and office examination, including clinical case examples, are described in the following sections. Table 135-1 provides a list of procedures and tests for each domain that range in their relative level of difficulty. Even if examination time is limited, every effort should be made to sample all domains to identify where the primary deficit resides and its secondary impact on other parts of the examination. For more comprehensive and precise measurement of mental abilities, including comparison of the patient’s performance against age- and education-relevant norms, it is desirable to have the patient undergo assessment by a skilled clinical neuropsychologist.
rn TABLE135-1. Primary Domains, Test Procedures, and Repercussion of Primary Deficits Domains (Components)
Description
Test Procedures
Repercussion of Primary Deficits.
WAKEFULNESS/ AROUSAL
Level of alertness/consciousness
Rate level of arousal (normal, drowsy, stuporous, comatose, hypervigilant)
Experienced mood Abiliky to sustain behavioral output, cooperate with exam
Assess from interview and observation: euthymic, dysphoric, hypomanic, etc.; labile or restricted affect, normal range; abulic, cooperative
Pervasive; affects performance on all tasks; reduces reliability of other findings for purposes of localization Pervasive; depression, mood instability, or poor cooperation invalidates test results; may lead to underestimating integrity of other domains; reduces reliability of other findings.
Sustained attention and detection of important events; tied to level of arousal
Auditory Continuous Performance: Present up to 300 letters (total of 5 minutes) in random sequence at the rate of one per second, 30 targets ("A") interspersed Digit Span: Present strings of random digits of increasing length, 2 trials at each length; span is longest string that can be repeated without error
(State dependent) MOOD/MOTNATION
(State dependent)
ATCENTION
(State-dependent) Vigilance
Span
Amount of information immediately grasped for further processing; linked to arousal
Perseverance
Sustained behavioral output; closely linked to motivation
Series Generation Tasks: Count back 20 to 1 (easy); recite months in forward then reverse sequence (intermediate); serial sevens (hard)
Response Inhibition
Inhibition of responsesto extraneous or distracting stimuli
Stroop Interference Test: Motor Go No Go procedure
Spontaneous Speech
Self-generated and responsive conversation
Auditory Comprehension
Understanding spoken language, including grammar and word meaning
Repetition
Verbatim repetition of speech
Note articulation, melody, rate (fluency), word-finding pauses, paraphasias, grammaticality in conversation and in speech elicited from a description of a scene or common task ("Describe how you would make a sandwich.") Ask questions that can be answered "Yes" or "No": Do dogs fly? Is a coffee pot alive? If a tiger is killed by a lion, is the lion alive? Is the tiger alive? Ask the patient to repeat: The red book is on the table. No ifs, ands, or buts.
Naming
Oral labeling of visually presented objects
Reading Comprehension
Comprehension of printed words (not necessarily able to read aloud)
Writing
Writing spontaneously and to dictation
Pervasive; affects performance on all tasks
Limits quantity of information intake, e.g., fewer story elements or words can be learned on memory tests, or grasped for language comprehension or repetition tasks Patient gives up easily; diminished spontaneous recall on memory tests; "pseudoneglect" on drawing and cancellation tests due to failure to persist at task Patient may respond impulsively in general, giving rise to high error rate despite presenred capacity
LANGUAGE
Show patient a watch and ask to name parts: face, hands, stem, crystal, band, clasp Present the following sentence and ask the patient to pick the correct word to complete it "The man drove his car down the to work." accelerator wheel road town Ask patient to write a spontaneous sentence and one to dictation; check for spelling, grammar
Even mild aphasia interferes with all tasks that rely on speech output (e.g., story or word list recall, digit span, similarities, orientation, etc.) Interferes with performance of all tasks that require comprehension of oral instructions Inabilityto repeat word lists and stories on memory tests; difficulty with digit span task despite normal attention Difficulty providing similarities or recalling specific words after a delay interval Difficulty performing tasks with printed instructions, written stimuli Difficulty performing tasks where writing is a component (eg., calculations, memory recall)
VlSUAySPATW PERCEPTION
Object/Form Perception Spatial Perception
Perception and discrimination of objects and geometric forms Perception of spatial orientation and direction
SPATIAL DISTRIBUTION OF AlTENnON LEARNING AND EXPLICIT MEMORY
Symmetric distribution of attention within both visual fields Acquisition of new information; retention over time; spontaneous recall; recognition
EXECUTIVE FUNCllONS
Complex mental operations involved in reasoning decisionmaking, planning, forethought, etc.
COMPORTMENT
Knowledge and application of rules of social conduct, judgment, insight
Ask if pairs of objects, faces, colors are the same or different Ask if pairs of angles are same or different Ask patient to reach for objects Paper-and-pencil visual target cancellation tasks Three Words Three Shapes Test; Drilled Word Span procedure Drill any information before testing recall after a delay of at least 5 minutes Obtain information from an informant who knows the patient well and note examples of impairments in real life activities Obtain information from an informant who knows the patient well
Y
Ways in which primary deficits interfere with performance on tests not specifically targeted by those tests.
Difficulty on drawing tasks, naming tasks. Difficulty on tasks requiring a spatial judgment Difficulty processing information/ stimuli in the unattendedfield May forget task instructions
Disruptive in daily living activities but may also interfere with planning any sequence of activities on tests in other domains (eg., any multiple choice response task) Most apparent in daily living although may be apparent in patient's lack of social graces -
Chapter 135
TESTING STATE-DEPENDENT DOMAINS Wakefulness, Mood, Motivation Wakefulness (or arousal) is at the basis of all conscious mental activity. Diminished arousal influences performance of tests in all other domains, despite the absence of a primary disturbance in those domains. The level of wakefulness or arousal should be documented before testing. If it is sufficiently impaired, it may be advisable to postpone the examination. The presence of a deficit in arousal reduces the extent to which failure on tests of any other domain represents a primary deficit in that domain or can be reliably localized. Diminished arousal implies interference with the major neurotransmitter projection systems, including the cholinergic pathways from the nucleus basalis and brainstem reticular activating system, serotonergic pathways from the raphe nucleus, noradrenergic pathways from the locus coeruleus, dopaminergic pathways from the substantia nigra and ventral tegmentum, and histaminergic pathways from the hypothalamus. Mechanisms of injury that interfere with these pathways and thereby cause a primary disturbance in all statedependent domains include alterations of the physiologic milieu via a toxic or metabolic disorder, structural damage to their origins, and extensive multifocal structural injury throughout the cerebral cortex or white matter that effectively disrupts cortical modulation by these systems. Mood is the patient’s current feeling state, and affect is the means whereby mood is conveyed in facial and body gestures and tone of voice. It is important to differentiate between the experience of mood and its conveyance. Some patients with focal, right-sided cerebral lesions may lose the ability to convey mood with facial and body gestures, resulting in a mismatch between feelings and appearance. Some patients with bilateral cerebral disease may display pseudobulbar affect or emotional incontinence, an exaggerated display of emotion that lacks the accompanying feeling state. Motivation is the capacity to initiate and sustain goal-directed behavior. A disturbance of motivation often is seen in the form of apathy or, in extreme cases, abulia. These symptoms and decreased initiative and impersistence should be differentiated from depressed mood. Similar to a disturbance of arousal, a disturbance of mood or diminished motivation can also lead to the impression of widespread cognitive deficiencies. Frequent “Don’t know” responses in the abulic patient should be followed up with prompting or cueing because encouragement may overcome the inertia. For example, a patient with abulia secondary to a toxic encephalopathy responded “Don’t know” to most questions asked of him. He denied knowledge of current news events. However, when cued with the name of a celebrity, he provided detailed information about the person and the event. His initial economy of mental effort was overcome by adapting the testing procedures to circumvent a lack of initiative. This method allowed us to conclude that there was no primary defect of memory and therefore no evidence of medial temporal involvement.
The domain of attention comprises several different processes that target internal and external stimuli in the service of current behavioral goals and drives. Not all aspects of attention are state dependent. However, even those that engage other neuroanatomic networks, such as working memory and response inhibition, are discussed in this section because they contribute to setting the
ExaminingMental State
853
overall information processing state within which the examination is conducted. Vigilance, or the maintenance of attention over time, is one component closely linked to the level of arousal. The continuous performance paradigm, in which the patient is asked to detect a particular target (e.g., the letter “A”) occurring repeatedly among a random series of similar stimuli (e.g., other letters) over at least 5 minutes, is one test of this aspect of attention. The digit span is a measure of the immediate span of attention. Normally, people under 65 can repeat a string of six to seven digits. A reduced digit span signifies a limitation on the amount of information that can be processed. For example, a patient with a digit span of four was able to immediately repeat only four items from a ten-item list with which she was presented. After a delay of 10 minutes, however, she recalled all four items. Although an absolute score of four is not considered normal for delayed recall on this test, it nevertheless indicated that she did not have a primary disturbance of retentive memory. Working memory is the capacity for holding information available for brief time intervals to process or manipulate it further. Reciting a string of digits in reverse sequence or reversing the sequence of the months of the year are tasks that tap working memory. Patients with working memory deficits can be easily distracted and may appear forgetful when they are having difficulty holding information long enough for it to be transferred to a more permanent store. Working memory is one component of attention that involves prefrontal cortex. Perseverance, or persistence, is the ability to sustain behavioral output and a coherent stream of thought. Reciting the months in reverse sequence is an intermediate-level test of perseverance that also tests working memory. The patient should first be asked to recite the months in forward sequence. The difference in time to complete both tasks can indicate whether there is a problem with perseverance. Typically, the forward sequence takes 5 to 8 seconds, and the reverse sequence may take twice as long without error. Generation of word lists over a 60-second interval (i.e., words that begin with a specific letter or that belong to a single semantic category) is also useful as a test of perseverance unless the patient has anomia or limited educational experience. Impersistence is reflected in an inability to sustain measured output. Perseveration, the repetition of elements within a task or of a previously appropriate response that is no longer relevant, is another symptom of impaired perseverance. Persistence depends on the level of arousal but may be selectively impaired by prefrontal cortex damage. Patients with impaired attention often are easily distracted. Some also are unable to inhibit an overt response to the distracting stimulus. Response inhibition is another component of attention that can be affected selectively by lesions of the frontal lobe. This function can be tested with a simple bedside adaptation of the “go-no go” procedure or the Stroop interference procedure (Fig. 135-2). In both tasks, competing and usually automatic response tendencies are first established. Normal performance requires the inhibition of one of the responses. In the “go-no go” procedure, the patient is asked to place one hand palm down on a table surface and to raise and quickly lower the index finger in response to a single loud tap of the examiner’s pencil. The patient is instructed not to respond if the examiner delivers two taps in quick succession. After a few practice trials, the examiner then delivers a random series of one or two taps. Deficits in response inhibition are manifested as errors of commission (i.e., lifting the finger in response to the “no go” signal).
854
Behavioral Neurologyand Epilepsy W
Behavioral Neurology
FIG. 135-2. A modification of the Stroop procedure. First ask the patient to read aloud the color words (white, black, and grey). Next,
ask the patient to name the colors in the middle box. Finally, ask the patient to name the colors of the ink of the words in the bottom box. The classic stimuli for this task are the colors red, green, and blue. However, this variation lends itself to being easily reproduced and brought to bedside.
Arousal, mood, motivation, and all aspects of attention are essential for complex mental activity. A primary deficit in any one of these domains has a ripple effect throughout the examination, even to the extent that other findings may be invalidated. Thus, caution must be exercised in interpreting findings in patients with primary impairments in these domains. The localizing value of symptoms in other domains is diminished in the presence of primary impairment in any of the state-dependent domains. The differential diagnosis of primary impairments in state-dependent domains is lengthy and, except in rare instances, does not implicate a single focal cortical lesion. Structural damage to components of the frontal network can also give rise to selective disturbances in attention and motivation because of its extensive connectivity with other areas of association cortex. TESTING CHANNEL-DEPENDENT DOMAINS Language Current notions of the neural control of language make obsolete the designation of aphasia as “receptive” or “expressive.” It is now understood that distinct components of language processing, namely morphosyntactic, semantic, lexical, and phonological, are modulated by different subsectors of the left cerebral neuroanatomic network supporting language and its connections with extralanguage brain regions. Lesions in the language network, therefore, can selectively impair one type of processing across all modalities of input and output. Traditional testing of language focuses on the integrity of different modalities of language use (i.e., auditory comprehension, repetition, reading comprehension, speaking, writing), but it is also necessary to specify the nature of the deficit. For example, a patient may meet classic criteria for the diagnosis of Broca’s aphasia, which specifies that comprehension is intact. However, lesions associated with Broca’s aphasia often interfere with
grammatical processing, and so comprehension of word order and words that convey syntactic information (i.e., prepositions, morphological endings) also is usually impaired despite preserved comprehension of nouns. To conclude that comprehension, or receptive language, is preserved in such a patient therefore would not be accurate. Speech is evaluated for articulation, melody, pitch, fluency, rate, grammaticality, and evidence of word-finding difficulty. Fluency in part is determined by the number of words uttered per unit time, or phrase length. Phrase length can range from one word per utterance (nonfluent) to seven or more (fluent). Fluency is also affected by the presence of dysarthria. Auditory comprehension should be tested with items requiring only a “yes” or “no” response, eliminating other factors such as speech or motor output (e.g., “DO dogs fly?”). Grammatical comprehension can be tested with questions such as “Do you put on your shoes before your socks?” A patient with a syntactic processing deficit may correctly answer the first question but not the second. Lengthy questions may exceed a patient’s immediate attention span, and commands that require a physical action may not be carried out despite preserved comprehension if apraxia is present. Reading comprehension can be tested by asking the patient to silently read a short sentence from which a word is missing and to select the missing word from four choices (Table 135-1). Repetition is tested by having the patient repeat a grammatically complex but short sentence, such as “No ifs, ands, or buts.” Writing is usually impaired in the same manner as speech in the patient with aphasia. An isolated disturbance of writing, or agraphia, however, may be a common manifestation of impaired attention in the acute confusional state. Naming of objects is a very sensitive test of the integrity of the language system because it is affected by lesions almost anywhere in the language network. An effort should be made to present less common items for naming, such as parts of objects (i.e., lapel of a jacket, hem of a skirt, crystal of a watch, eraser of a pencil). Naming deficits can represent a failure of access to the lexicon or may also occur with a disturbance of semantic processing. Visual or spatial perception deficits can interfere with naming and must be ruled out before failure to name on visual confrontation is interpreted. Visual agnosia can be differentiated from naming failure if the patient is able to name the item by tactile exploration. Modality-specific naming deficits (e.g., tactile anomia) are rare but can be tested by eliciting naming in response to objects presented visually, tactually, and auditorily. The melodic features of speech production, or prosody, can be selectively affected by lesions in the right cerebral hemisphere. Such alterations may make a patient incapable of conveying affect through tone of voice or using prosody as a device to lend emphasis in conversation. For example, depending on the conversation that precedes this utterance, saying “Margo plays the piano” or “Margo plays the piano” bears different referential meaning. If the preceding statement were “Does Margo play the harp?” then the latter prosodic pattern would be appropriate in response. Asking the patient to repeat sentences that vary in their emphasis or affective tone can serve as a test of this function. Aphasia can be localized to damage to the left perisylvian region of the brain. Further precision may be possible based on the clinical nature of the aphasia. Thus, nonfluent speech with preserved semantic comprehension often is associated with damage to Broca’s area and surrounding cortex. However, because of the nature of large-scale networks, the lesion may be located in a less expected portion of the network, such as the thalamus or
Chapter 135 W
Examining Mental State
855
even Wernicke’s area. In addition to the localizingvalue of aphasia, its presence necessitates testing the integrity of other domains with methods that bypass the aphasia (i.e., using nonverbal materials and pantomime to demonstrate to the patient the expected task performance). Visual Perception
Constructions often are used to assess visual perception. However, constructions also enlist other mental domains. Failure to draw a clock, copy a cuhe, or assemble puzzles, for example, can reflect executive function deficits in the presence of normal perception. Thus, it would be inaccurate to conclude that impaired constructions imply parietal lobe damage. However, if an alert, attentive, and cooperative patient cannot decide whether one geometric figure is in the same plane as another or whether two angles are similar (Fig. 135-3), then localization to networks involved in visual perception is more reliable. Prosopagnosia, the inability to recognize familiar faces, can be differentiated from a more basic facial discrimination problem by having the patient judge whether two photographs depict the same person. A disturbance of the spatial distribution of visual attention in the form of hemispatial neglect can be measured in the visual modality with target cancellation tasks (Fig. 135-4).Note the point of origin of the patient’s search. Patients with right cerebral lesions may begin on the right side of the page and search in an erratic fashion, even in the absence of clinical neglect. Deficits in visual perception and hemispatial neglect interfere with performance of all tests that entail visual inspection or reproduction of designs and figures. Hemispatial neglect can be localized to one sector of a large-scale network for the spatial distribution of attention. Persistent right-sided hemispatial neglect often is a sign of bilateral lesions. Disorders of spatial perception usually are associated with damage to the visual pathways that are directed dorsally to the parietal lobe, the “where pathways.” The
FIG. 135-3. (A) Object sorting task. Ask the patient to divide the objects into two groups, each characterized by a distinctive feature. Once this has been done, ask the patient to think of another way to divide the objects into two different groups. One strategy is to group all the ovals and all the hexagons. The other strategy is to group all the white objects and all the black objects. (B) Test for spatial perception. One of the fwe angles to the right of the vertical line must be matched to the sample on the left.
FIG. 135-4. Performance of a patient with left-sided hemispatial neglect on the visual target cancellation test of Weintraub and Mesulam. The task is to circle all the& The density of targets and their irregular arrangement is helpful in detecting subtle neglect when other similar measures may not be as sensitive.
classic disturbance of spatial perception seen in Balint’s syndrome, for example, is a result of biparietal damage. Disorders of object and color perception imply damage to the ventrofugal visual pathways, the “what pathways.” Prosopagnosia and some forms of visual object agnosia are associated with lesions in the lingual and fusiform gyri of the inferior temporo-occipital area and in the lateral and mesial aspects of temporal cortex.
Explicit Retentive Memory Orientation (e.g., to place, time, examiner’s identity) and the ability to learn new information and retain it over time are key elements of retentive memory. Knowledge of current news or personal events is an informal measure of the integrity of explicit memory. “Three Words-Three Shapes” is a simple bedside procedure to test learning, retention, and retrieval of verbal and nonverbal material in the visual modality (Fig. 135-5). After copying the six stimuli, without forewarning, the patient is asked to immediately reproduce them (incidental recall). If five of the six stimuli are recalled (defined as criterion level of learning) delayed recall can be tested 5, 15, and 30 minutes later (or at other intervals as time permits). If the patient recalls fewer than five from incidental memory, the examiner re-exposes the original stimuli for a 30-second interval, after which the patient is asked to immediately draw them again (study-recall trial). Drilling proceeds in this manner until at least five items are reproduced or five study-recall trials are exhausted. This procedure is necessary to ensure that the information for which retention will be tested has first been acquired and to control for the impact of poor attention. Then delayed recall is tested as described earlier. After the final delayed recall trial, multiple-choice recognition can be tested. The number of items recalled after each delay is a measure of the rate of forgetting, which is accelerated in the amnestic syndrome. The drilled word span procedure can also be used to test learning and recall. Select a list of words equal in length to the
856
BehavioralNeurology and Epilepsy Confusional State Primary Deficit Inattention
Behavioral Neurology
Probable Alzheimer's Disease Primary Deficit: Amnesia
a
B
Comportment, Executive Functions, and Reasoning
B
D
differentiating primary amnesia from memory failure secondary to attentional and motivational deficits. The amnestic syndrome is characterized by normal immediate recall and impaired delayed recall (i.e., rapid forgetting) in the context of a normal level of attention and motivation and normal language and perception. It is a sign of damage to the limbic system that is almost always bilateral. Patients with primary amnesia are not able to recall information after even brief distraction and after a delay interval. Inattentive patients may have difficulty initially learning information but then can retain it over time (Fig. 135-5). Occasionally, however, severely inattentive or abulic patients may be unable to spontaneously retrieve information despite remembering it, and this is often confirmed by normal recognition.
D
FIG. 135-5. Three Words-Three Shapes Test. After copying the three words @ride, hunger, and stution) and the three designs, incidental recall is tested, followed by testing of delayed recall. Left column: Sample taken from a 75-year-old woman in an acute confusional state caused by medication effects. Right column: Sample taken from a 64-year-old man with a progressive decline in memory subsequently autopsy-confirmed as Alzheimer's disease. (A) Copy; (B) incidental recall; (C) recall after three additional study-recall trials for the confused patient to reach criterion, and only one such trial for the amnestic patient; (0) spontaneous recall after a 30-minute delay. The confused patient took more trials to learn the stimuli but then retained them well after the delays. The amnestic patient needed only one additional trial to learn the stimuli but then forgot the information over time. In the first instance, there was no evidence of a primary disturbance of memory. In the second, primary amnesia accounted for test performance.
patient's digit span minus one (i.e., the word span). Drill these words until the patient can repeat them successfully three times in a row. If the patient still has difficulty with this list length, drop to a level at which the list is repeated without error. Test recall after a 60-second interval without distraction. Poor performance at this point indicates that the patient is internally distracted or lacks motivation. If recall is less than perfect, repeat the drilling procedure. Then, test recall after another 60 seconds filled with a distracting activity, and again after 3 minutes. Multiple-choice recognition is tested after the final delayed recall trial. Recall after each delay interval with distraction is a measure of retention and retrieval. Recognition testing can determine whether there is a deficit in retrieval. This procedure is especially helpful in
These domains are made up of mental processes that orchestrate behavior and make it adaptable to the social setting and moment-to-moment contingencies. Comportment consists of behaviors that support social interaction and the ability to alter behavior based on the social context. Executive functions are mental processes that organize and sequence behavior and guide decision making and the ability to act appropriately in uncertain or unexpected circumstances. Reasoning is the ability to abstract categoricalsimilarities and to move flexibly from one point of view to another in arriving at a solution to a problem. Impairments in these domains are among the most common in clinical practice. Testing judgment and reasoning in the clinician's office is exceedingly difficult. Asking a patient what should be done in the event of a fire in a movie theater is a useful measure of judgment only if the patient provides the wrong answer. A correct answer may only indicate conventional knowledge of the appropriate response and does not guarantee that the patient would act appropriately in the real situation where there are many contingencies and alternative options. A patient's insight into his or her own symptoms, decisionmaking ability, and reasoning about everyday issues and health care decisions can provide clues about the integrity of these domains. More reliable information about the patient's judgment, social behavior, and decision-making ability may need to be obtained by questioning family members or other informants. In general, with the patient's permission, the examiner should always seek corroboration from an informant because many forms of brain disease interfere with insight and adequate self-perception of symptoms. Proverb interpretation is commonly used as a test of reasoning, but it may not be suitable in patients with limited education. Moreover, responses to familiar proverbs may be highly overlearned. Reasoning tests that emphasize categorization and mental flexibility, such as object-sorting tasks (Fig. 135-3), can be used to demonstrate primary deficits in this domain. Deficits in executive functions may have a pervasive influence on performance of tests that entail organization and sequencing. For example, a patient with a disturbance of executive functions performed very poorly on a test that required matching a photograph of a face with one of six alternative choices. Because there was no other evidence that this patient had a primary disturbance of visual perception, the examiner adapted the testing procedure to prevent impulsive responses by exposing only one face at a time and asking whether it matched the stimulus face. With that adaptation, the patient demonstrated normal facial
Chapter 135
discrimination and the examiner reaffirmed a primary disturbance of executive functions. The frontal lobes and their extensive connections with other cortical and subcortical regions (frontal network) provide the neuronal substrate for these complex behaviors. The extensive connectivity of the frontal lobes helps to explain why many multifocal brain diseases (e.g., toxic and metabolic encephalopathy, multiple bilateral strokes, hydrocephalus) result in so-called frontal symptoms in the absence of structural injury to the frontal lobes. SUMMARIZING AND INTERPRETINGTHE EXAMINATION
At the completion of the examination, the clinician can review the patient’s performance and rank the domains in order of the level of impairment in each normal or mildly, moderately, or severely impaired. In many instances it is possible to pinpoint one primary domain of impairment. In others, there may be multiple domains of impairment. In yet others, a single deficit may interfere with performance of tests in other domains that themselves are not primarily involved. The clinician must determine whether there is one or more primary deficits and what the relative contribution of each is to the overall clinical picture. Reference to the hierarchy outlined in Fig. 135-1is helpful in this regard. Once the clinical profile is established, the neuroanatomic localization follows. Table 135-2 outlines some common neurobehavioral syndromes and their associated clinical profdes and neuroanatomic localization. The principles of examination and interpretation outlined in this chapter apply not only to patients with focal cerebral lesions but also to those with developmental syndromes and neurodegenerative diseases. Developmental syndromes, such as dyslexia and the social-emotional processing disorder, can be quite selective in terms of anatomic and behavioral specificity. Similarly, in early stages of neurodegenerative disease, pathology can be highly anatomically selective, giving rise to fairly behaviorally focal deficits that can be identified with the clinical profile approach outlined in this chapter. EXAMINING FOR DEMENTIA IN OLDER ADULTS
Rapid developments in the study of Alzheimer’s disease have refined clinical methods for detecting dementia and differentiating it from age-related cognitive change. The use of mental state screening tests has become common in the primary care setting. Instruments such as the Mini Mental State Examination and the
Examining Mental State
857
Blessed Dementia Scale and qualitative rating scales such as the Clinical Dementia Rating and the Global Deterioration Scale have all improved the quantification of dementia severity. These instruments are very helpful, once dementia is detected, to stage disease and track changes over time. However, as public awareness of the implications of mental decline with aging increases, patients are seeking medical assessment earlier in the course of illness, at a time when only mild cognitive change, and not dementia, may be present. Because screening instruments are insensitive to the earliest changes, it is advisable to have the patient undergo neuropsychological assessment that is more likely to detect subtle abnormalities of mental state. Such evaluation is conducted with the understanding that test scores play only a small role in the clinical neuropsychologist’s contribution to the assessment of dementia. For example, forms of dementia in which memory, language, and visual perception are not impaired, such as frontal lobe dementia, are more likely to be detected with specialized testing and interview techniques than on the routine mental state examination or even after administration of many standardized tests. The principles of examining mental state and interpreting the findings, outlined earlier, also apply to the evaluation of the patient with the progressive mental state changes of neurodegenerative or vascular dementia. The goal remains to identify the primary domain of impairment. This is easy to do in the very earliest stages of disease because it is now well established that most degenerative brain diseases tend to target specific brain regions at the onset. However, this may be more difficult once the disease has progressed to involve multiple cortical areas and multiple domains. Even in that circumstance, though, the examiner can assess the relative degree of impairment among the domains. Thus, the clinical syndrome of probable Alzheimer’s disease includes deficits in memory and other cognitive functions, but the memory deficits typically are more salient and continue to remain more pronounced than other deficits until late stages of illness. The challenge in identifjmg primary domains of impairment is well illustrated in the examination of a patient with primary progressive aphasia, a dementia syndrome in which language progressively deteriorates in the absence of other cognitive deficits for at least 2 years. Because memory testing usually relies on language, the examiner must demonstrate the integrity of memory by other means. Nonverbal recall tests offer one method. Gathering information about daily living activities that imply the presence of normal memory may provide the only means in the severely aphasic patient. One patient with severe language
w TABLE 135-2. Profiles of Common Neurobehavioral Syndromes on Mental State Testing RUMIN NNROC~GNIIM DOMINS
Syndrome
Aphasia syndrome Hemispatial neglect B a h t syndrome Acute confusional state Dyslexia Probable Alzheimer‘s disease Primary progressive aphasia Depression Schizophrenia
Attention
Mood
Language
Complex Visual Perception
Explicit Memory
Reasoning/ Comportment
UnderlyingAnatomy
Left perisylvian Right frontal, parietal, cingulate Bilateral occipito-parietal # 0 0 0 0 Frontal lobe or frontal network # Left perisylvan # Medial temporal (limbic), parietal # 0 0 Left perisylvian # # d 0 0 Transmitter projection systems # # Frontal network #, Primary domain of impairment +, Impairment may be present due to overlap in neuroanatomical networks subserving affected domains or to the multifocal nature of the causative disease agent 0,Performance on tests of this domain may suffer secondary to primary impairment
+
+
#
+
+
+
+
# #
+
858
Behavioral Neurology and Epilepsy rn Behavioral Neurology
comprehension and speech deficits traveled by air to Chicago from his home in New York and negotiated ground transportation to make his doctor’s appointment without assistance. In the case of frontotemporal dementia, the entire mental state examination might be normal, with the only evidence of abnormality coming from information from a family member or friend about changes in the patient’s characteristic behavior.
SUMMARY The examination of mental state unfolds in a dynamic interaction between the examiner and patient, driven by a firm understanding of psychological principles of behavior, the demands that even simple tasks make on mental processing, and principles of neurobehavioral organization. The selection of tests depends on how well each can test the examiner’s hypothesis about the nature of the mental state abnormality and by factors determined by the individual patient’s background. The detection of a clinical profile of primary and secondary deficits and areas of preserved functioning leads to identification of the anatomic networks affected by the disease. This profile can also be helpful in educating patients and those who care for them and in designing appropriate interventions to augment functional status.
ACKNOWLEDGMENTS Work on this chapter was supported in part by Alzheimer’s Disease Core Center grant AG13854 to Northwestern University, Chicago, Illinois. The author wants to thank Dr. Gabriel Uger and Dr. Gulustu Kaptanoglu for their critical reading of the manuscript and Caralynn Nowinski for technical assistance.
SUGGESTED READINGS Herndon RM (ed): Handbook of Neurologic Rating Scales. Demos Vermande, New York, 1997 Lezak M: Neuropsychological Assessment. 3rd Ed. Oxford University Press, New York, 1995 Mesulam MM Attention, confusional states and neglect. pp. 174-256. In Mesulam MM (ed):Principles of Behavioral and Cognitive Neurology. 2nd Ed. Oxford University Press, New York, 2000 Mesulam MM: Behavioral neuroanatomy: large-scale networks, association cortex, frontal syndromes, the limbic system, and hemispheric specializations. pp. 1-120. In Mesulam MM (ed): Principles of Behavioral and Cognitive Neurology. 2nd Ed. Oxford University Press, New York, 2000 Mesulam MM. The human frontal lobes: transcending the default mode through contingent encoding. pp. 8-30 In Stuss DT, Knight RT (eds): The Frontal Lobes. Oxford University Press, New York, 2002 Salmon DP, Thal LJ, Butters N, Heindel WC Longitudinal evaluation of dementia of the Alzheimer type: a comparison of 3 standardized mental status examinations. Neurology 4 0 12251230, 1990 Spreen 0, Strauss E A Compendium of Neuropsychological Tests. Oxford University Press, New York, 1998 Tombaugh TN, McIntyre NJ: The Mini-Mental State Examination: a comprehensive review [see comments]. J Am Geriatr SOC40922-935, 1992
Weintraub S: Neuropsychological assessment of mental state. pp. 121-173. In Mesulam MM (ed): Principles of Behavioral and Cognitive Neurology. Oxford University Press, New York, 2000 Weintraub S , Mesulam MM: Four neuropsychological profiles of dementia. In Boller F, Grafman J (eds): Handbook of Neuropsychology.Vol. 8. Elsevier, Amsterdam, 1993
136 Evaluation of Patients with Dementia Bruce H. Price and Martin A. Coldstein DEFINING DEMENTIA Dementia is a clinical syndrome, not a specific diagnosis; therefore, it can be produced by a wide variety of causes. Dementia can be defined as a sustained or progressive decline in cognition or comportment caused by chronic brain dysfunction. It can be reversible or irreversible, dramatically progressive or indolent, and can be characterized by isolated or multiple cognitive deficits. Occurring via acute or more commonly insidious onset mental decline, dementia gradually interferes with activities of daily living (ADLs) appropriate for age and background. In many ways dementia diagnosis and management are at the epicenter of revolutionary advances in basic and clinical neuroscience. In contrast to conditions that impede intellectual development, dementia involves the loss of acquired cognitive abilities. Dementia is therefore distinguished from mental retardation by the requirement that a patient’s function has declined from a previously higher capacity. A diagnosis of dementia implies cognitive impairments that compromise personal, social, or vocational function and persist for a minimum of several months. Deficits can occur in any
combination of comportmental, cognitive, affective, and perceptual domains. Several authors specify that impairment involve at least three of the following functional capacities: attentional matrix, language, memory, visuospatial skills, executive abilities, and personality. Although memory loss sometimes is considered a prerequisite to diagnosis, amnesia is neither ubiquitous nor necessarily prominent in all forms of dementia. Furthermore, cognitive and social abilities can be differentially affected by dementia; patients with severe but focal cognitive deficits can retain their functional independence, whereas those with mild impairments affecting socially critical functions may need extensive supervision. Table 136-1 provides the current international criteria standard for the diagnosis of dementia; Table 136-2 summarizes core components of the widely used Diagnostic and Statistical Manual, Fourth Edition, (DSM-IV) diagnostic criteria. Dementia severity can be gauged in social terms as well as by nature and degree of cognitive impairments. Dementia is considered mild when the affected person continues to conduct basic activities such as dressing, grooming, eating, and toileting without assistance. Patients with moderate dementia depend partially on
858
Behavioral Neurology and Epilepsy rn Behavioral Neurology
comprehension and speech deficits traveled by air to Chicago from his home in New York and negotiated ground transportation to make his doctor’s appointment without assistance. In the case of frontotemporal dementia, the entire mental state examination might be normal, with the only evidence of abnormality coming from information from a family member or friend about changes in the patient’s characteristic behavior.
SUMMARY The examination of mental state unfolds in a dynamic interaction between the examiner and patient, driven by a firm understanding of psychological principles of behavior, the demands that even simple tasks make on mental processing, and principles of neurobehavioral organization. The selection of tests depends on how well each can test the examiner’s hypothesis about the nature of the mental state abnormality and by factors determined by the individual patient’s background. The detection of a clinical profile of primary and secondary deficits and areas of preserved functioning leads to identification of the anatomic networks affected by the disease. This profile can also be helpful in educating patients and those who care for them and in designing appropriate interventions to augment functional status.
ACKNOWLEDGMENTS Work on this chapter was supported in part by Alzheimer’s Disease Core Center grant AG13854 to Northwestern University, Chicago, Illinois. The author wants to thank Dr. Gabriel Uger and Dr. Gulustu Kaptanoglu for their critical reading of the manuscript and Caralynn Nowinski for technical assistance.
SUGGESTED READINGS Herndon RM (ed): Handbook of Neurologic Rating Scales. Demos Vermande, New York, 1997 Lezak M: Neuropsychological Assessment. 3rd Ed. Oxford University Press, New York, 1995 Mesulam MM Attention, confusional states and neglect. pp. 174-256. In Mesulam MM (ed):Principles of Behavioral and Cognitive Neurology. 2nd Ed. Oxford University Press, New York, 2000 Mesulam MM: Behavioral neuroanatomy: large-scale networks, association cortex, frontal syndromes, the limbic system, and hemispheric specializations. pp. 1-120. In Mesulam MM (ed): Principles of Behavioral and Cognitive Neurology. 2nd Ed. Oxford University Press, New York, 2000 Mesulam MM. The human frontal lobes: transcending the default mode through contingent encoding. pp. 8-30 In Stuss DT, Knight RT (eds): The Frontal Lobes. Oxford University Press, New York, 2002 Salmon DP, Thal LJ, Butters N, Heindel WC Longitudinal evaluation of dementia of the Alzheimer type: a comparison of 3 standardized mental status examinations. Neurology 4 0 12251230, 1990 Spreen 0, Strauss E A Compendium of Neuropsychological Tests. Oxford University Press, New York, 1998 Tombaugh TN, McIntyre NJ: The Mini-Mental State Examination: a comprehensive review [see comments]. J Am Geriatr SOC40922-935, 1992
Weintraub S: Neuropsychological assessment of mental state. pp. 121-173. In Mesulam MM (ed): Principles of Behavioral and Cognitive Neurology. Oxford University Press, New York, 2000 Weintraub S , Mesulam MM: Four neuropsychological profiles of dementia. In Boller F, Grafman J (eds): Handbook of Neuropsychology.Vol. 8. Elsevier, Amsterdam, 1993
136 Evaluation of Patients with Dementia Bruce H. Price and Martin A. Coldstein DEFINING DEMENTIA Dementia is a clinical syndrome, not a specific diagnosis; therefore, it can be produced by a wide variety of causes. Dementia can be defined as a sustained or progressive decline in cognition or comportment caused by chronic brain dysfunction. It can be reversible or irreversible, dramatically progressive or indolent, and can be characterized by isolated or multiple cognitive deficits. Occurring via acute or more commonly insidious onset mental decline, dementia gradually interferes with activities of daily living (ADLs) appropriate for age and background. In many ways dementia diagnosis and management are at the epicenter of revolutionary advances in basic and clinical neuroscience. In contrast to conditions that impede intellectual development, dementia involves the loss of acquired cognitive abilities. Dementia is therefore distinguished from mental retardation by the requirement that a patient’s function has declined from a previously higher capacity. A diagnosis of dementia implies cognitive impairments that compromise personal, social, or vocational function and persist for a minimum of several months. Deficits can occur in any
combination of comportmental, cognitive, affective, and perceptual domains. Several authors specify that impairment involve at least three of the following functional capacities: attentional matrix, language, memory, visuospatial skills, executive abilities, and personality. Although memory loss sometimes is considered a prerequisite to diagnosis, amnesia is neither ubiquitous nor necessarily prominent in all forms of dementia. Furthermore, cognitive and social abilities can be differentially affected by dementia; patients with severe but focal cognitive deficits can retain their functional independence, whereas those with mild impairments affecting socially critical functions may need extensive supervision. Table 136-1 provides the current international criteria standard for the diagnosis of dementia; Table 136-2 summarizes core components of the widely used Diagnostic and Statistical Manual, Fourth Edition, (DSM-IV) diagnostic criteria. Dementia severity can be gauged in social terms as well as by nature and degree of cognitive impairments. Dementia is considered mild when the affected person continues to conduct basic activities such as dressing, grooming, eating, and toileting without assistance. Patients with moderate dementia depend partially on
Chapter 136
TMLE 136-1. ICD-10 Criteria for the Diagnosis of Dementia Impairment of short- and long-term memory (more accurately of anterograde memory) At least one of the following: Impairment of abstract thinking Impairedjudgment Other disturbance of higher cortical function Personality change Memory impairment and intellectual impairment causing significant social and occupational impairment Absence of occurrence exclusively during the course of delirium Either of the following: Evidence of an organic factor causing impaired memory and intellect Impaired memory and intellect cannot be accounted for by any nonorganic mental disorder Adapted from InternationalClassification of Disease.
others for these activities, and in severe stages these functions must be provided by caregivers. The same terms are used to describe the severity of neuropsychological deficits in dementia (e.g., mild, moderate, severe memory loss). To identify the underlying disease process causing a dementia, all aspects of the patient’s medical history, family history, and clinical examination (medical, neurologic, psychiatric) must be considered, along with appropriate laboratory investigations. Dementia features such as age at symptom onset, nature and severity of cognitive and behavioral deficits, and progression pattern are considered in evaluating the differential diagnosis of a dementia. Neuropathologic examination of the brain at autopsy usually conclusively establishes the nature of the underlying disorder and constitutes the gold standard against which accuracy of antemortem diagnosis is measured. The neuroanatomic, neurohistologic, and neurochemical underpinnings of dementia vary depending on specific causes. Most dementing processes preferentially involve certain cell types or neurotransmitter systems. Consequently, not all mental faculties
Evaluation of Patients with Dementia
859
are affected simultaneously. Cognitive profile often is dictated more by neuroanatomic lesion site than by specific histopathology. Several dementias reflect direct damage to cortical association areas (e.g., asymmetrical cortical degeneration). In other cases, dysfunction is secondary to impairment of interconnected subcortical areas such as basal ganglia, thalamus, and limbic structures. Disruption of white matter pathways, whether multifocal (as in multiple sclerosis) or confined to single areas such as the genu of the internal capsule (as in strategic infarct dementia), can critically slow or disconnect neocortical areas, thereby resulting in dementia. Degeneration of brainstem or basal forebrain nuclei that normally provide specific neurotransmitters to cerebral cortex can also contribute to dementia, particularly when involvement includes cholinergic or monoaminergic systems.
EPIDEMIOLOGY The overall prevalence of dementia is about 10% in patients over 65. Prevalence increases almost exponentially with age, from an estimated 2% in those under 65,8% to 25% in those 65 to 85, and 25% to 40% in those 85 and older. Prevalence is slightly greater in women than men. The incidence of dementia is more pertinent to diagnosis. Between ages 65 and 75, the number of new cases is less than 1:lOO per year. After age 75, yearly incidence rises to at least 2:lOO. In the East Boston study, yearly incidence of Alzheimer’s disease (AD) alone rose to 8.4 per 100 in individuals older than 85. In the Rotterdam study, a population-based prospective cohort study among almost 8000 subjects over age 55, overall prevalence was 6.4% and overall incidence was 1 per 100 person-years. Both prevalence and incidence increased strongly with age; typical incidence estimates for age 65, 75, and 95 were 1 per 1000, 1 per 100, and 1 per 10 person-years, respectively. It is estimated that one in six men and almost one in three women will suffer from dementia at some point.
TAU 136-2. Selected DSM-IV Dementia Criteria Dementia of the Alzheimer‘s type
Vascular dementia
Development of multiple cognitive deficits manifested by: Memory impairment One or more of the following: Aphasia Apraxia Agnosia Executive dysfunction The cognitive deficits in criteria A1 and A2 cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning The course is characterized by gradual onset and continuing cognitive decline The cognitive deficits in criteria A1 and A2 are not caused by any of the following: Other CNS conditions Systemic conditions Substance-induced conditions The deficits do not occur exclusively during the course of a delirium Development of multiple cognitive deficits manifested by Memory impairment One or more of the following: Aphasia Apraxia Agnosia Executive dysfunction The cognitive deficits in criteria A1 and A2 cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning Focal neurologic signs and symptoms or laboratory evidence indicative of cerebrovascular disease are judged etiologically related to the disturbance The deficits do not occur exclusively during the course of a delirium
Adapted from Diagnostikand StatistjcalManual of Mental Disorders, Fourth Edition.
860
BehavioralNeurology and Epilepsy
Behavioral Neurology
TMLE 136-3. Classifying Cognitive Dysfunction Cognitive Impairment
Primary or Secondary Process
Potential Reversibili
Examples
Encephalopathy Dementias
Secondary Secondary
Usually reversible Sometimes reversible Irreversible Irreversible
Toxic or metabolic B,, deficiency Creutzfeldtdakob disease Alzheimer's disease
Primary
DlFFERENTIATlNC DEMENTIA FROM OTHER MENTAL DISORDERS
When a patient is referred for assessment of cognitive decline, the first necessity is to differentiate dementia from other psychiatric disease, focal neurologic syndromes, and confusional states (Table 136-3). A principal goal of initial clinical evaluation is to find a treatable cause. Although there can be much phenomenologic overlap (e.g., subdural hematoma can manifest as delirium or as a reversible dementia), clinicians need to consider the following questions: Does this patient meet criteria for a dementia? If the patient is demented, is it secondary to a potentially reversible cause? If irreversible, what type of dementia is it? Although only about 10% to 15% of dementias are reversible, and only a fraction of these are completely reversible, the possibility of reversing or at least arresting the disorder by appropriate treatment justifies careful diagnostic investigation. Risk of missing a treatable dementia mandates screening investigation for reversible causes. Diagnosis is important in some cases for purposes of genetic counseling or for alerting family members and medical personnel of risk of an infectious etiologic process. DelirSum/EncephalopaUly/Acute Confusional State Several terms are applied to acute or subacute sensorium disturbance; delirium, encephalopathy, and acute or subacute confusional state are essentially equivalent clinically and can be used interchangeably. The sine qua non clinical feature of delirium is a clouded sensorium (see Chapter 139). Although dementia involves cognitive impairment in the context of an awake patient with a clear sensorium, acute confusional states often are misdiagnosed as dementia (Table 136-4). Patients with delirium commonly experience fluctuations in levels of consciousness, with consequent gross attentional impairments; in contrast, patients with dementia often have nearly normal attention spans throughout mild and moderate stages of illness. Abnormalities of level of consciousness
rn TMLE 136-4. Contrasting Features of Delirium and Dementia Feature
Delirium
Dementia
Onset Course Duration Attention
Acute or subacute Fluctuating Limited Impaired
Language Speech Visual hallucinations Tremor Myoclonus Electroencephalogram
Incoherent Slurred, dysarthria Common Common Common Prominent abnormalities (e.g., encephalopathic triphasic waves)
Insidious Persistent Chronic Intact until more advanced stages More coherent Usually intact Uncommon Uncommon Variable Minimal changes (e.g., slowing)
are unusual in dementia until the disorder is far advanced. Another key distinction between delirium and dementia is time course. Delirium by definition is acute or subacute, its onset occurring over hours to days. Amnedc Syndromes
Amnesia, a disorder of memory, can occur as a component of a multifaceted mental status change, such as delirium or dementia, or as an isolated abnormality. When occurring as an isolated cognitive deficit, it is sometimes clinically useful to consider amnesia as a distinct nosologic category (see Chapter 142 for detailed discussion).
Aging Although cognitive deficits in older adults often are attributed to aging, it is important to emphasize that normal aging is not associated with dramatic declines in recent memory or other cognitive functions. Aging is associated with increased susceptibility to a variety of medical disease processes, but major mental decline is not the natural course of old age. Although interpretation of what is normal cognitive aging is complicated by daunting methodologic issues, cognitive functions that should remain preserved over the lifespan include temporal orientation, immediate attention, vocabulary, and most visuospatial skills; delayed recall in healthy older adults can be preserved into the tenth decade. Mild age-related decrements involve difficulties with sustained attention, visual greater than verbal memory recall, confrontation naming, mental flexibility, and response speed. Episodic memory declines with age, but semantic, implicit, procedural, recognition, and working memory remain largely intact. Furthermore, mild age-related cognitive decrements may be counterbalanced by improvements in vocabulary, judgment, insight, and wisdom. In sum, normal cognitive aging, even into the ninth decade, is compatible with independent living. It is therefore inaccurate to attribute significant memory complaints or other cognitive impairment merely to consequences of normal aging. We summarize consensus opinion regarding normal agerelated cognitive changes in Table 136-6.
rn TABLE136-5. Medication Classes Often Associated with Encephalopathy Cholinergic antagonists Benzodiazepines Barbiturates Narcotics H, antagonists P-Blockers Sympathomimetics Digoxin Dopamine antagonists Dopamine anonists
Chapter 136
TABLE 136-6. Cognitive Changes Associated with Normal
Aging Finding with Functional Domain Attention
Normal Aging
Sustained Selective
Memory
Language Executive function Visuospatial function
Registration Short-term Long-term Working Syntax Naming Integration Planning Response inhibition Perceptual Constructional
Processing speed
Presenred into eighth decade Presenred into ninth decade Presenred Declines Presenred Impaired Presenred Gradual decline Declines Declines Declines Declines Declines Gradually progressive slowing
Evaluation of Patients with Dementia
861
APPROACH TO DIAGNOSIS Recognizing Dementia Barriers to detecting dementia in routine practice are formidable. Patients rarely seek medical attention for their symptoms; in fact, a lack of insight into the symptoms is a common feature of the early stages of the disorder. Assessment of dementia often is driven by family concerns, but this can be inefficient. Family members often delay bringing the person with symptoms of dementia to a physician. Reasons for delay include lack of ongoing contact with a failing older adult or lack of appreciation of the patient's loss of function and physician failure to respond to family concerns. Furthermore, physicians too often do not perform mental status examinations adequate for early dementia detection. Consequently, physicians detect dementia only occasionally in the absence of specific patient or family complaints. History from a collateral source, adequate mental status examination, and a competent neurologic examination are paramount to an accurate dementia diagnosis (Table 136-10).
rn TABLE 136-7. Mild Cognitive Impairment Criteria Memory complaint, preferably corroborated by an informant Objective memory impairment Normal general cognitive function Not demented
w TABLE136-8. Relative Alzheimer's Disease Incidence Rates, General Population Versus Patients with Mild Cognitive Impairment Dementia Incidence Rate Patient Population
per Year
General population
0.2%
Ages 65-69 Ages 85-89 Patients with mild connitive imoairment
Mild Cognbe Impairment
The diagnosis of mild cognitive impairment (MCI) has been the subject of increasing clinical and empiric attention. Although MCI is reviewed in Chapter 142, we briefly mention it here because the diagnosis becomes a consideration in the differential diagnosis of cognitive impairment and carries significant implications for long-term patient monitoring. Table 136-7 summarizes current criteria for MCI. The significance of MCI diagnosis is underscored by results of meta-analyses indicating that patients characterized as being cognitivelyimpaired but not meeting clinical criteria for dementia have a high risk of progressing to dementia in general and AD in particular (Table 136-8). The American Academy of Neurology (AAN) recently issued practice parameter guidelines for detecting MCI in the context of such epidemiologic data strongly suggesting MCI's relevance to early detection of dementia; the major recommendations are summarized in Table 136-9.
W
3.9% 6%-25%
TABLE 136-9. AAN Practice Recommendationsfor
Monitoring Patients with Mild Cognitive Impairment Patients with mild cognitive impairment should be recognized and monitored for cognitive and functional decline because of their higher risk for subsequent dementia. General cognitive screening instruments (eg., mini-mental status exam [MMSEI) are useful for detecting dementia when used in patient populations with suspected cognitive impairment (eg., caused by age or presence of memory dysfunction). Neuropsychologicalbatteries are useful in identifying patients with dementia, particularly when administered to a population at higher risk of cognitive impairment. Adapted from Peterson RC, Stevens JC, tanguli M et al: Practice parameters: early detection of dementia: mild cognitive impairment (an evidence-basedreview). Neurology 56:1133-1142,2001
rn TABLE136-10. Sample Schema for Initial Approach to Dementia Differential Diagnosis D
l
m
~G~ ~ A~R Ac~ ~ E I I I ~ C S
Histoy
Examination and Diagnostics
Syndrome
Presentation within weeks or months of symptom onset Motor abnormalities developing with cognitive impairment Alterations in judgment and social behavior Prominent anterograde amnesia of gradual onset Vascular disease
Seizures, headaches, unexplained motor abnormalities Extrapyramidal signs
Rapidly progressive dementia
Executive deficit exceeds anterograde amnesia Relative absence of extracognitive signs
Dementia associated with extrapyramidal features Frontotemporal dementia Alzheimer's disease
Focal lesions on imaging: infarcts
Vascular dementia
862 W TABLE 136-11.
Behavioral Neurology and Epilepsy
w Behavioral Neurology
AAN Practice Parameters for Using
Diagnostic Criteria Sets for Dementia Dementia Tvpe
Diamostic Criteria Set
Practice Parameter
General Alzheimer‘s disease
DSM-IIIR and DSM-IV NINCDS-ADRDA for probable AD DSM-IIIR for DAT Hachinski Ischemic Index Consortium for DLB
Routine guideline Routine guideline
Vascular dementia
Optional
Optional Dementia with Lewy bodies (DLB) Frontotemporal deConsensus diagnostic Optional criteria mentia Rapidly progressive Clinical criteria for O D Guideline Abbreviations: AD, Alzheimer‘s disease; UD, Creutzfeldt-Jakobdisease; DAT, dementia Alzheimer type; DSM, Diagnosticand Statistical Manual of Mental Disorders; NINCDS-ADRDA, National Institute of Neurologic, Communicative Disorders and Stroke-AD and Related Disorders Association. Adapted from Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnoses of dementia (an evidence-based review). Neurology 56:1143-1153,2001
Consensus Criteria and Practice Guidelines Specific individual diagnostic criteria sets have been formulated for most of the major categories of dementia to facilitate diagnostic standardization. How reliably these criteria sets are able to establish a neuropathologically correct diagnosis is addressed in detail for each dementia subtype’s respective section in this volume. In general, criteria of probable AD have good sensitivity for neuropathologic AD but less optimal specificity. Diagnostic criteria for vascular dementia (VAD), dementia with Lewy bodies (DLB), and fronto-temporal lobar dementia (FTLD) do not as neatly correspond to neuropathologic phenotypes; although there are strong clinical-pathologic relationships for these disorders in the majority of patients, many patients present with atypical or nonspecific symptom constellations. The most widely used general diagnostic criteria for dementia are based on definitions contained in the National Institute of Neurologic, Communicative Disorders and Stroke-AD and Related Disorders Association (NINCDS-ADRDA)Work Group and the DSM-IV. The DSM-IIIR definition of dementia was demonstrated to have good to very good reliability; the closely related NINCDS-ADRDA and DSM-IV definitions of dementia have not as yet been subjected to assessment reliability. The AAN issued a revised practice parameter for the diagnosis of dementia in May 2001; recommendations regarding use of diagnostic criteria sets are summarized in Table 136-11.
Diagnostic Workup Patient History. In general, most patients with dementia do not refer themselves. Relatives or associates usually note onset first. Referrals can often occur in crisis settings (e.g., on Monday mornings after a family reunion or Friday afternoons when a family is seeking a weekend respite). Table 136-12 covers the major areas of potential impairment that should be reviewed with a reliable informant (relative or close friend) in a dementia assessment. Detecting dementia in its early stages can be difficult. Routine activities may be less taxing than coping with change; therefore, disruption of ADLs may not be as apparent. The uninformed family can accept “senility” as a normal aging pattern. Highly functioning patients may be able to mask signs of dementia for a protracted time. Most mental status examinations have a ceiling
effect. Results within normal range may still reflect great decline compared with the person’s superior baseline talents. Preexisting asymptomatic lesions in the limbic and association cortex can become symptomatic with normal aging. A detailed patient history can help narrow the differential diagnosis (Table 136-13). Because cognitive impairment must be measured against that person’s baseline, his or her highest degree of formal education, life achievements, and premorbid personality traits should be established first. The family is often but not always a more reliable historian than the patient. Family members may disagree as to time of onset, initial deficits, and sequence of events. Some tend to
H TABLE 136-12.
Dementia Symptoms in Newly Diagnosed (Mild) Patients
Impaired orientation to time, place, person, or situation Impaired recent memory Asking the same question several times over a 5- to 10-minute period Forgetting recent events within a few hours or days Forgetting recent conversations Misplacing items repeatedly Forgetting names of familiar friends or family members Problems with finding words, loss of conversational skills Impaired judgment Loss of interest or inability to perform hobbies or chores, including Use of telephone Managing finances (e.g., checkbook, taxes, bills) Shopping Meal preparation Housekeeping Driving (having accidents, getting lost) Occupational activities Alterations in mood or behavior, such as Subtle changes in interpersonal relationships New-onset anxiety New-onset depression Agitation in the form of paranoia, irritability, or delusional or illogical thinking
TABLE 136-13. Patient History Survey Highest degree of formal education, life achievements, baseline personality traits Impact of decline on activities of daily living Work performance Financial accountability Walking, driving Grocery shopping Household chores Repetition of conversations Misplacement of personal belongings When did cognitive difficulties begin? What was the initial feature? Were the changes abrupt or insidious in onset? Did they resolve, persist without change, or worsen over time? In what sequence were deficits noted? Changes in self-care, personality, behavior Altered language, including word-finding difficulties, paraphasias, diminished fluency, comprehension, or writing Ataxia, incontinence, seizures Underlying illnesses, current medications History of poor nutrition, head trauma, cardiac disease, strokes, atherosclerotic risk factors, subarachnoid hemorrhage, meningitis Exposure to alcohol, illicit drugs, industrial toxins, human immunodeficiency virus, Lyme, syphilis Family history of dementia (e.g., Alzheimer‘s, Pick‘s, Huntington’s, Parkinson’s diseases; spinocerebellar degenerations; Tay-Sachs disease? Confirmed by laboratory tests or brain biopsy? Past or present depression in the patient or patient‘s family
Chapter 136 H Evaluation of Patients with Dementia
863
TABU 156-14. Distinguishing Features of Major Dementia Origins Feature
History
Association
Homosexuality IV drug use Hemophilia Blood transfusion
Human immunodeficiency virus dementia
Family history Headache Vital signs
General examination Cranial nerves
Hypothermia Hypertension Hypotension Bradycardia Meningismus Jaundice Kayser-Reischer rings Papilledema Argyll Robertson pupils Ophthalmoplegia Pseudobulbar palsy
Motor
Tremor Asterixis Myoclonus Rigidity
Chorea Other
Gait apraxia Polyneuropathywith hyporeflexia
use calendar events to date onset, but subtle decline preceding these events often can be elicited. After further reflection, usually during follow-up examination, a more accurate history may be forthcoming. A detailed travel, substance abuse, and sexual history is essential to identify specific pathologic risk factors. Past history of depression in the patient or family suggests a need for further inquiries regarding the possibility of a current mood disorder. Given their genetic implications, a family history of Alzheimer’s, Huntington’s, Parkinson’s disease, or spinocerebellar degeneration obviously influences investigation. Pattern recognition in the differential diagnosis of dementia is essential. For example, a patient with insidious onset of progressive amnesia over months to years suggests the possibility of AD. Language involvement in AD is common, but language impairments are unusual in normal pressure hydrocephalus. Subacute onset with rapid deterioration accompanied by myoclonus, pyramidal, and extrapyramidal signs is more typical of Creutzfeldt-Jakob disease (CJD). A previously fastidious person who over months to years suffers decline in personal hygiene, comportment, and planning with relative sparing of recent memory and language is more likely to have Pick‘s disease. Table 136-14 outlines clinical features helpful in organizing an effective diagnostic approach to dementia. Physical Examination. A thorough physical assessment, including a comprehensive neurologic examination, must be performed on all patients undergoing dementia evaluation.
Huntington’s disease Wilson‘s disease Brain tumor Chronic subdural hematoma Hypothyroidism Multi-infarct dementia Hypothyroidism Hypothyroidism Chronic meningitis Acquired hepatocerebral degeneration Wilson’s disease Brain tumor Chronic subdural hematoma Neurosyphilis Progressive supranuclear palsy Multi-infarct dementia Progressive supranuclear palsy Parkinson’s disease Wilson’s disease AIDS dementia complex Acquired hepatocerebral degeneration Creutzfeldt-Jakob disease AIDS dementia complex Acquired hepatocerebral degeneration Creutzfeldt-Jakob disease Progressive supranuclear palsy Wilson‘s disease Huntington’s disease Wilson’s disease Normal pressure hydrocephalus Neurosyphilis B,, deficiency AIDS dementia complex
Associated Neurologic Deficits. Recognition of associated elementary neurologic deficits can guide dementia differential diagnosis and subsequent investigations (Table 136-15). Impaired visual or auditory acuity can be misinterpreted by patients and their families as cognitive decline. On occasion, it is rewarding to witness the dramatic effects of improved sight and hearing. Normal elementary neurologic examination results in the context of dementia favor Alzheimer’s, Pick‘s, or nonspecific neurodegenerative diseases. Pseudobulbar affect suggests multiple deep lacunae or motor neuron disease, such as amyotrophic lateral sclerosis. Gait abnormalities suggest Parkinson’s disease, frontal network dysfunction, or normal pressure hydrocephalus. Visual field cuts, hemiparesis, and hemineglect are most consistent with cortical infarcts, but adult polyglucosan body disease can present this way as well. Supranuclear gaze paresis suggests progressive supranuclear palsy. Fasciculations, distal atrophy, and bulbar signs in the context of a frontal network dementia point to motor neuron disease. Choreiform movements are not seen in every patient with Huntington’s disease, particularly in those with onset after age 60. Cerebellar signs in the context of dementia constitute a different set of considerations. Mental Status and Neurocognitive Examination. The mental status examination helps corroborate a history of cognitive impairment or establish impairment in the absence of a good history in most forms of dementia. The mental status examination helps to determine whether it is the level or the content of consciousness that is impaired and whether cognitive dysfunction
864
Behavioral Neurology and Epilepsy W
Behavioral Neurology
rn TABLE136-15. Dementias Associated with Noncognitive Neurologic Deficits Abnonnali
Associations
Pseudobulbar affect
Bilateral strokes Demyelinating diseases Motor neuron diseases Parkinson's disease Vascular dementias Normal pressure hydrocephalus Neurosyphilis Progressive supranuclear palsy Tay-Sachs disease Huntington's disease Parkinson's disease Creutzfeldt-Jakob disease Wilson's disease Striatonigral degeneration Mass lesions Cortical strokes Brain abscess Adult polyglucosan body disease Progressive supranuclear palsy Wernicke-Korsakoff encephalopathy Stroke Progressive supranuclear palsy Multiple sclerosis Motor neuron disease Parkinson's disease Paraneoplasia Stroke Motor neuron disease (e.g., amyotrophic lateral sclerosis) Parkinson's disease with dementia Tay-Sachs disease Hallemorden-Spatz disease Parkinson's disease Progressive supranuclear palsy Huntington's disease Wilson's disease Striatonigral degeneration Metachromatic leukodystrophy Vitamin B,, folate deficiencies Thyroid disease Neoplasia Paraneoplasia Creutzfeldt-Jakob disease Paraneoplasia Spinocerebellar degeneration Tay-Sachs disease Gerstmann-Strausslerdisease Hallemorden-Soatz disease
Gait and station
Adventitial movements
Visual fields
Extraocular movements Dysarthria
Pyramidal and motor system
Extrapyramidal
Sensory
Cerebellar
utility for determining dementia origin are summarized in Table 136-16.
Because up to 20% of patients referred for evaluation of intellectual deterioration may have causes that are reversible (e.g., B,, deficiency) or carry potential for preventing of further deterioration (e.g., secondary prevention of vascular dementia progression with antihypertensives or aspirin), the need to avoid missing such diagnoses is imperative. Therefore, selecting which diagnostic investigations to perform becomes the challenge of balancing adequate investigation of dementia cause while minimizing unnecessary testing burden and cost to the patient. A variety of guidelines have been formulated to inform this process; Table 136-17 summarizes the most recent AAN practice parameter recommendations. Psychometrics and Neuropsychological Testing. Formal neuropsychological testing, with far greater diagnostic sophistication and standardized age-related norms, is significantly more precise and quantitatively informative than routine cognitive evaluation procedures (eg., mini-mental status examination). Specific tests of attentional matrix, frontal network functions, memory, language, and visuospatial abilities provide invaluable diagnostic profiles. Such testing also helps clarify possible contributions of normal aging, encephalopathy, and psychiatric disease.
TABLE 136-16. Investigations with Potential Utility in Dementia Diagnosis Blood
Cerebrospinal fluid
is global or circumscribed. To determine the scope of the cognitive dysfunction, various spheres of cognition are tested in turn. These include memory, language, parietal lobe functions (pictorial construction, right-left discrimination, localization of objects in space), and frontal lobe executive or diffuse cerebral cortical functions (judgment, abstraction, thought content, and the ability to perform previously learned acts). Essential components of a proper mental status examination are reviewed in detail in Chapter 135. laboratory Investigations. Dementia is a clinical syndrome principally diagnosed by clinical examination. In determining cause, and most importantly reversible cause, certain diagnostic tests are necessary. Given the many potential dementia origins, many tests are conceivably applicable, and an array of biochemical, hematologic, microbiologic, radiologic, electrophysiologic, and nuclear medicine investigations are available for investigating the cause of a dementia. Laboratory investigations with potential
Urine Biopsy Ophthalmologic screening Electrophysiologic
Radiologic
White blood cell count, hemoglobin and h e matocrit, platelets, differential, mean corpuscular volume Electrolytes Blood urea nitrogen, creatinine, liver function tests Prothrombin time, partial thromboplastin time, fibrinogen Erythrocyte sedimentation rate, antinuclear antibody B,2, folate Ceruloplasmin Lyme, VDRL, human immunodeficiency virus Serum drug levels Heavy metal screen Homocysteine, methylmalonic acid ApoE2.3.4 alleles AP42 peptide, Tau protein, PS-1 HD trinucleotide repeat Protein, cytology, VDRL, Lyme, AFB/viral/ fungal us Protein 14-3-3 Cysticercosis Ab AP42 peptide Tau protein UA
Neme Brain Slit lamp (e.g., Kayser-fleischer rings), pigmentary changes Electrocardiogram Electroencephalogram Muscle Small bowel CXR
Structural imaging magnetic resonance imaging gadolinium Functional imaging (single photon emission computed tomography, positron emission tomography) Multiple inventories
*
Neuropsychological testinn Abbreviations: VDRL Venereal Disease Research Laboratories test; AB, antibody; AFB, acid fast bacteria; CXR. chest x-ray; CXS. cultures; PS- 1, presenilin-1; U& urinalysis. ~~
Chapter 136
Evaluation of Patients with Dementia
865
TMIE 136-17. Summary AAN Practice Guidelines for Diagnostic Evaluation of Dementia Diagnostic Investigation
Practice Parameter
Blood
B,, assessment should be included in routine assessment.
Metabolic Endocrine Infectious
CSF
Structural neuroimaging (0,MRI) Linear or volumetric Cr or MRI Functional neuroimaging
Single photon emission computed tomography Positron emission tomography
Genetic testing
Hypothyroidism should be included in routine assessment. Unless patient has a specific risk factor or evidence of prior syphilitic infection, screening in patients with dementia is not justified. There are no CSF biomarkers recommended for routine use in diagnosing AD. Protein 14-3-3 is recommended for confirming or rejecting the diagnosis of UD. Routine use in all patients. Not recommended for routine use. Not recommended for routine use (absence of demonstrated superiority to clinical criieria). Not recommended for routine use. Apolipoprotein E not recommended for routine use in suspected AD. Not recommended for patients with suspected DLB or UD. Testing for tau mutations is not recommended for routine evaluation in oatients with m D .
Abbreviations: AD, Alzheimer‘s disease; UD, Creutzfeldt-Jakob disease; CSF, cerebrospinal fluid; 0, computed tomography; DLB, dementia with Lewy bodies; m D , frontotemporal lobar dementia; MRI, magnetic resonance imaging. Adapted from Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnoses of dementia (an evidencebased review). Neurology 56:1143-1153,2001
Among degenerative dementias, three patient groups can be grossly identified via principal deficits found on neuropsychological profile: those with amnesia; aphasia, agnosia, or apraxia; and motivation and comportment. The majority of patients with primary amnesia will be found, on postmortem examination, t o have had AD. The second group can demonstrate a mixture of disorders, with a preponderance of Alzheimer’s and vascular elements. Pathology in the third group is more heterogeneous but often includes frontotemporal dementias. Structural Neuroimaging STANDARDSTRU~RAL.Neuroimaging can be an essential aid in
diagnosing structural causes of cognitive dysfunction and demonstrating key findings supportive of a specific dementia origin. One study found the possibility of detecting a clinically significant but covert (i.e., no noncognitive signs or symptoms indicating lesion’s presence) structural lesion (e.g., neoplasm, subdural hematoma [SDH], normal pressure hydrocephalus [NPH]) to be approximately 5%. Table 136-18 summarizes some structural neuroradiographic findings potentially associated with cognitive dysfunction. Computed tomography (CT) and magnetic resonance imaging (MRI) brain scans can be extraordinarily powerful diagnostic aids.
They are easy, safe tests that can detect most intra-axial and extra-axial lesions. Recent AAN practice guidelines include structural neuroimaging with a noncontrast CT or MRI scan as a routine component of the initial evaluation of patients with dementia. CT generally provides adequate data for evaluating atrophy, ventricular system integrity, most hemorrhages (epidural, subdural, subarachnoid, intraparenchymal), and mass effects (e.g., of tumors, abscesses). Consequently, CT usually is adequate to exclude most structurally evident causes of cognitive dysfunction. Although CT usually yields adequate screening data, MRI’s capacity for multiplanar views and multiple imaging sequence modalities provides vastly more information about potential vascular, neoplastic, inflammatory, and infectious causes of cognitive impairment. Sagittal MRI is especially useful for demonstrating the selective lobar atrophies of certain dementia origins (e.g., the focal atrophy attendant to frontotemporal dementias, e.g., knifelike atrophy of the anterior third of the superior temporal gyrus in Pick‘s disease). And only gadoliniumenhanced MRI is truly adequate for ruling out certain serious and potentially treatable conditions (e.g., leptomeningeal disease). Despite promising utility of structural neuroimaging in the assessment of dementia, problems with interpretation are
a TMLE 156-18. Potential Findings on Structural Neuroimaging Associated with Cognitive Dysfunction Svndrome
lmaninn Modalii
Examde NeuroradionraDhic Finding
Subdural hematoma
cr
Normal pressure hydrocephalus Tumor
MRI T2 0,MRI Cr/MRI + contrast
Convexity hypodensity Convexity signal intensity Communicating hydrocephalus Variably enhancing mass lesion, single or multiple White matter signal intensities Lacunar lesions Cortical hypodensity Cortical signal intensity Cortical hyperdensity Cortical signal hypointensity Selective frontotemporal atrophy f Temporal or generalized atrophy Bilateral caudate atrophy Cystic putamenal lesions
Vascular dementia
Small vessel disease Large vessel disease
MRI T2, FLAIR
Subcortical white matter Subcortical gray matter Ischemic
Cr,MRI Cr
Hemorrhagic
Cr
MRI FlAlR MRI GE Frontotemporal lobar dementia Alzheimer‘s disease Huntington’s disease Wilson’s disease Abbreviations: CT,computed tomography; MRI, magnetic resonance imaging.
Cr,MRI Cr,MRI Cr,MRI CT, MRI
866
Behavioral Neurology and Epilepsy
Behavioral Neurology
common. Some patients with dementia can have completely normal structural scans; sulcal widening and ventricular dilation are found in many cognitively intact older adults; some nondemented patients can have multiple lesions without cognitive impact; degree of atrophy is not a reliable predictor of dementia severity; hippocampal atrophy is nonspecific (has also been reported in patients with hypoxia; traumatic brain injury; alcoholism; schizophrenia; and 30% of asymptomatic older adults); and T2 pulse sequence abnormalities on MRI are extremely nonspecific and bear an unclear relationship to type and severity of dementia. Therefore, as with all other tests, structural neuroimaging data must be interpreted within clinical context, bearing in mind these caveats. QUANTITATIVE STRUCTURAL. The hippocampal formation, parahippocampal gyrus, and temporal lobe in general are among brain regions most consistently and crucially implicated in neurodegenerative dementias, especially AD, even at an early stage. Indeed, presymptomatic hippocampal atrophy on MRI has been demonstrated in asymptomatic individuals at risk of autosomal dominant AD. In clinically diagnosed AD of moderate severity, MRI-based volumetric measurements show a reduction of up to 40% in the size of the hippocampus, amygdala, anterior temporal lobe and thalamus. But can structural neuroimaging-based measurements usefully discriminate patients with probable AD from normal older adults? One prospective study of quantitative CT using autopsyconfirmed diagnostic standards found that a medial temporal lobe width falling below the 5th percentile was 95% sensitive but only 40% specific for AD. Several studies without neuropathologic confirmation have reported the utility of medial temporal lobe atrophy, particularly hippocampal or entorhinal atrophy, for the dinical diagnosis of AD. In differentiating clinically diagnosed AD (NINCDS-ADRDA criteria) from normal older adults, the sensitivities of various medial temporal atrophy measures on CT or MRI range from 77% to 92%, with specificities ranging from 49% to 95%. Measurement of the hippocampal formation is arguably more sensitive than temporal lobe measurements in separating controls from people with AD. Neuropsychological assessments of recent memory are highly correlated with visually rated hippocampal atrophy, and hippocampal volume loss is strongly associated with neurofibrillary pathology in AD. Determination of the rate of change of hippocampal atrophy may be of diagnostic value but is unlikely to be of use in clinical practice. Given the proximity of temporal structures to skull bone, artifact hampers CT assessment; MRI provides better visualization of the medial temporal lobes, including the hippocampus. Furthermore, MRI capacity to provide coronal images, in a plane perpendicular to the long axis of the hippocampus, reduces artifact secondary to volume averaging. Normative data for volumetric measurements of the hippocampus and parahippocampal structures are available for comparison. Although automated volumetric techniques are more reliable, they are not widely available. Despite these promising findings, there are no studies determining the added value of hippocampal, entorhinal, or temporal volume measurement once a clinical diagnosis of dementia is made. Combining volumetric data with other potentially informative markers (e.g., apolipoprotein E [APO-E] genotyping, functional neuroimaging) may improve diagnostic accuracy. For clinical purposes, volumetric measurements are helpful but not necessary; visual inspection usually is sufficient.
Functional Neuroimaging Single Photon Emission Computed Tomography (SPEq.
Because perfusion abnormalities in certain dementias often reflect pathologic changes underlying cognitive decline, SPECT has been widely used to investigate dementia. The classic appearance of AD on SPECT is bilateral temporoparietal hypoperfusion. Two SPECT studies with autopsyconfirmed diagnoses examined the value of SPECT in the differential diagnosis of dementia. For differentiating AD from non-AD dementia, hypoperfusion in the temporoparietal lobe was reported to be 86% to 95% sensitive and 42% to 73% specific. Some studies combining assessment of hippocampal atrophy on structural neuroimaging with cerebral blood flow studies on SPECT have yielded sensitivity and specificity rates exceeding 90% in discriminating patients with AD from normal controls. Although encouraging, these figures are not consistently better than those obtained by diagnosis with established clinical criteria; the sensitivity of SPECT alone remains lower than that of clinical diagnosis. Although sensitivity increases as dementia severity worsens, pretest probability of AD also rises. The added value of SPECT is greatest for a positive test among patients with mild dementia in whom there was substantial doubt about the diagnosis of AD. Because frontal hypoperfusion with relative sparing of posterior cortex is characteristic of frontal lobe dementias, SPECT can sometimes be helpful in distinguishing frontotemporal lobar dementias (FTLD) from other dementias. Although temporoparietal hypoperfusion on SPECT is common to both AD and dementia with Lewy bodies (DLB), occipital hypoperfusion is more common in DLB. However, this finding remains insufficiently specific to be relied on for diagnosis. In vascular dementia, SPECT often reveals a scattered or patchy pattern, reflecting the variable localization of vascular-based insults. Despite the promising findings reviewed here, SPECT is generally not recommended in the routine diagnostic evaluation of cognitive impairment. Positron Emission Tomography (Pn). Like SPECT, PET is able to demonstrate functional abnormalities correlating with structural changes. However, PET has the added potential diagnostic value of quantifying neurotransmitter (e.g., cholinergic) and other neurochemical changes. For example, a direct comparison of PET and SPECT in their ability to differentiate AD from vascular dementia (VA) revealed higher diagnostic accuracy for PET regardless of dementia severity. PET scans in AD can demonstrate a characteristic but nonspecific bilateral temporoparietal hypometabolism. A sensitivity of 90% and specificity of 80% are reported when a composite metabolic ratio of affected to unaffected areas is used. In a study of dementia cases undergoing PET and later autopsy confirmation, visual interpretation of PET scans yielded a sensitivity of 93% and a specificity of 63%. FDG-PET may be superior to MRI measures of hippocampal atrophy because cerebral glucose metabolism changes antedate onset of memory decline but MRI hippocampal changes do not. PET may be helpful in distinguishing FTD from AD. Many patients with FTD show hypoperfusion of anterior cerebral cortex with relative sparing of posterior cortex. Like SPECT, despite the potential for significant diagnostic power, the decision to perform a PET scan on a patient being evaluated for cognitive decline must be made on a case-by-case basis. PET scanning appears promising for use as an adjunct
Chapter 136
to clinical diagnosis, but further prospective studies with PET are needed to establish its diagnostic value beyond a competent clinical diagnosis. Therefore, PET is generally not recommended in the routine diagnostic evaluation of cognitive impairment. Serum Genetic Markers. We briefly consider representative dementia subclasses individually. AD. In a large neuropathologically confirmed cohort of patients with dementia, apoliproprotein E4 assay slightly increased the positive predictive value of an AD diagnosis. Relative to the neuropathologic diagnosis of AD, the sensitivity of clinical diagnosis of AD was 92%, whereas sensitivity of having at least one APO-E4 allele was only 65%. In patients with clinical diagnosis of AD, the addition of APO-E testing increased the positive predictive value of a clinical diagnosis of AD by approximately 4% (from 90% to 94%) if an APO-E4 allele was present. In patients with a clinical diagnosis of non-AD, the absence of an APO-E4 allele increased the negative predictive value by 8% (from 64% to 72%). FTLD. A high prevalence of tau mutations was found in a Dutch population (17.8% of all FTLD cases and 40.3% of all familial FTLD cases). However, the diagnostic and prognostic yield from screening of sporadic cases of suspected FTLD for known tau gene mutations is likely to be very low and not routinely recommended. UD. Although familial CJD has been linked to a number of different mutations in the prion gene, and a polymorphism at one codon has been shown to be more common in sporadic CJD, there is no evidence that genetic analysis of the prion gene is of value in diagnosing suspected CJD. In sum, no serum genetic markers are recommended for the routine differential diagnosis of dementia. However, as etiologic mechanisms of dementia are further elucidated, genetic marker assays represent a promising diagnostic strategy. Cerebrospinal Fluid (CSF) Analysis. Although lumbar puncture generally is not indicated in the routine evaluation of clinically typical cognitive impairment, CSF analysis can be an important part of the investigation of atypical dementing processes warranting investigation for evidence of infection, inflammation, demyelination, neoplasia, or paraneoplastic disease, as well as searching for certain markers of neurodegenerative processes. Sensitivityof CSF P-amyloid (1-42) level as a diagnostic marker for AD is high. Reduced P-amyloid (1-42) in CSF of patients with AD compared with normal older adults has been repeatedly observed in multiple studies. In post hoc analyses, moderate sensitivities (78% to 92%) and specificities (81% to 83%) have been achieved in distinguishing patients with AD from normal older adults. Therefore, CSF P-amyloid (1-42) analyses may be of value in the clinical diagnosis of AD, especially in the early course of the disease, when drug therapy may have the greatest potential for being effective but clinical diagnosis is difficult. Unfortunately, it remains unclear whether CSF P-amyloid (1-42) retains diagnostic usefulness in patients with very mild AD. CSF tau is significantly elevated in AD, including early in the AD disease process. Furthermore, this elevation is stable over time, with a low intraindividual variation on repeated sampling. CSF tau can have sufficient sensitivity and specificity to differentiate AD from normal aging and depression, as demonstrated in a large community-based series of consecutive patients with AD. In another study, CSF tau distinguished AD from normal controls with 80% to 97% sensitivity and 86% to 95% specificity. However, CSF tau is found in patients with other neurodegenerative diseases
Evaluation of Patients with Dementia
867
and even nondegenerative neurologic conditions (e.g., stroke). Still, CSF tau assay may be useful in supporting an AD diagnosis early in the disease process when symptoms are vague and clinical diagnosis is difficult. Nevertheless, although sensitivity and specificity of CSF tau measurements appear good, there are no studies that determine the benefits of CSF tau over a precise clinical diagnosis. In contrast to patients with AD who demonstrate elevated CSF tau, patients with FTLD show a significant decrease in CSF tau concentration. CSF analysis for paraneoplastic antibodies in identifymg paraneoplastic limbic encephalitis can be invaluable in attempting to diagnose such a protean and elusive pathologic process. CSF analysis for protein 14-3-3, along with neuroimaging, has revolutionized the diagnosis of CJD. CSF protein 14-3-3 immunoassay has a reported sensitivity of up to 96% and specificity up to 99% for CJD diagnosis among dementia patients who have not had a stroke within one month of testing. Some studies have demonstrated CSF 14-3-3 as superior to electroencephalography (EEG) or MRI in identifymg CJD. However, other neurologic conditions (e.g., stroke, viral encephalitis, paraneoplastic disorders) can yield false positive results, and a negative 14-3-3 immunoassay does not absolutely rule out CJD. Electroencephalogram (EEG). Although utility of routine EEG in the differential diagnosis of dementia is questionable, EEG remains an inexpensive and noninvasive probe of brain function and can help support a specific dementia diagnosis. For example, EEG remains helpful in the diagnosis of CJD, and a correlation has been found between slow-frequency EEG band power and glucose metabolism in vascular dementia, correlating with specific regional metabolic differences. Furthermore, studies using quantitative EEG (qEEG) to predict timing of major clinical events (e.g., loss of ADLs, incontinence, death) have suggested potentially useful associations between voltage change lateralities and disease progression. As previously described, differentiating delirium from dementia is a primary task in the initial assessment of cognitive change. Although the distinction usually is clear-cut clinically, EEG can be useful in detecting a subtle delirium. Delirium characteristics on EEG include slowing or dropout of posterior dominant rhythm, generalized theta or delta slow-wave activity, poor background rhythm organization, and loss of EEG reactivity to eye opening and closing. These are paralleled by qEEG findings of increased absolute and relative slow-wave (theta and delta) power, reduced ratio of fast-to-slow band power, reduced mean frequency, and reduced occipital peak frequency. In alcohol and sedative withdrawal, EEG findings can include voltage attenuation and beta activity prominence. However, despite these fairly robust associations, specificity of EEG and qEEG findings in delirium relative to EEG changes in normal aging and dementia remains suboptimal. Brain Biopsy. Brain biopsy usually is the diagnostic investigation of last resort. The procedure carries several potential drawbacks: Specific histologic diagnosis is not always obtainable, false-positive and false-negative results occur, multiple potential complications (e.g., seizures) can subsequently develop, and anesthesia can worsen the patient’s mental state. However, in certain circumstances, when other diagnostic efforts fail, biopsy can be unavoidable and potentially life-saving (e.g., defining neoplastic disease). Sometimes, alternative disease-affected tissue targets can be considered (e.g., small bowel biopsy may obviate brain biopsy in the diagnosis of Whipple’s disease).
868
Behavioral Neurologyand Epilepsy
Behavioral Neurology
THE IMPORTANCE OF ACCURATE DIAGNOSIS TO CLINICAL MANAGEMENT Although careful diagnosis is always the foundation of highquality clinical management, thorough and accurate diagnosis is imperative for a syndrome as complicated, nuanced, and protean as dementia. This is further accentuated by the frequent need to engineer a multidisciplinary management team, provide family education and support, and prognosticate with reasonable precision. Functional characterization of dementia stages can be clinically helpful. Patients with mild dementias are capable of many ADLs. Those with moderate involvement usually need some level of direct daily assistance. Patients with advanced disease need nearly total assistance. Serial neurologic and neuropsychological monitoring after initial evaluation often clarify disease nature and course. Sudden deterioration after gradual decline suggests “beclouded dementia,” a dementia worsened by superimposed toxic, metabolic, or systemic insults. Autopsy verification establishes definitive diagnosis. Besides providing a basis for further understanding the pathophysiologies of dementias, the finality of diagnosis can help families achieve closure, move on, and understand possible genetic implications. We are entering a remarkable new era in the diagnosis and management of dementia. Dementias regarded as hopeless in the recent past are approached more optimistically. Emerging neurobiologic developments such as new neurotransmitter modulators, pathogenic enzyme inhibitors, genetic recombinant replacement therapies, and the decision-making empowerment bestowed by genetic counseling methods now mandate meticulous attention to dementia diagnosis. The assessment of dementia is no longer a sterile, hopeless intellectual exercise. It now takes a diligent effort that offers increasing hope to many patients and their families.
SUGGESTED READINGS
Desmond DW, Moroney JT, Sano M et al: Incidence of dementia after ischemic stroke: results of a longitudinal study. Stroke (33)922542262,2002
Freter S, Bergman H, Gold S et ak Prevalence of potentially reversible dementias and actual reversibility in a memory clinic cohort. CMAJ 159(6):657-662, 1998
Gifford DR, Holloway RG, Vickrey B G Systematic review of clinical prediction rules for neuroimaging in the evaluation of dementia. Arch Intern Med 160( 18):2855-2862,2000 Goldman W, Price JL, Storandt M et al: Absence of cognitive impairment or decline in preclinical Alzheimer’s disease. Neurology 56( 1):361-367, 200 1
Ihl R, Brinkmeyer J: Differentialdiagnosis of aging, dementia of the Alzheimer type, and depression with EEG-segmentation. Dement Geriatr Cogn Disord Switzerland 10(2):6449, 1999 Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnosis of dementia (an evidence-based review). Neurology 5 6 1143-1153,2001
Lyketsos CG, Lupez 0, Jones B et ak Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA 288( 12):1475-1483,2002 Patterson CJ, Gauthier S, Bergman H et al: The recognition, assessment, and management of dementing disorders: conclusions from the Canadian Consensus Conference on Dementia. CMAJ 160(S12):S1-15, 1999
Petersen RC, Stevens JC, Ganguli M et ak Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review). Neurology 56:1133-1142, 2001 Quinn J, Kaye J: The neurology of aging. Neurologist 7(2):98-112, 2001
Scheltens P Early diagnosis of dementia. J Neurol 246(1):16-20, 1999
Steffens DC, Morgenlander J C Initial evaluation of suspected dementia: asking the right questions. Postgrad Med 106(5):72-76, 79-80,82-83, 1999
Van Crevel H, van Goo1 WA, Walstra GJM: Early diagnosis of dementia: which tests are indicated? What are their costs? J Neurol 24673-78, 1999
Zekry D, Hauw JJ, Gold G Mixed dementia: epidemiology, diagnosis, and treatment. J Am Geriatr SOC50(8):1431-1438, 2002
Breteler MM, Ott A, Hofman A The new epidemic: frequency of dementia in the Rotterdam study. Haemostasis 28(3-4):117-123, 1998
137 Alzheimer’s Disease: Diagnosis, Pathophysiology,
and Treatment Kirk R. Daffner MAGNITUDE OF THE PROBLEM Alzheimer’s disease (AD) is the major cause of dementia in the United States and constitutes a significant and growing health care problem. The prevalence of AD has risen steadily as the average age of the population has increased. It has been estimated that up to 10% of Americans age 65 and older suffer from the disease, and for the population age 85 and older estimates of the prevalence have been as high as 47%. As many as 4 million Americans may suffer from AD, at a cost of more than $100 billion per year for
their care. Based on current estimates, if no effective preventive measures are developed, in 50 years there will be as manv as 14 million patients witi AD in the‘ United States alone.
CLINICAL PROFILE Neurodegenerative diseases such as AD must be understood as having a clinical and pathologic dimension. It is extremely rare to have access to brain tissue to make a pathologic diagnosis in living patients. The approach adopted has been to identify clinical
868
Behavioral Neurologyand Epilepsy
Behavioral Neurology
THE IMPORTANCE OF ACCURATE DIAGNOSIS TO CLINICAL MANAGEMENT Although careful diagnosis is always the foundation of highquality clinical management, thorough and accurate diagnosis is imperative for a syndrome as complicated, nuanced, and protean as dementia. This is further accentuated by the frequent need to engineer a multidisciplinary management team, provide family education and support, and prognosticate with reasonable precision. Functional characterization of dementia stages can be clinically helpful. Patients with mild dementias are capable of many ADLs. Those with moderate involvement usually need some level of direct daily assistance. Patients with advanced disease need nearly total assistance. Serial neurologic and neuropsychological monitoring after initial evaluation often clarify disease nature and course. Sudden deterioration after gradual decline suggests “beclouded dementia,” a dementia worsened by superimposed toxic, metabolic, or systemic insults. Autopsy verification establishes definitive diagnosis. Besides providing a basis for further understanding the pathophysiologies of dementias, the finality of diagnosis can help families achieve closure, move on, and understand possible genetic implications. We are entering a remarkable new era in the diagnosis and management of dementia. Dementias regarded as hopeless in the recent past are approached more optimistically. Emerging neurobiologic developments such as new neurotransmitter modulators, pathogenic enzyme inhibitors, genetic recombinant replacement therapies, and the decision-making empowerment bestowed by genetic counseling methods now mandate meticulous attention to dementia diagnosis. The assessment of dementia is no longer a sterile, hopeless intellectual exercise. It now takes a diligent effort that offers increasing hope to many patients and their families.
SUGGESTED READINGS
Desmond DW, Moroney JT, Sano M et al: Incidence of dementia after ischemic stroke: results of a longitudinal study. Stroke (33)922542262,2002
Freter S, Bergman H, Gold S et ak Prevalence of potentially reversible dementias and actual reversibility in a memory clinic cohort. CMAJ 159(6):657-662, 1998
Gifford DR, Holloway RG, Vickrey B G Systematic review of clinical prediction rules for neuroimaging in the evaluation of dementia. Arch Intern Med 160( 18):2855-2862,2000 Goldman W, Price JL, Storandt M et al: Absence of cognitive impairment or decline in preclinical Alzheimer’s disease. Neurology 56( 1):361-367, 200 1
Ihl R, Brinkmeyer J: Differentialdiagnosis of aging, dementia of the Alzheimer type, and depression with EEG-segmentation. Dement Geriatr Cogn Disord Switzerland 10(2):6449, 1999 Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnosis of dementia (an evidence-based review). Neurology 5 6 1143-1153,2001
Lyketsos CG, Lupez 0, Jones B et ak Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA 288( 12):1475-1483,2002 Patterson CJ, Gauthier S, Bergman H et al: The recognition, assessment, and management of dementing disorders: conclusions from the Canadian Consensus Conference on Dementia. CMAJ 160(S12):S1-15, 1999
Petersen RC, Stevens JC, Ganguli M et ak Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review). Neurology 56:1133-1142, 2001 Quinn J, Kaye J: The neurology of aging. Neurologist 7(2):98-112, 2001
Scheltens P Early diagnosis of dementia. J Neurol 246(1):16-20, 1999
Steffens DC, Morgenlander J C Initial evaluation of suspected dementia: asking the right questions. Postgrad Med 106(5):72-76, 79-80,82-83, 1999
Van Crevel H, van Goo1 WA, Walstra GJM: Early diagnosis of dementia: which tests are indicated? What are their costs? J Neurol 24673-78, 1999
Zekry D, Hauw JJ, Gold G Mixed dementia: epidemiology, diagnosis, and treatment. J Am Geriatr SOC50(8):1431-1438, 2002
Breteler MM, Ott A, Hofman A The new epidemic: frequency of dementia in the Rotterdam study. Haemostasis 28(3-4):117-123, 1998
137 Alzheimer’s Disease: Diagnosis, Pathophysiology,
and Treatment Kirk R. Daffner MAGNITUDE OF THE PROBLEM Alzheimer’s disease (AD) is the major cause of dementia in the United States and constitutes a significant and growing health care problem. The prevalence of AD has risen steadily as the average age of the population has increased. It has been estimated that up to 10% of Americans age 65 and older suffer from the disease, and for the population age 85 and older estimates of the prevalence have been as high as 47%. As many as 4 million Americans may suffer from AD, at a cost of more than $100 billion per year for
their care. Based on current estimates, if no effective preventive measures are developed, in 50 years there will be as manv as 14 million patients witi AD in the‘ United States alone.
CLINICAL PROFILE Neurodegenerative diseases such as AD must be understood as having a clinical and pathologic dimension. It is extremely rare to have access to brain tissue to make a pathologic diagnosis in living patients. The approach adopted has been to identify clinical
Chapter 137 W Alzheimer‘s Disease: Diagnosis, Pathophysiology, and Treatment
profiles that provide accurate estimates of the likelihood of underlying neuropathology. Patients with a clinical diagnosis of probable AD have a very high probability of having the plaques and tangles that define AD pathologically. Likewise, patients who have underlying Alzheimer’s pathology have the greatest risk of developing the clinical syndrome of probable AD. Probable AD presents clinically as an insidiously progressive illness in which memory decline is one of the salient features. Family members may note that the patient is increasinglyforgetful of appointments, names, and events, repeats the same stories or questions, and tends to misplace items. Early in the course of the disease, mental state testing tends to reveal preserved autobiographic information, variable recall of recent events, and subtle disorientation. Even in the mildest cases, acquisition of bits of information that exceed digit span is impaired. There is difficulty retrieving newly learned information even after short delays. Patients with such symptoms tend to perform better with recognition memory tasks. Over time, patients exhibit increasing problems with learning new information and even recognizing simple material. In addition to memory deficits, patients with probable AD also tend to exhibit disruptions in executive functions, language, and visual spatial abilities. Disturbance in complex attention (controlled information processing, response selectivity and inhibition, and divided attention) often is the first nonamnestic function to be affected. Studies have indicated that impairment of executive function is very strongly associated with the amount of care a patient needs, even after controlling for overall dementia severity. Language impairments are also extremely common. Patients tend to have naming difficulties and empty fluent speech, consistent with features of anornic, transcortical sensory, or Wernicke’s aphasia. The ability to generate lists of words based on semantic category (e.g., animals, grocery items) often is impaired. The addition of such a task to mental state tests has been shown to enhance diagnostic accuracy. Many patients exhibit abnormalities in visuospatial functioning, both the visuoconstructive (e.g., drawing cubes or intersecting pentagons) and visuoperceptual (e.g., matching the angles made by pairs of lines) aspects and are at risk of experiencing spatial disorientation. Table 137-1 summarizes clinical, imaging, biologic, and pathologic aspects of probable AD. Workup for a patient suspected of having Alzheimer’s disease should follow the guidelines reviewed in Chapter 136. A good history from a reliable informant about the patient’s baseline and changes in cognitive and behavioral status is invaluable. A detailed mental state examination, as reviewed in Chapter 135, is essential
TMLE 137-1. Probable Alzheimer‘s Disease: Summary Clinical Presentation
Pathophysiologic Information
Insidiously progressive decline in cognitive and functional status Major memory problems Disrupted executive functions, language, visuospatial functions Nonfocal neurologic examination
MRI/CT scans: generalized atrophy, loss of hippocampal volume SPECT: hypoperfusion in temporoparietal f frontal regions Genetics: chromosome 14.1.21 (autosomal dominant), chromosome 19 (APOE) Pathology: plaques and tangles most common Prominent distribution of pathology: limbic regions and association cortex
869
for establishing a patient’s current level of cognitive functioning and for illuminating a profile of salient deficits. Most challenging is to identify patients who are in the very earliest stages of the illness, when many of their basic activities of daily living are not clearly disrupted. As much as possible, a person’s current abilities should be compared with his or her own premorbid baseline functioning and not only with reported conventional norms for a particular age. It is essential to follow such patients longitudinally to establish a clearly progressive course. Although there is disagreement about the cost-effectiveness of clinical neuroimaging in dementia workups, computed tomography (CT) or magnetic resonance imaging (MRI) can rule out lesions such as strokes or tumors that may account for or contribute to a patient’s cognitive decline. Scattered foci of increased T2 signal or even more definitive areas of infarction should not automatically yield a diagnosis of vascular dementia, especially in patients whose clinical profile points to a progressive amnestic dementia. Patients presumed to have a vascular dementia often are found to have coexistent Alzheimer’s pathology. Also of note, several studies have suggested that in patients with underlying AD pathology, even a few subcortical lacunar infarcts can markedly reduce their cognitive and functional status. NEWER DIAGNOSTIC APPROACHES There is strong evidence that the pathologic process of Alzheimer’s disease precedes the development of a clinical dementia by years to decades. As prospects have grown for developing treatments that may slow the underlying disease process, there has been increasing interest in being able to diagnosis AD in its very early or preclinical stages. It has been shown that community-dwelling older adults who exhibit significant impairment in memory are at high risk of developing a clinical dementia over the ensuing 2 to 5 years. This observation has helped to define the category of mild cognitive impairment (MCI), which includes individuals not currently demented but who, for example, score greater than 1.5 standard deviations below norms for memory (see Chapter 142). MFU morphometric analysis of the medial temporal lobe structures has demonstrated significant focal atrophy in patients with probable Alzheimer’s disease and those in preclinical stages. Functional neuroimaging with, for example, single photon emission computed tomography (SPECT) has suggested that the most typical pattern in probable Alzheimer’s disease is bilateral temporoparietal hypoperfusion, with a variable degree of additional bifrontal perfusion abnormalities. Older adults in the preclinical stages of the illness appear to exhibit hypoperfusion of medial temporal, anterior and posterior cingulate, and thalamic regions. Several markers in the cerebrospinal fluid (CSF) may also have diagnostic utility. Compared with that of nondemented controls, the CSF of patients with probable AD tends to have a high level of the tau protein and a low level of amyloid-P peptide (AP). This CSF pattern yields a high specificity (0.81 to 0.95) but only modest sensitivity (0.60 to 0.85). Patients with AD also tend to have an elevated CSF neuronal thread protein, with a reported sensitivity of 0.62 to 0.89 and specificity of 0.88 to 0.95. The value of CSF markers for very early or preclinical diagnosis remains to be determined. CSF proteins are not measured routinely. Currently, genetic markers play a limited role in diagnosing most cases of AD. Autosomal dominant forms of AD (caused by mutations on chromosome 1,14, or 21) only account for a very small proportion of the illness. Their importance lies not in their frequency (which is quite low) but in the information that has been provided to
Behavioral Neurology and Epilepsy
870
Behavioral Neurology
neuroscientists about the pathophysiology of AD. The APOE4 genotype (coded by chromosome 19) is common among patients with AD (about 40% have one or more E4 alleles), but does not serve as a diagnostic test. APOE4 is most appropriately viewed as a susceptibilitygene that increases the risk of a lower age of onset of AD and whose influence occurs in a dose-dependent fashion. A recent study involving a large population of individuals suggested that APOE genotyping in combination with established clinical criteria can improve the specificity of diagnosis. DIAGNOSTIC CRITERIA The salient feature of the most commonly observed dementia syndrome in older adults is a progressive decline in memory that occurs in combination with other cognitive deficits such as executive dysfunction, language impairments, or visual-spatial compromise. On a pathologic plane, this clinical syndrome is most often associated with the plaques and tangles that pathologically define AD. The National Institute of Neurological and Communicative Disorders and StrokeAlzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) Work Group codified the clinical criteria associated with a high likelihood of Alzheimer’s pathology. Criteria for probable Alzheimer’s disease include the presence of dementia, progressive worsening of memory and other cognitive functions, deficits in two or more areas of cognition, no disturbance of consciousness, age of onset between 40 and 90, and the absence of systemic or central nervous system disorders that could account for the dementia. Use of these clinical criteria has yielded diagnostic accuracy in autopsy series of greater than 80%. Other neuropathologic causes of this pattern of progressive amnestic dementia cited in the literature that are much less common than AD include dementia with Lewy bodies, Pick‘s disease, and focal, nonspecific neuronal degeneration. The cognitive profile seen most typically in AD is consistent with the distribution of pathology in this disease and wellestablished brain-behavioral relationships. In the early stages of the illness, pathologic changes, especially the accumulation of neurofibrillary tangles, tend to involve limbic regions and over time spread to neocortical areas. The temporolimbic system has been shown to play a central role in memory processing. Thus, pathology in this region helps to explain the salient memory disturbance observed in Alzheimer’s disease (see Chapter 142). PATHOLOGY AND PATHOPHYSIOLOGY
AD is characterized pathologically by senile plaques (composed of dystrophic neurites and a central core of extracellular deposits of AP), neurofibrillary tangles (composed of paired helical filaments that contain an abnormally phosphorylated protein), significant loss of neurons, and diminished synaptic density. The limbic system and multimodal association areas are particularly ravaged, with the relative sparing of primary motor and sensory cortex.
Although the cholinergic system, arising from the basal forebrain, is significantlydisrupted, many other neurotransmitter systems are damaged as well. Given the wide range of pathology affecting multiple ascending neurotransmitter systems and multifocal areas of cortex involved in different aspects of cognition, it is not surprising that simple pharmacologic interventions for Alzheimer’s disease (e.g., with cholinesterase inhibitors) have had only limited efficacy. According to the amyloid cascade hypothesis (a dominant theory in AD research), AP plays a central role in the pathogenesis of the disease. Based on this model, AD results from excessive production or diminished clearance of AP. This 40- to 42-aminoacid protein is produced through the cleavage of P-amyloid precursor protein (APP) by proteases that have been designated p-secretase and y-secretase. It has been theorized that excessive AP leads to progressive neuronal damage, perhaps through inflammatory and oxidative injury. Increasing neuronal dysfunction and cell death are the source of progressive functional decline and dementia. According to this account, tau abnormalities do not occur early in the pathophysiologic process of AD. Among the strongest pieces of evidence supporting the central role of AP is the observation that the known genetic factors that predispose to AD are associated with an increase in AP peptides or plaques. Table 137-2 summarizes the key chromosomes involved in AD. Many believe that the merits of the amyloid cascade hypothesis will be put to the test through clinical trials involving y-secretase or p-secretase inhibitors that presumably will decrease AP production or immunization with AP, which may inhibit the formation of amyloid plaques and promote their clearance. TREATMENT STRATEGIES Treatment goals for AD are similar to those for any of the dementing illnesses and include the following: eliminating or managing other conditions that contribute to the further decline of a patient’s cognitive and functional status, ameliorating or treating cognitive symptoms, managing or treating behavioral symptoms, slowing the rate of disease progression, delaying the onset of the illness (note that a 5-year delay in onset of symptoms would reduce the number of AD cases by 50%), and preventing disease development. Table 137-3 summarizes treatments that are available, those have been tried without success, and those in current or anticipated clinical trials. Neurologists need to be advocates for their patients with probable AD whose medical problems may be overlooked or undertreated. Patients with probable AD, even very early in the illness, have very low cognitive reserve. They cannot tolerate additional insults to their central nervous system. As noted, among patients with a similar degree of underlying AD pathology, those who have even seemingly subtle subcortical lacunar strokes have been shown to exhibit much greater impairment in cognitive and functional status. We favor aggressive management of concomi-
TABLE137-2. Genetic Factors Predisposing to Alzheimer‘s Disease: Relationship to the P-Amyloid Phenotype Chromosome 21 19 14 1
Gene Defect
Age of Onset
Ap Phenotype
PAPP mutation APOE4 polymorphism Presenilin-1 mutations Presenilin-2 mutations
50s 60s and older 40s and older 50s
7 Production of total AP peptides or of AP, peptides 7 Density of AP plaques and vascular deposits 7 Production of AD, peptides Production of AO., DeDtides
Adapted from Selkoe DJ: The pathophysiology of Alzheimer‘s disease. In Scinto LFM, Daffner KR (eds): Early Diagnosis of Alzheimer‘s Disease. Humana Press, Totowa, NJ, 2000
Chapter 137 W
Alzheimets Disease: Diagnosis, Pathophysiology, and Treatment
871
TABLE137-3. Potential Treatments for Patients with Alzheimer's Disease Twe of Treatment
Medication
status
Comment
Cholinesterase Inhibitors
Tacrine (Cognex) Donepezil (Aricept) Rivastigmine (Exelon) Galantarnine (Reminyl) Metrifonate Hupenine A Milameline 58202026 Vitamin E Selegiline Acetyl-1 -carnithe Propentofylline Prednisone Cox II inhibitors Hydroxychloroquine NSAIDs AIT-082 Nerve Growth Factor Gene Therapy ySecretase Inhibitors P-Secretase Inhibitors Memantine Ampalex Ampakines Injected AP Nasal AP Passive Immunization with AP antibodies Ginkgo Estrogen
FDA approved FDA approved FDA approved FDA approved
The approved cholinesterase inhibitors are for symptomatic, treatment of cognitive and behavioral problems
Statins
Trials under way
Cholinergic Agonists Cerebroprotective Agents
Anti-Inflammatory Agents
Neurotrophic Factors Altering APP Processing to Reduce P-Amyloid Formation Excitatory Neurotransmitter Modulators Vaccine
Other Agents
Withdrawn ADCS study planned No proven efficacy Potential benefit Potential benefit No proven efficacy ? efficacy No proven efficacy No proven efficacy No proven efficacy On-going study No proven efficacy Phase I Phase I trials planned On-going study Phase I1 Phase I1 trial planned Phase II-HALTED No trial currently No trial currently Potential benefit No proven efficacy
? Neuroprotective glial cell modulator Ongoing Primary Prevention Study (NIA) of Naproxen and Celecoxib
Ongoing study of alternative dosages
NMDA antagonist AMPA receptor modulator AMPA receptor modulator Immune-mediated amyloid clearance
Ongoing Primary Prevention Study (Women's Health Initiative)
ADCS =Alzheimer's Disease Cooperative Study; NIA = National Institute on Aging.
tant medical conditions such as cerebrovasculardisease, endocrine disorders, sleep disturbance, pain, and side effects from various medications. The current standard of care for probable AD is to offer patients a trial of a cholinesterase inhibitor to try to ameliorate their symptoms. In general, studies of cholinesterase inhibitors have indicated that patients on these agents show mild but statistically significant improvement compared with patients on placebo in terms of cognitive measures and clinical assessment of global function. Neuropsychiatric symptoms (e.g., hallucinations, apathy, restlessness) also have tended to improve. Relative benefits can continue over several years, and treatment has tended to delay placement of patients into nursing homes. The first U.S. Food and Drug Administration (FDA)-approved cholinesterase inhibitor, tacrine, was frequently associated with elevated liver function test
values and gastrointestinal distress. Subsequent agents have been much better tolerated and include donepezil, rivastigmine, and galantamine. In absence of impartial head-to-head trials, there is limited evidence that one of these agents is more efficacious than another. Preliminary evidence suggests that if one of these medications is not beneficial to a particular patient, another one may prove helpful. Table 137-4 summarizes the dosing schedule and other features of these medications. Many dementia experts would also recommend treatment with vitamin E, a well-tolerated antioxidant. In one study, after adjusting for Mini-Mental State Examination scores at the start of the trial, researchers found that vitamin E delayed the development of severe dementia or death. Although the trial dosage was 2000 IU per day, many clinicians are prescribing lower dosages (e.g., 800 IU). Ginkgo biloba has also been shown to mildly
TABLE137-4. Currently Available Medications Medication
Dosage
Major Side Effects
Comment
Donepezil (Aricept)
Start: 5 mg Objective: 10 mg Increase to 10 mg after 4-6 wk Start: 1.5 mg bid Objective: 6 mg bid Increase by 3 mg -q2wk Start: 4 mg bid Objective: 12 mg bid Increase by 8 muday -q4wk 400-1 000 IU bid 40 mg tid Herbal (over-the-counter)
Gastrointestinal distress
Once-per-day dosing
Gastrointestinal distress
? Impact of its butyl cholinesterase activity on -1 disease progression
Gastrointestinal distress
? Impact of its modulation of nicotinic receptor on -1 disease progression
Increased risk of bleeding at very high dosages No major side effects Well tolerated
Well tolerated; may slow disease progression
Rivastigmine (Exelon) Galantarnine (Reminyl) Vitamin E Ginkgo biloba Huperzine A
N
2x/day (1 00 mg G 5 mg donepezil)
872
BehavioralNeurology and Epilepsy W Behavioral Neurology
TABLE157-5. Neuropsychiatric and Behavioral Problems
in AD Depression Apathy Hallucinations and sensory misperceptions Delusions and memory distortions Agitation and aggressiveness Wandering and restlessness Incontinence
improve cognitive status and functional assessment by caregivers and thus is another therapeutic option. Much excitement has been generated about a possible vaccine for AD utilizing AP peptides, which in mouse models of AD has been shown to promote the clearance of amyloid plaques and in some studies to improve cognitive function. Passive immunization with monoclonal antibodies to AP also have had promising results in mouse models of the disease. Unfortunately, clinical trials in humans of active immunization have been halted because of concerns about the development of treatment-related CNS inflammation. Efforts are underway to better define immune responses elicited by vaccines in order to improve their safety profile and augment understanding of the pathophysiological mechanisms underlying AD. Early trials also have begun for the y-secretase inhibitors, which theoretically should reduce the burden of AP. Epidemiologic studies have raised the possibility that treatment with estrogen, nonsteroidal anti-inflammatory drugs, and (cholesterol-lowering) statins may reduce the probability of developing a dementing illness. To date, clinical trials with anti-inflammatory agents (e.g., prednisone) and estrogen have been disappointing in patients who already carry the diagnosis of probable AD. Prospective studies are under way to help to determine whether these agents can play a role in preventing or delaying the onset of the disease. BEHAVIORAL ISSUES AND THEIR MANAGEMENT
Although the cognitive abnormalities in AD tend to be emphasized, changes in affect, personality, and behavior also are major problems for patients and their caregivers. Table 137-5 lists the most common neuropsychiatric and behavioral issues associated with AD. Fifteen to twenty percent of patients with AD develop symptoms of major depression, most often early in the course of their illness. Because depression may further erode daily functioning and cognitive performance, it is reasonable to have a low threshold for initiating treatment. However, medications for depression must be used judiciously, clearly identifylng target symptoms and watching closely for side effects. Selective serotonin reuptake inhibitors tend to be preferable to tricyclic antidepressants because of their low anticholinergicside effects. In general, it makes sense to avoid drugs with long half lives (e.g., fluoxetine hydrochloride) and to initiate therapy with low dosages. Delusions or fixed false beliefs are also common in AD, occurring in up to 40% of cases, probably more often in midcourse. They often involve the patient’s conviction that someone is stealing from them, that they are not in their own home, or that their spouse is not faithful. Hallucinationshave been reported in approximately 25% of patients with AD. Psychotic symptoms in AD have been associated with a more rapidly deteriorating course. Patients who become agitated or aggressive, especially if this represents a change from or marked exacerbation of their baseline state, may be suffering from a superimposed
toxic-metabolic process. An important service we can perform for our patients is to ensure that intercurrent illnesses or problems are ruled out (Table 137-6). These include infection, medication side effects, pain, constipation, sleep disturbance, or additional medical problems such as cardiac ischemia. Table 137-7 summarizes strategies to manage agitation and other behavioral problems. CONCLUSIONS
AD and the other degenerative dementias should be viewed as chronic illnesses. Rewards to clinicians come from supporting a patient and his or her family through the different stages of the illness. It is essentialto establish a therapeutic relationship with the caregiver and, when possible, the patient. Educating families and caregivers about the illness can enhance their empathy for the patient, increase their tolerance for a range of maladaptive behaviors, establish more realistic expectations, and allow them to prepare for the future. It is important to ensure that the home environment is safe (e.g., limited access to dangerous appliances or utensils) and to establish daily routines for the patient. Table 137-8 summarizes potential social and behavioral interventions. Typically, disruption of routines leads to confusion and to a deterioration in functional status. When unwanted behaviors emerge, it is worthwhile to review the context in which they arose to see whether simple manipulations of the patient’s schedule or environment may be beneficial. It is important to rule out
w TABLE157-6. Conditions to Identify and Treat Infections Medication side effects Metabolic disturbance Organ failure or disease Endocrine abnormalities Pain Sleep disturbance Constipation Cerebrovascular disease
W
TABLE 157-7. Treatment Strategies for Agitation and Behavioral Problems
Nonohamacolonic Amroaches
Phannacolonic Aimroaches
Rule out intercurrent illness and problems (e.g., infection, pain, constipation, sleep disturbance) Ensure a safe environment (limited access to dangerous utensils, appliances) Establish daily routines Limit noise levels Monitor schedule of light and darkness Use gentle distraction (move attention to something else) Calm, soothing approach Cueing Involvement in activities Improve sensory fidelity, if possible (hearing, vision)
Stabilizing anticonvulsant agents Valproic acid Cabapentin (particularly if the patient is also having problems with sleep or pain) Selective serotonin reuptake inhibitors (e.g., sertraline or citalopram) Sedating agents (e.g., trazodone) (although diminished arousal can make mental state worse) Avoid benzodiazepines in general (although on occasion medications such as lorazepam and oxazepam prove beneficial) Neuroleptics Low dosages of risperidoneas effective as haloperidol with fewer side effects. Olanzapine (especially if the patient is not sleeping at night) Quetiapine
Chapter 138
TMLE 157-8. Social and Behavioral Interventions lntewention
Potential Course of Action
Ensure a safe home environment Optimize cognitive abilities
Occupational and physical therapy consultation; home assessment Consider cognitive rehabilitation consultation early in the course: compensatoly strategies (memorization, organizational aides); teaching caregivers cueing and other ways to be helpful Consider power of attorney and guardianship early in the course when the patient is more able to express his or her wishes Education of families about the illness can Enhance empathy for the patient Increase tolerance for a range of maladaptive behaviors Establish more realistic expectations Allow preparation for the future Very high incidence of depression among caregivers Social work Alzheimefs Association (support groups)
Plan for the future
Support and educate caregivers
intercurrent illnesses or problems if a patient demonstrates a more rapid decline in status and exhibits what has been called a beclouded dementia. Communication with the patient’s internist and other physicians is crucial. Support for caregivers, the lifelines of our patients, is essential. Caregiver involvement with local chapters of the Alzheimer’s Association can help reduce the isolation and psychological burden. Social work input also can be extremely helpful to caregivers by increasing services at home, finding appropriate day programs, providing supportive counseling, and reviewing long-term plans for the patient. Studies suggest that such intervention can delay nursing home placement by an average of 6 months.
Non-Alzheimer Dementias
873
We have the tools to provide thoughtful care to our patients with probable AD. Fortunately, we are also approaching a new era in our understanding and treatment of AD. Our knowledge of the basic biology of the disease has grown tremendously. We are nearing the threshold of being able to identify the illness earlier and treating the underlying disease process much more effectively. Combining these new scientific advances with long-standing principles of humane care will help our patients to maintain as much independence and dignity as possible.
SUGGESTED READINGS Doody RS, Stevens JC, Beck C et ak Practice parameter: management of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 56:115&1166, 2001
Evans DA, Funkenstein HH, Albert MS et ak Prevalence of Alzheimer’s disease in a community population of older persons: higher than previously reported. JAMA 262:2551-2556, 1989 Growdon JH, Rosser M (eds): The Dementias. Butterworth-Heinemann, Boston, 1998 Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnosis of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 56:1143-1153, 2001 Mayeux R, Sano M: Treatment of Alzheimer’s disease. N Engl J Med 341(22):1670-1 679, 1999
Scinto LFM, Daffner KR (eds): Early Diagnosis of Alzheimer’s Disease. Humana Press, Totowa, NJ, 2000 Selkoe DJ: Translating cell biology into therapeutic advances in Alzheimer’s disease. Nature 399:23-31, 1999 Terry RD, Katzman R, Bick K L Alzheimer’s Disease. 2nd Ed. Raven Press, New York, 1999 Weintraub S, Mesulam MM: Four neuropsychological profiles in dementia. pp. 253-282. In Boller F, Spinnler H (eds): Handbook of Neuropsychology. Vol. 8. Elsevier, Amsterdam, 1993
138 Non-Alzheimer Dernentias Martin A. Goldstein and Bruce H. Price Although Alzheimer’s disease (AD) is the most common cause of dementia, as many as one third of cases have other causes. It is therefore important to include consideration of non-Alzheimer dementias during assessment of cognitive impairment.
DIFFERENTIAL DIAGNOSIS OF NON-AUHEIMER DEMENTIA CAUSES Familiarity with the clinical presentations of non-Alzheimer dementias facilitates their early identification and therefore can be crucial to successful management of this diagnostic class, which includes reversible and partially reversible syndromes. Table 138-1 lists major dementia types, and Table 138-2 gives estimated prevalences of dementia types derived from retrospective case reviews. Many of these syndromes are addressed in detail in other chapters.
Differentiation between cortical and subcortical dementia profiles can be clinically useful but often anatomically oversimplified because dysfunction is rarely limited to cortical or subcortical regions. Deficits tending to be caused by subcortical disease include slowed and inefficient cognitive processing and alterations in personality, mood, and behavior. Parkinson’s disease, Huntington’s disease, Wilson’s disease, progressive supranuclear palsy, normal pressure hydrocephalus, demyelinating diseases, leukodystrophies, and acquired immunodeficiency syndrome (AIDS)dementia are representative of this subtype. Other disorders such as CreutzfeldtJakob disease (CJD), diffuse Lewy body disease, or neurosyphilis can equally involve both cortical and subcortical structures. Amnesia, cognitive disorganization, and impaired visuospatial skills can be caused by either cortical or subcortical lesions. Table 138-3 contrasts clinical features of cortical and subcortical dementias, and Table 138-4 summarizes subcortical dementia causes.
Chapter 138
TMLE 157-8. Social and Behavioral Interventions lntewention
Potential Course of Action
Ensure a safe home environment Optimize cognitive abilities
Occupational and physical therapy consultation; home assessment Consider cognitive rehabilitation consultation early in the course: compensatoly strategies (memorization, organizational aides); teaching caregivers cueing and other ways to be helpful Consider power of attorney and guardianship early in the course when the patient is more able to express his or her wishes Education of families about the illness can Enhance empathy for the patient Increase tolerance for a range of maladaptive behaviors Establish more realistic expectations Allow preparation for the future Very high incidence of depression among caregivers Social work Alzheimefs Association (support groups)
Plan for the future
Support and educate caregivers
intercurrent illnesses or problems if a patient demonstrates a more rapid decline in status and exhibits what has been called a beclouded dementia. Communication with the patient’s internist and other physicians is crucial. Support for caregivers, the lifelines of our patients, is essential. Caregiver involvement with local chapters of the Alzheimer’s Association can help reduce the isolation and psychological burden. Social work input also can be extremely helpful to caregivers by increasing services at home, finding appropriate day programs, providing supportive counseling, and reviewing long-term plans for the patient. Studies suggest that such intervention can delay nursing home placement by an average of 6 months.
Non-Alzheimer Dementias
873
We have the tools to provide thoughtful care to our patients with probable AD. Fortunately, we are also approaching a new era in our understanding and treatment of AD. Our knowledge of the basic biology of the disease has grown tremendously. We are nearing the threshold of being able to identify the illness earlier and treating the underlying disease process much more effectively. Combining these new scientific advances with long-standing principles of humane care will help our patients to maintain as much independence and dignity as possible.
SUGGESTED READINGS Doody RS, Stevens JC, Beck C et ak Practice parameter: management of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 56:115&1166, 2001
Evans DA, Funkenstein HH, Albert MS et ak Prevalence of Alzheimer’s disease in a community population of older persons: higher than previously reported. JAMA 262:2551-2556, 1989 Growdon JH, Rosser M (eds): The Dementias. Butterworth-Heinemann, Boston, 1998 Knopman DS, DeKosky ST, Cummings JL et al: Practice parameter: diagnosis of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 56:1143-1153, 2001 Mayeux R, Sano M: Treatment of Alzheimer’s disease. N Engl J Med 341(22):1670-1 679, 1999
Scinto LFM, Daffner KR (eds): Early Diagnosis of Alzheimer’s Disease. Humana Press, Totowa, NJ, 2000 Selkoe DJ: Translating cell biology into therapeutic advances in Alzheimer’s disease. Nature 399:23-31, 1999 Terry RD, Katzman R, Bick K L Alzheimer’s Disease. 2nd Ed. Raven Press, New York, 1999 Weintraub S, Mesulam MM: Four neuropsychological profiles in dementia. pp. 253-282. In Boller F, Spinnler H (eds): Handbook of Neuropsychology. Vol. 8. Elsevier, Amsterdam, 1993
138 Non-Alzheimer Dernentias Martin A. Goldstein and Bruce H. Price Although Alzheimer’s disease (AD) is the most common cause of dementia, as many as one third of cases have other causes. It is therefore important to include consideration of non-Alzheimer dementias during assessment of cognitive impairment.
DIFFERENTIAL DIAGNOSIS OF NON-AUHEIMER DEMENTIA CAUSES Familiarity with the clinical presentations of non-Alzheimer dementias facilitates their early identification and therefore can be crucial to successful management of this diagnostic class, which includes reversible and partially reversible syndromes. Table 138-1 lists major dementia types, and Table 138-2 gives estimated prevalences of dementia types derived from retrospective case reviews. Many of these syndromes are addressed in detail in other chapters.
Differentiation between cortical and subcortical dementia profiles can be clinically useful but often anatomically oversimplified because dysfunction is rarely limited to cortical or subcortical regions. Deficits tending to be caused by subcortical disease include slowed and inefficient cognitive processing and alterations in personality, mood, and behavior. Parkinson’s disease, Huntington’s disease, Wilson’s disease, progressive supranuclear palsy, normal pressure hydrocephalus, demyelinating diseases, leukodystrophies, and acquired immunodeficiency syndrome (AIDS)dementia are representative of this subtype. Other disorders such as CreutzfeldtJakob disease (CJD), diffuse Lewy body disease, or neurosyphilis can equally involve both cortical and subcortical structures. Amnesia, cognitive disorganization, and impaired visuospatial skills can be caused by either cortical or subcortical lesions. Table 138-3 contrasts clinical features of cortical and subcortical dementias, and Table 138-4 summarizes subcortical dementia causes.
874
Behavioral Neurology and Epilepsy H Behavioral Neurology
TABU158-1., Differential Diagnosis of Dementia Causes in Adults Degenerative disorders
Vascular dementias
Myelinoclastic disorders
Traumatic conditions Neoplastic dementias
Hydrocephalic dernentias
Alzheimer's disease Frontotemporal dementias Dementias associated with movement disorders
Pick's disease
Parkinson's disease Dementia with Lewy bodies Huntington's disease Progressive supranuclear Pain/ Spinocerebellar degeneration Idiopathic basal ganglia calcification Striatonigral degeneration Motor neuron disease Hallervorden-Spatz disease Lacunar state (multiple subcortical infarcts) Binswanger's disease Mixed cortical and subcortical infarctions Mitochondria1encephalopathies (e.g., MELAS) CADASIL Demyelinating Multiple sclerosis Marchiafava-Bignarni disease Dysmyelinating Metachromatic leukodystrophy Adrenoleukodystrophy Cerebrotendinous xanthornatosis Ceroid lipofuscinosis (Kufs's disease) Polyglucosan body disease Tay-Sachs disease Subdural hematoma Dementia pugilistica Meningioma (especially subfrontal) Gliorna Metastatic lesions Leptorneningeal disease Paraneoplastic Communicating Normal pressure hydrocephalus Noncomrnunicating Aqueductal stenosis lntraventricular neoplasm lntraventricular cyst Basilar meningitis
Inflammatory conditions
Infectionrelated dementias
Metabolic disorders
Endocrinologic disorders Toxic exposures Psychiatric disorders
Systemic lupus erythematosus Temporal arteritis Sarcoidosis Sjogren-Larsson syndrome Granulomatous arteritis Syphilis Lyme disease Herpes encephalitis Chronic meningitis (tuberculosis, fungal) Brain abscess Progressive multifocal leukoencephalopathy Whipple's disease HIV encephalopathy CreuMeldt-Jakob disease Cerstrnann-Straussler disease Subacute sclerosing panencephalitis Hypoxia Hypercapnia Uremia Hepatic encephalopathy Anemia Vitamin deficiency states (B,, folate, niacin) Porphyria Hypoglycemia Wilson's disease Thyroid Adrenal Parathyroid Alcohol-related syndromes Other substance abuse Heavy metals Industrial solvents Depression Mania Schizophrenia Conversion reactions
SECONDARY DEMENTIAS H TABLE138-2. Estimated Prevalences of Common Causes of Dementia Culled from Clinical and
Epidemiologic Series Dementia Type
Relative Prevalence
Percentage Range
Alzheimef 50 25-75 Cerebrovascular" 15 5-30 l e v body 15 5-30 5 Other neurodegenerative 2-20 Alcohol-related 5 2-15 Toxic or metabolic 2 1-15 2 Neoplastic 1-10 Infectious 2 1-5 Acquired hydrocephalus 1-5 2 1 Post-traumatic 1-3 1 1-2 Miscellaneous aMixedAlzheimer and cerebrovascular represent a large proportionof each group's composition.
Potentially Reversible Secondary Dementias
Meta-analyses of dementia studies have revealed at least potential reversibility in approximately 13% of patients (see Table 138-5). The most common causes of reversible dementias are depression and iatrogenic (e.g., adverse drug effect),which together constitute about 50% of reversible dementias. Metabolic disorders are next, followed by normal pressure hydrocephalus. Other causes have indistinguishably small prevalences. Primary Psychiatric Disturbances DEPRESSION. Dementia and depression often are comorbid and can appear remarkably similar. Between 20% and 55% of older
adults with depression develop cognitive impairment phenomenologically consistent with a dementia syndrome; this has commonly been called pseudodementia but is more correctly called the
Chapter 138 W
Non-Alzheimer Dementias
875
TABLE138-3. Distinguishing Characteristics of Cortical and Subcortical Patterns of Dementia Function ~
Cortical Dementia
Subcortical Dementia
Normal Dysnomia Variable aphasias Poor insight Poor judgment Reduced abstraction impaired impaired Anterograde amnesia Agnosia Spared until late impaired Present Less common Disinhibition Apathy or abulia Cerebral cortex
Slowed Spared
~~
Psychomotor speed Language Executive function Memory
Recent
Retrieval and recall Recognition
Remote Motor Visuospatial Agnosias Depression Comportment Neuroanatomy
rn TABLE138-4. Major Causes of Subcortical Dementia Diseases of Subcortical Crav Matter
Diseases of white Matter
Parkinson's disease Huntington's disease Progressive supranuclear palsy Small vessel vascular disease
Small vessel vascular disease Multiple sclerosis Head injury Hydrocephalus Binswanger's encephalopathy HIV
dementia of depression or depression-related cognitive impairment (DRCI). Meta-analytic investigations demonstrate that new antidepressants not only treat depression comorbid with dementia but can also improve cognitive function, suggesting a high prevalence of superimposed DRCI among patients with dementia in general. Patients with DRCI are more likely to complain of memory and concentration problems than patients with degenerative dementia. Also in contrast to patients with degenerativedementia, those with depression can do reasonably well on formal mental status testing when depression-related confounds such as motivation and attention are minimized. Careful bedside mental status or neuropsychological assessment is necessary to establish dementia in a patient with both depressive affective symptoms and cognitive deficits. Although recall is impaired in both dementia and DRCI, depressed patients usually have preserved recognition, whereas patients with an amnestic degenerative dementia have impaired recognition and more intrusion errors. Cognitive testing in depression reveals performance variability and impaired attention with insufficient effort during memory encoding. Examiner tenacity at ensuring successful encoding of short-term memory items is essential to distinguish the memory epiphenomenon of depression-related attention impairment from a primary memory disturbance. Key differences often can be elicited in language functions, which are generally preserved in DRCI but often become impaired in a degenerative dementia. Similarly, apraxias, visuospatial deficits, and gross executive dysfunction, common features of degenerative dementias, are seen only in the most severe forms of DRCI.
Poor problem solving, global slowing impaired Preselved No temporal gradient Early involvement Normal Less significant or absent More common Apathy Subcortical structures Dorsolateral prefrontal cortex
Of note, depression can be an early symptom of several degenerative dementing processes. Despite initial improvement via antidepressant therapy, almost half of older adults with depression-related cognitive dysfunction develop irreversible degenerative dementias within 5 years. Patients with depression unaccompanied by cognitive impairment develop dementia at rates more comparable to that of the general population. Once a single episode of depression complicated by cognitive impairment is documented and treated in an older adult, that patient should be monitored closely for signs of relapse and incipient dementia thereafter. Regrettably, neither clinical features nor currently available biological markers reliably differentiate older adults with a primary dementia from those with DRCI. Nevertheless, consensus heuristics, summarized in Table 138-6,can sometimes be helpful when used cautiously.
Structural NORMAL PRESSURE HYDROCEPHALUS (NPH). Normal pressure hydrocephalus (NPH) can be a structural cause of dementia that is potentially treatable by surgery. A diagnosis originally pioneered by Adams, Hakim, and Fisher, NPH classically presents as a triad of gait apraxia, urinary urgency or incontinence, and mental status changes. Usually developing in late middle or old age, psychomotor slowing combines with cognitive findings suggestive of a mixed cortical and subcortical dementia. Importantly, parkinsonism, sensory complaints, and depression may be associated findings.
TAW15116 Example secondaly Causes'of Dementia cah?PON
Examole
Psychiatric Structural
Pseudodementia of depression Normal pressure hydrocephalus Subdural hematomas Wilson's disease Hypothyroidism Obstructive sleep apnea Vasculitis intracranialtumors Chronic meningitis Medication enceDhalooathv
Metabolic Endocrinologic Respiratory Inflammatory Neoplastic infectious iatrogenic
876 TABU 158-6.
Behavioral Neurologyand Epilepsy
Behavioral Neurology
Distinguishing Features of Dementia and Depression-Related Cognitive Impairment
Dementia
Insidious onset Progressive deterioration No history of depression Patient typically unaware of deficits, does not complain of memory loss Somatic complaints uncommon Variable affect Few vegetative symptoms Impairment often worsens at night Neurologic examination and lab studies often abnormal
Depression-Related Cognitive Dvsfunction
Abrupt onset Plateau of dysfunction History of depression Patient aware of and may exaggerate deficits, often ;om- plains of memory loss Somatic complaints or hypochondriasis common Depressed affect Prominent vegetative symptoms Impairment usually not worse at night Normal examination, normal lab studies
Some patients, especially those with hydrocephalus from meningitis or subarachnoid hemorrhage, can improve after ventriculoatrial, ventriculoperitoneal, or lumboperitoneal shunting. In idiopathic NPH, about half of patients experience sustained improvement, and about one third have a good or excellent response to shunting. Complications of shunting occur in about one third of patients and can include shunt infection, subdural hematoma, and shunt malfunction necessitating revision. NPH is reviewed in detail in Chapter 16. Subdural hematoma (SDH) is the most SUBDURAL HEMATOMA. readily treatable intracranial mass lesion that can cause cognitive dysfunction. Patients aged 50 to 70 years are most commonly affected. The most common precipitating factor is head trauma, which can often be minor. Factors increasing the risk of head trauma or severity of resulting SDH include alcoholism, cerebral atrophy, epilepsy, use of anticoagulants, ventricular shunts, and long-term hemodialysis. SDH is bilateral in about one sixth of cases. Clinical Manifestations. SDH can be clinically quiescent without overt symptoms evident for months. Headache is the most common initial symptom. Neurologic signs including cognitive dysfunction (ranging from mild nonspecific confusion to significant dementia) and contralateral hemiparesis are the most common findings, followed by papilledema and extensor plantar responses. Although seizures are uncommon, they can signal a previously undetected SDH. Diagnostic Investigations. SDH usually can be visualized on noncontrast computed tomography as an extraaxial crescentshaped hypodensity. Usually involving a portion of or, less commonly, an entire cerebral convexity, SDH can also occur above and below the tentorial dural regions. When SDH is convexity based, ipsilateral obliteration of cortical sulci is seen. If it is large, mass effects such as ventricular compression can occur. Neuroimaging should be carefully reviewed for evidence of bilateral subdural collections. Age of SDH can be estimated on computed tomography by evolution of the subdural defect from hyperdense (bright), representing presence of recently accumulated blood, progressing through successive shades of gray, culminating in isodense collections for which contrast infusion may be needed to visualize. Management. Symptomatic hematomas should be surgically evacuated. However, management can be complicated when SDH, especially bilateral SDH, is associated with significant cerebral
atrophy, as is common in older adults, because evacuation can result in recurrent bleeding as atrophy-related tensile forces on subdural space complicate healing. NEOPLASTIC.Brain tumors manifesting solely via progressive cognitive impairment are uncommon. Nevertheless, certain slowgrowing intracranial neoplasms occurring in strategic locations (e.g., frontal or temporal meningioma or low-grade glioma) can be a curable cause of secondary dementia. When otherwise clinically covert (i.e., in the absence of noncognitive neurologic signs), the threshold for performing screening neuroimaging becomes key (see Chapter 136). Metabolic. Almost any metabolic abnormality can affect cerebral function to such an extent as to cause cognitive dysfunction. Most of the major types are reviewed in other sections of this volume devoted to metabolic causes of acute confusional states, such as metabolic deliria (e.g., hepatic encephalopathy). Here we summarize a prototypical example of a metabolic disturbance associated with chronic cognitive dysfunction (i.e., a secondary dementia). WILSON'SDISEASE.Wilson's disease (WD), also known as hepatolenticular degeneration, is an autosomal recessive disorder of copper metabolism that produces neurologic and hepatic dysfunction. Prevalence of WD is approximately 30 per million population. A gene defect has been localized to the long arm of chromosome 13. Pathogenesis involves decreased binding of copper to the transport protein ceruloplasmin, resulting in excessive amounts of circulating unbound copper, eventually depositing in a variety of tissues, most notably brain, liver, kidney, and cornea. Although the average age of onset is 11 years for patients presenting with hepatic dysfunction and 19 years for those with neurologic manifestations, the disease can remain clinically covert until the sixth decade. Ocular and hepatic abnormalities are the most prominent nonneurologic complications of WD. Kayser-Fleischer rings, pathognomonic for WD, are bilateral brown corneal rings resulting from copper deposition and are present in almost all patients with neurologic involvement. The rings are sometimes subtle, detectable only by slit lamp examination. Hepatic involvement can take the form of an asymptomatic rise in liver enzymes, hepatitis, or jaundice; if involvement is chronic, cirrhosis can ensue, with portal hypertension-related complications. Neurologic manifestations reflect disproportionate involvement of the caudate, putamen, cerebellum, and cortex. Signs can include facial grimacing, dysarthria, dysphagia, hypokinesia, abnormal postures, rigidity, resting or postural tremor, choreiform movements, and ataxia. There is a tendency for a dystonic or parkinsonian picture with hyperreflexia and extensor plantar responses to predominate with disease onset before age 20 and for older patients to exhibit tremor, chorea, or ballismus. A wingbeating tremor is a common late manifestation. Seizures sometimes occur. The cognitive impairment of WD is consistent with a subcortical dementia profile marked by generalized thought process slowing, concentration impairment, and secondary memory deficits. Research has been performed to distinguish whether the visuomotor task slowing found in WD is more a product of motor involvement than cognitive deficiency; specially designed neuropsychological batteries controlling for manual dexterity effects confirm motor defect-independent slowing. Psychomotor impairment in WD may result from disrupted cortico-basal ganglionic connections. Associated psychiatric signs include affective, person-
Chapter 138
ality, and behavioral changes; psychoses, including hallucinations, are more rare presentations. Diagnostic testing reveals decreased serum copper (less than 80 pg/dL), low ceruloplasmin levels (less than 20 mg/dL), elevated 24-hour urinary copper excretion (more than 100 pg/24 hours), and abnormal liver function tests. Neuroimaging often demonstrates bilateral cortical and basal ganglia atrophy, with compensatory ventricular dilation. Inconsistently present and unusual characteristics visualizable on structural neuroimaging are basal ganglia cystic degeneration and cavitary necrosis. Liver biopsy reveals marked excess copper and cirrhosis. The principal differential diagnosis based on clinical symptoms is Huntington's disease. Management includes copper chelation by penicillamine and restriction of dietary copper. Treatment response can take months; serial serologic assays and slit lamp examinations can be used to track progress. Treatment is lifelong. Most patients treated early can expect a complete or nearly complete recovery. Siblings of affected patients should be screened for WD with neurologic examination including slit lamp evaluation and serum ceruloplasmin levels. Endocrine Disorders. Multiple endocrinologic disturbances can contribute to cognitive dysfunction. We focus on two prototypical endocrinopathiesknown to cause reversible dementias. HYPOTHYROIDISM. In addition to being a cause of an acute confusional state, hypothyroidism (myxedema) can cause a reversible global dementia characterized by generalized cognitive slowing and nonspecific memory impairment. Common psychiatric signs include depression sometimes complicated by psychotic features including paranoia and hallucinations. Associated neurologic manifestationscan be helpful in suggesting hypothyroidism as an underlying cause of a dementia. Symptoms can include headache, tinnitus, paresthesias, and generalized weakness. Signs include delayed relaxation of deep tendon reflexes, hearing impairment, and typical stigmata of hypothyroidism (e.g., dry skin, pretibial myxedema). Thyroid function tests usually confirm diagnosis. Cognitive dysfunction usually reverses significantly with thyroid hormone replacement. HYPOCORTISOUSM. Patients with severe or chronic adrenal insufficiency can present with mild to moderate cognitive impairment (5% to 20%), depression (20% to 40%), or psychosis (20% to 40%). At least partial reversibility of hypocortisolism-related dementia via exogenous steroid repletion is the rule. Nutritional Disorders VITAMIN B,, DEnaENcv. Vitamin B,, (cyanocobalamin) defi-
ciency can produce many neurologic complications including cognitive dysfunction ranging from a mild confusional state to severe dementia or psychosis (megaloblastic madness). Although presenting symptoms are most commonly caused by anemia, neurologic abnormalities can precede development of macrocytic anemia. Potential neurologic symptoms include peripheral neuropathy, subacute combined degeneration of the spinal cord, nutritional amblyopia (visual loss), distal paresthesias, gait ataxia, bandliie tightness around the trunk or limbs, and Lhermitte's sign (electric shock-like sensation along spine precipitated by rapid neck flexion). Associated leukopenia or thrombocytopenia can signal disease presence via infection andlor bleeding respectively. Like the acute confusional state associated with B,, deficiency, the dementia of B,, deficiency can occur with or without hematologic manifestations. The dementia consists of global
H Non-Alzheirner Dernentias
877
cognitive dysfunction with generalized slowing, impaired concentration, and memory disturbance. Psychiatric disturbances often are prominent and include depression, mania, and psychosis. Diagnostic clues include glossitis, yellow skin discoloration, and cutaneous hyperpigmentation. Spinal cord involvement is manifested by impaired vibratory and joint position sense, sensory ataxia, spastic paraparesis, extensor plantar responses, decreased deep tendon reflexes (especially in the legs), and urinary retention. Laboratory investigations reveal low B,, level (important to check because folate deficiency can cause the same set of hematologic abnormalities), macrocytic anemia, leukopenia with hypersegmented neutrophils, and thrombocytopenia with giant platelets. Schilling's test helps identify the cause of the B,, deficiency (the most common cause of B,, deficiency is pernicious anemia). Serum methylmalonic acid and homocysteine can also be useful measures. Both are elevated in B,, deficiency, but by better indexing tissue vitamin stores they can demonstrate relative deficiency when serum B,, levels are still normal. Some patients, particularly older adults, with normal B,, levels but elevated serum methylmalonic acid can manifest neuropsychiatric abnormalities, including cognitive impairment. Treatment of patients with such covert B,, deficiency often can produce at least partial improvement. WERNICKE'S ENCEPHALOPATHY AND KORSAKOFF'S SYNDROME. Wernicke's encephalopathy (WE) is produced by thiamine (vitamin B,) deficiency, a condition associated most commonly with alcoholism-related nutritional deficiency, but can be a component of many other syndromes involving nutritional compromise (e.g., hyperemesis gravidarum, cancer). Pathologically, WE is characterized by neuronal loss, demyelination, and gliosis in periventricular gray matter regions. Structures most commonly involved include medial thalamus, mammillary bodies, periaqueductal gray matter, and cerebellar vermis, as well as oculomotor, abducens, and vestibular nuclei. Onset of WE typically is abrupt but can be insidious. The classic syndrome comprises the triad of ophthalmoplegia, ataxia, and encephalopathy. However, in one postmortem study, the complete triad had been present in only one third of patients with Wernicke-related lesions found on autopsy. The most common ocular abnormalities are nystagmus, VI nerve palsy, 111 nerve palsy, horizontal gaze palsy, and vertical gaze palsy. Ataxia is typically cerebellar, primarily affecting gait; this can be aggravated by peripheral neuropathy-related sensory ataxia. Cognitive examination reveals global confusion with defective immediate and recent memory. Most patients have peripheral neuropathy (often both WE- and alcohol-related) with absent ankle jerks. Hypothermia and hypotension may occur, presumably secondary to hypothalamic involvement. Pupillary abnormalities, including mild anisocoria, and sluggish light reactivity are occasionally seen. Untreated, WE can progress to stupor and coma. Treatment entails prompt thiamine administration. Parented thiamine is continued for several days to ensure repletion of tissue stores. Ocular abnormalities usually begin to improve within days, ataxia and confusion within weeks. Ophthalmoplegia, vertical nystagmus, and acute confusion are generally reversible, usually within 1 month. However, horizontal nystagmus and ataxia resolve completely in only about 40% of cases. The major long-term complication of WE is alcohol amnestic disorder, commonly known as Korsakoff's syndrome. Korsakoff's syndrome is primarily a memory disorder of anterograde greater than retrograde capacity; other cognitive functions including
878
Behavioral Neurologyand Epilepsy rn Behavioral Neurology
TABLE138-7. General Features of Vascular Dementias History
Physical examination Neuroimaging
Onset of cognitive deficit associated with a stroke Symptomatic improvement after acute event Abrupt onset Stepwise deterioration Focal findings (e.g., hemiparesis, hemianopia) Infarct above tentorium Cognitive impairment corresponding to infarct foci seen on imaging
language are not usually affected. Severe disorientation usually is a consequence of recent memory impairment. Confabulation and impaired insight are common. Inflammatory Disorders. A variety of inflammatory disorders can affect cognitive function. Primary (e.g., primary CNS angiitis) and systemic vasculitides (e.g., Churg-Strauss vasculitis), granulomatous disorders (e.g., neurosarcoidosis), and other autoimmune syndromes (e.g., Hashimoto's encephalitis) can contribute to cognitive dysfunction. These are especially important to identify because the associated dementias can be at least partially reversible with anti-inflammatories (e.g., steroids), immunosuppression (e.g., azathioprine), immunotherapy (e.g., intravenous y-globulin, IV immunoglobulin), and plasmapheresis. See detailed discussion of these syndromes under separate headings in this volume.
Secondary Dementias: Usually Irreversible Vascular Dementias. Strokes, small and large, ischemic and hemorrhagic, cortical and subcortical, together are the second most common cause of dementia, accounting for up to 10% of late-life mental decline. After stroke, 20% to 25% of patients are demented. Diagnostic criteria for vascular dementia are more controversial than those for other dementia subtypes. The term vascular dementia implies presence of a clinical syndrome (dementia) caused by a specific disorder (cerebrovascular disease). Table 138-7 summarizes the features of vascular dementia. Diagnostic criteria for vascular dementia still must be validated by systematic clinicopathologic study. Until such criteria are better refined, vascular dementia is best conceptualized as a secondary dementia (i.e., cognitive dysfunction of brain injury secondary to cerebrovascular disease). Vascular dementia criteria currently in use include the State of California AD Diagnostic and Treatment Centers Criteria (the California criteria), the National Institute of Neurologic Disorders and Stroke, the Association Internationale pour la Recherche et l'Enseignement en Neurosciences (NINDS-AIREN) criteria, the Hachinski Ischemic Score (HIS), and those found in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSMIV).In studies comparing clinical diagnoses and neuropathologic findings, the NINDS-AIREN and the California criteria (as well as DSM-IIIR) had very low sensitivity but high specificity. A retrospective study using HIS was the only analysis in which diagnosis of vascular dementia appeared both sensitive and specific. The diagnosis of vascular dementia is supported by sudden onset of cognitive impairment in two or more domains, stepwise deterioration, asymmetries on neurologic examination, neuroimaging evidence of stroke, and presence of cerebrovascular risk
factors. The incidence of vascular dementia has declined over the last 2 decades, perhaps as a consequence of more effective stroke prevention. It is generally assumed that risk factors for vascular dementia are similar to those for stroke, with arterial hypertension and atherosclerotic disease leading factors. Vascular dementia can take several forms, as outlined in Table 138-8.
Marked differences in clinical presentation of these variants make it inappropriate to regard vascular dementia as a unitary diagnostic entity. Rather, vascular dementia represents a group of dementia types sharing the general common pathogenesis of brain injury secondary to derangement of cerebrovascular functional or structural integrity. A pleomorphic nature thereby arises from variations in type and location of cerebrovascular pathology. Abrupt onset of cognitive impairment supports a diagnosis of vascular dementia but by itself is not diagnostic. Vascular dementia characteristically progresses in a stepwise fashion, with new episodes of minor or major deterioration reflecting additional vascular events. Therefore, the temporal relationship between documented stroke and onset of cognitive impairment is key. The shorter the time difference between the two, the more vascular dementia should be considered as the cause. Multiple small infarctions of subcortical white matter pathways, disconnecting circuitry between cognitively important cortical centers, causes a leukoencephalopathy previously called Binswanger's disease. The resulting clinical situation has been likened to a highway damaged by potholes: destinations remain intact, but travel between these destinations is slowed. In these and other forms of vascular dementia, cognitive changes can be accompanied by abnormalities of motor and sensory functions that are often spared in the early stages of degenerative disorders such as AD. In the majority of patients assessed for dementia, an exclusive diagnosis of vascular dementia can rarely be made. Instead, clinicians are often confronted with patients having some vascular features together with a history that otherwise seems more compatible with a diagnosis of AD. Although epidemiologic studies are limited by diagnostic uncertainties, they suggest that stroke increases the risk of dementia. Recent neuropathologic analyses offer perspective on the difficulty of correctly diagnosing cerebrovascular pathology in dementia. Rather than considering vascular dementia as present or absent, these studies distinguished between presence of any vascular lesions and pure vascular pathology (where vascular pathology was both sufficient to account for cognitive symptoms
TABLE 138-8. Categories of Vascular Dementia Category
Clinical Presentation
Lacunar infarctions
Progressive dementia, focal deficits, apathy, frontal lobe syndrome, possibly absent history of clinically recognized strokes Sudden-onset aphasia, agnosia, anterograde amnesia, frontal lobe syndrome Stepwise appearance of cognitive and motor deficits Progressive dementia with remote or concurrent history of stroke Dementia, apathy, agitation, bilateral corticospinal and bulbar signs
Single strategic infarctions Multiple infarctions Mixed AD-vascular dementia White matter infarctions Binswanger's disease
Chapter 138 H Non-Alzheimer Dementias
and unaccompanied by other pathology). Although at least some vascular pathology existed in more than 40% of dementia cases coming to autopsy, pure vascular pathology accounted for dementia in only approximately 10%. Approximately 10% to 15% of autopsied dementia cases show a combination of Alzheimer and cerebrovascular pathology. One prospective autopsy series of patients with clinically diagnosed dementia found that dementia could not be attributed to the effects of cerebrovascular disease alone in any of the patients studied; 87% were found to have AD, either alone or in combination with cerebrovascular disease. All patients with cerebrovascular disease at autopsy had some concomitant neurodegenerative disease. Such clinical and pathologic admixtures are a common presentation for cerebrovascular disease. Therefore, clinicians should maintain a high index of suspicion for AD or other neurodegenerative processes in patients with dementia, even in the presence of documented cerebrovascular disease. Treatment of vascular dementia consists primarily of identifying and correcting predisposing cerebrovascular risk factors. The overall rate of progression can be slow compared with that of other causes of dementia, even spanning several decades, but some patients suffer from an accelerated evolution. Cerebral Autosomal Dominant Arteriopathy Subacute Infarcts and Leukoencephalopathy (CADASIL). CADASIL is an
increasingly recognized clinicopathologic syndrome. CADASIL causes subcortical lacunar infarction and dementia in more than 80% of cases. CADASIL can appear very similar to hypertensive microvascular disease (Binswanger's disease). Signs and symptoms of CADASIL tend to appear between ages 40 and 60, but changes are apparent on magnetic resonance imaging (MRI) much earlier. Approximately 30% of patients have migraines with aura; mood disorders are common. Neuropathologic findings include smooth muscle hypertrophy in small arteries, demyelination, gliosis in subcortical white matter and basal ganglia, and involvement of the corpus callosum. Given the autosomal dominant hereditary basis of this disease, family history is key. CADASIL is associated with a notch3 family gene on chromosome 19. Neoplastic Disease. Dementia secondary to cancer is mentioned earlier as a potentially reversible secondary dementia; here we discuss a specific irreversible cancer-related dementia. Paraneoplastic limbic encephalitis (PLE) is a rare disorder characterized by variably progressive cognitive and affective changes; less often, focal motor and sensory signs can occur. PLE is both an inflammatory and degenerative disorder of certain CNS gray matter regions occurring as a rare complication of a non-CNS cancer. Symptoms typically precede diagnosis of the underlying cancer. Symptoms usually develop over the course of several weeks. The disorder is characterized by profound impairment of recent memory corresponding to inability to learn new information (i.e. anterograde amnesia). Attention and registration are unaffected, and remote memory is less impaired. Confabulation occurs in some cases. Affective symptoms, especially anxiety and depression, are common early features. Hallucinations are a variable feature. The primarily amnestic syndrome sometimes progresses to a global dementia. Depending on the extent to which gray matter regions outside the limbic system are involved, cerebellar, pyramidal, bulbar, and peripheral nerve disturbances can coexist with cognitive, affective, and behavioral symptoms. Seizures, including complex partial or generalized, sometimes occur. MRI can reveal abnormal signal intensity in the medial temporal lobes. Diffuse slowing or bitemporal slow waves and
879
spikes are sometimes seen on electroencephalogram (EEG). CSF often demonstrates a modest mononuclear pleocytosis and mildly elevated protein. Serologic tests for detecting paraneoplastic antineuronal antibodies have become increasingly available. Excluding other potentially treatable disorders is of primary importance before settling on a diagnosis of PLE. Korsakoffs syndrome, also marked by antero-grade amnesia, should especially be considered since patients with cancer are susceptible to nutritional deficiency (previously stated under Korsakoffs). PLE can be static, progressive, or even remitting. No specific treatment is available except management of the underlying cancer. Radiation. The effects of radiation therapy on the brain can be extremely variable in type and time of onset; late effects, on the order of 10 years after treatment, are known. Clinical expression depends in part on type (e.g., focal beam or whole brain) and amount of radiation. MRI often demonstrates significant leukoencephalopathy. Infectious Dementias. Chronic CNS infectious processes can sometimes cause dementia as a primary manifestation; we briefly describe some major types. VIRAL ENCEPHALITIDES. Viral encephalitis is caused by viral infection of brain parenchyma, producing neuronal and glial degeneration, inflammatory infiltration, edema, and tissue necrosis. Viral encephalitis occurs worldwide, with a higher incidence in tropical regions. Between 1000 and 2000 cases per year in the United States are reported by the Centers for Disease Control. Investigators fail to identify an etiologic agent in up to 75% of presumed viral CNS infection cases. Indeed, the confusing term aseptic meningitis attests to the historic difficulty of definitively isolating an etiologic agent in presumed viral meningitides. Amplification of viral nucleic acids from CSF, as done by the polymerase chain reaction (PCR), for example, has greatly improved diagnosis of several acute, subacute, and chronic viral CNS infections. PCR has become the method of choice for rapid noninvasive diagnosis of herpes simplex virus (HSV) encephalitis; other herpes viruses that can now be diagnosed reliably include cytomegalovirus, varicella-zoster virus, Epstein-Barr virus, and human herpesvirus 6. In AIDS, PCR can help differentiate lesions caused by human immunodeficiency virus (HIV) itself or by opportunistic infections such as progressive multifocal leukoencephalopathy caused by JC virus or cytomegalovirus-related complications. Herpes €rtcepho/itis. HSV causes the most common form of sporadic, potentially fatal encephalitis in children older than 6 months and adults worldwide; herpes encephalitis is addressed in detail in Chapter 65. H/K Up to 70% of patients with HIV develop neurologic complications. Although neurologic disease typically occurs in the context of other AIDS-defining illnesses, neurologic signs can herald AIDS in up to 20% of patients with HIV. The spectrum of neurologic disorders that complicates HIV- 1 infection is extremely diverse. CNS complications can be divided into those caused by HIV infection itself and those caused by HIV-related secondary factors (e.g., opportunistic infections consequent to HIV-induced immunosuppression). HIV-related cognitive disorders are discussed in detail in Chapter 75. hawurns CreuMeM-hkob Disease.
SLOW VIRUS
CJD is one of the slow virus infections, also known as prion diseases after the presumed infectious agent and as transmissible spongiform encephalopathies
Behaworal Neurology and Epilepsy W Behavioral Neurology
880
(TSE), after the histopathologic changes associated with these infections. CJD is the most common human TSE. A new variant of sporadic CJD probably caused by the same agent as bovine spongiform encephalopathy was first described in 1996. Variability in CJD diagnostic criteria sets relying solely on clinical manifestations has led to different incidence rates in different series. CJD occurs primarily as a sporadic illness but also emerges in small family clusters. Sporadic CJD has an annual incidence of about one per million in the general population and occurs randomly worldwide. Inherited CJD has an annual incidence of about 1 per 10 million in the general population. Sporadic CJD is most often diagnosed in patients aged 50 to 70 years; there is generally an equal sex distribution. Although presumably dormant for many years, once clinically expressed, CJD produces a rapidly developing, progressive dementia that can be clinically variable. Initial complaints in approximately one third of patients are constitutional, consisting of fatigue, disordered sleep, or decreased appetite. Another third have nonfocal neuropsychiatric features at onset (eg., confusion or atypical behaviors). The remainder can present with prominent signs of corticospinal and extrapyramidal dysfunction, including gait disturbance and rigidity, as well as focal neurologic features, including ataxia, visual loss, aphasia, hemiparesis, or focal amyotrophy, sometimes leading to an erroneous initial clinical impression of stroke or motor neuron disease. Diagnosis becomes clearer with onset of cognitive decline and startle myoclonus to abrupt sound or touch. Pyramidal, extrapyramidal, and cerebellar signs eventually occur in the majority of patients. Seizures, especially myoclonic, occur in up to 20% of patients. Table 138-9 summarizes the principal clinical features of sporadic CJD. Although seizures are not a common complication of slow virus infection, there can be characteristic electroencephalographic changes. Early in the course of sporadic CJD, the EEG may show nonspecific slowing. Later, periodic, biphasic or triphasic, synchronous sharp wave complexes are superimposed on a slow background rhythm in 60% to 80% of cases on single EEG recordings. These characteristic complexes may disappear as myoclonus subsides in the terminal phase of the disease. Periodic triphasic complexes have shown a sensitivity and specificity of 67% and 86%, respectively, for CJD detection; if repeated recordings are obtained, more than 90% of patients may show periodic complexes within 12 weeks of onset. Until recently, diagnosis of CJD depended on clinical symptoms, characteristic EEG pattern (periodic sharp wave complexes),
W TAW 158-9.
Incidence of Neurologic Features of Sporadic CreuMeldt-Jakob Disease
Sign or Symptom Memory loss Behavioral disturbance Other neuropsychiatric dysfunction Myoclonus Cerebellar ataxia Pyramidal signs Periodic electroencephalographiccomplexes Extrapyramidal signs Visual disturbances Lower motor neuron signs
Frequency (%) 100
57 73 78
71 62 60
56 42 12
Adapted from Brown P et al: Human Spongiform encephalopathy. Ann Neurol35(5): 513-529,1994
and brain biopsy assessment. The introduction of 14-3-3 CSF protein Western blot immunodetection has greatly improved diagnostic accuracy (sensitivity up to 99% and specificity up to 96%). MRI demonstrates a characteristic “cortical ribboning” on diffusion-weighted imaging (DWI). Definitive diagnosis still entails identification of abnormal prion protein or related neuropathology in brain tissue obtained by biopsy or autopsy. However, with typical clinical presentation, rapid course, EEG showing periodic complexes, presence of 14-3-3 protein in CSF, and abnormal DWI MRI, the diagnosis of CJD is reasonably certain. Diagnostic criteria for new variant CJD derived from 35 confirmed deaths have indicated a median duration of illness of 14 months and median age of 29 years. In all cases, psychiatric symptoms such as depression, anxiety, and withdrawal were followed within a median of 6 months by neurologic symptoms such as dysesthesias and paresthesias. In some cases, neurologic symptoms were not accompanied by neurologic signs. Terminal stages of the disease typically have been characterized by progressive loss of function leading to akinetic mutism. Except for a case involving a young woman who is believed to have acquired new variant CJD while living in the UK, there have been no reported cases of new variant CJD in North America. CJD is uniformly fatal, with progression to death within 12 to 18 months of symptom onset. Management is supportive; there is no cure. Chapter 79 reviews prion diseases in further detail.
PRIMARY COGNITIVE DISORDERS Mild Cognitive lmpainnent Some older adults exhibit age-related memory deficits (previously called age-associated memory impairment or isolated memory impairment) but are not considered to have dementia because their general intellect is preserved and there is no significant impairment in activities of daily living. Patients with mild cognitive impairment (MCI) can have memory dysfunction similar to that of patients with mild AD, but the balance of their cognitive functions are similar to those of healthy age-matched controls. Although MCI has been thought to be a possible precursor to AD, dementia may not inexorably occur, even after many years of observation. The hypothesis that MCI, particularly impairment in episodic memory (because this cognitive system is affected earliest and most profoundly by AD), represents an early stage of AD has been a subject of increasing study. Positron emission tomography scans of patients with MCI demonstrate a pattern of hypometabolism more closely resembling that of patients with AD than that of a healthy elderly control group. Retrospective studies of nondemented nondepressed patients have revealed that memory loss alone rarely progresses to dementia at least 2 years after follow-up monitoring. But dementia risk is significantly higher among patients with clear cognitive impairment beyond memory loss. That is, nondemented patients with memory loss and impairment in at least one other cognitive domain, thereby meeting criteria for MCI but not yet meeting criteria for dementia, are more likely than those with age-normal memory impairment alone to develop AD. The annual conversion rate of MCI to frank dementia is estimated to vary from 12%to 15%. This is greater than the overall age-adjusted dementia incidence rate but still leaves many patients without dementia after up to 5 years of follow-up. Hippocampal
Chapter 138
Non-Alzheimer Dementias
881
TABLE 158-10. Clinical Features of Frontal-Variant Frontotemporal Lobar Dementia Core diagnostic features
Supportive diagnostic features
Insidious onset and gradual progression Early decline in social conduct Early impairment in personal conduct Early emotional blunting Early loss of insight Behavior Decline in personal hygiene Mental rigidity Distractibility and impersistence Hyperorality and dietary changes Perseverativeand stereotyped behavior Utilization behavior Speech and language Altered speech output (reduced, aspontaneous, or pressured) Stereotypy Echolalia Perseveration Mutism Physical signs Primitive reflexes With or without incontinence Hypokinesia With or without rigidity With or without tremor Investigations Neuropsychology Impaired executive tasks Absence of amnesia, aphasia, visuospatial dysfunction Electroencephalography Normal Neuroimaging Frontal or frontotemporal structural and functional abnormalities
atrophy has been shown to predict conversion to dementia in patients with MCI. There is also some preliminary evidence that CSF measures of AD-related pathology (e.g., CSF tau and P-amyloid) might predict dementia conversion among patients with MCI. Age is a strong predictor of conversion from MCI to dementia. In summary, there is converging evidence (e.g., psychometric, neuroimaging, neurogenetic) that MCI is characterized by a symptom pattern and prognosis that, though remaining benign in many cases, increasingly appears to exist within the same disease spectrum as other neurodegenerative cognitive disorders such as AD. Because even a minimum MCI-to-dementia conversion rate of 12% would in 5 years result in approximately 60% of patients with MCI converting to dementia, vigilant monitoring of patients with MCI is prudent.
Non-AD Neurodegenerative DementEas Identifymg a specific neurodegenerative dementia can sometimes seem as much art as science. However, with detailed clinical assessment, accurate diagnosis is possible (e.g., one study of interclinician reliability and diagnostic criteria validity for neurodegenerative dementias found near-perfect interrater agreement for diagnosing AD, frontotemporal lobar dementias, and progressive supranuclear palsy). Use of multiple diagnostic criteria for cortical and subcortical dementias increases clinical diagnostic accuracy. We will briefly review diagnostically relevant characteristics of the primary non-AD neurodegenerative dementias. Frontotemporal Lobar Dementias. Certain forms of degenerative disease disproportionately affect circumscribed areas of the frontal or frontotemporal cortex, producing a variety of clinical syndromes diagnostically grouped under the term fiontotemporal lobar dementia (FTLD). Although it is the third most common cause of degenerative cortical dementia after AD and dementia with Lewy bodies (DLB); (some epidemiologic studies place FTLD second), FTLD is much less common than AD, DLB, and vascular
dementia, especially in very old patients with dementia. Nevertheless, FTLDs are important to recognize because although insidious in onset, they usually progress to severe disability and sometimes fatality; their symptoms can mimic those of other disease states (particularly primary affective psychiatric disturbance); and management needs are very different from those of other dementias. Two histopathologic substrates primarily affecting frontal or temporal cortex underlie most FTLDs: microvacuolar change (frontal lobe degeneration type) and astrocytic gliosis with or without Pick bodies. Although the generic term FTLD refers to progressive circumscribed frontotemporal degeneration, distinct clinical syndrome phenomenology is determined primarily by neuropathologic distribution. Based on such differential neuroanatomic involvement, three prototypic neurobehavioral syndromes are recognized frontal-variant FTLD (fvFTLD; predominantly frontal pathology), semantic dementia (SD; predominant anterior temporal pathology), and primary progressive aphasia (PPA); mixed frontal, superior temporal). We briefly review each of these later in this chapter. Useful diagnostic criteria sets for FTLDs, with high interrater reliability (sensitivity and specificity up to 97%), have been formulated (e.g., Lund-Manchester groups). The American Academy of Neurology consensus criteria for FTLDs (an adaptation of the Lund-Manchester criteria) are presented for individual FTLD subtypes in Tables 138-10 through 138-12; common features of all major FTLDs are summarized in Table 138-13. Because of the complexity of the symptom and pathologic spectra of FTLDs, optimal evaluation and management entails cooperation across four disciplines: neurology, psychiatry, neuropsychology, and neuroimaging. fvFTLD is the FRONTAL VARIANTFRONTOTEMWN LOBARDEMENTIA. most common FTLD. Functional neuroanatomic division of the frontal lobe into three separate regions-medial, orbitobasal, and dorsolateral-provides a conceptual basis for organizing fvFTLD symptoms. For example, abulia can be associated with medial frontal-anterior cingulate involvement, social disinhibition and impulse dyscontrol with orbitobasal involvement, and executive
882
Behavioral Neurology and Epilepsy rn Behavioral Neurology
TABLE158-11. Clinical Features of Semantic Dementia Core diagnostic features
Supportive diagnostic features
Insidious onset and gradual progression Language disorder characterized by Content-impoverished but fluent speech Impaired naming and comprehension Semantic paraphasias Perceptual disorder characterized by associative agnosia (impaired recognition of object identity) Preserved perceptual matching and drawing reproduction Preserved single word repetition Preserved ability to read aloud and write orthographically regular words Speech and language Idiosyncratic word usage Surface dyslexia or dysgraphia Speech pressure Absence of phonemic paraphasias Behavior Loss of sympathy and empathy Narrow preoccupations Parsimony Physical signs Akinesia, rigidity, tremor Absence or late primitive reflexes Investigations Neuropsychology Profound semantic loss Preserved phonology, syntax Electroencephalography Normal Neuroimaging Anterior temporal abnormalities
T M L E158-11. Diagnostic Features of Primary Progressive Aphasia Core diagnostic features
Supportive diagnostic features
Insidious onset and gradual progression Nonfluent spontaneous speech with at least one of the following Agrammatism Phonemic paraphasias Anomia Speech and language
Behavior Physical signs Investigations
Neuropsychology Electroencephalography Neuroimaging
Stuttering or oral apraxia Impaired repetition Alexia, agraphia Late mutism Preservation of word meaning Early preservation of social skills Late behavioral changes similar to frontotemporal lobar dementias Late contralateral primitive reflexes Akinesia, rigidity, tremor Nonfluent aphasia Absence of severe amnesia Normal or minor asymmetrical slowing Dominant hemisphere frontotemporal abnormality
TABLE138-15. Features Common to All Frontotemporal Lobar Dementia Syndromes Supportive features Exclusion features
Relative exclusion features
Onset before 65 Family history of similar disorder in first-degree relative Pseudobulbar palsy, muscular weakness or wasting, fasciculations History Abrupt onset lctal events Head trauma related to onset Exam Early severe amnesia Spatial disorientation Logoclonic, festinant speech Loss of train of thought Myoclonus Corticospinal weakness Cerebellar ataxia Choreoathetosis Investigations Neuroimaging Multifocal lesions Predominant postcentral structural/functional deficit Lab CNS involvement by one or more of the following: Metabolic disorder Inflammatory disorder Infectious disorder History Chronic alcoholism Vascular disease Examination Hypertension
Chapter 138 H Non-Alzheimer Dementias
TABLE138-14. Clinical Features of Dementia with Lewy
Bodies Spontaneousextrapyramidal features Marked fluctuations of alertness Recurrent visual hallucinations Syncope and episodes of transient unresponsiveness Unprovoked falls Neuroleptic sensitivity Systematic delusions Nonvisual hallucinations
(e.g., organization, planning) dysfunction with dorsolateral prefrontal cortex involvement. Symptom admixtures commonly occur with disease progression. Personality alteration is prominent but highly variable, ranging from reduced volition and affective blunting to aggression and gross social inappropriateness. Such marked behavioral disturbances can be erroneously attributed to primary psychiatric disease, often prompting initial patient presentation to a psychiatrist. For example, progressive apathy can be mistaken for depression. Alternatively, contextually inappropriate ebullience and impaired judgment can mimic the manic phase of bipolar disorder. Multiple potential behavioral changes can manifest. Activity often becomes stereotyped. Rituals (e.g., eating same food at the same time every day), verbal and ideational perseveration (e.g., repeated use of same catch-phrase), and behavioral perseveration (e.g., watching the same video over and over) are common. Speech output often becomes abridged, sometimes culminating in mutism (often associated with an amotivational or hypokinetic state), although episodic speech excess and pressure can occur in some patients with fvFTLD and prominent disinhibition. Patients often display a food preference change (increased sweets), and behavioral features of Kliiver-Bucy syndrome (e.g., hypersexuality, hyperorality) often occur. The term dysexecutive syndrome has been applied to the constellation of cognitive deficits in fvFTLD. Dysfunction routinely involves cognitive domains including attention, abstraction, planning, organization, problem solving, judgment, and mental flexibility. Primary elements of language, perception, and spatial function are well preserved. Typically not significantly amnesic, patients usually are well oriented. Memory deficits tend to be a secondary epiphenomenon of frontal regulatory disturbances (i.e., inattention with consequent encoding deficiency, defective strategies for learning and retrieval) rather than manifestations of a primary anterograde amnesia. Executive deficits typically are more evident in inert, avolitional patients than in overactive, disinhibited patients. Poor insight regarding these impairments sadly complicates patient management. Pick’s disease is the primary form of fvFTLD. A distinctive but inconsistent neuropathologic correlate of Pick’s disease is the Pick body-a basophilic intraneuronal inclusion-affecting prefrontal cortex and anterior temporal lobes including mediotemporal limbis structures. Atrophy involving frontotemporal cortex and subjacent white matter is severe, ultimately producing “knifeedge” gyri (ulegyria) in these regions, with abrupt transitions between mildly and severely involved sectors (e.g., between the anterior and posterior segments of the superior temporal gyrus). Neuropsychological testing plays an essential role in fvFTLD evaluation. Simple cognitive screening tests, such as the MiniMental State Exam, lack sensitivity for early signs of executive
883
dysfunction and therefore are unreliable for detecting and monitoring fvFTLD. Useful neuropsychological tests are the Wisconsin Card Sorting Test, Stroop Test, and verbal fluency challenge. Test profiles typically reveal frontal system deficits, including attention, verbal fluency, abstraction, and executive function. Quantifiable tests involving decision making and risk taking, which are better able to detect orbitobasal frontal function, have been developed. Anterograde memory performance is variable; patients with fvFTLD tend to do worse on spontaneous recall than on recognition tasks. Non-temporally graded remote memory loss can occur late in the disease course. The most striking neuropsychological finding is how well subjects perform on tests of visuospatial ability, particularly when organization aspects are minimized. Structural neuroimaging usually demonstrates bilateral and symmetrical frontal atrophy. However, this is not universal, especially early in the disease process. Functional imaging may be more sensitive for early diagnosis of fvFTLD. Of functional imaging modalities commonly available, 99Technetium single photon emission computed tomography probably is the most sensitive and can detect frontal hypoperfusion before atrophy is evident. FTLDs w m WWLY LANGUAGE DISTUR~ANCE (FTLD-LD). As with other FTLD diagnostic subdivisions, controversy exists regarding nosologic classification of FTLDs whose primary symptoms involve language disturbance. The syndrome initially was suggested by Pick, and Mesulam’s 1982 report of patients with gradually progressive dysphasia within the context of otherwise preserved intellect and insight sparked contemporary interest in the phenomenon commonly called primary progressive aphasia. Although language disturbances in such FTLD-related dysphasias are heterogeneous, two distinct clinical prototypes can be identified semantic dementia (SD) and primary progressive aphasia (PPA). It is important to recognize patients with FTLD-related dysphasias because such patients can be mistakenly diagnosed with stroke, neoplasm, or even AD because of the focal nature of their deficit (i.e., isolated language impairment). Histopathologyunderlying primary aphasias is varied Pick’s or AD-like aphasias are most common; less common neuropathology includes lipofuscinosis, gliosis, and spongiform changes. In general, language impairment remains an isolated but increasingly severe aphasia in about half of cases; the balance eventually progress to a more global dementia. Temporal Lobe Variant FTLD: Semantic Dementia. SD involves progressive dysnomia and word comprehension impairment in the context of fluent, grammatical speech (it is therefore grossly similar to Wernicke’s aphasia). There is preservation of repetition and ability to read aloud and write orthographicallyregular words (i.e., words whose phonemes follow regular rules of spelling representation). Patients can also display associative agnosia (impaired understanding of visual percepts); therefore, there is loss of meaning for both verbal and nonverbal elements. Patients with semantic dementia typically complain of wordfinding difficulty. Though often painfully aware of their worsening expressive vocabulary,patients often are unaware of their impaired comprehension. Because syntactic and phonologic language structures remain intact, clinical signs are subtle in early stages. Although behavioral symptoms are generally absent or minimal at presentation, fvFTLD-lie features can emerge at later disease stages.
884
Behavioral Neurology and Epilepsy
Behavioral Neurology
Patients with SD demonstrate significant impairment on semantic memory tests. This is most apparent on tasks involving verbal output, such as category fluency tests, picture naming, and verbal definition tasks. Although able to read and write words with regular spelling-to-sound correspondence, patients with SD have difficulty reading and writing orthographically irregular words. This pattern, known as surface dyslexia or dysgraphia, has been attributed to loss of semantic support for pronunciation or spelling of irregular words. Episodic memory is spared, although quantitative assessment reveals impaired recall of more distant life events (a reversal of the usual temporal gradient of AD). Structural neuroimaging reveals anterior temporal neocortical atrophy, with inferior and middle temporal gyri predominantly affected. Asymmetries of temporal involvement reflect relative severity of impairment for verbal versus visual concepts (word meaning versus object recognition). Functional changes on single photon emission computed tomography usually precede detectable structural alterations, demonstrating dominant greater than nondominant temporal hypoperfusion. Primary Progressive Aphasia. PPA is a disorder of expressive language, characterized by effortful speech production, with phonologic and grammatical errors. Comprehension is well preserved. The language disorder occurs in the absence of impairment of other cognitive domains, although behavioral changes of fvFTLD may emerge late in the disease course. Patients present with complaints of speech dysfluency and distortion or word-finding difficulty. The pattern of cognitive deficits in primary progressive aphasia is in many ways the mirror image to that in semantic dementia. Patients perform well on tests of semantic memory except those involving phonologic competence. Although conversational speech is severely disrupted, anomia is mild. Structural neuroimaging usually reveals predominant left Sylvian fissure widening with atrophy of the insula, inferior frontal, and superior temporal lobes. NONSPECIFIC FTLDs. Frontal lobe dementias with nonspecific pathologic changes and atypical clinical symptom sets represent a loose category undergoing evolving nosologic description. For overview purposes, as a means of distinguishing these primary degenerative dementias, we simply call them nonspecific FTLDs. Nonspecific FTLDs often have cognitive and comportmental disturbances similar to Pick‘s disease. Both Pick’s and nonspecific FTLDs tend to have somewhat earlier average ages of onset (50 to 65 years) than AD, with longer survival times. Both disorders tend to occur within families; chromosome 17 abnormalities are being elucidated. A particularly virulent form of nonspecific FTLD occurs in combination with motor neuron disease of the kind seen in amyotrophic lateral sclerosis; memory can remain intact until late in the course of this variant but overall prognosis is poor, with progression to death in as few as 6 to 18 months. Despite the distinct clinical and investigative profiles of FTLDs, differentiation of this large class of non-AD dementias from AD can be diagnostically challenging. One study found that only stereotypy, changes in eating preference, disinhibition, and poor social awareness reliably separate FTLD from AD. Posterior Cortical Atrophy (PCA). PCA is a lobar dementia characterized by initial disturbances of visual perception and integration. Involvement of the occipitoparietal region produces visuospatial, attentional, and linguistic disturbances with relative sparing of personality, insight, and memory until late in the disease. PCA is sometimes called the visual variant of AD. Progression to a global dementia occurs in most cases.
Dementias Associated with Motor Disorders. Several forms of dementia involve the basal ganglia and their neocortical and subcortical projections. Consequently, these are associated with extrapyramidal movement disorders. PARKINSON’S DISEASE (PD). An estimated 30% to 40% of patients with PD develop dementia as part of their illness. It is thought that dementia in PD is underrecognized because of phenomenologically overwhelming problems with motor disturbances. PD-related dementia is characterized by psychomotor slowing, executive dysfunction, memory impairment, and visuospatial disturbances, as well as an increased propensity for depression. PD-related dementia is reportedly more common in patients with asymmetrical onset of parkinsonism affecting the nondominant side and accentuated gait disturbance relative to tremor. Cognitive symptoms may respond partially to dopaminergic pharmacotherapy in the early stages of the illnesses but tend to become refractory as the disease progresses and dementia becomes more severe. Recognition of dementia in PD is important because it is managed differently than dementia in AD. Therefore, a working knowledge of the clinical features of PD is essential. Both history and neurologic examination contribute to making a diagnosis of PD. A history of gait or balance problems, tremors, and extrapyramidal findings defines the movement disorder. Diagnostic criteria specifically for dementia in PD are evolving, as is the terminology. For example, some experts refer to the disorder that results when dementia and extrapyramidal signs and symptoms occur simultaneously as Parkinsonian dementia, or dementia associated with extrapyramidal disease. Psychometric testing may show slightly better recent memory and slightly worse executive functions than typical AD, but the pattern is nonspecific. For further discussion of cognitive changes associated with PD, see Chapter 118. DEMENTIA WITH L w BODIES. DLB probably is the second most common type of degenerative dementia after AD. DLB has clinical features that diagnostically overlap with AD and PD. Lewy bodies are eosinophilic intracytoplasmic inclusions that were originally described in the brainstem (substantia nigra) of patients with PD but occur with slight ultrastructural differences in cerebral (neocortical and paralimbic) neurons in several disorders. Despite its prevalence, clear consensus has not yet been reached regarding terminology, neuropathologic criteria, or clinical symptoms; universally accepted diagnostic criteria remain to be validated. DLB has been defined clinically by the presence of dementia, gait and balance disorder, prominent hallucinations and delusions, sensitivities to traditional antipsychotics, and fluctuations in alertness. Many studies investigating the accuracy of DLB diagnostic criteria against neuropathologic findings found high specificity (e.g., 94%) but low sensitivity (e.g., 34%). Heterogeneity of clinical presentation of DLB can yield low interrater reliability. Hallucinations, delusions, and affective disturbance all occur significantly more often in DLB, but can also occur in AD. Lack of specificity of DLB clinical diagnosis may be attributable to a similar amount of spontaneous extrapyramidal disturbance in DLB and non-DLB dementia. Prominent deficits in attention, visuospatial skills, and relative sparing of memory are neuropsychological features of DLB. However, neuropsychologic tests do not reliably differentiate DLB from AD or VAD. Also, even though patients with DLB tend to demonstrate less temporal lobe atrophy on MEU than do patients with AD, and more hypoperfusion in the occipital lobe on SPECT, neuroimaging has not proven successful in differentiating DLB from AD. Clinical presentation of DLB usually includes cognitive, affective, and motor components. Cognitive dysfunction can range
Chapter 138
from fluctuating impairment to sustained dementia. A superimposed fluctuation in alertness can sometimes mimic a deliriumlike component. Variable permutations of DLB-associated depressive features can include neurovegetative derangement, dysthymia, and psychomotor agitation. Delusions, if present, are typically depression congruent. The characteristic motor disturbance is parkinsonism, often with prominent bradykinesia. The parkinsonism, with or without resting tremor, occurs either spontaneously or in response to treatment with dopamine antagonists. Other features can include hallucinations, which tend to be complex and visual in nature, and frequent falling. In general, patients with DLB have greater visuospatial impairment and executive dysfunction than patients with AD. Rapid eye movement ( E M ) sleep is often disturbed Muscle tone normally decreases in REM sleep, but when patients with DLB attain REM sleep they do not become atonic. The result is that patients with DLB sometimes have a worrisome capacity to act out their dreams (i.e., develop REM sleep disorder). Lewy bodies are widely distributed in the cerebral cortex and substantia nigra in DLB. In contrast, Lewy bodies usually are confined to the substantia nigra in PD. Lewy bodies can occur with or without neuritic plaques or neurofibrillary tangles. Lesions that appear to be most relevant to cognitive decline in DLB are cortical Lewy bodies, Lewy-related neurites, senile plaques, neurofibrillary tangles, neuronal and synaptic loss, spongiform change, and cholinergic deficits. It is possible to operationally classify patients with cognitive decline and cortical Lewy bodies into three main groups: cortical DLB, cortical DLB with plaques, and cortical DLB with plaques and tangles; frequent overlap occurs. Approximately 25% of autopsied cases of AD have substantial numbers of Lewy bodies in both the brainstem and the neocortex. This clinical entity, sometimes called the Lewy body variant of AD, often is associated with increased senile plaque counts but usually lacks sufficient neurofibrillary tangles to meet criteria for a formal diagnosis of AD. However, the histopathology of DLB, PD, and AD can overlap, and a subgroup of patients can simultaneously meet criteria for DLB, PD, and AD. The diagnosis of DLB has several important implications for patient management. As neuroleptic use becomes a complicated process in any dementia with comorbid parkinsonism (because neuroleptic-related dopamine blockade can worsen parkinsonian motor disturbance), this caution becomes imperative in DLB. Patients with DLB often are exquisitely sensitive to neuroleptics, which can precipitously worsen the overall clinical profile. Other important management issues include making caregivers aware that hallucinations are common and that impaired postural stability and falling necessitates added supervision. Cholinesterase inhibitors have shown some efficacy for DLB-related cognitive and behavioral symptoms. PROGRESSIVE SUPRANUCLEAR PALSY (PSP). About 7% of patients with parkinsonian motor abnormalities suffer from progressive supranuclear palsy, a disorder affecting volitional vertical eye movements early in its course. PSP causes a dementia similar to that of PD in 50% to 75% of affected patients. PSP is the most common “dementia with parkinsonism” after DLB. Typical clinical findings in PSP are impaired vertical (downward) eye movements together with axial (truncal) postural disturbances and bulbar dysfunction. Recent studies suggest that PSP is a recessive disorder, in linkage dysequilibrium with the tau gene, rather than a sporadic disease. HUNTINGTON‘S DISEASE (HD). HD is a progressive, eventually fatal neuropsychiatric disease occurring in 5 to 10 per 100,000 in the
Non-Alzheimer Dementias
885
general population. A prototypical genetically based neurodegenerative disorder, HD is inherited as an autosomal dominant trait with complete penetrance. One third of patients with HD have psychiatric changes at onset, and an even greater number suffer cognitive decline. Executive dysfunction and memory impairment are cardinal features of the dementia of HD. Patients with HD display core deficits in frontal corticosubcortical circuits, which yield a multitude of cognitive deficits. Meta-analyses of HD cognitive studies indicate that patients with HD are most deficient on tests of delayed recall, followed by performance deficits on measures of memory acquisition, cognitive flexibility, abstraction, manual dexterity, sustained attention and verbal skills. See Chapter 126 for additional information about HD. Spinocerebellar Degenerations. Dementia can sometimes be a feature of inherited ataxias. The most common autosomal recessive form, Friedreich‘s ataxia, is characterized by early onset of gait ataxia, sensory deficits, and areflexia; cognitive deficits are sometimes present. The large and heterogeneous group of autosomal dominant forms of inherited ataxias, now collectively called spinocerebellar ataxias, can also sometimes include a component of sustained or progressive cognitive impairment. Dementia can also occur in the etiologically heterogeneous Ramsay Hunt syndrome, marked by the clinical dyad of progressive ataxia and myoclonus, and the less common dyssynergia cerebellaris myoclonica. Cortico-Basal Ganglionic Degeneration (CBGD). CBGD is a rare neurodegenerative disease, beginning during the sixth decade or later, marked by asymmetrical rigidity and postural disturbances that may predispose to falls. Focal myoclonus and tremors are occasionally associated features. Apraxias are characteristic of the dementia of CBGD and are usually apparent before cognitive dysfunction in other domains. Approximately 60% of patients experience “alien limb syndrome,” a phenomenon in which the affected limb assumes positions or carries out actions disconnected from the patient’s awareness. CBGD often is associated with asymmetrical cortical atrophy affecting the frontoparietal neocortex, with attendant reductions of cerebral metabolism in that region. Neuropathologic findings include patchy neuronal loss and gliosis in the cerebral cortex and substantia nigra, as well as a characteristic intraneuronal nigral inclusion body. CBGD typically progresses to global dementia; death usually ensues within 5 to 10 years. There is no known treatment. Motor Neuron Disease-Related Dementias. In the course of their disease, certain patients with FTLD develop clinical features compatible with a motor neuron disease (FTLD-MND). Previous reports have suggested that the functional pattern is similar in FTLD and FTLD-MND. However, some neuropathologic studies suggest greater involvement of medial temporal regions in FTLD-MND than in FTLD. Positron emission tomography scans of patients with FTLD and FTLD-MND suggest comparable frontal and lateral temporal hypometabolism in FTLD and FTLD-MND, but greater impairment of medial temporal lobe activity in FTLD-MND. This has prompted investigators to theorize a functional continuum between classic MND, FTLDMND, and FTLD. SUGGESTED READINGS Beghuis JP, Uldall KK, Lalonde B: Validity of two scales in identifying HIV-associated dementia. J Acquir Immune Defic Syndr 21(2): 1 3 6 140, 1999
886
Behavioral Neurology and Epilepsy
W
Behavioral Neurology
Bozeat S, Gregory CA, Lambon MA et al: Which neuropsychiatric and behavioral features distinguish frontal and temporal variants of frontotemporal dementia from Alzheimer’s disease? J Neurol Neurosurg Psychiatry 69:178-186, 2000 Bozoki A, Giordani B, Heidebrink JL et al: Mild cognitive impairments predict dementia in nondemented elderly patients with memory loss. Arch Neurol 58(3):411-416, 2001 Breteler MM, Ott A, Hofman A The new epidemic: frequency of dementia in the Rotterdam study. Haemostasis 28(3-4):117-123, 1998 Brie1 RC, McKeith IG, Barker WA et ak EEG findings in dementia with Lewy bodies and Alzheimer’s disease. J Neurol Neurosurg Psychiatry 66(3):401-403, 1999
Collins S, Boyd A, Fletcher A et al: Creutzfeldt-Jakobdisease: diagnostic utility of 14-3-3 protein immunodetection in cerebrospinal fluid. J Clin Neurosci 7(3):203-208, 2000 Freter S, Bergman H, Gold S et al: Prevalence of potentially reversible dementias and actual reversibility in a memory clinic cohort. CMAJ 159(6):657-662, 1998
Garraux G, Salmon E, Degueldre C et al: Medial temporal metabolic impairment in dementia associated with motor neuron disease. J Neurol Sci 168(2):145-150, 1999 Gomez-Tortosa E, Ingraham AO, Irizarry MC et al: Dementia with Lewy bodies. J Am Geriatr SOC46(11):1449-1458, 1998 Gregory CA, Serra-Mestres J, Hodges J R Early diagnosis of the frontal variant of frontotemporal dementia: how sensitive are standard neuroimaging and neuropsychologicaltests? Neuropsychiatry Neuropsychol Behav Neurol 12(2):128-135, 1999 Gultekin SH, Rosenfeld MR, Voltz R et ak Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings, and tumor association. Brain 123(7):1481-1494, 2000 Hardy J: Genetic dissection of neurodegenerative disease. Clin Neurosci Res l(1-2):134-141, 2001 Hodges J R Frontotemporal dementia (Pick‘s disease): clinical features and assessment. Neurology 56(S4):6-10, 2001 Iddon JL, Pickard JD, Cross JJL et ak Specific patterns of cognitive impairment in patients with idiopathic normal pressure hydrocephalus and Alzheimer’s disease: a pilot study. J Neurol Neurosurg Psychiatry 67~723-732, 1999
Ihl R, Brinkmeyer J: Differential diagnosis of aging, dementia of the Alzheimer type, and depression with EEG-segmentation. Dement Geriatr Cogn Disord 10(2):64-69, 1999 Leys D, Pasquier F, Parnetti L Epidemiology of vascular dementia. Haemostasis 28(3-4):134-150, 1998 Litvan I, Hutton M. Clinical and genetic aspects of progressive supranuclear palsy. J Geriatr Psychiatry Neurol 11(2):107-114, 1998
Looi JC, Sachdev PS: Differentiation of vascular dementia from AD on neuropsychological tests. Neurology 53(4):670-678, 1999 Lopez OL, Litvan I, Catt KE et al: Accuracy of four clinical diagnostic criteria for the diagnosis of neurodegenerative dementias. Neurology 53 (6):1292-1 299, 1999
Lowe J, Dickson D: Pathologic diagnostic criteria for dementia associated with cortical Lewy bodies: a review and proposal for a descriptive approach. J Neural Transm 51:lll-120, 1997 Lund and Manchester Groups: Consensus statement: clinical and neuropathological criteria for fronto-temporal dementia. J Neurol Neurosurg Psychiatry 4416-418, 1994 Meyers BS: Depression and dementia: comorbidities, identification, and treatment. J Geriatr Psychiatry Neurol 11(4):201-205, 1998 Miller BL, Gearhart R Neuroimaging in the diagnosis of fronto-temporal dementia. Dement Geriatr Cogn Disord 10(S1):71-74, 1999 Neary D, Snowden JS, Gustafson L et ak Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology 51:15461554, 1998
Nolan KA, Lino MM, Seligman AW et al: Absence of vascular dementia in an autopsy series from a dementia clinic. J Am Geriatr SOC 46(5):597404, 1998
Nyenhuis DL, Gorelick PB Vascular dementia: a contemporary review of epidemiology,diagnosis, prevention, and treatment. J Am Getriatr SOC 46( 11):1437-1448, 1998
Papka M, Rubio A, Schiffer RB: A review of Lewy body disease, an emerging concept of cortical dementia. J Neuropsychiatry Clin Neurosci 10(3):267-279, 1998 Patterson CJ, Gauthier S, Bergman H et al: The recognition, assessment, and management of dementing disorders: conclusions from the Canadian Consensus Conferenceon Dementia. CMAJ 160(S12):S1-15, 1990
Pinner G, Johnson H, Bouman WP et ak Psychiatric manifestations of normal-pressure hydrocephalus. Int Psychogeriatr 9(4):465-470, 1997 Poser S, Mollenhaeur B, Kraubeta A et ak How to improve the clinical diagnosis of Creutzfeldt-Jakobdisease. Brain 122( 12):2345-2351, 1999 Salloway S, Hong J: CADASIL syndrome: a genetic form of vascular dementia. J Geriatr Psychiatry Neurol 11(2):71-77, 1998 Scheltens P, Hijdra AH: Diagnostic criteria for vascular dementia. Haemostasis 28(3-4):151-157, 1998 Van Kooten F, Koudstaal PJ: Epidemiology of post-stroke dementia. Haemostasis 28(3-4):124-133, 1998 Zakzanis K K The subcortical dementia of Huntington’s disease. J Clin Exp Neuropsychol 20(4):565-578, 1998
139 Confusional States and Metabolic Encephalopathy Michael Ronthal Confusion (delirium) may be defined as a disorder of higher cognitive function characterized by loss of the normal coherent stream of thought or action. The label delirium often is used synonymously with confusional state. It is useful to reserve the former for agitated patients with autonomic instability and hallucinations as part of their confusion. Delirium therefore would be a good description for patients in alcoholic withdrawal and adequately describes the clinical picture in delirium tremens. Although the young are not immune, major risk factors for the development of a confusional state include age and the presence of
an underlying mild preexisting cognitive defect. Patients aged 65 and older account for more than 48% of all inpatient days of hospital care in the United States. Delirium develops in 20% to 30% of hospitalized patients. Each year delirium complicates hospital stays for more than 2.3 million people. Thirty to seventy percent of patients with confusion are not diagnosed by their health care providers, and many physicians remain oblivious to the fact that an acute confusional state is a n emergency and may signify the presence of a life-threatening illness. Reported hospital mortality rates for patients with confusion range from 10% to 65%, 2 to 20 times those of control patients.
886
Behavioral Neurology and Epilepsy
W
Behavioral Neurology
Bozeat S, Gregory CA, Lambon MA et al: Which neuropsychiatric and behavioral features distinguish frontal and temporal variants of frontotemporal dementia from Alzheimer’s disease? J Neurol Neurosurg Psychiatry 69:178-186, 2000 Bozoki A, Giordani B, Heidebrink JL et al: Mild cognitive impairments predict dementia in nondemented elderly patients with memory loss. Arch Neurol 58(3):411-416, 2001 Breteler MM, Ott A, Hofman A The new epidemic: frequency of dementia in the Rotterdam study. Haemostasis 28(3-4):117-123, 1998 Brie1 RC, McKeith IG, Barker WA et ak EEG findings in dementia with Lewy bodies and Alzheimer’s disease. J Neurol Neurosurg Psychiatry 66(3):401-403, 1999
Collins S, Boyd A, Fletcher A et al: Creutzfeldt-Jakobdisease: diagnostic utility of 14-3-3 protein immunodetection in cerebrospinal fluid. J Clin Neurosci 7(3):203-208, 2000 Freter S, Bergman H, Gold S et al: Prevalence of potentially reversible dementias and actual reversibility in a memory clinic cohort. CMAJ 159(6):657-662, 1998
Garraux G, Salmon E, Degueldre C et al: Medial temporal metabolic impairment in dementia associated with motor neuron disease. J Neurol Sci 168(2):145-150, 1999 Gomez-Tortosa E, Ingraham AO, Irizarry MC et al: Dementia with Lewy bodies. J Am Geriatr SOC46(11):1449-1458, 1998 Gregory CA, Serra-Mestres J, Hodges J R Early diagnosis of the frontal variant of frontotemporal dementia: how sensitive are standard neuroimaging and neuropsychologicaltests? Neuropsychiatry Neuropsychol Behav Neurol 12(2):128-135, 1999 Gultekin SH, Rosenfeld MR, Voltz R et ak Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings, and tumor association. Brain 123(7):1481-1494, 2000 Hardy J: Genetic dissection of neurodegenerative disease. Clin Neurosci Res l(1-2):134-141, 2001 Hodges J R Frontotemporal dementia (Pick‘s disease): clinical features and assessment. Neurology 56(S4):6-10, 2001 Iddon JL, Pickard JD, Cross JJL et ak Specific patterns of cognitive impairment in patients with idiopathic normal pressure hydrocephalus and Alzheimer’s disease: a pilot study. J Neurol Neurosurg Psychiatry 67~723-732, 1999
Ihl R, Brinkmeyer J: Differential diagnosis of aging, dementia of the Alzheimer type, and depression with EEG-segmentation. Dement Geriatr Cogn Disord 10(2):64-69, 1999 Leys D, Pasquier F, Parnetti L Epidemiology of vascular dementia. Haemostasis 28(3-4):134-150, 1998 Litvan I, Hutton M. Clinical and genetic aspects of progressive supranuclear palsy. J Geriatr Psychiatry Neurol 11(2):107-114, 1998
Looi JC, Sachdev PS: Differentiation of vascular dementia from AD on neuropsychological tests. Neurology 53(4):670-678, 1999 Lopez OL, Litvan I, Catt KE et al: Accuracy of four clinical diagnostic criteria for the diagnosis of neurodegenerative dementias. Neurology 53 (6):1292-1 299, 1999
Lowe J, Dickson D: Pathologic diagnostic criteria for dementia associated with cortical Lewy bodies: a review and proposal for a descriptive approach. J Neural Transm 51:lll-120, 1997 Lund and Manchester Groups: Consensus statement: clinical and neuropathological criteria for fronto-temporal dementia. J Neurol Neurosurg Psychiatry 4416-418, 1994 Meyers BS: Depression and dementia: comorbidities, identification, and treatment. J Geriatr Psychiatry Neurol 11(4):201-205, 1998 Miller BL, Gearhart R Neuroimaging in the diagnosis of fronto-temporal dementia. Dement Geriatr Cogn Disord 10(S1):71-74, 1999 Neary D, Snowden JS, Gustafson L et ak Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology 51:15461554, 1998
Nolan KA, Lino MM, Seligman AW et al: Absence of vascular dementia in an autopsy series from a dementia clinic. J Am Geriatr SOC 46(5):597404, 1998
Nyenhuis DL, Gorelick PB Vascular dementia: a contemporary review of epidemiology,diagnosis, prevention, and treatment. J Am Getriatr SOC 46( 11):1437-1448, 1998
Papka M, Rubio A, Schiffer RB: A review of Lewy body disease, an emerging concept of cortical dementia. J Neuropsychiatry Clin Neurosci 10(3):267-279, 1998 Patterson CJ, Gauthier S, Bergman H et al: The recognition, assessment, and management of dementing disorders: conclusions from the Canadian Consensus Conferenceon Dementia. CMAJ 160(S12):S1-15, 1990
Pinner G, Johnson H, Bouman WP et ak Psychiatric manifestations of normal-pressure hydrocephalus. Int Psychogeriatr 9(4):465-470, 1997 Poser S, Mollenhaeur B, Kraubeta A et ak How to improve the clinical diagnosis of Creutzfeldt-Jakobdisease. Brain 122( 12):2345-2351, 1999 Salloway S, Hong J: CADASIL syndrome: a genetic form of vascular dementia. J Geriatr Psychiatry Neurol 11(2):71-77, 1998 Scheltens P, Hijdra AH: Diagnostic criteria for vascular dementia. Haemostasis 28(3-4):151-157, 1998 Van Kooten F, Koudstaal PJ: Epidemiology of post-stroke dementia. Haemostasis 28(3-4):124-133, 1998 Zakzanis K K The subcortical dementia of Huntington’s disease. J Clin Exp Neuropsychol 20(4):565-578, 1998
139 Confusional States and Metabolic Encephalopathy Michael Ronthal Confusion (delirium) may be defined as a disorder of higher cognitive function characterized by loss of the normal coherent stream of thought or action. The label delirium often is used synonymously with confusional state. It is useful to reserve the former for agitated patients with autonomic instability and hallucinations as part of their confusion. Delirium therefore would be a good description for patients in alcoholic withdrawal and adequately describes the clinical picture in delirium tremens. Although the young are not immune, major risk factors for the development of a confusional state include age and the presence of
an underlying mild preexisting cognitive defect. Patients aged 65 and older account for more than 48% of all inpatient days of hospital care in the United States. Delirium develops in 20% to 30% of hospitalized patients. Each year delirium complicates hospital stays for more than 2.3 million people. Thirty to seventy percent of patients with confusion are not diagnosed by their health care providers, and many physicians remain oblivious to the fact that an acute confusional state is a n emergency and may signify the presence of a life-threatening illness. Reported hospital mortality rates for patients with confusion range from 10% to 65%, 2 to 20 times those of control patients.
Chapter 139
After 1 month, median rates of institutionalization and mortality are 44% and 16%, respectively. After 6 months the rates are 36% and 26%, respectively. When attempting to elicit the history, it soon becomes apparent that the patient is distractible and inattentive. These two signs are consistently present in all confused patients. Conversely, distractibility and inattention do not always imply confusion but are often encountered in the course of daily living. What leads to the diagnosis of confusion is the inability of the patient to interact with the examiner in an orderly, goal-directed, and coherent fashion, making it impossible to stay on track. When attention is low, distractibility is high. Some patients are agitated and hyperactive. Inattention in these patients is a global dysfunction and does not imply a loss of directed attention to hemibody or hemispace. One cause of global inattention is dysfunction of the subcortical arousal mechanisms in the brainstem; failure in this system may result in drowsiness, progressing to coma. However, this syndrome is not the subject of this chapter; rather, dysfunction in the supratentorial compartment is explored. PSYCHOLOGY OF AlTENTIONAL SYSTEMS Basic attentional mechanisms function at a subconscious level to allow normal cognitive and motor function. The system has survival value and is present in humans and animals during consciousness. The following characteristics can be defined.
Confusional States and Metabolic Encephaiopathy
887
PATHOPHYSIOLOGY OF CONFUSION A confused patient is distracted by trivial stimuli yet fails to react to stimuli of importance. He or she may suddenly shift attention at an inappropriate moment yet may maintain attention after it has become inappropriate. We are not dealing with a simple rise or fall in the arousal level but rather a more profound disruption of the normal hierarchy of rules. Action and thought lose their normal coherence, the patient responds in an inappropriate manner, and the line of thinking becomes jumbled.
PHYSICAL SIGNS As in any syndrome of disordered function, the diagnosis is made on the basis of examination and the eliciting of physical signs; here the signs are to be found in the mental status examination. Not all patients exhibit all the signs described, but at various times one or more of the following signs is found. A good research and clinical instrument to help with the diagnosis is the Confusion Assessment Method (CAM). This has been shown to be sensitive, specific, reliable, and easy to use. Four key features of delirium are defined
Acute onset and fluctuating course Inattention Disorganized thinking Altered level of consciousness
All confused patients are inattentive. Usually a few simple tests of Selectivity We are subject at all times to multiple external and internal environmental stimuli. If effective learning or action is to take place, only a limited number of these can be handled at any particular moment. Thus the predatory animal tracking prey must pay selective attention to the trail at the expense of many other surrounding stimuli. The nursing mother selects stimuli originating from her newborn infant at the expense of other environmental cues.
Coherence Coherence is the ability to maintain selective attention over time.
the attentional system suffice to establish abnormalities. Tests of attention are discussed in Chapter 135. Repeating months or days of the week backward, counting forward in threes, and repeating seven numbers forward or five backward are good screening tests. Loss of Coherence Loss of coherence is established upon attempting to elicit a consecutive history. The dialogue becomes bizarre; the topic shifts abruptly, or the patient may persist with a topic long since thought abandoned. Fragments of the program of action are preserved, but although individual movements are executed correctly, the overall program is lost. This represents one kind of ideational apraxia, as originally described by Hugo Liepmann.
Disorders of Memory
Distractibility Although selectivity and coherence allow effective thought and action, other coincident and simultaneous stimuli must be monitored at the same time. The animal must be capable of screening the environment and have a set of rules to determine the criteria that lead to a shift of focus. Thus, at a cocktail party, one is capable of a one-on-one conversation; the background bustle is filtered out. Yet if one’s name is spoken softly, one’s attention shifts automatically to the sound. The rules for distraction are complex and depend on the immediate state of the animal and on previous learning.
Although patients usually are amnestic for the episode of confusion when they recover, memory is sometimes distorted rather than lost during the confusional state. A paramnesia is an error of memory in which the answers to the questions are incorrect but the elements of the correct answer are present. Geographic paramnesia is the most common. Here the patient, when asked for orientation, may state that he or she is in another city or town yet may correctly identify the building or hospital. When confronted with the previous answer, he or she may claim to be in the “branch office” in the other town.
Propagation of Error Universality The monitoring system must register as many environmental stimuli as possible.
Once the error has been made, the patient persists in the delusion and brings other environmental elements into apparent coherence. For example, the patient may interpret the stand to which the
888
Behavioral Neurology and Epilepsy
Behavioral Neurology
intravenous infusion apparatus is attached as being a lamp in his or her living room. Inattentionto Environmental Stimuli
In true amnestic syndromes, the patient is hyperattentive to environmental cues and relies on them to function. The confused patient, in the example just mentioned, will deny that he or she is in a hospital or doctor’s office, even though the evidence is abundant. Occupational Jargon
The patient may use language reminiscent of his or her workplace. Occasionallythe patient speaks in military or legalistic style. When asked to name, say, a pair of spectacles, he or she may describe them as “an optical instrument for the purpose of increasing visual acuity.” Isolated or Predominant Disturbance of Writing
Spoken language usually is well preserved, although occasional anomia or neologisms may be seen. Conversely, writing often is disrupted, sometimes severely. Writing may degenerate to a scrawl; it often does not stay on the line but moves upward, and there are often perseverations of loops. The deficit cannot be ascribed to an aphasia but rather represents a breakdown in writing secondary to the basic attentional deficit. Unconcern4 t h or Denial of Illness
Confused patients may be fully aware of their illness but show unconcern or denial, a feature shared with patients who have right hemisphere lesions but are not confused. Unconscious Humor or Playful Behavior
Confused patients often are unintentionally funny. The apparent wit is the chance result of an incoherent stream of thought that results in the apposition of incongruous or inappropriate phrases and ideas. One patient who believed that he was at home, when confronted with the undeniable evidence of another patient in the next bed, thought for an instant and stated, “I’m going to charge him rent!” Gait Disorder
This is probably the most frequently missed sign: having established the diagnosis of confusion, we rarely get the patient up to walk. The gait disorder may be nonspecific in type, but occasionally asterixis may involve the lower limb muscles, resulting in sudden loss of tone with a sudden lurch downward. Hyperactivity
The patient may be hyperactive to the point of needing four-point restraints. He or she may be described as “wild” or “psychotic” and may be admitted to a psychiatric ward in “delirium.” Delirium tremens is one such hyperactive form of confusional state or encephalopathy characterized by the appearance of formed hallucinations, sometimes of animals, which may elicit fear.
CAUSES OF CONFUSION Intoxication The most common cause of a diffuse encephalopathy or confusional state is some sort of “brain intoxication.” The toxin may be exogenous (e.g., alcohol, street drugs, or pharmaceutical preparations), or it may be endogenous (e.g., organ failure or some other dysmetabolic state). Drug or alcohol withdrawal may be the precipitant. Failure of almost any of the body systems is a possible cause of confusion and must be assiduously sought. Sepsis-acute, subacute, or chronic-in any anatomic organ is a likely culprit. In these patients, treatment of the underlying systemic illness or withdrawal of the exogenous toxin is the treatment of the disordered cognitive state. It should be appreciated that recovery of brain function may be delayed for some days and sometimes weeks after correction of the causative abnormality. Patients with borderline or very mild dementia are particularly vulnerable to metabolic or toxic encephalopathy. In the presence of severe inattention and confusion it may not be possible to establish a true baseline, and it is only after recovery that the fixed or progressive deficits can be established. Some authors have called this vulnerable brain syndrome with confusion “beclouded dementia.” At the bedside, the clue to an intoxication is the presence of asterixis or, more rarely, multiple myoclonus. Cerebrospinal Fluid Pleocytosis
The presence of cells in the spinal fluid is a potent cause of confusion. The cells may be red cells, white cells, bacteria or some other infecting agent, or even malignant cells. A spinal tap is mandatory in the workup of these patients, even when a metabolic abnormality is suspected. Seizure
Patients may be confused either as part of a partial seizure or in the postictal state. On occasion anticonvulsant drugs themselves may be the culprit, but ordinarily confusion secondary to a seizure disorder responds to anticonvulsants. Because the seizure may not be immediately clinically apparent at the bedside, an electroencephalogram is part of the essential workup of these patients. Pain
Poor pain control in the postsurgical patient has been correlated with a higher incidence of confusion. Environmental Stressors
Sensory deprivation, particularly blindness as in cataract surgery, immobilization and forced restraint, and interference with circadian rhythms as in the intensive care unit are common contributing factors. Head Injury
Confusion may be the presenting syndrome immediately after an injury. It may be transient, as after a minor concussion, or it can be prolonged as part of the recovery phase of more serious injuries. Because there may be no clear history of head injury, a
Chapter 139
careful examination of the skull and scalp are essential in evaluating these patients. Structural Brain Lesions An acute or fairly rapidly progressive structural brain lesion may be the cause. These lesions, whether caused by stroke, focal inflammatory processes, or surgery, usually are found in the right hemisphere. The elementary examination may or may not demonstrate left body signs, and an imaging procedure sometimes is the only way to demonstrate the focal pathology. As noted earlier, all confused patients are inattentive, and it has been suggested with fairly good evidence that the right hemisphere is dominant for the function of attention. The predominance of right hemisphere lesions in this subgroup of patients therefore may reflect a disturbance of the basic underlying attentional matrix. It has been argued that confusion cannot be diagnosed in patients with left hemisphere lesions because they are aphasic. With sophisticated neuropsychological testing it can usually be shown, even in the presence of aphasia, that the patient is attentive and does not lack coherence. Multifocal brain disease, whatever the cause, is a potent cause of confusion. Patients with lesions of the undersurface of either the right or left occipital lobe may present with a hyperactive confusional state, sometimes to the degree that they may need physical restraint. In such cases it is impossible to examine the visual fields, and imaging is the only way to demonstrate the lesion. Focal lesions in the parahippocampal-fusiform-lingualgyri on either side of the brain probably are focal lesions in agitated confusional states. Agitation may also occur after infarction in the right middle cerebral artery territory.
rn Confusional States and Metabolic Encephalopathy
TABU159-1. Common Causes of Confusional States and the Appropriate Tests Cause
Sie
Test
Infection
Urinary tract Lung or bronchi
Urinalysis or culture Sputum analysis, radiograph Spinal tap Spinal tap As appropriate Spinal tap Blood or urine toxic screen
Meninges Brain Other organ Meningeal irritation Toxin
Exogenous Endogenous Renal Respiratory Cardiac Liver Endocrine Porphyria Withdrawal Alcohol Barbiturate
Blood urea nitrogen and creatinine Blood gases Examination, radiograph, ultrasound Liver function tests As appropriate Urine screen
Electrolyte screen Calcium Magnesium PH Glucose Red cell transketolase
Electrolyte disorder
Vitamin deficiency
Blood level Other system dysfunction Seizure Migraine Stroke Miscellaneous
As appropriate Electroencephalogram Occult neoplasm Blood diseases Space-taking lesion Postooerative state
WORKUP Confusional state or diffuse encephalopathy are simply labels used to describe a clinical syndrome. That syndrome, as can be seen from the preceding discussion, has many causes. The true test of the astute clinician is to find and treat the cause. The cause may be as mundane as a urinary tract infection or as obscure as an inborn error of metabolism that becomes apparent at a time of stress. The workup therefore may be long, arduous, and expensive. Many confused older adults are treated with multiple medications, and careful consideration and pruning of the drug list may be the most valuable intervention one can offer. Table 139-1 lists some common causes of confusional states and the appropriate tests. All patients should undergo a blood screen for organ failure, a workup for sepsis, an imaging process, an electroencephalogram, and a spinal tap for the reasons given earlier. A urine and blood toxic screen are added in suspicious circumstances. Some confused patients may need a more extensive workup; searching for the cause is a challenge to diagnostic skill. It might be argued that a complete and extensive workup including brain imaging, spinal fluid examination, and electroencephalogram is not cost-effective for the majority of patients in whom the cause of confusion is a systemic disease, organ failure, or exogenous toxin. It should not take longer than 24 hours to complete the basic workup for these conditions. In patients who are febrile without obvious source, are immunocompromised, have known vascular risk factors, have background cancer, or have obvious focal signs, specific neurologic studies should be done immediately as part of the workup.
889
Imaging study Imaging study Complete blood cell count Imaging study
TREATMENT The prime concern of the treating physician is to establish the cause of the confusional state and treat appropriately. That having been said, primary prevention and symptomatic treatment are also important. Education, support, reorientation, anxiety reduction, and preoperative medical assessment can be modestly successful in preventing confusion in young and old surgical patients, but often not in older medical patients. Identification and prevention of risk factors can be rewarding. In one recent study, cognitive impairment, sleep deprivation, immobility, visual impairment, hearing impairment, and dehydration were evaluated as risk factors, and the intervention was provided by a trained interdisciplinary team consisting of a geriatric nurse specialist, two specially trained elder life specialists, a certified therapeutic recreation specialist, a physical therapy consultant, a geriatrician, and trained volunteers. The incidence of delirium was 9.9% in the intervention group and 15% in the usual care group. The total number of days of delirium was 105 in the intervention group and 161 in the usual care group. Symptomatic treatment is best provided by a sitter who will prevent wandering. Although this may be economically difficult, restraints may make the situation worse and can lead to agitation. A quiet and nonstimulating environment may have a calming effect; ambient noise and bright lights should be toned down.
890
BehavioralNeurologyand Epilepsy
Behavioral Neurology
Agitation necessitates drug therapy; neuroleptic dosages should be monitored carefully if side effects are to be minimized. A suggested starting dosage is 0.25 to 0.5 mg haloperidol repeated up to four times in the first 24 hours. The newer antipsychotics have fewer parkinsonian side effects and may become the treatment of choice: risperidone 0.5 mg/day with a maximum of 4 mg and quetiapine 25 mg with a maximum 300 mg/day are good candidate drugs, but the results of controlled trial are awaited. Although widely used, anxiolytics have not been studied carefully. Lorazepam 0.5 mg/day up to 4 mg/day may be effective and has a shorter half life than diazepam. A benzodiazepine would be the drug of choice for alcohol or drug withdrawal-related confusional states. Antidepressants have been reported to be of some symptomatic benefit. Trazodone, beginning with 25 mglday and increasing to a maximum of 300 mg/day, is about as effective as haloperidol but with fewer side effects. Anecdotal reports support the use of fluvoxamine, fluoxetine, and sertraline. CHRONIC CONFUSION On occasion, especially after an acute right hemisphere stroke, the patient becomes confused and does not recover. The basic defect of attention persists, and the patient lapses into a chronic confusional state. It might be argued that these patients are essentially demented. The essential difference between dementia and chronic confusional state is that the dementia is progressive, and the chronic confusional state is static.
Chedru F, Geschwind N: Writing disturbances in acute confusional states.
Neuropsychologia 10343-353, 1972 Cole MG, Primeau F, McCusker J: Effectiveness of interventionsto prevent delirium in hospitalized patients: a systematic review. Can Med Assoc J 155(9):1263-1268, 1996 Devinsky 0, Bear D, Volpe BT: Confusional states following posterior cerebral artery infarction. Arch Neurol45160-163, 1988 Geschwind N Disorders of attention: a frontier in neuropsychology. Philos Trans R SOCLond B Biol Sci 298:173-185, 1982 Gnanamuthu C Confusional states and seizures: when are they related? Postgrad Med 84:149-158, 1988 Inouye SK Delirium in hospitalized older patients: recognition and risk factors. J Geriatr Psychiatry Neurol 11:118-125, 1998 Inouye SK, Bogardus ST, Charpentier PA et ak A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 340669-676, 1999 Lipowski ZJ: Delirium (acute confusional states). JAMA 258: 1789-1792, 1967 Mesulam MM: Attentional networks, confusional states, and neglect syndromes. pp. 174-256. In Mesulam M M Principles of Behavioral Neurology. 2nd ed. Oxford University Press, New York, 2000 Mesulam MM, Waxman SO, Geschwind N, Sahin TD: Acute confusional states with right middle cerebral artery infarctions. J Neurol Neurosurg Psychiatry 3984-89, 1976 Mulalley W, Ronthal M, Huff K, Geschwind N Chronic confusional state. N J Med 86541-544, 1989 Pousada L, Leipzig RM: Rapid bedside assessment of postoperative confusion in older patients. Geriatrics 4559-64, 66, 1990 Ribby KJ, Cox KR: Development, implementation and evaluation of a confusion protocol. Clin Nurse Specialist 10(5):241-247, 1996 Schmidley JW,Messing RO: Agitated confusional states in patients with right hemisphere infarctions Stroke 15:883-885, 1984
SUGGESTED READINGS Amit R Acute confusional state in childhood. Childs New Syst 4:255-258, 1988
140 Speech and Language Disorders Howard S. Kirshner Speech and language disorders have long attracted interest. Historically, they were the first higher functions to be directly associated with a specific area of the brain. In addition, human communication is the function that sets us apart most clearly from the animals. Speech and language disorders provide a window on the mind-body connection and link neurology to cognitive psychology, linguistics, and philosophy. For neurologists, speech and language disorders also have practical implications. They are among the most common of serious neurologic maladies. About 20% of strokes produce language disturbance, and a greater number affect speech articulation. Language deficits are common in patients with traumatic brain injuries, brain tumors, dementias, neurodegenerative diseases, and infections of the nervous system such as acquired immunodeficiency syndrome. Disorders of communication frustrate patients and families and challenge the abilities of physicians. In recent years, knowledge about language and the brain has expanded greatly. New developments include brain imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI), which provide a simultaneous view of
brain pathology to be correlated with behavioral study, and the functional imaging modalities of positron emission tomography, single photon emission computed tomography, and functional MRI, all of which provide a map of the functional activation of cortical areas during behavioral activities and tasks in both patients with aphasia and normal subjects. Finally, electrical mapping of the language cortex via direct electrical stimulation or transcranial magnetic stimulation, in preparation for epilepsy surgery, has provided an independent window on the organization of language in the brain. Cognitive neuroscientists and linguists have developed sophisticated linguistic models and test paradigms of the cognitive operations involved in language function. All of these advances have contributed to our understanding of language, building on the foundation based on studies of patients with strokes and other focal brain pathologies over the past 150 years. MOTOR SPEECH DISORDERS Motor speech disorders are abnormalities of the motor production of speech, or articulation, in the absence of abnormal language.
890
BehavioralNeurologyand Epilepsy
Behavioral Neurology
Agitation necessitates drug therapy; neuroleptic dosages should be monitored carefully if side effects are to be minimized. A suggested starting dosage is 0.25 to 0.5 mg haloperidol repeated up to four times in the first 24 hours. The newer antipsychotics have fewer parkinsonian side effects and may become the treatment of choice: risperidone 0.5 mg/day with a maximum of 4 mg and quetiapine 25 mg with a maximum 300 mg/day are good candidate drugs, but the results of controlled trial are awaited. Although widely used, anxiolytics have not been studied carefully. Lorazepam 0.5 mg/day up to 4 mg/day may be effective and has a shorter half life than diazepam. A benzodiazepine would be the drug of choice for alcohol or drug withdrawal-related confusional states. Antidepressants have been reported to be of some symptomatic benefit. Trazodone, beginning with 25 mglday and increasing to a maximum of 300 mg/day, is about as effective as haloperidol but with fewer side effects. Anecdotal reports support the use of fluvoxamine, fluoxetine, and sertraline. CHRONIC CONFUSION On occasion, especially after an acute right hemisphere stroke, the patient becomes confused and does not recover. The basic defect of attention persists, and the patient lapses into a chronic confusional state. It might be argued that these patients are essentially demented. The essential difference between dementia and chronic confusional state is that the dementia is progressive, and the chronic confusional state is static.
Chedru F, Geschwind N: Writing disturbances in acute confusional states.
Neuropsychologia 10343-353, 1972 Cole MG, Primeau F, McCusker J: Effectiveness of interventionsto prevent delirium in hospitalized patients: a systematic review. Can Med Assoc J 155(9):1263-1268, 1996 Devinsky 0, Bear D, Volpe BT: Confusional states following posterior cerebral artery infarction. Arch Neurol45160-163, 1988 Geschwind N Disorders of attention: a frontier in neuropsychology. Philos Trans R SOCLond B Biol Sci 298:173-185, 1982 Gnanamuthu C Confusional states and seizures: when are they related? Postgrad Med 84:149-158, 1988 Inouye SK Delirium in hospitalized older patients: recognition and risk factors. J Geriatr Psychiatry Neurol 11:118-125, 1998 Inouye SK, Bogardus ST, Charpentier PA et ak A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 340669-676, 1999 Lipowski ZJ: Delirium (acute confusional states). JAMA 258: 1789-1792, 1967 Mesulam MM: Attentional networks, confusional states, and neglect syndromes. pp. 174-256. In Mesulam M M Principles of Behavioral Neurology. 2nd ed. Oxford University Press, New York, 2000 Mesulam MM, Waxman SO, Geschwind N, Sahin TD: Acute confusional states with right middle cerebral artery infarctions. J Neurol Neurosurg Psychiatry 3984-89, 1976 Mulalley W, Ronthal M, Huff K, Geschwind N Chronic confusional state. N J Med 86541-544, 1989 Pousada L, Leipzig RM: Rapid bedside assessment of postoperative confusion in older patients. Geriatrics 4559-64, 66, 1990 Ribby KJ, Cox KR: Development, implementation and evaluation of a confusion protocol. Clin Nurse Specialist 10(5):241-247, 1996 Schmidley JW,Messing RO: Agitated confusional states in patients with right hemisphere infarctions Stroke 15:883-885, 1984
SUGGESTED READINGS Amit R Acute confusional state in childhood. Childs New Syst 4:255-258, 1988
140 Speech and Language Disorders Howard S. Kirshner Speech and language disorders have long attracted interest. Historically, they were the first higher functions to be directly associated with a specific area of the brain. In addition, human communication is the function that sets us apart most clearly from the animals. Speech and language disorders provide a window on the mind-body connection and link neurology to cognitive psychology, linguistics, and philosophy. For neurologists, speech and language disorders also have practical implications. They are among the most common of serious neurologic maladies. About 20% of strokes produce language disturbance, and a greater number affect speech articulation. Language deficits are common in patients with traumatic brain injuries, brain tumors, dementias, neurodegenerative diseases, and infections of the nervous system such as acquired immunodeficiency syndrome. Disorders of communication frustrate patients and families and challenge the abilities of physicians. In recent years, knowledge about language and the brain has expanded greatly. New developments include brain imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI), which provide a simultaneous view of
brain pathology to be correlated with behavioral study, and the functional imaging modalities of positron emission tomography, single photon emission computed tomography, and functional MRI, all of which provide a map of the functional activation of cortical areas during behavioral activities and tasks in both patients with aphasia and normal subjects. Finally, electrical mapping of the language cortex via direct electrical stimulation or transcranial magnetic stimulation, in preparation for epilepsy surgery, has provided an independent window on the organization of language in the brain. Cognitive neuroscientists and linguists have developed sophisticated linguistic models and test paradigms of the cognitive operations involved in language function. All of these advances have contributed to our understanding of language, building on the foundation based on studies of patients with strokes and other focal brain pathologies over the past 150 years. MOTOR SPEECH DISORDERS Motor speech disorders are abnormalities of the motor production of speech, or articulation, in the absence of abnormal language.
Chapter 140
Patients with motor speech disorders can comprehend both spoken and written language, and their speech output, if comprehensible at all, can be transcribed into normal language. These disorders include dysarthrias, disorders of speech articulation; dysphonias, abnormalities of voice; apraxia of speech; and stuttering.
Dysarthrias Dysarthrias involve the abnormal articulation of sounds or phonemes, especially distortions of consonant sounds, errors in the place of articulation, voicing, or opening of the velum. For example, a “p” sound and a “b” sound differ only in the initial voicing of the “p”; a dysarthric patient might consistently substitute “b” for “p.” Dysarthrias can be caused by mechanical difficulty in the larynx or vocal cords or by neurologic diseases. Neurogenic dysarthrias are classified into six categories: flaccid, spastic (and unilateral upper motor neuron), ataxic, hypokinetic, hyperkinetic, and mixed. Flaccid dysarthria is associated with lower motor neuron disorders affecting the bulbar muscles, neuromuscular junction, cranial nerves, or brainstem anterior horn cells. Examples include polymyositis, myasthenia gravis, and bulbar poliomyelitis. Flaccid dysarthria is characterized by breathy, nasal speech, with consonant errors. Spastic dysarthria is seen in patients with bilateral lesions of the motor cortex or corticobulbar tracts, such as in bilateral strokes. The speech has a harsh, strain-strangle quality, with slow rate, low pitch, and imprecise consonants. A lesser variant of spastic dysarthria, called unilateral upper motor neuron dysarthria, is a similar speech pattern but usually less severe, associated with a unilateral upper motor neuron lesion such as in stroke. This may be the most common type of dysarthria encountered by neurologists. Ataxic dysarthria, or scanning speech, associated with cerebellar disorders, involves irregular or slow rhythm of speech, with pauses and abrupt explosions of sound and abnormal or excessively equal stress on every syllable. Hypokinetic dysarthria, seen in Parkinson’s disease, is associated with decreased and monotonous loudness and pitch, increased rate with occasional pauses, and some consonant errors. Hyperkinetic dysarthria, seen in such diseases as Huntington’s disease and dystonia musculorum deformans, is characterized by excessive variation in rate, loudness, and timing, with distorted vowels. In dystonia, hyperkinetic dysarthria can also include harsh, strainstrangle speech with imprecise consonants. The final category, mixed dysarthria, involves combinations of the other types. Common causes include multiple sclerosis, which often combines spastic and ataxic characteristics, and amyotrophic lateral sclerosis, which links spastic and flaccid elements. With practice, a clinician can use speech patterns to confirm suspected neuroanatomic diagnoses.
Speech and Language Disorders
rather than distorted, as in dysarthria. The misarticulations increase with polysyllabic words that require multiple consonant shifts. Difficulty with initial consonants makes the speech hesitant and groping. Errors are inconsistent from one attempt to the next, in contrast to the more regular distortion of phonemes seen in dysarthria; for example, a patient attempting to repeat the word “artillery” five times might produce five different utterances. Apraxia of speech is rare in isolated form, but it often contributes to the aphasic deficit of Broca’s aphasia. Speech apraxia as part of an aphasia is defined by the inconsistent articulatory errors in the presence of preserved comprehension and by the patient’s ability to write better than speak. Lesions producing apraxia of speech often appear to involve the insula of the left hemisphere. Stuttering
Stuttering is an often hereditary disorder characterized by initial pauses and dysfluency of speech production, without other articulatory or language disorders. Stuttering usually is a childhood, developmental disorder, but a close imitation can occur in acquired brain lesions, including strokes or brain injury in either hemisphere. APHASIAS Language disorders, or aphasias, are defined as abnormalities of symbolic communication, or language, acquired as a result of brain disease. This definition distinguishes aphasias from motor speech disorders, from congenital or developmental language disorders (often called dysphasias), and from psychiatric thought disorders. Psychotic patients express bizarre, illogical language content in well-articulated, syntactically correct sentences; the abnormality lies in thought, not in its expression in language. Aphasia is diagnosed by a six-part bedside language evaluation (Table 140-l),used in conjunction with a neurologic history and examination. The first test item, spontaneous speech, can be ascertained during the clinical interview. Automatic sequences, such as the days of the week, are helpful in provoking speech output. The most important variable is fluency, the free-flowing quality of the utterances. The presence of articulatory errors or dysarthria should be noted, along with circumlocutions, wordfinding pauses, and paraphasic errors. These errors can be of the literal or phonemic type, involving substitution of an incorrect sound (“ben” for “pen”) or of the verbal or semantic type, involving substitution of an incorrect word (“spoon” for “fork”). Jargon speech is so replete with paraphasic errors that the meaning is unclear. Naming is evaluated with objects, body parts, colors,
m TAW 110-1. Bedside Language Examination
Dysphonias Dysphonias, or disorders of voicing, are part of dysarthria. Hoarseness can result from laryngitis or a paralyzed vocal cord. Neurogenic dysphonias include the breathy voice of myasthenia gravis and the whispered voice of Parkinson’s disease.
Apraxia of Speech Apraxia of speech is an inability to program sequences of phonemes, especially consonants. Consonants are substituted
891
Speech expression Spontaneous speech Automatic sequences Naming Auditory comprehension Repetition Reading Aloud Comprehension Wriiing Spontaneous Dictation Coovinn
892
Behavioral Neurology and Epilepsy
Behavioral Neurology
and parts of objects. Auditory comprehension is tested by asking the patient to follow spoken commands of one, two, and three steps. Care must be taken to exclude hearing loss, motor paralysis, or apraxia as the cause of a failure to follow commands; if doubt exists, comprehension can be tested by yeslno questions or by commands that require only a pointing response. Repetition is tested with polysyllabic words and phrases such as “Methodist Episcopal,” which are sensitive to dysarthria, and with sentences, especially grammatically complex, unfamiliar phrases such as “no ifs, ands, or buts,” which are sensitive to aphasia. If apraxia of speech is suspected, the patient is asked to repeat polysyllabic words such as “artillery” or “catastrophe” five times. Reading is tested by asking the patient to follow printed commands or to read paragraphs for meaning. Writing, the final element, is tested by spontaneous generation of sentences, writing to dictation, or copying. Muteness, or absence of speech, can be difficult to interpret. A mute patient may be aphasic but may suffer instead from severe dysarthria, a frontal lobe syndrome such as abulia or akinetic mutism, a basal ganglia disorder such as parkinsonism, a psychiatric disorder such as catatonia, or a mechanical disorder of the larynx. It is helpful to have some language production to analyze before diagnosing aphasia. In general, a mute aphasic cannot write or comprehend language normally. The physician uses the bedside language examination, together with the neurologic examination, to localize diseases in the nervous system. The history provides clues as to the cause of the disorder. For example, the sudden onset of fluent aphasia indicates an embolic stroke to the inferior division of the left middle cerebral artery, whereas a slowly developing anomia may indicate an early dementia or a left hemisphere brain tumor. More detailed examination of language function can be obtained by consultation with a speech and language pathologist or neuropsychologist. Standard language testing batteries such as the Boston Diagnostic Aphasia Examination or the Western Aphasia Battery are helpful in quantitating a language deficit, supporting a syndrome classification, and following progress during rehabilitation. Finally, neurodiagnostic and brain imaging studies confirm the medical diagnosis. CT scanning and MRI detect brain lesions such as strokes or brain tumors. Positron emission tomography and single photon emission computed tomography show the metabolic activity or blood flow of brain regions; activation of these regions can be studied during language tasks.
Handedness and Cerebral Dominance Approximately 99% of right-handed patients and most lefthanded patients have relative left hemisphere dominance for language. Both autopsy studies and measurements based on CT
and MRI scans have shown anatomic brain asymmetries, especially a larger superior temporal plane in the left cerebral hemisphere. Left hemisphere language dominance appears to be genetically programmed because temporal lobe asymmetries are found even in newborns and in illiterate people. Further knowledge of language dominance is emerging from testing of patients with epilepsy in preparation for surgical resection; the areas important for language are determined by the Wada test, in which sodium pentobarbital is injected into the internal carotid artery, or by intraoperative stimulation mapping of the language cortex. Such mapping has produced somewhat more variable localizations for the classic language centers than traditional, autopsy-based or even CT scan-based localization from stroke patients. Occasionally, aphasia develops in right-handed patients with right hemisphere lesions (“crossed aphasia”). Aphasia in lefthanders may be seen with lesions of either hemisphere but most commonly the left. Recent studies have shown less difference in initial language profiles or ultimate recovery between right- and left-handers than previously thought. Atypical syndromes occasionally are seen in left-handers, such as preserved comprehension in a patient with a large left hemisphere lesion, suggesting right hemisphere comprehension ability.
Classification and Diagnosis Aphasias have been classified into eight traditional syndromes: Broca’s, Wernicke’s, global, conduction, anomic, and three transcortical aphasias. In addition, two single-modality deficits, aphemia and pure word deafness, and syndromes of alexia and agraphia deserve attention. Finally, a newer category, subcortical aphasia, has emerged, based on subcortical lesion localization on brain imaging studies. Broca’s Aphasia. Broca’s aphasia is characterized by nonfluent speech, varying from mutism to hesitant, struggling efforts to speak (Table 140-2). The patient utters the principal, contentcarrying words, mainly nouns and verbs, of a sentence, omitting pronouns, prepositions, and articles, a phenomenon called telegraphic speech or agrammatism. Patients hesitate on names but often can indicate some knowledge of the word (tip-of-the-tongue phenomenon). Repetition is effortful and slow. Auditory comprehension is adequate for simple conversations and commands but breaks down on complex grammatical constructions, which are also difficult for the patient in expressive speech. Reading often is more affected than auditory comprehension. Writing is impaired, even with the nonparalyzed left hand. Patients with Broca’s aphasia are aware of their deficits, often becoming frustrated and depressed. The lesions of Broca’s aphasia involve the left frontal lobe, classically the posterior portion of the inferior frontal gyrus, anterior to the motor face area. Small lesions of Broca’s area permit
TMLE 140-2. Language Features of the Eight Classic Aphasias Syndrome
Broca’s Wernicke’s Global Conduction Anornic TCMA TCSA MTCA
Speech
Naming
Comprehension
Repetition
Nonfluent Anornic Mild Hesitant Fluent Paraphasic Poor Paraphasic Anornic Nonfluent Poor Poor Fluent f Impaired Normal Poor Fluent Anornic Normal Normal Nonfluent & Impaired Normal Normal Fluent Paraphasic Poor Normal Normal Nonfluent Poor Poor Abbreviations: MTCA, mixed transcortical aphasia; TCMA, transcortical motor aphasia; TCSA, transcortical sensory aphasia.
Reading
Writing
Mild Impaired Poor k Impaired Normal Impaired Poor Poor
Poor Poor spelling Poor f Impaired Normal & Impaired Poor spelling Poor
*
Chapter 140
nearly complete recovery, whereas larger left frontoparietal lesions produce an early global aphasia that evolves gradually into Broca’s aphasia. Associated damage in the subcortical and periventricular white matter (especially the periventricular white matter and subcallosal fasciculus) may be necessary to produce lasting loss of expressive speech. Aphemia is a transitory syndrome of muteness or nonfluent speech, with preserved writing and comprehension. Some authorities equate aphemia with isolated apraxia of speech. Lesions involve the face area of the motor strip, sometimes with extension into the inferior frontal gyrus and underlying white matter. Wernicke’s Aphasia. In contrast to patients with Broca’s aphasia, patients with Wernicke’s aphasia speak fluently, but with empty phrases, circumlocutions, and paraphasic errors of both literal and verbal type (Table 140-2). Naming may provoke bizarre, paraphasic substitutions. Auditory comprehension is severely impaired. Reading is affected much like auditory comprehension, but some patients show sparing of one or the other modality. Writing is well formed but contains spelling and word choice errors; in mild cases, writing may be a sensitive clue to the diagnosis of Wernicke’s aphasia. Patients with Wernicke’s aphasia usually are not depressed, but they may be unaware of their deficits and may become angry when not understood. Motor and sensory findings usually are absent, although some have right hemianopia. The lesion typically involves the classic Wernicke’s area in the left posterior superior temporal gyrus. Destruction of most of Wernicke’s area appears necessary for lasting loss of comprehension, but there is often associated damage in the supramarginal and angular gyri. Pure word deafness is a rare syndrome of inability to understand or repeat spoken language, in the absence of expressive language difficulty or deafness for nonverbal sounds. Classically, pure word deafness results from bilateral temporal lesions that disconnect Wernicke’s area from both auditory cortical areas. The syndrome also occurs with unilateral left temporal lesions. Global Aphasia. Global aphasia may be thought of as the sum of Broca’s and Wernicke’s aphasia, a loss of all six major language functions (Table 140-2). Spontaneous speech is nonfluent or mute, and the patient cannot name, repeat, understand, read, or write. Most patients have extensive left hemisphere damage and profound neurologic deficits of right hemiplegia, right hemisensory loss, and right hemianopia. When less severe deficits involve all language functions, the syndrome is called mixed aphasia. Conduction Aphasia. Conduction aphasia is a less common language syndrome in which repetition is affected out of proportion to other language modalities (Table 140-2). Speech is fluent but may be interrupted by pauses to correct literal paraphasic errors. Auditory comprehension is intact. Conduction aphasia was traditionally explained as a disconnection between Wernicke’s and Broca’s areas. Others have explained the repetition difficulty as a deficit of auditory verbal immediate memory. Lesions involve either the left temporal lobe, without destruction of Wernicke’s area, or the inferior parietal lobule. Anomic Aphasia. Anomic aphasia is a selective deficit of naming. Speech is fluent, except for word-finding pauses and circumlocutions, and the other language modalities are intact. This syndrome is less localizing than other types of aphasia. Anomic aphasia is seen with focal lesions of the left temporal or inferior parietal region and is often the last stage in recovery of language in almost any type of aphasia. Anomia is also common in encephalopathies, aging, and dementia.
H
Speech and Language Disorders
893
Transcortical Aphasias. The transcortical aphasias have in common the preservation of repetition. The word transcortical refers to disruption of areas of the association cortex (Lichtheim called these the “area of concepts”) that project onto the perisylvian language cortex, rather than of the language cortex itself. Transcortical motor aphasia (TCMA) resembles Broca’s aphasia in that there is marked dysfluency or difficulty initiating speech, but the patient with TCMA repeats normally. The lesions of TCMA spare Broca’s area but involve the adjacent left frontal cortex, medial frontal cortex, or subcortical white matter. Strokes causing transcortical motor aphasia generally are within the territory of the anterior cerebral artery, so the syndrome is relatively specific. Transcortical sensory aphasia resembles Wernicke’s aphasia except for the sparing of repetition. The lesions involve the posterior left temporo-occipital region or the temporal lobe itself; Boatman et al. found that stimulation of adjacent cortical areas in the left superior temporal region could produce either Wernicke’s or transcortical sensory aphasia. This syndrome also occurs in Alzheimer’s disease. Mixed transcortical aphasia, also called the syndrome of the isolation of the speech area, resembles global aphasia except that repetition is not only spared but may be excessive or palilalic. Some patients mimic and learn new song lyrics or complete poems if given the first lines. Reported cases have had large, watershed infarctions sparing the perisylvian language area or advanced dementing illnesses. Subcortical Aphasias. Unlike the other aphasia syndromes, subcortical aphasias are diagnosed by the location of the brain lesion rather than by language features. In recent years, aphasia syndromes increasingly have been associated with subcortical lesion sites. First, lesions of the left thalamus produce fluent aphasia, usually with better comprehension and repetition as compared with Wernicke’s aphasia. Patients may fluctuate between periods of drowsiness, with severe aphasia, and periods of alertness, with improved language function. Second, lesions of the left putamen, anterior limb of internal capsule, and caudate nucleus produce syndromes of dysarthria and nonfluent speech, with less abnormality of phrase length and repetition as compared with Broca’s aphasia. This atypical Broca-like aphasia is sometimes called the anterior subcortical aphasia syndrome. Lesions extending into the deep temporal white matter or temporal isthmus may impair comprehension, producing subcortical equivalents of Wernicke’s and global aphasia. Alexias and Agraphias. Because reading and writing are elementary language functions, acquired disorders of reading and writing should be considered aphasias, as opposed to congenital or developmental reading disorders, usually called dyslexias. The interesting disorders of acquired alexia and agraphia will be missed unless the neurologist takes care to test reading and writing. Alexia with agraphia is an acquired illiteracy, with intact spoken language modalities except for anomia and mild fluent, paraphasic speech (Table 140-3). The syndrome is associated with focal lesions of the left angular gyrus. Associated deficits include Gerstmann’s syndrome of agraphia, inability to calculate, right-left confusion, and finger agnosia, an inability to name or point to specific fingers on the patient’s or examiner’s hand. Pure alexia without agraphia (Table 140-3) is an isolated inability to read. The lesions involve the left posterior cerebral artery territory, including the left medial occipital and medial temporal lobes and the splenium of the corpus callosum. Some patients have difficulty naming colors. Most have at least a partial right hemianopia. Another common association is with decreased ability to encode new information (short-term memory loss),
894
BehavioralNeurology and Epilepsy
Behavioral Neurology
TABE 140-5. Language Features of the Classic Alexias Feature
Alexia with Agraphia
Fluent, often paraphasic
Speech Naming Repetition Comprehension Reading
+ Impaired
Writing Associated signs Localization
Severely impaired Right hemianopsia Left angular gyrus
Normal Intact or mildly impaired Severely impaired
Pure Alexia Without Agraphia
Normal Color anomia Normal Intact Impaired. f sparing of letters Normal Right hernianopsia Left occipital lobe, splenium
explained by damage to the hippocampus and adjacent medial temporal structures. Pure alexia has been explained as a disconnection between the intact right occipital visual cortex and the left hemisphere centers for decoding of visual language symbols. Alexia is also seen as part of the language deficit of aphasia (aphasic alexia). The alexia of Broca’s aphasia is called the third alexia. Neurolinguists have described four separate patterns of alexia: deep, phonologic, surface, and letter-by-letter alexia. Letter-by-letter alexia is identical to the syndrome of pure alexia without agraphia. Both deep and phonologic alexia involve the visual recognition of whole, familiar words, without the ability to decode graphemes into phonemes; surface dyslexia involves the opposite ability to convert graphemes laboriously into phonemes, without any recognition of words or phrases at a glance. The agraphias, like the alexias, can be divided into the rare pure agraphias and agraphia associated with aphasia. Agraphias have also been classified into deep, phonologic, and surface varieties. Language in Dementias. Aphasia usually is the result of focal, destructive lesions of the brain, but language disturbances also occur in acute encephalopathies and dementias. In probable Alzheimer’s disease, language deteriorates along a generally predictable gradient: naming of people and objects is deficient early in the course, along with simplification of discourse and language content; reading, writing, and auditory comprehension deteriorate during the middle stages; and in the terminal phase, articulation and expressive speech begin to fail. In linguistic terms, semantics fail first, then syntax, and finally phonology. A less common pattern of language deterioration with aging is called primary progressive aphasia. These disorders, though variable, often begin with loss of fluency in patients who may not develop a generalized dementia for several years. This syndrome is seen in patients with Pick’s disease, corticobasal degeneration, and a family of diseases called frontotemporal dementia. Only very rarely does a progressive, nonfluent aphasia turn out to be associated with Alzheimer’s disease.
communication deficit of right hemisphere lesions, although not strictly meeting the definition of aphasia, is socially disabling to patients, hindering readjustment to family and work environments. Recovery and Therapy
Patients with aphasia from acute brain injury or stroke improve spontaneously for several months. The aphasia type often changes during recovery; global aphasia evolves into Broca’s aphasia, and Wernicke’s aphasia may recover toward the profile of conduction or anomic aphasia. As mentioned earlier, anomic aphasia often is the last stage of recovery from any aphasia. Early recovery of language function may involve resolution of edema or reactivation of partially damaged tissue in the language cortex, but later recovery probably requires the reorganizationof new cortical areas for language function in either adjacent left hemisphere or analogous right hemisphere regions. The work of Heiss and colleagues in Germany indicates that right hemisphere activation on positron emission tomography scans always predicts incomplete recovery, and only left hemisphere activation permits full restitution of language capability. In general, such recovery is much more complete in children than in adults. Speech therapy, carried out by trained speech and language pathologists, aims to facilitate language recovery by a variety of methods. In traditional therapy, repeated practice is carried out to improve performance in the major communication modalities of speech, auditory comprehension, reading, and writing. The therapist focuses on specific language operations that are deficient, working first in an artificial language task and then applying these functions to communication in the real world. Repeated drills and stimulus-response paradigms are performed. A number of new speech therapy techniques have been developed. Melodic intonation therapy entrains musical intonation into speech, theoretically involving the right hemisphere in speech production. Visual action therapy uses simple gestures to convey meaning. Computer techniques originally developed for primate communication have enabled even severely aphasic patients to combine pictures of nouns and verbs, creating simple sentences that can be printed or transmitted to a voice synthesizer. Other augmentive speech devices permit simple, stereotyped language expression. Finally, pharmacologic agents are beginning to be used in language rehabilitation. Bromocriptine, a dopamine agonist used in Parkinson’s disease, increases speech production in some patients with transcortical motor aphasia. Amphetamines have also been used to facilitate language improvement; a research trial is in progress. Although the medical profession often considers speech therapy an unproved treatment, large, randomized trials have clearly established that speech therapy is effective in promoting better communication in aphasic patients, and several meta-analyses have also confirmed the efficacy of speech therapy.
Language and the Right Hemisphere
The right hemisphere, although dominant for language in only a small minority of people, plays an important role in communication. The elements of communication most affected by right hemisphere disease are prosody, or cadence and intonation of speech, and pragmatics, or practical, extralinguistic messages that normal speakers convey. Patients with right hemisphere disease sound flat in their intonation, and they may fail to comprehend emotional nuances, irony, sarcasm, and humor in the speech of others. They understand what is said but not how it is said. The
SUGGESTED READINGS Albert ML, Bachman DL, Morgan A, Helm-Estabrooh N Pharmacotherapy for aphasia. Neurology 382377-879, 1988 Alexander MP, Benson DF The aphasias and related disturbances. pp. 1-58. In Joynt RJ (ed): Clinical Neurology. Vol. 1. JB Lippincott, Philadelphia, 1993 Alexander MP, Naeser MA, Palumbo CL: Broca’s area aphasia: aphasia after lesions including the frontal operculum. Neurology 40:353-362, 1990
Chapter 141
Alexander MP, Naeser MA, Palumbo CL Correlation of subcortical CT lesion sites and aphasia profiles. Brain 110:961-991, 1987 Appell J, Kertesz A, Fisman M: A study of language functioning in Alzheimer’s patients. Brain Lang 22:23-30, 1982 Bakar M, Kirshner HS, Wertz R T Crossed aphasia: functional brain imaging with PET or SPECT. Arch Neurol 53:102&1032, 1996 Basso A, Farabola M, Pia Grassi M et al: Aphasia in left handers: comparison of aphasia profiles and language recovery in non-righthanded and matched right-handed patients. Brain Lang 38:233-252, 1990
Benson DF, Ardila A Aphasia: a clinical perspective. Oxford University Press, New York, 1996 Boatman D, Gordon B, Hart J et ak Transcorticalsensory aphasia: revisited and revised. Brain 123:1634-1642, 2000 Dronkers N F A new brain region for coordinating speech articulation. Nature 384:159-161, 1996 Duffy J R Motor speech disorders: substrates, differential diagnosis, and management. Mosby, St. Louis, 1995 Heiss WD, Kessler J, Thiel A et al: Differential capacity of left and right hemispheric areas for compensation of poststroke aphasia. Ann Neurol 45:430438, 1999
Higher-Order Visual Impairments
895
Kirshner HS: Behavioral Neurology: Practical Science of Mind and Brain, 2nd ed. Butterworth Heineman, Boston, 2002. Kirshner HS: Handbook of Neurological Speech and Language Disorders. Marcel-Dekker, New York, 1995 Kirshner HS, Alexander M, Lorch MP, Wertz RT Disorders of speech and language. Continuum 5:l-237, 1999 Kirshner HS, Casey PF, Henson J, Heinrich JJ: Behavioral features and lesion localization in Wernicke’s aphasia. Aphasiology 3:169-176, 1989 Ludlow CL, Rosenberg J, Salazar A et ak Site of penetrating brain lesions causing chronic acquired stuttering. Ann Neurol 22( 1):60-66, 1987
Ojemann G A Conical organization of language. J Neurosci 11:2281-2287, 1991
Posner MI, Petersen SE, Fox PT, Raichle M E Localization of cognitive operations in the human brain. Science 2401627-1631, 1988 Weintraub S, Rubin NP, Mesulam M: Primary progressive aphasia: longitudinal course, neuropsychological profiles, and language features. Arch Neurol47:1329-1335, 1990 Wertz RT, Weiss DG, Aten LJ et ak Comparison of clinic, home and deferred language treatment for aphasia: a VA cooperative study. Arch Neurol 143:653-658, 1986
141 Higher-Order Visual Impairments Michael P. Alexander Higher-order visual impairments are those that cannot be accounted for by deficits in visual acuity, visual fields, o r gaze mechanisms. Most higher-order visual impairments are caused by lesions in visual association cortex (Brodmann’s areas 18 and 19) or by the outflow from those regions to multimodal association cortex in the temporal lobe (particularly area 37) and hippocampus or in parietal lobes (particularly areas 7, 39, and 40). The clinical approach to these impairments is facilitated by the fact that the higher-order deficits are readily divided along three separate dimensions. The first dimension is lesion laterality. Damage to the left hemisphere causes deficits in processing visual stimuli for language content or associations. Deficits in processing visual material for some spatial relations, for some perceptual properties, and for some aspects of emotional content usually are caused by right hemisphere lesions. The second dimension is dorsal-ventral. Damage to the ventral (inferior) visual association cortex and pathways impairs discrimination and identification of stimuli: the “what” system. Damage to the dorsal (superior) visual association cortex and pathways impairs attentional, spatial, and kinesthetic analyses: the “where” system (Table 141-1).The third dimension is the scale of visual attention. Attention can be paid to large components of a visual array, such as overall configuration, sometimes called global attention or a “floodlight.” Attention can also be paid to small items within a visual array, such as specific letters or faces, sometimes called local attention or a “spotlight.” In normal subjects under normal conditions, visual attention may be a composite of the two or switch between them, either unconsciously o r consciously, as when searching for a face in a crowd. Damage to the left visual association cortex, particularly dorsal, reduces sensitivity to high spatial frequency (local o r detailed) properties of stimuli. Damage to the right reduces sensitivity to
low spatial frequency (global or configurational) aspects of stimuli. These differences in scale of attention underlie some of the characteristic findings of lateralized lesions: the markedly different error patterns in drawing and other spatial manipulations of visual stimuli and the very asymmetrical clinical manifestations of hemifield spatial neglect after right or left brain lesions. This chapter reviews the common higher-order deficits, attempting to place them in relation to the three dimensions just outlined. For each disorder, clinical assessment methods, treatment strategies (if any), and natural history are discussed.
TABLE141-1. Classification of Higher-Order Visual Impairments According to Whether the Lesion Is in the Superior or Inferior Visual Association Cortex Inferior (Temporo-Occipital Cortex) Visual System Disorders
Pure alexia Object agnosia Prosopagnosia
Left occipitotemporal Bilateral inferior occipitotemporal Large left inferomedial occipitotemporal Bilateral inferior occipitotemporal Large right inferomedial occipitotemporal
Superior (Parieto-Occipital Cortex) Visual System Disorders
Neglect Visually guided movements Balint‘s syndrome Primary dressing disorder (“dressing apraxia”) Ideational apraxia Visuoconstructive disorders
Contralateral parieto-occipital (left neglect more severe) Contralateral parieto-occipital Bilateral parieto-occipital Right superior parieto-occipital Left parietal Either left or riaht oarietal
Chapter 141
Alexander MP, Naeser MA, Palumbo CL Correlation of subcortical CT lesion sites and aphasia profiles. Brain 110:961-991, 1987 Appell J, Kertesz A, Fisman M: A study of language functioning in Alzheimer’s patients. Brain Lang 22:23-30, 1982 Bakar M, Kirshner HS, Wertz R T Crossed aphasia: functional brain imaging with PET or SPECT. Arch Neurol 53:102&1032, 1996 Basso A, Farabola M, Pia Grassi M et al: Aphasia in left handers: comparison of aphasia profiles and language recovery in non-righthanded and matched right-handed patients. Brain Lang 38:233-252, 1990
Benson DF, Ardila A Aphasia: a clinical perspective. Oxford University Press, New York, 1996 Boatman D, Gordon B, Hart J et ak Transcorticalsensory aphasia: revisited and revised. Brain 123:1634-1642, 2000 Dronkers N F A new brain region for coordinating speech articulation. Nature 384:159-161, 1996 Duffy J R Motor speech disorders: substrates, differential diagnosis, and management. Mosby, St. Louis, 1995 Heiss WD, Kessler J, Thiel A et al: Differential capacity of left and right hemispheric areas for compensation of poststroke aphasia. Ann Neurol 45:430438, 1999
Higher-Order Visual Impairments
895
Kirshner HS: Behavioral Neurology: Practical Science of Mind and Brain, 2nd ed. Butterworth Heineman, Boston, 2002. Kirshner HS: Handbook of Neurological Speech and Language Disorders. Marcel-Dekker, New York, 1995 Kirshner HS, Alexander M, Lorch MP, Wertz RT Disorders of speech and language. Continuum 5:l-237, 1999 Kirshner HS, Casey PF, Henson J, Heinrich JJ: Behavioral features and lesion localization in Wernicke’s aphasia. Aphasiology 3:169-176, 1989 Ludlow CL, Rosenberg J, Salazar A et ak Site of penetrating brain lesions causing chronic acquired stuttering. Ann Neurol 22( 1):60-66, 1987
Ojemann G A Conical organization of language. J Neurosci 11:2281-2287, 1991
Posner MI, Petersen SE, Fox PT, Raichle M E Localization of cognitive operations in the human brain. Science 2401627-1631, 1988 Weintraub S, Rubin NP, Mesulam M: Primary progressive aphasia: longitudinal course, neuropsychological profiles, and language features. Arch Neurol47:1329-1335, 1990 Wertz RT, Weiss DG, Aten LJ et ak Comparison of clinic, home and deferred language treatment for aphasia: a VA cooperative study. Arch Neurol 143:653-658, 1986
141 Higher-Order Visual Impairments Michael P. Alexander Higher-order visual impairments are those that cannot be accounted for by deficits in visual acuity, visual fields, o r gaze mechanisms. Most higher-order visual impairments are caused by lesions in visual association cortex (Brodmann’s areas 18 and 19) or by the outflow from those regions to multimodal association cortex in the temporal lobe (particularly area 37) and hippocampus or in parietal lobes (particularly areas 7, 39, and 40). The clinical approach to these impairments is facilitated by the fact that the higher-order deficits are readily divided along three separate dimensions. The first dimension is lesion laterality. Damage to the left hemisphere causes deficits in processing visual stimuli for language content or associations. Deficits in processing visual material for some spatial relations, for some perceptual properties, and for some aspects of emotional content usually are caused by right hemisphere lesions. The second dimension is dorsal-ventral. Damage to the ventral (inferior) visual association cortex and pathways impairs discrimination and identification of stimuli: the “what” system. Damage to the dorsal (superior) visual association cortex and pathways impairs attentional, spatial, and kinesthetic analyses: the “where” system (Table 141-1).The third dimension is the scale of visual attention. Attention can be paid to large components of a visual array, such as overall configuration, sometimes called global attention or a “floodlight.” Attention can also be paid to small items within a visual array, such as specific letters or faces, sometimes called local attention or a “spotlight.” In normal subjects under normal conditions, visual attention may be a composite of the two or switch between them, either unconsciously o r consciously, as when searching for a face in a crowd. Damage to the left visual association cortex, particularly dorsal, reduces sensitivity to high spatial frequency (local o r detailed) properties of stimuli. Damage to the right reduces sensitivity to
low spatial frequency (global or configurational) aspects of stimuli. These differences in scale of attention underlie some of the characteristic findings of lateralized lesions: the markedly different error patterns in drawing and other spatial manipulations of visual stimuli and the very asymmetrical clinical manifestations of hemifield spatial neglect after right or left brain lesions. This chapter reviews the common higher-order deficits, attempting to place them in relation to the three dimensions just outlined. For each disorder, clinical assessment methods, treatment strategies (if any), and natural history are discussed.
TABLE141-1. Classification of Higher-Order Visual Impairments According to Whether the Lesion Is in the Superior or Inferior Visual Association Cortex Inferior (Temporo-Occipital Cortex) Visual System Disorders
Pure alexia Object agnosia Prosopagnosia
Left occipitotemporal Bilateral inferior occipitotemporal Large left inferomedial occipitotemporal Bilateral inferior occipitotemporal Large right inferomedial occipitotemporal
Superior (Parieto-Occipital Cortex) Visual System Disorders
Neglect Visually guided movements Balint‘s syndrome Primary dressing disorder (“dressing apraxia”) Ideational apraxia Visuoconstructive disorders
Contralateral parieto-occipital (left neglect more severe) Contralateral parieto-occipital Bilateral parieto-occipital Right superior parieto-occipital Left parietal Either left or riaht oarietal
896
Behavioral Neurology and Epilepsy W
Behavioral Neurology
SYNDROMES OF IMPAIRED IDENTIFICATION OF COMPLEX VISUAL STIMULI: THE ” W H A T SYSTEMS Disorders of identification are produced by lesions in the ventral visual association cortex and its pathways. Pure Alexia
Pure alexia is the acquired inability to read despite preservation of adequate vision (acuity, fields, and attention) and preservation of other language capacities (thus, “pure” alexia or alexia without agraphia). Pure alexia is caused by lesions in the language-dominant (usually left) hemisphere’s occipitotemporal lobes (Table 141-2). It is not specific to any cause and may be seen after infarcts, hemorrhages, tumors, abscesses, and even focal degenerative disorders. Most cases in clinical practice are caused by left posterior cerebral artery territory infarctions. It has long been proposed that pure alexia is a disconnection of visual input from the language competent left temporal lobe. The disconnection is variably characterized as anatomic or psychophysiologic. The anatomic disconnection is straightforward. The most common lesion anatomy of pure alexia is a large medial occipitotemporal lesion producing right hemianopia and damaging the ventral, posterior callosal projections. This prevents processed visual information from passing from the right inferior association cortex to the left, at least via the most efficient pathways, thus impairing extraction of language information. White matter lesions subjacent to that area can also cause alexia by disrupting the input of left and right, visual association cortex into a critical cortical region for visual-language processing, with or without producing a right visual field deficit. Lesions in the left inferior occipitotemporal junction (areas 37 and 19) can also produce alexia, identifjmg that area as the critical site for visual-language associations. It is probably more accurate to characterize the disconnection as a disruption of language-specific visual information processing and cast it in different terms. There are a series of partially nested neural systems in the ventral left occipital and temporal lobes that progressively extract and code visual features distinct for letters and words. Damage to these systems or to the pathways linking them or carrying visual information to them impair reading without otherwise affecting language. There is abundant evidence from positron emission tomography and functional magnetic resonance imaging activation studies in normal subjects to support the existence and location of these systems. They operate at high spatial frequency. They require very rapid processing. In some patients pure alexia may be caused by an inability to process
W
TABLE141-2. Pure Alexia
Examination Oral reading Single letters Words Connected text Words Forced-choice comprehension Commonly associated signs Right visual field defect Color anornia Verbal mernorv deficits
the letter specific operations quickly enough to assemble words from letter stimuli. Few cases of “pure” alexia are totally pure. Right hemianopia is common, caused by damage to the geniculocalcarine pathways or calcarine cortex. Anomic aphasia is also common, although usually mild, reflecting damage to inferior temporal gyrus. A particularly severe color-naming deficit may be observed. The general naming deficit may be much more severe with visual presentation of objects than with either tactile presentation or spontaneous speech, so-called optic aphasia or visual anomia. Large lesions may produce object agnosia. Lesions that involve the hippocampus, parahippocampal gyrus, or the deep medial temporal white matter cause significant memory problems. The alexia is independent of any of these associated deficits. Patients are aware of their hemianopia and reading impairment but may be less aware of the associated deficits. Alexia testing is straightforward: Present stimuli in an uncrowded field to eliminate attentional, perceptual, and scanning problems. Begin with single letters and move to single words and then short, connected text. Ask the patient to read targets aloud. If unsuccessful, present an array of four to six written stimuli (letters or words) and ask the patient to point to them as you name them. Any patient complaining of alexia must be evaluated for other language deficits, especially writing, and for visual recognition or at least naming to visual presentation of other stimuli (e.g., colors, common objects). The same approach can be followed (naming colors or objects to visual presentation and then pointing to a specified color or object in an array of four to six; if impaired at the latter, naming objects that are palpated or described). Patients with severe pure alexia cannot read or recognize single letters, although they may still recognize iconic written stimuli, such as advertising signs, traffic signs, menu items, or their own names. When forced to choose between written words, they can show considerable capacity to recognize words. Certain classes of words are more readily recognized, even in the complete absence of ability to read the word aloud or indicate any recognition of its meaning. Emotionally charged words, proper names, and the names of highly imageable, concrete objects seem particularly likely to survive. Patients often are unaware that they have this recognition capacity. Improvement follows a typical course. Letter recognition improves, and as it does, patients begin to read letter by letter, assembling words by slowly reading off the letters. This becomes faster, and they seem to recognize entire short words. With more improvement, the letter-by-letter strategy will not be evident to an observer except on very long and unfamiliar words. At this point, the patient is no longer truly alexic, but reading is such an effort that it is rarely pursued. Furthermore, any impairment in verbal memory from medial temporal damage will make it almost impossible for the patient to recall what he or she so effortfully reads. Treatments are unproven. Superficial similarities in patients with pure alexia probably hide differences in the level of processing impairment. Most treatments have been attempted on only single patients and are of unknown general efficacy. If the patient cannot read single letters, there may be no reasonable treatment. Letter-by-letter reading improves with simple practice. Patients probably should use visually uncrowded text with well-marked margins. The content of the reading material should be familiar to the patient so that he or she does not have to struggle additionally for meaning beyond the individual words. Rapid, forced-choice word selection tasks may help the patient improve word recogni-
Chapter 141 W
tion without resorting to the laborious letter-by-letter strategy. Recall that therapy should be tempered if the patient also has verbal memory deficits. Object Agnosia
Object agnosia is characterized by an inability to recognize common objects despite adequate acuity and despite preserved capacity to recognize the objects through palpation or description. There are two prototypical forms of visual agnosia. In apperceptive agnosia, patients are unable to recognize objects, but they complain of impaired vision, not impaired recognition. Their corrected acuity is reduced, and visual fields are very hard to establish but usually are fullto perimetry techniques. They are able to recognize colors and movement. The usual cause of apperceptive agnosia is anoxia or carbon monoxide poisoning, and the lesion anatomy therefore has been laminar necrosis of the striate cortex. The agnosia is not specifically a deficit in recognition of well-perceived stimuli. It is a form of elemental perceptual impairment that precludes recognition. Patients with associative visual agnosia more accurately meet the defining criteria for agnosia. The patients complain of impaired recognition, not impaired vision. The usual cause is infarction, but traumatic contusions, tumors, and focal degenerative disorders have been described. The usual lesion anatomy is bilateral lesions in inferior temporo-occipital association cortex, but large left temporo-occipital lesions may also produce associative agnosia (Table 141-3). Depending on the lesion configuration, associated signs are somewhat variable. Patients with bilateral lesions usually have superior altitudinal visual field deficits. Disturbed color vision (achromatopsia) and impaired facial recognition (prosopagnosia) are common. If lesions extend into the medial temporal structures, including hippocampus, there may be significant memory impairments. Alexia and anomic aphasia may be present, depending on the extent of the left-sided lesion. Patients with large unilateral left lesions present a clinical problem of distinguishing agnosia from several boundary syndromes (Fig. 141-1). Very large left occipitotemporal lesions produce alexia and anomic aphasia and, as described earlier, may produce optic aphasia, in which patients recognize objects, are able to describe their use, usually recognize their names and can name them from a description, but are unable to name them from vision alone. In contrast, patients with object agnosia are unable to identify an object presented visually and thus be unable to describe its use or match it to its name. It is uncertain whether there is an unambiguous boundary between these syndromes. Many allegedly agnosic patients have been able to select a named object from an array, suggesting that the problem is not only visual recognition but also name retrieval or else that the visual recognition problem is only partial and facilitated by selection from limited possibilities (top-down facilitation.) Another boundary condition for associative agnosia is semantic amnesia or multimodal agnosia. Associative visual agnosia should be marked by preserved recognition and knowledge of objects in any format except visual. Thus, patients could define a described object, describe a named object, provide information about the object’s use, construction, and common location, and name an object placed in their hands. However, many patients with large left-sided lesions, usually large posterior cerebral artery infarctions, are unable to recognize an object through any sensory route (multimodal agnosia) or to provide any associated commonly
Higher-Order Visual Impairments
897
TMLE 141-5. Associative Visual Agnosia Examination Objects Naming Identification by description Categorization Matching to name Commonly associated signs Bilateral lesion Superior attitudinal visual field defect Prosopagnosia Achromatopsia Amnesia Left lesion Right visual field defect Alexia Anomic aphasia Semantic memory deficits Verbal memory deficits
known information about the object (semantic amnesia). Although rare, this loss of semantic knowledge has been described after herpes encephalitis or posterior cerebral artery territory infarctions. Loss of semantic memory is a hallmark of Alzheimer’s disease and the subtype of frontotemporal dementia now called semantic dementia, which may be synonymous with one form of Pick’s disease. It is believed that the posterior association cortices house the mechanisms critical to semantic knowledge. Agnosia testing is designed to define the level of recognition impairment and its modality specificity (Table 141-3). The patient is shown simple objects or pictures of objects (visually more challenging) and asked whether he or she can name them. If so, the patient may be simply anomic and therefore is asked to describe the object’s function. If not, the patient is anomic but should be asked to name it from description and palpation. This resolves whether the patient has a general anomia, visual anomia, or both. If he or she cannot provide any associated information about an object but can name it with tactile input, the patient should be asked to point to the named object in an array. If he or she can, the patient presumably has simply a very severe lexical-semantic deficit. If he or she cannot, the patient should be asked to sort objects or pictures into natural categories. If the patient cannot, he or she has definite agnosia, but categorization through other modalities should be probed (“Is a hammer a carpentry tool?” “ISa camel a type of fish?”).If impaired, he or she has multimodal agnosia and general semantic knowledge loss. Cases of visual agnosia and all of its boundary conditions have produced abundant information about how the brain organizes knowledge, in part by the sensory modality through which it is experienced and in part by the abstract (and verbal) categories. There are critical cortical regions for modality-specific and modality-independent associational networks. The exact neural structure of semantic systems is controversial. There is convincing evidence that different semantic domains (e.g., proper names, faces, letters) have regionally specific organizations. It is less clear whether the modality of access to semantic knowledge (e.g., sounds, vision, description) actually contains modality-specific knowledge or only delivers distinctive information to a single associative semantic system. Patients with isolated visual object agnosia have been used to argue for the former. Multimodal loss of semantic knowledge in dementias or after structural temporal lesions has been used to argue for the latter. Treatments of visual agnosia, multimodal agnosia, and semantic memory loss have not been reported. Many patients improve.
Behavioral Neurology and Epilepsy rn Behavioral Neurology
898
Patient shown an object or a picture of an object
Unable to name but describes and/or gestures its correct use
Unable to name or to describe or gesture its correct use
I
ANOMIA
AGNOSIA
No improvement if allowed to hold object or to hear object
Correctly names palpated objects or described objects
I
I
Multimodal agnosia
Visual agnosia
Unable to answer questions of common knowledge about object
Severe semantic knowledge impairment ("semantic amnesia")
No improvement if allowed to hold object or to hear object
Correctly names palpated objects or described objects
141-1mnowchart showingthe method by which agnosia may be distinguished from boundary syndromes that may resemble it.
1 Multimodal anomic agnosia
Visually specific anomia ("optic aphasia")
Unable to recognize correct name or match object to its name
Severe lexical impairment ("two-way naming" disorder)
Patients with bilateral inferior occipitotemporal lesions may be left with recognition deficits in areas that are particularly demanding perceptually: distinguishing faces and recognizing photographs, line drawings, or video clips. Patients with large left-sided unilateral lesions continue to have more clear-cut visual-language deficits (alexia and optic aphasia) and general language deficits (anomic aphasia) and less perceptual recognition impairment.
Prosopagnosia is defined by an inability to recognize familiar faces despite preservation of adequate acuity. Prosopagnosia usually is caused by bilateral lesions in inferior temporo-occipital cortex, most commonly infarcts. It has also been described in patients with focal progressive atrophy of the right temporal lobe, probably a variant of frontotemporal dementia. Patients with infarcts have
superior altitudinal visual field deficits (Table 141-4).Achromatopsia is also commonly seen. Depending on lesion extent in medial temporal regions, there may be considerable memory impairment. Some patients have only large right temporooccipital lesions. They usually have left hemianopia and impaired topographic memory. With either lesion configuration, impairments in other perceptually demanding visual discriminations have been reported, most notably a farmer unable to distinguish between the cows in his dairy herd. Note that prosopagnosia can be considered a modality-specificloss of knowledge. Normal rapid facial recognition appears to be a global perceptual task. In normal subjects the right hemisphere is faster and more reliable at recognizing familiar faces than the left. Permanent prosopagnosia is less common after unilateral right lesions than after bilateral injuries. This suggests that the right ventral occipitotemporal association cortex may be the critical processing node but that in
Chapter 141
most patients the left posterior association cortex can extract enough perceptual information for recognition, even if slowly. Testing for prosopagnosia takes some planning. Because it is a visual modality-specific deficit, the examiner must be careful to provide only visual information. Magazine pictures or family pictures are useful. If real people (i.e., family members) are used for testing, they must be cautioned not to speak or to wear distinctive clothing. This is not a test of perception that happens to use faces. It is a test of recognition of familiar, known faces. Patients with bilateral lesions may be anomic, but descriptions of the target’s occupation, relationship, and so on suffice to eliminate prosopagnosia. Semantic memory deficits can be differentiated from prosopagnosia by performance on strictly verbal tasks. A patient with prosopagnosia will have abundant knowledge of named people. No treatment has ever been proposed. Patients with large bilateral lesions usually improve through a stage of profound object agnosia. Perhaps because it is perceptually more demanding, facial recognition usually recovers less well than object agnosia, but the relative recoveries depend on lesion site, size, and laterality. Some patients have recovered from prosopagnosia but remained unable to recognize emotional expressions. ACHROMATOPSIA
Achromatopsiais the loss of color vision in a preserved visual field. It is usually caused by the same infarction in the inferior occipital lobes. It is often accompanied by prosopagnosia or alexia. It has been described as a migraine aura. It can be demonstrated in just the field contralateral to a ventral occipital lesion or in the entire spared field of patients with bilateral lesions. Patients with unilateral achromatopsia often are not aware of the problem. When bilateral, patients complain that their vision is bleached out or washed out or that illumination always seems poor. Damage to the occipitotemporalgyri (lingual and fusiform) causes contralateral achromatopsia. There is usually a superior visual field deficit with achromatopsia in the preserved inferior field. With rightsided lesions, prosopagnosia usually is present at least transiently. With left-sided lesions, alexia usually is present. With the demonstration in nonhuman primates that visual cortex is not simply a stepwise visual pattern analyzer, that different regions in the visual cortex have specific capacities to analyze particular aspects of a visual stimulus, an explanation became available for acquired color blindness. The color-specific region of visual cortex (V4) in experimental animals is the analogue of the lingual gyrus region in humans. Functional activation in positron emission tomography studies has also
TMLE 141-4. Prosopagnosia Examination Famous and familiar faces Naming Identificationby description Categorization Matchingto name Commonly associated signs Bilateral lesion Superior attitudinal visual field defects Achromatopsia Amnesia Right lesion Left visual field defed Topographic amnesia
Higher-Order Visual Impairments
899
identified the occipitotemporal regions as specifically tuned to color extraction. No treatment has been proposed. SYNDROMES OF IMPAIRED VISUAL AllENTlON
The disorders that result from impaired visual attention are produced by lesions in the dorsal visual association cortex and its outflow to parietal and frontal lobes and by lesions in parietal heteromodal association cortex. Directed attention is a very complex operation that uses a network including structures far from visual cortex. Neglect
Failure to attend to stimuli in extrapersonal space constitutes neglect. Neglect can be seen in either right or left hemispace after lesions in the contralateral hemisphere. Left hemispatial neglect is much more severe than right hemispatial neglect after comparable lesions, one of many pieces of evidence that the right hemisphere is dominant for attentional functions. Neglect may be seen after any structural lesions of any cause. Within the hemisphere, neglect can been seen with dorsolateral frontal, dorsolateral striatal, anterior cingulate, posterior thalamic, or parietal lesions. The manifestationsand mechanisms of neglect differ for these different lesion sites. Large lesions, damaging more than one of those regions, produce the most severe neglect. In clinical practice large infarctions in middle cerebral artery territory produce the most dramatic neglect. Large posterior cerebral artery territory infarctions involving posterior thalamus and occipital cortex also produce very dramatic neglect. The associated signs may be varied, depending on lesion size and site. However, neglect is independent of visual field deficits. Any combination of field deficits and neglect can be seen, depending on lesion site. Testing for neglect is readily accomplished at the bedside with paper and pencil. Although not the cause of or necessary for neglect, primary sensory deficits, including sensory extinction, should be defined. Among the many proposed tests of neglect, line bisection and line (or object) cancellation are most easily performed and sensitive. For line bisection the patient can be given a sheet of paper, presented in the midline, with numerous horizontal lines of various lengths distributed to the right and the left of the paper’s midline. Neglect is measured as systematic deviation from the midline. For cancellation tasks, the patient is given a sheet of paper with randomly arrayed lines or objects and told to mark each line or designated target object. Failure to cancel lines in parts of space defines neglect. Neglect may be apparent in other tests. When reading aloud, the patient may fail to read one end of each line of text. When the patient is quickly shown compound words (e.g., doghouse), one side of the word may be omitted. If the patient is asked to copy complex figures, the copy may start far to one side with failure to copy or disproportionate miscopying of one side. For all tests of neglect, patients with right-sided lesions show much more left neglect than patients with comparable left-sided lesions show right neglect. Patients with parietal lesions seem to show neglect because they fail to pay attention to contralateral hemispace. Thus, when a competing stimulus is present in right space, attention turns to the right. Patients with dorsolateral frontal and dorsolateral striatal lesions appear to show neglect because they fail to move attention to the contralateral hemispace. As long as stimuli are available to draw attention, the patient may move into the impaired hemispace. Only if the task requires the patient to generate his or her
900
Behavioral Neurology and Epilepsy
Behavioral Neurology
own strategy to move attention (e.g., on copying tasks) will evidence of neglect emerge. For parietal or frontal lesions, left hemispatial neglect is always much more noteworthy than right neglect after comparable lesions. Functional imaging studies have demonstrated that the distribution of attention to low-frequency features of a stimulus depends on right parietal lobe. This may account for the patient’s inability to cast a “spotlight” that includes all portions of a stimulus. Many aspects of the visual processing of neglected left field stimuli are normal in patients with neglect, even neglect combined with hemianopia. Patients with neglect are sensitive to center of mass, optic illusions, motion, and word meaning in the neglected fields as long as testing for awareness does not depend on conscious reporting of the left side of a stimulus. Overt demonstration of neglect is influenced by the target’s background and the visual context of testing. These preserved capacities are presumed to occur preattentively and represent automatic operations of the visual system. Treatment of left hemispatial neglect has been attempted in a variety of ways. The primary motivation for these treatments has been the frequent observation that left hemineglect is a significant factor in a bad functional outcome after rehabilitation for stroke. Treatments have been both direct and compensatory. In direct treatments, microcomputer presentation has been used to direct attention to the impaired side before presentation of stimuli. Patients can also be given practice in directing gaze in the horizontal plane to specific points in the impaired hemifield. Compensatory treatments are all techniques of providing a perceptual anchor in the neglected hemispace, such as a brightly colored marker down the left margin of books or on the bathroom mirror, with the patients instructed to always look to the marker. Both techniques seem to improve patients’ function in test circumstances and perhaps in self-care activities. The vestibular system can be stimulated to direct gaze, and presumably attention, into the neglected field with caloric or optokinetic input. Passive stimulation (vibration) and active movement of the left side, when possible, also appear to increase attention to the left side of space. Each of these techniques ameliorates neglect, but the effects are short-lived, and no practical applications have been devised. Right hemispatial neglect recovers quickly. Left hemispatial neglect, in addition to being more severe, is much slower to recover. Several studies of patients with stroke indicate that most recovery occurs within 4 to 6 weeks of onset. Patients with persistently severe neglect 4 weeks after onset may have incomplete long-term recovery and often do very poorly in rehabilitation. In Massachusetts, for example, only visual fields and acuity are considered relevant to driving, but patients with any degree of hemispatial neglect, regardless of their visual fields, should not drive. Significant neglect also probably precludes cooking at open stovetops and using power tools.
Visually Guided Movement As noted earlier, the superior visual association systems are involved in mechanisms of hemispatial attention (detection of the presence of a stimulus, its distance, and its direction of movement), not in mechanisms of visual recognition. This is commonly expressed as the view that dorsal visual systems (occipitoparietal) are concerned with the “where” of an object, and the ventral visual systems (occipitotemporal) are concerned with the “what” of an object. One implication of that dichotomy is that the parieto-occipital regions are concerned with generating movements toward a
detected object. This could involve eye movements to obtain fixation (the better to facilitate discrimination in the ventral systems) or limb movements to capture the object. For eye movements, active fixation must be disengaged, presumably by frontal to occipital projections, allowing new fixations to be made. For limb movements, there must be a cerebral representation of location that allows for size (large objects at a distance occupy the same retinal space as small objects that are near) and movement and that can represent space in both visual and kinesthetic forms so that rapid movement to a visually detected point can occur. The superior parietal lobe contains cells that serve this purpose, and projections to frontal cortex guide these movements. White matter pathways in the parietal lobe between the frontal gaze center (area 8) and the occipital gaze center (area 19) allow the fixation changes. AU these mechanisms work only in contralateral space, depending on parietal callosal connections to drive movement of limbs to a target in the field contralateral to the arm used (i.e., the left arm into right space). Damage to these parietal systems produces a deficit in directing gaze toward an object in space contralateral to the lesion and a deficit in directing the hand toward the object. These two deficits disappear as soon as the object is in central fixation because now both hemispheres have spatial information and guide the limbs. The deficits in eye movement are well known to clinicians, especially for patients with right brain lesions, as gaze preference, poor fixation or tracking into the impaired field, and impaired optokinetic nystagmus. The limb movement deficit, often called impaired visually guided reaching or optic ataxia, is not as well known because all bedside reaching tasks are done to a fixated target. If the patient is forced to reach to a target in the peripheral field, he or she will be unable to direct movement to the target. This is easily tested at bedside. First, proprioceptive deficits and visual field loss must be assessed. If they are absent, visually guided reaching can be tested by having the patient maintain central fixation on the examiner’s nose and then asking him or her to reach to a fingertip held a few degrees into the impaired side of space. Most patients, and in fact most neurologists, are amazed at how easily this is normally accomplished on the intact side. Any structural lesion in the posterior parietal lobe may produce these deficits. Because the superior parietal lobule (area 7) is particularly critical for visually guided reaching, the usual middle cerebral artery territory infarction may not cause a problem. Most reported cases have been tumors, penetrating trauma, spontaneous hemorrhages, or high watershed infarctions. They do not cause hemiparesis, hemiproprioceptive loss, or hemianopia, so the specific reaching deficit can be demonstrated. There is no known treatment for these deficits, but their prognosis generally is favorable because of the instantaneous correction produced by central fixation once gaze is appropriately directed. The same techniques described as direct treatment of neglect may be useful in accelerating recovery.
Balint‘s Syndrome Balint’s syndrome represents the effects of bilateral parietal lesions in which central visual fixation cannot compensate because neither hemisphere can generate normal visual attention or visual control of movement. Thus, it is as though patients have bilateral neglect, attending only to what is at fixation, neglecting nonfixated targets on either side. Furthermore, they may be trapped in fixation, unable to direct gaze volitionally to any other target. Finally, they have severe bilateral optic ataxia, even to targets in
Chapter 141
fixation, because neither hemisphere can represent location or spatially guided movement. These three elements-visual inattention, so-called psychic paralysis of gaze, and optic ataxiaconstitute Balint’s syndrome. Some patients have partial inferior altitudinal visual field defects. The disorder requires bilateral parietal lesions. Most reported cases have been through-and-through gunshot wounds or butterfly gliomas, but bilateral posterior parietal strokes, often watershed type, also can produce Balint’s syndrome. No treatment has been suggested. The prognosis is quite poor, and patients may actually function better if blindfolded because they will rely on proprioception exclusively.
RELATED DISORDERS OF SPATIAL-MOTOR CAPACITY Several cognitive disorders related to visuospatial impairments are not usually considered in this context and should be mentioned briefly.
Limb Praxis Apraxia is almost universally covered in papers on aphasia for several reasons. First, both are common after left-sided brain lesions, and they commonly co-occur. Second, both have a communicative intent, at least as praxis is usually tested. Third, both apraxia and aphasia are viewed as related to handedness. In the context of this chapter, it is important only to note that praxis involves learning to use the arm and hand for a large number of tasks. The constraints of the tasks are spatial and kinesthetic, not communicative. Throwing a ball entails activating a series of movements designed to bring the hand and fingers to a particular point where the ball can serve as a substitute for the hand to travel to a point specified in visual space. Stirring a cup of coffee is highly restricted by the spatial limits of the cup and the implications of that space for the restrictions of movement. Ideomotor apraxia is the inability to carry out learned movements in response to request or imitation. Limb praxis, as usually tested, probes the preservation of the movement patterns unconstrained by space or by the use of actual objects. Deficits in these movement patterns usually are ameliorated by spatial cues (such as a real object). Patients with ideational apraxia may be able to demonstrate correct movement patterns but cannot place them correctly in space. Thus, they cannot actually throw a ball, stir a cup, and so on. This has been called tool-use apraxia but is now considered the most transparent manifestation of ideational apraxia. Patients may have either apraxia in isolation or both ideational apraxia and ideomotor apraxia. Others may have such severe ideomotor apraxia that they do not even improve with the context of an actual object. Lesions can be in the praxis-dominant parietal lobe, usually the left, at least in right-handers, or they can be anywhere in the projections from the parietal lobe to the motor systems that control the movement, whether of the ipsilateral or contralateral hand. In fact, large corona radiata lesions often produce the most persistent ideomotor apraxia of the left hand associated with right hemiparesis. Ideational apraxia is also associated with lesions in the praxis-dominant hemisphere, usually large and including superior parietal lobe and deep white matter. These are the brain regions that code the neural basis for learned movements and also for the proper placement of the movements in space. The clinical assessment is straightforward. Once the patient’s comprehension is established, he or she is asked to pretend to carry out a number of learned movements. If the patient fails, he
Higher-Order Visual Impairments
901
or she is given actual objects to use. Nurses and therapists usually are aware of isolated ideational apraxia before neurologists. No treatment is known. Ideational apraxia has major implications for self-care. The prognosis usually is good, especially for very familiar movements of everyday care.
Dressing Apraxia Most patients who are unable to dress themselves fail for neurologically mundane reasons, severe weakness, visual neglect, or confusion. A very small number have trouble dressing because they cannot represent the spatial, kinesthetic components of visually guiding their limbs into the clothes. This is a primary dressing disorder (dressing upruxiu is a confusing term). Lesions producing this deficit are found in the right superior parietal region. No treatment has been suggested, but selecting clothes that are not visually confusing and laying them out in a manikin-like manner are helpful. The prognosis usually is favorable. Patients with Balint’s syndrome have both ideational apraxia and dressing apraxia.
DrawSng lmpainnents The topic of drawing impairments is too complex to address completely. Nevertheless, it should be clear that parieto-occipital lesions would produce deficits that would make drawing or copying difficult. Lesions of either hemisphere produce disturbances in these visuoconstructive tasks. The tasks entail at a minimum integration of movement with perception, complete attention to the entire visual target, and the ability to direct attention to subcomponents of the target. Patients with left parieto-occipital lesions usually conserve the overall design of the target (low spatial frequency), whether drawing from memory or copying. Probably because of coincident neglect and inability to register the configuration of the entire target, right posterior lesions produce much worse drawings and constructions than left posterior lesions. Patients with right-sided lesions may lose the overall design, attempting to place individual, well-constructed subparts (reflecting high spatial frequency) without respect to the total configuration. Patients with right-sided lesions may also start from the middle of the object and work to the right, never or incompletely returning to the left side. These differences in visuoconstructive deficits can be brought out by having the patient draw familiar but complex figures from memory (e.g., house, flower) and copying novel, complex geometric figures. This part of the examination, combined with neglect tests, takes no more than a few minutes and may be a much clearer window into the patient’s deficits than any other testing. There is almost no information about natural history of constructional impairments. The purpose of treatment would not be clear, and no specific treatments have been proposed.
CONCLUSION The clinical classification follows from answering four questions: Is there an impairment of visual discrimination or recognition? Is there an impairment in visual attention? Is there a deficit in visuospatially controlled movement (eye movements, limbs, or whole body)? Is the deficit demonstrated with language-based or non-languagebased tasks?
902
BehavioralNeurology and Epilepsy
rn
Behavioral Neurology
The higher-level visual processing disorders have been extraordinarily informative vehicles for constructing theories of how the brain carries out complex mental operations. Although some parts of these fascinating scientific questions have been addressed here, the primary focus has been clinical. In clinical practice these disorders are not uncommon, and this chapter has summarized the causes and clinical settings in which they are encountered and the most direct strategies of bedside diagnosis. To the extent that they are treatable, current treatment strategies have been reviewed.
SUGGESTED READINGS Benson DF, Greenberg J P Visual form agnosia. Arch Neurol 20:82-89, 1969
Coslett HB, Saffran E Simultanagnosia. Brain 114:1523-1545, 1991 Damasio AR, Benton AL: Impairment of hand movements under visual guidance. Neurology 29:170-174, 1979 Damasio A, Damasio H: The anatomical basis of pure alexia. Neurology 33~1573-1583, 1983
Damasio AR, Damasio H, Van Hoesen GW Prosopagnosia:anatomic basis and behavioral mechanisms. Neurology 32:331-341, 1982 Damasio AR, Yamada T, Damasio H: Central achromatopsia: behavioral, anatomic, and physiologic aspects. Neurology 30:1064-1071, 1980 DeRenzi E: Disorders of Space Exploration and Cognition. Wiley, Chichester, UK, 1982
DeRenzi E Prosopagnosia in two patients with CT scan evidence of damage restricted to the right hemisphere. Neuropsychologia24385389, 1986
DeRenzi E, Lucchelli F: Ideational apraxia. Brain 113:1173-1188, 1988 D’Esposito M, McGlinchey-Berroth R, Alexander MP et ak Dissociable cognitive and neural mechanisms of unilateral visual neglect. Neurology 43~2638-2644, 1993 Feinberg T, Heilman KM, Rothi LG Multimodal agnosia after unilateral left lesion. Neurology 36864-867, 1986 Halligan PW, Marshall JC: Figural modulation of visuo-spatial neglect: a case study. Neuropsychologia 29:619428, 1991 Henderson VW, Friedman RB, Teng EL, Weiner JM: Left hemisphere pathways in reading: inference from pure alexia without hemianopia. Neurology 35:962-968, 1985 Hodges JR, Patterson K, Oxbury S, Funnell E Semantic dementia. Brain 115:1783-1806, 1992
Marshall RS, Lazar RM, Krakauer JW, Sharma R Stimulus context in hemineglect. Brain 121:2003-2010, 1998 Mesulam MM: A cortical network for directed attention and unilateral neglect. Ann Neurol 10:309-325, 1981 Petersen SE, Fox PT, Posner MI, Raichle ME Activation of extrastriateand frontal cortical areas by visual words and word-like stimuli. Science 2491041-1044, 1990
Ro T, Rafal RD: Perception of geometric illusions in unilateral neglect. Neuropsychologia 34:973-978, 1996 Tyler HR Abnormalities of perception with defective eye movements. Cortex 4154-177, 1968 Zeki S: A century of cerebral achromatopsia. Brain 113:1727-1777, 1990
142 Disorders of Memory Ronald C. Petersen Memory complaints are common in clinical practice, especially as the patient population ages. Memory is an essential cognitive function, and even a mild impairment can disrupt one’s professional and social life. Occasionally memory disorders are the patient’s sole complaint and can be very disabling. Among cognitive complaints, memory dysfunction is the most common problem brought to the clinician’s attention, yet it can be perplexing to evaluate. The clinician must determine the following: Does a memory problem exist? What is the anatomic site of the problem? What is the mechanism of the disorder? What treatments are available?
DOES A MEMORY DISORDER EXIST? This can be a difficult question to answer. Patients and families often attribute any type of cognitive or emotional disorder to a memory problem. It is as if memory function is the final common pathway for a variety of cognitive complaints. The clinician must be certain that the patient is not referring to difficulties with attention, concentration, naming, or language. For example, it is typical for an older patient to complain of word-finding difficulties and attribute this to a poor memory. A major problem exists in the memory literature with respect to terminology. Memory functions are complex, so various terms
have developed over the years to describe different aspects of learning and recall performance. Although several sets of terminology relating to multiple theoretical models have evolved over the years, there are certain commonalties among the various theoretical approaches. These features can be appreciated by considering a classic amnestic syndrome such as that resulting from bilateral amygdalohippocampectomies or the alcoholic Wernicke-Korsakoff syndrome. In these examples, the primary cognitive dysfunction is one of impaired learning or acquisition of new information. The neurologic process thought to be disrupted in this disorder is consolidation or the actual formation of a more permanent memory trace. Failure of the consolidation process is also known as anterograde amnesia, referring to the inability to lay down new memories after the onset of the memory disorder. In dramatic cases of the amnestic syndrome, the clinician may spend much time interviewing and examining the patient with a seemingly normal interpersonal interaction. The clinician may then leave the room to return 5 minutes later and find the patient unaware of the previous interview or of having met the clinician. This dramatic amnesia results from a failure of consolidation. In the typical amnestic syndrome, information acquired before the onset of the memory disorder is variably recalled. Typically, older memories may be better preserved than more recently experienced events. This gradient may reflect an ongoing consolidation failure in recent days and months that may degrade the more recently acquired information. When a patient does not
902
BehavioralNeurology and Epilepsy
rn
Behavioral Neurology
The higher-level visual processing disorders have been extraordinarily informative vehicles for constructing theories of how the brain carries out complex mental operations. Although some parts of these fascinating scientific questions have been addressed here, the primary focus has been clinical. In clinical practice these disorders are not uncommon, and this chapter has summarized the causes and clinical settings in which they are encountered and the most direct strategies of bedside diagnosis. To the extent that they are treatable, current treatment strategies have been reviewed.
SUGGESTED READINGS Benson DF, Greenberg J P Visual form agnosia. Arch Neurol 20:82-89, 1969
Coslett HB, Saffran E Simultanagnosia. Brain 114:1523-1545, 1991 Damasio AR, Benton AL: Impairment of hand movements under visual guidance. Neurology 29:170-174, 1979 Damasio A, Damasio H: The anatomical basis of pure alexia. Neurology 33~1573-1583, 1983
Damasio AR, Damasio H, Van Hoesen GW Prosopagnosia:anatomic basis and behavioral mechanisms. Neurology 32:331-341, 1982 Damasio AR, Yamada T, Damasio H: Central achromatopsia: behavioral, anatomic, and physiologic aspects. Neurology 30:1064-1071, 1980 DeRenzi E: Disorders of Space Exploration and Cognition. Wiley, Chichester, UK, 1982
DeRenzi E Prosopagnosia in two patients with CT scan evidence of damage restricted to the right hemisphere. Neuropsychologia24385389, 1986
DeRenzi E, Lucchelli F: Ideational apraxia. Brain 113:1173-1188, 1988 D’Esposito M, McGlinchey-Berroth R, Alexander MP et ak Dissociable cognitive and neural mechanisms of unilateral visual neglect. Neurology 43~2638-2644, 1993 Feinberg T, Heilman KM, Rothi LG Multimodal agnosia after unilateral left lesion. Neurology 36864-867, 1986 Halligan PW, Marshall JC: Figural modulation of visuo-spatial neglect: a case study. Neuropsychologia 29:619428, 1991 Henderson VW, Friedman RB, Teng EL, Weiner JM: Left hemisphere pathways in reading: inference from pure alexia without hemianopia. Neurology 35:962-968, 1985 Hodges JR, Patterson K, Oxbury S, Funnell E Semantic dementia. Brain 115:1783-1806, 1992
Marshall RS, Lazar RM, Krakauer JW, Sharma R Stimulus context in hemineglect. Brain 121:2003-2010, 1998 Mesulam MM: A cortical network for directed attention and unilateral neglect. Ann Neurol 10:309-325, 1981 Petersen SE, Fox PT, Posner MI, Raichle ME Activation of extrastriateand frontal cortical areas by visual words and word-like stimuli. Science 2491041-1044, 1990
Ro T, Rafal RD: Perception of geometric illusions in unilateral neglect. Neuropsychologia 34:973-978, 1996 Tyler HR Abnormalities of perception with defective eye movements. Cortex 4154-177, 1968 Zeki S: A century of cerebral achromatopsia. Brain 113:1727-1777, 1990
142 Disorders of Memory Ronald C. Petersen Memory complaints are common in clinical practice, especially as the patient population ages. Memory is an essential cognitive function, and even a mild impairment can disrupt one’s professional and social life. Occasionally memory disorders are the patient’s sole complaint and can be very disabling. Among cognitive complaints, memory dysfunction is the most common problem brought to the clinician’s attention, yet it can be perplexing to evaluate. The clinician must determine the following: Does a memory problem exist? What is the anatomic site of the problem? What is the mechanism of the disorder? What treatments are available?
DOES A MEMORY DISORDER EXIST? This can be a difficult question to answer. Patients and families often attribute any type of cognitive or emotional disorder to a memory problem. It is as if memory function is the final common pathway for a variety of cognitive complaints. The clinician must be certain that the patient is not referring to difficulties with attention, concentration, naming, or language. For example, it is typical for an older patient to complain of word-finding difficulties and attribute this to a poor memory. A major problem exists in the memory literature with respect to terminology. Memory functions are complex, so various terms
have developed over the years to describe different aspects of learning and recall performance. Although several sets of terminology relating to multiple theoretical models have evolved over the years, there are certain commonalties among the various theoretical approaches. These features can be appreciated by considering a classic amnestic syndrome such as that resulting from bilateral amygdalohippocampectomies or the alcoholic Wernicke-Korsakoff syndrome. In these examples, the primary cognitive dysfunction is one of impaired learning or acquisition of new information. The neurologic process thought to be disrupted in this disorder is consolidation or the actual formation of a more permanent memory trace. Failure of the consolidation process is also known as anterograde amnesia, referring to the inability to lay down new memories after the onset of the memory disorder. In dramatic cases of the amnestic syndrome, the clinician may spend much time interviewing and examining the patient with a seemingly normal interpersonal interaction. The clinician may then leave the room to return 5 minutes later and find the patient unaware of the previous interview or of having met the clinician. This dramatic amnesia results from a failure of consolidation. In the typical amnestic syndrome, information acquired before the onset of the memory disorder is variably recalled. Typically, older memories may be better preserved than more recently experienced events. This gradient may reflect an ongoing consolidation failure in recent days and months that may degrade the more recently acquired information. When a patient does not
Chapter 142
recall information learned before the time of injury or ictal event, this is called retrograde amnesia. Although these abnormalities in memory function are prominent, patients with the amnestic syndrome have preserved general intellect, attention, and language. These preserved functions allow patients to carry on a reasonably normal conversation in the immediate time frame, but when patients are asked to recall information encountered in the recent past, they have great difficulties. In this sense, the amnestic syndrome is a rather pure disruption of memory function.
Information ProcessingModel Why does the amnestic syndrome occur? This question can be addressed by invoking an information processing model. Most information is received in the brain through sensory processing systems and is stored for a brief period of time in these systems. These processing networks initially are modality specific and then converge to bring together information regarding a perceptual event from a variety of sensory modalities. The sensory information is held in a temporary register that depends on attention and serves the function of holding the information for subsequent processing. As is shown in Figure 142-1, the temporary processing register is of limited capacity, and the information persists in this store for only a short period of time (seconds).While information is in this temporary register, some of it is selected for further processing, dependent on the experience of the individual and the requirements of the learning situation. For example, if one were to process information regarding a soft drink can, certain visual features of its shape, color, and size would be held in a visual information register briefly. If the can were held in the hand, somatosensory information also would be retained, and if one manipulated the can to hear the sound of bending aluminum, auditory information would also be held in a register for a brief period of time. AU this information ultimately would coalesce, but in its initial processing phase it would be held in the modalityspecific stores. This limited-processing temporary store can be assessed clinically by asking patients to recite digit spans such as telephone numbers. Typically, most people can process up to seven independent items of information and hold them for up to a minute without rehearsal. However, if the material is not rehearsed or further encoded, the information decays rapidly. The actual learning process entails encoding this information in terms of previous experiences and transferring it to a more
903
permanent memory register. This transfer process, previously called consolidation, is the primary site of dysfunction in most organic amnesias. In the amnestic syndrome, patients are able to recite a normal digit span but are unable to transfer information from this temporary store to a more permanent memory register. The transfer of information from the temporary store to the more permanent register can be assessed by providing the patient with a list of items, such as words, that exceeds the immediate memory span of approximately seven units or by requiring the patient to recall the information after a delay interval filled with intervening activities that prevent rehearsal. For example, to use the latter technique the clinician could present five or six words to patients and ask them to remember the words over a series of three or four learning trials. The clinician could then engage in other activities for perhaps 15 minutes and ask the patient to try to recall the five or six words after the 15-minute delay. This technique can be useful to the clinician for assessing this critical aspect of information processing involved in consolidation. Figure 142-1 presents a schematic of this information processing model and provides some terminology that corresponds to various aspects of the scheme and tasks that can be used to assess the various aspects of processing. Most investigators accept these features of memory function as universal but use a variety of terms to discuss these concepts in various theoretical models. Some of the more commonly used terms in various theoretical discussions of memory are defined in this chapter.
Psychological-Anatomic ProcessingModel One of the problems for the clinician in assessing memory disorders concerns the terminology and the literature. Many terms are used to describe various aspects of memory function. A popular model for memory has been proposed and refined by Dr. Larry Squire and colleagues at the University of California at San Diego. Figure 142-2 shows a modification of his model with putative anatomic loci for these functions. Most memory complaints clinicians deal with in the office setting concern declarative or explicit memory functions. This type of memory is accessible to the patients through conscious mechanisms, whereas the nondeclarative aspects of long-term memory generally are not accessible to consciousness. When patients complain of memory problems, they are referring to declarative or explicit memory processes as shown in Figure 142-2, and the anatomic substrate for
I'
Temporary Store
FIG. 142-1. Information processing scheme depicting a temporary store and a more permanent store. For each store, alternative terms in various theoretical models and office testing procedures are indicated.
Disorders of Memory
n Permanent Store
PrimaryMemory Working Memory
Long-term Memory Secondary Memory Recent, Remote Memory E#=, Semantic
Digit Span 3 or 4 Word Lists
Delayed Recall
Short-term Memory
Behavioral Neurologyand Epilepsy rn Behavioral Neurology
904
Long-term memory i
I Declarative I
NondecIarative (implicit)
(explicit)
Facts
Events
Procedures
I
Medial temporal lobe
ClassicaI conditioning I
Nonassociat ive learning
F
I
Limbic system
I
1
Fcortex
I Amygdala IlCerebelluml CP1019535B-1
FIG. 142-2. Model of memory including declarative and non-declarative memory processes as proposed by Dr. Larry Squire. (Adapted with permission from Squire LR: Memory and Brain. Oxford University Press, 1987.)
these disorders is likely to involve medial temporal lobe and limbic system structures. Figure 142-2 can be interpreted in the context of the following glossary.
Glossary Short-Term Memory. This terms refers to the limitedcapacity temporary storage buffer shown in Figure 142-1. It has a finite capacity, and information remains in the store for a brief period of time (seconds to a minute) without rehearsal. This type of store would hold a telephone number for a short time. It reflects an attentional rather than a memory process. This term often is used loosely in clinical practice and, without a specific definition, should be avoided. Long-Term Memory. This aspect of memory function refers to the more permanent large-capacity memory store also outlined in Figure 142-1. Long-term memory usually refers to our knowledge base of previously learned information. Occasionally, this store is divided into two components: recent memory and remote memory. These terms are defined imprecisely along a temporal dimension, with recent memory typically referring to memories hours to days in duration and remote memory referring to distant
past memories of many years. However, these terms are not specific. Primary Memory. This term is similar with respect to retention duration to the concept of short-term memory. Primary memory refers more to the processing nature of this type of memory than to the actual storage function. It tends to deemphasize a precise temporal gradient and describes the type of processing performed on material held in the temporary store. Secondary Memory. In a similar fashion, this term refers to memory processes that support retention across long retention intervals. It is somewhat similar to the long-term memory notion but emphasizes the processes involved in the storage and retrieval of previously learned information rather than the temporal dimension. Working Memory. This term refers to material held in primary memory on which further elaboration is done. This concept refers to the selection of material in the temporary store for further processing and encoding into the more permanent memory store. Working memory refers to encoding processes and the use of strategies for facilitating consolidation. This is a dynamic aspect of memory and can be impaired in attentional disorders.
Chapter 142
Episodic Memory. This term refers to memory for events that are related to a specific spatial or temporal context. There is no temporal dimension to this type of material; rather, this concept incorporates the specific situation in which an event was remembered. For example, when a person tries to learn a list of words in a particular setting, this material would be referred to as existing in episodic memory. This type of memory is severely affected in pathologic processes involving the medial temporal lobes and diencephalic structures and is impaired in most organic amnesias. Semantic Memory. This term typically is used in contrast to episodic memory to refer to information that is stored in the more permanent knowledge base without any reference to the specific learning context. For example, information that we have learned about a concept such as gravity would be incorporated into our semantic memory store despite the fact that we do not remember the specific context in which we acquired this information. This type of information forms our knowledge of the world and is resistant to disruption in many memory disorders. Declarative Memory. This refers to memory that is directly accessible to consciousness and is also significantly affected in most organic amnesias. Declarative memory refers to recently experienced information about which we are aware and often remember the circumstances in which it was learned. Damage to medial temporal and diencephalic structures can disrupt this type of memory. Procedural Memory. In contrast to declarative memory, this form of memory refers to skills and procedural operations. Certain overlearned motor skills and mechanical sequences are part of procedural memory. This type of memory often is spared in many organic amnesias and presumably involves structures in the basal ganglia rather than the medial temporal lobe or diencephalic structures. Encoding. Encoding is the acquisition or learning of new information. In particular, this term refers to the actual psychological representation of the new information with respect to previously learned material. That is, the new information is encoded with respect to the person’s knowledge of the world. Retrieval. This term refers to the spontaneous reproduction of information stored in the long-term or permanent memory store. That is, once information has been encoded or learned and it is recalled at a later point in time, the item often is referred to as being retrieved. This requires accessing previously learned information (i.e., one’s knowledge of the world) to reproduce the information. Recognition. This term refers to the matching of a piece of information to a previously experienced event. That is, in contrast to retrieval, where the item is reproduced spontaneously from memory, in recognition a newly presented item is matched with a previously learned or experienced piece of information. In this sense, it is useful at identifylng previouslylearned items as a means of testing memory. In this form of memory test, the to-beremembered items are presented to the person along with distractor items, and the person is asked to identify the correct items. A multiple-choice test is an example of a recognition exercise. Summary. As one can see, there are many terms that refer to multiple aspects of memory function. These terms are not mutually exclusive and at times refer to very similar concepts. The individual differences among the terms emanate from the theoretical background from which they are derived and pertain to one theoretical model or another. Each of these terms can be useful in
Disorders of Memory
905
specific instances, but the overall concept of temporary and more permanent memory stores ultimately may be more useful. Does a Memory Problem Exist?
Based on the information presented in this conceptual frame, the clinician can then decide whether the patient’s problem involves memory primarily or other cognitive functions. If the patient appears to be describing a failure of consolidation with preservation of attention, language, and other cognitive processes, then it is likely that the clinician is dealing with an organic memory disorder, and an evaluation is appropriate.
WHAT IS THE SITE OF THE PROBLEM? To a certain extent, the information processing scheme outlined in Figure 142-1 has anatomic analogues. For example, as is shown in Figure 142-3, the primary sensory receiving areas and the unimodal (modality-specific) association areas corresponding to each sensory modality provide the substrate for the input processing of sensory information. Superimposed on this sensory processing scheme are attentional functions, which are largely subserved by frontal and subcortical structures. One role of attention in sensory processing is to preserve the incoming information in the temporary holding store. In addition, certain association areas in the right hemisphere (temporoparietal and frontal association areas) may also contribute to the selective preservation of information in these temporary memory registers. After initial processing in the primary sensory and unimodal association areas, the information is elaborated upon and transferred through multimodal association areas residing largely in temporoparietal and frontal regions. These areas combine the individual modality-specific aspects of the stimulus to be remembered and further enrich the elaboration of the information. Using the example of a soft drink can cited earlier, all the properties of the individual modalities such as the visual, somatosensory, and auditory aspects of the can itself would coalesce into the multimodal sensory areas to provide a richer perception of the individual sensory experiences. The soft drink can not only would have visual features of a cylinder of a certain size but also would have somatosensory features of a smooth object and auditory features of an aluminum can. The information is then transferred from the multimodal association areas to the limbic system, largely through the entorhinal cortex and parahippocampal regions (Fig. 142-3). The experience is then processed through the perforant pathway of the entorhinal cortex into the hippocampal formation and limbic system, which is the anatomic basis for major aspects of the consolidation process. It is important to realize that the information is not stored in the hippocampal formation and limbic system but rather is processed in these regions and ultimately transferred back to cortical association areas where the neural networks exist, which embody the remembered information. The actual neural representation of the information to be remembered is diffusely distributed in neocortical regions, and these areas correspond to the more permanent aspects of storage in the information processing model. This interaction between the association areas and the limbic system is a dynamic process, with the remodeling of information in the more permanent stores taking place regularly. Consequently, memory should be viewed as a dynamic process with constant reorganization of information rather than as a passive system of storage of facts and information.
906
BehavioralNeurology and Epilepsy H Behavioral Neurology
FIG. 142-3. Anatomic localization of the flow of information from sensory association areas to temporolimbic structures for memory acquisition. (0) Somatosensory association area; (b) auditory association area; (c) visual association area.
Returning to our soft drink can example, it is at the point of the limbic system involvement that the soft drink can takes on meaning as a soft drink can based on our previous knowledge. In addition, if we have had previous personal experiences with certain types of soft drink cans, these aspects of the sensory event are brought to bear on remembering this particular perceptual event. In this model, although many areas of cortex and subcortical regions are involved in acquisition, the temporolimbic system is the critical focus of much of the consolidation activity. The clinician needs to focus on the temporolimbic system as a site of impairment in most organic amnesias with significant acquisition or consolidation defects. Most commonly encountered amnestic syndromes involve dysfunction of these structures. In summary, when encoding or acquisition processes are primarily involved, the most likely structures implicated are the medial temporal lobe including the entorhinal cortex, perforant pathway, hippocampal formation, thalamus, hypothalamus, surrounding third ventricular structures, basal forebrain, and multiple interconnecting pathways. Most disease processes that affect memory significantly involve these structures anatomically or pharmacologically. For severe memory disorders, the involvement must be bilateral. However, unilateral lesions can give materialspecific deficits such as verbal or nonverbal processing difficulties. The anatomic localization of retrieval processes is less clear but probably involves some aspect of limbic system processing as well as other regions of the cerebral cortex such as the prefrontal cortex. This region may be involved in attention and retrieval strategy generation, whereas the temporoparietal neocortex, in-
cluding higher-order association areas, may be where the neural networks that embody the material to be remembered reside. These structures subserve the anatomic localization of the more remote memories or knowledge base and consequently are preserved except in the setting of diffuse or advanced disease processes.
WHAT I S THE MECHANISM OF THE DISORDER? As with all neurologic disorders, the temporal course of the development of the symptoms is of paramount importance. This factor, coupled with other features of the history such as head trauma, alcohol use, concomitant cancer, vascular disease, or psychiatric illnesses, may all give the clinician insight into possible mechanisms (Table 142-1). Acute Memory Loss
From a temporal perspective, if the memory disturbance has come on acutely, the clinician should consider a vascular cause. Because many of the central limbic structures that subserve memory are in the distribution of the vertebrobasilar arterial system, these structures should be investigated. For example, ischemia to the medial temporal lobes or the thalamus can present with the acute onset of a memory impairment. Other conditions that can produce an acute memory loss include transient global amnesia, about which the precise mechanism is not known, but presumably some type of temporary dysfunction of these critical structures is involved. In certain other
Chapter 142
medical contexts, hypoxia, hypoglycemia, migraine, intracerebral hemorrhages (particularly resulting from anterior communicating artery aneurysm rupture), drug ingestion, or toxic exposure could produce an acute memory loss. In addition, psychogenic causes of amnesia must be considered in the appropriate context. Initially, an imaging study may be helpful to evaluate a possible infarct, hemorrhage, mass, or infection. A head computed tomography (CT) scan with and without contrast is helpful initially. However, a negative scan does not rule out all considerations because many of the structures involved in memory function may not be visualized well by CT because they reside in close proximity to the calvaria of the middle cranial fossa, which can produce artifacts on CT. Magnetic resonance imaging (MFU) may be preferred because of its increased sensitivity to detect small lesions in critical structures. Recently, MRIs using certain acquisition procedures have been particularly useful at detecting lesions, including atrophy in the medial temporal lobe region. If an infarct is detected in the thalamus, medial temporal lobe, or limbic system structures, then an investigation of the cause of this event, as discussed in Chapters 28 and 29, must be considered. If the patient complains of multiple acute episodes of memory loss, a complex partial seizure disorder of temporal lobe origin must be considered and pursued. As mentioned, if there is a history of head trauma or psychiatric disease, then these causes must be evaluated as well. Occasionally, transient ischemic attacks of the vertebrobasilar artery circulatory system can present with memory impairment, although usually other neurologic symptoms also occur. Transient global amnesia is a distinctive condition involving a pure amnestic problem of short duration. Typically patients with transient global amnesia cannot lay down any new memories for a period of several hours and have a retrograde amnesia of variable extent. The patient otherwise looks well and is neurologically intact. However, because of their inability to consolidate new information, they ask the same question repeatedly because they are unable to retain the answer that was given to them previously. The precise cause of this condition is not known, but it probably involves medial temporal lobe and limbic system structures on a transient basis. Other causes of temporary dysfunction of the temporolimbic system must be considered also, such as ischemia or a seizure disorder, but if there are no other features of these alternative conditions, transient global amnesia may be the best explanation.
TAW 142-1. Onset of Memory Disorders mme
Cause
Acute
Seconds to minutes
Subacute
Days to weeks
Chronic
Months to years
Vascular‘ ischemic Hemorrhagic Transient global amnesia* Seizure disorder‘ Migraine* Hypoxia infectious inflammatory Metabolic Toxic Neoplastic Degenerative Neoplastic Deficiency state Psychiatric
‘Can be episodic
Disorders of Memory
907
Finally, nonorganic or psychogenic conditions can present with an acute memory loss. Often these amnesias have certain features that distinguish them from organic memory problems. Typically, a retrograde amnesia is a prominent feature of the symptom complex, often in the setting of preserved learning and acquisition (i.e., no anterograde amnesia). These patients may claim to have forgotten their names, family information, and occasionally emotionally laden experiences. Although prominent isolated retrograde amnesia cases have been reported in association with brain injury, they are uncommon. In evaluating suspected nonorganic amnesias, the patient’s performance often provides clues. The patient may give inconsistent responses on tests, fail easier memory tasks such as recognition tests, and perform normally on free recall. Patients may forget information that is distinctly resistant to loss, such as personal identity. However, the clinician should also seek supporting psychiatric evidence for nonorganic amnesias before concluding that the memory deficit has no organic basis. Subacute Memory Loss A subacute (days to weeks) evolution of a memory disorder would raise the consideration of infectious, inflammatory, toxic, or metabolic causes. Other features of the history and examination should alert the clinician to consideration of infectious causes and possible cerebrospinal fluid analysis. Herpes simplex encephalitis must be considered, especially in the setting of altered cognition with seizures because this is a treatable condition. Some inflammatory conditions may present with a memory disorder including multiple sclerosis, central nervous system sarcoidosis, and Sjogren’s syndrome. Finally, in the appropriate clinical context, meningeal carcinomatosis or limbic encephalitis can present with a memory impairment, although usually with additional cognitive and neurologic findings. As always, a psychiatric explanation should be considered.
Chronic Memory Loss Finally, if the memory disorder has evolved over months to years, a degenerative disorder such as Alzheimer’s disease becomes much more likely in the appropriate age group. Other considerations include a neoplasm, particularly of the limbic system, deficiency state such as thiamine, or psychiatric conditions including depression. In a degenerative disease such as Alzheimer’s disease, acquisition processes and retrieval processes are affected early and may be the only manifestation of disease in the initial stages. Later, however, other cognitive functions become impaired, and memory is no longer an isolated defect. Occasionally, distinctions are drawn between predominantly cortical dementias, such as Alzheimer’s disease, and predominantly subcortical dementias, such as those seen in Parkinson’s disease, Lewy body dementia, vascular disease, progressive supranuclear palsy, or multiple sclerosis. In subcortical dementias, it is often more difficult for the patient to encode the material, but once it has been learned, it is recalled reasonably well, especially with cues. In cortical dementias such as Alzheimer’s disease, learning is impaired despite adequate effort, and recall with cues is also significantly impaired. The subcortical dementias may also have impaired attention, which contributes to the learning difficulties.The cortical-subcortical distinction must be made with some caution because there is often significant overlap. Investigations of chronic memory disorders include imaging studies, MFU
908
Behavioral Neurologyand Epilepsy
Behavioral Neurology
FIG. 142-4. Theoretical transition from normal aging through mild cognitive impairment to dementia in people who are ultimately destined to develop dementia. (Adapted from Neurologist 1:326344, 1995, with permission.)
or CT scan, and laboratory studies more typical of those associated with a dementia evaluation, as discussed in Chapter 136. Degenerative Memory Disorders of Aging: Mild Cognitive Impairment
Although memory disorders can wcur in patients of any age, most of these problems present in older patients. The clinician often is faced with a patient who asks, “Am I developing Alzheimer’s disease?” In the setting of mild forgetfulness in an older patient, this can be a perplexing question. In recent years, a great deal of research has been done on the concept of mild cognitive impairment. Mild cognitive impairment is regarded as a transitional state between normal aging and Alzheimer’s disease, as depicted in Figure 142-4. Presumably, people who develop Alzheimer’s disease do so over many years. The transition can be gradual. Mild cognitive impairment is defined by the criteria outlined in Table 142-2. The ultimate diagnosis of mild cognitive impairment is clinical. Essentially, these patients have a memory impairment that is out of proportion to what would be expected for their age and education, yet they are not demented. These patients are functioning independently in the community and do not appear impaired. However, when the patient is tested in a more rigorous setting, a memory impairment is apparent and significant. From a historical standpoint, these patients tend to forget important information more often than they have in the past. The casual forgetfulness for people’s names or locations of car keys probably is not significant, but forgetting an important event or appointment may be significant. For example, if a person is having difficulty remembering doctors’ appointments or social engagements to which he or she is committed, this may be meaningful. In particular, if this represents a change from the person’s previous behavior, and this is apparent to those who know the patient well, this may be of sufficient concern to merit an evaluation. Because the diagnosis of mild cognitive impairment is clinical, neuropsychological testing can be very helpful but is not definitive.
TABLE142-2. Clinical Criteria for Mild Cognitive Impairment
Memory complaint, preferably corroborated by an informant Objective memory impairment on clinical testing Largely preserved general cognitive functions Essentially normal activities of daily living Not demented
Ultimately, the clinician must decide who may qualify for this diagnosis. The recognition of this transitional state can be important because patients who meet these criteria have a 10% to 15% annual risk of going on to meet criteria for clinical Alzheimer’s disease. This figure is in contrast to normal subjects of the same age, who develop Alzheimer’s disease at a rate of 1% to 2% per year. No pharmacologic treatments have been demonstrated to be efficacious for mild cognitive impairment. However, counseling as to the nature of the condition and the likelihood of progression over subsequent years can be very useful to subjects for the purposes of future planning. Several clinical trials for mild cognitive impairment are currently under way involving 4000 to 5000 subjects worldwide. The American Academy of Neurology has recently endorsed the concept of mild cognitive impairment through an evidence-based review of the literature. They have published a practice parameter that recommends that clinicians identify, evaluate, and follow patients with a mild cognitive impairment because they are at a greater risk of developing Alzheimer’s disease. As the field evolves, effective treatments may be developed to forestall this progression.
EVALUATION OF MEMORY DISORDERS History The history from a patient with a memory disorder can be very important. Typically, the history should focus on the recall of recent events rather than recall of remote memories that may be preserved. In the course of taking a history, the patient can be asked about recent events in the news, including events of the past few days or significant news items of recent months, such as natural disasters, major crimes, or prominent political events. This line of questioning presumes that the patient has been exposed to these events and a family member can be asked to corroborate these items. Typically most people are aware of major weather events such as hurricanes, earthquakes, or floods that are commonly in the news. If a person is a sports fan, recent events can be tested by asking about performance of the patient’s favorite teams. These questions are meant to assess the acquisition of significant information most people would demonstrate if they have been exposed to the events. Often patients with memory problems are vague about the answers to these questions and provide little detail. The clinician needs to be certain that the patient is attentive and does not have a significant language problem (aphasia) when
Disorders of Memory
Chapter 142
assessing memory. Many people, as they age, are aware of word-finding problems, usually for names of people. They often attribute such problems to a failing memory, and this condition must be assessed because some naming deficits are a part of normal aging and represent a retrieval failure for previously learned information rather than an acquisition or learning problem. Occasionally in taking a history from a patient, certain details of the history itself may be lost. The clinician can get an impression of the severity of the problem by asking the patient to recount events of the past day or two in terms of travel, activities with family members, or how they got to the clinician’s office. Though not necessarily quantitative, these questions can reveal the possibility of a significant memory problem. Mental Status Evaluation An accurate mental status examination is an essential component
of evaluating someone with a memory disorder. As indicated, it is important to determine whether memory is in fact impaired or other cognitive deficits contribute to the problem. A complete discussion of mental status testing is found in Chapter 135. The clinician can use one of the standard mental status examinations available, such as the Mini-Mental State Exam or the Short Test of Mental Status, but must be aware of the limitations of these instruments. These tests usually use three- or four-word lists with a short recall interval and may underestimate early memory deficits. Alternatively, if the patient has difficulty with delayed recall with three or four words, there is probably a significant memory problem. The Short Test of Mental Status also assesses an element of learning by taking into account the number of trials the subject needs to learn the four words accurately. In general, office testing of memory should include sets of verbal and nonverbal materials that are presented over several learning trials. This will give an index of learning or acquisition. A several-minute delay, usually 15 to 30 minutes, should be interposed to assess delayed recall. Recent evidence indicates that in addition to acquisition deficits, delayed recall performance may be a sensitive index of early impairment. Based on the findings of the clinician in the office, specific recommendations can be made to the neuropsychologist for more extensive memory testing. The mental status examination should also include evaluation of attention and language functions (Chapters 139 and 140) to be certain that the patient is not significantly inattentive, leading to poor learning or acquisition, or that the patient does not have a significant aphasia with profound anomia. If the patient performs reasonably well in the general assessment of cognitive function but performs poorly with respect to acquisition or delayed recall, then
the clinician needs to pursue an investigation of the cause of the problem. Inconsistencies or a depressed affect may alert the clinician to psychiatric contributions to the cognitive impairment such as those found in depression. It may be helpful to augment the cognitive components of the mental status examination with an inventory of psychiatric symptoms. NeuropsychologicalTesting
Neuropsychological testing can be viewed as an extension of the mental status examination. The same principles involved in evaluating mental status in the office can be used in interpreting the results of neuropsychological testing. In general, the clinician is interested primarily in the results of the memory tests. The testing should involve acquisition of verbal material that exceeds the primary memory capacity and requires the transfer of information from the temporary memory store to the more permanent memory store. This usually involves multiple learning trials of a list of 10 to 15 words. A delay of approximately 15 to 30 minutes should be interposed between the final acquisition trial and a later recall test. The clinician should assess the patient’s ability to generate a learning curve, that is, improve recall on each successive learning trial. Ultimately the patient should recall more than five or six items over the several learning trials. That is, one should see evidence that the patient has transferred some information from the temporary memory store to the permanent memory store. As shown in Figure 142-5, learning curves can take on characteristic features of underlying disorders. Ideally, performance on these instruments should be assessed relative to age- and education-appropriate norms. After the delay interval, free recall for the material should be assessed, and retrieval performance of at least 50% of the initially acquired material should be achieved. However, this will vary with the age and education of the patient as well. Some neuropsychological learning instruments also involve the use of semantic cueing and facilitated recall. These measures are meant to assess the patient’s ability to use provided acquisition strategies and subsequent recall through the use of these semantic cues. These can be very sensitive tools to detect very early memory impairments involving damage to medial temporal lobe structures. An analogous set of nonverbal materials such as a complex geometric figure should be used as well. There are various instruments for assessing the learning and recall of visuospatial materials. The same principles as applied to verbal learning should be used to assess nonverbal recall. As with the mental status examination, neuropsychological testing should also assess other aspects of cognitive function including attention, language, visuospatial skills, higher reasoning
Normal
FIG. 142-5. Hypothetical learning curves in normal aging, Alzheimer‘s disease, and depression. The significant differences pertain to the slopes of the learning curves and the relation of performance on delayed recall to the final learning trial.
=
3
tx
909
Alzheimer’s Disease
I f . I/ 1
2
3
4
5
h h y
1
f 2
3
4
Trials
5
way
Depression
IT ; 1
2
3
4
5
Delay
Behavioral Neurology and Epilepsy W Behavioral Neurology
910
processes, praxis, and constructions. This will help the clinician determine whether memory is the sole cognitive function impaired or is impaired out of proportion to other mental abilities. It will also help the clinician determine whether other cognitive functions such as attention and language are having an impact on memory performance, thereby necessitating qualification of the memory test results. The combination of the clinician’s history, mental status examination, general neurologic examination, and neuropsychological testing should provide adequate information for a determination of a memory deficit. Occasionally, if performance is equivocal, some of the tests may need to be repeated at an appropriate interval using alternate test forms to determine the stability of the findings. Evaluations of Memory Disorders (Table 142-3) Neuroimaging. If memory function is the primary cognitive disorder affected, limbic system structures must be imaged. A CT scan with and without contrast is helpful, but MRI is more sensitive. Because the relevant structures often are difficult to
visualize on CT images, MRI evaluating temporal lobe structures, the thalamus, basal forebrain, and interconnecting pathways can be particularly useful. Occasionally contrast agents are helpful in bringing out subtle lesions or characterizing possible infarctions. In some instances, functional imaging scans such as positron emission tomography or single photon emission computed tomography are helpful in delineating certain memory disorders. In the early course of some diseases, structural changes may not be evident, and a functional impairment may be the only imaging index of impairment. To a certain extent, these scans are limited by the resolution of the particular instrument, but with improved spatial resolution, these techniques are becoming increasingly sensitive at evaluating medial temporal lobe structures. Because of their limited availability and expense, they should be reserved for selected cases. Electroencephalogram. Because complex partial seizure disorders of temporal lobe origin can present with episodic memory disturbances and occasional persistent memory deficits, an awake and asleep electroencephalogram may be necessary to assess a possible epileptogenic cause of the memory disorder. Careful attention must be paid to seizure foci in the medial temporal and
H TAW 142-3. Evaluation of Memory Disorders Imaging studies
CT MRI PET, SPECT Electroencephalogram Cerebrospinal fluid analysis Microbiology Gram stain Bacterial cultures Fungal cultures AFB cultures Viral cultures PCR: herpes simplex encephalitis, 6. burgdorferi Chemistry Protein Glucose VDRL FTA-Abs IgG index Oligoclonal bands Cell count Cytology Blood studies Chemistry group including glucose Hematology group Sedimentation rate Vitamin B,, Thyroid function studies Toxicology screen Alcohol level Optional ANA ENA Heavy metal screen HIV Lyme serology Copper Ceruloplasmin Anticardiolipin antibody Lupus anticoagulant Anti-Purkinje cell antibody Antineuronal nuclear antibody Arterial blood gas Abbreviations: AFB, acid-fast bacillus; ANA, antinuclear antibodies; CT,computed tomography; EN& extractable nuclear antigens; FIA-Abs, fluorescent treponemal antibody-absorption; HIV, human immunodeficiency virus; IgC, immunoglobulin C; MRI, magnetic resonance imaging; PCR. polymerase chain reaction; PET, positron emission tomography; SPECT, single photon emission computed tomography; VDRL, Venereal Disease Research Laboratory.
Chapter I42
inferior frontal region with this examination. The medial temporal lobe structures, including the amygdala and hippocampus, are among the most epileptogenic structures in the brain, and because they subserve memory, occasionally a subtle complex partial seizure disorder can be the cause of a memory deficit. This study ideally is done with sleep deprivation. Laboratory Evaluation. As indicated earlier, a variety of laboratory studies that assess various processes that are not necessarily specific for a memory dysfunction but can affect cognitive performance must be considered. Tests that can be considered in the appropriate clinical context include a chemistry group, hematology group, sedimentation rate, B,,, folic acid, thyroid function studies, antinuclear antibody, extractable nuclear antigen, 24-hour urine for heavy metals, human immunodeficiency virus, Lyme serology, toxicology screen, alcohol level, copper, ceruloplasmin, anticardiolipin antibodies, lupus anticoagulant, anti-Purkinje cell antibodies, paraneoplastic autoantibodies, and an arterial blood gas. In addition, a cerebrospinal fluid analysis for possible bacterial, fungal, mycobacterial, or viral infections, cell count, total protein, glucose, syphilis serology, immunoglobulin G index, immunoglobulin G synthesis rate, oligoclonal bands, and polymerase chain reaction for herpes simplex virus or Borrelia burgdorferi along with a cytologic examination for neoplastic cells can be considered. All of these tests must be evaluated in the appropriate clinical context, and as indicated earlier, vascular studies may be necessary as well as other evaluations for systemic diseases. Psychiatric Consultation. In the appropriate clinical context, a psychiatric consultation can be useful. Because many psychiatric conditions that may account for or contribute to a memory disorder are treatable, this aspect of the evaluation should be considered. The psychiatrist should be particularly attentive to disorders of mood and anxiety.
Disorders of Memory
91 1
laboratory monitoring. More recently, three additional drugs have been approved donepezil, rivastigmine, and galantamine. These last three drugs produce a modest effect on the symptoms of Alzheimer’s disease, e.g., memory impairment, and can also have positive behavioral effects. Cholinesterase inhibitors have potential side effects including an increase in gastrointestinal motility and theoretically heart rhythm effects or possible increase in bronchial secretions if a person has chronic obstructive pulmonary disease. These drugs can interact with other medications given for anesthesia. A variety of other drugs that work through other mechanisms have been used, such as adrenergic agents, serotonergic compounds, peptides, nootropics, calcium channel antagonists, and antioxidants. Most of these have been studied in the context of Alzheimer’s disease. Occasionally agents designed to augment catecholaminergic functioning have been helpful in treating attention and memory disorders. Compounds such as methylphenidate and bromocriptine have been successful occasionally in some conditions in which attention is the primary cognitive function impaired. Occasionally memory is affected in depression, so treatment of the primary underlying psychiatric disorder can secondarily augment memory function. Some of the newer antidepressants such as fluoxetine, sertraline, and paroxetine can be helpful. These may be activating and may augment attention, which secondarily improves memory. In addition, psychotherapy can be helpful in the appropriate context. The pharmacologic treatment of memory disorders is in its infancy, and a great deal remains to be learned about successful drug treatments. At present, a few drugs are available for altering certain neurotransmitter systems, and new drugs are being investigated. Behavioral Treatments
TREATMENT If a treatable cause of a memory impairment is disclosed during the evaluation of the imaging or laboratory tests, the offending process should be treated. For example, if a seizure disorder is found, appropriate antiepileptic drugs can be used. Similarly, if a neoplasm, infarct, or inflammatory process or an infection such as herpes simplex encephalitis is identified, strategies aimed at treating the underlying disorder should be considered. Often, however, a specific cause is not found or a single insult has occurred, and the patient is left with a significant memory problem. The two major approaches to treating memory disorders involve pharmacologic agents or behavioral measures. The overall state of treatment of these disorders is not particularly advanced, so most of the measures are meant to be palliative. Phannacologic Treatments
Most of the drugs designed to aid memory are modulators of one or more neurotransmitter systems. Because the cholinergic system is intimately involved in attention and memory functions by virtue of its projections in the limbic system, most of the early work on memory disorders has involved drugs designed to enhance cholinergic function. The U.S. Food and Drug Administration (FDA) has approved several drugs for treating Alzheimer’s disease. All of the currently available drugs are cholinesterase inhibitors. The first drug approved by the FDA was tacrine. This drug is no longer used to any significant extent because of the necessary
Most of the behavioral treatments for memory and other cognitive disorders occur in the setting of the treatment of traumatic brain injury. From a practical standpoint, patients with memory disorders can be taught to use external aids such as schedule books, diaries, and watch alarms or to keep a notepad and thereby circumvent many of the problems arising from memory disorders. Alternatively, internal strategies such as mental imagery, semantic elaboration, and mentally retracing one’s steps can also be useful. Often these techniques take training and effort for patients to become skillful at them. Some claim that cognitively impaired people may be incapable of mastering these complex mnemonic strategies. However, in certain instances these techniques can be helpful. Recently, several computer-assisted techniques have been developed to help patients learn new cognitive skills. Some patients can achieve success at acquiring domain-specific knowledge for learning job-related skills. For example, some amnesic patients can be taught the vocabulary and techniques necessary to operate a computer. In certain training settings, cognitive rehabilitation can be successful at enhancing memory and other cognitive functions.
Memory disorders are common in clinical practice, and their identification,evaluation, and treatment can be very rewarding for both the patient and the clinician. Principles of memory function can be applied to the assessment and evaluation of patients with a
912
Behavioral Neurology and Epilepsy W
Behavioral Neurology
memory disorder. Certain anatomic structures are known to be involved in various types of memory disorders, and the evaluation of these structures can be revealing. If a particular problem is disclosed through the evaluation process, remedial steps can be made. Alternatively, treatment strategies involving certain drugs and behavioral techniques can be helpful to patients with memory disorders. ACKNOWLEDGMENTS I would like to thank Donna Asleson for her superb secretarial assistance in preparing this manuscript. Preparation of this chapter was supported by grants from the National Institute on Aging, AG 06786 and AG 16574.
SUGGESTED READINGS Folstein MF, Folstein SE, McHugh PR “Mini-Mental State”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189-198, 1975 Gazzaniga M (ed): New Cognitive Neurosciences. 2nd Ed. MIT Press, Boston, 2000
Jack CR Jr, Petersen RC, Xu YC et al: Medial temporal atrophy on MRI in normal aging and very mild Alzheimer’s disease. Neurology 49786794, 1997 Kokmen E, Smith GE, Petersen RC et ak The Short Test of Mental Status: correlations with standardized psychometric testing. Arch Neurol 48~725-728, 1991 Mesulam MM (ed): Principles of Behavioral and Cognitive Neurology. 2nd Ed. Oxford University Press, New York, 2000 Petersen RC (ed): Mild Cognitive Impairment. Oxford University Press, New York, 2003 Petersen RC, Smith GE, Waring SC et ak