1600 John F. Kennedy Blvd. Ste 1800 Philadelphia, PA 19103-2899 PEDIATRIC NEUROLOGY: PRINCIPLES & PRACTICE
ISBN-13: 9780323033657 Volume 1: Part no. Volume 2: Part no. ISBN-10:
Copyright © 2006, 1999, 1994, 1989 by Mosby Inc All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Permissions may be sought directly from Elsevier’s Health Sciences Rights Department in Philadelphia, PA, USA: phone: (+1) 215 239 3804, fax: (+1) 215 239 3805, e-mail:
[email protected]. You may also complete your request on-line via the Elsevier homepage (http://www.elsevier.com), by selecting ‘Customer Support’ and then ‘Obtaining Permissions.’ Notice Knowledge and best practice in this field are constantly changing. As new research and experience broaden our knowledge, changes in practice, treatment, and drug therapy may become necessary or appropriate. Readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of the practitioners, relying on their own experience and knowledge of the patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions. To the fullest extent of the law, neither the Publisher nor the Editors assume any liability for any injury and/or damage to persons or property arising out of or related to any use of the material contained in this book. The Publisher Library of Congress Cataloging-in-Publication Data Pediatric neurology : principles & practice / [edited by] Kenneth F. Swaiman, Stephen Ashwal, Donna M. Ferriero.—4th ed. p. ; cm. Includes bibliographical references and index. ISBN 0-323-03365-2 1. Pediatric neurology. I. Swaiman, Kenneth F., 1931– II. Ashwal, Stephen, 1945– III. Ferriero, Donna M. [DNLM: 1. Nervous System Diseases—Child. 2. Nervous System Diseases—Infant. WS 340 P3713 2006] RJ486.P336.2006 618.92′8—dc22 2005043798 Acquisitions Editor: Susan Pioli Developmental Editor: Jennifer Shreiner Publishing Services Manager: Frank Polizzano Project Manager: Lee Ann Draud Design Direction: Steve Stave Printed in the United States of America Last digit is the print number: 9 8 7 6 5 4 3 2 1
9996004716 9996004775 0-323-03365-2
DEDICATION
It is our pleasure to dedicate this book to our spouses, Phyllis Sher, Eileen Ashwal, and Thomas Rando, who made it possible for us to spend the enormous amount of time planning, reading, and editing that was necessary to bring this text to fruition. It is impossible to adequately describe the value of their encouragement and support. No dedication of a book embracing this field would be meaningful without a tribute to the courage and perserverance of neurologically impaired children and their caretakers.
CONTRIBUTORS
Anthony A. Amato, MD
Rose-Mary N. Boustany, MD
Associate Professor of Neurology, Harvard Medical School; ViceChairman, Department of Neurology, Brigham and Women’s Hospital, Boston, Massachusetts Inflammatory Myopathies
Professor of Pediatrics and Neurobiology, Duke University Medical Center, Durham, North Carolina; Professor of Pediatrics and Biochemistry and Head, Clinical and Basic Neuroscience, American University of Beirut, Beirut, Lebanon Degenerative Diseases Primarily of Gray Matter
Stephen Ashwal, MD Distinguished Professor of Pediatrics and Chief of the Division of Child Neurology, Loma Linda University School of Medicine, Loma Linda, California Pediatric Neuroimaging; Congenital Structural Defects; Impairment of Consciousness and Coma; Hypoxic-Ischemic Encephalopathy in Infants and Older Children; Determination of Brain Death in Infants and Children; Neurologic Manifestations of Rheumatic Disorders of Childhood; Inflammatory Neuropathies; Neurologic Disorders Associated with Gastrointestinal Diseases, Nutritional Deficiencies, and Fluid-Electrolyte Disorders
Carol S. Camfield, MD
James F. Bale, Jr., MD
Enrique Chaves-Carballo, MD
Associate Chair and Professor, Department of Pediatrics, University of Utah School of Medicine; Attending Physician, Department of Pediatrics, Primary Children’s Medical Group, Salt Lake City, Utah Viral Infections of the Nervous System
Clinical Professor, Departments of Pediatrics and History of Medicine, Kansas University Medical Center, Kansas City, Kansas Syncope and Paroxysmal Disorders Other than Epilepsy
Claudia A. Chiriboga, MD, MPH
Tallie Z. Baram, MD, PhD Professor of Pediatrics, Anatomy/Neurobiology, and Neurology, University of California, Irvine, School of Medicine, Irvine, California Myoclonus, Myoclonic Seizures, and Infantile Spasms
Associate Professor of Clinical Neurology and Pediatrics, Columbia University College of Physicians and Surgeons; Associate Attending Physician, Department of Neurology, Columbia University Medical Center, New York, New York Neurologic Complications of Immunization
Richard J. Barohn, MD
Raymond W. M. Chun, MD
Professor, Department of Pediatrics, Dalhousie University Faculty of Medicine; Pediatrician, IWK Health Centre, Halifax, Nova Scotia, Canada Pediatric Epilepsy: An Overview
Peter R. Camfield, MD Professor, Department of Pediatrics, Dalhousie University Faculty of Medicine; Pediatric Neurologist, IWK Health Centre, Halifax, Nova Scotia, Canada Pediatric Epilepsy: An Overview
Professor and Chair, Department of Neurology, University of Kansas Medical Center and University of Kansas Hospital, Kansas City, Kansas Diseases of the Neuromuscular Junction
Professor Emeritus of Neurology and Pediatrics, University of Wisconsin Medical School, Madison, Wisconsin Interrelationships between Renal and Neurologic Diseases and Therapies
Mark L. Batshaw, MD
Michael E. Cohen, MD
Associate Dean for Academic Affairs and Professor and Chair, Department of Pediatrics, George Washington University School of Medicine and Health Sciences; Chief Academic Officer, Children’s National Medical Center, Washington, DC Inborn Errors of Urea Synthesis
Professor of Neurology and Pediatrics, State University of New York at Buffalo School of Medicine and Biomedical Sciences; Attending Physician, Women and Children’s Hospital, Buffalo, New York Tumors of the Brain and Spinal Cord, Including Leukemic Involvement
Samuel F. Berkovic, MD
Anne M. Connolly, MD
Epilepsy Research Centre and Department of Medicine, University of Melbourne, Melbourne; Director, Comprehensive Epilepsy Program, Austin Health, Heidelberg, Victoria, Australia Genetics of Epilepsy
Associate Professor of Neurology and Pediatrics, Washington University School of Medicine; Attending Physician, St. Louis Children’s Hospital and Barnes Jewish Hospital, St. Louis, Missouri Anterior Horn Cell and Cranial Motor Neuron Disease
Angela K. Birnbaum, PhD
Jeannine M. Conway, PharmD, BCPS
Associate Professor of Experimental and Clinical Pharmacology, College of Pharmacy, University of Minnesota, Minneapolis Minnesota Antiepileptic Drug Therapy in Children
Assistant Professor, Experimental and Clinical Pharmacology, College of Pharmacy, University of Minnesota, Minneapolis, Minnesota Antiepileptic Drug Therapy in Children
Contributors
David L. Coulter, MD
Patricia K. Duffner, MD
Associate Professor of Neurology, Harvard Medical School; Attending Neurologist, Children’s Hospital Boston, Boston, Massachusetts Ethical Issues in Child Neurology
Professor of Neurology and Pediatrics, State University of New York at Buffalo School of Medicine and Biomedical Sciences; Women and Children’s Hospital of Buffalo, Buffalo, New York Tumors of the Brain and Spinal Cord, Including Leukemic Involvement
Tina M. Cowan, PhD
vii
Associate Professor, Department of Pathology, Stanford University School of Medicine; Director, Biochemical Genetics Laboratory, Stanford University Medical Center, Stanford, California Aminoacidemias and Organic Acidemias
Ann-Christine Duhaime, MD
Natalie Z. Cvijanovich, MD
Adré J. du Plessis, MBChB, MPH
Clinical Assistant Professor, University of California, San Francisco, School of Medicine, San Francisco; Associate Physician, Critical Care, Children’s Hospital and Research Center at Oakland, Oakland, California Neonatal Brain Injury
Associate Professor of Neurology, Harvard Medical School; Senior Associate, Neurology, and Director, Fetal-Neonatal Neurology, Children’s Hospital Boston, Boston, Massachusetts Neurologic Disorders Associated with Cardiac Disease
Gregory M. Enns, MB, ChB
Soma Das, PhD
Assistant Professor of Pediatrics and Director, Biochemical Genetics Program, Stanford University School of Medicine; Attending Physician, Lucile Packard Children’s Hospital, Stanford, California Aminoacidemias and Organic Acidemias
Assistant Professor and Director, Clinical Molecular Genetics Laboratory, Department of Human Genetics, Pritzker School of Medicine at the University of Chicago, Chicago, Illinois Introduction to Genetics
Maria Descartes, MD Associate Professor, Department of Genetics and Department of Pediatrics, University of Alabama School of Medicine; Attending Physician, Children’s Hospital, Birmingham, Alabama Chromosomes and Chromosomal Abnormalities
Gabrielle Aline deVeber, MD, MHSc Associate Professor of Pediatrics, University of Toronto Faculty of Medicine; Staff Neurologist and Director, Children’s Stroke Program, The Hospital for Sick Children; Scientist, Population Health Sciences and Brain and Behavior Programs, The Hospital for Sick Children Research Institute, Toronto, Ontario, Canada Cerebrovascular Disease
Darryl C. De Vivo, MD Sidney Carter Professor of Neurology, Professor of Pediatrics, and Director Emeritus, Pediatric Neurology Division, Columbia University College of Physicians and Surgeons; Attending Neurologist and Attending Pediatrician, Columbia University Medical Center and New York–Presbyterian Hospital, New York, New York Mitochondrial Diseases
Salvatore DiMauro, MD Lucy G. Moses Professor of Neurology, Columbia University College of Physicians and Surgeons, New York, New York Mitochondrial Diseases
William B. Dobyns, MD Professor of Human Genetics, Neurology, and Pediatrics, Pritzker School of Medicine at the University of Chicago, Chicago, Illinois Congenital Structural Defects; Introduction to Genetics
Qing Dong, MD, PhD Adjunct Instructor, Department of Pediatrics, University of California, San Francisco, School of Medicine; Attending Physician, UCSF Children’s Hospital, San Francisco, California Endocrine Disorders of the Hypothalamus and Pituitary
Professor of Neurosurgery, Dartmouth Medical School, Hanover; Director, Pediatric Neurosurgery, Children’s Hospital at Dartmouth, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire Inflicted Childhood Neurotrauma
Diana M. Escolar, MD Associate Professor of Neurology and Pediatrics, Department of Neurology, George Washington University School of Medicine and Health Sciences; Investigator, Research Center for Genetic Medicine, and Director, Neuromuscular Program, Children’s National Medical Center and Children’s Research Institute, Washington, DC Muscular Dystrophies
Owen B. Evans, Jr., MD Professor and Chairman, Department of Pediatrics, University of Mississippi Medical Center, Jackson, Mississippi Normal Muscle
Lydia Eviatar, MD Professor of Neurology and Pediatrics, Albert Einstein College of Medicine, Bronx; Chief Emeritus, Pediatric Neurology, Schneider Children’s Hospital of Long Island Jewish Medical Center Health System, New Hyde Park, New York Vertigo
Donna M. Ferriero, MD Professor, Departments of Neurology and Pediatrics; Division Chief, Child Neurology; and Director, Neonatal Brain Disorders Center, University of California, San Francisco, School of Medicine, San Francisco, California Pathophysiology of Neonatal Hypoxic-Ischemic Brain Injury; Neonatal Brain Injury
Pauline A. Filipek, MD Associate Professor of Clinical Pediatrics and Neurology, University of California, Irvine, School of Medicine, Irvine; Director, For OC Kids, University Children’s Hospital at UCI Medical Center, Orange, California Autistic Spectrum Disorders
Yitzchak Frank, MD Professor of Clinical Neurology and Pediatrics, Mount Sinai School of Medicine; Adjunct Professor of Neurology, New York University School of Medicine; Pediatric Neurologist, Mount Sinai Medical Center, New York, New York Neurologic Disorders Associated with Gastrointestinal Diseases, Nutritional Deficiencies, and Fluid-Electrolyte Disorders
viii
Contributors
Douglas Fredrick, MD
Alan Hill, MD, PhD
Associate Professor of Clinical Ophthalmology and Pediatrics, University of California, San Francisco, School of Medicine; Director of Pediatric Ophthalmology, University of California, San Francisco, Medical Center, San Francisco, California Vision Loss
Professor, Department of Pediatrics, Division of Neurology, University of British Columbia Faculty of Medicine; Division of Neurology, British Columbia Children’s Hospital, Vancouver, British Columbia, Canada Hypoxic-Ischemic Cerebral Injury in the Newborn
Hudson H. Freeze, PhD
Deborah G. Hirtz, MD
Adjunct Professor of Medicine, University of California, San Diego, School of Medicine; Professor and Director, Glycobiology and Carbohydrate Chemistry Program, The Burnham Institute, La Jolla, California Disorders of Glycosylation
Program Director, Clinical Trials, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland Autistic Spectrum Disorders
Bhuwan P. Garg, MB, BS
Professor of Medicine (Neurology) and Pediatrics, Dartmouth Medical School, Hanover; Chief, Section of Neurology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire Generalized Seizures
Professor of Neurology, Indiana University School of Medicine; Department of Child Neurology, James Whitcomb Riley Hospital for Children, Indianapolis, Indiana Disorders of Micturition and Defecation; Poisoning and DrugInduced Neurologic Diseases
Elizabeth E. Gilles, MD Assistant Professor of Pediatrics and Neurology, University of Minnesota Medical School, Minneapolis; Staff Child Neurologist, Gillette Children’s Specialty Healthcare, St. Paul, Minnesota Inflicted Childhood Neurotrauma
Christopher C. Giza, MD Assistant Professor, Divisions of Neurosurgery and Pediatric Neurology, David Geffen School of Medicine at UCLA, Los Angeles, California Traumatic Brain Injury in Children
Carol A. Glaser, DVM, MD Associate Clinical Professor of Pediatrics, University of California, San Francisco, School of Medicine, San Francisco; Chief, Viral and Rickettsial Disease Laboratory, California Department of Health Services, Richmond, California Fungal, Rickettsial, and Parasitic Diseases of the Nervous System
Joseph G. Gleeson, MD Associate Professor of Neurosciences, University of California, San Diego, School of Medicine, La Jolla; Attending Physician, Children’s Hospital and Health Center, San Diego, California Congenital Structural Defects
Meredith Rose Golomb, MD, MSc
Gregory L. Holmes, MD
Barbara A. Holshouser, PhD Associate Professor of Radiology, Loma Linda University School of Medicine; Medical Physicist, Department of Radiology, Loma Linda University Medical Center, Loma Linda, California Pediatric Neuroimaging
Susan T. Iannaccone, MD Jimmy and Elizabeth Wescott Distinguished Chair in Pediatric Neurology and Professor of Neurology and Pediatrics, University of Texas Southwestern Medical Center at Dallas; Director of Child Neurology, Children’s Medical Center; Director of Neuromuscular Disease and Neurorehabilitation, Texas Scottish Rite Hospital for Children, Dallas, Texas Anterior Horn Cell and Cranial Motor Neuron Disease
Rebecca N. Ichord, MD Assistant Professor, Departments of Neurology and Pediatrics, University of Pennsylvania School of Medicine; Attending Physician, Department of Neurology, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania Perinatal Metabolic Encephalopathies
Edward M. Kaye, MD Consulting Neurologist, Children’s Hospital Boston, Boston; Vice President for Clinical Research, Genzyme Corporation, Cambridge, Massachusetts Disorders Primarily of White Matter
Assistant Professor, Indiana University School of Medicine; Attending Physician, Riley Hospital for Children, Indianapolis, Indiana Neonatal Brain Injury
John T. Kissel, MD
Cecil D. Hahn, MD, MPH
Ophir Klein, MD, PhD
Instructor, Department of Neurology, Harvard Medical School; Staff Physician, Department of Neurology, Children’s Hospital Boston, Boston, Massachusetts Neurologic Disorders Associated with Cardiac Disease
Clinical Fellow, Division of Genetics, Department of Pediatrics, University of California, San Francisco, School of Medicine, San Francisco, California Aminoacidemias and Organic Acidemias
Chellamani Harini, MD
Edwin H. Kolodny, MD
Fellow in Epilepsy and Clinical Neurophysiology, Children’s Hospital Boston, Boston, Massachusetts Spinal Cord Injury
Bernard A. and Charlotte Marden Professor and Chairman, Department of Neurology, New York University School of Medicine; Director, Department of Neurology, New York Medical Center, New York, New York Lysosomal Storage Diseases
Professor and Interim Chair, Department of Neurology, The Ohio State University, Columbus, Ohio Inflammatory Myopathies
Contributors
Bruce R. Korf, MD, PhD
David E. Mandelbaum, MD, PhD
Wayne H. and Sara Crews Finley Professor of Medical Genetics and Chair, Department of Genetics, University of Alabama at Birmingham School of Medicine, Birmingham, Alabama Chromosomes and Chromosomal Abnormalities; Phakomatoses and Allied Conditions
Professor of Clinical Neurosciences and Pediatrics, Brown Medical School; Director, Division of Child Neurology, Rhode Island and Hasbro Children’s Hospitals, Providence, Rhode Island Attention-Deficit–Hyperactivity Disorder
Suresh Kotagal, MD
Stephen M. Maricich, PhD, MD
Professor, Department of Neurology, Mayo Clinic College of Medicine; Chair, Division of Child Neurology, and Consultant, Department of Child Neurology, Mayo Clinic, Rochester, Minnesota Sleep-Wake Disorders; Increased Intracranial Pressure
Fellow, Baylor College of Medicine; Fellow, Texas Children’s Hospital, Houston, Texas The Cerebellum and the Hereditary Ataxias
Robert L. Kriel, MD Professor, Departments of Neurology, Pediatrics, and College of Pharmacy, University of Minnesota Medical School; Pediatric Neurologist, Hennepin County Medical Center, Minneapolis, Minnesota Antiepileptic Drug Therapy in Children
Steven M. Leber, MD, PhD Professor of Pediatrics and Neurology, University of Michigan Medical School and C. S. Mott Children’s Hospital, Ann Arbor, Michigan The Internet and Its Resources for the Child Neurologist
Melissa Lee, MD Assistant Professor, Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Baltimore, Maryland Neuropsychopharmacology
Robert T. Leshner, MD Professor of Neurology and Pediatrics, George Washington University School of Medicine and Health Sciences; Attending Neurologist, Center for Genetic Medicine, Department of Neurology, Children’s National Medical Center, Washington, DC Muscular Dystrophies
Donald W. Lewis, MD Professor of Pediatrics and Neurology, Eastern Virginia Medical School; Pediatric Neurologist, Children’s Hospital of the King’s Daughters, Norfolk, Virginia Headaches in Infants and Children
Paul F. Lewis, MD Associate Professor of Pediatrics, Oregon Health and Science University; Public Health Physician, Acute and Communicable Disease Program, Oregon Department of Human Services, Portland, Oregon Fungal, Rickettsial, and Parasitic Diseases of the Nervous System
Uta Lichter-Konecki, MD, PhD Assistant Professor of Pediatrics, George Washington University School of Medicine and Health Sciences; Assistant Professor of Pediatrics, Children’s Research Institute, Children’s National Medical Center, Washington, DC Inborn Errors of Urea Synthesis
Kenneth J. Mack, MD, PhD Associate Professor of Neurology, Mayo Clinic, Rochester, Minnesota The Internet and Its Resources for the Child Neurologist
ix
Christopher J. Mathias, DPhil, DSc Professor of Neurovascular Medicine, National Hospital for Neurology and Neurosurgery, University College London; Professor of Neurovascular Medicine, Imperial College London at St. Mary’s Hospital, London, United Kingdom Disorders of the Autonomic Nervous System: Autonomic Dysfunction in Pediatric Practice
Claire McLean, MD Assistant Professor of Pediatrics, Keck School of Medicine of University of Southern California; Attending Physician, Children’s Hospital of Los Angeles, Los Angeles, California Pathophysiology of Neonatal Hypoxic-Ischemic Brain Injury
Julie A. Mennella, PhD Member and Director of Education Outreach, Monell Chemical Senses Center, Philadelphia, Pennsylvania Taste and Smell
Laura R. Ment, MD Professor, Departments of Pediatrics and Neurology, Yale University School of Medicine; Attending Physician, Yale–New Haven Hospital, New Haven, Connecticut Intraventricular Hemorrhage of the Preterm Neonate
David J. Michelson, MD Assistant Professor of Child Neurology, Loma Linda University School of Medicine, Loma Linda, California Spinal Fluid Examination; Cognitive and Motor Regression
Jonathan W. Mink, MD, PhD Associate Professor of Neurology, Neurobiology and Anatomy, and Pediatrics, University of Rochester Medical Center School of Medicine and Dentistry; Chief, Child Neurology, Golisano Children’s Hospital at Strong Memorial Hospital, Rochester, New York Movement Disorders
Wendy G. Mitchell, MD Professor of Neurology and Pediatrics, Keck School of Medicine of the University of Southern California; Director, Child Neurology Training Program, Children’s Hospital of Los Angeles, Los Angeles, California Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy
Eli M. Mizrahi, MD Head, Peter Kellaway Section of Neurophysiology; Vice-Chairman, Department of Neurology; and Professor of Neurology and Pediatrics, Baylor College of Medicine; Chief, Neurophysiology Service, Methodist Hospital and St. Luke’s Episcopal Hospital; Chief, Clinical Neurophysiology Laboratory Services, Texas Children’s Hospital, Houston, Texas Neonatal Seizures
x
Contributors
Lawrence D. Morton, MD
Marc C. Patterson, MD
Associate Professor of Neurology and Pediatrics, Medical College of Virginia Campus of Virginia Commonwealth University School of Medicine; Director, Clinical Neurophysiology, Virginia Commonwealth University Health Systems, Richmond, Virginia Status Epilepticus
Professor and Head, Division of Pediatric Neurology, Departments of Neurology and Pediatrics, Columbia University College of Physicians and Surgeons; Director of Pediatric Neurology, Morgan Stanley Children’s Hospital of New York–Presbyterian, New York, New York Diseases Associated with Primary Abnormalities in Carbohydrate Metabolism; Disorders of Glycosylation
Hugo W. Moser, MD Professor, Departments of Neurology and Pediatrics, Johns Hopkins University School of Medicine; Director, Neurogenetics Research Center, Kennedy Krieger Institute, Baltimore, Maryland Peroxisomal Disorders
Richard T. Moxley III, MD Professor of Neurology and Pediatrics, University of Rochester Medical Center School of Medicine and Dentistry; Director, Neuromuscular Disease Center, University of Rochester Medical Center, Rochester, New York Chanellopathies: Myotonic Disorders and Periodic Paralysis
SakkuBai Naidu, MD Professor, Department of Neurology, Johns Hopkins University School of Medicine; Director, Neurogenetics Unit, Kennedy Krieger Institute, Baltimore, Maryland Peroxisomal Disorders
Ruth Nass, MD Professor of Clinical Neurology, New York University School of Medicine, New York, New York Developmental Language Disorders
Douglas R. Nordli, Jr., MD Associate Professor of Pediatrics and Neurology, Feinberg School of Medicine, Northwestern University; Lorna S. and James P. Langdon Chair of Pediatric Epilepsy, Children’s Memorial Hospital, Chicago, Illinois Focal and Multifocal Seizures
Robert Ouvrier, MD Petre Foundation Professor of Paediatric Neurology, Department of Paediatrics, University of Sydney, Sydney; Attending Physician, Children’s Hospital at Westmead, Westmead, New South Wales, Australia Peripheral Neuropathies
Seymour Packman, MD Professor, Department of Pediatrics, and Director, Biochemical Genetics Service and Neurometabolic Program and Clinics, University of California, San Francisco, School of Medicine, San Francisco, California Aminoacidemias and Organic Acidemias
John Colin Partridge, MD, MPH Clinical Professor, Department of Pediatrics, University of California, San Francisco, School of Medicine; Attending Neonatologist, University of California, San Francisco, Medical Center and San Francisco General Hospital, San Francisco, California Pain Management and Palliative Care
John M. Pellock, MD Professor and Chairman, Division of Child Neurology, and Vice Chairman, Department of Neurology, Medical College of Virginia Campus of Virginia Commonwealth University School of Medicine, Richmond, Virginia Status Epilepticus
Ronald M. Perkin, MD, MA Professor and Chairman, Department of Pediatrics, Brody School of Medicine at East Carolina University; Medical Director, Children’s Hospital of Eastern North Carolina; Chief of Pediatrics, Pitt County Memorial Hospital, Greenville, North Carolina Hypoxic-Ischemic Encephalopathy in Infants and Older Children
Lauren Plawner, MD Assistant Clinical Professor, Departments of Pediatrics and Neurology, University of California, San Francisco, School of Medicine; Pediatric Neurologist, Department of Pediatrics, Kaiser Permanente Medical Center, San Francisco, California Congenital Structural Defects
Isabelle Rapin, MD Professor of Neurology and Pediatrics, Albert Einstein College of Medicine; Attending Neurologist and Child Neurologist, Jacobi Medical Center and Montefiore Medical Center, Bronx, New York Hearing Impairment
Gerald V. Raymond, MD Associate Professor, Department of Neurology, Johns Hopkins University School of Medicine; Neurologist, Neurogenetics Research Center, Kennedy Krieger Institute, Baltimore, Maryland Peroxisomal Disorders
Jong M. Rho, MD Associate Professor of Clinical Neurology, University of Arizona College of Medicine, Tucson; Associate Director of Child Neurology, Children’s Health Center, St. Joseph’s Hospital and Medical Center, Phoenix; Director of Pediatric Epilepsy Research, Barrow Neurological Institute, Phoenix, Arizona Neurophysiology of Epilepsy
Sarah M. Roddy, MD Associate Professor of Pediatrics and Neurology, Loma Linda University School of Medicine; Attending Physician, Loma Linda University Children’s Hospital, Loma Linda, California Breath-Holding Spells and Reflex Anoxic Seizures
Stephen M. Rosenthal, MD Professor of Pediatrics, University of California, San Francisco, School of Medicine, San Francisco, California Endocrine Disorders of the Hypothalamus and Pituitary
Gregory M. Pastores, MD
N. Paul Rosman, MD
Associate Professor of Neurology and Pediatrics, New York University School of Medicine; Director, Neurogenetics Laboratory, New York University Medical Center, New York, New York Lysosomal Storage Diseases
Professor of Pediatrics and Neurology, Boston University School of Medicine; Pediatric Neurologist, Boston Medical Center, Boston, Massachusetts Spinal Cord Injury
Contributors
Robert S. Rust, MD, MA
Elliott H. Sherr, MD, PhD
Worrell Professor of Epileptology and Neurology and Professor of Pediatrics, University of Virginia School of Medicine, Charlottesville, Virginia Interrelationships between Renal and Neurologic Diseases and Therapies
Assistant Professor of Neurology, University of California, San Francisco, School of Medicine; Attending Physician, UCSF Children’s Hospital, San Francisco, California Mental Retardation and Global Developmental Delay
Terence D. Sanger, MD, PhD Assistant Professor, Stanford University School of Medicine; Division of Child Neurology, Lucile Packard Children’s Hospital, Stanford, California Movement Disorders
Professor, Departments of Neurology/Neurosurgery and Pediatrics, McGill University Faculty of Medicine; Division of Pediatric Neurology, Montreal Children’s Hospital–McGill University Health Centre, Montreal, Quebec, Canada Mental Retardation and Global Developmental Delay
Urs B. Schaad, MD
Shlomo Shinnar, MD, PhD
Professor of Pediatrics, University of Basel; Medical Director and Chairman, Department of Pediatrics, University Children’s Hospital, Basel, Switzerland Bacterial Infections of the Nervous System
Professor of Neurology and Pediatrics and Hyman Climenko Professor of Neuroscience Research, Albert Einstein College of Medicine; Director, Comprehensive Epilepsy Management Center, Montefiore Medical Center, Bronx, New York Febrile Seizures
Ingrid E. Scheffer, MBBS, PhD
Michael I. Shevell, MD
Professor, Department of Medicine and Paediatrics, University of Melbourne, Melbourne; Paediatric Neurologist, Austin Health, Heidelberg; Paediatric Neurologist, Monash Medical Centre, Clayton, Victoria, Australia Genetics of Epilepsy
Stanford K. Shu, MD
Mark S. Scher, MD
Professor of Pediatrics and Neurology, University of Michigan Medical School, Ann Arbor, Michigan Pathophysiology of Neonatal Hypoxic-Ischemic Brain Injury
Professor of Pediatrics, Case Western Reserve University School of Medicine; Division Chief, Pediatric Neurology, and Director of Pediatric Sleep/Epilepsy and Fetal Neonatal Neurology Programs, Rainbow Babies and Children’s Hospital and University Hospitals of Cleveland, Cleveland, Ohio Pediatric Neurophysiologic Evaluation
Nina Felice Schor, MD, PhD Professor of Pediatrics, Neurology, and Pharmacology; Chief, Division of Child Neurology; Associate Dean for Medical Student Research, University of Pittsburgh School of Medicine; Carol Ann Craumer Chair of Pediatric Research and Director, Pediatric Center for Neuroscience, Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania Neurologic Manifestations of Rheumatic Disorders of Childhood
Frederick L. Schuster, PhD Viral and Rickettsial Disease Laboratory, California Department of Health Services, Richmond, California Fungal, Rickettsial, and Parasitic Diseases of the Nervous System
Bennett A. Shaywitz, MD Professor of Pediatrics and Neurology, Yale University School of Medicine, New Haven, Connecticut Dyslexia
Sally E. Shaywitz, MD Professor of Pediatrics, Yale University School of Medicine, New Haven, Connecticut Dyslexia
Robert Sheets, MD Assistant Clinical Professor of Pediatrics, University of California, San Diego, School of Medicine, La Jolla; Pediatric Rheumatologist, Children’s Hospital of San Diego, San Diego, California Neurologic Manifestations of Rheumatic Disorders of Childhood
xi
Assistant Professor of Child Neurology, Loma Linda University School of Medicine, Loma Linda, California Cognitive and Motor Regression
Faye S. Silverstein, MD
Harvey S. Singer, MD Haller Professor of Pediatric Neurology, Johns Hopkins University School of Medicine; Director, Child Neurology, Johns Hopkins Hospital, Baltimore, Maryland Tourette Syndrome and Its Associated Neurobehavioral Problems
John T. Sladky, MD Professor of Pediatrics and Neurology, Emory University School of Medicine; Division Chief, Child Neurology, Children’s Healthcare of Atlanta; Division Chief, Child Neurology, Grady Health System, Atlanta, Georgia Inflammatory Neuropathies
Stephen A. Smith, MD Director, Neuromuscular Laboratory, Department of Pathology, Hennepin County Medical Center, Minneapolis, Minnesota; Director, Neuromuscular Program, Department of Neurology, Gillette Children’s Specialty Healthcare, St. Paul, Minnesota; Director, Neuromuscular Laboratory, Department of Pathology, Parkview Hospital, Pueblo, Colorado Peripheral Neuropathies
Carl E. Stafstrom, MD, PhD Professor of Neurology and Pediatrics, University of Wisconsin Medical School; Chief, Section of Pediatric Neurology, University of Wisconsin Hospital, Madison, Wisconsin Neurophysiology of Epilepsy
Jonathan B. Strober, MD Assistant Clinical Professor of Neurology and Pediatrics, University of California, San Francisco, School of Medicine, San Francisco, California Congenital Myopathies
xii
Contributors
Kenneth F. Swaiman, MD
Ann H. Tilton, MD
Director Emeritus, Division of Pediatric Neurology, and Professor Emeritus of Neurology and Pediatrics, University of Minnesota Medical School, Minneapolis, Minnesota General Aspects of the Patient’s Neurologic History; Neurologic Examination of the Older Child; Neurologic Examination after the Newborn Period until 2 Years of Age; Neurologic Examination of the Term and Preterm Infant; Muscular Tone and Gait Disturbances; Cerebral Palsy; Diseases Associated with Primary Abnormalities in Carbohydrate Metabolism
Professor and Section Chair of Child Neurology, Louisiana State University Health Sciences Center; Co-Director of Rehabilitation, Child Neurology, Children’s Hospital of New Orleans, New Orleans, Louisiana Pediatric Neurorehabilitation Medicine
Kathryn J. Swoboda, MD Associate Professor of Neurology and Adjunct Associate Professor of Pediatrics, University of Utah School of Medicine, Salt Lake City, Utah Diagnosis and Treatment of Neurotransmitter-Related Disorders
Ilona S. Szer, MD Professor of Clinical Pediatrics, University of California, San Diego, School of Medicine, La Jolla; Director, Pediatric Rheumatology, Children’s Hospital of San Diego, San Diego, California Neurologic Manifestations of Rheumatic Disorders of Childhood
Martin G. Täuber, MD Professor and Co-Director, Institute for Infectious Diseases, University of Bern; Director, Clinic and Policlinic for Infectious Diseases, University Hospital Insel, Bern, Switzerland Bacterial Infections of the Nervous System
Rabi Tawil, MD Associate Professor of Neurology, Pathology, and Laboratory Medicine, University of Rochester Medical Center School of Medicine and Dentistry; Co-Director; Neuromuscular Disease Clinic, University of Rochester Medical Center, Rochester, New York Chanellopathies: Myotonic Disorders and Periodic Paralysis
Donald A. Taylor, MD Director of Pediatric Clinical Neurophysiology, St. Mary’s Hospital, Richmond, Virginia Impairment of Consciousness and Coma
Ingrid Tein, MD, BSc Associate Professor of Pediatrics, Laboratory Medicine, and Pathobiology, University of Toronto Faculty of Medicine; Director, Neurometabolic Clinic and Research Laboratory, and Senior Scientist, The Research Institute, The Hospital for Sick Children, Toronto, Ontario, Canada Metabolic Myopathies
Elizabeth A. Thiele, MD, PhD Associate Professor of Neurology, Harvard Medical School; Director, Carol and James Herscot Center for Tuberous Sclerosis Complex, Massachusetts General Hospital, Boston, Massachusetts Phakomatoses and Allied Conditions
Joseph R. Thompson, MD Professor of Radiology, Loma Linda University School of Medicine; Pediatric Neuroradiologist, Department of Radiology, Loma Linda University Medical Center, Loma Linda, California Pediatric Neuroimaging
Doris A. Trauner, MD Professor and Chief of Pediatric Neurology, University of California, San Diego, School of Medicine, La Jolla, California Developmental Language Disorders
Mendel Tuchman, MD Professor of Pediatrics, Biochemistry, and Molecular Biology, George Washington University School of Medicine and Health Sciences; Vice Chair for Research and Scientific Director, Children’s Research Institute, Children’s National Medical Center, Washington, DC Inborn Errors of Urea Synthesis
Roberto Tuchman, MD Associate Professor of Neurology, University of Miami Miller School of Medicine, Miami; Director, Developmental and Behavioral Neurology, Miami Children’s Hospital Dan Marino Center, Weston, Florida Epileptiform Disorders with Cognitive Systems
Marjo S. van der Knaap, MD, PhD Professor of Child Neurology, University Medical Center, Amsterdam, The Netherlands Disorders Primarily of White Matter
Michèle Van Hirtum-Das, MD Resident, Child Neurology, Children’s Hospital of Los Angeles, Los Angeles, California Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy
V. Venkataraman Vedanarayanan, MD Professor of Neurology and Professor of Pediatrics, University of Mississippi School of Medicine; Attending Physician, University of Mississippi Medical Center, Jackson, Mississippi Normal Muscle
Ann Wagner, PhD Chief, Neurodevelopmental Disorders Branch, Division of Pediatric Translational Research and Treatment Development, National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland Autistic Spectrum Disorders
John T. Walkup, MD Associate Professor, Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine; Deputy Director, Division of Child and Adolescent Psychiatry, Johns Hopkins Hospital, Baltimore, Maryland Neuropsychopharmacology
Laurence E. Walsh, MD Assistant Professor of Clinical Neurology and Medical and Molecular Genetics, Indiana University School of Medicine; Director, Section of Child Neurology, James Whitcomb Riley Hospital for Children, Indianapolis, Indiana Poisoning and Drug-Induced Neurologic Diseases
Contributors
xiii
Maria B. Weimer, MD
Nathaniel D. Wycliffe, MD
Assistant Professor of Clinical Neurology, Louisiana State University Health Sciences Center; Staff Child Neurologist, Children’s Hospital, New Orleans, Louisiana Pediatric Neurorehabilitation Medicine
Assistant Professor of Radiology, Loma Linda University School of Medicine; Neuroradiologist and Director of Head and Neck Radiology, Department of Radiology, Loma Linda University Medical Center, Loma Linda, California Pediatric Neuroimaging
James W. Wheless, MD Professor of Neurology and Pediatrics and Director, Texas Comprehensive Epilepsy Program, University of Texas Health Science Center at Houston–Medical School; Director, Epilepsy Monitoring Unit, and Director, EEG and Clinical Neurophysiology, Memorial Hermann and Memorial Hermann Children’s Hospitals, Houston, Texas The Ketogenic Diet
Huda Y. Zoghbi, MD
Gil I. Wolfe, MD
Duke University Medical Center, Durham, North Carolina Degenerative Diseases Primarily of Gray Matter
Dr. Bob and Jean Smith Foundation Distinguished Chair in Neuromuscular Disease Research and Associate Professor, Department of Neurology, University of Texas Southwestern Medical Center, Dallas, Texas Diseases of the Neuromuscular Junction
Yvonne Wu, MD, MPH Assistant Professor, Departments of Neurology and Pediatrics, University of California, San Francisco, School of Medicine, San Francisco, California Cerebral Palsy
Professor of Pediatrics, Molecular and Human Genetics, Neurology, and Neuroscience, Baylor College of Medicine; Investigator, Howard Hughes Medical Institute, Houston, Texas The Cerebellum and the Hereditary Ataxias
Adam Zucker, MD
Mary L. Zupanc, MD Professor, Departments of Neurology and Pediatrics, Medical College of Wisconsin; Director Comprehensive Epilepsy Center, Children’s Hospital of Wisconsin, Milwaukee, Wisconsin Epilepsy Surgery in the Pediatric Population
PREFACE TO THE FOURTH EDITION
S
ince publication in 1999 of the third edition of Pediatric Neurology: Principles & Practice, the discipline of child neurology has progressed and reached new levels of complexity. Advances in molecular biology and neuroimaging have fueled an explosion of knowledge that has translated into a richer understanding of nervous system development and function. Researchers and clinicians alike believe that, during the next decade, novel and targeted treatments will be the product of such fundamental advances in knowledge. Successful treatment of children with both common and rare neurologic disorders will be a reality. This fourth edition reflects the enormous growth and intricacy of the basic and clinical neurosciences. The entire text has been revised and reorganized. There are many new chapters that reflect areas of child neurology that are becoming increasingly relevant clinically (e.g., neurogenetics, neuropsychopharmacology, neurorehabilitation, ethics), as well as new chapters on diseases that were previously unrecognized (e.g., PNTD, CDG). Many chapters have new authors who bring to these discussions new insights into disease mechanisms. Also, the two senior editors are extremely fortunate to have Donna M. Ferriero join us to provide her expertise to ensure maintenance of the quality of this publication. The two volumes are divided into 16 parts, encompassing 95 chapters as outlined in the table of contents. Parts I and II contain information regarding selected aspects of the pediatric neurologic examination in a general sense, as well as the different motor and sensory systems, and these discussions are followed by a comprehensive review of the pertinent neurodiagnostic testing procedures and their clinical application. Part III covers important aspects of neonatal neurology and the long-term sequelae of acquired and developmental abnormalities that can result in chronic disorders, such as cerebral palsy, developmental delay, and epilepsy. Part IV documents the vast array of genetic and neurometabolic disorders that occur in infants and children; this section also provides many of the fundamental concepts of molecular biology and neurochemistry that constitute the scientific basis of these diseases. Part V describes the major neurobehavioral disorders of childhood and includes chapters on autism and the neuropsychiatric problems that accompany Tourette syndrome and a new chapter on neuropsychopharmacology. Part VI focuses on pediatric epilepsy and contains new chapters on the neurophysiology and neurogenetics of pediatric epilepsy. Also included are chapters on the various types of pediatric epilepsy, epileptiform disorders with cognitive symptomatology, the ketogenic diet, surgical treatment, and the learning and behavioral problems associated with epilepsy.
The second volume encompasses many of the serious and complex central and peripheral nervous system diseases that confront child neurologists and allied health professionals. Part VII reviews the nonepileptiform paroxysmal disorders, including headache, syncope, and sleep disorders. Parts VIII and IX deal with conditions that are degenerative in nature and cause severe loss of motor and mental function. These conditions include gray and white matter diseases that can cause ataxia, movement disorders, progressive spasticity, and dementia. Part X contains chapters on traumatic and nontraumatic brain injury in infants and older children. Because neurologists are frequently asked to provide consultation for many of these conditions, chapters on disorders of consciousness, nonaccidental trauma, anoxic brain injury, and traumatic brain and spinal cord injury are included, as well as a current review of the issues related to brain death determination. Parts XI (infection) and XII (tumors and cerebrovascular and vasculitic diseases) extensively cover the major diseases that directly or indirectly cause serious neurologic symptoms and are presented primarily from a clinical perspective. The neuromuscular diseases are reviewed in Part XIII, which contains chapters on the classic neuromuscular disorders including the anterior horn cell diseases, disorders of the peripheral nervous system, neuromuscular junction, inflammatory neuropathies, metabolic myopathies, and channelopathies. Parts XIV and XV include important chapters that review many pediatric systemic (e.g., endocrine, renal, cardiac, gastrointestinal) conditions that are known to cause neurologic symptoms, as well as chapters on poisonings, complications of immunizations, and autonomic nervous system disorders. This volume concludes with Part XVI, which has been revised extensively and includes new and revised chapters on pediatric neurorehabilitation, pain and palliative care management, ethical issues in child neurology, and an update on the Internet as it relates to child neurology. We hope that the reader will find this book a useful resource and that the information will benefit the many children who suffer from these conditions. It is our wish that the greater world community will increase support for the care of neurologically impaired children and the research necessary to provide further understanding of neurologic diseases. This support is necessary to facilitate discovery of new therapies that will improve the survival and quality of life of these unfortunate and brave children. Kenneth F. Swaiman Stephen Ashwal Donna M. Ferriero
PREFACE TO THE FIRST EDITION
I
t is concurrently tiring, humiliating, and intellectually revitalizing to compile a book containing the essence of the information that embraces one’s life work and professional preoccupation. For me, there is a certain mothto-the-flame phenomenon that cannot be resisted; therefore this new book has been produced. Pediatric neurology has come of age since my initial interest and subsequent immersion in the field. Concentrated attention to the details of brain development and function has brought much progress and understanding. Studies of disease processes by dedicated and intelligent individuals accompanied by a cascade of new technology (e.g., neuroimaging techniques, positron emission tomography, DNA probes, synthesis of gene products, sophisticated lipid chemistry) have propelled the field forward. The simultaneous increase of knowledge and capability of pediatric neurologists and others who diagnose and treat children with nervous system dysfunction has been extremely gratifying. Although once within the realm of honest delusion of a seemingly sane (but unrealistic) devotee of the field, it is no longer possible to believe that a single individual can fathom, much less explore, the innumerable rivulets that coalesce to form the river of knowledge that currently is pediatric neurology. Streams of information in certain areas sometimes peacefully meander for years; suddenly, when knowledge of previously obscure areas is advanced and the newly gained information becomes central to understanding basic pathophysiologic entities, a once small stream gains momentum and abruptly flows with torrential force.
This text is an attempt to gather the most important aspects of current pediatric neurology and display them in a comprehensible manner. The task, although consuming great energies and concentration, cannot be accomplished completely because new conditions are described daily. The advancement of the field necessitated that preparation of this text keep pace with current knowledge and present new and valuable techniques. My colleagues and I have made every effort to discharge this responsibility. Because of continuous scientific progress, controversies are extant in some areas for varying periods; wherever possible, these areas of conflict are indicated. This book is divided into four unequal parts. Part I contains a discussion of the historic and clinical examination. Part II contains information concerning laboratory examination. Chapters relating to the symptom complexes that often reflect the chief complaints of neurologically impaired children compose Part III. Part IV provides detailed discussion of various neurologic diseases that afflict children. Although every precaution has been taken to avoid error, bias, and prejudice, inevitably some of these demons have become embedded in the text. The editor assumes full responsibility for these indiscretions. It is my fervent hope that the reader will find this book informative and stimulating and that the contents will provide an introduction to the understanding of many of the conditions that remain mysterious and poorly explained. Kenneth F. Swaiman, MD Autumn 1988
ACKNOWLEDGMENTS
W
e wish to thank Arlene Carpenter, Diana Laulainen-Schein, Ann Elliott, and Kei Kaneshiro for their time and effort, which so efficiently affected manuscript flow, editing, and preparation, as well as the innumerable other tasks necessary to complete this book. We also wish to thank the librarians at the University of Minnesota Medical School and at the Coleman and Del Webb Libraries at Loma Linda University School of Medicine for
their help, advice, and willingness at any time to obtain information that we required. In addition, we wish to thank the editorial and publishing staff at Elsevier, especially Susan Pioli, Jennifer Shreiner, and Lee Ann Draud. Without their diligence, persistence, insight, and flexibility, we would have never been able to complete this project.
CHAPTER 1
General Aspects of the Patient’s Neurologic History Kenneth F. Swaiman
Modern technology does not and cannot substitute for skilled history taking. The crucial role of obtaining the patient’s neurologic history directly from the patient or a member of the patient’s family cannot be stressed enough. The history-taking procedure should elicit specific information and be directed so as to exclude or ensure inclusion of pertinent conditions in the differential diagnosis of the child’s condition. The information obtained during the history-taking session is critical during the subsequent analysis and synthesis of all patient data. The clinician should be involved in a dynamic diagnostic quest throughout the interview and during the review of previous medical and other relevant records. A systematic approach to the medical history is mandatory; however, the clinician must be alert to significant leads that may eventually prove essential to the diagnostic process. The history-taking session is not a netting operation with data to be subsequently sorted; rather, the data should be dynamically synthesized as they are collected and then used to alter the direction and depth of the questioning process. The process of identifying a differential diagnosis should begin at the outset of questioning. In a broad sense, certain umbrella categories encompass virtually all etiologic mechanisms that underlie the differential diagnosis. Inevitably, there is some overlap (e.g., vascular occlusion in MELAS, a metabolic condition; mass effect of a brain abscess, an infectious condition). The fundamental pathologic processes, simplistically identified, are infectious, traumatic, metabolic, endocrinologic, toxic (exogenous and endogenous), congenital structural malformations, vascular, neoplastic, degenerative (usually of unknown or obscure cause), and idiopathic. Each of these categories has many subsets with which the clinician who evaluates neurologic problems in children must be familiar. The likelihood that one of the broad umbrella classifications applies to the problem of the pediatric patient must be judged while the history is obtained, during which time some categories will gain in probability and some will become increasingly remote. The information gathered during the history-taking session may be vital in the process of literature and database searches that may subsequently prove necessary. The precise role of genetic determination (i.e., gene product formation and use) in all familial pathologic processes is exceedingly important now that the human genome has been mapped. Most chronic neurologic complaints are complex, and the neurologist’s involvement is often preceded by involvement of other professionals and agencies. If the parents are the primary caregivers, both the mother and father should be present if possible. When grandparents or other caregivers are involved in attending to the child, they should be present. Review of past medical and developmental histories is an essential component of a good history-taking session.
Information should be sought from records and from questioning the mother about health problems, including infertility, and diseases that occurred during pregnancy. With increasing data accumulating regarding adverse pediatric outcomes with assisted reproductive technologies [Jackson et al., 2004], it is important to ask whether conception was achieved naturally and, if not, what method of assisted reproductive technology was employed. Gestational information about infection, radiation, acute trauma, chronic illnesses such as diabetes mellitus, and toxins, including illicit drugs, tobacco, and alcohol, may prove invaluable. Further information about medications that the mother received, including over-the-counter preparations, should be probed. It is important to record the expected and actual dates of delivery. Review of birth records, including those of the mother, may reveal information concerning difficulties with pregnancy and problems in the perinatal period that are not known or remembered by the parents. Details of the intrapartum period, including associated hypertension, drugs administered, length of stages of delivery, occurrence of chorioamnionitis, and if possible, information concerning placental pathology and the general appearance of the newborn at time of birth, may prove enlightening. It is important to determine the status of the newborn infant. Information should be sought concerning Apgar scores, depression of activity, neonatal seizures, presence of hypotonia, and whether tracheal intubation and ventilatory support was needed. The patient’s caregivers should be questioned carefully about the nature and results of previously performed tests, including electrodiagnostic tests, brain-imaging studies, biochemical studies (e.g., quantitative assays of amino acids, organic acids, lactic acid, and lysosomal enzymes), biopsies, and chromosomal studies. The caregivers should also be asked about whether medication or other treatment has been administered or advised and about the result of such therapies. The primary problem of the child is embodied in the chief complaint. A combination of chief complaints may prove more specific and narrows the diagnostic spectrum (e.g., a 6-month-old male with delayed development and cataracts). The differential diagnosis initially is based on the chief complaint, which should therefore be documented as accurately as possible. The caregiver’s or patient’s description should be quoted verbatim, when possible. The period of onset and whether the symptoms began acutely or gradually should be carefully determined. The clinician should not substitute medical terminology in place of the terms used by the caregivers or patient when recording the chief complaint. Medical terms must be explained fully so that responses are complete and pertinent.
4
Clinical Evaluation / 1
1. 2. 3. 4.
Is the process acute or insidious? Is it focal or generalized? Is it progressive or static? At what age did the problem begin?
The order in which disease findings develop and the precise time of onset of symptoms and signs may be critical factors in the process of accurate diagnosis. The presence of repeated episodes or associated phenomena should be determined. Detailed questions should be asked of the caregivers and child to elucidate the facts.
Neurologic impairment
Vascular conditions
the history meaningful and complete may be the seemingly trivial information that is not readily recalled or divulged. The accomplished clinician can uncover this information by directed and specific inquiry. The chief complaint should trigger the process of differential diagnosis in the examiner’s thinking, which begins as a listing of the disease conditions that could cause the chief complaint at the child’s age. The following four specific questions should be answered, if possible, in taking the history of the current illness:
Toxic conditions
1 2 3 4 5 6 7 2 3 4 2 3 4 5 6 1 2 3 4 Days Weeks Months Years
1 2 3 4 5 6 7 2 3 4 2 3 4 5 6 1 2 3 4 Days Weeks Months Years
Infectious conditions
Degenerative and neoplastic conditions
Neurologic impairment
Neurologic impairment
Neurologic impairment
Notwithstanding these goals, the actual complaint may be imprecisely described because the caregivers’ memories, language, or observations may be inaccurate and because the child may be unable to provide detailed information. The clinician should make every attempt to question the child directly. Even a preschool-aged child may provide helpful information. Sometimes, adults who participate in the session may not be objective or capable of accuracy. Most commonly however, the observations and concerns of the caregiver should be given every consideration and essence of credibility. It is extremely unwise to disregard these components of the history when comments are somewhat unusual or incompatible with the clinician’s diagnostic bias. The features associated with the chief complaint compose the history of the present illness. The questioning should provide an incisive interaction between caregiver (or patient) and clinician and should be directed at formulating the differential diagnosis. This portion of the communication process requires skill and perseverance. An all-inclusive neurologic history is impossible; however, that which makes
Neurologic impairment
1 2 3 4 5 6 7 2 3 4 2 3 4 5 6 1 2 3 4 Days Weeks Months Years
1 2 3 4 5 6 7 2 3 4 2 3 4 5 6 1 2 3 4 Days Weeks Months Years
Metabolic conditions
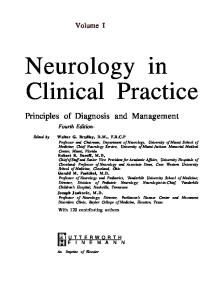
1 2 3 4 5 6 7 2 3 4 2 3 4 5 6 1 2 3 4 Days Weeks Months Years FIGURE 1-1. Patterns of onset and courses of neurologic conditions. The arrow in each graph signifies the point of clinical recognition. (Adapted from Baker AB. Outline of clinical neurology. Dubuque, Iowa: William C Brown, 1958.)
Swaiman / General Aspects of the Patient’s Neurologic History
Sequelae of traumatic events develop over a period of minutes to a day (Fig. 1-1). Although the clinical manifestations of cerebrovascular events normally develop over minutes to hours, the underlying process may be longstanding; therefore, acute onset of vascular symptoms may be the result of a subacute or chronic process. Infectious processes, electrolyte imbalances, and toxic processes (endogenous or exogenous) usually reach their zenith within a day to several days. Degenerative diseases, inborn metabolic disorders, and neoplastic conditions usually progress insidiously over weeks or months.
5
Based on the chronologic aspects of the history, the clinician should ask questions related to the most likely pathologic processes. For example, when the history suggests a subacute process, the clinician should probe for characteristics associated with an infectious process (e.g., exposure to a known infectious source, recent infection, vomiting, diarrhea, fever) or with specific toxins (e.g., overthe-counter medications, prescribed medications, insecticides, other toxins found around the home). Evaluation of whether a condition is focal or generalized is embedded in the neurologic diagnostic process. A focal
FIGURE 1-2. Denver Developmental Screening Test (Denver II) directions. (From Frankenburg WK, Dodds JB, Archer P, et al. The Denver II: A major revision and restandardization of the Denver Developmental screening test. Pediatrics 1992;89:91.)
6
Clinical Evaluation / 1
FIGURE 1-2. cont’d.
Swaiman / General Aspects of the Patient’s Neurologic History
neurologic lesion is not necessarily one that causes focal manifestations but is one that can be related to dysfunction in a circumscribed neuroanatomic location. For example, a focal lesion in the brainstem may cause ipsilateral cranial nerve and contralateral corticospinal tract involvement. If the difficulties are not focal within this definition, they usually result from a generalized process or from several lesions (i.e., multifocal). Neoplastic and vascular diseases frequently result in focal processes; occasionally, trauma results in such abnormalities. Generalized or multifocal conditions are usually associated with degenerative, congenital, metabolic, or toxic abnormalities. The clinician must always attempt to determine whether the condition is progressive or static. A detailed developmental history is often the best means of substantiating whether a condition is progressive or static. The history should include a log of motor milestones and should contain specific information regarding motor, language, and adaptive-social behavior. Questions should be crafted to obtain evidence that the child is no longer capable of motor or intellectual activities that were previously performed. This information is essential to the diagnosis of progressive disease, which is usually preceded by a period of normal development. Occasionally, previous formal neurologic and psychometric evaluations may be available. Documentation may be forthcoming from family photographs, family video tapes, or baby books. In progressive conditions, documentation of increasing loss of normal function or an increase in any symptoms, including pain, is essential. Conditions that are static or improve spontaneously are usually the result of traumatic or anoxic episodes, congenital abnormalities, acute toxicity, or resolving infection. The Denver Developmental Screening Test (DDST) [Frankenburg and Dodds, 1967], the revised form [Frankenburg et al., 1981], the Denver II screening test (Fig. 1-2) [Frankenburg et al., 1992], or other developmental surveys allow a more precise approach to the determination of whether gains or losses of skills have occurred and aid in the decision about whether a process is progressive or static. The DDST has undergone a major revision and restandardization and is available as the Denver Developmental Screening Test II (DDST II, or Denver II). The DDST II has replaced the older versions of the DDST. Standardization testing for the Denver II included evaluating each item to determine if significant differences among different subpopulations existed. These subpopulations included gender, ethnic group (i.e., black, white, or Hispanic), maternal education (i.e., less than 12 grades completed or more than 12 grades completed), and place of residence (i.e., rural, semirural, or urban). The Denver II differs from the DDST in the selected items, test form, and interpretation. The total number of items has been increased from 105 to 125, and items that were judged as difficult to administer or interpret have been modified or eliminated. Most of the new items are in the language section. The technical manual should be consulted if a delay is identified because it may be caused by sociocultural differences. The DDST II has been modified for use in different language and cultural norms [Lejarraga et al., 2002; Lim et al., 1996]. The test form for the Denver II resembles the DDST in the vertical placement of items. Key Denver items have been
7
eliminated so that the age scale coincides with the American Academy of Pediatrics’ suggested schedule for health maintenance examinations to facilitate use of the Denver II during these visits. The norms for the distribution bars are in accordance with the new standardization data. A valuable addition to the front of the form is a checklist for documentation of the child’s behavior during testing. Scoring and interpretation changes have also been made. If a child is able to perform an item depicted to the right of the age line, the performance is designated as advanced. If a child fails or refuses an item that is depicted completely to the right of the age line, the score for the item is deemed normal. If the child passes, fails, or refuses an item on which the age line falls between the 25th and 75th percentile lines, performance is designated as normal. If the child refuses or fails an item on which the age line falls on or between the 75th and 90th percentile lines, performance is designated as a caution. If the child is unable to pass an item depicted entirely to the left of the age line, performance is designated as a delay. Sufficient items should be administered to establish basal and ceiling levels in each sector. To screen only for developmental delays, only items located completely to the left of the child’s age line should be administered. Retesting is recommended after 1 to 3 months for performance scored as a caution. Retesting for one or more delays, as well as refusals, should be performed within 2 weeks. It is essential that examiners, caregivers, and educational personnel recognize that the Denver II provides an evaluation of the child’s current developmental level and is not a predictor of the future rate of development or eventual maximum attainment. The test may be used for early identification of neurologic deficits [Hallioglu et al., 2001]. Abnormalities in more complex and abstract functioning may not be recognizable until a later age and will require more sophisticated testing vehicles. Alteration in the child’s biologic or environmental status may affect developmental rate and achievement and should be investigated and taken into account in the evaluation if appropriate. The clinician should ask specific questions regarding the age of attainment of developmental landmarks and should make every attempt to discern whether the child is delayed in many areas of development or has developed normally in some areas but not in others. Children who have normal motor development but also have hearing impairment may have delayed speech. However, the presence of neuromuscular disease may cause obvious retardation of motor development but may allow normal development of social and language skills. A specific form may be used by the examiner as a guideline to the history-taking procedure (Fig. 1-3). There are many systems for recording history and the subsequent examination. The form printed in this chapter may be modified to the specific needs of the patient and the clinician. The question of hyperactivity is often at the core of the caregiver’s complaint. A rating scale may be completed by teachers to aid the clinician in diagnosis (Fig. 1-4) [Connors, 1969]. The problem is discussed in more detail in Chapter 36. School behavior can also be assessed by caregivers, as shown in Box 1-1. Many children are involved in some planned day activity, day care, or school program after the age of 2 or 3 years. text continues on page 15
8
Clinical Evaluation / 1
GENERAL HISTORY FORM PREGNANCY Gestation data Birth date Expected date Birth weight Birth occipitofrontal circumference (from old records)
Medication taken by mother (check each one taken) Vitamins Iron Calcium Hormones Weight reduction medication Diuretics Contraceptives Sedatives, tranquilizers Antiepileptics Other Illnesses (record month of pregnancy in which illness occurred) Colds, flu, etc. Kidney, bladder infection Rubella (German measles) Rashes Other infectious diseases Exposures to infectious diseases Diabetes Kidney disease Surgery Radiographs Other (explain) Labor and delivery Breech or unusual presentation Forceps use Delay in respiration or cry (Apgar scores if available) Was oxygen administration necessary? Type of anesthesia employed for mother
Newborn period Jaundice Cyanosis Infection Seizures Anemia Other Medications administered Home from hospital in
days
DEVELOPMENT (indicate month skill attained) Smiled Laughed out loud First words Put words together (e.g., “Daddy, bye-bye”) Complete sentences Rolled over Sat without support Crawled Pulled to standing Walked around furniture Walked unassisted Rode tricycle ILLNESSES
Hospitalizations Age:
Reason:
Age:
Reason:
Age:
Reason:
Operations Age:
Reason:
Age:
Reason:
Injuries Age:
Reason:
Age:
Reason:
FIGURE 1-3. The general history form can be used for obtaining the medical history, developmental history, and family history of children with neurologic problems. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
Swaiman / General Aspects of the Patient’s Neurologic History
GENERAL HISTORY FORM —cont’d
Has child ever been unconscious? Age: Reason: Age:
Describe: If child has had a convulsion, describe (first event, subsequent events, duration, warning, postconvulsion behavior, etc.)
Reason:
Has child ever been poisoned? Name of poison Has child ever had an electroencephalogram (EEG)? Age: SEIZURE HISTORY
Reason:
Ages: With fever Ages: Without fever Does child daydream often?:
Results:
MEDICATION Has child ever been treated with medication other than for colds and minor infections? If yes, please give age and reason and medication Has child ever taken any of the following medications? Drug Carbamazepine (Tegretol) Clonazepam (Klonopin) Ethosuximide (Zarontin) Gabapentin (Neurontin) Lamotrigine (Lamictal) Levcetiracetem (Keppra) Oxcarbazepine (Trileptal) Phenobarbital (Luminal) Phenytoin (Dilantin) Primidone (Mysoline) Tiabagine (Gabitril) Topiramate (Topamax)
FIGURE 1-3. cont’d.
Age/duration
Indicate age and reason below. Reason
Results
9
10
Clinical Evaluation / 1
GENERAL HISTORY FORM —cont’d Drug
Age/duration
Reason
Results
Valproic acid (Depakene/Depakote) Vigabatrin Zonisamide (Zonegran) Other antiepileptic drugs Amitriptyline (Elavil) Buproprion (Wellbutrin) Chlorpromazine (Thorazine) Dextroamphetamine (Dexedrine, Adderall) Diazepam (Valium) Fluoxetine (Prozac) Haloperidol (Haldol) Imipramine (Tofranil) Methylphenidate (Ritalin, Concerta) Paroxetine (Paxil) Pemoline (Cylert) Risperidone (Risperdal) Thioridazine (Mellaril) Sertraline (Zoloft) Other psychopharmacologic drugs FAMILY HISTORY Are there family members suffering or who have suffered from: Ataxia Blindness Cerebral palsy FIGURE 1-3. cont’d.
Deafness Dementia Mental retardation
Movement disorders Seizures Weakness
Swaiman / General Aspects of the Patient’s Neurologic History
11
Teacher Questionnaire—School Behavioral Assessment Date
Pupil’s name
Teacher: Please place a checkmark in the appropriate column for each item. Choose the degree of activity that best describes the child’s behavior. Degree of activity Observation
Not at all
Rarely
Fairly often
Very often
Classroom behavior Constantly fidgets Hums and makes other odd noises Demands must be met immediately—easily frustrated Coordination poor Restless or overactive Excitable, impulsive Inattentive, easily distracted Fails to finish things started—short attention span Overly sensitive Overly serious or sad Daydreams Sullen or sulky Cries often and easily Disturbs other children Quarrelsome Mood changes quickly and drastically Obnoxious behavior Destructive Steals Lies Temper outbursts, explosive and unpredictable behavior Childish and immature Easily frustrated in efforts Difficulty in learning
FIGURE 1-4. Teacher questionnaire for behavioral assessment. (Adapted from Conners CK. A teacher rating scale for use in drug studies with children. Am J Psychiatry 1967;126:884.)
12
Clinical Evaluation / 1 Teacher Questionnaire—School Behavioral Assessment–cont’d Date
Pupil’s name
Teacher: Please place a checkmark in the appropriate column for each item. Choose the degree of activity that best describes the child’s behavior. Degree of activity Observation Group participation Isolates self from other children Seems unaccepted by group Seems easily led No sense of fair play Seems to lack leadership Does not get along with opposite sex Does not get along with same sex Teases other children or interferes with their activities Denies mistakes and blames others Attitude toward authority Submissive Defiant Impudent Shy Fearful Excessive demands for teacher’s attention Stubborn Overly anxious to please Uncooperative Attendance problem FIGURE 1-4. cont’d.
Not at all
Rarely
Fairly often
Very often
Swaiman / General Aspects of the Patient’s Neurologic History
BOX 1-1
Parents/Caretaker Questionnaire—School Behavioral Assessment Pupil’s name
Date
School performance Have teachers expressed concern about your child’s learning? Yes No If yes, please list the grade at which concern was expressed and the subject(s) of concern.
Grade
Subject(s)
Have teachers expressed concern about your child’s behavior? Yes No If yes, please list the grade at which concern was expressed and the behavior of concern.
Grade
Behavior(s)
Have teachers expressed concern about your child’s relationships with other children? If yes, please list the grade at which concern was expressed and the behavior of concern.
Grade
Yes
No
Problem
Has your child repeated any grades? Yes No If yes, what grade(s) was repeated and what reason(s) was given?
Has your child received special education services? Yes No If yes, please list the grade and type of service provided. Services in schools include: Chapter 1 or Title 1 support; Learning Disabilities; Emotional Behavioral Disorder; Physical and Other Health Impairment; Mildly Mentally Handicapped, Trainable Mentally Handicapped; Adaptive Physical Education; Speech and Language; Occupational Therapy; and Physical Therapy.
Grade
Service
Courtesy Division of Pediatric Neurology, University of Minnesota Medical School.
13
14
Clinical Evaluation / 1
SCHOOL REPORT This report is confidential and for our use only I. Identifying information Grade Name Birthdate Address School School phone School address Teacher Principal Retention II. Child’s school history (please attach a transcript of grades, results of and achievement tests, including results of IQ tests, and previous psychologic and/or speech evaluations) III. Special characteristics (check all that apply under each category) Slightly Severe Reading level Above below difficulty Average grade Intense
Average
Indifferent
Resistant
Aggressive
Average
Shy
Withdrawn
Absorbed
Attentive
Needs urging
Easily distracted
Relationship to authority figures
Too deferent
Cooperative
Sometimes rebels
Defiant
Relationship with peers
Well liked by all
Normal
one or two friends
Isolated
Achievement
“Overachiever”
Up to ability
Sporadic
Severe problems
Never misses
Normal absence
Frequent absence
Extended absence
Normal
Questionable
Visual defect
Normal
Questionable
Hearing loss
Average for age
Poor
Handicapped (describe)
Minor difficulty
Severe difficulty
Motivation
Behavior Attention
Attendance
Eyesight
Hearing
Motor coordination Excellent Speech
No problem
FIGURE 1-5. School information form that can be used to obtain child’s school history from school, day care center, or day activity center. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
Swaiman / General Aspects of the Patient’s Neurologic History
15
SCHOOL REPORT—cont’d Other health problems (specify)
Special help given
Remedial reading
Speech therapy
Special education
Tutoring
IV.
Briefly give your impression of the child’s behavior in school: any examples or anecdotes would be appreciated
V.
Attitude towards school
Other
Attitude towards peers Attitude towards self Attitude towards teacher VI.
Are there any problems that you think need special attention?
VII.
What do you like best about this child?
Yes
No
(please describe in detail)
What do his or her classmates like best? VIII.
What do you think can be done to help the child overcome his or her current difficulties? What resources are available in the school, school district, or community?
IX.
What is your impression of the home environment of the child (stimulating, average, detrimental)? Describe any specific features that you think may be important.
X.
What is the relationship between school personnel and the child’s parents?
Signature Title Date FIGURE 1-5. cont’d.
A questionnaire, as in Figure 1-5, can be devised that will allow supervisory personnel to record intellectual, motor, and emotional characteristics. It is essential that an adequate family history be recorded. Ages of siblings (including those who have died and those aborted), parents, grandparents, uncles, and aunts should be available. It is particularly helpful to gain health history details of deceased siblings and relatives, because familial conditions that might otherwise go undiscovered are often revealed. Questions concerning neurologic diseases initially should be specific; then more generalized questions should be asked because caregivers may not understand the more specific
approach. The presence of epilepsy, cerebral palsy, deafness, mental retardation, movement disorders, blindness, ataxia, weakness, or progressive intellectual and motor deterioration must be determined. Less sophisticated names, such as fainting spells, nervous breakdowns, strokes, and palsies, may strike a responsive chord. It is imperative that the clinician ask if any family members suffer from the same problems that affect the patient. Autosomal-dominant traits may be present in successive generations, although the degree of expressivity may vary. Autosomal-recessive traits often do not manifest in successive generations but may be present in siblings. Consanguinity must be considered when autosomal-recessive
16
Clinical Evaluation / 1
disease is part of the differential diagnosis. X-linked recessive conditions are manifest in male siblings, male first cousins, and maternal uncles. Careful questioning of the mother, if possible, is highly desirable. Although mitochondrial diseases may be inherited through transmission of maternal DNA, paternal inheritance patterns are also possible [Schwartz and Vissing, 2003]. If a genetic condition is suspected, it is wise to examine siblings, parents, and other family members to augment the history. REFERENCES Baker AB. Outline of clinical neurology. Dubuque, Iowa: William C Brown, 1958. Conners CK. A teacher rating scale for use in drug studies with children. Am J Psychiatry 1969;126:152. Frankenburg WK, Dodds JB. Denver developmental screening test. J Pediatr 1967;71:181. Frankenburg WK, Fandal AW, Sciarillo W, et al. The newly abbreviated and revised Denver Developmental Screening Test. J Pediatr 1981;99:995.
Frankenburg WK, Dodds JB, Archer P, et al. The Denver II: A major revision and restandardization of the Denver Developmental screening test. Pediatrics 1992;89:91. Hallioglu O, Topaloglu AK, Zenciroglu A, et al. Denver developmental screening test II for early identification of the infants who will develop major neurological deficit as a sequelae of hypoxic-ischemic encephalopathy. Pediatr Int 2001;43:400. Jackson R, Gibson KA, Wu YW, Croughan MS. Perinatal outcomes in singletons following in vitro fertilization: A meta-analysis. Obstet Gynecol 2004;103:551. Lim HC, Chan T, Yoong T. Standardisation and adaptation of the Denver Developmental Screening Test (DDST) and Denver II for use in Singapore children. Singapore Med J 1994;35:156. Lim HC, Ho LY, Goh LH, et al. The field testing of Denver Developmental Screening Test Singapore: A Singapore version of Denver II Developmental Screening Test. Ann Acad Med Singapore 1996;25:200. Lejarraga H, Pascucci MC, Krupitzky S, et al. Psychomotor development in Argentinean children aged 0-5 years. Paediatr Perinat Epidemiol 2002;16:47. Schwartz M, Vissing J. New patterns of inheritance in mitochondrial disease. Biochem Biophys Res Commun 2003;310:247.
CHAPTER 2
Neurologic Examination of the Older Child Kenneth F. Swaiman
The neurologic examination of children is described in this and the next two chapters. The material is organized on the basis of age for convenience of presentation; however, because it is usually feasible to perform a more rigorous examination of older children, detailed discussion of the conventional neurologic examination of children is provided in this chapter, including evaluation of the cranial nerves. Examination of a child older than 2 years should be as informal as possible while maintaining a basic flow pattern to permit complete evaluation. The older child has acquired a large repertory of skills since infancy (Box 2-1). For children between 2 and 5 years old, the Denver Developmental Screening Test II may be useful in evaluating various motor skills [Frankenburg et al., 1992] (see Chapter 1). Many neurologic functions of children between the ages of 2 and 4 years are examined in the same manner as those of children younger than 2 years. As is the case with younger children, some patients between 2 and 4 years old may be most comfortable sitting on a caregiver’s lap. The examining room should be equipped with small toys, dolls, and pictures with which to interest the child and provide for ease of interaction. Observation and play techniques are essential means of monitoring intellectual and motor function. Children may choose to move about the examining room and may be attracted to these various playthings. After 4 years of age, the components of the neurologic examination are more conventional and routine, and by adolescence, the examination is much the same as the adult examination.
OBSERVATION Much can be learned by observation during the historytaking session. Older children should sit in a chair or perform tasks, such as reading or drawing with crayons or colored pencils. If the child participates actively in the history-taking procedure, the child’s understanding and contribution to the session allow the examiner to make judgments about the child’s intellectual skills. The child’s language skills can be assessed. Stuttering, dysarthria, nasal speech, dysphonia, and problems of articulation are evident. This session also provides an additional opportunity to evaluate facial movements. Head nodding, lip twitching, eye blinking, and staring may be evidence of epilepsy. Movement disorders involving the face, such as chorea or tics, and other movement disorders involving the neck, limbs, and trunk (i.e., athetosis, chorea, dystonia, myoclonus, tics, and spasms) may be noticeable. This portion of the examination provides an opportunity to assess the child’s behavior. Impulsivity, short attention span, and relative dependence may be evident. The child may be
unable to sit or play quietly. Distractibility may be evident in response to minor external stimuli. The caregiver-child interaction may also be observed during this time. The caregiver may threaten or use physical force or obsequiously cajole the child. The child’s response may be inappropriate. The following questions must be answered. Does the child respond positively to the caregiver’s interaction? Does the child attempt to manipulate the caregiver? Is the response transient or persistent? Is the caregiver’s attitude one of caring or hostility?
SCREENING GROSS MOTOR FUNCTION Sometime between 4 and 6 years of age, most children of normal intelligence participate in a motor screening examination. A rapid screening component is advisable because the child may lose interest, become distractible, or become tired and oppositional. The child should stand before the examiner. Whenever possible during the entire the examination, the examiner should demonstrate each of the various motor acts with precision and good humor. A smiling examiner is much more likely to be accepted by the child. Then, for example, the examiner should ask the child to watch as he or she hops on either foot. The child should then be asked to hop in place on each foot (first one then the other) “just the way I did.” The same technique should then be used to have the child tandem walk forward and backward, toewalk, and heel-walk. The child should be asked to rise from a squatting position. The child should then be asked to stand with the feet close together, eyes closed, and arms and hands outstretched. This maneuver allows simultaneous assessment of Romberg’s sign and adventitious movements, particularly of the face, arms, and hands. The child should then be asked to perform finger-to-nose movements with the eyes closed and finger-to-finger-to-nose movements with the eyes open. After this rapid screening procedure, the examiner can begin a more detailed and systematic evaluation, bearing in mind any suggested abnormalities evident during the screening process.
PHYSICAL EXAMINATION Deep Tendon Reflexes Deep tendon reflexes (i.e., muscle stretch reflexes) are readily elicited by conventional means with a reflex hammer while the child is sitting quietly. In the case of the biceps reflex, it may be helpful for the examiner to place his or her thumb on the tendon and strike the positioned thumb to elicit the
18
Clinical Evaluation / 2
Box 2-1 EMERGING PATTERNS OF BEHAVIOR FROM 1 TO 5 YEARS OF AGE 15 Months Motor: Walks alone; crawls up stairs Adaptive: Makes tower of two cubes; makes a line with crayon; inserts pellet into bottle Language: Jargon; follows simple commands; may name a familiar object (ball) Social: Indicates some desires or needs by pointing; hugs parents 18 Months Motor: Runs stiffly; sits on small chair; walks up stairs with one hand held; explores drawers and waste baskets Adaptive: Piles three cubes; initiates scribbling; imitates vertical stroke; dumps pellet from bottle Language: 10 words (average); names pictures; identifies one or more parts of body Social: Feeds self; seeks help when in trouble; may complain when wet or soiled; kisses parents with pucker 24 Months Motor: Runs well; walks up and down stairs one step at a time; opens doors; climbs on furniture Adaptive: Makes tower of six cubes; circular scribbling; imitates horizontal strokes; folds paper once imitatively Language: Puts three words together (subject, verb, object) Social: Handles spoon well; tells immediate experiences; helps to undress; listens to stories with pictures 30 Months Motor: Jumps Adaptive: Makes tower of eight cubes; makes vertical and horizontal strokes but generally will not join them to make a cross; imitates circular stroke; forming closed figure Language: Refers to self by pronoun “I”; knows full name Social: Helps put things away; pretends in play 36 Months Motor: Goes up stairs altenating feet; rides tricycle; stands momentarily on one foot Adaptive: Makes tower of nine cubes; imitates construction of “bridge” of three cubes; copies a circle; imitates a cross Language: Knows age and gender; counts three objects correctly; repeats three numbers or a sentence of six syllables Social: Plays simple games (in “parallel” with other children); helps in dressing (unbuttons clothing and puts on shoes); washes hands 48 Months Motor: Hops on one foot; throws ball overhand; uses scissors to cut out pictures; climbs well Adaptive: Copies bridge from model; imitates construction of “gate” of five cubes; copies cross and square; draws a man with two to four parts besides head; names longer of two lines Language: Counts four pennies accurately; tells a story Social: Plays with several children with beginning of social interaction and role playing; goes to toilet alone 60 Months Motor: Skips Adaptive: Draws triangle from copy; names heavier of two weights Language: Names four colors; repeats sentences of 10 syllables; counts 10 pennies correctly Social: Dresses and undresses; asks questions about meanings of words; domestic role playing Adapted from Behrman RE, et al. Nelson textbook of pediatrics, 14th ed. Philadelphia: WB Saunders, 1992.
reflex. If the child is crying or overtly resists, the examiner should postpone this portion of the examination. The child may be reassured if the examiner taps the brachioradialis reflex of the caregiver before performing the same act on the child. Deep tendon reflexes customarily examined include the biceps, triceps, brachioradialis, patellar, and Achilles reflexes. Each tendon reflex is mediated at a specific spinal segmental level or levels (Table 2-1) [Haymaker and Woodhall, 1962; Hollinshead, 1969]. Hyperactive reflexes or clonic responses to tapping of the reflex result from corticospinal dysfunction. Hyperreflexia may also be indicated by an abnormal “spread”
of responses, which includes contraction of muscle groups that usually do not contract when a specific reflex is being elicited (i.e., crossed thigh adductor or finger flexor reflexes). Although a bilateral brisk reflex response may be normal, particularly when only one reflex is involved, unilateral hyperreflexia virtually always signals a pathologic process. Hyporeflexia may be associated with lower motor unit involvement (e.g., anterior horn cell disease, peripheral neuropathy, myopathy). However, hyporeflexia may occasionally be found with central depression, impaired central control of the gamma loop (central hypotonia), or involvement of
Swaiman / Neurologic Examination of the Older Child
TABLE 2-1 Muscle Stretch (Tendon) Reflexes REFLEX
NERVE
SEGMENTAL LEVEL
Biceps Brachioradialis Gastrocnemius and soleus (ankle jerk) Hamstring Jaw Quadriceps (knee jerk) Triceps
Musculocutaneous Radial Tibial
C5, C6 C5, C6 L5, S1, S2
Sciatic Trigeminal Femoral Radial
L4. L5, S1, S2 Pons L2-L4 C6, C8
the posterior root (intramedullary or extramedullary). With anterior horn cell involvement (e.g., infantile spinal muscular atrophy), the patellar reflexes are greatly diminished or absent early because the cells subserving the proximal muscles of the legs are profoundly involved first. Sensory involvement, particularly peripheral, is often detectable in patients with neuropathies. Similarly, the distal deep tendon reflexes tend to be involved earlier and to a greater degree. Reflexes may be normal early in the course of certain myopathies, including the muscular dystrophies, and may become absent later. Disease generally decreases muscle tone and may decrease tendon reflexes because of effects on the gamma loop. Enhancement of tendon reflex responses when reflexes are seemingly absent can be promoted by having the child squeeze an object such as a block or ball or perform the more traditional Jendrassik maneuver (i.e., hooking the fingers together while flexed and then attempting to pull them apart).
Other Reflexes A flexor (plantar) toe sign response is normal in children. Impairment of corticospinal tract function leads to extensor responses. The Babinski reflex is elicited by firm, steady, slow stroking from posterior to anterior of the lateral margin of the sole with an object such as a key or a tongue blade. The stimulus should not be painful. A positive response is a slow, tonic hyperextension of the great toe. This response is the constant and necessary feature of a positive response. The other four toes may also hyperextend, or they may slowly spread apart (i.e., fanning). Flicking the patient’s nail (second or third finger) downward with the examiner’s nail (i.e., the Hoffmann reflex) results in flexion of the distal phalanx of the thumb. No response or a muted response occur in normal children; a brisk or asymmetric response occurs in the presence of corticospinal tract involvement. Abdominal reflexes are obtained by stroking the abdomen from lateral to medial with strokes beginning just above the umbilicus, lateral to the umbilicus, and just below the umbilicus directed toward the umbilicus. Unilateral absence of the reflex usually is associated with acquired corticospinal tract dysfunction. The cremasteric reflex is elicited in males by stroking the inner aspects of the thigh in a caudal-rostral direction and observing the contraction of the scrotum. The reflex is normally present and symmetric. Absence or asymmetry may indicate corticospinal tract involvement.
19
Developmental reflexes are discussed in Chapter 3. The persistence of developmental reflexes beyond the expected age of extinction is usually an indication of corticospinal tract impairment [Zafeiriou, 2004].
Cerebellar Function Head tilt may be associated with tumors of the cerebellum. The tilt is usually ipsilateral to the involved cerebellar hemisphere, but exceptions are common. Herniation of the cerebellar tonsils through the foramen magnum resulting from increased intracranial pressure may cause head tilt; neoplasms that induce increased intracranial pressure, other than those of the cerebellum, may cause head tilt. Cerebellar function is also evaluated during testing of station and gait (see Chapter 5). Cerebellar dysfunction is usually associated with hypotonia. Tremor in cerebellar disease occurs with action (intention). Cerebellar function is assessed in a number of ways. Hand patting (i.e., alternating pronation and supination of the hand on the thigh while the other hand remains stationary on the other thigh) is a good method for assessing dysdiadochokinesis. The maneuver is repeated with each hand separately to assess the presence of mirror movements (i.e., synkinesis). Other tests that monitor cerebellar integrity include repetitive finger tapping (thumb to forefinger), foot tapping, and finger-to-nose, finger-to-finger (examiner’s)-to-nose, and heel-to-knee-to-shin stroking. These movements are an index of cerebellar function when limb strength and sensation are intact. Breaks in rhythm and nonfluidity of movement, as well as dysmetria, which is suggestive of cerebellar dysfunction, are evident during this phase of the examination.
Cranial Nerve Examination In older children, the cranial nerve examination may be performed in a systematic fashion, beginning with the first cranial nerve and testing through the twelfth. Examination of infants and younger children usually requires some modification of the sequence and may need some ingenious improvisation of the procedure, according to the degree of cooperation of the child. As is the case with all examinations of infants and young children, the less-threatening portions of the examination should be performed first.
Olfactory Nerve: Cranial Nerve I Olfactory nerve function is rarely impaired in childhood. Cranial nerve I can be evaluated by having the child smell pleasant aromas (e.g., chocolate, vanilla, peppermint) through each nostril while the other is manually occluded. Olfactory sensation is intact if the child appreciates a change in odor; precise identification is often impracticable. Anosmia occurs most commonly in children with upper respiratory infections or after head trauma, often occipital. Neoplasms in the inferior frontal lobe or cribriform plate regions can cause anosmia. Unilateral anosmia is more worrisome than bilateral anosmia because of the possibility of a unilateral neoplasm.
Optic Nerve: Cranial Nerve II Examination of cranial nerve II, the optic nerve, is one of the critical portions of the neurologic examination because of
20
Clinical Evaluation / 2
the long anterior-to-posterior span of the visual pathways within the brain. Formal visual acuity testing is possible with a Snellen chart or a “near card” in older children. Visual acuity and visual field testing should be performed in an appropriately lighted room. The visual test objects should be easily visible and without glare. Occasionally, when subtle changes are being investigated, it is efficacious to hold the visual field test object against a background of less contrast, increasing the difficulty of identification. Function can be difficult to evaluate in the very young child. Gross vision can be assessed in children younger than 3 or 4 years of age by their ability to recognize familiar items of various sizes, shapes, and colors. Beyond 4 years of age, the E test is useful. The child is taught to recognize the E and to discern the direction in which the three “arms” are pointing and point a finger accordingly. Most older children can be taught the essentials of the test in less than a minute. During the acuity evaluation, Es of different sizes, rotated in different directions, are presented to the child. For each eye, the visual field (range of vision) is assessed by confrontation with an object that is moved from a temporal to nasal direction along radii of the field. A small (3-mm), white or red test object or toy can be used. A modification of the same procedure can be used for double simultaneous testing by moving two test objects or penlights simultaneously from the temporal to the nasal fields and then from the superior and inferior portions of the temporal and nasal fields while the child looks directly at the examiner’s nose. Finger counting can be used if acuity is grossly distorted. In cases of extreme impairment, perception of a rapidly moving finger can be used. Visual acuity is rarely affected by papilledema until there is scarring of the optic nerve head. This lack of acuity change is in marked contrast to the early loss of visual activity that accompanies inflammation of the optic nerve.
The optic disc (i.e., optic nerve head) of the older child is sharply defined and often salmon colored, which differs from the pale gray color of the disc in an infant. In the presence of a deep cup in the optic disc, the color may appear pale, but the pallor is localized to the center of the disc. The pallor of optic atrophy occurs centrally and peripherally and is accompanied by a decreased number of arterioles in the disc margins. Most commonly, papilledema is associated with elevation of the optic disc, distended veins, and lack of venous pulsations. Hemorrhages may surround the disc. Before papilledema is obvious, there may be blurring of the nasal disc margins and hyperemia of the nerve head. Pupils should be observed in light that allows them to remain mildly mydriatic. The diameter, regularity of contour, and responsivity of the pupils to light should be examined. The upper lid is usually at the margin of the pupil. In Horner’s syndrome, impairment of the sympathetic pathway results in a miotic pupil, mild ptosis, and defective sweating over the ipsilateral side of the face (Fig. 2-1). Dragging a finger over the child’s forehead may aid in the recognition of anhidrosis. The fixed, dilated pupil usually is associated with other signs of oculomotor nerve dysfunction and may signify cerebral tonsillar herniation. The presence or absence of the pupillary light reflex differentiates between peripheral and cortical blindness. Lesions of the anterior visual pathway (i.e., retina to lateral geniculate body) result in the interruption of the afferent limb of the pupillary light reflex, producing an absent or decreased reflex. Anterior visual pathway interruption can cause amblyopia in one eye. In this situation, the pupil fails to constrict when stimulated with direct light; however, the consensual pupillary response (i.e., response when the other eye is illuminated) is intact. Various degrees of visual loss may modify this phenomenon so that the full response to direct stimulation is delayed, but the consensual reflex is brisk. The deficient pupillary reflex is revealed by alternately aiming a light source toward one eye and then the other. In the eye with decreased vision, consensual pupillary constriction is greater than the response to direct light stimulation (Marcus Gunn pupil); the pupil of the affected eye may dilate slightly during direct stimulation.
Oculomotor, Trochlear, and Abducens Nerves: Cranial Nerves III, IV, and VI
FIGURE 2-1. Bilateral oculomotor nerve paralysis. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
The oculomotor, trochlear, and abducens cranial nerves control extraocular motor movements; these nerves must operate synchronously or diplopia ensues. Cranial nerve III innervates the superior, inferior, and medial recti; the inferior oblique; and the eyelid elevator (levator palpebra superioris). Cranial nerves IV and VI innervate the superior oblique muscle and the lateral rectus muscle, respectively. Unfortunately, for purposes of understanding, the function of extraocular muscles depends somewhat on the direction of gaze. The lateral and medial recti are abductors and adductors of the globe, respectively. The superior rectus and inferior oblique are elevators, and the inferior rectus and superior oblique are depressors. The oblique muscles act in the vertical plane while an eye is adducted. The recti muscles serve this function when an eye is abducted (Fig. 2-2). When directed forward (i.e., primary position), the oblique muscles effect
Swaiman / Neurologic Examination of the Older Child ELEVATION Superior rectus Inferior oblique
21
FIGURE 2-2. Extraocular muscle movement. A, In primary position. B, In abduction and adduction. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
A
DEPRESSION Inferior rectus Superior oblique Superior rectus
Inferior oblique
A b d u c Lateral rectus
A b d u c
A d d u c Medial rectus
t i o n
Inferior rectus
t i o n
Superior rectus
Medial rectus
Superior oblique
torsion around the anteroposterior axis (rotation) of the globes [Cogan, 1966]. The eye position that results from paralysis of each eye muscle is listed in Table 2-2. In heterophorias, also called phorias, both globes are directed normally on near or far objects during fixation; however, one or both deviate when one eye is occluded TABLE 2-2 Extraocular Muscle Paralysis PARETIC MUSCLE
CRANIAL NERVE
EYE DEVIATION
Inferior oblique Inferior rectus Lateral rectus Medial rectus Superior oblique
III III VI III IV
Superior rectus
III
Down and out Up and in Medial Lateral Upward and outward (head tilted) Down and in
t i o n
Lateral rectus
B
Inferior rectus
while the other eye fixes. Forcing fixation of the uncovered eye by alternately covering each eye confirms the diagnosis of heterophorias. This predisposition may be evident when the child is febrile or fatigued. Exophoria is a predisposition to divergence, whereas esophoria is a predisposition to convergence. Eye deviations detectable during binocular vision are heterotropias, also called tropias. Adduction tropias are esotropias; abduction tropias are exotropias. Tropias are most often caused by compromised extraocular muscle innervation. Extraocular palsies can frequently be detected by observation of eye movements. A red glass is placed in front of an eye, and a focused, relatively intense white light is aimed at the eyes from various visual fields while the child fixes on the light. A merged, solitary, red-white image is perceived when extraocular movements are normal; however, when muscle paresis is present, the child reports a separation of the red and white images when looking in the direction of action of the affected muscle. The farthest peripheral image
22
Clinical Evaluation / 2
is the one perceived by the abnormal eye; this eye can be identified by the color of the image. Minimal extraocular muscle palsies may be heralded by delayed eye movement to the appropriate final position. Volitional turning of the head accompanies paresis of the lateral rectus muscle to forestall diplopia; the head is deviated toward the paretic muscle, and the eyes are directed ahead. In superior oblique or superior rectus muscle palsies, tilting of the head toward the shoulder opposite the side of the paretic eye muscle occurs. Extraocular muscle dysfunction is associated with many conditions that affect the brainstem, cranial nerves, neuromuscular junction, or muscles. Among the diseases are ophthalmoplegic migraine, cavernous sinus thrombosis, brainstem glioma, myasthenia gravis, and congenital myopathy. Cranial nerve VI function may be impaired by increased intracranial pressure, irrespective of cause. Squint, usually esotropia, often accompanies decreased visual acuity in infants and young children [Smith, 1967]. Ptosis and extraocular muscle paralysis accompany dysfunction of cranial nerve III. Ptosis resulting from oculomotor nerve compromise is usually more pronounced than is the malposition of the lid associated with Horner’s syndrome. This symptom is of great diagnostic aid because the lid does not significantly elevate when the patient is asked to look up. Complete oculomotor nerve paralysis, although uncommon, causes the eye to position downward and outward. Poor adduction and elevation are also evident (see Fig. 2-1). Version eye positioning may accompany irritative or destructive brainstem lesions and cerebral hemispheral lesions. In destructive brainstem conditions the conjugate eye movement (version) deviation is toward the opposite side. Destructive cerebral hemispheral lesions will cause the eyes to deviate toward the side of the lesion; conversely, an irritative cerebral hemispheral lesion causes the eyes to turn away from the side of the lesion. Eye-movement deviations of the binocular disconjugate (nonparallel) type caused by brainstem dysfunction also occur in children. Vertical gaze paresis results from dysfunction of the tectal area of the midbrain. Patients with a pineal tumor or hydrocephalus may be unable to elevate the eyes for upward gaze. Brainstem lesions, especially those in the midbrain or pons, may disrupt the medial longitudinal fasciculus. The resultant impairment of conjugate eye movement is referred to as an internuclear ophthalmoplegia. These lesions engender weakness of medial rectus muscle contraction of the adducting eye, which is accompanied by a monocular nystagmus in the abducting eye. Occasionally, paresis of lateral rectus muscle movement in the abducting eye may occur. Medial longitudinal fasciculus involvement may be unilateral or bilateral and may be associated with a number of brainstem conditions, including hemoglobinopathies, demyelinating disease, or brainstem vascular disease [Cogan, 1966]. Internal ophthalmoplegia consists of a fully dilated pupil that is unreactive to light or accommodation. Extraocular muscle function is normal when each muscle is tested separately. The oculomotor nerve, nucleus, or ciliary ganglion may be sites of involvement. External ophthalmoplegia results in ptosis and paralysis of all extraocular muscles. Pupillary reactivity is normal.
This pattern of involvement may accompany myasthenia gravis, hyperthyroidism, ocular myopathy, Möbius’ syndrome, tumors or vascular lesions of the brainstem, Wernicke’s disease, botulism, and lead intoxication. Opticokinetic nystagmus is a useful test in evaluating the eye movements of children. A drum or tape with stripes or figures is slowly rotated or drawn before the child’s eyes in horizontal and vertical directions. With fixation, the child should visually track the object in the direction the tape is being drawn, with a rapid, rhythmic movement (refixation) of the eyes in the reverse direction to enable fixation on the next figure or stripe. Absence of such a response may result from failure of fixation, amaurosis, or disturbed saccadic eye movements. The child who appears clinically blind because of a conversion reaction exhibits a normal opticokinetic nystagmus response. Children who manifest congenital nystagmus and have an opticokinetic nystagmus response in the vertical plane likely have adequate functional sight. Absence of opticokinetic nystagmus in the presence of congenital nystagmus heralds reduced visual acuity. If asymmetry of an opticokinetic nystagmus response is evident, lateral lesions in the posterior half of the cerebral hemisphere are likely present. The lesion is on the side that manifests reduced or absent opticokinetic nystagmus reactivity. The area of involvement is generally in the posterotemporal, parietal, or occipital areas. Hemianopic field defects may exist. Spontaneous nystagmus (i.e., involuntary oscillatory movements of the eye) may be horizontal, vertical, or rotary; a patient can exhibit all three types. The movements may consist of a slow and fast phase, giving rise to the term jerk nystagmus. However, the phases may be of equal duration and amplitude, appearing pendular. Nystagmus, especially vertical nystagmus, is most commonly induced by medications (e.g., barbiturates, phenytoin, carbamazepine, benzodiazepines). Such nystagmus often has a jerk component and is usually most prominent in the direction of gaze. Vertical nystagmus that is not associated with medications indicates brainstem dysfunction. A few beats of horizontal nystagmus with extreme lateral gaze is usually normal. Persistent horizontal nystagmus indicates dysfunction of the cerebellum or brainstem vestibular system components; the nystagmus is coarser (i.e., the amplitude of movements greater) when the direction of gaze is toward the side of the lesion. A rare condition, seesaw nystagmus, is characterized by disconjugate (alternating) movement of the eyes, which move upward and downward in a seesaw motion. This type of nystagmus accompanies lesions in the region of the optic chiasm (see Chapter 6).
Trigeminal Nerve: Cranial Nerve V Cranial nerve V, the trigeminal nerve, has motor and sensory functions. The motor division of the trigeminal nerve innervates the masticatory muscles: masseter, pterygoid, and temporalis. Temporalis muscle atrophy manifests as scalloping of the temporal fossa. The masseter muscle bulk may be assessed by palpation while the patient firmly closes the jaw. Pterygoid muscle strength is evaluated by having the patient open the mouth and “slide” the jaw from one side to the other while the examiner resists movements with the hand to assess muscle strength. The jaw reflex is elicited when the
Swaiman / Neurologic Examination of the Older Child
23
examiner places a finger on the patient’s chin while the mouth is slightly open and taps the finger to stretch the masticatory muscles. A rapid muscle contraction with closure of the mouth is the reflex response. This stretch reflex receives its afferent and efferent nerve control from cranial nerve V; the segmental level is located in the midpons. The expected reflex reaction is absent with motor nucleus and peripheral trigeminal nerve compromise. Conversely, this reflex is overactive in the presence of supranuclear lesions; rarely, jaw clonus may be evident. Because of weakness of the ipsilateral pterygoid muscles, unilateral impairment of the trigeminal nerve causes deviation of the jaw toward the side of the lesion. Cranial nerve V is also responsible for sensation involving the face and the anterior half of the scalp (Fig. 2-3). Brainstem compromise can effect clearly delineated laminar sensory deficits; however, mapping of such deficits is difficult in children. The corneal reflex, provided its sensory input by the trigeminal nerve, may be diminished or absent after trauma, in cerebellopontine angle tumors, in brainstem tumors, in cavernous sinus thrombosis, in Gradenigo’s syndrome, or in childhood collagen-vascular diseases.
Facial Nerve: Cranial Nerve VII Taste sensation over the anterior two thirds of the tongue, secretory fibers (parasympathetic) innervating the lacrimal and salivary glands, and innervation of all facial muscles are accomplished by cranial nerve VII. Complete motor dysfunction on one side of the face ensues when the cranial nerve VII pathway is disrupted in the nucleus, pons, or peripheral nerve. The patient is unable to move the forehead upward, close the eye forcefully, or elevate the corner of the mouth on the side of the affected nerve (Figs. 2-4 and 2-5). Central (supranuclear) facial nerve impairment produces only paresis of the muscles involving the lower face, with resultant drooping of the angle of the mouth, disappearance or diminution of the nasal labial fold, and widened palpebral fissure. The muscles of the forehead, which are innervated bilaterally, are unaffected. Cardiofacial syndrome is a congenital weakness that causes failure of depression of the angle of the mouth and is unrelated to facial nerve palsy.
FIGURE 2-4. Right facial paralysis of the peripheral type. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
Ophth. C2 C2,3
Max.
Mand.
C2,3
FIGURE 2-3. Facial sensation supplied by the trigeminal nerve. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
FIGURE 2-5. The Möbius syndrome is manifested by bilateral palsy of cranial nerves VI and VII.
Taste sensation in the anterior two thirds of the tongue is in part provided by the chorda tympani nerve, which traverses the path of the facial nerve for a short distance. Testing of taste sensation is difficult. Evaluation of taste requires that the patient extend the tongue and that the examiner hold the tip of the tongue with a piece of gauze and place salty, sweet, acidic, and sour and bitter materials, usually represented by salt, sugar, vinegar, and quinine, on the anterior portion of the tongue. The patient’s tongue must remain outside of the mouth
24
Clinical Evaluation / 2
until the test is completed. An older patient should be able to identify each substance.
Auditory Nerve: Cranial Nerve VIII Function and evaluation of cranial nerve VIII are discussed in detail in Chapters 7 and 8. Although cranial nerve VIII is known as the auditory nerve, it has auditory and vestibular functions. Gross auditory impairment may be suspected during the history-taking session while the child is in the room. The child may not respond directly to questions or to directions from the caregivers. More specific testing with whispered language, the ticking of a watch, a party noisemaker, or a tuning fork may be used to gain more information. Patients who fail to develop speech or who have slow speech development, as well as those who have difficulty with fluency and articulation, may have hearing impairment. Older children can cooperate with formal audiometric testing. Such testing may not be possible in younger infants, but brainstem auditory-evoked potentials may provide the necessary information concerning hearing impairment and the level of dysfunction within the nervous system. The clinical evaluation and caloric testing can be used for gross assessment of vestibular function. More complex evaluation should be undertaken if the screening tests or the complaint indicate a need for more detailed assessment. Complaints of nausea, ataxia, vertigo, or unexplained vomiting, singly or in combination, may indicate labyrinthine and vestibular pathologic origins. Caloric testing can be performed with relative ease. While the patient is in the supine position, the head is flexed at 30 degrees. Ice water (10 mL) is injected over 30 seconds into one external auditory canal at a time. The conscious patient develops coarse nystagmus toward the ipsilateral ear; no eye deviation occurs. If the patient has some degree of obtundation, there is a modification of the response. The eyes become tonically deviated ipsilaterally, with accompanying nystagmus occurring contralaterally. If the patient is comatose, cold water stimulation usually causes tonic deviation ipsilaterally and no nystagmus; if the coma is profound or the patient is brain dead, no eye changes occur.
absence of other findings. The integrity of cranial nerves IX and X is necessary for a gag response. Although the larynx can be studied under direct or indirect laryngoscopy, the presence of stridor, hoarseness, or dystonia suggests the need for more detailed examination of the brainstem and cranial nerve IX integrity.
Spinal Accessory Nerve: Cranial Nerve XI Cranial nerve XI provides innervation for the trapezius and sternocleidomastoid muscles. Cranial nerve XI comprises some fibers from C1 and C2 and some from the motor nucleus in the brainstem and is unique in combining brainstem and cervical cord origins. The trapezius muscles are assessed when the patient is asked to shrug the shoulders against resistance placed by the examiner. Atrophy of the muscle and drooping of the shoulder provide further information on the status of the trapezius. The sternocleidomastoid muscle is tested by exerting resistance against the child’s head while the child attempts rotation to one side. Weakness of the sternocleidomastoid muscle results in an inability to rotate the head to the contralateral side. Muscle bulk of the sternocleidomastoid muscle is readily palpable and is readily visible in the presence of moderate-to-severe atrophy. Congenital or acquired lesions in the area of the foramen magnum most commonly cause difficulties of cranial nerve XI.
Hypoglossal Nerve: Cranial Nerve XII The tongue muscle is the primary responsibility of cranial nerve XII. Atrophy and fasciculation of the tongue occur when the ipsilateral hypoglossal nucleus or hypoglossal nerve is involved. The protruded tongue deviates toward the involved side because contraction of the normally innervated tongue muscle causes protrusion and is unopposed. The child cannot push the tongue against the cheek of the unaffected side. Speech may be muffled or dysarthric. Bilateral involvement of hypoglossal nuclei or cranial nerve XII may be severely incapacitating. The tongue muscle may be markedly
Glossopharyngeal and Vagus Nerves: Cranial Nerves IX and X Examination of the larynx, pharynx, and palate provides most of the desired information concerning the function of cranial nerves IX and X. Unilateral paresis of the soft palate causes an ipsilateral droop, even when the patient is expelling air through the open mouth or gagging in response to a tongue blade. Bilateral involvement causes a flaccid, soft palate bilaterally. With bilateral paresis, the voice becomes nasal, and regurgitation of fluids occurs during drinking. During evaluation of swallowing, the child should be asked to swallow up to 10 times to determine the efficacy of swallowing and stamina. The examiner can evaluate the difficulty and the relative movements of the hyoid during swallowing. The gag reflex is mediated through cranial nerve IX and is elicited by touching the posterior pharyngeal mucosa with a tongue blade. Normal individuals may have absence or a seemingly disproportionately violent response; assessing the importance of changes in the gag reflex is difficult in the
FIGURE 2-6. Fasciculation of the tongue, especially of the right lateral border, in a patient with group 2 Werdnig-Hoffman disease. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
Swaiman / Neurologic Examination of the Older Child
atrophied, and fasciculations of the tongue may be very prominent (Fig. 2-6). The patient may be unable to protrude the tongue beyond the lips, and there is marked dysarthria with unintelligibility of speech. Although chewing and swallowing are somewhat affected by unilateral tongue weakness, bilateral involvement results in gross difficulty. Cranial nerve XII dysfunction may result from supranuclear bulbar palsy from unilateral or bilateral corticobulbar tract involvement. Although the signs and symptoms may resemble those of involvement of the hypoglossal nucleus or nerve, lower motor unit signs such as fasciculations and atrophy are absent. Certain movement disorders, particularly dystonia, may interfere with normal tongue movements and confound the examiner.
Sensory System Cooperation of the pediatric patient is paramount to the success of the sensory examination. Vibration sense and joint and position sense are usually easily tested in all four limbs. Touch may be assessed by a single stimulus or by double simultaneous stimulation of two skin areas. The latter tests extinction of perception over an involved area. Testing should include areas of the face, trunk, and limbs. The ability to localize the area of contact of a tactile stimulus, topagnosis, is monitored by touching the patient, whose eyes are closed, on the face, arm, hand, leg, or foot with the examiner’s finger or a cotton swab; the child is asked to point to or verbally identify the area. The loss of ability to localize the stimulus is associated with parietal lobe dysfunction.
In a more sophisticated test, the patient is touched on two parts of the body simultaneously (i.e., double simultaneous stimulation test). Extinction is the term used to denote failure of the child to perceive both stimuli. The contralateral parietal lobe to the side on which the unidentified stimulus was applied is the site of dysfunction. Pain, as tested with pinprick, must be assessed gently, rapidly, and in a nonthreatening and playful manner. Testing for segmental sensory level during childhood is sometimes an essential portion of the examination. Because the patient must be attentive and cooperative, the examination often must be repeated for corroboration. Segmental sensory innervations of the arm and leg are illustrated in Figures 2-7, 2-8, and 2-9 [Keegan and Garrett, 1948]. The nipples are at approximately the T5 level and the umbilicus at the T10 level. Cortical sensory function can be tested in the older child. So-called cortical sensory functions require attentiveness and cooperation and involve complex processing. Because the tests are primarily of parietal lobe function, testing of these functions assumes and requires intact sensory neurologic pathways from the diverse cutaneous specialized nerve endings, muscles, and joints and subsequent connections with the parietal lobe. Stereognosis is the recognition of familiar objects by touch. After the patient closes the eyes, objects are placed by the examiner in one of the child’s hands and then the other. The patient should recognize the objects by size, texture, and form. Objects may include a button, safety pin, or key. Coins are particularly useful because older patients can be asked to differentiate among them. The patient must be able
FIGURE 2-7. Segmental sensory innervation of the arm. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School; adapted from Keegan JJ, Garrett FD. The segmental distribution of the cutaneous nerves in the limbs of man. Anat Rec 1948;102:409. Reprinted with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc.)
Ventral C3
C6
C4 C5 T1
C7 C8 C3 Dorsal C6
C7 C8
25
C4 C5 C6 C7 C8 T1
26
Clinical Evaluation / 2
Dorsal
ulation is determined. Normal findings have been reported for children 2 to 12 years old [Cope and Antony, 1992]. Testing of this modality is frequently performed over the fingertips. Differences in perception over homologous areas on both sides are sought. Absence or impairment of two-point discrimination results from parietal lobe dysfunction.
Ventral
L1 L2 L3 L4 L5 S1 S2 S3 S4 S5
Skeletal Muscles S2 L1
L2
L2
L3
L3 L5
Tone, bulk, and strength of the skeletal muscles should be determined during this portion of the examination. The segmental innervation patterns of the trunk muscles and the extremities and the motor functions of the spinal nerves are described in Tables 2-3, 2-4, and 2-5. The strength of limb muscles is assessed, when possible, by testing the child’s ability to counteract resistance imposed by the examiner on proximal and distal muscle groups or individual muscles. Norms cited for gross motor outcomes in young children with brain injury are useful in assessing children with apparent motor difficulties [Golumb et al., 2004].
S2
Muscle Testing S1 L4
L4 S1
L5 FIGURE 2-8. Segmental sensory innervation of the leg. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School, adapted from Keegan JJ, Garrett FD. The segmental distribution of the cutaneous nerves in the limbs of man. Anat Rec 1948;102:409. Reprinted with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc.)
to manipulate the objects freely with the fingers and palms. Absence of stereognosis is astereognosis. Astereognosis usually results from lesions of the parietal lobe. Graphesthesia is the ability to recognize numbers, letters, or other readily identifiable symbols traced on the skin. It is necessary to ascertain that the child is capable of identifying the symbols. This ability can be determined best by tracing the symbols in a preliminary trial while the child’s eyes are open. When the patient’s eyes are closed, the figures are traced over the palm or forearm. Failure to identify the symbols is called dysgraphesthesia. By 8 years of age, most children are able to correctly identify all single digits. The ability to distinguish between closely approximated stimulation at two points is two-point discrimination. The minimal distance between two simultaneous points of stim-
The skeletal muscles selected in the subsequent text are responsible for primary movements (Table 2-6). The material presented is adapted from Baker [1958]. Frequently, more than one muscle participates in the movement. For this reason, while testing the selected muscles, the examiner should observe and palpate surrounding muscles to detect any substitution of action of other muscles. The following scoring system is useful for recording muscle power*: 5: Normal power 4: Inability to maintain position against moderate resistance 3: Inability to maintain position against slight resistance or gravity 2: Active movement with gravity eliminated 1: Trace of contraction 0: No contraction While testing for muscle function, it is most convenient for the patient to maintain a fixed position against force. The examiner can assess the strength of various muscles by instituting the action of the antagonist. This strategy obviates the necessity of providing new directions for each muscle tested and simplifies the procedure for patient and examiner. The fixed positions depicted in Figure 2-10 are used routinely here and are referred to by the following letters: Position A: The arm is adducted, the forearm flexed at the elbow, and the wrist placed across the xiphoid process. Position B: The child lies on the back with the lower extremity flexed at 90 degrees at the hip and knee. The examiner should support the lower limb at the ankle. Position C: The child lies on the back with the leg and foot in normal extension. *Adapted from Medical Research Council. War memorandum, no. 7. Aids to the investigation of peripheral nerve injuries, 2nd ed. London, His Majesty’s Stationery Office, 1943 (reprinted 1960).
Swaiman / Neurologic Examination of the Older Child
27
C2
C3 C2 C4 C4 C5
T2 T3 T4
T2
T5 T6 T7 T8 T9 T10 T11 T12
C6 T1
C6
T1
C7
C5 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 L1 L2 S2 S3
C3 C5 T2
C6
C6
L1
L2
T1
T1
S4 S5
C7 L2
C8
C8
S3 S2
L3 L3
L5 L4
L5 L4
S1 S1 FIGURE 2-9. Radicular cutaneous fields.
When the weakness of any muscle group prevents the use of any of these positions, substitute positions should be improvised. Unfortunately, while examining young children, problems with cooperation or coordination may make it difficult to evaluate maximal strength; only gross testing may be possible, during which various functions are tested by using game playing or gross maneuvers, such as the “wheelbarrow” maneuver (i.e., walk on the hands while the examiner holds the child’s feet and moves slowly forward). Arm and shoulder strength can also be assessed by using functional operations. The child is asked to lean against a wall with the legs placed a foot or two from the wall edge and the arms outstretched with the palms against the wall. Strength of the shoulder girdle and arm extension can be evaluated. Winging of the scapulas also is evident. Alter-
natively, the child can be placed on the floor and asked to “wheelbarrow.” The child should be placed on the floor and asked to rise without aid. The normal child will spring erect. The child with weakness of the hip extensors will engage in Gowers’ maneuver and climb up the legs and push off into the erect position (Fig. 2-11). During examination of gait, the examiner must be aware of the presence of normal associated movements of the arms, circumduction of the legs, footdrop, unusual positions of the feet, and waddling (see Chapter 5). The presence of a limp may also be evident. Muscle bulk is evaluated by gentle palpation and observation. Abnormalities include atrophy and fasciculations that accompany anterior horn cell disease and muscle hypertrophy, particularly of the gastrocnemius and deltoid muscles associated with Duchenne’s muscular dystrophy and
28
Clinical Evaluation / 2
TABLE 2-3 Motor Functions of the Spinal Nerves NERVES
MUSCLES*
FUNCTION
Cervical plexus (C1–C4) Cervical Phrenic
Deep cervical Scalene Diaphragm
Flexion, extension, and rotation of the neck Elevation of the ribs (inspiration) Inspiration
Pectorales major and minor Serratus anterior Levator scapulae Rhomboid Supraspinatus Infraspinatus Lattisimus dorsi Teres major Subscapularis Deltoid Teres minor Biceps brachii Coracobrachialis Brachialis Flexor carpi radialis Palmaris longus Flexor digitorum sublimis Flexor pollicis longus Flexor digitorum profundus (radial half) Pronator quadratus Pronator teres Abductor pollicis brevis Flexor pollcis brevis Lumbricals I, II, III
Adduction and depression of the arm downward and medially Fixation of scapula on raising the arm Elevation of scapula Drawing the scapula upward and inward Outward rotation of the arm Elevation and outward rotation of the arm
Suprascapular Subscapular Axillary Musculocutaneous Median
Ulnar
⎧ ⎪ ⎨ ⎪ ⎩
Brachial plexus (C5–T1) Anterior Long thoracic Dorsal scapular
Opponens pollicis brevis Flexor carpi ulnaris Flexor digitorum profundus (ulnar half) Adductor pollicis Hypothenar Lumbricals III, IV
Extensor indicis proprius
Adduction of metacarpus I Abduction, opposition, flexion of the little finger Flexion of the first phalanx and extension of the other phalanges of fourth and fifth fingers Same action as preceding. Also spreading apart of fingers and bringing them together Extension of the forearm Flexion of the forearm Extension and radial flexion of the hand Extension of proximal phalanges of second through fifth fingers Extension of the proximal phalanx of the little finger Extension and ulnar deviation of the hand Supination of the forearm Abduction of metacarpus I Extension of the proximal phalanx of the thumb Abduction of first metacarpus and extension of the distal phalanges of the thumb Extension of the proximal phalanx of the index finger
Thoracic and abdominal
Elevation of the ribs, expiration, abdominal compression, etc.
Iliopsoas Sartorius Quadriceps femoris Pectineus ⎧ Adductor longus ⎪⎪ ⎪ Adductor brevis ⎨ Adductor magnus ⎪⎪⎪ ⎩ Gracilis Obturator externis
Flexion of the leg at the hip Inward rotation of the leg together with flexion of the upper and lower leg Extension of the lower leg
Gluteus medius Gluteus minimus Tensor fasciae latae Piriformis Gluteus maximus
Abduction and inward rotation of the leg, also under certain circumstances, an outward rotation Flexion of the leg at the hip Outward rotation of the leg Extension of the leg at the hip
Interossei Radial
Thoracic nerves Thoracic Lumbar plexus (T12–L4) Femoral Obturator
Sacral plexus (L5–S5) Superior gluteal
Inward rotation and abductiion of the arm toward the back Inward rotation of the arm Raising of arm to the horizontal Outward rotation of the arm Flexion and supination of the forearm Elevation and adduction of the arm Flexion of the forearm Flexion and radial deviation of the hand Flexion of the hand Flexion of the middle phalanges of second through fifth fingers Flexion of the distal phalanx of the thumb Flexion of the distal phalanges of second and third fingers Pronation Pronation Abduction of metacarpus I at right angles to palm Flexion of proximal phalanx of thumb Flexion of the proximal phalanges and extension of the other phalanges of first, second, and third fingers Opposition of metacarpus I Flexion and ulnar deviation of the hand Flexion of distal phalanges of fourth and fifth fingers
Triceps brachii Brachioradialis Extensor carpi radialis Extensor digitorum communis Extensor digit quinti propius Extensior carpi ulnaris Supinator Abductor pollicis longus Extensor pollicis brevis Extensor pollicis longus
Adduction of the leg Adduction and outward rotation of the leg
Swaiman / Neurologic Examination of the Older Child
29
TABLE 2-3 Motor Functions of the Spinal Nerves—cont’d
Inferior gluteal Sciatic
MUSCLES*
FUNCTION ⎧ ⎪ ⎨ ⎪ ⎩
NERVES
Obturator internus Gemelli Quadratus femoris Biceps femoris Semitendinosus Semimembranosus Tibialis anterior Extensor digitorum longus Extensor hallucis brevis Peroneus Gastrocnemius Soleus Tibialis posterior Flexor digitorum longus Flexor hallucis longus Flexor digitorum brevis Flexor hallucis brevis Plantar ⎧ ⎪ ⎨ ⎪ ⎩
Peroneal Deep Superficial Tibialis
Pudendal
Perineal anal sphincters
Outward rotation of the leg Flexion of the leg at the hip Dorsiflexion and supination of the foot Extension of the toes Extension of the great toe Pronation of the foot Plantar flexion of the foot Adduction of the foot Flexion of the distal phalanges II through V Flexion of distal phalanx I Flexion of middle phalanges II through V Flexion of middle phalanx I Spreading and bringing together and flexion of the proximal phalanges of the toes Closure of sphincters of the pelvic organs; participation in the sexual act; contraction of pelvic floor
*Various muscles may receive still other nerve supplies than those mentioned. The following are the principal accessory nerve supplies: the brachial muscle receives fibers from the radial nerve; the flexor digitorum sublimis, from the ulnar; the adductor pollicis, from the median; the pectineus, from the femoral; the adductor magnus, from the tibial. From Haymaker W. Bing’s local diagnosis in neurological diseases, 15th ed. St. Louis: Mosby, 1969.
Position A
Position B
Position C
FIGURE 2-10. Position of the limbs for muscle strength (see Table 2-6).
FIGURE 2-11. Gowers’ maneuver indicates weakness of truncal and proximal lower extremity muscles. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
other dystrophies, as well as myotonia congenita. Muscle tenderness, nerve tenderness, and nerve hypertrophy can also be assessed by palpation. Myotonia can be elicited by tapping over the thenar eminence and deltoid muscles. Tapping the tongue should be performed at the end of the examination
30
Clinical Evaluation / 2 Table 2-4
Segmental Innervation of Muscles of Extremities THORACIC SEGMENTS
CERVICAL SEGMENTS 4
5
6
7
8
1
Supraspinatus
Shoulder
Teres minor Deltoid Infraspinatus Subscapular Teres major Biceps brachii
Arm
Brachialis Coracobrachialis Triceps brachii Anconeus Brachioradialis Supinator Extensor carpi radialis Pronator teres Flexor carpi radialis Flexor pollicis longus Abductor pollicis longus
Forearm
Extensor pollicis brevis Extensor pollicis longus Extensor digitorum communis Extensor indicis proprius Extensor carpi ulnaris Extensor digiti V proprius Flexor digitorum subimis Flexor digitorum profundus Pronator quadratus Flexor carpi ulnaris Palmaris longus From Haymaker W. Bing’s local diagnosis in neurological diseaes, 15th ed. St. Louis: Mosby, 1969.
Continued
Swaiman / Neurologic Examination of the Older Child
Table 2-4
Segmental Innervation of Muscles of Extremities—cont’d
THORACIC SEGMENTS 12
LUMBAR SEGMENTS 1
2
SACRAL SEGMENTS
3
4
5
1
2
Iliopsoas Tensor fasciae latae Gluteus medius Gluteus minimus Hip
Quadratus femoris Gemellus inferior Gemellus superior Gluteus maximus Obturator internus Piriformis Sartorius Pectineus Adductor longus Quadriceps femoris Gracilis
Thigh
Adductor brevis Obturator externus Adductor magnus Adductor minimus Articularis genu Semitendinosus Semimembranosus Biceps femoris Tibialis anterior Extensor hallucis longus
Leg
Popliteus Plantaris Extensor digitorum longus Soleus From Haymaker W. Bing’s local diagnosis in neurological diseaes, 15th ed. St. Louis: Mosby, 1969.
3
31
32
Clinical Evaluation / 2 Table 2-4
Segmental Innervation of Muscles of Extremities—cont’d CERVICAL SEGMENTS 4
5
THORACIC SEGMENTS 6
7
8
1
Abductor pollicis brevis Flexor pollicis brevis Opponens pollicis Flexor digiti V
Hand
Opponens digiti V Adductor pollicis Palmaris brevis Abductor digiti V Lumbricals Interossei THORACIC SEGMENTS 12
LUMBAR SEGMENTS 1
2
3
SACRAL SEGMENTS 4
5
1
2
Gastrocnemius Peroneus longus Peroneus brevis
Leg—cont’d
Tibialis posterior Flexor digitorum longus Flexor hallucis longus Extensor hallucis brevis Extensor digiti brevis Flexor digiti brevis Abductor hallucis Flexor hallucis brevis Lumbricals
Foot
Abductor hallucis Abductor digiti V Flexor digiti V brevis Opponens digiti V Quadratus plantae Interossei
3
Swaiman / Neurologic Examination of the Older Child
Table 2-5
Segmental Innervation of Trunk Muscles
CERVICAL SEGMENTS 1
2
3
33
4
5
6
7
LUMBAR SEGMENTS
THORACIC SEGMENTS 8
1
2
3
4
5
6
7
8
9
10 11 12
1
2
3
4
SACRAL SEMENTS 5
1
2
3
4
COCCYX 5
DEEP LONG MUSCLES OF THE BACK Short deep neck muscles
Splenius muscles
Levator, sphincter ani, perineal, and coccygeal
Serratus posterior inferior
Serratus posterior superior
Latissimus dorsi
Trapezius
Levator scapulae Rhomboids Longus capitis
Longus colli
Rectus abdominis External oblique, abdominal
Scalenes
Pectoralis major
Transverse abdominal
Pectoralis minor
Internal oblique, abdominal
Subclavius
Quadratus lumborum
Serratus anterior Diaphragm
Intercostal muscles
From Haymaker W. Bing’s local diagnosis in neurological diseaes, 15th ed. St. Louis: CV Mosby, 1969.
and only when other elements of the history or examination make this evaluation essential. Tapping individual muscles with the reflex hammer elicits the myotatic reflex, which may be useful in the detection of myopathy because the reflex is absent in myopathies. Muscle tone is evaluated when the child is relaxed so that resistance to passive movement can be monitored. Aside from passive movement of limbs at joints, the examiner also assesses the extensibility of muscles by shaking the limbs and determining the range of motion. Tone may be decreased in the presence of cerebellar disease and anterior horn cell disease. Tone may be increased because of the rigidity associated with basal ganglia disease and spasticity associated with corticospinal tract dysfunction.
GAIT EVALUATION The evaluation of gait is discussed in detail in Chapter 5, but a brief outline is presented here. The child should be asked to walk back and forth normally, preferably in a corridor, and up and down steps. The examiner should observe whether the gait is wide or narrow based, whether there are symmetric reciprocal movements of the arms, and whether the legs and feet move in a symmetric and normal fashion. The child should also be asked to run because running exaggerates neurologic impairment. Flexion or extension of an arm with subsequent athetosis not present during walking may be apparent during running.
34
Clinical Evaluation / 2
TABLE 2-6 Muscle Testing MUSCLE
INNERVATION
NORMAL FUNCTION
TEST*
Supraspinatus
C4–C5
Initiates arm abduction
Deltoid
C5–C6
Lower trapezius
C2–C4
Serratus
C5–C7
Infraspinatus Subscapularis and teres major Pectoral and latissimus dorsi Brachioradialis
C5 C5–C8 C5–C8 C5–C6 radial
Abduction of arm between 15 and 90 degrees Elevation of arm above shoulder Fixes the medial border of the scapula External rotation of the arm Internal rotation of the arm Adduction of the arm Flexion of elbow
Holding the patient at his or her side, have the patient attempt to abduct the limb Have the patient maintain abduction of arm at 45 degrees against resistance Have patient maintain elevation of arm above the shoulder against resistance Using position A, apply pressure in axis of the humerus
Biceps
Flexion of elbow
Triceps Pronators
C5–C6 musculocutaneous C7–C8 C6–C7
Supinators
C5–C6
Supinates forearm
Flexors of wrist
C7-median/ulnar
Extensors of wrist
C7-radial
Extensors of the digits
C7-radial
Flexors of fingers (grip) Adductor of thumb
C7-median/ulnar T1-ulnar
Opponens thumb
T1-median
Interossei
T1-ulnar
Extends forearm Pronates forearm
Extends fingers
Back muscles
Extends the back
Abdominal muscles
Contracts the abdominal wall
Intercostal muscles
Raises the rib cage
Diaphragm
C4
Iliopsoas
L2 femoral
Participates in respiration and facilitates coughing Flexion of hip on abdomen
Adductors of hip
L2–L3 obturator
Adducts leg at the hip
Gluteus medius and minimus
L4–L5
Abduction of leg at the hip
Quadriceps Hamstrings Tibialis anticus
L3 femoral S1–S2 sciatic L4 peroneal
Extension of the knee Flexors of the knee Dorsiflexion of the foot
Triceps surae
L5–S2 tibial
Plantar flexion of the foot
Posterior tibial
L4 tibial
Inverts the foot
Peroneals
L5 peroneal
Everts the foot
Dorsiflexors of toes
S1 peroneal
Plantar-flexors of toes
S2 tibial
Gluteus maximus
S1–S2
*Use this table in conjunction with Figure 2-10.
Extension of the leg at the hip
Using position A, apply downward pressure on forearm Using position A, pull the wrist away from the body Using position A, abduct the arm in the midaxillary line Using position A, (forearm must be pronated), push downward at the wrist Using position A but with forearm supinated, push downward at wrist Using position A, push upward at wrist Using position A, rotate forearm so the upper border of the hand turns outward Using position A, rotate the forearm so that the upper border of the hand turns inward Using position A but with hand supinated, push down on the palmar surface of the hand Using position A but with hand pronated, push down on the dorsal surface of the hand Using position A but with hand pronated, push down on the first phalanx of each digit Using position A, have patient squeeze hard Using position A, with thumb adducted, pull upward on the thumb Using position A with hand supinated, have patient resist the separation of the tip of the little finger from the tip of the extended thumb Using position A but with hand supinated and fingers spread apart, attempt to approximate the fingers Using position C, place hand beneath patient’s back and have the patient arch the back With patient in supine position, place hand on patient’s abdomen and have patient attempt to rise from a recumbent position With patient in supine position, observe action of intercostals on deep inspiration; observe excursion and observe for symmetry of excursion of chest Have patient cough and observe the epigastric impulse Using position B, place hand above knee and push downward Using position B, place hand on the medial surface of the thigh and push inward Using position B, place hand on outer aspect of the thigh and push outward Using position B, attempt to further flex the leg at the knee Using position B, attempt to extend the leg at the knee Using position C, place hand on the dorsal surface of the foot and push in a plantar direction Using position C, place hand on ball of foot and push in the direction of the patient Using position C, grasp the foot at the arch and rotate so that the plantar surface turns outward Using position C, grasp the foot at the arch and rotate so that the plantar surface turns inward Using position C, push in a plantar direction against the dorsal surface of the toes Using position C, place hand on the plantar surface of the toes and push in the direction of the patient With patient lying on the side and with the lower limbs maintained in normal extension, place hand on back of thigh and push forward
Swaiman / Neurologic Examination of the Older Child
Among the abnormal gaits are those that can be characterized as cerebellar, spastic, waddling, and steppage. These gait types are discussed further in Chapter 5. REFERENCES Baker AB. An outline of clinical neurology. Dubuque, Iowa: William C Brown, 1958. Cogan DG. Neurology of the ocular muscles. Springfield, Ill: Charles C Thomas, 1966. Cope EB, Antony JH. Normal values for two-point discrimination. Pediatr Neurol 1992;8:251. Frankenburg WK, Dodds JB, Archer P, et al. The Denver II: A major revision and restandardization of the Denver Developmental screening test. Pediatrics 1992;89:91. Golumb MR, Garg BP, Williams LS. Measuring gross motor recovery in young children with early brain injury. Pediatr Neurol 2004;31:311 Haymaker W. Bing’s local diagnosis in neurological diseases, 15th ed. St. Louis: CV Mosby, 1969. Haymaker W, Woodhall B. Peripheral nerve injuries. Philadelphia: WB Saunders, 1962. Hollinshead WH. Functional anatomy of the limbs and back. 3rd ed. Philadelphia: WB Saunders, 1969. Keegan JJ, Garrett FD. The segmental distribution of the cutaneous nerves in the limbs of man. Anat Rec 1948;102:409. Medical Research Council, War Memorandum No 7. Aids to the investigation of peripheral nerve injuries. 2nd ed. London: His Majesty’s Stationery Office, 1943. (Reprinted 1960.) Smith JL, ed. Neuro-ophthalmology: Symposium of the University of Miami and the Bascom Palmer Eye Institute, Vol. 3. St. Louis: CV Mosby, 1967. Zafeiriou DI. Primitive reflexes and postural reactions in the neurodevelopmental examination. Pediatr Neurol 2004;31:1.
SUGGESTED READING Brett EM. Normal development and neurological examination beyond the newborn period. In: Paediatric Neurology, 3rd ed. London: Churchill Livingstone, 1997.
35
Dekaban A. Examination. In: Dekaban A, ed. Neurology of early childhood. Baltimore: Williams & Wilkins, 1970. Dodge PR. Neurologic history and examination. In: Farmer TW, ed. Pediatric neurology. New York: Paul B Hoeber, 1964. Egan DF. Developmental examination of infants and preschool children. Clinics in developmental medicine, no. 112. Oxford: MacKeith Press, 1990. Fenichel GM. Clinical pediatric neurology: a signs and symptoms approach, 3rd ed. Philadelphia: WB Saunders, 1997. Fenichel GM. The neurological consultation. In: Fenichel GM, ed. Neonatal neurology, 3rd ed. New York: Churchill Livingstone, 1990. Haerer AF. Dejong’s the neurologic examination. Philadelphia: Lippincott, 1992. Illingworth RS. The development of the infant and young child, 9th ed. Baltimore: Williams & Wilkins, 1987. Kestenbaum A. Clinical methods of neuro-ophthalmologic examination. New York: Grune & Stratton, 1961. Menkes, JH, Sarnat HB. Textbook of Child Neurology, 6th ed. Baltimore: Williams & Wilkins, 2003. Nellhaus G. Composite international and interracial graphs. Pediatrics 1968;41:106. Paine RS. Neurologic examination of infants and children. Pediatr Clin North Am 1960;7:41. Paine RS. Neurologic conditions in the neonatal period: diagnosis and management. Pediatr Clin North Am 1961;8:577. Paine RS. The evolution of infantile postural reflexes in the presence of chronic brain syndromes. Dev Med Child Neurol 1964;6:345. Paine RS, Brazelton TB, Donovan DE, et al. Evolution of postural reflexes in normal infants and in the presence of chronic brain syndromes. Neurology 1964;14:1036. Paine RS, Oppe TE. Neurological examination of children. London: William Heinemann, 1966. Peiper A. Cerebral function in infancy and childhood. New York: Consultants Bureau Enterprises, 1963. Popich GA, Smith DW. Fontanels: Range of normal size. J Pediatr 1972;80:749. Sauer C, Levinsohn MW. Horner’s syndrome in childhood. Neurology 1976;26:216. Volpe JJ. The neurological examination: Normal and abnormal features. In: Volpe JJ, ed. Neurology of the newborn, 4th ed. Philadelphia: WB Saunders, 2001.
CHAPTER 3
Neurologic Examination after the Newborn Period until 2 Years of Age Kenneth F. Swaiman
Systematic acquisition of skills and responses results from maturation of physiologic processes and anatomic structures of the developing central and peripheral nervous systems. Adequate neurologic assessment depends on comparing the results of the infant’s examination with established norms (Table 3-1) [Gesell and Amatruda, 1956; Illingsworth, 1987; Zafeiriou, 2004]. Because it is critical that the infant remain calm and cooperative for the longest possible time during the examination, the least intrusive portions of the examination should be done first. A review of Chapter 2 can assist in understanding the material in this chapter.
APPROACH TO THE EVALUATION Experienced examiners develop individual approaches to and sequences for the evaluation [Brett, 1997]. Most schemes embody much of the following material. Although arbitrary, examination of the infant can be subdivided into stages. Observation occupies most of the first stage. Some observations are made during the history-taking session. Caregivers should undress the child except for the undershirt, underwear, plastic pants, or diaper. The child should
TABLE 3-1 Child Development from 2 Months through 2 Years 2 Months Keeps hands predominantly fisted Lifts head up for several seconds while prone Startles in response to loud noise Follows with eyes and head over 90-degree arc Smiles responsively Begins to vocalize single sounds 3 Months Occasionally holds hands fisted Lifts head up above body plane and holds position Holds an object briefly when placed in hand Turns head toward object, fixes and follows fully in all directions with eyes Smiles and vocalizes when talked to Watches own hands, stares at faces Laughs 4 Months Holds head steady while in sitting position Reaches for an object, grasps it, brings it to mouth Turns head in direction of sound Smiles spontaneously 5 to 6 Months Lifts head while supine Rolls from prone to supine Lifts head and chest up in prone position Exhibits no head lag Transfers object from hand to hand Babbles Sits with support Localizes direction of sound 7 to 8 Months Sits in tripod fashion without support Stands briefly with support Bangs object on table Reaches out for people Mouths all objects Says “da-da,” “ba-ba” Data from Frankenburg et al, 1981; Illingsworth RS, 1987; Knobloch H et al, 1980.
9 to 10 Months Sits well without support, pulls self to sit Stands holding on Waves “bye-bye” Drinks from cup with assistance Uses pincer grasp 11 to 12 Months Walks with assistance Uses two to four words with meaning Creeps well Assists in dressing Understands a few simple commands 13 to 15 Months Walks by self, falls easily Says several words, uses jargon Scribbles with crayon Points to things wanted 18 Months Climbs stairs with assistance, climbs up on chair Throws ball Builds two- to four-block tower Feeds self Takes off clothes Points to two or three body parts Uses many intelligible words 24 Months Runs, walks up and down stairs alone (both feet per step) Speaks in two- or three-word sentences Turns single pages of book Builds four- to six-block tower Kicks ball Uses pronouns “you,” “me,” and “I”
38
Clinical Evaluation / 3
remain on the caregiver’s lap. At first the clinician should continue questioning the caregivers about pertinent aspects of the history. Usually, the child becomes reassured that the clinician means well. Observation allows limited assessment of cranial nerve function, unusual facies, gross structural deformities (including those of the head and neck), symmetry of strength and movements of the extremities, and unusual posturing. At the beginning of the second stage, while the child remains on the caregiver’s lap, the head, deep tendon reflexes, muscle tone, superficial and deep sensation, gross response to sound, and visual fields can be evaluated. Examination of the plantar responses (e.g., Babinski’s reflex) also can be done. The caregiver is then asked to undress the child completely, and the child is placed on a table. During this segment of the examination, more interactive assessment of muscle function and further assessment of the developmental reflexes, traction response, parachute response, and sitting and standing abilities takes place. The sensory examination is best done at this time. The third stage may require help from a caregiver or assistant. At this time, examination of the abdomen, genitalia, back, and anal area is accomplished. Examination of the mouth, tongue, and sternocleidomastoid muscles should also be done. If previously deferred, measurement of the occipitofrontal circumference (OFC) is mandatory. The fundi and ears are examined. At the beginning of the fourth stage of the examination, the child is placed on the floor so that assessment of crawling, walking, and running can be accomplished.
EVALUATION OF THE PATIENT Stage 1 Stage 1 of the evaluation should be done with ease in the approach. The examiner should avoid quick movements or display of instruments that could be interpreted as threatening. Smiling at the infant and speaking in soft and reassuring tones are highly effective methods. The child should sit on the caregiver’s lap and face the examiner. It is preferable that the child be placed in this position during the history-taking session so that familiarity with the examiner and the room is developed. Observations made of the child while in this position during the initial conversation may provide much information to the skilled examiner. The sequence of examination should be flexible and should be determined by the child’s comfort and temperament and by the natural postures and positions assumed by the child. The examiner must be highly sensitive to the child’s mood and defer those parts of the examination that appear to upset the child until last. Flexibility on the part of the examiner may be the key to a successful session. Nevertheless, a reasonably complete examination should be done. The clinician must not lose sight of the need for all pertinent data to be collected. It is imperative that the clinician systematically conduct that portion of the examination related to the chief complaint. The clinician should make judgments concerning the facial and extraocular movements and the asymmetry and
character of limb movements. The child’s state of alertness, awareness of surroundings, and affect should be evident. The child’s vocalization should be age appropriate.
Head Examination of the head must be done systematically, and the examiner should observe for asymmetry, indentations, and protuberances. Evaluation of all the cranial sutures and associated fontanels can be carried out by gentle palpation. The dimensions of the anterior fontanel should be carefully recorded [Popich and Smith, 1972]. The examiner should determine by observation and palpation the presence of suture synostosis, suture separation, a bulging fontanel, frontal bossing, and unusual shapes of the head, including trigonocephaly, marked dolichocephaly or brachycephaly, and plagiocephaly. If the child is comfortable, the occipitofrontal circumference should be measured. If the child becomes agitated from placement of the tape measure, the measurement should be deferred until later (stage 3). The largest measured circumference should be recorded and plotted on a standardized graph of normative data. (When hydrocephalus is suspected in the early months of life, studies using ultrasonography, computed tomography [CT], or magnetic resonance imaging [MRI] should be obtained.) Simultaneously, unusual masses under the scalp and gross asymmetries of the skull should be sought. If possible, the tenseness of the anterior fontanel should be evaluated when the child is held in an upright position. The size of the anterior fontanel varies [Popich and Smith, 1972]. The anterior fontanel pulsates in unison with the heartbeat, becomes fuller or bulging when the child cries, and may be full in disease states in which there is increased intracranial pressure. The posterior fontanel usually admits only a finger at time of birth and usually is not palpable by the time the child is 2 months old. Other fontanels are usually difficult to palpate readily, except in pathologic states. Occasionally, accessory fontanels may be found along the sutures, particularly the sagittal suture. They usually are benign abnormalities. The cranium is auscultated for the presence of unusual intracranial bruits. However, intracranial bruits occur commonly in childhood, and cautious interpretation is advised. Asymmetric bruits and those that can be suppressed by carotid artery suppression are frequently pathologic. Vascular abnormalities, such as vein of Galen malformations, produce extremely loud bruits. The vein of Galen malformation is associated with increasing occipitofrontal circumference, high-output cardiac failure, and infant distress while in the supine position. The child also may have seizures. Ultrasound and CT examinations of the newborn brain may provide information about the presence of hemorrhage, ventricular size, and amplitude of cerebral pulsations. MRI evaluation is often feasible but may require sedation at this age. Sometimes, when more sophisticated methods are not readily available, the use of transillumination with a flashlight may suggest the presence of a fluid compartment within the brain or over the cortical mantle. Such findings are associated with hydranencephaly, porencephaly, subdural effusions, caput succedaneum, hydrocephalus, and infiltrated intravenous sites.
Swaiman / Neurologic Examination after the Newborn Period until 2 Years of Age
Cranial Nerves Examination of cranial nerve function can be done primarily through observation. More details concerning examination of each cranial nerve can be found in Chapter 2. Using bright objects facilitates the assessment of extraocular muscle movements. Nystagmus and strabismus may be detected during this portion of the examination. If the child appears uninterested in bright objects, the possibility of a visual defect or an underlying intellectual defect must be considered. Rolling movements of the eyes and dysconjugate gaze suggest gross visual impairment. Double simultaneous stimulation—bringing two bright objects into different visual fields (one in each temporal area) simultaneously—normally causes the child to look from one object to the other. Failure to take notice of one object may indicate homonymous hemianopsia. A tape with repetitive bars or objects should be drawn horizontally and then vertically across the child’s field of vision. Lack of opticokinetic response results from lack of visual fixation or from gross impairment of vision. Unusual transient deviations of the eyes may occur in the first year of life [Echenne and Rivier, 1992]. A beam from a small flashlight should be directed at each eye to allow evaluation of pupillary responses, anisocoria, and the red retinal reflex. The examiner should initially direct the light beam at the child’s hand or abdomen so that the child is aware of the safety of the procedure. The presence of abnormalities, such as symmetry of the palpebral fissures, the relative size of the two globes, the angulation of the eyes compared with other facial components and with the ears, cataracts, conjunctival telangiectases, colobomas of the iris, ptosis, proptosis, and malformed or eccentrically placed pupils, can be determined at this time. Hair color, patterning distribution, and texture should be assessed. During the entire examination, the examiner should observe the child’s facial movements closely. Smiling at the child, tickling the child, or making unusual noises or facial grimaces often causes the child to smile or laugh, allowing observation of the nasolabial folds. The presence of facial weakness from central or peripheral cranial nerve VII dysfunction should be determined. Widening of the ipsilateral palpebral fissure is indicative of facial nerve weakness. It is essential that the examiner distinguish between central and peripheral facial nerve palsies; the latter include involvement of the muscles of the forehead. In the younger infant, sucking and rooting reflexes can be obtained. Tongue thrusting, drooling, and unusual shapes of the lips should be evident. Sometimes, the child can be induced to protrude the tongue if the examiner urges the child to imitate the examiner’s tongue movements. Deformity, atrophy, or abnormal positioning of the tongue can be observed. Basic responses to rubbing together of the fingers, ringing a bell, or using a toy noisemaker that generates noise at a modest volume may provide much information. A tuning fork may also be used. The examiner must be careful not to confuse response to a visual cue (e.g., the movement needed to elicit noise from a toy) for response to the sound. The infant turns the head toward the sound, and there is arrest of motor activity. A child older than 6 months usually reaches for the noisemaker. If the child fails to perform
39
satisfactorily, formal audiometry and auditory-evoked response testing should be obtained.
Motor Evaluation Observation is the most efficacious approach in motor evaluation. The examiner should systematically observe the symmetry of movements of arms and legs and notice any gross discrepancies in muscle bulk or limb length. Definite hand preference before 24 months suggests a central or peripheral nervous system impairment of the opposite hand and arm. In this situation, leg movement and use should be carefully studied to detect the presence of hemiparesis. Most commonly, there is also a decrease in spontaneous movement of the affected limb. Unusual posturing of the limbs may indicate paresis or incipient extrapyramidal disease. Evaluation of muscle tone, the resistance of muscle to passive stretch, is an important facet of the motor examination. The muscle tone of the arms and legs can be assessed by the examiner gently shaking and moving the feet and hands while the child is relaxed. Tone and range of motion can be assessed by shaking the arms and hands about the various joints. Pronation and supination of the hands and forearms provide further information about range of motion and the possibility of spasticity or rigidity. Greater than normal resistance indicates increased tone, whereas less than normal resistance indicates decreased tone. This portion of the examination is most difficult for the novice because reasonable experience is required to make accurate judgments. Limitation of movement may also indicate joint contracture. During the examination, the infant may well resist attempts to move the arms, providing the examiner with some sense of muscle strength. Spontaneous muscle movements, particularly those against gravity, provide the most information concerning muscle strength. Upper motor neuron unit involvement, such as that in hemiparesis, may manifest by limited flexion of the arm at the elbow, decreased movement of the extremity, persistent fisting, and adduction of the thumb against the palm. Patients with brachial plexus injury of Erb’s type often hold the arm in a position of internal rotation and adduction at the shoulder. Interaction with the infant by using toys and other interesting objects may help to evaluate limb strength, range of motion, and coordination of limb movements. If the child is sufficiently cooperative, individual muscle testing, when appropriate, should be carried out. There is a normal sequence as the child becomes more adept at grasping objects with the hands. Grasping an object with both hands and holding the object before the face, transferring the object from hand to hand, and placing the object in the mouth all provide information concerning the infant’s motor control. The infant’s grasping skills are best demonstrated when progressively smaller objects are presented. When 4 to 5 months old, the child is able to grasp an object with the entire hand (Fig. 3-1); at 7 months, the grasp is done by the thumb and the neighboring two fingers (Fig. 3-2); and the pincer grasp, in which the thumb and forefinger are used, should be present by 9 to 11 months (Fig. 3-3). The palmar grasp reflex (i.e., obligate grasp reflex) should gradually diminish from 3 to 6 months of age. The persistence of the obligate grasp reflex beyond 6
40
Clinical Evaluation / 3 FIGURE 3-1. Entire hand grasp of 4-month-old infant. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
FIGURE 3-2. Use of two fingers and thumb in the grasp of a 7-month-old infant. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
months of age may signal corticospinal tract dysfunction. Observation of the child’s ability to raise the arms and to abduct and adduct the arms while reaching for a proffered object provides valuable information concerning proximal muscle strength. Simultaneously, the presence of intention tremor and of the avoidance response of early athetosis may be evident. Congenital malformations of the fingers and hands can be readily determined during this portion of the examination. Examination of the hips should include assessment of range of motion; decreased excursion may signify spasticity or subluxation of the hip joints. Subluxation may exist separately or as a result of spasticity. Initially, examination of the legs should consist of evaluation of muscle symmetry and mass. The presence and symmetry of spontaneous motor movements should be evaluated. Assessment of tone is similar to that done with the arms and hands. Gently shaking the feet and movements about the hip and knee joints are monitored. Tightness of the Achilles tendon should also be evaluated. Decreased range of motion and inability of the feet to readily dorsiflex beyond 90 degrees are abnormal. Deep tendon reflexes that are very brisk may indicate upper motor neuron unit disease. Asymmetry is particularly worrisome because of the association with pathologic
FIGURE 3-3. Pincer grasp with the thumb and forefinger of an 11-month-old infant. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
conditions. Absent deep tendon reflexes are likely to be associated with anterior horn cell disease or peripheral neuropathy. The crossed adductor reflex is elicited when the patellar reflex is stimulated and resultant contraction of the adductor muscles occurs in the opposite leg. This response is normal until approximately 1 year of age. When this response persists, particularly unilaterally, it suggests the presence of corticospinal tract difficulty. Elicitation of the plantar response is as important in children as in adults. There is no consensus of opinion about the latest time at which an extensor response is detectable. At least in one report, an extensor response was obtained in 50% to 75% of 1-year-old infants [Dodge, 1964]. Using careful techniques, Hogan and Milligan [1971] found that the initial response is flexor in 93% of normal infants. In this study, the claim was made that the usual response in the newborn period is flexor in origin. This report contrasts with the experience of many examiners. In any event, asymmetric extensor toe signs or extensor toe signs that persist beyond the age of 1 year should be considered pathologic. Pathologic toe signs are indicative of upper motor neuron unit disease. Ankle clonus is often present in the neonatal period; it is rarely sustained. There are usually three to six beats of ankle clonus. Ankle clonus should disappear by 2 months of age. The persistence of ankle clonus and extensor toe signs suggests the possibility of upper motor neuron unit disease. Cerebellar function is difficult to assess and requires an interchange of objects between infant and examiner and observation of the infant during play to monitor tremor, dysmetria, truncal sway while sitting, and fine motor coordination. Titubation may be evident. Decreased tone may accompany cerebellar dysfunction but has many other causes.
Sensory Testing The patient should respond to stroking of the extremities by awareness and by withdrawal of the limbs. The infant should also acknowledge the sensory contact by eye deviation and facial responses. Using a tuning fork with contact over bony
Swaiman / Neurologic Examination after the Newborn Period until 2 Years of Age
41
FIGURE 3-4. Segmental distribution of the cutaneous nerves of an infant. (Modified from Fanaroff AA, Martin RJ. Neonatal-perinatal medicine: Diseases of the fetus and infant, 5th ed. St Louis: CV Mosby, 1992.)
C4 13 5 C5
C4 4 T2 6
C4 T2 C6
7 8 9
T1
11 C7
L1 L2
10
C6
12
C3 C4 C5 T3 5 7 T1 9 11 L1
4 6 8 10 12
L2
C8
C7
L1
C8 L2
S4 S5
C7 L2 S2
L3 L4
S3 L3 L2
L3 L4
L5
L5 L5
S1
S1
areas often causes arrest of motion and a wide-eyed look of wonder in the child who cannot otherwise describe the sensation. Proprioception cannot be directly evaluated at this age, but observations of sitting positions, gait, and posture may provide some clues about normality of function. Stroking of the skin may elicit a response and provide information about light touch perception (Fig. 3-4). Using a pin or gentle pinching for pain evaluation should be reserved until late in the examination; careless use of the pin can destroy rapport with the patient. The child may cry or make short, whimpering sounds. Decreased muscle bulk may not be appreciated because of the large amount of subcutaneous fat, and muscle atrophy may be undetected. The examiner should be careful to palpate muscle mass beneath the fat and not misinterpret the subcutaneous tissue as muscle. The skin of the infant is observed for obvious areas of abnormality that may suggest certain conditions, including neuroectodermal neurocutaneous disorders. Examination of the spine may indicate the presence of scoliosis, sinus tracts, scars, dimples, and hemangiomas. Unusual skin lesions or hair growth over the spine suggest the presence of an underlying mesodermal defect, including diastematomyelia. The spine should be palpated along its entire course for defects. Abdominal and cremasteric reflexes are present at birth. The abdominal reflex is elicited by stroking the skin of the upper, middle, and lower portions of the abdomen. Each stroke elicits a muscle contraction mediated by a different group of thoracic and lumbar nerves. The response results in the retraction of the umbilicus toward the stimulated side. The various spinal cord segmental levels involved in the reflex range from T8 to T12. The cremasteric reflex is elicited by stroking the inner thigh, beginning 3 to 5 cm below the inguinal crease. The cremasteric reflex results in an elevation of the testicles
S1
because of contraction of the overlying smooth muscles. Cremasteric reflexes are mediated by spinal nerves L1 and L2.
Stage 2 For stage 2 of the evaluation the child should be placed on a table with the caregiver standing close by for reassurance to the child and assistance, if necessary, to the examiner. Motor evaluation can be carried out on an examining table or on a larger, carpeted surface. By 3 months of age, an infant can hold the head and chest off the table while in the prone position. Good head control while sitting with support is evident by 4 months of age. The child should be able to sit without support and maintain adequate balance by 8 to 9 months of age. Unassisted assumption of the sitting position should occur by 10 months of age. The child should crawl by 10 months, pull to a standing position by 10 months, and creep by 11 months. The child should walk with support by 12 months and without support by 13 to 14 months. Lack of these abilities should be evaluated in concert with other findings. Trunk, shoulder, and pelvic girdle tone and strength should be evaluated further. The child is observed while held in vertical and horizontal suspension. A hypotonic child, when held in horizontal suspension, often droops over the examiner’s arm [Paine, 1960]. In vertical suspension, the child may slide through the examiner’s hands. The child may be unable to maintain a standing posture when the feet are placed on the table surface. Increased tone, or hypertonicity, usually the result of spasticity, may manifest by a backward curve of the extended head, neck, and back while in horizontal suspension. The legs may be extended and may “scissor” while the child is in vertical suspension, and the child may stand on the toes when the feet are allowed to touch the table (Fig. 3-5).
42
Clinical Evaluation / 3 FIGURE 3-5. Extended legs, scissoring, toe stance, and fisting in an infant with spastic quadriplegia. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
TABLE 3-2 Most Commonly Used Motor Performance Tools Developmental Scales Amiel-Tison [Amiel-Tison, 1968] Amiel-Tison [Amiel-Tison, 2002] Bayley [Bayley, 1961] Brazelton [Brazelton and Nugent, 1995] Dubowitz [Dubowitz et al., 1999] Haataja [Haataja et al., 1999] Peabody [Reed, 1985] Prechtl [Prechtl and Beintema, 1964] Developmental Screening Tests Denver Developmental Screening Test (Denver II) [Frankenburg et al., 1992] Battelle Screening Test [Glascoe and Byrne, 1993] Clinical Adaptive Test (CAT)/Clinical Linguistic and Auditory Milestone Scale (CLAMS) [Leppert et al., 1998] Knobloch Revised Screening Inventory [Knobloch et al., 1980] General Movements (GMs) Assessment [Dargassies 1997; Prechtl 1997; Prechtl et al., 1997]
Motor Performance Instruments Through the years, several instruments have been devised that are useful for evaluating motor performance in relation to chronologic age. These instruments have provided norms for evaluating expected rate of motor development for a number of different assessments and maneuvers [Zafeiriou, 2004]. The instruments that are most commonly used are found in Table 3-2.
Motor Assessment Instruments Alberta Infant Motor Scale (AIMS) [Piper et al., 1992] Early Motor Pattern Profile (EMPP) [Morgan, 1988] Gross Motor Function Measure (GMFM) [Russell et al. 2002] Movement Assessment Inventory (MAI) [Kaye and Whitfield, 1988] Test of Infant Motor Performance (TIM) [Campbell et al., 1993] Adapted from Zafeiriou DI. Primitive reflexes and postural reactions in the neurodevelopmental examination. Pediatr Neurol 2004;31:1.
Developmental Reflexes Developmental reflexes are patterned responses that are achieved by certain ages. General development of the nervous system can be assessed by eliciting these reflexes. Occasionally, they may have localizing value, but usually, they do not. The abnormalities may be the continued presence of a reflex that should have dissipated, absence or poor manifestation of the expected response, or a response that is not symmetric. These reflexes and means of elicitation are listed in Tables 3-3 and 3-4 [Zafeiriou, 2004]. Although the Moro reflex may be demonstrated by several maneuvers, essentially, the position of the head in relation to the trunk must be altered in the supine position. Eliciting this reflex is correctly done while the child is in the supine position; the head is lifted off the padded examining table and then allowed to fall approximately 30 degrees in relation to the trunk [Parmelee, 1964]. The examiner should allow the head to fall onto his or her hand. The expected response is extension and abduction of the arms and extension of the fingers. This posturing is followed by adduction of the arms at the shoulder. The child often emits a cry (Fig. 3-6). An abnormality in the Moro reflex does not signify a specific area of involvement but rather a diffuse process, usually depression of the central nervous system (CNS). Generalized weakness or severe spasticity may also cause limitation of the Moro reflex. If the Moro reflex is asymmetric, motor abnormalities, such as Erb’s and Klumpke’s
FIGURE 3-6. The Moro response to rapid extension of the neck in a 2-dayold infant. The abduction phase of arm movement is illustrated. A cry usually accompanies the response, and the leg position varies.
brachial plexus palsies, or fractures of the humerus or clavicle should be considered [Dekaban, 1970]. Spastic hemiplegia may also result in an asymmetric Moro reflex. An exaggerated Moro reflex may indicate pathologic CNS irritability. Although the Moro reflex usually exists in children up to 5 or 6 months old, the manifestation of the reflex changes with maturation. When children are 2 months old, the Moro reflex is incomplete. The usual pattern is that the adduction phase is greatly attenuated. The tonic neck reflex reaches a peak when the child is 2 months old but may be detected in the neonatal period. The
Swaiman / Neurologic Examination after the Newborn Period until 2 Years of Age
43
TABLE 3-3 Eliciting Primitive Reflexes Reflex
Position
Method
Response
Age at Disappearance
Palmar grip Plantar grip
Supine Supine
Flexion of fingers, fist making Flexion of toes
6 months 15 months
Galant
Prone
Asymmetric tonic neck
Supine
Placing the index finger in the palm of the infant Pressing a thumb against the sole just behind the toes Scratching the skin of the infant’s back from the shoulder downward, 2-3 cm lateral to the spinous processes Rotation of the infant’s head to one side for 15 seconds
Suprapubic extensor
Supine
Pressing the skin over the pubic bone with the fingers
Crossed extensor
Supine
Passive total flexion of one lower extremity
Rossolimo
Supine
Heel
Supine
Moro
Supine
Babinski
Supine
Light tapping of toes 2 through 4 at their plantar surfaces Tapping on the heel with a hammer, with the infant’s hip and knee joints flexed and the ankle joint in neutral position Sudden head extension produced by a light drop of the head Striking along the lateral aspect of the sole, extending from the heel to the head of the fifth metatarsal
Incurvation of the trunk, with the concavity on the stimulated side
4 months
Extension of the extremities on the chin side and flexion of those on the occipital side Reflex extension of both lower extremities, with adduction and internal rotation into talipes equinus Extension of the other lower limb, with adduction and internal rotation into talipes equinus Tonic flexion of the toes at the first metacarpophalangeal joint Rapid reflex extension of the lower extremity in question
3 months
Abduction followed by adduction and flexion of upper extremities Combined extensor response: simultaneous dorsiflexion of the great toe and fanning of the remaining toes
6 months
4 weeks 6 weeks 4 weeks 3 weeks
Presence always abnormal
Data from Futagi et al., 1992; Vojta 1988; Zafeiriou DI, 2004; Zafeiriou et al., 1995; Zafeiriou et al., 1999a; Zafeiriou et al., 1999b; Zafeiriou et al., 2000.
TABLE 3-4 Eliciting Postural Reactions Reaction
Position
Method
Traction
Supine
Horizontal suspension
Prone
Vertical suspension
Vertical
Vojta response
Vertical
Collis horizontal suspension
Prone
Collis vertical suspension
Prone
Peiper-Isbert vertical suspension
Prone
Placing the examiner’s index finger in the infant’s hand and pulling the infant at a 45-degree angle to the examination bed Suspending the infant by placing the hands around the infant’s thorax without providing support for the head or legs Placing both hands in the axillae without grasping the thorax and lifting the infant straight up facing the examiner Suspension from the vertical to the horizontal position facing the examiner by placing both hands around the infant’s thorax Placing one hand around the upper arm and the other around the upper leg and suspending the infant in the horizontal position, parallel to the examination bed Placing one hand around the upper leg and suspending the infant in the vertical position with the head directed downward Placing the examiner’s hands around the upper leg of the infant and suspending the infant in the vertical position with the head directed downward
Data from Vojta, 1988; Zafeiriou et al., 1998; Zafeiriou, 2004.
reflex gradually diminishes and is absent in children 6 months of age and older. To elicit the reflex, the head is turned to one side while the child is supine and the shoulders fixed. The arm and leg on the side toward which the face is turned extend, and the arm and leg on the opposite side flex. The degree of response varies widely but is usually symmetric. In any event, a normal infant does not remain in the reflex position when the reflex is elicited. If the struggling infant does not escape the reflex response, the response is abnormal. The response should not exist beyond 6 months of age [Paine et al., 1964]. A unilateral reflex may indicate a lesion in the hemisphere opposite the direction in which the face is turned. The same consideration holds true if the response is
obligate or persists beyond the expected age. The weak child may also have an abnormal response secondary to central or peripheral motor unit involvement. Sitting or standing is impaired when the child has an overactive tonic neck reflex. Athetoid and spastic infants may also have an exaggerated response. An object or the examiner’s finger is placed in the palm of the infant’s hand to elicit the palmar grasp reflex. The child has an involuntary flexion response and grasps the object. This reflex subsides by 3 to 6 months of age, and voluntary grasping is evident. The obligatory involuntary grasp reflex may persist and often indicates infantile hemiplegia [Paine, 1964].
44
Clinical Evaluation / 3
To elicit the Landau reflex, the infant is held prone in horizontal suspension by the examiner. The examiner flexes the infant’s head. Flexion of the legs and trunk is the normal response. This response is present in most infants by 5 months of age and absent by 2 years of age [Cupps et al., 1976]. Virtually all normal infants have a positive Landau response by 10 months of age. When held in horizontal suspension, 55% of infants spontaneously elevate their heads above the horizontal plane by age 5 months and 95% by 6 months [Paine et al., 1964]. The placing reflex response can be demonstrated by holding the upright infant in a manner that causes the dorsal surface of the infant’s feet to touch the underside of a tabletop. The infant flexes the legs at the hips and knees so that contact with the underside of the surface ceases. One of the most useful maneuvers is the traction response. The response is elicited while the infant is lying supine. The examiner grasps each hand of the infant and pulls the infant gently and slowly, allowing the infant to assist, to a sitting position. Marked head lag with little resistance to the examiner’s pulling efforts is present in the newborn period (Fig. 3-7). After a month or so, when the child comes forward, the infant’s head comes forward with neck flexion and then transiently is extended at the neck. Usually by 3 to 5 months of age at the latest, the infant is able to pull against the examiner with arm flexion at the elbow, hold the head and trunk in a straight line, and otherwise actively participate while the examiner pulls the infant to the upright position. No head lag is observed, and little or no forward motion of the head occurs as the child reaches the upright position. Asymmetry signals a neurologic difficulty. A traction response, in which the infant is brought to a sitting position only transiently followed by rapid assumption of a standing position because the legs are extended at the hips and knees, suggests bilateral corticospinal tract difficulty. A valuable measure of vestibular function in the newborn can be obtained by holding the infant in a supine position; the feet are closest to the examiner. The examiner, with the infant lying on the arm, rotates in one direction and then reverses direction. The eyes of the infant deviate in the
FIGURE 3-7. The traction maneuver causes little response in a 2-day-old infant. There is little or no perceptible flexion of the neck or the arms at the elbows.
direction of rotation accompanied by intermittent nystagmus to the opposite side. Extraocular movements may also be assessed during this maneuver. It is essential that the examiner take into account the overall pattern of developmental responses. An abnormality of one reflex does not indicate significant neurologic abnormality. There are other developmental reflexes, but those discussed here appear to be the most often evaluated and the most useful.
Stage 3 Examination of the optic fundi should be carried out with the infant supine on the table, on the caregiver’s lap, or sometimes held over the caregiver’s shoulder with the infant’s head held tightly to the caregiver’s head. Abnormalities of the fundi, including vascular changes, abnormalities of the optic disc, retinal changes, and abnormalities of the lens and media, should be sought (see Chapter 6). Mydriatic agents are rarely needed, although both mydriatic agents and sedation occasionally are necessary. During the first few months of life, the optic discs may be somewhat gray. This normal finding should not be confused with optic atrophy. Changes in the retina include chorioretinitis and retinitis pigmentosa. The discs may be hypoplastic or swollen. The general portion of the examination follows. The presence of hepatosplenomegaly should be determined because many storage diseases, which also affect the brain, may be the cause of organ enlargement. The anal sphincter should be examined for tone and the presence of an anal cutaneous reflex. Congenital anomalies of the genitalia should be sought. The remainder of the general examination, particularly the intrusive aspects, such as evaluating the auditory meati, tympanic membranes, mouth, and teeth, should be done at this time.
Stage 4 If the child crawls, stands, or walks, the child should be placed on the floor. If the child crawls, the floor should be carpeted or a suitable pad should be provided. The child should be encouraged to crawl, walk, or run by rolling a ball across the room or sliding an object such as a block across the floor. Waddling, footdrop, limp, or ataxia may be evident. The manner in which the child stoops and bends to retrieve a ball or block may show premature hand dominance, athetosis, tremor, or weakness of the legs. The child should be observed when arising from the floor to a standing position to determine the presence of Gowers’ maneuver (see Fig. 2-11). The clinician should make every attempt to evaluate the child’s gait to determine the presence of hemiparesis or ataxia (see Chapter 5). Unlike in the examination of adults, the testing of individual muscle groups in infants is usually impracticable. Nevertheless, evaluation of spontaneous movements and use of some specific maneuvers (e.g., traction response, wheelbarrow maneuver, arising from the floor) can provide information about spasticity, weakness, and incoordination. As is the case at all stages of childhood, a comparison of the examination findings must be made with expected norms. Further examination of muscle strength can be accomplished by using the parachute response; the examiner holds
Swaiman / Neurologic Examination after the Newborn Period until 2 Years of Age
45
General Considerations
FIGURE 3-8. Abnormal parachute response. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
the child in the prone position over an examining table and thrusts the patient toward the table surface. A fully developed response when the child is 8 months old consists of arm extension and extension of the wrists, allowing the palms of the hands to make contact with the table. The infant supports body weight with arms and shoulders. Each arm and shoulder can be tested individually if the opposite arm is pulled from the table by the examiner, forcing the child to support most of the body weight on one arm and shoulder. A somewhat older infant may be induced to “wheelbarrow” and move forward on the hands (Fig. 3-8), further demonstrating arm and shoulder strength (see Chapter 2). The child should then be invited to crawl. Formal individual muscle testing can be used in the older child whenever necessary. The sensory examination is difficult and is usually limited to rather gross evaluation of touch and pain; however, it can be accomplished with persistence and patience. Examination of touch, position sense, and vibration sense should be done first. When a tuning fork is placed on the appropriate bony prominence, a look of surprise—usually of bemusement—appears. Evaluation of pain should be done last and only after the examiner demonstrates to the child the method that will be used. The child should be asked to stand in one place with the feet together and then asked to close the eyes to be evaluated for Romberg’s sign. The examiner should observe the child for titubation of the head, nystagmus, and dysmetria while reaching for objects. Finger-to-nose and finger-to-fingerto-nose tests while the eyes are closed are frequently accomplished in children older than 3 years. The heel-toshin test is frequently not possible in children younger than 4 years. Depending on the maturity and abilities of the older infant, many of the maneuvers suggested in Chapter 2 for the older child are applicable. Assessment of the deep tendon reflexes is best carried out with the child in a caregiver’s or assistant’s lap. The biceps response in most infants is difficult to elicit, but the triceps and brachioradialis reflexes are usually detected. Patellar tendon and Achilles tendon responses are normally present and easy to elicit. Toe signs can be evaluated as in older children.
Throughout the examination, the clinician should evaluate the child’s alertness, interest in the surroundings, and ability to learn during the examination. The child’s speech pattern should also be assessed. By 15 months of age, the child should have spoken 2 to 6 words, and by 18 months, 2 to 20 words. Short phrases consisting of two or three words are usually part of the child’s repertoire by 21 to 24 months. By 2 years of age, most children have a vocabulary of up to 50 words. Using specific scales to evaluate intelligence and development levels is of some help but may not be reliable. It is therefore important that the examiner become proficient in informal means of assessing these characteristics. A new site, PediNeuroLogicExam (http://medstat.med.utah.edu/ pedineurologicexam/) provides text and movies demonstrating the changing examination as the child matures and the approach to examining the young patient. REFERENCES Amiel-Tison C. Neurological evaluation of the maturity of newborn infants. Arch Dis Child 1968;43:89. Amiel-Tison C. Update of the Amiel-Tison neurologic assessment for the term neonate or at 40 weeks’ corrected age. Pediatr Neurol 2002;27:196. Bayley N. The Bayley scales of infant development. New York: The Psychological Corporation 1969. Brazelton T, Nugent K. Neonatal Behavior Assessment Scale, 3rd ed. London: MacKeith Press, 1995. Brett EM. Normal development and neurological examination beyond the newborn period. In: Brett EM, ed. Paediatric Neurology, 3rd ed. London: Churchill Livingstone, 1997. Campbell S, Osten E, Kolobe T, et al. Development of the test of infant motor performance. Phys Med Rehabil Clin 1993;4:541. Cupps C, Plescia MG, Houser C. The Landau reaction: A clinical and electromyographic analysis. Dev Med Child Neurol 1976;18:41. Dargassies SS. Neurological development in the full term and premature neonate. New York: Excerpta Medica, 1997. Dekaban A. Examination. In: Dekaban A, ed. Neurology of Early Childhood. Baltimore: Williams & Wilkins, 1970. Dodge PR. Neurologic history and examination. In: Farmer TW, ed. Pediatric Neurology. New York: Paul B. Hoeber, Medical Book Department of Harper & Brothers, 1964. Dubowitz LMS, Dubowitz V, Mercuri E. The neurological assessment of the preterm and full-term infant, 2nd ed. London: MacKeith Press, 1999 Echenne B, Rivier E. Benign paroxysmal tonic upward gaze. Pediatr Neurol 1992;8:154. Fanaroff AA, Martin RJ. Neonatal-perinatal medicine: Diseases of the fetus and infant, 5th ed. St. Louis: CV Mosby, 1992. Frankenburg WK, Sciarillo W, Burgess D. The newly abbreviated and revised Denver Developmental Screening Test. J Pediatr 1981; 99:995. Frankenburg WK, Dodds J, Archer P, et al. The Denver II: A major revision and restandardization of the Denver Developmental Screening test. Pediatrics 1992;89:91. Futagi Y, Tagawa T, Otani K. Primitive reflex profiles in infants: Differences based on categories of neurological abnormality. Brain Dev 1992;14:294. Gesell A, Amatruda CS. Developmental diagnosis. New York: Paul B. Hoeber, Medical Books Department of Harper & Brothers, 1956. Glascoe F, Byrne KE. The usefulness of the Battelle Developmental Inventory Screening Test. Clin Pediatr 1993;32:237. Haataja L, Mercuri E, Regev R, et al. Optimality score for the neurological examination of the infant at 12 and 18 months of age. J Pediatr 1999;135:153. Hogan GR, Milligan JE. The plantar reflex of the newborn. N Engl J Med 1971;285:502. Illingsworth RS. The development of the infant and young child, 9th ed. Baltimore: Williams & Wilkins, 1987.
46
Clinical Evaluation / 3
Kaye L, Whitfield MF. The eighth month movement assessment of infants as a prediction of cerebral palsy in high-risk infants (Abstract). Dev Med Child Neurol 1988;30 (Suppl 57):11. Knobloch H, Stevens F, Malone A. The Revised Developmental Screening Inventory. Houston, Texas: Gesell Developmental Test Materials, 1980. Leppert MLO, Shank TP, Shapiro BK, et al. The Capute Scales: CAT/CLAMS—tool for the early detection of mental retardation and communicative disorders. Ment Retard Dev Disabl Res Rev 1998; 4:14. Morgan A. Early diagnosis of cerebral palsy using a profile of abnormal motor patterns. Dev Med Child Neurol 1988;30 (Suppl 57):12. Paine RS. Neurologic examination of infants and children. Pediatr Clin North Am 1960;7:41. Paine RS. The evolution of infantile postural reflexes in the presence of chronic brain syndromes. Dev Med Child Neurol 1964;6:345. Paine RS, Brazelton TB, Donovan DE. Evolution of postural reflexes in normal infants and in the presence of chronic brain syndromes. Neurology 1964;14:1036. Parmelee AH Jr. A critical evaluation of the Moro reflex. Pediatrics 1964;33:773. Piper MC, Pinnell LE, Darrah J, et al. Construction and validation of the Alberta Infant Motor Scale (AIMS). Can J Publ Health 1992; 83 (Suppl 2):46. Popich GA, Smith DW. Fontanels: Range of normal size. J Pediatr 1972;80:749. Prechtl H, Beintema D. Neurological examination of the full term infant. London: Heinemann, 1964. Prechtl HF. State of the art of a new functional assessment of the young nervous system. An early predictor of cerebral palsy. Early Hum Dev 1997;24:1. Prechtl HF, Eisenpieler C, Cioni G, et al. An early marker for neurological deficits after perinatal brain lesions. Lancet 1997;349:1361. Reed H. Review of Peabody developmental motor scales and activity cards. In: Mitchell J, ed. The ninth mental measurements yearbook. Lincoln: University of Nebraska Press, 1985:1119. Russell D, Rosenbaum PL, Avery LM, et al. Gross Motor Function Measure (GMFM-66 and GMFM-68). User’s manual. London: MacKeith Press, 2002. Vojta V. Die cerebralen Bewegungstoerungen im Kindesalter, 4te Auflage. Stuttgart: Ferdinand Enke Verlag, 1988. Zafeiriou DI. Plantar grasp reflex in high-risk infants at the first year of life. Pediatr Neurol 2000;22:75. Zafeiriou DI. Primitive reflexes and postural reactions in the neurodevelopmental examination. Pediatr Neurol 2004;31:1. Zafeiriou DI, Tsikoulas IG, Kremenopoulos GM. Prospective follow-up of primitive reflex profiles in high-risk infants: Clues to an early diagnosis of cerebral palsy. Pediatr Neurol 1995;13:148. Zafeiriou DI, Tsikoulas I, Kremenopoulos G, et al. Using postural reactions as a screening test to identify high-risk infants with cerebral palsy: A prospective study. Brain Dev 1998;20:307. Zafeiriou DI, Tsikoulas I, Kremenopoulos G, et al. Moro reflex profile in high-risk infants at the first year of life. Brain Dev 1999a; 21:216. Zafeiriou DI, Tsikoulas I, Kremenopoulos G, et al. Plantar response profile of high-risk infants at the first year of life. J Child Neurol 1999b;14:514.
SUGGESTED READING Dodge HW. Cephalic bruits in children. J Neurosurg 1956;13:527. Egan DF. Developmental examination of infants and preschool children. Clinical developmental medicine, No. 112. Oxford: MacKeith Press, 1990. Fenichel GM. Clinical pediatric neurology: A signs and symptoms approach, 3rd ed. Philadelphia: WB Saunders, 1997. Hack M, Mostow A, Miranda SB. Development of attention in preterm infants. Pediatrics 1976;58:669. Haymaker W. Bing’s local diagnosis in neurological diseases, 15th ed. St. Louis: CV Mosby, 1969. Kamin DF, Hepler RS, Foos RY. Optic nerve drusen. Arch Ophthalmol 1973;89:359. Keegan JJ, Garrett FD. The segmental distribution of the cutaneous nerves in the limbs of man. Anat Rec 1948;102:409. Kestenbaum A. Clinical methods of neuro-ophthalmologic examination. New York: Grune & Stratton, 1961. Knobloch H, Pasamanick B. Predicting intellectual potential in infancy. Am J Dis Child 1963;166:43. Korobkin R. The relationship between head circumference and the development of communicating hydrocephalus following intraventricular hemorrhage. Pediatrics 1975;56:74. Lubchenco LO, Hansman M, Boyd E. Intra-uterine growth in length and head circumference as estimated from live births at gestational ages from 26 to 42 weeks. Pediatrics 1966;37:403. Miller G, Heckmatt JZ, Dubowitz LMS, et al. Use of nerve conduction velocity to determine gestational age in infants at risk and in very-lowbirth-weight infants. J Pediatr 1983;103:109. Moosa A, Dubowitz V. Assessment of gestational age in newborn infants: Nerve conduction velocity versus maturity score. Dev Med Child Neurol 1972;14:290. Nellhaus G. Composite international and interracial graphs. Pediatrics 1968;41:106. Nelson KB, Eng GD. Congenital hypoplasia of depressor anguli oris muscle: Differentiation from congenital facial palsy. J Pediatr 1972;81:16. O’Neill E. Normal head growth and prediction of head size in infantile hydrocephalus. Arch Dis Child 1961;36:241. Paine RS. Neurologic conditions in the neonatal period: Diagnosis and management. Pediatr Clin North Am 1961;8:577. Paine RS, Oppe TE. Neurological examination of children. London: William Heinemann Medical Books, 1966. Peiper A. Cerebral function in infancy and childhood. New York: Consultants Bureau Enterprises, 1963. Prechtl HFR. The neurological examination of the full term newborn infant, 2nd ed. London: William Heinemann Medical Books, 1977. Robinson RJ. Assessment of gestational age by neurologic examination. Arch Dis Child 1966;41:437. Sauer C, Levinsohn MW. Horner’s syndrome in childhood. Neurology 1976;26:216. Scher MS, Barmada MA. Gestational age by electrographic, clinical, and anatomical criteria. Pediatr Neurol 1987;3:256. Sonksen PM. The assessment of vision in the preschool child. Arch Dis Child 1993;68:513. Volpe JJ. The neurological examination: normal and abnormal features. In: Volpe JJ, ed. Neurology of the newborn, 4th ed. Philadelphia: WB Saunders, 2001. Volpe JJ, Pasternak JF, Allan WC. Ventricular dilation preceding rapid head growth following neonatal intracranial hemorrhage. Am J Dis Child 1977;131:1212.
CHAPTER 4
Neurologic Examination of the Term and Preterm Infant Kenneth F. Swaiman
THE TERM INFANT Monitoring of the fetus routinely takes place during the intrapartum period through electronic fetal monitoring [Volpe, 2001a]. Alterations in fetal heart rate patterns prove to be valuable in assessing the fetus. The term infant is assessed immediately after birth. Apgar scores are routinely obtained for term infants at the time of birth. The categories for scoring are described in Table 4-1. Details of the scoring and the total scores often provide useful information concerning the newborn’s status for the examiner and subsequent health-care providers. Use of the Sarnat score is of value in assessing term infants who are encephalopathic at birth (Table 4-2) [Sarnat and Sarnat, 1976]. The neurologic examination of a term infant should be conducted in a quiet and evenly lighted area that is suitably warmed so that the infant remains comfortable after removal of clothing and covering. When the infant is in a stable condition, thorough examination during the first day is customary. If possible, another examination should be performed on the second or third day of life several hours after feeding so that the infant is optimally responsive. This examination is usually performed just before discharge. In emergent situations, the infant should be evaluated after stabilization has been achieved. It is often necessary to examine the infant on several occasions to confirm the presence and monitor the evolution of abnormal findings. Many protocols for the examination of the term infant (gestational age of 38 to 42 weeks) have been written [Ashwal, 1995; Brazelton, 1973; Dubowitz and Dubowitz, 1981; Paine, 1960; Peiper, 1963; Prechtl, 1977]; some investigators have addressed the subject as part of the discussion of neonatal neurology [Fenichel, 2001; Volpe, 2001b]. Estimation of gestational age is discussed in this chapter. It is essential that the examination of the term infant be conducted in a systematic manner. Examination of the sick neonate may be difficult because of the presence of monitoring wires, sensors, catheters, eye shields, and infusion lines; however, systematic order in the sequence and extent of examination must be maintained to provide optimal information. These sick infants often must be examined on multiple occasions for sequential monitoring purposes and to complete portions of the examination not possible at the first encounter.
Observation A proper examination begins with observation. The infant’s clothing should be removed slowly and gently, and the diaper should be opened only for the period in which the covered area is evaluated. The examiner should make no quick
moves. It is a common error to begin handling the infant before an adequate observation period. The examiner should delineate the presence of congenital abnormalities, including midline defects of the cranium, face, palate, and spine. Midline defects are often associated with abnormalities of the neural tube. Abnormalities of the trunk, limbs, and skin are readily observed. Skin pigmentation changes are important because of the shared ectodermal beginnings of the integument and the nervous system. In particular, the presence of abnormalities associated with neurocutaneous syndromes should be ascertained, even though manifestations may not be present in the newborn. Freckling in the axillary areas is highly suggestive of neurofibromatosis. Assessment of most cranial nerves can be accomplished in part through observation. The cranial nerves enabling eye movements and facial movements can be readily monitored. Gross motor abilities of the newborn infant can be partially evaluated by observation. The head is preferentially turned to the right for longer periods than to the left. Term infants have predominant flexor tone, with resultant flexion of the arms at the elbows and of the legs at the knees. Bilateral fisting of the hands, including adduction and infolding of the thumbs (i.e., cortical thumbs), is expected. Limb position and posturing should be roughly symmetric. While supine, the infant manifests spontaneous limb movements that are often asymmetric and have a rapidly jerking quality. Jitteriness or tremulousness of the hands or jaw is sometimes spontaneous. These movements may indicate hyperexcitability of the central nervous system (CNS). Causes of hyperexcitability are discussed later in this chapter. The examiner should mentally quantitate frequency and amplitude of limb movements. Diminished frequency or amplitudes of arm movements may indicate brachial plexus injury; involvement of an arm and ipsilateral leg may indicate hemiparesis. While prone, the infant normally maintains a flexed posture of the arms and legs, with resultant elevation of the pelvis and flexion of the hips and knees. The infant’s respiratory rhythm and chest movement should be observed to indicate adequate contraction of intercostal muscles. Although diaphragmatic breathing is normally accentuated in the newborn, the absence of intercostal muscle participation and a “sucking in” of the sternum may indicate anterior horn cell disease, neuromuscular junction disease, or spinal cord injury. The presence of a pectus excavatum deformity in the newborn should not be regarded as an isolated congenital deformity until neuromuscular conditions in which the diaphragm overpowers the intercostal muscles have been excluded. The level of alertness increases with CNS maturation. At 37 weeks’ gestation, crying is common during wakefulness. At term, the infant remains alert for reasonable periods and
48
Clinical Evaluation / 4
TABLE 4-1 Apgar Scoring SIGN
0
1
2
1 MIN
5 MIN
10 MIN
Heart rate Respiratory effort Muscle tone Reflex response* Color Total Apgar rating
Absent Absent Limp No response Blue, pale
Slow, below 100 Slow, irregular Some flexion of extremities Grimace Body pink, extremities blue
Over 100 Good crying Active motion Cough or sneeze Completely pink
— — — — — —
— — — — — —
— — — — — —
*Catheter inserted in nostril. Adapted from Apgar V. A proposal for a new method of evaluation of the newborn infant. Curr Res Anesthesiol 1953;32:360.
TABLE 4-2 Distinguishing Features of the Three Clinical Stages of Postanoxic Encephalopathy in Term Newborns FEATURE
STAGE 1
STAGE 2
STAGE 3
Level of consciousness Neuromuscular control Muscle tone Posture Stretch reflexes Segmental myoclonus Complex reflexes Suck Moro Oculovestibular Tonic neck Autonomic function Pupils Heart rate Bronchial and salivary secretions Gastrointestinal motility Seizures Electroencephalographic findings
Hyperalert
Lethargic or obtunded
Stuporous
Normal Mild distal flexion Overactive Present
Mild hypotonia Strong distal flexion Overactive Present
Flaccid Intermittent decerebration Decreased or absent Absent
Weak Strong; low threshold Normal Slight Generalized sympathetic Mydriasis Tachycardia Sparse
Weak or absent Weak, incomplete, high threshold Overactive Strong Generalized parasympathetic Miosis Bradycardia Profuse
Absent Absent Weak or absent Weak or absent Both systems depressed Variable; often unequal; poor light reflex Variable Variable
Normal or decreased None Normal (awake)
Increased; diarrhea Common; focal or multifocal Early: low-voltage continuous delta and theta; later: periodic pattern (awake); seizures: focal 1-1.5 Hz spike and wave 2-14 days
Variable Uncommon (excluding decerebration) Early: periodic pattern with isopotential phases; later: totally isopotential
Duration
Less than 24 hours
Hours to weeks
From Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress: A clinical and electroencephalographic study. Arch Neurol 1876;33:696.
responds to visual, auditory, and tactile stimulation. Crying is often forceful. Sleep and wake periods are clearly delineated.
Cranial Vault Evaluation Among the most important facets of the examination is the measurement of the occipitofrontal (head) circumference. For the most part, this measurement is a reflection of brain growth. However, undue enlargement may be associated with cephalohematoma, subdural fluid collection, hydrocephalus, hydranencephaly, macrocephaly, or megalencephaly (Chapter 19). Serial measurements provide an index of brain growth in sick neonates. Microcephaly may be associated with many conditions, including intrauterine infection, hereditary abnormalities, maternal substance abuse, and poor nutrition. The shape of the head influences the measure of the circumference. The nearer the head shape approximates a perfect circle, the smaller is the head circumference com-
pared with the circumference of a noncircular head, despite the fact that the area of a plane through the maximal circumference and the brain volumes are the same. A similar relationship exists between a perfect sphere and the volume contained within it. The occipitofrontal circumference should be plotted on a graph standardized for gender, race, and gestational age to determine if the measurement falls within the normal range (i.e., two standard deviations above or below the mean) (Fig. 4-1) [Braun et al., 2004]. On the average, occipitofrontal circumference increases 2 cm during the first month of life, 6 cm during the first 4 months, 7 cm during the first 6 months, and 12 cm during the first 12 months of life [Fujimura and Seryu, 1977]. Infants delivered vaginally may have some deformity of the head because of scalp and subcutaneous edema with resulting caput succedaneum formation; vacuum extraction delivery often results in caput formation. Infants delivered by cesarean section usually have relatively round heads. The caput deformity, usually transient, produces an increased diameter and may confound accurate occipitofrontal circumference measurements. Ceph-
Swaiman / Neurologic Examination of the Term and Preterm Infant
49
FIGURE 4-1. Head circumference charts. (From Nellhaus G. Composite international and interracial graphs. Pediatrics 1968;41:106.)
alohematomas, which are delimited by the periosteum of the individual cranial bones, produce asymmetry of the head and increase the occipitofrontal circumference. Most occur over the parietal bones. A caput succedaneum, unlike a cephalohematoma, extends over two or more cranial bones and is
not restricted to the subperiosteal (subgaleal) space (see Chapter 17). The anterior fontanel, readily palpable at birth, is concave or flat in relation to the surrounding cranium. The fontanel should be assessed with the child held in the sitting position if there is any question of increased pressure. The
50
Clinical Evaluation / 4
fontanel may bulge during crying or in the presence of pathologic increased intracranial pressure. Unfortunately, the presence of normal conformation of the fontanel does not guarantee normal pressure; conversely, a bulging anterior fontanel strongly suggests increased intracranial pressure. The anterior fontanel varies in size but usually ranges from 1 to 3 cm in its longest dimension [Popich and Smith, 1972]. The fontanel pulsates synchronously with the infant’s pulse. The posterior fontanel in the neonate usually is open but admits only a fingertip. The presence of an enlarged posterior fontanel suggests the possibility of intrauterine increased intracranial pressure. From time to time, particularly in the presence of wormian bones, auxiliary fontanels may be palpable. A detailed discussion of the infant skull can be found in Chapter 19. The cranial sutures (e.g., sagittal, metopic, lambdoidal, squamosal) are readily palpable in the newborn. Infants delivered vaginally may manifest overriding of the sutures that with normal head growth resolves during the first week of life. The sagittal and lambdoidal sutures are most frequently involved. The sutures are readily separated from one another with palpation. The abrupt steplike contour of the overriding bone at the suture interface distinguishes this condition from that of premature closure of the sutures. When a suture closes prematurely, growth continues along the line of apposition of the bones across the suture. For example, sagittal synostosis causes an increase in the anteroposterior diameter (i.e., scaphocephaly). Increased bitemporal diameter occurs in the presence of coronal synostosis (i.e., brachycephaly). Asymmetric suture closure may lead to grossly asymmetric head shape (i.e., plagiocephaly). Auscultation over the infant skull, particularly the anterior fontanel and neck vessels, usually reveals a venous hum in a number of locations. Rarely, systolic-diastolic bruits, particularly those that are focal and asymmetric, indicate the presence of an arteriovenous malformation [Dodge, 1956]; however, these bruits may be heard in normal infants. Cranial ultrasound, computed tomography (CT), and magnetic resonance imaging are often informative concerning subdural hematomas, cystic lesions, hemorrhages, and enlarged ventricles. Before more advanced methodology, the use of transillumination with a flashlight or more sophisticated light source often indicated the possibility of a subdural effusion, subdural hematoma, or cystic lesions [Dodge and Porter, 1961].
Developmental Reflexes Developmental reflexes are primitive reflexes with complex responses and largely reflect the integrity of the brainstem and spinal cord; the role of higher centers, although of importance, is not fully known. Many of these reflexes are present at birth and undergo modification during the first 6 months of life. Detailed discussion of these reflexes is presented in Chapter 3. Their persistence beyond the expected date of dissipation suggests maturational lag or impaired CNS function. This group includes the Moro, rooting, grasping, tonic neck, stepping, and placing reflexes. Generalized diminution of the manifestation of these reflexes suggests diffuse depression of brain function. Asymmetry indicates central or peripheral nervous system dysfunction that must be further localized.
Motor Function Gentle manipulation of the infant’s limbs allows for assessment of muscle tone and strength. Tone is defined as resistance to passive movement (see Chapter 5). Tone at each large joint should be evaluated while the infant is at rest. Spontaneous movements and resistance of the infant to limb and trunk movement provide a measure of muscle strength. The examiner should recall any clues from the observation period suggesting muscle weakness and corroborating changes in tone and strength at this time. The infant should be supine with the head in the midposition while tone is evaluated so that the tonic neck reflex does not augment tone unilaterally. The newborn infant should be held in the horizontal position while attitude and posture of the limbs and trunk are observed. The infant should then be held in vertical suspension again to determine whether the expected flexor tone of the limbs is present and symmetric. When held in the vertical position the hypotonic and weak infant tends to slide through the examiner’s hands. The infant’s arms are held loosely at the sides, and the expected configuration of the shoulder girdle is poorly maintained. In the horizontal position, the infant appears to be looped over the examiner’s arms. Infants with increased tone manifest an opisthotonic position in conjunction with obligate extension in both vertical and horizontal positions. Although it usually manifests in older infants, scissoring (i.e., crossing of the legs because of excessive, involuntary adductor magnus contraction) may be evident. The most common cause of generalized decreased tone is depression of CNS function, which may result from hypoxic-ischemic encephalopathy, neonatal sepsis, intraventricular hemorrhage, subdural hemorrhage, or metabolic abnormalities (e.g., hypoglycemia). Congenital malformations, including neuronal migration disorders, may be associated with hypotonia. Tone and strength may be decreased in a number of neuromuscular conditions, including spinal muscular atrophy, neonatal myasthenia gravis, congenital myopathies, and neonatal myotonic dystrophy. Muscle tone may be increased in a variety of conditions that cause a neonatal encephalopathy, including many metabolic disorders, hypoxic-ischemic encephalopathy, neonatal stroke, intrauterine infection, congenital malformations, and trauma. While the infant is being handled, stimulation may engender jittery or tremulous movements of the jaw or limbs. Such movements are arrhythmic and do not have a definite phasic composition. The movements usually terminate when stimulation ends, although noises or abrupt changes in light may trigger them. Sometimes, there may be spontaneous tremulousness. Crying enhances the frequency and range of the movements. Such tremulousness may indicate metabolic abnormalities (e.g., electrolyte imbalance), bleeding, congenital CNS defects (structural or functional), infections, or drug withdrawal syndromes. Exaggerated and persistent tremulousness may indicate relative irritability of the cerebral cortex and potential risk for subsequent, significant neurologic dysfunction including seizures. Deep tendon reflexes are elicited using a reflex hammer and are often brisk in the newborn, although they may be normally absent [Critchley, 1968]. They may be inordinately enhanced by upper motor neuron abnormalities and are further facilitated by crying. CNS depression may be asso-
Swaiman / Neurologic Examination of the Term and Preterm Infant
ciated with reduced deep tendon reflexes. The examiner should confirm that the deep tendon reflexes are symmetric, because asymmetry may indicate central or peripheral nervous system impairment. If previous examination has suggested the possibility of hemiparesis, deep tendon reflexes should be carefully evaluated for asymmetry; they are usually increased on the affected side. Deep tendon reflex asymmetry in the arms may be associated with upper motor neuron abnormality, but asymmetrically absent deep tendon reflexes suggest peripheral involvement, possibly the result of brachial plexus injury. Nerve conduction studies in newborns may provide an index of neurologic maturity [Dubowitz et al., 1968]. Controversy remains over the significance of the plantar response in the newborn period in term infants. Although some investigators have reported that the Babinski sign is flexor and symmetric in the newborn period [Hogan and Milligan, 1971], this is more likely caused by obtaining a plantar grasp than a Babinski response if only the sole of the foot is used to elicit the response. The plantar response is extensor for at least the first month of life and usually through the first year of life. However, at all times, the response should always be bilaterally symmetric. Persistence of extensor toesign responses beyond infancy suggests corticospinal tract impairment and may be associated with alterations in tone and other deep tendon reflex abnormalities. Ankle clonus is frequently elicited in the newborn; rarely are there more than eight beats in normal infants. The clonus is enhanced during crying and may be facilitated during hyperexcitable states, such as those associated with metabolic abnormalities, infection, and subarachnoid hemorrhage. Sustained ankle clonus has the same significance in term newborns as in later life and suggests dysfunction of the corticospinal tracts. A reflex akin to the plantar response has been described for the hand in term and preterm newborns. The examiner strokes the ulnar aspect of the infant’s palm with the thumb, beginning distally and stroking proximally from the small finger to the hypothenar eminence. The normal response is
51
gradual extension of the fingers, beginning with the small finger and continuing to the middle fingers [Modanlou, 1988]. Lack of response or gross alteration of response may be observed in the presence of corticospinal tract dysfunction.
Cranial Nerve Examination A more detailed discussion of the cranial nerve examination is found in Chapter 2. Cranial nerve I, the olfactory nerve, is infrequently tested but may be evaluated by the use of pleasant but definitive aromatic substances, such as cinnamon and cloves [Sarnat, 1978]. The infant usually manifests an arrest of activity, arousal, and sucking activity when exposed to these aromas. Virtually all neonates born after more than 32 weeks’ gestation respond [Sarnat, 1978]. Evaluation of cranial nerves II, III, IV, and VI involves assessment of the eyes. The pupils should be symmetric, and there should be an equal bilateral response to light. A bright light causes the infant to blink or hold the lids closed. The presence of ptosis or increased height of the palpebral fissure should be evaluated. The examiner should ascertain the presence of heterochromia, although it may not be evident until later. Examination of the optic fundi may be difficult but is necessary. Numerous changes, including chorioretinitis (i.e., salt-and-pepper pigmentary changes), may be observed. Hemorrhages are commonly detected after vaginal delivery, even in the absence of traumatic delivery. The optic nerve may be hypoplastic, as manifested by a small, pearl-colored optic disc. The color of the optic disc in the newborn infant is grayish white. Retinal hemorrhages may be found in a large percentage of otherwise normal infants who have no history of abnormal delivery and who later prove to be neurologically normal [Besio et al., 1979]. Further discussion of funduscopic characteristics is presented in Chapter 6. The newborn infant turns toward a light of moderate intensity and fixes on a bright object or the examiner’s face. Most often, the newborn’s eyes are symmetrically open or FIGURE 4-2. Horner’s syndrome (left eye). (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School.)
52
Clinical Evaluation / 4
closed. If one eye is open and the other closed, there should be a shifting from one side to the other. Width of palpebral fissures should be equal; if not, the presence of ptosis should suggest an abnormality of cranial nerve III function, sympathetic innervation dysfunction, neuromuscular junction difficulty, weakness of the levator muscle of the lid, or abnormality of the lid connective tissue. Among the conditions to be considered are congenital myasthenia gravis, myotonic dystrophy, Horner’s syndrome (Fig. 4-2), Möbius’ syndrome, congenital myopathies, and Duane’s syndrome. Occasionally, central or peripheral seventh nerve paresis may result in asymmetry of the palpebral fissure. Extraocular movements should be monitored while a child is lying quietly. Slight lapses of conjugate gaze are common in the newborn period. Newborn visual acuity is difficult to assess, but black and white–patterned objects can be used. The examiner’s face is often the best “target.” The intended object of focus is moved slowly in the infant’s field of vision, less than a foot from the infant’s eyes. The infant slowly follows with eye movement, particularly in lateral directions. Prolonged gaze may occur in the newborn period [Brazelton et al., 1976]. Opticokinetic nystagmus may be elicited by using a striped, rotating drum or striped cloth strip, which is slowly pulled across the infant’s visual field in the vertical and horizontal directions. The response is the same as in older children (see Chapter 2). Although small-excursion, lateral-gaze nystagmus may be present in the newborn, the grosser to-and-fro pattern of congenital nystagmus, which is oscillatory in nature, is usually unmistakable. Although unusual, nystagmus associated with mild esotropia or exotropia may be evident in the newborn. Wild, jerky nystagmus of congenital opsoclonus is a startling and readily discernible finding suggesting midbrain involvement. Doll’s-eye movement is elicited by the examiner gently rotating the infant’s head from one side to the other when the infant is asleep. The eyes move conjugately in the direction opposite to the rotation of the head. Movement of the head in the vertical position (upward and downward) causes similar movements in the vertical plane. Failure of the eyes to move in the expected manner or direction indicates abnormalities of the cranial nerves or brainstem nuclei. Failure of abduction is associated with cranial nerve VI impairment or lateral rectus muscle impairment. Failure of normal movement in the medial direction implicates medial rectus muscle or cranial nerve III impairment. To gain further information, the infant may be held supine on the examiner’s arm as the examiner rotates and watches the infant’s eyes. This oculovestibular maneuver causes movement so that there is lateral conjugate deviation in the direction of the rotation. When the rotational movement is terminated abruptly, the eye movements reverse. It is possible to assess the integrity of cranial nerves III and VI with this maneuver. Cranial nerve VII involvement may be the result of the position of the infant in the maternal pelvis and delivery by pressure incurred during forceps delivery or by agenesis of the motor nucleus of cranial nerve VII. Facial movements are readily observed during crying; an asymmetry of mouth movement may indicate cranial nerve VII involvement. During crying, the angle of the mouth is depressed on the normal side. The syndrome referred to as asymmetric crying facies may manifest this way [Nelson and Eng, 1972]. This
syndrome results from weakness of the lower lip caused by hypoplasia of the depressor muscle of the mouth angle. This phenomenon is a congenital abnormality and does not signal cranial nerve VII involvement. This condition also may be associated with somatic atrophy, vertebral and rib abnormalities, renal dysgenesis, and most importantly, cardiac defects (i.e., atrial or ventricular septal defect) [Pape and Pickering, 1972]. Hearing in term infants has been evaluated by sophisticated testing techniques that indicate some ability to localize and discriminate. However, meaningful hearing evaluation during routine neurologic examination is difficult to accomplish because of simultaneous visual cues and variable responses. The use of brainstem auditory-evoked potential testing has greatly improved the ability to evaluate hearing response during the neonatal period. Vestibular function can be monitored by the oculovestibular maneuver described previously. Assessment of cranial nerves IX, X, and XII may be facilitated by evaluating the infant’s cry; however, impairment of crying may occur because of central rather than peripheral abnormalities. An infant with generally depressed CNS function often cries infrequently, and the cry is weak and may be high pitched. The volume and tone of the cry should be assessed. An irritable child with a hyperexcitable nervous system may have a high-pitched shriek, whereas unusual cries such as that associated with the cri du chat syndrome are similar to a cat’s cry. Observation of the infant during crying is a valuable adjunct to certain portions of the examination. During the lusty segments of crying, the infant’s tongue and palate may be readily inspected. Asymmetry or loss of tongue bulk may indicate abnormalities of cranial nerve XII or its nucleus. The presence of fasciculations may indicate spinal muscular atrophy. More complex forms of the Möbius syndrome may also involve the tongue. Tongue fasciculations must be identified when the child is quiet and not crying. The fasciculations occur along the lateral margins and underside of the tongue. Cranial nerves V, VII, IX, X, and XII are involved in sucking and swallowing. Swallowing dysfunction requires close scrutiny to determine which cranial nerve or nerves are involved. The gag reflex is present in term newborns and requires normal function of cranial nerves IX and X. Tests for pain and sensation are imprecise at this age, and the gross response of infants to stroking and pinprick with withdrawal, crying, and change in sucking rates may be the only information possible. More sophisticated testing can be devised during which heart and respiratory rates are monitored. If necessary, in the presence of olfactory, gustatory, visual, tactile, or auditory stimuli, sophisticated monitoring and scoring of body activity may be performed [Brazelton, 1976]. All such sensory stimuli produce habituation in the newborn [Lipsitt, 1977]. Lack of habituation or failure to respond to these stimuli is abnormal; however, the abnormality may be specific for the sensory mechanism or merely may be a reflection of generalized CNS depression.
THE PRETERM INFANT The neurologic evaluation of the preterm infant is a major challenge to the clinician. Much of the information in this
Swaiman / Neurologic Examination of the Term and Preterm Infant
chapter concerning the term infant is applicable to the preterm infant. The fragility of the patient, the changing developmental norms coupled with the uncertainty of the length of gestation, and the frequent need for life-support systems and associated paraphernalia, which interfere with the examination and the spontaneity of movement, all complicate the process. Modern imaging techniques permit correlation of clinical examination and image alterations never before available. The use of cranial ultrasound examination and, when feasible, CT has permitted the timely diagnosis of intraventricular and hemispheral hemorrhage and early hydrocephalus in preterm infants. The information provided is greater in quality and quantity than has been available previously. The designation of an infant as preterm is related primarily to length of gestation. Term gestation is 38 to 42 weeks from conception, and preterm therefore is any period less than 38 weeks, although most clinicians would not consider a baby preterm or premature between 36 and 38 weeks. Expected developmental milestones are based on gestation [Mercuri, 2003]. The clinician must estimate gestational age to facilitate interpretation of the observations and findings made during the neurologic examination. An infant whose birth weight is low compared with length of gestation (e.g., intrauterine growth retardation, small for gestational age) exhibits different growth patterns or neurologic findings than the infant whose weight is appropriate for gestational age. In a parallel fashion, preterm infants born of diabetic mothers may weigh more than 2500 g, but these infants manifest findings consistent with their preterm status during the neurologic evaluation. The designation of extremely low birth weight infants has been assigned to those infants who weigh less than 1000 g at birth [Doyle et al., 2004; Kilbride, 2004]. Most of these infants are at 28 weeks or less gestation. The very low birth weight infants are those who weigh less than 1500 g at birth. In the absence of intrauterine growth retardation, most infants of this birth weight are born after 31 to 32 weeks’ gestation [Lubchenco et al., 1966]. The neurologic examination of these infants is reviewed in this portion of the chapter; the expected results of the examination should be based on the gestational age as determined from the various tables and illustrations.
General Examination It is not possible with any great assurance to estimate gestational age from the date of the first day of the mother’s last menstrual period [Lubchenco, 1970]. Nevertheless, a number of physical findings evident during the examination can prove helpful in this evaluation [Farr et al., 1966a, 1966b; Lubchenco, 1970; Usher and McLean, 1969]. Among the most valuable findings are skin texture and color, quantity of breast tissue and ear cartilage, and the stage of development of the external genitalia. No single characteristic can determine the gestational age. The estimate should be based on the average of expected findings (Table 4-3). The combination of findings based on physical characteristics and neuro-
Box 4-1 SELECTED GESTATIONAL AGE–DEPENDENT ELECTROENCEPHALOGRAPHIC PATTERNS BASED ON CONVOLUTIONAL MEASUREMENTS Less than 28 Weeks Prominent occipital theta/alpha Prominent vertex-central delta brush Rhythmic occipital delta (50% >50% >75%
Adapted from Cepeda et al., 1978; Dubowitz et al., 1981; Lazzara et al., 1980; Moylan et al., 1978; Ment unpublished data, NS27116 Randomized Indomethacin IVH Prevention Trial, 1997.
Cerebrospinal Fluid Studies Several investigators have demonstrated that examination of the cerebrospinal fluid in preterm infants undergoing unremarkable sepsis evaluations routinely reveals 0 to 20 white blood cells (predominantly lymphocytes and monocytes per high-power field), the absence of red blood cells, and protein values of 100 to 200 mg/dL. In patients with new-onset intraventricular hemorrhage, cerebrospinal fluid findings include large numbers of red blood cells, white cells in direct proportion to the ratio of peripheral red blood cells to white blood cells, elevations of protein, and low glucose values. Cerebrospinal fluid protein levels and red blood cell counts have been reported to correlate with the grade of intraventricular hemorrhage. Subjects with grades 3 or 4 intraventricular hemorrhage generally are found to have cerebrospinal fluid protein concentrations of 500 to 1000 mg/dL and red blood cell values in excess of 1,000,000/mm3. In contrast, patients with grade 2 intraventricular hemorrhage generally demonstrate cerebrospinal fluid protein values of less than 500 mg/dL and red blood cell values of 10,000 to 250,000/mm3. Patients with germinal matrix hemorrhage, or grade 1 intraventricular hemorrhage, generally have no evidence for red blood cells within the cerebrospinal fluid unless they have also experienced a subarachnoid bleed; similarly, infants with grade 1 intraventricular hemorrhage usually have normal cerebrospinal fluid protein levels. Profound hypoglycorrhachia, with cerebrospinal fluid glucose values below 10 mg/dL, may be found in infants with all grades of hemorrhage, although this is also more common in patients with high-grade hemorrhage. Days to weeks after the primary hemorrhage, examination of the cerebrospinal fluid demonstrates decreasing red blood cell numbers but elevated white blood cell counts in excess of 500 to 1000 white blood cells/mm3 and persistent hypoglycorrhachia. The latter two findings may lead the clinician to suspect bacterial meningitis, a diagnosis that can be determined only by cerebrospinal fluid culture studies.
OUTCOMES Although recent advances in neonatal intensive care have resulted in increased survival rates for many critically ill and very preterm neonates, the neurodevelopmental fate of verylow-birth-weight infants remains uncertain. Depending on the birth weight of the patient cohort and the years in which
Ment / Intraventricular Hemorrhage of the Preterm Neonate
they were born, the incidence of major neurodevelopmental handicaps ranges from 12% to 36%, and the prevalence of cerebral palsy is reported to be rising [Anderson et al., 2003; Bhutta et al., 2002; Hack et al., 2000b, 2002; Saigal et al., 2003; Vohr et al., 2000; Wood et al., 2000]. These groups of very-low-birth-weight infants have an increased incidence of more subtle intellectual and behavioral problems at school age [Aylward, 2003; Bhutta et al., 2002; Horwood et al., 1998; McCarton et al., 1997; McCormick et al., 1990, 1996; Pinto-Martin et al., 1999; Taylor et al., 2000b]. In the neonatal period, infants with intraventricular hemorrhage are at risk for the development of seizures and post-hemorrhagic hydrocephalus. Depending on the birth weights and gestational ages of the cohorts studied and the investigator’s method for determining seizures, the reported incidence of seizures in preterm infants with intraventricular hemorrhage was 5% to 10%. Similarly, the incidence of post-hemorrhagic hydrocephalus depends on the gestational age of the population reported, on the investigator’s diagnoses, and on the grade of intraventricular hemorrhage; as many as 25% to 50% of infants with grades 3 or 4 intraventricular hemorrhage may experience posthemorrhagic hydrocephalus [Whitelaw, 2001b]. The mortality rate is higher for infants with intraventricular hemorrhage compared with their gestational age–matched peers without hemorrhage. However, in most series in which the causes of death are given, infants with intraventricular hemorrhage are likely to succumb to other lesions believed attributable to changes in blood flow, such as necrotizing enterocolitis and bronchopulmonary dysplasia [Fanaroff et al., 2003; Schmidt and David, 2001]. Infants with intraventricular hemorrhage more commonly have abnormal cranial sonograms at 40 weeks’ conceptional age than infants with no evidence of intraventricular hemorrhage [Allan et al., 1997].
Post-hemorrhagic Hydrocephalus Post-hemorrhagic hydrocephalus is diagnosed in the infant who meets all of the following criteria: presence of intraventricular blood, increasing ventriculomegaly (most commonly diagnosed by cranial ultrasonography), and evidence for increased intracranial pressure (defined as an opening pressure of greater than 140 mm H2O by lumbar puncture or, if indicated, cerebral ventricular tap) [Whitelaw, 2001b]. In infants with post-hemorrhagic hydrocephalus, the ventricular width at the intraventricular foramen by sonographic measurement exceeds 4 mm over the 97th percentile for gestational age [Levene, 1981]. Post-hemorrhagic hydrocephalus is most common in infants with high grades of hemorrhage and less common in infants with the lowest gestational ages. It is rare to diagnose post-hemorrhagic hydrocephalus in an infant born after less than 26 weeks’ gestation, even in the presence of grade 4 intraventricular hemorrhage. In contrast, post-hemorrhagic hydrocephalus is routinely detected in infants of 30 to 34 weeks’ gestational age who have suffered only grade 2 hemorrhage. In most instances, the sequence of events resulting in post-hemorrhagic hydrocephalus begins with multiple small clots throughout the ventricles. Although post-hemorrhagic hydrocephalus is traditionally thought to represent a communicating hydrocephalus with obstruction to the passage
321
of cerebrospinal fluid at the level of the arachnoid villi, it is also probable that the cerebrospinal fluid is reabsorbed across the ependyma into small penetrating vessels within the developing white matter. Obstruction to flow may also occur at the level of these vessels or, less commonly, at the foramina of Luschka and Magendie in the posterior fossa [Deonna et al., 1975; Whitelaw, 1997]. In the presence of a block in the normal cerebrospinal fluid flow pathways, ventriculomegaly develops, and periventricular white matter damage may ensue. Suggested mechanisms for periventricular white matter injury after post-hemorrhagic hydrocephalus include raised pressure and edema, damaging effects of the free iron released into the cerebrospinal fluid during clot lysis, and proinflammatory cytokines [Savman et al., 2001]. A small percentage of infants with intraventricular hemorrhage may develop acute obstruction at the level of the aqueduct because of clots obstructing cerebrospinal fluid flow; these infants present with signs of acutely increased intracranial pressure (i.e., apnea, bulging fontanel, split sutures, and lethargy or coma) and require immediate neurosurgical attention. There is some evidence that there is an endogenous attempt to lyse clots in the cerebrospinal fluid by the preterm brain, but levels of plasminogen are low, and those of plasminogen activator inhibitor-1 (PAI-1) high in newborn cerebrospinal fluid [Hansen et al., 1997; Whitelaw, 1993]. Transforming growth factor-β1 (TGF-β1) is released into the cerebrospinal fluid of preterm infants after intraventricular hemorrhage; TGF-β1 upregulates genes for extracellular matrix proteins such as fibronectin and laminin and is critical for wound healing. TGF-β1 is virtually undetectable in the cerebrospinal fluid of infants without intraventricular hemorrhage; those with the greatest frequency of developing post-hemorrhagic hydrocephalus have the highest levels of TGF-β1 [Whitelaw et al., 1999]. When treating infants with post-hemorrhagic hydrocephalus, the physician must protect the neonate from damage from increased intracranial pressure and avoid the need for permanent cerebrospinal fluid drainage procedures. Previously advocated therapies included repeated lumbar punctures or ventricular taps; inhibition of cerebrospinal fluid production by acetazolamide or furosemide, or both; and intraventricular fibrinolytic therapy for clot lysis, but they have all been found to lack effect. Similarly, external ventricular drains and subcutaneous ventricular reservoirs have not been examined in controlled trials and are associated with significant risk of infection [Pang et al., 1986; Whitelaw, 2000a, 2000b, 2001a]. For these reasons, conservative management of post-hemorrhagic hydrocephalus in the absence of symptoms of increased intracranial pressure is generally recommended. Infants with intraventricular or intraparenchymal hemorrhage should undergo frequent determinations of occipitofrontal circumference [Ehrenkranz et al., 1999] and ultrasonographic determinations of ventricular size [Whitelaw, 2001b]. Although progressive ventriculomegaly may develop as early as the fourth or fifth postnatal day (see Fig. 16-13), the occipitofrontal circumference of the preterm infant may not increase until many days later because of the adaptive response of the preterm brain to absorb those subarachnoid fluid collections typically found over the convexities before exhibiting the more classic signs of increasing pressure
322
Perinatal Acquired and Congenital Neurologic Disorders / 16
A
B
FIGURE 16-14. Intraventricular hemorrhage leading to post-hemorrhagic hydrocephalus (PHH). A, Coronal view shows where the blood has ruptured beyond the ependyma to enter the lateral ventricles, filling but not distending them. B, PHH is shown on a subsequent ultrasound scan, which demonstrates the interval enlargement of the lateral ventricles, third ventricle, and foramina of Monro. The development of PHH does not alter the grading of the original intraventricular hemorrhage.
[Wigglesworth et al., 1976]. MRI studies of infants with ultrasound-diagnosed post-hemorrhagic hydrocephalus (Fig. 16-14) may reveal intraventricular hemorrhage, ventriculomegaly, and evidence for periventricular infarction (Fig. 16-15). Because prolonged increased intracranial pressure may result in poor feeding, lethargy, apnea, and ultimately in
optic atrophy, if ventricular size and occipitofrontal circumference determinations persistently increase, neurosurgical consultation for ventriculoperitoneal shunt or third ventriculostomy can be electively planned. Infants with acute signs of increased intracranial pressure and ventriculomegaly with blockage at the aqueduct require immediate neurosurgical intervention.
Cerebral Palsy
FIGURE 16-15. Magnetic resonance imaging (MRI) demonstrates posthemorrhagic hydrocephalus. Axial MRI of a preterm infant reveals a large, left-sided intraventricular hemorrhage; acute ventricular dilation; and parenchymal infarction. (Courtesy of Andrew Whitelaw, MD, Southmead Hospital, University of Bristol Medical School, Bristol, UK.)
Cerebral palsy is an important and well-established outcome for preterm infants that has been monitored in some centers for more than 40 years [Hagberg et al., 1996]. Data suggesting that the incidence of cerebral palsy is increasing in the United States have attributed this finding to the increasing survival rates of many preterm and very-low-birth-weight infants [Allen, 2000; Hutton et al., 2000]. Several investigators have demonstrated that the risk factors for spastic motor handicap in preterm infants include abnormal cranial ultrasound findings [Doyle, 2001; Hack et al., 2000b; Wood et al., 2000]. Cranial ultrasound findings repeatedly found to be associated with disabling cerebral palsy include parenchymal involvement of intraventricular hemorrhage, cystic periventricular leukomalacia, and ventriculomegaly [Allan et al., 1997; Bass et al., 1999; de Vries et al., 1998; de Vries et al., 2004; Hansen et al., 2004; Piecuch et al., 1997; PintoMartin et al., 1995, 1999; van de Bor et al., 1993]. The authors of these eight studies compared ultrasound findings with the incidence of cerebral palsy in more than 2500 verylow-birth-weight preterm children between the ages of 2 and 9 years. Significant associations for grade 4 intraventricular hemorrhage, periventricular leukomalacia, and ventriculomegaly with cerebral palsy were found in all. In the study of Pinto-Martin, grade 4 intraventricular hemorrhage was
Ment / Intraventricular Hemorrhage of the Preterm Neonate
Cognitive Outcome in Preterm Infants with Intraventricular Hemorrhage Numerous studies have demonstrated that school-aged children of low birth weight (25) in disorders of oxidative phosphorylation compared with pyruvate dehydrogenase complex disorders, in which the lactate-to-pyruvate ratio is usually normal. The clinical course may be benign in cases with only skeletal muscle involvement (e.g., benign infantile mitochondrial myopathy) or intractable and fatal in cases with intractable acidosis (e.g., lethal infantile mitochondrial disease). Diagnosis is difficult because of the extreme phenotypic and genotypic variability and because histologic and histochemical diagnostic techniques are difficult and not widely available. The limited treatment options generally have relied on supportive strategies to minimize catabolic stresses and on administration of carnitine and the respiratory chain cofactors nicotinamide and riboflavin.
Fructose Intolerance Fructose-1,6-biphosphatase (FDPase) deficiency is an autosomal-recessive disorder causing a profound defect in gluconeogenesis. It manifests as a severe, acute metabolic
355
encephalopathy in the first month of life, with marked, fasting-induced lactic acidosis, ketoacidosis, and hypoglycemia, usually without other organ involvement except for hepatomegaly. The characteristic clinical and biochemical features should suggest the diagnosis, but confirmation rests on enzyme assay of a liver biopsy specimen. Treatment is similar to that for type I glycogenosis and includes restriction of fructose and sucrose intake.
Fatty Acid Oxidation Defects Fatty acid oxidation defects represent a broad spectrum of disorders, most of which manifest beyond the neonatal period as acute encephalopathies with nonketotic hypoglycemia provoked by fasting or catabolic stress (see Chapter 23). In these disorders, one of several enzymes is deficient in the pathway for degradation of lipids to fatty acids to acetyl-CoA or ketone body production (see Fig. 18-4). Several of these disorders have been reported with prominent and distinctive presentations in neonates, including carnitine palmitoyl transferase II deficiency and mitochondrial trifunctional protein deficiency. Acyl-CoA dehydrogenase deficiencies (i.e., long-chain [LCAD], mediumchain [MCAD], or short-chain [SCAD] forms) more typically manifest beyond the neonatal period. These disorders share a constellation of clinical features that include the rapid onset of a fulminant metabolic encephalopathy with hypoglycemia, moderate hyperammonemia, low or moderate ketonuria (i.e., disproportionately low for the degree of hypoglycemia), and metabolic acidosis. Associated clinical features may include hepatomegaly, cardiomyopathy, and myopathy. The pathogenesis of neurologic symptoms has been attributed to the combined effects of direct toxicity from accumulated free fatty acids, insufficient glucose and ketones to fuel the Krebs cycle, and inhibition of mitochondrial energy production by the disturbed ratio of acyl-CoA to free CoA. The characteristic clinical features should suggest the diagnosis, which can be further supported by finding decreased levels of total plasma carnitine and specific patterns of elevated plasma levels of acylcarnitine intermediates as follows: C16 and C18 species in carnitine palmitoyl transferase II deficiency, C14 species in LCAD, C6 to C8 species in MCAD, and C4 species in SCAD. Definitive diagnosis rests on assay of enzyme activity from cultured skin fibroblasts. Treatment involves supportive measures, glucose administration, carnitine supplementation, and modification of feeding schedules to minimize fasting states. Creatine supplements have been suggested for patients with mitochondrial trifunctional protein deficiency. Recurrent decompensations can be minimized by early initiation of intravenous glucose during intercurrent illnesses and avoidance of fasting. Long-term outcome depends on the frequency and severity of decompensations. Mitochondrial trifunctional protein is distinguished among these disorders by the high proportion of cases (about 50%) presenting in the neonatal period [den Boer et al., 2003]. It has two types of presentations. The first is a neonatal presentation consisting of fulminant acute illness with rapid onset of depressed consciousness, heart failure, diffuse hypotonia, and weakness with absent tendon reflexes, severe lactic acidosis, and death of most from heart
356
Perinatal Acquired and Congenital Neurologic Disorders / 18
failure. The second is a subacute, infantile presentation with gradually progressive emergence of hypotonia, diffuse weakness, and cardiomyopathy. Multisystem involvement has been reported, including retinopathy, peripheral neuropathy, myopathy, cardiomyopathy, and liver disease. Carnitine palmitoyl transferase II deficiency has several phenotypes, with onset in adulthood, infancy, or the neonatal period. The latter is the least common and most severe form [Sigauke et al., 2003], and it is reported to be universally fatal. Affected infants often have prenatally detected cerebral lesions and malformations, including ventriculomegaly, agenesis of the corpus callosum, polymicrogyria, periventricular cystic leukomalacia, and subependymal hemorrhages. Neurologic symptoms that appear at birth or within the first few days of life include seizures, depressed consciousness, and hypotonia with myopathic features. Cardiomyopathy leading to circulatory failure is common. The metabolic findings are typical of fatty acid oxidation defects as described earlier. Management is supportive and symptomatic but ineffective in most cases. Definitive biochemical diagnosis is a prelude to genetic testing, which can provide a basis for family counseling and management of future pregnancies. A number of states have incorporated carnitine palmitoyl transferase II in neonatal metabolic screening programs in the hope of promoting early diagnosis.
former of acidosis, ketosis, or lactic acidosis and by specific metabolites in urinary organic acid profiles, as described earlier. Transient hyperammonemia of the newborn is a poorly understood disorder, characterized by severe transient hyperammonemia associated with respiratory distress syndromes or herpes simplex infection. It is distinguished from the genetically determined enzyme defects by its earlier onset (first 24 hours of life) and its association with prematurity and pulmonary disease. The pathophysiology of hyperammonemic encephalopathy is complex and is in part related to astrocyte swelling and dysfunction due to excessive glutamine accumulation [Takahashi et al., 1991]. Treatment of acute, severe hyperammonemic coma in the neonate is best achieved with hemodialysis to rapidly reduce plasma ammonia levels to at least three times the upper limit of normal. Use of pressors and volume to maintain adequate cerebral perfusion pressure is preferable to the use of hyperventilation or osmotic diuresis in managing intracranial hypertension. Careful protein restriction and administration of drugs to enhance excretion of excessive metabolites are tailored according to the specific enzyme defect and are thoroughly described elsewhere [Scriver et al., 2001]. Longterm outcome is variable. Motor and cognitive deficits depend on the severity and frequency of hyperammonemic decompensations.
Subacute Epileptic Encephalopathies
Urea Cycle Disorders Urea cycle defects manifesting in the neonate are characterized by the onset between 1 and 4 days of age of severe hyperammonemia with rapidly progressive lethargy and vomiting, progressing to coma with signs of cerebral edema. Associated features may include respiratory alkalosis and hypothermia. First-stage laboratory assessments reveal no other major abnormalities. A presumptive diagnosis can be made from results of plasma amino acid, urine organic acid, and urinary orotate excretion profiles (Fig. 18-5). Elevated plasma glutamine levels are common to all the urea cycle disorders. Organic acidopathies and congenital lactic acid disorders that may cause hyperammonemia can be distinguished from urea cycle disorders by the presence in the
Glycine Cleavage Defects Glycine cleavage defects are a group of autosomal-recessive disorders leading to accumulation of glycine (Fig. 18-6). The most common form is a neonatal-onset progressive encephalopathy with depressed consciousness and seizures, usually myoclonic, associated with an EEG pattern of burst suppression. Glycine toxicity appears to be maximal in the neonatal period, and it may spontaneously diminish after Glucose
3-Pglycerate Glutamate
Oxaloacetate 1
␣-ketoglutarate
D-Serine
Aspartate
2 1
L-Serine
Citrulline NH4
Argininosuccinate 3
4 Carbamyl phosphate
2
HCO3Orotate
Ornithine
Arginine
FIGURE 18-5. Urea cycle defects: 1, argininiosuccinate synthetase; 2, argnininosuccinase; 3, ornithine transcarbamylase; 4, carbamylphosphatate synthetase.
Glycolipids, myelin synthesis
Purine, pyrimidine biosynthesis
Glycine
3
MTHF
NH3 + CO 2
FIGURE 18-6. Disorders of serine and glycine metabolism: 1, 3-phosphoglycerate dehydrogenase; 2, serine hydroxymethyl transferase; 3, glycine cleavage system. MTHF, methylenetetrahydrofolate.
Ichord / Perinatal Metabolic Encephalopathies
1 month of age. Lifelong, severe cognitive and motor handicaps and intractable epilepsy are the rule among survivors, although there is considerable variability among survivors [Applegarth and Toone, 2004]. Factors that predict a poorer outcome include earlier age of symptom onset, presence of cerebral dysgenesis, and severity of glycine level elevation. Neurologic manifestations occur as a result of excessive stimulation of central nervous system glycine receptors, which are inhibitory in spinal cord and excitatory in brain by means of a co-agonist effect at the N-methyl-D-aspartate (NMDA) subtype of glutamate receptors. Biochemical abnormalities are limited to the finding of elevated glycine levels in plasma (onefold to eightfold above normal) and cerebrospinal fluid (15-fold to 30-fold above normal). In cases with equivocal plasma elevations of glycine concentrations, the diagnosis can be made by finding a cerebrospinal fluid–to-plasma ratio above 0.08. Glycine cleavage defects can be distinguished from the hyperglycinemia that accompanies organic acidopathies by the presence of ketosis in the latter and by characteristic organic acid excretion profiles. There are no proven therapies. Attempts to reduce glycine levels by dietary restriction and benzoate administration have not ameliorated the neurologic abnormalities. Seizures generally have been resistant to standard antiepileptic drugs.
357
Treatment with dextromethorphan, an NMDA-receptor antagonist, has had limited success in a small number of reported cases [Hamosh et al., 1992].
Pyridoxine Deficiency or Dependency Pyridoxine dependency disorder results from a relative or absolute lack of GABA synthesis from presumed defective binding of glutamic acid decarboxylase with its cofactor pyridoxal-5-phosphate, resulting in GABA deficiency (Fig. 18-7). GABA is the major inhibitory neurotransmitter in mammalian brain, a deficiency of which readily accounts for the clinical manifestations of intractable seizures and severe cortical dysfunction. Affected infants have neonatalonset seizures or, in some cases, in utero–onset seizures with no other metabolic abnormalities. Seizures are usually unresponsive to standard antiepileptic drugs. In a group of six affected neonates, Mikati and colleagues [1991] observed a unique EEG pattern consisting of generalized bursts of 1- to 4-Hz, sharp- and slow-wave activity [Mikati et al., 1991]. Isolated reports have suggested that the diagnosis can be supported by the findings of decreased cerebrospinal fluid GABA and increased cerebrospinal fluid glutamate levels [Kurlemann et al., 1987], which normalize after treatment with pyridoxine. Definitive diagnosis rests on the demon-
NEURON ASTROCYTE
Glutamine Gutamine
Glucose Pyruvate
Lactate
Glutamate
Glutamate GABA
Glutamate GABA
MITOCHONDRION Acetyl-CoA
Krebs cycle 2 Succinate
Succinic semialdehyde
␣-ketoglutarate
Glutamine
Glutamate
Glutamine
Glutamate
GABA
Transmembrane transporter
1 Pyridoxine
GABA
FIGURE 18-7. Schematic of relationships between intermediate metabolism and the major neuronal neurotransmitters glutamate and γ-aminobutyric acid (GABA). Selected defects affecting GABA metabolism include pyridoxine dependency or deficiency (1) and succinic semialdehyde dehydrogenase deficiency (2).
358
Perinatal Acquired and Congenital Neurologic Disorders / 18
stration of a normalized EEG pattern and control of seizures on intravenous administration of 50 to 100 mg of pyridoxine. Management requires lifelong pharmacologic doses of pyridoxine (10 to 100 mg/day).
Sulfite Oxidase and Molybdenum Cofactor Deficiency Molybdenum cofactor deficiency and isolated sulfite oxidase deficiency are closely related autosomal recessive diseases involving defects in xanthine metabolism and sulfite degradation pathways. Molybdenum cofactor is essential for the function of xanthine dehydrogenase and sulfite oxidase (Fig. 18-8). The mechanism of the brain injury is multifactorial, involving direct toxic effects of sulfite metabolites on cellular architecture, damage to mitochondria, thiamine degradation, and impaired mucopolysaccharide synthesis. These two distinct genetic defects share a similar clinical manifestation, consisting of acute or subacute evolution of a severe, neonatal-onset epileptic encephalopathy with diffuse, severe cavitary leukomalacia. Infants are usually born at term uneventfully, and they develop seizures in the first week of life that progress over the ensuing weeks in association with arrested development, acquired microcephaly, and early appearance of diffuse hypertonicity, evolving to severe, mixed motor and cognitive handicaps in survivors. Most children do not survive infancy. The clinical and radiographic features in the early stages mimic those seen in children with hypoxic-ischemic encephalopathy. The absence of a history of severe peripartum hypoxia or circulatory decompensation should prompt a search for other diagnoses. The severe cavitary leukomalacia seen in these patients is distinctive and is not typically seen after perinatal hypoxia-ischemia. It is more severe in cases of isolated sulfite oxidase deficiency than in cases with molybdenum cofactor deficiency [Dublin et al., 2002]. There are no associated malformative anomalies, systemic metabolic perturbations, or abnormalities affecting other organ systems. Diagnostic biochemical characteristics include increased urinary excretion of sulfites, thiosulfate, S-sulfocysteine, and taurine. Patients with molybdenum cofactor deficiency have low serum and urinary levels of uric acid and increased urinary levels of xanthine and hypoxanthine. These findings may vary according to protein intake and nutritional status. Patients with isolated sulfite oxidase deficiency have normal uric acid metabolite levels.
GMP
Guanosine sulfite
Amino acids
salts
Folinic Acid–Responsive Syndrome Hyland and Arnold [2002] have described a distinct syndrome of folinic acid–responsive seizures in a number of neonates who have refractory epileptic encephalopathies of unknown origin. Typically, the term neonates were born uneventfully, have no syndromic stigmata or other systemic disease, and develop refractory epilepsy in the first weeks or months of life. Analysis of cerebrospinal fluid for neurotransmitters by high-performance liquid chromatography reveals an unidentified peak. Treatment with folinic acid was found to be highly effective for controlling seizures in reported cases [Hyland and Arnold, 2002].
Menkes’ Disease Menkes’ disease is an X-linked recessive disorder that causes defective function of the intestinal copper transport protein, resulting in low tissue levels of copper and, secondarily, deficient function of numerous enzymes for which copper is a cofactor. The clinical phenotype invariably consists of severe neonatal-onset, chronic encephalopathy with refractory epilepsy. Infants typically have central hypotonia and developmental arrest with microcephaly. Distinguishing findings on examination, other than neurologic abnormalities, include redundant and hyperelastic skin; coarse, brittle hair; thin or absent eyebrows and eyelashes; and poor temperature stability. When examined under a microscope, hair fibers display the classic appearance of pili torti. Non-neurologic manifestations include vasculopathy with excess tortuosity and fragility, leading to thromboembolic stroke or subdural hemorrhage. This disease should be suspected in the setting of early infantile epileptic encephalopathy with the characteristic physical stigmata, and the diagnosis is supported by the biochemical findings of low levels of ceruloplasmin and serum copper. Treatment of patients with Menkes’ disease is supportive, with an emphasis on anticonvulsant management. Correction
IMP 3
Sulfur-containing
The diagnosis may be confirmed by enzyme assay of biopsied liver or cultured skin fibroblasts. Treatment is supportive, with an emphasis on optimizing anticonvulsant therapy. Dietary intervention with cysteine and thiamine supplementation and methionine restriction has been beneficial in isolated cases [Boles et al., 1993].
4 Guanine
3 Inosine 4 Hypoxanthine 5
2
1
MBD
Xanthine 5
Detoxification & degradation products
Uric acid
AMP 3 Adenosine 4 Adenine
FIGURE 18-8. Defects in purine metabolism caused by deficiencies in molybdenum cofactor deficiency (1) and isolated sulfite oxidase deficiency (2). Enzymes in purine metabolism are shown as 5’nucleotidase (3), purine nucleoside phosphorylase (4), and xanthine dehydrogenase(5), which requires molybdenum as a cofactor. AMP, adenosine monophosphate; GMP, guanosine monophosphate; IMP, inosine monophosphate; MBD, molybdenum.
Ichord / Perinatal Metabolic Encephalopathies
359
of serum copper levels with dietary supplements has been tried, with no beneficial effect on the neurologic manifestations of the disease.
limited benefit for the neurodevelopmental disability. Longterm outcome is variable, with most children affected by some degree of cognitive impairment.
Glucose Transporter Defects
Serine Biosynthesis Defects
DeVivo and associates [2002] characterized a deficiency syndrome arising from mutations in the neuronal glucose transporter GLUT1 (now designated SCL2A1). The disease manifests as early infantile-onset epileptic encephalopathy associated with a low cerebrospinal fluid concentration of glucose (mean, 30 mg/dL). The onset of seizures occurs between 4 weeks and 18 months of age, with a mean of 5 months. They include all clinical seizure types (i.e., focal, generalized, and myoclonic) and are resistant to antiepileptic drugs [Leary et al., 2003]. Affected infants have neurodevelopmental impairment of variable severity and acquired microcephaly. The cardinal biochemical feature is a decreased ratio of cerebrospinal fluid glucose relative to the plasma glucose concentration, typically less than 33%, which contrasts with the relatively high ratio of cerebrospinal fluid-to-blood glucose seen in term and premature newborns of 70% to 80% [Sarff et al., 1976], accompanied by low levels of the GLUT1 glucose transporter assayed in red blood cells. Conventional anatomic neuroimaging with CT or MRI is typically normal, whereas metabolic imaging with 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) reveals a distinctive pattern of hypometabolism in the thalami and mesial temporal regions [Pascual et al., 2002]. The ketogenic diet is the mainstay of treatment, resulting in good control of seizures in most patients, but it has
Defects in serine biosynthesis manifest as neonatal-onset, chronic encephalopathies with prominent refractory epilepsy [de Koning and Klomp, 2004]. Affected infants are neurologically abnormal at birth, with intrauterine growth retardation, congenital microcephaly, cataracts, seizures, and neurodevelopmental impairment. A distinctive pattern of leukoencephalopathy is seen on MRI, characterized by hypomyelination, vacuolar changes, and gliosis, which may improve after treatment with serine and glycine supplementation. The disease involves defective serine biosynthesis caused by 3-phosphyglycerate dehydrogenase deficiency (see Fig. 18-6). Clinical manifestations have been attributed to multiple mechanisms, including loss of neurotrophic effects of serine; impaired synthesis of glycine, which acts as a glutamate receptor co-agonist; and impaired synthesis of 5-methyltetrahydrofolate (5-MTHF), which is a cofactor for numerous brain enzyme pathways. Diagnosis can be made by finding low cerebrospinal fluid concentrations of serine, glycine, and 5-MTHF. In contrast to many inborn errors of metabolism, this disorder is potentially treatable by high-dose dietary supplementation of serine (200 to 600 mg/kg/day) and glycine (200 mg/kg/day).
SAICAR 1
SAICA riboside
AICAR 2 AICA riboside FAICR 2
S-Ado
S-AMP 1
GMP
IMP
AMP
Guanosine
Inosine
Adenosine
Guanine
Hypoxanthine
Adenine
Xanthine
Uric acid FIGURE 18-9. Defects in purine biosynthesis caused by deficiencies in adenylosuccinate lyase (1) and AICA riboside transformylase (2). AICA, 5-amino-4-imidazolecarboxamide riboside; AMP, adenosine monophosphate; FAICR, formyl-5-amino-4-imidazolecarboxamide riboside; GMP, GMP, guanosine monophosphate; IMP, inosine monophosphate; S-Ado, succinyladenosine; SAICA, succinyl-5- amino4-imidazolecarboxamide riboside.
Purine Biosynthesis Defects Defects of purine biosynthesis have been described with clinical manifestation in the neonatal period involving adenylosuccinate lyase or riboside transformylase enzyme deficiencies (Fig. 18-9) [Castro et al., 2002; Marie et al., 2004]. These infants are typically born uneventfully at term, manifest a severe neonatal encephalopathy with hypotonia and seizures, and have mildly dysmorphic facies. Neuroimaging may be normal initially, but over time may disclose diffuse atrophy. The long-term course is characterized by persistent, severe static encephalopathy with profound mental retardation, blindness due to optic atrophy, refractory epilepsy, and growth failure. The cardinal biochemical features include massive urinary excretion of the riboside metabolites 5-amino-4-imidazolecarboxamide ribosiduria (AICA) and succinyl-5-amino-4-imidazolecarboxamide ribosiduria (SAICA) in urine and cerebrospinal fluid. These metabolites give a positive result on the Bratton-Marshall test, which screens for high concentrations of succinyl purines. Diagnosis is confirmed by high-resolution thinlayer chromatography analysis of urine for succinyl purines. Affected infants may have disturbed glucose and lipid metabolism as a result of impaired hepatic gluconeogenesis, fatty acid, and cholesterol synthesis. Management is symptomatic and supportive because there is no definitive or curative treatment. L-Amino
Acid Decarboxylase Deficiency
L-Amino acid decarboxylase deficiency (L-ADD) is a defect of biogenic amine neurotransmitter metabolism, causing
360
Perinatal Acquired and Congenital Neurologic Disorders / 18 Tyrosine
6 3-o-methyldopa
5
L-dopa
5-HT
2
2
Dopamine
Serotonin
GTP
3
4
BH4 2
5-HIAA
Phenylalanine 1
BH2
Tyrosine
3 Norepinephrine
VLA
tryptophan
1
HVA L-dopa
4 Epinephrine
VMA
FIGURE 18-10. Defects in biogenic amine neurotransmitter metabolism: 1, tyrosine hydroxylase + BH4; 2, aromatic L-amino acid decarboxylase + B6; 3, dopamine β-hydroxylase; 4, phenylethanolamine-N-methyltransferase; 5, tryptophan hydroxylase + BH4; 6, catechol-ortho-methyl transferase (COMT). Affected metabolites and cofactors include homovanillic acid (HVA), vanillylmandelic acid (VMA), vanillactic acid (VLA), 5-hydroxy-tryptamine (5-HT), 5-hydroxy-indole acetic acid (5-HIAA), tetrahydrobiopterin (BH4).
a combined deficiency of brain dopamine, serotonin, norepinephrine, and epinephrine (Fig. 18-10) [Swoboda et al., 2003]. Patients commonly present in the first weeks of life with a progressive disorder affecting multiple levels of the nervous system. Symptoms and signs include lethargy, hypotonia, suck and swallow dysfunction, and seizures, sometimes associated with hypoglycemia and acidosis. Autonomic dysfunction leads to ptosis, hypotension, gastric and intestinal dysmotility, and poor temperature regulation. With advancing age, a distinctive movement disorder appears, consisting of dystonia, athetosis, oculogyric crises, and nonepileptic myoclonus. Diagnosis rests on evaluation of cerebrospinal fluid neurotransmitter profiles, which demonstrate increased levels of the biogenic amine precursors L-dopa and 5-hydroxytryptamine and decreased levels of the neurotransmitter metabolites homovanillic acid (HVA) and 5hydroxy-indole acetic acid (5-HIAA). Similar profiles of neurotransmitter amino acids are measured in plasma and urine. A clue to this disorder is the finding on a urine organic acid profile of elevated vanillacetic acid, a breakdown product from an alternate degradative pathway for L-dopa. Management is symptomatic and supportive. Attempts to treat by replacing deficient neuroactive amines have been hindered by the lack of an effective targeted delivery system. Outcome is poor for most patients, who develop mixed, severe motor and cognitive disabilities and chronic movement disorders that are refractory to symptomatic treatment.
Chronic Encephalopathies without Multiorgan Involvement Hyperphenylalaninemia Hyperphenylalaninemia causes a chronic encephalopathy with neonatal onset due to one of several defects in the metabolism of phenylalanine. These include phenylalanine hydroxylase deficiency, tetrahydrobiopterin (BH4) synthesis deficiency, and guanosine triphosphate cyclohydrolase deficiency (Fig. 18-11). In classic phenylketonuria caused by phenylalanine hydroxylase deficiency, plasma phenylalanine concentrations exceed 1000 μM, and liver biopsy reveals that phenylalanine hydroxylase activity is severely deficient
Biogenic amines
Fumarate
Acetoacetate
Gluconeogenesis
Ketogenesis
FIGURE 18-11. Defects in amino acid metabolism leading to hyperphenylalaninemia: 1, phenylalanine hydroxylase; 2, dihydropterin reductase; 3, guanine triphosphate (GTP) cyclohydrolase; 4,6-pyruvyltetrabiopterin synthase. BH2, dihydrobiopterin; BH4, tetrahydrobiopterin.
(A and R196H [Demelas et al., 2001]. D, DCX (band) mutation. The bottom row images demonstrate diffuse, thick, subcortical band heterotopia with no apparent gradient. The patient was a female with a missense mutation of DCX in exon 5: 668G>T and G223V [Matsumoto et al., 2001]. (Courtesy of Dr. William B. Dobyns, The University of Chicago, Department of Human Genetics, Chicago, Illinois. Images from patients LR00185 [A], LR00-056 [B], LP97-140a1 [C], and LP94-049 [D].)
412
Perinatal Acquired and Congenital Neurologic Disorders / 19
does not occur with other types of lissencephaly to be described later. Less common types often are associated with intermediate-thickness (8 to 12 mm) cortex, agenesis of the corpus callosum, or severe cerebellar hypoplasia [Dobyns and Truwit, 1995; Dobyns et al., 1999a; Hourihane et al., 1993; Kato et al., 1999; Ross et al., 2001]. Lissencephaly and subcortical band heterotopia are distinguished by both the pattern and the severity of the malformation. The pattern or gradient can be anterior more severe than posterior (a > p), posterior more severe than anterior (p > a), or, least often seen, anterior similar to posterior (a = p). The patterns and grades of lissencephaly and subcortical band heterotopia have become very important in distinguishing the different syndromes and genes associated with lissencephaly and subcortical band heterotopia [Dobyns et al., 1999b; Kato and Dobyns, 2003; Pilz et al., 1998]. Examples of the patterns associated with each of the major LIS genes are shown in Figures 19-29 and 19-30. Of importance, lissencephaly is frequently confused with severe, primary microcephaly and with polymicrogyria. Differentiating these clinical entities is important, because management and counseling depend critically on the correct diagnosis. CLINICAL CHARACTERISTICS
Children with lissencephaly or severe subcortical band heterotopia typically appear normal as newborns, although a few demomstrate apnea, poor feeding, or hypotonia. With most types of lissencephaly, seizures are uncommon during the first days of life. The epileptic spectrum is homogeneous, often starting as nonspecific seizures between 3 and 6
months of age, occasionally later. These are quickly followed by infantile spasms with hypsarrhythmia in a majority of children. In many children, the infantile spasms respond at first to corticotropin or other antiepileptic drugs, but almost all affected children will go on to have frequent seizures and severe mental retardation. Typical seizure types include myoclonic, tonic, and tonic-clonic; many meet criteria for Lennox-Gastaut syndrome. Profound mental retardation, early hypotonia, mild spastic quadriplegia, and opisthotonus also are seen. Many patients require a gastrostomy because of poor nutrition and repeated episodes of aspiration pneumonia [Dobyns et al., 1992]. By contrast, most patients with subcortical band heterotopia and uncommon patients with partial lissencephaly have mild to moderate mental retardation, although both normal intelligence and severe mental retardation have been seen. Other clinical features are minimal pyramidal signs and dysarthria [Barkovich et al., 1994; D’Agostino et al., 2002; Dobyns et al., 1996a]. Seizures usually begin in childhood but may appear much later, and multiple types occur that may be difficult to control. Cognitive development may slow after onset of seizures. The frequency and severity vary greatly. EEG investigations usually demonstrate generalized spike-and-wave discharges or multifocal abnormalities [Battaglia, 1996; D’Agostino et al., 2002; Palmini et al., 1991a]. Neurologic outcome usually correlates with the thickness of the subcortical band heterotopia as seen on MRI. Children with X-linked lissencephaly with abnormal genitalia are almost all males and have even more severe clinical problems [Kato et al., 2004]. Frequent and sometimes continuous seizures typically are seen on the first day
TABLE 19-16 Genes Associated with Malformations of Neuronal Migration and Cortical Organization GENE(S)
SYNDROME(S)
CLINICAL TESTING
Syndromes with Lissencephaly and Subcortical Band Heterotopia ARX XLAG, ACC, ISS, MR + DCX ILS, SBH, MR + LIS1 ILS, SBH + LIS1 and 14-3-3ε MDS + RELN LCH group B –
REFERENCE(S)
Bienvenu et al., 2002; Kato et al., 2004; Stromme et al., 2002b Gleeson et al., 1998, 2000b; Matsumoto et al., 2001 Cardoso et al., 2000, 2002; Pilz et al., 1998 Cardoso et al., 2003 Hong et al., 2000
Syndromes with Cobblestone Malformation FCMD FCMD, WWS
–
FKRP
MEB, WWS
–
LARGE POMT1 POMGnT1
MEB WWS, MEB MEB
– – –
Beltran-Valero de Bernabe et al., 2003; Kobayashi et al., 1998; Kondo-Iida et al., 1999; Silan et al., 2003 Beltran-Valero de Bernabe et al., 2004; Louhichi et al., 2004; Topaloglu et al., 2003 Longman et al., 2003 Beltran-Valero de Bernabe et al., 2002; Currier et al., 2005 Diesen et al., 2004; Taniguchi et al., 2003; Yoshida et al., 2001
–
Fox et al., 1998; Sheen et al., 2001
–
Sheen et al., 2003a, 2004
–
Chang et al., 2003; Piao et al., 2004
Syndromes with Periventricular Nodular Heterotopia FLNA Periventricular nodular heterotopia ARFGEF2 Microcephaly with periventricular nodular heterotopia Syndromes with Polymicrogyria GRP56 BFPP
ACC, agenesis of the corpus callosum; BFPP, bilateral frontoparietal polymicrogyria; FCMD, Fukuyama’s congenital muscular dystrophy; ILS, isolated lissencephaly sequence; ISS, infantile spasms; LCH, lissencephaly with cerebellar hypoplasia; MDS, Miller-Dieker syndrome; MEB, muscle-eye-brain disease; MR, mental retardation; WWS, WalkerWarburg syndrome; XLAG, X-linked lissencephaly with abnormal genitalia.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
of life, often in the delivery room, and generally do not respond to any form of therapy. Affected children also commonly have persistent hypothermia, hypotonia, very poor feeding, chronic diarrhea, and ambiguous or severely hypoplastic genitalia. The feeding problems and diarrhea combine to lead to very poor nutrition. LISSENCEPHALY SYNDROMES
Several different lissencephaly syndromes have been delineated that correlate well with the four LIS genes and one modifier gene identified to date. The most common lissencephaly syndromes are Miller-Dieker syndrome, isolated
A
B
C
D
413
lissencephaly sequence, subcortical band heterotopia, several types of lissencephaly with cerebellar hypoplasia, and X-linked lissencephaly with abnormal genitalia (XLAG). Most of these include the classic or four-layered (previously type 1) form of lissencephaly [Crome, 1956], whereas XLAG is characterized by a three-layered cortex [Bonneau et al., 2002], and one form of lissencephaly with cerebellar hypoplasia is associated with an unusual two-layered cortex [Kerner et al., 1999]. The syndromes associated with the cobblestone malformation (type 2 lissencephaly) are discussed in the next section. The different patterns of lissencephaly and associated genes are summarized in Table 19-16. FIGURE 19-30. Subtypes of lissencephaly (LIS) caused by LIS1 or unknown mutations. Midsagittal (left column), parasagittal (middle column), and axial (right column) magnetic resonance images from patients with four different forms of LIS. A, LIS1 (Miller-Dieker). The top row images depict severe, grade 1 LIS with diffuse agyria and no apparent gradient, very thick (15 to 20 mm) cortex, mildly enlarged lateral ventricles, intact corpus callosum that appears mildly flattened frontally, and normal brainstem and cerebellum. The patient was a female with MillerDieker syndrome with a large deletion of 17p13.3 extending from PAC95H6 to the telomere, with loss of LIS1, 14-3-3ε, and many other genes [Cardoso et al., 2003]. B, LIS1 (deletion). The second row images demonstrate grade 3 LIS with frontal pachgyria, posterior agyria, thick (15 to 20 mm) cortex, mildly enlarged lateral ventricles, the typical flattened corpus callosum, and normal brainstem and cerebellum. The patient was a female with typical ILS with mosaic deletion of PAC95H6 and LIS1 [Dobyns et al., 1999b]. C, LIS1 (missense). The third row images show mild frontal lobe hypoplasia, a transitional zone of thick cortex in the midfrontal region, and extensive posterior subcortical band heterotopia. The patient was an adult male with a missense mutation of LIS1 in exon 6: c.499T>C and S169P [Pilz et al., 1999]. D, LCH (no mutations identified). The bottom row images demonstrate severe, grade 1 LIS with diffuse agyria and no apparent gradient, very thick (15 to 20 mm) cortex, mildly enlarged lateral ventricles, intact corpus callosum that appears mildly small and flattened frontally, mild brainstem hypoplasia, moderate cerebellar vermis hypoplasia, and a large fluid collection beneath the cerebellum. The patient was a female in whom results of tests for LIS1 were negative. (Courtesy of Dr. William B. Dobyns, The University of Chicago, Department of Human Genetics, Chicago, Illinois. Images from patients LR01-167 [A], LP95132 [B], LP94-051 [C], and LP97041 [D].)
414
Perinatal Acquired and Congenital Neurologic Disorders / 19
Miller-Dieker syndrome is a striking multiple-congenitalanomaly syndrome characterized by classic lissencephaly, typical facial appearance, and variable other birth defects such as heart malformations. The facial features include prominent forehead, bitemporal hollowing, short nose with upturned nares, protuberant upper lip with thin vermilion border, and small jaw. The brain malformation consists of severe lissencephaly with no apparent gradient (see Figs. 19-29 and 19-30), although rare patients may have the same p > a gradient seen in patients with isolated lissencephaly sequence with LIS1 mutations [Cardoso et al., 2003; Dobyns et al., 1991]. All patients with Miller-Dieker syndrome have large deletions of chromosomal region 17p13.3 that include LIS1, 14-3-3, and all intervening genes, which indicates that the 14-3-3 gene is an important modifying factor for lissencephaly [Cardoso et al., 2003; Dobyns et al., 1991]. The isolated lissencephaly sequence consists of classic lissencephaly with a normal facial appearance except for mild bitemporal hollowing and small jaw [Dobyns et al., 1984, 1992]. Different patterns of lissencephaly have been found with mutations of the two known causative genes, DCX and LIS1. Isolated lissencephaly sequence associated with mutations of the X-linked DCX gene is characterized by either severe lissencephaly with no apparent gradient or lissencephaly with a clear a > p gradient (see Fig. 19-29B, C), and normal facial appearance [Dobyns et al., 1999b; Pilz et al., 1998]. Isolated lissencephaly sequence associated with mutations or deletions of the LIS1 gene is characterized by lissencephaly with a p > a gradient or, very rarely, a = p gradient (see Fig. 19-29B). Facial appearance may be normal or have subtle dysmorphism similar to that in Miller-Dieker syndrome but much less severe [Cardoso et al., 2003; Dobyns et al., 1992]. Subcortical band heterotopia occurs as an isolated malformation with rare exceptions. Most patients are female, because the most common cause is heterozygous mutations of the DCX gene on the X chromosome [Dobyns et al., 1996a; Matsumoto et al., 2001]. This represents the “carrier” phenotype found in female relatives of males with DCX-related lissencephaly. Many affected males, however, also have been reported [D’Agostino et al., 2002]. Mutations of DCX and LIS1, the same two genes that cause isolated lissencephaly sequence, have been identified that result in somewhat different patterns of malformation. Subcortical band heterotopia associated with mutations of DCX gene is characterized by diffuse thick subcortical band heterotopia with no apparent gradient (see Fig. 19-29D), or by partial frontal thin subcortical band heterotopia with an obvious a > p gradient [Gleeson et al., 2000a; Matsumoto et al., 2001]. Subcortical band heterotopia associated with mutations or deletions of the LIS1 gene is characterized by partial posterior thin or intermediate bands with an obvious p > a gradient (see Fig. 19-30C). This is a rare cause of subcortical band heterotopia, and most patients have mosaic mutations of LIS1 [D’Agostino et al., 2002; Pilz et al., 1999; Sicca et al., 2003] or deletions of 17p13.3 (unpublished data). The rare Baraitser-Winter syndrome consists of facial dysmorphism, typically including trigonocephaly and shallow orbits, colobomas of both iris and retina, and lissencephaly with an a > p gradient [Baraitser and Winter, 1988; Ramer et al., 1995; Rossi et al., 2003]. The lissencephaly
usually is relatively mild, with pachygyria most severe in the mid-frontal region that undergoes transition posteriorly to subcortical band heterotopia and then to a more normal gyral pattern, thus resembling the DCX pattern. The cause and pattern of inheritance are unknown. Lissencephaly with cerebellar hypoplasia comprises a small percentage of patients with lissencephaly syndromes. The most common type, designated lissencephaly with cerebellar hypoplasia group a, resembles isolated lissencephaly sequence, but with the addition of mild or, rarely, moderate cerebellar vermis hypoplasia. Indeed, some of these patients have mutations of DCX or LIS1, although the frequency is much less than among patients with typical isolated lissencephaly sequence. Lissencephaly with cerebellar hypoplasia group b consists of pachgyria with a subtle a > p gradient, moderate (8 to 10 mm) cortical thickness, globular hippocampus and small, afoliar cerebellum. Some patients with this imaging appearance have had mutations of RELN. In most patients with lissencephaly with cerebellar hypoplasia, mutation analysis of DCX and LIS1 is normal. Lissencephaly with cerebellar hypoplasia group c was defined based only on fetal pathologic examinations, which now appear to resemble the changes in lissencephaly with cerebellar hypoplasia group f. Lissencephaly with cerebellar hypoplasia group d resembles isolated lissencephaly sequence except that the lissencephaly is severe, typically generalized agyria, and the cerebellar vermis and hemispheres are usually small (see Fig. 19-30D). Results of mutational analysis of DCX and LIS1 were normal in several patients in this group. Lissencephaly with cerebellar hypoplasia group e consists of frontal agyria with an abrupt transition to a mildly simplified or normal cortex posteriorly. Lissencephaly with cerebellar hypoplasia group f consists of lissencephaly with agenesis of the corpus callosum, severe cerebellar hypoplasia, and a rare two-layered cortex. A similar two-layered cortex was found in brains in both lissencephaly with cerebellar hypoplasia group c and group f, so these groups likely should be combined into a single group c/f pending further experience. XLAG consists of variant lissencephaly in genotypic males with p > a gradient and intermediate (8 to 10 mm) thickness of cortex, agenesis of the corpus callosum that is most often complete, abnormal basal ganglia that often are cavitated or indistinct, severe postnatal microcephaly, and abnormal genitalia that are ambiguous or severely hypoplastic. Affected children have profound mental retardation, hypothalamic dysfunction with poor temperature regulation, intractable epilepsy with onset typically on the first day of life, infancy-onset dyskinesia that may be difficult to distinguish from seizures, and chronic diarrhea [Dobyns et al., 1999a; Kato et al., 2004]. Female relatives, including some mothers, have isolated agenesis of the corpus callosum. Mutations of the ARX gene have been found in almost all patients [Kato et al., 2004; Kitamura et al., 2002]. Other syndromes with lissencephaly and agenesis of the corpus callosum exist but appear to be very rare. Of importance, less severe mutations of the same gene, ARX, have been found in boys with cryptogenic infantile spasms, infancy-onset dyskinesia, and some less specific mental retardation and epilepsy syndromes [Bienvenu et al., 2002; Kato et al., 2003; Scheffer et al., 2002; Stromme et al., 2002a, 2002b, 2003; Turner et al., 2002; Wellington, 2003].
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
Studies in a mouse model have found that nonradial migration of inhibitory interneurons from the embryonic ganglionic eminence (the origin of the basal ganglia) to the neocortex is disrupted with loss of Arx [Kitamura et al., 2002]. A second X-linked gene associated with cryptogenic infantile spasms, CDKL5 or STK9, might have similar pathogenesis [Kalscheuer et al., 2003; Tao et al., 2004; Weaving et al., 2004]. GENETIC TESTING
All forms of lissencephaly and subcortical band heterotopia are genetic, and genetic testing is currently available for at least 80% of patients with lissencephaly or subcortical band heterotopia, although this varies with the specific phenotype. When lissencephaly or subcortical band heterotopia is suspected but the exact syndrome diagnosis is uncertain, the most productive order of testing is chromosome analysis and fluorescence in situ hybridization searching for deletions of chromosome 17p13.3 that include the LIS1 gene, followed by sequencing of LIS1, then DCX, and finally ARX. However, knowledge regarding the phenotype can be used by experienced specialists to change the order of tests, such as ordering testing of DCX first in females with subcortical band heterotopia or ARX first for males with lissencephaly and severe genital hypoplasia. Genetic testing for lissencephaly and subcortical band heterotopia is important, because several syndromes are associated with high risks of recurrence. This risk is especially great for parents who are carriers of a rearrangement of chromosome 17 and for mothers who carry ARX or DCX mutations. In Miller-Dieker syndrome, chromosome analysis identifies visible deletions of 17p13.3 in approximately 60% to 70% of patients, and fluorescence in situ hybridization detects deletions in the remaining patients. In approximately 30% of families, one parent is the carrier of a balanced chromosome rearrangement. The recurrence risk in these families is approximately 33% [Pollin et al., 1999]. For isolated lissencephaly sequence, the parents should be tested whenever mutations or small deletions of LIS1 have been found. When their results are normal, the recurrence risk is low, as we have not seen recurrence in more than 100 families. The possibility of recurrence exists with mosaicism in one parent, so the availability of prenatal diagnosis for future pregnancies is important. When mutations of DCX are found, the rules for X-linked inheritance apply [Dobyns et al., 2004]. Carrier testing in the mother is indicated, and fathers of female probands also are tested because such testing has identified one father who was a mosaic carrier of the mutation found in his affected daughter. The recurrence risk is 50% when the mother is found to be a carrier [Matsumoto et al., 2001], although this varies somewhat according to the phenotype in the affected child. The frequency of mosaicism among carrier mothers is high [Gleeson et al., 2000b; Matsumoto et al., 2001]. Recurrences in siblings in families when results of mutation analysis are negative have been described [Kuzniecky, 1994; Ramirez et al., 2004], and counseling is recommended for a 10% to 15% recurrence risk in this situation. When no testing has been done, counseling is more difficult. For subcortical band heterotopia, the same rules apply as for isolated lissencephaly sequence, except that the large majority of cases of subcortical band heterotopia are asso-
415
ciated with mutations of DCX, so most affected persons need counseling for X-linked inheritance. When mutations of LIS1 are found, these follow the same rules as for isolated lissencephaly sequence, except that mosaicism is more likely and would indicate a much lower risk of recurrence in siblings. When testing is negative, counseling is again recommended for a 10% to 15% recurrence risk, because both autosomal-dominant and autosomal-recessive forms of inheritance have been noted [Deconinck et al., 2003]. The inheritance of XLAG also is X-linked, and a large majority of patients with this phenotype have mutations of ARX. Thus, counseling for X-linked inheritance and testing for ARX mutations usually are indicated. Mothers often are carriers, some of whom have agenesis of the corpus callosum. The counseling for rare lissencephaly syndromes such as Baraitser-Winter syndrome and lissencephaly with cerebellar hypoplasia is less clear. Recurrence in several types of lissencephaly with cerebellar hypoplasia is possible, so counseling for autosomal-recessive inheritance is appropriate. Testing for RELN mutations is not available clinically. ANTENATAL DIAGNOSIS
Normal fetuses in the second and early third trimesters have a smooth brain surface with reduced number of gyri compared with the brain of a full-term child. Children with lissencephaly also have a reduced number of gyri. At present, it is not possible to differentiate lissencephaly from normal fetal brain reliably until the third trimester, usually between 32 and 36 weeks of gestation. Thus, fetal ultrasound examination and even fetal MRI performed before this time cannot reliably differentiate between normal and abnormal, and these tests should not be used. Successful prenatal diagnosis of lissencephaly has been performed by ultrasound late in the third trimester. When a chromosome abnormality or gene mutation has been identified in the affected child from a family, however, this result can be used for prenatal diagnosis for future pregnancies in that family. This has been used many times, as molecular diagnosis is now possible for a majority of patients with lissencephaly or subcortical band heterotopia. MANAGEMENT
Children with the most common lissencephaly syndromes, such as Miller-Dieker syndrome, isolated lissencephaly sequence, and subcortical band heterotopia, are often not recognized to have problems as newborns. A few children, especially those with Miller-Dieker syndrome, may have poor feeding and high bilirubin, but seizures are rare. By contrast, males with XLAG typically have severe seizures beginning on the first day of life and also have chronic hypothermia and diarrhea. Optimal management begins with early recognition and accurate counseling regarding the prognosis, because parents of children with the more severe forms may choose to limit life-sustaining interventions such as ventilation during severe illnesses. All or almost all children with lissencephaly or subcortical band heterotopia have seizures, often including infantile spasms, which may be difficult to treat. Early diagnosis and aggressive attempts to control seizures usually prove helpful in maintaining function. The epilepsy may consist of most types of seizures, and mixed types are common. Many children with lissencephaly go on
416
Perinatal Acquired and Congenital Neurologic Disorders / 19
A
B
C
D FIGURE 19-31. Subtypes of cobblestone lissencephaly. Midsagittal (left column), parasagittal (middle column), and axial (right column) magnetic resonance images from patients with four different cobblestone malformation syndromes. A, FCMD mutation. The top row images demonstrate mild frontal pachygyria with 7- to 8-mm-thick cortex, normal to mildly simplified gyral pattern posteriorly, widely open sylvian fissures especially on the left, moderately enlarged lateral ventricles, intact but stretched corpus callosum, normal brainstem, and moderate cerebellar hypoplasia and atrophy. These images are from a Japanese child with Fukuyama’s congenital muscular dystrophy (FCMD), who most likely is homozygous for the Japanese founder mutation consisting of addition of a 3-kb retrotransposon into the 3′ untranslated region of the FCMD gene [Kobayashi, 1998]. B, POMGnT1 mutation. The second row images show moderate frontal pachgyria with an 8- to 12-mm-thick cortex that extends into the parietal lobe, patches of abnormal white matter with high T2 signal intensity, hypoplastic brainstem especially in the pons, moderate cerebellar hypoplasia, and a few small cysts in the high white matter. The patient was a male with muscle-eye-brain disease due to a homozygous mutation of POMGnT1 in exon 20: c.1813delC and H573fs (patient CC described by Yoshida and colleagues [2001] and Taniguchi and associates [2003]). C, FKRP mutation. The third row images demonstrate diffuse agyria with an irregular surface, diffusely abnormal white matter with high T2 signal intensity, moderately enlarged lateral ventricles, very thin corpus callosum, hypoplastic brainstem with a prominent tectum, severe hypoplasia of the cerebellar vermis, moderate hypoplasia of the cerebellar hemispheres, large posterior fossa fluid collection, and overall enlarged posterior fossa. The patient was a female with a form of Walker-Warburg syndrome intermediate between the classic syndrome and muscle-eye-brain disease—the kink of the upper brainstem typically seen in Walker-Warburg is not present. She has a missense mutation of FKRP: c.953C>T and C318Y (patient 2 described by Beltran-Valero de Bernabe and co-workers [2004]). D, No mutation identified. The bottom row images show diffuse agyria with an irregular surface, diffuse abnormal signal of white matter with very high T2 signal intensity, very thin and likely hypoplastic corpus callosum, moderate to severely enlarged lateral ventricles, severe hypoplasia of the brainstem with the typical Walker-Warburg kinking at the junction of the pons and midbrain, severe cerebellar hypoplasia, small fluid collection in the posterior fossa, and overall small posterior fossa. This female has Walker-Warburg syndrome with no known mutation, although only POMT1 has been tested. (Courtesy of Dr. William B. Dobyns, The University of Chicago, Department of Human Genetics, Chicago, Illinois. Images from patients LR01-058 [A], LP95-146 [B], LP97-123 [C], and LR00-181 [D].)
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
417
to have the Lennox-Gastaut seizure syndrome, and their seizures may be managed as for those in patients with other causes for Lennox-Gastaut syndrome. They often have motor control problems (mixed hypotonia and spasticity), feeding problems, and gastroesophageal reflux, as in children with cerebral palsy, which may be managed similarly.
syndrome is the most severe, Fukuyama’s congenital muscular dystrophy the least severe, and muscle-eye-brain disease intermediate, and with the widest range of severity. This likely represents a semantic issue, because muscle-eyebrain disease is the diagnosis used for any intermediate phenotype.
OUTCOME
COBBLESTONE MALFORMATION SYNDROMES
Children with Miller-Dieker syndrome, severe isolated lissencephaly sequence (lissencephaly grades 1 to 3 and the more severely affected grade 4), most forms of lissencephaly with cerebellar hypoplasia, or XLAG have severe-toprofound mental retardation, mixed seizure types that often are intractable, chronic feeding problems that lead to recurrent pneumonia, and shortened lifespan. Most boys with XLAG die within the first several months of life, with a few living for 3 to 5 years. About half of all children with MillerDieker syndrome (defined as having large 17p13 deletions) pass away during the first 2 to 3 years of life, and few live past age 10 years. About half of the children with typical isolated lissencephaly sequence live for close to or beyond 10 years, but few live past 20 years. Most patients with mild isolated lissencephaly sequence (lissencephaly grade 4 that is not complete), lissencephaly with cerebellar hypoplasia group b, Baraitser-Winter syndrome, or subcortical band heterotopia live much longer.
Fukuyama’s congenital muscular dystrophy consists of relatively mild cobblestone complex, moderate-to-severe mental retardation and epilepsy, and severe congenital muscular dystrophy with progressive weakness, joint contractures, and elevated serum creatine kinase [Fukuyama and Osawa, 1984; Osawa et al., 1991]. The brain malformation is less severe than seen in either muscle-eye-brain disease or Walker-Warburg syndrome (see Fig. 19-31A). The causative FCMD gene was identified, as well as a common founder mutation, in the Japanese population [Kobayashi et al., 1998; Kondo-Iida et al., 1999]. This phenotype has not been associated with any other gene. Muscle-eye-brain disease consists of moderate cobblestone dysplasia with severe mental retardation, epilepsy, complex eye abnormalities, and congenital muscular dystrophy or myopathy with weakness, contractures, and elevated serum creatine kinase. The brain malformation typically is more severe frontally and is intermediate in severity between Fukuyama’s congenital muscular dystrophy and Walker-Warburg syndrome (see Fig. 19-31B). The white matter changes normalize somewhat over time, so in older patients this malformation can be confused with polymicrogyria, especially the frontoparietal type associated with mutations of GPR56 (see later). The brainstem and cerebellum are hypoplastic, but the brainstem lacks the distinctive kink at the midbrain-pons junction seen in most patients with Walker-Warburg syndrome. The eye anomalies consist of retinal and choroidal hypoplasia, optic nerve pallor, high-grade myopia, anterior chamber-angle abnormalities, glaucoma, iris hypoplasia, cataracts, and rare colobomas [Santavuori et al., 1989]. Although the most typical form of muscle-eye-brain disease occurs with mutations of POMGnT1, this syndrome has been associated with mutations of four different genes (see Table 19-16). Biochemical deficiency has been demonstrated in muscle [Zhang et al., 2003]. Walker-Warburg syndrome consists of severe cobblestone malformation leading to agyria (lissencephaly), as well as the most severe brainstem and cerebellar malformations of any of the cobblestone group of syndromes (see Fig. 19-31C, D). Most patients have hydrocephalus, and approximately 25% have occipital cephaloceles [Dobyns et al., 1985, 1989]. All patients with Walker-Warburg syndrome have profound mental retardation, epilepsy, eye abnormalities similar to those in muscle-eye-brain disease, and the same congenital muscular dystrophy or myopathy with elevated serum levels of creatine kinase and contractures as seen in muscle-eye-brain disease. Walker-Warburg syndrome has been associated with mutations of three different genes (see Table 19-16).
Cobblestone Complex Lissencephaly Cobblestone complex (previously “type 2 lissencephaly”), or cobblestone lissencephaly, is a severe brain malformation observed in three overlapping syndromes, all genetic with autosomal-recessive inheritance: Fukuyama’s congenital muscular dystrophy, muscle-eye-brain disease, and WalkerWarburg syndrome. The brain malformation consists of cobblestone cortex (a term first proposed by Haltia); abnormal white matter; enlarged ventricles, often with hydrocephalus; small brainstem; and small dysplastic cerebellum [Dobyns et al., 1985, 1989; Dubowitz, 1994; Haltia et al., 1997; Takada et al., 1988; Walker, 1942]. The abnormal cortex is severely disorganized with no recognizable layers and with disruption by abnormal vascular channels and fibroglial bands that extend into and often obstruct the subarachnoid space. The changes are widespread in the most severe syndrome (Walker-Warburg syndrome), which led to the term type 2 or cobblestone lissencephaly, but are less extensive in the other syndromes. The white matter is poorly myelinated with large numbers of heterotopic neurons. Associated brain abnormalities include obstructive hydrocephalus, brainstem hypoplasia, and cerebellar hypoplasia with cysts. The typical appearance of Fukuyama’s congenital muscular dystrophy, muscle-eye-brain disease, and Walker-Warburg syndrome on brain imaging is shown in Figure 19-31. In a few patients, absent septum pellucidum, absent corpus callosum, or occipital cephaloceles may be noted. The brain malformation frequently is associated with eye malformations and likely always associated with congenital muscular dystrophy. CLINICAL CHARACTERISTICS
The clinical course in all three syndromes consists of severe to profound mental retardation, severe hypotonia, mild distal spasticity, and typically poor vision. Walker-Warburg
GENETIC TESTING
All of the syndromes associated with the cobblestone malformation have definite autosomal-recessive inheritance.
418
Perinatal Acquired and Congenital Neurologic Disorders / 19
All of the known genes code for proteins known or suspected to be involved with glycosylation, particularly O-mannosylation of α-dystroglycan [Hewitt and Grewal, 2003; Ross, 2002]. Homozygous null mutations of αdystroglycan cause embryonic lethality in mice, but a brainspecific mouse knockout resulted in a brain malformation that closely resembles the cobblestone malformation [Moore et al., 2002]. Mutation analysis for these genes has been done in several research laboratories but is not available clinically. An enzymatic diagnostic test to assess function of POMGnt1 has been developed [Zhang et al., 2003], and testing for POMT1 may become available. ANTENATAL DIAGNOSIS
All or almost all patients with Walker-Warburg syndrome or muscle-eye-brain disease have greatly enlarged lateral ventricles, and many have frank hydrocephalus; many have a small cerebellum, and a few have gross microphthalmia. Each of these may be detected on prenatal ultrasound examination, usually in the mid- to late second trimester, and genetic ultrasound study has been used for prenatal diagnosis. Most affected fetuses should be detected, although no large series has been reported. Molecular genetic testing is possible only when a specific mutation has been identified in the proband. MANAGEMENT
Children with these syndromes have both the cobblestone brain malformation and congenital muscular dystrophy and so have a combination of hypotonia (from the brain and muscle disease) and spasticity (from the brain malformation). The muscle disease may be progressive, and the combination makes orthopedic and rehabilitation management more difficult. Although the causative genes may be the same, it is important to distinguish between these clinical syndromes as the prognosis and thus the management is different. Walker-Warburg syndrome is a very severe disorder associated with profound mental retardation and congenital hypotonia, and few children with true Walker-Warburg syndrome live past the age of 3 years. Some children who were reported to live longer than this might be better classified as having muscle-eye-brain disease. Once again, optimal management begins with early recognition and accurate counseling regarding the prognosis, because parents of children with Walker-Warburg syndrome may choose to limit life-sustaining interventions such as ventilation during severe illnesses. Seizures occur but are rarely as severe as those seen in patients with lissencephaly or subcortical band heterotopia. Careful seating is essential owing to severe hypotonia, and contractures need to be managed with physical therapy and splinting when needed. Congenital glaucoma and buphthalmos require care by an ophthalmologist. Treatment of other eye anomalies that can interfere with vision, such as retinal non-attachment or detachment, cataracts, and corneal opacity, should be considered on an individual basis, in view of the overall poor prognosis. The congenital muscular dystrophy probably progresses slowly over time, but this is not apparent clinically owing to the severe hypotonia and short survival period. Muscle-eye-brain disease and Fukuyama’s congenital muscular dystrophy are less severe, with survival into the teens and beyond; some patients have survived into their 40s. Seizures are common but less severe than in lissen-
cephaly or subcortical band heterotopia. The muscle disease slowly progresses, so that frequent evaluations to assess orthopedic, seating, and other rehabilitation needs are important. Children with Fukuyama’s congenital muscular dystrophy who learn to walk typically lose this skill several years later. Children with muscle-eye-brain disease have the same eye abnormalities as those found in Walker-Warburg syndrome, whereas children with Fukuyama’s congenital muscular dystrophy have only minor eye anomalies, if any. MANAGEMENT IN THE NEWBORN PERIOD
Most children with Walker-Warburg syndrome and some with muscle-eye-brain disease have congenital hydrocephalus, which usually requires a shunt. Children with Walker-Warburg syndrome and occipital cephaloceles usually do not have hydrocephalus at birth. Excision of the cephaloceles is frequently followed by hydrocephalus, however, so at the time of cephalocele removal, prophylactic shunt placement should be considered. Walker-Warburg syndrome is the most severe, with survival beyond 3 years rare. Fukuyama’s congenital muscular dystrophy is the least severe, with moderate-to-severe mental retardation, only minor eye abnormalities, and survival well into the second decade of life. Muscle-eye-brain disease is the most variable, with some cases almost as severe as Walker-Warburg syndrome and others associated with survival into the third or fourth decade. All children have severe (muscle-eye-brain disease and Fukuyama’s congenital muscular dystrophy) or profound (Walker-Warburg syndrome) mental retardation.
Neuronal Heterotopias Neuronal heterotopias consist of groups of neurons in an inappropriate location, typically either below or above the cerebral cortex although other abnormal locations are known. The most common type of heterotopia is located immediately adjacent to the lateral ventricles, known as periventricular or subependymal nodular heterotopia. Other types may be found in the subcortical white matter, throughout the thickness of the cerebral mantle, above the pia, or in several other locations. Examples of several types are shown in Figure 19-32. PERIVENTRICULAR NODULAR HETEROTOPIA
Periventricular nodular heterotopia consists of nodular masses of gray matter that line the ventricular walls and protrude into the lumen, resulting in an irregular outline (see Fig. 19-32A). Periventricular nodular heterotopia is a relatively common malformation that may be unilateral or bilateral, symmetric or asymmetric, and contiguous or noncontiguous [Dobyns et al., 1996a; Dubeau et al., 1995]. When the nodules are single or few in number, symptoms such as seizures may result, but such findings are unlikely to help with diagnosis. When the lesions are bilateral and numerous, a genetic basis is likely. Bilateral periventricular nodular heterotopia often is associated with hypoplasia of the corpus callosum or cerebellum, especially when the nodules are diffuse and contiguous, and have been associated with polymicrogyria. Pathology On gross examination, periventricular or subependymal heterotopia is seen as nodular masses of gray matter that line
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
419
FIGURE 19-32. Subtypes of heterotopia. Midsagittal (left column), parasagittal (middle column), and axial (right column) magnetic resonance images from patients with three different types of heterotopia. A, The top row images depict bilateral, nearly contiguous periventricular nodular heterotopia (PNH), an overlying normal gyral pattern, and mild cerebellar vermis hypoplasia, with all other structures normal. This is the typical pattern associated with mutations of FLNA, although testing has not been performed in this adult female patient. B, The second row images demonstrate a large mass of nodular heterotopia in the left frontal lobe that compresses the left lateral ventricle and extends up to fill much of the subcortical white matter. The overlying cortex appears normal. The mass of heterotopia enlarges the left frontal lobe so that it pushes across the midline to compress the right frontal lobe. This is the characteristic appearance of (giant) subcortical nodular heterotopia. C, The single axial image shows a rare transmantle heterotopia, which consists of a column of heterotopic cells that extends from the ventricular surface to the cortex. The lack of a cleft differentiates this condition from schizencephaly. (Courtesy of Dr. William B. Dobyns, The University of Chicago, Department of Human Genetics, Chicago, Illinois. Images from patients LR01-357m, LR03-202, and LR04-420m.)
A
B
C the walls of the lateral ventricles. Microscopically, the abnormal tissue contains both neurons and glial cells and forms clusters of rounded, irregular nodules separated by layers of myelinated fibers. The individual heterotopia may have no apparent disorganization or rudimentary lamination. Periventricular nodular heterotopia can be induced in the developing rat by intraperitoneal injection of the cytotoxic agent methylazoxymethanol acetate at embryonic day 15. In this model, reciprocal connections between the periventricular nodular heterotopia and normal cortex have been found supporting the hypothesis that neurons in the periventricular nodular heterotopia were destined for the cortex before the interruption of their migration [Colacitti et al., 1999]. Additional evidence comes from a report describing an elderly patient with Alzheimer’s disease and periventricular nodular heterotopia who had amyloid plaques in both the cortex and the nodular masses [Joseph, 1997]. Clinical Characteristics The most frequent manifestation of periventricular nodular heterotopia is epilepsy, occurring in 80% to 90% of patients. The age at onset is variable, but onset often is delayed until early adulthood [Battaglia et al., 1997]. Most patients have one or more types of partial seizures, which often are intractable. The associated EEG abnormalities are not specific, consisting of infrequent interictal discharges that may be
generalized, multifocal or focal. Pseudotemporal lobe localization has also been reported [Battaglia et al., 1997; Sisodiya et al., 1999]. Studies using depth electrodes in patients with periventricular nodular heterotopia and epilepsy have found the nodules to be intrinsically epileptogenic [Kothare et al., 1998]. A few patients have had chronic headache or other incidental symptoms, whereas others discovered during family evaluations are asymptomatic. Most patients with periventricular nodular heterotopia, especially females, have normal intelligence, although the curve may be shifted slightly to the left, with an average intelligence quotient (IQ) of approximately 85. Affected males are more likely to have mental retardation, reflecting the high frequency of the X-linked form of periventricular nodular heterotopia, which has a relatively mild phenotype, and possibly the existence of other X-linked periventricular nodular heterotopia syndromes. A skewed gender ratio toward females has been observed among patients with bilateral periventricular nodular heterotopia. Periventricular Nodular Heterotopia Syndromes Unilateral periventricular nodular heterotopia is less common than the bilateral form. In one large series, 14 patients had bilateral compared with 6 with unilateral periventricular nodular heterotopia [Dubeau et al., 1995]. The clinical manifestations are similar, including some patients without
420
Perinatal Acquired and Congenital Neurologic Disorders / 19
epilepsy and some with mental retardation. As suggested by anecdotal experience, unilateral periventricular nodular heterotopia may occur as part of other malformation syndromes. X-linked periventricular nodular heterotopia due to mutations of the filamin-A (FLNA) gene is the most common heterotopia syndrome and was recognized on the basis of observations of a skewed gender ratio toward females among sporadic patients, and reports of several families with multiple affected females and a decrease in the number of sons born to affected women, which suggested prenatal lethality of affected males [Dobyns et al., 1996a; Huttenlocher et al., 1994]. The causative gene was mapped to Xq28, and mutations were identified in FLNA [Eksioglu et al., 1996; Fox et al., 1998]. Females with this syndrome usually have bilateral, contiguous periventricular nodular heterotopia, with normal intelligence or mild learning problems and seizures [Dobyns et al., 1996a; Poussaint et al., 2000]. The phenotype in males varies widely, ranging from the mild female phenotype to prenatal lethality [Dobyns et al., 1996a; Guerrini et al., 2004; Huttenlocher et al., 1994; Sheen et al., 2001]. Several other causative genes for typical periventricular nodular heterotopia probably exist, because mutations of FLNA are detected in only 80% of familial and 20% of sporadic patients [Sheen et al., 2001]. Several pedigrees consistent with autosomal-recessive inheritance have been reported [Sheen et al., 2003a], and periventricular nodular heterotopia has been observed with two different deletions of chromosome 5p [Sheen et al., 2003b]. A few females have had periventricular nodular heterotopia and Ehlers-Danlos syndrome [Cupo et al., 1981; Thomas et al., 1996]. A rare autosomal-recessive syndrome of severe congenital microcephaly with bilateral periventricular nodular heterotopia has been described, and the causative gene identified as ARFGEF2 [Sheen et al., 2004]. Several other syndromes with periventricular nodular heterotopia have been described predominantly in males, including periventricular nodular heterotopia with syndactyly and severe mental retardation [Dobyns et al., 1997], with frontonasal malformation and moderate mental retardation [Guerrini and Dobyns, 1998], with short gut that in retrospect suggests a mutation of FLNA [Evrard, 1992; Nezelof et al., 1976], with nephrosis [Palm et al., 1986], and possibly with agenesis of the corpus callosum [Vles et al., 1990, 1993]. Finally, periventricular nodular heterotopia associated with overlying polymicrogyria has been reported [Leeflang et al., 2003] and may be relatively common. Genetic Testing Mutation analysis of FLNA and ARFGEF2 has so far been performed only in specialized research laboratories. For FLNA, the limiting factor is primarily its large size, which makes sequencing expensive. The availability of less costly methods is likely to eventually make this more available. Antenatal Diagnosis Periventricular nodular heterotopia and other heterotopias cannot be visualized reliably at prenatal ultrasound examination, and fetal MRI has not been evaluated for this purpose. When mutations of FLNA or ARFGEF2 have been identified, currently available only in research laboratories, diagnostic testing for the specific mutation is possible. The large majority of females with mutations of FLNA have nor-
mal intelligence, however, so prenatal diagnosis would be used more often for male fetuses. Management All patients with periventricular nodular heterotopia are at high risk for seizures, which should be treated aggressively. Temporal lobe surgery for patients with periventricular nodular heterotopia and associated hippocampal sclerosis generally has not been successful [Li et al., 1997]. Outcome The outcome is remarkably variable. Most affected persons with a few nodular masses and no underlying syndrome, as well as almost all females with X-linked periventricular nodular heterotopia and some others with bilateral periventricular nodular heterotopia syndromes, have normal intelligence or only mild learning disabilities. Other syndromes, especially those in males, are associated with severe mental retardation. Most patients have seizures, although onset may not occur until adulthood, and the seizures may be intractable. OTHER TYPES OF HETEROTOPIA
Although much less common and less recognized, other types of heterotopia are known. Subcortical nodular heterotopia consists of a large mass of heterotopic tissue expanding a portion of one cerebral hemisphere (see Fig. 19-32B). This lesion is rarely if ever bilateral and often is associated with ipsilateral periventricular nodular heterotopia, agenesis of the corpus callosum, and cerebellar vermis hypoplasia. Overlying cortical dysplasia may be seen rarely [Barkovich, 2000; Barkovich and Kjos, 1992b]. Despite the large size of the heterotopia, development may be normal or nearnormal, and onset of seizures may not begin until the third decade of life. Some patients have overlying cortical dysplasia, which leads to more severe problems including mental retardation. Transmantle heterotopia consist of a column of gray matter without nodular features that extends from the ventricular wall up to the cortical surface, where it is surrounded by a typically small area of cortical dysplasia (see Fig. 19-32C). All cases reported to date have been sporadic. Periventricular laminar heterotopia is rare and differs from periventricular nodular heterotopia in lack of nodularity. Several types likely exist, with some heterotopias appearing smooth and others ribbon-like. Excessive white matter neurons have been reported in patients undergoing epilepsy surgery and in postmortem studies. These abnormalities most often are seen in the temporal lobe and occasionally are seen in the frontal lobes. Isolated heterotopic neurons in the white matter in normal brains also are most numerous in the temporal lobes [Emery et al., 1997; Rojiani et al., 1996]. The clinical correlates of the pathologic disorder are not well understood, although these neurons appear to be increased in patients undergoing temporal lobe resections for seizures [Hardiman et al., 1988]. MRI studies may reveal an abnormal white-gray matter junction if the number of ectopic cells is large. No familial recurrence or specific gender or racial predominance has been observed.
Malformations of Cortical Organization This group includes malformations in which most neurons reach the cortex but do not form normal cortical layers or
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
intracortical connections, which suggests a later embryologic origin than the true neuronal migration malformations. The disorders in this group are characterized by an abnormal gyral pattern with moderately increased thickness of the cortex, typically 5 to 10 mm, in contrast with the normal thickness of 3 to 4 mm in most regions. The major malformations in this category include four-layered and unlayered polymicrogyria, schizencephaly, focal cortical dysplasia with normal cell types, and microdysgenesis.
Polymicrogyria and Schizencephaly Polymicrogyria is a cortical malformation characterized by abnormal cortical lamination, excessive cortical infolding
A
B
C
D
421
resulting in many small gyri separated by shallow sulci, fusion of the cortical molecular layer, and variable associated abnormalities such as heterotopia and enlarged ventricles. Schizencephaly consists of a deep cleft lined by cortex that extends from the pial surface down to the ventricular wall, and polymicrogyria involving cortex of the cleft and surrounding brain surface. Polymicrogyria and schizencephaly must be considered together as rare patients have schizencephaly on one side of the brain and polymicrogyria without a cleft on the other. Pathologic examination of the cortex in both polymicrogyria and schizencephaly typically shows a simplified fourlayered cortex that consists of the marginal layer, a
FIGURE 19-33. Subtypes of polymicrogyria (PMG) and schizencephaly. Midsagittal (left column), parasagittal (middle column), and axial (right column) magnetic resonance images from patients with four different malformations with polymicrogyria. A, The top row images demonstrate bilateral frontoparietal PMG with extensive involvement of the frontal and parietal lobes, extended sylvian fissure, patches of very bright T2 signal of white matter (again more severe frontally), mildly enlarged lateral ventricles, thin corpus callosum, and hypoplasia of the brainstem and cerebellum. The patient was a female with a missense mutation of the GPR56 gene in exon 3: 112C3T and R38W [Piao et al., 2004]. B, The second row images show bilateral perisylvian PMG involving the entire perisylvian region, with extension into the posterior parietal region, extended sylvian fissures, and otherwise normal brain structure. The patient was a male with X-linked perisylvian PMG [Villard et al., 2002]. C, The third row images demonstrate bilateral mesial parietooccipital PMG with irregular and highly infolded cortex in the medial parietal and occipital regions and mildly enlarged lateral ventricles posteriorly. D, The bottom row images demonstrate bilateral open lip schizencephaly with a small occipital cleft on the right, a large parieto-occipital cleft on the left, enlarged and dysplastic lateral ventricles on the right, partial agenesis of the corpus callosum, and normal brainstem and cerebellum. (Courtesy of Dr. William B. Dobyns, The University of Chicago, Department of Human Genetics, Chicago, Illinois. Images from patients LP93-017a2 [A], LP99146a1 [B], LP98-090 [C], and LR00-029 [D].)
422
Perinatal Acquired and Congenital Neurologic Disorders / 19
superficial cellular zone continuous with normal layers II to IV, a thin cell-sparse zone, and a deeper cellular zone continuous with layers V and VI that merges imperceptibly into the white matter. The cortex is thinner than normal, but appears thickened due to infolding or festooning of the cortical ribbon, which in more severely affected areas may resemble columns [Crome, 1952; Ferrer, 1984; Levine et al., 1974]. The walls of the shallow sulci are fused in their deeper portions, and have small penetrating blood vessels. The small and tightly packed microgyri mimic the appearance of pachygyria, leading to frequent misdiagnosis by clinicians. Less often, these layers cannot be distinguished and the malformation is designated “unlayered” polymicrogyria. This distinction persists in the literature, although a careful review demonstrates that both the four-layered and unlayered types have been found in patients with similar forms of schizencephaly, lending some uncertainty to the validity of this separation. MRI in polymicrogyria demonstrates loss of the normal gyral pattern, an irregular or pebbled brain surface, increased numbers of small, approximately 2- to 5-mmwide gyri separated by very shallow sulci, and an irregular border between the cortex and underlying white matter (Fig. 19-33). The cortex is mildly to moderately thick, usually 5 to 10 mm, compared with the normal thickness of 3 to 4 mm. The underlying white matter often is thinner than usual, and in several rare polymicrogyria syndromes, additional striking white matter abnormalities are seen. Whenever the perisylvian region is involved, the sylvian fissures extend further posteriorly and upward than usual to merge with cortex of the parietal convexity. MRI in schizencephaly reveals the same cortical abnormalities plus the deep cleft, which can be open or closed; the sides of an open-lipped cleft are separated by cerebrospinal fluid, whereas the sides of closed-lip clefts are apposed and may appear as a column of gray matter [Barkovich and Kjos, 1992a].
mental delay and mental retardation, seizures, spasticity, and the associated musculoskeletal and feeding problems. These vary greatly in severity, so that predicting outcome in young infants may be difficult, but some general guidelines have emerged from clinical experience with many patients. The major prognostic factors across all types of polymicrogyria and schizencephaly include head size at birth, the localization and extent of polymicrogyria, and the motor examination. The most unfavorable prognostic factors are microcephaly, especially severe congenital microcephaly with birth head size more than 3 SD below the mean, involvement of extensive areas of the brain, especially the frontal lobes, and the presence of spastic quadriparesis. Involvement of the primary motor cortex is typically associated with spasticity. Patients with polymicrogyria restricted to the perisylvian region, especially the posterior perisylvian region, often have pseudobulbar palsy with the accompanying severe oromotor and speech apraxia. Patients with unilateral or very asymmetric polymicrogyria or schizencephaly, and those with relatively small regions of the brain affected, especially when the frontal lobes are spared, may have mild cognitive and motor deficits. Nevertheless, all are at high risk for seizures, which have been reported in more than 80% of patients, most with severe epilepsy. The seizures consist of atypical absences, tonic-atonic attacks, and generalized tonic-clonic seizures. EEG abnormalities include generalized spike-and-wave or multifocal abnormalities. A syndrome consisting of unilateral central polymicrogyria and transient nonconvulsive status epilepticus has been reported [Caraballo et al., 1999]. Many patients have epilepsy that remains relatively amenable to medical treatment until puberty, when seizures become intractable. They may improve again after puberty has passed. In many patients, the seizures remain under relatively good control during adult years and may abate with medication adjustments.
PATHOGENESIS
POLYMICROGYRIA AND SCHIZENCEPHALY SYNDROMES
For most but not all brain malformations, evidence supporting nongenetic causes such as teratogens or external agents is weak or does not exist. For polymicrogyria, recent experience again demonstrates several genetic causes but also supports extrinsic causes such as intrauterine viral infections and impaired vascular supply to the fetus. This possibility complicates diagnosis, genetic counseling, and research but must always be taken into consideration. The best-understood causes are reviewed along with other genetic syndromes. CLINICAL CHARACTERISTICS
Polymicrogyria and schizencephaly only rarely involve the entire brain, and the clinical presentations associated with these malformations vary according to head size and the localization and extent of the cortical malformation. When the correct interpretation of brain imaging studies as lissencephaly or polymicrogyria is in doubt, the clinical examination can be helpful. A large majority of patients with lissencephaly have diffuse hypotonia with no spasticity or minimal spasticity in the distal extremities, whereas most patients with polymicrogyria or schizencephaly have spasticity. The most common clinical problems found in patients with polymicrogyria or schizencephaly include develop-
The number of syndromes with polymicrogyria or schizencephaly has been expanding rapidly during the past decade, most with different regional patterns of polymicrogyria or different associated brain malformations. Based on a study of more than 200 patients still in progress, the perisylvian form of polymicrogyria appears to be by far the most common, accounting for about two thirds of patients [R.J. Leventer and W.B. Dobyns, unpublished data]. This and other forms are listed in Table 19-17. Seven of these have been reported at least once, whereas several others have been recognized but are not yet fully delineated. In addition, polymicrogyria occurs in numerous multiple congenital anomaly syndromes, including Adams-Oliver syndrome, Aicardi’s syndrome, homozygous PAX6 syndrome, micro syndrome, and thanatophoric dysplasia [Aicardi et al., 1965; Amor et al., 2000; Donnenfeld et al., 1989; Glaser et al., 1994; Graham et al., 2004; Hall-Craggs et al., 1990; Savarirayan et al., 1999; Shigematsu et al., 1985; Yamaguchi and Honma, 2001]. Bilateral Frontal Polymicrogyria Bilateral frontal polymicrogyria consists of bilateral and symmetric polymicrogyria of the frontal lobes extending back to the precentral sulcus posteriorly and the frontal
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
423
TABLE 19-17 Polymicrogyria-Schizencephaly: Types and Syndromes SYNDROME
INHERITANCE (Causative Genes)
Established Syndromes with Polymicrogyria (PMG) Frontal PMG (only) AR, sporadic Frontoparietal PMG with brainstem AR (GPR56) and cerebellar hypoplasia Perisylvian PMG AD, AR, XL, chromosomal, sporadic Lateral parieto-occipital PMG Sporadic Mesial parieto-occipital PMG Sporadic Schizencephaly CMV, sporadic, vascular Septo-optic dysplasia with schizencephaly Suspected Syndromes with PMG* Diffuse PMG MIC with diffuse PMG MIC with diffuse PMG and PNH MIC with asymmetric PMG Familial schizencephaly Parasagittal PMG Perisylvian or diffuse PMG with diffusely abnormal white matter Perisylvian PMG with frontal PNH Posterior-temporal PMG and PNH
CMV, sporadic, vascular
AR, XL, sporadic Sporadic Sporadic AR, XL AR Sporadic Sporadic
REFERENCE(S)
Guerrini et al., 2000 Chang et al., 2003; Piao et al., 2004 Gropman et al., 1997; Guerreiro et al., 2000; Kuzniecky et al., 1993; Villard et al., 2002 Ferrie et al., 1995 Guerrini et al., 1997 Barkovich and Kjos, 1992a; Barkovich et al., 1989; Barth and van der Harten, 1985; Iannetti et al., 1998; Norman, 1980; Sener, 1998 Kuban et al., 1989; Miller et al., 2000; Sener, 1996
See legend
Sporadic Sporadic
AD, autosomal dominant; AR, autosomal recessive; CMV, cytomegalovirus; MIC, microcephaly (below −3 standard deviations at birth); PNH, periventricular nodular heterotopia; XL, X-linked. *The suspected syndromes have been identified by an informal PMG study group (A.J. Barkovich, W.B. Dobyns, R. Guerrini, R. Kuzniecky, and R. Leventer) but have not been fully delineated. Diffuse or generalized PMG has been reported [Chang et al., 2004], but the series was composed largely of patients we classify as having severe perisylvian PMG or Adams-Oliver syndrome.
operculum inferiorly. Most patients present with developmental delay and mild spastic quadriparesis and have variable mental retardation, language impairment, and epilepsy [Guerrini et al., 2000]. Bilateral Frontoparietal Polymicrogyria Bilateral frontoparietal polymicrogyria is a syndrome of autosomal recessive inheritance characterized by polymicrogyria involving the frontal and parietal lobes, with variable extension to the posterior temporal and occipital lobes (see Fig. 19-33A). Accompanying features include brainstem and cerebellar hypoplasia, patchy abnormal white matter signal changes, and enlarged ventricles [Chang et al., 2003]. No pathologic examinations have been reported, so the classification as polymicrogyria is based only on brain imaging. Clinical experience indicates that the microgyri tend to be less prominent than with other forms of polymicrogyria, so future pathologic studies might demonstrate a polymicrogyria variant or possibly a form of cobblestone malformation. The white matter signal changes and cerebellar hypoplasia resemble the abnormalities seen with the cobblestone malformation, with which it can easily be confused [Dobyns et al., 1996b]. Numerous patients have been reported, often classified as having other malformations, so it may prove to be a relatively common malformation [Dobyns et al., 1996b; Farah et al., 1997; Harbord et al., 1990; Straussberg et al., 1996; Sztriha and Nork, 2000]. The clinical features include global developmental delay and mental retardation of at least moderate severity, seizures, dysconjugate gaze, and bilateral pyramidal and cerebellar signs.
The locus for bilateral frontoparietal polymicrogyria was mapped to chromosomal region 16q12-q21, and the gene recently was identified as GPR56, an orphan G proteincoupled receptor with a large extracellular domain whose function is not yet understood [Piao et al., 2002, 2004]. Perisylvian Polymicrogyria Perisylvian polymicrogyria, also known as the congenital bilateral perisylvian syndrome, was first described in 1926 but has been widely recognized only in the past decade [Kuzniecky et al., 1993]. In the most typical form, patients present with prominent pseudobulbar paresis, in the form of swallowing difficulties and aspiration, inability to protrude the tongue, dysarthria and facial diplegia. They also have mild-to-severe mental retardation and seizures. At the mild end of severity, the syndrome certainly overlaps with congenital suprabulbar palsy, also known as Worster-Drought syndrome [Clark et al., 2000; Nevo et al., 2001]. It may manifest with much greater severity, however. For example, children may have developmental delay, poor palatal function, hypotonia, arthrogryposis, hemiparesis, apnea, motor deficits, micrognathia, and pectus excavatum [Gropman et al., 1997]. Seizures of varying types and severity have been reported in 58% to 87% of children [Gropman et al., 1997; Kuzniecky et al., 1994a, 1994b]. Brain imaging most often shows polymicrogyria that involves the sylvian fissures and surrounding opercular cortex [Kuzniecky and Andermann, 1994], but the extent and associated clinical findings vary greatly (see Fig. 19-33B). In the least severe form, perisylvian polymicrogyria may be restricted to a small region of the posterior sylvian fissure,
424
Perinatal Acquired and Congenital Neurologic Disorders / 19
whereas in the most severe form, it may involve the entire brain but appears most severe in the perisylvian regions and typically spares the mesial occipital regions (personal observation). Perisylvian polymicrogyria may be bilateral and symmetric, bilateral and highly asymmetric, or unilateral. In most cases, highly asymmetric or unilateral polymicrogyria has a perisylvian distribution. Perisylvian polymicrogyria usually is sporadic, although numerous families with multiple affected persons have been reported. Most studies have suggested X-linked inheritance, and a locus was mapped to Xq28, but data from other families suggest autosomal-dominant or autosomal-recessive inheritance [Bartolomei et al., 1999; Borgatti et al., 1999; Caraballo et al., 2000; Guerreiro et al., 2000; Villard et al., 2002]. It also has been associated with structural chromosome abnormalities. The most frequent of these is deletion 22q11.2, with approximately 10 patients reported [Bingham et al., 1998; Ehara et al., 2003; Ghariani et al., 2002; Kawame et al., 2000; Sztriha et al., 2004; Worthington et al., 2000], although other less common loci also have been described, such as deletion 1p36 [Shapira et al., 1999] and deletion 1q44 [Zollino et al., 2003]. Mesial Parieto-occipital Polymicrogyria Bilateral mesial or parasagittal parieto-occipital polymicrogyria is an uncommon subtype of polymicrogyria associated with epilepsy [Guerrini et al., 1997]. Brain imaging shows a very focal and typically symmetric malformation (see Fig. 19-33C). Although the location in watershed regions of the anterior and posterior cerebral arteries suggests postmigratory perfusion failure as a possible etiology, the consistent focal location suggests disruption of a developmental gene, so the cause is not known. No familial recurrence has been reported. The clinical presentation is related primarily to epilepsy, with mean age at onset of 9 years. Most patients have had partial seizures, with or without minor automatisms, that were typically intractable. Interictal EEG tracings show diffuse and bilateral parieto-occipital or temporal abnormalities. Intelligence and findings on the neurologic examination were normal in most patients, although some had mild mental retardation. Occipital Polymicrogyria Several patients with polymicrogyria restricted to the occipital lobes were reported along with other cortical pathologies such as focal cortical dysplasia [Kuzniecky et al., 1997]. Most presented with seizures, with mean age at onset of 8 years. Epileptic visual symptoms correlated well with the EEG abnormalities and the brain imaging findings. Most patients had normal results on visual field testing. Cortical resections resulted in good seizure control. Schizencephaly Schizencephaly, or “cleft brain,” is a relatively common brain malformation characterized by full-thickness clefts extending from the brain surface to the ventricular wall (see Fig. 19-33D). Most but not all of these clefts are located in the region of the sylvian fissures [Barkovich and Kjos, 1992a; Barkovich and Norman, 1988]. The clefts may be open and therefore filled with cerebrospinal fluid, or closed with the sides of the cleft touching. They are lined by dysplastic cortex that has the appearance of either four-layered or unlayered polymicrogyria, and polymicrogyria surrounds the sides of the cleft for variable distances [Crome, 1952; Norman et al., 1995]. It
usually has been considered to be due to an encephaloclastic process secondary to fetal ischemic injury, typically in the distribution of the middle cerebral artery, based on the pathologic appearance [Friede, 1989] and an association with twinning [Barth and van der Harten, 1985; Norman, 1980; Sugama and Kusano, 1994], congenital cytomegalovirus infections [Barkovich and Lindan, 1994; Hayward et al., 1991; Iannetti et al., 1998; Sener, 1998], and rarely other factors in which the fetal vascular supply is affected, such as maternal warfarin therapy [Barth, 1992; Levine et al., 1974; Pati and Helmbrecht, 1994]. Rare examples of familial schizencephaly have been reported, however, which supports causal heterogeneity [Hilburger et al., 1993; Robinson, 1991]. Schizencephaly usually occurs with no associated brain malformation other than polymicrogyria, but a syndrome of septooptic dysplasia (absent septum pellucidum and optic nerve hypoplasia) together with schizencephaly has been reported [Aicardi and Goutieres, 1981; Barkovich et al., 1989; Kuban et al., 1989; Sener, 1996] and some affected infants also have agenesis of the corpus callosum. A few patients with septooptic dysplasia have had polymicrogyria without clefts rather than schizencephaly, again demonstrating the relationship between these malformations [Miller et al., 2000]. Clinical experience suggests that in many if not most patients with typical schizencephaly, the septum pellucidum is absent or partially absent, so isolated schizencephaly and septo-optic dysplasia with schizencephaly may well be part of a single spectrum. Clefts are not seen in the well-defined regional polymicrogyria syndromes, however, implying that multiple causes may lead to polymicrogyria. The clinical manifestations in schizencephaly are related to the size and type of defect. Children with unilateral schizencephaly typically have mild or moderate impairments, whereas those with bilateral lesions usually have more severe mental retardation, epilepsy, and generalized spasticity [Barkovich and Kjos, 1992a; Granata et al., 1996; Packard et al., 1997]. Clinical findings usually are commensurate with the size of the lesion [Aniskiewicz et al., 1990; Barkovich and Kjos, 1992a]. Children with closed-lip schizencephaly may present with hemiparesis or motor delay, whereas those with open-lip schizencephaly are more likely to present with hydrocephalus or seizures. In one series, 57% of patients had seizures, 91% had associated cerebral developmental anomalies, and 45% had absent septum pellucidum [Packard et al., 1997]. In patients with larger clefts, seizures usually are focal and often intractable, but clinical variability is observed. Despite gross structural lesions, EEG localization often is regional rather than focal. The central location of the lesions and widespread areas of epileptogenic activity often render surgery impossible. Mutations of the EMX2 homeobox gene were reported in several patients with schizencephaly [Brunelli et al., 1996; Faiella et al., 1997]. The clinical findings in these patients were not described, however, and several of the sequence changes were intronic and open to alternative interpretations. This result has never been confirmed by further reports, and the proposed association likely is not true, although a definitive study has not appeared. Genetic Testing All patients with polymicrogyria should have chromosome analysis performed, as well as fluorescence in situ hybridization analysis for deletions of 22q11.2 (DiGeorge’s syn-
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
425
drome region) and fluorescence in situ hybridization with a set of subtelomeric probes to pick up small deletions of 1p36, 1q44, and possibly other regions of interest. These tests are indicated even if the child does not look like he or she has DiGeorge’s or velocardiofacial syndrome. Sequencing of GPR56, the causative gene for bilateral frontoparietal polymicrogyria, is not available clinically, although testing on a research basis has been possible in some instances.
varying recurrence risks. Preliminary data suggest a recurrence risk of 5% to 10% for families with female probands and of 10% to 20% for families with affected male probands, which reflects a mild skewing of the gender ratio toward males and the known X-linked inheritance [Guerreiro et al., 2000]. The recurrence risk for schizencephaly, including septooptic dysplasia with schizencephaly is very low.
Antenatal Diagnosis As with lissencephaly and subcortical band heterotopia, it is not possible to differentiate polymicrogyria from normal fetal brain reliably until the third trimester, usually between 32 and 36 weeks of gestation. Thus, fetal ultrasound examination and even fetal MRI performed before this time cannot reliably differentiate between normal and abnormal and should not be used. The clefts in schizencephaly may be seen by imaging, but their time of origin is unclear; this is less important, because the recurrence risk for schizencephaly is extremely low. When a specific chromosome abnormality or gene mutation has been identified in the affected child from a family, this result can be used for prenatal diagnosis for future pregnancies in that family.
Focal cortical dysplasia without balloon cells or other abnormal cell types, also designated architectural dysplasia, is a mild cortical malformation characterized by abnormal cortical lamination and ectopic neurons in white matter [Colombo et al., 2003b; Palmini et al., 2004; Tassi et al., 2002]. Brain imaging demonstrates subtle lobar or gyral hypoplasia, mild atrophy of underlying white matter, moderately increased T2 and decreased T1 signal intensity of white matter, and sometimes mild blurring of the gray-white border and mildly increased thickness of the cortex [Colombo et al., 2003a, 2003b; Palmini et al., 1991b]. The distinction between pure focal cortical dysplasia (architectural dysplasia) and focal cortical dysplasia with abnormal cell types (cytoarchitectural dysplasia and Taylor-type dysplasia) is clear with histopathologic examination but is not always possible on brain imaging [Colombo et al., 2003b]. Microdysgenesis is a similar but microscopic malformation that consists of neurons in the marginal layer, subtle changes in laminar architecture, and excess neurons in white matter [Meencke and Janz, 1984; Thom et al., 2001]. No changes are seen on brain imaging. Both pure focal cortical dysplasia (architectural dysplasia) and microdysgenesis require histopathologic confirmation for diagnosis, typically obtained only after epilepsy surgery, and both may occur with hippocampal sclerosis, the so-called dual pathology.
Management Optimal management begins with early recognition and accurate counseling regarding the prognosis, because parents of children with the more severe forms may choose to limit lifesustaining interventions such as ventilation during severe illnesses. Many children with polymicrogyria have much less severe problems, however, and must be approached individually. A large majority of patients with polymicrogyria have seizures, which may prove difficult to treat. Early diagnosis and aggressive attempts to control seizures usually prove helpful in maintaining function. The epilepsy may consist of almost any type of seizures, and mixed types are common. Some children have severe seizures during puberty that become easier to control later on. Patients with polymicrogyria and schizencephaly often have motor control problems, especially spasticity, feeding problems, and gastroesophageal reflux, as in children with cerebral palsy or lissencephaly, which may be managed similarly. The orthopedic problems often are more severe than in lissencephaly and may be managed as for any child with spastic cerebral palsy. Outcome The outcome for patients with polymicrogyria or schizencephaly is highly variable and related to head size at birth, extent of brain involvement, and severity of changes on the neurologic examination. The most useful indicators for a poor outcome include congenital microcephaly (below −2 SD, and especially below −3 SD), bilateral involvement of large brain regions, and spastic quadriparesis. Counseling The recurrence risk for autosomal recessive forms of polymicrogyria is typically 25%, and persons with rare subtypes with unknown inheritance patterns should be counseled for the possibility of recessive inheritance and the accompanying 25% risk. Both perisylvian and the very rare true diffuse forms of polymicrogyria sometimes have X-linked inheritance. The most common perisylvian form of polymicrogyria has multiple potential genetic causes, with widely
Focal Cortical Dysplasia and Microdysgenesis
CLINICAL CHARACTERISTICS
Because confirmation of the diagnosis usually is obtained only in patients with severe epilepsy leading to surgical treatment, the full spectrum of clinical manifestations have not been well described. Cortical dysplasia without balloon cells and milder forms of microdysgenesis are usually reported in patients with epilepsy [Kuzniecky et al., 1991]. As for focal dysplasias associated with balloon cells, the clinical abnormalities correlate with location of the lesions. Both are found most frequent in the frontal lobes, followed by the temporal regions. In most individuals, the malformations do not follow any boundaries between various regions and usually involve more than a single gyrus or lobe. Familial recurrence has not been reported, and the causes are not known.
Management and Outcome Management primarily involves treatment of the epilepsy. The associated seizures are focal in origin, as would be expected from the pathology, and may become intractable. The outcome is related to the success of seizure management.
HYDROCEPHALUS Hydrocephalus results from obstruction of cerebrospinal fluid egress from the ventricular system, reduced absorption from arachnoid villi, or rarely, excess production of cerebro-
426
Perinatal Acquired and Congenital Neurologic Disorders / 19
spinal fluid within an abnormal choroid plexus [Aronyk, 1993]. The excess cerebrospinal fluid enlarges the cerebral ventricles and elevates intracranial pressure, which produces the clinical manifestations of hydrocephalus. Hydrocephalus is a common problem. It is estimated that approximately 125,000 persons are living with shunts and that 33,000 shunts are placed annually in the United States [Bondurant and Jimenez, 1995].
Pathophysiology Most of the cerebrospinal fluid (70%) is secreted by the choroid plexus within the cerebral ventricles. Extrachoroidal cerebrospinal fluid production in subarachnoid sites and by way of a transependymal route has been documented [Fishman, 1980]. About 20% or more of cerebrospinal fluid is derived from brain extracellular fluid created as a by-product of cerebral metabolism [Rekate, 1997]. Normally, rates of production (0.35 mL per minute) and absorption of cerebrospinal fluid are equal. Total cerebrospinal fluid volume is 65 to 140 mL in children and 90 to 150 mL in adults. The process of cerebrospinal fluid formation by the choroid plexus includes plasma ultrafiltration and secretion. Secretion, an energy-dependent process, is initiated by hydrostatic pressure in the choroidal capillaries and by active transport of sodium. The enzymes sodium-potassium ATPase and carbonic anhydrase partly regulate cerebrospinal fluid secretion [Fishman, 1980]. By contrast, the process of cerebrospinal fluid reabsorption is not an energy-dependent process [Rekate, 1997]. After formation, cerebrospinal fluid exits from the lateral ventricles through the foramen of Monro into the third ventricle (Fig. 19-34). Cerebrospinal fluid then traverses the aqueduct of Sylvius into the fourth ventricle and enters the
Superior cerebral vein
subarachnoid space through the foramina of Luschka and Magendie. Information gained from MRI analysis of cerebrospinal fluid movement demonstrates pulsatile toand-fro motion of cerebrospinal fluid within the lateral ventricles, produced from a brain-pumping motion that ejects the cerebrospinal fluid and causes a net downward flow [Feinberg and Mark, 1987]. Cerebrospinal fluid is absorbed into the vascular system through the arachnoid villi within the arachnoid granulations covering the brain and spinal cord leptomeninges [Alksne and Lovings, 1972; Welch, 1975]. A layer of endothelium within the arachnoid villi separates the subarachnoid cerebrospinal fluid space from the vascular system. Water and electrolytes pass freely across these arachnoid membranes. Larger proteins and macromolecules cannot pass through intercellular junctions but are selectively transported across the cytoplasm of endothelial cells by an active process involving micropinocytosis [Alksne and Lovings, 1972]. Cerebrospinal fluid also is absorbed by the choroid plexus, leptomeninges, ventricular ependyma, and lymphatics [Fishman, 1980]. Increased absorption through the arachnoid villi protects the brain from transient increases in intracranial pressure [Mann et al., 1978].
Classification Because many processes and structures affect cerebrospinal fluid dynamics [Davson, 1972], hydrocephalus results from multiple causes [Guiffre et al., 1995]. Inadequate absorption of cerebrospinal fluid is the prime mechanism producing hydrocephalus. A blockage of cerebrospinal fluid circulation at any point from the site of production to the site of absorption through the arachnoid villi enlarges the proximal cerebral ventricles because of excessive cerebrospinal fluid accumulation.
Arachnoidal granulation
Superior sagittal sinus Arachnoid Subarachnoid space Dura Choroid plexus of lateral ventricle
Foramen of Monro
Great cerebral vein Aqueduct of Sylvius Cisterna interpeduncularis Cisterna superior Foramen of Luschka Choroid plexus of fourth ventricle Foramen of Magendie Cisterna cerebellomedullaris
FIGURE 19-34. Cerebrospinal fluid circulation. The lightly stippled area indicates the position of the lateral ventricle.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
Hydrocephalus is classified as either noncommunicating (i.e., obstructive) or communicating. In the noncommunicating form, ventriculomegaly occurs rostral to the site of obstructed cerebrospinal fluid flow. Vulnerable blockage sites include the foramina of Monro, aqueduct of Sylvius, third and fourth ventricles, and the outflow foramina of the fourth ventricle. In communicating hydrocephalus, the cerebrospinal fluid flows from the enlarged ventricular system into the spinal and cranial subarachnoid space. In addition, cerebrospinal fluid accumulates as a result of impaired cerebrospinal fluid absorption by the pacchionian granulations or obstruction within the subarachnoid space over the cerebral hemispheres or around the incisura of the tentorium. Increased intracranial venous pressure from sinus thrombosis or bilateral jugular catheterization also may cause communicating hydrocephalus secondary to decreased cerebrospinal fluid absorption, especially in infants younger than 18 months of age [Rosman and Shands, 1978; Wu and Swaiman, 1982]. Rarely, excessive production of cerebrospinal fluid from a choroid plexus papilloma may cause hydrocephalus.
Pathologic Findings Acute hydrocephalus results from sudden obstruction of cerebrospinal fluid flow or absorption. The precise pathologic features of hydrocephalus vary depending on the age of onset, the rate of ventricular enlargement, and the degree of ventriculomegaly. Typically, elevated cerebrospinal fluid pressure initially enlarges the frontal horns of the lateral ventricles, followed by enlargement of the entire ventricular system above the site of obstruction. Ependymal cells are injured, and periventricular glial cells proliferate, resulting in a layer of reactive gliosis. The pathologic findings may be a result of reduction in blood flow to the white matter causing hypoxic injury, and/or toxicity to the white matter due to buildup of waste products not removed appropriately because of changes in the extracellular matrix [Del Bigio, 2004]. Separation of the ependymal lining of the ventricles enhances permeability, which increases the edema of adjacent white matter (transependymal fluid absorption). MRI may demonstrate periventricular edema. The expanding ventricles flatten the cerebral gyri and obliterate the sulci over the cortical surface. Unless the acute obstruction is relieved, the increasing pressure may hinder cerebral blood flow, cause cerebral herniation, and compromise brainstem function. Nonprogressive hydrocephalus occurs when cerebrospinal fluid absorption compensates for the excess cerebrospinal fluid accumulation, resulting in arrested hydrocephalus. However, ventricular enlargement may progress insidiously without clinical symptoms. In infants, continued ventricular dilation results in separation of cranial sutures and a progressive increase in head circumference. The increasing pressure and ventricular enlargement are associated with necrosis of brain parenchyma. White matter is more vulnerable to destruction than cerebral gray matter in the presence of progressive hydrocephalus [Rubin et al., 1972]. The corpus callosum may also be preferentially affected with evidence of transcallosal swelling, thickening, or demyelination [Spreer et al., 1996; Suh et al., 1997]. These effects do not appear to be associated with cognitive changes nor neuropsychologic evidence of callosal disconnection.
427
Clinical Characteristics Rapid head enlargement, vomiting, lethargy, and irritability are the first signs of acute hydrocephalus in infants. Hydrocephalus may progress insidiously with only excessive head enlargement. Headache, lethargy, and vomiting are typical symptoms in children. Patients with arrested hydrocephalus may be asymptomatic but are at risk to develop symptoms of increased intracranial pressure when the hydrocephalus progresses. In preterm infants, ventricular enlargement may progress with a delay in concomitant excessive head enlargement [Volpe, 2000]. Evaluation of the patient with an enlarged head entails consideration of the many causes of macrocephaly, including hydrocephalus. Evaluation should include a history of trauma or CNS infection, which may obstruct cerebrospinal fluid drainage or impair absorption, leading to hydrocephalus. The family history may demonstrate X-linked hydrocephalus caused by stenosis of the aqueduct of Sylvius or may reveal familial megalencephaly. Besides hydrocephalus, causes of increasing head size include chronic subdural effusions or hematoma, pseudotumor cerebri, neurofibromatosis, metabolic abnormalities of bone or brain, cerebral gigantism (Soto’s syndrome), and benign familial forms (Box 19-7) [DeMyer, 1972]. Rapid head growth, enlarged subarachnoid space, and little or no ventricular enlargement define the entity of external hydrocephalus, which may be part of the clinical spectrum of benign familial macrocephaly [Alvarez et al., 1986]. External hydrocephalus is probably a benign condition that requires no treatment. Considerations in the differential diagnosis of hydrocephalus are listed in Box 19-7. Communicating hydrocephalus is the most common form; obstructive hydrocephalus is less frequent and is usually caused by a congenital defect such as aqueductal stenosis (Fig. 19-35). Subarachnoid or intraventricular hemorrhage, meningitis, intrauterine viral infections, elevated cerebrospinal fluid protein, and other conditions compromising cerebrospinal fluid absorption by the arachnoid granulations are typical causes of communicating hydrocephalus. Principal causes of obstructive hydrocephalus include tumors, congenital malformations, aqueductal stenosis, Arnold-Chiari malformation, DandyWalker syndrome, arteriovenous malformation involving the vein of Galen, intraventricular hemorrhage, and other vascular abnormalities. Hydrocephalus and pseudomeningocele may follow posterior fossa surgery. Hydrocephalus has been reported in association with endocardial fibroelastosis and cataracts (HEC syndrome) and may be due to intrauterine infection or a yet-to-be-determined genetic disorder [Devi et al., 1995]. Autosomal-recessive and X-linked recessive [Castro Gago et al., 1996] and X-linked dominant [Ferlini et al., 1995] forms of hydrocephalus are recognized. X-linked hydrocephalus can be part of the L1 spectrum of disorders, caused by mutations in the L1 cell adhesion molecule (CAM). L1CAM belongs to the immunoglobulin superfamily and is found on the membranes of axons and Schwann cells during development of the nervous system. It plays a role in cell adhesion, axon growth and path-finding, neuronal migration and myelination [Wong et al., 1995]. The L1 disorders initially were described as different entities: HSAS (X-linked hydrocephalus with stenosis of aqueduct of Sylvius,
428
Perinatal Acquired and Congenital Neurologic Disorders / 19
Box 19-7 DIFFERENTIAL DIAGNOSIS OF HYDROCEPHALUS Congenital Malformations Agenesis of the corpus callosum Autosomal-recessive aqueductal stenosis Aqueductal stenosis Arachnoid cyst Cerebellar agenesis Arnold-Chiari malformation Basilar impression Dandy-Walker malformation Encephalocele Peters’ anomaly Porencephaly Infectious Causes Congenital syphilis Cytomegalic inclusion disease Mumps Postmeningitis Postencephalitis Toxoplasmosis Miscellaneous Elevated cerebrospinal fluid protein content with endocardial fibroelastosis, cataracts Neoplasms Brainstem glioma Cerebellar astrocytoma Choroid plexus papilloma Colloid cyst of third ventricle Ependymoma Histiocytosis X Leukemia Lymphoma Medulloblastoma Neuroblastoma Pinealoma Syndromes Achondroplasia Agyria and retinal dysplasia
Apert’s syndrome Cockayne’s syndrome Coffin-Lowry syndrome Crouzon’s syndrome Biemond’s syndrome Fryns’ syndrome Hirschsprung’s disease Gaucher-like disease Glutaricaciduria type I Hurler syndrome Incontinentia pigmenti Larsen’s syndrome Klippel-Trenaunay-Weber syndrome Knobloch’s syndrome Krabbe’s disease Meckel-Gruber syndrome Mucopolysaccharidosis VI Muscle-eye-brain disease Myotubular myopathy Myotonic dystrophy Neurofibromatosis Osteopetrosis Ruvalcaba syndrome Thoracic dysplasia Shprintzen-Goldberg syndrome VACTERL association Walker-Warburg syndrome X-linked aqueductal stenosis (CRASH syndrome) Traumatic Causes Hemorrhage Hypoxic-ischemic encephalopathy Posterior fossa surgery Vascular Causes Arteriovenous malformation Jugular vein catheterization Vein of Galen malformation Venous sinus thrombosis
CRASH, corpus callosum agenesis, retardation, adducted thumbs, spastic paraparesis, hydrocephalus; VACTERL, vertebral anomalies, anal atresia, cardiac defect, tracheoesophageal fistula with esophageal atresia, renal abnormalities, limb abnormalities.
spastic paraparesis type 1, X-linked agenesis of the corpus callosum) and MASA (mental retardation, aphasia, shuffling gait, adducted thumbs) syndrome. Through the 1990s it became clear that these disorders all were the result of a mutation in a single gene, L1CAM [Fransen et al., 1995, 1997; Jouet et al., 1994; Vits et al., 1994]. Thus, some investigators have suggested that these separately named conditions all now be lumped into the acronym CRASH (corpus callosum agenesis, retardation, adducted thumbs, shuffling gait, and hydrocephalus), but others have objected to the negative implications of this name [Schrander-Stumpel, 1998; Schrander-Stumpel and Fryns, 1998]. The clinical phenotype is variable, even within a single family, but some genotypephenotype correlations can be made [Fransen et al., 1998]. Oversecretion of cerebrospinal fluid from choroid plexus papillomas produces hydrocephalus in children, a symp-
tom typically but not universally present before the age of 3 years [Carson et al., 1997; Hamilton, 1996]. The lateral ventricles in children and the fourth ventricle in adults are the most common sites for this tumor. Head circumference measurements provide evidence of an enlarged cranial vault and intracranial volume. Rapid growth evidenced by serial measurements of increasing head circumference is the most important indication of progressive hydrocephalus. The normal rate of head growth during infancy is 2 cm per month during the first 3 months of life, 1 cm per month during the second 3 months, and 0.5 cm per month until 1 year of age. Closure of the anterior fontanel occurs by age 18 months, but closure is delayed in patients with hydrocephalus. Abnormal head shape, particularly occipital prominence, often indicates the likely diagnosis. Severe cranial asym-
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
A
429
B
FIGURE 19-35. Hydrocephalus secondary to aqueductal obstruction in a 29-year-old female patient. A, Acquired aqueductal obstruction or stenosis with distended third ventricle and proximal aqueduct of Sylvius (arrow). Note enlarged frontal horns elevating thinned corpus callosum (arrowheads) on this image from a T1-weighted magnetic resonance imaging (MRI) study. B, Distended temporal and occipital horns are evident, as well as distended proximal aqueduct (arrow), on this axial image from a spin density–weighted MRI study. (Courtesy of Joseph R. Thompson, Department of Radiation Sciences, Loma Linda University School of Medicine, Loma Linda, Calif.)
metry suggests either a porencephalic cyst or a lateral ventricle dilated after stenosis of one foramen of Monro. Biparietal enlargement is often observed with bilateral subdural hematomas. Frontal bossing is common in uncomplicated hydrocephalus. A cranial bruit may indicate an arteriovenous malformation. Papilledema is rarely observed in the infant’s fundi because the cranial sutures spread in response to increased pressure; however, papilledema is common with onset in older children. Retinal hemorrhages associated with acute hydrocephalus may occur but are quite rare. Chronic hydrocephalus is associated with optic nerve atrophy, which is indicated by a pale optic disc and attenuated arterioles. Chorioretinitis suggests an infectious cause, including cytomegalic inclusion disease, lues, and toxoplasmosis. Cranial nerve abnormalities usually are present. The eyes may be rotated to an extreme downward position, producing a “setting sun” sign. This phenomenon may be intermittent and likely indicates a disturbance of the superior colliculus, such as that occurring in Parinaud’s syndrome. Upper eyelid retraction (Collier’s sign), which may occur with lesions of the rostral midbrain and third ventricle, also contributes to the setting sun phenomenon. Abducens nerve paralysis with attendant turning out of the affected eye often is present and constitutes a false localizing sign. Abnormal head movements described as like those of a “bobble-head doll” may be a sign of hydrocephalus,
especially when associated with a third ventricular cyst or aqueductal stenosis [Coker, 1986]. In some patients, the bobble-head doll syndrome may precede the signs and symptoms of increased intracranial pressure. Hyperreflexia, knee and/or ankle clonus, spasticity, and poor head control often are evident on examination. Cutaneous changes over the spine (e.g., bulge, dimple, hemangioma, hypertrichosis) may signal the presence of spina bifida. Skull radiographs may provide evidence of chronic, elevated intracranial pressure, such as excessive convolutional skull markings and separation of cranial sutures, which may occur until the age of 12 years. An enlarged posterior fossa is associated with Dandy-Walker syndrome; a small posterior fossa suggests Arnold-Chiari malformation. Periventricular calcifications accompany cytomegalic inclusion disease; disseminated calcification occurs with toxoplasmosis. Neuroimaging (e.g., CT, MRI, cranial ultrasonography) is essential in delineating the presence and etiology of hydrocephalus (Fig. 19-36). In complex anomalies, the site of obstruction can be documented using CT with contrast material (metrizamide) administered into the cerebrospinal fluid by lumbar or ventricular puncture. In utero diagnosis of fetal hydrocephalus with ultrasonography has potential therapeutic implications (Fig. 19-37). MRI also may be used to diagnose fetal hydrocephalus and may be helpful in determining long-term outcome based on the etiology and progression [Oi et al., 1998].
430
Perinatal Acquired and Congenital Neurologic Disorders / 19
FIGURE 19-36. Hydrocephalus. A, This computed tomography (CT) scan demonstrates enlarged lateral and third ventricles caused by obstruction of the aqueduct of Sylvius by a venous angioma. Note the lucency in the periventricular white matter indicating transependymal edema. B, This CT scan of the posterior fossa reveals a small fourth ventricle, which confirms the diagnosis of aqueductal stenosis in A. Note the vascular malformation. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School, Minneapolis, Minn.)
A
B
FIGURE 19-37. Hydrocephalus detected in utero. This fetal ultrasonogram demonstrates massive ventricular dilation during the third trimester of pregnancy. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School, Minneapolis, Minn.)
Proton MR spectroscopy may be useful in neurosurgical management to assist in differentiating patients with cerebral atrophy (reduced NAA/Cr levels; presence of lactate) from those with hydrocephalus [Bluml et al., 1997]. Functional MRI is being investigated for imaging of cerebrospinal fluid motion in patients with hydrocephalus. It may be useful in patients with newly diagnosed hydrocephalus or in those with suspected shunt malfunction [Feinberg, 1995]. Enlarged ventricles without elevated pressure may occur with cerebral atrophy (hydrocephalus ex vacuo), cerebral malformations (lissencephaly), and nonprogressive arrested hydrocephalus. Radiologic findings that suggest elevated pressure include compressed sulci and transependymal edema surrounding the frontal horns (see Fig. 19-36A).
Management Shunting of cerebrospinal fluid to facilitate absorption usually is required for progressive or symptomatic hydrocephalus [McLaurin et al., 1989; Portnoy et al., 1998; Rekate,
1997]. In the presence of noncommunicating hydrocephalus, removal of the obstruction is preferred. This situation occurs infrequently in comparison with communicating hydrocephalus. If no documented obstruction or operable lesion is present and the hydrocephalus is slight and slowly progressive, a trial period of observation or medical management may be indicated, especially in preterm infants. Hydrocephalus in the preterm infant presents a therapeutic dilemma [Volpe, 2000]. In such infants, hydrocephalus may develop as a result of intraventricular hemorrhage originating from the periventricular germinal matrix. The intraventricular hemorrhage may lead to hydrocephalus by occlusion of the arachnoid granulations by breakdown products of the hemorrhage, although this theory remains unproved. Shunting for these infants frequently is unnecessary and hazardous [Brockmeyer et al., 1989]. The course of the ventricular dilation is variable; patients may demonstrate an arrest or reduction in ventriculomegaly with no treatment. Complications of shunting in this age group include a collapsed cortical mantle, subdural hemorrhage, marked cerebral conformational changes, and extensive intraparenchymal hemorrhage [Bass et al., 1995]. In view of the high morbidity for shunt placement in premature infants, multiple other interventions have been used. Studying the effectiveness of these interventions is challenging because of the variable course of posthemorrhagic ventricular dilation and the multiple other insults that occur in these infants. Acetazolamide and furosemide have been used to reduce cerebrospinal fluid output. A small study found a nonsignificant trend toward reduced shunt rates with use of diuretic therapy [Libenson et al., 1999]. The results of a larger, multicenter, randomized controlled trial, however, did not support the use of diuretics [Kennedy et al., 2001]. Shunt placement or death, the primary outcome measures, were higher in the diuretic treatment group (with furosemide and acetazolamide) than in the standard therapy group, although not significantly so. The principal secondary outcome measure of death in the first year of life or neurodevelopmental disability was significantly higher in infants
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
receiving diuretic therapy. In addition, nephrocalcinosis developed in 25% of infants in the diuretic treatment group. Repeated lumbar punctures to remove cerebrospinal fluid are a common method of attempting to prevent ventricular dilation after intraventricular hemorrhage, and as a therapy to manage symptomatic hydrocephalus. The theory is that removal of cerebrospinal fluid containing blood and protein might allow the normal resorption of cerebrospinal fluid to be restored. There have been two trials of repeated lumbar punctures in preventing the development of hydrocephalus [Anwar, et al., 1985; Mantovani, 1980], and two trials of infants with intraventricular hemorrhage and progressive ventricular dilation that examined the effect of lumbar punctures [Dykes, 1989] or lumbar punctures or ventricular tapping [Ventriculomegaly Trial Group, 1990]. In addition, a Cochrane review performed a meta-analysis on the foregoing four studies [Whitelaw, 2005]. None of the studies demonstrated that cerebrospinal fluid tapping decreased the need for a shunt or decreased the likelihood of death or disability. The Ventriculomegaly Trial found a higher incidence of cerebrospinal fluid infections in those infants who received cerebrospinal fluid taps. The Cochrane review concluded that cerebrospinal fluid tapping for infants at risk of or having developed post-hemorrhagic hydrocephalus could not be recommended. However, the reviewer additionally said that despite the lack of evidence, cerebrospinal fluid tapping should still be considered for symptomatic raised intracranial pressure. Likewise, despite the lack of evidence, some experts continue to recommend the use of cerebrospinal fluid tapping in specific situations. Volpe [2000] advocates its use in infants with persistent slowly progressive ventricular dilation after intraventricular hemorrhage. He stresses that a sufficient quantity of cerebrospinal fluid must be removed, approximately 10 to 15 mL/kg. Some studies have examined the use of intraventricular fibrinolytics to prevent the development of hydrocephalus after intraventricular hemorrhage. So far, it appears that this is ineffective [Whitelaw, 1997]. Another option in patients with rapidly progressive ventriculomegaly who are too small for ventriculoperitoneal shunt placement, is placement of a direct ventricular drainage system. This includes an external ventricular drain, a subgaleal ventricular reservoir, or a subgaleal shunt. These devices can be used until the infant is large enough for permanent shunt placement. In addition, 25% of patients with these devices have arrest of their hydrocephalus, and do not require permanent shunt placement [Garton and Piatt, 2004]. Most hydrocephalic patients require placement of an extracranial shunt. These shunts redirect cerebrospinal fluid flow or circulation into the peritoneal or pleural cavity. Refinements of the Holter, Pudenz, and Hakim valves continue to be developed [McLaurin et al., 1989; Rekate, 1997; Turner, 1995]. Shunts cause cerebrospinal fluid to flow unidirectionally under the aegis of a valve system. Pressures required to overcome valve resistance are preset and can be used in patients with different pressure requirements. Ventriculoperitoneal shunting is the most accepted initial procedure. Use of an antisiphon device developed in the 1970s improved the success rate of shunting by reducing overdrainage of cerebrospinal fluid but was also associated with complications [DaSilva and Drake, 1991]. Many new
431
valve types have been used in the hopes that they would decrease the incidence of shunt malfunction. Orbis-Sigma valves or Delta valves have flow/pressure characteristics that reduce overdrainage [Drake and Kestle, 1996]. However, use of these did not reduce time to first shunt failure [Kestle et al., 2000; Rekate, 1997]. Programmable valves are an alternative system that allow multiple pressure settings; as the child grows, adjustments in flow can be made. Study of the time to shunt failure with these valves, however, did not show any difference from standard valves [Pollack et al., 1999]. Similarly, studies on varying ventricular catheter position and endoscope-assisted catheter placement have found no improvement in outcome [Bierbrauer et al., 1990; Kestle et al., 2003]. Endoscopic third ventriculostomy is an alternative to cerebrospinal fluid shunting in appropriate patients [Barlow and Ching, 1997; Jones et al., 1996]. This creates an outlet in the floor of the third ventricle. Ventriculostomy is particularly useful in patients with congenital aqueductal stenosis that requires cerebrospinal fluid diversion and in selected patients with intracranial cysts or loculated cystic ventricular cerebrospinal fluid collections [Drake, 1993]. The ventriculostomy remains patent in 70% of patients. The ventricles do not decrease in size to the degree they do with a ventriculoperitoneal shunt, so determining the function of a ventriculostomy by neuroimaging can be difficult [Kestle, 2003]. In selected patients, ventriculoatrial shunting can also be used. However, the number of repeat surgeries to adjust the length of the atrial catheter or to revise the distal end favors ventriculoperitoneal shunt placement [Vernet et al., 1995]. The overall failure rate of shunts is 40% in the first year after placement. Common reasons for failure are obstruction, infection, disconnection, overdrainage, and loculated ventricles. Shunt malfunction caused by disconnection, kinking, or obstruction of the tubing results in typical signs and symptoms of increased intracranial pressure. Fever may occur if infection is present. In one series of patients whose shunts were tapped, normal cerebrospinal fluid values correlated with an overall incidence of complications of 39.2%, whereas abnormal cerebrospinal fluid values were correlated with a complication rate of 90.9% [Caldarelli et al., 1996]. Rates of infective complications were 2.7% in the patients with normal cerebrospinal fluid and 77.3% in patients with abnormal cerebrospinal fluid. In patients being evaluated for shunt malfunction, continuous intracranial pressure monitoring may provide additional information to determine the need for shunt revision [Fouyas et al., 1996]. Other complications of ventriculoperitoneal shunts include peritonitis, cerebrospinal fluid ascites, inguinal hernia, intraabdominal cysts, intracranial granulomas, gastrointestinal obstruction, migration of the shunt within the peritoneal cavity, headache, and perforation of abdominal viscera [Borgbjerg et al., 1995; Caldarelli et al., 1996; Ersahin et al., 1996; Key et al., 1995a; Sgouros et al., 1995]. Abdominal pseudocysts manifest with nausea, vomiting, and abdominal distention and pain; abdominal ultrasonography may demonstrate the cysts [Hann et al., 1985-1986]. Thromboembolic phenomena, cardiac dysrhythmias, cardiovascular perforation, endocarditis, catheter embolization, pulmonary thromboembolism, and immune complex shunt nephritis are special complications of ventriculoatrial shunts [Borgbjerg et al.,
432
Perinatal Acquired and Congenital Neurologic Disorders / 19
1995; Lam et al., 1997; McLaurin et al., 1989; Sleigh et al., 1993]. Correction of long-standing hydrocephalus may cause subdural hematomas. Staphylococcus epidermidis and Staphylococcus aureus are the most common causes of shunt-related infection, which usually occurs within 2 months of shunt placement. The infection rate varies but typically is less than 5% [Quigley et al., 1989]. Infection rates of 1% or less have been reported and have been attributed to optimal surgical technique [Choux et al., 1992; Kanev et al., 2003]. Organisms that ordinarily are nonpathogenic may cause infection in the presence of shunt tubing in the ventricles, body cavities, or circulation. Whenever suppurative infection is suspected, appropriate blood and cerebrospinal fluid specimens for culture must be obtained, the organism isolated, and sensitivities determined to facilitate effective antimicrobial therapy. Most shunts can be tapped to obtain cerebrospinal fluid specimens and to assess cerebrospinal fluid dynamics. If infection leads to impairment of the shunt mechanism, removal and replacement usually are required; temporary insertion of an external ventriculostomy may be necessary until the infection is controlled. Prophylactic antibiotics during shunt placement have significantly reduced the incidence of early-onset shunt infections [Venes, 1976]; however, this conclusion is not universally accepted [Shurtleff et al., 1985-1986; Slight et al., 1985].
Fetal Ventriculomegaly and Hydrocephalus The frequent use of prenatal ultrasound examination has led to increasing identification of fetal ventriculomegaly. Neurologists and geneticists often are called on to counsel families regarding this finding. One difficulty is that ventriculomegaly has a myriad of potential causes. In addition, the differentiation of fetal ventriculomegaly due to a developmental or destructive process of the periventricular white matter from fetal hydrocephalus can be challenging and sometimes impossible on prenatal ultrasound studies. Most experts define fetal ventriculomegaly as a lateral ventricular atrial measurement of greater than 10 mm between 15 and 40 weeks of gestation [Cardoza et al., 1988]. Ventriculomegaly is said to be mild when the measurement is between 10 and 15 mm, and severe at greater than 15 mm. Fetal ventriculomegaly is associated with a variety of congenital anomalies, chromosomal abnormalities, and congenital infections; thus, evaluation typically consists of karyotyping, screening for TORCH infections (toxoplasmosis, other infections [e.g., hepatitis B, syphilis, herpes zoster], rubella, cytomegalovirus infection, herpes simplex), and detailed ultrasound examination. Ventriculomegaly with atrial enlargement to greater than 15 mm is associated with a greater chance of abnormal neurologic development [Graham et al., 2001]. Studies of outcome in fetuses with mild ventriculomegaly tend to be small and methodologically variable, so comparing results is difficult. Kelly and associates [2001] reviewed the literature; on combining the data, they found that of almost 500 patients with mild ventriculomegaly, the incidence of chromosomal abnormalities was 9%. If no other malformations were identified, the incidence of chromosomal abnormalities was 4%. The incidence of other abnormalities varied, ranging from 33% to 61%. Studies of neurologic outcome in children with isolated mild fetal ventriculomegaly are small,
use little standardized testing, and have short monitoring periods. In these studies, the incidence of developmental delay varies, ranging from 0% to 36% [Alagrappan et al., 1994; Arora et al., 1998; Bloom et al., 1997; Bromley et al., 1991; Goldstein et al., 1990; Patel et al., 1994; Pilu et al., 1999; Senat et al., 1999; Vergani et al,. 1998]. In view of the conflicting results, it is difficult to know how to counsel families. The role of prenatal MRI in providing additional information is still being clarified. In one study of MRI in 36 fetuses with isolated mild ventriculomegaly the MRI results aided management in five cases: In two cases, ventriculomegaly was ruled out (MRI was normal); in two cases, germinal matrix hemorrhages were found; and in one case, periventricular cystic lesions and abnormal sulcation were detected [Valsky et al., 2004]. Studies of fetal hydrocephalus are likewise fraught with the difficulty of distinguishing hydrocephalus from ventriculomegaly due to other causes. A subset of patients can be more clearly determined to have hydrocephalus—for example, those with aqueductal stenosis, Dandy-Walker syndrome, and Chiari II malformation. Patients with prenatally diagnosed hydrocephalus have a worse outcome than that in patients diagnosed at birth or in the neonatal period [von Koch et al., 2003]. This finding has led to various trials of fetal surgical management, including percutaneous cephalocentesis [Birnholz and Frigoletto, 1981], and ventriculoamniotic shunt placement [Clewell et al., 1982; Frigoletto et al., 1982; Manning et al., 1986]. Overall, patients did not fare well, possibly as a result of poor patient selection. Accordingly, a voluntary moratorium on fetal surgery for hydrocephalus is in place. Interest in fetal shunting may be renwed, however, given that advances in neuroimaging may improve patient selection and surgical technique has improved [von Koch et al., 2003].
Prognosis The neurologic and intellectual disabilities among patients with hydrocephalus depend on many factors, including etiology and degree of hydrocephalus, thickness of the cortical mantle and corpus callosum [Fletcher et al., 1992], requirement for a shunt, and presence of other brain anomalies [Dennis et al., 1981; Laurence, 1969]. Associated conditions such as intraventricular hemorrhage, CNS infection [McLone et al., 1982], and hypoxia may dictate the ultimate prognosis more than the hydrocephalus. The predictive value of cortical mantle thickness remains controversial [Hunt and Holmes, 1976]. A series of 233 patients with congenital hydrocephalus were evaluated for longer than 20 years; 13.7% died. The average number of shunt revisions was 2.7. In this series of 233 patients, of 115 who underwent psychological evaluation, approximately 63% showed normal performance, whereas 30% had mild retardation, and 7% had severe retardation [Lumenta and Skotarczak, 1995]. A more recent study of 155 children followed from 1978 to 1983 found that the children with congenital hydrocephalus were less likely to require special education placement (29%) than were those in whom hydrocephalus was due to meningitis (52%) or intraventricular hemorrhage (60%) [Casey et al., 1997]. Epilepsy also is more prevalent among patients with hydrocephalus, and complications of shunt surgery appear
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
to play a relatively minor role in its development [Piatt and Carlson, 1996]. Intellectual sequelae include significant scatter among Wechsler Intelligence Scale for Children-Revised (WISC-R) subtest scores, often with greater impairment of performance and motor tasks, as well as of nonverbal compared with verbal skills [Brookshire et al., 1995; O’Brien and Harris, 1993]. Normal intellectual function is present in 40% to 65% of patients who receive appropriate treatment [Dennis et al., 1981]. The probability of normal intelligence is enhanced if shunts are placed early and proper function is maintained. A study of 99 children ranging in age from 6 to 13 years with shunted or arrested hydrocephalus demonstrated a close correlation between the area of the corpus callosum and nonverbal cognitive skills and motor abilities [Fletcher et al., 1996]. Behavioral problems also are more common in children with hydrocephalus, irrespective of etiology [Fletcher et al., 1995].
Aqueductal Stenosis Aqueductal stenosis leads to a form of noncommunicating hydrocephalus. Partial or complete obstruction of the aqueduct of Sylvius is associated with congenital structural malformations, hemorrhage, infection, neoplasms, and vascular malformations. Concomitant occlusion of the subarachnoid space may occur. Specific pathologic types of aqueductal stenosis, including congenital narrowing, aqueductal forking, septum formation, and aqueductal gliosis, are difficult to differentiate clinically [Drachman and Richardson, 1961]. The inflammatory process subsequent to neonatal meningitis and intraventricular hemorrhage can cause aqueductal gliosis. Hereditary aqueductal stenosis is transmitted as an X-linked recessive trait [Edwards, 1961]. Rare cases of autosomal recessive inheritance also are reported [Castro Gago et al., 1996]. Aqueductal stenosis as part of the MASA syndrome (X-linked hydrocephalus with stenosis of aqueduct of Sylvius) and the L1CAM spectrum of disorders is described earlier (in the section on clinical characteristics). Aqueductal stenosis may accompany Arnold-Chiari malformations, myelomeningocele, and neurofibromatosis. Aqueductal stenosis also may be secondary to an existing communicating hydrocephalus [Nugent et al., 1979]. In experimental animals, vitamin A excess, mumps encephalitis, and other viral infections cause aqueductal gliosis with associated aqueductal stenosis and hydrocephalus [Volpe, 2000]. In humans, mumps encephalitis has been associated with acquired aqueductal stenosis and hydrocephalus after a latent period of 3 months to 4 years [Spataro et al., 1976]. The pathogenesis in experimental animals and humans may be the propensity for selective infection of ependymal cells by the mumps virus [Volpe, 2000]. Patients with congenital aqueductal stenosis are hydrocephalic at birth. Cranial ultrasonography demonstrates enlarged lateral and third ventricles with a normal or small fourth ventricle. Other neuroimaging techniques may detect tumor, vascular malformation, and associated congenital anomalies (see Figs. 19-35 and 19-36). Remarkably, some patients with congenital and even earlyacquired aqueductal stenosis are asymptomatic until later childhood or early adult life; some remain free of symptoms. When they become apparent, manifestations include findings
433
consistent with chronic increased intracranial pressure, such as an enlarged head, headache, seizures, gait disturbance, decreased visual acuity, dementia, and occasionally cerebrospinal fluid rhinorrhea [Little et al., 1975]. Hypothalamic-pituitary disturbance may occur, including precocious or delayed puberty, impotence, short stature, obesity, hypothyroidism, temperature instability, diabetes insipidus, and amenorrhea. Abnormalities of growth hormone, antidiuretic hormone, thyroid-stimulating hormone, gonadotropins, and gonadotropin-releasing hormone have been documented [Fiedler and Krieger, 1975; Hier and Wiehl, 1977]. Treatment is similar to that for progressive hydrocephalus. After shunting procedures, patients with hypothalamic-pituitary disturbance often improve.
INTRACRANIAL ARACHNOID CYSTS Intracranial arachnoid cysts are benign, nongenetic developmental cysts that contain spinal fluid and occur within the arachnoid membrane [Gosalakkal, 2002]. The mechanism of formation during embryogenesis is uncertain [Hirano and Hirano, 2004; Naidich et al., 1985-1986]. Several mechanisms could account for the enlargement of these cysts including secretion by the cells forming the cyst walls, a unidirectional valve, or liquid movements secondary to pulsations of the veins [Gosalakkal, 2002]. The cysts occur in proximity to arachnoid cisterns, most often in the sylvian fissure (Table 19-18). Common neurologic features are headache, seizures, hydrocephalus, focal enlargement of the skull, and signs and symptoms of elevated intracranial pressure and developmental delay, as well as specific signs or symptoms resulting from neural compression. Some arachnoid cysts remain asymptomatic [Mason et al., 1997]. Progressive enlargement and intracystic or subdural hemorrhage are potential complications. Suprasellar arachnoid cysts may produce neuroendocrine dysfunction, hydrocephalus, and optic nerve compression. Posterior fossa cysts are now more frequently recognized with the use of MRI and CT and frequently require surgical treatment [Domingo and Peter, 1996]. In a series of 61 children with arachnoid cysts, about 53% of cases were diagnosed before age 1 year, 42% were supratentorial, and 46% infratentorial [Pascual-Castroviejo et al., 1991]. Macrocephaly was the presenting symptom in 72%, and associated features included cranial asymmetry in 39%, aqueductal stenosis in 16%, and agenesis of the corpus TABLE 19-18 Distribution of Arachnoid Cysts LOCATION
PERCENT OF CYSTS
Sylvian fissure Cerebellopontine angle Quadrigeminal area Vermian area and sellar-suprasellar area Interhemispheric fissure Cerebral convexity Clival area
49% 11% 10% 9% 5% 4% 3%
Modified from Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial cysts. J Neuropathol Exp Neurol 1981;40:61.
434
Perinatal Acquired and Congenital Neurologic Disorders / 19
A
B
FIGURE 19-38. Arachnoid cyst. A, A cystic mass with signal intensity suggestive of cerebrospinal fluid is seen to deform the right temporal lobe (arrows) on this parasagittal image from a T1-weighted magnetic resonance imaging (MRI) study. B, Note the eroded appearance of the greater sphenoid wing (arrows) from the arachnoid cyst on this axial image from a spin density–weighted MRI study. (Courtesy of Joseph R. Thompson, Department of Radiation Sciences, Loma Linda University School of Medicine, Loma Linda, Calif.).
callosum in 13%. Developmental delay was a common finding. Skull radiographs may suggest the diagnosis; CT or MRI is the definitive diagnostic procedure [Weiner et al., 1987] (Fig. 19-38). Injection of contrast medium into the cyst to document communication with the ventricular system is seldom necessary.
Clinical Presentations Symptoms vary depending on the size of the cyst and its location. Several common locations have been well described in the literature. Sylvian Fissure/Middle Cranial Fossa. Nearly two thirds of pediatric arachnoid cysts are located in the sylvian fissure/middle cranial fossa [Gosalakkal, 2002]. They may increase in volume, opening the fissure and exposing the middle cerebral artery. This exposure may result in compression and underdevelopment of the anterior superior surface of the temporal lobe. The origins of these cysts have been the subject of debate since they were first described. Controversy remains concerning whether they originate directly from the meninges adjacent to the temporal pole or whether partial agenesis of the temporal lobe favors secondary formation of the cyst. Headaches are the most common presenting symptom; proptosis, contralateral motor weakness, and seizures also may occur. In 10% of children, developmental delay may be present. Treatment, as discussed later, depends on clinical symptoms. Recent studies have suggested some cognitive improvement after surgical treatment [Raeder et al., 2005]. Children with bitemporal arachnoid cysts also should be evaluated for the possibility of glutaricaciduria type 1 [Lutcherath et al., 2000]. Bitemporal
arachnoid cysts also have been reported in children with neurofibromatosis [Martinez-Lage et al., 1993] Sellar Region Cysts. Both suprasellar and intrasellar cysts can occur in children. Suprasellar cysts can cause third ventricular obstructive hydrocephalus at the level of the foramen of Monro and may be associated with visual impairment and endocrine dysfunction [Mohn et al., 1999]. Progressive head enlargement, growth retardation, developmental delay, and bitemporal hemianopsia have all been described. [Gosalakkal, 2002]. A bobble-head doll syndrome with involuntary head movements secondary to increased pressure on the third ventricle and dorsomedial thalamic nuclei is responsible [Fioravanti et al., 2004]. Endoscopic surgical approaches are now preferred. Posterior Fossa Arachnoid Cysts. Arachnoid cysts of the posterior fossa are uncommon and must be differentiated from other cystic malformations of the posterior fossa such as the Dandy-Walker malformation [Gosalakkal, 2002]. Macrocrania and raised intracranial pressure are frequently observed. Cerebellar cysts demonstrate nystagmus and other cerebellar signs. Other rare manifestations reported include cervical spinal cord compression, which may improve after posterior fossa cystoperitoneal shunting or endoscopic surgery. In such patients, gait disturbances and headache are commonly seen. Posterior fossa cysts may be very large [Lancon and Ellis, 2004] and also can occur in families [Sinha and Brown, 2004].
Complications Several clinical complications are believed to be associated with arachnoid cysts, although the relation between cyst
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
presence and development of symptoms remains controversial; thus, the decision to operate is difficult and must be made on a patient-by-patient basis. Surgery is indicated when the cyst is causing obstructive hydrocephalus or if neuroimaging demonstrates mass effect with compression of normal brain or brainstem structures. The relation between symptoms such as attention-deficit disorder, aphasia, or migraine-like headaches is uncertain, and correlation between cyst location and specific symptoms or congruent EEG abnormalities is necessary before symptoms can be attributed to the cyst. Epilepsy. Anecdotal studies suggest a relation between seizure reduction after removal of arachnoid cysts [D’Angelo et al., 1999]. The relation between the presence of arachnoid cysts and occurrence of seizures when the intracranial pressure is normal is uncertain, however, and differences in outcomes whether patients are managed medically or surgically are similar [Koch et al., 1995]. In addition, interictal and ictal EEG may not correspond to the site of the arachnoid cyst, raising the question of whether the presence of an EEG abnormality is incidental. Subdural Hematoma and Hygroma. Subdural hematomas and hygromas are infrequently encountered complications of arachnoid cysts of the middle cranial fossa and are particularly rare with cysts in other regions [Donaldson et al., 2000]. Minor head trauma has been suggested to be a precipitating factor. Arachnoid cysts of the middle cranial fossa were found in 2.43% of patients with chronic subdural hematomas or hygromas in one report [Parsch et al., 1997]. Neuropsychiatric Disorders. Attention-deficit–hyperactivity disorder, speech delay, and developmental delay have been found in association with arachnoid cysts, particularly in the temporal lobe, but a causal relation remains uncertain [Millichap, 1997]. Mental impairment and developmental delay have been associated with large arachnoid cysts [Gosalakkal, 2002], and the presence of cysts and developmental delay may be part of a common developmental process. Recent studies have suggested improvements in cognition after surgical treatment [Raeder et al., 2005]. The increased incidence of arachnoid cysts in conditions such as Down syndrome, mucopolysaccharidosis, schizencephaly, and neurofibromatosis suggests a higher incidence in children with underlying abnormalities of the brain [Gosalakkal, 2002]. Aphasia, including that of Landau-Kleffner syndrome, also has been associated with the presence of left sylvian arachnoid cysts. Even in patients in whom CT and MRI failed to reveal mass effect, positron emission tomography (PET) has demonstrated hypometabolism in speech areas. Postoperative improvement in PET studies corresponded to improvement in vocabulary [De Volder et al., 1994].
Management When symptoms warrant, surgical intervention to decompress the cyst, including endoscopic management or shunting procedures, is required [Abbott, 2004; Germano et al., 2003; Godano et al., 2004; Raffel and McComb, 1988]. Arachnoid cysts may occur with or without hydrocephalus. The success rate of fenestration is higher in those patients without hydrocephalus (i.e., 73% required no additional treatment) than in hydrocephalus patients (32%) [Fewel et al., 1996]. About
435
12% of patients with hydrocephalus treated with fenestration alone may require a cystoperitoneal shunt. In general, cyst fenestration should be the primary procedure in patients without hydrocephalus. If hydrocephalus is present, cyst fenestration is still recommended, but a ventriculoperitoneal shunt should be placed if hydrocephalus is marked or after fenestration if the hydrocephalus is progressive [Fewel et al., 1996]. Congenital intraspinal cysts also can occur and require surgical evaluation [Chang, 2004]
CONGENITAL ABNORMALITIES OF THE SKULL Classification The congenital abnormalities of skull ossification listed in Box 19-8 include primary skull or bone disorders and skull abnormalities associated with CNS and systemic disorders. Neurologic features of these disorders may include abnormal head size and shape, hydrocephalus, localized scalp mass or skull deformity, headache, proptosis, pulsating exopthalmos, premature or delayed closure of the cranial sutures and fontanels, large or small fontanels, and progressive compression of neural and vascular structures leading to elevated intracranial pressure and cranial nerve or spinal cord injury [Lachman, 1997]. Many bone diseases that affect the skull cause or are associated with skeletal abnormalities. Other noteworthy features include short stature, syndactyly, polydactyly, and frequent fractures of long bones. Examination of the skull includes determination of the greatest head circumference; palpation to detect ridging or separation of sutures, size of the fontanels, and skull defects or softening; and assessment of skull configuration and symmetry. The head circumference should be recorded sequentially and compared with appropriate growth charts [National Center for Health Statistics, 2005; Nellhaus, 1968]. The skull radiograph often is diagnostic. Skull disorders can be classified into abnormalities of sutures or ossification. The terminology used to describe skull abnormalities [Burrows and Leeds, 1981] includes sclerosis (increased density), hyperostosis (increased thickness), erosion (thinning from pressure resorption), destruction (from infiltration), and deformity (misshapen skull).
Normal Development and Anatomy The skeletal system develops from the mesodermal germ layer during the third week of gestation [Beals and Joganic, 2004]. The mesenchyme or embryonic connective tissue, a mesodermal derivative, forms the fibroblasts, chondroblasts, and osteoblasts. The large surface bones of the skull ossify directly from the mesenchymal tissues (membranous ossification) to form the cranial vault, or membranocranium. The smaller bones of the base of the skull and part of the occipital bone change from mesenchyme to cartilage before ossification (endochondral ossification) and compose the chondrocranium. The cranial vault and chondrocranium encase the brain and are collectively called the neurocranium. The term viscerocranium refers to the remaining bones of the skull and face, which are derived partly from the neural crest cells in the head region. The base of the
436
Perinatal Acquired and Congenital Neurologic Disorders / 19
Box 19-8 CONGENITAL ABNORMALITIES OF OSSIFICATION OF THE SKULL Decreased Ossification Associated major neural defect Anencephaly Cranium bifidum Dandy-Walker syndrome Encephalocele Holoprosencephaly Hydranencephaly Hydrocephalus Porencephaly Bone disorder or variation Biparietal thinning Cleidocranial dysostosis Fibrous dysplasia (monostotic, polyostotic) Hypophosphatasia Large sinus grooves Metopic fontanel Neurofibromatosis (sphenoid bone and lambdoid suture defects) Osteogenesis imperfecta Pacchionian granulations Parietal foramina Persistent emissary foramina Persistent fontanels Pyknodysostosis Sinus pericranii Venous lakes Increased Density and/or Thickness of the Skull (Sclerosis, Hyperostosis) Craniotubular bone-modeling disorders Craniodiaphyseal dysplasia Craniometaphyseal dysplasia Dysosteosclerosis Osteopetrosis Sclerosteosis Van Buchem’s syndrome Aminopterin embryopathy Craniosynostosis Fibrous dysplasia (monostotic, polyostotic) Myotonia congenita (Thomsen’s disease) Myotonic dystrophy Neurofibromatosis Pyknodysostosis Thickened normal cranial vault Tuberous sclerosis Deformity of the Cranial Base Achondroplasia Basilar impression Osteogenesis imperfecta Skeletal dysplasia Modified from Jacobson RI. Neurol Clin 1985; 3:119.
skull, including the foramen magnum, is prone to developmental defects, probably as a result of the more complex intrinsic control of endochondral bone formation. The membranous skull bones are joined by connective tissue at the sagittal, coronal, lambdoidal, metopic, and squamosal sutures (Fig. 19-39). These sutures are easily palpated in neonates and may be overriding as a consequence of normal cranial molding during delivery. The anterior fontanel is the soft spot at the junction of the frontal and parietal bones, which is the intersection of the metopic, coronal, and sagittal sutures. Normal closure of the anterior fontanel occurs between 6 and 20 months with a fibrous suture union. The oblique diameter of the anterior fontanel in neonates ranges from 0.6 to 3.6 cm [Duc and Largo, 1986]. A large, persistent anterior fontanel may constitute a normal variation or a pathologic feature of many disorders (Box 19-9) [Tan, 1976]. The posterior fontanel located at the junction of the lambdoidal and sagittal sutures closes by the age of 3 months. A third fontanel, actually a defect in ossification, may occur 2 cm anterior to the posterior fontanel in 6.3% of normal preterm and term infants and is common in infants with Down syndrome and congenital rubella [Chemke and Robinson, 1969]. Mature suture closure occurs by age 12 years, but completion of bony fusion continues at least through the third decade of life. Elevated intracranial pressure may separate the sutures, especially the sagittal suture, until ages 10 to 12 years. The timing of closure of the sutures and fontanels are listed in Table 19-19. Many developmental skull variations exist. Wormian bones are small, multiple bones that occur in sutures, particularly in the lambdoidal suture. They may be a normal variation but often occur in hydrocephalus and other skull disorders (see Box 19-9). Parietal foramina are symmetric, full-thickness congenital defects in the parietal bones close to the midline. They often are familial and may have no pathologic significance.
Genetic Mechanisms of Craniofacial Development A number of gene families have been shown to play important roles in craniofacial development [Aleck, 2004; Cobourne, 2000]. These genes act as regulators of gene transcription and are intimately involved with the control of complex interactions between multiple downstream genes. In vertebrates, Hox genes pattern the hindbrain and branchial regions of the developing head up to and including structures derived from the second branchial arch. The first branchial arch and more rostral regions of the head are patterned by groups of homeobox genes more divergent than the original Hox clusters. These gene families include several classes of homeobox genes: paired class (Oxt, Goosecoid, and Ant/Hesx1), antennapedia class (Emx and Hex/ Prh), Lim class (Lim1), and winged class (Forkhead and Hnf3) [Cohen, 2002]. Later during development, these genes function in brain patterning and neurogenesis. More recent studies as outlined by Trainor and colleagues [2003] suggest that neural crest cells can respond and adapt to the environment in which they migrate and, furthermore, that the cranial mesoderm plays an important role in patterning the identity of the migrating neural crest cells. These results support a new model called the neural crest plasticity and
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
A
B
independent gene regulation model as a mechanism for describing neural crest and craniofacial development.
The Neural Crest The neural crest plays an important role in facial and cranial development [Chambers and McGonnell, 2002; Cobourne, 2000]. The facial mesenchyme is derived principally from the neural crest and not the mesoderm of the embryonic third germ layer. Neural crest cells migrate extensively throughout the embryo, and in the developing head, the cephalic neural crest migrates from the posterior midbrain and hindbrain regions into the branchial arch system. The ectomesenchymal neural crest cells then interact with epithelial and mesodermal cell populations present within the arches, leading to the formation of craniofacial bones, cartilages, and connective tissues. It is the rhombencephalic-derived neural crest that will give rise to the majority of the branchial arch mesenchyme. Development of the mid- and lower regions of the craniofacial complex is associated with these branchial regions. Neural crest cells that migrate and form the bulk of the facial mesenchyme arise from the same axial level of neural tube as the rhombomeres whose neurons will ultimately innervate that mesenchyme. Neural crest cells destined for the first branchial arch migrate from rhombomeres 1 and 2, whereas those for the second and third arches migrate from rhombomeres 4 and 6. The even-numbered rhombomeres (2, 4, and 6) contain the exit points for cranial nerves V, VII, and IX, which will innervate branchial arches 1, 2, and 3 [Cobourne, 2000]. Members of the zinc-finger transcription factor family (e.g., Slug, Snail), as well as bone morphogenetic proteins, fibroblast growth factors (FGFs) and members of the Wnt signaling family are recognized for their roles in neural crest induction, differentiation, and development [Trainor et al., 2003].
Gene Regulatory Mechanisms A role for Hox genes in patterning regions of the developing head and neck has been suggested. Expression domains of
437
FIGURE 19-39. A, Posteroanterior radiographic view of a 9-month-old infant’s skull. B, Lateral skull film from the same infant. 1, coronal suture; 2, lambdoidal suture; 3, sagittal suture; 4, mendosal suture; 5, squamosal suture; 6, metopic suture, partially fused; 7, occipital mastoid suture. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School, Minneapolis, Minn.)
certain of the Hox genes cluster, however, do not extend into the first branchial arch or more rostral head regions, indicating that Hox genes are not involved in specification of neural crest from these more anterior levels [Cobourne, 2000]. The ems (empty spiracle) and otd (orthodenticle) gene families also are expressed in the anterior regions of the developing head in Drosophila. In mice, it has been found that Otx-2 is essential for formation of the rostral head, and craniofacial malformations may include loss of the lower jaw structures and the eye. As described by Cobourne [2000], these defects are consistent with human otocephalic mutations. Other homeobox-containing genes are expressed in the maxillary and mandibular arches and developing facial primordia. These genes include Msx-1, Msx-2, Dlx1-6, and Barx-1. Msx-1 and Msx-2 are strongly expressed in the neural crest–derived mesenchyme of the developing facial prominences and participate in skull and face development [Ferguson, 2000]. Members of the Dlx gene family also are required for the development of neural crest–derived skeletal elements of the first and second branchial arches. Goosecoid is another homeobox-containing transcription factor that in the wild type of mice has been detected at later stages of development in the osteogenic mesenchyme of the developing mandible, tongue, and middle ear. Goosecoid mutants have been associated with development of a hypoplastic mandible, as well as other osseous defects including involvement of the maxillary, palatine, and pterygoid bones. The endothelin-1 gene (ET1) is another gene that has been associated with facial anomalies in mice. It normally encodes a vasoactive peptide expressed in vascular endothelial cells that plays a role in the regulation of blood pressure, but targeted disruption of ET1 in mice is associated with marked reduction in tongue size, micrognathia, and cleft palate [Kurihara et al., 1994] The Sonic hedgehog gene (SHH) is the vertebrate homolog of the Drosophila hedgehog segment polarity gene. In the vertebrate embryo, SHH encodes a signaling peptide that is involved in mediating long- and short-range patterning [Cobourne, 2000]. Mutations of SHH in the human [Belloni
438
Perinatal Acquired and Congenital Neurologic Disorders / 19
Box 19-9 DIFFERENTIAL DIAGNOSIS OF SKULL ABNORMALITIES IN INFANTS Conditions Associated with Skull Softening Cleidocranial dysostosis Craniotabes Lacunar skull Osteogenesis imperfecta Multiple wormian bones Rickets Conditions Associated with Delayed Closure of the Anterior Fontanel Achondroplasia Aminopterin embryopathy Cerebrohepatorenal syndrome (Zellweger’s syndrome) Cleidocranial dysostosis Congenital rubella Down syndrome Hallermann-Streiff syndrome Hypophosphatasia Hypothyroidism Increased intracranial pressure—hydrocephalus, pseudotumor cerebri Malnutrition Osteogenesis imperfecta Pyknodysostosis Rickets Trisomies 13 and 18 Conditions Associated with Wormian Bones No pathologic significance Cleidocranial dysostosis Hydrocephalus (chronic) Hypophosphatasia Hypothyroidism Kinky hair disease Osteogenesis imperfecta Pyknodysosteogenesis Rickets (healing phase) Data from Burrows EH, Leeds NE. Neuroradiology, vol 1. New York: Chuchill Livingstone, 1981; and Lemire RJ, Loeser JD, Leech RW, et al. Normal and abnormal development of the human nervous system. Hagerstown, MD: Harper & Row, 1975.
TABLE 19-19 Timing of Closure of Sutures and Fontanels SUTURE/FONTANEL
CLOSURE
SKULL SHAPE
Metopic suture Coronal suture
9 months to 2 years 40 years
Sagittal suture
40 years
Lambdoid suture
40 years
Trigonocephaly Unilateral harlequin deformity, plagiocephaly Scaphocephaly/ dolichocephaly Unilateral: plagiocephaly Bilateral: brachycephaly
Anterior fontanel Posterior fontanel Anterior-lateral fontanel (pterion) Anterior fontanel (asterion)
15–18 months 3–6 months 3 months 2 years
From Aviv RI, Rodger E, Hall CM. Craniosynostosis. Clin Radiol 2002;57:93–102.
appears to play an important role in development of the mesoderm. FGFRs belong to a subgroup of the receptor tyrosine kinase family of signal transduction molecules and serve as the major binding proteins for FGFs. FGFR1, FGFR2, and FGFR3 are expressed widely during embryogenesis. FGFR1 and FGFR2 expression is noted in cartilage and bone precursors, whereas FGFR3 is found in highest concentration in the developing CNS but also in bone precursors involved with endochondral bone formation [FloresSarnat, 2002]. A detailed discussion of this topic is beyond the scope of this chapter, and the reader is referred to several recent monographs [Francis-West et al., 2003; Sperber, 2001] and reviews [Cobourne, 2000; Cohen, 2002; Trainor et al., 2003; Wilkie and Morriss-Kay, 2001] of this rapidly expanding field. An excellent and very comprehensive publication, Inborn Errors of Development: The Molecular Basis of Morphogenesis, is highly recommended [Epstein et al., 2004]. A review of selected genetic malformations, their chromosomal locations, and the associated mutationbearing genes is provided in Table 19-20.
Deformational Plagiocephaly et al., 1996; Roessler et al., 1996] lead to significant craniofacial abnormalities such as holoprosencephaly and cyclopia. Later in development, Shh is expressed in the ectoderm of the frontonasal and maxillary processes and has been found to be essential for their normal development. Transient loss of Shh signaling in chick embryos in regions of the developing face can result in defects analogous to hypotelorism and cleft lip/palate, whereas excess Shh leads to mediolateral widening of the frontonasal process resulting in hypertelorism [Cobourne, 2000]. Identification of mutations in Twist and fibroblast growth factor receptors (FGFRs) in craniosynostosis demonstrates their importance as critical signaling molecules during normal cranial development [Flores-Sarnat, 2002]. Twist is a class II basic helix-loop-helix transcription factor originally identified in Drosophila that also is present in humans and
Deformational or positional plagiocephalies (from the Greek, meaning “oblique head”) are common in children and frequently are confused with craniosynostosis [Persing et al., 2003]. Deformational plagiocephalies have been referred to by many names, such as benign positional molding, posterior plagiocephaly, occipital plagiocephaly, frontal plagiocephaly, and plagiocephaly without synostosis [Huang et al., 1998]. The incidence of plagiocephaly has been estimated to be as low as 1 in 300 live births to as high as 48% of typical healthy infants younger than 1 year, depending on the sensitivity of the criteria used to make the diagnosis [Persing et al., 2003]. By contrast, the incidence of isolated lambdoid craniosynostosis is quite rare, estimated to be approximately 3 in 100,000 births (0.003%). Two forms of plagiocephaly are recognized: deformational frontal plagiocephaly if the front of the cranial vault
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
439
TABLE 19-20 Selected Genetic Disorders with Craniofacial Anomalies DISORDER Achondrogenesis type 1B Achondrogenesis type 2 Achondroplasia Acromesomelic dysplasia Alagille’s syndrome Albright’s hereditary osteodystrophy Apert’s syndrome Atelosteogenesis type II Bannayan-Riley-Ruvalcaba/Cowden syndrome Beare-Stevenson cutis gyrata syndrome Bloom’s syndrome Boston-type craniosynostosis Branchio-otorenal syndrome Camptomelic dysplasia Chondrodysplasia punctata, X-linked dominant type Chondrodysplasia punctata, X-linked recessive type Chondrodysplasia, rhizomelic type Cleft lip/palate, ectodermal dysplasia (AR) Cleidocranial dysplasia Conradi-Hunermann type Crouzon’s disease Crouzonodermoskeletal syndrome Diastrophic dysplasia Ectrodactyly-ectodermal dysplasia–clefting (EEC) syndrome Ellis–van Creveld syndrome Familial adenomatous polyposis/Gardner’s syndrome FG syndrome Fibrous dysplasia Fragile X syndrome Greig’s cephalopolysyndactyly Hay-Wells syndrome Holoprosencephaly (all types)
Hypochondroplasia Hypodontia Hypodontia/clefting Hypohidrotic ectodermal dysplasia Jackson-Weiss syndrome Jansen’s metaphyseal chondrodysplasia Langer-Giedion syndrome Mandibuloacral dysplasia Marfan’s syndrome McCune-Albright syndrome Mucolipidosis II Mucolipidosis III Mucopolysaccharidosis IH Mucopolysaccharidosis II Mucopolysaccharidosis IIIA Mucopolysaccharidosis IIID Mucopolysaccharidosis IS Mucopolysaccharidosis IVA Mucopolysaccharidosis IVB Mucopolysaccharidosis VI Mucopolysaccharidosis VII Muenke’s syndrome Multiple endocrine neoplasia type 2B Neurofibromatosis type 1 Neurofibromatosis type 2 Nevoid basal cell carcinoma syndrome
CHROMOSOMAL LOCATION(S)
MUTATION-BEARING GENE(S)
5q31-q34 12q13.1-q13.3 4p16.3 20q11.2 20p12 20q13 10q25.3-q26 5q31-q34 10q23 10q25.3-q26 15q26.1 5q34-q35 8q13.3 17q24.3 Xp11.22-p11.23 Xp22.3 6q22-q24 11q23 6p21
DTDST COL2A1 FGFR3 CDMP1 JAG1 GNAS1 FGFR2 DTDST PTEN FGFR2 BLM MSX2 EYA1 SOX9 3β-Hydroxysterol ARSE PEX PVRL1 RUNX2 D7 isomerase FGFR2 FGFR3 DTDST TP63 EVC FAP-GS FGS1 GNAS1 FMR1 GLI3 TP63 SIX3 GLI2 CRIPTO SHH FAST1 PTCH ZIC2 TGIF FGFR3 PAX9 MSX1 EDA2 EDA3 EDA1 FGFR2 [PTH/PTHrP]R TRPS1 and EXT1 LMNA FBN1 GNAS1 GNPTA GNPTA IDA IDS HSS GNS IDA GALNS GLBI ARSB GUSB FGFR3 RET NF1 NF2 PTCH
10q25.3-q26 4p16.3 5q31-q34 3q27 4p16 5q21-q22 Xq12-q21.31 20q13 Xq27.3 7p13 3q27 2p21 2q14 3p21-p23 7q36 8q24.3 9q22.3 13q32 18p11.3 4p16.3 14q12-q13 4p16 2q11-q13 2q11-q13 Xq12.2-q13.1 10q25.3-q26 3p21.1-p22 8q24.11-q24.13 1q21 15q21 20q13 4q21-q23 4q21-q23 4p16.3 Xq27.3-q28 17q25.3 12q14 4p16.3 16q24.3 3p21.33 5q13.3 7q21.11 4p16.3 10q11.2 17q11.2 22q11.21-q13.1 9q22.3
continued
440
Perinatal Acquired and Congenital Neurologic Disorders / 19
TABLE 19-20, cont’d Selected Genetic Disorders with Craniofacial Anomalies DISORDER Opitz’s BBB/G syndrome Osteogenesis imperfecta Papillon-Lefevre syndrome Parietal foramina Peutz-Jeghers syndrome Pfeiffer’s syndrome Popliteal pterygium syndrome Pfeiffer’s syndrome Pyknodysostosis Rieger’s syndrome Rubinstein-Taybi syndrome SADDAN syndrome Saethre-Chotzen syndrome Septo-optic “dysplasia” Simpson-Golabi-Behmel syndrome Smith-Lemli-Opitz syndrome Soto’s syndrome Spondyloepiphyseal dysplasia congenita Stickler’s syndrome Thanatophoric dysplasia type 1 Thanatophoric dysplasia type 2 Townes-Brocks syndrome Treacher Collins syndrome Trichodento-osseous syndrome Trichorhinophalangeal syndrome Tuberous sclerosis Van der Woude’s syndrome Waardenburg’s syndrome type 1 Waardenburg’s syndrome type 2 Wiedemann-Beckwith syndrome
CHROMOSOMAL LOCATION(S)
MUTATION-BEARING GENE(S)
Xp22 7q22.1 17q21.31-q22.05 11q14 5q34-q35 11p11.2 19p13.3 8p11.2-p12 1q32-q41 10q25.3-q26 1q21 4q25-q27 16p13.3 4p16.3 7p21 3p21.1 Xq26 11q12-q13 5q35 12q13.1-q13.3 6p21 12q13.1-q13.3 4p16.3 4p16.3 16q12.1 5q33-q33.1 17q21 8q24.12 9q33-q34 16p13.3 1q32-q41 2q37 3p12-p14 11p15.5
MID1 COL1A2 COL1A1 CTSC MSX2 ALX4 STK11 FGFR1 IRF6 FGFR2 CTSK RIEG CBP FGFR3 TWIST HESX1 GPC3 DHCR7 NSD1 COL2A1 COL11A1 COL2A1 FGFR3 FGFR3 SALL1 TCOF1 DLX3 TRPS1 TSC1 TSC2 IRF6 PAX3 MITF IGF2, p57KIP2
SADDAN, severe achondroplasia with developmental delay and acanthosis nigricans. From Cohen MM Jr. Malformations of the craniofacial region: Evolutionary, embryonic, genetic, and clinical perspectives. Am J Med Genet 2002;115:245-268.
is involved [Hansen and Mulliken, 1994] and deformational posterior plagiocephaly when the posterior aspects of the skull are affected [Pollack et al., 1997]. In children with deformational frontal plagiocephaly, one side of the forehead is flat, sometimes the cheek and lower jaw are small, an ear is positioned farther back, and the eyelid opening may look smaller. All of these characteristics occur on the same side as the flattened forehead. About two thirds of infants with deformational frontal plagiocephaly have a head tilt toward the shoulder on the affected side as a result of torticollis. In children with deformational posterior plagiocephaly, the back of the head is flat on one side, the ear on that side is further forward than normal, and often, minor flattening of the forehead is seen on the opposite side. Deformational posterior plagiocephaly also can be bilateral, occurring on both sides. Table 19-21 summarizes features of deformational frontal plagiocephaly and deformational posterior plagiocephaly and compares clinical features of these entities with those in children with isolated coronal or lambdoid synostosis. Plagiocephaly typically is present at or shortly after birth and usually is due to in utero or intrapartum molding associated with uterine constraint, multiple births, birth injury from forceps or vacuum-assisted delivery, and prematurity [Persing et al., 2003]. In a majority of infants, plagiocephaly
resolves spontaneously during the first few months of life. In some infants who continue to rest their head asymmetrically on the flattened side of the occiput the deformity may persist. Before the 1990s, a majority of plagiocephalies involved the frontal regions, but this predilection has shifted, with deformational posterior plagiocephaly more common at present. Presumably this evolved because of the recommendations of the American Academy of Pediatrics and others that infants be placed on their backs for sleep [American Academy of Pediatrics, 1992], because prone and side sleeping during early infancy had been linked with sudden infant death syndrome.
Diagnosis and Treatment Confirmation of deformational frontal plagiocephaly or deformational posterior plagiocephaly requires skull radiographs or CT scanning that demonstrates the absence of synostosis [Glat et al., 1996]. Management of deformational plagiocephaly involves counseling of parents, mechanical adjustments, and exercises as reviewed in a clinical report from the American Academy of Pediatrics [Ellenbogen et al., 2000; Persing et al., 2003]. Parental assistance in
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
TABLE 19-21 Distinctions between Common Synostoses and Deformational Plagiocephalies Unicoronal Synostosis versus Frontal Deformational Plagiocephaly ANATOMIC FEATURE
CORONAL SYNOSTOSIS
FRONTAL DEFORMATIONAL PLAGIOCEPHALY
Ipsilateral superior orbital rim Nasal root Ipsilateral cheek Chin deviation Ipsilateral palpebral fissure Anterior fontanel deviation
Up and high
Down
Ipsilateral Forward Contralateral Wide, low
Midline Backward Ipsilateral Narrow, high
Contralateral
None
Lambdoid Synostosis versus Occipital Deformational Plagiocephaly ANATOMIC FEATURE
LAMBDOID SYNOSTOSIS
OCCIPITAL DEFORMATIONAL PLAGIOCEPHALY
Posterior bossing
Contralateral occipitoparietal Contralateral Posterior and low Tilted
Contralateral occipital Ipsilateral Anterior No tilt
Frontal bossing Ipsilateral ear Skull base
From Aviv RI, Rodger E, Hall CM. Craniosynostosis. Clin Radiol 2002;57:93–102.
performing exercises is required, to reduce the likelihood of development of a severe deformity. Parents should be instructed when their infants are 2 to 4 weeks of age to place the child in the supine position for sleeping, alternating positions (i.e., left and right occiputs); when awake, the infant should be placed in the prone position. Infants should spend minimal time in car seats (when not a passenger in a vehicle) or other seating that maintains the supine position. Once deformational plagiocephaly has developed, these same preventive strategies may be used to reduce progression. It also is important to monitor head shape closely until the physician is certain that improvement will continue, usually when the infant is old enough to sit, crawl, or spend less time lying on the back. In children with neurologic disorders such as cerebral palsy, microcephaly, or global delay, this time frame is likely to be much longer than in children who are unaffected. Because torticollis can worsen plagiocephaly, neck rotation exercises should be implemented. As outlined in the American Academy of Pediatrics report, exercises to stretch the sternocleidomastoid muscle should be done with each diaper change [Persing et al., 2003]. One hand is placed on the child’s upper chest, and the other hand rotates the child’s head gently so that the chin touches the shoulder for approximately 10 seconds. The head is then rotated toward the opposite side for the same duration. A second exercise that stretches the trapezius muscle should then be done. The head is tilted so that the infant’s ear touches his or her shoulder for approximately 10 seconds and should be repeated contralaterally. Progression or lack of improvement warrants referral to a pediatric neurosurgeon, a general neurosurgeon with expertise in pediatrics, or a craniofacial surgeon or craniofacial team to establish the diagnosis and direct subsequent management, which may include molding helmets or surgery
441
[Kaufman et al., 2004]. Referral to a physical therapist also should be considered if torticollis does not improve with neck-stretching exercises within 2 to 3 months. Skullmolding helmets, usually used in infants 4 to 12 months of age, may help correct atypical skull shapes, although repositioning of infants may be equally effective. Surgery may be necessary in approximately 10% of children with deformational plagiocephaly when the deformities are severe and resistant to nonsurgical measures [David and Menard, 2000; Littlefield, 2004; O’Broin et al., 1999; Rekate, 1998].
Craniosynostosis Although clinical descriptions of craniosynostosis date back to Hippocrates and Galen, the first modern scientific investigator to describe the anatomic structure of calvarial sutures and the results of their premature closure was Sommering in 1800 [Jimenez et al., 2002]. It was Virchow, however, who first coined the term craniostenosis, in 1851, and who proposed that bone growth occurs perpendicular to an open suture and that premature fusion of sutures results in calvarial deformities secondary to restrictive bone growth perpendicular to the closed suture and compensatory bone growth in directions parallel to the fused suture. Subsequently, the American surgeon Lane performed the first surgical procedure for craniosynostosis in a 9-monthold infant with microcephaly, and the French surgeon Lannelogue performed bilateral strip craniectomies for sagittal synostosis in 1890 [Jimenez et al., 2002]. In 1894 Jacobi reported his unsuccessful treatment of 33 microcephalic patients with presumed craniosynostosis, and this had the effect of dampening interest in the surgical treatment of craniosynostosis for the next 30 years. Surgical treatment for craniosynostosis to prevent blindness and other associated complications was reintroduced by Faber and Town in 1927. Their successful outcomes, combined with low morbidity and mortality, fostered wide acceptance of the concept of surgical correction for craniosynostosis; since then, many surgical techniques have been introduced.
Pathogenesis Primary craniosynostosis results from premature fusion of single or multiple cranial sutures that deforms the skull or face. The process of premature fusion begins in utero and can be detected in neonates. The primary pathologic bony defect restricts normal growth across the affected sutures and consequently may limit adequate brain growth, resulting in neurologic deficits. In other infants, postnatal onset of craniosynostosis may develop [Connolly et al., 2004]. Primary craniosynostosis occurs in up to 1 in 2000 to 1 in 2500 births. The shape and size of the skull depend on adequate brain growth without restriction. Inadequate brain growth, such as that occurring in microcephaly or after surgical shunting of severe hydrocephalus, may also result in premature closure of cranial sutures—secondary craniosynostosis. Secondary craniosynostosis does not further compromise the already impaired brain growth. The etiology of primary craniosynostosis may be a defect in the mesenchymal layer of the ossification centers within the skull. Pathologic examination reveals obliterated sutures
442
Perinatal Acquired and Congenital Neurologic Disorders / 19
that can be distinguished from normal suture closure [Albright and Byrd, 1981]. Evidence for a systemic disorder of mesenchymal tissue and ossification includes the craniosynostosis syndromes associated with facial and skeletal deformities [Cohen, 1988]. Mechanical factors also may cause craniosynostosis (e.g., experimental bony defects, such as a ridge placed across a suture, intrauterine compression, inadequate brain development) [Jones, 1997]. Another often-mentioned but controversial explanation ascribes craniosynostosis to a deformity of the cranial base that alters the tensile forces on the sutural sites of attachment of the dura mater [Albright and Byrd, 1981]. Failure of the bony microspicules that
normally bridge sutures to fracture, with the resultant sutural bony buildup, also has been suggested [Burke et al., 1995]. In infants and children, craniosynostosis may result from chromosomal disorders, hematologic disorders with bone marrow hyperplasia, endogenous or exogenous hyperthyroidism, and abnormal calcium and phosphorus metabolism, including that of rickets, hypercalcemia, and hypophosphatasia. Most patients have isolated craniosynostosis of unknown etiology, however. Over the past decade, the role of the dura in maintaining sutural patency has been extensively studied [Panchal and Uttchin, 2003]. The dura appears to initially play an induc-
TABLE 19-22 Major Craniosynostosis Syndromes SYNDROME
GENETICS
FGFR-Related Craniosynostosis Syndromes Apert’s syndrome (ACS1) AD 10q26 FGFR2 Crouzon’s disease (CFD1) Jackson-Weiss syndrome Pfeiffer’s syndrome (ACS5)
AD 10q26 FGFR2 AD FGFR2 AD 10q23-q2 FGFR2 8p12-p11.2 FGFR1
Muenke’s syndrome
4p16.3 FGFR3
Beare-Stevenson syndrome
10q26 FGFR2
TWIST-Related Craniosynostosis Syndromes Saethre-Chotzen syndrome 7p21 (ACS3) AD TWIST gene Baller-Gerold syndrome AR MSX-Related Craniosynostosis Syndromes Boston-type craniosynostosis AD 5q34-35 MSX2 gene
Fibrillin-Related Craniosynostosis Syndromes Shprintzen-Goldberg syndrome AD 15q21.1 Other Craniosynostosis Syndromes Antley-Bixler syndrome
7q11.2
Carpenter’s syndrome (ACS2)
AR
Hunter-McAlpine syndrome
AD 17q23-24
CLINICAL FEATURES
Multiple synostoses, with coronal most common, severe fusion syndactyly of hands and feet, hypertelorism, proptosis; downslanting palpebral fissures; mental retardation common Two subgroups: 1. Classic: above with mid-digital hand mass with single nail common to digits 2 through 4 2. Atypical: above but without mid-digital hand mass Coronal craniosynostosis, shallow orbits, proptosis, parrot-beaked nose, short upper lip, hypoplastic maxilla
Coronal and basal skull suture involvement, broad big toes, tarsal fusion, syndactyly, craniofacial abnormalities Coronal synostosis; broad, short thumbs and toes, polydactyly, syndactyly Three subgroups [Cohen, 1993]: 1. Classic type with broad, short thumbs and toes, polydactyly, normal neurologic outcome (AD) 2. Cloverleaf skull with Pfeiffer’s hands (sporadic) 3. Similar to 2 but without cloverleaf skull (AD) Coronal craniosynostosis, on radiograph abnormalities of hands and feet, including thimble-like middle phalanges, coned epiphyses, and carpal and tarsal fusions; hearing loss, developmental delay Craniosynostosis, ear defects, cutis gyrata, acanthosis nigricans, anogenital anomalies, skin tags, and prominent umbilical stump Asymmetric coronal synostosis with facial asymmetry, plagiocephaly, low-set frontal hairline, ptosis, brachydactyly, syndactyly, seizures, hearing loss, cervical spine fusion Multiple synostoses, radial aplasia, short stature, imperforate anus, rectovaginal fistula, mental retardation Four phenotypes described: 1. Fronto-orbital recession 2. Frontal bossing 3. Turribrachycephaly due to coronal craniosynostosis 4. Cloverleaf skull Synostosis of multiple sutures, mandibular and maxillary hypoplasia, multiple abdominal hernias, exophthalmos, mental retardation Craniosynostosis, severe midface hypoplasia, proptosis, choanal atresia/stenosis, frontal bossing, dysplastic ears, depressed nasal bridge, radiohumeral synostosis, long bone fractures and femoral bowing, and urogenital abnormalities Acrocephaly or turricephaly with brachydactyly, syndactyly, preaxial polydactyly, soft tissue syndactyly, obesity, hypogenitalism; mental retardation may occur Brachyphalangia, mental retardation, almond-shaped palpebral fissures, downturned or small mouth, short stature
ACS, acrocephalosyndactyly; AD, autosomal dominant; AR, autosomal recessive; CFD1, craniofacial dysostosis type 1. Data from Online Mendelian Inheritance in Man (OMIM), 2005.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
tive role; later, it assumes a permissive role in maintaining sutural patency through various signaling factors. Previous studies have documented an increased level of TGF-β and messenger RNA levels locally, indicating an interaction between the dura and overlying sutures at the time of closure [Most et al., 1998]. Other studies have demonstrated that dura mater transplanted from beneath normally patent sutures to sites of sutural fusion in a naturally occurring craniosynostotic rabbit model successfully kept these sites from re-obliterating [Mooney et al., 2001]. The interaction between the brain and patency of the overlying sutures has been amply proved by clinical evidence showing the premature closure of sutures in the presence of microcephaly and continuing patency in the presence of hydrocephalus [Panchal and Uttchin, 2003]. Secondary craniosynostosis also can develop after placement of a shunt in a child with hydrocephalus (shunt-induced craniosynostosis) because of a drop in intracranial pressure and diminution of neural thrust. The neural thrust and patency of the overlying sutures are closely integrated through the dura. The dura also serves as an intermediary source of signaling, which is mediated by transforming growth factor, FGFR, Twist, and MSX2. Many theories have been advanced to explain craniosynostosis; the vast array of clinical syndromes has defied a unifying hypothesis [Becker and Hinton, 1995; Cohen, 1988, 2000; Epstein et al., 2004; Flores-Sarnat, 2002]. The etiology of craniosynostosis must include contributions from developmental, mechanical, metabolic, and genetic factors that influence skull growth. More recently, several of the syndromic forms of craniosynostosis have been associated with identified
443
deletions of genes (Table 19-22 and Fig. 19-40) that code for the FGFRs [De Moerlooze et al., 1997; Epstein et al., 2004; Muller et al., 1997; Mulliken and Warman, 1996]. Crouzon’s disease is associated with a deletion of the FGFR2 gene on chromosome 10 [Bresnick et al., 1995]. Specifically, lower levels of FGFR2 staining could be demonstrated from stenosed sutures removed at surgery. Children with nonsyndromic craniosynostoses did not demonstrate this abnormality. Members of the FGF family and their receptors play essential roles in regulating cellular proliferation, differentiation, and tissue patterning during vertebrate embryogenesis [Yamaguchi and Rossant, 1995]. A report including 61 persons from 20 unrelated families found coronal synostosis resulting from an amino acid substitution that results from a single point mutation in the FGFR3 gene on 4p [Muenke et al., 1997]. Other syndromic forms of craniosynostosis, including Pfeiffer’s, JacksonWeiss, and Apert’s syndromes, or autosomal-dominant nonsyndromic forms also are associated with mutations involving the FGFR2 gene [Muller et al., 1997; Steinberger et al., 1996]. In some cases of Crouzon’s disease and Pfeiffer’s syndrome, mutations of the FGFR1 and FGFR3 gene have been observed. Mutations of the transcriptional regulator gene MSX2 and TWIST genes have also been reported in patients with craniosynostosis [Wilkie, 1995]. In many of the disorders associated with these gene defects, highly variable phenotypes exist even within one family. Thus, the clinically distinct craniosynostotic syndromes are extremes of a spectrum of craniofacial abnormalities and not nosologic entities [Muller et al., 1997; Steinberger et al., 1996].
Greig: 7p, GLI-3 Stickler: 12q, COL2A1; : 6p, COL11A2 DiGeorge: 22q Velocardiofacial: 22q Van der Woude: 1q Treacher Collins: 5q Saethre-Chotzen: 7p Cleidocranial dysplasia: 6p
Waardenburg I: 2q, PAX3 II: 3p, MITF Boston type CS: 5q, MSX2 Apert: 10q, FGFR2 Crouzon: 10q, FGFR2 Pfeiffer: 8p, FGFR1 : 10q, FGFR2
Holoprosencephaly: 2p, 7q Jackson-Weiss; 10q, FGFR2 Adelaide type CS: 4p Achondroplasia: 4p, FGFR3 Thanatophoric dysplasia: 4p, FGFR3
FIGURE 19-40. Syndromes associated with craniofacial malformations and craniosynostosis (CS) and their respective genetic abnormalities. (Courtesy of Dr. John B. Mulliken. Updated from a figure in Mulliken and Warman, 1996; the engraving of the full-term infant skull was originally taken from JBM Bougery, Traité complet de L’Anatomie de l’Homme, vol. 1, plate 14, Paris, 1831.)
444
Perinatal Acquired and Congenital Neurologic Disorders / 19
Clinical Characteristics Normal skull growth occurs perpendicular to each suture. If one suture is fused before birth, compensatory growth during infancy occurs parallel to that fused suture or across the non-united sutures, producing a characteristic abnormal head shape. More complex abnormalities of head shape and size occur with multiple suture fusion, such as cloverleaf skull malformation (kleeblattschädel). The deformity of the skull may be mild at birth; during ensuing rapid head growth the abnormal shape is exaggerated. Craniosynostosis is usually sporadic and occurs without associated anomalies. The rate of prevalence is about 0.04% to 0.1%. Approximately 2% to 8% of patients with isolated craniosynostosis have a familial defect. Craniosynostosis is occasionally associated with various anomalies and genetic and sporadic craniofacial disorders, including Apert’s, Saethre-Chotzen, and Carpenter’s syndromes and Crouzon’s disease, which have extracranial manifestations such as syndactyly, polydactyly, dysmorphic facies, midfacial hypoplasia, beaklike nose, and proptosis [Cohen, 1988]. Bilateral coronal and basal skull synostoses are common with these genetic disorders. Neuropathologic findings occasionally associated with craniosynostosis include holoprosencephaly, agenesis of the corpus callosum, hydrocephalus, Arnold-Chiari malformation, and myelodysplasia [Friede, 1989]. Choanal atresia also may accompany craniosynostosis and requires early surgical intervention. Cosmetic defects, restriction of brain growth with elevated intracranial pressure, and associated maldevelopment of facial and orbital structures are the important clinical features and focus of evaluation. Hydrocephalus, mental retardation, and symptoms associated with spinal cord anomalies also may develop [Hemmer et al., 1987; Noetzel et al., 1985]. Obstructive sleep apnea may also occur [Tajima and Imai, 1994]. Clinical diagnostic features of craniosynostosis include abnormal asymmetric craniofacial appearance, sutural ridging, and early closure of the fontanels. A small fontanel also may result from hyperthyroidism, primary microcephaly, a wormian bone (anterior fontanel bone), and other normal variations. In a neonate, palpable ridging of a suture suggests premature synostosis. Positional or birth molding needs to be excluded. The sutures can be separated with gentle palpation in the cases of overriding sutures resulting from birth molding. Cloverleaf skull or kleeblattschädel usually occurs as a result of premature closure of the cranial sutures, with accompanying hydrocephalus, proptosis, visual loss, and cranial base and midfacial hypoplasia [Goh et al., 1997; Zuccaro et al., 1996]. This rare malformation is associated with various congenital syndromes. Plain skull radiographs are usually diagnostic of craniosynostosis; hyperostotic bony fusion and obliteration of the suture characterize primary craniosynostosis. Highresolution three-dimensional CT reconstruction scanning is the radiologic procedure of choice for determining the extent of premature bone fusion [Abrahams and Eklund, 1995; Benson et al., 1996; Vannier et al., 1994]. In secondary craniosynostosis resulting from microcephaly, complete bone fusion is usually not observed, and the skull typically is symmetric. MRI is particularly useful in identifying the wide variety of
primary and secondary CNS malformations described in patients with craniosynostoses [Tokumaru et al., 1996].
Classification Several overlapping classifications of the craniosynostoses are commonly used. The most common is based according TABLE 19-23 Classification of Craniosynostosis TYPE
DISORDER
Primary head shape syndrome
Scaphocephaly Brachycephaly Plagiocephaly
Associated conditions
SUTURE(S) AFFECTED
Sagittal Coronal Coronal, lambdoidal, or both (unilateral) Trigonocephaly Metopic Oxycephaly Multiple Apert’s syndrome Coronal and basal skull Carpenter’s syndrome Coronal and basal skull Crouzon’s disease Coronal and basal skull Chromosomal abnormality Endocrine: hyperthyroidism (endogenous and exogenous), hypophosphatasia, hypercalcemia, rickets Hematologic diseases with bone marrow hyperplasia Inadequate brain growth: microcephaly, post-shunted hydrocephalus
Modified from Jacobson RI. Neurol Clin 1985;3:117.
FIGURE 19-41. Sagittal synostosis. Plain skull film from a 6-week-old infant demonstrates premature fusion and sclerosis of the sagittal suture. Note the elongated skull—scaphocephaly. (Courtesy of the Division of Pediatric Neurology, University of Minnesota Medical School, Minneapolis, Minn.)
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
FIGURE 19-42. Spiral computed tomography in craniosynostosis. The arrow on the ridged surface indicates the synostosis. The patient was a 6-month-old child. (From Binaghi S, Gudinchet F, Rilliet B. Three-dimensional spiral CT of craniofacial malformations in children. Pediatr Radiol 2000;30:856.)
to the abnormal shape of the skull produced by the prematurely closed suture or sutures [Cohen, 1988; McIntyre, 1997]. In practice, craniosynostosis is described by the involved suture or sutures (Table 19-23). Craniosynostoses are also classified as “primary” (idiopathic or genetic) or “secondary” (secondary to systemic or neurologic diseases). Other classifications have divided the craniosynostoses into “syndromic” and “nonsyndromic” groups. With the advent of determining the underlying molecular etiologies of craniosynostosis, genetic classification schemes are currently evolving [Epstein et al., 2004; Flores-Sarnat, 2002; Steinberger et al., 1996]. Sagittal Synostosis. Premature fusion of the sagittal suture (scaphocephaly) is the most common form of craniosynostosis, comprising approximately 60% of all types. Most patients are boys; the defect may be familial and is usually not syndromic. The anteroposterior diameter of the skull is elongated and the transverse diameter decreased (Figs. 19-41 and 19-42). This abnormal head shape is present at birth, with palpable ridging over the sagittal suture. The neurologic examination is normal in most patients [Boop et al., 1996a]. Scaphocephaly (dolichocephaly) in premature infants results from positional molding and not from premature suture closure. Coronal Synostosis. Bilateral coronal synostosis (brachycephaly) comprises about 20% of cases of craniosynostosis and is more common in females (Fig. 19-43). The skull is shorter in the anteroposterior diameter but is widened with a high vault; the occiput and forehead are flattened. The anterior fontanel is displaced anteriorly, and ridging may be palpated over the prematurely closed coronal sutures. Neurologic features, especially in untreated cases, include proptosis, strabismus, papilledema, and optic atrophy [Gupta et al., 1993]. The skull radiograph may document an elliptic orbit, or harlequin eye sign, on the side of the coronal synostosis (Fig. 19-44). Single Synostosis. Single synostosis, or plagiocephaly, describes the asymmetric skull without indicating which suture is involved. Unilateral closure of a coronal suture,
445
FIGURE 19-43. Three-dimensional craniofacial shaded surface display. Study performed in a 2-day-old infant with compound craniosynostosis secondary to Crouzon’s syndrome demonstrates bilateral incomplete coronal synostosis associated with compensatory widening of the metopic (large arrow) and temporoparietal (small arrows) sutures. (From Binaghi S, Gudinchet F, Rilliet B. Three-dimensional spiral CT of craniofacial malformations in children. Pediatr Radiol 2000;30:856.)
lambdoidal suture, or both causes an asymmetric skull. In lambdoidal synostosis, the ipsilateral ear is displaced anteriorly, one frontal bone is larger than the other, and the occipital bones manifest a similar but contralateral asymmetry [Hinton et al., 1984]. The head shape is skewed to resemble a parallelogram. Both lambdoidal synostosis and deformational forces have been implicated as potentially causal in the pathogenesis of this deformity [Dias and Klein, 1996]. Enlarged subarachnoid spaces also have been observed in children with occipital plagiocephaly; this feature may increase the compliance and malleability of the calvaria and sutures and predispose the affected child to the development of a positional deformity [Sawin et al., 1996]. A similar head shape occurs in infants with congenital torticollis but without craniosynostosis. Congenital muscular torticollis, or congenital wryneck, consists of head tilt and unilateral shortening and contracture of the sternocleidomastoid muscle. During early infancy the head and face become progressively deformed, producing asymmetry of the head that may mimic plagiocephaly from craniosynostosis—that is, flat contralateral occiput and ipsilateral face and frontal area. Characteristic clinical features include head tilt towards the side of the affected muscle with the chin turned to the opposite side. By contrast, patients with coronal plagiocephaly have head tilt that is due to extraocular muscle dysfunction rather than to the skull deformity [Gosain et al., 1996]. Metopic Synostosis. Premature closure of the metopic suture (trigonocephaly) results in a pointed forehead with a prominent ridge in the midforehead area. The eyes are close together, the forehead is narrow, and the anterior skull appears triangular when viewed from above. Some patients may have related abnormalities, including mental retardation, cleft palate, coloboma, anomalies of the urinary tract, and holoprosencephaly. The incidence of metopic synostosis ranges from 1 in 7000 to 1 in 70,000 live births. It usually occurs as an isolated synostosis and several subtypes have
446
Perinatal Acquired and Congenital Neurologic Disorders / 19
A
B
C
D
FIGURE 19-44. Unilateral coronal synostosis in a 1-year-old male infant. A, Axial cut from a computed tomography (CT) study with bone windowing demonstrates “contraction” of skull base on the left side of the synostosis (arrows). B, Cut-away ventral view of inner calvaria from the same study as in A using CT with three-dimensional reconstructions. Note elevated left sphenoidal wing (arrow). C, Viewing skull from above, with the same threedimensional data, the sagittal suture (arrow) can be seen to be rotated away from the synostotic suture and the flattened contour of the skull around it. D, Flattened skull deformity is well demonstrated looking from below. (Courtesy of Joseph R. Thompson, Department of Radiation Sciences, Loma Linda University School of Medicine, Loma Linda, Calif.)
been categorized based on the severity of the skull base deformity. In 10% to 20% of patients, other sutures are involved, and in 2% to 5% of patients, the condition is familial. Intracranial hypertension has been observed in some patients but is never severe [Collmann et al., 1996]. Disorders of visual function, such as astigmatism and strabismus, can occur with trigonocephaly [Denis et al., 1994]. About one third of patients with metopic synostosis are found to have cognitive and behavioral abnormalities on long-term follow-up evaluation [Sidoti et al., 1996]. Agenesis of the corpus callosum may also be recognized in some patients with trigonocephaly. In children born with fetal
valproate syndrome, it is important to be aware of the possibility of metopic suture synostosis, which some authorities believe should be considered part of the syndrome. Early surgical intervention in such patients may improve cognitive outcome [Lajeunie, et al., 2001]. Multiple Synostosis. Premature closure of both coronal and sagittal sutures results in oxycephaly. This abnormality may cause increased intracranial pressure and significant neurologic sequelae. Examination often reveals optic atrophy or papilledema, exophthalmos, and choanal atresia. Auditory and vestibular disturbances result from narrowing of the internal auditory canal. Turricephaly involves synostoses of
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
447
TABLE 19-24 Prevalence and Molecular Basis of FGFR-Related Craniosynostosis Syndromes
From http://www.geneclinics.org.
the coronal, sphenofrontal, and frontoethmoidal sutures with both shortening of the anteroposterior diameter of the skull, as well as the skull appearing excessively high and narrow. Both oxycephaly and turricephaly usually do not appear before the age of 2 years. Secondary turricephaly may occur after initial correction of coronal synostoses [Sonstein et al., 1996].
Nonsyndromic Craniosynostoses Nonsyndromic craniosynostoses usually can be identified by a combination of suture involvement and morphologic appearance. There remains a group of patients with nonsyndromic craniosynostoses who have been difficult to classify. A study of 53 such patients representing 3.6% of patients with craniosynostosis categorized these patients into the following two groups: (1) those with two-suture disease and (2) a “complex” group in which more than two sutures were affected [Chumas et al., 1997]. Group 1 patients (68%) demonstrated no progression over time, to suggest a more diffuse pansynostosis. The sagittal suture was the most commonly involved, and a trend for these patients to have a higher intelligence quotient was noted. Group 2 patients presented at a slightly earlier age (1 year) with severe morphologic changes and multiple suture involvement, with bilateral involvement of lambdoid and sagittal sutures being the most common.
Syndromic Craniosynostoses In the past decade, understanding of many of the classic craniosynostosis syndromes has changed dramatically because the genetic bases for these disorders are being determined (see Tables 19-20 and 19-22).
FGFR-RELATED CRANIOSYNOSTOSIS SYNDROMES Diagnosis of most of the FGFR-related craniosynostosis syndromes is based on the clinical findings of bilateral
coronal craniosynostosis or cloverleaf skull, characteristic facial features, and variable hand and foot abnormalities. The exception is Muenke’s syndrome, which may have unilateral coronal synostosis or megalencephaly without craniosynostosis; its diagnosis depends on identification of a mutation in the FGFR3 gene. A summary of the prevalence and molecular basis of FGFR-related craniosynostosis syndromes is given in Table 19-24.
Apert’s Syndrome First described in 1906, Apert’s syndrome (acrocephalosyndactyly type 1) is inherited as an autosomal dominant trait, occurs in approximately 1 in 65,000 births, and accounts for approximately 4.5% of all patients with craniosynostosis. Apert’s syndrome maps to chromosomal region 10q26 and is caused by a mutation of the FGFR2 gene; in nearly all cases in which the mutation has been identified, it occurs in one of two adjacent sites of the gene, either position 252 or position 253 [Anderson et al., 2004; Ibrahimi et al., 2005]. The 253 mutation appears to be associated with the more severe forms, with regard to the severity of syndactyly and to mental outcome [Lajeunie et al., 1999]. Unregulated FGF2 signaling caused by mutations in FGFR2 suggests increased constitutive receptor activity in Apert mutant osteoblasts and an autocrine loop involving the FGF2 pathway in modulation of Apert osteoblast behavior [Baroni et al., 2005]. In most patients, the mutant allele is paternal in origin. Paternal bias for point mutations is seen in other genetic conditions, but the skewing seen in Apert’s syndrome in favor of paternal mutations is considered unusual and possibly is related to a paternal age effect [Glaser et al., 2003]. Discovery of mutations in FGFR genes allows definitive antenatal diagnosis of Apert’s syndrome [Hansen et al., 2004]. Multiple sutures are involved, with the coronal most frequently affected [Renier et al., 2000]. These patients are readily recognized at birth because of the associated severe fusion syndactyly involving the hands and feet, hypertelorism, proptosis, and down-slanting palpebral fissures.
448
Perinatal Acquired and Congenital Neurologic Disorders / 19
Hydrocephalus is common. Radiologic investigation of the cervical spine is indicated in patients with Apert’s syndrome. Fusion of the cervical vertebrae, primarily at the C5 to C6 level, occurs in 68% (single fusion 37%; multiple fusions 31%) [Kreiborg et al., 1992]. Patients with Apert’s syndrome have “interrupted eyebrows,” presumably resulting from an underlying bony defect. In older children and adolescents, hyperhidrosis of the hands and acneiform lesions are common skin manifestations. Patients with Apert’s syndrome have varying degrees of mental retardation [Sarimski, 1997]. In one study of 29 patients, 48% had a normal or borderline IQ, 31% had mild mental retardation (IQ of 50 to 70), 14% were moderately retarded (IQ of 35 to 49), and 7% were severely retarded (IQ less than 35) [Patton et al., 1988]. Moderate-to-severe language impairment, relatively normal performance IQ, and difficulties with attention, speech and oral motor skills also have been reported [Shipster et al., 2002]. Other problems that have received attention are a higher incidence of autism [Artigas-Pallares et al., 2005], obstructive sleep apnea [Pijpers et al., 2004], visual loss without other symptoms of intracranial hypertension [Bartels, et al., 2004], and hearing loss [Huang et al., 2004]. The mean intracranial volume also is increased in persons with Apert’s syndrome irrespective of whether the genotype is 252 or 253 [Anderson, et al., 2004]. Early craniectomy does not appear to improve intellectual outcome. Cohen and Kreiborg [1990] observed that many patients with Apert’s syndrome had ventriculomegaly or CNS malformations that frequently involved the corpus callosum or limbic structures. Other malformations in previously reported cases included megalencephaly, gyral abnormalities, encephalocele, pyramidal tract abnormalities, hypoplasia of cerebral white matter, and heterotopic gray matter [Cohen and Kreiborg, 1990]. By contrast, Reiner and colleagues [1996] found an IQ greater than 70 in half the children who had corrective surgery before age 1 year versus only 7.1% of those operated on later. They also found that anomalies of the septum pellucidum correlated with IQ, whereas malformations of the corpus callosum and ventricular size did not. More recent studies involving 18 patients with Apert’s syndrome have reported the absence of CNS anomalies in 44% of patients [Yacubian-Fernandes, et al., 2004]. The remaining patients had ventricular enlargement, corpus callosum hypoplasia, septum pellucidum hypoplasia, cavum vergae and a posterior fossa arachnoid cyst. Herniation of the cerebellar tonsils may also occur [Fearon et al., 2001]. Abnormalities of venous drainage that particularly affect the sigmoid-jugular sinus complex can produce a state of venous hypertension that may cause raised intracranial pressure with resultant blindness [Taylor et al., 2001]. In such patients in whom this is suspected, cerebral angiography or MR venography is necessary.
Crouzon’s Disease Crouzon’s disease accounts for approximately 5% of patients with craniosynostosis at birth and is due to closure of the coronal and basal skull sutures. This disorder was first reported in 1912. An autosomal-dominant pattern of inheritance is recognized in about three fourths of patients; the remaining cases are sporadic. Crouzon’s disease maps to chromosome 10q26, and in some series, mutations in the
FGFR2 gene have been reported in about half of the patients [Glaser et al., 2000; Reardon et al., 1994]. Recent studies of patients with the Crouzon and Pfeiffer types of craniosynostosis have found that mutations in the FGFR2 cluster at two critical cysteine residues, 278 and 342 [Kress et al., 2000].The spectrum of mutations overlap the two syndromes and reflect the phenotypic similarities observed in both patient groups. Associated features include hypertelorism, shallow orbits, exophthalmos, external strabismus, parrot-beaked nose, short upper lip, hypoplastic maxilla, and relative mandibular prognathism. Mental function in patients with Crouzon’s disease varies from normal in some series to up to 26% of patients with mental retardation [Hunter and Rudd, 1977; Kapp-Simon et al., 1993; Noetzel et al., 1985]. In a more recent series, 12% of patients had evidence of decreased mental function [Proudman et al., 1995]. Hydrocephalus is common in patients with Crouzon’s disease and may evolve over time [Hoefkens et al., 2004]. About 28% require surgical treatment, and 73% of these patients have chronic tonsillar herniation [Cinalli et al., 1995; David et al., 2002]. Syringomyelia may also occur [Fujisawa et al., 2002]. Other CNS anomalies are reported in about 14% of patients [Proudman et al., 1995]. Obstructive sleep apnea may also develop in children with Crouzon’s syndrome [Mitsukawa et al., 2004]. A rare form of Crouzon’s disease with acanthosis nigricans has been reported and is associated with an FGFR3 mutation in all patients [Meyers et al., 1995].
Jackson-Weiss Syndrome Jackson-Weiss syndrome has been reported in a large Amish kindred with coronal and basal skull craniosynostosis, enlarged great toes, and craniofacial abnormalities. JacksonWeiss syndrome is an autosomal-dominant disorder and resembles Pfeiffer’s syndrome except for the absence of thumb abnormalities [Jackson et al., 1976]. Jackson-Weiss syndrome maps to the same region (10q23-q26) as for Crouzon’s disease [Li et al., 1994], and at least six different mutations in the FGFR2 gene have been demonstrated [Heike et al., 2001; Jabs et al., 1994]. The evolution of craniofacial deformities seen in patients with the Jackson-Weiss syndrome seems to parallel those described with Crouzon’s disease and suggests similar evaluation and management strategies [Stankovic et al., 1994].
Pfeiffer’s Syndrome Pfeiffer’s syndrome is a form of acrocephalopolysyndactyly (type 5a) that differs from Apert’s syndrome (type 1) because of the presence of polydactyly. Since Pfeiffer’s original description in 1964, three subtypes have been categorized (see Table 19-24) [Cohen, 1993, 2000]. Patients have synostosis of the coronal and basal skull sutures, broad, short thumbs, and big toes. The proximal phalanx of the thumb usually is either triangular or trapezoid and occasionally is fused with the distal phalanx so that the thumb points outward. Developmental outcomes of patients with Pfeiffer’s syndrome are variable; most patients with type 1 Pfeiffer’s syndrome have normal development and a generally favorable outcome [Cohen, 1993]. A more recent report of Pfeiffer’s syndrome in six children with types 2 and 3 found essentially normal development in three, mild delay in two, and moderate delay in one [Robin et al., 1998].
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
The classic type of Pfeiffer’s syndrome (type 1) is an autosomal-dominant disorder that has been associated with deletions of either the FGFR2 gene that maps to chromosome 10 (the original family reported by Pfeiffer was of this type) or to the FGFR1 locus on chromosome 8 [Ibrahimi et al., 2004; Muenke et al., 1994; Schell et al., 1995]. Moderate-to-severe conductive hearing or mixed hearing loss is common in patients with Pfeiffer’s syndrome [Vallino-Napoli, 1996]. CT abnormalities include external auditory canal stenosis or atresia, or either hypoplasia or enlargement of the middle ear cavity and hypoplastic ossicles. Prenatal diagnosis has been reported in several cases based on ultrasound findings of craniosynostosis, hypertelorism, extreme proptosis, and broad thumbs [Nazzaro et al., 2004]. Elevated intracranial pressure may occur in patients with Pfeiffer’s syndrome and requires surgical intervention [Gosain, et al., 1996] The type 2 form consists of a cloverleaf skull deformity with Pfeiffer’s hands and feet and ankylosis of the elbows [Oyamada et al., 2003]. Most patients with the type 2 form have significant developmental lags, but normal development can occur [Soekarman et al., 1992]. Type 2 cases all have been sporadic, in all likelihood caused by new mutations in the FGFR2 gene or in another unidentified gene. Most patients die shortly after birth from severe pulmonary or CNS abnormalities (cloverleaf skull and hydrocephalus), prematurity, or postoperative complications [Plomp et al., 1998; Teebi et al., 2002]. Type 3 is similar to type 2 but without the cloverleaf skull deformity [Robin et al., 1998]. Ocular proptosis is severe, and the anterior cranial base is markedly short. Various visceral malformations have been found in patients with type 3. Early demise is also characteristic of type 3, which has only occurred sporadically [Cohen and Barone, 1994]. Although children with types 2 and 3 have an increased risk for neurodevelopmental difficulties, a favorable outcome can be achieved in some cases with aggressive medical and surgical management [Robin et al., 1998].
Muenke’s Craniosynostosis This new clinical syndrome, first reported in 1997, is known as FGFR3-associated coronal synostosis syndrome and maps to chromosomal region 4p16.3 [Muenke et al., 1997]. It may ultimately be determined to be one of the most common genetic causes of craniosynostosis. In addition to craniosynostosis, affected persons may have radiographic abnormalities of the hands and feet, including thimble-like middle phalanges, coned epiphyses, carpal and tarsal fusions, and brachydactyly [Graham et al., 1998]. In some reports, mental retardation is a common feature (44%) [Reardon et al., 1997]. Muenke’s craniosynostosis is caused by a point mutation (C749G) on the FGFR3 gene, resulting in a Pro250Arg substitution. This substitution usually occurs as a new mutation and manifests as one of the highest documented rates for any transversion in the human genome [RannanEliya et al., 2004]. The P250R mutation also has been reported in families with autosomal dominant congenital moderately severe bilateral sensorineural deafness in which some of the family members also had craniosynostosis [Holloway et al., 1998]. In more recent studies, the P250R mutation was identified in 20 probands from 27 unrelated families (74%), whereas only 6 of 35 sporadic cases (17%)
449
were found to have this mutation, and in both the familial and the sporadic cases, females were more severely affected [Lajeunie et al., 1999]. EEG abnormalities with bitemporal discharges and poor gray-white matter differentiation, defective gyri, and abnormally shaped hippocampi have been reported in Muenke’s syndrome [Grosso et al., 2003]. It is likely that patients previously described as having the Adelaide form of craniosynostosis have Muenke’s craniosynostosis.
Beare-Stevenson Syndrome Fewer than 10 patients with this disorder, which is associated with FGFR2 [Przylepa et al., 1996] and FGFR3 mutations [Roscioli et al., 2001], have been described. The disorder is associated with craniosynostosis, ear defects, cutis gyrata, acanthosis nigricans, anogenital anomalies, skin tags, and a prominent umbilical stump.
TWIST-RELATED CRANIOSYNOSTOSIS SYNDROMES Saethre-Chotzen Syndrome Saethre-Chotzen syndrome is an autosomal-dominant disorder with coronal and basal skull synostosis. The coronal synostosis is frequently asymmetric, causing plagiocephaly and facial asymmetry. Partial soft tissue syndactyly of the second and third digits and third and fourth toes is common. The thumbs and big toes are normal. Strabismus, ptosis, low frontal hair line, a long, thin pointed nose, and unusually shaped ears with a prominent crus are common [Carter et al., 1982; von Gernet et al., 1996]. Torticollis, clinodactyly of the fourth and fifth toes, large halluxes, and sensorineural hearing loss and cervical vertebral body fusion may occur [Clauser et al., 2000; Legius et al., 1989]. In some patients with Saethre-Chotzen syndrome, delayed onset of development of craniosynostosis has been reported [De Heer et al., 2004b]. Obstructive sleep apnea has also been reported [Pijpers et al., 2004]. Neurologic manifestations of Saethre-Chotzen syndrome include seizures and abnormal EEGs in slightly less than half the patients and significant neuroimaging abnormalities [Elia et al., 1996]. Cervical spine fusion (primarily at the C2-3 level) that is progressive during childhood occurs in about half the patients [Anderson et al., 1997a]. Conductive hearing loss resulting from cranial bone involvement (stapes ankylosis, small or even absent mastoids), atresia of the ear canal, or chronic ear infections may occur [Ensink et al., 1996]. Saethre-Chotzen syndrome is caused by mutations in the TWIST gene on chromosome 7p21 [Gripp et al., 2000]. To date, more than 80 different mutations in TWIST have been reported [Brueton et al., 1992; De Heer et al., 2004a; El Ghouzzi et al., 1997; Howard et al., 1997]. The TWIST gene product is a transcription factor containing a basic helixloop-helix (b-HLH) domain, required in head mesenchyme for cranial neural tube morphogenesis in mice [El Ghouzzi et al., 1997]. The TWIST gene was selected as a candidate gene for patients with Saethre-Chotzen syndrome, because the expression pattern and mutant phenotypes in Drosophila and mouse were consistent with the human phenotype [Howard et al., 1997]. In one study of 37 patients with classic features of Saethre-Chotzen syndrome, the overall detection rate for TWIST mutations was 68%. The risk for developmental delay
450
Perinatal Acquired and Congenital Neurologic Disorders / 19
in patients with deletions involving the TWIST gene is approximately 90%, or eight times more common than in patients with intragenic mutations [Cai et al., 2003]. Other investigators have reported a mutation of the FGFR3 gene in a large family with autosomal-dominant craniosynostosis suggestive of Saethre-Chotzen syndrome, in which linkage to the Saethre-Chotzen syndrome loci on 7p had been excluded [Golla et al., 1997]. A recent study found that 82% of patients with the Saethre-Chotzen phenotype had detectable genetic changes in the TWIST gene or of FGFR3 and it was suggested that initial screening for the FGFR3 P250R mutation, followed by sequencing of TWIST and then fluorescence in situ hybridization for deletion detection of TWIST, is sufficient to detect mutations in greater than 80% of patients with the Saethre-Chotzen phenotype [Chun et al., 2002]. The overlap in clinical features and the presence, in the same genes, of mutations for more than one craniosynostotic condition—such as Saethre-Chotzen syndrome, Crouzon’s disease, and Pfeiffer’s and Muenke’s syndromes—support the hypothesis that TWIST and FGFR genes are components of the same molecular pathway involved in the modulation of craniofacial and limb development in humans [Paznekas et al., 1998]. Studies using human mutant calvaria osteoblastic cells from a child with Saethre-Chotzen syndrome with a TWIST mutation found increased cell growth, collagen expression, and osteogenic capability, but inhibition of osteocalcin gene expression. In part, this may explain the development of the premature cranial ossification in patients with SaethreChotzen syndrome [Yousfi et al., 2001].
Baller-Gerold Syndrome Baller-Gerold syndrome is a rare form of craniosynostosis described by Baller in 1950 and Gerold in 1959. Essential features include radial or thumb aplasia with craniosynostosis (coronal, lambdoid or metopic) resulting in acrocephaly. Fewer than 50 cases have been described, and some authorities question whether this should be considered a separate syndrome, because overlap with Saethre-Chotzen syndrome is well recognized [Cohen and Toriello, 1996; Gripp et al., 1999; Temtamy et al., 2003]. Although this initially was thought to be an autosomal-recessive disorder, recent studies suggest an autosomal-dominant pattern of inheritance associated with a nonsense mutation in TWIST, a gene associated with SaethreChotzen syndrome [Gripp et al., 1999; Seto et al., 2001]. Baller-Gerold syndrome after fetal exposure to sodium valproate also has recently been reported [de Oliveira et al., 2005]. Short stature, spine and pelvic skeletal anomalies, cardiac or urinary tract anomalies, imperforate anus, and rectovaginal fistulas are reported. Mental retardation, congenital hydrocephalus, polymicrogyria, and partial agenesis of the corpus callosum have been noted in some patients [Dunac et al., 1995; Gripp et al., 1999; Lewis et al., 1991; Rossbach et al., 1996]. Other cases of presumed Baller-Gerold syndrome have been rediagnosed as Roberts’ syndrome, Fanconi’s pancytopenia, Rothmund-Thomson syndrome, or VACTERL association (vertebral anomalies, anal atresia, cardiac defect [most often ventricular septal defect], tracheoesophageal fistula with esophageal atresia, renal abnormalities, limb abnormalities [most often radial dysplasia]) [Temtamy et al., 2003]. These reports have led to a narrowed redefinition of Baller-Gerold syndrome based on the exclusion of cytogenetic and hematopoetic abnormalities and the
absence of additional malformations in patients with craniosynostosis and preaxial upper limb abnormalities [Gripp et al., 1999].
MSX-RELATED CRANIOSYNOSTOSIS SYNDROMES Boston-Type Craniosynostosis Fewer than 30 patients with this form of craniosynsostosis have been reported; most have been from one family [Warman et al., 1993]. Four general phenotypes emerged: (1) fronto-orbital recession; (2) frontal bossing; (3) turribrachycephaly due to coronal craniosynostosis; and (4) cloverleaf skull. Short first metatarsals are present. Headaches, seizures, myopia, and visual deficits may occur. The gene for this disorder is located on 5q. Mutations in MSX2 are causative [Jabs et al., 1993]. Inheritance is autosomal dominant, with complete penetrance and variable expression.
FIBRILLIN-RELATED CRANIOSYNOSTOSIS SYNDROMES Shprintzen-Goldberg Syndrome Shprintzen-Goldberg syndrome is rare (fewer than 40 patients reported), is also known as the marfanoid craniosynostosis syndrome, and consists of multiple suture synostoses in association with severe exophthalmos, maxillary and mandibular hypoplasia, soft tissue hypertrophy of the palatal shelves, low-set ears with soft and pliable auricles, multiple abdominal hernias, arachnodactyly, and camptodactyly. Hypotonia, mental retardation, and obstructive apnea are common. Shprintzen-Goldberg syndrome, which maps to 15q21.1, is distinct from the velocardiofacial syndrome, also known as Shprintzen’s syndrome (22q11 deletion), that is characterized by cleft palate, cardiovascular anomalies, typical facies, and learning disorders [Carlson et al., 1997]. Skeletal abnormalities in patients with ShprintzenGoldberg syndrome include progressive bowing of long bones, metaphyseal flaring, large persistent anterior fontanel, 13 pairs of ribs, vertebral abnormalities that develop by the second year of life, and progressive osteopenia. Communicating hydrocephalus is common [Ades et al., 1995] and epilepsy has been reported [Tanaka et al., 1993]. Abnormalities of the first and second cervical vertebrae, dilation of the lateral ventricles, microcephaly, hypoplasia of the corpus callosum and Arnold-Chiari I malformations have also been documented [Greally et al., 1998; Hassed et al., 1997; Saal et al., 1995]. MR imaging abnormalities, osteopenia, and progressive hydrocephalus are also found in this disorder as well as ventriculomegaly and Chiari-I malformations [Greally et al., 1998; Hassed et al., 1997; Ohnuma et al., 1997]. Overlap with patients who have marfanoid features has also been recognized [Lacombe and Battin, 1993; Saal et al., 1995] and several investigators have found that ShprintzenGoldberg syndrome is associated with mutations of the same gene (fibrillin-1) that is involved in Marfan’s syndrome [Sood et al., 1996]. Fibrillins 1 and 2 are major components of extracellular microfibrils and are widely distributed in connective tissue throughout the body and are responsible for the biomechanical properties of most tissues and organs [Ramirez and Pereira, 1999]. Fibrillins are cysteine-rich glycoproteins made predominantly of multiple repeats homologous to the calcium-binding epidermal growth factor module. Fibrillins polymerize extracellularly as parallel bun-
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
451
dles of head-to-tail monomers. Binding to calcium rigidifies the structure of the monomers. Mutations in the fibrillin-1 (FBN1) gene, at 15q21.1, have been found to cause Marfan’s syndrome, a dominantly inherited disorder characterized by clinically variable skeletal, ocular, and cardiovascular abnormalities. Fibrillin-1 mutations have been found not only in Shprintzen-Goldberg syndrome but also in several other related connective tissue disorders, such as severe neonatal Marfan’s syndrome, dominant ectopia lentis, familial ascending aortic aneurysm, and isolated skeletal features of Marfan’s syndrome [Hayward and Brock, 1997]. Fibrillin-2 alterations cause the overlapping phenotype of congenital contractural arachnodactyly.
acrocephaly or turricephaly (coronal and basal skull sutures), peculiar facies, brachydactyly and syndactyly of the hands and preaxial polydactyly and syndactyly of the toes, and congenital heart disease [Cohen et al., 1987]. Fewer than 50 persons with Carpenter’s syndrome have been described. Obesity, mental retardation, hypogonadism, cryptorchidism, umbilical hernia, and bone abnormalities occur. Hearing loss is a rare complication [Tarhan et al., 2004]. Craniosynostosis variants considered within the clinical spectrum of Carpenter’s syndrome include Summitt’s syndrome, Goodman’s syndrome, and Sakati-Nyhan syndrome. Dental abnormalities including prolonged retention of primary teeth and hypodontia have been reported [Blankenstein et al., 2001]. Mental retardation is not an invariable feature of this syndrome.
OTHER CRANIOSYNOSTOSIS SYNDROMES
Hunter-McAlpine Syndrome
Craniosynostosis can be a finding in greater than 150 genetic disorders [Cohen, 2000]. In addition to those disorders in which specific genetic abnormalities have been described, several other craniosynostosis syndromes have been described that have yet to have a specific gene abnormality determined. They are included here because they are more common and have features that suggest their diagnosis based on clinical criteria.
Hunter-McAlpine syndrome is a form of craniosynostosis that was first described by Hunter and Rudd [1977] and consists of brachyphalangia, mental retardation, and facial dysmorphism. Patients have a small or downturned mouth, almond-shaped palpebral fissures, short stature, and acralskeletal abnormalities. Fewer than 10 cases of this autosomal dominant disorder have been reported. Thomas and colleagues [1996] described a 9-year-old boy with this disorder in whom a deletion at 17q23.1-q24.2 was detected. Considerable phenotypic variability within families exists. More recently, the original family members with this disorder and another reported patient were found to have a duplication of 5q35-qter [Hunter et al., 2005]. Debate also exists regarding whether the Hunter-McAlpine syndrome is identical to the Ruvalcaba syndrome or represents a type of trichorhinophalangeal syndrome.
Antley-Bixler Syndrome Fewer than 50 cases of this autosomal-recessive disorder have been reported since its original description in 1975. Cardinal features include craniosynostosis, radiohumeral synostosis, multiple joint contractures, arachnodactyly, femoral bowing, severe midface hypoplasia, proptosis, choanal atresia/stenosis, frontal bossing, dysplastic ears, depressed nasal bridge, long bone fractures, ambiguous genitalia and urogenital abnormalities [Hassell and Butler, 1994]. Renal agenesis and imperforate anus may occur as well [LeHeup et al., 1995]. Early death, usually due to respiratory complications linked to upper airway obstruction, occurred in about half of the reported cases. Coronal and lambdoid sutures are affected, giving the head a trapezoidal shape (“trapezoidocephaly”). Approximately one third of patients have survived, many with normal intelligence; others have varying degrees of disability [Bottero et al., 1997; Hassell and Butler, 1994]. Hydrocephalus and the Arnold-Chiari malformation have been described in some children with Antley-Bixler syndrome [Lee et al., 2001]. Although mutations in the FGFR2 gene have been found in some patients with Antley-Bixler syndrome [Chun et al., 1998], genetic heterogeneity of this syndrome has been proposed. In addition, particularly in infants with ambiguous genitalia, unique abnormalities in steroidogenesis (apparent decreased activity of 17α-hydroxylase, 17,20-lyase, and 21-hydroxylase) have been reported [Adachi et al., 2004]. Some investigators have suggested that the skeletal findings and altered steroidogenesis are not associated with genes specific to individual sterol or steroid pathways but rather are related to NADPH cytochrome P-450 reductase or cytochrome b5, which is common to these pathways [Cragun et al., 2004; Fukami et al., 2005].
Carpenter’s Syndrome Carpenter’s syndrome (acrocephalopolysyndactyly type II) also is a rare autosomal-recessive form of craniosynostosis, originally described in 1909, with major features consisting of
Lowry-MacLean Syndrome Lowry-MacLean syndrome is a rare syndrome of presumed autosomal-dominant inheritance that consists of multiple congenital anomalies and mental retardation with cleft palate, eventration of the diaphragm, congenital heart disease, glaucoma, craniosynostosis (usually coronal), and growth failure [Kousseff et al., 1994; Lowry and MacLean, 1977]. Congenital glaucoma and a Crouzon-like facial appearance are recognized [Al-Torki et al., 1997].
Evaluation Evaluation and management of children with craniosynostosis require radiologic and neuroimaging confirmation, molecular genetic testing, and a team of specialists including neurosurgeons, craniofacial surgeons, anesthesiologists, otorhinolaryngologists, child neurologists, geneticists, speech pathologists, psychologists, and physical and occupational therapists. Although conventional skull radiographs are helpful and frequently diagnostic, most centers recommend threedimensional CT scans [Binaghi et al., 2000]. Some centers have questioned their need in the management of single-suture craniosynostosis, however [Cerovac et al., 2002]. Such scans can depict suture patency, extent of synostosis, and the degree of calvarial deformity and can differentiate true synostosis from deformational plagiocephaly [Flores-Sarnat, 2002; Panchal and Uttchin, 2003]. MRI also should be considered, because it may detect underlying brain malformations that may not be seen with three-dimensional CT scans, which are
452
Perinatal Acquired and Congenital Neurologic Disorders / 19
Apert’s syndrome
Crouzon’s and Pfeiffer’s syndromes
SaethreChotzen syndrome
Muenke’s syndrome
Unilateral coronal synostosis
FGFR2 (P252W S253R)
FGFR2 (IIIa, IIIc) sequence
TWIST sequence
FGFR3 (P250R)
FGFR3 (Pro250Arg) FGFR2 TWIST
Stop
Stop
–
+
+
–
Stop
FGFR3 (P250R)
FGFR3 (P250R)
focused on delineating the severity of the cranial vault dysplasia. In one report comprising 217 children with craniofacial anomalies, brain anomalies were present in 36%, absent in 36%, and undefined in 28%. Craniosynostosis occurred in 74% of these children, and a syndromic diagnosis was established in 50% [Okkerse et al., 2004]. CNS malformations reported in association with craniosynostosis include DandyWalker malformation, partial agenesis of the corpus callosum, holoprosencephaly, and the appearance of blunted gyri under the area of suture synostosis [Flores-Sarnat, 2002]. The yield from molecular testing of children with craniosynostosis likely will increase over the next decade as genetic abnormalities are identified. In one recent report, a molecular diagnosis was made in 51% of 99 patients who had one of the common bilateral coronal craniosynostosis syndromes [Chun et al., 2003]. The diagnostic yield in patients with unilateral coronal synostosis is lower, at 7% [Lajeunie et al., 1999], 11% [Gripp et al., 1998], and 17% [Mulliken et al., 2004] in reported series. Although the yield is lower for patients with unilateral coronal synostosis, screening is recommended by most investigators for the purpose of genetic counseling [Mulliken et al., 2004; Zackai et al., 2000]. An algorithm for this evaluation modified from the work of Chun and colleagues [2003] is presented in Figure 19-45. Several Web-based resources are available that provide current recommendations, laboratory sites, and contact information (http://www.geneclinics.org/ and http://rarediseases.info.nih. gov/html/resources/info_cntr.html).
Reconstructive Surgery Numerous approaches have been developed to treat the various forms of craniosynostosis [Posnick and Ruiz, 2000]. The goals of treatment of primary craniosynostosis are fourfold: (1) to ensure normal brain growth, (2) to prevent increased intracranial pressure, (3) to prevent compromise of visual and auditory function, and (4) to improve skull and facial appearance [Bruce, 1996; Keating, 1997; Thauvoy et al., 1995]. Patients with microcephaly or cerebral atrophy resulting in secondary craniosynostosis do not benefit from
FIGURE 19-45. Diagnostic strategy for molecular testing of craniosynostosis. Apert’s syndrome and Muenke’s syndrome patients are screened for recurrent mutations in FGFR2 and FGFR3, respectively. For Crouzon’s syndrome and Pfeiffer’s syndrome patients, FGFR2 exons IIIa and IIIc are initially sequenced, and for Saethre-Choutzen syndrome patients, TWIST is sequenced. If the sequencing is positive for a mutation, further screening is not necessary. If the sequencing is negative, patients are tested for the FGFR3 P250R mutation. (From Chun K, Teebi AS, Azimi C, et al. Screening of patients with craniosynostosis: Molecular strategy. Am J Med Genet A 2003;120:470. Reprinted with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc.)
surgery because the defect in skull growth is secondary to the already impaired brain growth. The general management of craniofacial syndromes can be summarized as follows [Panchal and Uttchin, 2003]: Step I: Correction of craniosynostosis between the ages of 3 and 6 months. Step II: Correction of syndactyly between the ages of 1 and 2 years. Step III: Correction of midface retrusion with distraction techniques by the age of 4 to 5 years. Timing and progress of the distraction may vary, depending on the severity of obstructive sleep apnea, malocclusion, and psychologic disturbance. Step IV: Correction of hypertelorism and turricephaly, if present, at age 4 to 6 years. This may be done in conjunction with, or separately from, step III. Step V: Await full maturity and perform Le Fort I or Le Fort III procedure in conjunction with mandibular osteotomy to normalize appearance and correct malocclusion. The ultimate configuration of the skull and face depends on the location and number of the prematurely fused sutures and the age of the patient. In sagittal suture synostosis, cosmetic improvement is the main indication for surgery although in some children raised intracranial pressure may be present and is the primary reason for treatment. With multiple suture synostosis or cases involving the coronal suture or sutures, early surgical correction is essential to prevent neurologic sequelae and to provide the best cosmetic result [Sgouros et al., 1996b]. Wide linear craniectomy to reopen the sutures is usually performed 1 to 3 months after birth and if possible always before 6 months of age [Boop et al., 1996b; Salkind et al., 1986]. A wide range of procedures have been attempted, ranging from partial morcellation to extensive calvarial remodeling, including total ablation of the cranial vault in some patients [Flores-Sarnat, 2002; Panchal and Uttchin, 2003; Posnick and Ruiz, 2000]. Absorbable plating systems, rather than
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
those that are titanium based, have been of significant benefit by ensuring rigid fixation and a better outcome [Panchal and Uttchin, 2003]. Endoscopically assisted (minimally invasive) craniosynostosis repair is being used as an alternative to traditional open craniosynostosis repair [Jimenez et al., 2002]. Advantages included decreased blood loss, operative time, and hospital stay, while providing esthetic results and safety comparable with those associated with traditional open methods of repair. Nevertheless, the difficulties inherent in endoscopic visualization may result in complications such as development of dural tears or leptomeningeal cysts [Aryan et al., 2004]. Distraction osteogenesis has been applied to the craniofacial skeleton, as well as the long bones of the extremities [Matsumoto et al., 2003]. This technique does not require bone grafting and allows correction of craniofacial deformities with less invasion. The distraction procedures can expand the overlying soft tissues simultaneously. Hydroxyapatite also is commonly used after cranial vault remodeling for osseous defects that have failed to ossify or to augment the temporal hollowing and minor asymmetry that may occur after cranial vault remodeling. Suture separation may need to be repeated if the suture reunites prematurely; repeat surgery is more likely in cases of multiple synostosis in which more extensive remodeling is necessary [McLaurin et al., 1989]. Patients with severe facial deformities, such as in Crouzon’s disease, may need total calvarial vault reconstruction [Burstein et al., 1994; McCarthy et al., 1990]. Major surgical advances involve an intracranial approach to correct the major craniofacial deformities, and a team approach to the management of such patients is beneficial [David et al., 1982; Marchac and Renier, 1982; Renier et al., 2000]. This technique attempts to change the entire facial structure by detaching the facial and orbital bones from the cranium and moving them into a more normal configuration. Patients with craniosynostosis that is secondary, occurring after ventriculoperi-toneal shunting for hydrocephalus, may require modifications in surgical management to maintain the contour and prevent recurrent collapse of the cranial vault [Shuster et al., 1995]. In some patients, craniosynostosis appears later in childhood with the development of midfacial hypoplasia and hypertelorism. The skull shape is normal at birth and the sutures are open in infancy, but later, multiple-suture craniosynostosis develops that requires surgery. Although the patients initially do not display manifestations of craniosynostosis, increased intracranial pressure frequently develops subsequently, which can have devastating consequences. In one series, a majority of such persons were diagnosed as having Crouzon’s syndrome, and most had FGFR2 mutations [Connolly et al., 2004].
Increased Intracranial Pressure Children with complex and to a lesser extent isolated forms of craniosynostosis may have raised intracranial pressure before surgery that remits postoperatively [Bristol et al., 2004; David et al., 1996; Panchal and Uttchin, 2003]. In one study, raised intracranial pressure was present in 28/53 patients with syndromic craniofacial dysostosis and in 20/83 nonsyndromic patients [Thompson et al., 1995]. Another report found papilledema in 12% of 122 children with
453
craniosynostosis [Tuite et al., 1996a]. In this study, papilledema was a specific (98%) indicator of raised intracranial pressure, but its sensitivity was age-dependent. It was 100% sensitive in children older than 8 years, but only 22% sensitive in younger children. A higher incidence of the classic “beaten copper” appearance on skull x-ray is found in those patients with increased intracranial pressure and craniosynostosis [Tuite et al., 1996b]. The cause of increased intracranial pressure in patients with craniosynostosis has been thought to be due to either decreased intracranial volume or impeded venous drainage. Premature fusion of skull sutures is assumed to restrict skull growth [Gault et al., 1992]. Obstruction of the sigmoid sinuses at the skull base resulting in venous sinus hypertension and increased intracranial pressure also has been reported [Saine-Rose et al., 1984]. Abnormal cerebrospinal fluid hydrodynamics occur in about 8% of patients with craniosynostosis and include progressive hydrocephalus, nonprogressive ventriculomegaly, and subarachnoid space dilation [Cinalli et al., 1998]. Hydrocephalus occurs much more frequently in patients with syndromic craniosynostosis (12%) than in those with isolated craniosynostosis (less than 1%). Patients with kleeblattschädel almost always have hydrocephalus. Patients with Crouzon’s disease also are more likely to have hydrocephalus than in other syndromes [Cinalli et al., 1998]. In one patient with Crouzon’s disease, hydrocephalus was thought to be due to increased intracranial venous pressure, secondary to bilateral jugular foraminal stenosis [Martinez Perez et al., 1996]. In Apert’s syndrome, nonprogressive ventriculomegaly without increased intracranial pressure occurs frequently. Patients with syndromic craniosynostosis are also likely to have venous sinus obstruction and/or chronic tonsillar herniation. Patients also require evaluation for anomalous intracranial venous drainage before corrective surgery [Anderson et al., 1997b]. Chronic tonsillar herniation is a common MRI finding in patients with Crouzon’s disease (73%), in contrast with patients with Apert’s syndrome (2%) [Cinalli et al., 1995]. This finding is not necessarily related to the presence of hydrocephalus and is believed to be due to the premature synostosis of the lambdoid suture in the first 24 months of age. Studies have suggested that the incidence of delayed, asymptomatic increases in intracranial pressure after initial cranioplasty in children with complex craniosynostosis is surprisingly high and ranges from 3% to 36% [Pollack et al., 1996; Siddiqi et al., 1995; Stavrou et al., 1997]. Reported findings include bulging fontanel, progressive frontal bone protrusion, intermittent headaches, irritability, vomiting, proptosis, papilledema, visual failure, optic atrophy, and progressive head enlargement. Repeat surgery to expand the cranial vault is necessary in these patients. In other patients, signs or symptoms of increased intracranial pressure may be clinically difficult to detect and require lumbar puncture and measurement of intracranial pressure [Campbell et al., 1995]. Prompt evaluation of neonates and young infants with suspected craniosynostosis offers the optimal choice of early intervention. Surgery results in substantial cosmetic improvement and prevents neurologic sequelae with minimal complications. Correction of complex malformations by correcting posterior skull defects may relieve pressure on
454
Perinatal Acquired and Congenital Neurologic Disorders / 19
anterior orbital and frontal structures and allow completion of the repair when the child is older [Sgouros et al., 1996a]. In some children, obstructive sleep apnea develops secondary to narrowing of the nasopharyngeal space, and surgical intervention to enlarge the nasopharyngeal space can reduce the severity of these symptoms [Edwards et al., 1992]. In some patients, skull-molding helmets can be used to correct abnormal skull shapes due to deformational plagiocephaly resulting from positional molding or due to craniosynostosis [Kane et al., 1996; Strohecker, 1996]. Guidelines to an approach to intracranial pressure evaluation and management in children with craniosynostosis have been suggested [Cohen and Persing, 1998; Mouradian, 1998]. In the absence of definitive data on the incidence of intracranial hypertension and the long-term outlook for children with single-suture synostosis, for children with confirmed sagittal, lambdoid, and metopic synostosis whose parents have chosen surgical intervention, intracranial pressure monitoring is unlikely to improve clinical management. For children whose parents wish to avoid intracranial surgery, measurement of intracranial pressure may provide a means of assessing potentially damaging consequences of the synostosis. Children presenting later than 1 year of age, particularly those with developmental delay or other signs of increased intracranial pressure, may be referred for intracranial pressure monitoring. All children with confirmed synostosis should be monitored closely by a craniofacial surgeon, a pediatric neurosurgeon, a pediatric ophthalmologist, and a neurodevelopmental specialist for signs and symptoms of increased intracranial pressure, and treatment should be planned accordingly.
Cognitive Outcomes Reported cognitive outcomes in children with craniosynostosis are variable. Depending on the suture involved, rates of global delay range from 0% to a high of 66% [Kapp-Simon, 1998; Kapp-Simon et al., 1993; Lekovic et al., 2004]. This variability has been attributed to whether or not the child has a syndromic form of synostosis, the presence of associated medical problems and issues related to case ascertainment, and the different populations studied. A majority of studies of children with single suture craniosynostosis have normal development during the first year of life [Kapp-Simon, 1998], although other investigations have demonstrated cognitive delays before any surgical interventions were performed [Panchal et al., 2001]. Early studies did not reveal a correlation between neurocognitive outcomes and chronic raised intracranial pressure [Renier et al., 1982]. Other studies also have not found that surgery improves neurodevelopmental outcome [Kapp-Simon, 1998; Kapp-Simon et al., 1993]. Correlation between intelligence and severity of the craniofacial deformity was demonstrated in some studies [Kapp-Simon et al., 1993] but not in others [Turtas et al., 1993]. Postoperative head circumference and volume measurements are reduced in patients with mental impairment. Speech and language disorders also may occur in children with craniosynostosis. In one study of children with isolated sagittal synostosis, 37% of children had impairment, and in most it was moderate to severe in severity [Shipster et al., 2003]. Raised intracranial pressure, perinatal risk factors, otitis media, and previous surgery were not associated with speech
impairment. Other studies have found evidence of reading or spelling disorders and learning disability in 50% of children with isolated sagittal synostosis [Magge et al., 2002].
Other Complications Other complications that can occur in children with craniosynostosis include cerebral salt wasting syndrome, developing after cranial vault remodeling [Lee et al., 2004; Levine et al., 2001]. This may be confused with the syndrome of inappropriate antidiuretic hormone release (SIADH), but cerebral salt wasting syndrome is associated with increased urine output and increased urine sodium concentration and volume contraction. Obstructive sleep apnea also is common in syndromic craniosynostosis, and in one study it was suspected from questionnaire results in 53% of patients [Pijpers et al., 2004]. Visual failure caused by raised intracranial pressure in craniosynostosis also can develop [Stavrou et al., 1997]. In some patients, monitoring visualevoked potentials is helpful, because abnormalities may develop before the appearance of papilledema or other signs of increased intracranial pressure [Mursch et al., 1999]. Corneal ulcers also may occur in some forms of craniosynostosis (e.g., Apert’s syndrome) [Ueeck et al., 2001].
Klippel-Feil Syndrome Although not a congenital malformation of the skull, the Klippel-Feil syndrome is included here because the primary abnormality relates to bone development. The cardinal feature of Klippel-Feil syndrome is a decreased number and partial or complete fusion of the cervical vertebrae [Ulmer et al., 1993]. The anomaly is the result of failure of segmentation of cervical vertebrae and mesodermal somites before the fourth week of gestation. It is a heterogeneous disorder in terms of both its clinical expression and its genetic basis. Klippel-Feil syndrome most often occurs sporadically. It also can be inherited as an autosomal-dominant disorder with variable expression and reduced penetrance, as an autosomal recessive disorder, or as an X-linked disorder (as part of Wildervanck’s syndrome). The specific genes involved in causing Klippel-Feil syndrome have not yet been identified, but several candidate genes and genetic foci have been suggested. In one report, autosomal dominant inheritance cosegregated with a pericentric inversion involving chromosome 8 (q22.2-q23.3) [Clarke et al., 1995]. This gene has been labeled SGM1 (segmental-1) and is associated with vertebral fusions and vocal impairment [Clarke et al., 1996]. A balanced translocation between 5q11.2 and 17q23 has also been reported in at least one Klippel-Feil syndrome patient [Fukushima et al., 1995]. Lowry and associates [2001] described a family in which an abnormality in the FGFR3 gene was associated with coronal craniosynostosis, Klippel-Feil syndrome, and Sprengel’s shoulder. Another group of investigators [McGaughran et al., 2003] screened 63 Klippel-Feil syndrome patients for mutations in the PAX1 gene, which is implicated in vertebral segmentation defects in mice. These workers found that 6 of the patients had mutations in the coding region. They suggested that PAX1, alone or in conjunction with other genetic or environmental factors, plays a role in the development of Klippel-Feil syndrome.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
Clinical Characteristics The classic triad of Klippel-Feil syndrome is a short neck, limitation of neck motion, and a low occipital hairline. The head appears to sit directly on the shoulders, without an intervening neck. Head and neck movements are limited except for some flexion and extension. The scapulae are elevated or discrepant in size. Less than 50% of patients have all three cardinal features, and there are many other reported associated features. These include facial asymmetry often associated with torticollis, fused and anomalous ribs including cervical ribs, hemivertebra, scoliosis or kyphosis, platybasia, Sprengel’s deformity, myelodysplasia, Arnold-Chiari malformation, diastematomyelia, syringomyelia, and hydrocephalus. The average age at clinical presentation in one series of patients was 9 years, with neurologic symptoms seen in about 40% of patients [Baba et al., 1995; Guille et al., 1995]. Additional abnormalities include cardiopulmonary, urogenital, and gastrointestinal anomalies; congenital deafness; absent ulna; and absent vagina [McKusick, 1994]. MRI scanning and CT myelography most commonly reveal cervical spondylosis, disk herniation, cervical dysraphism, or Arnold-Chiari malformations [Ulmer et al., 1993]. Klippel-Feil syndrome occurs as part of the Wildervanck syndrome in association with congenital perceptive deafness, abducens palsy, and Duane’s syndrome (cervico-oculoacoustic syndrome) [Gupte et al., 1992]. Wildervanck’s syndrome is almost completely limited to females and may be responsible for at least 1% of deafness among females. Otologic defects have been reported in about one third of patients with Klippel-Feil syndrome and are caused either by dysplasia of the labyrinth, internal auditory canal, or middle and outer ear [Dubey and Ghosh, 1993]. Deafness is usually sensorineural or mixed and is rarely conductive in nature. Three types of cervical vertebral fusion have been described [Baba et al., 1995]. In type 1, massive fusion of many cervical and upper thoracic vertebrae into bony blocks occurs. In type 2, fusion at only one or two interspaces is present, although hemivertebrae or occipitoatlantal fusion may be present. In type 3, both cervical fusion and lower thoracic or lumbar fusion are seen. A fourth type associated with sacral agenesis has also been reported [Raas-Rothschild et al., 1988]. Clarke and associates [1998] introduced a new KlippelFeil syndrome classification that attempted to integrate the clinical phenotype with the mode of inheritance. Fusions involving C1 were described as KF1, in which severe associated anomalies are present and inheritance is recessive. In KF2, C2-3 fusion is dominant and is the most rostral; the mode of inheritance is dominant. In KF3, C2-3 or C3-4 fusion is most rostral and often is a single isolated fusion; reduced penetrance inheritance is characteristic. KF4 is Wildervanck’s syndrome with presumed X-linked dominant inheritance. With regard to the neurologic symptoms, weakness and atrophy of arm muscles may be profound. Paraplegia may result from bony impingement on the spinal cord. Sympathetic dysfunction also may be prominent. Mirror movements (synkinesias) of the extremities, particularly the arms and hands, may be subtle or so overt that they are disabling. These movements have been ascribed to abnormalities of pyramidal decussation [Farmer et al., 1990]. Obstructive sleep apnea, bradypnea, and stridor have been reported in Klippel-Feil syn-
455
drome patients in conjunction with the presence of hindbrain abnormalities [Rosen et al., 1993]. Patients with Klippel-Feil syndrome and hypermobility of the upper cervical segment are at risk for neurologic sequelae; those with alteration in motion of the lower cervical segment are predisposed to degenerative disease [Pizzutillo et al., 1994]. Another group of investigators found that the more numerous the occipito-C1 abnormalities, the more significant the neurologic risk [Rouvreau et al., 1998]. Occasionally, patients may present with an acute neurlogic syndrome (e.g., quadriplegia) after relatively minor neck trauma [Smith and Griffin, 1992].
Management Comprehensive evaluation of all patients with Klippel-Feil syndrome is indicated because of the varied possible associated anomalies. Appropriate radiologic imaging of the cervical spine is required to define the cervical abnormalities, and any potential for spinal cord or radicular compression. This may include MRI with lateral views in flexion and extension [Rouvreau et al., 1998]. Imaging of the thoracic and lumbosacral spine is needed to look for other spinal anomalies and to monitor for the development of scoliosis. Periodic neurologic examinations are necessary to assess for cranial nerve abnormalities, cervical radiculopathy or myelopathy, or symptoms of Chiari malformation or hydrocephalus. Cardiac evaluation, renal ultrasound, and audiologic testing are necessary due to possible associated problems in these systems [Tracy et al., 2004]. The precise nature of the cervical abnormality and other associated problems dictates the intervention for the particular patient. For some, modification of activity is all that is necessary; patients with progressive symptomatic segmental instability or neurologic compromise may require surgical stabilization (e.g., anterior or posterior arthrodeses or laminectomies). Neurosurgical treatment (posterior fossa decompression or ventricular shunting) may be indicated as may surgery for gastroesophageal reflux (fundoplication) [Baba et al., 1995; Guille et al., 1995; Johnson, 1992].
ABNORMALITIES OF OSSIFICATION: SCLEROSIS AND HYPEROSTOSIS Craniotubular Bone-Modeling Disorders These disorders (see Box 19-9) are caused by disequilibrium between the processes of bone formation and resorption that leads to defective modeling and remodeling of bone [Paterson, 1997]. Neurologic features often include cranial nerve deficits, brainstem compression, abnormal head shape, and elevated intracranial pressure [Stein et al., 1983]. Osteopetrosis is discussed as an example of these disorders, although distinct cellular and metabolic defects likely are responsible for each one.
Osteopetrosis Osteopetrosis, a disease of defective bone resorption, results in generalized bone sclerosis and fragility, constriction of cranial foramina, and bone marrow failure, which leads to anemia, thrombocytopenia, hepatosplenomegaly, and sus-
456
Perinatal Acquired and Congenital Neurologic Disorders / 19
ceptibility to infection [Kocher and Kasser, 2003]. Three clinically distinct forms of osteopetrosis are recognized— the infantile malignant autosomal-recessive form, the intermediate autosomal-recessive form, and the adult autosomaldominant form, which is characterized by sclerosis, predominantly involving the spine, the pelvis, and the skull base [Kocher and Kasser, 2003; Walpole et al., 1990]. The autosomal recessive, malignant infantile type is the only one with significant neurologic features. Carpal tunnel syndrome [Lachman, 1997] or syringomyelia [Sari and Demirci, 1996] may develop in patients with autosomaldominant osteopetrosis. An isolated case of severe neurologic involvement has been seen with the dominant form [Walpole et al., 1990].
Pathogenesis The basic defect in the process of endochondral ossification is impaired lysosomal function of osteoclasts and their precursor cells, monocytes. Bone formation by osteoblasts continues and becomes excessive without the dynamic remodeling and resorption of bone by the osteoclasts; thus, the marrow cavity becomes filled. The precursor monocytes also are defective, leading to susceptibility to infection. Localization of the gene for autosomal-dominant osteopetrosis to chromosomal region 1p21 has been reported [Van Hul et al., 1997]. Osteopetrosis may be due to intrinsic defects to either the osteoclast-monocyte lineage or the mesenchymal cells that constitute the microenvironment that supports osteoclast ontogeny and activation. Implicated factors include specific proto-oncogenes, growth factors, and immune regulators. In many patients, the disease is caused by defects in either the proton pump (the α3 subunit of vacuolar-type H+-ATPase, encoded by the gene variously termed ATP6i or TCIRG1) or the ClC-7 chloride channel (ClCN7 gene). These pumps are responsible for acidifying the bone surface beneath the osteoclast [Steward, 2003]. A subset of patients with the intermediate autosomal-recessive form has been characterized with carbonic anhydrase II isoenzyme deficiency [Borthwick et al., 2003]. Evidence of a defect in the gene for macrophage colony-stimulating factor (CSF1) in the osteopetrotic mouse (op/op) has been found [Yoshida et al., 1990]. Transplantation of normal bone marrow cells into the op/op mouse, however, has not resulted in resolution of the bone defect. In addition, no definite evidence indicates that a mutation in the CSF1 gene is responsible for osteopetrosis in humans [Orchard et al., 1992].
Clinical Characteristics Although the osteopetroses generally are thought of as bone diseases, the most serious consequences of these disorders are seen in the nervous system. Cranial nerves, blood vessels, and the spinal cord are compressed by either gradual occlusion or lack of growth of skull foramina [Steward, 2003]. The typical patient with osteopetrosis is an infant with poor vision, optic atrophy, anemia, hepatosplenomegaly, and immune dysfunction. The risk for developing visual or hematologic impairment in the first year of life is approximately 75%, and the probability of survival until the age of 6 years is approximately 30% [Gerritsen et al., 1994a]. Considerations in the differential diagnosis include
certain lysosomal storage diseases. Neurologic complications result from bleeding, infection, fractures, and encroachment on neural structures from overgrowth of the skull. Cranial nerves, the carotid arteries, and the jugular veins may be compressed by progressive obliteration of the cranial foramina. Typical neurologic symptoms and signs in infants include progressive blindness and deafness, anosmia, headaches, optic atrophy, proptosis, seizures, facial nerve paralysis, other cranial nerve palsies, macrocephaly with frontal and parietal bossing, hypotonia, spasticity, developmental delay, and sleep apnea [Ainsworth et al., 1993; Benecke, 1993; Carter et al., 1988; Steward, 2003]. Hypotonia results from CNS dysfunction; findings on electromyography and muscle histology are normal. Elevated intracranial pressure occurs secondary to hydrocephalus or pseudotumor cerebri, which may develop as a result of obstruction of venous drainage or intracranial hemorrhage [Rosman and Shands, 1978; Wu and Swaiman, 1982]. Visual impairment usually results from optic nerve compression. Some patients without evidence of optic nerve encroachment may have primary retinal degeneration with abnormalities on electroretinograms, primary optic nerve dysmyelination, or optic atrophy from increased intracranial pressure or compression of the retinal veins [Haines et al., 1988]. A neurodevelopmental follow-up study of 23 children with the severe autosomal recessive form of osteoporosis noted the following: (1) 8 patients were blind, 11 were visually impaired, and 4 had satisfactory vision; (2) 2 patients had hearing loss; (3) motor delay initially was mild and worsened to severe, followed by gradual improvement, so that by age 4 years, all but two children were ambulatory; and (4) language and intellectual function was variably impaired, with many patients having significant deficits [Charles and Key, 1998]. Useful diagnostic studies for osteopetrosis include skeletal radiography and bone biopsy. CT and MRI of the skull and brain and plain skull radiographs may demonstrate enlarged ventricles, cerebral atrophy, hydrocephalus, and thickened skull bones with narrow cranial foramina at the base of the skull [Cure et al., 2000; Herman and McAlister, 1991]. MRI also may demonstrate tonsillar herniation, proptosis, and dural venous sinus stenosis. Acquired cephaloceles can occur, and optic nerve atrophy and optic canal stenosis are present in a majority of patients. Middle ear fluid is present in greater than half of the patients. Petrous carotid canal and internal carotid or vertebral artery stenotic lesions in patients with malignant osteopetrosis with evidence of extramedullary hematopoiesis can be detected using CT scanning and MR angiography. Dandy-Walker syndrome and agenesis of the corpus callosum also have been associated with the severe autosomal-recessive form of osteopetrosis [Ben Hamouda et al., 2001]. Delayed myelination has been observed in some patients with developmental retardation. Prominent cerebrospinal fluid spaces over the frontal lobes may be present in normal patients [Elster et al., 1992]. Syringomyelia also may occur [Sari and Demirci, 1996]. Abnormal visual- and auditory-evoked potentials result from compression of optic and auditory nerves. Anemia, leukopenia, and thrombocytopenia secondary to marrow replacement by the thickened bone are common.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
A rare and poorly understood form of the neuronopathic osteopetrosis disease has been associated with infantile neuroaxonal dystrophy [Rees et al., 1995]. It causes rapid neurodegeneration and death within the first year. Although characterized by the finding of widespread axonal spheroids and accumulation of ceroid lipofuscin, the biochemical basis of this disease remains unknown [Steward, 2003]. In addition, a form of osteopetrosis associated with renal tubular acidosis has been described [Borthwick et al., 2003].
Management Management of patients with osteopetrosis requires a comprehensive approach to characteristic clinical problems including hematologic and metabolic abnormalities, fractures, deformity, back pain, bone pain, osteomyelitis, and neurologic sequelae [Kocher and Kasser, 2003]. Specific neurosurgical treatment should be considered early in the course of the disease, to prevent permanent sequelae. The possibility of elevated intracranial pressure should be investigated before any surgery. Progressive hydrocephalus can be managed with a shunting procedure; caution is advised in this decision because mild, nonprogressive hydrocephalus or ventricular enlargement from cerebral atrophy may occur in many patients and not require treatment. Patients should be evaluated for progressive loss of vision and hearing. Visual-evoked potentials are useful for monitoring the progression of optic nerve compromise, to determine the optimal timing and response to decompressive surgery. Neurosurgical procedures to unroof the optic foramina and decompress the encroached optic nerves can prevent further deterioration. In patients with either the recessive or the dominant forms of osteopetrosis, localized cervical or lumbar back pain may develop secondary to spondylolysis that usually can be managed with a lumbosacral corset or a thoracolumbosacral orthosis [Martin et al., 1997]. Until recently, congenital osteopetrosis was a fatal disease with progressive neurologic involvement. Complications from the bleeding diathesis and infection were the usual causes of death. Medical treatment of osteopetrosis is based on efforts to stimulate host osteoclasts or provide an alternative source of osteoclasts. Stimulation of host osteoclasts has been attempted with calcium restriction, calcitriol, steroids, parathyroid hormone, and interferon. Bone marrow transplantation has been used for infantile malignant osteopetrosis, with resultant cure [McMahon et al., 2001]. Because osteopetrosis likely represents a spectrum of underlying causative disorders resulting in osteoclast dysfunction, effective therapies most likely need to be individualized [Gerritsen et al., 1994b; Kocher and Kasser, 2003; Solh et al., 1995]. Bone marrow transplantation offers treatment when a suitable matched donor is available, with survival rates as high as 79% [Gerritsen et al., 1994b; Solh et al., 1995]. Neurologic deterioration may be halted, and some patients may experience improvement with respect to already existing neurologic abnormalities (usually vision); therefore, early diagnosis and referral are necessary to achieve the best neurologic outcome [Hwang et al., 2000]. Experimental treatment with calcitriol produces bone but not clinical improvement [Gerritsen et al., 1994b; Key et al., 1984]. Interferon-γ also has been used, with evidence to suggest neurologic
457
improvement [Charles and Key, 1998; Key et al., 1995b]. Cord blood transplantation in one case report resulted in bone resorption without normalization of neurologic findings [Locatelli et al., 1997]. The brain isoenzyme of creatine kinase (BB-CK) is elevated in children with osteopetrosis but not in other sclerosing bone disorders [Whyte et al., 1996]. The reasons for this elevation remain unclear. Assay of BB-CK in fetal blood could potentially be used for prenatal diagnosis of malignant osteopetrosis but requires further investigation.
Fibrous Dysplasia of Bone Fibrous dysplasia is a developmental disorder of bone that can manifest in a monostotic or polyostotic form. Primarily affecting adolescents and young adults, it accounts for 7% of benign bone tumors [Ippolito et al., 2003; Parekh et al., 2004]. Localized areas of bone are replaced by dense fibrous tissue, causing slowly progressive erosion, hyperostosis, bone deformity, and frequent fractures of long bones. Fibrous dysplasia has been associated with multiple endocrine and nonendocrine disorders, and with McCune-Albright syndrome and Mazabraud’s syndrome (i.e., fibrous dysplasia with intramuscular or juxtamuscular myxomas). Manifestations of fibrous dysplasia and the McCuneAlbright syndrome appear to be due to increased activity of tissues regulated by the accumulation of cyclic adenosine monophosphate. Overproduction of cyclic adenosine monophosphate is mediated by activating mutations of the alpha stimulatory guanine nucleotide-binding protein (Gs alpha) [Perdigao et al., 2004; Spiegel, 1997]. Specifically, upregulation of the Gs alpha protein appears to be due to missense mutations of the Gs alpha gene [Weinstein et al., 1991]. During maturation, precursor osteogenic cells form normal osteoblasts; this pattern of expression is retained in fibrous dysplasia. Fibrotic areas consist of an excess of cells with features of preosteogenic cells, whereas the lesional bone formed within fibrotic areas represents the output of mature but abnormal osteoblasts [Riminucci et al., 1997]. Osteoblasts involved with the de novo deposition of lesional bone in fibrous dysplasia produce a bone matrix enriched in certain anti-adhesion molecules and poor in the pro-adhesive molecules. These findings are in contrast with the high levels of proadhesive proteins found in normal de novo bone. Fibrous dysplasia may thus be considered a disease of cells in the osteogenic lineage that is triggered by the effects of excess cyclic adenosine monophosphate on bone cell function [Riminucci et al., 1997]. Increased cell proliferation and inappropriate cell differentiation result in overproduction of a disorganized fibrotic bone matrix [Marie et al., 1997]. The monostotic form involves only one bone in each patient, often a rib or the skull. The fronto-orbital regions, including the frontal, maxillary, and sphenoid bones, the anterior base of the skull, and the orbit, are most often affected. The polyostotic form—McCune-Albright syndrome—involves multiple bones in a similar manner but also includes endocrine and dermatologic manifestations. Skull and facial bones are involved in 10% to 25% of cases of monostotic fibrous dysplasia and in 50% of the polyostotic variety [Brown et al., 1995]. The three major radiographic classifications of fibrous dysplasia are pagetoid, sclerotic, and cystic. The monostotic
458
Perinatal Acquired and Congenital Neurologic Disorders / 19
form affects both genders equally; the polyostotic form is more common in females, particularly with endocrine manifestations. In one recent series, the ethmoid bones were most commonly involved (71%), followed by the sphenoid (43%), frontal (33%), maxilla (29%), temporal (24%), parietal (14%), and occipital (5%) bones, and the most common presenting features included atypical facial pain and headache, complaints referable to the sinuses, proptosis and diplopia, hearing loss, and facial numbness [Lustig et al., 2001]. Clinical features manifest between ages 5 and 15 years. Progressive facial, orbital, and skull deformity and asymmetry become apparent during skeletal growth; the bone deformity often stabilizes after completion of puberty. A hard scalp mass and local pain often are the chief complaints. Complications of the skull dysplasia include cosmetic deformity and compression of neural foramina, especially the optic foramina, producing progressive visual loss, proptosis, and extraocular muscle weakness [Seiff, 1997]. In some patients, the gradual development of a small posterior fossa due to fibrous dysplasia of the occipital bone, with consequent tonsillar herniation resulting in syringomyelia, has been noted [Chandy, 1999]. Fibrous dysplasia also may manifest with conductive hearing loss resulting from stenosis of the external auditory canal [Morrissey et al., 1997]. Sensorineural hearing loss usually has been attributed to involvement of the otic capsule. Less common, long-term complications include (1) malignant transformation of the dysplastic bone into osteosarcomas, fibrosarcomas, or chondrosarcomas and (2) hemorrhage into the dysplastic bone. Both cause a rapidly enlarging scalp mass and local pain [Beuerlein et al., 1997; Graf and Perret, 1980; Rodenberg et al., 1996]. The risk of malignant transformation, which carries with it a poor prognosis, is 0.5%, with a predilection for the craniofacial region, the polyostotic form, and male gender [Ruggieri et al., 1994]. Swelling, local pain, and progressive radiographic changes suggest malignant transformation. Rare complications include the development of intramuscular myxomas [Limouzy et al., 1996] and spinal involvement with paraparesis [Przybylski et al., 1996]. Spinal lesions and scoliosis also may occur in patients with polyostotic fibrous dysplasia [Leet et al., 2004]. On rare occasions, epilepsy also has been reported as an initial manifestation of the polyostotic form [Soler et al., 1999]. The diagnosis of fibrous dysplasia can be suspected from the presence of typical facial features and, in the polyostotic form, from the associated extraskeletal manifestations. Skull radiographs demonstrate characteristic hyperostotic areas with a ground-glass opaque appearance in combination with radiolucent cysts, usually in the frontal or parietal bones. The base of the skull, particularly the sphenoid, sella turcica, roof of the orbit, and frontal bones, demonstrates diffuse sclerosis and thickening. CT and MRI also demonstrate cortical bone destruction [Sener, 1997a; Yao et al., 1994]. The alkaline phosphatase level may be elevated, but plasma phosphorus and calcium concentrations are normal. Bone biopsy is necessary for diagnosis in uncertain cases to exlude tumor or osteomyelitis, particularly in the monostotic form without confirmatory extraskeletal manifestations [Andrisano et al., 1991]. Surgical treatment is indicated for patients with progressive compression of neural structures or rapidly growing or painful lesions suggesting late complications such
as malignant transformation or hemorrhage [Bibby and McFadzean, 1994; Jan et al., 1994; Papay et al., 1995; Posnick et al., 1993]. Although encasement of the optic canal in fibrous dysplasia causes narrowing of the canal, subsequent visual loss is not invariable, and prophylactic decompression of the optic nerve may not necessarily be indicated on the basis of the presence of fibrous dysplasia on diagnostic images alone [Lee et al., 2002]. Local radiation is of no value as a primary treatment. Cosmetic surgery is best considered after the completion of puberty and skeletal maturation. In addition to orthopedic treatment, administration of bisphosphonate pamidronate intravenously every 6 months has been reported to reduce the severity of bone pain, the rate of bone turnover assessed by biochemical markers, and the size of the radiologic lesions [Chapurlat et al., 1997; Kos et al., 2004; Schoenau and Rauch, 2002]. Aminobisphosphonate, which is available in the United States, also has been used successfully [Weinstein, 1997].
MCCUNE-ALBRIGHT SYNDROME The McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia, pigmentary patches of the skin (e.g., café au lait spots), and endocrinologic abnormalities, including precocious puberty, short stature, thyrotoxicosis, pituitary gigantism, and Cushing’s syndrome [de Sanctis et al., 1999; Hannon et al., 2003]. Asymmetric involvement of the skull and facial bones is a common and prominent feature of McCune-Albright syndrome. Deafness and blindness result from involvement of the cranial foramina [Bocca et al., 1998]. Pathologic fractures, bone deformities, and pseudoarthrosis are frequent presenting manifestations. A particularly characteristic area of bone involvement is the proximal femur, which results in the “shepherd’s crook” deformity. Severe craniofacial hyperostosis can occur [Viljoen et al., 1988]. Skin involvement consists primarily of large café au lait spots with irregular margins (i.e., “coast of Maine” configuration) as compared with the more regularly outlined “coast of California” lesions characteristic of neurofibromatosis. The café au lait spots usually are unilateral and on the same side as the bone lesions and usually do not cross the midline; the nape of the neck is a common site of involvement. Endocrine manifestations are common in McCuneAlbright syndrome [Hannon et al., 2003]. Precocious puberty, usually manifesting with vaginal bleeding, occurs in more than 50% of females and is the most common endocrinopathy [DiMeglio and Pescovitz, 1997]. Hyperthyroidism occurs in approximately 20% to 40% of patients. Gigantism (excessive growth hormone secretion), hyperprolactinemia, hyperadrenocorticism, and gynecomastia also occur. Nonendocrine manifestations of McCune-Albright syndrome include hypophosphatemia, hepatobiliary dysfunction, splenic and pancreatic hyperplasia, pancreatitis, intestinal polyps, abnormal cardiac muscle, and sudden death [DiMeglio and Pescovitz, 1997]. McCune-Albright syndrome should not be confused with Albright’s hereditary osteodystrophy, an autosomal dominant disorder also associated with defects in G proteins [Spiegel, 1997]. Patients with Albright’s hereditary osteodystrophy have characteristic physical features (short stature, obesity, round face, brachydactyly) and variable biochemical
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
changes (pseudohypoparathyroidism or pseudopseudohypoparathyroidism). Most patients with Albright’s hereditary osteodystrophy have decreased activity of the guanine nucleotide-binding protein (Gs protein) that stimulates cyclic adenosine monophosphate [Phelan et al., 1995]. Loss of G alpha subunit function leads to tissue resistance to multiple hormones whose receptors couple to the G alpha subunit [Ringel et al., 1996]. Pamidronate treatment has been successfully used in patients with McCune-Albright syndrome [Matarazzo et al., 2002].
ABNORMALITIES OF OSSIFICATION: LYTIC LESIONS Lacunar Skull Lacunar skull is characterized by defects in the inner table of the cranial vault (membranous bone). This condition occurs in newborns and is associated with spina bifida and other major structural anomalies of the CNS and in some metabolic disorders [Cole, 2000]. Lacunar skull is not caused by elevated intracranial pressure and usually resolves over 6 months. Skull radiographs demonstrate a mixed pattern of decreased densities described as “soap bubble” rarefactions. Sinus pericranii is a parieto-occipital vascular scalp mass that is fluctuant and swells with elevated venous pressure and occurs with crying and the supine position [Wen et al., 2004]. Thus, the diagnosis can be confirmed during the physical examination. This lesion is a persistent connection between an intracranial dural sinus, usually the sagittal sinus, and the venous system of the scalp. Spontaneous partial thrombosis can occur; MRI and MR venography are particularly useful in detection of sinus pericranii and its complications [Azusawa et al., 2000; Carpenter et al., 2004]. Persistent emissary veins constitute a similar lesion but involve intracranial veins instead of a dural sinus. Both types erode the skull; the radiographic pattern may simulate parietal foramina, which constitutes a normal variation. Surgical treatment is elective and may not be necessary. In extensive or progressive lesions, treatment includes ligation of the anomalous connection. Traumatic scalp hemorrhage is a potential complication in untreated patients.
Cleidocranial Dysplasia Cleidocranial dysplasia is a congenital disorder of bone development characterized by persistently open or delayed closure of cranial sutures and wormian bones, hypoplastic and/or aplastic clavicles, wide pubic symphysis, dental anomalies, and short stature [Cooper et al., 2001; Mundlos, 1999]. Dental anomalies and delayed skeletal development are prominent features. Delayed ossification of membranous bones affects the frontal, parietal, and occipital bones. Cleidocranial dysplasia is inherited as an autosomal dominant trait, and the human CBFA1 gene has been identified as the responsible gene [Winer et al., 2003]. Autosomal-recessive inheritance also occurs [McKusick, 1994]. Chromosomal translocations, deletions, insertions, nonsense and splice-site mutations, as well as missense mutations of the RUNX2 gene which is an osteoblast transcription factor have been described in patients with cleidocranial
459
dysplasia [Otto et al., 2002; Yoshida et al., 2003]. The runt box (Runx) is a highly conserved DNA-binding and protein-protein interaction domain that defines a family of heterodimeric transcription factors with essential roles in development [Coffman, 2003]. Runx proteins have essential functions in cell proliferation and differentiation, and in mammals they are both proto-oncogenes and tumor suppressors. Whereas Runx1 is essential for mature hematopoiesis and Runx2 for osteochondrogenesis, Runx3 has a function in the nervous system [Otto et al., 2003]. Physical examination reveals a broad head with a decreased anteroposterior diameter and frontal bossing. The sagittal suture and the large anterior and posterior fontanels remain open. Spasticity and mental retardation may occur. The shoulders can be closely adducted. Absence of the clavicles may result in injury to the unprotected brachial plexus and atrophy of the muscles of the hand. Short stature and multiple unerupted supernumerary teeth are common [Seow and Hertzberg, 1995]. Associated anomalies may include syringomyelia, partial agenesis of the corpus callosum, scoliosis, spina bifida, cervical ribs, and pelvic deformities [Vari et al., 1996]. Skull radiography demonstrates defective ossification, wide sutures, and multiple wormian bones; the chest x-ray examination reveals hypoplastic or absent clavicles. The only treatment available for cleidocranial dysplasia is to protect the brachial plexus from pressure injury to prevent pain and muscular atrophy. Hearing loss, as a presenting symptom of cleidocranial dysplasia, also has been reported [Dhooge et al., 2001]. In some patients with cleidocranial dysplasia, unilateral sensorineural hearing loss and ataxia has been a prominent feature [Scherer et al., 2001]. The combination of skull defects in the form of enlarged parietal foramina and deficient ossification of the clavicles is known as parietal foramina with cleidocranial dysplasia. It is considered to be distinct from classic cleidocranial dysplasia [Garcia-Minaur et al., 2003].
ABNORMALITIES OF THE CRANIAL BASE Achondroplasia Achondroplasia is a common form of human dwarfism with characteristically rhizomelic shortening of extremities, relative macrocephaly, short stature, dysmorphic features, congenital skeletal abnormalities, and neurologic involvement. It is transmitted in an autosomally dominant manner and about 80% of the cases result from sporadic mutations without a positive family history [Jones, 1997; McKusick, 1994; Su et al., 2004; Tanaka, 1997]. It is the most common skeletal dysplasia and occurs in about 1 in 15,000 to 40,000 live births. The basic defect is in endochondral bone formation, which explains the impaired growth of the base of the skull (endochondral bone), with a compensatory increase in growth of the normal membranous bones of the cranial vault. Achondroplasia is caused by mutation in the FGFR3 gene, which maps to chromosomal locus 4p16.3 [Rousseau et al., 1994; Shiang et al., 1994]. In 97% of the patients, a glycine-to-arginine substitution occurs at position 380 within the FGFR3 transmembrane domain, leading to receptor
460
Perinatal Acquired and Congenital Neurologic Disorders / 19
overactivation. This FGFR tyrosine kinase is expressed by chondrocytes in the growth plate of developing long bones and plays a crucial role in bone growth [Aviezer et al., 2003]. FGFR3 is expressed in developing bone, cochlea, brain, and spinal cord [Colvin et al., 1996]. Mutations in the FGFR3 gene enable abnormal cartilage growth plate differentiation and insufficient bone development [Su et al., 2004]. Prenatal detection for achondroplasia is available [Li et al., 2004]. The relation between the presence of brain FGFR3 transcripts and the increased occurrence of megalencephaly in patients with achondroplasia is being investigated. Prenatal screening for achondroplasia is available using polymerase chain reaction and chorionic villus sampling [Bellus et al., 1994; Shiang et al., 1994]. Screening has been recommended for pregnancies at risk for homozygous achondroplastic fetuses [Shiang et al., 1994].
Clinical Characteristics The diagnosis usually is readily apparent and is based on the physical examination findings of short-limbed dwarfism, prominent forehead, mid-facial hypoplasia, macrocephaly, exaggerated lumbar lordosis, limitation of elbow extension, genu varum, and a trident hand [Hall, 1988]. Although achondroplasia is an autosomal-dominant disorder, most cases (80%) represent a new mutation without a known family history. Skeletal radiographs demonstrate early fusion of the spheno-occipital synchondrosis at the base of the skull, short tubular bones, J-shaped sella turcica, and anterior beaking of the lumbar vertebrae. Symptoms and signs include dysphagia, poor head control, apnea, cyanotic episodes, hypotonia, delayed motor milestones, and weakness. Progressive obesity is a major problem and aggravates the morbidity associated with lumbar stenosis, joint problems, and early cardiovascular mortality. Most patients have normal intelligence and can lead a normal life, although some have mild deficits in visualspatial tasks or mild mental retardation associated with other neurologic or respiratory complications [Cohen et al., 1967; Hecht et al., 1991; Thompson et al., 1999]. Neurologic symptoms occur in approximately 20% to 47% of patients [Haga, 2004; Ruiz Garcia et al., 1997]. Neurologic and skeletal abnormalities include quadriparesis, paraplegia, macrocephaly, brachycephaly, hydrocephalus, true megalencephaly, platybasia, basilar impression, small foramen magnum, midfacial hypoplasia, lumbar lordosis, kyphosis, syringomyelia, diastematomyelia, Arnold-Chiari malformation, and stenosis of the spinal canal [Jones, 1997; Yamada et al., 1981; Yundt et al., 1996]. Conductive hearing loss is common and secondary to frequent otitis media. Temporal bone morphologic changes described in patients with achondroplasia (narrowing of the skull base, “towering” petrous ridges, abnormal orientation of inner and middle ear structures) do not appear to correlate with the degree of sensorineural or conductive hearing loss [Shohat et al., 1993]. Infants with achondroplasia are at risk for apnea and unexpected sudden death resulting from brainstem dysfunction and constriction of the cranial base [Bland and Emery, 1982; Pauli et al., 1984]. Polysomnographic studies during sleep frequently are abnormal [Zucconi and Bruni, 2001]. Abnormalities include upper airway obstruction with
obstructive apnea, central apnea, and abnormal electromyographic activity of accessory muscles of respiration. Correlation between somatosensory-evoked response abnormalities or foramen magnum size and polysomnographic abnormalities has not been observed [Waters et al., 1995]. Trigeminal neuralgia [Takada et al., 2001] and facial palsy [Cerqueiro-Mosquera et al., 2001] also may occur. Progressive neurologic deterioration involves brainstem, spinal cord, or nerve root compression and hydrocephalus secondary to spinal canal stenosis, vertebral subluxation, and impaired growth of the base of the skull (cartilaginous bone), which has a small deformed foramen magnum [Hamamci et al., 1993; Mueller et al., 1977; Wieting and Krach, 1994]. Cervicomedullary junction compression is a prominent finding in some patients and can cause pain, ataxia, incontinence, apnea, and respiratory arrest. One of the signs can be progressive quadriparesis, which can be a presenting symptom and may be caused by a vascular lesion, as well as by cord compression. Also, nerve root compression in the neural foramina can cause symptoms and signs in the limbs [Gordon, 2000; Pauli et al., 1995; Ryken and Menezes, 1994]. Stenosis of the spinal canal results from increased endochondral ossification with premature synostosis of the ossification centers of the vertebral body and the posterior arch, with thickening of the lamina, shortening of the pedicles, and reduced height of the vertebral bodies [Hamamci et al., 1993]. Prolapsed intervertebral disks, osteophytes, and progressive thoracolumbar kyphosis also contribute to the narrowing of the spinal canal. For patients with craniospinal junction compression, symptoms and treatment are similar to those for patients with basilar impression. Cauda equina compression resulting from lumbar stenosis may cause leg pain with exercise. Hydrocephalus, a narrow foramen magnum, spinal deformity, and spinal canal stenosis can cause neurologic problems leading to disabilities in locomotion, communication, and learning. Malfunctions of the otolaryngeal system such as otitis media, upper respiratory obstruction, deafness, speech delay, and malocclusion are interrelated and also can lead to disabilities in communication and learning [Haga, 2004]. Hydrocephalus likely is due to stenosis, compression of the fourth ventricle or medullary foramina, and increased intracranial venous pressure from bilateral jugular venous compression or stenosis [Erdincler et al., 1997; Gordon, 2000; Pierre-Kahn et al., 1980]. The development of hydrocephalus, which occurs in about 15% of patients, can be monitored more effectively by using head circumference charts normalized for children with achondroplasia and by performing cranial ultrasound examinations in infants [Horton et al., 1978]. Apart from the treatment for hydrocephalus, the most important decision often is the question of whether to surgically correct the cervical medullary compression [Ho et al., 2004]. Risk factors such as brisk reflexes, small foramen magnum, or central hypopnea can be an indication for surgery, but timing can be difficult, because the cord compression can resolve spontaneously [Gordon, 2000]. Pseudotumor cerebri may occur in some patients, perhaps as a result of obstruction of venous drainage [Rosman and Shands, 1978]. Using MRI, dynamic changes in brain morphometry and in cerebrospinal fluid dynamics in children with achondroplasia have been described [Bruhl et al., 2001; DiMario
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
et al., 1995]. A rostral displacement of the brainstem and gradual compression of the frontal lobes resulting from enlargement of the ventricles are the most significant features. These changes occur in association with an increase in venous sinus distention and suggest that hydrocephalus in these patients may be related to chronic hydrostatic pressure changes. Interruption of cerebrospinal fluid flow due to narrowing of the craniocervical junction also has been demonstrated; this finding may be helpful in determining whether surgical decompression is warranted [Bruhl et al., 2001].
Management Recommendations for the management of achondroplasia previously have been reviewed [Horton and Hecht, 1993; Nicoletti et al., 1988]. Management of neurologic complications begins with careful and regular clinical assessment, especially in searching for symptoms and signs of elevated intracranial pressure; hearing loss; or brainstem, spinal cord, and nerve root compression. Serial measurements of growth and head circumference using growth curves standardized for achondroplasia are important. Many patients have enlarged ventricles, possibly representing atrophy or nonprogressive arrested hydrocephalus, which does not require specific treatment. Shunting procedures should be considered only in patients with evidence of progressive ventriculomegaly and in those with symptoms of elevated intracranial pressure associated with ventriculomegaly. Serial CT, MRI, somatosensory-evoked potentials, and polysomnography are important in the follow-up management of these patients. Surgical enlargement of the foramen magnum in patients with severe stenosis needs to be considered. The diagnosis of pseudotumor cerebri should be considered in symptomatic patients without enlarged ventricles; medical management is indicated. The large head of the achondroplastic fetus creates an increased risk of intracranial bleeding during delivery. Obstructive sleep apnea in infants and abnormal respiratory function require early recognition and management [Nelson et al., 1988]. Patients with achondroplasia are also at greater risk for sudden unexpected death in the first year of life presumably because of cervicomedullary junction compression [Pauli et al., 1995]. Lower limb hyperreflexia, central apnea or hypopnea detected with polysomnography, and reduced foramen magnum measurements are more common in those patients who develop symptoms of cervicomedullary compression [Pauli et al., 1995]. Because of this risk, early evaluation with MRI and consideration for early surgical intervention in those patients with cervicomedullary compression has been recommended [Keiper et al, 1999; Pauli et al., 1995; Yamada et al., 1996]. In some patients, papilledema secondary to increased intracranial pressure may become intractable and result in optic atrophy. Treatment with nerve unsheathing and shunting is required [Landau and Gloor, 1994]. Evaluation of progressive spinal cord and nerve root involvement includes spinal radiography, electromyography, MRI, and CT [Hamamci et al., 1993; Thomas et al., 1988; Wang et al., 1987]. Somatosensory-evoked potentials may provide a noninvasive method to monitor spinal cord function sequentially in these high-risk patients [Boor et al., 1999]. Lumbar puncture should be performed only after the absence of significant hydrocephalus is documented and the
461
risks and benefits of the procedure are considered. Patients with progressive paraparesis; brainstem, spinal cord, or nerve root compression; or bowel and bladder dysfunction need immediate evaluation and possible decompressive laminectomy or suboccipital decompression [Nelson et al., 1988; Pauli et al., 1995; Reid et al., 1987; Ryken and Menezes, 1994]. Spinal cord infarction secondary to spinal stenosis may also occur [Wieting and Krach, 1994]. Spinal stenosis, which typically manifests in early adulthood, usually requires lumbar laminectomy. Recombinant human growth hormone has been used in children with achondroplasia, but the clinical indications, long-term effects, and duration of treatment require continued evaluation [Shohat et al., 1996; Stamoyannou et al., 1997]. Careful monitoring and control of weight to within 1 standard deviation of the mean weight-for-height curves also have been recommended [Hunter et al., 1996]. Waters and colleagues [1995] studied the results of treatment of obstructive sleep apnea in achondroplasia. Treatment included adenotonsillectomy, weight loss, and nasal mask continuous positive airway pressure. Patients with achondroplasia frequently require orthopedic intervention for spinal deformities and for limb lengthening [Ain et al., 2004; Aldegheri et al., 2001] and tethered cord release [Archibeck et al., 1997].
Basilar Impression Basilar impression (platybasia) is a congenital skeletal malformation that combines deformity of the osseous structures of the base of the skull with invagination of the foramen magnum and upper cervical spine into the posterior fossa [Bassi et al., 1992; Sawin and Menezes, 1997]. The foramen magnum is small and deformed. The floor of the posterior fossa and the odontoid process are displaced upward, further narrowing the foramen magnum and compressing the medulla and upper cervical spinal cord [McLaurin et al., 1989]. Metabolic bone disease such as osteomalacia, osteogenesis imperfecta, congenital hypothyroidism, rickets, and Paget’s disease may result in acquired basilar impression. The congenital condition is inherited as an autosomal-dominant trait with variable expression [McKusick, 1994].
Clinical Characteristics Neurologic symptoms most often begin after age 10 years. Neck stiffness, progressive spasticity and weakness of the legs, occipital headaches, and difficulty in walking are common complaints. Basilar impression should be considered in patients with progressive cerebellar ataxia or spastic paraparesis and brainstem or cervical cord syndromes, which might be mistaken for multiple sclerosis, spinal cord tumors, Arnold-Chiari malformation, and syringomyelia. Basilar impression may be associated with the Arnold-Chiari malformation and aqueductal stenosis; in such instances, hydrocephalus may be a feature. The progressive symptoms are attributed to pressure on the medulla and upper cervical spinal cord, similar to that in other craniocervical junction defects. Interference with the local blood supply and direct compression of neural structures have been postulated as pathogenic mechanisms. Physical examination reveals a short neck, low hairline, painful torticollis, restricted neck motion, and a loss of
462
Perinatal Acquired and Congenital Neurologic Disorders / 19
TABLE 19-25 Clinical Features of Osteogenesis Imperfecta Subtypes
From Steiner RD, Pepin, MG, Byers, PH. Osteogenesis imperfecta. See http://genetests.org and the review under “Osteogenesis Imperfecta”, 2005.
the normal cervical spine lordosis. Neurologic findings may include downbeat or periodic alternating nystagmus, fixed or intermittent cranial nerve impairment, bilateral corticospinal tract signs, ataxia, weakness, and sensory loss in the hands [Burrows, 1981]. The diagnosis is confirmed by a lateral radiograph of the skull. The odontoid process extends above a line drawn from the hard palate to the posterior edge of the foramen magnum (Chamberlain’s line). MRI and CT clearly define the existence of neural compression and should replace myelography [Koenigsberg et al., 2005].
Management Surgical decompression of the posterior fossa and the upper cervical cord is the treatment for symptomatic patients with congenital basilar impression [Harkey et al., 1990; McLaurin et al., 1989; Sawin and Menezes, 1997; Tuite et al., 1996b]. Decompressive surgery should be avoided in children with acquired basilar impression resulting from a metabolic bone disease because surgery may worsen the deformity.
Osteogenesis Imperfecta Osteogenesis imperfecta is a group of hereditary disorders of collagen manifested by bone fragility, fractures with minimal or absent trauma, short stature, dentinogenesis
imperfecta, blue sclerae, and postpubertal hearing loss [Rauch and Glorieux, 2004; Steiner et al., 2005]. Laxity of joints and skin and cardiovascular disease also may be features, depending on the type of osteogenesis imperfecta [Byers, 1993; Marini and Gerber, 1997; Tosi, 1997]. The clinical features of osteogenesis imperfecta represent a continuum ranging from perinatal lethality to a presentation with severe skeletal deformities, mobility impairments, and very short stature to a nearly asymptomatic presentation associated with a mild predisposition to fractures, normal stature, and normal lifespan. Fractures can occur in any bone but are most common in the extremities. Osteogenesis imperfecta is characterized by gray or brown teeth that may appear translucent and that wear down and break easily. Before the molecular basis of osteogenesis imperfecta was understood, this condition was classified into four types on the basis of mode of inheritance, clinical presentation, and radiographic findings. With detailed radiographic and bone morphologic studies and molecular genetic analyses, the classification has expanded to seven types (Table 19-25) [Steiner et al., 2005]. Osteogenesis imperfecta types I to V are inherited in an autosomal-dominant manner. Osteogenesis imperfecta type VII is inherited in an autosomal recessive manner, and the mode of inheritance of osteogenesis imperfecta type VI is not yet certain. The four well-recognized types of osteogenesis imperfecta are a dominant form with blue sclerae; a perinatal lethal form; a progressive deforming form
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
with normal sclerae; and a dominant form with normal sclerae [Byers, 1993]. Joint motion, muscle strength, and functional ability vary, depending on the type of osteogenesis imperfecta present [Engelbert et al., 1997; Rauch and Glorieux, 2004; Wilkinson et al., 1997]. Type I patients characteristically have normal strength and generalized hypermobility of the joints without decreased joint motion. In type III patients, the lower and, to a lesser extent, the upper extremities have weak musculature and severe deformities, whereas in type IV patients, proximal muscles are weaker and the upper and lower extremities are equally affected. Bruck’s syndrome is a recessively inherited phenotypic disorder featuring the unusual combination of skeletal changes resembling osteogenesis imperfecta with congenital contractures of the large joints [Ha-Vinh et al., 2004]. The gene for this rare disorder has been localized to chromosomal region 17p12, and the underlying molecular defect is a deficiency of bone-specific telopeptide lysyl hydroxylase, which results in aberrant cross-linking of bone collagen. Molecular defects of type 1 collagen are the major cause of osteogenesis imperfecta types I to IV [Cole, 1997]. Osteogenesis imperfecta types V to VII are not due to COL1A mutations, and the defects for these three forms of osteogenesis imperfecta are not yet well established. For types I to IV, the proportion of cases caused by a de novo mutation in either COL1A1 or COL1A2 varies according to the severity of disease: Approximately 60% of persons with mild osteogenesis imperfecta have de novo mutations; virtually 100% of persons with lethal (type II) osteogenesis imperfecta and a smaller proportion of those with osteogenesis imperfecta type II have a de novo mutation. Whereas the milder forms are due to quantitative abnormalities of type 1 collagen, the more severe forms are due to both quantitative and qualitative type 1 collagen abnormalities. The mutant type 1 collagen molecules are susceptible to degradation with loss of normal and mutant collagen chains that severely impair the formation of the extracellular matrix and cause an abnormal architecture of dermis and bone. Prenatal diagnosis is available using analysis of collagen synthesized by cells cultured from chorionic villus biopsies or direct mutation identification or analysis of polymorphic restriction sites in the COL1A1 gene of type 1 collagen [Nuytinck et al., 1998; Pepin et al., 1997]. Treatment includes cesarean birth, if prenatal diagnosis is known, and immobilization of the neck postnatally [Pauli and Gilbert, 1986]. The value of surgery later in life is uncertain, although recent reports indicate clinical improvement in patients who have an associated Arnold-Chiari malformation or basilar impression [Harkey et al., 1990; Tominaga et al., 1991]. Extremity deformities also can be surgically corrected [Luhmann et al., 1998]. Because of the high incidence of progressive hearing loss, regular hearing evaluations after adolescence are recommended. Defective skull ossification, fractures, and neurologic complications develop in infants with the more severe and often lethal types II and III. Neurologic complications include intracranial hemorrhage [Sayre et al., 1987], basilar impression, upper cervical cord compression, hydrocephalus, and macrocephaly [Hayes et al., 1999; Sawin and Menezes, 1997], which may lead to respiratory insufficiency and death. Bone mineral density is decreased in osteogenesis imperfecta, especially of the lumbar spine [Reinus et
463
al., 1998]. Pulmonary hypoplasia and chest wall constriction also may produce respiratory compromise. Conductive or mixed-type hearing loss occurs in about 50% of families, beginning in late childhood [Imani et al., 2003] or adolescence and progressing over time to profound deafness, tinnitus, and vertigo [Garretsen et al., 1997]. Reflex sympathetic dystrophy syndrome also may occur [Neri et al., 1997]. Deformities of the upper limbs have been reported in 37.1% of patients with osteogenesis imperfecta, with many showing significant functional impairments [Amako et al., 2004]. Other studies examining the natural history of osteogenesis imperfecta have found that total joint range of motion decreases significantly over time, especially in the lower extremities [Engelbert et al., 2004]. Although no significant changes in total muscle strength were found in this study, an increase in self-care needs and a decrease in mobility were reported. In addition to surgery, specific occupational and physical therapy programs are integral parts of the treatment of patients with osteogenesis imperfecta [Zeitlin et al., 2003]. Osteogenesis imperfecta type II has been shown to be associated with neuropathologic alterations, specifically perivenous microcalcifications, and impaired neuroblast migration. A recent study of nine osteogenesis imperfecta patients, a majority of whom had type II osteogenesis imperfecta, found hippocampal malrotation, agyria, abnormal neuronal lamination, migrational defects, diffuse hemorrhage, periventricular leukomalacia and calcifications, and white matter gliosis. These findings were interpreted as supporting the contention that collagen mutations might negatively impact CNS development [Emery et al., 1999]. Cerebrovascular abnormalities have been described in patients with osteogenesis imperfecta, presumably caused by the vascular fragility resulting from the collagen abnormality. These have included a cerebrovasculopathy of largecaliber intracranial vessels manifested by stenosis, thrombosis, and occlusion and a moya-moya pattern [Albayram et al., 2003]. Carotid and vertebral artery dissections also have been reported [Rouviere et al., 2004; Zuccoli et al., 2002]. Bisphosphonate treatment for moderate-to-severe forms of osteogenesis imperfecta also is now recommended [Licata, 2005]. Cyclic intravenous or oral administration of dimethylaminohydroxypropylidene bisphosphonate (pamidronate) in children with type I or III osteogenesis imperfecta has resulted in increased bone density and reductions in the frequency of new fractures [Astrom and Soderhall, 1998; Bembi et al., 1997; Fujiwara et al., 1998; Landsmeer-Beker et al., 1997]. Bisphosphonates were selected because of their ability to inhibit osteoclastic bone resorption and to increase bone density [Shaw, 1997]. At present, however, the best treatment regimen and the long-term outcomes of bisphosphonate therapy are unknown. Although this treatment does not constitute a cure, it constitutes a potentially beneficial adjunct to physiotherapy, rehabilitation, and orthopedic care. Gene-based therapy at present remains in the early stages of preclinical research [Niyibizi et al., 2004; Rauch and Glorieux, 2004]. Bisphosphonates usually are given intravenously, although oral forms have been tried, with no demonstrable decrease in fracture incidence compared with that in control subjects [Dimeglio et al., 2005]. When a child presents with one or more unexplained or recurrent fractures, nonaccidental trauma also must be considered [Chapman and Hall, 1997]. Conversely, osteo-
464
Perinatal Acquired and Congenital Neurologic Disorders / 19
TABLE 19-26 Selected Common Cleft Lip and Palate Disorders Associated with Major Neurologic Manifestations and Developmental Delay
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
465
TABLE 19-26, cont’d Selected Common Cleft Lip and Palate Disorders Associated with Major Neurologic Manifestations and Developmental Delay
466
Perinatal Acquired and Congenital Neurologic Disorders / 19
TABLE 19-26, cont’d Selected Common Cleft Lip and Palate Disorders Associated with Major Neurologic Manifestations and Developmental Delay
From Steiner RD, Pepin MG, Byers PH. (Updated 1/28/05). Osteogenesis imperfecta. In: GeneReviews at GeneTests: Medical Genetics Information Resource (database online). Copyright, University of Washington, Seattle. 1997-2005. Available at http://www.genetests.org. Accessed 5/4/05.
genesis imperfecta could be mistaken for child abuse [Kruse et al., 1997]. Collagen analysis to exclude milder forms of osteogenesis imperfecta, especially type IV, is recommended only in cases in which the diagnosis of osteogenesis imperfecta remains in doubt [Ablin and Sane, 1997]. Cases in infancy of bilateral chronic subdural hematoma as the initial presentation of osteogenesis imperfecta type I have been reported and were considered to be due to impaired bone calcification, vascular fragility, and permanent friction between multiple bone fragments of the skull, although nonaccidental trauma could not be eliminated as a diagnostic possibility [Groninger et al., 2005]. Retinal hemorrhages in addition to subdural hematomas also have been reported in patients with type I osteogenesis imperfecta after minor trauma [Ganesh et al., 2004]. In a recent study using cultured fibroblasts from 262 children in whom nonaccidental trauma was suspected, 11 had alterations consistent with the diagnosis of osteogenesis imperfecta; in 11 others, the diagnosis could not be excluded [Marlowe et al., 2002]. Referring physicians correctly identified children with osteogenesis imperfecta in only 6 of the 11 instances and did not identify osteogenesis imperfecta by examination in 3. The authors of this study suggested that in view of the inability to identify all children with osteogenesis imperfecta by clinical examination in situations of suspected nonaccidental trauma, laboratory testing for osteogenesis imperfecta (and other genetic disorders that predispose for fractures) was valuable in discerning the basis for fractures [Marlowe et al., 2002].
DISORDERS ASSOCIATED WITH CLEFT LIP AND PALATE Clefts of the lip or palate, or both, are among the most common birth defects worldwide, with an incidence of between 1 in 600 and 1 in 1000 live births. It is the fourth most common congenital disorder in humans [Cobourn, 2004; Cox, 2004; Stanier and Moore, 2004]. The Online Mendelian Inheritance in Man catalog (http://www3.ncbi.nlm.nih.gov/ Omim) lists more than 400 single-gene causes of cleft lip/
palate. A majority (i.e., 70%) of cases of this disorder are nonsyndromic, in which cleft lip/palate occurs in isolation of other phenotypes. When one or more additional features are involved, clefts are referred to as syndromic. Collectively, cleft lip/palate has a major clinical impact requiring surgical, dental, orthodontic, speech, hearing, and psychologic treatments or therapies throughout childhood. The etiology of cleft lip/palate is complex and thought to involve both major and minor genetic influences, with variable interactions from environmental factors. Several monographs published in the past decade and more recently provide much information about these disorders and their evaluation and management [Berkowitz, 1996; Canady et al., 1999; Gorlin, 1990; Jones, 2000; Sperber, 2001; Turvey, 1996; Wyszynski, 2002]. Table 19-26 presents a selected list of the most common disorders in which neurologic involvement may be significant in children with cleft lip/palate.
Embryology The lip and palatal regions are developed from the embryonic primary and secondary palates [Wong and Hagg, 2004]. The primary palate contributes to the lip, anterior toothbearing alveolus, and the anterior palate up to the incisal foramen. The secondary palate contributes to the remaining hard and soft palates. During the fourth week of gestation, neural crest cells from the anterior neural tube migrate to form the facial primordia, from which the nasal and the lateral maxillary processes fuse to form the primary palate. The secondary palate begins to form in the sixth week of gestation. Palatal shelves initially appear as two downward extensions from the inner side of the left and right maxilla along the lateral surface of the tongue. In the ninth week, the two palatal shelves undergo a rapid horizontal transformation, by moving over the tongue and fusing with each other and with the nasal septum. Failure in the fusion of primary or secondary palates leads to clefts of the respective areas. Thus, the resultant defect appears commonly as cleft lip with or without cleft palate or isolated cleft palate.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
Genetic and Environmental Factors An in-depth review of the molecular basis of cleft lip/palate is beyond the scope of this chapter. Several recent reviews have summarized available data on this subject [Cobourn, 2004; Cox, 2004; Lidral and Murray, 2004; Wong and Hagg, 2004]. Overall, four categories of genes for which there are results suggestive of a genetic susceptibility to cleft lip/palate are (1) genes expressed in a particular area of the embryo or in a particular period of palatal arch development, such as TGF-α, TGF-β2, and TGF-β3; (2) genes having biologic activities linked to pathogenesis of cleft lip/palate without direct involvement (e.g., the retinoic acid receptor, the methylenetetrahydrofolate reductase receptor and the folic acid receptor; (3) genes or loci identified in experimental animals as the homeotic genes MSX1 and MSX2; (4) genes involved in the interaction with the xenobiotic metabolism, such as those in the P-450 cytochrome system [Bianchi et al., 2000].
Recently Discovered Genes Causing Syndromic Cleft Lip or Palate Some of the more important recently discovered genes are summarized next and in Table 19-27. T-Box Transcription Factor-22 Gene. X-linked cleft palate is characterized by isolated cleft palate and “tonguetie” (ankyloglossia), and the gene has been localized to chromosomal region Xq21. Mutations of the T-box transcription factor-22 gene (TBX22) were demonstrated in a large Icelandic family with X-linked cleft palate and in several other families [Braybrook et al., 2001]. Animal experiments have found that expression of TBX22 is highly restricted to the palatal shelves and the base of the tongue corresponding to the frenulum. Involvement of TBX22 in nonsyndromic cleft lip/palate has recently been suggested. Poliovirus Receptor–Like-1 Gene. Cleft lip/palateectodermal dysplasia syndrome, inherited as an autosomal recessive trait, is characterized by cleft lip with or without cleft palate, hidrotic ectodermal dysplasia, syndactyly, and occasionally mental retardation. Mutations of the poliovirus receptor–like-1 gene (PVRL1) have been demonstrated in families with this dosorder. Now known as nectin, the protein product of PVRL1 was initially identified as poliovirus receptor-related protein that functioned as a CAM [Takahashi et al., 1999]. TABLE 19-27 Candidate Genes or Loci Involved in Nonsyndromic Cleft Lip and Palate
From Wong FK, Hagg U. An update on the aetiology of orofacial clefts. Hong Kong Med J 2004;10:331.
467
Interferon Regulatory Factor-6 Gene. Van der Woude’s syndrome is the most common form of syndromic cleft lip/ palate and accounts for 2% of all cases of cleft lip/palate. This syndrome is characterized by cleft lip with or without cleft palate, isolated cleft palate, pits or mucous cysts on the lower lip, and hypodontia. Popliteal pterygium syndrome includes all of the features of Van der Woude’s syndrome plus popliteal pterygium, syngnathia, distinct toenail abnormality, syndactyly, and genitourinary malformations. In families with Van der Woude’s syndrome and popliteal pterygium syndrome, localization to chromosomal region 1q32-q41 has been demonstrated, and mutations in the interferon regulatory factor-6 gene (IRF6) have been described [Kondo et al., 2002]
Candidate Genes for Nonsyndromic Cleft Lip or Palate Transforming Growth Factor-α Gene. The gene encoding transforming growth factor-α (TGFA) has been associated with nonsyndromic cleft lip/palate. The combined effects of TGFA mutations and environmental influences in this disorder have suggested that the presence of the rare TGFA variant (TaqI C2 allele) associated with maternal smoking results in a six- to eightfold increase in the risk of cleft palate and a twofold increase in the risk of cleft lip with or without cleft palate [Hwang et al., 1995; Shaw et al., 1996]. In addition, lack of multivitamin use during the first trimester of pregnancy in infants with the TGFA TaqI C2 allele appears to increase the relative risk for cleft lip with or without cleft palate three- to eightfold [Shaw et al., 1998]. Drosophila Msh Homeobox Homolog-1 Gene. MSX1 (Drosophila msh homeobox homolog-1 gene) mutations cause an autosomal dominant form of tooth agenesis and more recently have been identified in patients with cleft lip with or without cleft palate [Jezewski et al., 2003]. It is suggested that MSX1 mutations contributed to 2% of all cases of nonsyndromic cleft lip/palate. A recent study showed that the combined genetic background of rare variants of TGFA and MSX1 could increase the risk of cleft palate up to 9.7 times, demonstrating the significance of gene-gene interaction in the etiology of nonsyndromic cleft lip/palate [Jugessur et al., 2003a]. 5,10-Methylenetetrahydrofolate Reductase Gene. The association between folic acid deficiency and neural tube defects is well established (see also Chapter 90). 5,10-Methylenetetrahydrofolate reductase (MTHFR) is the enzyme responsible for catalyzing the conversion of 5,10-methylenetetrahydrofolate into 5-methyl-tetrahydrofolate. The MTHFR C677T genotype is a risk factor for neural tube defects. In nonsyndromic cleft lip/palate, the MTHFR C677T genotype in the mother conferred a risk of cleft lip/palate in offspring that was increased 4.6-fold [Prescott et al., 2002]. In association with folate deficiency during pregnancy, the MTHFR thermally labile variant could lead to a 10-fold increased risk of cleft lip/palate [van Rooij et al., 2003]. Transforming Growth Factor-b3 Gene. Mice lacking the gene encoding TGF-β3 (TGFB3) have cleft palate because of defective adhesion of opposing palatal shelves. In humans, TGFB3 has been associated with nonsyndromic cleft lip/palate [Jugessur et al., 2003a]. Other Genes and Loci. Numerous other genes and proteins have been associated with cleft lip/palate. Table 19-27 summarizes some of these factors.
468
Perinatal Acquired and Congenital Neurologic Disorders / 19
Environmental Factors Smoking. The relation between maternal smoking and cleft lip/palate is not strong but is significant [Wong and Hagg, 2004]. Several studies have consistently yielded a relative risk of about 1.3 to 1.5 [Wyszynski and Wu, 2002]. The combined effect of maternal smoking and certain maternal or fetal genotypes may further increase the risk of cleft lip/palate. Maternal glutathione S-transferase θ-1 (GSTT1) genotype, combined with smoking, increases the risk of cleft lip/palate by a factor of 4.9, and maternal smoking plus infant MSX1 genotypes increases the risk by 7.16. Alcohol Use. Heavy maternal drinking, in addition to causing fetal alcohol syndrome, increases the risk of cleft lip/palate by 1.5 to 4.7 in a dose-dependent manner [Munger et al., 1996]. Investigators have found that mothers who have more than five drinks per occasion increase the risk of cleft lip/palate in their offspring by a factor of 3.4 [Shaw and Lammer, 1999]. Low-level alcohol consumption, however, does not appear to increase the risk of cleft lip/palate, and the relation between alcohol use and genotypes on the risk of cleft lip/palate has yet to be determined [Wong and Hagg, 2004]. Use of Folic Acid and Multivitamins. The relation of folate to cleft lip/palate is discussed in an earlier section. Folate deficiency with the background of the TGFA TaqI C2 genotype also has been found to increase the risk of cleft lip/palate [Jugessur et al., 2003b]. Defective maternal vitamin-dependent homocysteine metabolism also is a risk factor for cleft lip/palate in offspring. As reviewed by Wong and Hagg [2004], the role of folic acid supplementation in the prevention of cleft lip/palate has been investigated in several studies. Low-dose folate supplementation by fortifying cereal grain products did not protect against cleft lip/ palate; only high-dose supplementation (e.g., 10 mg daily) was effective.
Associated Neurologic, Neurocognitive, and Speech and Language Impairments A majority of the patients with nonsyndromic cleft lip/palate have normal neurologic function and do not have any longterm neurologic, neuropsychologic, or neurobehavioral problems. Persons with syndromic clefting are more likely to encounter difficulties in these domains. The literature on these coexistent conditions is small, but in the past decade, new interest aimed at a better understanding of these associated problems has developed. Of interest, some very-long-term clinical studies spanning more than 5 decades that examined aspects of quality of life in patients with cleft lip/ palate have been published [Christensen and Mortensen, 2002].
Speech and Language Functioning Children with cleft lip/palate are at risk for speech and language disorders, which can be identified during infancy [Kapp-Simon and Krueckeberg, 2000]. These include limitations in phonemic repertoire, poor intelligibility, and delays in expressive and receptive language skills [KappSimon and Krueckeberg, 2000; Scherer and D’Antonio, 1995]. Conventional audiologic evaluations such as pure tone audiometry, word discrimination audiometry, and acoustic immittance measures may find abnormalities in
these children, as well as evidence of auditory processing disorders [Minardi et al., 2004; Schnitt et al., 2004]. A study of 54 children with cleft lip/palate found normal intelligibility in 53%, mild hypernasality in 23.5%, and mild hyponasality in 29% [Timmons et al., 2001]. Dysphonia was present in 41% of patients with cleft lip/palate.
Neurologic Involvement Very little information is available concerning brain morphology or neurologic function in children with cleft lip/ palate. In one study of adult males with nonsyndromic clefting, MRI found enlarged anterior regions of the cerebrum, and decreased volumes of the posterior cerebrum and cerebellum compared to age matched controls [Nopoulos et al., 2002a]. The most severely affected region was the left temporal lobe. Structural abnormalities also were believed to be directly related to cognitive dysfunction. A second study from the same group of investigators found evidence of an enlarged cavum septum pellucidum in 8% of adults with cleft lip/palate and also demonstrated an inverse relation between IQ and presence of the cavum [Nopoulos et al., 2001]. Similar studies have not been performed in children.
Neurocognitive and Neurobehavioral Disorders Studies of cognitive function in children are complicated by the heterogeneous sampling described in most studies. In one report of 84 patients, 46% of children with cleft lip/ palate had a learning disability, 47% had deficient educational progress, and 27% had repeated a grade [Broder et al., 1998]. Male patients with cleft palate only had a significantly higher rate of learning disorders. A longitudinal study of 16 children with cleft lip/palate using the Bayley Scales of Infant Development found that the children had lower scores on the mental and motor scales of the Bayley Scales of Infant Development, and on tests of language comprehension and expression, than corresponding scores of control subjects [Jocelyn et al., 1996]. Early studies that have been recently confirmed found that cognitive and motor development based on Bayley Scales of Infant Development scores was in the average range during the first year of life but then regressed during the second year [Kapp-Simon and Krueckeberg, 2000]. A third study of 148 children with all types of cleft lip/palate found Bayley Scales of Infant Development scores in the normal range; however, the presence of systemic congenital malformations was associated with lower scores [Swanenburg de Veye et al., 2003]. Reading problems in children with cleft lip/palate also have been evaluated. Children with nonsyndromic cleft lip/ palate show symptoms similar to a naming-memory deficit model of developmental dyslexia. Reading treatment should therefore avoid sight word approaches and focus on oral phonics [Richman et al., 2003]. Mental retardation does occur in patients with cleft lip/ palate, but its prevalence is unknown. One study of 56 persons with cleft lip/palate and mental retardation found that 46.8% had an isolated cleft palate and that 46.3% had multiple anomalies, syndromes, or associated medical findings [Strauss and Broder, 1993]. Common findings included cardiopulmonary defects, seizures, and deviations in head size. Adults with nonsyndromic cleft lip/palate have lower full scale IQ, performance IQ, and verbal IQ scores than corresponding scores in control subjects with specific deficits in verbal fluency [Nopoulos et al., 2002b].
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects
Psychiatric problems of children and adults with cleft lip/palate have been investigated to a very limited degree. In one 1978 study of 10 children, problems with excessive dependency, mental retardation, and developmental deviations were noted [Simonds and Heimburger, 1978]. Through the Danish Facial Cleft Database, 6462 patients with cleft lip/ palate born between 1936 and 1987 were evaluated over time. The risk of hospitalization for mental disorders was increased in patients with cerebral palsy, but not to any substantial degree in patients with cleft lip/palate. Both groups had an increased risk of mental retardation and substance abuse, but the risk for schizophrenia or bipolar illness was not increased compared with that in the background population. Also, no evidence indicates that the psychosocial stressors associated with cleft lip/palate and its treatment had any impact on the risk for mental illness requiring hospitalization [Christensen and Mortensen, 2002].
Management Caring for the child with cleft palate requires a multidisciplinary approach that begins with evaluation for other possible congenital anomalies, decisions about timing of repair, and choice of techniques. Postoperative follow-up evaluation similarly requires a team approach and should include an otolaryngologist, an orthodontist, and a speech therapist [Batra et al., 2003; Sadove et al., 2004]. The role of neurologic evaluation and the need for neuroimaging in children with nonsyndromic or syndromic clefting have not been systematically studied. Children diagnosed with multiple anomalies or a specific syndrome are more likely to have neurologic and developmental disorders, and evaluation for such disorders should be considered. If children with nonsyndromic cleft lip/palate are meeting their developmental goals and if their families, pediatricians, or primary care physicians are not concerned about any overt problems, then the yield from neurologic evaluation is likely to be limited. REFERENCES Abbott R. The endoscopic management of arachnoidal cysts. Neurosurg Clin N Am 2004;15:9. Ablin DS, Sane SM. Non-accidental injury: Confusion with temporary brittle bone disease and mild osteogenesis imperfecta. Pediatr Radiol 1997;27:111. Abou-Zahr F, Bejjani B, Kruyt FA, et al. Normal expression of the Fanconi anemia proteins Faa and Fac and sensitivity to mitomycin C in two patients with Seckel syndrome. Am J Med Genet 1999;83:388. Abrahams JJ, Eklund JA. Diagnostic radiology of the cranial base. Clin Plast Surg 1995;22:373. Acampora D, Gulisano M, Broccoli V, et al. OTX genes in brain morphogenesis. Prog Neurobiol 2001;64:69. Adachi M, Tachibana K, Asakura Y, et al. Compound heterozygous mutations of cytochrome P450 oxidoreductase gene (POR) in two patients with Antley-Bixler syndrome. Am J Med Genet A 2004;128A:333. Adamsbaum C, Robain O, Cohen PA, et al. Focal cortical dysplasia and hemimegalencephaly: Histological and neuroimaging correlations. Pediatr Radiol 1998;28:583. Ades LC, Morris LL, Power RG, et al. Distinct skeletal abnormalities in four girls with Shprintzen-Goldberg syndrome. Am J Med Genet 1995;57:565. Adzick NS, Sutton LN, Crombleholme TM, Flake AW. Successful fetal surgery for spina bifida. Lancet 1998;352:1675. Ahmetoglu A, Isik Y, Aynaci O, et al. Proteus syndrome associated with liver involvement: Case report. Genet Couns 2003;14:221. Aicardi J, Goutieres F. The syndrome of absence of the septum pellucidum with porencephalies and other developmental defects. Neuropediatr 1981;12:319.
469
Aicardi J, Lefebvre J, Lerique-Koechlin A. A new syndrome: Spasm in flexion, callosal agenesis, ocular abnormalities. Eletroenceph Clin Neurophysiol 1965;19:609. Ain MC, Browne JA. Spinal arthrodesis with instrumentation for thoracolumbar kyphosis in pediatric achondroplasia. Spine 2004;29:2075. Ainsworth JR, Bryce IG, Dudgeon J. Visual loss in infantile osteopetrosis. J Pediatr Ophthalmol Strabismus 1993;30:201. Alagappan R, Browning PD, Laorr A, et al. Distal lateral ventricular atrium: Reevaluation of normal range. Radiology 1994;193:405. Albayram S, Kizilkilic O, Yilmaz H, et al. Abnormalities in the cerebral arterial system in osteogenesis imperfecta. AJNR Am J Neuroradiol 2003;24:748. Albrecht S, Haber RM, Goodman JC, et al. Cowden syndrome and Lhermitte-Duclos disease. Cancer 1992;70:869. Albright AL, Byrd RP. Suture pathology in craniosynostosis. J Neurosurg 1981;54:384. Aldana PR, Ragheb J, Sevald J, et al. Cerebrospinal fluid shunt complications after urological procedures in children with myelodysplasia. Neurosurgery 2002;50:313-318; discussion 318. Aldegheri R, Dall’Oca C. Limb lengthening in short stature patients. J Pediatr Orthop B 2001;10:238. Alderton GK, Joenje H, Varon R, et al. Seckel syndrome exhibits cellular features demonstrating defects in the ATR-signalling pathway. Hum Mol Genet 2004;13:3127. Aleck K. Craniosynostosis syndromes in the genomic era. Semin Pediatr Neurol 2004;11:256. Aleksic S, Budzilovich G, Greco MA, et al. Encephalocele (cerebellocele) in the Goldenhar-Gorlin syndrome. Eur J Pediatr 1983;140:137. Alksne JF, Lovings ET. Functional ultrastructure of the arachnoid villus. Arch Neurol 1972;27:371. Allen WP, Stevenson RE, Thompson SJ, Dean JH. The impact of prenatal diagnosis on NTD surveillance. Prenat Diagn 1996;16:531. Alles AJ, Sulik KK. Pathogenesis of retinoid-induced hindbrain malformations in an experimental model. Clin Dysmorphol 1992;1:187. Al-Torki NA, Sabry MA, Al-Awadi SA, et al. Lowry-Maclean syndrome with osteopenic bones and possible autosomal dominant inheritance in a Bedouin family. Am J Med Genet 1997;73:491. Alvarez LA, Maytal J, Shinnar S. Idiopathic external hydrocephalus: Natural history and relationship to benign familial macrocephaly. Pediatrics 1986;77:901. Amako M, Fassier F, Hamdy RC, et al. Functional analysis of upper limb deformities in osteogenesis imperfecta. J Pediatr Orthop 2004;24:689. Ambler M, Pogacar S, Sidman R. Lhermitte-Duclos disease (granule cell hypertrophy of the cerebellum): Pathological analysis of the first familial cases. J Neuropathol Exp Neurol 1969;28:622. American Academy of Pediatrics, Task Force on Positioning and Sudden Infant Death Syndrome. Positioning and SIDS. Pediatrics 1992;89:1120. Amir N, Gross-Kieselstein E, Hirsch HJ, et al. Weaver-Smith syndrome. A case study with long-term follow-up. Am J Dis Child 1984;138:1113. Amor DJ, Leventer RJ, Hayllar S, et al. Polymicrogyria associated with scalp and limb defects: Variant of Adams-Oliver syndrome. Am J Med Genet 2000;93:328. Anderson FM. Occult spinal dysraphism: A series of 73 cases. Pediatrics 1975;55:826. Anderson NG, Jordan S, MacFarlane MR, Lovell-Smith M. Diastematomyelia: diagnosis by prenatal sonography. AJR Am J Roentgenol 1994;163:911. Anderson PJ, Hall CM, Evans RD, et al. The cervical spine in Saethre-Chotzen syndrome. Cleft Palate Craniofac J 1997a;34:79. Anderson PJ, Harkness WJ, Taylor W, et al. Anomalous venous drainage in a case of non-syndromic craniosynostosis. Childs Nerv Syst 1997b;13:97. Anderson PJ, Netherway DJ, Abbott AH, et al. Analysis of intracranial volume in Apert syndrome genotypes. Pediatr Neurosurg 2004;40:161. Anderson SA, Eisenstat DD, Shi L, et al. Interneuron migration from basal forebrain to neocortex: Dependence on DLX genes. Science 1997;278:474. Anderson SA, Marin O, Horn C, et al. Distinct cortical migrations from the medial and lateral ganglionic eminences. Development 2001;128:353. Andrisano A, Soncini G, Calderoni PP, et al. Critical review of infantile fibrous dysplasia: Surgical treatment. J Pediatr Orthop 1991;11:478. Andy OJ, Stephan H. The septum in the human brain. J Comp Neurol 1968;133:383. Aniskiewicz AS, Frumkin NL, Brady DE, et al. Magnetic resonance imaging and neurobehavioral correlates in schizencephaly. Arch Neurol 1990;47:911. Anteby EY, Yagel S. Route of delivery of fetuses with structural anomalies. Eur J Obstet Reprod Biol 2003;106:5. Anwar M, Kadam S, Hiatt IM, et al. Serial lumbar punctures in prevention of post-hemorrhagic hydrocephalus in preterm infants. J Pediatr 1985;107:446.
470
Perinatal Acquired and Congenital Neurologic Disorders / 19
Archer CA, Darwish H, Smith K Jr. Enlarged cisternae magnae and posterior fossa cysts simulating Dandy-Walker syndrome on computed tomography. Radiology 1978;127:681. Archibeck MJ, Smith JT, Carroll KL, et al. Surgical release of tethered spinal cord: Survivorship analysis and orthopedic outcome. J Pediatr Orthop 1997;17:77. Arnett B. Arnold-Chiari malformation. Arch Neurol 2003;60:898. Aronyk KE. The history and classification of hydrocephalus. Neurosurg Clin N Am 1993;4:599. Arora A, Bannister CM, Russell S, et al. Outcome and clinical course of prenatally diagnosed cerebral ventriculomegaly. Eur J Pediatr Surg 1998;8:63. Arslanian SA, Rothfus WE, Foley TP Jr, et al. Hormonal, metabolic, and neuroradiologic abnormalities associated with septo-optic dysplasia. Acta Endocrinol (Copenh) 1984;107:282. Artigas-Pallares J, Gabau-Vila E, Guitart-Feliubadalo M. Syndromic autism: II. Genetic syndromes associated with autism. Rev Neurol 2005;40 (Suppl 1):S151. Aryan HE, Meltzer HS, Gerras GG, et al. Leptomeningeal cyst development after endoscopic craniosynostosis repair: Case report. Neurosurgery 2004;55:235. Astrom E, Soderhall S. Beneficial effect of bisphosphonate during five years of treatment of severe osteogenesis imperfecta. Acta Paediatr 1998;87:64. Aubry MC, Aubry JP, Dommergues M. Sonographic prenatal diagnosis of central nervous system abnormalities. Childs Nerv Syst 2003;19:391. Aviezer D, Golembo M, Yayon A. Fibroblast growth factor receptor-3 as a therapeutic target for achondroplasia—genetic short limbed dwarfism. Curr Drug Targets 2003;4:353. Aviv RI, Rodger E, Hall CM. Craniosynostosis. Clin Radiol 2002;57:93. Azusawa H, Ozaki Y, Shindoh N, et al. Usefulness of MR venography in diagnosing sinus pericranii: Case report. Radiat Med 2000;18:249. Baba H, Maezawa Y, Furusawa N, et al. The cervical spine in the Klippel-Feil syndrome. A report of 57 cases. Int Orthop 1995;19:204. Badie B, Mendoza D, Batzdorf U. Posterior fossa volume and response to suboccipital decompression in patients with Chiari I malformation. Neurosurgery 1995;37:214. Bale JF, Jr. Congenital infections. Neurol Clin 2002;20:1039-1060, vii. Ball WS Jr. Pediatric neuroradiology. New York: Lippincott-Raven, 1997. Banerji NK, Millar JH. Chiari malformation presenting in adult life. Its relationship to syringomyelia. Brain 1974;97:157. Baraitser M, Winter RM. Iris coloboma, ptosis, hypertelorism, and mental retardation: A new syndrome. J Med Genet 1988;25:41. Barkovich AJ. Morphologic characteristics of subcortical heterotopia: MR imaging study. AJNR Am J Neuroradiol 2000;21:290. Barkovich AJ. Pediatric neuroimaging. New York: Lippincott Williams & Wilkins, 2005. Barkovich AJ, Kjos BO. Schizencephaly: Correlation of clinical findings with MR characteristics. AJNR Am J Neuroradiol 1992a;13:85. Barkovich AJ, Kjos BO. Gray matter heterotopias: MR characteristics and correlation with developmental and neurological manifestations. Radiology 1992b;182:493. Barkovich AJ, Lindan CE. Congenital cytomegalovirus infection of the brain: Imaging analysis and embryologic considerations. AJNR Am J Neuroradiol 1994;15:703. Barkovich AJ, Norman D. MR imaging of schizencephaly. AJR Am J Roentgenol 1988;150:1391. Barkovich AJ, Norman D. Absence of the septum pellucidum: A useful sign in the diagnosis of congenital brain malformations. AJR Am J Roentgenol 1989;152:353. Barkovich AJ, Ferriero DM, Barr RM, et al. Microlissencephaly: A heterogeneous malformation of cortical development. Neuropediatr 1998;29:113. Barkovich AJ, Fram EK, Norman D. Septo-optic dysplasia: MR imaging. Radiology 1989;171:189. Barkovich AJ, Guerrini R, Battaglia G, et al. Band heterotopia: Correlation of outcome with magnetic resonance imaging parameters. Ann Neurol 1994;36:609. Barkovich AJ, Koch TK, Carrol CL. The spectrum of lissencephaly: Report of ten patients analyzed by magnetic resonance imaging. Ann Neurol 1991;30:139. Barkovich AJ, Kuzniecky RI, Bollen AW, et al. Focal transmantle dysplasia: A specific malformation of cortical development. Neurology 1997;49:1148. Barkovich AJ, Kuzniecky RI, Dobyns WB, et al. A classification scheme for malformations of cortical development. Neuropediatrics 1996;27:59.
Barkovich AJ, Kuzniecky RI, Jackson GD, et al. Classification system for malformations of cortical development: Update 2001. Neurology 2001;57:2168. Barlow P, Ching HS. An economic argument in favour of endoscopic third ventriculostomy as a treatment for obstructive hydrocephalus. Minim Invasive Neurosurg 1997;40:37. Baroni T, Carinci P, Lilli C, et al. P253R fibroblast growth factor receptor-2 mutation induces RUNX2 transcript variants and calvarial osteoblast differentiation. J Cell Physiol 2005;202:524. Barr M, Cohen M. Holoprosencephaly: Parents’ report of their experiences, problems, and solutions. Proc Greenwood Genet Center, 1998. Barr M, Cohen MM. Holoprosencephaly survival and performance. Am J Med Genetics 1999;89:116. Barr M, Hanson JW, Currey K, et al. Holoprosencephaly in infants of diabetic mothers. J Pediatr 1983;102:565. Bartels MC, Vaandrager JM, de Jong TH, et al. Visual loss in syndromic craniosynostosis with papilledema but without other symptoms of intracranial hypertension. J Craniofac Surg 2004;15:1019. Barth PG. Migrational disorders of the brain. Curr Opin Neurol Neurosurg 1992;5:339. Barth PG. Pontocerebellar hypoplasias. An overview of a group of inherited neurodegenerative disorders with fetal onset. Brain Dev 1993;15:411. Barth PG. Pontocerebellar hypoplasia—how many types? Eur J Paediatr Neurol 2000;4:161. Barth PG, van der Harten JJ. Parabiotic twin syndrome with topical isocortical disruption and gastroschisis. Acta Neuropathol 1985;67:345. Barth PG, Blennow G, Lenard HG, et al. The syndrome of autosomal recessive pontocerebellar hypoplasia, microcephaly, and extrapyramidal dyskinesia (pontocerebellar hypoplasia type 2): Compiled data from 10 pedigrees. Neurology 1995;45:311. Barth PG, Mullaart R, Stam FC, et al. Familial lissencephaly with extreme neopallial hypoplasia. Brain Dev 1982;4:145. Barth PG, Vrensen GF, Uylings HB, et al. Inherited syndrome of microcephaly, dyskinesia and pontocerebellar hypoplasia: A systemic atrophy with early onset. J Neurol Sci 1990;97:25. Bartolomei F, Gavaret M, Dravet C, et al. Familial epilepsy with unilateral and bilateral malformations of cortical development. Epilepsia 1999;40:47. Bass T, White LE, Wood RD, et al. Rapid decompression of congenital hydrocephalus associated with parenchymal hemorrhage. J Neuroimaging 1995;5:249. Bassi P, Corona C, Contri P, et al. Congenital basilar impression, correlated neurological syndromes. Eur Neurol 1992;32:238. Batra P, Duggal R, Parkash H. Genetics of cleft lip and palate revisited. J Clin Pediatr Dent 2003;27:311. Battaglia A. Seizures and dysplasias of cerebral cortex in dysmorphic syndromes. In: Guerrini R, Andermann F, Canapicchi R, et al., eds. Dysplasias of cerebral cortex and epilepsy. Philadelphia: Lippincott-Raven, 1996, p 199. Battaglia G, Granata T, Farina L, et al. Periventricular nodular heterotopia: Epileptogenic findings. Epilepsia 1997;38:1173. Beals SP, Joganic EF. Form and function in craniofacial deformities. Semin Pediatr Neurol. 2004;11:238. Becker AJ, Urbach H, Scheffler B, et al. Focal cortical dysplasia of Taylor’s balloon cell type: Mutational analysis of the TSC1 gene indicates a pathogenic relationship to tuberous sclerosis. Ann Neurol 2002;52:29. Becker LE, Hinton DR. Pathogenesis of craniosynostosis. Pediatr Neurosurg 1995;22:104. Bell WO, Sumner TE, Volberg,FM. The significance of ventriculomegaly in the newborn with myelodysplasia. Childs Nerv Syst 1987;3:239. Belloni E, Martucciello G, Verderio D, et al. Involvement of the HLXB9 homeobox gene in Currarino syndrome. Am J Hum Genet 2000;66:312. Belloni E, Muenke M, Roessler E, et al. Identification of Sonic hedgehog as a candidate gene responsible for holoprosencephaly. Nat Genet 1996;14:353. Bellus GA, Escallon CS, de Luno RO, et al. First-trimester prenatal diagnosis in couple at risk for homozygous achondroplasia. Lancet 1994;344:1511. Beltran-Valero De Bernabe D, Currier S, Steinbrecher A, et al. Mutations in the O-mannosyltransferase gene POMT1 give rise to the severe neuronal migration disorder Walker-Warburg syndrome. Am J Hum Genet 2002;71:1033. Beltran-Valero de Bernabe D, van Bokhoven H, van Beusekom E, et al. A homozygous nonsense mutation in the fukutin gene causes a Walker-Warburg syndrome phenotype. J Med Genet 2003;40:845. Beltran-Valero de Bernabe D, Voit T, Longman C, et al. Mutations in the FKRP gene can cause muscle-eye-brain disease and Walker-Warburg syndrome. J Med Genet 2004;41:e61.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Bembi B, Parma A, Bottega M, et al. Intravenous pamidronate treatment in osteogenesis imperfecta. J Pediatr 1997;131:622. Ben Hamouda H, Sfar MN, Braham R, et al. Association of severe autosomal recessive osteopetrois and Dandy-Walker syndrome with agenesis of the corpus callosum. Acta Orthop Belg 2001;67:528. Benecke JE Jr. Facial nerve dysfunction in osteopetrosis. Laryngoscope 1993;103:494. Benke PJ. The isotretinoin teratogen syndrome. JAMA 1984;251:3267. Benson ML, Oliverio PJ, Yue NC, et al. Primary craniosynostosis: Image features. AJR Am J Roentgenol 1996;166:697. Berkowitz S. Cleft lip and palate: With an introduction to other craniofacial anomalies: Perspectives in management. San Diego, Calif: Singular Publishing Group, 1996. Beuerlein ME, Schuller DE, DeYoung BR. Maxillary malignant mesenchymoma and massive fibrous dysplasia. Arch Otolaryngol Head Neck Surg 1997;123:106. Bianchi F, Calzolari E, Ciulli L, et al. Environment and genetics in the etiology of cleft lip and cleft palate with reference to the role of folic acid. Epidemiol Prev 2000;24:21. Bibby K, McFadzean R. Fibrous dysplasia of the orbit. Br J Ophthalmol 1994;78:266. Bienvenu T, Poirier K, Friocourt G, et al. ARX, a novel prd-class-homeobox gene highly expressed in the telencephalon, is mutated in X-linked mental retardation. Hum Mol Genet 2002;11:981. Bierbrauer KS, Storrs BB, McLone DG. A prospective randomized study of shunt function and infections as a function of shunt placement. Pediatr Neurosurg 1990;16:287. Biesecker LG, Happle R, Mulliken JB, et al. Proteus syndrome: Diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet 1999;84:389. Biggio JR Jr, Owen J, Wenstrom KD, Oakes WJ. Can prenatal ultrasound findings predict ambulatory status in fetuses with open spina bifida? Am J Obstet Gynecol 2001;185:1016. Binaghi S, Gudinchet F, Rilliet B. Three-dimensional spiral CT of craniofacial malformations in children. Pediatr Radiol 2000;30:856. Bingham PM, Lynch D, McDonald-McGinn D, et al. Polymicrogyria in chromosome 22 deletion syndrome. Neurology 1998;51:1500. Birnbacher R, Messerschmidt AM, Pollak AP. Diagnosis and prevention of neural tube defects. Curr Opin Urol 2002;12:461. Birnholz JC, Frigoletto FD. Antenatal treatment of hydrocephalus. N Engl J Med 1981;304:1021. Bland JD, Emery JL. Unexpected death of children with achondroplasia after the perinatal period. Dev Med Child Neurol 1982;24:489. Blankenstein R, Brook AH, Smith RN, et al. Oral findings in Carpenter syndrome. Int J Paediatr Dent 2001;11:352. Bloom SL, Bloom DD, DellaNebbia C, et al. The developmental outcome of children with antenatal mild isolated ventriculomegaly. Obstet Gynecol 1997;90:93. Bluml S, McComb JG, Ross BD. Differentiation between cortical atrophy and hydrocephalus using 1H MRS. Magn Reson Med 1997;37:395. Bobabilla-Morales L, Corona-Rivera A, Corona-Rivera JR, et al. Chromosome instability induced in vitro with mitomycin C in five Seckel syndrome patients. Am J Med Genet 2003;123A:148. Bocca G, de Vries J, Cruysberg JR, et al. Optic neuropathy in McCune-Albright syndrome: An indication for aggressive treatment. Acta Paediatr 1998;87:599. Bodensteiner JB, Schaefer GB. Wide cavum septum pellucidum: A marker of disturbed brain development. Pediatr Neurol 1990;6:391. Boltshauser E, Isler W. Joubert syndrome: Episodic hyperpnea, abnormal eye movements, retardation and ataxia, associated with dysplasia of the cerebellar vermis. Neuropadiatrie 1977;8:57. Boltshauser E, Martin F, Altermatt S. Outcome in children with spaceoccupying posterior fossa arachnoid cysts. Neuropediatrics 2002;33:118. Boltshauser E. Cerebellum—small brain but large confusion: A review of selected cerebellar malformations and disruptions. Am J Med Genet A 2004;126:376. Bond J, Roberts E, Mochida GH, et al. ASPM is a major determinant of cerebral cortical size. Nat Genet 2002;32:316. Bond J, Scott S, Hampshire DJ, et al. Protein-truncating mutations in ASPM cause variable reduction in brain size. Am J Hum Genet 2003;73:1170. Bondurant CP, Jimenez DF. Epidemiology of cerebrospinal fluid shunting. Pediatr Neurosurg 1995;23:254. Bonneau D, Toutain A, Laquerriere A, et al. X-linked lissencephaly with absent corpus callosum and ambiguous genitalia (XLAG): Clinical, magnetic resonance imaging, and neuropathological findings. Ann Neurol 2002;51:340.
471
Boop FA, Chadduck WM, Shewmake K, et al. Outcome analysis of 85 patients undergoing the pi procedure for correction of sagittal synostosis. J Neurosurg 1996a;85:50. Boop FA, Shewmake K, Chadduck WM. Synostectomy versus complex cranioplasty for the treatment of sagittal synostosis. Childs Nerv Syst 1996b;12:371. Boor R, Fricke G, Bruhl K, Spranger J. Abnormal subcortical somatosensory evoked potentials indicate high cervical myelopathy in achondroplasia. Eur J Pediatr 1999;158:662. Bordarier C, Aicardi J. Dandy-Walker syndrome and agenesis of the cerebellar vermis: Diagnostic problems and genetic counselling. Dev Med Child Neurol 1990;32:285. Borgatti R, Triulzi F, Zucca C, et al. Bilateral perisylvian polymicrogyria in three generations. Neurology 1999;52:1910. Borgbjerg BM, Gjerris F, Albeck MJ, et al. Frequency and causes of shunt revisions in different cerebrospinal fluid shunt types. Acta Neurochir Wien 1995;136:189. Born CM, Meisenzahl EM, Frodl T, et al. The septum pellucidum and its variants. An MRI study. Eur Arch Psychiatry Clin Neurosci 2004;254:295. Borthwick KJ, Kandemir N, Topaloglu R, et al. A phenocopy of CAII deficiency: A novel genetic explanation for inherited infantile osteopetrosis with distal renal tubular acidosis. J Med Genet 2003;40:115. Bosman C, Boldrini R, Dimitri L, et al. Hemimegalencephaly. Histological, immunohistochemical, ultrastructural and cytofluorimetric study of six patients. Childs Nerv Syst 1996;12:765. Bottero L, Cinalli G, Labrune P, et al. Antley-Bixler syndrome. Description of two new cases and a review of the literature. Childs Nerv Syst 1997;13:275. Botto LD, Moore CA, Khoury MJ, Erickson JD. Neural-tube defects. N Engl J Med 1999;341:1509. Bowman RM, McLone DG, Grant JA, et al. Spina bifida outcome: A 25-year prospective. Pediatr Neurosurg 2001;34:114. Braybrook C, Doudney K, Marcano AC, et al. The T-box transcription factor gene TBX22 is mutated in X-linked cleft palate and ankyloglossia. Nat Genet 2001;29:179. Breningstall G, Janousek S, Marker S, Tubman D. Syringohydromyelia and diastematomyelia in patients with myelomeningocele detected by magnetic resonance imaging. Ann Neurol 1990;28:433. Bresnick S, Schendel S. Crouzon’s disease correlates with low fibroblastic growth factor receptor activity in stenosed cranial sutures. J Craniofac Surg 1995;6:245. Brickman JM, Clements M, Tyrell R, et al. Molecular effects of novel mutations in Hesx1/HESX1 associated with human pituitary disorders. Development 2001;128:5189. Bristol RE, Lekovic GP, Rekate HL. The effects of craniosynostosis on the brain with respect to intracranial pressure. Semin Pediatr Neurol 2004;11:262. Brock DJ, Barron L, van Heyningen V. Prenatal diagnosis of neural-tube defects with a monoclonal antibody specific for acetylcholinesterase. Lancet 1985;1:5. Brockmeyer DL, Wright LC, Walker ML, et al. Management of posthemorrhagic hydrocephalus in the low-birth-weight preterm neonate. Pediatr Neurosci 1989;15:302. Broder HL, Richman LC, Matheson PB. Learning disability, school achievement, and grade retention among children with cleft: A two-center study. Cleft Palate Craniofac J 1998;35:127. Bromley B, Benacerraf BR. Difficulties in the prenatal diagnosis of microcephaly. J Ultrasound Med 1995;14:303. Bromley B, Frigoletto FD Jr, Benacerraf BR. Mild fetal lateral cerebral ventriculomegaly: Clinical course and outcome. Am J Obstet Gynecol 1991;164:863. Brookshire BL, Fletcher JM, Bohan TP, et al. Verbal and nonverbal skill discrepancies in children with hydrocephalus: A five-year longitudinal follow-up. J Pediatr Psychol 1995;20:785. Brown EW, Megerian CA, McKenna MJ, et al. Fibrous dysplasia of the temporal bone: Imaging findings. AJR Am J Roentgenol 1995;164:679. Brown LY, Odent S, David V. Holoprosencephaly due to mutations in ZIC2: Alanine tract expansion mutations may be caused by parental somatic recombination. Hum Mol Genet 2001;10:791. Bruce DA. Consensus: Craniofacial synostoses. Apert and Crouzon syndromes. Childs Nerv Syst 1996;12:734. Brueton LA, van Herwerden L, Chotai KA, et al. The mapping of a gene for craniosynostosis: Evidence for linkage of the Saethre-Chotzen syndrome to distal chromosome 7p. J Med Genet 1992;29:681. Bruhl K, Stoeter P, Wietek B, et al. Cerebral spinal fluid flow, venous drainage and spinal cord compression in achondroplastic children: Impact of
472
Perinatal Acquired and Congenital Neurologic Disorders / 19
magnetic resonance findings for decompressive surgery at the craniocervical junction. Eur J Pediatr 2001;160:10. Brunelle F. Arteriovenous malformation of the vein of Galen in children. Pediatr Radiol 1997;27:501. Brunelli S, Faiella A, Capra V, et al. Germline mutations in the homeobox gene EMX2 in patients with severe schizencephaly. Nat Genet 1996;12:94. Bruner JP, Tulipan N, Paschall RL, et al. Fetal surgery for myelomeningocele and the incidence of shunt-dependent hydrocephalus. JAMA 1999;282:1819. Bullen PJ, Rankin JM, Robson SC. Investigation of the epidemiology and prenatal diagnosis of holoprosencephaly in the North of England. Am J Obstet Gynecol 2001;184:1256. Burke MJ, Winston KR, Williams S. Normal sutural fusion and the etiology of single sutural craniosynostosis: The microspicule hypothesis. Pediatr Neurosurg 1995;22:241. Burrows EH, Leeds NE. Neuroradiology, vol 1. New York: Churchill Livingstone, 1981. Burrows EH. Clinical relevance of radiological abnormalities of the craniovertebral junction. Br J Radiol 1981;54:195. Burstein FD, Hudgins RJ, Cohen SR, et al. Surgical correction of severe scaphocephalic deformities. J Craniofac Surg 1994;5:228. Butler MG, Hall BD, Maclean RN, et al. Do some patients with Seckel syndrome have hematological problems and/or chromosome breakage? Am J Med Genet 1987;27:645. Buyse G, Verpoorten C, Vereecken R, Casaer P. Treatment of neurogenic bladder dysfunction in infants and children with neurospinal dysraphism with clean intermittent (self)catheterisation and optimized intravesical oxybutynin hydrochloride therapy. Eur J Pediatr Surg 1995;5(Suppl 1):31. Byers PH. Osteogenesis imperfecta. In: Royce PM, Steinmann B, eds. Connective tissue and its heritable disorders: Molecular, genetic, and medical aspects. New York: Wiley-Liss, 1993. Byrd SE, Darling CF, McLone DG. Developmental disorders of the pediatric spine. Radiol Clin North Am 1991;29:711. Cai C, Oakes WJ. Hindbrain herniation syndromes: The Chiari malformations (I and II). Semin Pediatr Neurol 1997;4:179. Cai J, Goodman BK, Patel AS, et al. Increased risk for developmental delay in Saethre-Chotzen syndrome is associated with TWIST deletions: An improved strategy for Twist mutation screening. Human Genet 2003;114:68. Caldarelli M, Di Rocco C, Colosimo CJr, et al. Surgical treatment of late neurological deterioration in children with myelodysplasia. Acta Neurochir (Wien) 1995;137:199. Caldarelli M, Di Rocco C, La Marca F. Shunt complications in the first postoperative year in children with meningomyelocele. Childs Nerv Syst 1996;12:748. Campbell JW, Albright AL, Losken HW, et al. Intracranial hypertension after cranial vault decompression for craniosynostosis. Pediatr Neurosurg 1995;22:270. Canady J, Karnell M, Marsh, J. Cleft lip and cleft palate: The first four years. Chapel Hill, NC: Cleft Palate Foundation, 1999. Canick JA, Kellner LH, Bombard AT. Prenatal screening for open neural tube defects. Clin Lab Med 2003;23:385. Capovilla G, Lorenzetti ME, Montagnini A, et al. Seckel’s syndrome and malformations of cortical development: Report of three new cases and review of the literature. J Child Neurol 2001;16:382. Caraballo R, Cersosimo R, Fejerman N. A particular type of epilepsy in children with congenital hemiparesis associated with unilateral polymicrogyria. Epilepsia 1999;40:865. Caraballo RH, Cersosimo RO, Mazza E, et al. Focal polymicrogyria in mother and son. Brain Dev 2000;22:336. Cardoso C, Leventer RJ, Dowling JJ, et al. Clinical and molecular basis of classical lissencephaly: Mutations in the LIS1 gene (PAFAH1B1). Hum Mutat 2002;19:4. Cardoso C, Leventer RJ, Matsumoto N, et al. The location and type of mutation predict malformation severity in isolated lissencephaly caused by abnormalities within the lis1 gene [in process citation]. Hum Mol Genet 2000;9:3019. Cardoso C, Leventer RJ, Ward HL, et al. Refinement of a 400-kb critical region allows genotypic differentiation between isolated lissencephaly, Miller-Dieker syndrome, and other phenotypes secondary to deletions of 17p13.3. Am J Hum Genet 2003;72:918. Cardoza JD, Goldstein RB, Filly RA. Exclusion of fetal ventriculomegaly with a single measurement: The widlth of the lateral ventricular atrium. Radiology 1988;169:711. Carlson C, Sirotkin H, Pandita R, et al. Molecular definition of 22q11 deletions in 151 velo-cardio-facial syndrome patients. Am J Hum Genet 1997;61:620.
Carpenter JS, Rosen CL, Bailes JE, et al. Sinus pericranii: Clinical and imaging findings in two cases of spontaneous partial thrombosis. AJNR Am J Neuroradiol 2004;25:12. Carson BS, Weingart JD, Guarnieri M, Fisher PG. Third ventricular choroid plexus papilloma with psychosis. Case report. J Neurosurg 1997;87:103. Carter CO, David PA, Laurence KM. A family study of major central nervous system malformations in South Wales. J Med Genet 1968;5:81. Carter CO, Evans K. Spina bifida and anencephalus in greater London. J Med Genet 1973;10:209. Carter CO, Till K, Fraser V, et al. A family study of craniosynostosis, with probable recognition of a distinct syndrome. J Med Genet 1982;19:280. Carter M, Stokes D, Wang W. Severe obstructive apnea in a child with osteopetrosis. Clin Pediatr 1988;27:108. Casey AT, Kimmings EJ, Kleinlugtebeld AD, et al. The long-term outlook for hydrocephalus in childhood. A ten-year cohort study of 155 patients. Pediatr Neurosurg 1997;27:63. Castro-Gago M, Alonso A, Eiris Punal J. Autosomal recessive hydrocephalus with aqueductal stenosis. Childs Nerv Syst 1996;12:188. Cauli B, Audinat E, Lambolez B, et al. Molecular and physiological diversity of cortical nonpyramidal cells. J Neurosci 1997;17:3894. Caviness VS Jr. Normal development of cerebral neocortex. In: Evrard R, Minkowski A, eds. Developmental neurobiology. New York: Raven Press, 1989;1. Centers for Disease Control and Prevention. Spina bifida and anencephaly before and after folic acid mandate—United States, 1995-1996 and 19992000. MMWR Morb Mortal Wkly Rep 2004;53:362 (available at http://www.ncbi.nlm.nih.gov/entrez). Cerovac S, Neil-Dwyer JG, Rich P, et al. Are routine preoperative CT scans necessary in the management of single suture craniosynostosis? Br J Neurosurg 2002;16:348. Cerqueiro-Mosquera J, Penrose-Stevens A, et al. Facial palsy and achondroplasia: A rare association. Ann Plast Surg 2001;47:203. Chambers D, McGonnell IM. Neural crest: facing the facts of head development. Trends Genet 2002;18:381. Chan A, Robertson EF, Haan EA, et al. Prevalence of neural tube defects in South Australia, 1966-91: Effectiveness and impact of prenatal diagnosis. BMJ 1993;307:703. Chan, A, Robertson EF, Haan EA, et al. The sensitivity of ultrasound and serum alpha-fetoprotein in population-based antenatal screening for neural tube defects. South Australia 1986-1991. Br J Obstet Gynaecol 1995;102:370. Chandy MJ. Occipital fibrous dysplasia tonsillar herniation and cervical syringomyelia. Br J Neurosurg 1999;13:217. Chang BS, Piao X, Bodell A, et al. Bilateral frontoparietal polymicrogyria: Clinical and radiological features in 10 families with linkage to chromosome 16. Ann Neurol 2003;53:596. Chang BS, Piao X, Giannini C, et al. Bilateral generalized polymicrogyria (BGP): A distinct syndrome of cortical malformation. Neurology 2004;62:1722. Chang IC. Surgical experience in symptomatic congenital intraspinal cysts. Pediatr Neurosurg 2004;40:165. Chao A, Wong AM, Hsueh C, et al. Integration of imaging and pathological studies in Meckel-Gruber syndrome. Prenat Diagn 2005;25:267. Chapman S, Hall CM. Non-accidental injury or brittle bones. Pediatr Radiol 1997;27:106. Chapurlat RD, Delmas PD, Liens D, et al. Long-term effects of intravenous pamidronate in fibrous dysplasia of bone. J Bone Miner Res 1997;12:1746. Charles JM, Key LL. Developmental spectrum of children with congenital osteopetrosis. J Pediatr 1998;132:371. Charney EB, Rorke LB, Sutton, LN, Schut L. Management of Chiari II complications in infants with myelomeningocele. J Pediatr 1987;111:364. Chemke J, Robinson A. The third fontanelle. J Pediatr 1969;75:617. Chen KS, Hung PC, Wang HS, Jung SM, Ng SH. Medulloblastoma or cerebellar dysplastic gangliocytoma (Lhermitte-Duclos disease)? Pediatr Neurol 2002;27:404. Chenn A, Walsh CA. Regulation of cereberal cortical size by control of cell cycle exit in neural precursors. Science 2002;297:365. Chenn A, Walsh CA. Increased neuronal production, enlarged forebrains and cytoarchitectural distortions in beta-catenin overexpressing transgenic mice. Cerebral Cortex 2003;13:599. Cherubini E, Conti F. Generating diversity at GABAergic synapses. Trends Neurosci 2001;24:155. Chitayat D, Moore L, Del Bigio MR, et al. Familial Dandy-Walker malformation associated with macrocephaly, facial anomalies, developmental delay, and brain stem dysgenesis: Prenatal diagnosis and postnatal outcome in brothers. A new syndrome? Am J Med Genet 1994;52:406.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Chou SM, Gilbert EF, Chun RW, et al. Infantile olivopontocerebellar atrophy with spinal muscular atrophy (infantile OPCA + SMA). Clin Neuropathol 1990;9:21. Choux M, Genitori L, Lang D, Lena G. Shunt implantation: reducing the incidence of shunt infection. J Neurosurg 1992;77:875. Christensen K, Mortensen PB. Facial clefting and psychiatric diseases: A follow-up of the Danish 1936-1987 Facial Cleft Cohort. Cleft Palate Craniofac J 2002;39:392. Christophe C, Dan B. Magnetic resonance imaging cranial and cerebral dimensions: Is there a relationship with Chiari I malformation? A preliminary report in children. Eur J Paediatr Neurol 1999;3:15. Chumas PD, Cinalli G, Arnaud E, et al. Classification of previously unclassified cases of craniosynostosis. J Neurosurg 1997;86:177. Chun K, Siegel-Bartelt J, Chitayat D, et al. FGFR2 mutation associated with clinical manifestations consistent with Antley-Bixler syndrome. Am J Med Genet 1998;77:219. Chun K, Teebi AS, Azimi C, et al. Screening of patients with craniosynostosis: Molecular strategy. Am J Med Genet A 2003;120:470. Chun K, Teebi AS, Jung JH, et al. Genetic analysis of patients with the Saethre-Chotzen phenotype. Am J Med Genet 2002;110:136. Cinalli G, Renier D, Sebag G, et al. Chronic tonsillar herniation in Crouzon’s and Apert’s syndromes: The role of premature synostosis of the lambdoid suture. J Neurosurg 1995;83:575. Cinalli G, Sainte-Rose C, Kollar EM, et al. Hydrocephalus and craniosynostosis. J Neurosurg 1998;88:209. Clark M, Carr L, Reilly S, et al. Worster-Drought syndrome, a mild tetraplegic perisylvian cerebral palsy: Review of 47 cases. Brain 2000;123:2160. Clarke RA, Catalan G, Diwan AD, et al. Heterogeneity in Klippel-Feil syndrome: A new classification. Pediatr Radiol 1998;28:967. Clarke RA, Kearsley JH, Walsh DA. Patterned expression in familial KlippelFeil syndrome. Teratology 1996;53:152. Clarke RA, Singh S, McKenzie H, et al. Familial Klippel-Feil syndrome and paracentric inversion inv(8)(q22.2q23.3). Am J Hum Genet 1995;57:1364. Clarren SK, Alvord EC Jr, Sumi SM, et al. Brain malformations related to prenatal exposure to ethanol. J Pediatr 1978;92:64. Clauser L, Galie M, Hassanipour A, et al. Saethre-Chotzen syndrome: Review of the literature and report of a case. J Craniofac Surg 2000;11:480. Clewell WH, Johnson ML, Meier PR, et al. A surgical approach to the treatment of fetal hydrocephalus. N Engl J Med 1982;306:1320. Cobourne MT. Construction for the modern head: Current concepts in craniofacial development. J Orthod 2000;27:307. Cobourne MT. The complex genetics of cleft lip and palate. Eur J Orthod 2004;26:7. Cochrane DD, Wilson RD, Steinbok P, et al. Prenatal spinal evaluation and functional outcome of patients born with myelomeningocele: Information for improved prenatal counselling and outcome prediction. Fetal Diagn Ther 1996;11:159. Codero D, Marcucio R, Hu D, et al. Temporal perturbations in Sonic hedgehog signaling elicit the spectrum of holoprosencephaly phenotypes. J Clin Invest 2004;114:485. Coffman JA. Runx transcription factors and the developmental balance between cell proliferation and differentiation. Cell Biol Int 2003;27:315. Cohen DM, Green JG, Miller J, et al. Acrocephalopolysyndactyly type II—Carpenter syndrome: Clinical spectrum and an attempt at unification with Goodman and Summitt syndromes. Am J Med Genet 1987;28:311. Cohen ME, Rosenthal AD, Matson DD. Neurological abnormalities in achondroplastic children. J Pediatr 1967;71:367. Cohen MM Jr. Pfeiffer syndrome update, clinical subtypes, and guidelines for differential diagnosis. Am J Med Genet 1993;45:300. Cohen MM Jr. Malformations of the craniofacial region: Evolutionary, embryonic, genetic, and clinical perspectives. Am J Med Genet 2002;115:245. Cohen MM Jr, Barone CM. Reply to Dr. Winter. Am J Med Genet 1994;49:358. Cohen MM Jr, Kreiborg S. The central nervous system in the Apert syndrome. Am J Med Genet 1990;35:36. Cohen MM Jr, Lemire RJ. Syndromes with cephaloceles. Teratology 1982;25:161. Cohen MM Jr, Toriello HV. Is there a Baller-Gerold syndrome? Am J Med Genet 1996;61:63. Cohen MM. Craniosynostosis update 1987. Am J Med Genet 1988;4 (Suppl):99. Cohen MM. Perspectives on holoprosencephaly. I. Epidemiology, genetics, and syndromology. Teratology 1989a;40:211. Cohen MM. Perspectives on holoprosencephaly: Part III. Spectra, distinctions, continuities, and discontinuities. Am J Med Genet 1989b;34:271.
473
Cohen MM. Craniosynostosis: Diagnosis, evaluation and management. Cary, NC: Oxford University Press, 2000. Cohen SR, Persing JA. Intracranial pressure in single-suture craniosynostosis. Cleft Palate Craniofac J 1998;35:194. Cohen T, Zeitune M, McGillivray BC, et al. Segregation analysis of microcephaly. Am J Med Genet 1996;65:226. Coker S. Bobble-head doll syndrome due to trapped fourth ventricle and aqueduct. Pediatr Neurol 1986;2:115. Colacitti C, Sancini G, DeBiasi S, et al. Prenatal methylazoxymethanol treatment in rats produces brain abnormalities with morphological similarities to human developmental brain dysgeneses. J Neuropathol Exp Neurol 1999;58:92. Cole WG. The Nicholas Andry Award—1996. The molecular pathology of osteogenesis imperfecta. Clin Orthop 1997;343:235. Collmann H, Sorensen N, Krauss J. Consensus: Trigonocephaly. Childs Nerv Syst 1996;12:664. Colombo N, Citterio A, Galli C, et al. Neuroimaging of focal cortical dysplasia: Neuropathological correlations. Epileptic Disord 2003a;5 (Suppl 2):S67. Colombo N, Tassi L, Galli C, et al. Focal cortical dysplasias: MR imaging, histopathologic, and clinical correlations in surgically treated patients with epilepsy. AJNR Am J Neuroradiol 2003b;24:724. Colvin JS, Bohne BA, Harding GW, et al. Skeletal overgrowth and deafness in mice lacking fibroblast growth factor receptor 3. Nat Genet 1996;12:390. Connolly JP, Gruss J, Seto ML, et al. Progressive postnatal craniosynostosis and increased intracranial pressure. Plast Reconstr Surg 2004;113:1313. Cooper SC, Flaitz CM, Johnston DA, et al. A natural history of cleidocranial dysplasia. Am J Med Genet 2001;104:1. Corsello G, Giuffre M. Osteodysplastic primordial dwarfism (ODPD): Notes on brain imaging. Am J Med Genet 1998;80:90. Cowan WM. Development of the nervous system. In: Asbury AK, McKhann GM, McDonald WI, eds. Diseases of the nervous system, clinical neurobiology. Philadelphia: WB Saunders, 1992. Cowan WM, Jessell TM, Zipursky SL, eds. Molecular and cellular approaches to neural development. New York: Oxford University Press, 1997. Cox TC. Taking it to the max: The genetic and developmental mechanisms coordinating midfacial morphogenesis and dysmorphology. Clin Genet 2004;65:163. Cragun DL, Trumpy SK, Shackleton CH, et al. Undetectable maternal serum uE3 and postnatal abnormal sterol and steroid metabolism in Antley-Bixler syndrome. Am J Med Genet A 2004;129:1. Crandall BF, Chua C. Detecting neural tube defects by amniocentesis between 11 and 15 weeks’ gestation. Prenat Diagn 1995;15:339. Crino PB, Miyata H, Vinters HV. Neurodevelopmental disorders as a cause of seizures: Neuropathologic, genetic, and mechanistic considerations. Brain Pathol 2002;12:212. Croen LA, Shaw GM, Lammer EJ. Holoprosencephaly: Epidemiologic and clinical characteristics of a California population. Am J Med Genet 1996;64:465. Croen LA, Shaw GM, Lammer EJ. Risk factors for cytogenetically normal holoprosencephaly in California: A population-based case-control study. Am J Med Genet 2000;90:320. Crome L. Microgyria. J Pathol Bacteriol 1952;64:479. Crome L. Pachygyria. J Pathol Bacteriol 1956;71:335. Cupo LN, Pyeritz RE, Olson JL, et al. Ehlers-Danlos syndrome with abnormal collagen fibrils, sinus of Valsalva aneurysms, myocardial infarction, panacinar emphysema and cerebral heterotopia. Am J Med 1981;71:1051. Cure JK, Key LL, Goltra DD, et al. Cranial MR imaging of osteopetrosis. AJNR Am J Neuroradiol 2000;21:1110. Currier SC, Lee CK, Chang BS, et al. Mutations in POMT1 are found in a minority of patients with Walker-Warburg syndrome. Am J Med Genet A 2005;133:53. Cutting LE, Cooper KL, Koth CW, et al. Megalencephaly in NF1: Predominantly white matter contribution and mitigation by ADHD. Neurology 2002;59:1388. Czeizel AE, Dudas I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N Engl J Med 1992;327:1832. Dabora SL, Jozwiak S, Franz DN, et al. Mutational analysis in a cohort of 224 tuberous sclerosis patients indicates increased severity of TSC2, compared with TSC1, disease in multiple organs. Am J Hum Genet 2001;68:64. D’Agostino MD, Bastos A, Piras C, et al. Posterior quadrantic dysplasia or hemi-hemimegalencephaly: A characteristic brain malformation. Neurology 2004;62:2214. D’Agostino MD, Bernasconi A, Das S, et al. Subcortical band heterotopia (SBH) in males: Clinical, imaging and genetic findings in comparison with females. Brain 2002;125:2507.
474
Perinatal Acquired and Congenital Neurologic Disorders / 19
Daly LE, Kirke PN, Molloy A, et al. Folate levels and neural tube defects. Implications for prevention. JAMA 1995;274:1698. Dandy WE, Blackfan KD. Internal hydocephalus: An experimental, clinical, and pathological study. Am J Dis Child 1914;8:406. D’Angelo V, Gorgoglione L, Catapano G. Treatment of symptomatic intracranial arachnoid cysts by stereotactic cyst-ventricular shunting. Stereotact Funct Neurosurg 1999;72:62. D’Arcangelo G, Miao GG, Chen SC, et al. A protein related to extracellular matrix proteins deleted in the mouse mutant reeler. Nature 1995;374:719. Das BB, Rajegowda BK, Bainbridge R, Giampietro PF. Caudal regression syndrome versus sirenomelia: A case report. J Perinatol 2002;22:168. DaSilva MC, Drake JM. Complications of cerebrospinal fluid shunt antisiphon devices. Pediatric Neurosurg 1991;17:304. Dattani MT, Martinez-Barbera JP, Thomas PQ, et al. Mutations in the homeobox gene HESX1/Hesx1 associated with septo-optic dysplasia in human and mouse. Nat Genet 1998;19:125. David DJ. Cephaloceles: Classification, pathology, and management—a review. J Craniofac Surg 1993;4:192. David DJ, Menard RM. Occipital plagiocephaly. Br J Plast Surg 2000;53:367. David DJ, White J, Sprod R, Bagnall A. Nasendoscopy: Significant refinements of a direct-viewing technique of the velopharyngeal sphincter. Plast Reconstr Surg 1982;70:423. David LR, Velotta E, Weaver RG Jr, et al. Clinical findings precede objective diagnostic testing in the identification of increased ICP in syndromic craniosynostosis. J Craniofac Surg 2002;13:676. David LR, Wilson JA, Watson NE, et al. Cerebral perfusion defects secondary to simple craniosynostosis. J Craniofac Surg 1996;7:177. Davidoff AM, Thompson CV, Grimm JM, et al. Occult spinal dysraphism in patients with anal agenesis. J Pediatr Surg 1991;26:1001. Davila-Gutierrez G. Agenesis and dysgenesis of the corpus callosum. Semin Pediatr Neurol 2002;9:292. Davson H. Dynamic aspects of cerebrospinal fluid. Dev Med Child Neurol 1972;14 (Suppl 6):1. De Heer IM, Hoogeboom AJ, Eussen HJ, et al. Deletion of the TWIST gene in a large five-generation family. Clin Genet 2004a;65:396. De Heer IM, Hoogeboom J, Vermeij-Keers C, et al. Postnatal onset of craniosynostosis in a case of Saethre-Chotzen syndrome. J Craniofac Surg 2004b;15:1048. De Moerlooze L, Dickson C. Skeletal disorders associated with fibroblast growth factor receptor mutations. Curr Opin Genet Dev 1997;7:378. de Oliveira RS, Lajeunie E, Arnaud E, et al. Baller-Gerold syndrome after fetal exposure to sodium valproate. Am J Med Genet A 2005;134:113. de Rijk-van Andel JF, Arts WFM, Hofman A, et al. Epidemiology of lissencephaly type I. Neuroepidemiology 1991;10:200. De Robertis EM, Kuroda H. Dorsal-ventral patterning and neural induction in Xenopus embryos. Annu Rev Cell Dev Biol 2004;20:285. de Sanctis C, Lala R, Matarazzo P, et al. McCune-Albright syndrome: A longitudinal clinical study of 32 patients. J Pediatr Endocrinol Metab 1999;12:817. De Volder AG, Michel C, Thauvoy C, et al. Brain glucose utilisation in acquired childhood aphasia associated with a sylvian arachnoid cyst: Recovery after shunting as demonstrated by PET. J Neurol Neurosurg Psychiatry 1994;57:296. Deconinck N, Duprez T, des Portes V, et al. Familial bilateral medial parietooccipital band heterotopia not related to DCX or LIS1 gene defects. Neuropediatrics 2003;34:146. DeFelipe J, Garcia Sola R, Marco P, et al. Selective changes in the microorganization of the human epileptogenic neocortex revealed by parvalbumin immunoreactivity. Cereb Cortex 1993;3:39. Dekaban AS, Priestly BL. Megalencephaly. In: Vinken PJ, Bruyn G, eds. Handbook of clinical neurology. Amsterdam: North Holland, 1977, p 647. Dekaban AS. Abnormalities in children exposed to x-radiation during various stages of gestation: Tentative timetable of radiation injury to the human fetus. I. J Nucl Med 1968;9:471. Del Bigio MR. Cellular damage and prevention in childhood hydrocephalus. Brain Pathol 2004;14:317. Del Rio JA, Martinez A, Auladell C, et al. Developmental history of the subplate and developing white matter in the murine neocortex. Neuronal organization and relationship with the main afferent systems at embryonic and perinatal stages. Cereb Cortex 2000;10:784. Delague V, Bareil C, Bouvagnet P, et al. A new autosomal recessive non-progressive congenital cerebellar ataxia associated with mental retardation, optic atrophy, and skin abnormalities (CAMOS) maps to chromosome 15q24-q26 in a large consanguineous Lebanese Druze Family. Neurogenetics 2002;4:23.
Delague V, Bareil C, Bouvagnet P, et al. Nonprogressive autosomal recessive ataxia maps to chromosome 9q34-9qter in a large consanguineous Lebanese family. Ann Neurol 2001;50:250. Demelas L, Serra G, Conti M, et al. Incomplete penetrance with normal MRI in a woman with germline mutation of the DCX gene. Neurology 2001;57:327. Demenais F, Le Merrer M, Briard ML, Elston RC. Neural tube defects in France: Segregation analysis. Am J Med Genet 1982;11:287. DeMyer W. Megalencephaly in children. Clinical syndromes, genetic patterns, and differential diagnosis from other causes of megalocephaly. Neurology 1972;22:634. DeMyer W. Megalencephaly: Types, clinical syndromes, and management. Pediatr Neurol 1986;2:321. DeMyer W. Microcephaly, micrencephaly, megalocephaly and megalencephaly. In: Swaiman KF, ed. Pediatric neurology. St. Louis: Mosby, 1999, p 301. DeMyer W, Zeman W. Alobar holoprosencephaly (arhinenecephaly) with median cleft lip and palate: Clinical, nosologic, and electroencephalographic considerations. Confin Neurol 1963;23:1. DeMyer W, Zeman W, Palmer CG. The face predicts the brain: Diagnostic significance of median facial anomalies for holoprosencephaly (arhinencephaly). Pediatrics 1964;34:256. Denis D, Genitori L, Bardot J, et al. Ocular findings in trigonocephaly. Graefes Arch Clin Exp Ophthalmol 1994;232:728. Dennis M, Fitz CR, Netley CT, et al. The intelligence of hydrocephalic children. Arch Neurol 1981;38:607. des Portes V, Boddaert N, Sacco S, et al. Specific clinical and brain MRI features in mentally retarded patients with mutations in the Oligophrenin-1 gene. Am J Med Genet A 2004;124:364. des Portes V, Pinard JM, Smadja D, et al. Dominant X linked subcortical laminar heterotopia and lissencephaly syndrome (XSCLH/LIS): Evidence for the occurrence of mutation in males and mapping of a potential locus in xq22. J Med Genet 1997;34:177. Devi AS, Eisenfeld L, Uphoff D, et al. New syndrome of hydrocephalus, endocardial fibroelastosis, and cataracts (HEC syndrome). Am J Med Genet 1995;56:62. Devlin AM, Cross JH, Harkness W, et al. Clinical outcomes of hemispherectomy for epilepsy in childhood and adolescence. Brain 2003;126:556. Dhooge I, Lantsoght B, Lemmerling M, et al. Hearing loss as a presenting symptom of cleidocranial dysplasia. Otol Neurotol 2001;22:855. Dias MS, Klein DM. Occipital plagiocephaly: Deformation or lambdoid synostosis? II. A unifying theory regarding pathogenesis. Pediatr Neurosurg 1996;24:69. Dias MS, Pang D. Split cord malformations. Neurosurg Clin North Am 1995;6:339. Dickett S, ed. Pediatric neuropathology. Baltimore: Williams & Wilkins, 1995. Diesen C, Saarinen A, Pihko H, et al. POMGNT1 mutation and phenotype spectrum in muscle-eye-brain disease. J Med Genet 2004;41:e115. DiMario FJ Jr, Ramsby GR, Burleson JA, et al. Brain morphometric analysis in achondroplasia. Neurology 1995;45:519. Dimeglio LA, Ford L, McClintock C, et al. A comparison of oral and intravenous bisphosphonate therapy for children with osteogenesis imperfecta. J Pediatr Endocrinol Metab 2005;18:43. DiMeglio LA, Pescovitz OH. Disorders of puberty: Inactivating and activating molecular mutations. J Pediatr 1997;131:S8. Dixon-Salazar T, Silhavy JL, Marsh SE, et al. Mutations in the AHI1 gene, encoding jouberin, cause Joubert syndrome with cortical polymicrogyria. Am J Hum Genet 2004;75:979. Dobyns WB. Primary microcephaly: New approaches for an old disorder. Am J Med Genet 2002;112:315. Dobyns WB, Barkovich AJ. Microcephaly with simplified gyral pattern (oligogyric microcephaly) and microlissencephaly: Reply. Neuropediatr 1999;30:104. Dobyns WB, Truwit CL. Lissencephaly and other malformations of cortical development: 1995 update. Neuropediatr 1995;26:132. Dobyns WB, Andermann E, Andermann F, et al. X-linked malformations of neuronal migration. Neurology 1996a;47:331. Dobyns WB, Berry-Kravis E, Havernick NJ, et al. X-linked lissencephaly with absent corpus callosum and ambiguous genitalia. Am J Med Genet 1999a;86:331. Dobyns WB, Curry CJR, Hoyme HE, et al. Clinical and molecular diagnosis of Miller-Dieker syndrome. Am J Hum Genet 1991;48:584. Dobyns WB, Elias ER, Newlin AC, et al. Causal heterogeneity in isolated lissencephaly. Neurology 1992;42:1375.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Dobyns WB, Filauro A, Tomson BN, et al. Inheritance of most X-linked traits is not dominant or recessivve, just X-linked. Am J Med Genet 2004;129A:136. Dobyns WB, Guerrini R, Czapansky-Beilman DK, et al. Bilateral periventricular nodular heterotopia (BPNH) with mental retardation and syndactyly in boys: A new X-linked mental retardation syndrome. Neurology 1997;49:1042. Dobyns WB, Kirkpatrick JB, Hittner HM, et al. Syndromes with lissencephaly. II: Walker-Warburg and cerebro-oculo-muscular syndromes and a new syndrome with type II lissencephaly. Am J Med Genet 1985;22:157. Dobyns WB, Pagon RA, Armstrong D, et al. Diagnostic criteria for WalkerWarburg syndrome. Am J Med Genet 1989;32:195. Dobyns WB, Patton MA, Stratton RF, et al. Cobblestone lissencephaly with normal eyes and muscle. Neuropediatrics 1996b;27:70. Dobyns WB, Stratton RF, Greenberg F. Syndromes with lissencephaly. I: Miller-Dieker and Norman-Roberts syndromes and isolated lissencephaly. Am J Med Genet 1984;18:509. Dobyns WB, Truwit CL, Ross ME, et al. Differences in the gyral pattern distinguish chromosome 17–linked and X-linked lissencephaly. Neurology 1999b;53:270. Docherty TB, Herbaut AG, Sedgwick EM. Brainstem auditory-evoked potential abnormalities in myelomeningocele in the older child. J Neurol Neurosurg Psychiatry 1987;50:1318. Dodge NN, Dobyns WB. Agenesis of the corpus callosum and Dandy-Walker malformation associated with hemimegalencephaly in the sebaceous nevus syndrome. Am J Med Genet 1995;56:147. Dolk H. The predictive value of microcephaly during the first year of life for mental retardation at seven years. Dev Med Child Neurol 1991;33:974. Domingo Z, Peter J. Midline developmental abnormalities of the posterior fossa: Correlation of classification with outcome. Pediatr Neurosurg 1996;24:111. Donahue LR, Cook SA, Johnson KR, et al. Megencephaly: A new mouse mutation on chromosome 6 that causes hypertrophy of the brain. Mamm Genome 1996;7:871. Donaldson JW, Edwards-Brown M, et al. Arachnoid cyst rupture with concurrent subdural hygroma. Pediatr Neurosurg 2000;32:137 Donnenfeld AE, Packer RJ, Zackai EH, et al. Clinical, cytogenetic, and pedigree findings in 18 cases of Aicardi syndrome. Am J Med Genet 1989;32:461. Doolin MT, Barbaux S, McDonnell M, et al. Maternal genetic effects, exerted by genes involved in homocysteine remethylation, influence the risk of spina bifida. Am J Hum Genet 2002;71:1222. Drachman DA, Richardson EP. Aqueductal narrowing, congenital and acquired: A critical review of the histologic criteria. Arch Neurol 1961;5:552. Drake JM, Kestle J. Rationale and methodology of the Multicenter Pediatric Cerebrospinal Fluid Shunt Design trial. Pediatric Hydrocephalus Treatment Evaluation Group. Childs Nerv Syst 1996;12:434. Drake JM. Ventriculostomy for treatment of hydrocephalus. Neurosurg Clin N Am 1993;4:657. Drugan A, Weissman A, Evans MI. Screening for neural tube defects. Clin Perinatol 2001;28:279. Dubeau F, Tampieri D, Lee N, et al. Periventricular and subcortical nodular heterotopia: A study of 33 patients. Brain 1995;118:1273. Dubey SP, Ghosh LM. Klippel-Feil syndrome with congenital conductive deafness: Report of a case and review of literature. Int J Pediatr Otorhinolaryngol 1993;25:201. Dubourg C, Lazaro L, Pasquier L, et al. Molecular screening of SHH, ZIC2, SIX3, and TGIF genes in patients with features of holoprosencephaly spectrum: Mutation review and genotype-phenotype correlations. Hum Mut 2004;24:43. Dubowitz V. 22nd ENMC sponsored workshop on congenital muscular dystrophy held in Baarn, The Netherlands, 14-16 May 1993. Neuromusc Disord 1994;4:75. Duc G, Largo RH. Anterior fontanel: Size and closure in term and preterm infants. Pediatrics 1986;78:904. Dunac A, Van Bogaert P, David P, et al. Mid-portion agenesis of corpus callosum in a presumed Baller-Gerold syndrome. Neuropediatrics 1995;26:273. Dykes FD, Dunbar B, Lazarra A, et al. Posthemorrhagic hydrocephalus in high risk infants: Natural history, management and long-term outcome. J Pediatr 1989;114:611. Dyste GN, Menezes AH. Presentation and management of pediatric Chiari malformations without myelodysplasia. Neurosurgery 1988;23:589. Dyste GN, Menezes AH, VanGilder JC. Symptomatic Chiari malformations. An analysis of presentation, management, and long-term outcome. J Neurosurg 1989;71:159.
475
Edwards JH. The syndrome of sex-linked hydrocephalus. Arch Dis Child 1961;36:486. Edwards TJ, David DJ, Martin J. Aggressive surgical management of sleep apnea syndrome in the syndromal craniosynostoses. J Craniofac Surg 1992;3:8. Ehara H, Maegaki Y, Takeshita K. Pachygyria and polymicrogyria in 22q11 deletion syndrome. Am J Med Genet 2003;117A:80. Eksioglu YZ, Scheffer IE, Cardenas P, et al. Periventricular heterotopia: An X-linked dominant epilepsy locus causing aberrant cerebral cortical development. Neuron 1996;16:77. El Ghouzzi V, Le Merrer M, Perrin-Schmitt F, et al. Mutations of the TWIST gene in the Saethre-Chotzen syndrome. Nat Genet 1997;15:42. Elia M, Musumeci SA, Ferri R, et al. Saethre-Chotzen syndrome: A clinical, EEG and neuroradiological study. Childs Nerv Syst 1996;12:699. Ellenbogen RG, Gruss JS, Cunningham ML. Update on craniofacial surgery: The differential diagnosis of lambdoid synostosis/posterior plagiocephaly. Clin Neurosurg 2000;47:303. Emery JA, Roper SN, Rojiani AM. White matter neuronal heterotopia in temporal lobe epilepsy: A morphometric and immunohistochemical study. J Neuropathol Exp Neurol 1997;56:1276. Elster AD, Theros EG, Key LL, Chen MY. Cranial imaging in autosomal recessive osteopetrosis. Part II. Skull base and brain. Radiology 1992;183:137. Emery SC, Karpinski NC, Hansen L, Masliah E. Abnormalities in central nervous system development in osteogenesis imperfecta type II. Pediatr Dev Pathol 1999;2:124. Eng C. Will the real Cowden syndrome please stand up: Revised diagnostic criteria. J Med Genet 2000;37:828. Engelbert RH, Uiterwaal CS, Gerver WJ, et al. Osteogenesis imperfecta in childhood: Impairment and disability. A prospective study with 4-year follow-up. Arch Phys Med Rehabil 2004;85:772. Engelbert RHH, van der Graaf Y, van Empelen R, et al. Osteogenesis imperfecta in childhood: Impairment and disability. Pediatrics 1997;99:E3. Englund C, Fink A, Lau C, et al. Pax6, tbr2, and tbr1 are expressed sequentially by radial glia, intermediate progenitor cells, and postmitotic neurons in developing neocortex. J Neurosci 2005;25:247. Ensink RJ, Marres HA, Brunner HG, et al. Hearing loss in the Saethre-Chotzen syndrome. J Laryngol Otol 1996;110:952. Epstein CJ, Erickson RF, Boris AW. Inborn errors of development: The molecular basis of morphogenesis. New York: Oxford University Press, 2004. Erdincler P, Dashti R, Kaynar MY, et al. Hydrocephalus and chronically increased intracranial pressure in achondroplasia. Childs Nerv Syst 1997;13:345. Ersahin Y, Mutluer S, Tekeli G. Abdominal cerebrospinal fluid pseudocysts. Childs Nerv Syst 1996;12:755. Estin D, Cohen AR. Caudal agenesis and associated caudal spinal cord malformations. Neurosurg Clin North Am 1995;6:377. Evans PD, Anderson JR, Vallender EJ, et al. Reconstructing the evolutionary history of microcephalin, a gene controlling human brain size. Hum Mol Genet 2004a;13:1139. Evans PD, Anderson JR, Vallender EJ, et al. Adaptive evolution of ASPM, a major determinant of cerebral cortical size in humans. Hum Mol Genet 2004b;13:489. Evrard P, de Saint-Georges. P, Kadhim HJ, et al. Pathology of prenatal encephalopathies. In: French J, ed. Child neurology and developmental disabilities. Baltimore: Paul H. Brookes, 1989, p 153. Evrard P. Normal and abnormal development of the brain. In: Rapin I, Segalowitz S, eds. Handbook of neuropsychology. Amsterdam: Elsevier, 1992, p 11. Fagiolini M, Hensch TK. Inhibitory threshold for critical-period activation in primary visual cortex. Nature 2000;404:183. Faiella A, Brunelli S, Granata T, et al. A number of schizencephaly patients including 2 brothers are heterozygous for germline mutations in the homeobox gene EMX2. Eur J Hum Genet 1997;5:186. Faivre L, Le Merrer M, Lyonnet S, et al. Clinical and genetic heterogeneity of Seckel syndrome. Am J Med Genet 2002;112:379. Fantes J, Ragge NK, Lynch SA, et al. Mutations in SOX2 cause anophthalmia. Nat Genet 2003;33:461. Farah S, Sabry MA, Khuraibet A, et al. Lissencephaly associated with cerebellar hypoplasia and myoclonic epilepsy in a Bedouin kindred: A new syndrome? Clin Genet 1997;51:326. Fargnoli MC, Orlow SJ, Semel-Concepcion J, et al. Clinicopathologic findings in the Bannayan-Riley-Ruvalcaba syndrome. Arch Dermatol 1996;132:1214. Farmer SF, Ingram DA, Stephens JA. Mirror movements studied in a patient with Klippel-Feil syndrome. J Physiol Lond 1990;428:467.
476
Perinatal Acquired and Congenital Neurologic Disorders / 19
Fearon JA, Swift DM, Bruce DA. New methods for the evaluation and treatment of craniofacial dysostosis-associated cerebellar tonsillar herniation. Plast Reconstr Surg 2001;108:1855. Feinberg DA. Functional magnetic resonance imaging. Application to degenerative brain disease and hydrocephalus. Neuroimaging Clin N Am 1995;5:125. Feinberg DA, Mark AS. Human brain motion and cerebrospinal fluid circulation demonstrated with MR velocity imaging. Radiology 1987;163:793. Felder B, Stegmann K, Schultealbert A, et al. Evaluation of BMP4 and its specific inhibitor NOG as candidates in human neural tube defects (NTDs). Eur J Hum Genet 2002;10:753. Feltes CH, Fountas KN, Dimopoulos VG., et al. Cervical meningocele in association with spinal abnormalities. Childs Nerv Syst 2004;20:357. Ferguson MWJ. A hole in the head. Nat Genet 2000;24:330. Ferlini A, Ragno M, Gobbi P, et al. Hydrocephalus, skeletal anomalies, and mental disturbances in a mother and three daughters: A new syndrome. Am J Med Genet 1995;59:506. Ferrer I. A Golgi analysis of unlayered polymicrogyria. Acta Neuropathol 1984;65:69. Ferrie CD, Jackson GD, Giannakodimos S, et al. Posterior agyria-pachygyria with polymicrogyria: Evidence for an inherited neuronal migration disorder. Neurology 1995;45:150. Fewel ME, Levy ML, McComb JG. Surgical treatment of 95 children with 102 intracranial arachnoid cysts. Pediatr Neurosurg 1996;25:165. Fiedler R, Krieger DT. Endocrine disturbances in patients with congenital aqueductal stenosis. Acta Endocrinol 1975;80:1. Filly RA, Chinn DH, Callen PW. Alobar holoprosencephaly: Ultrasonographic prenatal diagnosis. Radiology 1984;151:455. Fioravanti A, Godano U, Consales A, et al. Bobble-head doll syndrome due to a suprasellar arachnoid cyst: Endoscopic treatment in two cases. Childs Nerv Syst 2004;20:770. Fisher NL, Smith DW. Occipital encephalocele and early gestational hyperthermia. Pediatrics 1981;68:480. Fishman RA. Cerebrospinal fluid in diseases of the nervous system. Philadelphia: WB Saunders, 1980. Flannery DB, Kahler SG. Neural tube defects in trisomy 18. Prenat Diagn 1986;6:97. Fletcher JM, Bohan TP, Brandt ME, et al. Cerebral white matter and cognition in hydrocephalic children. Arch Neurol 1992;49:818. Fletcher JM, Bohan TP, Brandt ME, et al. Morphometric evaluation of the hydrocephalic brain: Relationships with cognitive development. Childs Nerv Syst 1996;12:192. Fletcher JM, Brookshire BL, Landry SH, et al. Behavioral adjustment of children with hydrocephalus: Relationships with etiology, neurological, and family status. J Pediatr Psychol 1995;20:109. Flores-Sarnat L. Hemimegalencephaly: Part 1. Genetic, clinical, and imaging aspects. J Child Neurol 2002;17:373. Flores-Sarnat L. New insights into craniosynostosis. Semin Pediatr Neurol 2002;9:274. Flores-Sarnat L, Sarnat HB, Davila-Gutierrez G, et al. Hemimegalencephaly: Part 2. Neuropathology suggests a disorder of cellular lineage. J Child Neurol 2003;18:776. Flynn JM, Herrera-Soto JA, Ramirez NF, et al. Clubfoot release in myelodysplasia. J Pediatr Orthop B 2004;13:259. Forrester MB, Merz RD. Epidemiology of holoprosencephaly in Hawaii, 1986-97. Paediatr Perinat Epidemiol 2000;14:61. Fouyas IP, Casey AT, Thompson D, et al. Use of intracranial pressure monitoring in the management of childhood hydrocephalus and shunt-related problems. Neurosurgery 1996;38:726. Fox JW, Lamperti ED, Eksioglu YZ, et al. Mutations in filamin 1 prevent migration of cerebral cortical neurons in human periventricular heterotopia. Neuron 1998;21:1315. Francis-West PH, Robson L, Evans DJ. Craniofacial development: The tissue and molecular interactions that control development of the head. Adv Anat Embryol Cell Biol 2003;169:III. Fransen E, Lemmon V, Van Camp G, et al. CRASH syndrome: Clinical spectrum of corpus callosum hypoplasia, retardation, adducted thumbs, spastic paraparesis and hydrocephalus due to mutations in one single gene, L1. Eur J Hum Genet 1995;3:273. Fransen E, Van Camp G, D’Hooge R, et al. Genotype-phenotype correlation in L1 associated diseases. J Med Genet 1998;35:399. Fransen E, Van Camp G, Vits L, Willems, PJ. L1-associated diseases: Clinical geneticists divide, molecular geneticists unite. Hum Mol Genet 1997;6:1625. Friede RL. Developmental neuropathology. New York: Springer-Verlag, 1989.
Friede RL, Roessmann U. Chronic tonsillar herniation: An attempt at classifying chronic hernitations at the foramen magnum. Acta Neuropathol (Berl) 1976;34:219. Frieden IJ, Reese V, Cohen D. PHACE syndrome. The association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol 1996;132:307. Frigoletto FD, Birnholza JC, Greene MF. Antenatal treatment of hydrocephalus by ventriculoamniotic shunting. JAMA 1982;248:2496. Fujisawa H, Hasegawa M, Kida S, et al. A novel fibroblast growth factor receptor 2 mutation in Crouzon syndrome associated with Chiari type I malformation and syringomyelia. J Neurosurg 2002;97:396. Fujiwara I, Ogawa E, Igarashi Y, et al. Intravenous pamidronate treatment in osteogenesis imperfecta. Eur J Pediatr 1998;157:261. Fukami M, Horikawa R, Nagai T, et al. Cytochrome P450 oxidoreductase gene mutations and Antley-Bixler syndrome with abnormal genitalia and/or impaired steroidogenesis: Molecular and clinical studies in 10 patients. J Clin Endocrinol Metab 2005;90:414. Fukushima Y, Ohashi H, Wakui K, et al. De novo apparently balanced reciprocal translocation between 5q11.2 and 17q23 associated with Klippel-Feil anomaly and type A1 brachydactyly. Am J Med Genet 1995;57:447. Fukuyama Y, Osawa M. A genetic study of the Fukuyama type congenital muscular dystrophy. Brain Dev 1984;6:373. Fukuzawa R, Sato S, Sullivan MJ, et al. Autopsy case of microcephalic osteodysplastic primordial “dwarfism” type II. Am J Med Genet 2002;113:93. Ganesh A, Jenny C, Geyer J, et al. Retinal hemorrhages in type I osteogenesis imperfecta after minor trauma. Ophthalmology 2004;111:1428. Garcia-Minaur S, Mavrogiannis LA, Rannan-Eliya SV, et al. Parietal foramina with cleidocranial dysplasia is caused by mutation in MSX2. Eur J Hum Genet 2003;11:892. Garretsen AJ, Cremers CW, Huygen PL. Hearing loss (in nonoperated ears) in relation to age in osteogenesis imperfecta type I. Ann Otol Rhinol Laryngol 1997;106:575. Garton HJ and Piatt JH. Hydrocephalus. Pediatr Clin North Am 2004;51:305. Gault DT, Renier D, Marchac D, et al. Intracranial pressure and intracranial volume in children with craniosynostosis. Plast Reconstr Surg 1992;90:377. Germano A, Caruso G, Caffo M, et al. The treatment of large supratentorial arachnoid cysts in infants with cyst-peritoneal shunting and Hakim programmable valve. Childs Nerv Syst 2003;19:166. Gerritsen EJ, Vossen JM, van Loo IH, et al. Autosomal recessive osteopetrosis: Variability of findings at diagnosis and during the natural course. Pediatrics 1994a;93:247. Gerritsen EJ, Vossen JM, Fasth A, et al. Bone marrow transplantation for autosomal recessive osteopetrosis. A report from the Working Party on Inborn Errors of the European Bone Marrow Transplantation Group. J Pediatr 1994b;125:896. Gerszten PC, Albright AL. Relationship between cerebellar appearance and function in children with Dandy-Walker syndrome. Pediatr Neurosurg 1995;23:86. Ghariani S, Dahan K, Saint-Martin C, et al. Polymicrogyria in chromosome 22q11 deletion syndrome. Eur J Paediatr Neurol 2002;6:73. Gilbert JN, Jones KL, Rorke LB, et al. Central nervous system anomalies associated with meningomyelocele, hydrocephalus, and the Arnold-Chiari malformation: Reappraisal of theories regarding the pathogenesis of posterior neural tube closure defects. Neurosurgery 1986;18:559. Giuliano F, David A, Edery P, et al. Macrocephaly–cutis marmorata telangiectatica congenita: Seven cases including two with unusual cerebral manifestations. Am J Med Genet 2004;126A:99. Glaser RL, Broman KW, Schulman RL, et al. The paternal-age effect in Apert syndrome is due, in part, to the increased frequency of mutations in sperm. Am J Hum Genet 2003;73:939. Glaser RL, Jiang W, Boyadjiev SA, et al. Paternal origin of FGFR2 mutations in sporadic cases of Crouzon syndrome and Pfeiffer syndrome. Am J Hum Genet 2000;66:768. Glaser T, Jepeal L, Edwards JG, et al. PAX6 gene dosage effect in a family with congenital cataracts, aniridia, anophthalmia and central nervous system defects. Nat Genet 1994;7:463. Glat PM, Freund RM, Spector JA, et al. A classification of plagiocephaly utilizing a three-dimensional computer analysis of cranial base landmarks. Ann Plast Surg 1996;36:469. Gleeson JG, Allen KM, Fox JW, et al. Doublecortin, a brain-specific gene mutated in human X-linked lissencephaly and double cortex syndrome, encodes a putative signaling protein. Cell 1998;92:63.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Gleeson JG, Keeler LC, Parisi MA, et al. Molar tooth sign of the midbrain-hindbrain junction: Occurrence in multiple distinct syndromes. Am J Med Genet 2004;125A:125. Gleeson JG, Luo RF, Grant PE, et al. Genetic and neuroradiological heterogeneity of double cortex syndrome. Ann Neurol 2000a;47:265. Gleeson JG, Minnerath S, Kuzniecky RI, et al. Somatic and germline mosaic mutations in the doublecortin gene are associated with variable phenotypes. Am J Hum Genet 2000b;67:574. Godano U, Mascari C, Consales A, et al.. Endoscope-controlled microneurosurgery for the treatment of intracranial fluid cysts. Childs Nerv Syst 2004;20:839. Goh KY, Ahuja A, Fok TF, et al. Cloverleaf skull—when should one operate? Singapore Med J 1997;38:217. Gohlich-Ratmann G, Baethmann M, Lorenz P, et al. Megalencephaly, mega corpus callosum, and complete lack of motor development: A previously undescribed syndrome. Am J Med Genet 1998;79:161. Golden JA. Holoprosencephaly: A defect in brain patterning. J Neuropathol Exp Neurol 1998;57:991. Golden JA, Chernoff GF. Multiple sites of anterior neural tube closure in humans: Evidence from anterior neural tube defects (anencephaly). Pediatrics 1995;95:506. Golden JA, Rorke LB, Bruce DA. Dandy-Walker syndrome and associated anomalies. Pediatr Neurosci 1987;13:38. Goldstein RB, La Pidus AS, Filly RA, et al. Mild lateral cerebral ventricular dilatation in utero: Clinical significance and prognosis. Radiology 1990;176:237. Golla A, Lichmer P, von Gernet S, et al. Phenotypic expression of the fibroblast growth factor receptor 3 (FGFR3) mutation P250R in a large craniosynostosis family. J Med Genet 1997;34:683. Gonchar Y, Burkhalter A. Three distinct families of gabaergic neurons in rat visual cortex. Cereb Cortex 1997;7347. Gordon N. The neurological complications of achondroplasia. Brain Dev 2000;22:3. Gorlin RJ. Syndromes of the head and neck, 3rd ed. Cary, NC: Oxford University Press, New York, 1990. Gosain AK, Steele MA, McCarthy JG, et al. A prospective study of the relationship between strabismus and head posture in patients with frontal plagiocephaly. Plast Reconstr Surg 1996;97:881. Gosalakkal JA. Intracranial arachnoid cysts in children: A review of pathogenesis, clinical features, and management. Pediatr Neurol 2002;26:93. Graf CJ, Perret GE. Spontaneous recurrent hemorrhage as an unusual complication of fibrous dysplasia of the skull. J Neurosurg 1980;52:570. Graham D, Johnson TR Jr, Winn K, Sanders RC. The role of sonography in the prenatal diagnosis and management of encephalocele. J Ultrasound Med 1982;1:111. Graham E, Duhl A, Ural S. The degree of antenatal ventriculomegaly is related to pediatric neurological morbidity. J Matern Fetal Med 2001;10:258. Graham JM Jr, Braddock SR, Mortier GR, et al. Syndrome of coronal craniosynostosis with brachydactyly and carpal/tarsal coalition due to Pro250Arg mutation in FGFR3 gene. Am J Med Genet 1998;77:322. Graham JM Jr, Hennekam R, Dobyns WB, et al. Micro syndrome: An entity distinct from COFS syndrome. Am J Med Genet 2004;128A:235. Granata T, Battaglia G, D’Incerti L, et al. Schizencephaly: Clinical findings. In: Guerrini R, Andermannn F, Canapicchi R, et al, eds. Dysplasias of cerebral cortex and epilepsy. Philadelphia: Lippincott-Raven, 1996. Granata T, Battaglia G, D’Incerti L, et al. Schizencephaly: Neuroradiologic and epileptologic findings. Epilepsia 1996;37:1185. Granata T, Farina L, Faiella A, et al. Familial schizencephaly associated with EMX2 mutation. Neurology 1997;48:1403. Greally MT, Carey JC, Milewicz DM, et al. Shprintzen-Goldberg syndrome: A clinical analysis. Am J Med Genet 1998;76:202. Griffith BP, Booss J. Neurologic infections of the fetus and newborn. Neurol Clin 1994;12:541. Gripp KW, McDonald-McGinn DM, Gaudenz K, et al. Identification of a genetic cause for isolated unilateral coronal synostosis: A unique mutation in the fibroblast growth factor receptor 3. J Pediatr 1998;132:714. Gripp KW, Stolle CA, Celle L, et al. TWIST gene mutation in a patient with radial aplasia and craniosynostosis: Further evidence for heterogeneity of Baller-Gerold syndrome. Am J Med Genet 1999;82:170. Gripp KW, Zackai EH, Stolle CA. Mutations in the human TWIST gene. Hum Mutat 2000;15:150. Groninger A, Schaper J, Messing-Juenger M, et al. Subdural hematoma as clinical presentation of osteogenesis imperfecta. Pediatr Neurol 2005;32:140. Gropman AL, Barkovich AJ, Vezina LG, et al. Pediatric congenital bilateral perisylvian syndrome: Clinical and MRI features in 12 patients. Neuropediatrics 1997;28:198.
477
Grosso S, Farnetani MA, Berardi R, et al. Medial temporal lobe dysgenesis in Muenke syndrome and hypochondroplasia. Am J Med Genet A 2003;120:88. Guerreiro MM, Andermann E, Guerrini R, et al. Familial perisylvian polymicrogyria: A new familial syndrome of cortical maldevelopment. Ann Neurol 2000;48:39. Guerrini R, Carrozzo R. Epileptogenic brain malformations: Clinical presentation, malformative patterns and indications for genetic testing. Seizure 2002;11 (Suppl A):532. Guerrini R, Dobyns WB. Bilateral periventricular nodular heterotopia with mental retardation and frontonasal malformation. Neurology 1998;51:499. Guerrini R, Barkovich AJ, Sztriha L, et al. Bilateral frontal polymicrogyria: A newly recognized brain malformation syndrome. Neurology 2000;54:909. Guerrini R, Dubeau F, Dulac O, et al. Bilateral parasagittal parietooccipital polymicrogyria and epilepsy. Ann Neurol 1997;41:65. Guerrini R, Mei D, Sisodiya S, et al. Germline and mosaic mutations of FLN1 in men with periventricular heterotopia. Neurology 2004;63:51. Guerrini R, Sicca F, Parmeggiani L. Epilepsy and malformations of the cerebral cortex. Epileptic Disord 2003;5 (Suppl 2):S9. Guggisberg D, Hadj-Rabia S, Viney C, et al. Skin markers of occult spinal dysraphism in children: A review of 54 cases. Arch Dermatol 2004;140:1109. Guiffre R, Pastore FS, De Santis S. Connatal (fetal) hydrocephalus: An acquired pathology? Childs Nerv Syst 1995;11:97. Guille JT, Miller A, Bowen JR, et al. The natural history of Klippel-Feil syndrome: Clinical, roentgenographic, and magnetic resonance imaging findings at adulthood. J Pediatr Orthop 1995;15:617. Gupta S, Ghose S, Rohatgi M, et al. The optic nerve in children with craniosynostosis. A pre and post surgical evaluation. Doc Ophthalmol 1993;83:271. Gupte G, Mahajan P, Shreenivas VK, et al. Wildervanck syndrome (cervicooculo-acoustic syndrome). J Postgrad Med 1992;38:180. Haga N. Management of disabilities associated with achondroplasia. J Orthop Sci 2004;9:103. Hahn JS, Plawner LL. Evaluation and management of children with holoprosencephaly. Pediatr Neurol 2004;31:79. Haines SJ, Erickson DL, Wirtschaffer JD. Optic nerve decompression for osteopetrosis in early childhood. Neurosurgery 1988;23:470. Hall JG, Flora C, Scott CI Jr, et al. Majewski osteodysplastic primordial dwarfism type II (MOPD II): Natural history and clinical findings. Am J Med Genet 2004;130A:55. Hall JG. The natural history of achondroplasia. In: Nicoletti B, Kopits SE, Ascani E, et al, eds. Human achondroplasia: A multidisciplinary approach. New York: Plenum Press, 1988. Hall-Craggs MA, Harbord MG, Finn JP, et al. Aicardi syndrome: MR assessment of brain structure and myelination. AJNR Am J Neuroradiol 1990;11:532. Haltia M, Leivo I, Somer H, et al. Muscle-eye-brain disease: A neuropathological study. Ann Neurol 1997;41:173. Hamamci N, Hawran S, Biering Sorensen F. Achondroplasia and spinal cord lesion. Three case reports. Paraplegia 1993;31:375. Hamilton RL. Case of the month. May 1996—hydrocephalus in a 9 month old infant. Brain Pathol 1996;6:533. Hann YS, Engelhard H, McLone DG. Abdominal CSF pseudocyst: Clinical features and surgical management. Pediatr Neurosci 1985–86;12:75. Hannon TS, Noonan K, Steinmetz R, et al. Is McCune-Albright syndrome overlooked in subjects with fibrous dysplasia of bone? J Pediatr 2003;142:532. Hansen M, Mulliken JB. Frontal plagiocephaly. Diagnosis and treatment. Clin Plast Surg 1994;21:543. Hansen WF, Rijhsinghani A, Grant S, et al. Prenatal diagnosis of Apert syndrome. Fetal Diagn Ther 2004;19:127. Hanssen AM, Werquin H, Suys E, et al. Cowden syndrome: Report of a large family with macrocephaly and increased severity of signs in subsequent generations. Clin Genet 1993;44:281. Happle R. Mosaicism in human skin. Understanding the patterns and mechanisms. Arch Dermatol 1993;129:1460. Happle R. Dohi memorial lecture. New aspects of cutaneous mosaicism. J Dermatol 2002;29:681. Harbord MG, Boyd S, Hall-Craggs MA, et al. Ataxia, developmental delay and an extensive neuronal migration abnormality in 2 siblings. Neuropediatrics 1990;21:218. Hardiman O, Burke T, Phillips J, et al. Microdysgenesis in resected temporal neocortex: Incidence and clinical significance in focal epilepsy. Neurology 1988;38:1041.
478
Perinatal Acquired and Congenital Neurologic Disorders / 19
Harkey HL, Crockard HA, Stevens JM, et al. The operative management of basilar impression in osteogenesis imperfecta. Neurosurgery 1990;27:782. Harley EH. Pediatric congenital nasal masses. Ear Nose Throat J 1991;70:28. Harris CP, Townsend JJ, Norman MG, et al. Atelencephalic aprosencephaly. J Child Neurol 1994;9:412. Hassed S, Shewmake K, Teo C, et al. Shprintzen-Goldberg syndrome with osteopenia and progressive hydrocephalus. Am J Med Genet 1997;70:450. Hassell S, Butler MG. Antley-Bixler syndrome: Report of a patient and review of literature. Clin Genet 1994;46:372. Ha-Vinh R, Alanay Y, Bank RA, et al. Phenotypic and molecular characterization of Bruck syndrome (osteogenesis imperfecta with contractures of the large joints) caused by a recessive mutation in PLOD2. Am J Med Genet A 2004;131A:115 Hayani A, Suarez CR, Molnar Z, et al. Acute myeloid leukaemia in a patient with Seckel syndrome. J Med Genet 1994;31:148. Hayes M, Parker G, Ell J, Sillence D. Basilar impression complicating osteogenesis imperfecta type IV: The clinical and neuroradiological findings in four cases. J Neurol Neurosurg Psychiatry 1999;66:357. Hayward C, Brock DJ. Fibrillin-1 mutations in Marfan syndrome and other type-1 fibrillinopathies. Hum Mutat 1997;10:415. Hayward JC, Titelbaum DS, Clancy RR, et al. Lissencephaly-pachygyria associated with congenital cytomegalovirus infection. J Child Neurol 1991;6:109. Hecht JT, Thompson NM, Weir T, et al. Cognitive and motor skills in achondroplastic infants: Neurologic and respiratory correlates. Am J Hum Genet 1991;41:208. Heeg M, Broughton NS, Menelaus MB. Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434. Heike C, Seto M, Hing A, et al. Century of Jackson-Weiss syndrome: Further definition of clinical and radiographic findings in “lost” descendants of the original kindred. Am J Med Genet 2001;100:315. Heins N, Malatesta P, Cecconi F, et al. Glial cells generate neurons: The role of the transcription factor pax6. Nat Neurosci 2002;5:308. Hemmer KM, McAlister WH, Marsh JL. Cervical spine anomalies in the craniosynostosis syndromes. Cleft Palate J 1987;24:328. Herman TE, McAlister WH. Inherited diseases of bone density in children. Radiol Clin North Am 1991;28:149. Hernandez-Diaz S, Werler MM, Walker AM, Mitchell AA. Neural tube defects in relation to use of folic acid antagonists during pregnancy. Am J Epidemiol 2001;153:961. Hevner RF, Shi L, Justice N, et al. TBR1 regulates differentiation of the preplate and layer 6. Neuron 2001;29:353. Hewitt JE, Grewal PK. Glycosylation defects in inherited muscle disease. Cell Mol Life Sci 2003;60:251. Hier DB, Wiehl AC. Chronic hydrocephalus associated with short stature and growth hormone deficiency. Ann Neurol 1977;2:246. Hilburger AC, Willis JK, Bouldin E, et al. Familial schizencephaly. Brain Dev 1993;15:234. Hinton DR, Becker LE, Muakkassa KF, et al. Lambdoid synostosis. I. The lambdoid suture: Normal development and pathology of synostosis. J Neurosurg 1984;61:333. Hirano A, Hirano M. Benign cysts in the central nervous system: Neuropathological observations of the cyst walls. Neuropathology 2004;24:1. Hirsch JF, Pierre-Kahn A, Renier D, et al. The Dandy-Walker malformation. A review of 40 cases. J Neurosurg 1984;61:515. Ho KL, Chang CH, Yang SS, et al. Neuropathologic findings in thanatophoric dysplasia. Acta Neuropathol 1984;63:218. Ho NC, Guarnieri M, Brant LJ et al. Living with achondroplasia: Quality of life evaluation following cervico-medullary decompression. Am J Med Genet A 2004;131A:163. Hockley AD, Goldin JH, Wake MJ. Management of anterior encephalocele. Childs Nerv Syst 1990;6:444. Hoefkens MF, Vermeij-Keers C, Vaandrager JM. Crouzon syndrome: Phenotypic signs and symptoms of the postnatally expressed subtype. J Craniofac Surg 2004;15:233. Hollway GE, Suthers GK, Battese KM, et al. Deafness due to Pro250Arg mutation of FGFR3. Lancet 1998;351:877. Holroyd S, Reiss AL, Bryan RN. Autistic features in Joubert syndrome: A genetic disorder with agenesis of the cerebellar vermis. Biol Psychiatry 1991;29:287. Honein MA, Paulozzi LJ, Mathews TJ, et al. Impact of folic acid fortification of the US food supply on the occurrence of neural tube defects. JAMA 2001;285:2981. Hong SE, Shugart YY, Huang DT, et al. Autosomal recessive lissencephaly with cerebellar hypoplasia is associated with human Reln mutations. Nat Genet 2000;26:93.
Hori A, Tamagawa K, Eber SW, et al. Neuropathology of Seckel syndrome in fetal stage with evidence of intrauterine developmental retardation. Acta Neuropathol (Berl) 1987;74:397. Horton WA, Hecht JT. The chondrodysplasias. In: Royce PM, Steinmann B, eds. Connective tissue and its heritable disorders: Molecular, genetic, and medical aspects. New York: Wiley-Liss, 1993. Horton WA, Rotter JI, Rimoin DL, et al. Standard growth curves for achondroplasia. J Pediatr 1978;93:435. Hourihane JOB, Bennett CP, Chaudhuri R, et al. A sibship with a neuronal migration defect, cerebellar hypoplasia and lymphedema. Neuropediatrics 1993;24:43. Howard TD, Paznekas WA, Green ED, et al. Mutations in Twist, a basic helix-loop-helix transcription factor in Saethre-Chotzen syndrome. Nat Genet 1997;15:36. Hoyt WF, Kaplan SL, Grumbach MM, et al. Septo-optic dysplasia and pituitary dwarfism. Lancet 1970;1:893. Huang CL, Larue DT, Winer JA. GABAergic organization of the cat medial geniculate body. J Comp Neurol 1999;415:368. Huang F, Sweet R, Tewfik TL. Apert syndrome and hearing loss with ear anomalies: A case report and literature review. Int J Pediatr Otorhinolaryngol 2004;68:495. Huang MH, Mouradian WE, Cohen SR, et al. The differential diagnosis of abnormal head shapes: Separating craniosynostosis from positional deformities and normal variants. Cleft Palate Craniofac J 1998;35:204. Hunt GM. The Casey Holter lecture. Non-selective intervention in newborn babies with open spina bifida: The outcome 30 years on for the complete cohort. Eur J Pediatr Surg 1999;9(Suppl 1):5. Hunt GM, Holmes AE. Factors relating to intelligence in treated cases of spina bifida cystica. Am J Dis Child 1976;130:823. Hunter AG. Neural tube defects in Eastern Ontario and Western Quebec: demography and family data. Am J Med Genet 1984;19:45. Hunter AG, Dupont B, McLaughlin M, et al. The Hunter-McAlpine syndrome results from duplication 5q35-qter. Clin Genet 2005;67:53. Hunter AG, Rudd NL. Craniosynostosis. II. Coronal synostosis: Its familial characteristics and associated clinical findings in 109 patients lacking bilateral polysyndactyly or syndactyly. Teratology 1977;15:301. Hunter AGW, Hecht JT, Scott CI Jr. Standard weight for height curves in achondroplasia. Am J Med Genet 1996;62:255. Huong TT, Goldbatt E, Simpson DA. Dandy-Walker syndrome associated with congenital heart defects: Report of three cases. Dev Med Child Neurol Suppl 1975;35;35. Huttenlocher PR, Taravath S, Mojtahedi S. Periventricular heterotopia and epilepsy. Neurology 1994;44:51. Hwang JM, Kim IO, Wang KC. Complete visual recovery in osteopetrosis by early optic nerve decompression. Pediatr Neurosurg 2000;33:328. Hwang SJ, Beaty TH, Panny SR, et al. Association study of transforming growth factor alpha (TGF alpha) TaqI polymorphism and oral clefts: Indication of gene-environment interaction in a population-based sample of infants with birth defects. Am J Epidemiol 1995;141:629. Iannetti P, Nigro G, Spalice A, et al. Cytomegalovirus infection and schizencephaly: Case reports. Ann Neurol 1998;43:123. Ibrahimi OA, Chiu ES, McCarthy JG, et al. Understanding the molecular basis of Apert syndrome. Plast Reconstr Surg 2005;115:264. Ibrahimi OA, Zhang F, Eliseenkova AV, et al. Proline to arginine mutations in FGF receptors 1 and 3 result in Pfeiffer and Muenke craniosynostosis syndromes through enhancement of FGF binding affinity. Hum Mol Genet 2004;13:69. Imani P, Vijayasekaran S, Lannigan F. Is it necessary to screen for hearing loss in the paediatric population with osteogenesis imperfecta? Clin Otolaryngol 2003;28:199. Ippolito E, Bray EW, Corsi A, et al. Natural history and treatment of fibrous dysplasia of bone: A multicenter clinicopathologic study promoted by the European Pediatric Orthopaedic Society. J Pediatr Orthop B 2003;12:155. Iskandar BJ, Oakes WJ, McLaughlin C, et al. Terminal syringohydromyelia and occult spinal dysraphism. J Neurosurg 1994;81:513. Izenberg N, Rosenblum M, Parks JS. The endocrine spectrum of septo-optic dysplasia. Clin Pediatr (Phila) 1984;23:632. Jaber L, Merlob P, Shohat M. High incidence of central nervous system malformations associated with marked parental consanguinity in an Israeli Arab community. Biomed Pharmacother 1994;48:351. Jabs EW, Li X, Scott AF, et al. Jackson-Weiss and Crouzon syndromes are allelic with mutations in fibroblast growth factor receptor 2. Nat Genet 1994;8:275. Jabs EW, Muller U, Li X, et al. A mutation in the homeodomain of the human MSX2 gene in a family affected with autosomal dominant craniosynostosis. Cell 1993;75:443.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Jackson AP, Eastwood H, Bell SM, et al. Identification of microcephalin, a protein implicated in determining the size of the human brain. Am J Hum Genet 2002;71:136. Jackson AP, McHale DP, Campbell DA, et al. Primary autosomal recessive microcephaly (MCPH1) maps to chromosome 8p22-pter. Am J Hum Genet 1998;63:541. Jackson CE, Weiss L, Reynolds WA. Craniosynostosis, midface hypoplasia, and foot abnormalities: An autosomal dominant phenotype in a large Amish kindred. J Pediat 1976;88:963. Jacobson RI. Abnormalities of the skull in children. Neurol Clin 1985;3:117. Jamieson CR, Fryns JP, Jacobs J, et al. Primary autosomal recessive microcephaly: MCPH5 maps to 1q25-q32. Am J Hum Genet 2000;67:1575. Jamieson CR, Govaerts C, Abramowicz MJ. Primary autosomal recessive microcephaly: Homozygosity mapping of MCPH4 to chromosome 15. Letter to the editor. Am J Hum Genet 1999;65:1465. Jan M, Dweik A, Destrieux C, et al. Fronto-orbital sphenoidal fibrous dysplasia. Neurosurgery 1994;34:544. Jezewski PA, Vieira AR, Nishimura C, et al. Complete sequencing shows a role for MSX1 in non-syndromic cleft lip and palate. J Med Genet 2003;40:399. Jimenez DF, Barone CM, Cartwright CC, et al. Early management of craniosynostosis using endoscopic-assisted strip craniectomies and cranial orthotic molding therapy. Pediatrics 2002;110:97. Jocelyn LJ, Penko MA, Rode HL. Cognition, communication, and hearing in young children with cleft lip and palate and in control children: A longitudinal study. Pediatrics 1996;97:529. Johnson MC. Klippel-Feil syndrome revisited: Diagnostic pitfalls impacting neurosurgical management. Childs Nerv Syst 1992;8:322. Jones AC, Shyamsundar MM, Thomas MW, et al. Comprehensive mutation analysis of TSC1 and TSC2 and phenotypic correlations in 150 families with tuberous sclerosis. Am J Hum Genet 1999;64:1305. Jones BV, Ball WS, Tomsick TA, et al. Vein of Galen aneurysmal malformation: Diagnosis and treatment of 13 children with extended clinical follow-up. AJNR Am J Neuroradiol 2002;23:1717. Jones KL. Smith’s recognizable patterns of human malformation. Philadelphia: WB Saunders, 1997. Jones MC. The genetics of cleft lip and palate: Information for families. Chapel Hill, NC: Cleft Palate-Craniofacial Program, 2000. Jones RF, Kwok BC, Stening WA, et al. Third ventriculostomy for hydrocephalus associated with spinal dysraphism: Indications and contraindications. Eur J Pediatr Surg 1996;1 (Suppl):5. Joseph JT. Periventricular heterotopias display cortical degenerative neuropathology. Neurology 1997;49:884. Joubert M, Eisenring JJ, Andermann F. Familial dysgenesis of the vermis: A syndrome of hyperventilation, abnormal eye movements and retardation. Neurology 1968;18:302. Jouet M, Rosenthal A, Armstrong G, et al. X-linked spastic paraplegia (SPG1), MASA syndrome and X-linked hydrocephalus result from mutations in the L1 gene. Nat Genet 1994;7:402. Joy HM, Barker CS, Small JH, Armitage M. Trans-sphenoidal encephalocele in association with Dandy-Walker complex and cardiovascular anomalies. Neuroradiology 2001;43:45. Jugessur A, Lie RT, Wilcox AJ, et al. Variants of developmental genes (TGFA, TGFB3, and MSX1) and their associations with orofacial clefts: A case-parent triad analysis. Genet Epidemiol 2003a;24:230. Jugessur A, Lie RT, Wilcox AJ, et al. Cleft palate, transforming growth factor alpha gene variants, and maternal exposures: Assessing gene-environment interactions in case-parent triads. Genet Epidemiol 2003b;25:367. Just M, Schwarz M, Ludwig B, et al. Cerebral and spinal MR-findings in patients with postrepair myelomeningocele. Pediatr Radiol 1990;20:262. Kalscheuer VM, Tao J, Donnelly A, et al. Disruption of the serine/threonine kinase 9 gene causes severe X-linked infantile spasms and mental retardation. Am J Hum Genet 2003;72:1401. Kane AA, Mitchell LE, Craven KP, et al. Observations on a recent increase in plagiocephaly without synostosis. Pediatrics 1996;97:87. Kanev PM, Sheehan JM. Reflections on shunt infection. Pediatr Neurosurg 2003;39:285. Kannu P, Kelly P, Aftimos S. Microcephalic osteodysplastic primordial dwarfism type II: A child with cafe au lait lesions, cutis marmorata, and moyamoya disease. Am J Med Genet 2004;128A:98. Kantaputra PN. Apparently new osteodysplastic and primordial short stature with severe microdontia, opalescent teeth, and rootless molars in two siblings. Am J Med Genet 2002;111:420. Kapp-Simon KA, Figueroa A, Jocher CA, et al. Longitudinal assessment of mental development in infants with nonsyndromic craniosynostosis with and without cranial release and reconstruction. Plast Reconstr Surg 1993;92:831.
479
Kapp-Simon KA, Krueckeberg S. Mental development in infants with cleft lip and/or palate. Cleft Palate Craniofac J 2000;37:65. Kapp-Simon KA. Mental development and learning disorders in children with single suture craniosynostosis. Cleft Palate Craniofac J 1998;35:197. Kato M, Dobyns WB. Lissencephaly and the molecular basis of neuronal migration. Hum Mol Genet 2003;12 (Suppl 1):R89. Kato M, Das S, Petras K, et al. Mutations of Arx are associated with striking pleiotropy and consistent genotype-phenotype correlation. Hum Mutat 2004;23:147. Kato M, Das S, Petras K, et al. Polyalanine expansion of Arx associated with cryptogenic West syndrome. Neurology 2003;61:267. Kato M, Takizawa N, Yamada S, et al. Diffuse pachygyria with cerebellar hypoplasia: A milder form of microlissencephaly or a new genetic syndrome? Ann Neurol 1999;46:660. Kaufman BA, Muszynski CA, Matthews A, et al. The circle of sagittal synostosis surgery. Semin Pediatr Neurol 2004;11:243. Kawaguchi Y, Kubota Y. Physiological and morphological identification of somatostatin- or vasoactive intestinal polypeptide-containing cells among GABAergic cell subtypes in rat frontal cortex. J Neurosci 1996;16:2701. Kawame H, Kurosawa K, Akatsuka A, et al. Polymicrogyria is an uncommon manifestation in 22q11.2 deletion syndrome. Letter to the editor. Am J Med Genet 2000;94:77. Keating RF. Craniosynostosis: Diagnosis and management in the new millennium. Pediatr Ann 1997;26:600. Keeler RF, Binns W. Teratogenic compounds of Veratrum californicum (Durand). V. Comparison of cyclopian effects of steroidal alkaloids from the plant and structurally related compounds from other sources. Teratology 1968;1:5. Keiper GL Jr, Koch B, Crone KR. Achondroplasia and cervicomedullary compression: Prospective evaluation and surgical treatment. Pediatr Neurosurg 1999;31:78. Kelley RI, Robinson D, Puffenberger EG, et al. Amish lethal microcephaly: A new metabolic disorder with severe congenital microcephaly and 2-ketoglutaric aciduria. Am J Med Genet 2002;112:318. Kelley RL, Roessler E, Hennekam RC, et al. Holoprosencephaly in RSH/Smith-Lemli-Opitz syndrome: Does abnormal cholesterol metabolism affect the function of Sonic hedgehog? Am J Med Genet 1996;66:478. Kelly EN, Allen VM, Seaward G, et al. Mild ventriculomegaly in the fetus, natural history, associated findings and outcome of isolated mild ventriculomegaly: A literature review. Prenat Diagn 2001;21:697. Kennedy CR, Ayers S, Campbell MJ, et al. Randomized, controlled trial of acetazolamide and furosemide in posthemorrhagic ventricular dilation in infancy: Follow-up at 1 year. Pediatrics 2001;108:597. Kerner B, Graham JM Jr, Golden JA, et al. Familial lissencephaly with cleft palate and severe cerebellar hypoplasia. Am J Med Genet 1999;87:440. Kestle J, Drake J, Cochrane D, et al. Lack of benefit of endoscopic ventriculperitoneal shunt insertion: A multicenter randomized trial. J Neurosurg 2003;98:284. Kestle J, Drake, J, Milner R, et al. Long-term follow-up data from the Shunt Design Trial. Pediatr Neurosurg 2000;33:230. Kestle JR. Pediatric hydrocephalus: Current management. Neurol Clin N Am 2003;21:883. Key CB, Rothrock SG, Falk JL. Cerebrospinal fluid shunt complications: An emergency medicine perspective. Pediatr Emerg Care 1995a;11:265. Key L, Carnes D, Cole S, et al. Treatment of congenital osteopetrosis with high-dose calcitrol. N Engl J Med 1984;310:409. Key LL Jr, Rodriguiz RM, Willi SM, et al. Long-term treatment of osteopetrosis with recombinant human interferon gamma. N Engl J Med 1995b;332:1594. Kitamura K, Yanazawa M, Sugiyama N, et al. Mutation of Arx causes abnormal development of forebrain and testes in mice and X-linked lissencephaly with abnormal genitalia in humans. Nat Genet 2002;32:359. Klinge L, Schaper J, Wieczorek D, et al. Microlissencephaly in microcephalic osteodysplastic primordial dwarfism: A case report and review of the literature. Neuropediatrics 2002;33:309. Knab K, Langhans B, Behrens R, Strehl AE. The neuropathic bowel in spina bifida—a cross-sectional study in 226 patients. Eur J Pediatr Surg 2001;11(Suppl 1):S41. Knight SJ, Lese CM, Precht KS, et al. An optimized set of human telomere clones for studying telomere integrity and architecture. Am J Hum Genet 2000;67:320. Kobayashi K, Nakahori Y, Miyake M, et al. An ancient retrotransposal insertion causes Fukuyama-type congenital muscular dystrophy. Nature 1998;394:388. Koch CA, Voth D, Kraemer G, et al. Arachnoid cysts: Does surgery improve epileptic seizures and headaches? Neurosurg Rev 1995;18:173.
480
Perinatal Acquired and Congenital Neurologic Disorders / 19
Koch MC, Stegmann K, Ziegler A, et al. Evaluation of the MTHFR C677T allele and the MTHFR gene locus in a German spina bifida population. Eur J Pediatr 1998;157:487. Kocher MS, Kasser JR. Osteopetrosis. Am J Orthop 2003;32:222 Koenig SB, Naidich TP, Lissner G. The morning glory syndrome associated with sphenoidal encephalocele. Ophthalmology 1982;89:1368. Koenigsberg RA, Vakil N, Hong TA, et al. Evaluation of platybasia with MR imaging. AJNR Am J Neuroradiol 2005;26:89. Kondo S, Schutte BC, Richardson RJ, et al. Mutations in IRF6 cause Van der Woude and popliteal pterygium syndromes. Nat Genet 2002;32:285. Kondo-Iida E, Kobayashi K, Watanabe M, et al. Novel mutations and genotype-phenotype relationships in 107 families with Fukuyama-type congenital muscular dystrophy (FCMD). Hum Mol Genet 1999;8:2303. Konz KR, Chia JK, Kurup VP, et al. Comparison of latex hypersensitivity among patients with neurologic defects. J Allergy Clin Immunol 1995;95:950. Koren G, Kennedy D. Safe use of valproic acid during pregnancy. Can Fam Physician 1999;45:1451. Kos M, Luczak K, Godzinski J, et al. Treatment of monostotic fibrous dysplasia with pamidronate. J Craniomaxillofac Surg 2004;32:10. Kothare SV, VanLandingham K, Armon C, et al. Seizure onset from periventricular nodular heterotopias: Depth-electrode study. Neurology 1998;51:1723. Kothari MJ, Bauer SB. Urodynamic and neurophysiologic evaluation of patients with diastematomyelia. J Child Neurol 1997;12:97. Kousseff BG, Ranells JD. Lowry-Maclean syndrome does exist. Am J Med Genet 1994;53:300. Kovar C, Plawner LL, Sweet VT, et al. Cognitive profiles of children with holoprosencephaly. Arch Clin Neuropsychol 2001;16:781. Kreiborg A, Barr M Jr, Cohen MM Jr. Cervical spine in the Apert syndrome. Am J Med Genet 1992;43:704. Kress W, Collmann H, Busse M, et al. Clustering of FGFR2 gene mutations in patients with Pfeiffer and Crouzon syndromes (FGFR2-associated craniosynostoses). Cytogenet Cell Genet 2000;91:134. Krimer LS, Goldman-Rakic PS. Prefrontal microcircuits: Membrane properties and excitatory input of local, medium, and wide arbor interneurons. J Neurosci 2001;21:3788. Kriss VM, Kriss TC, Desai NS, Warf BC. Occult spinal dysraphism in the infant. Clin Pediatr (Phila) 1995;34:650. Kroon AA, Smit BJ, Barth PG, et al. Lissencephaly with extreme cerebral and cerebellar hypoplasia. A magnetic resonance imaging study. Neuropediatrics 1996;27:273. Kruse RW, Harcke HT, Minch CM. Osteogenesis imperfecta (OI) may be mistaken for child abuse. Pediatr Emerg Care 1997;13:244. Kuban KC, Teele RL, Wallman J. Septo-optic-dysplasia-schizencephaly. Radiographic and clinical features. Pediatr Radiol 1989;19:145. Kumar R, Jain MK, Chhabra DK. Dandy-Walker syndrome: Different modalities of treatment and outcome in 42 cases. Childs Nerv Syst 2001;17:348. Kurihara Y, Kurihara H, Suzuki H, et al. Elevated blood pressure and craniofacial abnormalities in mice deficient in endothelin-1. Nature 1994;368:703. Kuzniecky R, Andermann F. The congenital bilateral perisylvian syndrome: Imaging findings in a multicenter study. CBPS study group. AJNR Am J Neuroradiol 1994;15:139. Kuzniecky R, Andermann F, Guerrini R. Infantile spasms: An early epileptic manifestation in some patients with the congenital bilateral perisylvian syndrome. J Child Neurol 1994a;9(4):420. Kuzniecky R, Andermann F, Guerrini R. The epileptic spectrum in the congenital bilateral perisylvian syndrome. CBPS Multicenter Collaborative Study. Neurology 1994b;44:379. Kuzniecky R, Garcia JH, Faught E, et al. Cortical dysplasia in temporal lobe epilepsy: Magnetic resonance imaging correlations. Ann Neurol 1991;29:293. Kuzniecky R, Gilliam F, Morawetz R, et al. Occipital lobe developmental malformations and epilepsy: Clinical spectrum, treatment, and outcome. Epilepsia 1997;38:175. Kuzniecky R, Morawetz R, Faught E, et al. Frontal and central lobe focal dysplasia: Clinical, EEG and imaging features. Dev Med Child Neurol 1995;37:159. Kuzniecky R. Familial diffuse cortical dysplasia. Arch Neurol 1994;51:307. Kuzniecky RI, Andermann F, Guerrini R. The congenital bilateral perisylvian syndrome: Study of 31 patients. The Congenital Bilateral Perisylvian Syndrome Multicenter Collaborative Study. Lancet 1993;341:608. Lachman RS. Neurologic abnormalities in the skeletal dysplasias: A clinical and radiological perspective. Am J Med Genet 1997;69:33.
Lacombe D, Battin J. Marfanoid features and craniosynostosis: Report of one case and review. Clin Dysmorphol 1993;2:220. Lajeunie E, Barcik U, Thorne JA, et al. Craniosynostosis and fetal exposure to sodium valproate. J Neurosurg 2001;95:778. Lajeunie E, Cameron R, El Ghouzzi V, et al. Clinical variability in patients with Apert’s syndrome. J Neurosurg 1999;90:443. Lajeunie E, El Ghouzzi V, Le Merrer M, et al. Sex related expressivity of the phenotype in coronal craniosynostosis caused by the recurrent P250R FGFR3 mutation. J Med Genet 1999;36:9. Lam CH, Villemure JG. Comparison between ventriculoatrial and ventriculoperitoneal shunting in the adult population. Br J Neurosurg 1997;11:43. Lammer EJ, Sever LE, Oakley GP Jr. Teratogen update: Valproic acid. Teratology 1987;35:465. Lancon JA, Ellis AL. Giant posterior fossa arachnoid cyst. Pediatr Neurosurg 2004;40:151. Landau K, Gloor BP. Therapy-resistant papilledema in achondroplasia. J Neuroophthalmol 1994;14:24. Landsmeer-Beker EA, Massa GG, Maaswinkel-Mooy PD, et al. Treatment of osteogenesis imperfecta with the bisphosphonate olpadronate (dimethylaminohydroxypropylidene bisphosphonate). Eur J Pediatr 1997;156:792. Langkau N, Martin N, Brandt R, et al. TSC1 and TSC2 mutations in tuberous sclerosis, the associated phenotypes and a model to explain observed TSC1/TSC2 frequency ratios. Eur J Pediatr 2002;161:393. Lary JM, Edmonds LD. Prevalence of spina bifida at birth—United States, 1983-1990: A comparison of two surveillance systems. MMWR CDC Surveill Summ 1996;45:15. Lasjaunias P, Ter Brugge K, Lopez Ibor L, et al. The role of dural anomalies in vein of Galen aneurysms: Report of six cases and review of the literature. AJNR Am J Neuroradiol 1987;8:185. Laubscher B, Deonna T, Uske A, et al. Primitive megalencephaly in children: Natural history, medium term prognosis with special reference to external hydrocephalus. Eur J Pediatr 1990;149:502. Laurence KM. Neurological and intellectual sequelae of hydrocephalus. Arch Neurol 1969;20:73. Lavdas AA, Grigoriou M, Pachnis V, et al. The medial ganglionic eminence gives rise to a population of early neurons in the developing cerebral cortex. J Neurosci 1999;19:7881. Lee HJ, Cho DY, Tsai FJ, et al. Antley-Bixler syndrome, description of two new cases and review of the literature. Pediatr Neurosurg 2001;34:33. Lee JS, FitzGibbon E, Butman JA, et al. Normal vision despite narrowing of the optic canal in fibrous dysplasia. N Engl J Med 2002;347:1670. Lee SJ, Huh EJ, Byeon JH. Two cases of cerebral salt wasting syndrome developing after cranial vault remodeling in craniosynostosis children. J Korean Med Sci 2004;19:627. Leech RW, Shuman RM. Holoprosencephaly and related midline cerebral anomalies: A review. J Child Neurol 1986;1:3. Leeflang EP, Marsh SE, Parrini E, et al. Patient with bilateral periventricular nodular heterotopia and polymicrogyria with apparently balanced reciprocal translocation t(1;6)(p12;p12.2) that interrupts the mannosidase alpha, class 1A, and glutathione S-transferase A2 genes. J Med Genet 2003;40:e128. Leet AI, Magur E, Lee JS, et al. Fibrous dysplasia in the spine: Prevalence of lesions and association with scoliosis. J Bone Joint Surg Am 2004;86A:531. Legius E, Fryns JP, Van den Berghe H. Aural cephalosyndactyly: A new craniosynostosis syndrome or a variant of the Saethre-Chotzen syndrome? J Med Genet 1989;26:522. LeHeup BP, Masutti JP, Droulle P, et al. The Antley-Bixler syndrome: Report of two familial cases with severe renal and anal anomalies. Eur J Pediatr 1995;154:130. Lekovic GP, Bristol RE, Rekate HL. Cognitive impact of craniosynostosis. Semin Pediatr Neurol 2004;11:305. Lemire RJ, Loeser JD, Leech RW, Alvord EC. Normal and abnormal development of the human nervous system. Hagerstown, MD: Harper & Row, 1975. Lennon CA, Gray DL. Sensitivity and specificity of ultrasound for the detection of neural tube and ventral wall defects in a high-risk population. Obstet Gynecol 1999;94:562. Lepinard C, Coutant R, Boussion F, et al. Prenatal diagnosis of absence of the septum pellucidum associated with septo-optic dysplasia. Ultrasound Obstet Gynecol 2004;25:73. Letinic K, Zoncu R, Rakic P. Origin of gabaergic neurons in the human neocortex. Nature 2002;417:645. Levine DN, Fisher MA, Caviness VS Jr. Porencephaly with microgyria: A pathologic study. Acta Neuropathol 1974;29:99.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Levine JP, Stelnicki E, Weiner HL, et al. Hyponatremia in the postoperative craniofacial pediatric patient population: A connection to cerebral salt wasting syndrome and management of the disorder. Plast Reconstr Surg 2001;108:1501. Levy HL, Lobbregt D, Barnes PD, et al. Maternal phenylketonuria: Magnetic resonance imaging of the brain in offspring. J Pediatr 1996;128:770. Levy WJ, Mason L, Hahn JF. Chiari malformation presenting in adults: A surgical experience in 127 cases. Neurosurgery 1983;12:377. Lewis AJ, Simon EM, Barkovich AJ, et al. Middle interhemispheric variant of holoprosencephaly. Neurology 2002;59:1860. Lewis ME, Rosenbaum PL, Paes BA. Baller-Gerold syndrome associated with congenital hydrocephalus. Am J Med Genet 1991;40:307. Li LM, Dubeau F, Andermann F, et al. Periventricular nodular heterotopia and intractable temporal lobe epilepsy: Poor outcome after temporal lobe resection. Ann Neurol 1997;41:662. Li X, Lewanda AF, Eluma F, et al. Two craniosynostotic syndrome loci, Crouzon and Jackson-Weiss, map to chromosome 10q23-q26. Genomics 1994;22:418. Li Y, Holzgreve W, Page-Christiaens GC, et al. Improved prenatal detection of a fetal point mutation for achondroplasia by the use of size-fractionated circulatory DNA in maternal plasma—case report. Prenat Diagn 2004;24:896. Liaw D, Marsh DJ, Li J, et al. Germline mutations of the PTEN gene in Cowden disease, an inherited breast and thyroid cancer syndrome. Nat Genet 1997;16:64. Libenson MH, Kaye EM, Rosman NP, et al. Acetazolamide and furosemide for posthemorrhagic hydrocephalus of the newborn. Pedatr Neurol 1999;20:185. Licata AA. Discovery, clinical development, and therapeutic uses of bisphosphonates (CE) (April). Ann Pharmacother 2005;39:668. Lidral AC, Murray JC. Genetic approaches to identify disease genes for birth defects with cleft lip/palate as a model. Birth Defects Res A Clin Mol Teratol 2004;70:893. Lieblich JM, Rosen SE, Guyda H, et al. The syndrome of basal encephalocele and hypothalamic-pituitary dysfunction. Ann Intern Med 1978;89:910. Limouzy F, Durroux R, Chiron P, et al. Fibrous dysplasia associated with intramuscular myxoma. Rev Chir Orthop Reparatrice Appar Mot 1996;82:336. Liptak GS, Bloss JW, Briskin H, et al. The management of children with spinal dysraphism. J Child Neurol 1988;3:3. Lipton HL, Preziosi TJ, Moses H. Adult onset of the Dandy-Walker syndrome. Arch Neurol 1978;35:672. Little JR, Houser OW, MacCarty CS. Clinical manifestations of aqueductal stenosis in adults. J Neurosurg 1975;43:546. Littlefield TR. Cranial remodeling devices: Treatment of deformational plagiocephaly and postsurgical applications. Semin Pediatr Neurol 2004;11:268. Locatelli F, Beluffi G, Giorgiani G, et al. Transplantation of cord blood progenitor cells can promote bone resorption in autosomal recessive osteopetrosis. Bone Marrow Transplant 1997;20:701. Loebstein R, Koren G. Pregnancy outcome and neurodevelopment of children exposed in utero to psychoactive drugs: The Motherisk experience. J Psychiatry Neurosci 1997;22:192. Loft AG, Hogdall E, Larsen SO, Norgaard-Pedersen B. A comparison of amniotic fluid, alpha-fetoprotein, and acetylcholinesterase in the prenatal diagnosis of open neural tube defects and anterior abdominal wall defects. Prenat Diagn 1993;13:93. Longman C, Brockington M, Torelli S, et al. Mutations in the human large gene cause MDC1D, a novel form of congenital muscular dystrophy with severe mental retardation and abnormal glycosylation of alpha-dystroglycan. Hum Mol Genet 2003;12:2853. Lorber J, Schofield JK. The prognosis of occipital encephalocele. Z Kinderchir Grenzgeb 1979;28:347. Louhichi N, Triki C, Quijano-Roy S, et al. New FKRP mutations causing congenital muscular dystrophy associated with mental retardation and central nervous system abnormalities. Identification of a founder mutation in Tunisian families. Neurogenetics 2004;5:27. Lowry RB, Jabs EW, Graham GE., et al. Syndrome of coronal craniosynostosis, Klippel-Feil anomaly, and sprengel shoulder with and without Pro250Arg mutation in the FGFR3 gene. Am J Med Genet 2001;104:112. Lowry RB, MacLean JR. Case reports: A syndrome of mental retardation, cleft palate, eventration of diaphragm, congenital heart defect, glaucoma, growth failure and craniosynostosis. Birth Defects Orig Art Ser 1977;XIII:203. Luhmann SJ, Sheridan JJ, Capelli AM, et al. Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88.
481
Lumenta CB, Skotarczak U. Long-term follow-up in 233 patients with congenital hydrocephalus. Childs Nerv Syst 1995;11:173. Lund JS, Lewis DA. Local circuit neurons of developing and mature macaque prefrontal cortex: Golgi and immunocytochemical characteristics. J Comp Neurol 1993;328:282. Lundberg YW, Cabrera RM, Greer KA, et al. Mapping a chromosomal locus for valproic acid–induced exencephaly in mice. Mamm Genome 2004;15:361. Lustig LR, Holliday MJ, McCarthy EF, et al. Fibrous dysplasia involving the skull base and temporal bone. Arch Otolaryngol Head Neck Surg 2001;127:1239. Lutcherath V, Waaler PE, Jellum E, et al. Children with bilateral temporal arachnoid cysts may have glutaric aciduria type 1 (GAT1); operation without knowing that may be harmful. Acta Neurochir (Wien) 2000;142:1025. Lynch SA, Wang Y, Strachan T, et al. Autosomal dominant sacral agenesis: Currarino syndrome. J Med Genet 2000;37:561. Magge SN, Westerveld M, Pruzinsky T, et al. Long-term neuropsychological effects of sagittal craniosynostosis on child development. J Craniofac Surg 2002;13:99. Maher CO, Cohen-Gadol AA, Raffel C. Cortical resection for epilepsy in children with linear sebaceous nevus syndrome. Pediatr Neurosurg 2003;39:129. Majewski F, Goecke T. Studies of microcephalic primordial dwarfism I: Approach to a delineation of the Seckel syndrome. Am J Med Genet 1982;12:7. Majewski F, Goecke TO. Microcephalic osteodysplastic primordial dwarfism type II: Report of three cases and review. Am J Med Genet 1998;80:25. Majewski F, Ranke M, Schinzel A. Studies of microcephalic primordial dwarfism II: The osteodysplastic type II of primordial dwarfism. Am J Med Genet 1982;12:23. Malatesta P, Hartfuss E, Gotz M. Isolation of radial glial cells by fluorescentactivated cell sorting reveals a neuronal lineage. Development 2000;127:5253. Malinger G, Lev D, Kidron D, et al. Differential diagnosis in fetuses with absent septum pellucidum. Ultrasound Obstet Gynecol 2004;25:42. Mann JD, Butler AB, Rosenthal JE, et al. Regulation of intracranial pressure in rat, dog, and man. Ann Neurol 1978;3:156. Manning FA, Harrison ME, Rodeck C. Catheter shunts for fetal hydronephrosis and hydrocephalus. Report of the International Fetal Surgery Registry. N Engl J Med 1986;315:336. Mantovani JF, Pasternak JF, Mathew OP, et al. Failure of daily lumbar punctures to prevent the development of hydrocephalus following intraventricular hemorrhage. J Pediatr 1980;97:278. Marchac D, Renier D. Craniofacial surgery for craniosynostosis. Boston: Little, Brown, 1982. Maria BL, Boltshauser E, Palmer SC, Tran TX. Clinical features and revised diagnostic criteria in Joubert syndrome. J Child Neurol 1999a;14:583. Maria BL, Quisling RG, Rosainz LC, et al. Molar tooth sign in Joubert syndrome: Clinical, radiologic, and pathologic significance. J Child Neurol 1999b;14:368. Maria BL, Zinreich SJ, Carson BC, et al. Dandy-Walker syndrome revisited. Pediatr Neurosci 1987;13:45. Marie PJ, de Pollak C, Chanson P, et al. Increased proliferation of osteoblastic cells expressing the activating Gs alpha mutation in monostotic and polyostotic fibrous dysplasia. Am J Pathol 1997;150:1059. Marin O, Rubenstein JL. A long, remarkable journey: Tangential migration in the telencephalon. Nat Rev Neurosci 2001;2:780. Marini JC, Gerber NL. Osteogenesis imperfecta. Rehabilitation and prospects for gene therapy. JAMA 1997;277:746. Marin-Padilla M. Notochordal-basichondrocranium relationships: Abnormalities in experimental axial skeletal (dysraphic) disorders. J Embryol Exp Morphol 1979;53:15. Marlowe A, Pepin MG, Byers PH. Testing for osteogenesis imperfecta in cases of suspected non-accidental injury. J Med Genet 2002;39:382. Marsh DJ, Dahia PL, Zheng Z, et al. Germline mutations in PTEN are present in Bannayan-Zonana syndrome. Nat Genet 1997;16:333. Martin HP. Microcephaly and mental retardation. Am J Dis Child 1970;119:128. Martin RP, Deane RH, Collett V. Spondylolysis in children who have osteopetrosis. J Bone Joint Surg Am 1997;79:1685. Martinez Perez D, Vander Woude DL, Barnes PD, et al. Jugular foraminal stenosis in Crouzon syndrome. Pediatr Neurosurg 1996;25:252. Martinez-Lage JF, Garcia Santos JM, Poza M, et al. Bilateral temporal arachnoid cysts in neurofibromatosis. J Child Neurol 1993;8:383. Martinez-Lage JF, Poza M, Sola, J, et al. The child with a cephalocele: Etiology, neuroimaging, and outcome. Childs Nerv Syst 1996;12:540.
482
Perinatal Acquired and Congenital Neurologic Disorders / 19
Mason TB 2nd, Chiriboga CA, Feldstein NA, et al. Intracranial arachnoid cyst in a developmentally normal infant: Case report and literature review. Pediatr Neurol 1997;16:59. Matalon S, Schechtman S, Goldzweig G, Ornoy A. The teratogenic effect of carbamazepine: A meta-analysis of 1255 exposures. Reprod Toxicol 2002;16:9. Matarazzo P, Lala R, Masi G, et al. Pamidronate treatment in bone fibrous dysplasia in children and adolescents with McCune-Albright syndrome. J Pediatr Endocrinol Metab 2002;15 (Suppl 3):929. Matell M. Ein fall von heterotopie der frauen substanz in den beiden hemispheren des grosshirns. Arch Psychiatr Nervenkr 1893;25:124. Mathieu JP, Decarie M, Dube J, Marton D. [Diastematomyelia. Study of 69 cases (author’s transl)]. Chir Pediatr 1982;23:29. Matsumoto K, Nakanishi H, Kubo Y, et al. Advances in distraction techniques for craniofacial surgery. J Med Invest 2003;50:117. Matsumoto N, Leventer RJ, Kuc JA, et al. Mutation analysis of the DCX gene and genotype/phenotype correlation in subcortical band heterotopia. Eur J Hum Genet 2001;9:5. Matsunaga E, Shiota K. Holoprosencephaly in human embryos: Epidemiologic studies of 150 cases. Teratology 1977;16:261. McCarthy JG, Epstein FJ, Wood-Smith D. Craniosynostosis. In: McCarthy JG, ed. Plastic surgery, vol 4. Philadelphia: WB Saunders, 1990. McComb JG. Spinal and cranial neural tube defects. Semin Pediatr Neurol 1997;4:156. McDonald CM. Rehabilitation of children with spinal dysraphism. Neurosurg Clin North Am 1995;6:393. McDonnell,GV, McCann JP. Why do adults with spina bifida and hydrocephalus die? A clinic-based study. Eur J Pediatr Surg 2000;10(Suppl 1):31. McGaughran JM, Oates A, Donnai D, et al. Mutations in PAX1 may be associated with Klippel Feil syndrome. Eur J Hum Genet 2003;11:468. McIntosh R, Merritt KK, Richards MR, et al. The incidence of congenital malformations: A study of 5,964 pregnancies. Pediatrics 1954;14:505. McIntyre FL. Craniosynostosis. Am Fam Physician 1997;55:1173. McKusick VA. Mendelian inheritance in man: A catalog of human genes and genetic disorders, 11th ed. Baltimore: Johns Hopkins University Press, 1994. McLaurin RL, Schut L, Venes JL, et al. Pediatric neurosurgery: Surgery of the developing nervous system, 2nd ed. Philadelphia: WB Saunders, 1989. McLone DG, Dias MS. The Chiari II malformation: Cause and impact. Childs Nerv Syst 2003;19:540. McLone DG, Czyzewski D, Raimondi AJ, et al. Central nervous system infections as a limiting factor in the intelligence of children with meningomyelocele. Pediatrics 1982;70:335. McMahon C, Will A, Hu P, et al. Bone marrow transplantation corrects osteopetrosis in the carbonic anhydrase II deficiency syndrome. Blood 2001;97:1947. Mecke S, Passarge E. Encephalocele, polycystic kidneys, and polydactyly as an autosomal recessive trait simulating certain other disorders: The Meckel syndrome. Ann Genet 1971;14:97. Medical Research Council Vitamin Study. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. Lancet 1991;338:131 (available at http://www.ncbi.nlm.nih.gov/entrez). Medical Taskforce on Anencephaly. The infant with anencephaly. N Engl J Med 1990;322:669. Meencke HJ, Janz D. Neuropathological findings in primary generalized epilepsy: A study of eight cases. Epilepsia 1984;25:8. Megarbane A, Delague V, Ruchoux MM, et al. New autosomal recessive cerebellar ataxia disorder in a large inbred Lebanese family. Am J Med Genet 2001;101:135. Meinecke P, Passarge E. Microcephalic osteodysplastic primordial dwarfism type I/III in sibs. J Med Genet 1991;28:795. Mendonca JL, Natal MR, Viana SL, et al. Rhombencephalosynapsis: CT and MRI findings. Neurol India 2004;52:118. Meuli M, Meuli-Simmen C, Hutchins GM, et al. In utero surgery rescues neurological function at birth in sheep with spina bifida. Nat Med 1995;1:342. Meyer-Heim AD, Klein A, Boltshauser E. Cervical myelomeningocele— follow-up of five patients. Eur J Paediatr Neurol 2003;7:407. Meyers GA, Orlow SJ, Munro IR, et al. Fibroblast growth factor receptor 3 (FGFR3) transmembrane mutation in Crouzon syndrome with acanthosis nigricans. Nat Genet 1995;11:462. Michejda M, Bacher J. Functional and anatomic recovery in the monkey brain following excision of fetal encephalocele. Pediatr Neurosci 1985;12:90. Michelson DJ, Ashwal S. Tethered cord syndrome in childhood: Diagnostic features and relationship to congenital anomalies. Neurol Res 2004;26:745.
Milhorat TH, Capocelli AL Jr, Anzil AP, et al. Pathological basis of spinal cord cavitation in syringomyelia: Analysis of 105 autopsy cases. J Neurosurg 1995;82:802. Milhorat TH, Chou MW, Trinidad EM, et al. Chiari I malformation redefined: Clinical and radiographic findings for 364 symptomatic patients. Neurosurgery 1999;44:1005. Milhorat TH, Johnson WD, Miller JI, et al. Surgical treatment of syringomyelia based on magnetic resonance imaging criteria. Neurosurgery 1992;31:231-244; discussion 244. Milhorat TH, Kotzen RM, Anzil AP. Stenosis of central canal of spinal cord in man: Incidence and pathological findings in 232 autopsy cases. J Neurosurg 1994;80:716. Milhorat TH, Nobandegani F, Miller JI, et al C. Noncommunicating syringomyelia following occlusion of central canal in rats. Experimental model and histological findings. J Neurosurg 1993;78:274. Miller A, Guille JT, Bowen JR. Evaluation and treatment of diastematomyelia. J Bone Joint Surg Am 1993;75:1308. Miller SP, Shevell MI, Patenaude Y, et al. Septo-optic dysplasia plus: A spectrum of malformations of cortical development. Neurology 2000;54:1701. Millichap JG. Temporal lobe arachnoid cyst-attention disorder syndrome: Role of the electroencephalogram in diagnosis. Neurology 1997;48:1435. Minardi CG, Souza AC, Netto MP, et al. Auditory abilities in children with cleft lip and/or palate according to Fisher’s. Acta Otorrinolaringol Esp 2004;55:160. Ming JE, Muenke M. Multiple hits during early embryonic development: Digenic diseases and holoprosencephaly. Am J Hum Genet 2002;71:1017. Mirzaa G, Dodge NN, Glass I, et al. Megalencephaly and perisylvian polymicrogyria with postaxial polydactyly and hydrocephalus: A rare brain malformation syndrome associated with mental retardation and seizures. Neuropediatrics 2004;35:353. Mitsukawa N, Satoh K, Hayashi T, et al. A reflectable case of obstructive sleep apnea in an infant with Crouzon syndrome. J Craniofac Surg 2004;15:874. Miyata T, Kawaguchi A, Okano H, et al. Asymmetric inheritance of radial glial fibers by cortical neurons. Neuron 2001;31:727. Mohn A, Schoof E, Fahlbusch R, Wenzel D, et al. The endocrine spectrum of arachnoid cysts in childhood. Pediatr Neurosurg 1999;3:316. Mooney MP, Burrows AM, Smith TD, et al. Correction of coronal suture synostosis using suture and dura mater allografts in rabbits with familial craniosynostosis. Cleft Palate Craniofac J 2001;38:206. Moore CA, Toriello HV, Abuelo DN, et al. Macrocephaly–cutis marmorata telangiectatica congenita syndrome: A distinct disorder with developmental delay and connective tissue abnormality. Am J Med Genet 1997;70:67. Moore LL, Bradlee ML, Singer MR, et al. Folate intake and the risk of neural tube defects: An estimation of dose-response. Epidemiology 2003;14:200. Moore SA, Saito F, Chen J, et al. Deletion of brain dystroglycan recapitulates aspects of congenital muscular dystrophy. Nature 2002;418:422. Morrissey DD, Talbot JM, Schleuning AJ 2nd. Fibrous dysplasia of the temporal bone: Reversal of sensorineural hearing loss after decompression of the internal auditory canal. Laryngoscope 1997;107:1336. Most D, Levine JP, Chang J, et al. Studies in cranial suture biology: Upregulation of transforming growth factor-beta1 and basic fibroblastic growth factorm RNA correlates with posterior frontal cranial suture fusion in the rat. Plast Reconstr Surg 1998;101:1431. Mouradian WE. Controversies in the diagnosis and management of craniosynostosis: A panel discussion. Cleft Palate Craniofac J 1998;35:190. Moynihan L, Jackson AP, Roberts E, et al. A third novel locus for primary autosomal recessive microcephaly maps to chromosome 9q34. Am J Hum Genet 2000;66:724. Mueller SM, Bell W, Cornell S, et al. Achondroplasia and hydrocephalus: A computerized tomographic, roentgenographic, and psychometric study. Neurology 1977;27:430. Muenke M, Gripp KW, McDonald-McGinn DM, et al. A unique point mutation in the fibroblast growth factor receptor 3 gene (FGFR3) defines a new craniosynostosis syndrome. Am J Hum Genet 1997;60:555. Muenke M, Schell U, Hehr A, et al. A common mutation in the fibroblast growth factor receptor 1 gene in Pfeiffer syndrome. Nat Genet 1994;8:269. Muller U, Steinberger D, Kunze S. Molecular genetics of craniosynostotic syndromes. Graefes Arch Clin Exp Ophthalmol 1997;235:545. Mulliken JB, Gripp KW, Stolle CA, et al. Molecular analysis of patients with synostotic frontal plagiocephaly (unilateral coronal synostosis). Plast Reconstr Surg 2004;113:1899. Mulliken JB, Warman ML. Molecular genetics and craniofacial surgery. Plast Reconstruct Surg 1996;97:666. Mundlos S. Cleidocranial dysplasia: Clinical and molecular genetics. J Med Genet 1999;36:177.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Munger RG, Romitti PA, Daack-Hirsch S, et al. Maternal alcohol use and risk of orofacial cleft birth defects. Teratology 1996;54:27. Murray JC, Johnson JA, Bird TD. Dandy-Walker malformation: Etiologic heterogeneity and empiric recurrence risks. Clin Genet 1985;28:272. Mursch K, Enk T, Christen HJ, et al. Venous intracranial haemodynamics in children undergoing operative treatment for the repair of craniosynostosis. A prospective study using transcranial colour-coded duplex sonography. Childs Nerv Syst 1999;15:110. Naidich TP, McLone DG, Radkowski MA. Intracranial arachnoid cysts. Pediatr Neurosci 1985-86;12:112. Nanni L, Ming JE, Bocian M, et al. The mutational spectrum of the Sonic hedgehog gene in holoprosencephaly: SHH mutations cause a significant proportion of autosomal dominant holoprosencephaly. Hum Mol Genet 1999;8:2479. National Center for Health Statistics, 2005. Head growth charts. Available at http://www.cdc.gov/nchs/about/major/nhanes/growthcharts/charts.htm Nazzaro A, Della Monica M, Lonardo F, et al. Prenatal ultrasound diagnosis of a case of Pfeiffer syndrome without cloverleaf skull and review of the literature. Prenat Diagn 2004;24:918. Nelen MR, van Staveren WC, Peeters EA, et al. Germline mutations in the PTEN/MMAC1 gene in patients with Cowden disease. Hum Mol Genet 1997;6:1383. Nellhaus G. Head circumference from birth to eighteen years. Pediatrics 1968;41:106. Nelson FW, Hecht JT, Horton WA, et al. Neurological basis of respiratory complications in achondroplasia. Ann Neurol 1988;24:89. Nelson KB, Deutschberger J. Head size at one year as a predictor of four-year IQ. Dev Med Child Neurol 1970;12:487. Neri R, Martini A, Trippi D, et al. Reflex sympathetic dystrophy syndrome with microtrabecular fracture in a patient with osteogenesis imperfecta. Clin Rheumatol 1997;16:363. Nevo Y, Segev Y, Gelman Y, et al. Worster-Drought and congenital perisylvian syndromes—a continuum? Pediatr Neurol 2001;24:153. Nezelof C, Jaubert F, Lyon G. Syndrome familial associant grele court, malrotation intestinale, hypertrophie du pylore et malformation cerebrale: Etude anatomo-clinique de trois observations. Ann Anat Pathol (Paris) 1976;21:401. Nicoletti B, Kopits SE, Ascani E, et al. Human achondroplasia: A multidisciplinary approach. New York: Plenum Press, 1988. Niida Y, Lawrence-Smith N, Banwell A, et al. Analysis of both Tsc1 and Tsc2 for germline mutations in 126 unrelated patients with tuberous sclerosis. Hum Mutat 1999;14:412. Nishikawa M, Sakamoto H, Hakuba A, et al. Pathogenesis of Chiari malformation: A morphometric study of the posterior cranial fossa. J Neurosurg 1997;86:40. Niyibizi C, Wang S, Mi Z, et al. Gene therapy approaches for osteogenesis imperfecta. Gene Ther 2004;11:408. Noctor SC, Flint AC, Weissman TA, et al. Neurons derived from radial glial cells establish radial units in neocortex. Nature 2001;409:714. Noetzel MJ, Marsh JL, Palkes H, et al. Hydrocephalus and mental retardation in craniosynostosis. J Pediatr 1985;107:885. Nohria V, Oakes WJ. Chiari I malformation: A review of 43 patients. Pediatr Neurosurg 1990;16:222. Nopoulos P, Berg S, Canady J, et al. Structural brain abnormalities in adult males with clefts of the lip and/or palate. Genet Med 2002a;4:1. Nopoulos P, Berg S, VanDemark D, et al. Increased incidence of a midline brain anomaly in patients with nonsyndromic clefts of the lip and/or palate. J Neuroimaging 2001;11:418. Nopoulos P, Berg S, VanDemark D, et al. Cognitive dysfunction in adult males with non-syndromic clefts of the lip and/or palate. Neuropsychologia 2002b;40:2178. Norman MG. Bilateral encephaloclastic lesions in a 26 week gestation fetus: Effect on neuroblast migration. Can J Neurol Sci 1980;7:191. Norman MG, McGillivray BC, Kalousek DK, et al. Congenital malformations of the brain: Pathologic, embryologic, clinical, radiologic and genetic aspects. New York: Oxford University Press, 1995. Norman MG, Roberts M, Sirois J, et al. Lissencephaly. Can J Neurol Sci 1976;3:39. Norman RM. Cerebellar hypoplasia in Werdnig-Hoffmann disease. Arch Dis Child 1961;36:96. Northrup H, Volcik KA. Spina bifida and other neural tube defects. Curr Probl Pediatr 2000;30:313. Nowak DA, Trost HA. Lhermitte-Duclos disease (dysplastic cerebellar gangliocytoma): A malformation, hamartoma or neoplasm? Acta Neurol Scand 2002;105:137.
483
Nugent FR, Al-Mefty O, Chou S. Communicating hydrocephalus as a cause of aqueductal stenosis. J Neurosurg 1979;51:812. Nuytinck L, Coppin C, De Paepe A. A four base pair insertion polymorphism in the 3′ untranslated region of the COL1A1 gene is highly informative for null-allele testing in patients with osteogenesis imperfecta type I. Matrix Biol 1998;16:349. O’Brien MS, Harris ME. Long-term results in the treatment of hydrocephalus. Neurosurg Clin N Am 1993;4:625. O’Broin ES, Allcutt D, Earley MJ. Posterior plagiocephaly: Proactive conservative management. Br J Plast Surg 1999;52:18. O’Driscoll M, Ruiz-Perez VL, Woods CG, et al. A splicing mutation affecting expression of ataxia-telangiectasia and Rad3-related protein (Atr) results in Seckel syndrome. Nat Genet 2003;33:497. Ohnuma K, Imaizumi K, Masuno M, et al. Magnetic resonance imaging abnormalities of the brain in Goldberg-Shprintzen syndrome. Am J Med Genet 1997;73:230. Oi S, Honda Y, Hidaka M, et al. Intrauterine high-resolution magnetic resonance imaging in fetal hydrocephalus and prenatal estimation of postnatal outcomes with “perspective classification.” J Neurosurg 1998;88:685. Oi S, Matsumoto S. A proposed grading and scoring system for spina bifida: Spina Bifida Neurological Scale (SBNS). Childs Nerv Syst 1992;8:337. Okajima K, Ito T, Wakita A, et al. Male siblings with dyserythropoiesis, microcephaly and intrauterine growth retardation. Clin Dysmorphol 2002;11:107. Okkerse JM, Beemer FA, de Jong TH, et al. Condition variables in children with craniofacial anomalies: A descriptive study. J Craniofac Surg 2004;15:151. Okumura K, Sasaki Y, Ohyama M, et al. Bannayan syndrome—generalized lipomatosis associated with megalencephaly and macrodactyly. Acta Pathol Jpn 1986;36:269. Oldfield EH, Muraszko K, Shawker TH, et al. Pathophysiology of syringomyelia associated with Chiari I malformation of the cerebellar tonsils. Implications for diagnosis and treatment. J Neurosurg 1994;80:3. Olsen CL, Hughes JP, Youngblood LG, et al. The epidemiology of holoprosencephaly and phenotypic characteristics of affected children: New York State, 1984-1989. Am J Med Genet 1997;73. OMIM. Online Mendelian Inheritance in Man, OMIM. URL: http://www.ncbi.nlm.nih.gov/omim/, J.H.U.B. McKusick-Nathans Institute for Genetic Medicine, MD) and National Center for Biotechnology Information, National Library of Medicine. Bethesda, MD, 2000. O’Neill OR, Piatt JH Jr, Mitchell P, Roman-Goldstein S. Agenesis and dysgenesis of the sacrum: Neurosurgical implications. Pediatr Neurosurg 1995;22:20. Opitz JM, Holt MC. Microcephaly: General considerations and aids to nosology. J Craniofac Genet Dev Biol 1990;10:175. O’Rahilly R, Muller F. The embryonic human brain: An atlas of developmental stages. New York: Wiley-Liss, 1994. Orchard PJ, Dahl N, Aukerman SL, et al. Circulating macrophage colony-stimulating factor is not reduced in malignant osteopetrosis. Exp Hemat 1992;20:103. Osaka K, Tanimura T, Hirayama A, Matsumoto S. Myelomeningocele before birth. J Neurosurg 1978;49:711. Osawa M, Arai Y, Ikenaka H, et al. Fukuyama type congenital progressive muscular dystrophy. Acta Paediatr Jpn 1991;33:261. Otto F, Kanegane H, Mundlos S. Mutations in the RUNX2 gene in patients with cleidocranial dysplasia. Hum Mutat 2002;19:209. Otto F, Lubbert M, Stock M. Upstream and downstream targets of Runx proteins. J Cell Biochem 2003;89:9. Ou CY, Stevenson RE, Brown VK, et al. 5,10 Methylenetetrahydrofolate reductase genetic polymorphism as a risk factor for neural tube defects. Am J Med Genet 1996;63:610. Ouellette EM, Rosett HL, Rosman NP, et al. Adverse effects on offspring of maternal alcohol abuse during pregnancy. N Engl J Med 1977;297:528. Owens DF, Kriegstein AR. Is there more to GABA than synaptic inhibition? Nat Rev Neurosci 2002;3:715. Oyamada MK, Ferreira HS, Hoff M. Pfeiffer syndrome type 2—case report. Sao Paulo Med J 2003;121:176. Ozonoff S, Williams BJ, Gale S, Miller JN. Autism and autistic behavior in Joubert syndrome. J Child Neurol 1999;14:636. Packard AM, Miller VS, Delgado MR. Schizencephaly: Correlations of clinical and radiologic features. Neurology 1997;48:1427. Paek BW, Farmer DL, Wilkinson CC, et al. Hindbrain herniation develops in surgically created myelomeningocele but is absent after repair in fetal lambs. Am J Obstet Gynecol 2000;183:1119.
484
Perinatal Acquired and Congenital Neurologic Disorders / 19
Pagon RA, Chandler JW, Collie WR, et al. Hydrocephalus, agyria, retinal dysplasia, encephalocele (HARD +/– E) syndrome: An autosomal recessive condition. Birth Defects Orig Artic Ser 1978;14:233. Palm L, Hagerstrand I, Kristoffersson U, et al. Nephrosis and disturbances of neuronal migration in male siblings—a new hereditary disorder? Arch Dis Child 1986;61:545. Palmini A, Andermann F, Aicardi J, et al. Diffuse cortical dysplasia, or the “double cortex” syndrome: The clinical and epileptic spectrum in 10 patients. Neurology 1991a;41:1656. Palmini A, Andermann F, Olivier A, et al. Neuronal migration disorders: A contribution of modern neuroimaging to the etiologic diagnosis of epilepsy. Can J Neurol Sci 1991b;18 (4 Suppl):580. Palmini A, Najm I, Avanzini G, et al. Terminology and classification of the cortical dysplasias. Neurology 2004;62 (6 Suppl 3):S2. Panchal J, Amirsheybani H, Gurwitch R, et al. Neurodevelopment in children with single-suture craniosynostosis and plagiocephaly without synostosis. Plast Reconstr Surg 2001;108:1492. Panchal J, Uttchin V. Management of craniosynostosis. Plast Reconstr Surg 2003;111:2032. Pang D. Sacral agenesis and caudal spinal cord malformations. Neurosurgery 1993;32:755-778; discussion 778. Pang D, Dias MS, Ahab-Barmada M. Split cord malformation: Part I: A unified theory of embryogenesis for double spinal cord malformations. Neurosurgery 1992;31:451. Papay FA, Morales L Jr, Flaharty P, et al. Optic nerve decompression in cranial base fibrous dysplasia. J Craniofac Surg 1995;6:5. Parekh SG, Donthineni-Rao R, Ricchetti E, et al. Fibrous dysplasia. J Am Acad Orthop Surg 2004;12:305. Parisi MA, Bennett CL, Eckert ML, et al. The NPHP1 gene deletion associated with juvenile nephronophthisis is present in a subset of individuals with Joubert syndrome. Am J Hum Genet 2004;75:82. Parisi MA, Dobyns WB. Human malformations of the midbrain and hindbrain: Review and proposed classification scheme. Mol Genet Metab 2003;80:36. Parsch CS, Krauss J, Hofmann E, et al. Arachnoid cysts associated with subdural hematomas and hygromas: Analysis of 16 cases, long-term follow-up, and review of the literature. Neurosurgery 1997;40:483. Pascual-Castroviejo I, Roche MC, Martinez Bermejo A, et al. Primary intracranial arachnoidal cysts. A study of 67 childhood cases. Childs Nerv Syst 1991;7:257. Patel MD, Filly AL, Hersh DR, et al. Isolated mild fetal cerebral ventriculomegaly: Clinical course and outcome. Radiology 1994;192:759. Paterson CR. Osteogenesis imperfecta and other heritable disorders of bone. Baillieres Clin Endocrinol Metab 1997;11:195. Pati S, Helmbrecht GD. Congenital schizencephaly associated with in utero warfarin exposure. Reprod Toxicol 1994;8:115. Pattison L, Crow YJ, Deeble VJ, et al. A fifth locus for primary autosomal recessive microcephaly maps to chromosome 1q31. Am J Hum Genet 2000;67:1578. Patton MA, Goodship J, Hayward R, et al. Intellectual development in Apert’s syndrome: A long term follow up of 29 patients. J Med Genet 1988;25:164. Pauli RM, Gilbert EF. Upper cervical cord compression as cause of death in osteogenesis imperfecta type II. J Pediatr 1986;108:579. Pauli RM, Horton VK, Glinski LP, et al. Prospective assessment of risks for cervicomedullary-junction compression in infants with achondroplasia. Am J Hum Genet 1995;56:732. Pauli RM, Scott CJ, Wassman ER, et al. Apnea and sudden unexpected death in infants with achondroplasia. J Pediatr 1984;104:342. Pavone L, Curatolo P, Rizzo R, et al. Epidermal nevus syndrome: A neurological variant with hemimegalencephaly, gyral malformation, mental retardation, seizures and facial hemihypertrophy. Neurology 1991;41:266. Paznekas WA, Cunningham ML, Howard TD, et al. Genetic heterogeneity of Saethre-Chotzen syndrome, due to TWIST and FGFR mutations. Am J Hum Genet 1998;62:1370. Peach B. Arnold-Chiari malformation: Anatomic features of 20 cases. Arch Neurol 1965;12:613. Peiffer A, Singh N, Leppert M, et al. Microcephaly with simplified gyral pattern in six related children. Am J Med Genet 1999;84:137. Pepin M, Atkinson M, Starman BJ, et al. Strategies and outcomes of prenatal diagnosis for osteogenesis imperfecta: A review of biochemical and molecular studies completed in 129 pregnancies. Prenat Diagn 1997;17:559. Perdigao PF, Pimenta FJ, Castro WH, et al. Investigation of the GSalpha gene in the diagnosis of fibrous dysplasia. Int J Oral Maxillofac Surg 2004;33:498. Persing J, James H, Swanson J, et al. Prevention and management of positional skull deformities in infants. American Academy of Pediatrics Committee on
Practice and Ambulatory Medicine, Section on Plastic Surgery and Section on Neurological Surgery. Pediatrics 2003;112:199. Petersen MC, Wolraich M, Sherbondy A, Wagener J. Abnormalities in control of ventilation in newborn infants with myelomeningocele. J Pediatr 1995;126:1011. Petersson S, Pedersen NL, Schalling M, et al. Primary megalencephaly at birth and low intelligence level. Neurology 1999a;53:1254. Petersson S, Sandberg Nordqvist A, Schalling M, et al. The megencephaly mouse has disturbances in the insulin-like growth factor (IGF) system. Brain Res Mol Brain Res 1999b;72:80. Petrini J, Damus K, Johnston RB Jr. An overview of infant mortality and birth defects in the United States. Teratology 1997;56:8. Phelan MC, Rogers RC, Clarkson KB, et al. Albright hereditary osteodystrophy and de1(2) (q37.3) in four unrelated individuals. Am J Med Genet 1995;58:1. Piao X, Basel-Vanagaite L, Straussberg R, et al. An autosomal recessive form of bilateral frontoparietal polymicrogyria maps to chromosome 16q12.2-21. Am J Hum Genet 2002;70:1028. Piao X, Hill RS, Bodell A, et al. G protein–coupled receptor–dependent development of human frontal cortex. Science 2004;303:2033. Piatt JH Jr, Carlson CV. Hydrocephalus and epilepsy: An actuarial analysis. Neurosurgery 1996;39:722. Pierre-Kahn A, Hirsch JF, Renier D, et al. Hydrocephalus and achondroplasia: A study of 25 observations. Child’s Brain 1980;7:205. Pijpers M, Poels PJ, Vaandrager JM, et al. Undiagnosed obstructive sleep apnea syndrome in children with syndromal craniofacial synostosis. J Craniofac Surg 2004;15:670. Pillay PK, Awad IA, Little JR, et al. Symptomatic Chiari malformation in adults: A new classification based on magnetic resonance imaging with clinical and prognostic significance. Neurosurgery 1991;28:639. Pilu G, Falco P, Gabrielli S, et al. The clinical significance of fetal isolated cerebral borderline ventriculomegaly: Report of 31 cases and review of the literature. Ultrasound Obstet Gynecol 1999;14:320. Pilz DT, Kuc J, Matsumoto N, et al. Subcortical band heterotopia in rare affected males can be caused by missense mutations in DCX (XLIS) or LIS1. Hum Mol Genet 1999;8:1757. Pilz DT, Matsumoto N, Minnerath S, et al. LIS1 and XLIS (DCX) mutations cause most classical lissencephaly, but different patterns of malformation. Hum Mol Genet 1998;7:2029. Pizzutillo PD, Woods M, Nicholson L, et al. Risk factors in Klippel-Feil syndrome. Spine 1994;19:2110. Placzek M. The role of the notochord and floor plate in inductive interactions. Curr Opin Genet Dev 1995;5:499. Plawner LL, Delgado MR, Miller VS, et al. Neuroanatomy of holoprosencephaly as a predictor of function: Beyond the face predicting the brain. Neurology 2002;59:1058. Plomp AS, Hamel BC, J, et al. Pfeiffer syndrome type 2: Further delineation and review of the literature. Am J Med Genet 1998;75:245. Poetke M, Frommeld T, Berlien HP. PHACE syndrome: New views on diagnostic criteria. Eur J Pediatr Surg 2002;12:366. Pollack I, Albright A, Adelson P, et al. A randomized, controlled study of a programmable shunt valve versus a conventional valve for patients with hydrocephalus. Neurosurgery 1999;45:1399. Pollack IF, Losken HW, Biglan AW. Incidence of increased intracranial pressure after early surgical treatment of syndromic craniosynostosis. Pediatr Neurosurg 1996;24:202. Pollack IF, Losken HW, Fasick P. Diagnosis and management of posterior plagiocephaly. Pediatrics 1997;99:180. Pollack IF, Pang D, Albright AL, Krieger D. Outcome following hindbrain decompression of symptomatic Chiari malformations in children previously treated with myelomeningocele closure and shunts. J Neurosurg 1992;77:881. Pollin TI, Dobyns WB, Crowe CA, et al. Risk of abnormal pregnancy outcome in carriers of balanced reciprocal translocations involving the Miller-Dieker syndrome (MDS) critical region in chromosome 17p13.3. Am J Med Genet 1999;85:369. Portnoy HD, Amirjamshidi A, Hoffman HJ, et al. Shunts: Which one, and why? Surg Neurol 1998;49:8. Posnick JC, Goldstein JA, Armstrong D, et al. Reconstruction of skull defects in children and adolescents by the use of fixed cranial bone grafts: Long-term results. Neurosurgery 1993;32:785. Posnick JC, Ruiz RL. The craniofacial dysostosis syndromes: Current surgical thinking and future directions. Cleft Palate Craniofac J 2000;37:433. Poussaint TY, Fox JW, Dobyns WB, et al. Periventricular nodular heterotopia in patients with filamin-1 gene mutations: Neuroimaging findings. Pediatr Radiol 2000;30:748.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Prabhu SS, Aldape KD, Bruner JM, Weinberg JS. Cowden disease with Lhermitte-Duclos disease: Case report. Can J Neurol Sci 2004;31:542. Prescott NJ, Winter RM, Malcolm S. Maternal MTHFR genotype contributes to the risk of non-syndromic cleft lip and palate. J Med Genet 2002;39:368. Proudman TW, Clark BE, Moore MH, et al. Central nervous system imaging in Crouzon’s syndrome. J Craniofac Surg 1995;6:401. Przybylski GJ, Pollack IF, Ward WT. Monostotic fibrous dysplasia of the thoracic spine. A case report. Spine 1996;21:860. Przylepa KA, Paznekas W, Zhang M, et al. Fibroblast growth factor receptor 2 mutations in Beare-Stevenson cutis gyrata syndrome. Nat Genet 1996;13:492. Quigley MR, Reigel DH, Kortyna R. Cerebrospinal fluid shunt infections: Report of 41 cases and a critical review of the literature. Pediatr Neurosci 1989;15:111. Raas-Rothschild A, Goodman RM, Grunbaum M, et al. Klippel-Feil anomaly with sacral agenesis: An additional subtype, type IV. J Craniofac Genet Dev Biol 1988;8:297. Raeder MB, Helland CA, Hugdahl K, et al. Arachnoid cysts cause cognitive deficits that improve after surgery. Neurology 2005;64:160. Raffel C, McComb JG. To shunt or to fenestrate: Which is the best treatment for arachnoid cysts in pediatric patients? Neurosurgery 1988;23:338. Rahbar R, Resto VA, Robson CD, et al. Nasal glioma and encephalocele: Diagnosis and management. Laryngoscope 2003;113:2069. Raible F, Brand M. Divide et impera—the midbrain-hindbrain boundary and its organizer. Trends Neurosci 2004;27:727. Rajab A, Mochida GH, Hill A, et al. A novel form of pontocerebellar hypoplasia maps to chromosome 7q11-21. Neurology 2003;60:1664. Ramaekers VT, Heimann G, Reul J, et al. Genetic disorders and cerebellar structural abnormalities in childhood. Brain 1997;120:1739. Ramer JC, Lin AE, Dobyns WB, et al. Previously apparently undescribed syndrome: Shallow orbits, ptosis, coloboma, trigonocephaly, gyral malformations, and mental and growth retardation. Am J Med Genet 1995;57:403. Ramirez D, Lammer EJ, Johnson CB, et al. Autosomal recessive frontotemporal pachygyria. Am J Med Genet 2004;124A:231. Ramirez F, Pereira L. The fibrillins. Int J Biochem Cell Biol 1999;31:255. Rannan-Eliya SV, Taylor IB, De Heer IM, et al. Paternal origin of FGFR3 mutations in Muenke-type craniosynostosis. Hum Genet 2004;115:200. Rasmussen SA, Moore CA, Khoury MJ, et al. Descriptive epidemiology of holoprosencephaly and arhinencephaly in metropolitan Atlanta, 1968-1992. Am J Med Genet 1996;66:320. Rauch F, Glorieux FH. Osteogenesis imperfecta. Lancet 2004;363:1377. Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: Embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989;31:109. Reardon W, Wilkes D, Rutland P, et al. Craniosynostosis associated with FGFR3 Pro250-to-Arg mutation results in a range of clinical presentations including unisutural sporadic craniosynostosis. J Med Genet 1997;34:632. Reardon W, Winter RM, Rutland P, et al. Mutations in the fibroblast growth factor receptor 2 gene cause Crouzon syndrome. Nat Genet 1994;8:98. Rees H, Ang LC, Casey R, et al. Association of infantile neuroaxonal dystrophy and osteopetrosis: A rare autosomal recessive disorder. Pediatr Neurosurg 1995;22:321. Reid CS, Ryeritz RE, Kopits SE, et al. Cervicomedullary compression in young patients with achondroplasia: Value of comprehensive neurologic and respiratory evaluation. J Pediatr 1987;110:522. Reiner D, Arnaud E, Cinalli G, et al. Prognosis for mental function in Apert’s syndrome. J Neurosurg 1996;85:66. Reinus WR, McAlister WH, Schranck F, et al. Differing lumbar vertebral mineralization rates in ambulatory pediatric patients with osteogenesis imperfecta. Calcif Tissue Int 1998;62:17. Rekate HL. Occipital plagiocephaly: A critical review of the literature. J Neurosurg 1998;89:24. Rekate HL. Recent advances in the understanding and treatment of hydrocephalus. Semin Pediatr Neurol 1997;4:167. Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial cysts. J Neuropathol Exp Neurol 1981;40:61. Renier D, Lajeunie E, Arnaud E, et al. Management of craniosynostosis. Childs Nerv Syst 2000;16:645. Renier D, Sainte-Rose C, Marchac D, et al. Intracranial pressure in craniosynostosis. J Neurosurg 1982;57:370. Richman LC, Ryan SM. Do the reading disabilities of children with cleft fit into current models of developmental dyslexia? Cleft Palate Craniofac J 2003;40:154. Riedl SW, Mullner-Eidenbock A, Prayer D, et al. Auxological, ophthalmological, neurological and MRI findings in 25 Austrian patients
485
with septo-optic dysplasia (SOD). Preliminary data. Horm Res 2002;58 (Suppl 3):16. Riminucci M, Fisher LW, Shenker A, et al. Fibrous dysplasia of bone in the McCune-Albright syndrome: Abnormalities in bone formation. Am J Pathol 1997;151:1587. Ringel MD, Schwindinger WF, Levine MA. Clinical implications of genetic defects in G proteins. The molecular basis of McCune-Albright syndrome and Albright hereditary osteodystrophy. Medicine (Baltimore) 1996;75:171 Rintoul NE, Sutton LN, Hubbard AM, et al. A new look at myelomeningoceles: Functional level, vertebral level, shunting, and the implications for fetal intervention. Pediatrics 2002;109:409. Ritscher D, Schinzel A, Boltshauser E, et al. Dandy-Walker(like) malformation, atrio-ventricular septal defect and a similar pattern of minor anomalies in 2 sisters: A new syndrome? Am J Med Genet 1987;26:481. Roach E, Demyer W, Conneally PM, et al. Holoprosencephaly: Birth data, genetic and demographic analyses of 30 families. Birth Defects Orig Artic Ser 1975;11:294. Robain O, Lyon G. Familial micrencephalies due to cerebral malformation: Clinical and anatomical review. Act Neuropathol (Berlin) 1972;20:96. Roberts E, Hampshire DJ, Pattison L, et al. Autosomal recessive primary microcephaly: An analysis of locus heterogeneity and phenotypic variation. J Med Genet 2002;39:718. Roberts E, Jackson AP, Carradice AC, et al. The second locus for autosomal recessive primary microcephaly (MCPH2) maps to chromosome 19q13.1-13.2. Eur J Hum Genet 1999;7:815. Robin NH, Scott JA, Arnold JE, et al. Favorable prognosis for children with Pfeiffer syndrome types 2 and 3: Implications for classification. Am J Med Genet 1998;75:240. Robinson RO. Familial schizencephaly. Dev Med Child Neurol 1991;33:1010. Robinson S, Cohen AR. Cowden disease and Lhermitte-Duclos disease: Characterization of a new phakomatosis. Neurosurgery 2000;46:371. Rodenberg J, Jensen OM, Keller J, et al. Fibrous dysplasia of the spine, costae and hemipelvis with sarcomatous transformation. Skeletal Radiol 1996;25:682. Rodriguez JI, Garcia M, Morales C, et al. Trisomy 13 syndrome and neural tube defects. Am J Med Genet 1990;36:513. Roessler E, Muenke M. How a hedgehog might see holoprosencephaly. Hum Mol Genet 2003;12:R15. Roessler E, Belloni E, Gaudenz K, et al. Mutations in the human Sonic hedgehog gene cause holoprosencephaly. Nat Genet 1996;14:357. Rojiani AM, Emery JA, Anderson KJ, et al. Distribution of heterotopic neurons in normal hemispheric white matter: A morphometric analysis. J Neuropathol Exp Neurol 1996;55:178. Rosano A, Botto LD, Botting B, Mastroiacovo P. Infant mortality and congenital anomalies from 1950 to 1994: An international perspective. J Epidemiol Comm Health 2000;54:660. Roscioli T, Flanagan S, Mortimore RJ, et al. Premature calvarial synostosis and epidermal hyperplasia (Beare-Stevenson syndrome–like anomalies) resulting from a P250R missense mutation in the gene encoding fibroblast growth factor receptor 3. Am J Med Genet 2001;101:187. Rosen CL, Novotny EJ, D’Andrea LA, et al. Klippel-Feil sequence and sleep-disordered breathing in two children. Am Rev Respir Dis 1993;147:202. Rosenberg MJ, Agarwala R, Bouffard G, et al. Mutant deoxynucleotide carrier is associated with congenital microcephaly. Nat Genet 2002;32:175. Rosman NP, Shands KN. Hydrocephalus caused by increased intracranial venous pressure: A clinicopathological study. Ann Neurol 1978;3:445. Ross AJ, Ruiz-Perez V, Wang Y, et al. A homeobox gene, HLXB9, is the major locus for dominantly inherited sacral agenesis. Nat Genet 1998;20:358-361. Ross DL, Liwnicz BH, Chun RWM, et al. Hypomelanosis of Ito (incontinentia pigmenti achromians)—a clinicopathologic study: Macrocephaly and gray matter heterotopias. Neurology 1982;32:1013. Ross JJ, Frias JL. Microcephaly. In: Vinken PJ, Bruyu GW, eds. Congenital malformations of the brain and skull, part 1. Amsterdam: Elsevier Holland Biomedical Press, 1977, p 507. Ross ME. Full circle to cobbled brain. Nature 2002;418:376. Ross ME, Allen KM, Srivastava AK, et al. Linkage and physical mapping of xlinked lissencephaly/SBH (XLIS): A gene causing neuronal migration defects in human brain. Human Molecular Genetics 1997;6:555. Ross ME, Swanson K, Dobyns WB. Lissencephaly with cerebellar hypoplasia (LCH): A heterogeneous group of cortical malformations. Neuropediatrics 2001;32:256. Rossbach HC, Sutcliffe MJ, Haag MM, et al. Fanconi anemia in brothers initially diagnosed with VACTERL association with hydrocephalus, and subsequently with Baller-Gerold syndrome. Am J Med Genet 1996;61:65.
486
Perinatal Acquired and Congenital Neurologic Disorders / 19
Rossi M, Guerrini R, Dobyns WB, et al. Characterization of brain malformations in the Baraitser-Winter syndrome and review of the literature. Neuropediatrics 2003;34:287. Rothenberg SP, da Costa MP, Sequeira JM, Cracco J, et al. Autoantibodies against folate receptors in women with a pregnancy complicated by a neural-tube defect. N Engl J Med 2004;350:134. Rouse B, Azen C, Koch R, et al. Maternal Phenylketonuria Collaborative Study (MPKUCS) offspring: Facial anomalies, malformations, and early neurological sequelae. Am J Med Genet 1997;69:89. Rousseau F, Bonaventure J, Legeai-Mallet L, et al. Mutations in the gene encoding fibroblast growth factor receptor-3 in achondroplasia. Nature 1994;371:252. Rouviere S, Michelini R, Sarda P, et al. Spontaneous carotid artery dissection in two siblings with osteogenesis imperfecta. Cerebrovasc Dis 2004;17:270. Rouvreau P, Glorion C, Langlais J, et al. Assessment and neurologic involvement of patients with cervical spine congenital synostosis as in Klippel-Feil syndrome: Study of 19 cases. J Pediatr Orthop B 1998;7:179. Rubenstein JLR, Puelles L. Development of the nervous system. In: Epstein CJ, Erickson RP, Wynshaw-Boris A, eds. Inborn errors of development. Oxford: Oxford University Press, 2004:75. Rubin RC, Hochwald G, Liwnicz B, et al. The effect of severe hydrocephalus on size and number of brain cells. Dev Med Child Neurol 1972;27 (Suppl):117. Rudnik-Schoneborn S, Sztriha L, Aithala GR, et al. Extended phenotype of pontocerebellar hypoplasia with infantile spinal muscular atrophy. Am J Med Genet A 2003;117:10. Ruggieri P, Sim FH, Bond JR, et al. Malignancies in fibrous dysplasia. Cancer 1994;73:1411. Ruiz Garcia M, Tovar Baudin A, Del Castillo Ruiz V, et al. Early detection of neurological manifestations in achondroplasia. Childs Nerv Syst 1997;13:208. Ryken TC, Menezes AH. Cervicomedullary compression in achondroplasia. J Neurosurg 1994;81:43. Rypens F, Sonigo P, Aubry MC, et al. Prenatal MR diagnosis of a thick corpus callosum. AJNR Am J Neuroradiol 1996;17:1918. Saal HM, Bulas DI, Allen JF, et al. Patient with craniosynostosis and marfanoid phenotype (Shprintzen-Goldberg syndrome) and cloverleaf skull. Am J Med Genet 1995;57:573. Sadler TW. Langman’s medical embryology. Baltimore: Williams & Wilkins, 1995. Sadove AM, van Aalst JA, Culp JA. Cleft palate repair: Art and issues. Clin Plast Surg 2004;31:231. Saine-Rose C, LaCombe J, Pierre-Kahn A, et al. Intracranial venous sinus hypertension: Cause or consequence of hydrocephalus in infants? J Neurosurg 1984;60:727. Salkind G, Sutton LN, Bruce DA, et al. Management of trigonocephaly. Surg Neurol 1986;25:159. Santavuori P, Somer H, Sainio K, et al. Muscle-eye-brain disease (MEB). Brain Dev 1989;11:147. Sari A, Demirci A. Radiographic type I autosomal dominant osteopetrosis with syringohydromyelia. Neuroradiology 1996;38:532. Sarimski K. Cognitive functioning of young children with Apert’s syndrome. Genet Couns 1997;8:317. Sarnat HB, Flores-Sarnat L. Cajal-Retzius and subplate neurons: Their role in cortical development. Europ J Paediatr Neurol 2002;6:91. Sarnat HB. Cerebral dysgenesis: Embryology and clinical expression. New York: Oxford University Press, 1992. Savarirayan R, Thompson EM, Abbott KJ, et al. Cerebral cortical dysplasia and digital constriction rings in Adams-Oliver syndrome. Am J Med Genet 1999;86:15. Sawaya R, McLaurin RL. Dandy-Walker syndrome. Clinical analysis of 23 cases. J Neurosurg 1981;55:89. Sawin PD, Menezes AH. Basilar invagination in osteogenesis imperfecta and related osteochondrodysplasias: Medical and surgical management. J Neurosurg 1997;86:950. Sawin PD, Muhonen MG, Menezes AH. Quantitative analysis of cerebrospinal fluid spaces in children with occipital plagiocephaly. J Neurosurg 1996;85:428. Sayre MR, Roberge RJ, Evans TC. Non-traumatic subdural hematoma in a patient with osteogenesis imperfecta and renal failure. Am J Emerg Med 1987;5:298. Schady W, Metcalfe RA, Butler P. The incidence of craniocervical bony anomalies in the adult Chiari malformation. J Neurol Sci 1987;82:193. Schaefer GB, Bodensteiner JB, Buehler BA, et al. The neuroimaging findings in Sotos syndrome. Am J Med Genet 1997;68:462.
Scheffer IE, Wallace RH, Phillips FL, et al. X-linked myoclonic epilepsy with spasticity and intellectual disability: Mutation in the homeobox gene ARX. Neurology 2002;59:348. Schell U, Hehr A, Feldman GJ, et al. Mutations in FGFR1 and FGFR2 cause familial and sporadic Pfeiffer syndrome. Hum Mol Genet 1995;4:323. Scherer A, Messing-Junger AM, Lackmann GM. Cleidocranial dysostosis, unilateral sensorineural hearing loss and gait disturbances: A clear-cut case of diagnostic mimicry? Neuropediatrics 2001;32:275. Scherer NJ, D’Antonio LL. Parent questionnaire for screening early language development in children with cleft palate. Cleft Palate Craniofac J 1995;32:7. Schneidau T, Franco I, Zebold K, Kaplan W. Selective sacral rhizotomy for the management of neurogenic bladders in spina bifida patients: Long-term follow-up. J Urol 1995;154:766. Schnitt DE, Agir H, David DJ. From birth to maturity: A group of patients who have completed their protocol management. Part I. Unilateral cleft lip and palate. Plast Reconstr Surg 2004;113:805. Schoenau E, Rauch F. Fibrous dysplasia. Horm Res 2002;57 (Suppl 2):79. Schrander-Stumpel CT, Fryns JP. Congenital hydrocephalus: Nosology and guidelines for clinical approach and genetic counselling. Eur J Pediatr 1998;157:355. Schrander-Stumpel CT. What’s in a name? Am J Med Genet 1998;79:228. Seckel HPG. Bird-headed dwarfs: Studies in developmental anthropology including human proportions. Springfield, Ill: Charles C Thomas, 1960. Seiff SR. Optic nerve decompression in fibrous dysplasia: Indications, efficacy, and safety. Plast Reconstr Surg 1997;100:1611. Seller MJ, Mazzaschi R, Ogilvie CM, Mohammed S. A trisomy 2 fetus with severe neural tube defects and other abnormalities. Clin Dysmorphol 2004;13:25. Sells CJ. Microcephaly in a normal school population. Pediatrics 1977;59:262. Senat MV, Bernard JP, Schwarzler P et al. Prenatal diagnosis and follow up of 14 cases of unilateral ventriculomegaly. Ultrasound Obstet Gynecol 1999;14:327. Sener RN. An extensive type of polyostotic fibrous dysplasia. Pediatr Radiol 1997a;27:339. Sener RN. Schizencephaly and congenital cytomegalovirus infection. J Neuroradiol 1998;25:151. Sener RN. Septo-optic dysplasia associated with cerebral cortical dysplasia (cortico-septo-optic dysplasia). J Neuroradiol 1996;23:245. Seow WK, Hertzberg J. Dental development and molar root length in children with cleidocranial dysplasia. Pediatr Dent 1995;17:101. Sepulveda W, Dezerega V. First-trimester sonographic diagnosis of holoprosencephaly. J Ultrasound Med 2004;23:761. Sertie AL, Quimby M, Moreira ES, et al. A gene which causes severe ocular alterations and occipital encephalocele (Knobloch syndrome) is mapped to 21q22.3. Hum Mol Genet 1996;5:843. Seto ML, Lee SJ, Sze RW, et al. Another TWIST on Baller-Gerold syndrome. Am J Med Genet 2001;104:323. Sgouros S, Goldin JH, Hockley AD, et al. Posterior skull surgery in craniosynostosis. Childs Nerv Syst 1996a;12:727. Sgouros S, Goldin JH, Hockley AD, et al. Surgery for unilateral coronal synostosis (plagiocephaly): Unilateral or bilateral correction? J Craniofac Surg 1996b;7:284. Sgouros S, Malluci C, Walsh AR, Hockley AD. Long-term complications of hydrocephalus. Pediatr Neurosurg 1995;23:127. Shanske A, Caride DG, Menasse-Palmer L, et al. Central nervous system anomalies in Seckel syndrome: Report of a new family and review of the literature. Am J Med Genet 1997;70:155. Shapira SK, Heilstedt HA, Starkey DE, et al. Clinical and pathological characterization of epilepsy in patients with monosomy 1p36 and the search for candidate genes (abstract 564). Am J Hum Genet 1999;65(4 Suppl):A107. Shaw GM, Lammer EJ. Maternal periconceptional alcohol consumption and risk for orofacial clefts. J Pediatr 1999;134:298. Shaw GM, Wasserman CR, Lammer EJ, et al. Orofacial clefts, parental cigarette smoking, and transforming growth factor-alpha gene variants. Am J Hum Genet 1996;58:551. Shaw GM, Wasserman CR, Murray JC, et al. Infant TGFalpha genotype, orofacial clefts, and maternal periconceptional multivitamin use. Cleft Palate Craniofac J 1998;35:366. Shaw NJ. Bisphosphonates in osteogenesis imperfecta. Arch Dis Child 1997;77:92. Sheen VL, Dixon PH, Fox JW, et al. Mutations in the X-linked filamin 1 gene cause periventricular nodular heterotopia in males as well as in females. Hum Mol Genet 2001;10:1775.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Sheen VL, Ganesh VS, Topcu M, et al. Mutations in ARFGEF2 implicate vesicle trafficking in neural progenitor proliferation and migration in the human cerebral cortex. Nat Genet 2004;36:69. Sheen VL, Topcu M, Berkovic S, et al. Autosomal recessive form of periventricular heterotopia. Neurology 2003a;60:1108. Sheen VL, Wheless JW, Bodell A, et al. Periventricular heterotopia associated with chromosome 5p anomalies. Neurology 2003b;60:1033. Shenefelt RE. Morphogenesis of malformations in hamsters caused by retinoic acid: Relation to dose and stage at treatment. Teratology 1972;5:103. Shevell MI, Majnemer A. Clinical features of developmental disability associated with cerebellar hypoplasia. Pediatr Neurol 1996;15:224. Shiang R, Thompson LM, Zhu YZ, et al. Mutations in the transmembrane domain of FGFR3 cause the most common genetic form of dwarfism, achondroplasia. Cell 1994;78:335. Shigematsu H, Takashima S, Otani K, et al. Neuropathological and Golgi study on a case of thanatophotoric dysplasia. Brain Dev 1985;7:628. Shimamura K, Hartigan DJ, Martinez S, et al. Longitudinal organization of the anterior neural plate and neural tube. Development 1995;121:3923. Shipster C, Hearst D, Dockrell JE, et al. Speech and language skills and cognitive functioning in children with Apert syndrome: A pilot study. Int J Lang Commun Disord 2002;37:325. Shipster C, Hearst D, Somerville A, et al. Speech, language, and cognitive development in children with isolated sagittal synostosis. Dev Med Child Neurol 2003;45:34. Shohat M, Flaum E, Cobb SR, et al. Hearing loss and temporal bone structure in achondroplasia. Am J Med Genet 1993;45:548. Shohat M, Tick D, Barakat S, et al. Short-term recombinant human growth hormone treatment increases growth rate in achondroplasia. J Clin Endocrinol Metab 1996;81:4033. Shrimpton AE, Braddock BR, Hoo JJ. Narrowing the map of a gene (MRXS9) for X-linked mental retardation, microcephaly, and variably short stature at Xq12-q21.31. Am J Med Genet 2000;92:155. Shurtleff DB, Stuntz JT, Hayden PW. Experience with 1201 cerebrospinal fluid shunt procedures. Pediatr Neurosci 1985-86;12:49. Shuster BA, Norbash AM, Schendel SA. Correction of scaphocephaly secondary to ventricular shunting procedures. Plast Reconstr Surg 1995;96:1012. Sicca F, Kelemen A, Genton P, et al. Mosaic mutations of the LIS1 gene cause subcortical band heterotopia. Neurology 2003;61:1042. Siddiqi SN, Posnick JC, Buncic R, et al. The detection and management of intracranial hypertension after initial suture release and decompression for craniofacial dysostosis syndromes. Neurosurgery 1995;36:703. Sidman RL, Rakic P. Development of the human central nervous system. In: Haymaker W, Adams RD, eds. Histology and histopathology of the nervous system. Springfield, Ill: Charles C Thomas, 1982, p 3. Sidoti EJ Jr, Marsh JL, Marty-Grames L, et al. Long-term studies of metopic synostosis: Frequency of cognitive impairment and behavioral disturbances. Plast Reconstr Surg 1996;97:276. Siebert JR, Cohen MM, Sulik KK, et al. Holoprosencephaly. An overview and atlas of cases. New York: Wiley-Liss, 1990. Siffel C, Wong LY, Olney RS, Correa A. Survival of infants diagnosed with encephalocele in Atlanta, 1979-98. Paediatr Perinat Epidemiol 2003;17:40. Sigaudy S, Toutain A, Moncla A, et al. Microcephalic osteodysplastic primordial dwarfism Taybi-Linder type: Report of four cases and review of the literature. Am J Med Genet 1998;80:16. Silan F, Yoshioka M, Kobayashi K, et al. A new mutation of the fukutin gene in a non-Japanese patient. Ann Neurol 2003;53:392. Silveri M, Capitanucci ML, Capozza N, et al. Occult spinal dysraphism: Neurogenic voiding dysfunction and long-term urologic follow-up. Pediatr Surg Int 1997;12:148. Simeoni J, Guys JM, Mollard P, et al. Artificial urinary sphincter implantation for neurogenic bladder: A multi-institutional study in 107 children. Br J Urol 1996;78:287. Simon EM, Hevner R, Pinter JD. The dorsal cyst in holoprosencephaly and the role of the thalamus in its formation. Neuroradiology 2001;43:787. Simon EM, Hevner R, Pinter JD, et al. Assessment of the deep gray nuclei in holoprosencephaly. Am J Neuroradiol 2000;21:1955. Simon EM, Hevner R, Pinter JD, et al. The middle interhemispheric variant of holoprosencephaly. Am J Neuroradiol 2002;23:151. Simonds JF, Heimburger RE. Psychiatric evaluation of youth with cleft lip-palate matched with a control group. Cleft Palate J 1978;15:193. Singhal B, Mathew KM. Factors affecting mortality and morbidity in adult spina bifida. Eur J Pediatr Surg 1999;9(Suppl 1):31. Sinha S, Brown JI. Familial posterior fossa arachnoid cyst. Childs Nerv Syst 2004;20:100.
487
Sisodiya SM, Free SL, Thom M, et al. Evidence for nodular epileptogenicity and gender differences in periventricular nodular heterotopia. Neurology 1999;52:336. Sleigh G, Dawson A, Penny WJ. Cor pulmonale as a complication of ventriculo-atrial shunts reviewed. Dev Med Child Neurol 1993;35:74. Slight P, Gundling K, Plotkin SA, et al. A trial of vancomycin for prophylaxis of infections after neurosurgical shunts. N Engl J Med 1985;312:921. Smith BA, Griffin C. Klippel-Feil syndrome. Ann Emerg Med 1992;21:876. Snodgrass WT, Adams R. Initial urologic management of myelomeningocele. Urol Clin North Am 2004;31:427. Soekarman D, Fryns JP, van den Berghe H. Pfeiffer acrocephalosyndactyly syndrome in mother and son with cloverleaf skull anomaly in the child. Genet Couns 1992;3:217. Soler R, Ivanez V, Munoz-Torrero JJ, et al. Epileptic seizures as the first sign of fibrous bone dysplasia. Rev Neurol 1999;28:976. Solh H, Da Cunha AM, Giri N, et al. Bone marrow transplantation for infantile malignant osteopetrosis. J Pediatr Hematol Oncol 1995;17:350. Sonigo-Cohen P, Schmit P, Zerah M, et al. Prenatal diagnosis of diastematomyelia. Childs Nerv Syst 2003;19:555. Sonstein WJ, Hall CD, Argamaso RV, et al. Management of secondary turricephaly in craniofacial surgery. Childs Nerv Syst 1996;12:705. Sood S, Eldadah ZA, Krause WL, et al. Mutation in fibrillin-1 and the marfanoid-craniosynostosis (Shprintzen-Goldberg) syndrome. Nat Genet 1996;12:209. Spataro RF, Lin SR, Horner FA, et al. Aqueductal stenosis and hydrocephalus: Rare sequelae of mumps virus infection. Neuroradiology 1976;12:11. Sperber GH. Craniofacial Development. New York: BC Decker, 2001. Spiegel AM. The molecular basis of disorders caused by defects in G proteins. Horm Res 1997;47:89. Spohr HL, Willms J, Steinhausen HC. Prenatal alcohol exposure and long-term developmental consequences. Lancet 1993;341:907. Spreer J, Ernestus RI, Lanfermann H, et al. Lesions of the corpus callosum in hydrocephalic patients with ventricular drainage—a CT study. Acta Neurochir Wien 1996;138:174. Stamoyannou L, Karachaliou F, Neou P, et al. Growth and growth hormone therapy in children with achondroplasia: A two-year experience. Am J Med Genet 1997;72:71. Stanhope R, Preece MA, Brook CG. Hypoplastic optic nerves and pituitary dysfunction. A spectrum of anatomical and endocrine abnormalities. Arch Dis Child 1984;59:111. Stanier P, Moore GE. Genetics of cleft lip and palate: Syndromic genes contribute to the incidence of non-syndromic clefts. Hum Mol Genet 2004;13 (Spec No 1):R73. Stankovic B, Krstic V, Stankov B, et al. Jackson-Weiss syndrome registered in four successive generations. The facies of Crouzon’s syndrome with foot abnormalities. Doc Ophthalmol 1994;85:281. Stashinko EE, Clegg NJ, Kammann HA, et al. A retrospective survey of perinatal risk factors of 104 living children with holoprosencephaly. Am J Med Genet 2004;128:114. Stavrou P, Sgouros S, Willshaw HE, et al. Visual failure caused by raised intracranial pressure in craniosynostosis. Childs Nerv Syst 1997;13:64. Stein SA, Witkop C, Hill S, et al. Sclerostenosis: Neurogenetic and pathophysiologic analysis of an American kinship. Neurology 1983;33:267. Stein SC, Schut L. Hydrocephalus in myelomeningocele. Childs Brain 1979;5:413. Steinberger D, Reinhartz T, Unsold R, et al. FGFR2 mutation in clinically nonclassifiable autosomal dominant craniosynostosis with pronounced phenotypic variation. Am J Med Genet 1996;66:81. Steinbok P. Dysraphic lesions of the cervical spinal cord. Neurosurg Clin North Am 1995;6:367. Steinbok P, Cochrane DD. Cervical spinal dysraphism. J Neurosurg 1995;83:569. Steinbok P, Irvine B, Cochrane DD, Irwin BJ. Long-term outcome and complications of children born with meningomyelocele. Childs Nerv Syst 1992;8:92. Steiner RD, Pepin, MG, Byers, PH. Osteogenesis imperfecta. Available at http://genetests.org/ and review under “Osteogenesis Imperfecta,” 2005. Steinlin M, Blaser S, Boltshauser E. Cerebellar involvement in metabolic disorders: A pattern-recognition approach. Neuroradiology 1998;40:347. Stevenson KL. Chiari type II malformation: Past, present, and future. Neurosurg Focus 2004;16:E5. Stevenson RE, Allen WP, Pai GS, et al. Decline in prevalence of neural tube defects in a high-risk region of the United States. Pediatrics 2000;106:677. Steward CG. Neurological aspects of osteopetrosis. Neuropathol Appl Neurobiol 2003;29:87.
488
Perinatal Acquired and Congenital Neurologic Disorders / 19
Stone AR, Silveri M, Capitanucci ML, et al. Neurourologic evaluation and urologic management of spinal dysraphism. Neurosurg Clin North Am 1995;6:269. Stoodley MA, Brown SA, Brown CJ, Jones NR. Arterial pulsation-dependent perivascular cerebrospinal fluid flow into the central canal in the sheep spinal cord. J Neurosurg 1997;86:686. Stovner LJ, Bergan U, Nilsen G, et al. Posterior cranial fossa dimensions in the Chiari I malformation: Relation to pathogenesis and clinical presentation. Neuroradiology 1993 35:113. Strauss RP, Broder H. Children with cleft lip/palate and mental retardation: A subpopulation of cleft-craniofacial team patients. Cleft Palate Craniofac J 1993;30:548. Straussberg R, Basel-Vanagaite L, Kivity S, et al. An autosomal recessive cerebellar ataxia syndrome with upward gaze palsy, neuropathy, and seizures. Neurology 2005;64:142. Straussberg R, Gross S, Amir J, et al. A new autosomal recessive syndrome of pachygyria. Clin Genet 1996;50:498. Strohecker B. External cranial vault molding helmets. Plast Surg Nurs 1996;16:74. Stromme P, Bakke SJ, Dahl A, et al. Brain cysts associated with mutation in the aristaless-related homeobox gene, ARX. J Neurol Neurosurg Psychiatry 2003;74:536. Stromme P, Mangelsdorf ME, Scheffer IE, et al. Infantile spasms, dystonia, and other X-linked phenotypes caused by mutations in aristaless-related homeobox gene, ARX. Brain Dev 2002a;24:266. Stromme P, Mangelsdorf ME, Shaw MA, et al. Mutations in the human ortholog of aristaless cause X-linked mental retardation and epilepsy. Nat Genet 2002b;30:441. Su YN, Lee CN, Chien SC, et al. Rapid detection of FGFR3 gene mutation in achondroplasia by DHPLC system-coupling heteroduplex and fluorescence-enhanced primer-extension analysis. J Hum Genet 2004;49:399. Sugama S, Kusano K. Monozygous twin with polymicrogyria and normal co-twin. Pediatr Neurol 1994;11:62. Sugimoto T, Yasuhara A, Nishida N, et al. MRI of the head in the evaluation of microcephaly. Neuropediatrics 1993;24:4. Sugio Y, Tsukahara M, Kajii T. Two Japanese cases with microcephalic primordial dwarfism: Classical Seckel syndrome and osteodysplastic primordial dwarfism type II. Jpn J Hum Genet 1993;38:209. Suh DY, Gaskill Shipley M, Nemann MW, et al. Corpus callosal changes associated with hydrocephalus: A report of two cases. Neurosurgery 1997;41:488. Sulik KK, Johnson MC. Embryonic origin of holoprosencephaly: Interrelationship of the developing brain and face. Scan Electron Microsc 1982; Pt 1:309. Supprian T, Sian J, Heils A, et al. Isolated absence of the septum pellucidum. Neuroradiology 1999;41:563. Sutton JB. The lateral recesses of the fourth ventricle: Their relation to certain cysts and tumors of the cerebellum and to occipital meningocele. Brain 1887;9:352. Swanenburg de Veye HF, Beemer FA, Mellenbergh GJ, et al. An investigation of the relationship between associated congenital malformations and the mental and psychomotor development of children with clefts. Cleft Palate Craniofac J 2003;40:297. Sztriha L, Nork M. Bilateral frontoparietal polymicrogyria and epilepsy. Pediatr Neurol 2000;22:240. Sztriha L, Al-Gazali L, Varady E, et al. Microlissencephaly. Pediatr Neurol 1998;18:362. Sztriha L, Al-Gazali LI, Varady E, et al. Autosomal recessive micrencephaly with simplified gyral pattern, abnormal myelination and arthrogryposis. Neuropediatrics 1999;30:141. Sztriha L, Guerrini R, Harding B, et al. Clinical, MRI, and pathological features of polymicrogyria in chromosome 22q11 deletion syndrome. Am J Med Genet 2004;127A:313. Taggart JK, Walker AE. Congenital atresia of the foramens of Luschka and Magendie. Arch Neurol Psychiatry 1942;48:583. Tajima S, Imai K. Obstructive sleep apnea attack in complex craniosynostosis. Acta Otolaryngol Suppl Stockh 1994;517:17. Tajima T, Hattorri T, Nakajima T, et al. Sporadic heterozygous frameshift mutation of HESX1 causing pituitary and optic nerve hypoplasia and combined pituitary hormone deficiency in a Japanese patient. J Clin Endocrinol Metab 2003;88:45. Takada K, Nakamura H, Takashima S. Cortical dysplasia in Fukuyama congenital muscular dystrophy (FCMD): A Golgi and angioarchitectonic analysis. Acta Neuropathol 1988;76:170.
Takada Y, Morimoto T, Sugawara T, et al. Trigeminal neuralgia associated with achondroplasia. Case report with literature review. Acta Neurochir (Wien) 2001;143:1173. Takahashi K, Nakanishi H, Miyahara M, et al. Nectin/PRR: An immunoglobulin-like cell adhesion molecule recruited to cadherin-based adherens junctions through interaction with afadin, a PDZ domaincontaining protein. J Cell Biol 1999;145:539. Talwar D, Baldwin MA, Horbatt CI, et al. Epilepsy in children with meningomyelocele. Pediatr Neurol 1995;13:29. Tan KL. Wide sutures and large fontanels in the newborn. Am J Dis Child 1976;130:386. Tanaka H, Ito J, Cho K, et al. Hirschsprung disease, unusual face, mental retardation, epilepsy, and congenital heart disease: Goldberg-Shprintzen syndrome. Pediatr Neurol 1993;9:479. Tanaka H. Achondroplasia: Recent advances in diagnosis and treatment. Acta Paediatr Jpn 1997;39:514. Taniguchi K, Kobayashi K, Saito K, et al. Worldwide distribution and broader clinical spectrum of muscle-eye-brain disease. Hum Mol Genet 2003;12:527. Tao J, Van Esch H, Hagedorn-Greiwe M, et al. Mutations in the X-linked cyclin–dependent kinase-like 5 (CDKL5/stk9) gene are associated with severe neurodevelopmental retardation. Am J Hum Genet 2004;75:1149. Tarhan E, Oguz H, Safak MA, et al. The Carpenter syndrome phenotype. Int J Pediatr Otorhinolaryngol 2004;68:353. Tassi L, Colombo N, Garbelli R, et al. Focal cortical dysplasia: Neuropathological subtypes, EEG, neuroimaging and surgical outcome. Brain 2002;125:1719. Taybi H. Microcephalic osteodysplastic primordial dwarfism and cephalo-skeletal dysplasia (Taybi-Linder syndrome). Am J Med Genet 1992;43:628. Taylor DC, Falconer MA, Bruton CJ, et al. Focal dysplasia of the cerebral cortex in epilepsy. J Neurol Neurosurg Psychiat 1971;34:369. Taylor WJ, Hayward RD, Lasjaunias P, et al. Enigma of raised intracranial pressure in patients with complex craniosynostosis: The role of abnormal intracranial venous drainage. J Neurosurg 2001;94:377. Teebi AS, Kennedy S, Chun K, et al. Severe and mild phenotypes in Pfeiffer syndrome with splice acceptor mutations in exon IIIc of FGFR2. Am J Med Genet 2002;107:43. Temtamy SA, Aglan MS, Nemat A, et al. Expanding the phenotypic spectrum of the Baller-Gerold syndrome. Genet Couns 2003;14:299. ten Donkelaar HJ, Wesseling P, Semmekrot BA, et al. Severe, non X-linked congenital microcephaly with absence of the pyramidal tracts in two siblings. Acta Neuropathol (Berl) 1999;98:203. Thauvoy C, Scholtes JL, Moulin D, et al. Craniostenosis and craniofacial dysmorphia. Acta Neurol Belg 1995;95:147. Thom M, Sisodiya S, Harkness W, et al. Microdysgenesis in temporal lobe epilepsy. A quantitative and immunohistochemical study of white matter neurones. Brain 2001;124:2299. Thomas IT, Frias JL, Williams JL, et al. Magnetic resonance imaging in the assessment of medullary compression in achondroplasia. Am J Dis Child 1988;142:989. Thomas JA, Manchester DK, Prescott KE, et al. Hunter-McAlpine craniosynostosis phenotype associated with skeletal anomalies and interstitial deletion of chromosome 17q. Am J Med Genet 1996;62:372. Thomas P, Bossan A, Lacour JP, et al. Ehlers-Danlos syndrome with subependymal periventricular heterotopias. Neurology 1996;46:1165. Thomas PQ, Dattani MT, Brickman JM, et al. Heterozygous HESX1 mutations associated with isolated congenital pituitary hypoplasia and septo-optic dysplasia. Hum Mol Genet 2001;10:39. Thompson DN, Harkness W, Jones B, et al. Subdural intracranial pressure monitoring in craniosynostosis: Its role in surgical management. Childs Nerv Syst 1995;11:269. Thompson NM, Hecht JT, Bohan TP, et al. Neuroanatomic and neuropsychological outcome in school-age children with achondroplasia. Am J Med Genet 1999;88:145. Tibbles L, Wiley MJ. A comparative study of the effects of retinoic acid given during the critical period for inducing spina bifida in mice and hamsters. Teratology 1988;37:113. Timmons MJ, Wyatt RA, Murphy T. Speech after repair of isolated cleft palate and cleft lip and palate. Br J Plast Surg 2001;54:377. Toelle SP, Yalcinkaya C, Kocer N, et al. Rhombencephalosynapsis: Clinical findings and neuroimaging in 9 children. Neuropediatrics 2002;33:209. Tokumaru AM, Barkovich AJ, Ciricillo SF, et al. Skull base and calvarial deformities: Association with intracranial changes in craniofacial syndromes. AJNR Am J Neuroradiol 1996;17:619.
Gleeson, Dobyns, Plawner, and Ashwal / Congenital Structural Defects Tolmie JL, McNay M, Stephenson JBP, et al. Microcephaly: Genetic counseling and antenatal diagnosis after the birth of an affected child. Am J Med Genet 1987;27:583. Tominaga T, Koshu K, Ogawa A, et al. Transoral decompression evaluated by cine-mode magnetic resonance imaging: A case of basilar impression accompanied by Chiari malformation. Neurosurgery 1991;28:883. Topaloglu H, Brockington M, Yuva Y, et al. FKRP gene mutations cause congenital muscular dystrophy, mental retardation, and cerebellar cysts. Neurology 2003;60:988. Torregrosa A, Marti-Bonmati L, Higueras V, et al. Klippel-Trenaunay syndrome: Frequency of cerebral and cerebellar hemihypertrophy on MRI. Neuroradiology 2000;42:420. Tosi LL. Osteogenesis imperfecta. Curr Opin Pediatr 1997;9:94. Towfighi J, Housman C. Spinal cord abnormalities in caudal regression syndrome. Acta Neuropathol (Berl) 1991;81:458. Tracy MR, Dormans MD, Kusumi K. Klippel-Feil syndrome: Clinical features and current understanding of etiology. Clin Orthop Relat Res 2004;424:183. Trainor PA, Melton KR, Manzanares M. Origins and plasticity of neural crest cells and their roles in jaw and craniofacial evolution. Int J Dev Biol 2003;47:541. Trimborn M, Bell SM, Felix C, et al. Mutations in microcephalin cause aberrant regulation of chromosome condensation. Am J Hum Genet 2004;75:261. Tubbs RS, Webb DB, Oakes WJ. Persistent syringomyelia following pediatric Chiari I decompression: Radiological and surgical findings. J Neurosurg Spine 2004;100:460. Tuite GF, Chong WK, Evanson J, et al The effectiveness of papilledema as an indicator of raised intracranial pressure in children with craniosynostosis. Neurosurgery 1996a;38:272. Tuite GF, Evanson J, Chong WK, et al. The beaten copper cranium: A correlation between intracranial pressure, cranial radiographs, and computed tomographic scans in children with craniosynostosis. Neurosurgery 1996b;39:691. Tuli S, Provias JP, Bernstein M. Lhermitte-Duclos disease: Literature review and novel treatment strategy. Can J Neurol Sci 1997;24:155. Tulipan N, Bruner JP. Myelomeningocele repair in utero: A report of three cases. Pediatr Neurosurg 1998;28:177. Tulipan N, Bruner JP, Hernanz-Schulman M, et al. Effect of intrauterine myelomeningocele repair on central nervous system structure and function. Pediatr Neurosurg 1999a;31:183. Tulipan N, Hernanz-Schulman M, Lowe LH, Bruner JP. Intrauterine myelomeningocele repair reverses preexisting hindbrain herniation. Pediatr Neurosurg 1999b;31:137. Turner G, Partington M, Kerr B, et al. Variable expression of mental retardation, autism, seizures, and dystonic hand movements in two families with an identical ARX gene mutation. Am J Med Genet 2002;112:405. Turner JT, Cohen MM Jr, Biesecker LG. Reassessment of the Proteus syndrome literature: Application of diagnostic criteria to published cases. Am J Med Genet 2004;130A:111. Turner MS. The treatment of hydrocephalus: A brief guide to shunt selection. Surg Neurol 1995;43:314. Turtas S, Tondi M, Tola G, et al. Neuropsychological evaluation in a series of 17 cases operated on for craniosynostosis. Acta Neurochir Wien 1993;120:123. Turvey TA. Facial clefts and craniosynostosis: Principles and management. Philadelphia: WB Saunders, 1996. Ueeck B, Le B, Goodman S, et al. Corneal ulcers in patients with Apert syndrome. J Craniofac Surg 2001;12:134. Uhl M, Pawlik H, Laubenberger J, et al. MR findings in pontocerebellar hypoplasia. Pediatr Radiol 1998;28:547. Ulmer JL, Elster AD, Ginsberg LE, et al. Klippel-Feil syndrome: CT and MR of acquired and congenital abnormalities of cervical spine and cord. J Comput Assist Tomogr 1993;17:215. Vachha B, Adams R. Language sample analysis in children with myelomeningocele and shunted hydrocephalus. Eur J Pediatr Surg 2003;13(Suppl 1):S36. Vallino-Napoli LD. Audiologic and otologic characteristics of Pfeiffer syndrome. Cleft Palate Craniofac J 1996;33:524. Valsky DV, Liat BS, Porat S, et al. The role of magnetic resonance imaging in the evaluation of isolated mild ventriculomegaly.J Ultrasound Med 2004;23:519. Van Allen MI, Kalousek DK, Chernoff GF, et al. Evidence for multi-site closure of the neural tube in humans. Am J Med Genet 1993;47:723. van der Put NM, Eskes TK, Blom HJ. Is the common 677C—>T mutation in the methylenetetrahydrofolate reductase gene a risk factor for neural tube defects? A meta-analysis. QJM 1997;90:111.
489
van der Put NM, Steegers-Theunissen RP, Frosst P, et al. Mutated methylenetetrahydrofolate reductase as a risk factor for spina bifida. Lancet 1995;346:1070. Van Esch H, Poirier K, de Zegher F, et al. ARX mutation in a boy with transsphenoidal encephalocele and hypopituitarism. Clin Genet 2004;65:503. Van Hul W, Bollerslev J, Gram J, et al. Localization of a gene for autosomal dominant osteopetrosis (Albers-Schonberg disease) to chromosome 1p21. Am J Hum Genet 1997;61:363. van Rooij IA, Vermeij-Keers C, Kluijtmans LA, et al. Does the interaction between maternal folate intake and the methylenetetrahydrofolate reductase polymorphisms affect the risk of cleft lip with or without cleft palate? Am J Epidemiol 2003;157:583. Vannier MW, Pilgram TK, Marsh JL, et al. Craniosynostosis: Diagnostic imaging with three-dimensional CT presentation. AJNR Am J Neuroradiol 1994;15:1861. Vari R, Puca A, Meglio M. Cleidocranial dysplasia and syringomyelia. Case report. J Neurosurg Sci 1996;40:125. Venes JL. Control of shunt infection. Report of 150 consecutive cases. J Neurosurg 1976;45:311. Venes JL, Black KL, Latack JT. Preoperative evaluation and surgical management of the Chiari II malformation. J Neurosurg 1986;64:363. Ventriculomegaly Trial Group. Randomised trial of early tapping in neonatal post haemorrhagic ventricular dilatation. Arch Dis Child 1990;65:3. Vergani P, Ghidini A, Strobelt N, et al. Prognostic indicators in the prenatal diagnosis of agenesis of corpus callosum. Am J Obstet Gynecol 1994;170:753. Vergani P, Locatelli A, Strobelt N, et al. Clinical outcome of mild fetal ventriculomegaly. Am J Obstet Gynecol 1998;178:218. Vernet O, Campiche R, de Tribolet N. Long-term results after ventriculo-atrial shunting in children. Childs Nerv Syst 1995;11:176. Vigevano F, Bertini E, Boldrini R, et al. Hemimegalencephaly and intractable epilepsy: Benefits of hemispherectomy. Epilepsia 1989;30:833. Viljoen DL, Versfeld GA, Losken W, et al. Polyostotic fibrous dysplasia with cranial hyperostosis: New entity or most severe form of polyostotic fibrous dysplasia? Am J Med Genet 1988;29:661. Villard L, Nguyen K, Cardoso C, et al. A locus for bilateral perisylvian polymicrogyria maps to Xq28. Am J Hum Genet 2002;70:1003. Vits L, Van Camp G, Coucke P, et al. MASA syndrome is due to mutations in the L1CAM gene. Nat Genet 1994;7:408. Vles JSH, De Die-Smulders C, Van der Hoeven M, et al. Corpus callosum agenesis in two male infants of a heterozygotic triplet pregnancy. Genet Couns 1993;4:239. Vles JSH, Fryns JP, Folmer K, et al. Corpus callosum agenesis, spastic quadriparesis and irregular lining of the lateral ventricles on CT-scan. A distinct X-linked mental retardation syndrome? Genet Couns 1990;38:97. Volpe JJ. Neurology of the newborn. Philadelphia: WB Saunders, 2000. von Gernet S, Schuffenhauer S, Golla A, et al. Craniosynostosis suggestive of Saethre-Chotzen syndrome. Clinical description of a large kindred and exclusion of candidate regions on 7p. Am J Med Genet 1996;63:177. Von Koch CS, Gupta N, Sutton LN, et al. In utero surgery for hydrocephalus. Childs Nerv Syst 2003;19:574. Wald N. Folic acid and the prevention of neural tube defects. Ann N Y Acad Sci 1993;678:112. Wald N, Cuckle H, Nanchahal K. Amniotic fluid acetylcholinesterase measurement in the prenatal diagnosis of open neural tube defects. Second report of the Collaborative Acetylcholinesterase Study. Prenat Diagn 1989;9:813. Wald NJ, Law MR, Morris JK, Wald DS. Quantifying the effect of folic acid. Lancet 2001;358:2069. Walker AE. Lissencephaly. Arch Neurol Psychiatry 1942;48:13. Walpole IR, Nicoll A, Goldblatt J. Autosomal dominant osteopetrosis type II with “malignant” presentation: Further support for heterogeneity? Clin Genet 1990;38:257. Walters J, Ashwal S, Masek T. Anencephaly: Where do we now stand? Semin Neurol 1997;17:249. Wang H, Rosenbaum AE, Reid CS, et al. Pediatric patients with achondroplasia: CT evaluation of the craniocervical junction. Radiology 1987;164:515. Wang P, Chang FM, Chang CH, et al. Prenatal diagnosis of Joubert syndrome complicated with encephalocele using two-dimensional and three-dimensional ultrasound. Ultrasound Obstet Gynecol 1999;14:360. Warman ML, Mulliken JB, Hayward PG, et al. Newly recognized autosomal dominant disorder with craniosynostosis. Am J Med Genet 1993;46:444. Wassarman KM, Lewandoski M, Campbell K, et al. Specification of the anterior hindbrain and establishment of a normal mid/hindbrain organizer is dependent on GBX2 gene function. Development 1997;124:2923.
490
Perinatal Acquired and Congenital Neurologic Disorders / 19
Wassmer E, Davies P, Whitehouse WP, et al. Clinical spectrum associated with cerebellar hypoplasia. Pediatr Neurol 2003;28:347. Waters KA, Everett F, Sillence DO, et al. Treatment of obstructive sleep apnea in achondroplasia: Evaluation of sleep, breathing, and somatosensoryevoked potentials. Am J Med Genet 1995;59:460. Waterson J R, DiPietro MA, Barr M. Apert syndrome with frontonasal encephalocele. Am J Med Genet 1985;21:777. Watson WJ, Chescheir NC, Katz VL, Seeds JW. The role of ultrasound in evaluation of patients with elevated maternal serum alpha-fetoprotein: A review. Obstet Gynecol 1991;78:123. Weaving LS, Christodoulou J, Williamson SL, et al. Mutations of CDKL5 cause a severe neurodevelopmental disorder with infantile spasms and mental retardation. Am J Hum Genet 2004;75:1079. Weiner SN, Pearlstein AE, Eiber A. MR imaging of intracranial arachnoid cysts. J Comput Assist Tomogr 1987;11:236. Weinstein LS, Shenker A, Gejman PV, et al. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N Engl J Med 1991;325:1688. Weinstein RS. Long-term aminobisphosphonate treatment of fibrous dysplasia: Spectacular increase in bone density. J Bone Miner Res 1997;12:1314. Welch K. The principle of physiology of the cerebrospinal fluid in relation to hydrocephalus including normal pressure hydrocephalus. Adv Neurol 1975;13:247. Wellington C. A spectrum of neurological phenotypes caused by mutations in the X-linked aristaless-related homeobox gene, ARX. Clin Genet 2003;63:177. Wen CS, Chang YL, Wang HS, et al. Sinus pericranii: From gross and neuroimaging findings to different pathophysiological changes. Childs Nerv Syst 2005;21:482 (epub 2004 Oct 15). Whitelaw A. Intraventricular streptokinase after intraventricular hemorrhage in newborn infants. Cochrane Database Syst Rev 2001;1:CD000498. Whitelaw A. Repeated lumbar or ventricular punctures in newborns with intraventricular hemorrhage. Cochrane Database Syst Rev 2005;1:CD000216. Whyte MP, Chines A, Silva DP Jr, et al. Creatine kinase brain isoenzyme (BBCK) presence in serum distinguishes osteopetroses among the sclerosing bone disorders. J Bone Miner Res 1996;11:1438. Wichterle H, Turnbull DH, Nery S, et al. In utero fate mapping reveals distinct migratory pathways and fates of neurons born in the mammalian basal forebrain. Development 2001;128:3759. Wieselthaler NA, van Toorn R, Wilmshurst JM. Giant congenital melanocytic nevi in a patient with brain structural malformations and multiple lipomatosis. J Child Neurol 2002;17:289. Wieting JM, Krach LE. Spinal cord injury rehabilitation in a pediatric achondroplastic patient: Case report. Arch Phys Med Rehabil 1994;75:106. Wilkie AO, Morriss-Kay GM. Genetics of craniofacial development and malformation. Nat Rev Genet 2001;2:458. Wilkie AO, Slaney SF, Oldridge M, et al. Apert syndrome results from localized mutations of FGFR2 and is allelic with Crouzon syndrome. Nat Genet 1995;9:165. Wilkinson JM, Scott BW, Bell MJ. The prognosis for walking in osteogenesis imperfecta. J Bone Joint Surg Br 1997;79:339. Wilson C, Aftimos S, Pereira A, McKay R. Report of two sibs with Knobloch syndrome (encephalocele and vitroretinal degeneration) and other anomalies. Am J Med Genet 1998;78:286. Wilson ME, Lindsay DJ, Levi CS, et al. US case of the day. Dandy-Walker variant with agenesis of the corpus callosum. Radiographics 1994;14:678. Winer N, Le Caignec C, Quere MP, et al. Prenatal diagnosis of a cleidocranial dysplasia–like phenotype associated with a de novo balanced t(2q;6q)(q36;q16) translocation. Ultrasound Obstet Gynecol 2003;22:648. Wininger SJ, Donnenfeld AE. Syndromes identified in fetuses with prenatally diagnosed cephaloceles. Prenat Diagn 1994;14:839. Winship IM. Sotos syndrome—autosomal dominant inheritance substantiated. Clin Genet 1985;28:243. Wisniewski K, Dambska M, Sher JH, et al. A clinical neuropathological study of the fetal alcohol syndrome. Neuropediatrics 1983;14:197. Wong E, Kenwrick S, Willems PJ, et al. Mutations in the cell adhesion molecule L1 cause mental retardation. Trends Neurosci 1995;18:168. Wong FK, Hagg U. An update on the aetiology of orofacial clefts. Hong Kong Med J 2004;10:331. Wong LY, Paulozzi LJ. Survival of infants with spina bifida: A population study:1979-94. Paediatr Perinat Epidemiol 2001;15:374. Wood JW, Johnson KG, Omori Y. In utero exposure to the Hiroshima atomic bomb. An evaluation of head size and mental retardation: Twenty years later. Pediatrics 1967;39:385. Worthington S, Arbuckle S, Nelson P, et al. Carbohydrate deficient glycoprotein syndrome type I: A cause of cerebellar vermis hypoplasia. J Paediatr Child Health 1997;33:531.
Worthington S, Turner A, Elber J, et al. 22q11 deletion and polymicrogyria— cause or coincidence? Clin Dysmorphol 2000;9:193. Wu XR, Swaiman KF. Reversible hydrocephalus caused by bilateral jugular vein catheterization. Brain Dev 1982;4:397. Wyllie E, Baumgartner C, Prayson R, et al. The clinical spectrum of focal cortical dysplasia and epilepsy. J Epilepsy 1994;7:303. Wyszynski DF. Cleft lip and palate: From origin to treatment. New York: Oxford University Press, 2002. Wyszynski DF, Wu T. Use of U.S. birth certificate data to estimate the risk of maternal cigarette smoking for oral clefting. Cleft Palate Craniofac J 2002;39:188. Yachnis AT. Rhombencephalosynapsis with massive hydrocephalus: Case report and pathogenetic considerations. Acta Neuropathol (Berl) 2002;103:301. Yacubian-Fernandes A, Palhares A, Giglio A, et al. Apert syndrome: Analysis of associated brain malformations and conformational changes determined by surgical treatment. J Neuroradiol 2004;31:116. Yakovley PI, Wadsworth RC. Schizencephalies: A study of the congenital clefts in the cerebral mantle. I: Clefts with fused lips. J Neuropathol Exp Neurol 1946a;5:116. Yakovley PI, Wadsworth RC. Schizencephalies: A study of the congenital clefts in the cerebral mantle. II: Clefts with hydrocephalus and lips separated. J Neuropathol Exp Neurol 1946b;5:169. Yamada H, Nakamura S, Tajima M, et al. Neurological manifestations of pediatric achondroplasia. J Neurosurg 1981;54:49. Yamada Y, Ito H, Otsubo Y, Sekido K. Surgical management of cervicomedullary compression in achondroplasia. Childs Nerv Syst 1996;12:737. Yamaguchi K, Honma K. Autopsy case of thanatophoric dysplasia: Observations on the serial sections of the brain. Neuropathology 2001;21:222. Yamaguchi TP, Rossant J. Fibroblast growth factors in mammalian development. Curr Opin Genet Dev 1995;5:485. Yao L, Eckardt JJ, Seeger LL. Fibrous dysplasia associated with cortical bony destruction: CT and MR findings. J Comput Assist Tomogr 1994;18:91. Yasuda Y, Konishi H, Matsuo T, et al. Aberrant differentiation of neuroepithelial cells in developing mouse brains subsequent to retinoic acid exposure in utero. Am J Anat 1989;186:271. Yoshida A, Kobayashi K, Manya H, et al. Muscular dystrophy and neuronal migration disorder caused by mutations in a glycosyltransferase, POMGNT1. Dev Cell 2001;1:717. Yoshida H, Hayashi SI, Kunisada T, et al. The murine mutation osteopetrosis is in the coding region of the macrophage colony-stimulating factor gene. Nature 1990;345:442. Yoshida T, Kanegane H, Osato M, et al. Functional analysis of RUNX2 mutations in cleidocranial dysplasia: Novel insights into genotypephenotype correlations. Blood Cells Mol Dis 2003;30:184. Young ID, Barrow M, Hall CM. Microcephalic osteodysplastic primordial short stature type II with cafe-au-lait spots and moyamoya disease: Another patient. Am J Med Genet 2004;127A:218. Yousfi M, Lasmoles F, Lomri A, et al. Increased bone formation and decreased osteocalcin expression induced by reduced TWIST dosage in SaethreChotzen syndrome. J Clin Invest 2001;107:1153. Yundt KD, Park TS, Tantuwaya VS, et al. Posterior fossa decompression without duraplasty in infants and young children for treatment of Chiari malformation and achondroplasia. Pediatr Neurosurg 1996;25:221. Zackai EH, Gripp KW, Stolle CA. Craniosynostosis: Molecular testing—a necessity for counseling. Am J Med Genet 2000;92:157. Zeitlin L, Fassier F, Glorieux FH. Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77. Zelnik N, Dobyns WB, Forem SL, et al. Congenital pontocerebellar atrophy in three patients: Clinical, radiologic and etiologic considerations. Neuroradiology 1996;38:684. Zhang W, Vajsar J, Cao P, et al. Enzymatic diagnostic test for muscle-eye-brain type congenital muscular dystrophy using commercially available reagents. Clin Biochem 2003;36:339. Zlotogora J, Amitai Y, Kaluski DN, Leventhal A. Surveillance of neural tube defects in Israel. Isr Med Assoc J 2002;4:1111. Zollino M, Colosimo C, Zuffardi O, et al. Cryptic t(1;12)(q44;p13.3) translocation in a previously described syndrome with polymicrogyria, segregating as an apparently X-linked trait. Am J Med Genet 2003;117A:65. Zuccaro G, Dogliotti P, Bennum R, et al. Treatment of cloverleaf skull syndrome. Childs Nerv Syst 1996;12:695. Zuccoli G, Guidetti D, Nicoli F, et al. Carotid and vertebral artery dissection: Magnetic resonance findings in 15 cases. Radiol Med (Torino) 2002;104:466. Zucconi M, Bruni O. Sleep disorders in children with neurologic diseases. Semin Pediatr Neurol 2001;8:258.
CHAPTER 20
Cerebral Palsy Kenneth F. Swaiman and Yvonne Wu
DEFINITION AND CLINICAL CHARACTERIZATION Cerebral palsy is a nonspecific, descriptive term pertaining to disordered motor function that is evident in early infancy and is characterized by changes in muscle tone (typically spasticity or rigidity), muscle weakness, involuntary movements, ataxia, or a combination of these abnormalities. The condition is the result of brain dysfunction and is not episodic or progressive. Although tone and postural abnormalities may become more pronounced during early childhood, qualitative changes are uncommon. The full extent of motor disability may not be evident until the age of 3 or 4 years. Intellectual, sensory, and/or behavioral difficulties may accompany cerebral palsy; however, they are not included in the diagnostic criteria. For the most part, these accompanying difficulties can be managed with conventional approaches to each entity [Gross-Tsur, 2002]. Children with cerebral palsy often exhibit other neurologic impairments including mental retardation (52%), hearing impairment (12%), and speech and language disorders (38%) [Ashwal et al., 2004]. Epilepsy occurs in 34% to 94% of children with cerebral palsy, depending on the study population. Cerebral palsy encompasses a wide range of brain disorders associated with impaired motor function. As a result, the definition of cerebral palsy varies depending on the purpose for which the term is being used [Badawi et al., 1998c]. Consensus is lacking on whether a child with a known underlying pathologic condition (e.g., neuronal migrational defect, metabolic disease) should be included under the rubric of cerebral palsy, or whether the degree of disability also should be taken into account. The prevalence of the condition will clearly depend on how it is defined and on the age at diagnosis, because children with mild impairment may experience substantial improvement or dissolution of abnormal findings during maturation [Nelson and Ellenberg, 1982]. Nevertheless, the designation of cerebral palsy as an entity, irrespective of underlying conditions, is valuable, because afflicted children commonly have similar medical care, rehabilitation, and social services needs.
EPIDEMIOLOGY Cerebral palsy occurs in 1.2 to 2.5 children per 1000 live births. Despite the lack of a consistent definition, population prevalence rates from four continents have remained relatively constant over several decades. Numerous cerebral palsy registries exist throughout the world [Cans et al., 2004]. In the United States, the prevalence of cerebral palsy increased slightly from 1.7 to 2.0 per 1000 live births between the mid-1970s and late 1980s [Winter et al., 2002]. As estimated from these rates, 8000 children with cerebral palsy are born annually in the United States.
Prematurity is the single most important risk factor for cerebral palsy. The risk of cerebral palsy in very-low-birthweight infants is as high as 8% to 10%, whereas the risk in term infants is only 1.0 to 1.5 per 1000 live births [Grether et al., 1992; Hagberg et al., 2001; Topp et al., 2001; Wu et al., 2003]. An increase in the rate of cerebral palsy among preterm infants during the mid-1980s was attributed to increased survival of low-birth-weight infants [Colver et al., 2000; Pharoah et al., 1990; Topp et al., 2001]. Subsequent longitudinal studies of cerebral palsy in the late 1980s and 1990s, however, suggest that the rate of cerebral palsy among preterm infants has remained constant or even decreased during this more recent period [Clark and Hankins, 2003; Hagberg et al., 2001; O’Shea et al, 1998; Winter et al., 2002]. Nevertheless, preterm infants still constitute 50% to 60% of all infants with cerebral palsy. The prevalence of cerebral palsy among term infants has not diminished over the past 3 decades, despite the introduction of electronic fetal monitoring during the 1970s and the subsequent sharp rise in births by cesarean section [Clark and Hankins, 2003; Colver et al., 2000; Topp et al., 2001; Winter et al., 2002]. The unchanged prevalence is disappointing in view of the fact that perinatal deaths, stillbirths, and birth asphyxia as measured by low Apgar scores all have dropped dramatically in recent decades. Longitudinal data in the United States suggest that a slight increase in cerebral palsy prevalence among infants with normal birth weight is responsible for the significant increase in total cerebral palsy prevalence reported over a 15-year period [Winter et al., 2002]. Although the severity of cerebral palsy within an Australian population increased during this period [Blair, 2001], suggesting that perhaps more infants who would have died in previous times are being saved, workers in England have described a decrease in severity of cerebral palsy among term infants over a similar (18-year) period [Colver et al., 2000]. An infant who is the product of a multiple gestation carries a higher risk for cerebral palsy. Twins, who constitute 2% of the population, contributed 10% to the prevalence of cerebral palsy in one U.S. study [Grether et al., 1992]. The increased risk of cerebral palsy among infants of multiple gestation is partly due to the higher rate of prematurity. Twins born at term, however, also exhibit an increased risk for cerebral palsy [Petterson et al., 1993; Pharoah, 2001]. Death in utero of a co-twin, such as from twin-twin transfusion, places the surviving twin at particularly high risk for neurologic and other complications [Grether et al., 1993; Szymonowicz et al., 1986]. Blacks have an increased risk of cerebral palsy when compared with whites [Murphy et al., 1993]. This finding is due in part to an increased rate of prematurity. The risk of cerebral palsy among black infants born at term, however,
492
Perinatal Acquired and Congenital Neurologic Disorders / 20
also is elevated, for reasons that are poorly understood [Wu et al., 2003]. Life expectancy of patients with cerebral palsy is related to the type of involvement and the severity of motor disability. Severe quadriplegia has been associated with a shortened life expectancy. Other significant variables include associated disabilities and availability of quality medical care. The risk of death is highest in the first 5 years of life [Blair et al., 2001]. As mortality data have become available, it has become clear that with reasonable medical attention, a majority of affected persons will survive into adult life [Evans et al., 1990; Eyman et al., 1990; Hutton et al., 1994; Plioplys, 2003; Plioplys et al., 1998; Strauss et al., 1998].
ETIOLOGY A wide range of causative disorders and risk factors have been identified for cerebral palsy. Table 20-1 lists some of the more common etiologic categories and risk factors broadly classified into the following groups: perinatal brain injury, brain injury related to prematurity, developmental abnormalities, prenatal risk factors, and postnatal brain injury. These factors may co-exist and interact with each other in contributing to the pathogenesis of brain injury resulting in cerebral palsy.
Perinatal Brain Injury Intrapartum hypoxia-ischemia is a well-described cause of cerebral palsy, especially in the setting of an acute intra-
TABLE 20-1 Selected Etiologic Disorders and Risk Factors in Cerebral Palsy* Perinatal Brain Injury Hypoxia-ischemia Neonatal stroke (arterial and venous) Traumatic brain injury Intracranial hemorrhage Brain Injury Related to Prematurity Periventricular leukomalacia Intraventricular hemorrhage Developmental Abnormality Brain malformation Genetic abnormality Metabolic abnormality Postnatal Brain Injury Kernicterus Central nervous system infection Prenatal Risk Factors Maternal chorioamnionitis Intrauterine growth retardation Toxin exposure Congenital TORCH infections *Note that many of these conditions may coexist in a child with cerebral palsy. TORCH, toxoplasmosis, other infections, rubella, cytomegalovirus infection, herpes simplex.
partum event such as uterine rupture, placental abruption, or cord prolapse. The extent to which hypoxic-ischemic brain injury is responsible for cerebral palsy, however, has been a major source of controversy. Epidemiologic studies suggest that in a minority (between 6% and 28%) of affected children, cerebral palsy is due to perinatal asphyxia [Hagberg et al., 2001; Nelson and Grether 1998]. The form of cerebral palsy most often associated with hypoxic-ischemic brain injury is spastic quadriparesis. The term perinatal asphyxia is confusing and deserves further clarification. Traditionally, this term has been defined by clinical signs and symptoms including low Apgar scores, meconium-stained amniotic fluid, and low cord pH. Yet the clinical findings used to define this term are not specific for hypoxic-ischemic brain injury [Blair, 1993]. Although various groups of investigators have defined specific criteria that can be used to establish intrapartum hypoxiaischemia as the underlying cause of cerebral palsy [MacLennan, 1999], still lacking is a widely accepted evidencebased standard for determining when cerebral palsy is due to hypoxia-ischemia. Neonatal encephalopathy has emerged as the preferred term to describe the clinical syndrome traditionally called perinatal asphyxia, because it is an all-embracing term that does not imply a single underlying etiologic disorder [Leviton and Nelson, 1992]. Signs and symptoms of brain dysfunction that constitute neonatal encephalopathy include low Apgar scores, failure to initiate and/or maintain respiration, depressed consciousness, abnormal tone (usually flaccidity), depression of developmental reflexes, and seizures during the first 48 hours of life. The clinical syndrome of neonatal encephalopathy may be preceded by a variety of prenatal and intrapartum risk factors [Badawi et al., 1998b] and usually is associated with acute brain injury occurring around the time of birth [Cowan et al., 2003]. Signs and symptoms of neonatal encephalopathy are strongly predictive of cerebral palsy in the child. For instance, term infants whose immediate postpartum course comprises of a 5-minute Apgar score of 5 or less, continuing neurologic abnormalities, and seizures in the first days of life constitute a group at high risk for chronic motor disability (55%) and for death or disability combined (70%) [Ellenberg and Nelson, 1988]. The risk of cerebral palsy is increased 30-fold in infants with a 5-minute Apgar score of less than 7, and 80-fold in infants with a 5-minute Apgar score of 3 or less [Moster et al., 2001; Thorngren-Jerneck and Herbst, 2001; Wu et al., 2003]. Perinatal arterial ischemic infarction, commonly referred to as neonatal stroke, may be responsible for greater than half of all cases of hemiplegic cerebral palsy in term infants [Humphreys et al., 2000; Uvebrant, 1988; Wu et al., 2003]. Among children with cerebral palsy who are referred for neuroimaging, 13% to 37% are diagnosed with a neonatal stroke [Ashwal et al., 2004]. Although the term perinatal implies an event that occurs before the age of 7 days the term is not clearly defined, whereas neonatal refers to an event within 28 days of life [Lynch and Nelson, 2001], the two entities are often lumped together under the single category of “neonatal stroke.” Newborns with arterial ischemic infarction either may present acutely during the neonatal period, with neurologic symptoms such as seizures, or may be clinically asymptomatic until several months of age, when pathologic handed-
Swaiman and Wu / Cerebral Palsy
ness or seizures are first noted [Golomb et al., 2001]. The risk of cerebral palsy after perinatal arterial stroke is especially high among infants with delayed presentation; this finding is not surprising given that hemiparesis is the most common presenting symptom in this group [Golomb et al., 2001; Wu et al., 2004]. Involvement of the internal capsule also portends a poorer motor outcome after perinatal arterial stroke [Mercuri et al., 1999; Wu et al., 2004]. Other cerebrovascular conditions, such neonatal sinovenous thrombosis, also can lead to cerebral palsy. In a population-based study of pediatric stroke in Canada, 43% of all cases of sinovenous thrombosis occurred during the neonatal period [deVeber and Andrew, 2001]. Risk factors for neonatal sinovenous thrombosis include systemic illness, polycythemia, coagulation abnormalities and extracorporeal membrane oxygen (ECMO) therapy, and motor sequelae such as cerebral palsy were more common if sinovenous thrombosis led to development of venous infarction [deVeber and Andrew, 2001; Wu et al., 2002]. Periventricular venous infarction [Takanashi et al., 2003], intraparenchymal hemorrhage, and birth trauma also may lead to cerebral palsy (please refer to Chapter 17 for further discussion of birth trauma).
Brain Injury Related to Prematurity Preterm infants have a disproportionate share of the cases of spastic diplegia but can manifest any cerebral palsy subtype. Both intraventricular hemorrhage and white matter necrosis may occur before or after birth. Cystic periventricular leukomalacia is the strongest risk factor for cerebral palsy among preterm infants and is reviewed in Chapter 14. The extent to which hypoxia-ischemia is a contributor to cerebral palsy in the very-low-birth-weight infant is not well established. Defects in autoregulation of cerebral blood flow may be important, as well as postnatal risk factors such as lung disease and hypotension. Recent evidence suggests that inflammation also contributes to the pathogenesis of white matter injury in preterm infants [Dammann and Leviton, 1997; Wu and Colford, 2000]. Periventricular leukomalacia and intraventricular hemorrhage are reviewed in Chapter 14.
Developmental Abnormalities Brain malformations originating from intrauterine maldevelopment may underlie the neurologic impairment seen in children with cerebral palsy. As a group, children with cerebral palsy have a higher incidence of congenital malformations both within and outside of the brain. Populationbased studies of cerebral palsy suggest that 9% to 14% of affected children have a brain malformation [Croen et al., 2001; Wu et al., 2003]. The most common malformations in term children are cortical dysplasia/polymicrogyria, schizencephaly, and pachygyria/lissencephaly; complex brain malformations are the most frequent category among preterm infants with cerebral palsy [Ashwal et al., 2004]. A genetic or metabolic disorder may be associated with a specific brain malformation that causes cerebral palsy. For instance, children with Zellweger’s syndrome typically have polymicrogyria and other cortical malformations. MillerDieker syndrome also is a known cause of lissencephaly. Glutaricaciduria type I may masquerade as dyskinetic cerebral palsy [Hauser and Peters, 1998], and arginase deficiency
493
mimics diplegic cerebral palsy [Prasad et al., 1997]. Children with cerebral palsy who demonstrate either progressive decline or atypical features such as dysmorphisms, macrocephaly, or a strong family history should be tested for an underlying genetic or metabolic disorder.
Prenatal Risk Factors A number of maternal conditions have been associated with an increased risk of cerebral palsy in the offspring. Intrauterine inflammation, or chorioamnionitis, has received increasing attention as a potential risk factor [Grether and Nelson, 1997; Leviton et al., 1999; Wu and Colford, 2000]. Epidemiologic studies suggest that maternal intrapartum fever, a clinical or histologic diagnosis of chorioamnionitis, and serologic markers of inflammation in the fetus all confer an increased risk of cerebral palsy. In term infants, chorioamnionitis, often diagnosed by the presence of intrapartum maternal fever, is a particularly strong risk factor for spastic quadriplegia [Grether and Nelson, 1997; Wu et al., 2003]. Maternal fever during labor also increases the chance that the neonate will have low Apgar scores and characteristics of neonatal encephalopathy [Badawi et al., 1998a; Lieberman et al., 2000]. It is hypothesized that the fetal inflammatory response that occurs in the setting of an inflammatory intrauterine environment is responsible for brain injury leading to cerebral palsy [Dammann et al., 2002; Nelson et al., 1998]. Yet the mechanism by which intrauterine inflammation might cause cerebral palsy remains controversial and unexplained. Furthermore, the manner in which inflammation may interact with hypoxia-ischemia to injure the newborn brain also is unknown. Intrauterine growth restriction is associated with an increased risk of cerebral palsy, especially in term infants [Jarvis et al., 2003; Topp et al., 1996]. Infants who are large for gestational age also have been reported to be at higher risk [Uvebrant and Hagberg, 1992]. Prothrombotic abnormalities, including factor V Leiden mutation and presence of anticardiolipin antibodies, have been found with increased frequency among infants with perinatal arterial infarction and may contribute to the pathogenesis of cerebral palsy [Gunther et al., 2000; Hagstrom et al., 1998]. A history of infertility also has been found to be associated with an increased risk of neonatal encephalopathy, developmental delay, and cerebral palsy [Badawi et al., 1998b; Ericson et al., 2002; Stromberg et al., 2002]. A number of toxins have been described to cause cerebral palsy, such as benzyl alcohol preservative and in utero alcohol exposure [Benda et al., 1986; Burd et al., 2003]. Ingestion of methyl mercury by pregnant women in the Minamata Bay disaster resulted in the birth of children who were spastic, microcephalic, and mentally retarded. Congenital infections, often referred to as TORCH infections (toxoplasmosis, rubella, cytomegalovirus, and herpes simplex infection), also can infect the fetus and produce serious encephalitides with motor sequelae [Sever, 1985]. The pathogenesis of cerebral palsy is complex and multifactorial. Among infants with thromboembolic stroke in the newborn period, multiple risk factors often are observed [Gunther et al., 2000; Wu et al., 2002]. When signs of hypoxia-ischemia and markers of infection both are present in a newborn, the risk for cerebral palsy is markedly heightened [Nelson and Grether, 1998]. Similarly, chorio-
494
Perinatal Acquired and Congenital Neurologic Disorders / 20
amnionitis is a particularly strong risk factor for cerebral palsy among term infants who are found on head imaging to have suffered hypoxic-ischemic brain injury [Wu et al., 2003]. Studies of placental abnormalities in cerebral palsy also suggest that a combination of both thrombotic and inflammatory findings confers the highest risk of adverse neurologic outcome [Redline and O’Riordan, 2000].
Postnatal Brain Injury Cerebral palsy may result from brain injury occurring during the neonatal period. For instance, neonatal meningitis from group B streptococcal and other infections may cause brain damage leading to cerebral palsy. Other types of postnatal brain injury including hypoxia-ischemia and traumatic brain injury from nonaccidental trauma also may cause cerebral palsy. Bilirubin toxicity continues to be a significant problem in spite of recent progress in management of hyperbilirubinemic neonates [Shapiro, 2003]. Although bilirubin levels below 25 mg/dL may be associated with kernicterus [SooraniLunsing et al., 2001], more commonly bilirubin levels greater than 25 to 30 mg/dL lead to kernicterus, a wellknown cause of dyskinetic cerebral palsy. Symptoms of kernicterus in a jaundiced newborn usually are present by the second or third day of life. The child becomes listless and sucks poorly. Fever may be present, and crying becomes weak. The Moro and deep tendon reflexes become difficult to elicit, and general muscle tone becomes decreased. After several weeks, tone increases, and the infant manifests extension of the back with opisthotonos and marked extension of the extremities [Van Praagh, 1961]. The full clinical pattern of kernicterus infrequently is present in a single affected patient. Signs and symptoms consist of choreoathetosis, dystonia, tremors, and rigidity. Upward gaze and, on rare occasion, horizontal gaze may be impaired. Sensorineural hearing loss is common. Mental retardation, microcephaly, and spasticity may be present. A clinical score for assessing bilirubin-induced dysfunction in newborns has been recommended [Johnson et al., 1999]. Unconjugated bilirubin damages mitochondria and is toxic to neurons and to astrocytes [Ostrow et al., 2004]. Microscopic examination reveals yellow granules that are found not only in the nerve cells but also in the interstitial tissue. These changes occur in the first few days of involvement. Neurons are grossly pyknotic, and in children who live for longer periods, large areas of cell loss, gliosis, and demyelination are evident.
GENERAL PATHOLOGIC FEATURES Subependymal and intraventricular hemorrhages, sometimes associated with hypoxia-ischemia, may result in chronic motor impairment in preterm infants. Severe cystic changes in white matter in preterm infants often are accompanied by motor dysfunction [Bejar et al., 1986; de Vries et al., 1987]. Diminished blood flow in distal vessels to periventricular white matter, metabolic disturbances, and infection may precede white matter destruction [Leviton and Gilles, 1984]. In term, asphyxiated infants, an impairment of the blood flow in parasagittal areas has been documented by positron emission tomography [Volpe et al., 1985].
In studies of patients with documented motor disabilities, clinical neuropathologic correlative studies have been unsystematic, variously selective, and valuable in methods of evaluation, description, and interpretation. Use of current quantitative techniques of neuropathologic stains for cell processes has been minimal, and examination of fine structure in brains not demonstrating obvious perinatal destructive lesions has been limited as well [Nelson et al., 1994]. The presence of microcephaly at birth, dysmorphic features, and congenital anomalies outside the nervous system suggests early developmental defects.
CLINICAL FEATURES AND DIAGNOSIS Delay in attaining developmental milestones is the most distinctive presenting complaint in children with cerebral palsy. A detailed history and thorough physical and neurologic examinations are crucial in the diagnostic process. Records of the mother’s pregnancy and delivery and of the infant’s early neonatal period may be invaluable. Video recordings may be helpful. Physical and neurologic abnormalities may be subtle. The clinician should be cautious about diagnostic pronouncements unless the findings are unequivocal. Prognostic statements generally are not appropriate until after several serial examinations and history review sessions. The clinical findings often change with maturation; both severity and distribution may be altered. A child with cerebral palsy who has been hypotonic may become hypertonic. A number of infants with mild abnormalities subsequently demonstrate a decrease or, in some instances, a disappearance of motor dysfunction [Nelson and Ellenberg, 1982]. The clinical picture should not include evidence of progressive disease or loss of skills previously acquired. Any suggestion of progression of disability should result in expansion of the differential diagnosis to explain the progression. The history should focus on an attempt to identify a specific cause and should especially investigate familial or metabolic disease that might have implications for treatment or family counseling [Barabas and Taft, 1986]. The neurologic evaluation of the infant depends on the assessment of infantile developmental reflexes, muscle tone, deep tendon reflexes, and plantar responses. The use of standard developmental screening tests (e.g., the Denver Developmental Screening Test II) may provide quantitative evidence of motor delay, as well as evidence of delay in acquisition of other skills. Other constituents of the neurologic examination also are important and should be carefully documented by the examiner. Several approaches to evaluating infants have been well described [Capute et al., 1984; Ellison, 1984; Paine, 1964] (see Chapter 4). Although no one plan can suffice to establish the diagnosis of cerebral palsy, an algorithm for evaluation of the child with cerebral palsy has been published (Fig. 20-1) [Ashwal et al., 2004]. This algorithm provides an approach that should prove to be useful.
Further Diagnostic Evaluation The diagnosis of cerebral palsy often is indicated by delayed developmental milestones, the persistence of developmental reflexes, the presence of pathologic reflexes, and the failure to
Swaiman and Wu / Cerebral Palsy
495
FIGURE 20-1. Algorithm for the evaluation of the child with cerebral palsy (CP). Screening for associated conditions (mental retardation, vision/hearing impairments, speech and language delays, oral motor dysfunction, and epilepsy) is recommended. Neuroimaging (magnetic resonance imaging [MRI] is preferred to computed tomography [CT]) is recommended for further evaluation if the etiology has not been previously determined. In some children, additional metabolic or genetic testing may be indicated. EEG, electroencephalogram. (From Ashwal S, Russman BS, Blasco PA, et al. Practice parameter: Diagnostic assessment of the child with cerebral palsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2004;62:851-863.)
develop maturational reflexes in a timely fashion, such as the traction response and the parachute response (see Chapter 4). Diagnostic tests designed to establish the etiology of cerebral palsy have been recently reviewed as part of a practice parameter [Ashwal et al., 2004]. An abnormality is documented on head magnetic resonance imaging (MRI) (in 89% of cases) or computed tomography (CT) (in 77%) in a large percentage of patients; therefore, all children with cerebral palsy should undergo a neuroimaging study, preferably MRI [Accardo et al., 2004]. Because of the reported low incidence of metabolic and genetic disorders among children with cerebral palsy, testing for these disorders is indicated only in children in whom the history or clinical examination includes atypical features or if a specific diagnosis is not established with neuroimaging. Children with a brain malformation also warrant consideration for further
testing to determine if an underlying genetic or metabolic disorder is present. The high incidence rates for mental retardation (52%), epilepsy (45%), ophthalmologic defects (28%), speech and language disorders (38%), and hearing impairment (12%) [Ashwal et al., 2004] make it imperative that all children with cerebral palsy be screened for mental retardation, ophthalmologic and hearing impairments, and speech and language disorders; nutrition, growth, and swallowing also should be closely monitored.
CLASSIFICATION The nosology applied to cerebral palsy is often varied and sometimes confusing. Agreement among clinical observers concerning a specific patient may be lacking [Blair and
496
Perinatal Acquired and Congenital Neurologic Disorders / 20
Stanley, 1985]. The classification of cerebral palsy patients remains somewhat unsettled and continues to require revision [Shapiro, 2004]. The use of conventional neurologic terms in descriptions of patients in recent years has made classification somewhat more understandable.
Functional Classification The Gross Motor Function Classification System (GMFCS) has become increasingly accepted for characterizing children with cerebral palsy. Selection of 85 items in this classification system was based on literature review and clinical judgment [Russell et al., 1989]. The scale was further refined, and the number of items was reduced to 66 (GMFM-66) [Russell et al., 2002]. The validated Gross Motor Function Classification System (GMFCS) provides an easy and straightforward way to classify severity of motor impairment into one of the five levels [Palisano et al., 1997]. The GMFCS scale has been found to predict GMFM scores [Palisano et al., 2000] and is simpler to use. Some evidence suggests that family reporting may be utilized to enhance the use of the GMFCS [Morris et al., 2004]. In recent years, the GMFCS has been applied to develop five distinct motor development curves for use in prognostication [Rosenbaum et al., 2002]. Many other scales and inventories are in use, however [Shapiro, 2004]. These include the modified Ashworth scale, passive Range of Motion measurements, Selective Motor Control scale, and the Pediatric Evaluation of Disability Inventory [Ostensjo et al., 2004]. Adequacy of performance of everyday activities is best predicted by the child’s ability to perform gross motor tasks [Ostensjo et al., 2004].
SPECIFIC CEREBRAL PALSY SYNDROMES Cerebral palsy can be classified by the predominant type of motor abnormality—spasticity, choreoathetotic, dystonic, hypotonic, ataxic, or mixed—as well as by the distribution of limb involvement—hemiplegia, quadriplegia, or diplegia. The most common clinical cerebral palsy syndromes are discussed next.
Spastic Hemiplegia Clinical Findings Although children may manifest obvious hemiplegia in the second year of life, specific difficulties may not be observed during the first 3 to 5 months of life. After a perinatal stroke, an infant may be neurologically normal until the development of pathologic handedness at approximately 4 to 6 months of age. For unexplained reasons, the left hemisphere (right side) is affected in two thirds of patients, and perinatal stroke is more common on the left than on the right [Crothers and Paine, 1959; Nelson and Lynch, 2004]. During the examination, the child exhibits impaired gross and fine motor coordination, has difficulty moving the hand quickly, and frequently is unable to grasp small items with a pincer grasp. The obligate palmar grasp reflex, which usually is absent by age 6 months and frequently rudimentary
after age 4 months, may be obligate. Weakness of the wrist and forearm often is associated with limitation of range of motion of supination. The range of elbow extension may be restricted. Attempts at reaching for objects may be accompanied by athetotic posturing with flexion of the wrist and hyperextension of the fingers (avoidance reaction). Facial involvement is unusual. Only 10% of affected patients, including those with extensive hemiplegia, have homonymous hemianopia [Black, 1988]. Children with hemiparesis have a circumductive gait with a variable degree of abnormality. Most commonly the child walks on the toes and swings the affected leg over a nearly semicircular arc during the course of each step. In contrast with the leg, the affected arm usually moves less than normal and does not participate in normal reciprocal motion during ambulation. An equinovarus positioning of the foot is seen; weakness and lack of full range of motion of dorsiflexion often are present. Further evidence of upper motor neuron involvement on the hemiplegic side includes hyperreflexia of the deep tendon reflexes, ankle clonus, and extensor toe signs. Such children usually have intact cremasteric and abdominal reflexes. Growth retardation of the abnormal side, usually more prominent in the distal arm and hand or distal leg and foot, may be manifest. An indication of the presence of growth impairment may be obtained when the thumb and thumbnail of the affected side are compared with their normal opposite members and found to be smaller. Growth discrepancy of the leg may result in significant difficulties during walking, leading to orthopedic problems involving the proximal leg and the lower spinal vertebrae. Although frequently overlooked, corticosensory impairment and hemineglect of the affected side are common. Examination for the integrity of stereognosis and graphesthesia usually reveals varying degrees of compromise [Brown et al., 1987; Skatvedt, 1960]. Perlstein and Hood [1955] reported that approximately 28% of patients with infantile hemiplegia have some degree of mental retardation. Seizures occur in approximately one third of patients who have spastic hemiplegia. Mental retardation is highly correlated with epilepsy in hemiplegic patients [Aicardi, 1990; Uvebrant, 1988]. Prognosis is difficult to establish in patients with hemiplegic cerebral palsy. Review of birth history and findings on EEG and CT scans in 52 children was performed by Cohen and Duffner [1981]. They concluded that the birth history was of little value in judging prognosis. EEG and neuroimaging findings provide a better correlation with the development of seizures and mental impairment. Furthermore, if anatomic abnormalities of the cerebral cortex, commissural pathways, or association pathways are present, these children are more likely to experience seizures and mental retardation.
Pathologic Findings Because various underlying conditions may lead to spastic hemiplegia, the neuropathologic findings also vary. Development of infarction with subsequent cystic formation in the distribution of the middle cerebral artery frequently is observed. The pathogenesis of the thromboembolic infarction is infrequently determined, although potential embolic sources include the placenta, the heart, and an intracranial or extra-
Swaiman and Wu / Cerebral Palsy
497
cranial vessel [Guzetta et al., 1986; Nelson and Lynch, 2004; Uvebrant, 1988]. The vascular insult may be prenatal [Asindi et al., 1988] or perinatal [Baumann et al., 1987; Wiklund et al., 1991]. The degree of involvement varies. In an extreme form, the white and gray matter overlying the lateral ventricle may be so greatly thinned that the ventricle may extend into the area, with the development of a porencephalic cyst. Examination of the brain demonstrates generalized atrophy in the affected hemisphere. Although the affected areas may be small and few in number, large areas of gross cortical thinning, with loss of underlying white matter and extensive dilation of the adjoining lateral ventricle, may be seen. Microscopic examination confirms disruption of the neuronal laminar pattern, neuronal loss, and associated gliosis of variable extent. In preterm infants, asymmetric periventricular leukomalacia with resultant loss of white matter and ventricular dilation may be present [Uvebrant, 1988; Wiklund et al., 1991]. In one report on use of CT scanning in 111 children with hemiplegia, findings were normal in 29%. Periventricular atrophy was present in 42%, maldevelopment in 17%, and cortical-subcortical atrophy in 12%; miscellaneous abnormalities were noted in 3% [Wiklund et al., 1991].
pneumonia during the first years of life. Almost 50% of children with spastic quadriplegia experience generalized tonic-clonic seizures [Ingram, 1964]. In addition, a large but indeterminate number of these children are grossly developmentally delayed [Crothers and Paine, 1959]. Neurologic examination demonstrates marked spasticity and accompanying signs of corticospinal tract involvement, including hyperactive deep tendon reflexes, ankle clonus, and extensor toe signs. Weakness of dorsiflexion of the feet associated with equinovarus deformities is common. Marked spasticity of the hip muscles may lead to subluxation of the femur and associated acetabular pathologic conditions. Radiographs may be necessary to exclude the abnormal positioning of the head of the femur. Flexion contractures of the wrists and elbows of various degrees and spasticity of the arm muscles are readily apparent. Ophthalmologic evaluation of children with spastic quadriplegia more commonly reveals visual impairment in these children than in children with athetoid cerebral palsy [Preakey et al., 1974]. The incidence of auditory, visual, motor, and learning disability is much higher in children with spastic quadriplegia than in children with spastic hemiplegia, spastic diplegia, and ataxic cerebral palsy [Robinson, 1973].
Spastic Quadriplegia
Pathologic Findings
Clinical Findings
Neuropathologic changes in children with spastic quadriplegia include cystic degeneration as the final outcome of softening, necrosis, and edema of the central white matter, as well as cyst formation. Although cortical abnormalities are almost always present, involvement is not as extensive as that found in white matter. Multicystic encephalomalacia and brain malformations commonly are present [Benda, 1952; Chutorian et al., 1979]. Studies using diffusion-tensor imaging of central white matter pathways suggest disruption of connections to sensory cortex in these children [Hoon et al., 2002]. Mantle sclerosis may be found in patients with mild-tomoderate quadriplegia. Necrosis of the subcortical white matter is accompanied by degeneration of the overlying cortical laminar pattern. Underlying status spongiosus may be the end stage of a grouping of numerous small subcortical cysts. Gliosis is prominent in the area usually occupied by neurons, and the meninges are grossly thickened. The extent of the lesions varies, with involvement ranging from an entire hemisphere to an entire lobe to portions of one lobe. Mantle sclerosis may be bilateral but is almost always more profound in one hemisphere. Alterations in brainstem structure also are commonly present [Wilson et al., 1982].
Little [1861] first described cerebral palsy. He used the term spastic rigidity in place of the modern term spasticity. As part of his original treatise, he wrote: Spastic cerebral palsy has the characteristics of upper motor unit involvement, such as hyperreflexia and increased tone, often with ankle clonus, crossed adductor reflexes, and extensor toe signs. Both lower extremities are more or less generally involved. Sometimes the affection of one limb only is observed by the parent, but examination usually shows a smaller degree of affection in the limb supposed to be sound. The contraction in the hips, knees, and ankles is often considerable. The flexors and adductors of thighs, the flexors of knees, and the gastrocnemii, preponderate. In most cases, after a time, owing to structural shortening of the muscles and of the articular ligaments, and perhaps to some changes of form of articular surface, the thighs cannot be completely abducted or extended, the knees cannot be straightened, nor can the heels be properly applied to the ground. The upper extremities are sometimes held down by preponderating action of pectorals, teres major and teres minor, and latissimus dorsi; the elbows are semiflexed, the wrists partially flexed, pronated, and the fingers incapable of perfect voluntary direction. Sometimes the upper extremities appear unaffected with spasm or want of volition, sometimes a mere awkwardness in using them exists.
Spastic quadriplegia is characterized by a generalized increase in muscle tone. The legs are involved more than the arms, and paucity of limb movement is characteristic. Opisthotonic posturing may be evident in early infancy and may persist through the first year of life. Movement of the head often initiates forced extension of the arms and legs, resulting in a position similar to that in decerebrate rigidity. Accompanying supranuclear bulbar palsy, the result of bilateral corticobulbar tract impairment, may produce difficulties with swallowing and articulation. The incoordination of the oropharyngeal muscles may predispose the patient to recurrent
Spastic Diplegia Clinical Findings Spastic diplegia is characterized by bilateral leg involvement and commonly some degree of upper extremity impairment. Preterm infants are particularly prone to spastic diplegia. Approximately 80% of preterm infants who manifest motor abnormalities have spastic diplegia [McDonald, 1963]. In recent years, the survival of very small preterm infants has resulted in a larger group of more severely neurologically impaired survivors [Hagberg et al., 1989a, 1989b].
498
Perinatal Acquired and Congenital Neurologic Disorders / 20
Some infants with spastic diplegia manifest ataxia after further maturation. These infants have a great increase of tone of the leg muscles and accompanying difficulties in coordination and strength. Impairment may be asymmetric. When a small child is held in the vertical position by the examiner and the plantar surfaces of the feet are lightly bounced on the examining table, adduction of the legs (scissoring) and obligatory extension (extensor thrust) are seen. The feet also are kept in an equinovarus posture. Further examination reveals weakness of dorsiflexion of the feet. In older children, this same spasticity causes them to toe-walk. As expected, signs of upper motor unit involvement are easily demonstrable in the legs (e.g., hyperactive deep tendon reflexes, bilateral ankle clonus, extensor toe signs). Striking spasticity of the hip muscles may lead to subluxation of the femur and associated acetabular pathologic conditions and further restriction of motion. Radiographs may be necessary to exclude the abnormal positioning of the femoral head. The arms may be affected but usually only to a mild degree. The child may hold the arms in unusual fixed postures, either extended or flexed during walking, and may have clumsy, reciprocating, swinging arm movements or hold both arms flexed at the elbows. Affected children may extend their arms, pronate their hands, and clench their fists during running. Associated athetosis makes this latter posturing more likely. Vasomotor instability, often manifested by cold extremities and variable and sometimes unpredictable patterns of sweating, may prove troublesome for the patient. After a variable period, usually 18 months to 2 years in children with moderate involvement, spasticity is increasingly accompanied by contractures that maintain the hips in flexion, knees in flexion, and the feet in an equinovarus position. For reasons that are unclear—either disuse or probably hemispheric (parietal) lobe dysfunction—marked retardation of growth of leg length may be a feature.
subcortical gray matter regions can be uniformly associated with the individual movement abnormality or specific combination of these movements. Patients are unable to smoothly perform meaningful movements because of interfering movements and involvement of inappropriate agonist and antagonist muscles (see Chapter 58). Extrapyramidal cerebral palsy involves defects of posture and involuntary movement (e.g., athetosis, ballismus, chorea, dystonia); increased tone usually is associated with these conditions and is of the “lead pipe” or rigid variety. Extrapyramidal cerebral palsy can be divided arbitrarily into two primary clinical subtypes—choreoathetotic and dystonic. Each may be accompanied by other extrapyramidal movements. Other classifications and subdivisions have been proposed [Kyllerman, 1983]. No classification is fundamentally satisfactory.
CHOREOATHETOTIC CEREBRAL PALSY
Examination of the brain of infants with spastic diplegia may reveal porencephalic cysts and abnormalities of gyral size (microgyria). Periventricular leukomalacia in the path of fibers coursing through the internal capsule that subserve leg function explain the clinical symptoms in many of these infants [Benda, 1952; Christensen and Melchior, 1967]. Preterm infants are particularly susceptible to these germinal matrix periventricular lesions, although the pathologic and clinical patterns also may develop in term infants [Hagberg et al., 1975a, 1975b]. CT or preferably MRI confirms the presence of periventricular leukomalacia and various degrees of ventricular dilation. The presence of atrophy, abnormal gray matter configuration, and marked leukomalacia is correlated with severe impairment [Yokochi et al., 1990]. MRI studies appear to be more sensitive than CT studies and correlate well with clinical impairment [Yokochi et al., 1990].
Choreoathetotic cerebral palsy is characterized by largeamplitude, involuntary movements. The most obvious and dominating movement component is athetosis. Chorea is present in variable degree. Tremor, myoclonus, and even some element of dystonia also may be evident. Athetosis usually involves the distal limbs. Athetosis results in slow, writhing involuntary movements. Other common features are finger and toe extension and rotation of the limb and its long axis. The resultant pattern of these movements culminates in bizarre transient positions of the limbs. Chorea may involve the face, limbs, and rarely the trunk. The choreiform movements can be characterized as asymmetric, fleeting, incoordinated, involuntary contractions of individual muscle groups. The combination of athetoid and choreiform movements results in a pattern of distal extremity movement, ongoing hypertonia, and rotary writhing movements of the limbs. Athetotic posturing may be evident in the first year of life when the child begins to reach for objects. The movements, as generally is true of most involuntary movements, are not present during sleep. Movements are more prominent during stress or illness, and their intensity changes from day to day. As expected from the pathologic findings, evidence of upper motor neuron unit impairment (e.g., hyperactive deep tendon reflexes, ankle clonus, positive extensor toe signs), as well as seizures, spasticity, and mental retardation, may be present. Children with choreoathetosis may have marked difficulty with speech that is characterized by great variability in rate and explosive changes in volume. Ballismus, a movement disorder in which the arms and legs are violently flung about, may be an extreme form of choreoathetotic cerebral palsy. Most of the activity takes place at the shoulders and hips. Although patients with ballismus are said to have a shortened life expectancy and do not survive beyond the second decade, few data are available, and clinicopathologic correlation is undefined.
Extrapyramidal Cerebral Palsy
DYSTONIC CEREBRAL PALSY
The extrapyramidal cerebral palsy classification is rather broad based, but for all practical purposes, little in the way of pathogenetic lesions or specific involvement of cortical or
The dystonic form of cerebral palsy is uncommon. The extrapyramidal form of cerebral palsy is often, but not always, preceded by hypoxic-ischemic brain injury or kernicterus.
Pathologic Findings
Swaiman and Wu / Cerebral Palsy
Requirement for respiratory support and hypoxic-ischemic encephalopathy at birth usually is documented in the patient history. The dystonic movements are not unlike those in other conditions associated with dystonia. The trunk muscles and proximal portions of the limbs are predominantly affected. Movements may be slow and persistent, particularly of the head and neck, which may be pulled to one side or the other, or retrocollis may be present. At times the movements may consist of rapid and repetitive retractions of the head. The trunk may be literally twisted into many fixed positions that may appear bizarre. Corticospinal tract findings may be evident in children who have choreoathetosis. On pathologic examination, the brains of these children may reveal large areas of patchy necrosis of the cortical laminar pattern, venous congestion in the cortex, ventricular dilation, and accompanying white matter loss that may be related to demyelination and central necrosis. Fibrosis in the meninges also may be present. Both cortex and basal ganglia may be jointly involved in these patients. Cortical lesions associated with necrosis in areas adjacent to the ventricles may be the result of occlusion of the vein of Galen. Obstruction of this major vessel triggers a chain of events, including rupture of blood vessels, primarily veins, with ensuing multiple hemorrhages in the areas served by the branches of the internal cerebral veins. The hemorrhages result in subependymal necrosis and subsequent pathologic dilation of the lateral ventricles and associated atrophy of the basal ganglia. If obstruction is extremely widespread, the internal capsule may be involved, and further symptoms and signs of corticospinal tract involvement arise. In one report, patients with severe athetoid cerebral palsy originating perinatally were divided into two groups neuropathologically: the “globo-Luysian group” and the “thalamoputaminal group.” The major abnormal sites in the globo-Luysian group were the pallidum and subthalamic nucleus, and in the thalamoputaminal group, the thalamus and putamen. The causative pathologic condition in the globo-Luysian group was primarily perinatal severe jaundice, and the cause in the thalamoputaminal group was predominantly neonatal asphyxia. The patients in the thalamoputaminal group demonstrated lower mental ability and suffered from more intractable convulsions than those in the globo-Luysian group. In the globo-Luysian group, rigidity and spasticity were frequently demonstrated, with fluctuation of athetoid movements, whereas in the thalamoputaminal group, various abnormalities of muscle tone and rather restricted athetosis were observed [Hayashi et al., 1991]. MRI studies in 22 children with athetotic cerebral palsy frequently revealed high-intensity areas in the thalamus and putamen in T2-weighted images. Of 16 children with known perinatal asphyxia, 14 had lesions in the basal ganglia, thalamus, and/or cerebral white matter. MRI findings were normal in 7 of the 22 children [Yokochi et al., 1991].
Hypotonic (Atonic) Cerebral Palsy Infants with hypotonic cerebral palsy almost always have associated leg weakness. Although hypotonic, the arms may manifest near-normal strength and coordination. In the past, this combination of clinical findings led to the use of the term atonic diplegia to describe such children.
499
Diagnosis is difficult because of the plethora of possibilities. Most children with generalized hypotonia have so-called central hypotonia (see Chapter 5), resulting from inadequate control of the motor pathways and subsequent disruption of gamma loop function. Others, with absent or hypoactive deep tendon reflexes, may have involvement of the lower motor neuron unit (i.e., anterior horn cell, peripheral nerve, neuromuscular junction, muscle). Extrapyramidal (choreoathetotic and dystonic) cerebral palsy may be preceded by a hypotonic phase. Atonic cerebral palsy is relatively uncommon compared with other forms of cerebral palsy; it often is associated with slow attainment of motor milestones and the presence of normal or hyperactive deep tendon reflexes. Children with atonic cerebral palsy, when suspended while held under the arms, flex both legs at the hips (Förster’s sign). Although in the past it has been thought that muscle tone almost always increases with maturation in this form of cerebral palsy [Ingram, 1964], experience has taught that in a sizable number of cases, spasticity does not develop, but the child remains hypotonic. The causes leading to this condition and the associated anatomic location of brain involvement are unknown. It is through their effect on the gamma motor neuron that portions of the central nervous system (e.g., motor cortex, thalamus, basal ganglia, vestibular nuclei, reticular formation, cerebellum) modify tone, with ensuing hypotonia.
Ataxic Cerebral Palsy The last common form of cerebral palsy is the ataxic form. It sometimes coexists with spastic diplegia [Hagberg et al., 1975b]. This form usually is associated with other motor abnormalities; however, the diagnosis is applied only when the predominant manifestation is cerebellar dysfunction. Patients with ataxic cerebral palsy may have impairment of intellectual ability, but they are rarely grossly delayed [Clement et al., 1984]. Motor difficulties often are not apparent until late in the first year of life. Early manifestations include hypotonia, truncal ataxia with sitting, dysmetria, and gross incoordination. The motor involvement results in delayed attainment of motor skills; independent walking may not occur until age 3 or 4 years and then may be performed only with great difficulty and frequent falling. Compromise of writing skills and other skills that demand good fine motor coordination often adversely affects educational endeavors. Examination often reveals nystagmus, dysmetria, hypotonia, and a wide-based gait. The result on Romberg testing with the eyes open is positive. Likely sites of involvement are the cerebellum and adjacent brainstem. Because of the large number of conditions associated with ataxia, the clinician must exclude conditions in which ataxia predominates in early childhood (see Chapter 57). Ataxia, especially if accompanied by mental retardation, may not be properly included among cerebral palsy conditions but may be the result of one of many inherited conditions [Hagberg et al., 1984]. The pathologic features of ataxic cerebral palsy are poorly defined and inconstant. Discussion of these features is confounded by the fact that total absence of the vermis may not give rise to cerebellar symptoms in certain congenital
500
Perinatal Acquired and Congenital Neurologic Disorders / 20
conditions, whereas aplasia of the vermis may be associated with nonprogressive ataxia [Bordarier and Aicardi, 1990]. Cerebellar hemispheric lesions may or may not be present in patients with ataxic cerebral palsy. The lack of correlation of evident structural changes with functional impairment is emphasized by CT studies. In one report, CT evaluation of patients with ataxic cerebral palsy revealed that the posterior fossa was normal in 38% and abnormal in 28%. By contrast, the cerebral hemispheres were abnormal in 55% of the patients [Miller and Cala, 1989].
Mixed Cerebral Palsy Mixed cerebral palsy includes manifestations of both spastic and extrapyramidal types; often an ataxic component is present. Patients with predominantly spastic quadriplegia may have a mild-to-marked degree of choreoathetosis. Conversely, frequently patients in whom choreoathetosis predominates also may manifest upper motor neuron unit involvement. These patterns of motor impairment are the result of compromise of large areas of the brain with sequelae of basal ganglia, cortex, and subcortical disruption. Characteristics of these patients are discussed in the sections describing individual types. Most patients can be categorized into the types discussed on the basis of predominant manifestations.
GENERAL PROGNOSIS FOR MOTOR FUNCTION A number of factors affect the prognosis of the child with cerebral palsy: the clinical type of cerebral palsy; the degree of delay in meeting milestones noted at evaluation; the pathologic reflexes present, and the degree of associated deficits in intelligence, sensation, and emotional adjustment [Sala and Grant, 1995]. Cognitive level is difficult to assess in the young child with motor impairments but can be gauged even in the severely affected child [McCarty et al., 1986]. It is necessary to consider the cognitive level despite the challenges posed in assessment, because the level of mental function may be the factor that really determines the quality of life the child will enjoy. Children with hemiplegia but with no other major problems almost always walk by the age of approximately 2 years; some benefit from use of a short leg brace, often needed only for temporary assistance. The presence of a small hand on the hemiplegic side, with a thumbnail that is narrower than that of the other thumb, may be associated with sensory dysfunction of parietal origin, and the sensory defect may limit the development of fine motor skills in that hand. About 25% of children with hemiplegias have hemianopsia; recognition of this deficit allows the clinician to advise placing the affected child in an area of the classroom that maximizes useful vision. Because most daily activities can be accomplished with only one hand, using the affected hand only as a “helper,” with small adaptations, such as shoes that do not require lacing and tying, hemiplegic children of reasonable intelligence can be expected to achieve independence in daily living. Seizures may be a problem in children with hemiplegia. More than 50% of children with spastic diplegia learn to walk, commonly by the age of approximately 3 years, but gait often is abnormal, and some children require assistance
devices such as crutches. Hand activities commonly are involved to some degree, although the impairment may be subtle. Abnormalities of extraocular movement are relatively common. Of children with spastic quadriplegia, 25% require total care; approximately 33% walk, usually after the age of 3 years. Intellectual function often is the most life-limiting concomitant problem, and involvement of the bulbar musculature may add further difficulties. Marked truncal hypotonia with pathologic reflexes or persisting rigidity is associated with an unfavorable outlook. A majority of such children have grave intellectual limitations. The prognosis for walking has been evaluated recently in large populations of children with cerebral palsy. The validated GMFCS can help predict whether the child will eventually achieve the ability to walk 10 steps unsupported. [Rosenbaum et al., 2002]. Furthermore, a child’s motor function at age 2 years can be used to evaluate the prognosis for future ambulation at three levels of competency, with the help of ambulation charts reflecting the combined experience of greater than 5000 children with cerebral palsy (Fig. 20-2) [Wu et al., 2004].
REFERENCES Accardo J, Kammann H, Hoon AH Jr. Neuroimaging in cerebral palsy. J Pediatr 2004;145 (Suppl 2):S19. Aicardi J. Epilepsy in brain-injured children with cerebral palsy. Dev Med Clin Neurol 1990;32:191. Ashwal S, Russman BS, Blasco PA, et al. Practice parameter: Diagnostic assessment of the child with cerebral palsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2004;62:851. Asindi AA, Stephenson JBP, Young DG. Spastic hemiparesis and presumed prenatal embolisation. Arch Dis Child 1988;63:68. Badawi N, Kurinczuk JJ, Keogh JM, et al. Intrapartum risk factors for newborn encephalopathy: The Western Australian case-control study. BMJ 1998a;317:1554. Badawi N, Kurinczuk JJ, Keogh JM, et al. Antepartum risk factors for newborn encephalopathy: The Western Australian case-control study. BMJ 1998b;317:1549. Badawi N, Watson L, Petterson B, et al. What constitutes cerebral palsy? Dev Med Child Neurol 1998c;40:520. Barabas G, Taft LT. The early signs and differential diagnosis of cerebral palsy. Pediatr Ann 1986;15:203. Barnett AL, Guzzetta A, Mercuri E, et al. Can the Griffiths scales predict neuromotor and perceptual-motor impairment in term infants with neonatal encephalopathy? Arch Dis Child 2004;89:637. Bartley J, Carroll JE. Stem cell therapy for cerebral palsy. Expert Opin Biol Ther 2003;3:514. Baumann RJ, Carr WA, Shuman RM. Patterns of cerebral arterial injury in children with neurological disabilities. J Child Neurol 1987;2:298. Bejar R, Coen RW, Merritt TA, et al. Focal necrosis of the white matter (periventricular leukomalacia): Sonographic, pathologic and electroencephalographic features. Am J Neuroradiol 1986;7:1073. Benda CE. Developmental disorders of mentation and cerebral palsies. New York: Grune & Stratton, 1952. Benda GI, Hiller JL, Reynolds JW. Benzyl alcohol toxicity: Impact on neurologic handicaps among surviving very low birthweight infants. Pediatrics 1986;77:507. Black PD. Ocular defects in children with cerebral palsy. BMJ 1988;281:487. Blair E. A research definition for “birth asphyxia”? Dev Med Child Neurol 1993;35:449. Blair E. Trends in cerebral palsy. Indian J Pediatr 2001;68:433. Blair E, Stanley F. Interobserver reliability in the classification of cerebral palsy. Dev Med Child Neurol 1985;27:615.
Swaiman and Wu / Cerebral Palsy
501
FIGURE 20-2. Ambulation charts showing the probabilities of four levels of ambulation over time. The graphs combine the data for 5366 children with cerebral palsy who were nonambulatory at age 2 years, 3152 of whom were monitored past age 6 years. Separate charts are provided for those with different levels of motor function at age 2 years. Rolling refers to the ability to roll over from front to back or from back to front. Sitting refers to the ability to maintain a sitting position without support or the ability to achieve a sitting position without assistance. (From Wu YW, Day SM, Strauss DJ, Shavelle RM. Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Blair E, Watson L, Badawi N, et al. Life expectancy among people with cerebral palsy in Western Australia. Dev Med Child Neurol 2001;43:508. Bordarier C, Aicardi J. Dandy-Walker syndrome and agenesis of the cerebellar vermis: Diagnostic problems and genetic counseling. A review. Dev Med Child Neurol 1990;32:285. Brown JK, Van Rensburg F, Walsh G, et al. A neurological study of hand function of hemiplegic children. Dev Med Child Neurol 1987;29:287. Burd L, Cotsonas-Hassler TM, Martsolf JT, Kerbeshian J, Recognition and managment of fetal alcohol syndrome. Neurotoxicol Teratol 2003;25:681–688. Cans C, Surman G, McManus V, et al. Cerebral palsy registries. Semin Pediatr Neurol 2004;11:18–22. Capute AJ, Palmer FB, Shapiro BK, et al. Primitive reflex profile: A quantitation of primitive reflexes in infancy. Dev Med Child Neurol 1984;26:375. Christensen E, Melchior J. Cerebral palsy—a clinical and neuropathological study. Clin Dev Med 1967;25:1.
Chutorian AM, Michener RC, Defendini R, et al. Neonatal polycystic encephalomalacia: Four new cases and review of the literature. J Neurol Neurosurg Psychiatry 1979;42:154. Clark SL, Hankins GD. Temporal and demographic trends in cerebral palsy—fact and fiction. Am J Obstet Gynecol 2003;188:628. Clement MC, Briard JL, Ponsot G, et al. Ataxies cerebelleuses congenitales nonprogressives. Arch Fr Pediatr 1984;41:685. Cohen ME, Duffner, PK. Prognostic indicators in hemiparetic cerebral palsy. Ann Neurol 1981;9:353. Colver AF, Gibson M, Hey EN, et al. Increasing rates of cerebral palsy across the severity spectrum in north-east England 1964-1993. The North of England Collaborative Cerebral Palsy Survey. Arch Dis Child Fetal Neonatal Ed 2000;83:F7. Cowan F, Rutherford M, Groenendaal F, et al. Origin and timing of brain lesions in term infants with neonatal encephalopathy. Lancet 2003;361:736. Croen LA, Grether JK, Curry CJ, et al. Congenital abnormalities among children with cerebral palsy: More evidence for prenatal antecedents. J Pediatr 2001;138:804.
502
Perinatal Acquired and Congenital Neurologic Disorders / 20
Crothers B, Paine RS. The natural history of cerebral palsy. Cambridge: Harvard University Press, 1959. Dammann O, Kuban KC, Leviton A. Perinatal infection, fetal inflammatory response, white matter damage, and cognitive limitations in children born preterm. Ment Retard Dev Disabil Res Rev 2002;8:46. Dammann O, Leviton A. Maternal intrauterine infection, cytokines, and brain damage in the preterm newborn. Pediatr Res 1997;42:1. de Vries LS, Connell JA, Dubowitz LMS, et al. Neurological, electrophysiological and MRI abnormalities in infants with extensive cystic leukomalacia. Neuropediatrics 1987;18:61. deVeber G, Andrew M. Cerebral sinovenous thrombosis in children. Canadian Pediatric Ischemic Stroke Study Group. N Engl J Med 2001;345:417. Ellenberg JH, Nelson KB. Cluster of perinatal events identifying infants at high risk for death or disability. J Pediatr 1988;113:546. Ellison PH. Neurologic development of the high-risk infant. Clin Perinatol 1984;11:41. Ericson A, Nygren KG, Olausson PO, et al. Hospital care utilization of infants born after IVF. Hum Reprod 2002;17:929. Evans PM, Evans SJW, Alberman E. Cerebral palsy: Why we must plan for survival. Arch Dis Child 1990;65:1329. Eyman RK, Grossman HJ, Chaney RH, et al. The life expectancy of profoundly handicapped people with mental retardation. N Engl J Med 1990;323:584. Golomb MR, MacGregor DL, Domi T, et al. Presumed pre- or perinatal arterial ischemic stroke: Risk factors and outcomes. Ann Neurol 2001;50:163. Grether JK, Cummins SK, Nelson KB. The California Cerebral Palsy Project. Paediatr Perinat Epidemiol 1992;6:339. Grether JK, Nelson KB, Cummins SK. Twinning and cerebral palsy: Experience in four northern California counties, births 1983 through 1985. Pediatrics 1993;92:854. Grether JK, Nelson KB. Maternal infection and cerebral palsy in infants of normal birth weight [published erratum appears in JAMA 1998;279:118]. JAMA 1997;278:207. Gross-Tsur V, Shalev RS, Badihi N, et al. Efficacy of methylphenidate in patients with cerebral palsy and attention-deficit hyperactivity disorder (ADHD). J Child Neurol 2002;17:863. Gunther G, Junker R, Strater R, et al. Symptomatic ischemic stroke in full-term neonates: Role of acquired and genetic prothrombotic risk factors. Stroke 2000;31:2437. Guzzetta F, Shackelford GD, Volpe S, et al. Periventricular intraparenchymal echodensities in the premature newborn: Critical determinant of neurologic outcome. Pediatrics 1986;78:995. Hagberg B, Hagberg G, Beckung E, et al. Changing panorama of cerebral palsy in Sweden. VIII. Prevalence and origin in the birth year period 1991-94. Acta Paediatr 2001;90:271. Hagberg B, Hagberg G, Olow I. The changing panorama of cerebral palsy in Sweden 1954-1970. I. Analysis of the general changes. Acta Paediatr Scand 1975a;64:187. Hagberg B, Hagberg G, Olow I. The changing panorama of cerebral palsy in Sweden 1954-1970. II. Analysis of the various syndromes. Acta Paediatr Scand 1975b;64:193. Hagberg B, Hagberg G, Olow I. The changing panorama of cerebral palsy in Sweden: IV. Epidemiological trends 1959-78. Acta Paediatr Scand 1984;73:433. Hagberg B, Hagberg G, Olow I, et al. The changing panorama of cerebral palsy in Sweden: V. The birth year period 1979-52. Acta Paediatr Scand 1989a;78:283. Hagberg B, Hagberg G, Zetterstrom R. Decreasing perinatal mortality— increase in cerebral palsy morbidity? Acta Paediatr Scand 1989b;78:664. Hagstrom JN, Walter J, Bluebond-Langner R, et al. Prevalence of the factor V Leiden mutation in children and neonates with thromboembolic disease. J Pediatr 1998;133:777. Hauser SE, Peters H. Glutaric aciduria type 1: An underdiagnosed cause of encephalopathy and dystonia-dyskinesia syndrome in children. J Paediatr Child Health 1998;34:302. Hayashi M, Satoh J, Sakamoto K, et al. Clinical and neuropathological findings in severe athetoid cerebral palsy: A comparative study of globo-Luysian and thalamo-putaminal groups. Brain Dev 1991;13:47. Hoon AH Jr, Lawrie WT Jr, Melhem ER, et al. Diffusion tensor imaging of periventricular leukomalacia shows affected sensory cortex white matter pathways. Neurology 2002;59:752.
Humphreys P, Whiting S, Pham B. Hemiparetic cerebral palsy: Clinical pattern and imaging in prediction of outcome. Can J Neurol Sci 2000;27:210. Hutton JL, Cooke T, Pharoah POD. Life expectancy in children with cerebral palsy. BMJ 1994;309:431. Ingram TTS. Paediatric aspects of cerebral palsy. Edinburgh: ChurchillLivingstone, 1964. Jarvis S, Glinianaia SV, Torrioli MG, et al. Cerebral palsy and intrauterine growth in single births: European collaborative study. Lancet 2003;362:1106. Johnson L, Brown AK, Bhutania VK. BIND—a clinical score for bilirubin induced neurologic dysfunction in newborns. Pediatrics 1999;104:746. Johnston MV. Clinical disorders of brain plasticity. Brain Dev 2004;26:73. Koman LA, Smith BP, Shilt JS. Cerebral palsy. Lancet 2004;364:28. Kyllerman M. Reduced optimality in pre- and perinatal conditions in dyskinetic cerebral palsy. Distribution and comparison to controls. Neuropediatrics 1983;14:29. Leviton A, Gilles FH. Acquired perinatal leukoencephalopathy. Ann Neurol 1984;16:1. Leviton A, Nelson KB. Problems with definitions and classifications of newborn encephalopathy. Pediatr Neurol 1992;8:85. Leviton A, Paneth N, Reuss ML, et al. Maternal infection, fetal inflammatory response, and brain damage in very low birth weight infants. Developmental Epidemiology Network Investigators. Pediatr Res 1999;46:566. Lieberman E, Lang J, Richardson DK, et al. Intrapartum maternal fever and neonatal outcome. Pediatrics 2000;105:8. Little WJ. On the influence of abnormal parturition, difficult labours, premature birth, and asphyxia neonatorum on the mental and physical condition of the child, especially in relation to deformities. Trans Obstet Soc London 1861;3:293. Lynch JK, Nelson KB. Epidemiology of perinatal stroke. Curr Opin Pediatr 2001;13:499. MacLennan A. A template for defining a causal relation between acute intrapartum events and cerebral palsy: International consensus statement. BMJ 1999;319:1054. McCarty SM, St. James P, Berninger VW, et al. Assessment of intellectual functioning span in severe cerebral palsy. Dev Med Child Neurol 1986;28:364. McDonald AD. Cerebral palsy in children of very low birth weight. Arch Dis Child 1963;38:579. Mercuri E, Rutherford M, Cowan F, et al. Early prognostic indicators of outcome in infants with neonatal cerebral infarction: A clinical, electroencephalogram, and magnetic resonance imaging study. Pediatrics 1999;103:39. Miller G, Cala LA. Ataxic cerebral palsy—clinico-radiologic correlations. Neuropediatrics 1989;20:84. Minear WL. A classification of cerebral palsy. Pediarics 1956;18:841–852. Moster D, Lie RT, Irgens LM, et al. The association of Apgar score with subsequent death and cerebral palsy: A population-based study in term infants. J Pediatr 2001;138:798. Murphy CC, Yeargin-Allsopp M, Decoufle P, et al. Prevalence of cerebral palsy among ten-year-old children in metropolitan Atlanta, 1985 through 1987. J Pediatr 1993;123:S13. Nelson KB, Dambrosia JM, Grether JK, et al. Neonatal cytokines and coagulation factors in children with cerebral palsy. Ann Neurol 1998;44:665. Nelson KB, Ellenberg JH. Children who “outgrew” cerebral palsy. Pediatrics 1982;69:529. Nelson KB, Grether JK. Potentially asphyxiating conditions and spastic cerebral palsy in infants of normal birth weight. Am J Obstet Gynecol 1998;179:507. Nelson KB, Lynch JK. Stroke in newborn infants. Lancet Neurol 2004;3:150–158. Nelson KB, Swaiman KF, Russman BS. Cerebral palsy. In: Swaiman KF, ed. Pediatric neurology: Principles and practice. St Louis: Mosby, 1994. Oeffinger DJ, Tylkowski CM, Rayens MK, et al. Gross Motor Function Classification System and outcome tools for assessing ambulatory cerebral palsy: A multicenter study. Dev Med Child Neurol 2004;46:311. O’Shea TM, Preisser JS, Klinepeter KL, et al. Trends in mortality and cerebral palsy in a geographically based cohort of very low birth weight neonates born between 1982 to 1994. Pediatrics 1998;101:642.
Swaiman and Wu / Cerebral Palsy Ostensjo S, Carlberg EB, Vollestad NK. Motor impairments in young children with cerebral palsy: Relationship to gross motor function and everyday activities. Dev Med Child Neurol 2004;46:580. Ostrow JD. Pascolo L, Brites D, Tribelli C. Molecular basis of bilirubininduced neurotoxicity. Trends Mol Med 2004;10:65–70. Paine RS. The evolution of infantile postural reflexes in the presence of chronic brain syndromes. Dev Med Child Neurol 1964;6:345. Palisano RJ, Hanna SE, Rosenbaum PL, et al. Validation of a model of gross motor function for children with cerebral palsy. Phys Ther 2000;80:974–985. Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39:214–223. Perlstein M, Hood P. Infantile spastic hemiplegia. Am J Med 1955;34:391. Petterson B, Nelson KB, Watson L, et al. Twins, triplets, and cerebral palsy in births in Western Australia in the 1980s. BMJ 1993;307:1239. Pharoah PO. Twins and cerebral palsy. Acta Paediatr Suppl 2001;90:6. Pharoah PO, Cooke T, Cooke RW, et al. Birthweight specific trends in cerebral palsy. Arch Dis Child 1990;65:602. Plioplys AV. Survival rates of children with severe neurologic disabilities: A review. Semin Pediatr Neurol 2003;10:120. Plioplys AV, Kasnicka I, Lewis S, et al. Survival rates among children with severe neurologic disabilities. South Med J 1998;91:161. Prasad AN, Breen JC, Ampola MG, et al. Argininemia: A treatable genetic cause of progressive spastic diplegia simulating cerebral palsy: Case reports and literature review. J Child Neurol 1997;12:301. Preakey A, Wilson J, Wilson B. Sensory and perceptual function in the cerebral palsied; perceptual relationships. J Nerv Ment Dis 1974;158:70. Redline RW, O’Riordan MA. Placental lesions associated with cerebral palsy and neurologic impairment following term birth. Arch Pathol Lab Med 2000;124:1785. Robinson R. The frequency of other handicaps in children with cerebral palsy. Dev Med Child Neurol 1973;15:305. Rosenbaum PL, Walter SD, Hanna SE, et al. Prognosis for gross motor function in cerebral palsy: Creation of motor development curves. JAMA 2002;288:1357. Russell DJ, Avery LM, Rosenbaum PL, et al. Improved scaling of the gross motor function measure for children with cerebral palsy: Evidence of reliability and validity. Phys Ther 2000;80:873. Russell DJ, Rosenbaum PL, Avery LM, et al. Gross Motor Function Measure (GMFM-66 and GMFM-88) user’s manual. London: Mac Keith Press, 2002. Russell DJ, Rosenbaum PL, Cadman DT, et al. The Gross Motor Function Measure: A means to evaluate the effects of physical therapy. Dev Med Child Neurol 1989;31:341. Sala DA, Grant AD. Prognosis for ambulation in cerebral palsy. Dev Med Child Neurol 1995;37:1020. Scheidt PC, Bryla DA, Nelson KB, et al. NICHD phototherapy clinical trial: Six year follow-up. Pediatrics 1990;85:455. Sever JL. TORCH tests and what they mean. Am J Obstet Gynecol 1985;152:495. Shapiro BK. Cerebral palsy: A reconceptualization of the spectrum. J Pediatr 2004;145 (2 Suppl):S3. Shapiro SM. Bilirubin toxicity in the developing nervous system. Pediatr Neurol 2003;29:410. Skatvedt M. Sensory, perceptual and other non-motor defects in cerebral palsy. Little Club Clin Dev Med 1960;1:115. Soorani-Lunsing I, Woltil HA, Hadders-Algra M. Are moderate degrees of hyperbilirubinemia in healthy term neonates really safe for the brain? Pediatr Res 2001;50:701. Steer PJ. Premature labour. Arch Dis Child 1991;66:1167. Strauss DJ, Shavelle RM, Anderson TW. Life expectancy of children with cerebral palsy. Pediatr Neurol 1998;18:143. Stromberg B, Dahlquist G, Ericson A, et al. Neurological sequelae in children born after in-vitro fertilisation: A population-based study. Lancet 2002;359:461. Szymonowicz W, Preston H, Yu VY. The surviving monozygotic twin. Arch Dis Child 1986;61:454. Takanashi J, Barkovich AJ, Ferriero DM, et al. Widening spectrum of congenital hemiplegia: Periventricular venous infarction in term neonates. Neurology 2003;61:531. Thorngren-Jerneck K, Herbst A. Low 5-minute Apgar score: A population-based register study of 1 million term births. Obstet Gynecol 2001;98:65.
503
Topp M, Langhoff-Roos J, Uldall P, et al. Intrauterine growth and gestational age in preterm infants with cerebral palsy. Early Hum Dev 1996;44:27. Topp M, Uldall P, Greisen G. Cerebral palsy births in eastern Denmark, 1987-90: Implications for neonatal care. Paediatr Perinat Epidemiol 2001;15:271. Uvebrant P. Hemiplegic cerebral palsy. Aetiology and outcome. Acta Paediatr Scand Suppl 1988;345 (Suppl):1. Uvebrant P, Hagberg G. Intrauterine growth in children with cerebral palsy. Acta Paediatr 1992;81:407. Van Praagh R. Diagnosis of kernicterus in the neonatal period. Pediatrics 1961;28:870. Volpe JJ. Neurology of the newborn, 4th ed. Philadelphia: WB Saunders, 2001. Volpe JJ, Herscovitch P, Perlman JM, et al. Positron emission tomography in the asphyxiated term newborn: Parasagittal impairment of cerebral blood flow. Ann Neurol 1985;17:287. Wiklund LM, Uvebrant P, Flodmark O. Computed tomography as an adjunct in etiological analysis of hemiplegic cerebral palsy. I: Children born preterm. Neuropediatrics 1991;22:50. Wilson ER, Mirra S, Schwartz JF. Congenital diencephalic and brain stem damage: Neuropathologic study of three cases. Acta Neuropathol 1982;57:70. Winter S, Autry A, Boyle C, et al. Trends in the prevalence of cerebral palsy in a population-based study. Pediatrics 2002;110:1220. Wu YW, Colford JM. Chorioamnionitis as a risk factor for cerebral palsy: A meta-analysis. JAMA 2000;284:1417. Wu YW, Day SM, Strauss DJ, et al. Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264. Wu YW, Escobar GJ, Grether JK, et al. Chorioamnionitis and cerebral palsy in term and near-term infants. JAMA 2003;290:2677. Wu YW, March WM, Croen LA, et al. Perinatal stroke in children with motor impairment: A population-based study. Pediatrics 2004;114:612. Wu YW, Miller SP, Chin K, et al. Multiple risk factors in neonatal sinovenous thrombosis. Neurology 2002;59:438. Yokochi K, Aiba K, Kodama M, et al. Magnetic resonance imaging in athetotic cerebral palsied children. Acta Paediatr Scand 1991;80:818. Yokochi K, Hosoe A, Shimabukuro S, et al. Gross motor patterns in children with cerebral palsy and spastic diplegia. Pediatr Neurol 1990;6:245.
SUGGESTED READINGS Bleck EE. Orthopaedic management in cerebral palsy. Clinics in Developmental Medicine No. 99. Philadelphia: Lippincott-Raven, 1987. Bobath K. Neurophysiological basis for the treatment of cerebral palsy. Clinics in Developmental Medicine No. 75. Philadelphia: LippincottRaven, 1991. Broggi G, Angelini L, Bono R, et al. Long-term results of stereotactic thalmotomy for cerebral palsy. Neurosurgery 1983;12:195. Burke JP, O’Keefe M, Bowell R. Optic nerve hypoplasia, encephalopathy, and neurodevelopmental handicap. Br J Ophthalmol 1991;75:236. Colditz PB, Henderson-Smart DJ. Electronic fetal heart rate monitoring during labour: Does it prevent perinatal asphyxia and cerebral palsy? Med J Aust 1990;153:88. Cooper IS, Riklan M, Amin I, et al. Chronic cerebellar stimulation in cerebral palsy. Neurology 1976;26:744. Crofts BJ, King R, Johnson A. The contribution of low birth weight to severe vision loss in a geographically defined population. Br J Ophthalmol 1998;82:9. Davidoff RA. Antispasticity drugs: Mechanism of action. Ann Neurol 1985;17:107. Dennis J, Johnson MA, Mutch LMM, et al. Acid-base status at birth in term infants and outcome at 4.5 years. Am J Obstet Gynecol 1989;161:213. Dinnage R. The child with cerebral palsy. National Children’s Bureau Bibliographies 2. Albany, NY: Delmar, 1986. Faust D, Ziskin J. The expert witness in psychology. Science 1988;239:31. Fenichel GM, Lane DA, Livengood JR, et al. Adverse events following immunization: Assessing probability of causation. Pediatr Neurol 1989;5:287. Gahm NH, Russman BS, Cerciello RL, et al. Chronic cerebellar stimulation for cerebral palsy: A double-blind study. Neurology 1981;31:87.
504
Perinatal Acquired and Congenital Neurologic Disorders / 20
Galjaard H, Prechtl HFR, Velickovic M. Early detection and management of cerebral palsy. Topics in the Neurosciences. Norwell, Mass: Kluwer Academic Press, 1988. Geralis E. Children with cerebral palsy: A parents’ guide. New York: Cambridge University Press, 1992. Gorter JW, Rosenbaum PL, Hanna SE, et al. Limb distribution, motor impairment, and functional classification of cerebral palsy. Dev Med Child Neurol 2004;46:461. Gross H, Jellinger K, Kaltenback E, et al. Infantile cerebral disorders: Clinical neuropathological correlations to elucidate the aetiological factors. J Neurol Sci 1968;7:551. Hoyme HE, Higginbottom MC, Jones KL. Vascular etiology of disruptive structure defects in monozygotic twins. Pediatrics 1981;67:288. Ingram T. A study of cerebral palsy in the childhood population of Edinburgh. Arch Dis Child 1955;117:395. Koeda T, Suganuma I, Kohno Y, et al. MR imaging of spastic diplegia: Comparative study between preterm and term infants. Neuroradiology 1990;32:187. Krageloh-Mann I, Hagberg B, Petersen D, et al. Bilateral spastic cerebral palsy—pathogenetic aspects from MRI. Neuropediatrics 1992;23:46. Landau WM, Hunt CC. Dorsal rhizotomy, a treatment of unproven efficacy. J Child Neurol 1990;5:174. Leviton A, Paneth N. White matter damage in preterm newborns—an epidemiologic perspective. Early Hum Dev 1990;24:1. Malamud N, Itabashi HH, Castor J, et al. An etiologic and diagnostic study of cerebral palsy. J Pediatr 1964;65:270. Melone PJ, Ernest JM, O’Shea MD, et al. Appropriateness of intrapartum fetal heart rate management and risk of cerebral palsy. Am J Obstet Gynecol 1991;165:272. Meyer BA, Dickinson JE, Chambers C, et al. The effect of fetal sepsis on umbilical cord blood gases. Am J Obstet Gynecol 1992;166:612. Miller F, Bachrach SJ. Cerebral palsy: A complete guide for caregiving. In: Johns Hopkins Press Health Book. Baltimore: Johns Hopkins University Press, 1998. Miller G, Clark CD. The cerebral palsies: Causes, consequences, and management. Boston: Butterworth-Heinemann, 1998. Morris C, Bartlett D. Gross Motor Function Classification System: Impact and utility. Dev Med Child Neurol 2004;46:60. Morris C, Galuppi BE, Rosenbaum PL. Reliability of family report for the Gross Motor Function Classification System. Dev Med Child Neurol 2004;46:455. Narayan RK, Loubser PG, Jankovic J, et al. Intrathecal Baclofen for intractable axial dystonia. Neurology 1991;41:1141. Nelson KB, Ellenberg JH. Apgar scores as predictors of chronic neurologic disability. Pediatrics 1981;68:36.
Nelson KB, Ellenberg JH. Cerebral palsy. 1. Univariate analysis of risks. Am J Dis Child 1985a;139:1031. Nelson KB, Ellenberg JH. Predictors of low and very low birth weight and the relation of these to cerebral palsy. JAMA 1985b;254:1473. Nelson KB, Leviton A. How much of neonatal encephalopathy is due to birth asphyxia? Am J Dis Child 1991;145:1325. Nelson KB. Prenatal origin of hemiparetic cerebral palsy: How often and why? Pediatrics 1991;88:1059. Paludetto R. Neonatal complications specific to twin (multiple) births (twins transfusion syndrome, intrauterine death of cotwin). J Perinat Med 1991;19 (Suppl 1):246. Peacock W, Staudt LA. Spasticity in cerebral palsy and the selective posterior rhizotomy procedure. J Child Neurol 1990;5:179. Perlman JM, Tack ED. Renal injury in the asphyxiated newborn infant: Relationship to neurologic outcome. J Pediatr 1988;113:875. Phelan JP, Ock Ahn M, Korst L, et al. Intrapartum fetal asphyxial brain injury with absent multiorgan system dysfunction. J Matern Fetal Med 1998;7:19. Scrutton D. Management of the motor disorders of children with cerebral palsy. Clinics in Developmental Medicine No. 90. New York: Cambridge University Press, 1991. Seidman DS, Paz I, Laor A, et al. Apgar scores and cognitive performance at 17 years of age. Obstet Gynecol 1991;77:875. Stanley F. Epidemiology of the cerebral palsies. Clinics in Developmental Medicine No. 87. Philadelphia: Lippincott-Raven, 1991. Sussman MD. The use of casts as an adjunct to physical therapy management of cerebral palsy patients. Proceedings: Orthopedic Aspects of Developmental Disabilities. University of North Carolina School of Medicine, Chapel Hill, 1978:47. Vogt C, Vogt O. Zur psychiatrischen Wurdingung der anatonschen Entdekung und Wertung des Status marmoratus striat. J Psychol Neurol 1928;37:387. Volpe JJ. Value of MR in definition of the neuropathology of cerebral palsy in vivo. Am J Neuroradiol 1992;13:79. Volpe JJ. Neurology of the newborn, 3rd ed. Philadelphia: WB Saunders, 1995. Watt J, Sims D, Harchom F. A controlled study of inhibition casting as an adjunct to physiotherapy for cerebral-palsied children. Dev Med Child Neurol 1986;28:480. Wiley ME, Damiano DL. Lower-extremity strength profiles in spastic cerebral palsy. Dev Med Child Neurol 1998;40:100. Young RR. Physiologic and pharmacologic approaches to spasticity. Neurol Clin 1987;5:529.
CHAPTER 21
Introduction to Genetics William B. Dobyns and Soma Das
In the broadest sense, genes are simply units of hereditary information; the genome is the totality of all the hereditary information in a cell or organism; and genetics may be defined as the study of genes and genomes. With the advent of modern molecular biology and the Human Genome Project, all aspects of genetics have come to play a more prominent role in the day-to-day evaluation and management of children with neurologic diseases, most of which have a genetic basis. This chapter presents a brief synopsis of the most important principles of genetics, to serve as background for information presented elsewhere in this text. More detailed information on genetics is available in many excellent textbooks, such as Genetics in Medicine [Nussbaum et al., 2001], Genes VIII [Lewin, 2003], and Human Molecular Genetics [Strachan and Read, 1999]. The last is availble online, along with several other relevant publications, at the National Center for Biotechnology Information web site (Table 21-1).
MOLECULAR BASIS OF HEREDITY Modern theories of molecular biology hold that all information needed for function of cells and organisms is contained in macromolecules composed of simple repeating units. The flow of genetic information is (almost) exclusively unidirectional: DNA → RNA → protein. That is, the sequence of deoxyribonucleic acid (DNA) specifies the syn-
thesis and sequence of ribonucleic acid (RNA) by a process known as transcription. Messenger RNA in turn specifies the synthesis and sequence of polypeptides, which are the building blocks of proteins, by a process known as translation. Other forms of RNA function independently. This theory is the central dogma of molecular biology. Accordingly, this chapter begins with a review of the structure and function of these three macromolecules. Several of the processes involved in gene (and protein) expression, including gene structure and organization, RNA processing, and epigenetics, are then reviewed. Epigenetics refers to modification of genes other than changes in the DNA sequence, especially addition of methyl groups to the DNA, which alter gene expression. The two most important epigenetic changes found to be relevant to clinical disorders to date are imprinting and X-inactivation.
Structure and Function of DNA DNA is a large polymer or macromolecule composed of linear sequences of simple repeating units. The specific sequence of these units contains all of the genetic information of an individual cell or organism. The structure of DNA in its native state was deduced by Watson and Crick in 1953 [Watson and Crick, 1953]. The basic repeating unit of DNA is the nucleotide, which consists of a five-carbon sugar known as deoxyribose; a phosphate group; and a nitrogencontaining base, which may be either a purine or a pyri-
TABLE 21-1 Genetic Information Sites Available on the Internet SITE
*
INTERNET ADDRESS
Disease-Oriented Web Sites GeneTests, GeneReviews* OMIM† via NCBI and direct
http://www.genestar.org/ or http://www.genereviews.org/ or http://www.genetests.org/ http://www.ncbi:.nlm.nih.gov/ or http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=OMIM
Genome Data Web Sites Ensemble‡ HUGO§ Human Genome Project|| NCBI homepage (Entrez)¶ NCBI SNP database (dbSNP) UCSC Genome browser**
http://www.ensembl.org/Homo_sapiens/ http://www.gene.ucl.ac.uk/nomenclature/ http://www.ornl.gov/sci/techresources/Human_Genome/home.shtml http://www.ncbi.nlm.nih.gov/ http://www.ncbi.nlm.nih.gov/projects/SNP/ http://genome.ucsc.edu/
The disease summaries in GeneReviews all are authored by experts and peer reviewed, so they typically are highly accurate and up to date. OMIM, Online Mendelian Inheritance in Man. The disease summaries in OMIM typically are done by staff with oversight and contain both dated and new data, so the information typically is confirmed from a second source. ‡ Ensemble Human Genome Browser. § Human Gene Nomenclature web site. || Human Genome Project Information maintained by the U.S. Department of Energy Office of Science. ¶ National Center for Biotechnology Information. ** University of California–Santa Clara Genome Bioinformatics site. †
508
Genetic, Metabolic, and Neurocutaneous Disorders / 21
midine (Fig. 21-1A). In DNA, the purine base may be either adenine (A) or guanine (G), and the pyrimidine base may be either thymine (T) or cytosine (C). Nucleotides polymerize into long chains by formation of phosphodiester bonds between the 5′ carbon position of one deoxyribose molecule and the 3′ carbon of the preceding deoxyribose molecule (see Fig. 21-1B). Each DNA molecule consists of two strands of nucleotides that are held together by weak hydrogen bonds between pairs of bases: A pairs only with T, and G pairs only with C. These paired units are known as base pairs (bp). In the native state, the two strands wind around each other to form a double helix that resembles a right-hand spiral staircase with two unequal grooves known as the major and minor grooves (Fig. 21-2). A single turn of the helix measures 3.4 nm and contains 10 nucleotides. Each strand has a directionality imparted by the deoxyribose sugar backbone. Adjacent nucleotides are linked by phosphodiester bonds between the 5′ and 3′ carbon atoms of the sugar residues, so that one end of the DNA strand has an unlinked 5′ carbon (the 5′ end) and the other end of the strand has an unlinked 3′ carbon atom (the 3′ end). The two strands are antiparallel— that is, they run in opposite directions so that the 5′ end of one strand is paired with the 3′ end of the other. Within living cells, DNA is associated with proteins and supercoiled into more complex structures known as chromosomes, which are described later in the chapter.
Thus, when the sequence of one DNA strand is known, the sequence of the opposite or complementary strand may be predicted. Thus, precise replication of DNA is possible, a process that involves initiation, elongation, and termination stages. The process begins with recognition of an “origin of replication.” Such points of origin are specific DNA sequences recognized by a protein complex known as the primosome that occur every 50 to 300 kilobases (kb) of DNA; the unit kb (kilobases) refers to 1000 sequential nucleotides. The two parental DNA strands must first be separated by helicase, an enzyme that unwinds the supercoiled DNA helix to create a replication fork. The process of elongation occurs at the site of the replication fork or replisome. Synthesis of new strands begins with the addition of approximately 10 RNA bases by a protein complex known as primase and then continues with chain elongation using the original strands as templates. This process is known as semiconservative replication. Both initiation or RNA priming and chain elongation involve large protein complexes that include several DNA polymerases. Five distinct DNA polymerases have been isolated in mammalian systems including human cell cultures (Table 21-2). They are able to copy DNA only by adding nucleotides to the 3′ end of the growing chain, so DNA can elongate only in the 5′ to 3′ direction. Thus, the template DNA can be read only in the reverse or 3′ to 5′ direction. As DNA is unwound, the replication fork necessarily unwinds one strand in the
5'
3'
O O
O
H
O
H C
C
H
H
C
O
P
C
H
O Purines
Pyrimidines
C
C N
C
HC
C
HN
C
H
CH3
N
N
–
H Thymine (T)
Adenine (A) O C
N
N
Guanine (G)
A
C
O
H
O
–
C
O
H
O
H
C
C
C
H
G
CH2
C
O H
O H C C H
CH O
N
H C
O
C
C
O
P
O
O
P
H C
N H
C
H
H2C
C
N CH
C
H C
O
NH2
C
O
H
N
O H
H2N
CH
C
CH2
T
O
C
N CH
C
A
H2C
O
NH2
HN
O
–
O
P O
H 5'
H Cytosine (C)
3'
B
FIGURE 21-1. A, The chemical structure of DNA depicts the four bases of DNA. B, The chemical structure of the sugar-phosphate backbone and 3′-5′ phosphodiester bonds.
O
Dobyns and Das / Introduction to Genetics
A. Double
B. Nucleosome fiber
helix
C. Solenoid
509
D. Interphase nucleus
(beads-on-a-string)
Nucleosome Portion of an interphase chromosome Each loop contains 100,000 bp of DNA ~200 bp DNA
2 nm
~10 nm
~30 nm
FIGURE 21-2. Several levels of protein packaging of DNA provide the structural support for chromosomes. A and B, The right-handed double helix of DNA wraps around a histone core to form nucleosomes. C and D, The nucleosomes are packed into a solenoid structure, and loops of solenoids compose an interphase chromosome. (Modified from Thompson MR, McInnes RR, Willard F, et al. Genetics in medicine, 5th ed. Philadelphia: WB Saunders, 1991.)
TABLE 21-2 DNA Polymerases in Mammalian Systems POLYMERASE
LOCATION
FUNCTION
3′ TO 5′ EXONUCLEASE
α(I) β γ δ(III) ε(II)
Nuclear Nuclear Mitochondrial Nuclear Nuclear
Priming, especially of lagging strand DNA repair Replicates mitochondrial DNA Synthesis or elongation DNA repair
No No Yes Yes Yes
3′ to 5′ direction and the other in the 5′ to 3′ direction. The 3′ to 5′ or leading strand is replicated in a continuous fashion at the replication fork by DNA polymerases α(I), which primes the reaction, and δ(III), which synthesizes the DNA chain. The new strand is complementary and so elongates in the opposite or 5′ to 3′ direction. The 5′ to 3′ or lagging strand cannot be copied continuously because this would require synthesis of the complementary new strand in a 3′ to 5′ direction, which is not possible, because DNA polymerases are able to synthesize DNA only in the 5′ to 3′ direction. Thus, the lagging strand is copied by DNA polymerases α(I) and δ(III) in small segments of 100 to 1000 base pairs in the opposite direction from the replication fork. These are known as Okazaki fragments. DNA replication is described as semidiscontinuous because of the continuous replication of the leading strand and the discontinuous replication of the lagging strand. The Okazaki fragments are then joined by another enzyme, DNA ligase. DNA replication is a long process, requiring about 8 hours in most human cells in culture. Thus, the function of DNA is to reliably encode and store the genetic information needed for the cell and organism to function. It has no direct
functions itself but rather acts by directing synthesis of both RNA and protein.
Structure and Function of RNA RNA differs chemically from DNA in the substitution of ribose for deoxyribose in the sugar backbone of the molecule and of uridine (U) for thymine as one of the pyrimidine bases. Also, RNA normally exists as a single-stranded rather than double-stranded molecule. Recent advances have demonstrated far more diverse functions for RNA than was previously appreciated, particularly involving genes that produce functional RNA products that do not code for proteins. These probably represent at least 5% of all human genes as suggested by current knowledge [Strachan and Read, 1999]. Several distinct classes of RNA molecules have been recognized, most of which are involved with regulating or assisting gene expression. Ribosomal RNA. Ribosomal RNAs (rRNAs) are functional RNA transcripts that constitute one of the main components of cytoplasmic ribosomes. The genes coding for the major form of cytoplasmic rRNA are located in multiple
510
Genetic, Metabolic, and Neurocutaneous Disorders / 21
TABLE 21-3 Classification of Amino Acids by Side Chain AMINO ACID
CODE
Neutral and Hydrophobic Alanine Isoleucine Leucine Methionine Phenylalanine Proline Tryptophan Valine
ala ile leu met phe pro trp val
A I L M F P W V
Acidic Aspartic acid Glutamic acid
asp glu
D E
AMINO ACID
CODE
Neutral and Polar Asparagine Cysteine Glutamine Glycine Serine Threonine Tyrosine
asn cys glu gly ser thr tyr
N C Q G S T Y
Basic Arginine Histidine Lysine
arg his lys
R H K
copies on the short arms of the acrocentric chromosomes (13, 14, 15, 21, 22); these genes produce a single large 45S primary transcript that is cleaved into 28S, 18S, and 5.8S rRNA classes, designated by their separation in centrifugation gradients and by several associated proteins. Multiple copies of another gene on chromosome 1 produce 5S rRNA. Transfer RNA. Transfer RNAs (tRNAs) are small RNA transcripts that bind specific amino acids and transport them to ribosomes for use during protein synthesis. More than 40 subfamilies of tRNA genes are known, dispersed across the genome. Messenger RNA. Messenger RNAs (mRNAs) are the RNA transcripts of all genes that encode polypeptides and some other genes that encode the unprocessed forms of functional RNAs. Messenger RNA molecules are large. All mRNA transcripts undergo further processing, including excision of large segments of noncoding RNA known as introns, the addition of 7-methylguanosine to the first 5′ nucleotide, forming a CAP structure, cleavage of the 3′ end at a specific point downstream from the end of the coding sequence, and addition of the polyA tail at a site specified in part by the sequence AAUAAA, which is located in the 3′ untranslated region (3′ UTR) of the gene. The polyA tail appears to increase the stability of mRNA. The fully processed mRNA is transported to the cytoplasm where translation occurs. Small Nuclear RNA. Small nuclear RNA (snRNA) transcripts are small, uridine-rich RNA transcripts that associate with specific proteins to form ribonucleoprotein particles (RNPs). Some of them function in RNA splicing (removing introns from mRNA). They comprise a large family of genes dispersed across the genome. Small Nucleolar RNA. Small nucleolar RNAs (snoRNAs) are small RNA transcripts that are present in the nucleolus and have important roles in specific cleavage reactions and base-specific modifications during maturation of ribosomal RNA. About 200 snoRNA genes have been identified. MicroRNA. MicroRNAs (miRNAs) are another class of small noncoding genes that regulate the expression of proteinencoding genes at the post-transcriptional RNA level [Denli et al., 2004]. The process begins with transcription (synthesis) of primary RNA transcripts that range in size from several hundred to several thousand kb. These transcripts are recognized
and cut into precursor miRNAs in the nucleus by a protein known as Dicer, moved to the cytoplasm, and processed into mature miRNAs. The mature miRNAs join the RNA-induced silencing complex (RISC) that recognizes and cleaves (or otherwise silences) a target gene. This process has been demonstrated in many organisms, including mammals, and appears likely to play a key role in regulation of many genes.
Structure and Function of Polypeptides and Proteins Proteins are composed of one or more polypeptide chains. Polypeptides are large polymers or macromolecules composed of linear sequences of repeating units known as amino acids, which are more complex than the repeating units of DNA or RNA. Amino acids consist of a three-carbon backbone with an amino group attached to carbon 1 and a carboxyl group to carbon 3. They differ in the composition of a side chain attached to carbon 2. With rare exceptions, all polypeptides and proteins in nature are built from different sequences of 20 amino acids (Table 21-3). The side chains may be neutral and hydrophobic, neutral and polar, basic, or acidic. The simplest amino acid is valine, which has a hydrogen ion as the side chain. The process of information transfer from RNA polypeptides and proteins is known as translation. It is based on the genetic code, the system by which the base sequence of mRNA specifies the amino acid sequence of a polypeptide chain. In this nearly universal code, each set of three adjacent bases in the mRNA transcript constitutes a codon, and different combinations of bases within the codon specify the individual amino acids (Table 21-4). The small tRNA molecules serve as the molecular link between mRNA codons and amino acids. One segment of each tRNA transcript contains a three-base anticodon that is complementary to a specific codon on the mRNA, whereas another segment contains a binding site for one of the 20 amino acids. With a total of only 20 amino acids and only 64 possible codons, most amino acids are specified by more than one codon. For some of the different amino acids, the base in the third position in the triplet may be either of the purines, either of the pyrimidines, or sometimes any of the four bases. For this reason, the third position in the codon sometimes is called the
Dobyns and Das / Introduction to Genetics
TABLE 21-4 The Nuclear Genetic Code U U
C
A
G
UUU UUC UUA UUG CUU CUC CUA CUG AUU AUC AUA AUG GUU GUC GUA GUG
C phe phe leu leu leu leu leu leu ile ile ile met val val val val
UCU UCC UCA UCG CCU CCC CCA CCG ACU ACC ACA ACG GCU GCC GCA GCG
A ser ser ser ser pro pro pro pro thr thr thr thr ala ala ala ala
UAU UAC UAA UAG CAU CAC CAA CAG AAU AAC AAA AAG GAU GAC GAA GAG
G tyr tyr stop stop his his gln gln asn asn lys lys asp asp glu glu
UGU UGC UGA UGG CGU CGC CGA CGG AGU AGC AGA AGG GGU GGC GGA GGG
cys cys stop trp arg arg arg arg ser ser arg arg gly gly gly gly
wobble position. Arginine and leucine are each specified by six codons, whereas only methionine and tryptophan are specified by a single codon. Three codons signal termination of translation and accordingly are called stop codons.
Transcription The process of information transfer from DNA to RNA is known as transcription. Synthesis of RNA begins at a specific transcription start site and continues in a 5′ to 3′ direction with regard to the RNA product. The DNA strand that corresponds to the RNA sequence is known as the coding or sense strand. This strand, however, is not used as the template for synthesis of an RNA molecule. Rather, the complementary DNA strand, known as the noncoding or antisense strand, actually serves as the template and is read in the 3′ to 5′ direction. The RNA product is known as a transcript.
Translation The process of information transfer from RNA to polypeptide or protein is known as translation. This process takes place in the cytoplasm on small structures known as ribosomes, macromolecules composed of the four species of rRNA noted earlier. They function like small migrating factories that travel along an mRNA template engaging in rapid cycles of peptide bond synthesis. The process consists of initiation, elongation, and termination stages. The ribosome contains a large site that binds about 35 bp of mRNA and two adjacent sites for binding the smaller aminoacyl-tRNA molecules. The first is the acceptor or A site, which holds the incoming aminoacyl-tRNA. The second is the donor or P site, which is occupied by a tRNA carrying the growing polypeptide chain. Translation begins with mRNA binding to the ribosome at the site of the first AUG base triplet, which specifies the amino acid methionine, and also serves as the start signal for synthesis of the polypeptide chain and establishes the reading frame of the mRNA. The mRNA and tRNA then move in the same direction along the ribosome, with the tRNA moving from the A site to the P site, and the mRNA sliding over three bases, allowing recognition of the next codon. Bonding between the mRNA codon and tRNA anticodon brings the appropriate amino acid into position on the ribosome to form a new pep-
511
tide bond to the carboxyl end of the growing polypeptide chain. As part of this reaction, the polypeptide chain is released from the tRNA at the P site but remains bonded to the tRNA at the A site. The tRNA and mRNA then move another three base pairs along the chain, and the process is repeated. This reaction continues until one of the stop codons is reached. Thus proteins are synthesized from the amino to the carboxyl terminus, which corresponds to translation from the 5′ to the 3′ end of the mRNA molecule, and methionine is always the first amino acid of each polypeptide chain, although it usually is removed before protein synthesis is completed.
Gene Structure and Organization As noted earlier, a gene has been traditionally defined as a unit of genetic information. This concept has gradually progressed to a more useful definition, which states that a gene is a sequence of chromosomal DNA that is required for production of a functional product, whether the product is RNA or protein [Nussbaum et al., 2001]. By convention, genetic information is always read in the 5′ to 3′ direction, whether encoded in DNA or RNA—in an upstream to downstream direction. The nomenclature regarding the 5′ and 3′ positions of the sugar backbone can be confusing. The 5′ carbon of the first nucleotide of a sequence is joined by a phosphodiester bond to a nucleotide not involved in the sequence, whereas its 3′ carbon is joined to the 5′ carbon of the second nucleotide, and so on. The last nucleotide of the sequence has a 3′ carbon, which joins another uninvolved nucleotide.
Genes Genes are composed of a continuous length of DNA with predominantly definable starts and end points, which include the sequence that codes for the RNA or polypeptide product. This part of the gene is known as the coding region. It has become clear, however, that the structure of a gene is complex and includes much more than the coding sequence of the protein. All genes include additional sequences on either end of the coding region—the 5′ and 3′ UTRs—that do not code for an RNA product or polypeptide. These regions function to regulate transcription and RNA stability. The gene is considered to include the entire sequence represented in the RNA product because some mutations within noncoding regions can impair gene function. A model of a typical human gene is shown in Figure 21-3. Promoter sequences required for regulation and initiation of RNA transcription are present at the 5′ end of the gene, such as the CAT and TATA boxes whose sequences are tightly conserved among many different genes and species. Downstream from the promoter sequences is a specific sequence that signals the start of transcription. Even further downstream is an initiator codon, AUG, which codes for methionine. This triplet signals the start of the actual coding sequence for the polypeptide product, as discussed in an earlier section. The region between the transcription and translation start sites is the 5′ UTR. The next segment of the gene is the coding region. The coding regions of most genes in prokaryotes and lower eukaryotes are colinear, which means that the coding sequence corresponds exactly to the sequence of amino acids
512
Genetic, Metabolic, and Neurocutaneous Disorders / 21 Introns 5' UTR
Highly-conserved regions
3' UTR
Transcription start site (RNA)
Exons
Translation start site (protein)
Translation end site (protein) Transcription end site (RNA)
FIGURE 21-3. The structure of a typical human gene.
in the polypeptide. By contrast, most higher eukaryotic genes including human genes contain additional sequences that lie within the coding region, interrupting the sequence that represents the polypeptide. The regions that code for the final polypeptide (or functional RNA) product are known as exons, whereas the regions that are missing from the final mRNA product are introns. The removal of introns from the final mRNA product is known as splicing and is regulated by a large complex of proteins and functional RNA transcripts. The coding sequence ends at one of three specific stop codons: UAA, UAG, or UGA. The last segment of the gene is the 3′ UTR, which contains a polyadenylation signal and presumably a signal to end transcription, although no transcription stop sequence has been identified. The length of a gene may vary, ranging from less than 1 kb to several hundred kb. The longest gene known, which codes for dystrophin, spans more than 2000 kb of genomic sequence, although this is not the largest protein produced in the cell.
modified in several ways to become functional, especially for mRNA. The first modification to mRNA is the addition of a CAP structure to the 5′ end and is followed by the removal or splicing of introns. The mechanism of mRNA splicing depends on the specific nucleotide sequences at the exon/intron boundaries called splice junctions (Fig. 21-4). The most important of these is the GT-AG rule: Introns almost always start with GT (actually GU, because this occurs in RNA), which is therefore called the splice donor site, and end with AG, which is called the splice acceptor site. Several additional specific sequences are also needed, including sequences within the intron just after the GT splice donor site, at a highly conserved branch site located about 40 bp before the end of the intron and just before the AG splice acceptor site. The splicing mechanism produces the following: (1) cleavage at the 5′ donor site splice junction just before the invariant G, (2) nucleolytic attack by the terminal G of the splice donor site at the invariant A of the branch site to form a “lariat”-shaped structure, and (3) cleavage at the 3′ splice acceptor site at the 3′ splice junction, leading to release of the intronic RNA as a lariat or loop, and splicing of the two exons. These reactions are catalyzed by large complexes composed of snRNA and specific proteins. The snRNAs involved have specific sequences that allow binding with conserved intronic sequences or the recognition sites of other snRNAs. The snRNA–protein–target RNA complexes form large particles known as spliceosomes. Once a 5′ splice site is recognized, the complex scans the RNA sequence until it encounters a branch site, which aids in identifying the nearby 3′ splice acceptor site. This process does not necessarily happen in linear order along the RNA. Rather, the order likely is determined by the vagaries of RNA folding. The last steps involve
Regulatory Regions Many genes have highly conserved sequences either upstream or downstream of the transcribed gene that are involved in regulating expression. These elements seem to be particularly common for genes involved with RNA processing and transcriptional control [Bejerano et al., 2004]. Current understanding of these regions, however, remains limited.
RNA Processing Transcription of DNA gives rise to a precursor RNA that corresponds exactly to the genome sequence but must be
Splice donor site
5'
C A AG GT AGT A G
Exon
Branch site
T C T A C N A C T CG T Intron
Splice acceptor site
CCCCCCCCCCC C G N AG 3' TTTTTTTTTTT T A Exon
FIGURE 21-4. Consensus sequences at the splice-donor, branch, and splice-acceptor sites in introns of higher eukaryotes. The GT at the start of the intron, the A near the end of the branch site, and the AG that ends the intron are essentially invariant, whereas most others represent the majority nucleotide. When two nucleotides are depicted at a single position, no preference is signified regarding which is listed on the top or or on the bottom. A, adenine; C, cytosine; G, guanine; N, any nucleotide; T, thymine. (Modified from Strachan T, Read AP. Human molecular genetics. New York: Wiley-Liss, 1996.)
Dobyns and Das / Introduction to Genetics
cleavage of part of the 3′ UTR, which occurs at a specific point downstream from the end of the coding sequence, and addition of a long sequence of adenosine nucleotides that is called the polyA tail. The site of the polyA tail is specified in part by the sequence AAUAAA, which is located within the 3′ UTR.
Imprinting and X-Inactivation Several regions of the genome are subject to inactivation under special circumstances, with no changes to the DNA sequence. The processes involved thus represent a form of “epigenetic” modification. The two processes reviewed here, imprinting and X chromosome inactivation, both can result in a phenotype when disrupted.
Imprinting The process by which certain genes in specific chromosomal regions are expressed from only one chromosome, depending on the parental origin of the chromosome, is known as “imprinting.” Although the mechanism remains unknown, a key component involves allele-specific DNA methylation, found predominantly at the carbon 5 position of about 80% of all cytosines that are part of symmetrical CpG dinucleotides [Jiang et al., 2004; Strachan and Read, 1999; Weksberg et al., 2003]. This process is controlled by regulatory imprinting “centers” located nearby on the same chromosome as that of the silenced or “imprinted” gene. In effect, then, two alleles of the same gene that are identical in nucleotide sequence but derived from opposite parents are regulated differently in the same nucleus. This process is reversible, so that the silent, imprinted allele can be reactivated and the active allele silenced when passed through the germ line of the opposite-sex parent. Most imprinted genes are found in large clusters of greater than 1 Mb (megabase pairs) in length. Imprinted clusters have been identified in chromosomes 6q24, 7p11.2, 11p15.5, 14q32, 15q11-q13, and 20q13.2, and others may exist as well [Cavaille et al., 2002; Gardner et al., 2000; Hall, 1990; Jiang et al., 2004; Weksberg et al., 2003; Wylie et al., 2000]. Imprinted regions all share several common characteristics including differential DNA methylation, allele-specific RNA transcription, antisense transcripts, histone modifications, and differences in timing of replication.
X-Inactivation In cells with two (or more) X chromosomes, all but one undergo extensive gene silencing by methylation. This phenomenon, known as X chromosome inactivation (Xi), causes one of the two X chromosomes in cells of female mammals to become transcriptionally inactive early in embryonic development [Lyon, 1961, 2002]. In mutant cells with more than two X chromosomes, all but one becomes inactivated. This has the effect of balancing gene dosage of X-linked genes between male and female cells. The process of Xi is random, so that on average the maternally and paternally derived X chromosomes each are inactivated in approximately 50% of cells. Alterations from this pattern are seen in female carriers of some X-linked diseases, resulting in skewing of Xi. This alteration can be favorable, with decreased severity of the phenotype, or unfavorable, with increased severity of the phenotype.
513
CELL CYCLE AND CHROMOSOMAL BASIS OF HEREDITY Current knowledge regarding the chromosomal basis of heredity and that concerning the cell cycle are inextricably linked, because the intracellular structures now known as chromosomes were first seen in cells undergoing cell division. The existence of chromosomes was foreshadowed by some of Gregor Mendel’s work. For years after he described independent sorting of genetic traits, occasional exceptions to Mendel’s law of segregation were discovered. Certain traits were found that were typically inherited as a group. These observations were eventually explained by the discovery of chromosomes. The nuclear material of a cell, or chromatin, appears relatively homogeneous during most of the cell cycle but condenses into a number of distinct rodshaped organelles during cell division. These tiny structures were called chromosomes because they stain darkly with various biologic dyes.
Cell Cycle Humans begin life as a single diploid cell or zygote that gives rise to all of the cells of the body by a combination of cell growth and cell division, with the latter including both asexual (mitosis) and sexual (meiosis) cell division. The life cycle of somatic cells is divided into four stages. After cell division, the cell enters the G1 (gap 1) resting phase, during which DNA synthesis does not occur. Some differentiated cells, such as neurons, stop growth in a modified G1 phase known as G0. Late in G1, the cell passes a critical point after which it proceeds through the rest of the cell cycle at a standard rate. G1 is followed by the S phase, during which DNA synthesis or replication occurs. The genetic material is duplicated in the form of two chromatids (future chromosomes) joined by attachment to a single centromere. The cell then enters the G2 (gap 2) resting phase, which is much shorter than G1. The G1, S, and G2 phases together constitute interphase.
Mitosis Somatic cell division, or mitosis, is an elaborate mechanism that distributes one chromatid of each duplicated chromosome to each of the two daughter cells. The process is continuous but has been divided into the following five stages: prophase, prometaphase, metaphase, anaphase, and telophase (Fig. 21-5). In prophase, the chromatin begins to condense, the nucleolus disappears, and the mitotic spindle begins to form. Prophase is followed by prometaphase, during which the nuclear membrane disappears, allowing the chromosomes to disperse in the cell and attach to the spindle by paired kinetochores located at the centromere. In metaphase, the chromosomes are maximally contracted and arranged at the equatorial plane of the cell. In anaphase, the replicated chromosomes separate at the centromere, allowing the two chromatids to become daughter chromosomes, which move to opposite ends of the cell. In telophase, the chromosomes decondense, the nuclear membrane re-forms, and the nucleus returns to the interphase appearance. Shortly afterward, the cytoplasm divides to form two daughter cells. For routine studies, chromosomes are examined during metaphase. For
514
Genetic, Metabolic, and Neurocutaneous Disorders / 21 FIGURE 21-5. Diagram of mitosis demonstrating two chromosome pairs.
Interphase Prophase
Prometaphase
MITOSIS
Metaphase
Anaphase
Telophase
Interphase
high-resolution studies, they are examined before the point of maximal contraction, during prophase or prometaphase.
Meiosis Reproductive cell division, or meiosis, is an even more complex mechanism in which two successive cell divisions, known as meiosis 1 and meiosis 2, give rise to the haploid germ cells (Fig. 21-6). Meiosis is of critical importance in understanding many of the methods of modern molecular genetics and the pathogenesis of many genetic diseases. In meiosis 1, the chromosome number is reduced from the diploid to the haploid number. The key step consists of close pairing of homologous chromosomes during prophase 1, which is further divided into several stages. During leptotene,
the chromosomes first become visible, with homologs located close together. During zygotene, the homologs begin to pair closely along their entire length, held together by a thin protein-containing structure known as a synaptonemal complex. During pachytene, synapsis or pairing is completed, and the homologs appear as a bivalent. Pachytene is the stage during which exchange of homologous segments between nonsister chromatids occurs, which is known as recombination or crossing over. The remaining steps are similar to mitosis, except that it is the paired homologs that are pulled apart rather than the centromeres. In meiosis 2, which closely resembles mitosis, the chromatids separate at the centromere to form daughter chromosomes. Ova and sperm have remarkably different timing, but the sequence of meiosis is the same.
Dobyns and Das / Introduction to Genetics
515
Interphase Prophase 1 (crossing over) Prometaphase 1
Metaphase 1
Anaphase 1
MEIOSIS
Telophase 1
Metaphase 2
Anaphase 2
Gametes FIGURE 21-6. Diagram of meiosis depicting two chromosome pairs.
Chromosomal Basis of Heredity Chromosome Structure The nuclear DNA is dispersed among 23 or 24 separate linear structures—the chromosomes, each of which consists of a single, uninterrupted double helix that contains 50 to 250 Mb of DNA—and a group of associated proteins that
form the support structure or scaffolding. The scaffolding consists of five basic proteins called histones and several more acidic nonhistone proteins. Two copies of each of four histones—H2A, H2B, H3, and H4—join to form an octamer. The DNA double helix wraps almost twice around the octamer, which involves about 140 bp. Adjacent octamers are separated by a short spacer segment of 20 to 60 bp that
516
Genetic, Metabolic, and Neurocutaneous Disorders / 21
is associated with histone H1. The complex of DNA and core histones is known as a nucleosome (see Fig. 21-2). Strings of nucleosomes are further compacted into a secondary helical structure known as a solenoid. These structures have a diameter of about 30 nm (see Fig. 21-2) and contain six nucleosomes per turn. The solenoids are packed into large loops of 10 to 100 kb of DNA, which are attached to a nonhistone protein scaffolding. These loops pack together loosely to form interphase chromosomes. During early prophase, they pack together more closely to form knoblike thickenings known as chromomeres, which then coalesce further to form the bands observed in prometaphase and metaphase chromosomes when stained with appropriate dyes. The alternating light and dark bands that characterize all nuclear chromosomes with a variety of staining methods likely reflect the compartmentalization of the genome into isochores, defined as large regions with variation in base composition or variable spacing of scaffold attachment regions. The dark bands observed with Giemsa staining are AT rich, replicate late in the DNA synthesis phase of the cell cycle, and contain relatively few genes. The light bands observed with Giemsa are GC rich, replicate early, and contain many genes. Some are greatly enriched for GC and contain high concentrations of genes. Most, although not all, such bands are located near the ends or telomeres of chromosomes and therefore are known as T bands.
Specialized Regions All nuclear chromosomes have specialized regions that are required for chromosome integrity and function, including centromeres, telomeres, and origins of replication. Centromeres are DNA sequences that act in cis. That is, they act on the same chromosome on which they are located and are responsible for the segregation of chromosomes during cell division. Centromeres contain extensive repeats of an approximately 171-bp unit known as alpha-satellite DNA, the sequence of which differs slightly between each chromosome. Fragments of chromosomes that lack a centromere, known as acentric fragments, are lost during cell division. The two ends of a chromosome are called telomeres and also are required for chromosome stability. In humans, they consist of long arrays of tandem repeats of the sequence TTAGGG, which extend about 5 to 20 kb. DNA polymerases are unable to replicate the telomeres because of the lack of a template. This problem is resolved by the enzyme telomerase, which contains an RNA component to serve as a template to prime further synthesis on the leading strand. Further extension of the leading strand provides the needed template for the lagging strand. Origins of replication are specialized sequences where DNA replication begins and thus are important in maintaining chromosome number and integrity. They consist of autonomously replicating sequence (ARS) elements that contain a core consensus sequence and some imperfect copies of the core sequence and extend about 50 bp. A human consensus ARS has been identified [Strachan and Read, 1999]. Regions of variable staining known as heterochromatin consist of long arrays of repeat sequences as short as 5 bp. These regions are located primarily in the pericentromeric regions of chromosomes 1, 9, and 16, and in distal Yq. The
five human acrocentric chromosomes have small satellites attached to the short arm by short stalks or secondary constrictions that contain the rRNA genes.
Chromosome Number Each human somatic cell contains 46 chromosomes that consist of 22 matched pairs known as autosomes and two sex chromosomes: XX in females and XY in males (Fig. 21-7). By contrast, human germ cells contain only 23 chromosomes, consisting of one of each kind of autosome and a single sex chromosome. The former is known as the diploid or 2n number, and the latter is known as the haploid or 1n number. The autosomes are numbered according to length, with chromosome 1 being the longest and chromosome 21 the shortest. Although chromosome 21 is slightly shorter than chromosome 22, the numbers were retained for historical reasons. The two members of each pair of autosomes and the two X chromosomes in females carry the same genes and are known as homologous chromosomes, or homologs. Although they appear similar under the microscope, homologs are not strictly identical. They contain essentially the same genes, but the nucleotide sequence differs at thousands of positions.
Chromosome Identification Individual chromosomes may be seen only when tightly contracted during cell division. Each chromosome consists of two chromatids, which are joined at the primary constriction, or centromere. In standard cytogenetic nomenclature, the centromere divides the chromosome into two arms, designated the p or short arm and the q or long arm. The tip of each arm is the telomere. Human chromosomes are classified into the following three types according to the position of the centromere: (1) metacentric, in which the centromere is centrally placed and the two arms are of about equal length; (2) submetacentric, in which the centromere is off center and the arms are of unequal length; and (3) acrocentric, in which the centromere is near one end.
ORGANIZATION OF THE HUMAN GENOME The human genome comprises the total of all genetic information in the cell. It is divided into two separate compartments—a complex nuclear genome and a much simpler mitochondrial genome. The mitochondrial genome consists of a single circular DNA molecule that is present in many copies in each mitochondrion, and the nuclear genome is distributed among 23 (in females) or 24 (in males) linear structures known as chromosomes. The available data regarding the genome have become much more extensive and accurate with completion of the Human Genome Project. A few of the most useful Human Genome Project–related web sites are listed in Table 21-1.
The Nuclear Genome The human nuclear genome consists of approximately 3 × 109 base pairs (bp), or 3000 Mb of DNA. About 75% of this represents unique or single-copy DNA, which includes genes and some important regulatory elements; the remaining 25% consists of several classes of repetitive DNA
Dobyns and Das / Introduction to Genetics 36.3– 36.2– 36.1– 35– 34.3– 34.2– 34.1– 33– 32–
25– 24– 23– 22– 21– 16– 15– 14– 13– 12– 11.2– 11.1– 11.1– 11.2– 12– 13– 14.1– 14.2– 14.3– 21–
31– 22– 21– 13– 12– 11– 11– 12– 21– 22– 23– 24– 25–
22–
31–
32–
26– 25– 24– 23– 22–
14– 13–
33– 34– 35– 36–
41– 42– 43– 44–
37–
1 25– 24– 23– 22–
2
13– 12– 11– 11.1– 11.2– 12– 13–
21– 22– 23– 24– 25– 26– 27–
21– 22– 23– 24– 25– 26.1– 26.2– 26.3– 27– 28– 29–
31–
15.3– 15.2– 15.1– 14–
13–
12– 11.1– 11.1– 11.2– 12– 13.1– 13.2– 13.3–
24–
32–
16– 15.3– 15.2– 15.1– 14– 13– 12– 11– 11– 12–
21–
23–
517
14– 15– 21– 22–
28–
23–
31.1– 31.2– 31.3– 32– 33– 34– 35–
31–
3
32– 33– 34– 35–
4
5
22– 21–
21.3– 21.2– 21.1– 12– 11.2– 11.1– 11– 12– 13– 14– 15– 16–
23– 22– 21– 12– 11.2– 11.1– 11.1– 11.2– 12– 13–
11.2– 11.1– 11.1– 11.2– 21–
21–
22–
21.1– 21.2– 21.3–
31–
22–
32– 33– 34– 35– 36–
23–
22– 23– 24– 25– 26– 27–
6 13– 12– 11.2– 11.1– 11– 12– 13– 14–
13– 12– 11.2– 11.1– 11.1– 11.2– 12– 13–
22– 31– 32– 33– 34–
32–
13 13.3– 13.2– 13.1– 12– 11– 11– 12– 13.1– 13.2– 13.3– 13.4–
14 13– 12– 11.2– 11.1– 11.1– 11.2– 12– 13.1– 13.2– 13.3–
19
20
11.2– 11.1– 11.1– 11.2–
13–
21–
15–
14– 21– 22–
23– 24– 25–
23–
34–
26–
24– 25–
9
13.3– 13.2– 13.1– 12– 11.2– 11.1– 11.1– 11.2– 12.1– 12.2– 13– 21– 22– 23– 24–
15
14– 15–
13–
31– 32– 33–
8
13– 12– 11.2– 11.1– 11– 12– 13–
14– 13– 12– 11.2– 11.1– 11– 12–
22–
22– 23– 24– 25– 26–
31–
13– 12– 11– 11– 12–
22–
13– 12– 11.2– 11.1– 11.1– 11.2– 12– 13– 14– 15– 21–
21– 22– 23– 24–
21–
15– 14– 13– 12–
21–
24.1– 24.2– 24.3–
7
24– 23– 22– 21–
10
13– 12– 11.2– 11.1– 11.1– 11.2– 12– 21–
13– 12– 11.2– 11.1– 11.1– 11.2– 12–
22–
13–
21
FIGURE 21-7. Standardized diagram or idiogram of human chromosomes at the 400-band stage.
11
21–
21–
22–
11.4– 11.3– 11.2– 11.1– 11– 12– 13–
23–
18
21–
11.3– 11.2– 11.1– 11.1– 11.2–
22– 23– 24– 25– 26– 27– 28–
12–
22
12
22.3– 22.2– 22.1–
12–
17
13– 12– 11.2– 11.1– 11.1– 11.2– 21–
22– 23– 24.1– 24.2– 24.3–
11.3– 11.2– 11.1– 11.1– 11.2–
22– 23– 24– 25–
16
21–
Y
X
518
Genetic, Metabolic, and Neurocutaneous Disorders / 21
[Lander et al., 2001; Nussbaum et al., 2001; Venter et al., 2001].
Genes and Conserved Noncoding DNA Somewhat surprisingly, recent estimates predict that the human genome contains only 30,000 to 40,000 genes, far fewer than earlier estimates, which account for only about 1.2% of nuclear DNA [Lander et al., 2001; Venter et al., 2001]. Another 5% of the human genome is more conserved than would be expected from estimates of neutral evolution, which suggests that many of these regions have specific, regulatory functions [Chiaromonte et al., 2003; Waterston et al., 2002]. Studies of these highly conserved regions of DNA have used different thresholds, such as stretches of more than 100 bp with 70% to 80% conservation between mouse and human. Some of these regions have been found to contain important noncoding elements [Dermitzakis et al., 2002, 2003; Frazer et al., 2004; Hardison, 2000]. More stringent analysis demonstrates that the human genome contains 481 sequences of 200 or more bp that are 100% conserved among human, mouse, and rat [Bejerano et al., 2004]. These segments were designated “ultra-conserved elements” and are preferentially located near genes involved in RNA processing or regulation of transcription and development. Similarly, about 5000 sequences of 100 bp or more are conserved among these three species, which emphasizes that noncoding sequences are common and important.
Repetitive DNA Repetitive DNA in the human genome consists of several classes of DNA whose nucleotide sequence is repeated, either exactly or with minor variations, hundreds to millions of times. Some classes are clustered, whereas others are dispersed throughout the genome. Clustered, repeated sequences constitute 10% to 15% of the genome and are collectively called satellite DNA because of their separation from other DNA on density centrifugation. Satellite DNA consists of head-to-tail or tandem arrayed repeat sequences that can extend for several thousand kb. Dispersed, repeat sequences constitute 6% to 10% of the genome and belong to several different classes. Minisatellite or variable number of tandem repeat (VNTR) sequences are dispersed, intermediatelength (15 to 65 bp) repeats that usually span only several kb. The Alu family of DNA repeats includes about 500,000 related sequences that are each about 300 bp in length and together make up about 3% of the genome. The L1 family of repeats includes about 10,000 related sequences that extend up to 6 kb in length and make up another 3% of the genome. The cytosine-adenine (CA) repeat family includes 50,000 to 100,000 sequences consisting of short tandem repeats of the cytosine-adenine dinucleotide (or guanine-thymine on the complementary strand). Although the origin of these sequences is not known, no functions have been identified, and it appears likely that they simply exploit cellular processes to propagate themselves. Several classes have been useful as polymorphic DNA markers.
Low Copy Repeats Segmental duplications known as low copy repeats (LCRs) are DNA sequences of 10 to 250 kb present in multiple copies with greater than 95% sequence identity that
make up approximately 5% of the human genome [Babcock et al., 2003; Bailey et al., 2002; Cheung et al., 2001; Stankiewicz and Lupski, 2002]. LCRs are dynamic regions of the genome because specific repeats tend to cluster within the same genomic regions, where they mediate unequal nonhomologous recombination events producing segmental deletions and duplications. Several of these have been associated with well-known developmental disorders in humans such as Williams’ syndrome in 7q11.23, Angelman’s syndrome and Prader-Willi syndrome in 15q12, hereditary neuropathy with predisposition to pressure palsies and Charcot-Marie-Tooth neuropathy type 1A in 17p12, SmithMagenis syndrome in 17p11.2, and DiGeorge’s syndrome in 22q11.2 [Babcock et al., 2003].
Polymorphisms A mutation is a permanent change in the DNA of an individual organism, specifically a change in the nucleotide sequence anywhere in the genome [Nussbaum et al., 2001]. Genetic diseases and many cancers are caused by mutations that adversely affect function of one or more genes, although most mutations have little or no effect on gene function and therefore do not change the survival or reproductive fitness of an individual. Some of these persist in the population as morphologic variants known as polymorphisms. Sequence changes that have frequencies of less than 1% are known as rare variants, whereas those with frequencies of 1% or more are known as polymorphisms. By convention, a genetic polymorphism is defined as the occurrence of two or more variants or alleles in a region of DNA where at least two alleles appear with frequencies greater than 1%. Several different classes of polymorphisms occur in the genome, and several methods in molecular biology take advantage of the normal variation between individuals.
Minisatellites One of the most useful classes of polymorphisms in the genome is that of the minisatellite or VNTR DNA sequences. These are intermediate-length (15 to 65 bp) DNA sequences that are repeated one to several dozen times in tandem and usually span several kb in total length. They are highly polymorphic, and their extreme polymorphic nature coupled with the complexity of multilocus minisatellites makes them valuable for DNA fingerprinting applications such as forensic, paternity, and zygosity testing and linkage mapping. They also are inherently unstable and susceptible to mutation at a higher rate than observed for other sequences of DNA.
Microsatellites Microsatellites, also known as satellite DNA or short tandem repeats, are segments of DNA two to five nucleotides in length (dinucleotide, trinucleotide, tetranucleotide, or pentanucleotide repeats) that are scattered throughout the genome in noncoding regions between genes or within genes (in introns). They often are used as markers for linkage analysis because of the naturally occurring high variability in repeat number between individuals. These regions are inherently unstable and susceptible to mutations. The most common class of microsatellites is CA repeats (also called GT repeats), which consist of short tandem repeats
Dobyns and Das / Introduction to Genetics
of the dinucleotide CA on one strand and GT on the complementary strand. They thus take the form (CA)n/(GT)n, with n in the range of 6 to 30 [Weber and May, 1989]. The number of repeats within a (CA)n block varies greatly among different members of a species, producing a set of alleles that always differ in size by multiples of two bases. About 70% of the human population is heterozygous at any given (CA)n repeat locus, making these highly polymorphic. The human genome contains about 50,000 to 100,000 interspersed (CA)n blocks, which is enough to place 1 block every 30 to 60 kb if evenly spaced. For both VNTR and CA repeat sequences, the combination of high frequency in the genome and a high rate of polymorphism has made them very useful for gene mapping studies. Some microsatellite repeats, most often trinucleotide repeats, present within coding regions of genes or, less often, the 5′ or 3′ UTR, can expand to an abnormal length and are the basis of triplet repeat diseases such as Huntington’s disease, spinocerebellar ataxias, and fragile X syndrome.
Single-Nucleotide Polymorphisms Single-nucleotide polymorphisms (SNPs, pronounced “snips”) are DNA sequence variations that occur when a single nucleotide (A, T, C, or G) in the genome sequence is changed. For example, a SNP might change the DNA sequence TCACG to TTACG. The most common sequence change involves replacement of cytosine (C) with thymidine (T), accounting for about two thirds of all SNPs. As with other types of sequence variation, a SNP must occur in at least 1% of the population to be classified as a polymorphism. SNPs occur in both unique-sequence (coding and noncoding) and repetitive DNA and are responsible for about 90% of all human genetic variation. SNPs are found on average approximately every 100 to 300 bases along the entire human genome. Although most SNPs likely have no function, some are known to influence disease predisposition or responses to drugs and thus are proving to be very valuable in studying the causes of common human diseases. The current inventory of known SNPs can be found in the Human SNP database (dbSNP) on the NCBI Entrez web site (see Table 21-1). SNPs can affect restriction enzyme sites in the genome and are the basis of restriction enzyme fragment length polymorphisms (RFLPs). Restriction enzyme sites comprise specific DNA sequences scattered within the genome that are recognized and cleaved by bacterial restriction enzymes/ endonucleases (discussed in more detail later). Depending on the location of restriction enzyme sites, specific DNA fragment lengths are obtained on digestion with restriction endonucleases. The presence of a SNP at one of these restriction enzyme sites will affect cleavage by restriction enzymes, resulting in a different-sized DNA fragment that is the RFLP. RFLPs also can be produced by any change that alters the size of the DNA fragment on which the restriction site is located, such as deletions or duplications. RFLPs are a measure of naturally occurring variations or polymorphisms of normal DNA and are inherited according to mendelian principles. RFLPs have been useful for gene mapping.
519
Mitochondrial Genome Mitochondria are cellular organelles that are primarily responsible for cellular respiration and production of adenosine triphosphate. Each cell contains numerous mitochondria, and each mitochondrion contains many copies of a small 16.5-kb circular chromosome, adding up to thousands per cell. The mitochondrial chromosome contains 37 genes that code for two types of rRNA, 22 types of tRNA, and 13 polypeptides. The two DNA strands differ significantly in base composition, with a heavy strand rich in guanines that codes for 28 genes and a light strand rich in cytosines that codes for 9 genes. It is very densely packed, with 93% comprising coding sequence [Strachan and Read, 1999]. All of the genes coded by the mitochondrial chromosome are expressed only in the mitochondria. The rRNA genes differ in size from those in nuclear DNA. The genetic code by which tRNAs decipher mRNAs differs slightly from nuclear DNA. The 13 polypeptides function as subunits of the mitochondrial oxidative phosphorylation system. The nuclear genome encodes the remaining 80 or more subunits and also encodes all mitochondrial ribosomal proteins and many other essential genes, such as mitochondrial DNA and RNA polymerases.
Human Genome Project The importance of DNA, including both genes and noncoding regions, became increasingly apparent during the 1970s and 1980s, leading to one of the most ambitious scientific research projects ever undertaken—a plan to sequence the entire human genome. This project, which was begun in 1990, came to be known as the Human Genome Project. The goals of the project, as taken from the Human Genome Project web site (see Table 21-1), were as follows: • To identify all of the approximately 20,000 to 25,000 genes in human DNA • To determine the sequences of the 3 billion chemical bp that make up human DNA • To store this information in databases • To improve tools for data analysis • To transfer related technologies to the private sector • To address the ethical, legal, and social issues (ELSIs) that may arise from the project The successful completion of the Human Genome Project has had the effect of changing genetic research from “bottom up” to “top down” research. That is, a major goal of research before completion of the Human Genome Project was to determine the nucleotide sequence of genes associated with the disease under study. Following completion of the project, research now typically begins with the nucleotide sequence. Although the Human Genome Project has been officially completed, numerous difficult regions of duplicated DNA remain to be sequenced correctly, and data analysis of the entire project is ongoing. The latter will certainly continue for many years. The effects of the Human Genome Project, however, have been enormous. Research projects that once required several years now can be done in several weeks or months.
520
Genetic, Metabolic, and Neurocutaneous Disorders / 21
TECHNOLOGY OF CYTOGENETICS The modern field of cytogenetics began when methods for arresting cells during mitosis were developed, when chromosomes were contracted and could be visualized under the microscope with various stains. The human diploid chromosome number of 46 was discovered, and many different defects in chromosome number and structure were found, such as Down syndrome. The field has expanded with development of new computerized image recognition systems for chromosome identification and a variety of methods that make use of molecular genetics methodologies. Thus, the distinction between cytogenetics and molecular genetics has become blurred. In general, cytogenetics tests examine large regions of the genome, such as chromosomes or regions of chromosomes, whereas standard molecular genetics methods focus on much smaller regions of the genome, from single nucleotides to genes and gene regions.
Chromosome Analysis When methods for examining chromosomes under the microscope were first developed, individual chromosomes could not be identified because of solid staining. Instead, they were separated into seven groups (A to G) based on their length and centromere position. It is now possible to individually identify all 24 human chromosomes using several different staining techniques that take advantage of differences in chromatin structure and composition to produce a recognizable pattern of bands, as diagrammed in Figure 21-7. These methods are now used to examine the entire chromosome complement of an individual patient, which is known as the karyotype. The same term is used to describe the normal chromosome complement of a species. The three most commonly used staining methods are G-banding, R-banding, and Q-banding. For G-banding, the chromosomes are treated with trypsin and then Giemsa stain to produce the alternating light and dark bands known as G bands. For R-banding, the chromosomes are pretreated with heat and then stained with Giemsa. The resulting R bands are the exact reverse of those produced by G-banding. For Q-banding, the chromosomes are stained with quinacrine mustard and examined under fluorescent light. A specific pattern of bright and dim Q bands is seen, with the bright Q bands corresponding to the dark G bands. For standard chromosome analysis, cell division is arrested in metaphase, when 400 to 550 bands per haploid set can be seen. Analysis should be performed on cells with at least 550-band resolution. For high-resolution chromosome analysis, cell division is arrested in prophase before full contraction has occurred, when 550 to 850 bands per haploid set can be seen. This technique is labor intensive but may be useful for finding very small chromosome rearrangements. A uniform system of human chromosome classification and nomenclature was developed at a series of international conferences and most recently was revised in 1995 [ISCN, 1995]. In this system, chromosomes are separated into regions and subregions based on the banding pattern. For example, band 17p13.3 (read as “17-p-one-three-pointthree”) is found near the telomere of the short arm of chromosome 17.
During the past decade, computer image analysis systems have been developed that can locate chromosome spreads on the slide, recognize and automatically sort chromosomes, and help with analysis. Review by trained cytogenetic technicians is still required, however.
Fluorescence In Situ Hybridization Fluorescence in situ hybridization (FISH) is a technique used to detect specific chromosomes or chromosomal regions through hybridization (attachment) of fluorescently labeled DNA probes to denatured chromosomal DNA. Examination under fluorescent lighting detects the presence or absence of the hybridized fluorescent signal (and hence presence or absence of the chromosome material). This study usually is performed on metaphase chromosomes (Fig. 21-8) but also can be used on cells in interphase. Interphase FISH often is used for rapid detection of specific types of aneuploidy in fetal cells and for detection of certain deletions, duplications, and other abnormalities in tumor cells. In contrast with metaphase FISH, interphase FISH does not permit visualization of the actual chromosomes, so that most types of structural rearrangements cannot be detected. FISH can be used to examine a small set of chromosomal regions at once, usually 1 or 2, although study of 8 to 10 is possible
FIGURE 21-8. Fluorescence in situ hybridization (FISH) of a standard metaphase spread using a set of three overlapping cosmids at D17S379. The top arrow points to two D17S379 probe signals on the two chromatids of one chromosome 17 homolog. The bottom arrow points to the tip of the other chromosome 17 homolog, which lacks the normal signal and is thus deleted for this probe. The chromosome 17 centromeres are marked by a larger signal just below (top) or above (bottom) the arrows. Different colors are used for the D17S379 and 17 centromere probes so that they can be differentiated easily under the microscope. (Courtesy of David H. Ledbetter, Emory University, Atlanta, GA.)
Dobyns and Das / Introduction to Genetics
with special fluorescent markers. Telomere-specific FISH analysis is an example of hybridization with multiple probes simultaneously. Telomere-specific probes that correspond to the telomeres of all of the chromosomes are hybridized to metaphase chromosomes in groups and used to detect abnormalities at the ends of chromosomes that are not visible by routine chromosome analysis.
Comparative Genomic Hybridization Comparative genomic hybridization (CGH) is a molecular cytogenetics method developed to detect changes in copy number between two genomes, typically those of a control and an experimental subject. The alterations are classified as DNA gains and losses and reveal a characteristic pattern that includes mutations at chromosomal and subchromosomal levels. Equal amounts of DNA from two different sources (control and experimental) are labeled with two different fluorescent labels and hybridized to normal metaphase chromosome spreads. For example, control DNA may be labeled with red, and experimental subject DNA with green. When the control and the subject samples both contain a DNA fragment of interest, both labels are seen; this produces yellow fluorescence on the metaphase chromosome spread. When a given DNA fragment is deleted in the experimental subject, only the red control label is seen. When a given DNA fragment is duplicated in the subject, only the green subject label is seen. Array formats for CGH have been developed that have increased the resolution of this technique for detecting smaller deletions and duplications. Instead of hybridizing onto metaphase chromosome spreads, a set of DNA probes across the entire genome is used. The probes are placed on microarrays that can detect DNA fragments with the same sequence as for the probe. Several different methods have been developed using different probes such as bacterial artificial chromosome (BAC) DNA, complementary DNA (cDNA), or DNA fragments produced by cleavage of genomic DNA by the restriction enzyme BglII [Ishkanian et al., 2004; Lucito et al., 2003; Sebat et al., 2004]. These offer different resolution, with probes every approximately 15 to 100 kb. CGH technology has numerous advantages over FISH, including coverage of the entire genome, finer resolution, and lower cost per probe tested. Thus, clinical tests based on CGH technology are likely to replace FISH technology during the next few years.
TECHNOLOGY OF MOLECULAR GENETICS Molecular genetics is that branch of genetics concerned with the structure and function of genes at the molecular DNA level. The rapid gains in this field during the past decade have resulted from discovery of several new techniques that have made detailed analysis of both normal and abnormal genes possible. These discoveries have in turn led to better understanding of many important biologic processes, as well as the molecular basis for many genetic diseases. Several of these methods have proved to be of particular importance and are commonly used in research studies. Some familiarity with these procedures is helpful in understanding the nature and significance of new discoveries in this area.
521
This section presents a brief introduction to some of the more important procedures. More detailed information can be found in several laboratory manuals, especially Current Protocols in Human Genetics [Dracopoli et al., 1997].
DNA Clones A vector is a DNA molecule that can replicate itself in a host cell, such as a bacterium or yeast. Integration of DNA fragments into the vector with restriction endonucleases and DNA ligase results in propagation of the DNA fragment along with the vector, producing large quantities of the fragment of interest. Vectors with inserted recombinant DNA fragments of interest are known as clones, and the methods used to generate them are collectively known as cloning. Clones are chosen at random from clone libraries, which are large collections of clones originating from a specific source, such as the total genomic DNA or chromosome-specific DNA of a human or other organism. Several common types of vectors have been used including phage (bacterial virus) (up to 20-kb insert DNA), plasmids (accessory circular bacterial chromosomes, used to clone several kb of DNA), cosmids (approximately 35 to 45 kb), BACs (approximately 100 to 150 kb) and PACs (P1 plasmid artificial chromosomes) (approximately 100 to 150 kb), and YACs (yeast artificial chromosomes) (up to 1000 kb). The most commonly used at present are BACs and PACs [Stein, 1997], which have proved to be useful for FISH, CGH, and many other technologies. Creation of chromosome-specific DNA libraries by cloning followed by mapping and sequencing is the basis of the information obtained through the efforts of the Human Genome Project.
Restriction Enzymes Restriction enzymes or endonucleases are bacterial enzymes that recognize short, double-stranded DNA sequences and cut the DNA molecule at or near the recognition site [Lewin, 2003]. When a mutation occurs that changes as few as one of the base pairs in the sequence, it is no longer recognized and cut by the enzyme. Several hundred restriction endonucleases have been isolated. Most of the recognition sites are palindromes, which means that they read the same in the 5′ to 3′ direction on both strands, and most of the enzymes leave short overhangs of singlestranded DNA that are known as sticky ends. For example, the enzyme BamHI recognizes the sequence GGATCC and cuts it between the two G bases, leaving the following fourbase overhang: 5′–GGATCC–3′ → 5′–G 3′–CCTAGG–5′ → 3′–CCTAG
GATCC–3′ G–5′
Restriction endonucleases have several important uses in molecular biology. First, they are used to cut or “digest” large DNA molecules into a reproducible collection of a million or more smaller and more manageable DNA fragments that can be identified on the basis of their size. Second, a mutation at any of the recognition sites that changes the sequence or a mutation elsewhere that creates a new recognition site can potentially be detected. Finally, DNA molecules cut with the same restriction endonuclease all have the same sticky ends and may be joined using the enzyme DNA ligase. This condition allows specific DNA sequences of interest to be inserted into vectors and
522
Genetic, Metabolic, and Neurocutaneous Disorders / 21
introduced into cells such as the bacterium Escherichia coli or the yeast Saccharomyces cerevisiae (common bakers’ yeast), which then can be propagated to produce large amounts of the sequence of interest. DNA sequences inserted into a vector are known as recombinant DNA. This is the basis of DNA cloning.
Polymerase Chain Reaction The polymerase chain reaction (PCR) technique has revolutionized the field of molecular genetics. It is a simple but elegant method to amplify a small amount of DNA greater than a million-fold within a matter of hours. PCR results in the enrichment and amplification of a particular DNA region of interest from the total genome, making it more amenable to study, without the use of cloning or Southern blots (described later on). The region of DNA with known base sequence to be amplified, such as part of a gene, is selected, and two short DNA sequences flanking the region of interest are synthesized to serve as primers for amplification. To construct the primers, a short sequence of about 20 to 25 bp just upstream or 5′ of the target sequence on the DNA “sense” strand is chosen as a starting site, and an oligonucleotide (or primer) that is complementary to this short upstream sequence is synthesized. Another short sequence upstream or 5′ of the target sequence on the complementary (or “antisense”) strand also is chosen, and a
Cycle 1
5'
3'
5'
3' Denature
3'
5'
5'
3'
Anneal primer and extend
3'
5'
5'
3'
Cycle 2
Denature 3'
5'
3'
5'
5'
3'
5'
3'
3'
5' 3' Anneal primer and extend
5'
5'
3'
3'
5'
FIGURE 21-9. The polymerase chain reaction. Depiction of the cycling process of denaturation, annealing, and extension that results in the exponential amplification of DNA.
second complementary oligonucleotide is synthesized. The two primers thus flank the region of interest on opposite strands. The DNA is denatured to separate the strands, after which the oligonucleotides are hybridized to the complementary sequences. The short oligonucleotides then serve as primers for synthesis of a complete complementary DNA strand with appropriate deoxynucleotide triphosphate molecules (adenosine, cytosine, guanosine, and thymidine triphosphate [dATP, dCTP, dGTP, and dTTP]) being added, and is mediated by the enzyme DNA polymerase. Because both strands are copied, one round of amplification results in a complete second copy of the original target sequence. Repeated cycles of heat denaturation, hybridization of the primers, and DNA synthesis result in the exponential amplification of the target sequence. Within a few hours, more than a million copies of the sequence may be made (Fig. 21-9).
Methods of General Mutation Detection DNA Sequence Analysis DNA sequence analysis is the most sensitive and direct method for mutation detection. The most widely used method of DNA sequencing is the Sanger method, also known as dideoxy sequencing or chain termination. It is based on the use of synthetic nucleotide analogs—2,3-dideoxynucleoside triphosphates (ddNTPs). Dideoxy NTPs differ from nucleotides found in DNA in that they lack the 3′-hydroxyl group and, when integrated into a sequence, prevent the addition of further nucleotides. Because a phosphodiester bond cannot form between a dideoxynucleotide and the next incoming nucleotide, the DNA chain is terminated. DNA sequencing most commonly is performed by the method of cycle sequencing, in which the DNA region to be sequenced (which is first generated by PCR) is denatured and a short oligonucleotide is annealed to one of the template strands. DNA synthesis occurs in the presence of DNA polymerase, ddNTPs and nucleotides and starts from the 3′ end of the annealed oligonucleotide. As the DNA is synthesized, nucleotides are added onto the growing chain by the DNA polymerase; however, on occasion, a ddNTP is incorporated into the chain in place of a normal nucleotide, resulting in a chain-terminating event. At the end of the sequencing reaction multiple DNA molecules are present at such that at each nucleotide position, a proportion of molecules are terminated owing to the incorporation of a ddNTP. These products are separated by size on capillary or polyacrylamide gel electrophoresis systems, and the fluorescently labeled ddNTPs are detected. Each ddNTP is labeled with a different fluorophore. Shorter DNA molecules migrate faster than longer molecules on electrophoresis, and by analyzing the different fluorescent signal of all of the different-sized molecules, the DNA sequence can be determined. For example, ddCTP is labeled with a blue fluorophore. Everywhere a G residue exists in the template DNA, either a dCTP or a ddCTP will be incorporated into the synthesized strand. For every G residue in the template DNA, a proportion of molecules with a ddCTP at that site will be present. Each of these molecules will be of a different size, depending on where a G residue resides in the sequence, and will be distinguished by electrophoresis. The same applies for the other ddNTPs.
Dobyns and Das / Introduction to Genetics
Specialized DNA sequencing software exist that can convert the different fluorescent signal to different-color peaks that constitute a DNA sequence chromatogram.
Mutation Scanning Mutation scanning refers to methods used to determine the presence of a sequence change in a region of DNA (such as an exon of a gene). These methods need to be followed up by DNA sequencing, however, to determine the exact nature of the sequence change. Mutation scanning generally is less labor intensive, faster, and more cost-effective to perform than DNA sequencing and may be the method of choice when a large gene needs to be analyzed for the presence of mutations. The exons of the entire gene are subjected to mutation scanning, and only those exons that demonstrate the presence of a sequence change need to be sequenced to determine the precise nature of the sequence change. Various methods of mutation scanning exist that differ in their sensitivities of mutation detection [Cotton, 1997; Eng and Vijg, 1997; Grompe, 1993]. The general basis of most mutation scanning methods is the abnormal migration of a DNA fragment that contains a sequence change from a normal “wild-type” sequence. All are PCR-based methods—the DNA region to be studied is amplified by PCR before the different mutation scanning methods are performed. Single-Stranded Conformational Polymorphism. With the single-stranded conformational polymorphism (SSCP) technique, DNA fragments are denatured and made singlestranded. The single-stranded DNA takes on a specific conformation, depending on its sequence. A change in the DNA sequence will result in a change in the single-stranded conformation structure. Denatured fragments are separated on polyacrylamide gels under a series of differing conditions, and fragments with different conformation structures will migrate differently and can be detected. This method has an approximate sensitivity of 80% for detecting DNA sequence changes. Denaturing Gradient Gel Electrophoresis. With denaturing gradient gel electrophoresis (DGGE), DNA fragments are denatured and allowed to reanneal slowly. In the absence of a sequence change, the only DNA molecules that will be formed are homoduplexes (i.e., with no mismatch of DNA sequence between the complementary strands). In the presence of a sequence change, molecules representing both homoduplexes and heteroduplexes (i.e., a normalsense strand binds to a mutant antisense strand, or vice versa, to create a mismatch of DNA sequence at the position of the mutation) will be formed. These products are allowed to migrate on a polyacrylamide gel with an increasing gradient, and at a particular gradient, the structure of the heteroduplex molecules changes significantly and affects its migration, compared with that of the homoduplex molecules. For this technique it is important to have specialized GC clamps at the ends of the DNA fragment that enhance the difference between the heteroduplex and homoduplex molecules, and these are included in the PCR primers used to generate the DNA fragment. This method has a high sensitivity, approximately 98% to 100%. Denaturing High-Performance Liquid Chromatography. Denaturing high-performance liquid chromatography (DHPLC) also is based on the separation of DNA homoduplex from heteroduplex molecules. The
523
medium of separation is a column composed of a polystyrenedivinylbenzene copolymer to which DNA binds and gets released through interaction with specific buffers. At increased temperatures, heteroduplex molecules get released from the column faster than do homoduplex molecules and therefore can be detected. This method does not require the sophisticated GC clamps of DGGE and has a high sensitivity, close to 100%. Protein Truncation Test. As the name suggests, the protein truncation test (PTT) is used for the detection of mutations that result in a protein truncation, such as a frameshift or nonsense mutation. The starting material is generally RNA that is converted to cDNA by reverse transcription PCR. In vitro transcription and translation are performed, and the protein products are labeled and separated by sodium dodecyl sulfate (SDS) polyacrylamide gel electrophoresis. A DNA fragment that contains a truncation mutation will result in a protein product that will be shorter in length than a normal product and therefore can be detected. This technique will not detect mutations that do not result in protein truncation, such as missense mutations.
Southern Blot Analysis Southern blot analysis, named after its inventor, E.M. Southern, has been used extensively for DNA analysis, particularly for the detection of DNA abnormalities. With the advent of PCR techniques, the use of this analytic method is decreasing. It still remains useful, however, for the detection of large deletions or duplications that affect a part or the whole of a gene. Genomic DNA is digested with a restriction enzyme, which results in the production of different-sized DNA fragments that are separated on an agarose gel by electrophoresis. The separated DNA fragments are made singlestranded by treatment with an acid and then transferred and fixed onto a nylon membrane. The single-stranded fixed DNA is hybridized with a radioactively labeled probe specific for a certain gene. A probe can be a cloned fragment of a gene or a PCR product of a gene. The probe will hybridize to that region of the DNA where it finds its complementary sequence. Excess probe is washed off, and the nylon membrane is exposed to an x-ray film to reveal where the probe has bonded. When a large deletion, duplication, or other form of DNA rearrangement occurs, either deletion or creation of restriction enzyme sites can result. Using a probe that binds to the deleted, duplicated, or rearranged area will reveal a different pattern of hybridization based on what restriction enzymes have been affected. The presence of a different hybridization pattern compared with a normal control is indicative of a change in the DNA structure.
Methods for Detecting Specific Sequence Changes (Genotyping) Different methods exist for the detection of specific mutations in genes, especially point mutations or insertions and deletions of a few bp. These methods are useful for the detection of the common mutations present in diseases such as sickle cell anemia, cystic fibrosis, and hereditary hemochromatosis. These techniques are possible only when the base sequence and precise point mutation responsible for the disease phenotype are known.
524
Genetic, Metabolic, and Neurocutaneous Disorders / 21
Allele-Specific Oligonucleotide Hybridization For allele-specific oligonucleotide (ASO) hybridization, separate ASO probes complementary to either the normal or a specific mutant allele are synthesized. The probes consist of the point mutation or its normal counterpart and 9 to 12 base pairs flanking it on either side, for a total length of 19 to 25 base pairs. The probes then are hybridized to the DNA source under stringent conditions. Because the probes are short, they are highly sensitive to sequence changes at even a single nucleotide. A probe complementary to the normal allele will hybridize to the normal allele but not to the mutant allele, and vice versa. Thus, DNA from a person homozygous for the normal gene will hybridize to the ASO probe complementary to the normal DNA sequence but not to the probe complementary to the point mutation. DNA from persons homozygous for the mutation will hybridize to the ASO probe complementary to the mutation but not to the normal probe. Only DNA from heterozygotes will hybridize to both probes. It is important to remember that DNA from persons who are heterozygous for different mutations in the same gene—compound heterozygotes—also will hybridize to the normal probe. Several different formats have been developed to detect ASO probes ranging from radioactivity to chemiluminescence to fluorescence and can be performed in both solid and liquid phases.
Single-Base Extension Oligonucleotide primers of approximately 20 bp are designed to hybridize just upstream or downstream of the nucleotide to be genotyped, and an extension reaction— more specifically, a single-base extension (SBE) reaction— is performed in the presence of ddNTPs. In the case of a normal sequence, a ddNTP corresponding to the complementary normal nucleotide is added to the primer; in the case of a mutation, a ddNTP corresponding to the complementary mutant nucleotide is added to the primer. The ddNTPs generally are labeled with different fluorochromes, allowing their detection. In a person homozygous for a normal gene, extension will occur only with the ddNTP corresponding to the normal allele, whereas in a person homozygous for a mutated gene, extension will occur only with the ddNTP corresponding to the mutated allele. A heterozygous person will have both normal and mutated extension products. Several different formats have been developed to detect SBE products and can be performed in both solid and liquid phases.
DNA Arrays In DNA arrays, hundreds to thousands of DNA targets are arranged (arrayed) on a solid medium such as a glass slide or microchip. DNA arrays are of two main types—genotyping arrays and sequencing arrays. Genotyping arrays consist of hundreds to thousands of different ASO probes or SBE primers arrayed on a chip that allows the genotyping of a large number of different loci simultaneously. DNA sequencing arrays consist of a series of hundreds of thousands of approximately 20-bp oligonucleotides, spanning the length of a gene, that are arranged in a tiling fashion. For each nucleotide to be sequenced, four oligonucleotides are present that differ only at the central position and have an A, C, G, or T. Digested DNA is fluorescently labeled and hybridized to the tiled oligonucleotide chip under stringent con-
ditions. DNA hybridizes to those oligonucleotides that correspond to the correct sequence and the fluorescent signal read from which the DNA sequence is deciphered. DNA sequencing and genotyping arrays are available for several genes and are still largely used for research, although some clinical applications have been initiated. Expression arrays are different and refer to cDNA arrays to which RNA is hybridized and are used to determine the expression profile of hundreds of genes simultaneously. This technique is currently used only in the research setting.
Restriction Enzyme Analysis Some mutations result in the destruction or creation of a restriction enzyme site in the DNA sequence. PCR amplification of the region of interest, followed by digestion of the genomic DNA with the appropriate restriction enzyme and gel electrophoresis, can be performed to determine the presence or absence of a mutation that affects a restriction enzyme site. Destruction or creation of a restriction enzyme site will result in a different-sized DNA fragment compared with a normal control fragment. The sickle cell anemia mutation and the hereditary hemochromatosis mutation both affect restriction enzyme sites.
DNA Methylation Analysis DNA methylation analysis can be performed for the detection of abnormalities in imprinted genes. Of the two alleles of an imprinted gene, one allele is methylated at the promoter (silenced allele), and the other is unmethylated (expressed). Any aberration that affects the imprinting status (e.g., deletion or uniparental disomy) will affect the methylation pattern. Methylation can be assayed with the use of methylationsensitive restriction enzymes followed by Southern blot analysis or by methylation-specific PCR techniques. For methylation-specific PCR assays, genomic DNA is treated with the chemical sodium bisulfite that converts all cytosine molecules to thymidine, except if methylated. The methylated cytosine molecules are left unchanged. As a result, a methylated sequence will be changed in its nucleotide content, as compared with an unmethylated sequence after bisulfite treatment, and can be distinguished by the use of specific PCR primers. Genes subject to X-inactivation also are methylated and can be detected using the same method.
CLINICAL CYTOGENETICS Chromosome abnormalities may involve either the number or the structure of chromosomes. The former are considered genome mutations and the latter, chromosome mutations. The mechanisms involved in the two major types of mutations are quite different, but both may result in loss or gain of DNA in the nucleus. Both types may involve all of the cells of an organism or only a proportion. When only a proportion of cells are involved, the abnormality is termed mosaic, discussed in detail later in this section.
Abnormalities of Chromosome Number For germ and somatic cells, the normal chromosome complement consists of the haploid and the diploid number,
Dobyns and Das / Introduction to Genetics
Aneuploidy Aneuploidy is defined as any chromosome complement that deviates from a multiple of the haploid number. In most cases, it consists of either monosomy, which is defined as loss of an entire chromosome, or trisomy, which refers to gain of an entire chromosome. Aneuploidy is the most common and clinically significant type of chromosome disorder, occurring in 3% to 4% of all recognized pregnancies. Both monosomy and trisomy of autosomes are lethal during early pregnancy in a large majority of affected fetuses. Autosomal monosomy is uniformly lethal except for a few reports of liveborn children with monosomy 21. Monosomy X is prenatally lethal in most affected fetuses, but many survive and will have the phenotype of Turner’s syndrome. The effects of trisomy vary depending on the chromosome involved. Trisomy 16 is the most frequent autosomal trisomy at conception but is uniformly lethal before birth. The most common type of trisomy in liveborn infants is trisomy 21, which is the chromosome abnormality observed in 95% of children with Down syndrome. The only other autosomal trisomies observed at appreciable frequencies are trisomy 13 and trisomy 18, although trisomy 8 may be observed in mosaic form. The most common mechanism is nondisjunction, which is the failure of a pair of chromosomes to separate correctly during one of the two stages of meiosis, usually meiosis 1. The consequences of nondisjunction during meiosis 1 and 2 are somewhat different. If the error occurs during meiosis 1, the unbalanced gamete with 24 chromosomes contains both the maternal and the paternal members of the pair. If the error occurs during meiosis 2, the unbalanced gamete will contain either the maternally or the paternally derived chromosome but not both.
Mechanisms Some progress has been made recently in current understanding of the mechanisms causing or at least predisposing to structural chromosome rearrangements. Many appear to occur randomly, with no evidence of recurrent breakpoints. For example, no consistent breakpoints have been found for the interstitial deletions and reciprocal translocations involving chromosome band 17p13.3 [Cardoso et al., 2003]. In many other locations, the small duplicated regions known as LCRs can mediate several different types of rearrangements. These were first identified as the cause of common deletion or microdeletion syndromes, such as deletion (del) 2q13 with juvenile nephronophthisis and Joubert’s syndrome–related disorder [Parisi et al., 2004; Saunier et al., 2000], 7q11.23 in Williams’ syndrome [Osborne et al., 2001; Urban et al., 1996], del 15q11.2-q13
Site of crossover
Normal
Occasionally, fetuses with three or four times the normal haploid number of chromosomes have been observed. These abnormal chromosome complements are called triploidy (3n) and tetraploidy (4n). The few children who are liveborn survive only briefly after birth, unless the abnormality is mosaic (i.e., involves only a proportion of their cells). Failure of a maturational division in either egg or sperm results in triploidy, whereas failure of completion of an early division of the zygote causes tetraploidy.
Del Dup
Triploidy and Tetraploidy
gain of DNA sequence. The phenotypic effects often are severe. The chromosomes involved in the reconfiguration are known as derivative chromosomes. Many different types of rearrangements have been reported, as described in the following sections. Only those derivative chromosomes that contain a functioning centromere and telomeres, however, are stable and capable of being transmitted unaltered to daughter cells during mitosis or meiosis. Derivatives lacking a centromere or telomere are unstable and are lost during cell division. Some regions of the genome, such as 8p, contain a noncentromeric sequence that is sufficiently similar to function as a “neocentromere” during cell division [Giglio et al., 2001].
Normal
respectively. Any deviation from these numbers is associated with significant abnormalities. The most common types result from abnormal segregation of chromosomes in germ cells; epidemiologic studies have estimated a rate of abnormal segregation of approximately 1 per 25 to 50 meiotic cell divisions.
525
Abnormalities of Chromosome Structure Structural chromosome rearrangements consist of loss, gain, or altered position of segments of chromosomes, and many different types have been recognized. The estimated frequency is about 1 per 1700 cell divisions, making them much less frequent than aneuploidy. Rearrangements are termed balanced if the chromosome complement has a normal amount of genetic information, regardless of its location. They are termed unbalanced if there has been either loss or
FIGURE 21-10. Drawing of a recombination event between homologs resulting from mispaired low copy repeats (LCRs) during meiosis 1. On the left side of the drawing, the far right and far left chromatids have paired correctly, and the middle two chromatids have paired incorrectly. A crossover within the mispaired region results in one daughter chromosome with a duplication and another with a deletion (depicted on the right side of the drawing). The dark squares represent the LCRs.
526
Genetic, Metabolic, and Neurocutaneous Disorders / 21
in Angelman’s syndrome and Prader-Willi syndrome [AmosLandgraf et al., 1999], del17p12 in hereditary neuropathy with predisposition to pressure palsies [Chance et al., 1994], del17p11.2 in Smith-Magenis syndrome [Chen et al., 1997], and del22q11.2 in DiGeorge’s syndrome/ velocardiofacial syndrome [McDermid and Morrow, 2002]. The same LCRs are associated with duplications of the same regions, including duplication 15q11.2-q13 [Mohandas et al., 1999], 17p12 [Pentao et al., 1992], and 17p11.2 [Potocki et al., 2000]. A simple diagram of this mechanism is shown in Figure 21-10. Many of the LCRs are inverted with respect to each other, which can lead to very complex combinations of deletions and duplications. This can occur for LCRs on the same chromosome, as seen with Williams’ syndrome and some X chromosome rearrangements [Giglio et al., 2000; Osborne et al., 2001], or between homologous chromosomes. The latter appears to be more common when two matching LCRs on homologous chromosomes are inverted with respect to each other, a novel type of polymorphism [Giglio et al., 2001]. Similar mechanisms also can predispose to structural rearrangements between completely different chromosomes involving either an LCR or a gene cluster such as olfactory receptor clusters [Giglio et al., 2002; Spiteri et al., 2003].
Balanced and Unbalanced Chromosomal Rearrangements As noted previously, structural chromosome rearrangements that result in no net loss or gain of genomic sequence are balanced, whereas those that do result in a net loss or gain of material are unbalanced. Persons with balanced rearrangements usually are normal, unless one of the chromosomal breaks disrupts an important gene. More recent studies, however, have found that chromosome rearrangements that appear balanced often have submicroscopic loss or gain of material and so are actually unbalanced [Astbury et al., 2004b], and some chromosome rearrangements are more complex than standard chromosome analysis suggests [Astbury et al., 2004a]. A
Specific Types of Chromosome Rearrangements The most common structural rearrangements include terminal and interstitial deletions and duplications, reciprocal and robertsonian translocations, inversions, and rings. Examples of most of these are shown in Figure 21-11.
Deletions and Duplications A deletion consists of loss or gain of a chromosome segment. Deletions may be either interstitial or terminal, with terminal deletions including the telomere (see Figs. 21-8 and 21-11D), whereas most duplications are interstitial. Most interstitial deletions and duplications result from unequal crossing over in LCRs (see Fig. 21-10). Terminal deletions are more likely to result from simple chromosome breakage, although some apparently terminal deletions prove to be interstitial deletions in which one breakpoint happens to be close to the telomere. Any carrier of a deletion is hemizygous for the information on the corresponding segment of the normal homolog. Thus, small but cytogenetically visible deletions involving critical genes occasionally produce single-gene phenotypes such as lissencephaly or retinoblastoma. Duplicated segments usually are adjacent to each other and may be in the same orientation (direct dup), or inverted (inverted dup) with respect to one another. In general, the phenotypic effects of duplications are less severe than the effects of deletion of a similar segment. Small duplications also can result in single-gene phenotypes such as CharcotMarie-Tooth neuropathy [Chance et al., 1994], although this is recognized less often than with deletions.
Inversions Inversions are segments within a chromosome that are inverted with respect to the normal orientation and result from crossovers within existing duplicated segments (LCRs) or from two breaks within a single chromosome, followed by
B
C
D
E
FIGURE 21-11. Partial karyotypes of structural chromosome rearrangements. A, Pericentric inversion: 46,XX,inv(1)(p36.1q32). The pair on the left are stained for G bands, and the pair on the right, for C bands (centromere bands). B, Reciprocal translocation: 46,XX,t(2;4)(p22.2;q35.2). C, Robertsonian translocation: 45,XX,t(13q14q). D, Interstitial deletion: 46,XY,del(13)(q21.3q31). E, Ring: 46,XY,r(17)(p13.3q25.3). (Karyotypes in A from Johnson DD, Dobyns WB, Gordon H, et al. Hum Genet 1988;78:315; those in B, C, and D courtesy of B.A. Hirsch, Department of Laboratory Medicine and Pathology, University of Minnesota Medical School; karyotype in E from Dobyns WB, Stratton RF, Parke JT, et al. J Pediatr 1983;102:552.)
Dobyns and Das / Introduction to Genetics
inversion of the intervening segment and repair of the breaks. When the inverted segment includes the centrosome, the rearrangement is described as a pericentric inversion (see Fig. 21-11A), whereas rearrangements in which the inverted segment does not include the centrosome are designated as paracentric inversions. Both types of inversions may result in production of unbalanced gametes because of the effects of recombination within the inverted segment. With pericentric inversions, a loop is formed between the inverted chromosome and its homolog during meiosis 1 (Fig. 21-12). Recombination is somewhat but not completely suppressed within inversion loops, so crossovers are common in larger loops.
3
5 4
4 5
3
6
6
7
7
Normal
2
2
6
2
3
3
3
5
FIGURE 21-12. The effect of recombination within the loop of a pericentric inversion. A, A normal chromosome is depicted on the right, with loci 1 to 7 in order and the centromere located between loci 3 and 4. A pericentric inversion is depicted on the left, with the segment containing loci 3 to 5 and the centromere inverted. B, Pairing of the normal and inverted chromosomes during meiosis 1, with a crossover occurring within the inversion loop in the middle two chromatids. C, The four types of gametes produced after completion of meiosis include a normal chromosome, a derivative chromosome with duplication of the distal short arm and deletion of the distal long arm (dup p), the reverse derivative chromosome with duplication of the distal long arm and deletion of the distal short arm (dup q), and a balanced pericentric inversion.
4
4
4
4
5
5
5
3
6
2
6
6
7
1
7
7
Inversion
A
Recombination within a pericentric inversion loop produces derivative chromosomes in which segments distal to the breaks are either duplicated or deleted (see Fig. 21-12C). The effects on the phenotype are inversely proportional to the size of the inversion. Thus, the distal segments typically are large with small pericentric inversions, and most unbalanced offspring are spontaneously aborted. Liveborn children with birth defects are more likely with larger inversions that lead to relatively small distal segments. Crossovers within a paracentric inversion loop, which commonly result from crossovers within LCRs, result in acentric or dicentric chromosomes. Acrocentric chromosomes
Inversion
2
1
Dup q
2
7
Dup p
1
1
Normal
1
1
C 4
1
2 Crossover
5 4
6
5
7
3 3
1 2 6 7
B
527
528
Genetic, Metabolic, and Neurocutaneous Disorders / 21
are quickly lost during subsequent rounds of cell division. Dicentric chromosomes inactivate one of the two centromeres and are retained. For both, the loss or gain of chromosomal material and genes is so great that almost all affected embryos are spontaneously aborted, unless a large part of the derivative chromosome happens to break off and become lost. This mechanism has been proved and may be more common than appreciated [Giglio et al., 2002].
Reciprocal Translocations Reciprocal translocations consist of breaks in nonhomologous chromosomes, with a reciprocal exchange of the broken segments (see Fig. 21-11B). Usually only two chromosomes are involved, but complex translocations involving three or more chromosomes have been described and likely are more common than standard chromosome analysis has suggested [Astbury et al., 2004a]. Population studies have
Normal
Carrier t(3;6) Alternate
detected reciprocal or robertsonian translocations in about 1 in 500 newborns. Reciprocal translocations often result in the production of unbalanced gametes. During meiosis 1, the derivative chromosomes and their normal homologs form a quadriradial shape that may separate into pairs in one of three ways: alternate, adjacent 1, and adjacent 2 segregation. Alternate segregation produces balanced gametes that have either normal chromosomes or both derivatives, which are therefore balanced. Adjacent 1 segregation produces unbalanced gametes in which homologous centromeres separate into different daughter cells. It results in duplication of the distal segment of one derivative chromosome and deletion of the distal tip of the other. In most translocation carriers, alternate and adjacent 1 segregation account for a large majority of the gametes (Fig. 21-13). Adjacent 2 segregation also produces unbalanced gametes. In this uncommon
der(6)
der(3) Adjacent 1
FIGURE 21-13. Diagram of the alternative types of segregation and gametes produced in the carrier of a reciprocal translocation between the short arms of chromosomes 3 (solid black) and 6 (hatched). The top line represents the parental chromosome pairs, the middle line represents the four types of gametes produced by the father, and the bottom line represents four possible chromosome combinations that may be observed in offspring. Alternate segregation (depicted on the left) produces offspring with either normal chromosomes or the balanced translocation. Adjacent 1 segregation (depicted on the right) produces offspring with unbalanced karyotypes. Children with the derivative 6 karyotype [der(6)] have deletion of the distal segment of 6p and duplication of the distal segment of 3p. Children with the derivative 3 karyotype [der(3)] have deletion of 3p and duplication of 6p. In both alternate and adjacent 1 segregation, homologous centromeres pass to different daughter cells. In adjacent 2 segregation (not depicted), homologous centromeres pass to the same daughter cells, leading to even greater chromosomal imbalance.
Dobyns and Das / Introduction to Genetics
mechanism, homologous centromeres pass to the same daughter cell. The resulting nondisjunction produces 3:1 and even a 4:0 segregation. Reciprocal translocations often are detected in normal adults evaluated because of repeat fetal loss or after the birth of a child with multiple congenital anomalies caused by transmission of the translocation in unbalanced form. Apparently balanced reciprocal translocations sometimes are found in children with birth defects or abnormal development. In these instances, the abnormal phenotype usually results from either submicroscopic loss of genetic material or disruption of a gene at one of the breakpoints [Astbury et al., 2004b].
Robertsonian Translocations Robertsonian translocations involve two acrocentric chromosomes that fuse in or near the centromere region, with loss of the short arms (see Fig. 21-11C). Because the short arms contain repetitive DNA elements, especially rRNA, no phenotypic effects result. Carriers of a robertsonian translocation on chromosome 21 have a high risk of producing a child with translocation Down syndrome.
Insertions Insertions occur when a small segment of a chromosome is removed and inserted into a different region on the same or another chromosome. If the segment is inserted with the same orientation with respect to the centromere, it is known as a direct insertion. If it is inserted with the reverse TABLE 21-5 Examples of Chromosomal Abnormalities Using Standard Nomenclature (Short System) Rearrangement
Karyotype
Genome Mutations Triploidy Monosomy Trisomy
69,XXX 45,X (Turner’s syndrome) 47,XX,+21 (Down syndrome)
Deletion Terminal Interstitial
46,XY,del(8)(p21.1) 46,XX,del(17)(p11.2p11.2)
Duplication Direct Inverted
46,XY,dir dup (2)(p14p23) 46,XX,inv dup (11)(p12p15)
Paracentric Inversion Balanced Unbalanced
46,XX,inv(1)(p32p36.1) 46,XX, dup q, inv(1)(p32p36.1)
Pericentric Inversion Balanced Unbalanced
46,XX,inv(1)(p36.1q32) 46,XY,dup(q),inv(1)(p36.1q32)mat
Reciprocal Translocation Balanced 46,XY,t(–17,+der(17),t(7;17)(p22.3;p13.3)pat Ring 46,XY,r(17)(p13.3q22.3) Robertsonian Translocation Balanced 46,XX,rob(13;21) Unbalanced 46,XY,–13,+der(13),rob(13;21)mat del, deletion; der, derivative; dir, direct; dup, duplication; inv, inversion; mat, maternal; pat, paternal; r, ring; rob, robertsonian translocation; t, translocation.
529
orientation, it is called an inverted insertion. Insertions are rare because three separate chromosomal breaks are required. Segregation during meiosis can produce either abnormal offspring, with duplication or deletion of the inserted segment, or normal offspring and balanced carriers.
Rings Rings—ring chromosomes—are formed when a chromosome undergoes two breaks, usually one in each arm, and the broken ends are rejoined (see Fig. 21-11E). The two segments distal to the breaks are lost, resulting in deletion of both telomeres and adjacent regions of both the short and the long arms of the chromosome. Rings may not segregate properly during mitosis and meiosis, especially if a crossover occurs. Crossover often results in breakage followed by fusion, which may produce larger or smaller rings.
Isochromosomes and Dicentrics Isochromosomes are chromosomes in which one arm is missing and the other is duplicated as the result of misdivision of the centromere during meiosis 2. Isochromosomes also can result from translocation of an entire arm to its homolog with a breakpoint adjacent to the centromere. The most commonly observed isochromosome involves Xq. Dicentrics are rare chromosomes in which two segments, each containing a centromere, fuse end to end. They tend to break during mitosis because of the double centromeres.
Cytogenetic Nomenclature Detailed rules regarding nomenclature of chromosomes and chromosomal abnormalities have been published [ISCN, 1995]. Examples of most of the major types of abnormalities are listed in Table 21-5 using standard nomenclature. Note that breakpoints on the same chromosome are not separated by any punctuation, whereas breakpoints on different chromosomes are separated by a semicolon.
MUTATIONS AND GENETIC DISEASES The number of genetic changes causing disease, including neurologic disorders, is far too great to cover here, although many of these are reviewed in other chapters in this book. Here we review the general mechanisms that lead to genetic diseases, starting with a definition of mutation. As a very basic definition, a mutation is simply a permanent change in the DNA of an individual. The change most often is a change in the nucleotide sequence anywhere in the genome, although some chemical modifications of DNA can result in mutations as well. Such modifications are known as epigenetic mechanisms. Genetic diseases are caused by mutations that adversely affect function of one or more genes. The same is true for many types of cancer.
Classes of Mutations Mutations have been subdivided into three main types: genome, chromosome, and gene mutations. They may occur in either somatic or germ cells, although only germ cell mutations can be transmitted to offspring. All three occur often enough for affected individuals to be observed in clinical practice.
530
Genetic, Metabolic, and Neurocutaneous Disorders / 21
Genome and Chromosome Mutations Abnormalities of chromosome number, including triploidy, tetraploidy, and aneuploidy, are classified as genome mutations. Similarly, structural rearrangements are classified as chromosome mutations. Both of these were reviewed in the preceding section. Genome and chromosome mutations are rarely perpetuated to the next generation because most result in spontaneous abortions. Thus, the frequencies cited are probably underestimates.
Gene Mutations Gene mutations differ from genome and chromosome mutations because the segment of DNA involved is much smaller and the mechanisms are different. The most common types are base pair substitutions and small deletions or insertions that can be caused by an error during DNA replication or by base changes induced by extrinsic agents referred to as mutagens. Because genome and chromosome mutations usually are lethal, most significant heritable mutations are gene mutations.
DNA Replication Errors DNA replication normally is an accurate process. The DNA polymerases (see Table 21-2) insert an incorrect base only once in every 10 million bp. A series of DNA repair enzymes exist that are able to recognize and replace noncomplementary bases, correcting more than 99.9% of errors. The overall mutation rate is therefore only 10−10 per base pair per cell division. The human genome consists of about 6 × 109 base pairs, so this mutation rate results in less than 1 bp mutation per cell division. Nevertheless, an estimated 1015 cell divisions occur during the lifetime of an adult human. Thus, thousands of new mutations occur at virtually every position in the genome. Not surprisingly, inherited defects in DNA replication and repair enzymes lead to a striking increase in the frequencies of all types of mutations. Most of the mutations occur in somatic cells, where they may cause cancer or a genetic disease affecting only part of the body, such as segmental neurofibromatosis. Fewer mutations occur in germ cells. During oogenesis, female germ cells undergo mitosis approximately 22 times and begin meiosis only once during fetal life. The cells are suspended in meiosis from fetal life till shortly before ovulation during the reproductive years. Spermatogenesis consists of approximately 30 mitoses from conception until puberty and approximately 20 to 25 per year thereafter. Thus, the opportunity for mutations is expected to be far greater for sperm than for ova. This phenomenon has been confirmed in several genetic disorders, such as neurofibromatosis type 1, achondroplasia, and hemophilia A. It has been estimated that as many as 1 in 10 sperm in healthy males may carry a new deleterious mutation. Most are recessive or lethal and therefore not apparent in liveborn children.
Mutation Rate The mutation rate for any given gene or other DNA segment depends on both its size and its location. The location may be important because certain areas of the genome are known to be “hot spots” for recombination. The average mutation rate is about 1 × 10−6 mutation per locus per generation, but the rate varies by more than a thousand-fold for different genes. For example, the number of new mutations
per 106 gametes is 40 to 100 for Duchenne muscular dystrophy and neurofibromatosis 1, but only 2 to 5 for aniridia and hemophilia B. These statistics include only mutations causing genetic diseases. The rate of change of protein polymorphisms suggests a rate as high as 6 × 10−6 per locus per generation (a locus is the position of a gene on a chromosome).
Specific Types of Gene Mutations The development and widespread use of modern molecular techniques have led to the discovery of specific mutations at many different loci. From among these, many different types of mutations have been recognized, all of which have the potential for causing genetic diseases. They may be divided by size into single and multiple base changes. The latter may involve only one or a few bases or may involve millions of base pairs. In any specific gene, mutations are almost always heterogeneous, although some types may be more common than others. Thus, the specific mutations in unrelated persons with the same genetic disease often are different. A few notable exceptions to this rule have been identified, such as achondroplasia, which almost always is caused by a specific single base change in the fibroblast growth factor receptor 3 gene [Bellus et al., 1995].
Nucleotide Substitutions Point mutations or single-base substitutions represent one of the most common types of mutation. Most are related to an error in DNA synthesis by the enzyme DNA polymerase that was not corrected by DNA repair enzymes. Some combinations of nucleotides are mutation prone, however. More than 30% of point mutations found in some genetic diseases are the result of cytosine-to-thymine transitions, which are caused by methylation of cytosine residues to 5-methylcytosine, especially cytosine residues occurring as the first base in a 5′-CG-3′ dinucleotide pair. The latter then undergoes spontaneous deamination to thymidine. Thus, the 5′-CG-3′ doublet represents a “hot spot” for mutation in the human genome.
Deletions, Duplications, and Insertions The remainder of mutations consist of loss or gain of nucleotide bases somewhere in the genome; a variety of mechanisms for such changes are known. A deletion consists of any loss of DNA sequence, whereas a duplication consists of a second copy of a DNA sequence that is usually located immediately adjacent to the first copy. An insertion consists of a DNA sequence that has been removed or copied from one location and moved to a nonhomologous region elsewhere on the same chromosome or to a different chromosome. Deletions, duplications, and insertions that involve one or a few base pairs can be detected only by nucleotide sequencing. Larger deletions and duplications may be detected by several of the methods described earlier including direct sequencing, Southern blot analysis, FISH, and CGH.
Effects of Mutations on Gene Function The effect of mutations on gene function depends as much or more on the specific location of the mutation as on the size. Mutations that occur in DNA outside functioning genes
Dobyns and Das / Introduction to Genetics
usually have no consequences. Mutations within the boundaries of a gene may inactivate it or have little or no effect, depending on the nature of the change.
Missense Mutations A point mutation within the coding region of a gene can alter the genetic code by changing the nucleotide triplet and cause the replacement of one amino acid by another in the gene product, thus altering function of the gene product. Such mutations are called missense mutations and do not change the reading frame of the DNA sequence. The bestknown example is the A-to-T substitution in the sixth codon of the β-globin gene, which causes sickle cell anemia, by substituting valine for glutamic acid in the β-globin protein chain. Not all mutations within coding regions of a gene result in a missense mutation, however. All but 2 of the 20 amino acids are specified by more than one codon, most often differing in the third or “wobble” position of the triplet. The gene product will be identical if the new triplet codes for the same amino acid.
Nonsense (Chain Termination) Mutations Mutations that generate one of the three stop codons result in premature termination of translation, whereas those that alter a stop codon allow translation to continue until the next stop codon is reached. Those mutations that result in a premature stop codon are called nonsense mutations. In general, these mutations have no effect on transcription (DNA to RNA), but the shortened polypeptide may have lost critical functional domains of the protein, or the mRNA may be so unstable that it is rapidly degraded in the cell. The latter process is known as nonsense-mediated mRNA decay, a process by which mRNA species containing premature termination codons are recognized and degraded before translation, although this typically spares truncation mutations in the last coding exon [Frischmeyer and Dietz, 1999]. Both base substitutions and nucleotide loss or gain mutations may result in nonsense mutations.
RNA Splicing Mutations The sequence surrounding intron splice sites is highly conserved, and mutations of key nucleotides frequently prevent or reduce efficiency of splicing. The key nucleotide sequences at most splice junctions are shown in Figure 21-4. Splicing mutations may either inactivate existing splice sites or create new ones. In the first type, the mutation alters the splice donor, branch, or splice acceptor site, resulting in failure to correctly splice the intron at that site. This failure results in a large insertion of nucleotides that normally are not translated into the processed mRNA. This insertion is almost certain to introduce a stop codon within the next hundred or so codons, because 3 of the possible 64 triplet combinations are stop codons. In the second type, mutations within the intron create alternative splice donor or acceptor sites that compete with the normal splice sites during mRNA processing. Thus, a proportion of the mature mRNA will contain incorrectly spliced intron sequences. Both base substitutions and nucleotide loss-or-gain mutations may result in splicing mutations. One example of the first type is a G-to-C transition in the first position of the intron at the donor splice site in the
531
hexosaminidase A gene found in many Ashkenazi Jewish patients with Tay-Sachs disease [Nussbaum et al., 2001], as shown here: Normal allele: Tay-Sachs allele:
5′–CCAGGCTCTGgtaagggt–3′ 5′–CCAGGCTCTGctaagggt–3′
In this example, the bases in the exon are capitalized, whereas those in the intron are not, and the mutation is underlined.
Frameshift Mutations Small nucleotide loss-or-gain mutations may alter the reading frame of the mRNA product from the point of the mutation on, which results in a completely different amino acid sequence at the carboxyl end of the protein product or premature chain termination if a stop codon is encountered in the new reading frame. Any loss-or-gain mutation that involves a multiple of three bases maintains the reading frame, whereas a mutation that does not involve a multiple of three nucleotides changes the reading frame. Larger deletions that include one or more introns also may cause a frameshift mutation, because exon/intron splice sites may occur at any point in the reading frame, thereby splitting codons. If the exon just downstream from the deletion normally begins at a different position in the triplet than the deleted intron, the reading frame will be changed. By contrast, base substitutions do not cause frameshift mutations. Deletions and insertions cause dysfunction of the gene more often than point mutations because of the possibility of a frameshift. One of the best-known frameshift mutations is a single base deletion in the ABO blood group locus that results in the nonfunctional O allele. The deletion alters the reading frame at codon 86 until a premature stop codon is reached 30 codons later. The stop codon is normally out of frame and is therefore not read. With some intermediate-size deletions of approximately 1 kb to 1 Mb, one or more exons of a gene may be duplicated or deleted. About two thirds of these will change the reading frame and result in a frameshift mutation. Those that maintain the reading frame produce truncated products that may or may not retain function. These relatively small deletions and duplications are too small to be seen with chromosome analysis or FISH and cannot be found by sequencing, which is not sensitive to dosage (recall that all autosomal genes and X-linked genes in females have two copies of each gene). These may be rare or common mechanisms of mutation. For example, small deletions and duplications are the most common mutational types for Duchenne muscular dystrophy and Becker muscular dystrophy, both caused by mutations of the dystrophin or DMD gene. These are simple to detect for X-linked diseases in males, because only one gene copy is present. When any autosome of the X chromosome in a female is involved, the mutation can be detected by other methods, such as quantitative PCR assay.
Transcriptional Control Mutations Mutations involving promoter sequences in the 5′ UTR or other regulatory sequences in the 3′ UTR of a gene may result in a significant decrease in the amount of mature, processed mRNA produced. Both base substitutions and
532
Genetic, Metabolic, and Neurocutaneous Disorders / 21
nucleotide loss-or-gain mutations may result in transcriptional control abnormalities.
single allele or a pair of alleles. Only a single allele is present for most genes on the X chromosome in males, who have only one X chromosome. A pair of alleles is present for all genes on the autosomes, and for a subset of genes on the X chromosome located in “pseudoautosomal” regions, which have functional homologs on the Y chromosome. The observable expression of the genotype is the phenotype. Penetrance has been defined as the percentage of persons with a particular genotype who have the expected phenotype; this is an all-or-none phenomenon. Expressivity is defined as the extent to which a genetic trait or disease is expressed and may vary greatly between affected persons. The proband is the affected family member through whom a family is identified; the consultand is the person in the family who seeks advice, regardless of whether affected or not. A pedigree is a diagram of the family history that shows the family members, their relationships to the proband, and their status with regard to the hereditary condition. Some of the symbols used for pedigrees in medical genetics are illustrated in Figure 21-14. A more detailed standardized nomenclature has been proposed for publication of pedigrees [Bennet et al., 1995]. The most widely recognized patterns of inheritance are single-gene or “mendelian” patterns, which include autosomal-dominant, autosomal-recessive, and X-linked modes of inheritance; example pedigrees are shown in Figure 21-15. All of these result from mutations in a single gene. The disorder or trait is autosomal if located on human chromosomes 1 to 22 and X-linked when located on the X chromosome. The only true Y-linked trait is male sex determination (the SRY gene). Autosomal traits are considered dominant when expressed in both heterozygotes and homozygotes, and recessive when expressed only in homozygotes; neither of these terms really fits with X-linked
PRINCIPLES OF MEDICAL GENETICS Several principles of genetics derived from the chromosomal and molecular basis of heredity form the basis for the different patterns of inheritance observed in genetic diseases. A working understanding of the principles of inheritance is important for understanding the genetic diseases encountered in pediatric neurology clinics, for formulating an optimal management approach to patients with these diseases, and for providing accurate genetic counseling. The simplest and best-known patterns of inheritance involve mutations of single genes; however, more complex patterns of inheritance likely are more common. Here we review some of these principles and examine the basis for genetic counseling.
Patterns of Inheritance A discussion of inheritance requires familiarity with a special vocabulary. As reviewed previously, a gene is a sequence of DNA that is required for production of a functional product. The position of a gene on a chromosome is known as its locus. The alternative forms of a gene that may occupy a given locus are known as alleles. Different alleles typically result from one or more minor differences in nucleotide sequence. When both alleles at a given locus are identical, the person is said to be homozygous for that trait. When the alleles are different, the person is described as heterozygous. When only one allele is present, the person is hemizygous. The genetic constitution of an individual is the genotype. At any given locus, the normal genotype consists of either a
4
2
Male
Marriage
Female
Extramarital mating
Sex unspecified
Divorce
Number of children of sex indicated
Consanguineous mating
Affected Monozygotic twins
Heterozygotes for autosomal trait Carrier of X-linked recessive trait
Dizygotic twins
Proband ? Twins of unknown zygosity
Deceased individual Prenatal death
1
I
2
Miscarriage Adopted into a family II
1
2
Numbering individuals in pedigrees 3
Proband is II-2
Adopted out of a family No offspring
FIGURE 21-14. Common symbols used in pedigrees.
Dobyns and Das / Introduction to Genetics AD
AR
Heterozygous affected
533
XL
Carrier of X-linked disorder
Homozygous or hemizygous affected FIGURE 21-15. Examples of autosomal-dominant (AD), autosomal-recessive (AR), and X-linked (XL) pedigrees.
inheritance, as reviewed later on. The pattern of single-gene inheritance is modified in special cases in which mutations involve genes subject to imprinting or X inactivation, or involve only a proportion of cells in the body or affected tissue. Finally, many diseases have more complicated inheritance.
Autosomal-Dominant Inheritance The most important attributes of autosomal-dominant inheritance are expression of the trait in heterozygotes and male-to-male transmission (Fig. 21-15). The autosomaldominant pattern may be recognized because (1) the trait or disease typically appears in every generation, except that it may arise by new mutation in the first affected family member, (2) any child of an affected person has a 50% risk of inheriting the trait, (3) the offspring of unaffected family members also are unaffected, and (4) the trait may be transmitted by a parent of either sex to a child of either sex, and specifically may be transmitted from father to son, which distinguishes it from X-linked inheritance. Autosomal dominant inheritance is readily identified in most families but may be difficult to discern in others. When the disease occurs as a result of a new mutation, no relatives are affected. With reduced penetrance, low expressivity, and late age at onset, other affected family members may go unrecognized. Among the best examples for each of these characteristics are myotonic dystrophy and Huntington’s disease. Finally, incorrect information regarding family relationships, such as false paternity, may complicate interpretation of the pedigree. Most persons affected by a disorder of autosomaldominant inheritance are heterozygous, but rarely a homozygous person is encountered. Generally, the phenotype in homozygous persons is significantly more severe than in heterozygous persons. For example, one child born to parents who each had hereditary motor and sensory neuropathy type I had a much more severe neuropathy consistent with Dejerine-Sottas disease, or hereditary motor and sensory neuropathy type III [Killian and Kloepfer, 1979]. The best-known exception to this rule is Huntington’s disease, in which persons heterozygous for this trait cannot be distinguished from homozygotes.
Autosomal-Recessive Inheritance The most important attributes of autosomal-recessive inheritance are expression in homozygotes and equal gender distribution (see Fig. 21-15). This pattern may be recognized by the following four characteristics: (1) the trait or disease may affect multiple siblings but not parents, children, or other relatives, except in highly inbred populations, (2) each full sibling of an affected person has a 25% chance of inheriting the trait, (3) the parents are more likely than usual to be related, and (4) with rare exceptions, males and females are equally likely to be affected. In Western societies, a child with a disorder of autosomal-recessive inheritance may be the only affected person in the family owing to small family size and a tendency for parents of affected children to have fewer children after birth of a child with a genetic disease. This practice does not hold true in many other cultures, especially those with inbred populations. When the frequency of a rare recessive allele is relatively high within a family or population, the disease may appear in more than one generation. This pattern is known as pseudodominant inheritance. Some genes on the X chromosome have functional homologs on the Y chromosome, and traits or diseases associated with these genes will behave in the same manner as for autosomal loci. This pattern is known as pseudoautosomal inheritance. The risk of bearing a child with an autosomal-recessive disease or trait is increased when the parents are consanguineous or related by descent. More formally, the probability that a homozygote has received both alleles of a pair from an identical ancestral source is known as the coefficient of inbreeding. It also is the proportion of loci at which a person is homozygous by descent. For example, any child born to first cousins is homozygous at 1/16 of all loci. Although the relative risk of abnormal offspring is higher for first cousins than for unrelated parents, it is still low, at about 5%.
X-Linked Inheritance The inheritance of diseases and traits associated with genes located on the X chromosome differs markedly from autosomal forms of inheritance, becauses females have two X chromosomes whereas males have only one. Thus, when
534
Genetic, Metabolic, and Neurocutaneous Disorders / 21
mutations of an X-linked gene occur in males, no genetic “backup” is available. The situation in heterozygous (carrier) females is more complicated, owing to the phenomenon of X chromosome inactivation (Xi), which ensures that dosage for X-linked genes is the same in male and in female cells. Because Xi is random in most females, the maternally derived and paternally derived X chromosomes usually are active in about half of the cells in a female organism. Thus, mutation of one gene should cause no more than a 50% loss of function of the protein or other gene product. With this background, several mechanisms have been described that lead to disease expression in female carriers of X-linked mutations. First, some genes are dosage sensitive, so that 50% expression is not enough for normal function. Next, by chance or because of cell selection (usually favoring the normal allele), some females have skewing of X-inactivation such that one X chromosome is inactivated in a high proportion (80% to 100%) of cells. Unfavorable skewing will cause or worsen disease, whereas favorable skewing will prevent or reduce disease expression. Finally, skewing of X-inactivation also may result from mutations of the genes that actually control inactivation, especially the XIST gene, which is responsible for inactivation of one of the two X chromosomes. Not surprisingly, affected females usually have a less severe phenotype than that seen in affected males. The important characteristics of X-linked inheritance result from differential segregation of the X and Y chromosomes in males and females, and the differences in gene dosage. The most consistent characteristics include more severe phenotype in males than in females, transmission of disease through carrier females who are unaffected or less affected than males, and lack of male-to-male transmission (see Fig. 21-15). The last is explained by transmission of the Y chromosome from fathers to sons, whereas the disease genes TABLE 21-6 Rules for X-Linked Inheritance in Humans Rules Related to Segregation of the X and Y Chromosomes Hemizygous males transmit X chromosomes to daughters and Y chromosomes to sons. • Male-to-male transmission of X-linked disorders cannot occur. • Sons of hemizygous males never inherit the disorder. • Daughters of affected males all are heterozygous (carriers or affected). • All affected males in a family are related through heterozygous females. Heterozygous females transmit X chromosomes to both sons and daughters. • Fifty percent of sons of heterozygous females will be hemizygous males. • Fifty percent of daughters of heterozygous females also will be heterozygous females. Rules Related to Penetrance, Expressivity, and Sex Ratio Penetrance and Expressivity • In general, penetrance is higher and expressivity more severe in hemizygous males than in heterozygous females. Sex Ratio of Affected Persons • Males are predominantly affected when female penetrance is low. • Female-to-male ratio is close to 2:1 when female penetrance and male survival are high. • Females are predominantly affected, with prenatal lethality in males.
are located on the X chromosome. X-linked disorders traditionally have been divided into dominant and recessive subtypes, just as for autosomal single-gene disorders. This distinction was first made in fruit flies under experimental conditions but has never worked very well for human disorders. In a recent survey of more than 30 X-linked diseases, a remarkably wide range of penetrance, with many disorders intermediate between so-called X-linked dominant and recessive patterns, were found [Dobyns et al., 2004]. On the basis of these and other arguments, use of these subtypes should be discontinued. The rules for X-linked inheritance have been modified to reflect this change (Table 21-6). In many instances, children with X-linked diseases present primarily or frequently to pediatric neurologists, including those with adrenoleukodystrophy, the Duchenne and Becker forms of muscular dystrophy, fragile X syndrome, many X-linked mental retardation syndromes, two forms of X-linked lissencephaly, and many others. These diseases all result in more severe phenotypes in males than in females. Another class of X-linked disorders are “X-linked, male lethal” have proved to be particularly important in pediatric neurology. These diseases are observed almost exclusively in females and are thought to cause prenatal lethality in males or to cause a much more severe phenotype that is not recognized as the same disorder. Examples are Aicardi’s, Goltz’s, and Rett’s syndromes and orofaciodigital syndrome type I.
Genomic Imprinting In most single-gene disorders, the expression of a trait or disease is expected to be the same regardless of whether the gene was inherited from the mother or the father. Significant differences in expression based on the gender of the transmitting parent, however, have been observed in several disorders. This phenomenon is known as imprinting and reflects differences in the state of the maternal and paternal contributions to the genome, especially differential methylation of the maternally and paternally derived chromosomes. An imprinted gene can be imprinted or differentially methylated (i.e., differentially silenced) in all cells of the body, or only in selected tissues, such as brain. This differential silencing means that imprinted genes will be expressed from the maternally derived gene or from the paternally derived gene, but not from both. So if the functioning copy of an imprinted gene is lost owing to a deletion or mutation, the affected person is left with no functioning gene, and a disease phenotype will result. The underlying mechanisms are under study but still are not well understood [Hall, 1990; Jiang et al., 2004]. Imprinting disorders result from deletions or other types of mutations of genes within imprinted regions (or in the imprinting control regions). The most common of these result in infantile developmental disorders relevant for pediatric neurologists, such as BeckwithWiedemann syndrome due to defects of imprinted genes on 11p15.5 [Weksberg et al., 2003] and Angelman’s syndrome and Prader-Willi syndrome due to defects of imprinted genes on 15q11.2-q13 [Amos-Landgraf et al., 1999]. These disorders are reviewed elsewhere in this book.
Uniparental Disomy Defects of imprinted genes also may result from a rare mutation type known as uniparental disomy (UPD). UPD is
Dobyns and Das / Introduction to Genetics
defined as the presence of a diploid cell line containing two chromosome homologs inherited from the same parent. It is believed to result from nondisjunction, which produces trisomy for a particular chromosome. Trisomy is followed by loss of one of the three homologs, reducing the chromosome number back to normal. This mutation is known as uniparental isodisomy when the two homologs are identical and uniparental heterodisomy when they are different (as a result of crossing over, different regions of the affected chromosomes usually are involved). When UPD involves a chromosome with an imprinted region, problems occur. For example, a child may inherit two paternally derived chromosomes, in which case no maternally derived chromosome will be present. Any genes that are normally expressed only from the maternally derived gene will not be expressed at all. This is one cause of Angelman syndrome. The same type of problem occurs in reverse if the child inherits two maternally inherited chromosomes. No paternally derived genes will be present, and a disease will occur. This is one cause of Prader-Willi syndrome [Amos-Landgraf et al., 1999]. Very rarely, UPD can result in a genetic disease by causing homozygosity of a recessive disease gene. Because the two chromosomes are identical, they are homologous at all loci. If the involved chromosome contains any recessive disease loci, the person with the mutation will be homozygous and therefore affected.
Mosaicism Mosaic is a term used to refer to an individual organism or tissue that contains two or more cell lines that differ in DNA sequence, although they are derived from a single zygote. All organisms begin with a specific DNA sequence in the cell of origin or zygote. As cell division proceeds, some mutations occur that produce small differences among different cell lines. The presence of two or more cell lines differing in their DNA sequence but derived from a single zygote is known as mosaicism. Mosaicism is clinically important in many disorders and probably explains some unusual diseases in which only part of the body appears to be affected with a birth defect or genetic disease. A good example is segmental neurofibromatosis. This phenomenon can involve any tissue or group of tissues in the body. When mosaicism is found in lymphocytes, fibroblasts, or other somatic cells of the body, it is designated somatic mosaicism. The mosaic individual typically demonstrates at least mild signs of disease. When mosaicism is found only in germ cells (egg, sperm), it is known as gonadal mosaicism. The mosaic individual usually is identified as the parent of two or more children with a genetic disease, despite having no signs of the disease clinically or on mutation analysis. Mosaicism may begin with a somatic mutation in the germline of the affected person, which then persists in the clonal descendants of that cell, including a proportion of the ova or sperm. When the mutation exists only in the germline, the parent has no signs of the disease but may conceive multiple affected children. This phenomenon has been seen frequently in Duchenne muscular dystrophy due to mutations of the DMD gene, the autosomal-dominant form of osteogenesis imperfecta associated with mutations of the COL1A1 or COL1A2 gene, and X-linked lissencephaly due to mutations of the DCX
535
gene. The distinction between somatic and germline mosaicism is most likely artificial, however, because standard evaluations examine very few tissues.
Complex Inheritance The most important attributes of complex or multifactorial inheritance are lack of a clear pattern of inheritance in single families, although more than one relative may be affected, and a relatively low risk to first-degree relatives (approximately the square root of the population risk), typically in the range of 1% to 5%. This form of inheritance results from variation at two or more loci with two or more alleles each, often with a prominent environmental influence. This pattern also is referred to as polygenic (we prefer oligogenic) or multifactorial inheritance. Examples of traits inherited in this pattern are head circumference, autism, neural tube defects, and common forms of epilepsy. Some are continuous traits that can be measured, such as head circumference, whereas others fall into non-overlapping groups, such as autism and epilepsy. For continuous traits such as head circumference, children are likely to be intermediate between their parents, or closer to the mean than either parent (so-called regression to the mean).
Mitochondrial Inheritance Mitochondria are the cellular organelles that are primarily responsible for cellular respiration and production of adenosine triphosphate, both essential for cellular energy management. Each mitochondrion contains multiple copies of a small 16.5-kb circular chromosome that codes for 13 proteins and many rRNA and tRNA genes that differ in sequence from the nuclear rRNA and tRNA genes. The proteins all are components of the respiratory chain, and the remainder of the respiratory pathway enzymes are encoded by nuclear genes. The mitochondria in any one person are derived almost exclusively from the mother through the ovum. Each ovum contains hundreds of mitochondria, and each mitochondrion contains many copies of the circular mitochondrial chromosome. Sperm contain a few mitochondria, most of which are degraded rapidly by the proteasome-dependent protein degradation pathway of the ubiquitin system within the ovum after fertilization [Sutovsky et al., 2003]. A small paternal contribution of mitochondria, however, has been demonstrated in several species, such as sheep [Zhao et al., 2004]. The same likely is true for humans, as suggested by one example of paternal inheritance of a mitochondrial disorder [Schwartz and Vissing, 2002]. This must be very rare, however, owing to the small proportion of paternal compared with maternal mitochondria, and as indicated by studies in humans with mitochondrial diseases [Filosto et al., 2003; Zhao et al., 2004]. In patients with mutations of mitochondrial genes, a variable proportion of the mitochondrial chromosomes carry the mutation. Thus, diseases caused by mutations in mitochondrial DNA exhibit strict maternal inheritance (with very rare exceptions) and usually will exhibit phenotypic variation within a family owing to variation in the proportion of mutant and normal mitochondria between individuals [Zeviani et al., 1989]. Maternal inheritance may be recognized because (1) the incidence of the disease is equal in males and females, (2) the disease is transmitted from mother to offspring
536
Genetic, Metabolic, and Neurocutaneous Disorders / 21
of both genders but never from father to offspring, and (3) variable expression is common. These criteria have been met for several diseases associated with mitochondrial DNA mutations, including Kearns-Sayre syndrome, Leber’s hereditary optic neuropathy, MELAS (mitochondrial encephalomyopathy, lactic acidosis, and strokelike episodes), and MERRF (myoclonic epilepsy with ragged-red fibers).
Genetic Counseling Medical genetics differs from other specialties because family members other than the patient may be at high risk for a disease first recognized in the patient, who then becomes the proband. The person or persons actually seeking advice may not themselves be affected. Ideally, the patient or the parents or guardians of minor children or incompetent adults, and all other family members at risk, should be made aware of both the clinical and the reproductive consequences of a genetic disease. Genetic counseling is the process of providing this information. Although any physician may provide genetic counseling as part of
overall patient management, it is more commonly conducted in genetics clinics.
Standard of Care All physicians have a professional responsibility to make certain that genetic counseling has been provided in appropriate situations and to ensure that the counseling meets current standards of practice [ASHG/ACMG report, 1995]. Failure to provide this information may have tragic results. Perhaps the best example for pediatric neurologists is the birth of a second or even a third male with Duchenne muscular dystrophy in a family. Courts have upheld the principle of physician responsibility to provide accurate counseling on several occasions. For example, the parents of a child with Down syndrome claimed negligence because the mother had not been referred for prenatal diagnosis. In another case, parents who were tested for Tay-Sachs disease carrier status both were told that they were not carriers. They later had an affected child and filed a claim. Cases of this type are known as wrongful life claims.
TABLE 21-7 Recurrence Risks in Siblings for Selected Neurologic Disorders of Childhood DISORDER
EMPIRICAL RISK
REFERENCE(S)
Brain Malformations Agenesis of the corpus callosum Cerebellar vermis hypoplasia (variant)‡ Dandy-Walker malformation (true)§ Molar tooth malformation (Joubert’s syndrome)|| Holoprosencephaly (literature) Holoprosencephaly (author) Hydrocephalus Male sibling of male hydrocephalus proband Lissencephaly with all test results normal Lissencephaly with no testing done Neural tube defects
Low,* XL† 5–25%,* XL ~1% 25% 6% 10–15% 1–4%, XL 12%, XL 5–10%,* XL 1–33%,* XL 2–3%
Baraitser, 1997 Philip et al., 2003 Murray et al., 1985 Satran et al., 1999 Roach et al., 1975 Baraitser, 1997 Burton, 1979 Authors’ experience Authors’ experience Koch and Fuhrmann, 1985
Developmental Disorders Autism Cerebral palsy, spastic and symmetric Cerebral palsy, spastic and asymmetric Mental retardation (MR) Male sibling of male patient with MR Microcephaly Microcephaly (below ~3 SD at birth) Microcephaly, multiple congenital disorders
4–5% 10% 1–2% 4–5%, XL 6–12%, XL 12% 25% 6%
Jorde et al., 1991 Baraitser, 1997 Baraitser, 1997 Herbst and Baird, 1982 Herbst and Baird, 1982 Baraitser, 1997 Authors’ experience Baraitser, 1997
Seizure Disorders Benign rolandic epilepsy Febrile seizures Partial epilepsy Primary generalized epilepsy
8–24% 15% 5% 4–13%
Heijbel et al., 1975 Hauser et al., 1985; Tsuboi, 1987 Andermann, 1982 Metrakos and Metrakos, 1961
Other Neurologic Disorders Migraine
12–27%
Baraitser, 1997
*These figures are estimates based on the personal experience of one of us (WBD) and a conservative approach to risk counseling. Note that several figures are higher than published data, which we attribute to less complete ascertainment of affected siblings in older published studies. †X-linked inheritance has clearly been observed for certain disorders and needs to be taken into account for risk counseling. ‡ Cerebellar vermis hypoplasia sometimes is called a Dandy-Walker “variant.” § In typical DWM, the vermis is small and rotated well upward, with an enlarged, cystic fourth ventricle. || This includes several Joubert’s syndrome–related disorders such as Arima, COACH, Senior-Loken, and Varadi syndromes. COACH, cerebellar vermis hypoplasia, oligophrenia, congenital ataxia, coloboma, hepatic fibrocirrhosis; DWM, Dandy-Walker malformation; SD, standard deviation; XL, X-linked.
Dobyns and Das / Introduction to Genetics
Responsibility to Relatives The responsibility to provide genetic counseling does not formally extend beyond the consultand, or person seeking genetic advice. People with genetic disorders are entitled to the same confidentiality as for persons with any other type of disease. Nevertheless, the need for confidentiality does not mean that no effort should be made to inform relatives of a common risk. Whenever the genetic evaluation suggests that other family members or their future children may be at risk, the consultand should be encouraged to contact those persons or ask the physician (or designee) to contact them and advise them to seek genetic evaluation. A majority of people act responsibly in this regard, but exceptions do arise that may present an ethical dilemma for health-care practitioners providing the counseling.
Relevance for Pediatric Neurology The obligation to provide accurate genetic counseling is particularly important for pediatric neurologists. Many neurologic and neuromuscular diseases in children have a genetic basis or a genetic component, including some of the most common problems seen in clinics. For disorders such as Duchenne muscular dystrophy, neurofibromatosis type 1, and tuberous sclerosis, the genetic basis and need for genetic counseling are well known. For others, the genetic basis or contribution is not widely recognized. Febrile seizures, benign rolandic epilepsy, and some types of primary generalized epilepsy may affect many persons in a family and appear to have autosomal-dominant inheritance, although penetrance is not complete. Mental retardation, microcephaly, and cerebral palsy have a significant genetic component, with recurrence risks of 5% to 10%. Most brain malformations are sporadic, but familial recurrence of almost every known type of brain malformation has been described. Because of the possibility of recurrence in relatives, pediatric neurologists should take a genetic history and advise patients and parents of their genetic risks. Referrals from pediatric neurology clinics to genetics clinics should occur frequently. Even for single-gene disorders with a known risk of recurrence, referral usually is needed to provide an accurate presentation of methods of prevention such as prenatal diagnosis when this is available, artificial insemination by donor, contraception, sterilization, and adoption. If the parents decide to terminate a pregnancy, continued professional support is an appropriate and important part of genetic counseling.
Genetic Risk One of the most crucial steps in offering accurate genetic counseling is to estimate the risk of recurrence of a genetic disorder in other family members. Estimation is not difficult for most diseases with a single-gene pattern of inheritance, but even these may be complex because of late age at onset or incomplete penetrance. For many other disorders, empirical recurrence risk estimates are used. These risk figures are derived from previous experience with the same disorder. Although such figures generally are accurate, exceptions occur because of causal heterogeneity and lack of knowledge regarding many rare disorders. The recurrence risks for some of the more common diseases seen in pediatric neurology clinics are listed in Table 21-7. In any given family, the recurrence risk may be different; consultation
537
with a geneticist or genetic counselor may be helpful in providing this information.
Prenatal Diagnosis Prenatal diagnosis can now be performed for hundreds of genetic disorders, including many of those discussed in this chapter. The major methods used include chromosome analysis, enzyme assays and other biochemical tests, molecular genetic tests, and direct examination of the fetus by ultrasonography. The last is a far more rigorous procedure than routine prenatal ultrasonography and usually is referred to as high-resolution, level 2, or genetic ultrasonography. The purposes of prenatal diagnosis are to provide (1) a range of informed choices for parents at risk for having a child with an abnormality, (2) reassurance to reduce anxiety, especially among parents at high risk, and (3) an opportunity for parents, who otherwise would choose not to have children, to conceive and bear healthy children. The results of prenatal tests are normal in more than 98% of pregnancies evaluated, and parents are reassured that the infant will be unaffected by the condition in question. Of course, the infant remains at risk for other disorders, just as do children born to any other parents. In a small proportion of cases, the fetus is indeed found to have a serious defect. Because effective prenatal therapy is not possible for most disorders, the parents then have the option of terminating the pregnancy.
Genetics and Medicine Genetics has become one of the most rapidly expanding fields in all of biology, and it is likely that this trend will continue. The past few years have seen completion of the Human Genome Project and identification of many genes relevant to neurologic disorders of childhood. The next few years will see the isolation of new genes responsible for common and complex diseases and many more single-gene disorders. REFERENCES Amos-Landgraf JM, Ji Y, Gottlieb W, et al. Chromosome breakage in the Prader-Willi and Angelman syndromes involves recombination between large, transcribed repeats at proximal and distal breakpoints. Am J Hum Genet 1999;65:370. Andermann NE. Multifactorial inheritance of generalized and focal epilepsy. In: Anderson VE, Hauser WA, Penry VK, et al., eds. Genetic basis of the epilepsies. New York: Raven Press, 1982:355. ASHG/ACMG report. Points to consider: Ethical, legal, and psychosocial implications of genetic testing in children and adolescents. Am J Hum Genet 1995;57:1233. Astbury C, Christ LA, Aughton DJ, et al. Delineation of complex chromosomal rearrangements: Evidence for increased complexity. Hum Genet 2004a;114:448. Astbury C, Christ LA, Aughton DJ, et al. Detection of deletions in de novo “balanced” chromosome rearrangements: Further evidence for their role in phenotypic abnormalities. Genet Med 2004b;6:81. Babcock M, Pavlicek A, Spiteri E, et al. Shuffling of genes within low-copy repeats on 22q11 (lcr22) by Alu-mediated recombination events during evolution. Genome Res 2003;13:2519. Bailey JA, Gu Z, Clark RA, et al. Recent segmental duplications in the human genome. Science 2002;297:1003. Baraitser M. The genetics of neurological disorders, 3rd ed. Oxford: Oxford University Press, 1997. Bejerano G, Pheasant M, Makunin I, et al. Ultraconserved elements in the human genome. Science 2004;304:1321.
538
Genetic, Metabolic, and Neurocutaneous Disorders / 21
Bellus GA, Hefferon TW, Ortiz de Luna RI, et al. Achondroplasia is defined by recurrent g380r mutations of fgfr3. Am J Hum Genet 1995;56:368. Bennet RL, Steinhaus KA, Uhrich SB, et al. Recommendations for standardized human pedigree nomenclature. Am J Hum Genet 1995;56:745. Burton BK. Recurrence risks for congenital hydrocephalus. Clin Genet 1979;16:47. Cardoso C, Leventer RJ, Ward HL, et al. Refinement of a 400-kb critical region allows genotypic differentiation between isolated lissencephaly, Miller-Dieker syndrome, and other phenotypes secondary to deletions of 17p13.3. Am J Hum Genet 2003;72:918. Cavaille J, Seitz H, Paulsen M, et al. Identification of tandemly-repeated c/d snoRNA genes at the imprinted human 14q32 domain reminiscent of those at the Prader-Willi/Angelman syndrome region. Hum Mol Genet 2002;11:1527. Chance PF, Abbas N, Lensch MW, et al. Two autosomal dominant neuropathies result from reciprocal DNA duplication/deletion of a region on chromosome 17. Hum Mol Genet 1994;3:223. Chen KS, Manian P, Koeuth T, et al. Homologous recombination of a flanking repeat gene cluster is a mechanism for a common contiguous gene deletion syndrome. Nat Genet 1997;17:154. Cheung VG, Nowak N, Jang W, et al. Integration of cytogenetic landmarks into the draft sequence of the human genome. Nature 2001;409:953. Chiaromonte F, Weber RJ, Roskin KM, et al. The share of human genomic DNA under selection estimated from human-mouse genomic alignments. Cold Spring Harb Symp Quant Biol 2003;68:245. Cotton RG. Slowly but surely towards better scanning for mutations. Trends Genet 1997;13:43. Denli AM, Tops BBJ, Plasterk RHA, et al. Processing of primary microRNAs by the microprocessor complex. Nature 2004;432:231. Dermitzakis ET, Reymond A, Lyle R, et al. Numerous potentially functional but non-genic conserved sequences on human chromosome 21. Nature 2002;420:578. Dermitzakis ET, Reymond A, Scamuffa N, et al. Evolutionary discrimination of mammalian conserved non-genic sequences (CNGS). Science 2003;302:1033. Dobyns WB, Filauro A, Tomson BN, et al. Inheritance of most X-linked traits is not dominant or recessive, just X-linked. Am J Med Genet 2004;129A:136. Dracopoli NC, Haines JL, Korf BR, et al. Current protocols in human genetics, Quarterly Supplements ed. United States. Hoboken, NJ: John Wiley & Sons, 1997. Eng C, Vijg J. Genetic testing: The problems and the promise. Nat Biotechnol 1997;15:422. Filosto M, Mancuso M, Vives-Bauza C, et al. Lack of paternal inheritance of muscle mitochondrial DNA in sporadic mitochondrial myopathies. Ann Neurol 2003;54:524. Frazer KA, Tao H, Osoegawa K, et al. Noncoding sequences conserved in a limited number of mammals in the sim2 interval are frequently functional. Genome Res 2004;14:367. Frischmeyer PA, Dietz HC. Nonsense-mediated mRNA decay in health and disease. Hum Mol Genet 1999;8:1893. Gardner RJ, Mackay DJ, Mungall AJ, et al. An imprinted locus associated with transient neonatal diabetes mellitus. Hum Mol Genet 2000;9:589. Giglio S, Pirola B, Arrigo G, et al. Opposite deletions/duplications of the X chromosome: Two novel reciprocal rearrangements. Eur J Hum Genet 2000;8:63. Giglio S, Broman KW, Matsumoto N, et al. Olfactory receptor-gene clusters, genomic-inversion polymorphisms, and common chromosome rearrangements. Am J Hum Genet 2001;68:874. Giglio S, Calvari V, Gregato G, et al. Heterozygous submicroscopic inversions involving olfactory receptor-gene clusters mediate the recurrent t(4;8)(p16;p23) translocation. Am J Hum Genet 2002;71:276. Grompe M. The rapid detection of unknown mutations in nucleic acids. Nat Genet 1993;5:111. Hall JG. Genomic imprinting: Review and relevance to human diseases. Am J Hum Genet 1990;46:857. Hardison RC. Conserved noncoding sequences are reliable guides to regulatory elements. Trends Genet 2000;16:369. Hauser WA, Annegers JF, Anderson VE, et al. The risk of seizure disorders among relatives of children with febrile convulsions. Neurology 1985;35:1268.
Heijbel J, Blom S, Rasmuson M. Benign epilepsy of childhood with centro-temporal EEG foci: A genetic study. Epilepsia 1975;16:285. Herbst DS, Baird PA. Sib risks for nonspecific mental retardation in British Columbia. Am J Med Genet 1982;13:197. ISCN. An international system for human cytogenetic nomenclature. Basel: S Karger, 1995. Ishkanian AS, Malloff CA, Watson SK, et al. A tiling resolution DNA microarray with complete coverage of the human genome. Nat Genet 2004;36:299. Jiang YH, Bressler J, Beaudet AL. Epigenetics and human disease. Annu Rev Genomics Hum Genet 2004;5:479. Jorde LB, Hasstedt SJ, Ritvo ER. Complex segregation analysis of autism. Am J Hum Genet 1991;49:932. Killian JM, Kloepfer HW. Homozygous expression of a dominant gene for Charcot-Marie-Tooth neuropathy. Ann Neurol 1979;5:515. Koch M, Fuhrmann W. Sibs of probands with neural tube defects—a study in the Federal Republic of Germany. Hum Genet 1985;70:74. Lander ES, Linton LM, Birren B, et al. Initial sequencing and analysis of the human genome. Nature 2001;409:860. Lewin B. Genes VIII. Upper Saddle River, NJ: Prentice Hall, 2003;1056. Lucito R, Healy J, Alexander J, et al. Representational oligonucleotide microarray analysis: A high-resolution method to detect genome copy number variation. Genome Res 2003;13:2291. Lyon MF. Gene action in the X-chromosome of the mouse (Mus musculus l). Naturwissenschaften 1961;190:372. Lyon MF. X-chromosome inactivation and human genetic disease. Acta Paediatr Suppl 2002;91:107. McDermid HE, Morrow BE. Genomic disorders on 22q11. Am J Hum Genet 2002;70:1077. Metrakos K, Metrakos JD. Genetics of convulsive disorders, II. Genetic and electroencephalographic studies in centrencephalic epilepsy. Neurology 1961;11:474. Mohandas TK, Park JP, Spellman RA, et al. Paternally derived de novo interstitial duplication of proximal 15q in a patient with developmental delay. Am J Med Genet 1999;82:294. Murray JC, Johnson JA, Bird TD. Dandy-Walker malformation: Etiologic heterogeneity and empiric recurrence risks. Clin Genet 1985;28:272. Nussbaum RL, McInnes RR, Willard HF, et al. Thompson and Thompson genetics in medicine, 6th ed. Philadelphia: WB Saunders, 2001. Osborne LR, Li M, Pober B, et al. A 1.5 million-base pair inversion polymorphism in families with Williams-Beuren syndrome. Nat Genet 2001;29:321. Parisi MA, Bennett CL, Eckert ML, et al. The NPHP1 gene deletion associated with juvenile nephronophthisis is present in a subset of individuals with Joubert syndrome. Am J Hum Genet 2004;75:82. Pentao L, Wise CA, Chinault AC, et al. Charcot-Marie-Tooth type 1a duplication appears to arise from recombination at repeat sequences flanking the 1.5 Mb monomer unit. Nat Genet 1992;2:292. Philip N, Chabrol B, Lossi AM, et al. Mutations in the oligophrenin-1 gene (ophn1) cause X linked congenital cerebellar hypoplasia. J Med Genet 2003;40:441. Potocki L, Chen KS, Park SS, et al. Molecular mechanism for duplication 17p11.2—the homologous recombination reciprocal of the SmithMagenis microdeletion. Nat Genet 2000;24:84. Roach E, DeMeyer W, Conneally PM, et al. Holoprosencephaly: Birth data, genetic and demographic analyses of 30 families. Birth Defects 1975;11:294. Satran D, Pierpont ME, Dobyns WB. Cerebello-oculo-renal syndromes including Arima, Senior-Loken and COACH syndromes: More than just variants of Joubert syndrome. Am J Med Genet 1999;86:459. Saunier S, Calado J, Benessy F, et al. Characterization of the NPHP1 locus: Mutational mechanism involved in deletions in familial juvenile nephronophthisis. Am J Hum Genet 2000;66:778. Schwartz M, Vissing J. Paternal inheritance of mitochondrial DNA. N Engl J Med 2002;347:576. Sebat J, Lakshmi B, Troge J, et al. Large-scale copy number polymorphism in the human genome. Science 2004;305:525. Spiteri E, Babcock M, Kashork CD, et al. Frequent translocations occur between low copy repeats on chromosome 22q11.2 (lcr22s) and telomeric bands of partner chromosomes. Hum Mol Genet 2003;12:1823. Stankiewicz P, Lupski JR. Genome architecture, rearrangements and genomic disorders. Trends Genet 2002;18:74. Stein LD. Strategies for large-insert cloning and analysis. In: Dracopoli NC, Haines JL, Korf BR, et al, eds. Current protocols in human
Dobyns and Das / Introduction to Genetics genetics, Quarterly Supplements ed. United States. Hoboken, NJ: John Wiley & Sons, 1997:5.0.1. Strachan T, Read AP. Human molecular genetics, 2nd ed. New York: John Wiley & Sons, 1999. Sutovsky P, McCauley TC, Sutovsky M, et al. Early degradation of paternal mitochondria in domestic pig (Sus scrofa) is prevented by selective proteasomal inhibitors lactacystin and MG132. Biol Reprod 2003;68:1793. Tsuboi T. Genetic analysis of febrile convulsions: Twin and family studies. Hum Genet 1987;75:7. Urban Z, Helms C, Fekete G, et al. 7q11.23 deletions in Williams syndrome arise as a consequence of unequal meiotic crossover. Am J Hum Genet 1996;59:958. Venter JC, Adams MD, Myers EW, et al. The sequence of the human genome. Science 2001;291:1304. Waterston RH, Lindblad-Toh K, Birney E, et al. Initial sequencing and comparative analysis of the mouse genome. Nature 2002;420:520.
539
Watson JD, Crick FH. Molecular structure of nucleic acids: A structure for deoxyribose nucleic acid. Nature 1953;171:737. Weber JL, May PE. Abundant class of human DNA polymorphisms which can be typed using the polymerase chain reaction. Am J Hum Genet 1989;44:388. Weksberg R, Smith AC, Squire J, et al. Beckwith-Wiedemann syndrome demonstrates a role for epigenetic control of normal development. Hum Mol Genet 2003;12 (Spec No 1):R61. Wylie AA, Murphy SK, Orton TC, et al. Novel imprinted DLK1/GTL2 domain on human chromosome 14 contains motifs that mimic those implicated in IGF2/H19 regulation. Genome Res 2000;10:1711. Zeviani M, Bonilla E, DeVivo DC, et al. Mitochondrial diseases. Neurol Clin 1989;7:123. Zhao X, Li N, Guo W, et al. Further evidence for paternal inheritance of mitochondrial DNA in the sheep (Ovis aries). Heredity 2004;93:399.
CHAPTER 22
Chromosomes and Chromosomal Abnormalities Maria Descartes and Bruce R. Korf
The development of the human organism is directed by an estimated 30,000 genes, consisting of some 3 billion base pairs (bp) of DNA. These genes encode the structure of both proteins and noncoding RNAs, which together are responsible for the orderly unfolding of human development beginning from the fertilized egg (zygote), and for the maintenance of body structure and function. The entire pool of genetic information must be replicated with each cell division and a complete set of information apportioned to the two daughter cells. In addition, the full complement of genes must be transmitted from generation to generation through the germ cells. Genes do not exist as isolated entities within the cell nucleus but rather are arranged on structural units called chromosomes. Each chromosome contains hundreds or thousands of genes arranged in a linear order. This order is reproducible from cell to cell within an individual organism and from individual to individual in the population. The normal human chromosome complement consists of 46 chromosomes, including 22 pairs of nonsex chromosomes (autosomes) and either two X chromosomes in females or an X and a Y in males. Each of these chromosomes has a characteristic structure and includes a specific set of genes arranged in a specific order. The chromosomes are units that ensure the orderly distribution of a complete set of genetic information during cell division. Chromosome number and structure are tightly regulated, and deviations from the norm usually are associated with clinical problems. Multiple genes are simultaneously disrupted as a consequence of chromosomal abnormalities; accordingly, the phenotypic consequences usually are complex. Because of the complexity of the nervous system and its dependence on multiple genes, neurologic problems accompany most of the chromosomal disorders. Chromosomal abnormalities were among the first genetic disorders to be studied in the laboratory. Beginning in the late 1950s, with the advent of reliable techniques for chromosomal analysis, a set of syndromes resulting from changes in chromosome number or structure were described. Initially these were syndromes associated with loss or gain of entire chromosomes or large chromosome segments, such as Down syndrome, resulting from trisomy 21. Refinements in analytic technology have gradually improved the resolution of chromosomal analysis, permitting progressively smaller changes to be detected. Current techniques are beginning to bridge the gap between chromosomal anomalies visible with the light microscope and changes in individual genes at a submicroscopic level. At the same time, techniques have been developed that permit chromosomal analysis in nondividing cells and in various tissues that can be sampled prenatally. This chapter focuses on the approach to chromosomal disorders in pediatric neurology. The basic principles of
chromosome structure and function are considered, followed by a description of methods of chromosomal analysis. The various types of chromosomal abnormalities are then considered. This discussion is followed by an overview of the clinical approach to chromosomal abnormalities and then a brief clinical description of major chromosomal syndromes. The chapter closes with a look at future prospects for improving the power of cytogenetic analysis.
CHROMOSOME STRUCTURE AND FUNCTION The DNA double helix is a thread about 2 nm wide; if stretched, the DNA that makes up the entire genome would be approximately 2 meters in length. Within the nucleus, DNA is complexed with protein and folded into a highly organized structure. The basic unit of organization is known as the nucleosome [Turner, 1993]. Two copies each of the four histones—H2A, H2B, H3, and H4—bind with about 146 bases of DNA to form a globular structure (Fig. 22-1). Adjacent nucleosomes are separated by a variable length of DNA of up to 80 bases to form a structure resembling beads on a string. This string is the form in which DNA is transcribed to make messenger RNA (mRNA). Inactive chromatin is further folded into a more compact structure with histone H1 and nonhistone proteins. The most highly compacted state of chromatin occurs during the process of cell division. After DNA replicates, during the prophase stage of mitosis, chromatin condenses into the familiar structure of the mitotic chromosome [Boy de la Tour and Laemmli, 1988; Felsenfeld, 1996; Manuelidis and Chen, 1990]. The smallest chromosome segment resolvable with the light microscope may contain 105 to 106 bp, potentially including dozens of genes. Chromosome structure is best appreciated during this highly condensed phase (Fig. 22-2). The two chromatids represent replicated copies of the chromosome, each consisting of a single continuous double helix of DNA complexed with proteins as described. The chromatids remain joined at the centromere until anaphase, when the chromatids disjoin to the two daughter cells. The centromere divides the chromosome into a short arm (designated p, for petit) and a long arm (designated q). The ends of the chromosome consist of a specialized DNA sequence referred to as the telomere. Telomeres form a kind of cap necessary for chromosome replication [Cech, 2004]; maintenance of the telomere is thought to play a role in aging and also in malignancy. Although the basic role of DNA is to encode the amino acid sequence of proteins, much of the DNA does not serve a coding function. This noncoding DNA includes introns
542
Genetic, Metabolic, and Neurocutaneous Disorders / 22
DNA double helix
2 nm
“Beads-on-a-string” form of chromatin
11 nm
Chromatin fiber of packed nucleosomes
30 nm
Extended section of chromosome
300 nm
Condensed section of chromosome
700 nm
FIGURE 22-1. Schematic representation of DNA and chromosome organization. A, Orders of chromatin packing at metaphase. Width expressed in nanometers (nm). B, Relative size of chromosome band, the β-globin cluster of genes, and the β-globin gene, expressed in length of DNA (μm) and in the number of base pairs (bp) (1000 bp = 1 kilobase [kb]). (Modified from Albert B, Bray D, Lewis J, et al. Molecular biology of the cell. New York: Garland Publishing, 1983; Schmickel, 1986.)
A
*7800 m 15.5 15.4 15.3 15.2 15.1
14.3
14.2 14.1 13
12
11.2 11.12 11.11 17 12.1 12.2 12.3 13.1 13.2 13.3 13.4 13.5
14.1
14.2 14.3 21 22.1 22.2 22.3 23.1 23.2
23.3 24.1 24.2 24.3 25
700 nm
B
Chromatid of chromosome I I at prometaphase
5000 kb
*1700 m 60 kb 
␦
G␥
1 A␥
⑀
1600 kb
*22 m -like globin gene cluster *0.5 m -globin gene
*Total length of DNA
that separate parts of genes and are spliced out of the transcript to form the mature messenger RNA (mRNA), as well as DNA that forms the space between genes [Long et al., 1995]. In addition, stretches of DNA sequences that are repeated hundreds or thousands of times seem to serve a structural role. Large blocks of such repeated sequences occur near the centromeres [Willard, 1990]. These tend to remain highly condensed with protein throughout the cell cycle and are referred to as heterochromatin. The exact size and sequence composition of heterochromatic segments may not be highly conserved. Structural variants in these regions therefore may not be clinically significant.
The past decade saw a major worldwide effort to map the human genome and identify all of the genes. The Human Genome Project has resulted in delineation of an essentially complete human genome sequence and has produced major insights into the structure and function of the genome [Lander et al., 2001; Venter et al., 2001]. Although the exact number of genes is not known, it is estimated to be in the range of 30,000. It is clear that sequences that encode protein constitute a relatively small proportion of the genome. Many of the transcripts include RNAs that have functions other than serving as a template for proteins, and other parts of the genome include repeated sequences of unknown function.
Descartes and Korf / Chromosomes and Chromosomal Abnormalities Mid-metaphase banding
Prophase and prometaphase banding Band
1p35 Telomere
Band
6 3
P
Short arm
543
1p35.3 1p35.2 1p35.1
5 4 3 2 1
Negative or pale staining Q and G bands Positive R bands
Positive Q and G bands Negative R bands Sub-band
2 2 1 1
Variable bands
3 21
Centromere
1
Long arm Region
1
2
2
1 2 3 4 5
q
3
Band
4
1 2 21 3 4
Telomere Sister chromatids
CHROMOSOME
A
B FIGURE 22-2. A, Schematic anatomy of chromosome 1. B, An idiogram at different stages of condensation: R-banding. (Courtesy M.G. Mattei, Marseilles, France.)
METHODS OF CHROMOSOME ANALYSIS The history of clinical cytogenetics can be characterized as a series of technical advances each of which has led to the
recognition of new clinical syndromes resulting from chromosomal abnormalities. The modern era in human cytogenetics began with the discovery of methods to permit individual chromosomes to be identified in dividing cells.
544
Genetic, Metabolic, and Neurocutaneous Disorders / 22
The key breakthrough was the use of hypotonic treatment to spread apart the chromosomes, thereby avoiding overlaps [Hsu and Pomerat, 1953; Hughes, 1952]. This advance led, in 1956, to the discovery that the normal human chromosome number is 46, rather than 48 as had been previously thought [Tjio and Levan, 1956]. The second major advance was the discovery that the kidney bean extract phytohemagglutinin can stimulate lymphocytes to divide in culture, providing an easily obtained source of dividing cells for analysis [Nowell, 1960]. The first golden age of discovery of chromosomal abnormalities began with the recognition of trisomy 21 in persons with Down syndrome in 1959 [Lejeune and Gauthier, 1997] and continued through the early 1960s with the identification of other aneuploidy syndromes. Chromosome structure is most easily appreciated during mitosis, when the chromatin fiber is condensed and coiled into a characteristic structure. Spontaneously dividing cells are rarely available except in tumors or chorionic villus tissue used in prenatal diagnosis. Rather, cells are grown in short-term culture. For routine analysis, peripheral blood lymphocytes most commonly are used, although skin fibroblasts also may be cultured and analyzed. Phytohemagglutinin-stimulated peripheral blood usually is grown in culture for 3 days. Blocking the mitotic spindle with a drug such as colchicine leads to accumulation of dividing cells, which then are induced to swell by treatment with hypotonic saline, fixed, and spread onto a microscope slide. Chromosomes must be stained to be visualized with the light microscope. In the early days, cytogenetic stains that bound to either DNA or protein and that uniformly colored each chromosome were used. This practice made it difficult to identify chromosomes of similar size and shape and made it impossible to detect subtle rearrangements. Beginning in 1968, a number of stains were discovered that reveal a set of characteristic bands that permit precise identification of each chromosome and definition of chromosome regions [Caspersson et al., 1968]. Most laboratories use a form of G-banding, involving protease treatment of the chromosomes followed by Giemsa staining for routine analysis [Bickmore and Sumner, 1989]. The advent of chromosome banding stimulated a second wave of discovery of chromosomal syndromes during the 1970s. Subsequent developments in laboratory cytogenetics have gradually improved the resolution of chromosomal analysis. As the cell proceeds through mitosis, the chromosome gradually contracts, until anaphase, when the chromatids separate. If cells are collected during early prophase, chromosomes are highly extended, revealing a fine, highly detailed banding pattern [Yunis, 1976, 1981]. This banding pattern has facilitated recognition of subtle chromosome rearrangements involving small chromosome segments. Even with this approach, however, the resolution is limited to a few million bp of DNA, which may include dozens of genes. The gap between the light microscopic resolution of chromosome structure and the gene is being bridged by the technique of fluorescence in situ hybridization (FISH). This technique uses a fluorescently tagged segment of purified DNA corresponding to a specific gene or chromosome segment. Chromosomal DNA is separated into single strands on a microscope slide and incubated in a solution with single-stranded, fluorescently labeled DNA. Wherever this
FIGURE 22-3. Use of fluorescence in situ hybridization to detect submicroscopic deletions of chromosome 15. Each chromosome 15 is hybridized with two DNA probes, one for the region deleted in Prader-Willi and Angelman syndromes and one for a control region to mark chromosome 15. In this photograph, one copy of chromosome 15 demonstrates the normal two sets of hybridization signals, whereas the other demonstrates only one set, indicative of deletion. (Photograph courtesy of S. Weremowicz, Boston.)
“probe” DNA finds homologous DNA on the chromosome, a stable double helix forms. When this double helix is visualized with the light microscope, a bright spot is seen at the site on the chromosome that has bound to the probe (Fig. 22-3). FISH can be done using DNA probes isolated from single genes or with “cocktails” of multiple probes specific to a particular chromosome. Use of the latter lights up the entire chromosome, referred to as chromosome painting. FISH is used to detect deletions of small segments of DNA that cannot be visualized with the light microscope [Ligon et al., 1997] and has revealed a set of “microdeletion syndromes” resulting from deletions of contiguous genes. FISH also is helpful in the characterization of complex chromosome rearrangements or in the identification of chromosomal segments that participate in such rearrangements [Daniel et al., 1994]. Finally, FISH can permit visualization of chromosome regions in nondividing cells. This visualization can be used for rapid diagnosis of chromosome trisomies (if three fluorescent spots are seen to correspond with a particular chromosome, rather than the normal two) or for rapidly screening large numbers of nondividing cells for evidence of chromosomal mosaicism [Liehr et al., 1995; Lomax et al., 1994; Luquet et al., 2002]. FISH techniques also are being developed that stain each chromosome a different color, permitting “spectral karyotyping” with exceedingly high resolution and sensitivity for detection of subtle changes [Liehr et al., 2004]. Deletions and duplications are detected in most clinical laboratories by FISH. FISH focuses on only one region per analysis, so the technique is expensive and slow. New technologies are now available that allow genomewide screening. One of these methods is comparative genomic
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
hybridization (CGH). In CGH, differentially labeled total genomic DNA from a test and reference genomic DNA are co-hybridized to normal DNA metaphase chromosomes and/or fragments immobilized to a matrix. Repetitive sequences are blocked, and the resulting differences in hybridization provide representation of DNA copy-number variation [Pinkel et al., 1998; Pollack et al., 1999]. CGH can target metaphase chromosomes, total genomic DNA, cDNA, genomic clones, defined DNA, and nuclei acid sequences [Solinas-Toldo et al., 1997]. The resolution is in the range of 1.5 Mb (megabases) [Kriek et al., 2004].
TABLE 22-1 Common Chromosome Heteromorphisms CHROMOSOME(S)
STAIN
HETEROMORPHISM
1
G or Q
3
Q
9
G
16
G or C
Variation in size of heterochromatin on long arm; may be inverted Bright fluorescence of pericentromeric region Variation in size of heterochromatin on long arm; may be inverted Variation in size of heterochromatin on long arm; may be inverted Variation in size and fluorescence intensity of satellite region
13, 14, 15, 21, 22 G or Q
HUMAN KARYOTYPE
545
C, C-banding; G, G-banding; Q, Q-banding.
The normal human karyotype is depicted in Figure 22-4. Although each chromosome has a characteristic size and shape, chromosome morphology varies somewhat from person to person. These chromosome variants tend to occur in regions of the genome that do not encode genetic information and therefore are clinically silent. They are referred to as heteromorphisms and must be distinguished from clinically important chromosomal abnormalities. Common heteromorphisms include variations in the sizes of blocks of darkly stained regions at the centromeres of certain chromosomes (heterochromatic regions), large satellites of acrocentric chromosomes, and certain inversions (Table 22-1). Some chromosomal regions are prone to breakage and are
referred to as fragile sites. Most are clinically insignificant. The one major exception, fragile X, is described in detail in a later section.
CHROMOSOMAL ABNORMALITIES Most chromosomal abnormalities exert their phenotypic effects by increasing or decreasing the quantity of genetic material. Abnormalities can range from complete extra or missing chromosomes to small deletions or duplications.
FIGURE 22-4. Normal human karyotype.
546
Genetic, Metabolic, and Neurocutaneous Disorders / 22
With the discovery of genomic imprinting, it has become clear that inheritance of both copies of a chromosome from the same parent also can result in a phenotype. This section reviews the major classes of chromosomal abnormalities. Specific syndromes of neurologic interest are described later in the chapter.
Numeric Abnormalities The most straightforward of chromosomal abnormalities are alterations of chromosome number. Deviation from the normal diploid complement of 46 chromosomes is referred to as aneuploidy; an extra chromosome results in trisomy, whereas a missing chromosome constitutes monosomy. Although all of the possible chromosome trisomies have been observed in spontaneous abortions, trisomies 13, 18, and 21 are the only autosomal trisomies to be observed in a nonmosaic state in liveborns. All autosomal monosomies are lethal. The only viable monosomy involves the X chromosome (45,X, resulting in Turner’s syndrome). Aneuploidy results from an error in cell division referred to as nondisjunction, in which two copies of a chromosome go to the same daughter cell during meiosis or mitosis. Nondisjunction occurs most often in the first division of meiosis in the maternal germ line. Mitotic nondisjunction results in the presence of an aneuploid and a normal cell line—a condition referred to as mosaicism. The causes of nondisjunction are unknown. The only well-documented risk factor is maternal age. The term polyploidy refers to presence of a complete extra set of chromosomes: Triploidy represents three sets, with 69 chromosomes; tetraploidy represents four sets, or 92 chromosomes. Rarely, a triploid fetus will be liveborn, but in general, polyploidy is lethal. In a few instances, however, mosaicism for a diploid and a triploid cell line producing congenital anomalies has been compatible with long-term survival.
Deletions and Duplications Small deletions or duplications of chromosomal material result in increased or decreased gene “dosage.” Large deletions usually are lethal; monosomy for large chromosomal segments or entire chromosomes is not well tolerated. Application of FISH techniques has shown that a number of syndromes result from submicroscopic deletions. In these syndromes, groups of contiguous genes are thought to be removed, resulting in a defined set of congenital anomalies, as described later in this chapter. Deletion of genetic material from both ends of a chromosome can lead to fusion of the ends to form a ring-shaped structure. In addition to gene deletions, ring chromosomes tend to be unstable during cell division, resulting in some cells that lose the ring (and become monosomic for the chromosome) and others that have multiple copies of the ring.
Chromosome Inversions Inversions occur when there are two breaks in a chromosome and the intervening material flips 180 degrees. Inversions that span the centromere are referred to as pericentric, whereas those that do not are called paracentric.
Inversions generally do not result in added or lost genetic material and therefore usually are viewed as neutral changes. Disruption of a gene at one of the break points in the inversion, however, could upset function of that gene. Also, alteration of gene order at the borders of the inversion could affect the function of blocks of genes that are coordinately regulated (“position effect”). These considerations notwithstanding, usually chromosome inversions have no phenotypic effect. Crossing over within the inversion during meiosis may, however, result in deletions and duplications of chromosomal material. Although such an event in a paracentric inversion results in dicentric or acentric chromosomes that tend to be unstable, crossing over in a pericentric inversion can lead to genetically unbalanced but viable gametes.
Translocations Translocations involve the exchange of genetic material between chromosomes. In a balanced translocation the exchange is equal, with no loss or gain of genetic material. As with an inversion, it is possible for a gene to be disrupted at the point of exchange. Such a disruption has resulted, for example, in Duchenne muscular dystrophy in females with X-autosome translocations breaking the X within the dystrophin gene [Cockburn et al., 1992; Van Bakel et al., 1995]. More often, the carrier of a balanced reciprocal translocation is free of clinical signs or symptoms but is at risk for having offspring with unbalanced chromosomes. This risk is related to the nature of the products of segregation of the balanced translocation at meiosis. Aside from occasionally producing unbalanced gametes with 46 chromosomes, three of the four chromosomes involved in the meiotic configuration can segregate to the same germ cell (so-called 3:1 segregation), resulting after fertilization in 47 chromosomes including the rearranged chromosome. Some translocations involve three or more chromosomes. Chromosome painting can help identify the chromosomes that contribute to such a complex rearrangement. One specific type of translocation that is relatively common is the robertsonian translocation. This translocation results from a fusion of two acrocentric chromosomes (chromosomes 13, 14, 15, 21, or 22) at the centromeres. Carriers of a robertsonian translocation have 45 chromosomes and are clinically unaffected. The most common deleterious outcome is trisomy 21, in which a carrier for a robertsonian translocation involving chromosome 21 produces a gamete with both the translocation chromosome and a normal 21, resulting in trisomy 21 after fertilization. The risk for production of unbalanced gametes from a translocation carrier depends on the chromosomes involved, the specific break points of the translocation, and the gender of the carrier. Empirical data are available for some specific translocations [Daniel et al., 1989]. Risks include miscarriage and the birth of a liveborn child with congenital anomalies resulting from chromosome imbalance. The phenotype usually is a complex mixture of the results of loss or gain of at least two chromosome segments and therefore can be difficult to predict.
Marker Chromosomes A marker chromosome is defined as a chromosome with a centromere consisting of rearranged genetic material of
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
unknown origin. The prenatal incidence of supernumerary marker chromosomes (SMCs) is approximately 1 in 2500 live births, and 30% to 50% originate from chromosome 15 [Gardner and Sutherland, 1996]. In some cases, a marker will be a small bit of chromosome material almost at the limit of light microscopic resolution. Two thirds of de novo marker chromosomes can be associated with an abnormal outcome, whereas inherited ones can be passed from generation to generation without apparent clinical effects [Li et al., 2000]. Larger markers with more genetically active material are more likely to be of clinical significance. With the advent of FISH, the composition of marker chromosomes is increasingly likely to be defined, allowing these chromosomes to be characterized as derivative chromosomes resulting from translocations or other rearrangements.
Genomic Imprinting Although an individual normally receives a complete copy of autosomal genes from each parent, some genes are not expressed equally from the maternal and paternal genetic contributions. These genes are said to be imprinted [Driscoll et al., 1993; Hall, 1990; Sapienza, 1995]. The full complement of imprinted genes is not yet known, but several regions of the genome are known to include imprinted genes of clinical significance. Approximately 16 imprinted regions, each containing 1 to 10 genes, have been located to date [Lercher and Hurst, 2003]. Deletion of the expressed copy of an imprinted gene results in phenotypic effects, whereas deletion of the nonexpressed copy has no impact on development. Aside from deletion, another mechanism for genetic abnormality involving imprinted genes is uniparental disomy [Ledbetter and Engel, 1995]. Uniparental disomy is defined
547
as the inheritance of both copies of a chromosome from the same parent. Uniparental disomy likely results in most cases of “trisomy rescue,” in which a nondisjunction event occurs in a trisomic zygote, resulting in a return to a disomic karyotype. If the two retained chromosomes are from the same parent, the embryo, although having a normal chromosome number, will have uniparental disomy. Uniparental disomy also may occur in an embryo having trisomy because of a 3:1 disjunction of a balanced translocation. Major syndromes associated with imprinted genes are described in a later section of this chapter.
Cytogenetic Nomenclature Cytogeneticists describe findings of chromosomal analysis using a standardized system of nomenclature (International System of Cytogenetic Nomenclature). Detailed description of this system is beyond the scope of this chapter, but major terms used are listed in Table 22-2. The normal male karyotype is designated 46,XY, and the normal female karyotype is 46,XX. Any derivative chromosome is described after the sex chromosome constitution, and mosaic cell lines are separated by a slash (e.g., 46,XY/47,XY,+21 to designate mosaicism for trisomy 21).
CLINICAL APPROACH TO CHROMOSOMAL ABNORMALITIES Chromosomal analysis has been incorporated into the routine battery of tests available to the clinician. This section considers some of the more common indications for chromosomal analysis.
TABLE 22-2 Examples of Usage of Cytogenetic Nomenclature TERM
INTERPRETATION
46,XX 46,XY 47,XX,+21 46,XX/47,XX,+21 69,XXY 46,XY,inv(2)(p21q31)
Normal female karyotype Normal male karyotype Trisomy 21; “+” indicates additional chromosome, with specific chromosome identified Mosaic karyotype with normal and trisomy 21 cell line Triploid karyotype with XXY sex chromosome complement Male karyotype with inversion of chromosome 2, with break points at band p21 on short arm and band q31 on long arm (pericentric inversion) 46,XX,del(5)(p14) Male karyotype with deletion of short arm of chromosome 5, with break at band p14 46,XX,dup(1)(q22q25) Female karyotype with duplication of part of chromosome 1 between bands q22 and q25 on long arm 46,XX,r(7)(p22q36) Female karyotype with ring chromosome 7, with break points at p22 on the short arm and q36 on the long arm and fusion of the short and long arms into a ring structure 46,XY,t(2;5)(q21;q31) Male karyotype with balanced reciprocal translocation involving chromosomes 2 and 5, with break points at bands q21 and q31 on chromosomes 2 and 5, respectively 46,XX,der(1)(1;3)(p22;q13) Female karyotype with abnormal chromosome (“derivative chromosome”) with centromere of chromosome 1, resulting from segregation of a balanced translocation between chromosomes 1 and 3, with break points on 1 and 3 at bands p22 and q13, respectively 45,XX,der(13;21)(q10;q10) Female karyotype with robertsonian translocation representing fusion of chromosomes 13 and 21; balanced karyotype 46,XX,der(13;21)(q10;q10),+21 Female karyotype with robertsonian chromosome but with additional chromosome 21, resulting in trisomy 21 46,XX,add(19)(p13) Female karyotype with additional material of unknown origin attached to chromosome 19 at band p13 47,XY,+mar Male karyotype with additional chromosome of unknown origin (marker chromosome) 46,XX.ish del(22)(q11.2q11.2)(D22S75−) Female karyotype normal by standard cytogenetic analysis but with submicroscopic deletion at band 22q11.2 detected by FISH with probe D22S75 FISH, fluorescence in situ hybridization. Modified from Mitelman F, ed. An international system for cytogenetic nomenclature. Basel: S Karger, 1995.
548
Genetic, Metabolic, and Neurocutaneous Disorders / 22
Incidence of Chromosomal Abnormalities Estimates of the incidence of chromosomal abnormalities vary with the mode of ascertainment and the technology used for chromosomal analysis. In general, the incidence falls from conception to birth and then decreases with age after birth. The highest rates have been observed among products of conception from first-trimester spontaneous abortions. Upward of half of these conceptions demonstrated chromosomal abnormalities, most often triploidy or aneuploidy [Boue et al., 1973]. Estimates of incidence in the second trimester, based on results of amniocentesis, are higher than those at birth [Hook et al., 1983]. Jacobs and colleagues [1992] have estimated the frequency of balanced and unbalanced structural abnormalities in newborns based on the study of prenatal samples from 14,677 women. The frequency of unbalanced rearrangements was 0.061% and of balanced rearrangements, 0.522%.
Multiple Congenital Anomalies Genetic imbalance resulting from a chromosomal abnormality usually results in aberrant embryonic development. Most commonly this abnormal development involves multiple tissues, including the brain. Many specific syndromes can be recognized from a constellation of dysmorphic physical features and specific congenital anomalies. The clinician should be familiar with the most common syndromes, especially those resulting from trisomies 13, 18, and 21, as well as the sex chromosome aneuploidies (47,XXX, 47,XXY, and 45,X). Phenotypes resulting from duplication or deletion of smaller amounts of genetic material can be more difficult to identify clinically. Some of the more important syndromes are described in the next section. Some clues to the occurrence of a chromosomal abnormality are provided in Box 22-1. As a rule, chromosomal studies should be performed in a patient who exhibits congenital anomalies involving two or more tissues in whom a specific alternative diagnosis cannot be established and if the anomalies are not related to one another as cause and effect (e.g., hydrocephalus resulting from spina bifida).
Box 22-1 COMMON CLUES NEEDED FOR CHROMOSOMAL ANALYSIS Family History • Recurrent miscarriage • Infertility • Family history of congenital anomalies • Family history of balanced chromosome rearrangement Clinical Factors • Low birth weight/congenital microcephaly/dysmorphic features • Multiple congenital anomalies • Hemihypertrophy/significant body asymmetry • Pigmentary dysplasia (streaky hyper/hypopigmentation) • Infertility/delayed puberty • Unexplained developmental impairment
5qter 5pter
del(5)(pter) 5qter
FIGURE 22-5. Deletion of subtelomeric region of chromosome 5 demonstrated by fluorescence in situ hybridization. (Courtesy of A. Carroll, Birmingham, AL.)
Developmental Impairment In some chromosomal abnormalities, the phenotype is primarily that of developmental delay, with few or no congenital anomalies. Sometimes minor dysmorphic features are present, but these often are not noticed on routine examination. Fragile X syndrome and the presence of a supernumerary inverted duplication of chromosome 15 are examples. Chromosomal analysis and fragile X testing therefore should be considered in the evaluation of a child with unexplained developmental delay. Mental retardation is a common disorder that affects 1% to 3% of the population, and the cause is established in only 50% of the cases [Anderlid et al., 2002; Kriek et al., 2004]. Subtelomeric regions, localized proximal to the telomeres, are gene-rich regions. These subtelomeric regions have been found to be susceptible to chromosome changes (Fig. 22-5). It has been proposed that approximately 6% of the patients with idiopathic mental retardation have subtelomeric deletions or duplications [Flint, 1995]. These rearrangements can be detected by FISH analysis using subtelomeric probes [Anderlid et al., 2002].
Recurrent Miscarriage Chromosomal imbalance most often leads to miscarriage rather than to live birth. Carriers of balanced rearrangements, including translocations or inversions, may therefore come to attention through recurrent miscarriage [Flint and Gibb, 1996; Hook et al., 1989]. It is recommended that couples who have experienced two or more unexplained first trimester miscarriages be offered chromosomal analysis. Finding a balanced rearrangement permits genetic counseling of the couple, including offering prenatal diagnosis for future pregnancies. Other members of the family also may carry the balanced rearrangement and should be offered counseling and testing.
Prenatal Diagnosis Chromosomal analysis of a developing fetus can be achieved through collection of fetal cells by chorionic villus biopsy
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
(CVS), amniocentesis, or peripheral umbilical blood sampling (PUBS) [D’Alton and DeCherney, 1993]. CVS involves sampling part of the fetal placenta using a biopsy device either passed through the cervix or inserted by a needle through the mother’s abdomen [Pijpers et al., 1988; Smidt-Jensen and Hahnemann, 1988]. It is performed at 10 to 12 weeks of gestation. CVS offers the advantage of early testing, with results available before the pregnancy is obvious. Early testing provides more privacy to the couple if termination of pregnancy is elected, as well as resolution at an earlier point in the pregnancy. The complication rate is estimated at around 1%. There is evidence that performance of CVS before 10 weeks is associated with an increased risk of limb or orofacial anomalies [Froster and Jackson, 1996; Holmes, 1993]. Amniocentesis involves sampling amniotic fluid at 16 to 18 weeks of gestation. Fetal cells in the fluid are cultured and can be used for chromosomal analysis. The complication rate is approximately 0.5%. Some centers offer earlier testing at 14 weeks [Johnson et al., 1996; Wilson et al., 1997]. PUBS is offered after 20 weeks of gestation and involves sampling fetal blood by nicking the umbilical vein under ultrasound guidance. Single cell analysis also is possible using FISH, and has been applied to preimplantation diagnosis of trisomy or familial translocation [Sermon et al., 2004]. Indications for prenatal testing are listed in Box 22-2. General practice is to offer prenatal testing for pregnancies in which the risk of a chromosomal abnormality exceeds the risk of a complication of the procedure. For couples in which one partner carries a chromosome rearrangement, prenatal testing to detect unbalanced chromosomes can be offered. The actual risk of unbalanced chromosomes in the pregnancy depends on the nature of the rearrangement but generally is greater than 1%. The laboratory performing the prenatal testing must be informed of the details of the rearrangement, to ensure that subtle changes are detected. The recurrence risk for future trisomy for a couple who have had one pregnancy affected with trisomy is approximately 1% [Lister and Frota-Pessoa, 1980]. This risk is irrespective of the particular chromosome involved in the trisomy. The risk of trisomy rises with maternal age; it is standard to offer prenatal testing to women who will be 35 years of age or older at the time of delivery. Pregnancies are increasingly being monitored for fetal anomalies by ultrasound or maternal serum screening.
Box 22-2 COMMON INDICATIONS FOR PRENATAL CYTOGENETIC DIAGNOSIS • Parent is carrier of balanced chromosome rearrangement • Advanced maternal age (older than 35 years of age at time of delivery) • Abnormality on ultrasound examination • Congenital anomaly • Short femur/thickened nuchal skin (indications of trisomy 21) • Echogenic bowel • Maternal serum screen indicative of increased risk of trisomy 21 or 18
549
Ultrasound studies may identify a congenital anomaly or a feature, such as thickening of nuchal folds or short femur, each of which tends to be associated with chromosomal abnormalities [Bahado-Singh et al., 1995; Nyberg et al., 1990]. Maternal serum screening for α-fetoprotein, human chorionic gonadotropin (hCG), and unconjugated estriol can determine increased risk for trisomy 21 or trisomy 18 [Canick, 1990; Kloza, 1990; Knight and Palomaki, 1990; Staples et al., 1991]. Although such screening tests have relatively high frequencies of false-negative and falsepositive results, they can identify pregnancies for which further prenatal testing may be helpful. Integrated first- and second-trimester screening that uses both ultrasound technology and extended serum screening has been developed; with this approach, the false-positive rate has decreased and the detection rate for Down syndrome has increased in comparison with rates with second-trimester analyte screening alone [Fergal et al., 2003].
Chromosomes and Malignancy Genetic studies have revealed that cancer cells acquire their abnormal properties through a series of changes in the genetic information. These changes include gene mutations and chromosome rearrangements. The chromosome rearrangements result in abnormal gene dosage because of deletion or duplication, or in juxtapositions of genetic material that alter gene regulation. Consideration of the various genes that are involved in malignancy, many of which constitute oncogenes, is beyond the scope of this chapter. In several instances, however, specific chromosomal rearrangements have been associated with particular cancers. Chromosomal analysis can be helpful in these disorders to provide diagnostic information, to assess appropriate treatment and prognosis, and to follow response to therapy.
SPECIFIC CYTOGENETIC SYNDROMES Polyploidy Cytogenetics Tetraploidy is an infrequent chromosomal abnormality, but triploidy occurs fairly often. Most triploid embryos miscarry in the first trimester. In approximately 20% of first-trimester spontaneous abortions the conceptus is found to have a triploid karyotype. Liveborn infants with triploidy exhibit multiple congenital anomalies and rarely survive the newborn period. Those that do usually are mosaics (sometimes referred to as mixoploids, because diploid and triploid cell lines may arise from separate fertilizations) for a diploid and a triploid cell line.
Clinical Features The triploid phenotype is distinct and easily recognized [Philipp et al., 2004; Wertelecki et al., 1978]. Polyhydramnios or preeclampsia may complicate the pregnancy. The placenta may be large, and hydatidiform changes may be seen. Birth weight usually is low. Syndactyly involving
550
Genetic, Metabolic, and Neurocutaneous Disorders / 22
the third and fourth digits is characteristic. Craniofacial features include low-set, malformed ears, hypertelorism, and micrognathia. Cardiac, renal, and central nervous system malformations are common. Males may have dysplastic external genitalia. Recent studies of the parental origin of the three chromosome sets in triploidy have revealed that a majority of affected persons have two maternal sets, perhaps because of more frequent survival to term of triploid fetuses with two maternal sets of chromosomes (digynic triploids) [McFadden et al., 1993; Miny et al., 1995]. Long-term survivors often are mosaics and may have less obvious phenotypic features [Carakushansky et al., 1994]. Body asymmetry and pigmentary dysplasia may be clues to chromosomal mosaicism in general, including, in some cases, triploidy [Woods et al., 1994].
Management Most triploid fetuses are spontaneously aborted or are stillborn. Most liveborn infants with full triploidy die in the early days of life. Survivors require supportive care for their congenital anomalies and developmental impairment.
Aneuploidy Only a minority of aneuploid embryos survive to term; the rest miscarry, usually in the first trimester. Only the most common trisomy and monosomy syndromes compatible with live birth are considered in the following discussion.
Trisomy 13 (Patau’s Syndrome) Cytogenetics Trisomy 13 occurs in approximately 1 in 10,000 live births [Wyllie et al., 1994]. A majority of affected persons have 47 chromosomes, with an extra copy of chromosome 13. Approximately 25% have trisomy because of translocation between 13 and another acrocentric chromosome, usually chromosome 14 (robertsonian translocation). Mosaicism
occurs in a small proportion of cases and may ameliorate the phenotype. Duplication of part of chromosome 13 resulting from unbalanced translocation can result in abnormal phenotypic features, although not necessarily similar to those seen in full trisomy 13.
Clinical Features Trisomy 13 is associated with congenital anomalies involving most major organ systems (Fig. 22-6). Holoprosencephaly is the hallmark central nervous system anomaly [Moerman et al., 1988], occurring in about 80% of cases. Incomplete division of the cerebral hemispheres and basal ganglia may be present in various degrees. The optic nerves and chiasm may be hypoplastic. Olfactory bulbs usually are absent. The abnormalities may include cerebellar hypoplasia and Arnold-Chiari malformation. Infants with trisomy 13 who demonstrate holoprosencephaly usually have accompanying craniofacial anomalies. The eyes may be set closely together (hypotelorism) or even fused in a single orbit (cyclopia). Other ocular anomalies include microophthalmia, iris colobomata, cataracts, and retinal dysplasia. Premaxillary agenesis and cleft lip or palate also may be present. Ulcer-like defects in scalp skin (cutis aplasia) occur commonly. Limb anomalies include postaxial polydactyly in two thirds of patients and rocker-bottom foot. Congenital heart defects, especially ventricular septal defect (VSD), are common, as are renal anomalies, including cystic dysplasia. The phenotype overlaps to some degree with that of MeckelGruber syndrome (encephalocele, polydactyly, polycystic kidney), inherited as an autosomal-recessive trait. This overlap underlines the importance of confirming the clinical diagnosis of trisomy 13 by chromosomal analysis.
Management Few infants with trisomy 13 survive the newborn period, with apnea being the most common cause of death [Rasmussen et al., 2003; Wyllie et al., 1994]. Often the anomalies are too numerous and severe to be corrected. In
FIGURE 22-6. Newborn with trisomy 13. (Karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
the absence of life-threatening malformations, however, long-term survival has been well documented, albeit with severely impaired cognitive function [Baty et al., 1994a, 1994b].
Trisomy 18 (Edwards’ Syndrome) Trisomy 18 affects approximately 1 in 8000 live births. It is virtually always associated with a 47-chromosome karyotype, although a small proportion of affected newborns have a mosaic karyotype. Segregation of a parental balanced translocation may result in trisomy for part of the short or long arm of chromosome 18. Molecular analysis has revealed that most nondisjunction events that lead to trisomy 18 occur in maternal meiosis [Kupke and Müller, 1989].
Clinical Features Infants with trisomy 18 have low birth weight and microcephaly [Marion et al., 1988]. Other common features include a prominent occiput, low-set “simple” ears, and a small mouth (Fig. 22-7). Hands usually are tightly clenched in a characteristic configuration, with the fourth and fifth fingers overlapping the first and second. Terminal phalanges often are hypoplastic, and rocker-bottom foot may be present. Congenital heart defects, particularly redundancy of valve leaflets, occur in most cases [Balderston et al., 1990; Van Praagh et al., 1989]. Renal anomalies also are common. Brain malformations include heterotopias, agenesis of the corpus callosum, Dandy-Walker malformation, and ArnoldChiari malformation [Moerman et al., 1982]. Infants commonly are jittery and hypertonic and have apnea and seizures. Pigmentary dysplasia has been described in persons with mosaic trisomy 18 [Ohashi et al., 1992].
551
Management No definitive treatment exists for trisomy 18. Most affected infants die in the neonatal period [Embleton et al., 1996; Rasmussen et al., 2003]. Long-term survivors have developmental impairment and require supportive care [Root and Carey, 1994].
Trisomy 21 (Down Syndrome) Trisomy 21 is the most common and widely recognized of the autosomal trisomy syndromes. It occurs in approximately 1 in 700 live births, with a striking increase in frequency with advanced maternal age [Epstein, 1995; Hook and Cross, 1989]. The frequency of Down syndrome at birth may be lower in areas in which prenatal screening and testing are offered. Prenatal diagnosis is offered to women who will be older than 35 years of age at the time of delivery, and up to 60% of pregnancies at risk can be identified by second-trimester maternal serum screening. Full trisomy 21 occurs in about 95% of cases [Mutton et al., 1996]. Most of these result from nondisjunction in the first division of maternal meiosis [Antonarakis and Down Syndrome Collaborative Group, 1991]. Translocation, usually between chromosome 21 and another acrocentric chromosome, most often chromosome 14, is identified in approximately 4%. These are robertsonian translocations. A parent who carries such a translocation while having 45 chromosomes may be at risk for recurrence of Down syndrome in offspring. Rarely, patients with clinical Down syndrome have only a partial trisomy of 21. The analysis of these rare cases suggested the existence of a critical region for Down syndrome (21q22.1-q22.3). Another chromosomal region on proximal 21q also may be responsible for Down FIGURE 22-7. Patient with trisomy 18 at 7 years of age. (Karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
552
Genetic, Metabolic, and Neurocutaneous Disorders / 22
syndrome features [Antonarakis, 1998]. The remaining 1% of affected persons have a mosaic karyotype. The pathogenesis of the features of Down syndrome is attributed to increased dosage of genes on chromosome 21. The levels of gene expression apparently are tightly regulated, with increased levels of expression leading to aberrant development. Efforts are under way to identify specific genes responsible for specific components of the Down syndrome phenotype. New evidence indicates that dysregulation of several neuronal genes occurs in Down syndrome [Bahn et al., 2002]. One gene, called minibrain, has been localized to a region of chromosome 21 and may be involved in the cognitive phenotype [Hammerle et al., 2003; Smith et al., 1997].
Clinical Features Down syndrome consists of a set of characteristic physical features and developmental impairment (Fig. 22-8) [Cooley and Graham, 1991; Jackson et al., 1976; Preus, 1977]. Short stature and brachycephaly are characteristic, and mild microcephaly may be noted. Down syndrome growth charts are available and should be used to monitor growth in affected children [Cronk et al., 1988]. Craniofacial features include upslanted palpebral fissures, epicanthal folds, flat facial profile, and small, low-set ears with narrow ear canals. White speckles (Brushfield spots) may be seen on the iris.
A common finding is redundant folds of nuchal skin, which is one of the markers used for prenatal diagnosis by ultrasound examination [Gray and Crane, 1994]. Fingers are short, with incurving of the fifth finger (clinodactyly) and, often, a single transverse palmar crease. A wide space between the first and second toes is a frequent finding. The hallmark neurologic feature of Down syndrome is hypotonia. No gross central nervous system (CNS) malformation is consistently seen, although lack of normal growth of the brain is typical [Lott, 1986; Lott and Richardson, 1981]. Microscopic analysis has revealed impaired myelination, reduced density of neurons, malformed dendritic trees and spines, defective lamination of the cortex, and abnormality of synaptic density [Golden et al., 1994; Wisniewski, 1990]. Impaired neurologic development is a universal feature, but the degree of impairment varies widely [Pueschel et al., 1987]. Children with Down syndrome benefit from early intervention, physical therapy, and being reared in a family setting [Gath, 1981, 1990; Gath and Gumley, 1984]. An increased frequency of psychiatric problems, such as depression and behavioral problems including hyperactivity, disruptive behaviors, and repetitive behaviors, has been documented [Gath and Gumley, 1986; Myers and Pueschel, 1991; Pueschel et al., 1991]. Linguistic ability may be impaired out of proportion to cognitive impairment [Kernan, 1990; Kernan and Sabsay, 1996]. Seizures, including infantile spasms, may be seen with increased frequency but often FIGURE 22-8. A, Newborn with trisomy 21 (Down syndrome). B, Boy with Down syndrome at 12 years of age. (Karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
A
B
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
553
are related to medical complications or their treatment [Pueschel et al., 1991; Stafstrom et al., 1991]. An increased frequency of dementia, associated with pathologic changes of Alzheimer’s disease, has been described in patients with Down syndrome [Iwatsubo et al., 1995; Johannsen et al., 1996; Lai and Williams, 1989; Schupf et al., 1996]. This increased frequency may be accounted for, at least in part, by increased expression of the amyloid precursor protein, the locus for which is on chromosome 21 [Cataldo et al., 2003; Teller et al., 1996]. Congenital anomalies commonly associated with Down syndrome include heart and gastrointestinal defects. The most typical heart defect is common atrioventricular (AV) canal, although other anomalies, such as VSD or tetralogy of Fallot, may be seen [Marino et al., 1990]. Gastrointestinal malformations include duodenal atresia and Hirschsprung’s disease.
Nutritional supplementation has been recommended for children with Down syndrome, although the benefits are not clearly documented. Some encouraging results have been reported in clinical trials with the anticholinesterase inhibitor donepezil in management of dementia in patients with Down syndrome [Lott et al., 2002]. Parents of children with Down syndrome should be counseled regarding the natural history of the disorder, opportunities for intervention, and genetic recurrence risks and should be provided emotional support. Life expectancy for persons with Down syndrome has improved with advances in surgery and medical treatment of complications of the disorder. Survival into the seventh decade is not unusual [Baird and Sadovnick, 1989].
Management
The only other autosomal trisomy compatible with live birth is trisomy 8. Even this is lethal in utero, except as a mosaic karyotype [Kurtyka, 1988]. Phenotypic features include hypertelorism; camptodactyly and other joint contractures; long, slender habitus; absence of patellae; and deep creases of the palms and soles (Fig. 22-9). Asymmetric growth, presumably due to chromosomal mosaicism, also may be a feature.
The American Academy of Pediatrics has published guidelines for management of children with Down syndrome [American Academy of Pediatrics Committee on Genetics, 2001]. Children with Down syndrome frequently require surgery for correction of congenital anomalies, such as heart defects or gastrointestinal malformations. They have a markedly increased risk of respiratory infection, often requiring antibiotic treatment. The frequency of leukemia is increased in children with Down syndrome. Transient leukemoid reactions also may occur. Children with Down syndrome are at risk for atlantoaxial dislocation. Whether screening for dislocation should be offered for children with Down syndrome, particularly those who will participate in sports activities, has been the subject of controversy [American Academy of Pediatrics Committee on Sports Medicine and Fitness, 1995; Cremers et al., 1993; Morton et al., 1995; Risser et al., 1995]. All children with Down syndrome should be monitored for neurologic signs of cervical cord compression. The American Academy of Pediatrics recommends obtaining radiographs once during the preschool years for this purpose.
Trisomy 8
Turner’s Syndrome Cytogenetics Turner’s syndrome is associated with a 45,X karyotype, with a single X chromosome. Mosaicism is not uncommon, however, with a separate cell line containing either a normal 46,XX or XY karyotype, or 46 chromosomes including a structurally rearranged X or Y [Crocker, 1992; Hassold et al., 1988; Jacobs et al., 1990; Kuznetzova et al., 1995]. Unlike in other aneuploidy syndromes, the frequency of Turner’s syndrome does not increase with advancing maternal age [Warburton et al., 1997]. FIGURE 22-9. A and B, Patient with trisomy 8 at 18 months of age. C, Same patient with trisomy 8 at 18 years of age. Note the deep palmar and plantar creases that are commonly seen in these patients. (Karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
A
B
C
554
Genetic, Metabolic, and Neurocutaneous Disorders / 22 FIGURE 22-10. Girl with Turner’s syndrome: A, at 9 years of age; B, at 1 month of age; and C, at birth. (Courtesy of K. Khoury; karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
B A
C
Clinical Features Patients with Turner’s syndrome typically have a female phenotype, although those with a cell line including a Y chromosome may have some degree of virilization, often with ambiguous genitalia. At birth, infants may manifest pedal edema or diffuse edema (Fig. 22-10). Facial features include small mandible, narrow maxilla, and epicanthal folds. In older children and adults with Turner’s syndrome, short stature and webbing of the neck commonly are seen. The thorax is broad, with increased distance between the nipples. Extremity findings include cubitus valgus, short fourth metacarpal and metatarsal bones, and narrow or hyperconvex nails. Often multiple pigmented nevi are present on the skin. Congenital anomalies include anomalies of the lymphatic system, cardiac defects, especially coarctation of the aorta and bicuspid aortic valve, and renal anomalies, such as horseshoe kidney. Although mental retardation is rare, delays in both gross and fine motor development are common in females with Turner’s syndrome [Bender et al., 1993; Nijhuis van der Sanden et al., 2003; Salbenblatt et al., 1989]. Some patients display cognitive problems, but difficulties with visuospatial perception are most common [Bender et al., 1984; Pennington et al., 1982]. Hearing impairment is common and children should be monitored for deficits or progression of impairment.
have demonstrated increased growth with administration of growth hormone [Cianfarani et al., 1994; Ranke, 1995; Rocchiccioli et al., 1995]. Turner’s syndrome typically is associated with the presence of a streak gonad, lack of secondary sexual development, and infertility. Referral to an endocrinologist for hormonal induction of puberty should be done at an appropriate age [Hanton et al., 2003]. Intraabdominal gonads in patients with Turner’s syndrome who have a Y chromosome are at risk of transformation into gonadoblastoma and therefore should be removed.
Management
The diagnosis of Klinefelter’s syndrome usually is not suspected at birth. Affected males tend to be tall, with long limbs (Fig. 22-11). They display hypogonadism, and virilization may be incomplete at puberty; gynecomastia develops in some patients. Azoospermia and infertility are characteristic [Yoshida et al., 1997]. As in Turner’s syndrome, mental retardation is not a typical feature of Klinefelter’s syndrome, but learning disabilities, neuromotor developmental delay [Salbenblatt et al., 1987], and behavioral
Recommendations for diagnosis and management of Turner’s syndrome have been published [Rosenfeld et al., 1994; Seashore et al., 1995]. Newborns should be evaluated for renal and cardiac defects and monitored if these are found. Thyroid autoimmunity may a feature, so monitoring of thyroid function is required. Although not all children with Turner’s syndrome are growth hormone deficient, some
Klinefelter’s Syndrome Cytogenetics Klinefelter’s syndrome occurs in about 1 in 3000 males and is associated with a 47,XXY karyotype. The incidence increases as a function of maternal age [Carothers and Filippi, 1988]. Rare patients may have multiple X chromosomes (e.g., 48,XXXY or 49,XXXXY). Usually the presence of multiple X chromosomes in such persons is associated with more severe cognitive impairment.
Clinical Features
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
555
physical stigmata are absent. XYY is associated with a male phenotype and tall stature but no other physical features. Learning disabilities and neuromotor impairment occur commonly in 47,XXX females [Bender et al., 1983, 1989, 1993, 1995; Pennington et al., 1982; Salbenblatt et al., 1989]. The behavioral phenotype of XYY syndrome has been a source of some controversy because of reports associating the karyotype with criminal behavior. The frequency of learning disabilities and behavioral problems is increased among affected males, although a wide range of cognitive outcomes have been reported [Fryns et al., 1995; Robinson et al., 1979].
Structural Abnormalities
FIGURE 22-11. Boy with Klinefelter’s syndrome at age 13 years. (Courtesy of K. Khoury; karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
problems [Salbenblatt et al., 1981] are common. Receptive and expressive language problems also have been reported [Bender et al., 1983; Pennington et al., 1982].
Management Children with Klinefelter’s syndrome require support at home and school for learning and behavioral problems. Testosterone is administered, beginning in adolescence, to improve secondary sexual development.
Other Sex Chromosome Aneuploidies Two other major sex chromosome aneuploidies are 47,XXX and 47,XYY. The XXX aneuploidy is associated with a female phenotype and tall stature; usually other major
Structural abnormalties of chromosomes cause phenotypic effects resulting from deletions or duplications of genetic material. In some cases, these occur sporadically as a result of de novo chromosome rearrangements, whereas in others, they may be inherited as a consequence of segregation of a familial balanced translocation. Major structural abnormalities began to be recognized in the early days of clinical cytogenetics, with several syndromes identified between 1960 and 1970. The advent of chromosome banding led to a second wave of discovery of syndromes resulting from more subtle rearrangements. More recently, the application of FISH has further increased the resolution of cytogenetic analysis and revealed a chromosomal basis for a group of “microdeletion syndromes” [Dallapiccola et al., 1995]. Some small deletion or duplication syndromes are fairly well characterized in terms of phenotypic effects and may be recognized clinically. Clinical diagnosis often is complicated, however, by a number of factors. First, most of these syndromes are exceedingly rare and are much less common than the trisomy syndromes. Second, the exact extent of deleted or duplicated material may differ from one affected child to another, leading to subtle but important variation in clinical manifestations. Third, many of these syndromes are seen as a consequence of malsegregation of a familial balanced translocation. The usual consequence is imbalance of two or more
TABLE 22-3 Important Deletion/Duplication Syndromes ABNORMALITY
CLINICAL FEATURES
CNS INVOLVEMENT
REFERENCE
Deletion terminal short arm chromosome 1 Deletion 4p (Wolf-Hirschhorn syndrome) Deletion 5p (cri du chat syndrome)
Developmental delay, seizures
Shapira et al., 1997
Developmental delay, seizures
Estabrooks et al., 1995
Hypotonia, developmental delay
Overhauser et al., 1994
Developmental delay
Wilson et al., 1985
Hypertonia, developmental delay
Huret et al., 1988
Holoprosencephaly, developmental delay
Brown S, et al., 1993
Inverted duplicated 15
Minor dysmorphic features (hypertelorism, cleft lip) Cleft lip, hypertelorism, microcephaly, growth retardation Low birth weight, catlike cry, microcephaly, hypertelorism Growth retardation, microcephaly, hypertelorism, brachydactyly Metopic suture synostosis (trigonocephaly), upslanting palpebral fissures Microcephaly, high nasal bridge, hypertelorism; risk of retinoblastoma if q14 deleted No characteristic dysmorphism
Cheng et al., 1994
Deletion 18p
Growth retardation, hypertelorism
Deletion 18q
Growth retardation, midface hypoplasia, microcephaly
Developmental delay, autistic features Holoprosencephaly, developmental delay Developmental delay, behavioral problems
Trisomy 9p Deletion 9p Deletion 13q
CNS, central nervous system.
Schinzel et al., 1974 Kline et al., 1993
556
Genetic, Metabolic, and Neurocutaneous Disorders / 22
TABLE 22-4 Major Microdeletion Syndromes SYNDROME
MAJOR FEATURES
CHROMOSOME REGION
REFERENCE(S)
Monosomy 1p36
Severe psychomotor retardation, microcephaly, seizures, facial anomalies, and visual impairment Low-set malformed ears, digital anomalies, congenital heart defects Pre- and postnatal onset of growth retardation, microcephaly, characteristic facial appearance, seizures, unusual palmar creases, developmental delay Characteristic facies, supravalvar aortic stenosis, developmental impairment Exostoses, abnormal facies, developmental delay
1p36
Zenker et al., 2002
2q23q24.3
Mass et al., 2000
4p16
Clemens et al., 1998
7q11.23 elastin locus
Lowery et al., 1995
8q24.1 11p11.2
Prader-Willi syndrome
Multiple exostoses, biparietal foramina, minor craniofacial abnormalities, mental retardation Wilms’ tumor, aniridia, genitourinary dysplasia, mental retardation Retinoblastoma, mental retardation Hypotonia, blepharophimosis, ptosis, bulbous nose, long philtrum, upturned corners of mouth, mild developmental delay Hypotonia, developmental delay, obesity
Hou et al., 1995; Lüdecke et al., 1995 Hall et al., 2001
Angelman’s syndrome
Seizures, abnormal movements, mental retardation
15q12 UBE3A/E6-AP gene mutations
Interstitial 15q21 deletion
Mental retardation, growth retardation, beak-like nose with hypoplastic alae nasi, thin upper lip α-Thalassemia, mental retardation Microcephaly, characteristic facies, mental retardation Mental retardation, characteristic facies Lissencephaly, characteristic facies Peripheral neuropathy
15q21.1-q21.3
Knoll and Lalande, 1993 Kishino et al., 1997; Knoll and Lalande, 1993; Matsuura et al., 1997 Liehr et al., 2004
16p13.3 16p13.3 17p11.2 17p13.3 CMT: dup(17p12) HSPP: del(17p12)
Wilkie et al., 1990 Breuning et al., 1993 Greenberg et al., 1996 VanTuinen et al., 1988 Chance and Fischbeck, 1994
Intrahepatic biliary atresia, growth retardation, pulmonic stenosis, unusual facial features
20p11.2 Notched gene
Diamond-Blackfan anemia (DBA), mental retardation, skeletal malformations Cleft palate, conotruncal cardiac malformations, DiGeorge sequence (absent thymus, parathyroids), schizotypal and mood disorders Ichthyosis, anosmia
19q13.2
Li et al., 1997; Oda et al., 1997; Rand et al., 1995 Tentler et al., 2000
Ocular abnormalities, pathognomonic linear skin defects Mixed conductive sensorineural deafness, atypical Mondini-like dysplasia, dilated petrous facial canal and auditory meatus, large cochlear canal, wide posterior bulbous labyrinth
Interstitial 2q23 deletion Pitt-Rogers-Danks syndrome
Williams’ syndrome Langer-Giedion syndrome Potocki-Shaffer syndrome WAGR syndrome Retinoblastoma/mental retardation 14q terminal deletion
α-Thalassemia/mental retardation Rubinstein-Taybi syndrome Smith-Magenis syndrome Miller-Dieker syndrome Charcot-Marie-Tooth disease (CMT) type IA/hereditary susceptibility to pressure palsies (HSPP) Alagille’s syndrome 19q13 microdeletion DiGeorge’s/velocardiofacial syndrome Steroid sulfatase deficiency/ Kallmann’s syndrome Xp deletion syndrome X-linked progressive mixed deafness
distinct chromosome regions, resulting in a set of anomalies that combine the phenotypic effects of both segments. Some of the more common or clinically important deletion or duplication syndromes are summarized in Table 22-3. The microdeletion syndromes constitute a relatively recent addition to the list of disorders caused by chromosomal imbalance (Table 22-4). Most had been previously recognized as clinical entities, usually occurring sporadically and of unknown cause. In general, standard chromosomal analysis in persons with these syndromes is unrevealing. In rare instances, however, a chromosome deletion or other rearrangement drew
11p13 13q14 14q32.31-qter 15q12
Gessler et al., 1989; Rose et al., 1990 Janson et al., 1990 van Karnebeek et al., 2002
22q11
Arnold et al., 2001; Lindsay et al., 1995
Xp22.3
Ballabio et al., 1989
Xp22.3 Xq21
Paulger et al., 1997 Piussan et al., 1995
attention to a specific chromosome region, which was then subjected to further study using molecular techniques, especially FISH. This process has revealed deletions of chromosomal material in other persons with the same disorders but with chromosomal defects below the limits of resolution of the light microscope [Gopal Rao et al., 1995]. The clinical phenotypes of microdeletion syndromes may be explained in two ways. First, many of these are “contiguous deletion syndromes.” That is, a cluster of closely linked genes are simultaneously deleted, leading to a complex phenotype that reflects the contributions of multiple genes.
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
Specific components of the phenotype may be present or absent in any given case, depending on the extent of deletion. This mechanism is operative, for example, in the WAGR (Wilms’ tumor, aniridia, genitourinary dysplasia, and mental retardation) association, occurring with deletion of a region on the short arm of chromosome 11 [Gessler et al., 1989]. Depending on the extent of deletion, features may include Wilms’ tumor, aniridia, genitourinary anomalies, and developmental impairment, or some combination of these features. The second mechanism is that deletion results in altered or absent expression of one critical gene in the region that itself leads to a complex phenotype. Deletion is likely to be one of many mechanisms of mutation of the gene; thus, FISH analysis will not reveal the deletion in all affected persons. This mechanism accounts for Rubinstein-Taybi syndrome [Breuning et al., 1993], Angelman’s syndrome [Matsuura et al., 1997], and Alagille’s syndrome [Li et al., 1997; Oda et al., 1997; Rand et al., 1995]. These two mechanisms, of course, are not mutually exclusive. Deletion of a major gene may account for much of a particular phenotype, but deletion of contiguous genes may contribute additional phenotypic features in some patients.
Imprinting Disorders The recognition of the phenomenon of genomic imprinting has led to the discovery of a new class of genetic disorders
A
557
B
FIGURE 22-12. Boy with Prader-Willi syndrome: A, at 7 months of age; B, at 6 years of age. (Karyotype courtesy of M.G. Mattei, Marseilles, France.)
FIGURE 22-13. Boy with Angelman’s syndrome at 6 years of age. (Karyotype courtesy of M. Rochon, Sherbrooke, Quebec, Canada.)
558
Genetic, Metabolic, and Neurocutaneous Disorders / 22
associated with aberrations of imprinted genes. The prototype disorders are Prader-Willi and Angelman’s syndromes (Figs. 22-12 and 22-13). The features of these syndromes are described in Table 22-5. Although distinct from one another clinically, both have been found to be associated with deletions of the same region of chromosome 15 in about two thirds to three fourths of cases [Knoll and Lalande, 1993]. How this could account for such different phenotypic effects was a mystery until it was found that deletions resulting in PraderWilli syndrome invariably are of the paternal copy of the chromosome region, whereas maternal deletions occur in Angelman’s syndrome [Donlon, 1988; Knoll et al., 1989]. Most patients with Prader-Willi syndrome who do not have deletions have uniparental disomy for chromosome 15, with two maternal copies and no paternal 15 [Woodage et al., 1994]. Either mechanism—deletion or uniparental disomy— leads to deficiency of a gene or genes on chromosome 15 that are expressed in the paternal but not the maternal chromosome. Paternal uniparental disomy accounts for a low percentage of cases of Angelman’s syndrome [Nicholls et al., 1992; Saitoh et al., 1994]. Mutations in the UBE3A/E6-AP gene, located at 15q11.2, have been found in some patients with Angelman’s syndrome [Kishino et al., 1997; Matsuura et al., 1997]. This gene is imprinted in the brain [Albrecht et al., 1997; Rougeulle et al., 1997] and is the gene responsible for the Angelman syndrome phenotype. No single gene has so far been implicated in the pathogenesis of Prader-Willi syndrome. A small proportion of patients with Prader-Willi or Angelman’s syndrome may have a small deletion or other mutation that leads to aberrant imprinting of the region [Buiting et al., 1995]. These findings have led to major advances in genetic diagnosis of Prader-Willi and Angelman’s syndromes.
Chromosome 15 deletions usually are submicroscopic but are easily detected by FISH [Bettio et al., 1995; Delach et al., 1994; Dewald et al., 1996; Smith et al., 1995]. Defects in imprinting or uniparental disomy can be identified by studies of patterns of DNA methylation in the region [Beuten et al., 1996; Buiting et al., 1994; Dittrich et al., 1996; GillessenKaesbach et al., 1995; Monaghan et al., 1997; Van den Ouweland et al., 1995; Zeschnigk et al., 1997]. One particular cloned segment of DNA is methylated in the maternal but not the paternal genome. Failure to identify the methylated or nonmethylated copy of the sequence is indicative of deletion, uniparental disomy, or a mutation that alters the imprinting mechanism. Although the full extent of imprinted genes is not yet known, a growing list of clinical disorders have been found to be associated with imprinted regions (Table 22-6) [Ledbetter and Engel, 1995]. TABLE 22-6 Chromosome Regions Known to Include Imprinted Genes and Disorders Associated with Deletions or Uniparental Disomy for These Regions Chromosome Region
Disorder
15q11-q13
Prader-Willi syndrome or Angelman’s syndrome (see Table 22-5) Beckwith-Wiedemann syndrome (macrosomia, omphalocele, macroglossia, hemihypertrophy) Short stature (Russell-Silver syndrome) Short stature, developmental delay
11p 7q 14
TABLE 22-5 Comparison of Features of Prader-Willi and Angelman’s Syndromes Feature
Prader-Willi Syndrome*
Angelman’s Syndrome†
Diagnostic criteria
Major clinical criteria Neonatal hypotonia Feeding problems in infancy Rapid weight gain between 1 and 6 years of age Characteristic facies Hypogonadism Developmental delay Hyperphagia Minor criteria Decreased fetal movement Characteristic behaviors Sleep disturbances Short stature Small hands Narrow hands Esotropia/myopia Thick, viscous saliva Speech articulation defects Skin picking Supportive findings High pain threshold Decreased vomiting 70% to 75% deletion 15q11-q13 paternal sequence 20% to 25% maternal disomy Unknown
Consistent features (100%) Developmental delay Speech impairment Movement disorder (ataxia of gait, tremulous movement of limbs) Behavioral features: frequent laughter or smiling, hand flapping Frequent features (80%) Acquired microcephaly Seizures (usually in patients younger than 3 years) Abnormal EEG (high-amplitude 2- to 3-Hz spike-wave discharges) Associated features (20% to 80%) Flat occiput, occipital groove Protruding tongue Prognathism Wide mouth and widely spaced teeth Drooling, chewing, mouthing movements Strabismus Hypopigmentation Brisk lower limb deep tendon reflexes Sleep disturbance
Cytogenetic Uniparental disomy Gene
*Data from Holm V, et al. Pediatr 1993;91:398. †Data from Williams CA, et al. Am J Med Genet 1995;56:237. EEG, electroencephalogram.
65% to 75% deletion 15q11-q13 maternal sequence 2% paternal disomy Mutations in UBE3/E6-AP on chromosome 15
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
559
Fragile X Syndrome
TABLE 22-7
Fragile X syndrome often is considered along with chromosomal disorders, because fragility of the distal region of the X chromosome is a marker of the disorder. The condition is known to be the result of a mutation of a specific gene on the X chromosome, with the fragility of the X chromosome being a consequence of the nature of the mutation.
Number of CGG Repeats in Premutation Allele and Risk of Full Mutation*
Incidence The prevalence of fragile X syndrome has been estimated to be as high as 1 in 1000 males, making it one of the more common genetic causes of mental retardation. This estimate is based on the use of a chromosomal assay to diagnose fragile X syndrome. With use of a DNA-based assay, a recent study suggests that the true prevalence may be 1 in 2000 to 1 in 3000 [Morton et al., 1997].
Genetics The fragile X syndrome was identified as a unique entity that accounts for X-linked transmission of mental retardation when it was found that affected males exhibit fragility of the distal end of the X chromosome [Lubs, 1969]. This fragility is expressed at its highest frequency when cells for analysis are grown in culture medium deficient in thymidine, and the frequency is further increased by growth in the presence of 5-fluorodeoxyuridine, a thymidylate synthetase inhibitor [Sutherland, 1977]. For many years, growth of cells in special media followed by counting of the proportion that exhibited the fragile X phenotype was the mainstay of laboratory diagnosis [Dewald et al., 1992]. Fragile X syndrome exhibits the transmission pattern of X-linked inheritance, with no male-to-male transmission [Barbe et al., 1996; Barnes, 1989]. Unlike in classical Xlinked recessive traits, however, both males and females can be affected. Also, an unusual pattern of transmission was observed in large families, wherein the gene was transmitted from an unaffected male to an unaffected daughter, who then had affected children [Sherman et al., 1985]. This pattern of transmission is not expected for an X-linked trait, because males who carry the mutant gene should manifest the phenotype. This pattern came to be known as the Sherman paradox. The basis for both the Sherman paradox and the fragility of the X chromosome has come to light since the gene responsible for fragile X syndrome was cloned [Oberle et al., 1991; Verkerk et al., 1991; Yu et al., 1991]. The gene is designated FMR1 (fragile X mental retardation) and is expressed at high levels in neurons [Devys et al., 1993]. FMR1 includes a region near the promoter in which the triplet of bases CGG is repeated multiple times. The exact number of repeats is polymorphic, with repeat numbers ranging from 5 to 50 times in the general population [Kolehmainen, 1994]. Repeats within this range have no impact on the expression of FMR1 and have no phenotypic effect. Persons with fragile X syndrome, by contrast, have repeat numbers of more than 200, often substantially greater. This degree of expansion correlates with hypermethylation of the promoter region of the gene and lack of FMR1 expression.
No. of CGG Repeats
Risk of Expansion to Full Mutation
56 to 59 60 to 69 70 to 79 80 to 89 90 to 199
13.4% 20.6% 57.8% 72.9% 97.3%
*Risk that an FMR1 premutation allele in mother will expand to full mutation in offspring. Data from Nolin SL, et al. Am J Hum Genet 1996;59:1252.
The Sherman paradox is explained by the mechanism of transition from a wild type of allele to a mutant allele [Fu et al., 1991]. This transition occurs through an intermediate step known as premutation. Premutation alleles have repeat expansions in the range of approximately 50 to 200 repeats. These alleles tend to be unstable and may expand to full mutation in a subsequent generation. Nonmanifesting males, therefore, have premutations. Expansion to full mutation does not occur in males. The Sherman paradox is therefore explained by the passage of premutations from males to their daughters, who in turn pass full mutations to some of their offspring. The risk of expansion to full mutation is a function of the size of the premutation allele (Table 22-7) [Nolin et al., 1996; Turner et al., 1994]. Discovery of the molecular basis for fragile X syndrome has led to development of a robust DNA diagnostic test [Rousseau et al., 1991, 1994]. Most laboratories use a method based on Southern blot analysis, and a PCR-based assay can be used to precisely measure the size of permutation alleles [Brown et al., 1993; Kaplan et al., 1994]. Some patientss with fragile X have been found to be mosaics, having both a premutation and a full mutation allele [Cohen et al., 1996; Dobkin et al., 1996; Nolin et al., 1994]. Presumably these mutations arise by postzygotic expansion of a premutation. These patients may demonstrate the fragile X phenotype, although in some cases it may be milder than in a nonmosaic. Some persons with full mutations have some nonmethylated full mutation alleles, which also may ameliorate the phenotype [Hagerman et al., 1994]. The fragile X DNA assay has greatly improved both the sensitivity and the specificity of fragile X diagnosis. For patients tested in the past by cytogenetics alone, DNA testing should be offered either to confirm the fragile X diagnosis or to rule out a false-negative cytogenetic diagnosis. A separate fragile site has been identified on the X chromosome, designated fragile X type E (X-E) (distinguished from the classic fragile X, designated fragile X type A) [Holden et al., 1996]. Fragile X-E also is the result of a triplet repeat expansion in a different gene that is located near the fragile X-A gene. Fragile X-E also can be associated with X-linked mental retardation, although the full fragile X phenotype is not seen in affected persons. Fragile X-E apparently is rare compared with fragile X-A. Although expansion of the CGG repeat is the basis for fragile X syndrome in the vast majority of affected persons, other mutations also have been seen rarely [De Boulle et al., 1993]. In particular, several patients have been reported to
560
Genetic, Metabolic, and Neurocutaneous Disorders / 22
have deletions in the FMR1 gene [Albright et al., 1994; De Graaff et al., 1996; Mannermaa et al., 1996; Meijer et al., 1994; Quan et al., 1995a, 1995b; Tarleton et al., 1993]. The pathogenesis of fragile X syndrome appears to be due to lack of expression of FMR1 in neurons, so any mutation that causes this defect will produce the fragile X phenotype. The protein is an RNA-binding protein and is thought to be involved in regulation of mRNA translation in neurons [Zalfa and Bagni, 2004].
Clinical Features The major phenotypic feature of fragile X syndrome is the occurrence of mental retardation [Prouty et al., 1988]. Developmental milestones are delayed, including gross motor and language. Intelligence quotient (IQ) scores for affected males generally are less than 70 [Morton et al., 1997; Prouty et al., 1988], and IQ may decline with age [Hagerman et al., 1989; Wright-Talamante et al., 1996]. Although males with fragile X syndrome may display autistic-like features [Malmgren et al., 1992], they do not fulfill criteria for autism [Einfeld et al., 1989], and cognitive and adaptive abilities may exceed those seen in children with pervasive developmental disorder [Fisch et al., 1994a]. Behavioral features include shyness and avoidance of eye contact [Einfeld et al., 1994]. Males with fragile X syndrome may display distinctive features that can aid in diagnosis. Birth weight usually is normal, but head circumference and height tend to be above average [De Vries et al., 1995; Prouty et al., 1988]. The face may be long, and ears tend to be large [Loesch and Wilson, 1989; Loesch et al., 1988]. Macro-orchidism can be an important clinical clue to the diagnosis of fragile X syndrome but may not be evident until after puberty [Lachiewicz and Dawson, 1994].
Females with fragile X full mutations also may display cognitive impairment [Cronister et al., 1991; Fisch et al., 1994b; Hagerman et al., 1992; Sobesky et al., 1996]. The frequency of cognitive problems in females with full mutation is approximately 50%, no doubt as a result of the phenomenon of X-chromosome inactivation. If the X chromosome bearing the fragile X mutation is inactivated preferentially, the phenotypic effects of the full mutation may be ameliorated or even eliminated. The clinical recognition of fragile X syndrome can be challenging. The presence of an IQ of less than 70, family history compatible with X-linkage, elongated face, large or prominent ears, and attention deficit- and autistic-like behaviors are useful predictors [Giangreco et al., 1996]. Children suspected of having fragile X syndrome often are found to have other chromosomal anomalies, so standard cytogenetic analysis should be performed along with fragile X testing. Numerous other syndromes are associated with X-linked mental retardation, many of which are difficult to diagnose using clinical or molecular tests [Sutherland et al., 1994]. Premutation carriers do not have mental retardation but may present with one (or more) of three distinct clinical disorders: mild cognitive and/or behavioral deficits on the fragile X spectrum; premature ovarian failure; and a more recently described neurodegenerative disorder of older adult carriers: fragile X–associated tremor/ataxia syndrome (FXTAS) [Hagerman et al., 2004]. Involvement in FXTAS consists of progressive intention tremor, gait ataxia, parkinsonism, and autonomic dysfunction, with associated features of peripheral neuropathy with decreased sensation and vibration sense in the distal lower extremities, as well as cognitive deficits involving loss of memory and executive function. Neuroimaging demonstrates symmetric hyperintensities on T2-weighted MR images of the middle cerebellar peduncles, and eosinophilic, intranuclear inclusions
TABLE 22-8 Major Syndromes Associated with Disorders of DNA Replication and Repair SYNDROME
FEATURES
GENETIC CAUSE
REFERENCE(S)
Ataxia-telangiectasia
Ataxia, telangiectasia, immune deficiency, lymphoma Short stature, photosensitive skin, risk of malignancy, increased frequency of sister chromatid exchange Short stature, premature aging, malignancy Congenital anomalies, aplastic anemia, chromosome breakage increased with alkylating agents or mitomycin C Photosensitive skin, freckling, skin cancer Abnormal skin and hair, short stature, developmental impairment
Mutations in ATM gene; cell cycle checkpoint for repair of DNA damage Mutations in helicase gene involved in DNA replication and recombination
Telatar et al., 1996
Bloom’s syndrome
Werner’s syndrome Fanconi’s anemia
Xeroderma pigmentosum Trichothiodystrophy Cockayne’s syndrome Nijmegen’s breakage syndrome
Photosensitive skin, white matter degeneration, cerebral calcification, dwarfism Progessive microcephaly, growth retardation, immunodeficiency, and cancer predisposition
Ellis and German, 1996; Ellis et al., 1996
Helicase gene mutations (distinct from Bloom’s syndrome gene) Genetically heterogeneous
Epstein and Motulsky, 1996; Yu et al., 1997 Tischkowitz and Hodgson, 2003
Defective excision repair of ultraviolet light–induced DNA damage Defective excision repair of ultraviolet light–induced DNA damage; possible effect on transcription Defective excision repair of ultraviolet light–induced DNA damage; possible effect on transcription Defective response to DNA douse-strand breaks
Tanaka and Wood, 1994 Chu and Mayne, 1996; Takayama et al., 1996 Van der Horst et al., 1997 Varon R et al., 1998
Descartes and Korf / Chromosomes and Chromosomal Abnormalities
have been found in neurons and astrocytes throughout the brain [Hagerman and Hagerman, 2004].
Management Guidelines for the care of patients with fragile X syndrome have been published [Desposito et al., 1996]. Children with fragile X syndrome should be provided with full developmental assessment and require supportive services to enhance developmental outcome. Medical issues include hyperextensibility of joints [Hagerman et al., 1984], which may lead to orthopedic problems, and an increased frequency of mitral valve prolapse [Crabbe et al., 1993]. Diagnosis of fragile X syndrome should prompt a discussion with the parents about the genetic risks, and carrier testing should be offered not only to the immediate family but also to more distant relatives who may be carriers of a premutation [McConkie-Rosell et al., 1997; Staley-Gane et al., 1996; Von Koskull et al., 1994].
Chromosome Breakage Syndromes It has long been recognized that certain inherited disorders are associated with an increased frequency of spontaneous chromosome breakage. Many of these disorders include a prominent neurologic component (Table 22-8), and most are known to represent disorders of DNA replication or repair. In general, routine cytogenetic studies are not the ideal approach to diagnosis of these disorders, although detection of an increased rate of sister chromatid exchange is still used to diagnose Bloom’s syndrome [Chaganti et al., 1974], and finding of cells with rearrangements of chromosomes 7 and 14 may support a diagnosis of ataxia-telangiectasia. The genes responsible for most of these syndromes have been identified, however, and genetic analysis is increasingly being used to evaluate the patient with a suspected clinical diagnosis.
FUTURE OF CLINICAL CYTOGENETICS Technical developments have driven advances in the diagnosis and management of disorders resulting from chromosomal imbalance. Over the past several decades we have moved from the discovery of conditions that are due to the presence of a complete extra chromosome to the recognition of syndromes resulting from deletions of tiny amounts of genetic material. In some cases, such microdeletions will result in mutations that affect single genes. Continuing technical advances are likely to further increase the resolution of cytogenetic analysis and potentially bridge the gap between the light microscopic detection of chromosomal changes and changes at the singlegene level. FISH has played a major role in this effort and is being applied to the study of submicroscopic deletions at the gene level. FISH also is being used to detect subtle chromosome rearrangements. The development of sets of FISH probes that distinguish each chromosome with a unique color (“spectral karyotyping”) provides a means of identifying rearrangements involving small chromosome regions, even in tumor cells that typically include multiple rearrangements. FISH also is providing reagents for studies of nondividing cells, permitting analysis of interphase nuclei for aneuploidy.
561
This procedure can result in more rapid diagnosis of trisomy or detection of low levels of trisomic cells in individuals with mosaicism. The sequencing of the human genome is providing a new set of tools likely to further bridge the gap between cytologic and molecular analysis. It has become clear that small deletions or duplications of genetic material can underlie developmental disorders, and establishing clinical diagnoses for each of these conditions will be difficult. The use of comparative genomic hybridization with microarrays of cloned segments of human DNA may provide a means for generalized screening of the genome for such changes. It is doubtful that the etiology of all chromosomal abnormalities will ever be fully understood, because many seem to be the result of random genetic events. Decades of research have not disclosed any definitive risk factors for nondisjunction other than advanced maternal age. More sensitive techniques for examination of chromosomal abnormalities in germ cells may permit more precise studies of the incidence and risk factors of nondisjunction. Similarly, as the mechanisms of control of DNA replication and cell division are better understood, both environmental and genetic factors that may predispose to chromosomal abnormalities may come to light. Improved methods of noninvasive prenatal cytogenetic investigation may play an increasing role in prenatal diagnosis. The true power of modern genetic analysis is best appreciated when the physician can incorporate genetic studies into day-to-day practice without being concerned about the underlying technical details. That time has not yet arrived in the application of clinical cytogenetics. The clinician must be alert to the possibility of microdeletion syndromes or fragile X, for example. Nevertheless, understanding of the basis of neurologic disease has expanded to include an appreciation of the prominent role of genetic factors in most neurologic disorders, and such factors increasingly are proving to be the key to diagnosis and understanding of basic pathogenesis. REFERENCES Albrecht U, Sutcliffe JS, Cattanach BM, et al. Imprinted expression of the murine Angelman syndrome gene, UBE3A, in hippocampal and Purkinje neurons. Nat Genet 1997;17:75. Albright SG, Lachiewicz AM, Tarleton JC, et al. Fragile X phenotype in a patient with a large de novo deletion in Xq27-q28. Am J Med Genet 1994;51:294. American Academy of Pediatrics Committee on Genetics. Health supervision for children with Down syndrome. Pediatrics 2001;107:442. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Atlantoaxial instability in Down syndrome: Subject review. Pediatrics 1995;96:151. Antonarakis SE and Down Syndrome Collaborative Group. Parental origin of the extra chromosome in trisomy 21 as indicated by analysis of DNA polymorphisms. N Engl J Med 1991;324:872. Auerbach AD. Fanconi anemia. Dermatol Clin 1995;13:41. Bahado-Singh RO, Goldstein I, Uerpairojkit B, et al. Normal nuchal thickness in the midtrimester indicates reduced risk of Down syndrome in pregnancies with abnormal triple-screen results. Am J Obstet Gynecol 1995;173:1106. Baird PA, Sadovnick AD. Life tables for Down syndrome. Hum Genet 1989;82:291. Balderston SM, Shaffer EM, Washington RL, et al. Congenital polyvalvular disease in trisomy 18: Echocardiographic diagnosis. Pediatr Cardiol 1990;11:138.
562
Genetic, Metabolic, and Neurocutaneous Disorders / 22
Ballabio A, Bardoni B, Carrozzo R, et al. Contiguous gene syndromes due to deletions in the distal short arm of the human X chromosome. Proc Natl Acad Sci U S A 1989;86:100. Barbe B, Franke P, Maier W, et al. Fragile X syndrome. 1. An overview on its genetic mechanism. Eur Psychiatr 1996;11:227. Barnes DM. “Fragile X” syndrome and its puzzling genetics. Science 1989;243:171. Baty BJ, Blackburn BL, Carey JC. Natural history of trisomy 18 and trisomy 13: I. Growth, physical assessment, medical histories, survival, and recurrence risk. Am J Med Genet 1994a;49:175. Baty BJ, Jorde LB, Blackburn BL, et al. Natural history of trisomy 18 and trisomy 13: II. Psychomotor development. Am J Med Genet 1994b;49:189. Bender B, Fry E, Pennington B, et al. Speech and language development in 41 children with sex chromosome anomalies. Pediatrics 1983;71:262. Bender B, Puck M, Salbenblatt J, et al. Cognitive development of unselected girls with complete and partial X monosomy. Pediatrics 1984;73:175. Bender BG, Harmon RJ, Linden MG, et al. Psychosocial adaptation of 39 adolescents with sex chromosome abnormalities. Pediatrics 1995;96:302. Bender BG, Linden MG, Robinson A. Verbal and spatial processing efficiency in 32 children with sex chromosome abnormalities. Pediatr Res 1989;25:577. Bender BG, Linden MG, Robinson A. Neuropsychological impairment in 42 adolescents with sex chromosome abnormalities. Am J Med Genet 1993;48:169. Bettio D, Rizzi N, Giardino D, et al. FISH analysis in Prader-Willi and Angelman syndrome patients. Am J Med Genet 1995;56:224. Beuten J, Sutcliffe JS, Casey BM, et al. Detection of imprinting mutations in Angelman syndrome using a probe for exon α of SNRPN. Am J Med Genet 1996;63:414. Bickmore WA, Sumner AT. Mammalian chromosome banding—an expression of genome organization. Trends Genet 1989;5:144. Boue J, Boue A, Lazar P. The epidemiology of human spontaneous abortions with chromosomal anomalies. In Blandau RJ, ed. Aging gametes. Basel: S Karger, 1973. Boy de la Tour E, Laemmli UK. The metaphase scaffold is helically folded: Sister chromatids have predominantly opposite helical handedness. Cell 1988;55:937. Breuning MH, Dauwerse HG, Fugazza G, et al. Rubinstein-Taybi syndrome caused by submicroscopic deletions within 16p13.3. Am J Hum Genet 1993;52:249. Brown S, Gersen S, Anyane-Yeboa K, et al. Preliminary definition of a “critical region” of chromosome 13 in q32: Report of 14 cases with 13q deletions and review of the literature. Am J Med Genet 1993;45:52. Brown WT, Houck GE, Jr., Jeziorowska A, et al. Rapid fragile X carrier screening and prenatal diagnosis using a nonradioactive PCR test. JAMA 1993;270:1569. Buiting K, Dittrich B, Robinson WP, et al. Detection of aberrant DNA methylation in unique Prader-Willi syndrome patients and its diagnostic implications. Hum Mol Genet 1994;3:893. Buiting K, Saitoh S, Gross S, et al. Inherited microdeletions in the Angelman and Prader-Willi syndromes define an imprinting centre on human chromosome 15. Nat Genet 1995;9:395. Canick JA. Screening for Down syndrome using maternal serum alpha-fetoprotein, unconjugated estriol, and HCG. J Clin Immunoassay 1990;13:30. Carakushansky G, Teich E, Ribeiro MG, et al. Diploid/triploid mosaicism: Further delineation of the phenotype. Am J Med Genet 1994;52:399. Carothers AD, Filippi G. Klinefelter’s syndrome in Sardinia and Scotland. Comparative studies of parental age and other aetiological factors in 47,XXY. Hum Genet 1988;81:71. Caspersson T, de la Chapelle S, Foley GEKJ, et al. Chemical differentiation along metaphase chromosomes. Exp Cell Res 1968;49:219. Cataldo AM, Petanceska S, Peterhoff CM, et al. APP gene dosage modulates endosomal abnormalities of Alzheimer’s disease in a segmental trisomy 16 mouse model of Down syndrome. J Neurosci 2003;23:6788. Cech TR. Beginning to understand the end of the chromosome. Cell 2004;116:273. Chaganti RS, Schonberg S, German J. A manyfold increase in sister chromatid exchanges in Bloom’s syndrome lymphocytes. Proc Natl Acad Sci U S A 1974;71:4508.
Chance PF, Fischbeck KH. Molecular genetics of Charcot-Marie-Tooth disease and related neuropathies. Hum Mol Genet 1994;3:1503. Cheng SD, Spinner NB, Zackai EH, et al. Cytogenetic and molecular characterization of inverted duplicated chromosomes 15 from 11 patients. Am J Hum Genet 1994;55:753. Chu G, Mayne L. Xeroderma pigmentosum, Cockayne syndrome and trichothiodystrophy: Do the genes explain the diseases? Trends Genet 1996;12:187. Cianfarani S, Vaccaro F, Boscherini B. What is the rationale for growth hormone therapy in Turner’s syndrome? Lancet 1994;344:114. Cockburn DJ, Munro EA, Craig IW, et al. Mapping of X chromosome translocation breakpoints in females with Duchenne muscular dystrophy with respect to exons of the dystrophin gene. Hum Genet 1992;90:407. Cohen IL, Nolin SL, Sudhalter V, et al. Mosaicism for the FMR1 gene influences adaptive skills development in fragile X–affected males. Am J Med Genet 1996;64:365. Cooley WC, Graham JM Jr. Common syndromes and management issues for primary care physicians. Clin Pediatr 1991;30:233. Crabbe LS, Bensky AS, Hornstein L, et al. Cardiovascular abnormalities in children with fragile X syndrome. Pediatrics 1993;91:714. Cremers MJ, Bol E, de Roos F, et al. Risk of sports activities in children with Down’s syndrome and atlantoaxial instability. Lancet 1993;342:511. Crocker M. Rearrangements of the X chromosome and Turner syndrome. Hum Genet 1992;90:185. Cronister A, Schreiner R, Wittenberger M, et al. Heterozygous fragile X female: Historical, physical, cognitive, and cytogenetic features. Am J Med Genet 1991;38:269. Cronk C, Crocker AC, Pueschel SM, et al. Growth charts for children with Down syndrome: 1 month to 18 years of age. Pediatrics 1988;81:102. D’Alton ME, DeCherney AH. Current concepts: Prenatal diagnosis. N Engl J Med 1993;328:114. Dallapiccola B, Mingarelli R, Novelli G. The link between cytogenetics and mendelism. Biomed Pharmacother 1995;49:83. Daniel A, Hook EB, Wulf G. Risks of unbalanced progeny at amniocentesis to carriers of chromosome rearrangements: Data from United States and Canadian laboratories. Am J Med Genet 1989;33:14. Daniel A, Malafiej P, Preece K, et al. Identification of marker chromosomes in thirteen patients using FISH probing. Am J Med Genet 1994;53:8. De Boulle K, Verkerk AJMH, Reyniers E, et al. A point mutation in the FMR-1 gene associated with fragile X mental retardation. Nat Genet 1993;3:31. De Graaff E, De Vries BBA, Willemsen R, et al. The fragile X phenotype in a mosaic male with a deletion showing expression of the FMR1 protein in 28% of the cells. Am J Med Genet 1996;64:302. Delach JA, Rosengren SS, Kaplan L, et al. Comparison of high resolution chromosome banding and fluorescence in situ hybridization (FISH) for the laboratory evaluation of Prader-Willi syndrome and Angelman syndrome. Am J Med Genet 1994;52:85. De Vries BBA, Robinson H, Stolte-Dijkstra I, et al. General overgrowth in the fragile X syndrome: Variability in the phenotypic expression of the FMR1 gene mutation. J Med Genet 1995;32:764. Desposito F, Cho S, Frias JL, et al. Health supervision for children with fragile X syndrome. Pediatrics 1996;98:297. Devys D, Lutz Y, Rouyer N, et al. The FMR-1 protein is cytoplasmic, most abundant in neurons and appears normal in carriers of a fragile X premutation. Nat Genet 1993;4:335. Dewald G, Stallard R, Bader PI, et al. Toward quality assurance for metaphase FISH: A multi-center experience. Am J Med Genet 1996;64:539. Dewald GW, Buckley DD, Sprubeck JL, et al. Cytogenetic guidelines for fragile X studies tested in routine practice. Am J Med Genet 1992;44:816. Dittrich B, Buiting K, Horsthemke B. PW71 methylation test for Prader-Willi and Angelman syndromes. Am J Med Genet 1996;61:196. Dobkin CS, Nolin SL, Cohen I, et al. Tissue differences in fragile X mosaics: Mosaicism in blood cells may differ greatly from skin. Am J Med Genet 1996;64:296. Donlon TA. Similar molecular deletions on chromosome 15q11.2 are encountered in both the Prader-Willi and Angelman syndromes. Hum Genet 1988;80:322.
Descartes and Korf / Chromosomes and Chromosomal Abnormalities Driscoll DJ. Genomic imprinting in humans. Mol Genet Med 1994;4:37–77. Einfeld S, Molony H, Hall W. Autism is not associated with the fragile X syndrome. Am J Med Genet 1989;34:187. Einfeld SL, Tonge BJ, Florio T. Behavioural and emotional disturbance in fragile X syndrome. Am J Med Genet 1994;51:386. Ellis NA, German J. Molecular genetics of Bloom’s syndrome. Hum Mol Genet 1996;5:1457. Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell 1996;83:655. Embleton ND, Wyllie JP, Wright MJ, et al. Natural history of trisomy 18. Arch Dis Child Fetal Neonatal 1996;75:F38. Epstein CJ. Down syndrome, trisomy 21. In: Scriver CR, Beaudet AL, Sly WS, Valle D. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 1995;749–794. Epstein CJ, Motulsky AG. Werner syndrome: Entering the helicase era. BioEssays 1996;18:1025. Estabrooks LL, Breg WR, Hayden MR, et al. Summary of the 1993 ASHG Ancillary Meeting “Recent research on chromosome 4p syndromes and genes.” Am J Med Genet 1995;55:453. Felsenfeld G. Chromatin unfolds. Cell 1996;86:13. Fisch GS, Holden JJA, Simensen R, et al. Is fragile X syndrome a pervasive developmental disability? Cognitive ability and adaptive behavior in males with the full mutation. Am J Med Genet 1994a;51:346. Fisch GS, Simensen R, Arinami T, et al. Longitudinal changes in IQ among fragile X females: A preliminary multicenter analysis. Am J Med Genet 1994b;51:353. Flint S, Gibb DM. Recurrent second trimester miscarriage. Curr Opin Obstet Gynecol 1996;8:449. Froster UG, Jackson L. Limb defects and chorionic villus sampling: Results from an international registry, 1992-94. Lancet 1996;347:489. Fryns JP, Kleczkowska A, Kubien E, et al. XYY syndrome and other Y chromosome polysomies. Mental status and psychosocial functioning. Genet Couns 1995;6:197. Fu Y-H, Kuhl DPA, Pizzuti A, et al. Variation of the CGG repeat at the fragile X site results in genetic instability: Resolution of the Sherman paradox. Cell 1991;67:1047. Gath A. Down’s syndrome and the family. Hum Genet 1981;2 (Suppl):75. Gath A. Down syndrome children and their families. Am J Med Genet 1990;7 (Suppl):314. Gath A, Gumley D. Down’s syndrome and the family: Follow-up of children first seen in infancy. Dev Med Child Neurol 1984;26:500. Gath A, Gumley D. Behaviour problems in retarded children with special reference to Down’s syndrome. Br J Psychiatr 1986;149:156. Gessler M, Thomas GH, Couillin P, et al. A deletion map of the WAGR region on chromosome 11. Am J Hum Genet 1989;44:486. Giangreco CA, Steele MW, Aston CE, et al. A simplified six-item checklist for screening for fragile X syndrome in the pediatric population. Pediatrics 1996;129:611. Gillessen-Kaesbach G, Gross S, Kaya-Westerloh S, et al. DNA methylation based testing of 450 patients suspected of having Prader-Willi syndrome. J Med Genet 1995;32:88. Gopal Rao VVN, Roop H, Carpenter NJ. Diagnosis of microdeletion syndromes: High-resolution chromosome analysis versus fluorescence in situ hybridization. Am J Med Sci 1995;309:208. Gray DL, Crane JP. Optimal nuchal skin-fold thresholds based on gestational age for prenatal detection of Down syndrome. Am J Obstet Gynecol 1994;171:1282. Greenberg F, Lewis RA, Potocki L, et al. Multi-disciplinary clinical study of Smith-Magenis syndrome (deletion 17p11.2). Am J Med Genet 1996;62:247. Hagerman PJ, Hagerman RJ. The fragile-X premutation: A maturing perspective. Am J Hum Genet. 2004;74:805. Hagerman RJ, Hull CE, Safanda JF, et al. High functioning fragile X males: Demonstration of an unmethylated fully expanded FMR-1 mutation associated with protein expression. Am J Med Genet 1994;51:298. Hagerman RJ, Jackson C, Amiri K, et al. Girls with fragile X syndrome: Physical and neurocognitive status and outcome. Pediatrics 1992;89:395. Hagerman RJ, Leavitt BR, Farzin F, et al. Fragile-X–associated tremor/ataxia syndrome (FXTAS) in females with the FMR1 premutation. Am J Hum Genet 2004;74:1051. Hagerman RJ, Leehey M, Heinrichs W, et al. Intention tremor, parkinsonism, and generalized brain atrophy in male carriers of fragile X. Neurology 2001;57:127.
563
Hagerman RJ, Schreiner RA, Kemper MB, et al. Longitudinal IQ changes in fragile X males. Am J Med Genet 1989;33:513. Hagerman RJ, van Housen K, Smith AC, et al. Consideration of connective tissue dysfunction in the fragile X syndrome. Am J Med Genet 1984;17:111. Hall JG. How imprinting is relevant to human disease. Development 1990;110 (Suppl):141. Hammerle B, Elizalde C, Galceran J, et al. The MNB/DYRK1A protein kinase: Neurobiological functions and Down syndrome implications. J Neural Transm Suppl 2003;67:129. Hanton L, Axelrod L, Bakalov V, Bondy CA. The importance of estrogen replacement in young women with Turner syndrome. J Womens Health 2003;12:971. Hassold T, Benham F, Leppert M. Cytogenetic and molecular analysis of sex-chromosome monosomy Am J Hum Genet 1988;42:534. Holden JJA, Julien-Inalsingh C, Chalifoux M, et al. Trinucleotide repeat expansion in the FRAXE locus is not common among institutionalized individuals with non-specific developmental disabilities. Am J Med Genet 1996;64:420. Holmes LB. Report of National Institute of Child Health and Human Development Workshop on Chorionic Villus Sampling and Limb and Other Defects, October 20, 1992. Teratology 1993;48:7. Hook EB, Cross PK. Maternal age-specific rates of chromosome abnormalities at chorionic villus study: A revision. Am J Hum Genet 1989;45:474. Hook EB, Cross PK, Schreinemachers MS. Chromosomal abnormality rates at amniocentesis and in live-born infants. JAMA 1983;249:2034. Hook EB, Topol BB, Cross PK. The natural history of cytogenetically abnormal fetuses detected at midtrimester amniocentesis which are not terminated electively: New data and estimates of the excess and relative risk of late fetal death associated with 47,+21 and some other abnormal karyotypes. Am J Hum Genet 1989;45:855. Hou J, Parrish J, Lüdecke HJ, et al. A 4-megabase YAC contig that spans the Langer-Giedion syndrome region on human chromosome 8q24.1: Use in refining the location of the trichorhinophalangeal syndrome and multiple exostoses genes (TRPS1 and EXT1). Genomics 1995;29:87. Hsu TC, Pomerat CM. Mammalian chromosomes in vitro. II. A method for spreading the chromosomes of cells in tissue culture. J Hered 1953;44:23. Hughes A. Some effects of abnormal tonicity on dividing cells in chick tissue cultures. Q J Micr Sci 1952;93:207. Huret JL, Leonard C, Forestier B, et al. Eleven new cases of del(9p) and features from 80 cases. J Med Genet 1988;25:741. Iwatsubo T, Mann DM, Odaka A, et al. Amyloid β protein (Aβ) deposition: Aβ42(43) precedes Aβ40 in Down syndrome. Ann Neurol 1995;37:294. Jackson JF, North ERI, Thomas JG. Clinical diagnosis of Down’s syndrome. Clin Genet 1976;9:483. Jacobs PA, Betts PR, Cockwell AE, et al. A cytogenetic and molecular reappraisal of a series of patients with Turner’s syndrome. Ann Hum Genet 1990;54:209. Jacobs PA, Browne C, Gregson N, et al. Estimates of the frequency of chromosome abnormalities detectable in unselected newborns using moderate levels of banding. Med Genet 1992;29:103. Janson M, Kock E, Nordenskjöld M. Constitutional deletions predisposing to retinoblastoma. Hum Genet 1990;85:21. Johannsen P, Christensen JE, Mai J. The prevalence of dementia in Down syndrome. Dementia 1996;7:221. Johnson JAM, Wilson RD, Winsor EJT, et al. The Early Amniocentesis Study: A randomized clinical trial of early amniocentesis versus midtrimester amniocentesis. Fetal Diagn Ther 1996;11:85. Kaplan G, Kung M, McClure M, et al. Direct mutation analysis of 495 patients for fragile X carrier status/proband diagnosis. Am J Med Genet 1994;51:501. Kernan KT. Comprehension of syntactically indicated sequence by Down’s syndrome and other mentally retarded adults. J Ment Defic Res 1990;34:169. Kernan KT, Sabsay S. Linguistic and cognitive ability of adults with Down syndrome and mental retardation of unknown etiology. J Commun Disord 1996;29:401. Kishino T, Lalande M, Wagstaff J. UBE3A/E6-AP mutations cause Angelman syndrome. Nat Genet 1997;15:70. Kline AD, White ME, Wapner R, et al. Molecular analysis of the 18q− syndrome—and correlation with phenotype. Am J Hum Genet 1993;52:895.
564
Genetic, Metabolic, and Neurocutaneous Disorders / 22
Kloza EM. Low MSAFP and new biochemical markers for Down syndrome: Implications for genetic counselors. Birth Defects 1990;26:32. Knight GJ, Palomaki GE. Maternal serum alpha-fetoprotein screening and Down syndrome. J Clin Immunoassay 1990;13:23. Knoll JHM, Lalande M. Cytogenetic and molecular studies in the Prader-Willi and Angelman syndromes: An overview. Am J Med Genet 1993;46:2. Knoll JHM, Nicholls RD, Magenis RE, et al. Angelman and Prader-Willi syndromes share a common chromosome 15 deletion but differ in parental origin of the deletion. Am J Med Genet 1989;32:285. Kolehmainen K. Population genetics of fragile X: A multiple allele model with variable risk of CGG repeat expansion. Am J Med Genet 1994;51:428. Kriek M, White SJ, Bouma MC, et al. Genomic imbalances in mental retardation. J Med Genet 2004;41:(4):249–255. Kupke KG, Müller U. Parental origin of the extra chromosome in trisomy 18. Am J Hum Genet 1989;45:599. Kurtyka ZE. Trisomy 8 mosaicism syndrome. Clin Pediatr 1988;27:557. Kuznetzova T, Baranov A, Schwed N, et al. Cytogenetic and molecular findings in patients with Turner’s syndrome stigmata. J Med Genet 1995;32:962. Lachiewicz AM, Dawson DV. Do young boys with fragile X syndrome have macroorchidism? Pediatrics 1994;93:992. Lai F, Williams RS. A prospective study of Alzheimer disease in Down syndrome. Arch Neurol 1989;46:849. Lander ES, Linton LM, Birren B, et al. Initial sequencing and analysis of the human genome. Nature 2001;409:860. Ledbetter DH, Engel E. Uniparental disomy in humans: Development of an imprinting map and its implications for prenatal diagnosis. Hum Mol Genet 1995;4:1757. Lejeune J, Gauthier MTR. Etude des chromosomes somatiques de neuf enfants mongoliens. Comptes Rendus Hebdomadaires Seances Acad Sci 1997;248:1971. Li LH, Krantz ID, Deng Y, et al. Alagille syndrome is caused by mutations in human Jagged1, which encodes a ligand for Notch1. Nat Genet 1997;16:243. Liehr T, Grehl H, Rautenstrauss B. FISH analysis of interphase nuclei extracted from paraffin-embedded tissue. Trends Genet 1995;11:377. Liehr T, Starke H, Weise A, et al. Multicolor FISH probe sets and their applications. Histol Histopathol 2004;19:229. Ligon AH, Beaudet AL, Shaffer LG. Simultaneous, multilocus FISH analysis for detection of microdeletions in the diagnostic evaluation of developmental delay and mental retardation. Am J Hum Genet 1997;61:51. Lindsay EA, Goldberg R, Jurecic V, et al. Velo-cardio-facial syndrome: Frequency and extent of 22q11 deletions. Am J Med Genet 1995;57:514. Lister TJ, Frota-Pessoa O. Recurrence risks for Down syndrome. Hum Genet 1980;55:203. Loesch DZ, Lafranchi M, Scott D. Anthropometry in Martin-Bell syndrome. Am J Med Genet 1988;30:149. Loesch DZ, Wilson SR. Multivariate analysis of body shape in fragile X (Martin-Bell) syndrome. Am J Med Genet 1989;33:200. Lomax BL, Kalousek DK, Kuchinka BD, et al. The utilization of interphase cytogenetic analysis for the detection of mosaicism. Hum Genet 1994;93:243. Long M, de Souza SJ, Gilbert W. Evolution of the intron-exon structure of eukaryotic genes. Curr Opin Genet Dev 1995;5:774. Lott IT. The neurology of Down syndrome. In: Epstein CJ, ed. Neurobiology of Down syndrome. New York: Raven Press, 1986. Lott IT, Osann K, Doran E, Nelson L. Down syndrome and Alzheimer disease: Response to donepezil. Arch Neurol 2002;59:1133. Lott IT, Richardson EP. Neuropathological findings and the biology of neurofibromatosis. Adv Neurol 1981;29:23. Lowery MC, Morris CA, Ewart A, et al. Strong correlation of elastin deletions, detected by FISH, with Williams syndrome: Evaluation of 235 patients. Am J Hum Genet 1995;57:49. Lubs HA. A marker X chromosome. Am J Hum Genet 1969;21:231. Lüdecke H-J, Wagner MJ, Nardmann J, et al. Molecular dissection of a contiguous gene syndrome: Localization of the genes involved in the Langer-Giedion syndrome. Hum Mol Genet 1995;4:31. Luquet I, Mugneret F, Athis PD, et al. French multi-centric study of 2000 amniotic fluid interphase FISH analyses from high-risk pregnancies and review of the literature. Ann Genet 2002;45:77. Malmgren H, Gustavson K-H, Wahlström J, et al. Infantile autism-fragile X: Molecular findings support genetic heterogeneity. Am J Med Genet 1992;44:830.
Mannermaa A, Pulkkinen L, Kajanoja E, et al. Deletion in the FMR1 gene in a fragile-X male. Am J Med Genet 1996;64:293. Manuelidis L, Chen TL. Analytical cytogenetics: A unified model of eukaryotic chromosomes. Cytometry 1990;11:8. Marino B, Vairo U, Corno A, et al. Atrioventricular canal in Down syndrome: Prevalence of associated cardiac malformations compared with patients without Down syndrome. Am J Dis Child 1990;144:1120. Marion RW, Chitayat D, Hutcheon GNJA, et al. Trisomy 18 score: A rapid, reliable diagnostic test for trisomy 18. J Pediatr 1988;113:45. Matsuura T, Sutcliffe JS, Fang P, et al. De novo truncating mutations in E6-AP ubiquitin-protein ligase gene (UBE3A) in Angelman syndrome. Nat Genet 1997;15:74. McConkie-Rosell A, Spiridigliozzi GA, Iafolla T, et al. Carrier testing in the fragile X syndrome: Attitudes and opinions of obligate carriers. Am J Med Genet 1997;68:62. McFadden DE, Kwong LC, Yam IY, et al. Parental origin of triploidy in human fetuses: Evidence for genomic imprinting. Hum Genet 1993;92:465. Meijer H, De Graaff E, Merckx DML, et al. A deletion of 1.6 kb proximal to the CGG repeat of the FMR1 gene causes the clinical phenotype of the fragile X syndrome. Hum Mol Genet 1994;3:615. Miny P, Koppers B, Dworniczak B, et al. Parental origin of the extra haploid chromosome set in triploidies diagnosed prenatally. Am J Med Genet 1995;57:102. Mitelman F, ed. An international system for cytogenetic nomenclature. Basel: S Karger, 1995. Moerman P, Fryns J-P, Van der Steen K, et al. Spectrum of clinical and autopsy findings in trisomy 18 syndromes. J Hum Genet 1982;30:17. Moerman P, Fryns J-P, Van der Steen K, et al. The pathology of trisomy 13 syndrome. A study of 12 cases. Hum Genet 1988;80:349. Monaghan KG, Van Dyke DL, Feldman G, et al. Diagnostic testing: A cost analysis for Prader-Willi and Angelman syndromes. Am J Hum Genet 1997;60:244. Morton JE, Bundey S, Webb TP, et al. Fragile X syndrome is less common than previously estimated. J Med Genet 1997;34:1. Morton RE, Ali Khan M, Murray-Leslie C, et al. Atlantoaxial instability in Down’s syndrome: A five year follow up study. Arch Dis Child 1995;72:115. Mutton D, Alberman E, Hook EB. Cytogenetic and epidemiological findings in Down syndrome, England and Wales 1989 to 1993. National Down Syndrome Cytogenetic Register and the Association of Clinical Cytogeneticists. J Med Genet 1996;33:387. Myers BA, Pueschel S. Psychiatric disorders in persons with Down syndrome. J Nerv Ment Dis 1991;179(10):609–613. Nicholls RD, Pai GS, Gottlieb W, et al. Paternal uniparental disomy of chromosome 15 in a child with Angelman syndrome. Ann Neurol 1992;32:512. Nijhuis-Van der Sanden MW, Eling PA, Otten BJ. A review of neuropsychological and motor studies in Turner syndrome. Neurosci Biobehav Rev 2003;27:329. Nolin SL, Glicksman A, Houck GE Jr, et al. Mosaicism in fragile X affected males. Am J Med Genet 1994;51:509. Nolin SL, Lewis FA, Ye LL, et al. Familial transmission of the FMR1 CGG repeat. Am J Hum Genet 1996;59:1252. Nowell P. Phytohemagglutinin as an initiator of mitosis in cultures of normal human leucocytes. Cancer Res 1960;20:462. Nyberg DA, Resta RG, Hickok DE, et al. Femur length shortening in the detection of Down syndrome: Is prenatal screening feasible? Am J Obstet Gynecol 1990;162:1247. Oberle I, Rousseau F, Heitz D, et al. Instability of a 550-base pair DNA segment and abnormal methylation in fragile X syndrome. Science 1991;252:1097. Oda T, Elkahloun AG, Pike BL, et al. Mutations in the human Jagged1 gene are responsible for Alagille syndrome. Nat Genet 1997;16:235. Ohashi H, Tsukahara M, Murano I, et al. Pigmentary dysplasias and chromosomal mosaicism: Report of 9 cases. Am J Med Genet 1992;43:716. Overhauser J, Huang X, Gersh M, et al. Molecular and phenotypic mapping of the short arm of chromosome 5: Sublocalization of the critical region for the cri-du-chat syndrome. Hum Mol Genet 1994;3:247. Pennington BF, Bender B, Puck M, et al. Learning disabilities in children with sex chromosome anomalies. Child Dev 1982;53:1182. Pijpers L, Jahoda MGJ, Reuss A, et al. Transabdominal chorionic villus biopsy in second and third trimesters of pregnancy to determine fetal karyotype. BMJ 1988;297:822.
Descartes and Korf / Chromosomes and Chromosomal Abnormalities Preus M. A diagnostic index for Down syndrome. Clin Genet 1977;12:47. Prouty LA, Rogers RC, Stevenson RE, et al. Fragile X syndrome: Growth, development, and intellectual function. Am J Med Genet 1988;30:123. Pueschel SM, Bernier JC, Pezzullo JC. Behavioural observations in children with Down’s syndrome. J Ment Defic Res 1991;35:502. Pueschel SM, Gallagher PL, Zartler AS, et al. Cognitive and learning processes in children with Down syndrome. Res Dev Disabil 1987;8:21. Pueschel SM, Louis S, McKnight P. Seizure disorders in Down syndrome. Arch Neurol 1991;48:318. Quan F, Grompe M, Jakobs P, et al. Spontaneous deletion in the FMR1 gene in a patient with fragile X syndrome and cherubism. Hum Mol Genet 1995a;4:1681. Quan F, Zonana J, Gunter K, et al. An atypical case of fragile X syndrome caused by a deletion that includes the FMR1 gene. Am J Hum Genet 1995b;56:1042. Rand EB, Spinner NB, Piccoli DA, et al. Molecular analysis of 24 Alagille syndrome families identifies a single submicroscopic deletion and further localizes the Alagille region within 20p12. Am J Hum Genet 1995;57:1068. Ranke MB. Growth hormone therapy in Turner syndrome. Analysis of long-term results. Horm Res 1995;44 [Suppl] 3:35. Rasmussen SA, Wong LY, Yang Q, et al. Population-based analyses of mortality in trisomy 13 and trisomy 18. Pediatrics 2003;111:777. Risser WL, Anderson SJ, Bolduc SP, et al. Atlantoaxial instability in Down syndrome: Subject review. Pediatrics 1995;96:151. Robinson A, Lubs HA, Nielsen J, et al. Summary of clinical findings: Profiles of children with 47,XXY, 47,XXX and 47,XYY karyotypes. Birth Defects 1979;15:261. Rochiccioli P, Battin J, Bertrand AM, et al. Final height in Turner syndrome patients treated with growth hormone. Horm Res 1995;44:172. Root S, Carey JC. Survival in trisomy 18. Am J Med Genet 1994;49:170. Rose EA, Glaser T, Jones C, et al. Complete physical map of the WAGR region of 11p13 localizes a candidate Wilms’ tumor gene. Cell 1990;60:405. Rosenfeld RG, Tesch L-G, Rodriguez-Rigau LJ, et al. Recommendations for diagnosis, treatment, and management of individuals with Turner syndrome. Endocrinologist 1994;4:351. Rougeulle C, Glatt H, Lalande M. The Angelman syndrome candidate gene, UBE3A/E6-AP, is imprinted in brain. Nat Genet 1997;17:14. Rousseau F, Heitz D, Biancalana V, et al. Direct diagnosis by DNA analysis of the fragile X syndrome of mental retardation. N Engl J Med 1991;325:1673. Rousseau F, Heitz D, Tarleton J, et al. A multicenter study on genotype-phenotype correlations in the fragile X syndrome, using direct diagnosis with probe StBI2.3: The first 2,253 cases. Am J Hum Genet 1994;55:225. Saitoh S, Harada N, Jinno Y, et al. Molecular and clinical study of 61 Angelman syndrome patients. Am J Med Genet 1994;52:158. Salbenblatt JA, Bender BG, Puck MH, et al. Development of eight pubertal males with 47,XXY karyotype. Clin Genet 1981;20:141. Salbenblatt JA, Meyers DC, Bender BG, et al. Gross and fine motor development in 47,XXY and 47,XYY males. Pediatrics 1987;80:240. Salbenblatt JA, Meyers DC, Bender BG, et al. Gross and fine motor development in 45,X and 47,XXX girls. Pediatrics 1989;84:678. Sapienza C. Genome imprinting: An overview. Dev Genet 1995;17:185. Schinzel A, Schmid W, Luscher U, et al. Structural aberrations of chromosome 18. I. The 18p− syndrome. Arch Genet 1974;47:1. Schmickel RD. Chromosomal deletions and enzyme deficiencies. J Pediatr 1986;108:244. Schupf N, Kapell D, Lee JH, et al. Onset of dementia is associated with apolipoprotein E ε4 in Down’s syndrome. Ann Neurol 1996;40:799. Seashore MR, Cho S, Desposito F, et al. Health supervision for children with Turner syndrome. Pediatrics 1995;96:1166. Sermon K, Van SA, Liebaers I. Preimplantation genetic diagnosis. Lancet 2004;363:1633. Shapira SK, McCaskill C, Northrup H, et al. Chromosome 1p36 deletions: The clinical phenotype and molecular characterization of a common newly delineated syndrome. Am J Hum Genet 1997;61:642. Sherman SL, Jacobs PA, Morton NE, et al. Further segregation analysis of the fragile X syndrome with special reference to transmitting males. Hum Genet 1985;69:289. Smidt-Jensen S, Hahnemann N. Transabdominal chorionic villus sampling for fetal genetic diagnosis: Technical and obstetrical evaluation of 100 cases. Prenat Diagn 1988;8:7.
565
Smith A, Prasad M, Deng Z-M, et al. Comparison of high resolution cytogenetics, fluorescence in situ hybridisation, and DNA studies to validate the diagnosis of Prader-Willi and Angelman’s syndromes. Arch Dis Child 1995;72:397. Smith DJ, Stevens ME, Sudanagunta SP, et al Functional screening of 2 Mb of human chromosome 21q22.2 in transgenic mice implicates minibrain in learning defects associated with Down syndrome. Nat Genet 1997;16:28. Sobesky WE, Taylor AK, Pennington BF, et al. Molecular/clinical correlations in females with fragile X. Am J Med Genet 1996;64:340. Stafstrom CE, Patxot OF, Gilmore HE, et al. Seizures in children with Down syndrome: Etiology, characteristics and outcome. Dev Med Child Neurol 1991;33:191. Staley-Gane L, Flynn L, Neitzel K, et al. Expanding the role of the genetic counselor. Am J Med Genet 1996;64:382. Staples AJ, Robertson EF, Ranieri E, et al. A maternal serum screen for trisomy 18: An extension of maternal serum screening for Down syndrome. Am J Hum Genet 1991;49:1025. Sutherland GR. Fragile sites on human chromosomes: Demonstration of their dependence on the type of tissue culture medium. Science 1977;197:265. Sutherland GR, Brown WT, Hagerman R, et al. Sixth International Workshop on the Fragile X and X-Linked Mental Retardation. Am J Med Genet 1994;51:281. Takayama K, Salazar EP, Broughton BC, et al. Defects in the DNA repair and transcription gene ERCC2 (XPD) in trichothiodystrophy. Am J Hum Genet 1996;58:263. Tanaka K, Wood RD. Xeroderma pigmentosum and nucleotide excision repair of DNA. Trends Biochem Sci 1994;19:83. Tarleton J, Richie R, Schwartz C, et al. An extensive de novo deletion removing FMR1 in a patient with mental retardation and the fragile X syndrome phenotype. Hum Mol Genet 1993;2:1973. Telatar M, Wang ZJ, Udar N, et al. Ataxia-telangiectasia: Mutations in ATM cDNA detected by protein-truncation screening. Am J Hum Genet 1996;59:40. Teller JK, Russo C, DeBusk LM, et al. Presence of soluble amyloid beta-peptide precedes amyloid plaque formation in Down’s syndrome. Nat Med 1996;2:93. Tjio JH, Levan A. The chromosome number of man. Hereditas 1956;43:1. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet 2003;40:1. Turner AM, Robinson H, Wake S, et al. Counselling risk figures for fragile X carrier females of varying band sizes for use in predicting the likelihood of retardation in their offspring. Am J Med Genet 1994;51:458. Turner BM. Decoding the nucleosome. Cell 1993;75:5. Van Bakel I, Holt S, Craig I, et al. Sequence analysis of the breakpoint regions of an X;5 translocation in a female with Duchenne muscular dystrophy. Am J Hum Genet 1995;57:329. Van den Ouweland AMW, Van der Est MN, Wesby-van Swaay E, et al. DNA diagnosis of Prader-Willi and Angelman syndromes with the probe PW71 (D15S63). Hum Genet 1995;95:562. Van der Horst GTJ, Van Steeg H, Berg RJW, et al. Defective transcription-coupled repair in Cockayne syndrome B mice is associated with skin cancer predisposition. Cell 1997;89:425. Van Praagh S, Truman T, Firpo A, et al. Cardiac malformations in trisomy-18: A study of 41 postmortem cases. J Am Coll Cardiol 1989;13:1586. VanTuinen P, Dobyns WB, Rich DC, et al. Molecular detection of microscopic and submicroscopic deletions associated with MillerDieker syndrome. Am J Hum Genet 1988;43:587. Varon R, Vissinga C, Platzer M, et al. Nibrin, a novel DNA double-strand break repair protein, is mutated in Nijmegen breakage syndrome. Cell 1998;93(3):467. Venter JC, Adams MD, Myers EW, et al. The sequence of the human genome. Science 2001;291:1304. Verkerk AJMH, Pieretti M, Sutcliffe JS, et al. Identification of a gene (FMR-1) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile-X syndrome. Cell 1991;65:905. Von Koskull H, Gahmberg N, Salonen R, et al. FRAXA locus in fragile X diagnosis: Family studies, prenatal diagnosis, and diagnosis of sporadic cases of mental retardation. Am J Med Genet 1994;51:486. Warburton D, Kline J, Stein Z, et al. Monosomy X: A chromosome anomaly associated with young maternal age. Lancet 1997;1:161.
566
Genetic, Metabolic, and Neurocutaneous Disorders / 22
Wertelecki W, Graham JM Jr, Sergovich FR. The clinical syndrome of triploidy. Obstet Gynecol 1978;47:69. Wilkie AOM, Buckle VJ, Harris PC, et al. Clinical features and molecular analysis of the α thalassemia/mental retardation syndromes. I. Cases due to deletions involving chromosome band 16p13.3. Am J Hum Genet 1990;46:1112. Willard HF. Centromeres of mammalian chromosomes. Trends Genet 1990;6:410. Wilson GN, Raj A, Baker D. The phenotypic and cytogenetic spectrum of partial trisomy 9. Am J Med Genet 1985;20:277. Wilson RD, Johnson J, Windrim R, et al. The early amniocentesis study: A randomized clinical trial of early amniocentesis and midtrimester amniocentesis. 2. Evaluation of procedure details and neonatal congenital anomalies. Fetal Diagn Ther 1997;12:97. Wisniewski KE. Down syndrome children often have brain with maturation delay, retardation of growth, and cortical dysgenesis. Am J Med Genet 1990;7 (Suppl):274. Woodage T, Deng Z-M, Prasad M, et al. A variety of genetic mechanisms are associated with the Prader-Willi syndrome. Am J Med Genet 1994;54:219. Woods CG, Bankier A, Curry J, et al. Asymmetry and skin pigmentary anomalies in chromosome mosaicism. J Med Genet 1994;31:694. Wright-Talamante C, Cheema A, Riddle JE, et al. A controlled study of longitudinal IQ changes in females and males with fragile X syndrome. Am J Med Genet 1996;64:350.
Wyllie JP, Wright MJ, Burn J, et al. Natural history of trisomy 13. Arch Dis Child 1994;71:343. Yoshida A, Miura K, Nagao K, et al. Sexual function and clinical features of patients with Klinefelter’s syndrome with the chief complaint of male infertility. Int J Androl 1997;20:80. Yu CE, Oshima J, Wijsman EM, et al. Mutations in the consensus helicase domains of the Werner syndrome gene. Werner’s Syndrome Collaborative Group. Am J Hum Genet 1997;60:330. Yu S, Pritchard M, Kremer E, et al. Fragile X genotype characterized by an unstable region of DNA. Science 1991;252:1179. Yunis JJ. High resolution of human chromosomes. Science 1976;191:1268. Yunis JJ. Mid-prophase human chromosomes. The attainment of 2000 bands. Hum Genet 1981;56:293. Zakian VA. Telomeres: Beginning to understand the end. Science 1995;270:1601. Zalfa F, Bagni C. Molecular insights into mental retardation: Multiple functions for the fragile X mental retardation protein? Curr Issues Mol Biol 2004;6:73. Zeschnigk M, Lich C, Buiting K, et al. A single-tube PCR test for the diagnosis of Angelman and Prader-Willi syndromes based on allelic methylation differences at the SNRPN locus. Eur J Hum Genet 1997;5:94.
CHAPTER 23
Aminoacidemias and Organic Acidemias Gregory M. Enns, Tina M. Cowan, Ophir Klein, and Seymour Packman
Approximately 4% of individuals born in the United States have a genetic or partly genetic disorder. Inborn errors of metabolism contribute significantly to this total. Although individually rare, the aggregate incidence of metabolic disease is relatively high and may be greater than 1 in 1000 newborns. Newborn screening programs using tandem mass spectrometry, which can detect approximately 20 inborn errors of metabolism, typically have reported an incidence of 1 in 2000 to 1 in 4000. Because there are hundreds of known metabolic conditions, the aggregate estimate seems reasonable. Metabolic diseases infrequently produce symptoms immediately at birth, and they can manifest with slowly progressive encephalopathies. In this setting, histologic or biochemical abnormalities may be present in the fetal central nervous system by 4 to 5 months’ gestation. Inborn errors of metabolism also can manifest with rapid clinical deterioration in the newborn period or after an interval period of good health. Presenting clinical features are often nonspecific, and they may be misdiagnosed as infection, cardiovascular compromise, other causes of hypoxemia, trauma, primary brain anomalies, or the effects of a toxin. Recognition of patterns of clinical presentation and rapid implementation of laboratory investigations are essential for the initiation of appropriate therapy without delay. Unless appropriate therapy is initiated with dispatch, there is a high risk of morbidity or mortality, regardless of the cause of the acute illness. This chapter provides an overview of concepts of diagnosis and treatment for two categories of inborn errors: aminoacidopathies and organic acidemias. The general approaches described are broadly applicable to other heritable metabolic disorders, such as disorders of fatty acid oxidation, urea cycle disorders, and lactic acidosis syndromes. Descriptions of selected disorders of amino acid and organic acid metabolism are provided to illustrate and emphasize the approaches to diagnosis, treatment, and genetic counseling in this area of genetic medicine.
SIGNS AND SYMPTOMS Any infant, child, or adult who presents with neurodevelopmental delays, lethargy, feeding difficulties, vomiting, jaundice, failure to thrive, apnea or tachypnea, hypotonia or hypertonia, ataxia, movement disorders, seizures, or coma should be considered to suffer from diseases in one of two broad categories: disorders resulting from causes such as infection, cardiopulmonary dysfunction, other causes of hypoxemia, toxins, or trauma or from primary brain abnormalities or disorders caused by an inborn error of me-
tabolism. Because metabolic diseases are individually rare, there is a tendency to consider them only after excluding more common causes of acute or chronic illness or distress. However, the clinician must consider the possibility of an inborn error on initial presentation. In many cases, only rapid diagnosis and management can prevent death or significant morbidity. Appropriate laboratory investigations should be obtained immediately. Even conventional clinical laboratory tests such as those for blood gases, blood glucose, electrolytes, lactate, ammonia, liver function, hematologic counts and indices, and urinalysis (including pH, ketones, mellituria, and concentration) may provide valuable clues to the underlying diagnosis. The onset of symptoms of metabolic disease is generally postnatal, often appearing after an interval of apparent good health. This interval may be as short as a few hours or last several days to years. An affected individual may fare well until subjected to a catabolic insult (e.g., infection, fasting, dehydration) or an excessive protein or carbohydrate load, after which the infant, child, or adult may suddenly become strikingly ill. In a neonate, the absence of a normal period of apparent good health does not exclude an inborn error from diagnostic consideration. Neonatal distress from asphyxia or pregnancy complications may be the environmental stress that unmasks an underlying metabolic disease. Irritability and feeding difficulties may be associated with uncoordinated sucking or swallowing or with abnormal muscle tone. Persistent and severe vomiting and seizures may occur. In mildly affected patients, symptoms can disappear, only to recur in days or weeks. More severely affected infants and children have inexorable progression from lethargy to coma, episodic apnea, and death. More limited symptoms, often in the form of generalized or partial seizures, may occur in some instances. These can include staring spells, eye rolling or myoclonus, and various combinations of tone abnormalities, tremulousness, lethargy, and a weak cry. The electroencephalogram may suggest nonspecific, diffuse encephalopathy. Unless an inborn error is suspected, the child may be misdiagnosed as having hypoxic-ischemic encephalopathy, intraventricular hemorrhage, sepsis, heart failure, or gastrointestinal illness (e.g., pyloric stenosis, intestinal obstruction).
PHYSICAL FINDINGS A paucity of abnormal physical findings is the general rule in heritable metabolic diseases. Nevertheless, certain components of the physical examination should be emphasized. A detailed ocular examination is essential. Corneal clouding, cataracts, optic nerve abnormalities, and macular or
568
Genetic, Metabolic, and Neurocutaneous Disorders / 23
retinal pigmentary changes may be helpful in establishing a diagnosis. Hepatomegaly can occur with organic acidemias that may have a Reye syndrome–like presentation. Alopecia, abnormal hair, or nonspecific eczematoid dermatitis may be seen in some aminoacidopathies and organic acidemias. An unusual odor of the child’s body or urine has been associated with several organic acidemias and disorders of amino acid metabolism. Ketosis accompanies many of these conditions, and ketone bodies in the urine cause its sweet odor. Although dysmorphic features suggest the diagnosis of a congenital developmental disorder rather than a heritable metabolic disorder, craniofacial and structural abnormalities of organ systems are being recognized in an increasing number of inborn errors of intermediary metabolism.
LABORATORY APPROACHES TO DIAGNOSIS Because the clinical presentation of patients with metabolic disorders is often nonspecific and suggests a wide variety of conditions, a rational and systematic laboratory approach is imperative for rapid and accurate diagnosis to implement early and appropriate treatment. It is rarely possible to base a precise diagnosis on clinical findings or results of routine laboratory tests. Laboratory testing for the symptomatic patient can proceed at many levels, including metabolic screening tests, quantitative metabolite profiles, specific enzyme or other functional assays, and DNA mutation analysis. The specific laboratory approach is often dictated by the clinical and family history and by results of routine laboratory investigations. An extensive description of diagnostic algorithms for the laboratory evaluation of patients suspected of having a metabolic disease has been published [Saudubray and Charpentier, 2001]. For the acutely ill patient, a comprehensive evaluation should include quantitative assessment of plasma amino acids, urine organic acid analyses, plasma carnitine (free and total) levels, and identification and quantitation of acylcarnitines in plasma or serum. These tests should be ordered in conjunction with other basic tests, including hematologic cell counts, electrolytes, blood glucose, blood gases, uric acid, liver transaminases, ammonia, and lactic and pyruvic acid levels. This approach can identify many cases of amino acid disorders and organic acidemias. The interpretation of metabolic tests is greatly enhanced when the laboratory is made aware of the clinical, medication, and dietary history of the patient because these factors can significantly influence results. Depending on the clinical evaluation and results of basic chemistry studies, additional testing may be warranted; these may include levels of urine orotic acid (e.g., elevated in certain urea cycle defects) (see Chapter 24), cerebrospinal fluid glycine (together with the plasma glycine level, which is elevated in glycine encephalopathy), cerebrospinal fluid neurotransmitters (see Chapter 30), and urine S-sulfocysteine (elevated in sulfite oxidase deficiency or molybdenum cofactor deficiency). Laboratory investigations are most useful when samples are collected during an acute episode, because metabolic abnormalities are most pronounced at that time. However, subtle abnormalities can often be appreciated even between episodes, particularly if the laboratory is made aware of the
clinical evaluation at the time of testing. However, normal results, particularly if obtained when the patient is well, do not exclude a metabolic disorder and should be followed by repeat testing of specimens obtained during an acute illness if possible. Metabolic screening tests in urine can be useful in certain situations, particularly in the assessment of older patients with a nonspecific history of developmental delay or mental retardation. Such testing includes qualitative amino acid screening by thin-layer chromatography or paper chromatography, the ferric chloride test for phenylketones (for identification of phenylketonuria and tyrosinemia), the cyanide-nitroprusside test for sulfur-containing amino acids (for identification of homocystinuria), and other colorimetric or flocculation tests. When taken in conjunction with clinical and other laboratory finding, these tests can give an inexpensive and rapid indication of an abnormality, and they can be useful in determining the direction of more specific testing. These tests are not appropriate in the evaluation of an acutely ill patient, for whom specific, quantitative metabolic studies are essential. Depending on the results of initial metabolic studies, confirmation of the diagnosis or delineation of specific disease subtypes may be established by specific enzyme assays. If the expression of enzyme activity is tissue specific, a biopsy (e.g., skin, muscle, liver) may be required. After a precise biochemical diagnosis has been established, molecular studies for the specific gene mutation may be possible. In many cases, delineation of the specific mutations can provide important prognostic information and can be used in the testing of other family members and in prenatal diagnosis.
TREATMENT For all inborn errors, acute symptoms must be treated immediately, regardless of the cause, and often before the results of screening and specialized laboratory tests become available. The success of treatment is a function of time; the longer the neurologic derangements persist before treatment, the poorer the prognosis. Because acidosis (or alkalosis) is observed in these disorders, acid-base status must be corrected immediately, along with necessary adjustments in electrolyte balance and hydration. Glucose infusions should be used as a source of calories and used to control hypoglycemia, if present. Hemodialysis can improve a number of disorders of amino acid and organic acid metabolism, and it should be instituted if the evidence suggests such a disorder. Selective avoidance of a particular nutrient or class of nutrients is specific and crucial. This generally means avoidance of one or more specific micronutrients that can accumulate proximal to the metabolic block. Protein should be avoided in the acute phase of treatment of any child presenting with neurologic dysfunction; continuation of dietary protein in a child with an aminoacidopathy or organic acidemia can be lethal. The response to protein avoidance may be of diagnostic help. When specific nutritional restrictions are instituted for a known or suspected inborn error, attention must be paid to adequate total caloric intake—by parenteral or oral administration—to prevent catabolism and to avoid iatrogenic nutritional deficiencies.
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
Specific supplements may be invaluable as treatment adjuncts under the general strategy designed to remove toxic metabolites by alternative or minor pathways. In selected disorders, glycine supplementation promotes the formation of rapidly excreted and nontoxic acylglycine conjugates. Carnitine administration favors the formation and excretion of acetylcarnitine and other acylcarnitines, thereby ameliorating ketosis and the accumulation of toxic organic acid metabolites in organic acidemias. A number of inborn errors respond favorably and, in some instances, dramatically to the administration of vitamins, which stabilize or otherwise increase the catalytic activity of incompletely defective enzymes. Vitamins such as cobalamin (B12), pyridoxine, thiamine, biotin, riboflavin, lipoate, folate, and niacin, administered in pharmacologic doses, may be lifesaving. In a child who is gravely ill and whose course has been one of inexorable decline, it is appropriate to administer a battery of rationally chosen cofactors and supplements in the hope that the child’s biochemical lesion will respond to one of the pharmacologic agents.
INHERITANCE AND GENETIC COUNSELING Treatment of heritable metabolic disorders involves considerations beyond the acute phase of the illness and even beyond the prognosis of the proband. Because of the importance of genetic counseling to the family, the physician has an obligation to try to arrive at a diagnosis, however poor the prognosis for the proband. Identifying a specific entity enables the family to be counseled about recurrence risks. Most inborn errors of metabolism are inherited as autosomal recessive traits. There are a few disorders, such as the urea cycle defect of ornithine transcarbamylase deficiency, that are inherited as X-linked disorders. In the case of an autosomal recessive condition, the affected relative is a sibling of either gender. In X-linked disorders, the affected relative may be a maternal uncle, a brother, or a mildly affected mother or other female relative. Some disorders are caused by mitochondrial DNA mutations (see Chapter 28), and maternal transmission to all children in a sibship is observed. In all circumstances, a detailed family history may reveal an affected relative who has a similar illness, and this can be of diagnostic importance. Special attention should be given to a family history of stillbirths, unexplained deaths, and neurologic diseases or delayed development of any degree or severity. The therapeutic repertory for inborn errors is expanding beyond nutritional manipulations and restrictions of micronutrient precursors proximal to a metabolic block. Modalities being used or clinically investigated include cofactors as pharmacologic agents in vitamin-responsive inborn errors; enzyme inhibitors to prevent the synthesis of a toxic metabolite; enzyme-stabilizing agents; organ transplantation (e.g., liver, bone marrow); enzyme replacement therapy; and gene therapy. Such therapies may be intrusive and expensive. Genetic counseling for inborn errors must include a discussion of recurrence risk and address issues related to therapeutic options, prognosis, prenatal management, and the emotional, psychologic, and financial burdens of the birth and long-term treatment of children with such chronic disorders. Many of the inborn errors discussed in this chap-
569
ter and elsewhere can be diagnosed prenatally, giving families a number of reproductive options. The successful prenatal treatment of cofactor-responsive disorders and the expanding repertory of other novel postnatal treatment approaches augur an increasing focus on unique therapeutic opportunities in inborn errors.
AMINOACIDEMIAS Phenylketonuria Phenylketonuria, described by Asbørn Følling in 1934 [Følling, 1994], is caused by deficient activity of phenylalanine hydroxylase (PAH), a hepatic enzyme that converts phenylalanine to tyrosine (Fig. 23-1). The biochemical block results in the accumulation of phenylalanine, which is then converted to phenylpyruvic acid and phenyllactic acid, phenylketones that are excreted in the urine. Tetrahydrobiopterin is a necessary cofactor in the PAH reaction, and elevated phenylalanine levels rarely may be caused by inherited disorders of tetrahydrobiopterin synthesis, including guanosine triphosphate (GTP) cyclohydrolase I, 6-pyruvoyltetrahydrobiopterin synthase, pterin-4α-carbinolamine dehydratase, and dihydropteridine reductase deficiencies (see Fig. 23-1). Phenylalanine is neurotoxic, and untreated patients with classic phenylketonuria are typically mentally retarded. In the 1950s, a diet in which phenylalanine intake was restricted was shown to normalize plasma phenylalanine levels and stop urinary excretion of phenylpyruvic acid [Bickel et al., 1953]. Selective restriction of phenylalanine intake by using phenylalanine-free medical formulas and foods (and tyrosine supplementation), which provides enough additional protein and nutrients to support normal growth, remains the mainstay of phenylketonuria therapy. Mandatory population newborn screening for phenylketonuria, in combination with postnatal presymptomatic therapy, was begun in the 1960s using the Guthrie bacterial inhibition assay [Guthrie and Susi, 1963; Koch, 1997]. Modern newborn screening programs have switched to techniques that directly assay phenylalanine and tyrosine levels; the most recent innovation is tandem mass spectrometry. The presymptomatic institution of and continued adherence to specific dietary therapy prevents mental retardation. Phenylketonuria is a paradigmatic and landmark success story in biochemical genetics, and it is reviewed in some detail.
Classification A blood phenylalanine level above the normal range (30 to 110 μM) is referred to as hyperphenylalaninemia. Patients have been classified as having nonphenylketonuria hyperphenylalaninemia if their blood phenylalanine levels without dietary therapy are 360 to 600 μM. Classic phenylketonuria is characterized by untreated phenylalanine levels of more than 1000 μM [Scriver and Kaufman, 2001]. A range of reduced PAH-specific activity correlates broadly with the severity of the phenotype. When it has been measured directly (i.e., liver biopsy) or indirectly (i.e., 13 L-[1- C]phenylalanine breath test), residual liver PAHspecific activity is relatively high in milder hyperphenylal-
570
Genetic, Metabolic, and Neurocutaneous Disorders / 23 Phenylanine
Tyrosine
Phenylalanine hydroxylase
(1) 4␣–Hydroxytetrahydrobiopterin (2)
7,8–Dihydrobiopterin (BH2)
6–Pyruvoyltetrahydropterin 6–Pyruvoyltetrahydropterin (5) synthase
Tetrahydrobiopterin (BH4) (6) Sepiapterin reductase
Dihydroneopterin GTP cyclohydrolase
Carbinolamine dehydratase
Dihydropteridine reductase
(4) GTP
(3) NAD⫹
NADH
FIGURE 23-1. Regulation of phenylalanine hydroxylase activity. Phenylalanine is converted to tyrosine (1) by the holoenzyme phenylalanine hydroxylase (PAH). PAH requires tetrahydrobiopterin (BH4) as an active cofactor and is recycled by the sequential actions of carbinolamine dehydratase (2) and dihydropteridine reductase (3). BH4 is synthesized in vivo through a complex series of steps that involve guanosine triphosphate (GTP) cyclohydrolase (4), 6-pyruvoyltetrathydropterin synthase (5), and sepiapterin reductase (6). Genetic defects at any of these steps may be associated with hyperphenylalaninemia. (From Wilcox WR, Cederbaum SD. Amino acid metabolism. In: Rimoin D, Connor J, Pyeritz R, Korf B, eds. Principles and practice of medical genetics, 4th ed. Philadelphia: Churchill Livingstone, 2002:2406.)
aninemic patients, whereas enzyme activity is zero-to-low in the more severe cases of classic phenylketonuria [Bartholome et al., 1975]. Measured PAH activity also correlates to some degree with tolerance for dietary protein [Güttler et al., 1996]. Patients with classic phenylketonuria can tolerate very little phenylalanine in the diet (80% in most cases), but urine screening may miss it in some patients [Dhondt, 1984]. The measurement of DHPR activity in neonatal dried blood spots using a spectrophotometric assay is an effective method for diagnosis of DHPR deficiency. Urine pterin analysis and DHPR activity screening should be performed early in the management of a new patient with persistent hyperphenylalaninemia, or these disorders may be missed. Mutation analysis has yet to identify clear genotype-phenotype correlations [Blau et al., 1996].
Treatment The goals of therapy are to decrease the level of phenylalanine to an acceptable range (120 to 360 μM) and correct the neurotransmitter deficiencies with exogenous supplementation. The diet is similar to that used to treat classic phenylketonuria, but patients tend to have a higher phenylalanine tolerance (300 to 700 mg/day) [Blau et al., 2001]. Tetrahydrobiopterin supplementation (2 to 20 mg/kg/day) is also used to help control blood phenylalanine levels. Lower tetrahydrobiopterin doses (2 to 5 mg/kg/day) may be effective in GTPCH and PTPS deficiencies, whereas higher doses (up to 20 mg/kg/day) may be required in DHPR deficiency. L-Dopa and 5-hydroxytryptophan are administered in a dose of 1 to 10 mg/kg/day. Carbidopa, an inhibitor of peripheral aromatic amino acid decarboxylase, decreases the conversion rates of L-dopa to dopamine and 5-hydroxytryptophan to serotonin, allowing for the use of lower doses of these compounds; these therapeutic adjuncts may be especially helpful in severe forms of tetrahydrobiopterin deficiency. The optimal dose of each medication must be determined for each patient. Mild forms of disease may respond to tetrahydrobiopterin supplementation alone. Measuring levels of cerebrospinal fluid neurotransmitter metabolites (i.e., homovanillic acid and 5-hydroxyindolacetic acid) is useful in
575
monitoring the efficacy of treatment [Blau et al., 2001; Shintaku, 2002]. Side effects of therapy include choreoathetosis, dystonia, and on-off phenomena, which are also features of the underlying disorders [Tanaka et al., 1989]. Tachycardia, diarrhea, and anorexia are associated with 5-hydroxytryptophan administration [Dhondt, 1993]. L-Deprenyl, a monoamine oxidase inhibitor, has been useful in decreasing catabolism of L-dopa and 5-hydroxytryptophan, allowing lower dosing [Schuler et al., 1995; Spada et al., 1995, 1996]. A low concentration of cerebrospinal fluid folate is typical in DHPR deficiency, and it is treated by folinic acid supplementation (10 to 20 mg/day) [Shintaku, 2002]. Trimethoprim-sulfamethoxazole and methotrexate are DHPR inhibitors, and they may cause serious side effects in patients with tetrahydrobiopterin deficiency [Millot et al., 1995; Woody and Brewster, 1990]. Neurologic function may improve with therapy, but the overall prognosis for these disorders is largely unknown.
Hepatorenal Tyrosinemia Hepatorenal tyrosinemia (i.e., tyrosinemia type I) is characterized principally by liver, kidney, and peripheral nerve involvement. The clinical spectrum ranges from severe hepatic failure in early infancy to later presentations of chronic liver disease and rickets in an older child. The overall incidence is 1 case per 100,000 births. In Quebec the incidence is quite high, at 1 in 16,700 births [Bergeron et al., 1974].
Pathophysiology Hepatorenal tyrosinemia is caused by a deficiency of fumarylacetoacetate hydrolase, a distal enzymatic step in the processing of the amino acid tyrosine (Fig. 23-2). Some investigations suggest that metabolites of tyrosine accumulating proximal to the blocked reaction step are toxic to liver and kidney, acting as alkylating agents or by disruption of Tyrosine
Protein synthesis, dopamine, melanin, thyroid hormones (1) p-OH-phenylacetic acid p-OH-phenylpyruvic acid
p-OH-phenyllactic acid
(2) Homogentisic acid (3) Maleylacetoacetic acid (4) Fumarylacetoacetic acid
Succinyl acetone
(5) Fumaric acid
Acetoacetic acid
FIGURE 23-2. The tyrosine metabolic pathway involves several enzymes: tyrosine aminotransferase (1); p-OH-phenylpyruvic acid dioxygenase (2); homogentisic acid oxidase (3); maleylacetoacetic acid isomerase (4); and fumarylacetoacetic acid hydrolase (5). (From Wilcox WR, Cederbaum SD. Amino acid metabolism. In: Rimoin D, Connor J, Pyeritz R, Korf B, eds. Principles and practice of medical genetics, 4th ed. Philadelphia: Churchill Livingstone, 2002:2411.)
576
Genetic, Metabolic, and Neurocutaneous Disorders / 23
sulfhydryl metabolism [Russo et al., 2001]. One of the accumulating metabolites, succinylacetone, has been implicated in the peripheral neuropathy of tyrosinemia [Sassa and Kappas, 1983; Sassa et al., 1983].
Clinical Manifestations In states and countries that include tyrosinemia in newborn screening panels, infants are detected within the first weeks of life. Onset of disease manifestations may be sudden and may occur in the first month of life; a more gradual clinical course may also be seen. Children often manifest failure to thrive, and vomiting, diarrhea, and hepatosplenomegaly are common. Traditional classifications of acute and chronic disease have been replaced by assessment of disease status in target organs (e.g., peripheral nerve, liver, and kidney). Liver disease can include acute decompensations and cirrhosis. There is a high incidence of progression to hepatocellular carcinoma, likely caused by accumulation of mutagenic metabolites. Renal dysfunction ranges from mild tubular dysfunction to frank renal failure. Vitamin D–resistant renal rickets is a common feature. Neurologic involvement can include paresthesias, opisthotonic-like posture, bruxism and tongue biting, and in some cases, motor paralysis leading to respiratory failure and death [Mitchell et al., 1990]. Neurologic crises occur in up to 42% of individuals with tyrosinemia [Kvittingen, 1991]. These crises are biphasic, with an active period of pain, autonomic dysfunction, and sometimes paralysis lasting 1 to 7 days, followed by a period of recuperation. Succinylacetone blocks the heme biosynthetic pathway, and the neurologic crises—a major source of morbidity— therefore have a physiologic basis similar to those in porphyria [Russo et al., 2001].
Laboratory Tests Demonstration of increased serum amino acids in plasma or urine is pathognomonic. Variable hypertyrosinemia is nonspecific. Other findings include diminished serum phosphorus and elevated urinary excretion of phosphate, resulting from reduced tubular phosphorus reabsorption. Glucosuria and hyperaminoaciduria result from renal tubular impairment. Liver dysfunction results in hyperbilirubinemia and hypoproteinemia. Patients usually have leukopenia, anemia, and thrombocytopenia.
Management 2-[2-Nitro-4-trifluoromethylbenzoyl]-1,3-cyclohexanedione (NTBC) is an inhibitor of 4-hydroxyphenylpyruvate dioxygenase (4-HPD), a proximal step in tyrosine catabolism. Inhibition thereby prevents the synthesis of succinylacetone and related metabolites, which accumulate because of the enzymatic block at fumarylacetoacetate hydrolase, a distal step in the pathway. Treatment with this compound is effective within hours and dramatically reduces the risk of neurologic and hepatic crises [Holme and Lindstedt, 2000]. Dietary restriction of phenylalanine and tyrosine is used in combination with NTBC. Liver transplantation is curative for hepatic and nervous system disease, and it is used in those who are refractory to nonsurgical treatment.
Acute management of neurologic crises includes analgesia, glucose (which inhibits ALA synthetase), and symptomatic treatment of hypertension. Repletion of sodium, potassium, and phosphate is necessary. The use of barbiturates and other medications that aggravate porphyria should be avoided before stabilization on NTBC [Kang and Gerald, 1970].
Other Categories of Tyrosinemia Several causes of hypertyrosinemia exist in addition to fumarylacetoacetate hydrolase deficiency (see Fig. 23-2). Deficiency of tyrosine aminotransferase causes tyrosinemia type II (oculocutaneous tyrosinemia) [Hunziker, 1980]. In type II disease, developmental delay, corneal thickening, and hyperkeratosis of palms and soles occur, but there is usually no hepatorenal involvement. Type III disease is caused by deficiency of 4-HPD and has a spectrum of manifestations, ranging from clinically normal to severe mental retardation and neurologic anomalies, including ataxia [Cerone et al., 1997; Ruetschi et al., 2000]. A 4-HPD dysfunction can also cause Hawkinsinuria, a rare condition that can manifest with failure to thrive and metabolic acidosis, but it usually resolves as the patient’s metabolism matures [Borden et al., 1992]. Liver failure can lead to elevated tyrosine levels [Mitchell et al., 2001], as can postprandial testing and diseases such as vitamin C deficiency and hyperthyroidism. Premature infants may manifest transient tyrosinemia of the newborn because of temporary immaturity in the function of 4-HPD. This condition resolves spontaneously, but mild developmental delay has been reported [Nyhan, 1984].
Maple Syrup Urine Disease In 1954, Menkes and colleagues described four siblings who died in early infancy from a cerebral degenerative disease with onset occurring when they were 3 to 5 days old. Symptoms included feeding difficulty, irregular respiratory pattern, hypertonia, opisthotonus, and failure to thrive. All had urine with the smell of maple syrup [Menkes et al., 1954]. Soon thereafter, another patient with a similar history was found to have elevated levels of branched-chain amino acids in urine and blood, and the syndrome was initially referred to as maple sugar urine disease [Westall et al., 1957]. Maple syrup urine disease is caused by mitochondrial branched-chain α-ketoacid dehydrogenase complex deficiency (compared with the composite branched-chain amino acid pathways in Fig. 23-6). The enzymatic defect leads to accumulation of branched-chain amino acids and branched-chain α-ketoacids. Five forms of maple syrup urine disease (i.e., classic, intermediate, intermittent, thiamine-responsive, and dihydrolipoyl dehydrogenase [E3] deficiency) have been delineated based on clinical presentation, level of enzyme activity, and response to thiamine administration [Chuang and Shih, 2001].
Clinical Manifestations CLASSIC MAPLE SYRUP URINE DISEASE In the classic form, the clinical phenotype is one of severe neonatal encephalopathy, unless presymptomatic therapy is
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
initiated in areas where newborn screening for maple syrup urine disease is performed. Untreated neonates typically develop symptoms by the end of the first week of life. Feeding difficulties, alternating hypertonia and hypotonia, opisthotonic posturing, abnormal movements (“fencing” or “bicycling”) and seizures commonly occur. The characteristic urine smell develops on day 5 to 7 of life [Strauss and Morton, 2003a]. Unless an underlying inborn error of metabolism is suspected, affected children may be misdiagnosed as having sepsis and progress to coma and death. Ketosis is often found, and hypoglycemia may occur, but severe metabolic acidosis tends not to occur. Plasma amino acid analysis reveals elevated levels of branched-chain amino acids and the diagnostic presence of alloisoleucine in plasma [Schadewaldt et al., 1999]. Urine organic acid analysis demonstrates excretion of branched-chain α-ketoacids. Hyponatremia and cerebral edema are frequent sequelae during acute metabolic decompensation [Morton et al., 2002]. Other complications include pseudotumor cerebri, pancreatitis, and eye abnormalities [Burke et al., 1991; Kahler et al., 1994]. Ocular findings in untreated or late-diagnosed patients include optic atrophy, gray optic papilla, nystagmus, ophthalmoplegia, strabismus, and cortical blindness [Burke et al., 1991]. Children who survive the initial metabolic crisis typically have significant neurodevelopmental delays and spasticity [Chuang and Shih, 2001]. Although motor, visual, and learning deficits may occur, rapid identification of affected infants and careful institution of appropriate therapy can result in normal development [Kaplan et al., 1991; Morton et al., 2002]. Neuroimaging studies (Fig. 23-3) are typically abnormal in patients with untreated classic maple syrup urine disease who are in crisis. Computed tomographic (CT) scans appear normal in the first few days of life, but they reveal progression to marked generalized cerebral edema if the patient remains untreated [Brismar et al., 1990]. An unusual pattern of edema may occur, characterized by involvement of the cerebellar deep white matter, posterior brainstem, cerebral peduncles, posterior limb of the internal capsule, and posterior aspect of the centrum semiovale. Edema tends to subside in the second month of life [Brismar et al., 1990]. Patients with classic maple syrup urine disease in metabolic crisis with associated hyponatremia demonstrate a prominently increased T2 signal on brain MRI in the brainstem reticular formation, dentate nucleus, red nucleus, globus pallidus, hypothalamus, septal nuclei, and amygdala [Morton et al., 2002]. One report observed that brain MRI abnormalities were absent or only slight in sick patients with maple syrup urine disease in the absence of hyponatremia [Morton et al., 2002]. Cranial ultrasonography of neonates in acute metabolic crisis reveals symmetrically increased echogenicity of the periventricular white matter, basal ganglia, and thalami [Fariello et al., 1996]. Chronic changes, including hypomyelination of the cerebral hemispheres, cerebellum, and basal ganglia and cerebral atrophy, may supervene in poorly controlled patients. CT- and MRIdefined abnormalities and the clinical phenotype may improve after implementation of appropriate dietary therapy [Taccone et al., 1992]. Diffusion-weighted imaging and spectroscopy have also documented abnormalities during the acute phase of disease [Cavalleri et al., 2002]. Markedly restricted proton diffusion, suggestive of cytotoxic or intramyelinic sheath edema, was demonstrated in the brainstem,
577
basal ganglia, thalami, cerebellar and periventricular white matter, and cerebral cortex in six patients with maple syrup urine disease. MRS demonstrated abnormal elevations of branched-chain amino acids, branched-chain α-ketoacids, and lactate in the four patients. All of these changes were reversed after the institution of appropriate nutritional and antibiotic therapy to treat intercurrent illness [Jan et al., 2003]. A characteristic comblike electroencephalographic pattern may be demonstrated for some patients with classic maple syrup urine disease between the second and third weeks of life [Tharp, 1992]. This unusual rhythm pattern resolves with the institution of dietary therapy [Tharp, 1992].
INTERMEDIATE MAPLE SYRUP URINE DISEASE Children who have the intermediate form of maple syrup urine disease do not present in the neonatal period, despite having persistently elevated plasma levels of branched-chain amino acids. Developmental delay and failure to thrive are common. Severe neurologic impairment is absent; episodes of metabolic decompensation may occur, although severe ketoacidosis episodes are variable [Gonzalez-Rios et al., 1985a]. These children have a higher tolerance for dietary protein than those who have the classic form [Gonzalez-Rios et al., 1985a]. Rarely, patients with intermediate-type maple syrup urine disease respond to thiamine administration.
INTERMITTENT MAPLE SYRUP URINE DISEASE Patients with intermittent maple syrup urine disease typically come to medical attention when they are 5 months to 2 years old and after stress induced by infection or highprotein intake; some have been detected as late as the fifth decade of life [Chuang and Shih, 2001]. The intermittent form of maple syrup urine disease can be particularly difficult to diagnose, because affected individuals have normal levels of branched-chain amino acids and no odor between episodes of metabolic decompensation. Episodic decompensation is characterized by ataxia, disorientation, and altered behavior, which may progress to seizures, coma, and even death unless therapy is instituted. Early development and intellect are usually normal.
THIAMINE-RESPONSIVE MAPLE SYRUP URINE DISEASE The clinical course of patients with the thiamine-responsive variant of maple syrup urine disease is similar to that of the intermediate form of disease. Plasma levels of branchedchain amino acid and urine excretion of branched-chain α-ketoacids decline days to weeks after thiamine administration (10 to 1000 mg/day) is started [Scriver and Kaufman, 2001]. Patients are also treated with nutritional regimens similar to those used in other forms of maple syrup urine disease. Developmental delay may be present, but normal intelligence has also been documented [Scriver et al., 1971].
DIHYDROLIPOYL DEHYDROGENASE–DEFICIENT MAPLE SYRUP URINE DISEASE The dihydrolipoyl dehydrogenase (E3)–deficient form of maple syrup urine disease is characterized by ketoacidotic crises in infancy. There is also lactic acidemia because the
578
A
C
Genetic, Metabolic, and Neurocutaneous Disorders / 23
B
FIGURE 23-3. Maple syrup urine disease. A, Axial view, T2-weighted image shows edema in the internal capsules, lateral thalami, and globus pallidi. B, Axial view, calculated apparent diffusion coefficient image at the same level shows hypointensity, indicated by reduced water diffusion, in the affected areas. C, Proton magnetic resonance spectroscopy (echo time of 26 msec) shows a large peak at 0.9 ppm, believed to represent resonances of methyl protons from branched-chain amino acids and branched-chain αketoacids that accumulate as a result of defective oxidative decarboxylation of leucine, isoleucine, and valine. (Courtesy of Dr. A James Barkovich, University of California, San Francisco, CA.)
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
E3 subunit of the branched-chain α-ketoacid dehydrogenase complex is also required for catalytic function of pyruvate dehydrogenase and α-ketoglutarate dehydrogenase. In addition to the typical maple syrup urine disease metabolites, urine organic acid analysis reveals the presence of lactate, pyruvate, and α-ketoglutarate. The neonatal period is usually uneventful, but progressive neurologic deterioration, characterized by developmental delay, hypotonia or hypertonia, and dystonia, supervenes. Death in early childhood is common. Attempts at therapy have had limited success [Chuang and Shih, 2001; Sakaguchi et al., 1986].
Laboratory Tests Maple syrup urine disease can be detected easily and accurately by tandem mass spectrometry analysis of the newborn blood spot [Chace et al., 1995]. Although tandem mass spectrometry used in newborn screening is effective in diagnosing maple syrup urine disease, such screening is not yet universal. Urine screening tests for the presence of α-ketoacids (i.e., ferric chloride and 2,4-dinitrophenylhydrazine [DNPH]) may be positive, but the results are nonspecific and insensitive. Plasma amino acid analysis demonstrates elevations of leucine, isoleucine, and valine (5- to 10-fold greater than normal) [Strauss and Morton, 2003a]. Levels of branched-chain amino acids are greatly elevated in urine and cerebrospinal fluid [Chuang and Shih, 2001]. The detection of allo-isoleucine is diagnostic [Schadewaldt et al., 1999]. The branched-chain α-ketoacids 2-oxoisocaproic acid, 2-oxo-3-methylvaleric acid, and 2oxoisovaleric acid, derived from the branched-chain amino acids leucine, isoleucine, and valine, respectively, are found to be elevated on urine organic acid analysis during metabolic crises. Branched-chain amino acids levels and excretion of branched-chain α-ketoacids may be normal between episodes of decompensation in the intermittent form of disease. The branched-chain α-ketoacid dehydrogenase complex consists of three catalytic components—a thiamine pyrophosphate–dependent carboxylase [E1] with an α2β2 structure, a transacylase [E2], and a dehydrogenase [E3]— as well as two regulatory enzymes (a kinase and a phosphatase) [Chuang and Shih, 2001]. Deficient activity of this complex leads to the accumulation of leucine, isoleucine, and valine and their corresponding α-ketoacids. The decarboxylation activity can be measured in leukocytes, lymphoblasts, or fibroblasts, and it is loosely related to the clinical phenotype: 0% to 2% of normal activity in classic maple syrup urine disease and 3% to 30% activity in intermediate, 5% to 20% in intermittent, 2% to 40% in thiamine responsive, and 0% to 25% in E3 deficiency [Chuang and Shih, 2001; Scriver et al., 1971]. Because significant overlap exists between measured enzyme activity and clinical phenotype, enzymatic activity cannot be used to predict the clinical course with certainty.
Genetics Maple syrup urine disease is a pan-ethnic, autosomal-recessive condition that can be caused by mutations in any of the components of the mitochondrial branched-chain αketoacid dehydrogenase complex. In a study of 63 indi-
579
viduals, E1β subunit mutations were most common (38%), followed by E1α (33%), and E2 (19%) mutations [Nellis and Danner, 2001]. Branched-chain α-ketoacid dehydrogenase phosphatase or kinase mutations are also predicted to cause maple syrup urine disease, but such abnormalities have not yet been detected. The overall incidence is approximately 1 case per 150,000 people in the general population, but maple syrup urine disease is more common in Old Order Mennonites in southeastern Pennsylvania (1 in 176 births) [Danner and Doering, 1998]. A novel founder mutation in the E1β subunit has been reported in the Ashkenazi Jewish population [Edelmann et al., 2001]. In general, increased residual branched-chain α-ketoacid dehydrogenase activity should convey some advantage, but there is a wide overlap between measured enzymatic activities and clinical outcome. Given the complexity of the molecular genetics, the potential for modifier gene and environmental interactions, and the multiple clinical phenotypes associated with maple syrup urine disease, a lack of definitive genotype-phenotype relationships is not surprising.
Treatment Chronic care of the child with maple syrup urine disease includes regular visits to an integrated metabolic clinic for medical and nutritional assessment. Adequate calories (100 to 120 kcal/kg/day) and protein (2 to 3 g/kg/day) are needed for growth. Chronic valine or isoleucine deficiency may cause an exfoliative dermatitis, and supplementation of these amino acids is often needed [Koch et al., 1993]. Thiamine supplementation is administered to patients with thiamine-responsive forms of maple syrup urine disease. Because patients on restricted diets are at risk for micronutrient and essential fatty acid deficiencies, patients should be periodically monitored for such deficits and supplementation given as needed. Because significant metabolic intoxication may occur rapidly, even in patients with apparently well-controlled disease, it is crucial to have carefully considered home and hospital emergency protocols in place for each child [Morton et al., 2002; Strauss and Morton, 2003a]. Acute metabolic decompensation (e.g., fasting or illness severe enough to cause catabolism) is a medical emergency that requires prompt intervention. Initial intervention is aimed at correcting dehydration, starting high-dose intravenous thiamine, and providing adequate calories (approximately 120 to 140 kcal/kg/day) to prevent further protein catabolism and higher rise in plasma leucine levels. To this end, high-dextrose intravenous fluids (to provide approximately 10 mg/kg/min) and intralipid are often administered. Branched-chain amino acid–free parenteral nutrition or enteral formula, delivered by continuous nasogastric drip, can also be used [Nyhan et al., 1998; Parini et al., 1993]. The rate of decrease of leucine is slowed in the face of valine and isoleucine levels inadequate to stimulate protein synthesis. Acute valine and isoleucine deficiency can be avoided by careful supplementation of these amino acids [Parini et al., 1993]. Leucine is reintroduced to the diet after therapeutic levels are achieved [Morton et al., 2002]. In a study of 36 maple syrup urine disease patients, plasma leucine levels fell to less than 400 μM 2 to 4 days after the initiation of therapy with enteral and parenteral nutrition. Initial leucine levels ranged from 233 to 778 μM
580
Genetic, Metabolic, and Neurocutaneous Disorders / 23
in a group diagnosed on the first day of life (n = 18) and 1489 to 3359 μM in a group diagnosed between days 3 and 16 (n = 18). Over an 11-year period, neurologic examinations, gross motor development, and speech were normal in 34 of 36 children [Morton et al., 2002]. Enteral nutrition was also found to be beneficial when instituted within the first 20 days of life. Four patients receiving nasogastric drip feeding as the only treatment of neonatal classic maple syrup urine disease had normal development when 3 to 5 years old [Parini et al., 1993]. Hemodialysis and continuous venovenous extracorporeal removal therapies result in more rapid fall in plasma levels of branched-chain amino acids, but these modalities typically have been described in single case reports or small series with relatively short follow-up, and it is difficult to ascertain the long-term outcome of such intervention [Gouyon et al., 1996; Puliyanda et al., 2002]. Nevertheless, normal development has been reported for 8 of 12 children after continuous venovenous extracorporeal removal therapy [Jouvet et al., 2001]. Branched-chain amino acids levels often rebound after initial dialysis in cases of severe metabolic imbalance characterized by extremely high leucine levels, and dialysis may need to be repeated in such cases. Peritoneal dialysis is no longer routinely used; there is a tendency for leucine levels to plateau between 1000 and 1500 μM after 24 hours, limiting the utility of this therapeutic modality [Gortner et al., 1989]. Levels of branchedchain amino acids and branched-chain α-ketoacids tend to plateau with exchange transfusion therapy [Nyhan et al., 1998; Wendel et al., 1982]. Although enteral and intravenous therapy may be sufficient to manage many patients with maple syrup urine disease in acute crisis, various dialysis methods are commonly used and should be considered, especially when clearance of branched-chain amino acids by nutritional support is not effective or when other considerations such as life-threatening cerebral edema, renal imbalance, or cardiovascular abnormalities exist [Jouvet et al., 2001; Nyhan et al., 1998]. Liver transplantation has been performed rarely for maple syrup urine disease. Three patients who underwent successful transplantation were able to resume normal diets and were no longer at risk for metabolic deP
CHO ⫹ CH2⫺COOH
P
compensation [Wendel et al., 1999]. However, the inherent risks and expense of transplantation, when compared with the relative ease and success of nutritional therapy, make such invasive treatment the exception rather than the rule. Because hyponatremia and subsequent brain edema are serious and relatively common complications, it is important to monitor serum sodium and serum and urine osmolalities closely and replace urinary losses with saline [Morton et al., 2002]. Critical brain swelling and abnormal brainstem function may develop with only a moderate reduction in serum sodium level (by only 8 to 10 mEq/L) [Morton et al., 2002]. Low-dose diuretics may also be used to prevent water retention [Strauss and Morton, 2003a]. Mannitol is reserved for life-threatening episodes of increased intracranial pressure [Morton et al., 2002].
Glycine Encephalopathy Glycine encephalopathy, also known as nonketotic hyperglycinemia, is an autosomal-recessive disorder caused by defective function of the multimeric glycine cleavage enzyme system, leading to accumulation of glycine in all body tissues, including the central nervous system (Fig. 23-4). Gerritsen and colleagues [1965] described the initial patient in 1965. The glycine cleavage enzyme system has four components: the P protein (a pyridoxal phosphate–dependent glycine decarboxylase), the T protein (a tetrahydrofolatedependent protein), the H protein (a hydrogen carrier protein), and the L protein (lipoamide dehydrogenase). Infants with classic disease present in the first week of life with apnea, lethargy, severe hypotonia, and feeding difficulties [Hoover-Fong et al., 2004]. Respiratory failure, hiccups, and intractable seizures develop, and most infants die unless assisted ventilatory support is provided. Intermittent ophthalmoplegia is a relatively frequent finding [MacDonald and Sher, 1977]. The electroencephalogram commonly has a burst suppression pattern, but hypsarrhythmia has been reported rarely [Hoover-Fong et al., 2004]. Brain imaging results are normal for about one half of the neonatal-onset cases [Hoover-Fong et al., 2004]. Relatively common brain abnormalities include agenesis of the corpus
CH⫽N⫺CH2⫺COOH
NH2 S
glycine H
S
CO2
H
S⫺CH2⫺NH2 ⫹ P
P
CHO
CH⫽N⫺CH2⫺S
HS
H HS
T SH 5,10⫺CH2⫺THF ⫹ NH3 ⫹
L
H SH
NAD⫹
NAD⫹ ⫹ H⫹
FIGURE 23-4. The glycine cleavage system. Circles designate proteins with the active group shown. In the presence of P and H proteins, glycine is decarboxylated, and the remaining aminoethyl group binds to the reduced lipoic acid on the H protein. T protein is required to release ammonia and transfer the x carbon of glycine to tetrahydrofolate (THF), forming 5,10-CH2-THF. The L protein is necessary to regenerate the correct form of the H protein. (From Scriver C, Beudet A, Sly W, Valle D, eds. The metabolic and molecular basis of inherited disease, 8th ed. New York: McGraw-Hill, 2001:2066. Reprinted with permission from The McGraw-Hill Companies.)
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
callosum, progressive atrophy, and delayed myelination [Hoover-Fong et al., 2004]. Acute hydrocephalus, requiring shunting, may occur and is a poor prognostic sign [Van Hove et al., 2000]. 1H-MRS detects increased intracerebral levels of glycine, lactate, and creatine [Viola et al., 2002]. The lethal form of glycine encephalopathy appears to be associated with elevated levels of brain myo-inositol glycine, creatine, and N-acetylaspartate. Diffusion-weighted imaging has shown high-signal-intensity lesions in the pyramidal tracts, middle cerebellar pedicles, and dentate nuclei, likely reflecting myelin spongiosis [Sener, 2003]. Atypical and transient variants of glycine encephalopathy have also been reported in patients with cerebrospinal fluid–to-plasma glycine ratios of more than 0.08. Atypical forms manifest in infancy or early childhood after an uneventful pregnancy and neonatal period. Clinical features include seizures (in most cases) and relatively mild developmental delay. Atypical glycine encephalopathy documented by liver enzymology has also been reported in siblings with normal cerebrospinal fluid glycine levels and cerebrospinal fluid–to-plasma glycine ratios [Jackson et al., 1999]. Transient glycine encephalopathy is characterized by the same initial clinical and biochemical findings as the classic form, but it has only rarely been reported. In the transient form, cerebrospinal fluid and plasma glycine levels partially or completely resolve, and most patients have normal development [Aliefendioglu et al., 2003; Korman et al., 2004]. Transient elevations of cerebrospinal fluid glycine and the cerebrospinal fluid–to-plasma glycine ratio occurred in an asphyxiated patient with pyridoxine-dependent seizures [Maeda et al., 2000]. Diagnosis of glycine encephalopathy is established by detecting an elevated cerebrospinal fluid glycine concentration, typically 15 to 30 times normal, in association with an increased cerebrospinal fluid–to-plasma glycine ratio (normal < 0.02) [Applegarth and Toone, 2001; Hamosh and Johnston, 2001]. Classic neonatal-onset patients often have ratios higher than 0.2, whereas atypical patients have ratios of approximately 0.09 [Hamosh and Johnston, 2001]. A ratio higher than 0.08 is usually considered diagnostic for glycine encephalopathy. The plasma and cerebrospinal fluid samples should be obtained as closely as possible to one another, and the presence of blood in the cerebrospinal fluid invalidates the amino acid results [Applegarth and Toone, 2001]. Other causes of increased cerebrospinal fluid glycine levels include valproate therapy, brain trauma, and hypoxicischemic encephalopathy. Secondary elevations of plasma glycine, associated with ketosis, are often encountered in organic acidemias (e.g., methylmalonic, propionic, and isovaleric acidemias and β-ketothiolase deficiency) [Applegarth and Toone, 2001; Korman and Gutman, 2002]. Because sulfite oxidase deficiency (isolated or as part of molybdenum cofactor deficiency), folinic acid–responsive seizures, and disorders of neurotransmitters may have presentations similar to that of glycine encephalopathy, an aliquot of cerebrospinal fluid should also be frozen and saved for appropriate analyses in the event that the result of amino acid analysis is normal. Definitive confirmation of the diagnosis may be accomplished by assaying glycine cleavage enzyme in liver. Between 60% and 80% of patients with the classic neonatal form have defects in the P protein. T protein deficiency
581
occurs in 5% to 20% of cases, whereas H protein and L protein defects are rarely reported [Tada and Kure, 1993]. Prenatal diagnosis by glycine cleavage enzyme system measurement in uncultured chorionic villus samples has resulted in false-negative and false-positive results in at least 1% of cases studied [Applegarth et al., 2000]. DNA analysis, when mutations are known, remains the most reliable form of prenatal diagnosis [Kure et al., 1999]. Comprehensive mutation analysis in 68 families with glycine encephalopathy detected GLDC (P protein gene) or AMT (T protein gene) mutations in 68% of neonatal and 60% of infantile types, respectively. No GCSH (H protein gene) mutations were identified [Kure et al., 2003]. The L protein is a component of pyruvate dehydrogenase and branched-chain ketoacid dehydrogenase, as well as the glycine cleavage enzyme system. However, L protein deficiency leads to a variant form of maple syrup urine disease or pyruvate dehydrogenase deficiency, rather than glycine encephalopathy [Applegarth and Toone, 2001]. Few glycine encephalopathy patients have been identified who carry the same mutations, making genotype-phenotype correlations problematic, although some possible correlations have been found [Applegarth and Toone, 2004]. Three of four patients with transient glycine encephalopathy and homozygosity for a novel GLDC mutation (A802V) had a normal outcome after intensive therapy as neonates. High residual activity of the mutant enzyme and therapeutic intervention during a critical period of brain sensitivity may have contributed to the good outcome in some cases of transient or mild glycine encephalopathy. The three-dimensional structures of the T protein, H protein, and L protein have been determined, which can aid in understanding the molecular mechanisms underlying the effects of missense mutations on glycine cleavage enzyme system activity [Lee et al., 2004]. In postmortem examination specimens from infants who died because of glycine encephalopathy, brain glycine concentrations are elevated twofold to eightfold [Perry et al., 1977]. Neuropathology has demonstrated deficient myelination, abnormal cortical neuron morphology, and spongiosis of the white matter with associated astrocytic gliosis [Brun et al., 1979]. Treatment of glycine encephalopathy has not improved the overall dismal prognosis in the classic form of disease [Chien et al., 2004]. Therapy is focused on controlling seizures with antiepileptic drugs, decreasing tissue glycine levels, and administering N-methyl-D-aspartate (NMDA) receptor antagonists to diminish glycine-induced neuronal excitotoxicity. Valproate is contraindicated because it can inhibit the glycine cleavage enzyme system, and it can cause hyperglycinemia in patients without glycine encephalopathy [Jaeken et al., 1977]. Sodium benzoate is given because of its ability to conjugate to glycine to form hippurate, which can then be excreted in the urine. A glycine-specific mitochondrial enzyme, benzoyl–coenzyme A (CoA):glycine acyltransferase, catalyzes the condensation of benzoate and glycine to form hippurate [Webster et al., 1976]. Sodium benzoate therapy can reduce plasma levels of glycine to the normal range and may have a mild effect on cerebrospinal fluid glycine levels, but it does not affect the dismal prognosis. Because high-dose sodium benzoate therapy can result in carnitine deficiency, plasma carnitine levels should be monitored closely and appropriate supplementation
582
Genetic, Metabolic, and Neurocutaneous Disorders / 23
provided [Van Hove et al., 1995]. Dextromethorphan, an antagonist of the NMDA receptor, is also commonly used in therapy. Treatment with dextromethorphan may lead to improved seizure control and level of interaction in some patients. Ketamine has been used rarely, but it may provide benefit in controlling seizures and improving overall level of interaction [Boneh et al., 1996]. A low-protein diet has no proven efficacy and may result in severe protein malnutrition, micronutrient deficiency, and exfoliative dermatitis if not monitored carefully [Samady et al., 2000]. Sodium benzoate, alone or combined with imipramine, has been effective in improving clinical manifestations in milder forms of glycine encephalopathy [Neuberger et al., 2000; Wiltshire et al., 2000].
Cystathionine β-Synthase Deficiency Cystathionine β-synthase deficiency, the most common cause of homocystinuria, is characterized by multisystem involvement, including mental retardation, lens dislocations, occlusive vascular events, and skeletal deformities.
Pathophysiology The transsulfuration pathway converts methionine into cysteine. In cystathionine β-synthase deficiency, methionine, homocysteine, and homocystine accumulate in the blood and are excreted in large quantities in the urine [Christensen et al., 1991; Mudd et al., 1964]. Two major categories of β-synthase deficiency have been described, one responsive to pyridoxine and the other nonresponsive [Barber and Spaeth, 1969]. One half of patients with cystathionine βsynthase deficiency respond to pyridoxine therapy, and only modest restriction of methionine in their diet is required [Mudd et al., 1985]. Biochemical abnormalities in the central nervous system are thought to account for the occurrence of mental retardation and neurologic abnormalities. Synthesis of cystathionine, an important free amino acid in the brain [Brenton et al., 1965], is impaired, and this compound is virtually absent from the brain in affected individuals. Abnormalities in homocysteine, methionine, and other metabolites probably contribute to central nervous disease as well. Arterial and venous thromboses are prominent in many organs, including the brain. Large and medium-sized blood vessels (i.e., arteries, veins, and dural sinuses) are compromised. Fibrous thickening of the intima occurs, the vessel lumen may be compromised, and the media is also involved, with increased deposition of collagen and frayed,
Sulfur Amino Acid Metabolism and the Homocystinurias Homocysteine lies at a critical juncture between the transsulfuration and remethylation pathways of methionine metabolism, at which point homocysteine can be converted to cystathionine or methionine. The malfunctioning of three enzymes is known to cause homocystinuria: cystathionine β-synthase, methylene tetrahydrofolate reductase, and methionine synthase. The β-synthase enzyme is involved in the transsulfuration pathway (Fig. 23-5), and the latter two enzymes are involved in the sulfur conservation pathway. Several of the mutations that cause methylmalonic acidemia also cause homocystinuria, and these are discussed in the section on cobalamin complementation groups. A transport abnormality, selective intestinal malabsorption of vitamin B12, can also cause homocystinuria. The overall incidence of homocystinuria is approximately 1 case in 335,000 persons, but it varies from 1 in 65,000 in Ireland to 1 in 900,000 in Japan [Naughten et al., 1998].
Serine Methionine THF
Glycine (4)
(3) Methyl⫺B12
(2)
(6) β-adenosylmethionine
(5) Betaine
β-adenosylhomocysteine
N 5,10⫺methylene THF
Dimethylglycine
N5⫺methyl THF
Homocysteine Serine (1)
Homocystine
Cystathionine (7) Cysteine
Cystine
Cysteine sulphinic acid Pyruvate Sulfite (8) Sulfate
FIGURE 23-5. Abbreviated diagram for the transsulfuration pathway. The known genetic defects that cause homocystinuria are a deficiency of cystathionine β-synthase (1), N5,10methylenetetrahydrofolate reductase (2), methionine synthase or methionine synthase reductase (3), and deficient synthesis of methylcobalamin (4). Other defects in the pathway are cystathioninuria caused by γ-cystathionase deficiency (7), sulfite oxidase and molybdenum cofactor synthesis deficiencies (8), and hypermethioninemia from methionine adenosyltransferase deficiency (6). Betaine can be given therapeutically to treat homocystinuria by increasing remethylation of homocysteine by betaine-homocysteine methyltransferase (5). (From Wilcox WR, Cederbaum SD. Amino acid metabolism. In: Rimoin D, Connor J, Pyeritz R, Korf B, eds. Principles and practice of medical genetics, 4th ed. Philadelphia: Churchill Livingstone, 2002:2419.)
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
split smooth muscle fibers. A clotting diathesis is also involved [D’Angelo and Selhub, 1997]. An increased tendency of intravascular thrombosis may be related to abnormal adhesiveness of platelets. However, no single mechanism has been demonstrated to cause the vascular complications. Homocysteine elevation is an independent risk factor for arteriosclerotic vascular disease. This factor has been demonstrated for affected patients and for individuals in the general population who may have modest elevations in homocysteine concentrations. Degenerative changes in the fibers that hold the optic lens likely are caused by interference with fibrillin function [Sakai et al., 1986]. The bone disease likely results from abnormalities in connective tissue, such as defective fibrillin function or perhaps abnormal collagen cross-linking [Harris and Sjoerdsma, 1966].
Clinical Manifestations Four organ systems demonstrate major involvement: the central nervous, skeletal, ocular, and vascular systems [Mudd et al., 1985]. Other organs, such as the liver, hair, muscles, blood, and skin (e.g., hypopigmentation), may be involved. When the central nervous system is involved, the most frequent finding is mental retardation, which can manifest as developmental delay during the first year of life. There is a spectrum of cognitive function in untreated patients, with IQ scores ranging from 10 to 138. Intelligence in B6-responsive patients tends to be higher than in B6 nonresponders. Psychiatric disturbances are common, and seizures and extrapyramidal signs occasionally are seen. Focal neurologic signs point to a cerebrovascular occlusion. Patients identified on newborn screening who receive early treatment have normal cognitive function [Yap et al., 2001]. Skeletal abnormalities include osteoporosis, scoliosis, increased length of long bones, metaphyseal and epiphyseal anomalies, biconcave vertebrae, arachnodactyly, pes planus, and genu valgum. The skeletal and ocular findings may lead to confusion with Marfan’s syndrome. Involvement of the eye is manifested by ectopic lenses (i.e., dislocated downward) and myopia. Involvement occasionally is manifested by glaucoma, retinal changes, cataracts, and corneal changes. Thromboembolic events (arterial and venous), livedo reticularis, and malar flush are some of the vascular findings. Patients have suffered from pulmonary, cerebral, and renal infarction. Cerebral venous sinus thrombosis has been documented with scanning studies. An increased risk of myocardial infarction exists in patients with homocystinuria and in hyperhomocysteinemic members of the general population [Stampfer et al., 1992]. One half of patients will have a vascular event before age 30 years.
Laboratory Tests Homocystinuria occurs in all untreated patients [Isherwood, 1996], but this is not sufficient to establish the diagnosis, because it may occur in patients with other conditions. Serum amino acid analysis reveals elevated total homocysteine, low levels of cysteine, and elevated methionine. Direct assays are used to confirm the enzymatic deficiency,
583
and these can be performed on skin fibroblasts, liver, or leukocytes.
Treatment The goals of treatment are to reduce the severe hyperhomocysteinemia and other biochemical abnormalities. Supportive treatment of complications is essential. Treatment of patients who are B12 responsive consists of pyridoxine in combination with folic acid and vitamin B12 (Wilcken and Wilcken, 1997]. For vitamin B12 nonresponders, treatment is achieved with a methionine-restricted, cystine-supplemented diet (Komrower et al., 1966; Perry et al., 1966]. Pyridoxine, folic acid, and vitamin B12 have been used in pyridoxine nonresponders as cofactors of methionine metabolism to partially promote homocysteine conversions to other metabolites. Betaine, a methyl donor that remethylates homocysteine to methionine, is also an effective component of treatment [Wilcken et al., 1985].
Methionine Synthase Deficiency Methionine synthase lies at the intersection of folate, cobalamin, and sulfur-containing amino acid metabolism. Patients with defects in this enzyme have homocystinuria and low (or normal) methionine levels, but they do not have methylmalonic acidemia.
Pathophysiology Two complementation groups (CblE and CblG) have very similar clinical and laboratory presentations, and they are discussed together. These patients have isolated defects in methionine synthase function caused by mutations in the enzyme itself or abnormalities in the synthesis of the methylcobalamin cofactor.
Clinical Manifestations Most patients present in early infancy with poor feeding, emesis, lethargy, hypotonia, seizures, and developmental delay [Watkins and Rosenblatt, 1989]. There is usually a neurologic presentation, but this can vary and can include gait disturbances and multiple sclerosis-like features [Carmel et al., 1988]. There is a strong association with megaloblastic anemia.
Laboratory Tests Serum cobalamin and folate levels are normal or high, and methylmalonic aciduria is generally not seen [Tuchman et al., 1988]. Homocystinuria is a consistent feature, and CblE and CblG can be differentiated from other causes of homocystinuria by biochemical studies of cultured cells.
Treatment Administration of hydroxocobalamin in pharmacologic doses (with intramuscular administration at initial treatment stages) should begin as soon as the diagnosis is made. This typically leads to rapid biochemical improvement. Some patients also have improvement of anemia on folinic acid
584
Genetic, Metabolic, and Neurocutaneous Disorders / 23
[Harding et al., 1997]. Prenatal therapy has been used for early diagnoses with success [Rosenblatt et al., 1985].
Methylene Tetrahydrofolate Reductase Deficiency In methylene tetrahydrofolate reductase deficiency, the degree of clinical severity varies with enzyme activity. In addition to the severe and moderate cases discussed later, the common 677C→T polymorphism—which can cause mild elevations in homocysteine levels—appears to be a risk factor for hypercoagulable states in the population at large.
Pathophysiology Major findings are demyelination and vascular changes such as those seen in cystathionine β-synthase deficiency [Beckman et al., 1987]. Other changes include dilated cerebral ventricles, hydrocephalus, and microgyria [Kanwar et al., 1976; Wong et al., 1977]. Methylene tetrahydrofolate reductase deficiency is thought to result in low levels of brain folate [Levitt et al., 1971].
Clinical Manifestations Clinical findings vary with enzyme function and include developmental delay, motor and gait abnormalities, seizures, and psychiatric disease such as psychosis and schizophrenia [Haan et al., 1985; Mudd et al., 1972]. Patients rarely have megaloblastic anemia. Severe disease is often lethal. Age at presentation ranges from birth in severe cases to adulthood in milder ones.
Laboratory Tests Moderate hyperhomocysteinemia and homocystinuria are seen, with low or normal methionine levels. The homocysteine excretion is significantly lower than in cystathionine β-synthase deficiency [Fowler and Jakobs, 1998].
Treatment Severe disease is refractory to treatment, and, although several treatments have been tried (i.e., folate, methionine, pyridoxine, cobalamin, and carnitine), none has been particularly effective [Fowler, 1998]. Betaine has somewhat improved the prognosis [Al Tawari et al., 2002; Sakura et al., 1998].
Sulfite Oxidase Deficiency Deficiency of sulfite oxidase function may occur as an isolated enzyme defect or as part of a combined deficiency (see Fig. 23-5). This rare disorder results in abnormalities of metabolism of sulfated amino acids. The cardinal feature of this condition is severe seizures in the neonatal period. Although some therapies lead to mild improvements, there is no effective treatment.
Pathophysiology The molybdenum cofactor is composed of the metal and a small pterin group [Johnson et al., 1980a]. This prosthetic
group is required for the function of three enzymes: sulfite oxidase, xanthine dehydrogenase, and aldehyde oxidase [Johnson et al., 1980b]. Most patients have mutations in one of several enzymes of the cofactor synthetic chain, whereas a minority has mutations in the sulfite oxidase gene. Postmortem examination of patients with sulfite oxidase or cofactor deficiencies have found encephalopathy with loss of neurons and myelin, attributable largely to deficiency of sulfite oxidase function and accumulation of sulfite in the brain [Roth et al., 1985]. Absence of sulfite oxidase leads to alternate metabolic pathways for sulfites, including formation of S-sulfocysteine and thiosulfate [Mudd et al., 1967]. S-sulfocysteine may substitute for cysteine in connective tissue, leading to ocular lens dislocation.
Clinical Manifestations The clinical picture includes severe neurologic abnormalities, dislocated ocular lenses, and mental retardation [Mudd et al., 1967]. This presentation is similar in isolated sulfite oxidase deficiency cases and in patients in whom the cofactor is absent. Although some variability is seen among patients, the key feature is neonatal seizures. It is recommended that all patients with neonatal seizures have metabolic testing. Other neurologic signs can include opisthotonus, axial hypotonia with peripheral hypertonia, regression, and loss of milestones. Ophthalmologic abnormalities can include nystagmus, coloboma, and cortical blindness [Lueder and Steiner, 1995]. Craniofacial dysmorphology includes bitemporal narrowing with deep-set eyes, long palpebral fissures, thick lips, elongated philtrum, and a small nose. Heterozygote carriers are unaffected.
Laboratory Tests Positive sulfite test results are usually observed on urine dipstick, although false-negative results can occur [van der Klei-van Moorsel et al., 1991]. Quantitative plasma and urine amino acids have the characteristic cysteine metabolite S-sulfocysteine [Johnson and Rajagopalan, 1995]. Low levels of urinary urothion, a degradation product of molybdopterin, are essentially diagnostic of molybdenum cofactor deficiency, and an elevated urinary thiosulfate level is diagnostic of sulfite oxidase deficiency or molybdenum cofactor deficiency.
Treatment Management for this condition is largely supportive because therapies are often ineffective. Molybdenum cofactor is too unstable to be used therapeutically. Patients with milder forms of isolated sulfite oxidase deficiency may respond to a diet low in sulfur-containing amino acids [Touati et al., 2000].
Hartnup’s Disease Hartnup’s disease is an aminoaciduria that is usually clinically silent, but it can manifest with episodes of cerebellar ataxia and a pellagra-like rash. Incidence has been estimated at 1 case in 33,000 persons [Wilcken et al., 1977].
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
Pathophysiology The metabolic aberration in Hartnup’s disease results from an error in the transport of monoamino-monocarboxylic (neutral) amino acids that affects renal tubular reabsorption and intestinal absorption [Baron et al., 1956; Mahon and Levy, 1986; Scriver et al., 1987]. There is deficient transport of neutral amino acids, including glutamine, histidine, valine, phenylalanine, tyrosine, tryptophan, alanine, asparagine, citrulline, isoleucine, leucine, serine, and threonine. Large amounts of the amino acids and of the amides of glutamate and aspartate are excreted in the urine [Bonetti and Dent, 1954]. Two tissue-specific forms of Hartnup’s disease are recognized: renal plus intestinal involvement and renal involvement alone. Amino acids such as tryptophan remain in the intestinal lumen [Milne et al., 1960], where they are converted to indolic compounds by bacteria and then absorbed [Asatoor et al., 1963]; these compounds are toxic to the central nervous system. Urinary excretion of large amounts of indican (a tryptophan metabolite) is characteristic of the disease. Large quantities of neutral amino acids are excreted in the feces [Scriver, 1965]. The lack of tryptophan absorption leads to niacin deficiency, which results in the pellagralike symptoms and photosensitivity.
Clinical Manifestations Patients detected on newborn screening usually are clinically normal, and Hartnup’s disease is usually benign [Scriver et al., 1987]. Nevertheless, some patients are affected, suggesting a monogenic trait with strong polygenic influence [Scriver, 1988]. The most prominent neurologic feature in affected individuals is attacks of cerebellar ataxia, which vary in intensity. These episodes may persist for as long as 2 weeks before improvement is evident. Less common neurologic disabilities include spasticity, wide-based gait, double vision, nystagmus, dystonia, and tremulousness. Psychiatric disturbances consisting of fear, anxiety, and mood swings may occur, as may constant headaches. Clinical involvement varies considerably among symptomatic individuals. Neurologic symptoms are often accompanied by a rash on areas of sun-exposed skin [Baron et al., 1956]. The skin is dry and reddened, resembling pellagra (i.e., nicotinamide deficiency). Sun exposure usually exacerbates the lesions, as does sulfonamide administration. Skin may become hyperpigmented.
Laboratory Tests Urine has strikingly elevated levels of neutral amino acids, but basic and acidic amino acids in urine are relatively normal [Tada et al., 1967]. Serum levels of amino acids are normal or low [Cusworth and Dent, 1960].
585
tomatic patients should protect themselves from sunlight and other aggravating agents, such as photosensitizing drugs. Administration of nicotinic acid offsets deficiency in nicotinamide synthesis [Halvorsen and Halvorsen, 1963].
Histidinemia Histidinemia is benign in almost all affected individuals, although in rare cases, this condition may lead to central nervous system disease. The benign nature makes treatment unnecessary in almost all cases. Overall incidence has been estimated at between 1 in 8000 in Japan to 1 in 37,000 in Sweden [Virmani and Widhalm, 1993].
Pathophysiology Histidinemia results from deficiency of L-histidase (Lhistidine ammonia lyase) [Auerbach et al., 1962], resulting in accumulation of histidine and its metabolites in blood, urine, and cerebrospinal fluid and in a deficiency of urocanic acid [Levy et al., 1974]. Enzyme activity is essentially undetectable in liver and other tissues of patients but may be normal in skin [Woody et al., 1965].
Clinical Manifestations The initial patients identified with histidinemia were mentally retarded and had speech abnormalities; the group identified was likely a result of ascertainment bias. Prospective follow-up of newborns with histidinemia detected by newborn screening did not provide evidence of disease in affected individuals [Levy et al., 1974; Tada et al., 1982]. Although it is clear that histidinemia does not produce severe disease, there is still debate about possible minor effects on speech and intelligence.
Laboratory Tests The diagnosis is based on elevated plasma and urine levels of histidine.
Treatment Low-histidine diets have been successfully used to reduce blood histidine concentration; however, studies of mean IQ and general level of functioning revealed no statistical advantage of therapy. Therapy is not indicated for most patients who remain asymptomatic [Scriver and Levy, 1983]. If concern exists that elevated histidine is contributing to findings, consultation with a biochemical specialist is recommended.
ORGANIC ACIDEMIAS
Treatment
Propionic Acidemia
In the rare symptomatic patient, increasing amino acid intake in the form of a high-protein diet can overcome the deficient transport and loss of neutral amino acids [Scriver et al., 1987]. Conversely, poor nutrition can lead to attacks in patients who would otherwise be asymptomatic. Symp-
Propionic acidemia is caused by the deficiency of propionylCoA carboxylase (PCC), a biotin-requiring enzyme that catalyzes the conversion of propionyl-CoA to methylmalonylCoA in the metabolic pathways of valine, isoleucine, methionine, threonine, and odd-chain fatty acids (Fig. 23-6).
586
Genetic, Metabolic, and Neurocutaneous Disorders / 23 Extracellular space
bran e
Protein synthesis CH3
m em
CH3 CH
COOH CH3
NH2
CH3
CH
CH2
CH
COOH
CH3
CH
CH2
NH2
Valine
Cell Biotin
CH
CH3
CH
COOH
Cytosol
NH2
Isoleucine
Leucine Leucineisoleucinemia
Valinemia
(Dietary form) C N Protein
O Proteolytic degradation
2-Ketoisovaleric acid Maple syrup urine disease
Bioticyn
2-Keto-3-methylvaleric acid
Thiamine B1 Thiamine B1
Isobutyryl-CoA
Thiamine B1
2-Methylbutyryl-CoA
Isovaleryl-CoA Isovaleric acidemia
Biotinidase deficiency
Methacrylyl-CoA
Tiglyl-CoA
3-Methylcrotonyl-CoA CO2
ol
C
3–MethylcrotonylCoA carboxylase deficiency
Methylmalonyl-CoA semialdehyde
Biotin
2-Methylacetoacetyl-CoA
D-Methylmalonyl-CoA
3-Methylglutaconic aciduria
Propionyl-CoA Odd-chain fatty acids Threonine Methionine Methylcitric acidCholesterol
Propionic acidemia
Biotin
3-Methylglutaconyl-CoA
β-Ketothiolase deficiency
CO2
CO2
3-Hydroxy-3-methylglutaryl-CoA 3-Hydroxy-3-methylglutaric aciduria
L-Methylmalonyl-CoA
Acetoacetic acid + Acetyl-CoA cbIB
cbIA CbI1
Adenosyl CbI
Succinyl-CoA
3-Hydroxyisovaleric acid
3-Hydroxyisobutyryl-CoA 2-Methyl-3-hydroxybutyryl-CoA
s yto
Methylmalonic acidemia
2-Ketoisocaproic acid
Maple syrup urine disease
MMA
CbI2
cbIG CbI2 cbID
CO2 H2O
Acetone Mitochondria
Methyl Cbl
cbIE
cbIC
OHC3bl Cytosol
Methionine
Homocystin-II-uria
MMA
Homocysteine
MMAHCU
cbI F
OHC3bl
MM HC A U
Cell membrane
TCII
Lysosome OHCbl TCII
Extracellular space OHC3bl TCII
FIGURE 23-6. Pathways in the metabolism of the branched-chain amino acids, biotin, and vitamin B12 (cobalamin). Cbl, cobalamin; cbl, defect in metabolism of cobalamin; HCU, homocystinuria; MMA, methylmalonic academia; OHCbl, hydroxycobalamin; TC, transcobalamin. (From Rezvani I. Defects in metabolism of amino acids. In: Behrman R, Kliegman R, Jenson H, eds. Nelson textbook of pediatrics, 16th ed. Philadelphia: WB Saunders, 2000:355.)
This condition is estimated to occur in 1 of 50,000 to 100,000 livebirths. Propionyl-CoA carboxylase is a multimer consisting of six α subunits (PCCA) and six β subunits (PCCB), encoded by genes on chromosomes 13q22 and 3q21-q22, respectively. Biotin, the required cofactor, is bound to the α subunit to form the fully functional enzyme. More than 40 mutations in each of the PCC-subunit genes have been described in
propionic acidemia patients. There is growing evidence for genotype-phenotype correlations, with null mutations often associated with the most severe clinical outcomes [Clavero et al., 2002; Perez-Cerda et al., 2003]. A deficiency of PCC activity also results from mutations in two other genetic loci encoding enzymes in the biotin use and recycling pathway: holocarboxylase synthase and biotinidase. Primary defects in either enzyme lead to functional
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
deficiencies of all four biotin-requiring carboxylases, including PCC, and are discussed elsewhere in this chapter (see “Multiple Carboxylase Deficiencies”).
Clinical Manifestations The clinical presentation of propionic acidemia resembles that of the other so-called ketotic hyperglycinemias, including methylmalonic acidemia and isovaleric acidemia. More than 80% of propionic acidemia patients experience acute onset of symptoms within the first 3 months of life [Fenton et al., 2001; Sass et al., 2004a]. Symptoms of severe metabolic decompensation include vomiting, lethargy, and coma, accompanied by severe ketoacidosis, hyperammonemia, hyperglycinemia, and decreased serum carnitine. The disease is often fatal, particularly if diagnosis and implementation of treatment are delayed. Patients with onset in childhood or in adulthood have been described with episodes of neurologic decompensation associated with periods of ketoacidosis. Even for patients presenting later in life, the metabolic decompensation can be fatal [Lucke et al., 2004]. Patients with late-onset disease have been described with developmental delay or mental retardation but without a history of episodic ketoacidosis or hyperammonemia.
Diagnosis Urine organic acid analysis reveals a characteristic pattern of metabolite excretion, including 3-hydroxypropionic acid, propionylglycine, methylcitrate, and tiglylglycine. Samples collected during an acute episode can also have massive elevations of lactic, β-hydroxybutyric, and acetoacetic acids. Plasma acylcarnitine profile has markedly elevated propionylcarnitine, with elevations of acetylcarnitine in acute samples reflecting ketosis. There is often a significant deficiency of free and total carnitine, with an elevated ratio of acylcarnitine to free carnitine. The diagnosis is confirmed by demonstration of deficiency PCC activity in cultured fibroblasts. Assays of other carboxylases, including 3-methylcrotonyl-CoA carboxylase and pyruvate carboxylase, can be performed to exclude multiple carboxylase deficiency. Molecular studies for mutations in the PCCA and PCCB genes are available in a limited number of laboratories worldwide. Because abnormal elevations of propionylcarnitine are readily detected by tandem mass spectrometry, presymptomatic patients with propionic acidemia are identified in states in which expanded newborn screening by tandem mass spectrometry has been implemented. Early diagnosis of these patients, ideally before the onset of symptoms, allows initiation of specific therapies designed to reduce the risk of metabolic decompensation. Because expanded newborn screening has only recently been introduced to medical practice, the long-term outcome of propionic acidemia patients identified in this way has not been established [Leonard et al., 2003]. Some patients with propionic acidemia, particularly those with milder variant forms, have been missed by newborn screening. It is therefore important to maintain a high index of suspicion for patients presenting with symptoms compatible with this or any other organic acidemia, even in the face of normal newborn screening results.
587
Treatment Management of propionic acidemia patients during acute episodes is aimed at correcting the acidosis and hyperammonemia, and limiting catabolism of propionate precursors by restricting protein and providing fluids and glucose. If hyperammonemia is severe and persistent, dialysis and ammonia-scavenging medications (e.g., sodium benzoate, sodium phenylacetate) may be necessary. Long-term management of propionic acidemia consists of carnitine supplementation and a protein-restricted diet that includes supplementation with a special formula. Biotin supplementation has not been demonstrated to be effective [Fenton et al., 2001]. Liver transplantation has been performed in a small number of propionic acidemia patients, with preliminary results indicating a dramatic reduction in the risk for metabolic decompensation with less strict dietary restrictions. The long-term outcome of these patients is unknown [Yorifuji et al., 2004].
Methylmalonic Acidemias Several genetic defects can lead to methylmalonic acidemia, in which methylmalonic acid and its derivatives accumulate in physiologic fluids. These conditions are caused by deficiencies in transport and metabolism of vitamin B12, or cobalamin (Cbl), and by mutations in enzymes requiring this cofactor (see Fig. 23-6). Because of the variety of causative defects, this group of conditions has significant clinical heterogeneity and differences in response to therapy. Incidence is estimated at 1 case per 50,000 persons [Coulombe et al., 1981].
Pathophysiology The methylmalonic acidemias can be caused by defects in adenosylcobalamin-dependent methylmalonyl-CoA mutase, intracellular cobalamin metabolism, transcobalamin II deficiency, and intrinsic factor or by dietary cobalamin deficiency [Fowler, 1998]. Methylmalonyl-CoA mutase isomerizes methylmalonyl-CoA to succinyl-CoA, which then enters the tricarboxylic acid cycle and is converted to pyruvate. Methylmalonyl-CoA is a derivative of propionyl-CoA, which is a metabolite derived from isoleucine, valine, threonine, methionine, thymine, uracil, cholesterol, and odd-chain fatty acids. The major causes of methylmalonic academia are divided into several different complementation groups: mut0, mut–, CblA, CblB, CblC, CblD, CblF, and CblH [Rosenblatt and Cooper, 1990]. Mutase activity is completely and partially abolished in the mut0 and mut– groups, respectively. Defective adenosylcobalamin synthesis is responsible for CblA, CblB, and CblH. CblC and CblD cause methylmalonic acidemia and homocystinuria because of cobalamin reduction abnormalities that interfere with formation of adenosylcobalamin and methylcobalamin biosynthesis. Abnormal lysosomal transport of cobalamin leads to CblF disease, which also leads to combined methylmalonic acidemia and homocystinuria. CblE and CblG diseases involve defects in homocysteine metabolism; they are discussed in the section on homocystinuria (see “Sulfur Amino Acid Metabolism and the Homocystinurias”).
588
Genetic, Metabolic, and Neurocutaneous Disorders / 23
Clinical Manifestations There is significant variability in presentation depending on the particular enzymatic deficiency, although several complementation groups share the general characteristics of failure to thrive, developmental delay, megaloblastic anemia, and neurologic dysfunction [Cooper and Rosenblatt, 1987]. Mut0, mut–, CblA, and CblB patients often present in the first few weeks of life with poor feeding, dehydration, increasing lethargy, emesis, and hypotonia [Lindblad et al., 1968; Matsui et al., 1983; Rosenberg et al., 1968]. These patients exhibit a short interval of apparent good health before presentation with symptoms. Metabolic acidosis may be catastrophic. Mild mut– or other forms of methylmalonic acidemia decompensate later in infancy or in childhood with hypoglycemia, acidosis, seizures, and lethargy. A CblC patient can present early in infancy or in later childhood with myopathy, lower extremity paresthesias, and thrombosis due to homocystinuria [Enns et al., 1999a]. Severely affected children with CblC methylmalonic acidemia can also have ocular abnormalities such as retinopathy, nystagmus, and worsening vision, as well as hydrocephalus and microcephaly [Rosenblatt et al., 1997]. Cranial imaging usually reveals pathology of the basal ganglia and white matter. The two initial cases reported with CblD presented in later childhood with mental retardation and behavioral problems, although subsequent reports have documented infantile onset with hypotonia and seizures and early childhood presentations with ataxia and gait abnormalities [Goodman et al., 1970; Suormala et al., 2004]. CblF patients have been reported to have minor facial anomalies and hematologic defects [Shih et al., 1989]. Transcobalamin II deficiency can manifest as failure to thrive in the first months of life with neurologic disease and mental retardation [Hall, 1992]. A benign form of methylmalonic acidemia has been reported in otherwise healthy children. [Ledley et al., 1984].
Laboratory Tests Methylmalonic acidemia can clinically resemble other organic acidemias, necessitating analysis of urine organic acids for diagnosis. This test reveals large amounts of methylmalonic acid, as well as methylcitrate, propionic acid, and 3-hydroxypropionic acid [Barness et al., 1963; Rosenberg et al., 1968]. Serum amino acids sometimes demonstrate elevation of glycine and hyperhomocysteinemia in the groups in which methylcobalamin metabolism is affected. Ketosis and hyperammonemia are common. Total plasma homocysteine levels are elevated in CblC, CblD, and CblF diseases. Total and free carnitine levels tend to be low, and acylcarnitine profiles reveal increased propionylcarnitine. The cobalamin transport deficiencies are assessed by measuring serum cobalamin levels and absorption by the Schilling test [Cooper and Rosenblatt, 1987]. Determination of complementation group is performed through analysis of fibroblasts.
Treatment During acute metabolic crises, treatment is directed toward limiting catabolism and restricting protein intake. The usual protein intake is stopped, and fluid and glucose are given
intravenously. Pharmacologic treatment includes carnitine, intramuscular hydroxocobalamin, metronidazole, or neomycin to decrease intestinal propionate production, betaine, and folate [Ogier de Baulny et al., 1998; Roe and Bohan, 1982; Rosenblatt and Cooper, 1987; Thompson et al., 1990]. Improved growth and enhanced nutrition status are seen in patients with methylmalonic acidemia fed an elemental medical food [Yannicelli et al., 2003]. Patients should consume a diet low in the micronutrient precursors proximal to the metabolic block and with adequate calories and total protein to enable growth. Plasma methylmalonic acid levels are followed for metabolic control [Nyhan et al., 1973]. Several transplantations of liver and kidneys in infants and children with methylmalonic acidemia have been reported. Although this approach seems to protect against metabolic crises, it does not lead to complete biochemical correction [Leonard et al., 2001].
Isovaleric Acidemia Isovaleric acidemia can manifest with early metabolic crises, often leading to coma, or it can result in a later, chronic condition. Patients are usually developmentally normal, but mild-to-severe mental retardation has been reported. Supportive care during crises and specific treatments such as glycine and carnitine have helped to improve outcomes. Overall incidence is estimated at less than 1 case per 200,000 persons.
Pathophysiology Deficiency of the mitochondrial enzyme isovaleryl-CoA dehydrogenase, part of the leucine catabolic pathway (see Fig. 23-6), leads to accumulation of several metabolites [Rhead and Tanaka, 1980]. Although the toxicity of individual metabolites is not well understood, isovaleric acid is an inhibitor of the tricarboxylic acid cycle and of hematopoiesis in cultured cells [Bergen et al., 1982; Hutchinson et al., 1985].
Clinical Manifestations Approximately one half of patients present with an acute neonatal metabolic crisis, and the remainder have chronic, intermittent illness. Both forms result from the same inborn error, and the differences in presentation may reflect the timing of catabolic insults or genetic background. The acute form occurs in infants who are clinically well at birth but who, within the first several days of life, begin to vomit, refuse feeding, and become listless, dehydrated, and lethargic [Mendiola et al., 1984]. They may have seizures, and the odor of sweaty feet often is detected. Untreated patients progress to coma and often to death, which can be caused by metabolic acidosis or attendant features such as infection [Wilson et al., 1984]. Patients who survive have the chronic, intermittent form of the disease, and they may have normal development. In the chronic form, the first episode occurs during the first year of life after a trigger such as a mild infection or protein load. Recurrent episodes involve vomiting, acidosis with ketonuria, lethargy that can progress to coma, and the cheesy or sweaty feet odor. Most patients with isovaleric acidemia who survive crises intact
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
have normal development, but some have mild delay or even severe mental retardation.
Laboratory Tests Because clinical features of isovaleric academia can resemble several other conditions, analysis of urine organic acids is necessary. During crises, significant elevations of isovalerylglycine and 3-hydroxyisovaleric acid are seen in urine [Tanaka et al., 1968]. Other laboratory abnormalities include metabolic acidosis with mild to moderate ketonuria and lactic acidemia and sometimes include hyperammonemia. Hematologic abnormalities such as thrombocytopenia, neutropenia, and pancytopenia are common [Kelleher et al., 1980]. Hypocalcemia and hyperglycemia often occur.
Treatment During crises, treatment should be administered by a biochemical geneticist, and it is similar to that for other organic acidemias: protein restriction and glucose infusion to decrease protein catabolism. Management during intervening episodes includes protein restriction and supplementation with leucine-free foods. Two targeted treatment options, glycine and carnitine, conjugate with isovaleryl-CoA and lead to excretion of the nontoxic products [Cohn et al., 1978; Mayatepek et al., 1991].
3-Methylcrotonyl-CoA Carboxylase Deficiency 3-Methylcrotonyl-CoA carboxylase (MCC) deficiency, also known as 3-methylcrotonylglycinuria, is an autosomal recessive disorder in the catabolic pathway of leucine (see Fig. 23-6). MCC is a biotin-requiring enzyme consisting of two nonidentical subunits, α (MCCA) and β (MCCB), with the biotin-binding site located on the α subunit. Mutations have been identified in both subunits in patients with MCC deficiency, defining two complementation groups for this disorder [Baumgartner et al., 2001]. Although isolated MCC deficiency was once thought to be rare, an unexpectedly large number of patients have been identified in tandem mass spectrometry–based newborn screening programs, and the frequency is estimated at 1 case per 50,000 livebirths [Baumgartner et al., 2001]. Like propionyl-CoA carboxylase deficiency, MCC deficiency can arise from defects in the enzymes of the biotin use and recycling pathway: holocarboxylase synthase and biotinidase (see “Multiple Carboxylase Deficiencies”).
Clinical Manifestations The clinical presentation of MCC deficiency is highly variable and ranges from apparently benign to severe and life threatening. The classic presentation is in infancy or childhood, with rare cases occurring in the neonatal period [Bannwart et al., 1992]. Episodes are often associated with a mild infection or other stress, and they involve vomiting, feeding difficulties, lethargy, hypotonia, hyperreflexia, hypoglycemia, metabolic acidosis, and ketosis. Investigations of family members of affected patients have revealed a number of individuals with MCC deficiency with a normal clinical phenotype. MCC deficiency has been described in
589
healthy mothers of infants identified by expanded newborn screening programs with elevated metabolites suggestive of MCC deficiency [Gibson et al., 1998]. Clinical severity, or lack thereof, is not predicted by the severity of MCC mutation or amount of residual MCC activity, in that most mutations identified in patients are associated with absent or severely diminished MCC activity [Desviat et al., 2003].
Diagnosis The diagnosis of MCC deficiency is established through studies of urine organic acids and plasma acylcarnitine profile, and enzyme assays for MCC in cultured fibroblasts. Abnormalities include the characteristic excretion of 3hydroxyisovaleric acid and methylcrotonylglycine in urine and elevation of 3-hydroxyisovalerylcarnitine in plasma. Free carnitine is often significantly decreased, with an elevated ratio of acylcarnitine to free carnitine. Urine acylglycine analysis also reveals elevated excretion of 3-methylcrotonylglycine and is a useful adjunct test. In addition to assaying MCC activity, assays of other carboxylases, including propionyl-CoA carboxylase and pyruvate carboxylase, can be performed to exclude multiple carboxylase deficiency. Asymptomatic or presymptomatic patients with MCC deficiency are also detected in expanded newborn screening programs as having elevated 3-hydroxyisovalerylcarnitine in dried blood spots [Koeberl et al., 2003]. This finding should be followed with urine organic acid and acylcarnitine studies for the patient and the mother [Gibson et al., 1998].
Treatment Treatment of acute episodes is aimed at restoring glucose homeostasis and correcting acidosis. Long-term treatment with carnitine supplementation and dietary restriction of leucine has been found to result in normal growth and development [Sweetman and Williams, 2001]. Responsiveness to biotin has been demonstrated in a small number of cases [Baumgartner et al., 2004].
Multiple Carboxylase Deficiencies The biotin-responsive multiple carboxylase deficiencies include at least two autosomal recessive disorders with somewhat distinct but overlapping clinical manifestations, referable to enzymopathies affecting the biotinylation of the four mammalian carboxylases. The carboxylases all require biotin for catalytic activity and include cytosolic acetyl-CoA carboxylase, the rate-limiting step for the de novo synthesis of fatty acids; mitochondrial pyruvate carboxylase, catalyzing the conversion of pyruvate to oxaloacetate, a tricarboxylic acid cycle intermediate and a precursor for gluconeogenesis; mitochondrial methylcrotonyl-CoA carboxylase, catalyzing an intermediate reaction step in leucine catabolism; and mitochondrial propionyl-CoA carboxylase, which catalyzes an intermediate step in the conversion of isoleucine, valine, and other precursors to succinic acid (see Fig. 23-6). In each of these enzymes, the biotin is linked to the epsilon amino group of a lysine residue, situated within the highly conserved amino acid sequence of the biotin-binding site. The clinical presentations and metabolic derangements in the multiple carboxylase deficiencies mirror those of primary
590
Genetic, Metabolic, and Neurocutaneous Disorders / 23
deficiencies of each of the carboxylases and the clinical features of acquired nutritional biotin deficiency. The first patient was described in 1971 and was originally reported as having biotin-responsive β-methylcrotonylglycinuria [Gompertz et al., 1971]. A little more than a decade later, two different disorders—biotinidase deficiency, a defect in the recycling of biotin, and holocarboxylase synthase deficiency, a defect in the biotinylation of carboxylases— were characterized.
Biotinidase Deficiency CLINICAL MANIFESTATIONS Patients with biotinidase deficiency usually present in early to middle infancy, but they may come to medical attention in very early infancy or in later childhood. Because of the usual age of presentation, biotinidase deficiency was delineated as late-onset or infantile-onset multiple carboxylase deficiency [Packman et al., 1981b; Thoene et al., 1981]. Symptoms may be insidious or acute and can include lethargy, hypotonia, anorexia or vomiting, developmental delays, ataxia, seizures, and coma. Dermatologic manifestations are a frequent feature and can include alopecia, rashes, and mucocutaneous candidiasis. The rash bears resemblance to that seen in essential fatty acid deficiency or acrodermatitis enteropathica [Williams et al., 1983]. Hearing loss and optic atrophy can be significant long-term complications that do not uniformly respond to therapy. Patients presenting in later childhood or adolescence can come to medical attention because of motor weakness and spastic paresis or because of loss of visual acuity [Wolf, 2001]. When studied, neuropathologic findings in biotinidase deficiency have included changes suggestive of Leigh’s disease and Wernicke’s encephalopathy [Sander et al., 1980]. Such findings are consonant with the notion that neurologic sequelae may result from abnormal intracerebral lactate concentrations [Schurmann et al., 1997].
remaining bound to the lysine as a compound called biocytin. The release of biotin from biocytin requires the extracellular catalytic activity of biotinidase. In the absence of biotinidase, the cleavage of biocytin does not occur, and biotin is not released for reuse. Biotinidase may also be required for the release of biotin bound to dietary protein, resulting in reduced availability of dietary biotin. The failure to recycle biotin gradually leads to biotin deficiency, a secondary deficiency of biotin-dependent carboxylase activity, and the symptoms of biotinidase deficiency. Although the focus has been on the consequences of deficiency of the mitochondrial carboxylases, the contribution of acetyl-CoA carboxylase to the clinical manifestations also has been investigated [Gonzalez-Rios et al., 1985b; Packman et al., 1984, 1989; Proud et al., 1990]. Cells deficient in acetyl-CoA carboxylase cannot synthesize malonyl-CoA, required for de novo fatty acid synthesis and fatty acid elongation reactions. In such cells, the fatty acid pattern and composition of membranes and structural elements is abnormal, leading to speculation that such alterations may contribute to the dermatitis [Munnich et al., 1980], to the immunologic derangements reported in a number of patients [Cowan et al., 1979], and to some components of the neurologic manifestations.
DIAGNOSIS
The aberrant clinical chemistries include metabolic acidosis, with ketosis and lactic acidosis; hypoglycemia; hyperammonemia; and a distinct organic acid pattern that represents the combination of individual carboxylase deficiencies. The organic academia includes propionic acid, 3-hydroxypropionate, methylcitrate, and tiglylglycine, referable to propionyl-CoA carboxylase deficiency; lactic acid (and pyruvic acid and alanine), referable to pyruvate carboxylase deficiency; and 3-methylcrotonate, 3-methylcrotonylglycine, and 3-hydroxyisovaleric acid, referable to the derangement in the methylcrotonyl-CoA carboxylase step.
A small but significant fraction of cases ascertained because of clinical symptoms may not demonstrate the characteristic organic aciduria. Accordingly, serum biotinidase activity should be measured in any patient with features—especially cutaneous and neurologic features—that are consistent with biotinidase deficiency. Assay of serum biotinidase is a widely clinically available test. Enzyme activity can be measured in fibroblasts, peripheral blood leukocytes, and amniotic fluid or amniotic fluid cells if prenatal diagnosis is carried out. Many states have incorporated biotinidase testing on filter paper blood spots in state-sponsored newborn screening programs. Ascertainment of biotinidase deficiency in such newborn screening programs has led to the identification of two broad clinical cohorts of patients: those with profound biotinidase deficiency (less than 10% of control subjects) and children with partial biotinidase deficiency (10% to 30% of control subjects) [Wolf, 1991]. The combined incidence of profound and partial deficiency is estimated at 1 in 60,000, with the two forms each having approximately equal incidences. The natural history of partial deficiency is not entirely known. Because there are reports of patients with partial deficiency who have become symptomatic, it has been suggested that treatment for partial deficiency might be indicated [McVoy et al., 1990].
ETIOLOGY
TREATMENT
The defect in the infantile-onset form of biotin-responsive multiple carboxylase deficiency was determined by Wolf and colleagues [1983] to reside in a deficiency of biotinidase activity. Biotinidase is required in the recycling of biotin from carboxylases after the proteolytic degradative turnover of these enzymes (see Fig. 23-6). When a carboxylase is hydrolyzed, biotinyl lysine is released, with the biotin
Patients with biotinidase deficiency can be treated with pharmacologic dosages of biotin of 5 to 20 mg/day. Children with partial biotinidase deficiency have been treated with somewhat lower dosages of 1 to 5 mg/day. With treatment, the biochemical derangements (including the lactic acidosis) resolve, the dermatologic manifestations rapidly resolve, developmental delays are ameliorated or reversed, and there
LABORATORY TESTS
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
is often resolution of seizures and ataxia. Hearing and visual loss may remain as long-term complications and be refractory to treatment.
Holocarboxylase Synthase Deficiency CLINICAL MANIFESTATIONS Children with holocarboxylase synthase deficiency generally present in the first several days or weeks of life with severe and life-threatening metabolic encephalopathy. The clinical course is variably marked by irritability, lethargy, feeding problems, vomiting, tachypnea, hypertonia or hypotonia, and progression to seizures and coma. The timing of the acute presentation led to the initial characterization of patients as representing a neonatal-onset form of multiple carboxylase deficiency [Packman et al., 1981a, 1984]. Patients with milder forms of holocarboxylase synthase deficiency present later or have a more protracted clinical course [Packman et al., 1984]. These children may have alopecia, rash, ataxia, and developmental delays, a clinical presentation that overlaps that of biotinidase deficiency.
591
high- or low-biotin culture medium [Packman et al., 1984]. For prenatal diagnosis, both types of enzymatic assay approaches can be used [Packman et al., 1982]. As an adjunct to enzymatic assay and to achieve a rapid result, it is possible to measure the concentration of accumulating analytes (e.g., 3-hydroxyisovalerate, methylcitrate) in amniotic fluid, by stable isotope dilution analysis [Jakobs et al., 1984]. Prenatal diagnosis of holocarboxylase synthase deficiency has been performed [Packman et al., 1982]. In two pregnancies, prenatal treatment by administration of biotin to the mother during pregnancy [Packman et al., 1982; Roth et al., 1982) was successfully performed in paradigmatic studies of the application and efficacy of cofactor therapy in such settings.
TREATMENT
Abnormal clinical laboratory findings include metabolic acidosis (e.g., lactic acidosis, ketosis), hyperammonemia, evidence of the bone marrow toxicity of organic acidemias (e.g., thrombocytopenia), and the characteristic organic aciduria of multiple carboxylase deficiencies: 3-methylcrotonylglycine, 3-hydroxyisovalerate, lactate, 3-hydroxypropionate, methylcitrate, and tiglylglycine.
Patients respond well to oral biotin in pharmacologic doses. Generally, the starting dose is 10 mg/day. However, the KM for biotin can range from 3 to 70 times normal [Wolf, 2001]. Some patients may require a higher dose, because the mutant enzyme has a higher KM for biotin. There is also a suggestion that patients with mutant holocarboxylase synthase enzymes exhibiting a reduced Vmax may have a poorer response to biotin therapy than those with KM values for biotin mutations [Sakamoto et al., 1999]. Accordingly, careful monitoring of clinical status (including neurologic and cutaneous manifestations), of organic acid levels (including lactate), and of conventional clinical chemistries (i.e., ammonia, electrolytes, and ketones) is mandatory to arrive at optimal dosing of biotin. After treatment levels have been achieved, no dietary restrictions are required.
ETIOLOGY
3-Methylglutaconic Aciduria
The basic defect is in the activity of the enzyme holocarboxylase synthase [Burri et al., 1981], which catalyzes a two-step reaction that results in the covalent binding of biotin to apocarboxylases. All patients with deficient holocarboxylase synthase activity have shown detectable residual activity. Multiple mutations have been identified, with most resulting in the synthesis of an enzyme with an elevated Michaelis-Menten dissociation constant (KM) for biotin. Some patients have mutations that result in a normal KM for biotin but a reduced value for maximum velocity of enzymecatalyzed reactions (Vmax). These observations have led to speculation that a complete absence of holocarboxylase synthase activity might be lethal [Wolf, 2001].
At least four different conditions have the common feature of abnormal urinary excretion of 3-methylglutconic acid, and they are designated as 3-methyglutaconic aciduria types I, II, III, and IV. The metabolite 3-methylglutconic acid occurs in the leucine catabolic pathway and is converted by 3-methylglutaconyl-CoA hydratase to 3-hydroxy-3-methylglutaric acid, leading ultimately to ketone body formation and the production of cholesterol precursors. The clinical features, diagnosis, and treatment approaches for each type of 3-methylglutaconic aciduria are discussed in the following sections.
LABORATORY TESTS
DIAGNOSIS Holocarboxylase synthase assay can be performed in cultured fibroblasts or lymphocytes and in amniotic fluid cells [Packman et al., 1982]. An alternative enzymatic approach can be taken by measurements of individual carboxylase activities in fibroblasts cultured in low-biotin medium and in high-biotin medium. If grown in low-biotin medium, individual carboxylase activities will be low, but the activities will be normal or approach normal levels if the cells are grown in high-biotin medium. This assay result contrasts with that for biotinidase deficiency fibroblasts, which demonstrates normal activities whether grown in
Type I: Primary 3-Methylglutaconyl-CoA Hydratase Deficiency Primary 3-methylglutaconyl-CoA hydratase deficiency is a rare, autosomal recessive disorder caused by mutations in the 3-methylglutaconyl-CoA hydratase gene (AUH) and characterized by abnormal urinary excretion of 3-methylglutaconic and 3-hydroxyisovaleric acids. The 3-hydroxyisovaleric acid levels are not elevated in the other three types of 3-methylglutaconylaciduria. In the small number of patients reported with this disorder, the spectrum of clinical abnormalities ranges from mild to extremely severe. Although the presentation varies, many patients have had retardation, acidosis, hypoglycemia, hypotonia, and seizures. The diagnosis is suspected by the characteristic pattern of urine
592
Genetic, Metabolic, and Neurocutaneous Disorders / 23
organic acid excretion, and it is confirmed by assays for the 3-methylglutaconyl-CoA hydratase activity in cultured fibroblasts. Molecular studies to identify mutations in the AUH gene are available in only a limited number of laboratories. Treatment with leucine restriction or Lcarnitine supplementation may be effective in some patients [Sweetman and Williams, 2001].
Type II: Barth’s Syndrome Barth’s syndrome, also known as X-linked cardioskeletal myopathy and neutropenia, is characterized by mitochondrial abnormalities and abnormal excretion of 3-methylglutaconic acid. Barth’s syndrome is caused by mutations in the G4.5 gene (TAZ), which produces through alternate splicing a class of proteins called the tafazzins. Tafazzins are mitochondrial proteins thought to play a role in the structure and function of cardiolipin, a membrane lipid required for proper functioning of the mitochondrial electron transport chain. Clinically, cardiomyopathy and skeletal muscle weakness are usually apparent in affected males in the first year of life. Neutropenia can vary from mild to severe, even within the same patient. Many patients die before they are 4 years old, although some reports suggest an improvement in survival rates due to increased awareness of the diagnosis and more aggressive management of cardiomyopathy and infections [Barth et al., 2004]. No specific symptoms have been identified in heterozygous females, and there is no effective treatment for Barth’s syndrome.
Type III: Costeff’s Optic Atrophy Syndrome Costeff’s syndrome is a rare, autosomal-recessive disorder characterized by early-onset bilateral optic atrophy and choreiform movement disorder and by variable later-onset spasticity and mental retardation. Excretion of 3-methylglutaconic and 3-methylglutaric acids is moderately elevated, and the activity of 3-methylglutaconyl-CoA hydratase is normal. This disorder was once thought to be confined to patients of Iraqi Jewish background, but it has been described in non-Iraqi Jews [Kleta et al., 2002]. Linkage studies of large Iraqi Jewish families have identified mutations in the OPA3 gene, which encodes a protein of unknown function, as being the underlying cause of the disorder [Anikster et al., 2001]. The diagnosis is suspected on clinical grounds and confirmed by urine organic acid analysis. No effective treatment is available [Sweetman and Williams, 2001].
Type IV: Unclassified The type IV 3-methyglutaconic acidurias constitute a heterogeneous group of disorders. Patients share the common features of abnormal excretion and normal 3-methylglutaconyl-CoA hydratase activity. The abnormal 3-methylglutaconic aciduria may result from a variety of causes possibly affecting energy metabolism. The varied clinical features include severe psychomotor retardation, cerebellar dysgenesis, neonatal hypotonia, absent reflexes, and optic atrophy. No specific treatment is available [Sweetman and Williams, 2001].
β-Ketothiolase Deficiency Inherited β-ketothiolase deficiency, also known as mitochondrial acetoacetyl-CoA thiolase deficiency, is a rare autosomal recessive disorder caused by defects in mitochondrial acetoacetyl-CoA thiolase, also known as βketothiolase, T2, or 3-oxothiolase (see Fig. 23-6). This enzyme participates in the pathways of ketone body and isoleucine metabolism. It is related to, but distinct from, four other β-ketothiolase enzymes that participate in reactions of mitochondrial β-oxidation of short- and medium-chain fatty acids, cholesterol synthesis, and peroxisomal β-oxidation. Numerous mutations in the mitochondrial acetoacetyl-CoA thiolase gene (ACAT1) have been described in patients, with some completely abolishing β-ketothiolase activity and others associated with significant residual activity. The degree of clinical severity does not appear to be associated with the molecular severity of mutation nor the degree of residual activity [Fukao et al., 2001, 2003].
Clinical Manifestations There is wide clinical variability associated with βketothiolase deficiency, with most patients presenting with acute ketoacidosis between 5 to 24 months. Attacks are often accompanied by moderate hyperammonemia and hyperglycinemia. Patients are typically well between episodes, with attacks often precipitated by an intercurrent illness or other stress. A small number of patients have been reported with dystonia, which reflects basal ganglia damage, and with mental retardation [Mitchell and Fukao, 2001]. A β-ketothiolase deficiency has been described in asymptomatic siblings of affected patients.
Diagnosis Urine organic acid analysis of patients with β-ketothiolase deficiency reveals a characteristic pattern of 2-methyl-3hydroxybutyric and 2-methylacetoacetic acids, with variable excretion of 2-butanone and tiglylglycine. The diagnosis is confirmed by assays for β-ketothiolase activity in lymphocytes or cultured fibroblasts [Mitchell and Fukao, 2001].
Treatment Treatment of acute episodes is aimed at correcting ketoacidosis with fluids, glucose, and carnitine supplementation and includes careful monitoring of plasma ammonia, glucose, and electrolytes. Patients are managed long term with normal or slightly reduced protein intake and with careful monitoring of urine ketones during mild intercurrent illnesses. With appropriate treatment, the long-term prognosis for patients is excellent for those in whom neurologic damage has not occurred before diagnosis [Mitchell and Fukao, 2001].
Canavan’s Disease Canavan’s disease, also known as spongy degeneration of the brain, is an autosomal-recessive disorder caused by a deficiency of aspartoacylase (or N-acyl-L-aspartate amidohydrolase). This enzyme catalyzes the hydrolysis of N-
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
acetyl-L-aspartic acid (NAA) to aspartic acid and acetic acid, and it is particularly abundant in white matter of the brain. NAA itself is found only in the central nervous system, and its function is largely unknown [Beaudet, 2001]. Although the disorder is pan-ethnic, it occurs more frequently among patients of Ashkenazi Jewish descent, for whom the carrier frequency is estimated at 1 case per 40 persons. Two specific aspartoacylase mutations, E285A and Y231X, account for most of the disease alleles.
Clinical Manifestations Patients with Canavan’s disease are typically normal for the first 1 to 2 months of life, and they then develop hypotonia, poor head control, poor contact, and seizures, as well as macrocephaly and loss of early milestones. In most patients, neurologic abnormalities and macrocephaly are apparent by 6 months of age. Imaging studies demonstrate severe changes in the subcortical white matter and the lower layers of the gray matter, with relative sparing of the central white matter. Later features of the disorder may include spasticity, opisthotonus, and decerebrate or decorticate posturing. Most patients die within the first 3 years of life, although a small number of cases have been reported with later onset and a milder or more variable course [Beaudet, 2001].
593
stration of abnormal excretion of NAA. Enzyme assays for aspartoacylase activity are available in only a small number of laboratories worldwide and are typically unnecessary to establish a diagnosis. Molecular analysis for common aspartoacylase mutations in the Jewish and European populations can be used for confirmation of the diagnosis and carrier testing of family members. Prenatal diagnosis can be performed by DNA analysis in cases where parental mutations are known. Prenatal diagnosis has also been performed through assays of aspartoacylase activity in chorionic villi or amniocytes or NAA levels in amniotic fluid, but these approaches have been shown to be unreliable in a number of cases [Beaudet, 2001].
Treatment There is no known treatment for Canavan’s disease. The American College of Obstetrics and Gynecology (ACOG) has recommended that molecular carrier testing for Canavan’s disease be offered to all Ashkenazi Jewish patients [American College of Obstetrics and Gynecology, 2004]. Such carrier screening programs are aimed at disease prevention through the identification of couples at risk of having an affected child. As with similar screening programs for Tay-Sachs disease, this is expected to dramatically reduce the occurrence of infants with Canavan’s disease born in this population.
Diagnosis
Glutaric Aciduria Type 1
The diagnosis of Canavan’s disease is suspected on the basis of clinical evaluation and neuroimaging studies (Fig. 23-7) and confirmed by urine organic acid analysis and the demon-
In 1975, Goodman and colleagues [1975] described glutaric acidemia and aciduria in siblings with a neurodegenerative disorder beginning in infancy and characterized by 100 NAA
80
60
40 Cr
20 Ch
0
ppm 4.5
A
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
B
FIGURE 23-7. Patient with Canavan’s disease. A, Axial view, T2-weighted image shows abnormal hyperintensity in the cerebral hemispheric white matter, globus pallidi, and thalami. B, Proton magnetic resonance spectroscopy (echo time of 288 msec) shows a markedly increased N-acetyl-L-aspartic acid (NAA) peak. (From Barkovich AJ. Pediatric neuroimaging, 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2005.)
594
Genetic, Metabolic, and Neurocutaneous Disorders / 23
opisthotonus, dystonia, and athetosis. Glutaric acidemia type 1, also known as glutaryl-CoA dehydrogenase deficiency, is an autosomal-recessive condition caused by deficiency of glutaryl-CoA dehydrogenase activity and has an estimated prevalence of approximately 1 case per 100,000 persons [Lindner et al., 2004]. Glutaric acidemia type 1 is relatively common in the Old Order Amish in Lancaster County, Pennsylvania. Glutaric acidemia type 2 (i.e., multiple acyl-CoA dehydrogenase deficiency) is associated with defects in mitochondrial electron transfer flavoprotein or electron transfer flavoprotein dehydrogenase and is discussed further in Chapter 28. Glutaryl-CoA dehydrogenase is a key enzyme in the degradation pathway for lysine, hydroxylysine, and tryptophan. Deficiency results in accumulation of glutarate and, to a lesser extent, of 3hydroxyglutarate and glutaconate in body tissues, blood, cerebrospinal fluid, and urine. Glutaric acidemia type 1 is characterized by irreversible focal striatal necrosis after an acute illness, most often between the ages of 3 and 18 months. Affected children often have macrocephaly, dystonia, and dyskinesia [Strauss et al., 2003]. Macrocephaly may not be present at birth, but head growth velocity is increased [Hoffmann et al., 1996]. Intraretinal hemorrhages and subdural effusions may be mistaken for nonaccidental injury [Morris et al., 1999]. In some cases, the presentation is insidious, with gradual appearance of symptoms [Hoffmann et al., 1996]. Systemic manifestations typical of many other organic acidemias, such as pronounced metabolic ketoacidosis, hypoglycemia, and hyperammonemia, do not occur [Hoffmann et al., 1996; Kyllerman
et al., 2004; Strauss et al., 2003]. There appears to be a window of neurologic susceptibility to damage during the first years of life. Striatal injury is rarely encountered after age 3 years, although initial presentation as late as age 19 years has been described [Bahr et al., 2002; Strauss and Morton, 2003b]. The most characteristic head MRI finding in symptomatic children is symmetric widening of the sylvian fissure with poor operculization (“bat wing” appearance) caused by frontotemporal atrophy or hypoplasia (Fig. 23-8). Other features include basal ganglia injury, subdural effusions, ventriculomegaly, and delayed myelination [Neumaier-Probst et al., 2004]. Diffusion-weighted imaging may be more sensitive in demonstrating brain lesions than CT or MRI [Elster, 2004]. Urine organic acid analysis often documents highly elevated glutarate and lesser elevations of 3-hydroxyglutarate and glutaconate, but some children with a classic phenotype have low or undetectable levels of these metabolites (socalled low excretors) [Baric et al., 1999]. Newborn screening using tandem mass spectrometry has the potential for presymptomatic detection of glutaric acidemia type 1, although the existence of a low-excretor phenotype will undoubtedly result in missed cases [Lindner et al., 2004]. In a study of 215 patients, complete absence of glutaryl-CoA dehydrogenase activity was found in more than 50%, whereas 34% had a residual activity up to 5%, and a few had residual activity between 5% and 15% [Christensen et al., 2004]. Some correlations between severity of mutation and biochemical parameters have been established (e.g., patients
A
B
FIGURE 23-8. MRI in glutaric acidemia. A, Axial view, T2-weighted image shows markedly enlarged sylvian fissures bilaterally and abnormal hyperintensity of the central tegmental tract. B, Axial view, T2-weighted image at a slightly higher level shows abnormal hyperintensity of the lentiform nuclei bilaterally. (Courtesy of Dr. A. James Barkovich, University of California, San Francisco, CA.)
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias
with at least one mild mutation frequently have a lowexcretor phenotype). However, no correlation between clinical outcome and genotype or biochemical phenotype has been established [Christensen et al., 2004]. Increased glutarate and 3-hydroxyglutarate levels may induce an imbalance in glutamatergic and GABAergic neurotransmission by inhibiting glutamate decarboxylase, the key enzyme in γ-aminobutyric acid (GABA) synthesis, or through direct damage to striatal GABAergic neurons [Kolker et al., 2004]. 3-Hydroxyglutarate may mimic the excitatory neurotransmitter glutamate and thereby cause excitotoxic cell damage mediated through activation of NMDA receptors [Kolker et al., 2004]. Glutarate inhibits synaptosomal uptake of glutamic acid and produces striatal lesions when injected directly into rat brain [Goodman, 2004]. Other potential contributors to neurotoxicity include cytokine-induced cell damage, mitochondrial dysfunction, increased production of reactive oxygen species, and production of toxic quinolinic acid, an intermediate in tryptophan metabolism in brain [Goodman, 2004; Strauss and Morton, 2003b]. Other reports have emphasized the relatively weak neurotoxicity of glutarate and 3-hydroxyglutarate in animal models and primary neuronal cell cultures. The pathogenesis of striatal necrosis and brain lesions in glutaric acidemia type 1 remains the subject of intensive investigation [Freudenberg et al., 2004; Lund et al., 2004]. Animal models may help resolve these conflicting results. Treatment of glutaric acidemia type 1 is based on restriction of protein and lysine intake, carnitine and riboflavin supplementation, and rapid intervention in times of intercurrent illness [Muhlhausen et al., 2004]. Antioxidants and creatine have theoretical therapeutic advantages, but such compounds are not routinely used [Muhlhausen et al., 2004; Strauss et al., 2003]. Despite early identification and aggressive management, permanent neurologic damage occurs in approximately one third of patients [Strauss and Morton, 2003b]. Anticholinergic drugs, such as trihexyphenidyl, and botulinum toxin are beneficial in treating generalized or focal dystonia in patients with glutaric acidemia type 1 [Burlina et al., 2004]. Stereotactic pallidotomy has been performed in three children, with one improving only slightly [Muhlhausen et al., 2004; Rakocevic et al., 2004].
5-Oxoprolinuria Glutathione (L-γ-glutamyl-L-cysteinylglycine) is a key component in cellular protection from oxidant damage. 5-Oxoprolinuria (i.e., pyroglutamic aciduria) may be caused by defects in enzymes involved in the synthesis and degradation of glutathione, including glutathione synthetase and 5-oxoprolinase, or as a secondary finding in a variety of conditions that are associated with glutathione depletion, including inborn errors of metabolism unrelated to the glutathione cycle (e.g., methylmalonic acidemia, propionic acidemia, urea cycle defects, hepatorenal tyrosinemia, mitochondrial disorders), certain medication exposure (e.g., vigabatrin, acetaminophen, antibiotics), severe burns, multiorgan failure, and malnutrition [Mayatepek, 1999]. Glutathione synthetase deficiency is an autosomalrecessive condition that features massive urine excretion of 5-oxoproline. Clinical manifestations include metabolic
595
acidosis, mental retardation, ataxia, spasticity, seizures, psychiatric disturbances, recurrent bacterial infections, and hemolytic anemia [Ristoff et al., 2001]. Ophthalmologic findings, consisting of minor lens opacities, granular retinal hyperpigmentation, and abnormal electroretinography, were found in two sisters with glutathione synthetase deficiency [Larsson et al., 1985]. Head imaging may reveal brain atrophy [Al-Jishi et al., 1999]. Mild, moderate, and severe phenotypes have been described [Ristoff et al., 2001]. Postmortem examination has revealed generalized cerebellar atrophy, caused by a diffuse loss of granule cells, and ventriculomegaly, especially of the fourth ventricle [Skullerud et al., 1980]. Although patients with 5-oxoprolinase deficiency also excrete large amounts of 5-oxoproline, they are typically asymptomatic. The detection of developmental delay in some patients with 5-oxoprolinase deficiency may reflect ascertainment bias. The excessive urinary excretion of 5-oxoproline should be detected easily on urine organic acid analysis. 5-Oxoproline is derived from increased synthesis of γ-glutamylcysteine, and it is present in amounts that exceed the normal capacity of 5-oxoprolinase to convert it to glutamate [Wellner et al., 1974]. Definitive diagnosis is made by measuring erythrocyte glutathione synthetase activity or DNA analysis, or both. Varieties of missense and splice site mutations have been found in the GSS gene [Shi et al., 1996]. Treatment of glutathione synthetase deficiency includes correction of metabolic acidosis and high-dose supplementation with vitamins C and E [Ristoff et al., 2001]. Supplementation with N-acetylcysteine may also increase levels of plasma and leukocyte glutathione and may be of therapeutic benefit [Jain et al., 1994; Martensson et al., 1989]. Patients with glutathione synthetase deficiency should avoid medications associated with hemolytic crises in glucose-6-phosphate dehydrogenase deficiency.
Isobutyryl-CoA Dehydrogenase Deficiency Isobutyryl-CoA dehydrogenase deficiency is an autosomal recessive disorder of valine metabolism that was first described by Roe and colleagues [1998]. Defective enzyme activity results in impairment of the conversion of isobutyryl-CoA to methylacrylyl-CoA. The initial patient was a developmentally normal 2-year-old girl who developed a dilated cardiomyopathy at age 11 months. She had profound carnitine deficiency, and after carnitine supplementation, acylcarnitine analysis detected markedly increased levels of butyrylcarnitine and isobutyrylcarnitine. Urine organic acids were normal [Roe et al., 1998]. Mutations in the ACAD8 gene were later identified in this patient [Nguyen et al., 2002]. Tandem mass spectrometry newborn screening has identified asymptomatic children [Sass et al., 2004b]. It is uncertain whether children are at risk for serious clinical sequelae or whether therapy is needed.
3-Hydroxyisobutyric Aciduria 3-Hydroxyisobutyric aciduria is a rare autosomal-recessive disorder of valine metabolism, although the deficient enzyme has not been identified. The initial patient had repeated episodes of ketoacidosis, failure to thrive, and chronic lactic acidemia [Ko et al., 1991]. Microcephaly, dysmorphic facial
596
Genetic, Metabolic, and Neurocutaneous Disorders / 23
features (i.e., short, sloped forehead; telecanthus; downslanting palpebral fissures; long, prominent philtrum; and micrognathia), seizures, cerebral dysgenesis, brain atrophy, focal white matter abnormalities, and intracerebral calcification have also been described [Chitayat et al., 1992; Sasaki et al., 2001]. This condition has been misdiagnosed as cerebral palsy [Sasaki et al., 2001]. Although most patients have had prominent mental retardation, mild disease and normal intelligence have been reported [Boulat et al., 1995]. Treatment with carnitine and dietary valine and protein restriction appear to be beneficial [Ko et al., 1991; Sasaki et al., 2001].
2-Methylbutyryl-CoA Dehydrogenase Deficiency 2-Methylbutyryl-CoA dehydrogenase, also known as shortor branched-chain acyl-CoA dehydrogenase deficiency, catalyzes the conversion of 2-methylbutyryl-CoA to tiglylCoA in the isoleucine degradative pathway. Deficiency of this enzyme leads to increased 2-methylbutyrylglycine and 2-methylbutyrlycarnitine in physiologic fluids. A neonate with metabolic acidosis, hypoglycemia, and apnea was the initial reported case. MRI demonstrates ischemic changes bilaterally in parietal and occipital lobes with increased signal intensity in the lentiform nuclei [Gibson et al., 2000]. Motor delay, strabismus, and generalized muscular atrophy developed during the second year of life in another patient [Andresen et al., 2000]. Tandem mass spectrometry newborn screening identified elevated 5-carbon-saturated acylcarnitine species in eight children of Hmong ancestry. All were treated with a low-protein diet and carnitine supplementation. All patients remained asymptomatic at ages 3 to 14 months, except for one who developed mild hypotonia [Matern et al., 2003].
Mevalonate Kinase Deficiency Deficiency of mevalonate kinase, an essential enzyme in cholesterol and nonsterol isoprenoid biosynthesis, leads to two distinct clinical phenotypes: (1) mevalonic aciduria and hyperimmunoglobulinemia D and (2) periodic fever syndrome (HIDS). Both disorders are inherited as autosomal-recessive traits. Because abnormal isoprenoid synthesis can lead to fever and inflammation, these conditions are classified as autoinflammatory disorders [Houten et al., 2003]. Mevalonic aciduria is characterized by psychomotor retardation, failure to thrive, dysmorphic features (i.e., dolichocephaly, frontal bossing, down-slanting palpebral fissures, and low-set, posteriorly rotated ears), and intercurrent episodes of crisis that feature high fever, vomiting, and diarrhea. Severe cerebellar atrophy and associated ataxia are common. Ocular involvement (e.g., cataracts, retinal dystrophy), hypotonia, mild hepatosplenomegaly, and cholestatic liver disease also occur [Hoffmann et al., 1993]. Recurrent febrile crises tend to decrease with advancing age and are not present in all cases. Patients with HIDS have lifelong recurrent febrile episodes, lymphadenopathy, splenomegaly, arthralgias, and rashes that begin in infancy. HIDS is not associated with neurologic impairment, and patients are typically asymptomatic in between episodes of fever. Because phenotypic overlap between mevalonic aciduria and HIDS exists, these
conditions most likely represent a continuous spectrum of disease, rather than two distinct entities [Simon et al., 2004]. Mevalonic aciduria is diagnosed by detecting elevated mevalonic acid on urine organic acid analysis. Standard clinical chemical investigations find normal or slightly reduced cholesterol and elevated creatine kinase levels, especially during crises [Hoffmann et al., 1993]. Although the level of serum immunoglobulin D may be elevated in mevalonic aciduria, this finding is not invariable. An elevated serum IgD level is a marker for HIDS. Mild elevations of urine mevalonic acid may occur in HIDS during attacks [Cuisset et al., 2001]. Analyzing mevalonate kinase activity in lymphoblasts or using direct DNA analysis can confirm of the diagnosis. Most patients are compound heterozygotes for mutant alleles. Some mutations are common to mevalonic aciduria and HIDS [Cuisset et al., 2001]. Treatment for both conditions is largely supportive. Oral cholesterol supplementation, alone or with various combinations of ursodeoxycholic acid, ubiquinone, and vitamin E, did not result in improvement of clinical or biochemical parameters. Lovastatin administration has resulted in the development of severe clinical crises, but some patients have responded dramatically to corticosteroid therapy during acute clinical crises [Hoffmann et al., 1993]. REFERENCES Aliefendioglu D, Tana Aslan A, Coskun T, et al. Transient nonketotic hyperglycinemia: Two case reports and literature review. Pediatr Neurol 2003;28:151. Al-Jishi E, Meyer BF, Rashed MS, et al. Clinical, biochemical, and molecular characterization of patients with glutathione synthetase deficiency. Clin Genet 1999;55:444. Al Tawari AA, Ramadan DG, Neubauer D, et al. An early onset form of methylenetetrahydrofolate reductase deficiency: A report of a family from Kuwait. Brain Dev 2002;24:304. American College of Obstetrics and Gynecology. The ACOG committee opinion, no. 298, August 2004: Prenatal and preconceptional carrier screening for genetic diseases in individuals of Eastern European Jewish descent. Obstet Gynecol 2004;104:425. Andresen BS, Christensen E, Corydon TJ, et al. Isolated 2methylbutyrylglycinuria caused by short/branched-chain acyl-CoA dehydrogenase deficiency: Identification of a new enzyme defect, resolution of its molecular basis, and evidence for distinct acyl-CoA dehydrogenases in isoleucine and valine metabolism. Am J Hum Genet 2000;67:1095. Anikster Y, Kleta R, Shaag A, et al. Type III 3-methylglutaconic aciduria (optic atrophy plus syndrome, or Costeff optic atrophy syndrome): Identification of the OPA3 gene and its founder mutation in Iraqi Jews. Am J Hum Genet 2001;69:1218. Applegarth DA, Toone JR. Nonketotic hyperglycinemia (glycine encephalopathy): Laboratory diagnosis. Mol Genet Metab 2001;74:139. Applegarth DA, Toone JR. Glycine encephalopathy (nonketotic hyperglycinaemia): Review and update. J Inherit Metab Dis 2004;27:417. Applegarth DA, Toone JR, Rolland MO, et al. Non-concordance of CVS and liver glycine cleavage enzyme in three families with non-ketotic hyperglycinaemia (NKH) leading to false negative prenatal diagnoses. Prenat Diagn 2000;20:367. Asatoor AM, Craske J, London DR, et al. Indole production in Hartnup disease. Lancet 1963;1:126. Auerbach VH, Digeorge AM, Baldridge RC, et al. Histidinemia. A deficiency in histidase resulting in the urinary excretion of histidine and of imidazolepyruvic acid. J Pediatr 1962;60:487. Ayling JE, Bailey SW, Boerth SR, et al. Hyperphenylalaninemia and 7-pterin excretion associated with mutations in 4a-hydroxytetrahydrobiopterin dehydratase/DCoH: Analysis of enzyme activity in intestinal biopsies. Mol Genet Metab 2000;70:179. Bahr O, Mader I, Zschocke J, et al. Adult onset glutaric aciduria type I presenting with a leukoencephalopathy. Neurology 2002;59:1802.
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias Bannwart C, Wermuth B, Baumgartner R, et al. Isolated biotin-resistant deficiency of 3-methylcrotonyl-CoA carboxylase presenting as a clinically severe form in a newborn with fatal outcome. J Inherit Metab Dis 1992;15:863. Barber GW, Spaeth GL. The successful treatment of homocystinuria with pyridoxine. J Pediatr 1969;75:463. Baric I, Wagner L, Feyh P, et al. Sensitivity and specificity of free and total glutaric acid and 3-hydroxyglutaric acid measurements by stableisotope dilution assays for the diagnosis of glutaric aciduria type I. J Inherit Metab Dis 1999;22:867. Barkovich AJ: Pediatric neuroimaging, 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2005. Barness LA, Young D, Mellman WJ, et al. Methylmalonate excretion in a patient with pernicious anemia. N Engl J Med 1963;268:144. Baron DN, Dent CE, Harris H, et al. Hereditary pellagra-like skin rash with temporary cerebellar ataxia, constant renal amino-aciduria, and other bizarre biochemical features. Lancet 1956;271:421. Barth PG, Valianpour F, Bowen VM, et al. X-linked cardioskeletal myopathy and neutropenia (Barth syndrome): An update. Am J Med Genet A 2004;126:349. Bartholome K, Lutz P, Bickel H. Determination of phenylalanine hydroxylase activity in patients with phenylketonuria and hyperphenylalaninemia. Pediatr Res 1975;9:899. Bauman ML, Kemper TL. Morphologic and histoanatomic observations of the brain in untreated human phenylketonuria. Acta Neuropathol (Berl) 1982;58:55. Baumgartner MR, Almashanu S, Suormala T, et al. The molecular basis of human 3-methylcrotonyl-CoA carboxylase deficiency. J Clin Invest 2001;107:495. Baumgartner MR, Dantas MF, Suormala T, et al. Isolated 3methylcrotonyl-CoA carboxylase deficiency: Evidence for an allelespecific dominant negative effect and responsiveness to biotin therapy. Am J Hum Genet 2004;75:790. Beaudet AL. Aspartoacylase deficiency: Canavan disease. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:5799. Beblo S, Reinhardt H, Muntau AC, et al. Fish oil supplementation improves visual evoked potentials in children with phenylketonuria. Neurology 2001;57:1488. Beckman DR, Hoganson G, Berlow S, et al. Pathological findings in 5,10-methylene tetrahydrofolate reductase deficiency. Birth Defects Orig Artic Ser 1987;23:47. Bergen BJ, Stumpf DA, Haas R, et al. A mechanism of toxicity of isovaleric acid in rat liver mitochondria. Biochem Med 1982;27:154. Bergeron P, Laberge C, Grenier A. Hereditary tyrosinemia in the province of Quebec: Prevalence at birth and geographic distribution. Clin Genet 1974;5:157. Bickel H, Gerrard J, Hickmans EM. Influence of phenylalanine intake on phenylketonuria. Lancet 1953;265:812. Blau N, Barnes I, Dhondt JL. International database of tetrahydrobiopterin deficiencies. J Inherit Metab Dis 1996;19:8. Blau N, Thöny B, Cotton RGH, et al. Disorders of tetrahydrobiopterin and related biogenic amines. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease, Vol. II. New York: McGraw-Hill, 2001:1725. Boneh A, Degani Y, Harari M. Prognostic clues and outcome of early treatment of nonketotic hyperglycinemia. Pediatr Neurol 1996;15:137. Bonetti E, Dent CE. The determination of the optical configuration of naturally occurring amino acids using specific enzymes and paper chromatography. Biochem J 1954;57:77. Borden M, Holm J, Leslie J, et al. Hawkinsinuria in two families. Am J Med Genet 1992;44:52. Boulat O, Benador N, Girardin E, et al. 3-Hydroxyisobutyric aciduria with a mild clinical course. J Inherit Metab Dis 1995;18:204. Bourget L, Chang TM. Phenylalanine ammonia-lyase immobilized in microcapsules for the depletion of phenylalanine in plasma in phenylketonuric rat model. Biochim Biophys Acta 1986;883:432. Brenton DP, Cusworth DC, Gaull GE. Homocystinuria. Biochemical studies of tissues including a comparison with cystathioninuria. Pediatrics 1965;35:50. Brismar J, Aqeel A, Brismar G, et al. Maple syrup urine disease: Findings on CT and MR scans of the brain in 10 infants. AJNR Am J Neuroradiol 1990;11:1219. Brun A, Borjeson M, Hultberg B, et al. Neonatal non-ketotic hyperglycinemia: A clinical, biochemical and neuropathological study including electronmicroscopic findings. Neuropaediatrie 1979;10:195.
597
Buck PS. The child who never grew. New York: John Day, 1950. Burke JP, O’Keefe M, Bowell R, et al. Ophthalmic findings in maple syrup urine disease. Metab Pediatr Syst Ophthalmol 1991;14:12. Burlina AP, Zara G, Hoffmann GF, et al. Management of movement disorders in glutaryl-CoA dehydrogenase deficiency: Anticholinergic drugs and botulinum toxin as additional therapeutic options. J Inherit Metab Dis 2004;27:911. Burri BJ, Sweetman L, Nyhan WL. Mutant holocarboxylase synthetase: Evidence for the enzyme defect in early infantile biotin-responsive multiple carboxylase deficiency. J Clin Invest 1981;68:1491. Camfield CS, Joseph M, Hurley T, et al. Optimal management of phenylketonuria: A centralized expert team is more successful than a decentralized model of care. J Pediatr 2004;145:53. Carmel R, Watkins D, Goodman SI, et al. Hereditary defect of cobalamin metabolism (cblG mutation) presenting as a neurologic disorder in adulthood. N Engl J Med 1988;318:1738. Cavalleri F, Berardi A, Burlina AB, et al. Diffusion-weighted MRI of maple syrup urine disease encephalopathy. Neuroradiology 2002;44:499. Cerone R, Holme E, Schiaffino MC, et al. Tyrosinemia type III: Diagnosis and ten-year follow-up. Acta Paediatr 1997;86:1013. Chace DH, Hillman SL, Millington DS, et al. Rapid diagnosis of maple syrup urine disease in blood spots from newborns by tandem mass spectrometry. Clin Chem 1995;41:62. Chace DH, Millington DS, Terada N, et al. Rapid diagnosis of phenylketonuria by quantitative analysis for phenylalanine and tyrosine in neonatal blood spots by tandem mass spectrometry. Clin Chem 1993;39:66. Chien YH, Hsu CC, Huang A, et al. Poor outcome for neonatal-type nonketotic hyperglycinemia treated with high-dose sodium benzoate and dextromethorphan. J Child Neurol 2004;19:39. Chitayat D, Meagher-Villemure K, Mamer OA, et al. Brain dysgenesis and congenital intracerebral calcification associated with 3hydroxyisobutyric aciduria. J Pediatr 1992;121:86. Christensen B, Refsum H, Vintermyr O, et al. Homocysteine export from cells cultured in the presence of physiological or superfluous levels of methionine: Methionine loading of non-transformed, transformed, proliferating, and quiescent cells in culture. J Cell Physiol 1991;146:52. Christensen E, Ribes A, Merinero B, et al. Correlation of genotype and phenotype in glutaryl-CoA dehydrogenase deficiency. J Inherit Metab Dis 2004;27:861. Chuang DT, Shih VE. Maple syrup urine disease (branched-chain ketoaciduria). In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease, Vol. II. New York: McGraw-Hill, 2001:1971. Clavero S, Martinez MA, Perez B, et al. Functional characterization of PCCA mutations causing propionic acidemia. Biochim Biophys Acta 2002;1588:119. Cleary MA, Walter JH, Wraith JE, et al. Magnetic resonance imaging in phenylketonuria: Reversal of cerebral white matter change. J Pediatr 1995;127:251. Cockburn F, Clark BJ. Recommendations for protein and amino acid intake in phenylketonuric patients. Eur J Pediatr 1996;155 (Suppl 1): S125. Cohn RM, Yudkoff M, Rothman R, et al. Isovaleric acidemia: Use of glycine therapy in neonates. N Engl J Med 1978;299:996. Cooper BA, Rosenblatt DS. Inherited defects of vitamin B12 metabolism. Annu Rev Nutr 1987;7:291. Coulombe JT, Shih VE, Levy HL. Massachusetts Metabolic Disorders Screening Program. II. Methylmalonic aciduria. Pediatrics 1981;67:26. Cowan MJ, Wara DW, Packman S, et al. Multiple biotin-dependent carboxylase deficiencies associated with defects in T-cell and B-cell immunity. Lancet 1979;2:115. Cuisset L, Drenth JP, Simon A, et al. Molecular analysis of MVK mutations and enzymatic activity in hyper-IgD and periodic fever syndrome. Eur J Hum Genet 2001;9:260. Cusworth DC, Dent CE. Renal clearances of amino acids in normal adults and in patients with aminoaciduria. Biochem J 1960;74:550. D’Angelo A, Selhub J. Homocysteine and thrombotic disease. Blood 1997;90:1. Danner DJ, Doering CB. Human mutations affecting branched chain alpha-ketoacid dehydrogenase. Front Biosci 1998;3: D517. Desviat LR, Perez-Cerda C, Perez B, et al. Functional analysis of MCCA and MCCB mutations causing methylcrotonylglycinuria. Mol Genet Metab 2003;80:315.
598
Genetic, Metabolic, and Neurocutaneous Disorders / 23
Dhondt JL. Tetrahydrobiopterin deficiencies: Preliminary analysis from an international survey. J Pediatr 1984;104:501. Dhondt JL. Tetrahydrobiopterin deficiencies: Lessons from the compilation of 200 patients. Dev Brain Dysfunct 1993;6:139. Dipple KM, McCabe ER. Phenotypes of patients with “simple” Mendelian disorders are complex traits: Thresholds, modifiers, and systems dynamics. Am J Hum Genet 2000;66:1729. DiSilvestre D, Koch R, Groffen J. Different clinical manifestations of hyperphenylalaninemia in three siblings with identical phenylalanine hydroxylase genes. Am J Hum Genet 1991;48:1014. Dyer CA, Kendler A, Philibotte T, et al. Evidence for central nervous system glial cell plasticity in phenylketonuria. J Neuropathol Exp Neurol 1996;55:795. Edelmann L, Wasserstein MP, Kornreich R, et al. Maple syrup urine disease: Identification and carrier-frequency determination of a novel founder mutation in the Ashkenazi Jewish population. Am J Hum Genet 2001;69:863. Eisensmith RC, Martinez DR, Kuzmin AI, et al. Molecular basis of phenylketonuria and a correlation between genotype and phenotype in a heterogeneous southeastern US population. Pediatrics 1996;97:512. Eisensmith RC, Woo SL. Population genetics of phenylketonuria. Acta Paediatr Suppl 1994;407:19. Elster AW. Glutaric aciduria type I: Value of diffusion-weighted magnetic resonance imaging for diagnosing acute striatal necrosis. J Comput Assist Tomogr 2004;28:98. Enns GM, Barkovich AJ, Rosenblatt DS, et al. Progressive neurological deterioration and MRI changes in cblC methylmalonic acidaemia treated with hydroxocobalamin. J Inherit Metab Dis 1999a;22:599. Enns GM, Martinez DR, Kuzmin AI, et al. Molecular correlations in phenylketonuria: Mutation patterns and corresponding biochemical and clinical phenotypes in a heterogeneous California population. Pediatr Res 1999b;46:594. Fariello G, Dionisi-Vici C, Orazi C, et al. Cranial ultrasonography in maple syrup urine disease. AJNR Am J Neuroradiol 1996;17:311. Fenton WA, Gravel RA, Rosenblatt DS. Disorders of propionate and methylmalonate metabolism. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:2165. Fishler K, Azen CG, Henderson R, et al. Psychoeducational findings among children treated for phenylketonuria. Am J Ment Defic 1987;92:65. Følling I. The discovery of phenylketonuria. Acta Paediatr Suppl 1994;407:4. Fowler B. Genetic defects of folate and cobalamin metabolism. Eur J Pediatr 1998;157 (Suppl 2):S60. Fowler B, Jakobs C. Post- and prenatal diagnostic methods for the homocystinurias. Eur J Pediatr 1998;157 (Suppl 2):S88. Freudenberg F, Lukacs Z, Ullrich K. 3-Hydroxyglutaric acid fails to affect the viability of primary neuronal rat cells. Neurobiol Dis 2004;16:581. Fukao T, Scriver CR, Kondo N. The clinical phenotype and outcome of mitochondrial acetoacetyl-CoA thiolase deficiency (beta-ketothiolase or T2 deficiency) in 26 enzymatically proved and mutation-defined patients. Mol Genet Metab 2001;72:109. Fukao T, Zhang GX, Sakura N, et al. The mitochondrial acetoacetyl-CoA thiolase (T2) deficiency in Japanese patients: Urinary organic acid and blood acylcarnitine profiles under stable conditions have subtle abnormalities in T2-deficient patients with some residual T2 activity. J Inherit Metab Dis 2003;26:423. Gamez A, Wang L, Straub M, et al. Toward PKU enzyme replacement therapy: PEGylation with activity retention for three forms of recombinant phenylalanine hydroxylase. Mol Ther 2004;9:124. Gerritsen T, Kaveggia E, Waisman HA. A new type of idiopathic hyperglycinemia with hypo-oxaluria. Pediatrics 1965;36:882. Gibson KM, Bennett MJ, Naylor EW, et al. 3-Methylcrotonyl-coenzyme A carboxylase deficiency in Amish/Mennonite adults identified by detection of increased acylcarnitines in blood spots of their children. J Pediatr 1998;132:519. Gibson KM, Burlingame TG, Hogema B, et al. 2-Methylbutyrylcoenzyme A dehydrogenase deficiency: A new inborn error of L-isoleucine metabolism. Pediatr Res 2000;47:830. Gompertz D, Draffan GH, Watts JL, et al. Biotin-responsive beta-methylcrotonylglycinuria. Lancet 1971;2:22. Gonzalez-Rios MC, Chuang DT, Cox RP, et al. A distinct variant of intermediate maple syrup urine disease. Clin Genet 1985a;27:153. Gonzalez-Rios MC, Whitney SC, Williams ML, et al. Lipid metabolism in biotin-responsive multiple carboxylase deficiency. J Inherit Metab Dis 1985b;8:184.
Goodman SI. Development of pathogenic concepts in glutaryl-CoA dehydrogenase deficiency: The challenge. J Inherit Metab Dis 2004;27:801. Goodman SI, Markey SP, Moe PG, et al. Glutaric aciduria: A “new” disorder of amino acid metabolism. Biochem Med 1975;12:12. Goodman SI, Moe PG, Hammond KB, et al. Homocystinuria with methylmalonic aciduria: Two cases in a sibship. Biochem Med 1970;4:500. Gortner L, Leupold D, Pohlandt F, et al. Peritoneal dialysis in the treatment of metabolic crises caused by inherited disorders of organic and amino acid metabolism. Acta Paediatr Scand 1989;78:706. Gouyon JB, Semama D, Prevot A, et al. Removal of branched-chain amino acids and alpha-ketoisocaproate by haemofiltration and haemodiafiltration. J Inherit Metab Dis 1996;19:610. Gudinchet F, Maeder P, Meuli RA, et al. Cranial CT and MRI in malignant phenylketonuria. Pediatr Radiol 1992;22:223. Guthrie R, Susi A. A simple phenylalanine method for detecting phenylketonuria in large populations of newborn infants. Pediatrics 1963;32:338. Güttler F, Henriksen KF, Guldberg P. Phenylalanine tolerance and loading with relation to genotype in phenylalanine hydroxylase deficiency. Int Pediatr 1996;11:50. Haan EA, Rogers JG, Lewis GP, et al. 5,10-Methylenetetrahydrofolate reductase deficiency. Clinical and biochemical features of a further case. J Inherit Metab Dis 1985;8:53. Hall CA. The neurologic aspects of transcobalamin II deficiency. Br J Haematol 1992;80:117. Halvorsen K, Halvorsen S. Hartnup disease. Pediatrics 1963;1:29. Hamosh A, Johnston MV. Nonketotic hyperglycinemia. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease, Vol. II. New York: McGraw-Hill, 2001:2065. Hanley WB, Demshar H, Preston MA, et al. Newborn phenylketonuria (PKU) Guthrie (BIA) screening and early hospital discharge. Early Hum Dev 1997;47:87. Hanley WB, Feigenbaum AS, Clarke JT, et al. Vitamin B12 deficiency in adolescents and young adults with phenylketonuria. Eur J Pediatr 1996;155 (Suppl 1):S145. Harding CO, Arnold G, Barness LA, et al. Functional methionine synthase deficiency due to cblG disorder: A report of two patients and a review. Am J Med Genet 1997;71:384. Harris ED Jr, Sjoerdsma A. Collagen profile in various clinical conditions. Lancet 1966;2:707. Hoffmann GF, Athanassopoulos S, Burlina AB, et al. Clinical course, early diagnosis, treatment, and prevention of disease in glutaryl-CoA dehydrogenase deficiency. Neuropediatrics 1996;27:115. Hoffmann GF, Charpentier C, Mayatepek E, et al. Clinical and biochemical phenotype in 11 patients with mevalonic aciduria. Pediatrics 1993;91:915. Holme E, Lindstedt S. Nontransplant treatment of tyrosinemia. Clin Liver Dis 2000;4:805. Hommes FA, Moss L. Myelin turnover in hyperphenylalaninaemia. A re-evaluation with the HPH-5 mouse. J Inherit Metab Dis 1992;15:243. Hoover-Fong JE, Shah S, Van Hove JL, et al. Natural history of nonketotic hyperglycinemia in 65 patients. Neurology 2004;63:1847. Houten SM, Frenkel J, Waterham HR. Isoprenoid biosynthesis in hereditary periodic fever syndromes and inflammation. Cell Mol Life Sci 2003;60:1118. Huether G, Kaus R, Neuhoff V. Brain development in experimental hyperphenylalaninaemia: Myelination. Neuropediatrics 1982;13:177. Huijbregts SC, de Sonneville LM, van Spronsen FJ, et al. The neuropsychological profile of early and continuously treated phenylketonuria: Orienting, vigilance, and maintenance versus manipulation-functions of working memory. Neurosci Biobehav Rev 2002;26:697. Hunziker N. Richner-Hanhart syndrome and tyrosinemia type II. Dermatologica 1980;160:180. Hutchinson RJ, Bunnell K, Thoene JG. Suppression of granulopoietic progenitor cell proliferation by metabolites of the branched-chain amino acids. J Pediatr 1985;106:62. Huttenlocher PR. The neuropathology of phenylketonuria: Human and animal studies. Eur J Pediatr 2000;159 (Suppl 2):S102. Infante JP, Huszagh VA. Impaired arachidonic (20:4n-6) and docosahexaenoic (22:6n-3) acid synthesis by phenylalanine metabolites as etiological factors in the neuropathology of phenylketonuria. Mol Genet Metab 2001;72:185. Isherwood DM. Homocystinuria. BMJ 1996;313:1025.
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias Jackson AH, Applegarth DA, Toone JR, et al. Atypical nonketotic hyperglycinemia with normal cerebrospinal fluid to plasma glycine ratio. J Child Neurol 1999;14:464. Jaeken J, Corbeel L, Casaer P, et al. Dipropylacetate (valproate) and glycine metabolism. Lancet 1977;2:617. Jain A, Buist NR, Kennaway NG, et al. Effect of ascorbate or N-acetylcysteine treatment in a patient with hereditary glutathione synthetase deficiency. J Pediatr 1994;124:229. Jakobs C, Sweetman L, Nyhan WL, et al. Stable isotope dilution analysis of 3-hydroxyisovaleric acid in amniotic fluid: Contribution to the prenatal diagnosis of inherited disorders of leucine catabolism. J Inherit Metab Dis 1984;7:15. Jan W, Zimmerman RA, Wang ZJ, et al. MR diffusion imaging and MR spectroscopy of maple syrup urine disease during acute metabolic decompensation. Neuroradiology 2003;45:393. Johnson JL, Hainline BE, Rajagopalan KV. Characterization of the molybdenum cofactor of sulfite oxidase, xanthine, oxidase, and nitrate reductase. Identification of a pteridine as a structural component. J Biol Chem 1980;255:1783. Johnson JL, Rajagopalan KV. An HPLC assay for detection of elevated urinary S-sulphocysteine, a metabolic marker of sulphite oxidase deficiency. J Inherit Metab Dis 1995;18:40. Johnson JL, Waud WR, Rajagopalan KV, et al. Inborn errors of molybdenum metabolism: Combined deficiencies of sulfite oxidase and xanthine dehydrogenase in a patient lacking the molybdenum cofactor. Proc Natl Acad Sci U S A 1980;77:3715. Jouvet P, Jugie M, Rabier D, et al. Combined nutritional support and continuous extracorporeal removal therapy in the severe acute phase of maple syrup urine disease. Intensive Care Med 2001;27:1798. Kahler SG, Sherwood WG, Woolf D, et al. Pancreatitis in patients with organic acidemias. J Pediatr 1994;124:239. Kang ES, Gerald PS. Hereditary tyrosinemia and abnormal pyrrole metabolism. J Pediatr 1970;77:397. Kanwar YS, Manaligod JR, Wong PW. Morphologic studies in a patient with homocystinuria due to 5,10-methylenetetrahydrofolate reductase deficiency. Pediatr Res 1976;10:598. Kaplan P, Mazur A, Field M, et al. Intellectual outcome in children with maple syrup urine disease. J Pediatr 1991;119:46. Kayaalp E, Treacy E, Waters PJ, et al. Human phenylalanine hydroxylase mutations and hyperphenylalaninemia phenotypes: A metanalysis of genotype-phenotype correlations. Am J Hum Genet 1997;61:1309. Kelleher JF Jr, Yudkoff M, Hutchinson R, et al. The pancytopenia of isovaleric acidemia. Pediatrics 1980;65:1023. Kleta R, Skovby F, Christensen E, et al. 3-Methylglutaconic aciduria type III in a non-Iraqi-Jewish kindred: Clinical and molecular findings. Mol Genet Metab 2002;76:201. Ko FJ, Nyhan WL, Wolff J, et al. 3-Hydroxyisobutyric aciduria: An inborn error of valine metabolism. Pediatr Res 1991;30:322. Koch JH. Robert Guthrie: The PKU story. Pasadena: Hope Publishing House, 1997. Koch R, Moseley KD, Yano S, et al. Large neutral amino acid therapy and phenylketonuria: A promising approach to treatment. Mol Genet Metab 2003;79:110. Koch SE, Packman S, Koch TK, et al. Dermatitis in treated maple syrup urine disease. J Am Acad Dermatol 1993;28:289. Koeberl DD, Millington DS, Smith WE, et al. Evaluation of 3methylcrotonyl-CoA carboxylase deficiency detected by tandem mass spectrometry newborn screening. J Inherit Metab Dis 2003;26:25. Kolker S, Koeller DM, Okun JG, et al. Pathomechanisms of neurodegeneration in glutaryl-CoA dehydrogenase deficiency. Ann Neurol 2004;55:7. Komrower GM, Lambert AM, Cusworth DC, et al. Dietary treatment of homocystinuria. Arch Dis Child 1966;41:666. Korman SH, Boneh A, Ichinohe A, et al. Persistent NKH with transient or absent symptoms and a homozygous GLDC mutation. Ann Neurol 2004;56:139. Korman SH, Gutman A. Pitfalls in the diagnosis of glycine encephalopathy (non-ketotic hyperglycinemia). Dev Med Child Neurol 2002;44:712. Kure S, Kojima K, Ichinohe A, et al. A comprehensive mutation analysis of GLDC, AMT and GCSH in glycine encephalopathy. J Inherit Metab Dis 2003;26:66. Kure S, Rolland MO, Leisti J, et al. Prenatal diagnosis of non-ketotic hyperglycinaemia: Enzymatic diagnosis in 28 families and DNA diagnosis detecting prevalent Finnish and Israeli-Arab mutations. Prenat Diagn 1999;19:717.
599
Kvittingen EA. Tyrosinaemia type I—an update. J Inherit Metab Dis 1991;14:554. Kwok SC, Ledley FD, DiLella AG, et al. Nucleotide sequence of a full-length complementary DNA clone and amino acid sequence of human phenylalanine hydroxylase. Biochemistry 1985;24:556. Kyllerman M, Skjeldal O, Christensen E, et al. Long-term follow-up, neurological outcome and survival rate in 28 Nordic patients with glutaric aciduria type 1. Eur J Paediatr Neurol 2004;8:121. Larsson A, Wachtmeister L, von Wendt L, et al. Ophthalmological, psychometric and therapeutic investigation in two sisters with hereditary glutathione synthetase deficiency (5-oxoprolinuria). Neuropediatrics 1985;16:131. Ledley FD, Levy HL, Shih VE, et al. Benign methylmalonic aciduria. N Engl J Med 1984;311:1015. Lee HH, Kim do J, Ahn HJ, et al. Crystal structure of T-protein of the glycine cleavage system: Cofactor binding, insights into H-protein recognition, and molecular basis for understanding nonketotic hyperglycinemia. J Biol Chem 2004;279:50514. Lenke RR, Levy HL. Maternal phenylketonuria and hyperphenylalaninemia. An international survey of the outcome of untreated and treated pregnancies. N Engl J Med 1980;303:1202. Leonard JV, Vijayaraghavan S, Walter JH. The impact of screening for propionic and methylmalonic acidaemia. Eur J Pediatr 2003;162 (Suppl 1):S21. Leonard JV, Walter JH, McKiernan PJ. The management of organic acidaemias: The role of transplantation. J Inherit Metab Dis 2001;24:309. Levitt M, Nixon PF, Pincus JH, et al. Transport characteristics of folates in cerebrospinal fluid: A study utilizing doubly labeled 5methyltetrahydrofolate and 5-formyltetrahydrofolate. J Clin Invest 1971;50:1301. Levy HL, Shih VE, Madigan PM. Routine newborn screening for histidinemia. Clinical and biochemical results. N Engl J Med 1974;291:1214. Lindblad B, Lindblad BS, Olin P, et al. Methylmalonic acidemia. A disorder associated with acidosis, hyperglycinemia, and hyperlactatemia. Acta Paediatr Scand 1968;57:417. Lindner M, Kolker S, Schulze A, et al. Neonatal screening for glutaryl-CoA dehydrogenase deficiency. J Inherit Metab Dis 2004;27:851. Lucke T, Perez-Cerda C, Baumgartner M, et al. Propionic acidemia: Unusual course with late onset and fatal outcome. Metabolism 2004;53:809. Lueder GT, Steiner RD. Ophthalmic abnormalities in molybdenum cofactor deficiency and isolated sulfite oxidase deficiency. J Pediatr Ophthalmol Strabismus 1995;32:334. Lund TM, Christensen E, Kristensen AS, et al. On the neurotoxicity of glutaric, 3-hydroxyglutaric, and trans-glutaconic acids in glutaric acidemia type 1. J Neurosci Res 2004;77:143. MacDonald JT, Sher PK. Ophthalmoplegia as a sign of metabolic disease in the newborn. Neurology 1977;27:971. Maeda T, Inutsuka M, Goto K, et al. Transient nonketotic hyperglycinemia in an asphyxiated patient with pyridoxine-dependent seizures. Pediatr Neurol 2000;22:225. Mahon BE, Levy HL. Maternal Hartnup disorder. Am J Med Genet 1986;24:513. Martensson J, Gustafsson J, Larsson A. A therapeutic trial with Nacetylcysteine in subjects with hereditary glutathione synthetase deficiency (5-oxoprolinuria). J Inherit Metab Dis 1989;12:120. Matalon R, Koch R, Michals-Matalon K, et al. Biopterin responsive phenylalanine hydroxylase deficiency. Genet Med 2004;6:27. Matalon R, Surendran S, Matalon KM, et al. Future role of large neutral amino acids in transport of phenylalanine into the brain. Pediatrics 2003;112:1570. Matern D, He M, Berry SA, et al. Prospective diagnosis of 2methylbutyryl-CoA dehydrogenase deficiency in the Hmong population by newborn screening using tandem mass spectrometry. Pediatrics 2003;112:74. Matsui SM, Mahoney MJ, Rosenberg LE. The natural history of the inherited methylmalonic acidemias. N Engl J Med 1983;308:857. Mayatepek E. 5-Oxoprolinuria in patients with and without defects in the gamma-glutamyl cycle. Eur J Pediatr 1999;158:221. Mayatepek E, Kurczynski TW, Hoppel CL. Long-term L-carnitine treatment in isovaleric acidemia. Pediatr Neurol 1991;7:137. McVoy JR, Levy HL, Lawler M, et al. Partial biotinidase deficiency: Clinical and biochemical features. J Pediatr 1990;116:78.
600
Genetic, Metabolic, and Neurocutaneous Disorders / 23
Mendiola J Jr, Robotham JL, Liehr JG, et al. Neonatal lethargy due to isovaleric acidemia and hyperammonemia. Tex Med 1984;80:52. Menkes JH, Hurst PL, Craig JM. A new syndrome: Progressive familial infantile cerebral dysfunction associated with an unusual urinary substance. Pediatrics 1954;14:462. Millot F, Dhondt JL, Mazingue F, et al. Changes of cerebral biopterin and biogenic amine metabolism in leukemic children receiving 5 g/m2 intravenous methotrexate. Pediatr Res 1995;37:151. Milne MD, Crawford MA, Girao CB, et al. The metabolic disorder in Hartnup disease. Q J Med 1960;29:407. Mitchell G, Larochelle J, Lambert M, et al. Neurologic crises in hereditary tyrosinemia. N Engl J Med 1990;322:432. Mitchell GA, Fukao T. Inborn errors of ketone body metabolism. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:2327. Mitchell GA, Russo P, Dubois J, Alvarez F. Tyrosinemia. In: Suchy FJ, ed. Liver disease in children. St Louis: Mosby–Year Book, 2001:667. Moller HE, Weglage J, Bick U, et al. Brain imaging and proton magnetic resonance spectroscopy in patients with phenylketonuria. Pediatrics 2003;112:1580. Morris AA, Hoffmann GF, Naughten ER, et al. Glutaric aciduria and suspected child abuse. Arch Dis Child 1999;80:404. Morton DH, Strauss KA, Robinson DL, et al. Diagnosis and treatment of maple syrup disease: A study of 36 patients. Pediatrics 2002;109:999. Mudd SH, Finkelstein JD, Irreverre F, et al. Homocystinuria: An enzymatic defect. Science 1964;143:1443. Mudd SH, Irreverre F, Laster L. Sulfite oxidase deficiency in man: Demonstration of the enzymatic defect. Science 1967;156:1599. Mudd SH, Skovby F, Levy HL, et al. The natural history of homocystinuria due to cystathionine beta-synthase deficiency. Am J Hum Genet 1985;37:1. Mudd SH, Uhlendorf BW, Freeman JM, et al. Homocystinuria associated with decreased methylenetetrahydrofolate reductase activity. Biochem Biophys Res Commun 1972;46:905. Muhlhausen C, Hoffmann GF, Strauss KA, et al. Maintenance treatment of glutaryl-CoA dehydrogenase deficiency. J Inherit Metab Dis 2004;27:885. Munnich A, Saudubray JM, Coude FX, et al. Fatty-acid-responsive alopecia in multiple carboxylase deficiency. Lancet 1980;1:1080. Muntau AC, Roschinger W, Habich M, et al. Tetrahydrobiopterin as an alternative treatment for mild phenylketonuria. N Engl J Med 2002;347:2122. Naughten ER, Yap S, Mayne PD. Newborn screening for homocystinuria: Irish and world experience. Eur J Pediatr 1998;157 (Suppl 2):S84. Nellis MM, Danner DJ. Gene preference in maple syrup urine disease. Am J Hum Genet 2001;68:232. Neuberger JM, Schweitzer S, Rolland MO, et al. Effect of sodium benzoate in the treatment of atypical nonketotic hyperglycinaemia. J Inherit Metab Dis 2000;23:22. Neumaier-Probst E, Harting I, Seitz A, et al. Neuroradiological findings in glutaric aciduria type I (glutaryl-CoA dehydrogenase deficiency). J Inherit Metab Dis 2004;27:869. Nguyen TV, Andresen BS, Corydon TJ, et al. Identification of is obutyryl-CoA dehydrogenase and its deficiency in humans. Mol Genet Metab 2002;77:68. Nyhan W. Abnormalities in amino acid metabolism in clinical medicine. Norwalk, CT: Appleton-Century-Crofts, 1984. Nyhan WL, Fawcett N, Ando T, et al. Response to dietary therapy in B12 unresponsive methylmalonic acidemia. Pediatrics 1973;51:539. Nyhan WL, Rice-Kelts M, Klein J, et al. Treatment of the acute crisis in maple syrup urine disease. Arch Pediatr Adolesc Med 1998;152:593. Ogier de Baulny H, Gerard M, Saudubray JM, et al. Remethylation defects: Guidelines for clinical diagnosis and treatment. Eur J Pediatr 1998;157 (Suppl 2):S77. Okano Y, Eisensmith RC, Guttler F, et al. Molecular basis of phenotypic heterogeneity in phenylketonuria. N Engl J Med 1991;324:1232. Paans AM, Pruim J, Smit GP, et al. Neurotransmitter positron emission tomographic-studies in adults with phenylketonuria, a pilot study. Eur J Pediatr 1996;155 (Suppl 1):S78. Packman S, Caswell N, Gonzalez-Rios MC, et al. Acetyl CoA carboxylase in cultured fibroblasts: Differential biotin dependence in the two types of biotin-responsive multiple carboxylase deficiency. Am J Hum Genet 1984;36:80. Packman S, Cowan MJ, Golbus MS, et al. Prenatal treatment of biotin responsive multiple carboxylase deficiency. Lancet 1982;1:1435.
Packman S, Sweetman L, Baker H, et al. The neonatal form of biotin-responsive multiple carboxylase deficiency. J Pediatr 1981a;99:418. Packman S, Sweetman L, Yoshino M, et al. Biotin-responsive multiple carboxylase deficiency of infantile onset. J Pediatr 1981b;99:421. Packman S, Whitney SC, Fitch M, et al. Abnormal fatty acid composition of biotin-responsive multiple carboxylase deficiency fibroblasts. J Inherit Metab Dis 1989;12:47. Parini R, Sereni LP, Bagozzi DC, et al. Nasogastric drip feeding as the only treatment of neonatal maple syrup urine disease. Pediatrics 1993;92:280. Perez-Cerda C, Clavero S, Perez B, et al. Functional analysis of PCCB mutations causing propionic acidemia based on expression studies in deficient human skin fibroblasts. Biochim Biophys Acta 2003;1638:43. Perry TL, Dunn HG, Hansen S, et al. Early diagnosis and treatment of homocystinuria. Pediatrics 1966;37:502. Perry TL, Urquhart N, Hansen S. Studies of the glycine cleavage enzyme system in brain from infants with glycine encephalopathy. Pediatr Res 1977;11:1192. Pey AL, Perez B, Desviat LR, et al. Mechanisms underlying responsiveness to tetrahydrobiopterin in mild phenylketonuria mutations. Hum Mutat 2004;24:388. Phenylketonuria (PKU). Screening and management. NIH Consens Statement 2000;17:1. Phillips MD, McGraw P, Lowe MJ, et al. Diffusion-weighted imaging of white matter abnormalities in patients with phenylketonuria. AJNR Am J Neuroradiol 2001;22:1583. Pietz J, Benninger C, Schmidt H, et al. Long-term development of intelligence (IQ) and EEG in 34 children with phenylketonuria treated early. Eur J Pediatr 1988;147:361. Pietz J, Fatkenheuer B, Burgard P, et al. Psychiatric disorders in adult patients with early-treated phenylketonuria. Pediatrics 1997;99:345. Pietz J, Meyding-Lamade UK, Schmidt H. Magnetic resonance imaging of the brain in adolescents with phenylketonuria and in one case of 6pyruvoyl tetrahydropteridine synthase deficiency. Eur J Pediatr 1996;155 (Suppl 1): S69. Proud VK, Rizzo WB, Patterson JW, et al. Fatty acid alterations and carboxylase deficiencies in the skin of biotin-deficient rats. Am J Clin Nutr 1990;51:853. Puliyanda DP, Harmon WE, Peterschmitt MJ, et al. Utility of hemodialysis in maple syrup urine disease. Pediatr Nephrol 2002;17:239. Rakocevic G, Lyons KE, Wilkinson SB, et al. Bilateral pallidotomy for severe dystonia in an 18-month-old child with glutaric aciduria. Stereotact Funct Neurosurg 2004;82:80. Rezvani I: Defects in metabolism of amino acids. In: Behrman R, Kliegman R, Jenson H, eds. Nelson textbook of pediatrics, 16th ed. Philadelphia: WB Saunders, 2000:355. Rhead WJ, Tanaka K. Demonstration of a specific mitochondrial isovaleryl-CoA dehydrogenase deficiency in fibroblasts from patients with isovaleric acidemia. Proc Natl Acad Sci U S A 1980;77:580. Ristoff E, Mayatepek E, Larsson A. Long-term clinical outcome in patients with glutathione synthetase deficiency. J Pediatr 2001;139:79. Roe CR, Bohan TP. L-Carnitine therapy in propionicacidaemia. Lancet 1982;1:1411. Roe CR, Cederbaum SD, Roe DS, et al. Isolated isobutyryl-CoA dehydrogenase deficiency: An unrecognized defect in human valine metabolism. Mol Genet Metab 1998;65:264. Rosenberg LE, Lilljeqvist AC, Hsia YE. Methylmalonic aciduria. An inborn error leading to metabolic acidosis, long-chain ketonuria and intermittent hyperglycinemia. N Engl J Med 1968;278:1319. Rosenblatt DS, Aspler AL, Shevell MI, et al. Clinical heterogeneity and prognosis in combined methylmalonic aciduria and homocystinuria (cblC). J Inherit Metab Dis 1997;20:528. Rosenblatt DS, Cooper BA. Inherited disorders of vitamin B12 metabolism. Blood Rev 1987;1:177. Rosenblatt DS, Cooper BA. Inherited disorders of vitamin B12 utilization. Bioessays 1990;12:331. Rosenblatt DS, Cooper BA, Schmutz SM, et al. Prenatal vitamin B12 therapy of a fetus with methylcobalamin deficiency (cobalamin E disease). Lancet 1985;1:1127. Roth A, Nogues C, Monnet JP, et al. Anatomo-pathological findings in a case of combined deficiency of sulphite oxidase and xanthine oxidase with a defect of molybdenum cofactor. Virchows Arch A Pathol Anat Histopathol 1985;405:379.
Enns, Cowan, Klein, and Packman / Aminoacidemias and Organic Acidemias Roth KS, Yang W, Allan L, et al. Prenatal administration of biotin in biotin responsive multiple carboxylase deficiency. Pediatr Res 1982;16:126. Ruetschi U, Cerone R, Perez-Cerda C, et al. Mutations in the 4hydroxyphenylpyruvate dioxygenase gene (HPD) in patients with tyrosinemia type III. Hum Genet 2000;106:654. Russo PA, Mitchell GA, Tanguay RM. Tyrosinemia: A review. Pediatr Dev Pathol 2001;4:212. Sakaguchi Y, Yoshino M, Aramaki S, et al. Dihydrolipoyl dehydrogenase deficiency: A therapeutic trial with branched-chain amino acid restriction. Eur J Pediatr 1986;145:271. Sakai LY, Keene DR, Engvall E. Fibrillin, a new 350-kD glycoprotein, is a component of extracellular microfibrils. J Cell Biol 1986;103:2499. Sakamoto O, Suzuki Y, Li X, et al. Relationship between kinetic properties of mutant enzyme and biochemical and clinical responsiveness to biotin in holocarboxylase synthetase deficiency. Pediatr Res 1999;46:671. Sakura N, Ono H, Nomura S, et al. Betaine dose and treatment intervals in therapy for homocystinuria due to 5,10-methylenetetrahydrofolate reductase deficiency. J Inherit Metab Dis 1998;21:84. Samady JA, Schwartz RA, Shih LY, et al. Acrodermatitis enteropathica-like eruption in an infant with nonketotic hyperglycinemia. J Dermatol 2000;27:604. Sander JE, Malamud N, Cowan MJ, et al. Intermittent ataxia and immunodeficiency with multiple carboxylase deficiencies: A biotin-responsive disorder. Ann Neurol 1980;8:544. Sarkissian CN, Shao Z, Blain F, et al. A different approach to treatment of phenylketonuria: Phenylalanine degradation with recombinant phenylalanine ammonia lyase. Proc Natl Acad Sci U S A 1999;96:2339. Sasaki M, Iwata H, Sugai K, et al. A severely brain-damaged case of 3-hydroxyisobutyric aciduria. Brain Dev 2001;23:243. Sass JO, Hofmann M, Skladal D, et al. Propionic acidemia revisited: A workshop report. Clin Pediatr (Phila) 2004a;43:837. Sass JO, Sander S, Zschocke J. Isobutyryl-CoA dehydrogenase deficiency: Isobutyrylglycinuria and ACAD8 gene mutations in two infants. J Inherit Metab Dis 2004b;27:741. Sassa S, Kappas A. Hereditary tyrosinemia and the heme biosynthetic pathway. Profound inhibition of delta-aminolevulinic acid dehydratase activity by succinylacetone. J Clin Invest 1983;71:625. Sassa S, Kawakami M, Cerami A. Inhibition of the growth and differentiation of erythroid precursor cells by an endotoxin-induced mediator from peritoneal macrophages. Proc Natl Acad Sci U S A 1983;80:1717. Saudubray JM, Charpentier C. Clinical phenotypes: Diagnosis/algorithms. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:1327. Schadewaldt P, Bodner-Leidecker A, Hammen HW, et al. Significance of L-alloisoleucine in plasma for diagnosis of maple syrup urine disease. Clin Chem 1999;45:1734. Schmidt H, Ullrich K, Korinthenberg R, et al. Basal ganglion calcification in hyperphenylalaninemia due to deficiency of dihydropteridine reductase. Pediatr Radiol 1988;19:54. Schuler A, Blau N, Ponzone A. Monoamine oxidase inhibitors in tetrahydrobiopterin deficiency. Eur J Pediatr 1995;154:997. Schurmann M, Engelbrecht V, Lohmeier K, et al. Cerebral metabolic changes in biotinidase deficiency. J Inherit Metab Dis 1997;20:755. Scriver CR. Hartnup disease: A genetic modification of intestinal and renal transport of certain neutral alpha-amino acids. N Engl J Med 1965;273:530. Scriver CR. Nutrient-gene interactions: The gene is not the disease and vice versa. Am J Clin Nutr 1988;48:1505. Scriver CR, Kaufman S. Hyperphenylalaninemia: Phenylalanine hydroxylase deficiency. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease, Vol. II. New York: McGraw-Hill, 2001:1667. Scriver CR, Levy HL. Histidinaemia. Part I. Reconciling retrospective and prospective findings. J Inherit Metab Dis 1983;6:51. Scriver CR, Mackenzie S, Clow CL, et al. Thiamine-responsive maple-syrup-urine disease. Lancet 1971;1:310. Scriver CR, Mahon B, Levy HL, et al. The Hartnup phenotype: Mendelian transport disorder, multifactorial disease. Am J Hum Genet 1987;40:401. Scriver CR, Waters PJ. Monogenic traits are not simple: Lessons from phenylketonuria. Trends Genet 1999;15:267.
601
Sener RN. Nonketotic hyperglycinemia: Diffusion magnetic resonance imaging findings. J Comput Assist Tomogr 2003;27:538. Shi ZZ, Habib GM, Rhead WJ, et al. Mutations in the glutathione synthetase gene cause 5-oxoprolinuria. Nat Genet 1996;14:361. Shih VE, Axel SM, Tewksbury JC, et al. Defective lysosomal release of vitamin B12 (cb1F): A hereditary cobalamin metabolic disorder associated with sudden death. Am J Med Genet 1989;33:555. Shintaku H. Disorders of tetrahydrobiopterin metabolism and their treatment. Curr Drug Metab 2002;3:123. Simon A, Kremer HP, Wevers RA, et al. Mevalonate kinase deficiency: Evidence for a phenotypic continuum. Neurology 2004;62:994. Skullerud K, Marstein S, Schrader H, et al. The cerebral lesions in a patient with generalized glutathione deficiency and pyroglutamic aciduria (5-oxoprolinuria). Acta Neuropathol (Berl) 1980;52:235. Smith I, Beasley MG, Ades AE. Effect on intelligence of relaxing the low phenylalanine diet in phenylketonuria. Arch Dis Child 1991;66:311. Smith I, Knowles J. Behaviour in early treated phenylketonuria: A systematic review. Eur J Pediatr 2000;159 (Suppl 2):S89. Spada M, Blau N, Meli C, et al. Different strategies in the treatment of dihydropteridine reductase deficiency. Pteridines 1996;7:107. Spada M, Schuler A, Blau N, et al. Deprenyl in 6-pyruvoyl tetrahydropterin synthase deficiency (BH4 deficiency). Pteridines 1995;5:144. Stampfer MJ, Malinow MR, Willett WC, et al. A prospective study of plasma homocyst(e)ine and risk of myocardial infarction in US physicians. JAMA 1992;268:877. Strauss KA, Morton DH. Branched-chain ketoacyl dehydrogenase deficiency: Maple syrup disease. Curr Treat Options Neurol 2003a;5:329. Strauss KA, Morton DH. Type I glutaric aciduria. Part 2. A model of acute striatal necrosis. Am Med Genet 2003b;121C:53. Strauss KA, Puffenberger EG, Robinson DL, et al. Type I glutaric aciduria, part 1: Natural history of 77 patients. Am J Med Genet 2003;121C:38. Suormala T, Baumgartner MR, Coelho D, et al. The cblD defect causes either isolated or combined deficiency of methylcobalamin and adenosylcobalamin synthesis. J Biol Chem 2004;279:42742. Sweetman L, Williams JC. Branched chain organic acidurias. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:2125. Taccone A, Schiaffino MC, Cerone R, et al. Computed tomography in maple syrup urine disease. Eur J Radiol 1992;14:207. Tada K, Hirono H, Arakawa T. Endogenous renal clearance rates of free amino acids in prolinuric and Hartnup patients. Tohoku J Exp Med 1967;93:57. Tada K, Kure S. Non-ketotic hyperglycinaemia: Molecular lesion, diagnosis and pathophysiology. J Inherit Metab Dis 1993;16:691. Tada K, Tateda H, Arashima S, et al. Intellectual development in patients with untreated histidinemia. A collaborative study group of neonatal screening for inborn errors of metabolism in Japan. J Pediatr 1982;101:562. Tanaka K, Orr JC, Isselbacher KJ. Identification of beta-hydroxyisovaleric acid in the urine of a patient with isovaleric acidemia. Biochim Biophys Acta 1968;152:638. Tanaka Y, Matsuo N, Tsuzaki S, et al. On-off phenomenon in a child with tetrahydrobiopterin deficiency due to 6-pyruvoyl tetrahydropterin synthase deficiency (BH4 deficiency). Eur J Pediatr 1989;148:450. Tharp BR. Unique EEG pattern (comb-like rhythm) in neonatal maple syrup urine disease. Pediatr Neurol 1992;8:65. Thoene J, Baker H, Yoshino M, et al. Biotin-responsive carboxylase deficiency associated with subnormal plasma and urinary biotin. N Engl J Med 1981;304:817. Thompson GN, Chalmers RA, Walter JH, et al. The use of metronidazole in management of methylmalonic and propionic acidaemias. Eur J Pediatr 1990;149:792. Touati G, Rusthoven E, Depondt E, et al. Dietary therapy in two patients with a mild form of sulphite oxidase deficiency. Evidence for clinical and biological improvement. J Inherit Metab Dis 2000;23:45. Treacy EP, Delente JJ, Elkas G, et al. Analysis of phenylalanine hydroxylase genotypes and hyperphenylalaninemia phenotypes using L-[1-13C]phenylalanine oxidation rates in vivo: A pilot study. Pediatr Res 1997;42:430. Trefz FK, Blau N. Potential role of tetrahydrobiopterin in the treatment of maternal phenylketonuria. Pediatrics 2003;112:1566. Trefz FK, Burgard P, Konig T, et al. Genotype-phenotype correlations in phenylketonuria. Clin Chim Acta 1993;217:15.
602
Genetic, Metabolic, and Neurocutaneous Disorders / 23
Tuchman M, Kelly P, Watkins D, et al. Vitamin B12-responsive megaloblastic anemia, homocystinuria, and transient methylmalonic aciduria in cb1E disease. J Pediatr 1988;113:1052. Van der Klei-van Moorsel JM, Smit LM, Brockstedt M, et al. Infantile isolated sulphite oxidase deficiency: Report of a case with negative sulphite test and normal sulphate excretion. Eur J Pediatr 1991;150:196. Van Hove JL, Kishnani P, Muenzer J, et al. Benzoate therapy and carnitine deficiency in non-ketotic hyperglycinemia. Am J Med Genet 1995;59:444. Van Hove JL, Kishnani PS, Demaerel P, et al. Acute hydrocephalus in nonketotic hyperglycemia. Neurology 2000;54:754. Viola A, Chabrol B, Nicoli F, et al. Magnetic resonance spectroscopy study of glycine pathways in nonketotic hyperglycinemia. Pediatr Res 2002;52:292. Virmani K, Widhalm K. Histidinemia: A biochemical variant or a disease? J Am Coll Nutr 1993;12:115. Waisbren SE, Mahon BE, Schnell RR, et al. Predictors of intelligence quotient and intelligence quotient change in persons treated for phenylketonuria early in life. Pediatrics 1987;79:351. Waters PJ, Scriver CR. In vitro expression analysis of mutations in phenylalanine hydroxylase: Linking genotype to phenotype and structure to function. Hum Mutat 1998;11:4. Watkins D, Rosenblatt DS. Functional methionine synthase deficiency (cblE and cblG): Clinical and biochemical heterogeneity. Am J Med Genet 1989;34:427. Webster LT, Siddiqui UA, Lucas SV, et al. Identification of separate acyl-CoA:glycine and acyl-CoA:L-glutamine N-acyltransferase activities in mitochondrial fractions from liver of rhesus monkey and man. J Biol Chem 1976;251:3352. Weglage J, Ullrich K, Pietsch M, et al. Untreated non-phenylketonurichyperphenylalaninaemia: Intellectual and neurological outcome. Eur J Pediatr 1996;155 (Suppl 1):S26. Weglage J, Wiedermann D, Moller H, et al. Pathogenesis of different clinical outcomes in spite of identical genotypes and comparable blood phenylalanine concentrations in phenylketonurics. J Inherit Metab Dis 1998;21:181. Wellner VP, Sekura R, Meister A, et al. Glutathione synthetase deficiency, an inborn error of metabolism involving the gamma-glutamyl cycle in patients with 5-oxoprolinuria (pyroglutamic aciduria). Proc Natl Acad Sci U S A 1974;71:2505. Welsh MC, Pennington BF, Ozonoff S, et al. Neuropsychology of early-treated phenylketonuria: Specific executive function deficits. Child Dev 1990;61:1697. Wendel U, Langenbeck U, Lombeck I, et al. Exchange transfusion in acute episodes of maple syrup urine disease. Studies on branched-chain amino and keto acids. Eur J Pediatr 1982;138:293. Wendel U, Saudubray JM, Bodner A, et al. Liver transplantation in maple syrup urine disease. Eur J Pediatr 1999;158 (Suppl 2):S60. Westall RG, Dancis J, Miller S. Maple sugar urine disease. Am J Dis Child 1957;94:571.
Widaman KF, Azen C. Relation of prenatal phenylalanine exposure to infant and childhood cognitive outcomes: Results from the International Maternal PKU Collaborative Study. Pediatrics 2003;112:1537. Wilcken B, Yu JS, Brown DA. Natural history of Hartnup disease. Arch Dis Child 1977;52:38. Wilcken DE, Dudman NP, Tyrrell PA. Homocystinuria due to cystathionine beta-synthase deficiency—the effects of betaine treatment in pyridoxine-responsive patients. Metabolism 1985;34:1115. Wilcken DE, Wilcken B. The natural history of vascular disease in homocystinuria and the effects of treatment. J Inherit Metab Dis 1997;20:295. Wilcox WR, Cederbaum SD: Amino acid metabolism. In: Rimoin D, Connor J, Pyeritz R, Korf B, eds. Principles and practice of medical genetics, 4th ed. Philadelphia: Churchill Livingstone, 2002:2406. Williams ML, Packman S, Cowan MJ. Alopecia and periorificial dermatitis in biotin-responsive multiple carboxylase deficiency. J Am Acad Dermatol 1983;9:97. Wilson WG, Audenaert SM, Squillaro EJ. Hyperammonaemia in a preterm infant with isovaleric acidaemia. J Inherit Metab Dis 1984;7:71. Wiltshire EJ, Poplawski NK, Harrison JR, et al. Treatment of late-onset nonketotic hyperglycinaemia: Effectiveness of imipramine and benzoate. J Inherit Metab Dis 2000;23:15. Wolf B. Worldwide survey of neonatal screening for biotinidase deficiency. J Inherit Metab Dis 1991;14:923. Wolf B. Disorders of biotin metabolism. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001:3935. Wolf B, Grier RE, Allen RJ, et al. Biotinidase deficiency: The enzymatic defect in late-onset multiple carboxylase deficiency. Clin Chim Acta 1983;131:273. Wong PW, Justice P, Hruby M, et al. Folic acid nonresponsive homocystinuria due to methylenetetrahydrofolate reductase deficiency. Pediatrics 1977;59:749. Woody NC, Snyder CH, Harris JA. Histidinemia. Am J Dis Child 1965;110:606. Woody RC, Brewster MA. Adverse effects of trimethoprimsulfamethoxazole in a child with dihydropteridine reductase deficiency. Dev Med Child Neurol 1990;32:639. Yannicelli S, Acosta PB, Velazquez A, et al. Improved growth and nutrition status in children with methylmalonic or propionic acidemia fed an elemental medical food. Mol Genet Metab 2003;80:181. Yap S, Rushe H, Howard PM, et al. The intellectual abilities of early-treated individuals with pyridoxine-nonresponsive homocystinuria due to cystathionine beta-synthase deficiency. J Inherit Metab Dis 2001;24:437. Yorifuji T, Kawai M, Mamada M, et al. Living-donor liver transplantation for propionic acidaemia. J Inherit Metab Dis 2004;27:205. Zeman J, Bayer M, Stepan J. Bone mineral density in patients with phenylketonuria. Acta Paediatr 1999;88:1348.
CHAPTER 24
Inborn Errors of Urea Synthesis Mark L. Batshaw, Uta Lichter-Konecki, and Mendel Tuchman
Inherited urea cycle disorders represent a devastating group of inborn errors of metabolism that are associated with hyperammonemic encephalopathy and high mortality and morbidity rates. They comprise deficiencies in any of the six enzymes and two amino acid transporters involved in urea synthesis (Fig. 24-1). Accordingly, these disorders are named as follows (estimated prevalence rates are given) [Brusilow and Maestri, 1996; Tuchman, 1992; Yamanouchi et al., 2002]: • N-acetylglutamate synthase (NAGS) deficiency (prevalence unknown) • Carbamyl phosphate synthetase I (CPS I) deficiency (1 case per 62,000 population) • Ornithine transcarbamylase (OTC) deficiency (1 per 14,000) • Citrullinemia type II (mitochondrial aspartate/glutamate transport carrier [citrin] deficiency) (1 per 21,000 in Japan) • Argininosuccinate synthetase (ASS) deficiency (citrullinemia) (1 per 57,000) • Argininosuccinate lyase (ASL) deficiency (argininosuccinicaciduria) (1 per 70,000) • Arginase (ARG) deficiency (hyperargininemia) (1 per 353,000) • Hyperornithinemia-hyperammonemiahomocitrullinuria (HHH) syndrome (mitochondrial ornithine carrier deficiency) (prevalence unknown) These disorders are inherited as autosomal-recessive traits, except for ornithine transcarbamylase deficiency, which is X-linked. Because of the absence of mass newborn screening for these disorders, the true incidence of urea cycle disorders is unknown. Based on case reports and questionnaires about referred patients, the combined prevalence of all urea cycle disorders is estimated to be 1 per 8200 [Brusilow and Maestri, 1996]. Other than in arginase deficiency, infants with a complete deficiency of a urea cycle enzyme (N-acetylglutamate synthase, CPS I, ornithine transcarbamylase, argininosuccinate synthetase, or argininosuccinate lyase) commonly present in the newborn period with hyperammonemic coma. Despite aggressive treatment that relies primarily on hemodialysis, the mortality rate in infancy has been reported to approximate 50% [Maestri et al., 1999], and as demonstrated by our previous studies, virtually all of the survivors are left with developmental disabilities [Msall et al., 1984]. Patients with late-onset disease (those with partial enzyme deficiencies, including ornithine transcarbamylase–deficient female heterozygotes) may present at any age with hyperammonemic crises that carry a 10% mortality rate and a significant risk of developmental disabilities [Batshaw et al., 1986]. Even asymptomatic ornithine transcarbamylase–
deficient heterozygotes have been shown to have mild cognitive deficits [Batshaw et al., 1980; Gyato et al., 2004].
THE UREA CYCLE Dietary protein, on average, contains approximately 16% nitrogen. Greater than 90% of the nitrogen that is not used for anabolic processes normally is metabolized and excreted as urea. Therefore, substantial urea synthesis capacity (approximately 16 g per day in adults) is required [Linder, 1991]. With a deficiency of one of the urea cycle enzymes, an insufficient amount of urea will be formed, and nitrogen in the form of ammonia will accumulate. Accumulation in brain causes encephalopathic episodes. The urea cycle was proposed by Hans Krebs and Kurt Henseleit in 1932 and was the first cyclic pathway elucidated. Six enzymes and five cofactors or transporters are necessary for optimal urea cycle activity (see Fig. 24-1). The clinically most important cofactor is N-acetylglutamate, which is formed from acetyl coenzyme A (acetyl-CoA) and glutamate in a reaction catalyzed by N-acetylglutamate synthase. N-acetylglutamate synthase activates the first enzyme of the urea cycle, CPS I, which uses adenosine triphosphate and bicarbonate to synthesize carbamyl phosphate from ammonia, contributing the first atom of waste nitrogen to the cycle. CPS I is expressed in periportal hepatocytes and intestinal mucosa epithelial cells [Ryall et al., 1985]. It is the most abundant protein in liver mitochondria, accounting for 20% of the mitochondrial matrix protein [Lusty, 1978]. The enzyme consists of a single polypeptide with a molecular weight of 165,000 and approximately 1500 amino acid residues [Haraguchi et al., 1991]. The second enzyme in the urea cycle, ornithine transcarbamylase, like CPS I, is mitochondrial. Citrulline is formed by the action of ornithine transcarbamylase on carbamyl phosphate and ornithine. Once formed, citrulline is actively moved, by means of the ornithine transporter, out of the mitochondrion and into the cytosol, where it is conjugated with aspartate to form argininosuccinic acid by argininosuccinate synthetase. Here the second atom of waste nitrogen is contributed to the cycle by aspartate. A defect in argininosuccinate synthetase leads to citrullinemia, the accumulation of citrulline in blood. A second form of citrullinemia called type II or adult-onset citrullinemia is caused by deficient activity of the mitochondrial aspartate/glutamate transporter carrier, citrin. Argininosuccinic acid subsequently is cleaved to yield fumarate and arginine by the enzyme argininosuccinate lyase. A deficiency of this enzyme is called argininosuccinicaciduria, characterized by marked urinary excretion (and accumulation in blood) of argininosuccinic acid.
604
Genetic, Metabolic, and Neurocutaneous Disorders / 24
Glutamate AcCoA NAGS CoASH N-acetylglutamate
ORNT1 Urea
Ornithine
Ornithine
CPS I CP OTC
ARG
Aspartate
Citrulline Arginine
CITR
ORNT1
Fumarate AL Argininosuccinate
NH3 HCO3– 2 ATP
FIGURE 24-1. The urea cycle. AcCoA, acetyl coenzyme A; AL, argininosuccinate lyase; ARG, arginase; AS, argininosuccinate synthetase; CITR, citrin; CoASH, uncombined acetyl coenzyme A; CPS I, carbamyl phosphate synthetase I; NAGS, N-acetylglutamate synthase; ORNT1, ornithine transporter 1; OTC, ornithine transcarbamylase.
Citrulline AS
Aspartate
The final step in the urea cycle involves cleavage of arginine to form urea and ornithine by arginase. A defect here is termed argininemia. Once formed, ornithine is transported back into the mitochondrion by the ornithine transporter. A defect in this transporter leads to the marked accumulation of ornithine in blood, resulting in hyperornithinemiahyperammonemia-homocitrullinuria syndrome. The complete urea cycle is found only in hepatocytes.
CLINICAL DESCRIPTION OF UREA CYCLE DISORDERS N-Acetylglutamate Synthase Deficiency Inherited N-acetylglutamate synthase deficiency leads to hyperammonemia by causing a secondary deficiency of CPS I. This disorder has been reported to date in approximately two dozen patients [Bachmann et al., 1982; Elpeleg et al., 2002] but is likely to be underdiagnosed because of the lack of specific
biochemical markers and the physiologically low abundance of N-acetylglutamate synthase in the liver. N-acetylglutamate synthase deficiency is inherited as an autosomal-recessive disorder and has a phenotype that is similar to that in CPS I deficiency. It is characterized by hyperammonemia in the newborn period or later in life and can be fatal or lead to mental retardation and other developmental disabilities. Plasma amino acid analysis usually demonstrates an increased level of glutamine and reduced or absent levels of citrulline. Urinary orotic acid level is normal or low. N-acetylglutamate synthase activity in the liver has a variable degree of deficiency (ranging from undetectable to normal residual activity) that is unresponsive to L-arginine. Because enzyme analysis requires large amounts of liver tissue and may not be entirely reliable, analysis of genomic DNA for mutations in the N-acetylglutamate synthase gene is the best diagnostic method [Morizono et al., 2004]. Treatment of N-acetylglutamate synthase deficiency currently consists of a low-protein diet and use of ammonia-scavenging drugs (Table 24-1). A more
TABLE 24-1 Long-Term Alternative Pathway Treatment of Urea Cycle Disorders (UCDs)* DISORDER
L-CITRULLINE
L-ARGININE FREE BASE
SODIUM PHENYLBUTYRATE
N-CARBAMYLGLUTAMATE
NAGS deficiency
—
—
—
CPS I or OTC deficiency
0.17 g/kg/d or 3.8 g/m2/d
—
Citrullinemia
—
0.40-0.50 g/kg/d or 8.8-11.0 g/m2/d
Argininosuccinic acidemia
—
Argininemia
—
0.40-0.70 g/kg/d or 8.8-15.4 g/m2/d —
0.45-0.60 g/kg if 45 kg
Olanzapine
No
5-20 mg/day
Opiate antagonist
Naltrexone
Yes
0.5-1.5 mg/kg/day
Disruptive behaviors; SIB, aggression; hyperactivity, irritability Hyperactivity, social relatedness; SIB, aggression, anxiety, irritability, depression Aggression, SIB, agitation, restlessness, hyperactivity
Risk of tardive dyskinesia and acute dystonic reactions, sedation, weight gain Increased appetite, weight gain, mild sedation, tremor, hypersalivation Increased appetite, weight gain, sedation, tremor
α2 Adrenergic agonist
Clonidine
Yes
0.15-0.2 mg/day
Hyperactivity, irritability, stereotypies, inappropriate speech, oppositional behavior, aggression
Tricyclic antidepressant/SRI
Clomipramine
Yes
25-75 mg/day, max 5 mg/kg/day
Stereotypies, anger, compulsive behaviors, social interaction, irritability
SSRIs
Fluoxetine
Yes
20-80 mg/day
Citalopram
No
2.5-20 mg/day
Sertraline
No
12.5-50 mg/day
Venlafaxine
No
6-50 mg/day
Anxiety, depression, repetitive thoughts and behaviors, irritability Repetitive behaviors, mood swings, aggression, irritability Anxiety, behavioral problems, social interaction, aggression Compulsions, repetitive behavior, hyperactivity Hyperactivity, irritability Affective instability, impulsivity, aggression, repetitive behavior Impulsivity, mood instability
SRI/NE reuptake inhibitor Stimulant Antiepileptic drugs
Methylphenidate Yes Divalproex Yes sodium Levetiracetam Yes
0.3-0.6 mg/kg/day 20-40 mg/kg/day 125-500 mg bid.
Mild gastrointestinal symptoms, decreased appetite, drowsiness Bradycardia
Urinary retention, hyperactivity, sleep disturbances, dry mouth, dizziness, seizure threshold and ECG changes Behavioral activation, aggression Headache, sedation, agitation, aggressiveness, dyskinesia Activation, insomnia, gastrointestinal side effects Behavioral activation Withdrawal, irritability Mood lability, fatigue, insomnia, diarrhea, weight gain Disinhibition
*Indicates whether controlled pediatric trials have been conducted for the drug. CGI, Clinical Global Impressions scale; ECG, electrocardiographic; HA, hyperactivity; NE, norepinephrine; SIB, self-injurious behavior; SRI, serotonin reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
and not found to be useful. Dimethylglycine, which is closely related to the inhibitory transmitter glycine, has been proposed [Rimland, 1990] as helpful for autistic children and adults, but it was ineffective in a 3-month, double-blind, placebo-controlled trial of its use in eight subjects [Bolman and Richmond, 1999]. One survey [Levy et al., 2003] found that 32% of 284 children at a Pennsylvania regional autism center were using complementary and alternative medicine. The investigators suggested that it is important to respect the parents’ belief if the complementary medicine is not toxic, but if the treatment is potentially harmful, negotiating a safer replacement practice should be attempted. Reported dramatic improvement after the administration of secretin as part of endoscopy in three autistic children led to widespread use by parents. Subsequent blinded, randomized trials did not substantiate its efficacy [Chez et al., 2000; Coniglio et al., 2001; Dunn-Geier et al., 2000; Roberts et al., 2001; Sandler et al., 1999]. These trials included single- and repeated-dose protocols. It is challenging to perform clinical trials enrolling children with autism, but without well-designed, blinded studies, safe and effective therapies cannot be determined. Problems include standardization of diagnoses, heterogeneity of target problem behaviors, and lack of cooperation of subjects. Many
outcome measures are available, including global measures (Clinical Global Impression of Severity) and others targeted to specific symptoms. The National Institutes of Healthsponsored multicenter networks are planning and currently performing clinical trials (i.e., The Autism Research Units on Pediatric Psychopharmacology, The Studies to Advance Autism Research and Treatment Centers, and the Collaborative Programs of Excellence in Autism). Whenever feasible, parents should be encouraged to participate in clinical trials to make progress in validating new pharmacologic and behavioral therapies.
EDUCATIONAL AND BEHAVIORAL INTERVENTIONS The primary source of intervention for most children with autistic spectrum disorder is through the educational system. The Individual with Disabilities Education Act ensures a “free and appropriate” public education to “children” between the ages of 3 and 21 who have been diagnosed with learning disabilities. This act specifically covers autistic disorder, but whether the full range of autistic spectrum disorder is covered depends on the particular state’s definition of disabilities. The quality and extent of services that are
Hirtz, Wagner, and Filipek / Autistic Spectrum Disorders
provided vary from one community to another, even within a particular school district. The core deficits associated with autism affect all aspects of the individual’s life, necessitating a comprehensive approach to intervention [Lord and Bailey, 2002; Lord et al., in press; Wetherby et al., 1997]. Numerous comprehensive early intervention programs for children with autistic spectrum disorder have been developed and described [Dawson and Osterling, 1997; National Research Council, 2001; Rogers, 1998]. The National Research Council [2001] provides descriptions of 10 model programs considered representative of well-described, comprehensive treatment programs with at least some empiric support. None of these programs has been rigorously evaluated with regard to optimal time of initiation, mode of delivery, intensity, or duration. Given the great heterogeneity in the population with autistic spectrum disorders, intervention programs must be tailored to the needs of the individual. The National Research Council [2001] report describes the common elements of successful early intervention programs and makes several recommendations: • Intervention should begin early (as soon as an autistic spectrum disorder diagnosis is seriously considered). • Intervention should include active engagement in instructional programming for at least 25 hours per week, with full-year programming. • Intervention should include repeated, planned teaching opportunities that are one-to-one designs or delivered in a very small group, with individualized goals. • Intervention should include family support and parent training. • Intervention programs should have low student-toteacher ratios. • Program evaluation and assessment of the child’s progress should be ongoing. • Six kinds of intervention should have priority: communication, social skills, play skills, cognitive development, strategies to address problem behaviors, and functional academics. Methods based on applied behavior analysis for teaching skills and facilitating more appropriate and adaptive behaviors have been extensively tested for their effectiveness in children and adults with autism and other developmental disabilities [Dunlap and Fox, 2001; Lovaas, 1987; McEachin et al., 1993; Sheinkopf and Siegel, 1998; Smith et al., 2000]. Applied behavior analysis and comprehensive programs based on applied behavioral analysis are established on principles of behavior modification. By carefully analyzing the causes and consequences of a particular behavior, identifying an opposite, competing behavior (i.e., desired behavior) and consistently altering the consequences so that the desired behavior is rewarded, the instructor can teach new skills or transform inappropriate behaviors into more acceptable ones. This relatively simple principle has been developed into techniques that have been highly effective for teaching new skills, increasing the frequency of appropriate or adaptive behaviors, and decreasing the frequency of inappropriate or maladaptive behaviors. Behavioral techniques can be used to work on very specific social behaviors, such as making appropriate greetings and appropriate modes of expressing affection, sharing,
927
and playing interactively. Behaviors that have the potential to generalize to other settings should be taught. For instance, teaching a child to make eye contact with a speech therapist is of limited use unless the child also makes eye contact when conversing with parents, peers, and others. One way to increase generalization is to help parents reinforce and apply the behavioral techniques at home and in the community. For this reason, good behavioral programs always contain a parent-training component. When parents are taught how to apply behavioral techniques, with ongoing coaching, they can be effective in smoothing out interactions between the individual with autistic spectrum disorder and other family members. Parents are most likely to learn applied behavior analysis techniques when enrolling their children in a comprehensive treatment program. As these comprehensive treatment programs have evolved, there have been trends toward teaching parents to implement the programs, toward using the behaviormanagement techniques in settings that are more naturalistic and during typical activities, and toward developing goals based on the child’s unique developmental profile [Ingersoll et al., 2001]. There is also a trend, at least when applied to programs for children and adults with developmental disabilities, away from emphasizing the consequences of a behavior and toward an emphasis on understanding the triggers of a behavior, proactively providing cues or rehearsal of the appropriate behavior, making changes in the environment to avoid or minimize those triggers, and teaching more adaptive or appropriate responses when the triggers cannot be avoided. Some comprehensive treatment programs derive strategies from a developmental theoretical framework. For instance, the Denver Model [Rogers et al., 2000] emphasizes the need to establish interpersonal relationships as a foundation to achieving other developmental milestones. The Developmental Intervention Model [Greenspan and Wieder, 1997] is based on an assumption that social problems in autistic spectrum disorders are caused by abnormal or atypical processing of sensory information and difficulties with emotional regulation. The focus is on addressing sensory processing irregularities and establishment of emotional contact. Both programs emphasize improving parent-child relationships. Although most of these programs have not been extensively evaluated using rigorous scientific trials, there are theoretical reasons and some preliminary scientific evidence that they can be useful for many children with autistic spectrum disorders [National Research Council, 2001; Rogers, 1998]. Many well-established programs combine elements of behavioral and developmental orientations [Marcus et al., 2000; McGee et al., 2000]. Some have specifically evaluated the effectiveness of the parent-training components of their programs. Parent-training models that are promising based on evidence provided by their developers include the Learning Experiences Alternative Program for Preschoolers and Their Parents [Strain and Cordisco, 2000], the Denver Model [Rogers et al., 2000], the Individualized Support Program at the University of South Florida [Dunlap, 1999], the Pivotal Response Training Model [Koegel et al., 1999], and the Douglas Developmental Center Program [Harris et al., 2000]. Whatever the theoretical underpinning, well-established and effective programs always include an emphasis on parentchild relationships and overall family support [Dawson and Osterling, 1997]. There is evidence that parents can learn to use these methods and that doing so helps them feel better in
928
Neurobehavioral Disorders / 38
general and more satisfied and confident in their parenting role [Koegel et al., 1996; Ozonoff and Cathcart, 1998; Schreibman, 1997; Sofronoff and Farbotko, 2002]. There is much less evidence when considering intervention programs or treatment options for older children, adolescents, and adults with autistic spectrum disorder. There is growing recognition that although the needs of individuals with autism spectrum disorder change over time, there is need for lifelong support. In particular, transitions (e.g., to high school, to higher education or vocational training, to independent or assisted living) are critical periods during which supports already in place may be lost because of changes in eligibility or funding sources.
RESOURCES FOR FAMILIES An enormous amount of information is available to families on the Internet; they often need specific counseling regarding evaluation of treatments that are espoused without adequate scientific study. The American Academy of Pediatrics has a useful web site (http://www.aap.org/healthtopics/ autism.cfm). The National Institutes of Health web site (www.nih.gov) can be searched for current research, as can those of specific institutes, including the National Institute of Neurological Disorders and Stroke (www.ninds.nih.gov), National Institute of Child Health and Human Development (www.nichd.nih.gov), and the National Institute of Mental Health (www.nimh.nih.gov). The CDC’s National Center for Birth Defects and Developmental Disabilities has a web site (www.cdc.gov/ncbddd/dd/ddautism.htm) devoted to providing evidence-based information on autistic spectrum disorder and its treatment, including links to resources. The National Dissemination Center for Children with Disabilities (www.nichcy.org) has information on special education laws and on educational practices. Another effort, the First Signs program, is developing methods to inform physicians about the importance of early identification of autism, and it provides resources, including screening tools and referral guidelines. The First Signs web site (http://www.firstsigns.org) includes recommendations and information about obtaining autism screening instruments. Educational tools for families can be found on the Exploring Autism web site (http://www.exploringautism.com). An organization for autism research has a useful parent’s guide to understanding research on autism (www.researchautism.org). For practitioners, the AAN/CNS practice parameter for evaluation of children with autism and the detailed background paper can be found on the For OC Kids web site (http://www.forockids.org/en/forockids.php). A comprehensive review of the literature on treatment using applied behavior analysis and practical guidance for implementation is contained in Positive Behavioral Support: Including People with Difficult Behavior in the Community [Koegel et al., 1996]. DISCLAIMER The views expressed in this chapter are those of the authors and do not necessarily reflect the official position of the National Institute of Mental Health, the National Institute of Neurological Diseases and Stroke, the National Institutes of Health, or any other part of the U.S. Department of Health and Human Services.
REFERENCES Adrien JL, Perrot A, Sauvage D, et al. Early symptoms in autism from family home movies. Evaluation and comparison between 1st and 2nd year of life using I.B.S.E. scale. Acta Paedopsychiatr 1992;55:71. Allen DA, Rapin I. Autistic children are also dysphasic. In: Neruse H, Ornitz EM, eds. Neurobiology of infantile autism. Amsterdam: Elsevier Science Publishers, 1992. Allen DA. Autistic spectrum disorders: Clinical presentation in preschool children. J Child Neurol 1988;3:S48. Allen DA. Variability in the clinical presentation of autism: Issues of diagnosis and treatment in the preschool years. In: Amir N, Rapin I, Branski D, eds. Pediatric neurology: Behavior and cognition of the child with brain dysfunction. Basel: Karger, 1991. Aman MG, Langworthy KS. Pharmacotherapy for hyperactivity in children with autism and other pervasive developmental disorders. J Autism Dev Disord 2000;30:451. Amaral DG. The primate amygdala and the neurobiology of social behavior: Implications for understanding social anxiety. Biol Psychiatry 2002;51:11. American College of Medical Genetics. Policy statement. Fragile X syndrome: Diagnostic and carrier testing. Am J Med Genet 1994, 53:380. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 3rd ed. Washington, DC: American Psychiatric Association, 1980. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 3rd ed, revised. Washington, DC: American Psychiatric Association, 1987. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed. Washington, DC: American Psychiatric Association, 1994. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed. Text revision. Washington, DC: American Psychiatric Association, 2000. American Speech-Language-Hearing Association. Guidelines for the audiologic assessment of children from birth through 36 months of age. Committee on Infant Hearing, American Speech-Language-Hearing Association (ASHA). 1991;33(Suppl 5):37. Amir RE, Van den Veyver IB, Wan M, et al. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet 1999;23:185. Anderson LT, Campbell M, Adams P, et al. The effects of haloperidol on discrimination learning and behavioral symptoms in autistic children. J Autism Dev Disord 1989;19:227. Armstrong DD. Review of Rett syndrome. J Neuropathol Exp Neurol 1997;56:843. Asano E, Chugani DC, Muzik O, et al. Autism in tuberous sclerosis complex is related to both cortical and subcortical dysfunction. Neurology 2001;57:1269. Ashley-Koch A, Wolpert CM, Menold MM, et al. Genetic studies of autistic disorder and chromosome 7. Genomics 1999;61:227. Asperger H. “Autistic psychopathy” in childhood [Frith U, translator and annotator]. In: Frith U, ed. Autism and Asperger syndrome. New York: Cambridge University Press, 1991 [original work published 1944]. August GJ, Raz N, Papanicolaou AC, et al. Fenfluramine treatment in infantile autism,. Neurochemical, electrophysiological, and behavioral effects. J Nerv Ment Dis 1984;172:604. Auranen M, Vanhala R, Varilo T, et al. A genomewide screen for autism-spectrum disorders: Evidence for a major susceptibility locus on chromosome 3q25-27. Am J Hum Genet 2002;71:777. Aylward EH, Minshew NJ, Goldstein G, et al. MRI volumes of amygdala and hippocampus in non-mentally retarded autistic adolescents and adults. Neurology 1999;53:2145. Aylward EH, Minshew NJ, Field K, et al. Effects of age on brain volume and head circumference in autism. Neurology 2002;59:175. Bachevalier J, Merjanian PM. The contribution of medial temporal lobe structures in infantile autism: A neurobehavioral study in primates. Baltimore: Johns Hopkins University Press, 1994:146. Bachevalier J. Medial temporal lobe structures and autism: A review of clinical experimental findings. Neuropsychologia 1994;32:627. Badner J, Gershon E. Regional meta-analysis of published data supports linkage of autism with markers on chromosome 7. Mol Psychiatry 2002;7:56. Bailey A, LeCouteur A, Gottesman I, et al. Autism as strongly genetic disorder: Evidence from a British twin study. Psychol Med 1995;25:63.
Hirtz, Wagner, and Filipek / Autistic Spectrum Disorders Bailey A, Palferman S, Heavey L, et al. Autism: The phenotype in relatives. J Autism Dev Disord 1998;28:369. Bailey A, Phillips W, Rutter M. Autism: Towards an integration of clinical, genetic, neuropsychological, and neurobiological perspectives. J Child Psychol Psychiatry 1996;37:89. Baird G, Charman T, Baron-Cohen S, et al. A screening instrument for autism at 18 months of age: A 6-year follow-up study. J Am Acad Child Adolesc Psychiatry 2000;39:694. Baird G, Charman T, Cox A, et al. Screening and surveillance for autism and pervasive developmental disorders. Arch Dis Child 2001;84:468. Baron-Cohen S, Wheelwright S, Skinner R, et al. The autistic-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 2001;31:5. Baron-Cohen S. Mindblindness: An essay on autism and theory of mind. Cambridge, MA: MIT Press, 1995. Baron-Cohen S. The development of a theory of mind in autism: Deviance and delay? Psychiatr Clin North Am 1991;14:33. Bartlett CW, Flax JF, Logue MW, et al. Examination of potential overlap in autism and language Loci on chromosomes 2, 7, and 13 in two independent samples ascertained for specific language impairment. Hum Hered 2004;57:10. Bauman M, Kemper T. Neuroanatomic observations of the brain in autism. In: Bauman M, Kemper T, eds. The neurobiology of autism. Baltimore: Johns Hopkins University Press 1994. Bauman ML. Motor dysfunction in autism. In: Joseph AB, Young RR, eds. Movement disorders in neurology and psychiatry. Boston: Blackwell Scientific Publications, 1992. Bauman ML, Kemper TL. Is autism a progressive process? Neurology 1997;48 (Suppl):A285. Belsito KM, Law PA, Kirk KS, et al. Lamotrigine therapy for autistic disorder: A randomized, double-blind, placebo-controlled trial. J Autism Dev Disord 2001;31:175. Berthier ML. Corticocallosal anomalies in Asperger’s syndrome [Letter]. AJR Am J Roentgenol 1994;162:236. Berthier ML, Starkstein SE, Leiguarda R. Developmental cortical anomalies in Asperger’s syndrome: Neuroradiological findings in two patients. J Neuropsychiatry Clin Neurosci 1990;2:197. Bertrand J, Mars A, Boyle C, et al. Prevalence of autism in a United States population: The Brick Township, New Jersey, investigation. Pediatrics 2001;108:1155. Berument SK, Rutter M, Lord C, et al. Autism screening questionnaire: Diagnostic validity. Br J Psychiatry 1999;175:444. Betancur C, Corbex M, Spielewoy C, et al. Serotonin transporter gene polymorphisms and hyperserotonemia in autistic disorder. Mol Psychiatry 2002;7:67. Bettelheim B. The empty fortress; infantile autism and the birth of the self. New York: Free Press, 1967. Bishop DVM. Autism, Asperger’s syndrome and semantic-pragmatic disorder: Where are the boundaries? Br J Disord Commun 1989;24:107. Bjornsson HT, Fallin MD, Feinberg AP. An integrated epigenetic and genetic approach to common human disease. Trends Genet 2004;20:350. Black C, Kaye JA, Jick H. Relation of childhood gastrointestinal disorders to autism: Nested case-control study using data from the UK General Practice Research Database. BMJ 2002;325:419. Bolman WM, Richmond JA. A double-blind, placebo-controlled, crossover pilot trial of low dose dimethylglycine in patients with autistic disorder. J Autism Dev Disord 1999;29:191. Bolton P, MacDonald H, Pickles A, et al. A case-control family history study of autism. J Child Psychol Psychiatry 1994;35: 877. Bolton P, MacDonald H, Murhpy M, et al. Genetic findings and heterogeneity in autism. Psychiatr Genet 1991;2:S7A/2. Bonnet KA, Gao XK. Asperger syndrome in neurologic perspective. J Child Neurol 1996;11:483. Bradford Y, Haines J, Hutcheson H, et al. Incorporating language phenotypes strengthens evidence of linkage to autism. Am J Hum Genet 2001;105:539. Brasic JR, Barnett JY, Kaplan D, et al. Clomipramine ameliorates adventitious movements and compulsions in prepubertal boys with autistic disorder and severe mental retardation. Neurology 1994;44:1309. Briskman J, Happe F, Frith U. Exploring the cognitive phenotype of autism: Weak “central coherence” in parents and siblings of children with autism. II. Real-life skills and preferences. J Child Psychol Psychiatry 2001;42:309.
929
Buchsbaum MS, Hollander E, Haznedar MM, et al. Effect of fluoxetine on regional cerebral metabolism in autistic spectrum disorders: A pilot study. Int J Neuropsychopharmacol 2001;4:119. Buitelaar JK, van England H, De Kogel K, et al. The adrenocorticotrophic hormone (4-9) analog ORG 2766 benefits autistic children: Report on a second controlled clinical trial. J Am Acad Child Adolesc Psychiatry 1992;31:1149. Buitelaar JK, Willemsen-Swinkels SHN. Autism: Current theories regarding its pathogenesis and implications for rational pharmacotherapy. Paediatr Drugs 2000;2:67. Buxbaum JD, Silverman JM, Smith CJ, et al. Evidence for a susceptibility gene for autism on chromosome 2 and for genetic heterogeneity. Am J Hum Genet 2001;68:1514. Buxbaum JD, Silverman JM, Smith CJ, et al. Association between a GABRB3 polymorphism and autism. Mol Psychiatry 2002;7:311. California Department of Developmental Services. Autistic spectrum disorders. California Health and Human Services Agency, 2003. Campbell M, Anderson LT, Small AM, et al. Naltrexone in autistic children: Behavioral symptoms and attentional learning. J Am Acad Child Adolesc Psychiatry 1993;32:1283. Campbell M, Armenteros JL, Malone RP, et al. Neuroleptic-related dyskinesias in autistic children: A prospective, longitudinal study. J Am Acad Child Adolesc Psychiatry 1997;36:835. Carney RM, Wolpert CM, Ravan SA, et al. Identification of MeCP2 mutations in a series of females with autistic disorder. Pediatr Neurol 2003;28:205. Carper RA, Moses P, Tigue ZD, et al. Cerebral lobes in autism: Early hyperplasia and abnormal age effects. Neuroimage 2002;16:1038. Casanova MF, Buxhoeveden DP, Switala AE, et al. Minicolumnar pathology in autism. Neurology 2002;58:428. Centers for Disease Control and Prevention. Screening young children for lead poisoning: Guidance for state and local public health officials. Atlanta: Centers for Disease Control and Prevention, National Center for Environmental Health, November 1997. Chakrabarti S, Fombonne E. Pervasive developmental disorders in preschool children. JAMA 2001;285:3093. Charman T, Baron-Cohen S, Baird G, et al. Is 18 months too early for the chat? J Am Acad Child Adolesc Psychiatry 2002;41:235. Chen W, Landau S, Sham P, et al. No evidence for links between autism, MMR and measles virus. Psychol Med 2004;34:543. Chez MG, Buchanan CP, Bradley TB, et al. Secretin and autism: A two-part clinical investigation. J Autism Dev Disord 2000;30:87. Chudley AE, Gutierrez E, Jocelyn LJ, et al. Outcomes of genetic evaluation in children with pervasive developmental disorder. J Dev Behav Pediatr 1998;19:321. Chugani DC, Muzik O, Rothermel R, et al. Altered serotonin synthesis in the dentatothalamocortical pathway in autistic boys. Ann Neurol 1997;42:666. Chugani DC. Role of altered brain serotonin mechanisms in autism. Mol Psychiatry 2002;7:S16. Chugani HT, Da Silva E, Chugani DC. Infantile spasms: III. Prognostic implications of bitemporal hypometabolism on positron emission tomography. Ann Neurol 1996;39:643. Cohen DJ, Young JG, Lowe TL, et al. Thyroid hormone in autistic children. J Autism Dev Disord 1980;10:445. Coleman M, Blass JP. Autism and lactic acidosis. J Autism Dev Disord 1985;15:1. Collaborative Linkage Study of Autism (CLSA). An autosomal genomic screen for autism. Collaborative Linkage Study of Autism. Am J Med Genet 1999;88:609. Comi AM, Zimmerman AW, Frye VH, et al. Familial clustering of autoimmune disorders and evaluation of medical risk factors in autism. J Child Neurol 1999;14:388. Coniglio SJ, Lewis JD, Lang C, et al. A randomized, double-blind, placebo-controlled trial of single-dose intravenous secretin as treatment for children with autism. J Pediatr 2001;138:649. Connolly AM, Chez MG, Pestronk A, et al. Serum autoantibodies to brain in Landau-Kleffner variant, autism, and other neurologic disorders. J Pediatr 1999;134:607. Cook EH Jr, Rowlett R, Jaselskis C, et al. Fluoxetine treatment of children and adults with autistic disorder and mental retardation. J Acad Child Adosesc Psychiatry 1992;31:739. Cook EH, Leventhal BL. The serotonin system in autism. Curr Opin Pediatr 1996;8:348.
930
Neurobehavioral Disorders / 38
Cook EH Jr, Perry BD, Dawson G, et al. Receptor inhibition by immunoglobulins: Specific inhibition by autistic children, their relatives, and control subjects. J Autism Dev Disord 1993;23:67. Courchesne E, Carper R, Akshoomoff N. Evidence of brain overgrowth in the first year of life in autism. JAMA 2003;290:337. Courchesne E, Karns CM, Davis HR, et al. Unusual brain growth patterns in early life in patients with autistic disorder: An MRI study. Neurology 2001;57:245. Critchley HD, Daly EM, Bullmore ET, et al. The functional neuroanatomy of social behavior: Changes in cerebral blood flow when people with autistic disorder process facial expressions. Brain 2000;123:2203. Croen LA, Grether JK, Selvin S. Descriptive epidemiology of autism in a California population: Who is at risk? J Autism Dev Disord 2002;32:217. Croonenberghs J, Delmeire L, Verkerk R, et al. Peripheral markers of serotonergic and noradrenergic function in post-pubertal, Caucasian males with autistic disorder. Neuropsychopharmacology 2000;22:275. Curry CJ, Stevenson RE, Aughton D, et al. Evaluation of mental retardation: Recommendations of a Consensus Conference: American College of Medical Genetics. Am J Med Genet 1997;72:468. Dales L, Hammer SJ, Smith NJ. Time trends in autism and in MMR immunization coverage in California. JAMA 2001;285:1183. Davidovitch M, Patterson B, Gartside P. Head circumference measurements in children with autism. J Child Neurol 1996;11:389. Dawson G, Melzoff AN, Osterling J, et al. Children with autism fail to orient to naturally occurring social stimulti. J Autism Dev Disord 1998;28:479. Dawson G, Osterling J. Early intervention in autism. In: Guralnick MJ, ed. The effectiveness of early intervention. Baltimore: Brookes, 1997. Deb S, Prasad KB. The prevalence of autistic disorder among children with a learning disability. Br J Psychiatry 1994;165:395. DeFelice ML, Ruchelli ED, Markowitz JE, et al. Intestinal cytokines in children with pervasive developmental disorders. Am J Gastroenterol 2003;98:1777. DelGiudice-Asch G, Simon L, Schmeidler J, et al. Brief report: A pilot open clinical trial of intravenous immunoglobulin in children autism. J Autism Dev Disord 1999;29:157. DeLong GR, Ritch CR, Burch S. Fluoxetine response in children with autistic spectrum disorders: Correlation with familial major affective disorder and intellectual achievement. Dev Med Child Neurol 2002;44:652. Deuel RK. Autism: A cognitive development riddle. Pediatr Neurol 2002;26:349. D’Eufemia P, Celli M, Finocchiaro R, et al. Abnormal intestinal permeability in children with autism. Acta Paediatr 1996;85:1076. Devlin B, Bennett P, Cook EH Jr, et al. No evidence for linkage of liability to autism to HOXA1 in a sample from the CPEA Network. Am J Med Genet 2002;114:667. Didde R, Sigafoos J. A review of the nature and treatment of sleep disorders in individuals with developmental disabilities. Res Dev Disabil 2001;22:255. Dunlap G, Fox L. A demonstration of behavioral support for young children with autism. J Pos Behav Interv 1999;2:77. Dunlap G, Fox L. Early intervention and serious problem behaviors: A comprehensive approach. In: Koegel LK, Koegel RL, Dunlap G, eds. Positive behavioral support: Including people with difficult behavior in the community. Baltimore: Brookes, 2001. Dunn-Geier J, Ho HH, Auersperg E, et al. Effect of secretin on children with autism: A randomized controlled trial. Dev Med Child Neurol 2000;42:796. Dykens EM, Volkmar FR. Medical conditions associated with autism. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive developmental disorders, 2nd ed. New York: John Wiley & Sons, 1997. Eisenmajer R, Prior M, Leekam S, et al. Comparison of clinical symptoms in autism and Asperger’s disorder. J Am Acad Child Adolesc Psychiatry 1996;35:1523. Ekman G, Miranda-Linné F. Fenfluramine treatment of twenty children with autism. J Autism Dev Disord 1989;19:511. Evans-Jones LG, Rosenbloom L. Disintegrative psychosis in childhood. Dev Med Child Neurol 1978;20:462. Fatemi SH, Realmuto GM, Khan L, et al. Fluoxetine in treatment of adolescent patients with autism: A longitudinal open trial. J Autism Dev Disord 1998;28:303.
Feldman HM, Kolmen BK, Gonzaga AM. Naltrexone and communication skills in young children with autism. J Am Acad Child Adolesc Psychiatry 1999;38:587. Filiano JJ, Goldenthal MJ, Rhodes H, et al. Mitochondrial dysfunction in patients with hypotonia, epilepsy, autism and developmental delay: HEADD Syndrome. J Child Neurol 2002;17:435. Filipek PA. Quantitative magnetic resonance imaging in autism: The cerebellar vermis. Curr Opin Neurol 1995;8:134. Filipek PA. Medical aspects of autism. In: Volkmar FR, Klin A, Paul R, Cohen DJ, eds. Handbook of autism and pervasive developmental disorders, 3rd ed. New York: John Wiley & Sons, 2005. Filipek P, Accardo P, Ashwal S, et al. Practice parameter: Screening and diagnosis of autism. Neurology 2000;55:468. Filipek PA, Accardo PJ, Baronek G, et al. The screening and diagnosis of autistic spectrum disorders. J Autism Dev Disord 1999;29,437. Filipek PA, Juranek J, Nguyen MT, et al. Relative carnitine deficiency in autism. J Autism Dev Disord 2004;34:615. Filipek PA, Kennedy DN, Caviness VS Jr. Neuroimaging in child neuropsychology. In: Rapin I, Segalowitz S, eds. Handbook of neuropsychology, Vol. 6. Child neuropsychology. Amsterdam: Elsevier Science, 1992a. Filipek PA, Richelme C, Kennedy DN, et al. Morphometric analysis of the brain in developmental language disorders and autism. Ann Neurol 1992b;32:475. Findling RL, Maxwell K, Scotese-Wojtila L, et al. High-dose pyridoxine and magnesium administration in children with autistic disorder: An absence of salutary effects in a double-blind, placebo-controlled study. J Autism Dev Disord 1997;27:467. Finegan JA, Quarrington B. Pre-, peri-, and neonatal factors and infantile autism. J Child Psychol Psychiatry 1979;20:119. Fisch GS. Is autism associated with the fragile X syndrome? Am J Med Genet 1992;43:47. Folstein S, Rutter M. Infantile autism: A genetic study of 21 twin pairs. J Child Psychol Psychiatry 1977;18:297. Folstein SE, Rosen-Sheidley B. Genetics of autism: Complex aetiology for a heterogeneous disorder. Nat Rev Genet 2001;2:943. Folstein SE, Rutter ML. Autism: Familial aggregation and genetic implications. J Autism Dev Disord 1988;18:3. Folstein SE, Santangelo SL, Gilman SE, et al. Predictors of cognitive test patterns in autism families. J Child Psychol Psychiatry 1999;40:1117. Fombonne E. The epidemiology of autism: A review. Psychol Med 1999;29:769. Fombonne E. Is there an epidemic of autism? Pediatrics 2001;107:411. Fombonne E. Epidemiological trends in rates of autism. Mol Psychiatry 2002;7 (Suppl 2):S4. Fombonne E. Epidemiological surveys of autism and other pervasive developmental disorders: An update. J Autism Dev Disord 2003a;33:365. Fombonne E. The prevalence of autism. JAMA 2003b;289:87. Fombonne E, Chakrabarti S. No evidence for a new variant of measlesmumps-rubella–induced autism. Pediatrics 2001;108:E58. Fombonne E, Roge B, Claverie J, et al. Microcephaly and macrocephaly in autism. J Autism Dev Disord 1999;29:113. Friedman E. The “autistic syndrome” and phenylketonuria. Schizophrenia 1969;1:249. Gallagher L, Hawi Z, Kearney G, et al. No association between allelic variants of HOXA1/HOXB1 and autism. Am J Med Genet 2004;124:64. Gentile PS, Trentalange MJ, Zamichek W, et al. Brief report: Trace elements in the hair of autistic and control children. J Autism Dev Disord 1983;13: 205. Ghaziuddin M, Gerstein L. Pedantic speaking style differentiates Asperger syndrome from high-functioning autism. J Autism Dev Disord 1996;26:585. Gillberg C. The treatment of epilepsy in autism. J Autism Dev Disord 1991;21:61. Gillberg C, Gillberg IC. Infantile autism: A total population study of reduced optimality in the pre-, peri- and neonatal period. J Autism Dev Disord 1983;13:153. Goldman-Rakic P. The “psychic” neuron of the cerebral cortex. Ann NY Acad Sci 1999;868:13. Goodwin MS, Cowen MA, Goodwin TC. Malabsorption and cerebral dysfunction: A multivariate and comparative study of autistic children. J Autism Child Schizophr 1971;1:48. Gordon C, State R, Nelson J, et al. A double-blind comparison of clomipramine, desipramine, and placebo in the treatment of autistic disorder. Arch Gen Psychiatry 1993;50:441.
Hirtz, Wagner, and Filipek / Autistic Spectrum Disorders Gordon CT. Pharmacological treatment options for autism. Narrative. J Natl Alliance Autism Res 2003;Summer:12. Graf WD, Marin-Garcia J, Gao HG, et al. Autism associated with the mitochondrial DNA G8363A transfer RNA (Lys) mutation. J Child Neurol 2000;15:357. Greenspan SI, Wieder S. Developmental patterns and outcomes in infants and children with disorders in relating and communicating: A chart review of 200 cases of children with autistic spectrum disorders. J Dev Learn Disord 1997;1:87. Gutierrez GC, Smalley SL, Tanguay PE. Autism in tuberous sclerosis complex. J Autism Dev Disord 1998;28:97. Hagberg B, Aicardi J, Dias K, et al. A progressive syndrome of autism, dementia, ataxia, and loss of purposeful hand use in girls: Rett’s syndrome: Report of 35 cases. Ann Neurol 1983;14:471. Hagberg B. Rett’s syndrome: Prevalence and impact on progressive severe mental retardation in girls. Acta Paediatr Scand 1985;74:405. Handen BL, Johnson CR, Lubetsky M. Efficacy of methylphenidate among children with autism and symptoms of attention-deficit hyperactivity disorder. J Autism Dev Disord 2000;30:245. Happé F, Frith U. The neuropsychology of autism. Brain 1996;119:1377. Hardan AY, Minshew NJ, Harenski K, et al. Posterior fossa magnetic resonance imaging in autism. J Am Acad Child Adosesc Psychiatry 2001;40:666. Harnadek MC, Rourke BP. Principal identifying features of the syndrome of nonverbal learning disabilities in children. J Learn Disabil 1994;27:144. Harris SL, Handelman JS, Arnold MS, et al. The Douglass Developmental Disabilities Center: Two models of service delivery. In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000. Hashimoto T, Aihara R, Tayama M, et al. Reduced thyroid-stimulating hormone response to thyrotropin-releasing hormone in autistic boys. Dev Med Child Neurol 1991;33:313. Hashimoto T, Tayama M, Murakawa K, et al. Development of the brainstem and cerebellum in autistic patients. J Autism Dev Disord 1995;25:1. Hellings JA, Kelley LA, Gabrielli WF, et al. Sertraline response in adults with mental retardation and autistic disorder. J Clin Psychiatry 1996;57:333. Herbert MR, Ziegler DA, Makris N, et al. Localization of white matter volume increase in autism and developmental language disorder. Ann Neurol 2004;55:530. Hirsch E, Marescaux C, Maquet P, et al. Landau-Kleffner syndrome: A clinical and EEG study of five cases. Epilepsia 1990;31:756. Hollander E. Venlafaxine in children, adolescents, and young adults with autism spectrum disorders: An open retrospective clinical report. J Child Neurol 2000;15:132. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry 2001;62:530. Hollander E, King A, Delaney K, et al. Obsessive-compulsive behaviors in parents of multiplex autism families. Psychiatry Res 2003;117:11. Hollander E, Phillips A, Chaplin W, et al. A placebo controlled crossover trial of liquid fluoxetineon repetitive behaviors in childhood and adolescent autism. Neuropsychopharmaclogy 2005;30:582. Hong SE, Shugart YY, Huang DT, et al. Autosomal recessive lissencephaly with cerebellar hypoplasia is associated with human RELN mutations. Nat Genet 2000;26:93 Honomichl RD, Goodlin-Jones BL, Burnham M, et al. Sleep patterns of children with pervasive developmental disorders. J Autism Dev Disord 2002;32:553. Hornig M, Chian D, Lipkin WI. Neurotoxic effects of postnatal thimerosal are mouse strain dependent. Mol Psychiatry 2004;9:833. Howlin P, Moore A. Diagnosis in autism. A survey of over 1200 patients in the UK. Autism 1997;1:135. Hubl D, Bölte S, Feineis-Matthews S, et al. Functional imbalance of visual pathways indicates alternative face processing strategies in autism. Neurology 2003;61:1232. Hughes C, Russell J, Robbins T. Evidence for executive dysfunction in autism. Neuropsychologia 1994;40:477. Hultman CM, Sparèn P, Cnattingius S. Perinatal risk factors for infantile autism. Epidemiology 2002;13:417. IMGSAC. A full genome screen for autism with evidence for linkage to a region on chromosome 7q. International Molecular Genetic Study of Autism Consortium. Hum Mol Genet 1998;7:571.
931
IMGSAC. A genomewide screen for autism. Strong evidence for linkage to chromosomes 2q, 7q, and 16p. Am J Hum Genet 2001a;69:570. IMGSAC. Further characterization of the autism susceptibility locus AUTS1 on chromosome 7q. Hum Mol Genet 2001b;10:973. Ingersoll B, Schreibman L, Stahmer A. Differential treatment outcomes for children with autistic spectrum disorder based on level of peer social avoidance. J Autism Dev Disord 2001;31:343. Ingram JL, Peckham SM, Tisdale B, et al. Prenatal exposure of rats to valproic acid reproduces the cerebellar anomalies associated with autism. Neurotoxicol Teratol 2000a;22:319. Ingram JL, Stodgell CJ, Hyman SL, et al. Discovery of allelic variants of HOXA1 and HOXB1: Genetic susceptibility to autism spectrum disorders. Teratology 2000b;62:393. Insel TR, O’Brien DJ, Leckman JF. Oxytocin, vasopressin, and autism: Is there a connection? Biol Psychiatry 1999;45:145. Jamain S, Quach H, Quintana-Murci L, et al. Y chromosome haplogroups in autistic subjects. Mol Psychiatry 2002;7:217. Jamain S, Quach H, Betancur C, et al. Paris Autism Research International Sibpair Study. Mutations of the X-linked genes encoding neuroligins NLGN3 and NLGN4 are associated wit autism. Nat Genet 2003;34:27. Jaselskis CA, Cook EH, Fletcher KE, et al. Clonidine treatment of hyperactive and impulsive children with autistic disorder. J Clin Psychopharmacol 1992;12:322. Jensen VK, Larrieu JA, Mack KK. Differential diagnosis between attention-deficit/hyperactivity disorder and pervasive developmental disorder—not otherwise specified. Clin Pediatr 1997;36:555. Jiang YH, Bressler J, Beaudet AL. Epigenetics and human disease. Annu Rev Genomics Hum Genet 2004;5:479. Jolliffe T, Baron-Cohen S. Linguistic processing in high functioning adults with autism or Asperger’s syndrome. Is global coherence impaired? Psychol Med 2000;30:1169. Juul-Dam N, Townsend J, Courchesne E. Prenatal, perinatal, and neonatal factors in autism, pervasive developmental disorder-not otherwise specified, and the general population. Pediatrics 2001;107:1. Kadesjö B, Gillberg C, Hagberg B. Brief report: Autism and Asperger syndrome in seven-year-old children: A total population study. J Autism Dev Disord 1999;29:327. Kandt RS. Tuberous sclerosis complex and neurofibromatosis type 1: The two most common neurocutaneous diseases. Neurol Clin 2003;21:983. Kanner L. Autistic disturbances of affective contact. Nervous Child 1943;2:217. Kanwisher N, McDermott J, Chun MM. The fusiform face area: A module in human extra-striate cortex specialized for face perception. J Neurosci 1997;17:4302. Kawashima H, Mori T, Kashiwagi Y, et al. Detection and sequencing of measles virus from peripheral mononuclear cells from patients with inflammatory bowel disease and autism. Dig Dis Sci 2000;45:723. Kaye JA, del Mar Melero-Montes M, Jick H. Mumps, measles, and rubella vaccine and the incidence of autism recorded by general practitioners: A time trend analysis. BMJ 2001;322:460. Kemper TL, Bauman M. Neuropathology of infantile autism. J Neuropathol Exp Neurol 1998;57:645. Kielinen M, Linna SL, Moilanen I. Autism in Northern Finland. Eur Child Adolesc Psychiatry 2000;9:162. Kim SJ, Cox N, Courchesne R, et al. Transmission disequilibrium mapping at the serotonin transporter gene (SLC6A4) region in autistic disorder. Mol Psychiatry 2002;7:278. Klauck SM, Poustka F, Benner A, et al. Serotonin transporter (5-HTT) gene variants associated with autism? Hum Mol Genet 1997;6:2233. Klein KC, Diehl EB. Relationship between MMR vaccine and autism. Ann Pharmacother 2004;38:1297. Kleiman MD, Neff S, Rosman NP. The brain in infantile autism: Are posterior fossa structures abnormal. Neurology 1992;42:753. Kleinman J, Marciano P, Ault R. Advanced theory of mind in high-functioning adults with autism. J Autism Dev Disord 2001;31:29. Klin A, Sparrow SS, de Bildt A, et al. A normed study of face recognition in autism and related disorders. J Autism Dev Disord 1999;29:499. Klin A, Volkmar FR, Sparrow SS, et al. Validity and neuropsychological characterization of Asperger syndrome: Convergence with nonverbal learning disabilities syndrome. J Child Psychol Psychiatry 1995;36:1127. Klin A. Young autistic children’s listening preferences in regard to speech: A possible characterization of the symptom of social withdrawal. J Autism Dev Disord 1991;21:29.
932
Neurobehavioral Disorders / 38
Koegel LK, Koegel RL, Harrower JK, et al. Pivotal response intervention. I. Overview of approach. J Assoc Sev Hand 1999;24:174. Koegel LK, Koegel RL, Kellegrew D, et al. Parent education for prevention and reduction of severe problem behaviors. In: Koegel LK, Koegel RL, Dunlap G, eds. Positive behavioral support: Including people with difficult behavior in the community. Baltimore: Brookes, 1996. Kolmen BK, Feldman HM, Handen BL, et al. Naltrexone in young children: Replication study and learning measures. J Am Acad Child Adolesc Psychiatry 1997;36:1570. Korvatska E, Van de Water J, Anders TF, et al. Genetic and immunologic considerations in autism. Neurobiol Dis 2002;9:107. Kozinetz CA, Skender ML, MacNaughton N, et al. Epidemiology of Rett syndrome: A population based registry. Pediatrics 1993;91:445. Kuddo T, Nelson KB. How common are gastrointestinal disorders in children with autism? Curr Opin Pediatr 2003;15:339. Kuperman S, Beeghly JHL, Burns TL, et al. Association of serotonin concentration to behavior and IQ in autistic children. J Autism Dev Disord 1987;17:133. Kurita H. A comparative study of Asperger syndrome with highfunctioning atypical autism. Psychiatr Clin Neurosci 1997;51:67. Lainhart JE. Increased rate of head growth during infancy in autism. JAMA 2003;290:393. Lainhart JE, Piven J, Wzorek M, et al. Macrocephaly in children and adults with autism. J Am Acad Child Adolesc Psychiatry 1997;36:282. Lainhart JE, Ozonoff S, Coon H, et al. Autism, regression, and the broader autism phenotype. Am J Med Genet 2002;113:231. LaPerchia P. Behavioral disorders, learning disabilities and megavitamin therapy. Adolescence 1987;22:729. Laszlo A, Horvath E, Eck E, et al. Serum serotonin, lactate and pyruvate levels in infantile autistic children [Letter]. Clin Chim Acta 1994;229:205. Laumonnier F, Bonnet-Brilhault F, Gomot M, et al. X-linked mental retardation and autism are associated with a mutation in the NLGN4 gene, a member of the Neuroligin family. Am J Hum Genet 2004;74:552. Leboyer M, Philippe A, Bouvard M, et al. Whole blood serotonin and plasma beta-endorphin in autistic probands and their first-degree relatives. Biol Psychiatry 1999;45:158. LeCouteur A, Lord C, Rutter M. The Autism Diagnostic Interview–Revised (ADI-R). Los Angeles: Western Psychological Services, 2003. LeCouteur A, Trygstad O, Evered C, et al. Infantile autism and urinary excretion of peptides and protein-associated peptide complexes. J Autism Dev Disord 1988;18:181. Lerman-Sagie T, Leshinsky-Silver E, Watemberg N, et al. Should autistic children be evaluated for mitochondrial disorders? J Child Neurol 2004;19:379. Leslie AM. Pretense and representation: The origins of “theory of mind.” Psychol Rev 1987;94:412. Levy SE, Mandell DS, Merhar S, et al. Use of complementary and alternative medicine among children recently diagnosed with autistic spectrum disorder. J Dev Behav Pediatr 2003;24:418. Li J, Tabor HK, Nguyen L, et al. Lack of association between HoxA1 and HoxB1 gene variants and autism in 110 multiplex families. Am J Med Genet 2002;114:24. Lightdale JR, Siegel B, Heyman MB. Gastrointestinal symptoms in autistic children. Clin Perspect Gastroenterol 2001;1:56. Lijam N, Paylor R, McDonald MP, et al. Social interaction and sensorimotor gating abnormalities in mice lacking Dvl1. Cell 1997;90:895. Liu J, Nyholt DR, Magnussen P, et al. A genomewide screen for autism susceptibility loci. Am J Hum Genet 2001;69:327. Locascio JJ, Malone RP, Small AM, et al. Factors related to haloperidol response and dyskinesias in autistic children. Psychopharmacol Bull 1991;27:119. Loening-Baucke V. Constipation in children. N Engl J Med 1998;339:1155. Lord C. Follow-up of two-year-olds referred for possible autism. J Child Psychol Psychiatry 1995;36:1365. Lord C, Bailey A. Autism spectrum disorders. In: Rutter M, Taylor E, eds. Child and adolescent psychiatry, 4th ed. Oxford: Blackwell Publications, 2002. Lord C, Cook EH, Leventhal BL, et al. Autism spectrum disorders. Neuron 2000a;29:355. Lord C, Mulloy C, Wendelboe M, et al. Pre- and perinatal factors in high-functioning females and males with autism. J Autism Dev Disord 1991;21:197.
Lord C, Pickles A, McLennan J, et al. Diagnosing autism: Analyses of data from the Autism Diagnostic Interview. J Autism Dev Disord 1997;27:501. Lord C, Risi S, Lambrecht L, et al. The Autism Diagnostic Observation Schedule–Generic (ADOS-G): A standard measure of social and communication deficits associated with the spectrum of autism. J Autism Dev Disord 2000b;30:205. Lord C, Wagner A, Rogers S, et al. Challenges in evaluating psychosocial interventions for autistic spectrum disorders. J Autism Dev Disord. In press. Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol 1987;55:3. Lowe TL, Tanaka K, Seashore MR, et al. Detection of phenylketonuria in autistic and psychotic children. JAMA 1980;243:126. Lucarelli S, Frediani T, Zingoni AM, et al. Food allergy and infantile autism. Panminerva Medica 1995;37:137. Machado CJ, Bachevalier J. Non-human primate models of childhood psychopathology: The promise and the limitations. J Child Psychol Psychiatry 2003;44:64. Madsen KM, Lauritsen MB, Pedersen CB, et al. Thimerosal and the occurrence of autism: Negative ecological evidence from Danish population-based data. Pediatrics 2003;112:604. Maestrini E, Lai C, Marlow A, et al. The International Molecular Genetic Study of Autism (IMGSA) Consortium. Serotonin transporter (5-HTT) and g-aminobutyric acid receptor subunit b3 (GABRB3) gene polymorphisms are not associated with autism in the IMGSA families. Am J Med Genet 1999;88:492. Magnússon P, Saemundsen E. Prevalence of autism in Iceland. J Autism Dev Disord 2001;31:153. Malone RP, Cater J, Sheikh RM, et al. Olanzapine verus haloperidol in children with autistic disorder: An open pilot study. J Am Acad Child Adolesc Psychiatry 2001;40:887. Mandell DS, Listerud J, Levy SE, et al. Race differences in the age at diagnosis among Medicaid-eligible children with autism. J Am Acad Child Adolesc Psychiatry 2002;41:1447. Mantovani JF. Autistic regression and Landau-Kleffner syndrome: Progress or confusion? Dev Med Child Neurol 2000;42:349. Marazziti D, Muratori F, Cesari A, et al. Increased density of the platelet serotonin transporter in autism. Pharmacopsychiatry 2000;33:165. Marcus LE, Schopler E, Lord C. TEACCH services for preschool children. In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000. Mari M, Castiello U, Marks D, et al. The reach-to-grasp movement in children with autism spectrum disorder. Philos Trans R Soc Lond B Biol Sci 2003;358:393. Mason-Brothers A, Ritvo ER, Pingree C, et al. The UCLA–University of Utah epidemiologic survey of autism: Prenatal, perinatal, and postnatal factors. Pediatrics 1990;86:514. McBride PA, Anderson GM, Hertzig ME, et al. Effects of diagnosis, race, and puberty on platelet serotonin levels in autism and mental retardation. J Am Acad Child Adolesc Psychiatry 1998;37:767. McCormick MC. The autism “epidemic”: Impressions from the perspective of immunization safety review. Ambul Pediatr 2003;3:119. McCracken JT, McGough J, Shah B, et al. Research Units on Pediatric Psychopharmacology Autism Network. N Eng J Med 2002;347:314. McDougle CJ, Holmes JP, Bronson MR, et al. Risperidone treatment of children and adolescents with pervasive developmental disorders: A prospective open-label study. J Am Acad Child Adolesc Psychiatry 1997;36:685. McDougle CJ, Holmes JP, Carlson DC, et al. A double-blind, placebo-controlled study of risperidone in adults with autistic disorder and other pervasive developmental disorders. Arch Gen Psychiatry 1998;55:633. McDougle CJ, Naylor ST, Cohen DJ, et al. A double-blind, placebocontrolled study of fluvoxamine in adults with autistic disorder. Arch Gen Psychiatry 1996;53:1001. McDougle CJ, Scahill L, McCracken JT, et al. Research units on pediatric psychopharmacology (RUPP) autism network. Psychopharmacology 2000;9:201. McEachin JJ, Smith T, Lovaas OI. Long-term outcome for children with autism who received early intensive behavioral treatment. Am J Ment Retard 1993;97:359. McGee GG, Morrier MJ, Daly T. The Walden preschool. In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000.
Hirtz, Wagner, and Filipek / Autistic Spectrum Disorders Mehta UC, Patel I, Castello FV. EEG sedation for children with autism. J Dev Behav Pediatr 2004;25:102. Michelson AM. Selenium glutathione peroxidase: Some aspects in man. J Environ Pathol Toxicol Oncol 1998;17:233. Miladi N, Larnaout A, Kaabachi N, et al. Phenylketonuria: An underlying etiology of autistic syndrome. A case report. J Child Neurol 1992;7:22. Miles JH, Hadden LL, Takahashi TN, et al. Head circumference is an independent clinical finding associated with autism. Am J Med Genet 2000;95:339. Miles JH, Hillman RE. Value of a clinical morphology examination in autism. Am J Med Genet 2000;91:245. Minshew NJ, Goldstein G, Siegel DJ. Neuropsychologic functioning in autism: Profile of a complex information processing disorder. J Int Neuropsychol Soc 1997;3:303. Minshew NJ, Luna B, Sweeney JA. Oculomotor evidence for neocortical systems but not cerebellar dysfunction in autism. Neurology 1999;52:917. Moles A, Kieffer BL, D’Amato FR. Deficit in attachment behavior in mice lacking the u-opioid receptor gene. Science 2004;304:1983. Molloy CA, Manning-Courtney P. Prevalence of chronic gastrointestinal symptoms in children with autism and autistic spectrum disorders. Autism 2003;7:165. Moore ML, Eichner SF, Jones JR. Treating functional impairment of autism with selective serotonin-reuptake inhibitors. Ann Pharmacother 2004;38:1515. Moore V, Goodson S. How well does early diagnosis of autism stand the test of time? Follow-up study of children assessed for autism at age 2 and development of an early diagnostic service. Autism 2003;7:47. Moretti P, Bouwknecht JA, Teague R, et al. Abnormalities of social interactions and home cage behavior ina mouse model of Rett syndrome. Hum Mol Genet 2005;14:205. Mouridsen SE, Rich B, Isagu T. The natural history of somatic morbidity in disintegrative psychosis and infantile autism: A validation study, Brain Dev 1999;21:447. Muhle R, Trentacoste SV, Rapin I. The genetics of autism. Pediatrics 2004;113:e472. Mundy P. The neural basis of social impairments in autism: The role of the dorsal medial-frontal cortex and anterior cingulated system. J Child Psychol Psychiatry 2003;44:793. Mundy P, Neal AR. Neural plasticity, joint attention, and a transactional social-orienting model of autism. In: Glidden LM, ed. International review of research in mental retardation: Autism. San Diego, CA: Academy Press 2001;23:139. Murch SH, Anthony A, Casson DH, et al. Retraction of an interpretation. Lancet 2004;363:750. Naidu S. Rett syndrome: A disorder affecting early brain growth. Ann Neurol 1997;42:3. Naidu S. Rett syndrome: From discovery to current interest. J Child Neurol 2003;18:661. Namerow LB, Thomas P, Bostic JQ, et al. Use of citalopram in pervasive developmental disorders. J Dev Behav Pediatr 2003;24:104. National Research Council. Educating children with autism. Washington, DC: National Academy Press, 2001. Nelson K, Bauman M. Thimerosal and autism? Pediatrics 2003;111:674. Neul JL, Zoghbi HY. Rett Syndrome: A prototypical neurodevelopmental disorder. Neuroscientist 2004;10:118. Nicholson R, Awad G, Solman L. An open trial of risperidone in young autistic children. J Am Acad Adolesc Psychiatry 1998;37:372. Nicolson R, Szatmari P. Genetic and neurodevelopmental influences in autistic disorder. Can J Psychiatry 2003;48:526. Nurmi EL, Amin T, Olson LM, et al. Dense linkage disequilibrium mapping in the 15q11-q13 maternal expression domain yields evidence for association in autism. Mol Psychiatry 2003;8:624. Olsson I, Steffenburg S, Gillberg C. Epilepsy in autism and autistic-like conditions: A population-based study. Arch Neurol 1988;45:666. Opitz JM, Gilbert-Barness E, Ackerman J, et al. Cholesterol and development: The RSH (“Smith-Lemli-Opitz”) syndrome and related conditions. Pediatr Pathol Mol Med 2002;21:153. Ornitz EM. Neurophysiology of infantile autism. J Am Acad Child Psychiatry 1985;24:251. Osterling J, Dawson G. Early recognition of children with autism: A study of first birthday home videotapes. J Autism Dev Disord 1994;24:247. Ozonoff S, Cathcart K. Effectiveness of a home program intervention for young children with autism. J Autism Dev Disord 1998;28:25.
933
Ozonoff S. Components of executive function deficits in autism and other disorders. In: Russel J, ed. Autism as an executive disorder. Oxford, UK: Oxford University Press, 1997. Patja A, Davidkin I, Kurki T, et al. Serious adverse events after measlesmumps-rubella vaccination during a fourteen-year prospective followup. Pediatr Infect Dis J 2000;19:1127. Patzold LM, Richdale AL, Tonge BJ. An investigation into sleep characteristics of children with autism and Asperger’s disorder. J Paediatr Child Health 1998;34:528. Pavone L, Fiumara A, Bottaro G, et al. Autism and celiac disease: Failure to validate the hypothesis that a link might exist. Biol Psychiatry 1997, 42:72. Pedersen OS, Liu Y, Reichelt KL. Serotonin uptake stimulating peptide found in plasma of normal individuals and in some autistic urines. J Peptide Res 1999;53:641. Peltola H, Patja A, Leinikki P, et al. No evidence for measles, mumps, and rubella vaccine-associated inflammatory bowel disease or autism in a 14-year prospective study [Letter]. Lancet 1998;351:1327. Pennington BF, Ozonoff S. Executive functions and developmental psychopathology. J Child Psychol Psychiatry 1996;37:51. Percy A, Gillberg C, Hagberg B, et al. Rett syndrome and the autistic disorders. Neurol Clin 1990;8:659. Perry R, Pataki C, Munoz-Silva DM, et al. Risperidone in children and adolescents with pervasive developmental disorder: Pilot trial and follow-up. J Child Adolesc Psychopharmacol 1997;7:167. Persico AM, Militerni R, Bravaccio C, et al. Lack of association between serotonin transporter gene promoter variants and autistic disorder in two ethnically distinct samples. Am J Med Genet 2000;96:123. Peters SU, Beaudet AL, Madduri N, et al. Autism in Angleman syndrome: Implications for autism research. Clin Genet 2004;66:530. Pfeiffer SI. Efficacy of vitamin B6 and magnesium in the treatment of autism: A methodology review and summary of outcomes. J Autism Dev Disord 1995;25:481. Philippe A, Martinez M, Guilloud-Bataille M, et al. Genome-wide scan for autism susceptibility genes. Paris Autism Research International Sibpair Study. Hum Mol Genet 1999;8:805. Pickett J. Current investigations in autism brain tissue research. J Autism Dev Disord 2001;31:521. Pickles A, Starr E, Kazak S, et al. Variable expression of the autism broader phenotype: Findings from extended pedigrees. J Child Psychol Psychiatry 2000;41:491. Pierce K, Muller RA, Ambrose J, et al. Face processing occurs outside fusiform “face area” in autism: Evidence from functional MRI. Brain 2001;124:2059. Piven J, Chase GA, Landa R, et al. Psychiatric disorders in the parents of autistic individuals. J Am Acad Child Adolesc Psychiatry 1991a;30:471. Piven J, Tsai G, Nehme E, et al. Platelet serotonin, a possible marker for familial autism. J Autism Dev Disord 1991b;21:51. Piven J, Berthier ML, Starkstein SE, et al. Magnetic resonance imaging evidence for a defect of cerebral cortical development in autism. Am J Psychiatry 1990;147:734. Piven J, Palmer P. Psychiatric disorder and the broad autism phenotype: Evidence from a family study of multiple-incidence autism families. Am J Psychiatry 1999;156:557. Piven J, Simon J, Chase G, et al. The etiology of autism: Pre-, peri- and neonatal factors. J Am Acad Child Adolesc Psychiatry 1993;32:1256. Piven J, Arndt S, Bailey J, et al. An MRI study of brain size in autism. Am J Psychiatry 1995;152:1145. Plesner AM, Hansen FJ, Taudorf K, et al. Gait disturbance interpreted as cerebellar ataxia after MMER vaccination at 15 months of age: A follow-up study. Acta Paediatr 2000;89:58. Pletnikov MV, Rubin SA, Moran TH, et al. Exploring the cerebellum with a new tool: Neonatal Borna disease virus (BDV) infection of the rat’s brain. Cerebullum 2003;2:62. Plioplys AV. Intravenous immunoglobulin treatment of children with autism. J Child Neurol 1998;13:79. Pons R, Andreu AL, Checcarelli N, et al. Mitochondrial DNA abnormalities and autistic spectrum disorders. J Pediatr 2004;144:81. Porter B, Goldstein E, Galil A, et al. Diagnosing the “strange” child. Child Care Health Dev 1992;18:57. Prior M. Is there an increase in the prevalence of autism spectrum disorders? J Paediatr Child Health 2003;39:81. Purcell AE, Jeon OH, Zimmerman AW, et al. Postmortem brain abnormalities of the glutamate neurotransmitter system in autism. Neurology 2001;57:1618.
934
Neurobehavioral Disorders / 38
Quintana H, Birmaher B, Stedge D, et al. Use of methylphenidate in the treatment of children with autistic disorder. J Autism Dev Disord 1995;25:283. Rabionet R, Jaworski JM, Ashley-Koch A, et al. Analysis of the autism chromosome 2 linkage region: GAD1 and other candidate genes. Neurosci Lett 2004;372:209. Ramoz N, Reichert JG, Smith CJ, et al. Linkage and association of the mitochondrial aspartate/glutamate carrier SLC25A12 gene with autism. Am J Psychiatry 2004;161:662. Rapin I, Allen DA. Syndromes in developmental dysphasia and adult aphasia. In: Plum F, ed. Language, communication and the brain. New York: Raven Press, 1988. Rapin I. Autism. N Engl J Med 1997;337:97. Rapin I. Preschool children with inadequate communication: Developmental language disorder, autism, low IQ. London: MacKeith Press, 1996a. Rapin, I. Neurological examination. In: Rapin I, ed. Preschool children with inadequate communication: Developmental language disorder, autism, low IQ. London: MacKeith Press, 1996b. Rett A. On an until now unknown disease of a congenital metabolic disorder. Krankenschwester 1966;19:121. Riikonen R, Amnell G. Psychiatric disorders in children with earlier infantile spasms. Dev Med Child Neurol 1981;23:747. Rimland B. Dimethylglycine (DMG), a nontoxic metabolite, and autism. Autism Res Rev Int 1990;4:3. Risch N, Spiker D, Lotspeich L, et al. A genomic screen of autism: Evidence for a multilocus etiology. Am J Hum Genet 1999;65:493. Ritvo E, Mason-Brothers A, Freeman B, et al. The UCLA–University of Utah epidemiologic survey of autism: The etiologic role of rare diseases. Am J Psychiatry 1990;147:1614. Ritvo ER, Freeman BJ. National society for autistic children definition of the syndrome of autism. J Autism Child Schizophr 1978;8:162. Ritvo ER, Freeman BJ, Pingree C, et al. The UCLA–University of Utah epidemiologic survey of autism: Prevalence. Am J Psychiatry 1989;146:194. Roberts W, Weaver L, Brian J, et al. Repeated doses of porcine secretin in treatment of autism: A randomized, placebo-controlled trial. Pediatrics 2001;107:E71. Robins D. The Modified Checklist for Autism in Toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. J Autism Dev Disord 2001;31:131. Rodier PM, Bryson SE, Welch JP. Minor physical anomalies and physical measurements in autism: Data from Nova Scotia. Teratology 1997;55:319. Rodier PM, Ingram JL, Tisdale B, et al. Embryological origin for autism: Developmental anomalies of the cranial nerve motor nuclei. J Comp Neurol 1996;37:247. Rodier PM. Converging evidence for brain stem injury in autism. Dev Psychopathol 2002;14:537. Rogers S. An examination of the imitation deficits in autism. In: Nadel J, Butterworth G, eds. Imitation in infancy: Cambridge studies in cognitive perceptual development. New York: Cambridge University Press, 1999. Rogers SJ. Empirically supported comprehensive treatments for young children with autism. J Clin Child Psychol 1998;27:168. Rogers SJ, Hall T, Osaki D, et al. The Denver model: A comprehensive, integrated educational approach to young children with autism and their families. In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000. Rogers SJ, Wehner DE, Hagerman R. The behavioral phenotype in fragile X: Symptoms of autism in very young children with fragile X syndrome, idiopathic autism, and other developmental disorders. J Dev Behav Pediatr 2001;22:409. Rosenhall U, Nordin V, Sandstrom M, et al. Autism and hearing loss. J Autism Dev Disord 1999, 29:349. Rourke B. Nonverbal learning disabilities: The syndrome and the model. New York: Guilford, 1989. Rugino TA, Samsock TC. Levetiracetam in autistic children: An open-label study. J Dev Behav Pediatr 2002;23:225. Rutter M, Bailey A, Bolton P, et al. Autism: Syndrome of definition and possible genetic mechanisms. In: Plomin R, McLearn GE, eds. Nature, nurture and psychology. Washington, DC: American Psychological Association Press, 1993. Rutter M, Bailey A, Bolton P, et al. Autism and known medical conditions: Myth and substance. J Child Psychol Psychiatry 1994;35:311.
Rutter M, Bailey A, Lord C, et al. Social Communication Questionnaire. Los Angeles: Western Psychological Services, 2003. Rutter M, Bailey A, Simonoff E, et al. Genetic influences and autism. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive developmental disorders, 2nd ed. New York: John Wiley & Sons, 1997. Rutter M, Hersov R. Child psychiatry: Modern approaches. Oxford: Blackwell, 1977. Sanchez LE, Adams PB, Uysal S, et al. A comparison of live and videotape ratings: Clomipramine and haloperidol in autism. Psychopharmacol Bull 1995;31:371. Sanchez LE, Campbell M, Small AM, et al. A pilot study of clomipramine in young autistic children. J Am Acad Child Adolesc Psychiatry 1996;35:537. Sandler AD, Sutton KA, DeWeese J, et al. Lack of benefit of a single dose of synthetic human secretin in the treatment of autism and pervasive developmental disorder. N Engl J Med 1999;341:1801. Scambler D, Rogers S, Wehner E. Can the Checklist for Autism in Toddlers differentiate young children with autism from those with developmental delays? J Am Acad Child Adolesc Psychiatr 2001;40:1457. Schain RJ, Freedman DX. Studies on 5-hydroxyindole metabolism in autistic and other mentally retarded children. J Pediatr 1961;58:315. Scheuffgen K, Happe F, Anderson M, et al. High “intelligence,” low “IQ”? Speed of processing and measured IQ in children with autism. Dev Psychopathol 2000;12:83. Schopler E, Reichler R, Renner B. The Childhood Autism Rating Scale (CARS). New York: Irvington, 1986. Schopler E, Reichler RJ, DeVellis RF, et al. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000. Schopler E. Are autism and Asperger syndrome (AS) different labels or different disabilities? J Autism Dev Disord 1996;26:109. Schreck KA, Mulick JA. Parental report of sleep problems in children with autism. J Autism Dev Disord 2000;30:127. Schreibman L. Theoretical perspectives on behavioral intervention for individuals with autism. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive developmental disorders, 2nd ed. New York: Wiley & Sons, 1997. Schultz RT, Gauthier I, Klin A, et al. Abnormal ventral temporal cortical activity during face discrimination among individuals with autism and Asperger syndrome. Arch Gen Psychiatry 2000;57:331. Scott S. Mental retardation. In: Rutter M, Taylor E, Hersov L, eds. Child and adolescent psychiatry: Modern approaches, 3rd ed. Oxford: Blackwell Scientific Publications, 1994. Shannon M, Graef JW. Lead intoxication in children with pervasive developmental disorders. J Toxicol Clin Toxicol 1997;34:177. Shao Y, Wolpert CM, Raiford KL, et al. Genomic screen and follow-up analysis for autistic disorder. Am J Hum Gen 2002;114:99. Shearer TR, Larson K, Neuschwander J, et al. Minerals in the hair and nutrient intake of autistic children. J Autism Dev Disord 1982;12:25. Sheinkopf SJ, Siegel B. Home based behavioral treatment of young autistic children. J Autism Dev Disord 1998;28:15. Siegel B. The Pervasive Developmental Disorders Screening Test, Version II. Los Angeles: Western Psychological Services, 2004. Singh VK, Warren R, Averett R, et al. Circulating autoantibodies to neuronal and glial filament proteins in autism. Pediatr Neurol 1997;17:88. Skjeldal OH, Sponheim E, Ganes T, et al. Childhood autism: The need for physical investigations. Brain Dev 1998;20:227. Smalley SL. Autism and tuberous sclerosis. J Autism Dev Disord 1998;28:401. Smith T, Groen AD, Wynn JW. A randomized trial of intensive early intervention for children with pervasive developmental disorder. Am J Ment Retard 2000;5:269. Sofronoff K, Farbotko M. The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger syndrome. Autism 2002;6:271. Sparks BF, Friedman SD, Shaw DW, et al. Brain structural abnormalities in young children with autism spectrum disorder. Neurology 2002;59:184. Spence S. The genetics of autism. Semin Pediatr Neurol 2004;11:96. Steffenburg S, Gillberg C, Hellgren L, et al. A twin study of autism in Denmark, Finland, Iceland, Norway and Sweden. J Child Psychol Psychiatry 1989;30:405. Steffenburg S, Gillberg CL, Steffenburg U, et al. Autism in Angelman syndrome: A population-based study. Pediatr Neurol 1996;14:131.
Hirtz, Wagner, and Filipek / Autistic Spectrum Disorders Steffenburg S. Neuropsychiatric assessment of children with autism: A population-based study. Dev Med Child Neurol 1991;33:495. Steffenburg U, Hagberg G, Hagberg B. Epilepsy in a representative series of Rett syndrome. Acta Paediatrica 2001;90:34. Stehr-Green P, Tull P, Stellfeld M, et al. Autism and thimerosal-containing vaccines: Lack of consistent evidence for an association. Am J Prev Med 2003;25:101. Steingard RJ, Zimnitzky B, DeMaso DR, et al. Sertraline treatment of transition-associated anxiety and agitation in children with autistic disorder. J Child Adolesc Psychopharmacol 1997;7:9. Stone WL, Coonrod EE, Ousley OY. Screening tool for autism in two-year-olds (STAT): Development and preliminary data. J Autism Dev Disord 2000;30:607. Stone WL, Coonrod EE, Turner LM, et al. Psychometric properties of the STAT for early autism screening. J Autism Dev Disord 2004;34:691. Strain PS, Cordisco L. LEAP preschool. In: Handelman JS, Harris SL, eds. Preschool education programs for children with autism, 2nd ed. Austin, TX: Pro-Ed, 2000. Stratton K, Gable A, Shetty P, et al. Immunization safety review: Measles-mumps-rubella vaccine and autism. Washington, DC: National Academy Press, 2001. Sweeten TL, Bowyer SL, Posey DJ, et al. Increased prevalence of familial autoimmunity in probands with pervasive developmental disorders. Pediatrics 2003;112:E420. Szatmari P, Archer L, Fisman S, et al. Asperger’s syndrome and autism: Differences in behavior, cognition, and adaptive functioning. J Am Acad Child Adolesc Psychiatr 1995;34:1662. Szatmari P, MacLean JE, Jones MB, et al. The familial aggregation of the lesser variant in biological and nonbiological relatives of PDD probands: A family history story. J Child Psychol Psychiatry 2000;41:579. Taylor B, Miller E, Farrington CP, et al. Autism and measles, mumps, and rubella vaccine: No epidemiological evidence for a causal association. Lancet 1999;353:2026. Taylor B, Miller E, Lingam R, et al. Measles, mumps, and rubella vaccination and bowel problems or developmental regression in children with autism: Population study. BMJ 2002;324:393. Tolbert L, Haigler T, Waits MM, et al. Brief report: Lack of response in an autistic population to a low dose clinical trial of pyridoxine plus magnesium. J Autism Dev Disord 1993;23:193. Tordjman S, Gutknecht L, Carlier M, et al. Role of the serotonin transporter gene in the behavioral expression of autism. Mol Psychiatry 2001;6:434. Tsai LY, Stewart MA. Etiological implication of maternal age and birth order in infantile autism. J Autism Dev Disord 1983;13:57. Tuchman R, Rapin I. Epilepsy in autism. Lancet 2002;1:352. Tuchman RF, Rapin I. Regression in pervasive developmental disorders: Seizures and epileptiform electroencephalogram correlates. Pediatrics 1997;99:560. Tuchman RF, Rapin I, Shinnar S. Autistic and dysphasic children. II. Epilepsy. Pediatrics 1991;88:1219 Veenstra-VanderWeele J, Cook EH. Molecular genetics of autism spectrum disorder. Mol Psychiatry 2004;9:819. Verkerk AJ, Pieretti M, Sutcliffe JS, et al. Identification of a gene (FMR-1) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome. Cell 1991;65:905. Verstraeten T, Davis RL, DeStefano F, et al. Safety of thimerosalcontaining vaccines: A two-phased study of computerized health maintenance organization databases. Pediatrics 2003;112:1039. Volkmar FR. Childhood disintegrative disorder. Child Adolesc Psychiatry Clin North Am 1994;3:119. Volkmar FR, Cohen DJ. Nonautistic pervasive developmental disorders. In: Michels R, ed. Psychiatry. Philadelphia: JB Lippincott, 1991. Volkmar FR, Klin A, Marans W, et al. Childhood disintegrative disorder. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive developmental disorders, 2nd ed. New York: John Wiley & Sons, 1997. Volkmar FR, Lord C, Bailey A, et al. Autism and pervasive developmental disorders. J Child Psychol Psychiatry 2004;45:135. Volkmar FR, Nelson K. Seizure Disorder in Autism. J Am Acad Adolesc Psychiatry 1990;29:127. Volkmar FR, Pauls D. Autism. Lancet 2003;362:1133. Volkmar FR, Rutter M. Childhood disintegrative disorder: Results of the DMS-IV autism field trial. J Am Acad Child Adolesc Psychiatry 1995;34:1092. Volkmar FR, Stier DM, Cohen DJ. Age of recognition of pervasive developmental disorder. Am J Psychiatry 1985;142:1450.
935
Waage-Baudet H, Lauder JM, Dehart DB, et al. Abnormal serotonergic development in a mouse model for the Smith-Lemli-Opitz syndrome: Implications for autism. International J Dev Neurosci 2003;21:451. Wakefield AJ, Murch SH, Anthony A, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Lancet 1998;351:637. Walker-Smith J, Andrews J. Alpha-1-antitrypsin, autism, and coeliac disease. Lancet 1972;2:883. Wassink TH, Piven J, Vieland VJ, et al. Evidence supporting WNT2 as an autism susceptibility gene. Am J Med Genet 2001;105:406. Wecker L, Miller SB, Cochran SR, et al. Trace element concentrations in hair from autistic children. J Ment Defic Res 1985;29:15. Weissenbock H, Hornig M, Hickey WF, et al. Microglial activation and neuronal apoptosis in Bornavirus infection neonatal Lewis rats. Brain Pathol 2000;10:260. Wetherby AM, Schuler AL, Prizant BM. Enhancing language and communication: Theoretical foundations. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive developmental disorders, 2nd ed. New York: Wiley & Sons, 1997. Wiggs L, Stores G. Sleep patterns and sleep disorders in children with autistic spectrum disorders: Insights using parent report and actigraphy. Dev Med Child Neurol 2004;46:372. Willemsen-Swinkels SHN, Buitelaar JK, van Berckelaer-Onnes IA, et al. Brief report: Six months continuation treatment in naltrexoneresponsive children with autism: An open-label case-control design. J Autism Dev Disord 1999;29:167. Willemsen-Swinkels SHN, Buitelaar JK, van Engleland H. The effects of chronic naltrexone treatment in young autistic children: A double-blind placebo-controlled crossover study. Biol Psychiatry 1996;39:1023. Willemsen-Swinkels SHN, Buitelaar JK, Weijnen FG, et al. Placebocontrolled acute dosage naltrexone study in young autistic children. Psychiatry Res 1995;58:203. Williams RS, Hauser SL, Purpura DP, et al. Autism and mental retardation: Neuropathologic studies performed in four retarded persons with autistic behavior. Arch Neurol 1980;37:749. Williams JH, Whiten A, Singh T. A systematic review of action imitation in autistic spectrum disorder. J Autism Dev Disord 2004;34:285. Wilkerson DS, Volpe AG, Dean RS, et al. Perinatal complications as predictors of infantile autism. Intern J Neurosci 2002;112:1085. Wing L. Asperger’s syndrome: A clinical account. Psychol Med 1981;11:115. Wing L, Potter D. The epidemiology of autistic spectrum disorder: Is the prevalence rising? Ment Retard Dev Disord Res Rev 2002;8:151. Wing L. Wing Autistic Disorder Interview Checklist (WADIC). In: Rapin I, ed. Preschool children with inadequate communication: Developmental language disorder, autism, low IQ. London: MacKeith, 1996. Wolterink G, Daenen LE, Dubbeldam S, et al. Early amygdala damage in the rat as a model for neurodevelopmental psychopathological disorders. Eur Neuropsychopharmacol 2001;11:51. Woodhouse W, Bailey A, Rutter M, et al. Head circumference in autism and other pervasive developmental disorders. J Child Psychol Psychiatry 1996;37:665. World Health Organization. The ICD-10 classification of mental and behavioral disorders: Clinical descriptors and diagnostic guidelines. Geneva: World Health Organization, 1992. Yan W, Wilson CC, Haring JH. 5-HT1a receptors mediate the neurotrophic effect of serotonin on developing dentate granule cells. Dev Brain Res 1997;98:185. Yeargin-Allsopp M, Rice C, Karapurkar T, et al. Prevalence of autism in a US metropolitan area. JAMA 2003;289:49. Yirmiya N, Pilowsky T, Nemanov L, et al. Evidence for an association with the serotonin transporter promoter region polymorphism and autism. Am J Med Genet 2001;105:381. Yonan AL, Alarcon M, Cheng R, et al. A genomewide screen of 345 families for autism-susceptibility loci. Am J Hum Genet 2003;73:886. Yu CE, Dawson G, Munson J, et al. Presence of large deletions in kindreds with autism. Am J Hum Genet 2002;71:100. Yuwiler A, Shih JC, Chen CH, et al. Hyperserotoninemia and antiserotonin antibodies in autism and other disorders. J Autism Dev Disord 1992;22:33. Zappella M, Meloni I, Longo I, et al. Study of MECP2 gene in Rett syndrome variants and autistic girls. Am J Med Genet 2003;119B:102. Zwaigenbaum L, Szatmari P, Jones MB, et al. Pregnancy and birth complications in autism and liability to the broader autism phenotype. J Am Acad Child Adolesc Psychiatry 2002;41:572.
CHAPTER 39
Neuropsychopharmacology Melissa Lee and John T. Walkup
The practice of pediatric neuropsychopharmacology has grown increasingly complex in the past 2 decades. There have been dramatic increases in use of psychotropic medications despite limited empiric support and increasing concerns about the safety of these medications and their impact on growth and development. Historically, very few safe and effective medications were available to treat pediatric neuropsychiatric disorders, and children received no treatment or treatment that emphasized psychologic or behavioral interventions. With the rising availability of more tolerable and effective psychotropic medications and growing clinician comfort with prescribing for children, psychopharmacology has become standard practice for many neuropsychiatric disorders, resulting in increased use of medications in children [Zito et al., 2003] and more practitioners outside of child psychiatry prescribing psychotropic medications [Olfson et al., 2002]. The database for the safety and efficacy of psychotropic medications in children has increased dramatically in the past decade, although much remains to be done. There is support for the short-term efficacy of many commonly prescribed psychotropics, but there are few data on the longterm efficacy and safety of medication combinations commonly used in clinical practice, the comparative efficacy of modern psychologic treatments and psychopharmacology, and the proper sequence for staging psychologic and pharmacologic interventions. For example, there are excellent efficacy and safety data for the short-term treatment of attention-deficit–hyperactivity disorder (ADHD) with stimulants [Jensen et al., 2001], the treatment of anxiety disorders [Birmaher et al., 2003; RUPP, 2001; Rynn et al., 2001], treatment of obsessive-compulsive disorder [DeVeaugh-Geiss et al., 1992; Geller et al., 2001; March et al., 1998; Riddle et al., 2001], treatment of depression with antidepressants (e.g., the selective serotonin re-uptake inhibitors) [Emslie et al., 1997, 2002], and the use of atypical neuroleptics for affective disorders and behavioral problems in children [Findling et al., 2000]. However, there are few data on the short-term efficacy of mood stabilizers (e.g., lithium, anticonvulsants) for neuropsychiatric disorders. There is little information on the long-term usefulness of any psychotropic medication but increasing concerns about the long-term effects of psychotropic drugs on growth and development [MTA, 2004; Nilsson et al., 2004; Weintrob et al., 2002]. Medication combinations commonly used to treat children with multiple neuropsychiatric disorders (e.g., stimulants and selective serotonin re-uptake inhibitors for ADHD and anxiety or depression) have not been studied at all. An additional challenge for clinicians is the lack of correspondence between U.S. Food and Drug Administration
labeling for particular medications and data supporting safety and efficacy. Only a handful of psychotropic medications have Food and Drug Administration approval for use in the treatment of psychiatric conditions in children (Table 39-1). However, a number of studies supporting the safety and efficacy of psychotropic medication are not reflected in current labeling, leaving clinicians in an awkward position. As a result, most psychotropic medications prescribed for children are prescribed off-label. Off-label use of medications increased in the past 2 decades for a variety of indications, including stimulants for children younger than 5 years, selective serotonin re-uptake inhibitors for depression and anxiety, and atypical neuroleptics for mood disorders and aggression. Increased off-label use of these medications resulted from downward extension of a current indication to a younger age group (e.g., stimulants in children younger than 5 years, antidepressants in teens and children) and the availability of newer medications with a reduced potential for serious side effects compared with their predecessors. Sometimes, the benefit of off-label use has been extremely helpful (e.g., selective serotonin re-uptake inhibitors for anxiety disorders), but off-label prescribing of medications in advance of their achieving a good track record in clinical practice or the demonstration of efficacy in clinical trials may not be helpful. For example, based on its low sideeffect profile, a few positive case reports and open trials, and an aggressive marketing campaign, gabapentin was prescribed for the treatment of bipolar affective disorder; however, subsequent controlled trials have not supported its efficacy [Frye et al., 2000]. There has been a dramatic shift in the perceived safety of commonly prescribed psychotropic agents in children. Data suggest that longer-term use of stimulants may be associated with growth suppression [MTA, 2004], antidepressants for depression in children and adolescents may increase the risk for suicidal ideation or behavior early in the course of treatment [Hammad, 2004], and weight gain and risk for a metabolic syndrome are associated with neuroleptics [Allison and Casey, 2001; Lindenmayer et al., 2003; Wirshing et al., 1999] and some mood stabilizers [Yatham et al., 2002]. There is increasing public concern about the use of medications, particularly about the use of medications in vulnerable populations such as children. The decision about whether to use pharmacologic interventions mandates careful consideration of the benefits and the risks of treatment. To justify the use of medications, the child must first have a disorder or target symptoms with the potential for pharmacologic responsiveness. Second, the child’s level of impairment must cross a threshold of severity such that the lack of pharmacologic treatment, given all the potential risks, would cause more harm. Third, the
938
Neurobehavioral Disorders / 39
TABLE 39-1 Labeled and Off-Labeled Use of Neuropsychopharmacologic Agents in Children and Adolescents DRUG Stimulants Amphetamine, mixed salts Atomoxetine (nonstimulant) Dextroamphetamine Methylphenidate Pemoline Clonidine Guanfacine Tricyclic antidepressants Clomipramine Imipramine Nortriptyline Bupropion
LABELED USE
OFF-LABEL USE/CLINICAL PRACTICE
Narcolepsy (methylphenidate, dextroamphetamine)
None Enuresis (imipramine) Depression in adolescents (imipramine, nortriptyline) OCD (clomipramine in children > 10 yr) None
Venlafaxine
None
Mirtazapine
None
Serotonin re-uptake inhibitors Citalopram HBr Clomipramine Fluoxetine Fluvoxamine Paroxetine HCl Sertraline Lithium
OCD (fluoxetine, fluvoxamine, sertraline) Depressive disorders (fluoxetine)
Anticonvulsants Carbamazepine Gabapentin Lamotrigine Topiramate Valproate Typical neuroleptics Haloperidol Pimozide Atypical neuroleptics Aripiprazole Olanzapine Quetiapine Risperidone Ziprasidone
Seizure disorders
None
ADHD Aggression Depression in children Anxiety disorders ADHD Depression ADHD Depression Anxiety disorders ADHD Depression Anxiety disorders Depression Anxiety disorders
Bipolar affective disorder Aggression Bipolar affective disorder Aggression
Vocal or motor tics Severe behavioral disturbances
Psychotic disorders
None
Psychotic disorders Tourette’s syndrome Bipolar affective disorder Aggression
ADHD, attention-deficit–hyperactivity disorder; OCD, obsessive-compulsive disorder.
child’s symptoms must not have improved with nonpharmacologic interventions or these interventions are not readily available in the community. Fourth, the clinician must have the time available to adequately monitor patients for both common and rare, but significant, adverse events (e.g., suicidal ideation or behavior). Safe prescribing of medications for children also requires detailed documentation of the decision-making process and an active monitoring plan for outcome and adverse events. The likelihood of a child with a neuropsychiatric disorder presenting to a pediatric neurology practice is high. To treat these children effectively, the pediatric neurologist must have the ability to collect and integrate information from multiple sources (i.e., child, family, school, and other agencies) and to make a diagnostic formulation and treatment plan that addresses the neuropsychiatric symptoms and psychosocial factors that affect the delivery of care and the
assessment of outcome. Given the rapidly changing nature and increasing complexity of modern clinical care, pediatric neurologists need to define their comfort level in assessing and treating neuropsychiatric disorders and to determine how this may influence the scope of their practice. For neurologists who treat neuropsychiatric disorders, it is critical to keep abreast of this evolving field, especially new safety data that influence the standard of care. It may require a team of colleagues, including psychologists and psychiatrists, who can be involved in the assessment and treatment of these children with complex medical profiles. This chapter provides an overview of the major classes of medications used in pediatric neuropsychopharmacology, including stimulant medications, antidepressants, mood stabilizers, anxiolytics, and α2-agonists. In-depth discussions regarding comprehensive psychiatric assessments and multimodal treatments can be found in the basic textbooks in
Lee and Walkup / Neuropsychopharmacology
939
TABLE 39-2 Stimulant and Nonstimulant Medications for Attention-Deficit–Hyperactivity Disorder: Preparations, Pharmacology, and Dosing DRUG
PREPARATION
PHARMACOLOGY
DOSING
Methylphenidate, immediate release
Ritalin (5- and 10-mg tablets)
Time to peak plasma conc = 1-2 hr Half-life = 2-3 hr
Age ≥ 6 yr: 5 mg qd or bid; increase dose by 5 to 10 mg weekly; maximum dose of 60 mg/day Optimum dose between 0.3 and 0.7 mg/kg/dose, given bid or tid (total dose = 0.6 to 2.1 mg/kg/day) 8-hour dose of Rialin ER corresponds to titrated 8-hour dosage of immediate-release methylphenidate 8-hour dose of Methylin ER corresponds to titrated 8-hour dosage of immediate-release methylphenidate 8-hour dose of Metadate ER corresponds to titrated 8-hour dosage of immediate-release methylphenidate Once-daily dosing; may be opened and sprinkled on food
Methylin (5-, 10-, and 20-mg tablets) Methylphenidate, sustained release
Ritalin SR (20-mg tablets)
Time to peak plasma conc = 4-5 hr Duration of action = 8 hr
Methylphenidate, extended release
Methylin ER (10- and 20-mg tablets)
Time to peak plasma conc = 4.7 hr Duration of action = 8 hr
Metadate ER (10- and 20-mg tablets)
Time to peak plasma conc = 4-5 hr Duration of action = 8 hr
Metadate CD (10-, 20-, and 30-mg capsules)
Bimodal release of methylphenidate Time to first peak plasma conc = 1.5 hr Time to second peak plasma conc = 4.5 hr Bimodal release of Once-daily dosing; may be opened and methylphenidate sprinkled on food Time to first peak plasma conc = 1-3 hr Time to second peak plasma conc = 5-7 hr Bimodal release of 18 mg per day; increase gradually until methylphenidate clinical response achieved or maximum Time to first peak plasma conc = 1-2 hr daily dose of 54 mg (maximum daily Time to second peak plasma conc = 6-8 hr dose of 72 mg in adolescents) Time to peak plasma conc = 60-90 min Initial dose of 2.5 mg daily; increase Half-life = 2.2 hr gradually until clinical response achieved or maximum daily dose of 20 mg, given bid Time to peak plasma conc = 2-3 hr Ages 3-5 yr: 2.5 mg/day; increase by Half-life = 12 hr 2.5 mg once or twice weekly Age > 6yr: initial dose of 5 mg/day; increase by 5 mg once or twice weekly; maximum of 40 mg/day Optimum dose: 0.15 to 0.5 mg/kg/dose given bid or tid (total dose = 0.3 to 1.5 mg/kg/day) Time to peak plasma conc = 8 hr Once-daily dosing Dosing same as immediate-release form Time to peak plasma conc = 3 hr Age 3-5 yr: 2.5 mg/day; increase by Half-life = 7-8 hr 2.5 mg once or twice weekly Time to peak conc = 7 hr Age > 6 yr: initial dose of 5 mg/day; increase by 5 mg once or twice weekly; maximum of 40 mg/day Optimum dose: 0.15 to 0.5 mg/kg/dose given bid or tid (total dose = 0.3 to 1.5 mg/kg/day) Time to peak plasma conc = 2-4 hr Age ≥ 6 yr: initial dose of 37.5 mg/day; Half-life = 12 hr increase by 18.75 mg/week until clinical response or maximum of 112.5 mg/day. Half-life = 5.2 hr Children and adolescents < 70 kg: initial dose of 0.5 mg/kg/day qd or bid; starting with bid dosing may lessen gastrointestinal side effects; increase gradually to 1.2 mg/kg/day. Children, adolescents, or adults > 70 kg: initial dose of 40 mg/day; increase gradually to 80 mg; if less than optimal response by 3-4 wk, may increase to 100 mg if tolerated
Ritalin LA (20-, 30-, and 40-mg capsules) Methylphenidate, extended release, core Trilayer core tablets Dexmethylphenidate
Concerta (18-, 27-, 36-, 45-, and 54-mg tablets) Focalin (2.5-, 5-, and 10-mg tablets)
Dextroamphetamine, immediate release
Dexedrine (5-mg tablets)
Dextroamphetamine, sustained release Amphetamine, mixed salts
Dexedrine (5-, 10-, and 15-mg spansules) Adderall (5-, 10-, 20-, and 30-mgtablets) Adderall XR (10-, 20-, and 30-mg tablets)
Pemoline
Cylert (18.75-, 37.5-, and 75-mg tablets)
Atomoxetine
Strattera (10-, 18-, 25-, 40-, and 60-mg tablets)
940
Neurobehavioral Disorders / 39
child psychiatry. The American Academy of Child and Adolescent Psychiatry (AACAP) and the American Psychiatric Association (APA) have developed and published practice guidelines that summarize current thinking about the assessment and treatment of pediatric neuropsychiatric disorders.
STIMULANTS This section briefly describes the use stimulants in the treatment of ADHD (Table 39-2). A discussion of atomoxetine (Strattera), a nonstimulant medication approved for the treatment of ADHD in children and adults, is also included. Chapter 36 provides a detailed discussion of the diagnostic assessment and other modalities of treatment of ADHD.
Clinical Applications Stimulants have been in clinical use since 1937, when it was observed that a group of children in residential treatment showed marked improvement in their behavior with Benzedrine (D- and L-amphetamine) [Weiss and Weiss, 2002]. Since then, the criteria for ADHD have been refined, and other stimulant medications have been evaluated and demonstrated efficacy in numerous placebo-controlled studies [Jensen et al., 2001]. Approximately 70% to 80% of patients with ADHD have a positive response to stimulant medication. Stimulants, with the exception of pemoline, are the first-line treatment for ADHD. Pemoline, although effective [Pelham et al., 1990], has been associated with acute liver failure (see “Adverse Effects”), and it is generally not considered unless alternative medications have failed. Atomoxetine, a nonstimulant medication, has been approved for the treatment of ADHD in children and adults [Strattera, 2003]. Stimulant medications have generally been viewed as ineffective or contraindicated for hyperactivity in children with autism and by extension other pervasive developmental disorders. However, stimulants can be useful for some children. A single test dose of stimulant may be useful to identify children for whom a longer stimulant trial is contraindicated. Children who experience a significant worsening of ADHD (e.g., hyperactivity and irritability) or pervasive developmental disorder symptoms (i.e., tics or stereotypies) with a single dose may be excluded from further stimulant treatment. For children who tolerate a test dose, it may be prudent to complete a full trial [Di Martino et al., 2004]. Despite substantial data supporting the efficacy of stimulants, their use in children is controversial because there are concerns about safety. The lay public and media have expressed concerns about the potential for overdiagnosis of ADHD and overuse of stimulant medications in children. According to the U.S. Surgeon General, most children with psychiatric disorders are not assessed or treated [Satcher, 2001]. Despite the dramatic increases in stimulant use in the past 10 years [Zito et al., 2003], the ratio of stimulant use to prevalence of ADHD is less than 1:1, suggesting that undertreatment is a more prevalent and important issue [Jensen et al., 1999]. Stimulant medications have come under public fire because of their reported associations with tics, growth suppression, and addiction. This connection has caused some to question their safety in short- and long-term use (see
“Adverse Effects”). Overall, it is difficult to make causal links between stimulants and any but the most common adverse events, because most clinical trials for efficacy are not fully powered to detect rare or unexpected adverse events. Some studies suggest that children with ADHD who are treated early in life have a lower risk of abuse than children with ADHD who are not treated [Katusic et al., 2003; Wilens et al., 2003]. Prudent practice therefore necessitates use of the lowest possible doses with close monitoring in addition to nonpharmacologic intervention when available and appropriate. During the titration phase, children often are monitored monthly for symptoms, side effects, blood pressure, pulse, height, and weight. After a maintenance dose is achieved, visits every 3 to 4 months should suffice. The data show that medication alone is more beneficial than behavioral therapy alone in children 5 years of age and older. The combination is specifically helpful for oppositional behavior and familial tension. Detailed discussion with the family and teachers with full documentation in the medical record is essential.
Pharmacology Stimulants are sympathomimetic drugs that directly stimulate α- and β-adrenergic receptors. They also stimulate the release of dopamine from presynaptic nerve terminals and inhibit their re-uptake. The exact mechanism for efficacy on attention and hyperactivity in ADHD is unknown. Stimulant medications are available in immediate-release and sustained-release preparations (see Table 39-2).
Clinical Management Assessment A neuropsychiatric assessment of inattention, impulsivity, and hyperactivity involves gathering information from multiple sources, including the child, parents, teacher, therapist, or other individuals involved with the child (e.g., day care providers and coaches). Information can be gathered through clinical interview; patient, parent, and teacher rating scales; neuropsychologic testing; and medical evaluation, including laboratory screening [AACAP, 1997b]. The diagnostic criteria for ADHD are detailed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) [APA, 1994]. A thorough neuropsychiatric assessment is necessary because inattention, impulsivity, and hyperactivity can be complications of medical conditions, and they are commonly caused by other neuropsychiatric disorders. Children with ADHD often have co-occurring neuropsychiatric disorders, which can make it difficult to accurately determine whether ADHD symptoms are attributable to ADHD or to the co-occurring conditions. Medical and developmental problems in the differential include vision or hearing deficits, seizures, chronic medical illnesses, sleep deprivation, and poor nutrition [AACAP, 1997c]. Children who have unidentified intellectual deficits, learning disabilities, speech and language problems, or substance abuse may appear to exhibit ADHD symptoms. Neuropsychiatric conditions such as anxiety disorders, depressive disorders, and bipolar disorder have disturbances in attention, impulse control, and
Lee and Walkup / Neuropsychopharmacology
activity level that can be especially difficult to distinguish from ADHD. Identification of co-occurring conditions and risk factors for adverse effects is essential, because some medications may be contraindicated or medication management may require dosing modification or closer monitoring. For example, a patient with co-occurring ADHD and anxiety or depression may prompt the clinician to initiate treatment with an antidepressant first rather than a stimulant, depending on which of the two conditions is more impairing. A child with a pervasive developmental disorder may appear unresponsive to stimulants but may have an adverse behavioral reaction that can be severe. Similarly, a patient with a personal or family history of tic disorders may develop tics de novo or experience a worsening of existing tics during an initial stimulant trial, but evidence suggests that stimulants are unlikely to increase tic emergence relative to placebo [Kurlan, 2003]. A medical evaluation before initiating most psychotropic medications, including stimulants, is prudent to medically “clear” a child. The evaluation should include a recent medical history and a physical examination completed by the primary care provider. Any significant change in health during treatment requires repeat evaluation. Choice of laboratory screening procedures and imaging studies is guided by the medical history and findings on physical or neurologic examination. These may include lead level, thyroid function tests, genetic screening, metabolic studies, magnetic resonance imaging, and electroencephalography. Other assessments may be indicated, including occupational therapy, physical therapy, speech and language evaluation, and neuropsychology [AACAP, 1997b]. For stimulant medications, baseline height, weight, and family or personal history of a tic disorder are also important. Completing a baseline sexual history is often overlooked by physicians when treating adolescents because of the clinician’s lack of training or experience or because of discomfort with the topic. Monitoring for sexual side effects after medication initiation is essential because psychotropic medications can have a significant impact on sexual functioning and may affect the patients’ physical and mental health. Sexual side effects can be the cause of otherwise unexplained medication nonadherence. Some neuropharmacologic agents can interact with oral contraceptives, rendering them ineffective, and psychotropic medications may have teratogenic effects.
Medication Initiation and Titration Pharmacotherapy is only one component in the treatment of children and adolescents with ADHD. Patients and families should be informed of the benefits and limitations of medications and the importance of nonpharmacologic interventions in maximizing the benefits of treatment, including an appropriate school placement, behavior management training for parents, and consistency and structure at home and at school. Practitioners may not have the full range of skills necessary for the management of all aspects of ADHD, and the prescribing physician may wish to develop a treatment team to meet the often complex needs of children with ADHD. The starting dose of methylphenidate is 5 mg, given twice daily and dispensed after breakfast and lunch to minimize appetite-suppressant effects. The dose is increased at weekly
941
intervals by increments of 5 to 10 mg until the therapeutic effect is achieved or side effects are encountered. The manufacturer recommends a maximum daily dose of 60 mg [Ritalin, 2004]; however, some clinicians exceed this dose if higher doses are necessary to control symptoms and the patient is not experiencing adverse effects. Detailed informed consent and adequate monitoring and documentation are essential for safe prescribing. Severity of symptoms, afterschool activities, or homework demands may warrant a late afternoon dose. An alternative method is to calculate the dose by weight [Duncan, 1990]. The target dose falls between 0.3 and 0.7 mg/kg, administered two to three times each day (total dose of 0.6 to 2.1 mg/kg/day). With D-amphetamine and mixed salts preparations, the starting dose for children between the ages of 3 and 5 years is 2.5 mg/day, with incremental increases of 2.5 mg weekly until a therapeutic response is achieved. For children 6 years old or older, the starting dose is 5 mg given once or twice each day, with weekly increases of 5 mg until a therapeutic response is achieved. The manufacturer does not recommend exceeding 40 mg/day [Adderall, 2004; Dexedrine, 2002]. As with methylphenidate, some clinicians use higher doses if clinically indicated. Dosing by weight, the optimum dose may fall between 0.15 and 0.5 mg/kg, administered twice or three times daily, with a maximum daily dose of 0.3 to 1.5 mg/kg/day [Duncan, 1990]. Sustained-release preparations are administered after breakfast. Whether sustained-release preparations are as effective as their immediate-release counterparts has been debated [Birmaher et al., 1989; Fitzpatrick et al., 1992; Pelham et al., 1987] but rarely studied. In clinical practice, many patients experience comparable or greater benefit from sustained-release preparations because of the convenience of once-daily dosing, avoiding dosing at school, increasing compliance, and reducing rebound effects. The physician can start with a long-acting preparation and turn to the immediate-release form if the long-acting formulation is not completely effective.
Monitoring Stimulants Ongoing monitoring of medication efficacy involves assessment of the patient’s level of functioning in school, family, community, and peer groups. Data are collected from behavioral observations during office visits, parent and teacher reports, and parent and teacher ADHD rating scales. Patients require monitoring of possible side effects that can occur with short-term and long-term stimulant use. Heart rate, blood pressure, weight, height, and emergence of or changes in tic severity should be assessed routinely. Some clinicians consider the use of “drug holidays” on weekends or during the summer to limit children’s exposure to stimulants and minimize possible long-term adverse effects such as low weight and growth suppression. However, the practice of drug holidays is controversial, because it usually results in the rapid return of symptoms and accompanying impairment. To identify patients who may do well with drug holidays, clinicians can review symptoms and impairment from times of the day when children are not benefiting from stimulants, such as early morning or later in the evening. If patients do well during these times, it may be reasonable to consider more extended time off stimulants.
942
Neurobehavioral Disorders / 39
Drug holidays should be planned for times when there are no important school or social activities [AACAP, 1997c], and they should be reserved for patients whose families can provide adequate structure, behavior management, and supervision during these periods. Although hyperactive symptoms tend to improve as children mature, inattention and impulsivity often persist. Long-term stimulant treatment may be necessary as up to 80% of ADHD children continue to have symptoms into adolescence and 65% into adulthood [Barkley, 1996; Weiss and Hechtman, 1993].
Adverse Effects Although most children tolerate stimulant medications well, some do not. The most common side effects of stimulants are insomnia and nervousness [Ritalin, 2004]. Some children with ADHD experience sleep disturbance before exposure to stimulants. The child’s preexisting sleep history should be obtained, including other factors that may contribute to sleep disturbance (e.g., poor sleep hygiene, caffeine use, oppositional behavior, separation anxiety). Ironically, some children experience difficulty falling asleep related to hyperactivity, and they can benefit from a small dose of stimulant to help them stay in bed and fall asleep. In group comparisons, dosing three times daily with short-acting stimulants versus dosing two times daily was not found to increase sleep disturbance [Kent et al., 1995; Stein et al., 1996]; however, new-onset sleep delay after starting stimulants may be associated with a stimulant dose that is too high overall or with dosing stimulants too late in the day. Difficulty with falling asleep because of stimulants can be addressed with a combination of dose adjustment, improved sleep hygiene (i.e., straightforward ritual for falling asleep and removing distractions from the room such as televisions, video games, homework, and night lights), cooler room temperatures, roomdarkening shades, avoidance of late afternoon or evening doses of stimulants, switching to a different stimulant, or addition of a sedating medication with ADHD treatment effects such as clonidine [Brown and Gammon, 1992; Prince et al., 1996] or guanfacine. Statistically and clinically significant decreases in expected weight gain and even weight loss have been observed, and these effects appear to be dose related [MTA, 2004; Zeiner, 1995]. Because the impact on weight is mediated by stimulant-induced appetite suppression, administering stimulant doses immediately after meals [Swanson et al., 1983], allowing the child to eat later in the evening after the appetite suppressant effect of the stimulant has abated, or allowing drug holidays on weekends or evenings, may mitigate these effects. The possibility of growth suppression with long-term use of stimulants is a controversial topic. Studies have reported lower than expected heights in pre-adolescents with ADHD, but heights returned to normal by adulthood [Gittelman et al., 1985; Hechtman, 1985]. The apparent lack of impact on adult height was thought to result from the discontinuation of stimulants in adolescence. An alternative theory proposes that this pattern of growth was inherent in children with ADHD and not related to stimulant treatment. The dysregulation of several neurotransmitter systems associated with ADHD may alter neuroendocrine function, including those
involving growth [Spencer et al., 1998]. Adult height does not appear to be reduced after methylphenidate treatment in childhood [Klein and Mannuzza, 1988]. Follow-up of subjects in the Multimodal Treatment of ADHD (MTA) study suggests growth delay compared with a group that had growth above population norms from 14 to 24 months after starting medication. It is not clear whether growth suppression will continue and have a long-term impact, resolve with stimulant discontinuation, or resolve on its own [MTA, 2004]. Historically, stimulant treatment has been associated with the emergence of tics [Borcherding et al., 1990] or the exacerbation of preexisting tics [Law and Schachar, 1999]. Children at risk appeared to be those with a personal history or family history of tic disorders. However, the effect on tics is not absolute; only 25% to 30% of ADHD children with tics experienced significant worsening in some studies [Castellanos et al., 1997; Spencer et al., 1996]. In placebo-controlled trials, low to moderate doses of methylphenidate improve attention and behavior in children with chronic tic disorders without significantly worsening tics [Gadow et al., 1995, 1999]. In the Treatment of ADHD in Children with Tics (TACT) study, tic increases categorized as an adverse event occurred in nearly equal numbers of subjects on placebo (22%), clonidine (26%), and methylphenidate (20%). These data suggest that 20% to 26% of youngsters with tics will experience tic worsening shortly after initiation of any medication treatment, including placebo, lending support to the hypothesis that tic increases observed after starting stimulants reflect the natural waxing and waning of tic severity [TSSG, 2002]. Stimulants have been associated with nonsignificant increases in heart rate and blood pressure [Brown and Sexson, 1989; Tannock et al., 1995]. Although the product information for the stimulants warns of possible decreases in seizure threshold, no increase in seizure frequency was observed in children treated with stimulants who had co-occurring ADHD and seizure disorder [Feldman et al., 1989; Wroblewski et al., 1992]. There is no increased risk of addiction from appropriate treatment with stimulants for ADHD. Adolescents with ADHD treated with stimulants were less likely to abuse stimulants [Biederman, 2003; Faraone and Wilens, 2003; Hechtman, 1985]. Despite the impact on a broad range of ADHD symptoms, including irritability, stimulant medications can be associated with undesirable changes in mood and behavior [Gadow et al., 1992]. Some of these changes occur when the stimulant is reaching peak serum concentrations, or they may occur when serum concentrations are waning, so-called rebound effects. Effects associated with peak concentrations include dysphoria, anxiety, agitation, or the “zombie” effect (i.e., overfocused and passive). Rebound effects include overactivity, talkativeness, excitability, irritability, and insomnia [Rapoport et al., 1978; Zahn et al., 1980]. It is often difficult to determine whether such rebound symptoms are the reemergence of ADHD symptoms off stimulants or true withdrawal or rebound symptoms. These adverse behavioral effects can be managed in a variety of ways, including dose reduction or medication discontinuation and by improving late afternoon coverage by adding a low dose of immediate-release stimulant or by switching to a longacting stimulant [AACAP, 1997c]. Youngsters who experience these side effects on one of the stimulants do not necessarily have the same behavioral effects on another
Lee and Walkup / Neuropsychopharmacology
stimulant, and switching to another stimulant or alternative medication can be useful. Clinicians should be comfortable using all stimulant preparations to optimize treatment effects and minimize side effects. Pemoline (Cylert) has been associated with rare cases of acute hepatic failure. Since 1975, 15 cases have been reported to the Food and Drug Administration, and 12 of 15 cases resulted in death or necessitated liver transplantation. Although it is unclear whether the early detection of elevated liver enzyme levels can prevent progression of hepatic dysfunction, the manufacturer recommends obtaining baseline liver function tests and monitoring serum levels of alanine aminotransferase every 2 weeks during therapy. Alanine aminotransferase is considered significantly elevated if levels are more than twice the upper limit of normal [Cylert, 2004].
Drug Interactions If stimulant medications are administered concomitantly or within 2 weeks of receiving monoamine oxidase inhibitors, there is a significant risk of precipitating a hypertensive crisis. Methylphenidate may inhibit the metabolism of coumarin anticoagulants, some anticonvulsants (e.g., phenobarbital, phenytoin, carbamazepine, primidone), and tricyclic antidepressants (e.g., imipramine, desipramine, clomipramine). Foods and beverages with caffeine may increase both efficacy and adverse effects. Amphetamines inhibit adrenergic blockers. Gastrointestinal acidifying agents, including citrus juices, lower absorption of amphetamines. Urinary acidifying agents increase urinary excretion of methylphenidate. Both types of acidifying agents can lower blood levels and efficacy of amphetamines. Likewise, alkalinizing agents increase blood levels and potentiate the actions of amphetamines [Cylert, 2004]. The safety of combining stimulants, especially methylphenidate, with clonidine has been controversial. Clonidine has been helpful in managing sleep disturbance related to ADHD or stimulant treatment [Wilens et al., 1994]. The combination appears to help children with ADHD and co-occurring oppositional and conduct disorder [Hunt et al., 1990]. The combination also appears useful in the treatment of ADHD in children with tic disorders [TSSG, 2002]. Concerns about the interaction developed after the report of four deaths of children who apparently received clonidine and methylphenidate, as well as other medications in some cases [Fenichel, 1995]. Although the cases did not have a clear pattern of causality [Sallee et al., 2000a; Wilens et al., 1999], clinicians are more cautious about prescribing this combination. When combining clonidine and stimulants, careful screening is recommended for a personal and family history of cardiac abnormalities, arrhythmias, and non-vasovagal syncope, and a baseline and follow-up electrocardiogram (ECG) should be obtained.
NONSTIMULANT MEDICATION Atomoxetine Clinical Applications Atomoxetine is a nonstimulant medication that is approved for the treatment of ADHD in adults and children 6 years old
943
or older. It is a selective norepinephrine re-uptake inhibitor that is structurally more similar to fluoxetine than to stimulant medications. Atomoxetine potentially offers several advantages over stimulant medications: longer duration of action, lower misuse or abuse potential, lower risk of rebound effects, lower risk of precipitating tics or psychosis, and ease of prescribing because duplicate or paper prescriptions are not required and multiple refills are possible. Effectiveness of atomoxetine in children has been supported by placebo-controlled trials [Kelsey et al., 2004; Spencer et al., 2002]. Atomoxetine doses of 1.2 and 1.8 mg/kg/day administered in divided doses were superior to placebo and atomoxetine in a dose of 0.5 mg/kg/day; there was no clear superiority of 1.8 versus 1.2 mg/kg/day. Early clinical trials have used twice-daily dosing, but once-daily dosing also appears effective [Michelson et al., 2004]. Long-term treatment (9 months) with atomoxetine appears to be safe and well tolerated [Michelson et al., 2004]. The therapeutic effects observed in short-term treatment were maintained in significantly more children compared with placebo, and the children attained superior psychosocial functioning [Kratochvil et al., 2002]. When compared with methylphenidate treatment, atomoxetine was associated with comparable therapeutic effects [Michelson et al., 2003]. Efficacy of atomoxetine in adults with ADHD was demonstrated at doses of 60 to 120 mg/day [Strattera, 2003].
Pharmacology Atomoxetine is well absorbed through the gastrointestinal tract and is metabolized by the liver, predominantly by cytochrome P-450 2D6 (CYP2D6). A small percentage of the population (approximately 7% of whites and 2% of African Americans) has reduced activity of the cytochrome P-450 isoenzyme system. These individuals are considered to be “poor metabolizers” of medications whose predominant method of metabolism is this isoenzyme. Poor metabolizers can be expected to achieve higher than expected plasma concentrations on a given dose and a prolonged half-life compared with those with normal CYP2D6 activity. The half-life of atomoxetine in poor metabolizers is 21.6 hours, compared with 5.2 hours in normal metabolizers. Atomoxetine is 98% bound to plasma proteins, primarily serum albumin [Strattera, 2003].
Clinical Management Children should undergo standard psychiatric and medical assessment for ADHD (see “Clinical Management of Stimulant Medication”). No laboratory screening is required, although consideration for obtaining baseline and follow-up liver function studies should be considered in view of reports of severe acute liver dysfunction (described later). Baseline values for weight, heart rate, and blood pressure should be obtained. Concomitant use of medications with cardiovascular effects and medications that inhibit cytochrome P-450 necessitates dosage adjustment. Although the determination of cytochrome P-450 metabolizer status is not routinely available, it appears to be unnecessary because regular dosing parameters provide the time for assessment of outcome and adverse events that may be experienced by poor metabolizers.
944
Neurobehavioral Disorders / 39
In children, the usual starting dose of atomoxetine is 0.5 mg/kg/day, given in the morning or divided into morning and late afternoon doses. Starting with a split dosing regimen may decrease gastrointestinal side effects. The dose can be consolidated after a target dose is achieved. Decreasing side effects on initiation will ultimately lead to better compliance. The dose may be increased every 3 days to a target dose of 1.2 mg/kg/day. For adults or for children and adolescents weighing more than 70 kg, atomoxetine may be initiated at 40 mg/day. The dose may be increased gradually every 3 days to a maximum dose of 80 mg. If there is an inadequate response after a 2- to 4-week trial, the dose may be increased to 100 mg/day. Patients taking atomoxetine concomitantly with potent inhibitors of CYP2D6 should be maintained at the initial dose for at least 4 weeks before a dosage increase is considered. Dosage reduction is required in patients with hepatic impairment [Strattera, 2003]. In clinical practice, combination therapy may be used during initiation and titration of atomoxetine, especially in children with severe ADHD symptoms. The effectiveness and tolerability of combining atomoxetine with methylphenidate in children who have not responded to monotherapy have been reported in a few patients [Brown, 2004]. Discontinuation of atomoxetine does not require dose tapering. Abrupt discontinuation of atomoxetine has not been associated with an acute discontinuation syndrome [Wernicke et al., 2003].
Adverse Effects The most common side effects of atomoxetine in children and adolescents are upset stomach, decreased appetite, nausea, vomiting, dizziness, tiredness, and mood swings. Atomoxetine was associated with increases in heart rate of 6 beats per minute and increases in systolic and diastolic blood pressure of 1.5 mm Hg compared with placebo. In an analysis of short-term and long-term treatment with atomoxetine, increased systolic blood pressure was observed in adults, and increased diastolic blood pressure occurred in children and adolescents. Heart rate increased in both groups, and no prolongation of the QTc interval was observed [Strattera, 2003]. Seizures and prolonged QTc intervals were reported after an overdose with atomoxetine [Sawant and Daviss, 2004]. Two patients became severely ill from reversible liver failure while taking atomoxetine and other medications. Strattera labeling states that the medication should be discontinued when liver function test values are increased or when there is clinical evidence of jaundice. Use in patients with liver disease likely should be avoided.
Drug Interactions Inhibitors of CYP2D6 may increase serum concentrations of atomoxetine. Atomoxetine does not have significant effects on the cytochrome P-450 system. Combination with monoamine oxidase inhibitors may precipitate a hypertensive crisis. Atomoxetine has potential interactions with cardiovascular agents and adrenergic agonists. Albuterol’s tendency to increase heart rate and blood pressure may be potentiated by atomoxetine. No increase in the cardiovascular effects of methylphenidate was observed when atomoxetine was added, and no interactions between atomoxetine and other proteinbound medications were observed [Strattera, 2003].
ALPHA2-AGONISTS Clinical Applications Two α2-agonists, clonidine (Catapres) and guanfacine (Tenex), are prescribed in the treatment of ADHD, Tourette’s syndrome, aggressive or self-injurious behavior, and the physiologic symptoms of anxiety. The drugs are approved by the Food and Drug Administration for hypertension in adults. In clinical practice, clonidine is a second-line treatment for ADHD. Clonidine has been shown to improve behavior of children with ADHD; however, the degree of its effect in a meta-analysis was less than that of stimulants, and it was associated with many side effects [Connor et al., 1999]. Greater improvement was seen with hyperactivity and impulsivity [Hunt, 1987; Hunt et al., 1982] and frustration tolerance [Hunt, 1987] than with distractibility. Children have been maintained on clonidine for up to 5 years with continued benefit [Hunt et al., 1990, 1991]. The combination of clonidine and methylphenidate has been helpful in adolescents with co-occurring ADHD and oppositional or conduct disorder [Hunt et al., 1990]. This combination allowed the dose of methylphenidate to be reduced by 40% [Hunt et al., 1990]. In children with co-occurring ADHD and tic disorders, those treated with clonidine experienced improvements in both conditions [Steingard et al., 1993]. Clonidine has been used to treat sleep disturbances in children with ADHD [Wilens et al., 1994], and it appears to be helpful in managing severe aggression [Kemph et al., 1993]. Findings of studies looking at the use of clonidine in Tourette’s syndrome have been mixed [Leckman et al., 1982], but significant improvements in tics and behavior have been reported [Cohen et al., 1980; Comings, 1990; Leckman et al., 1991]. Limited data exist on guanfacine. One open trial demonstrated its effectiveness in ADHD [Hunt et al., 1995]. Findings for patients with ADHD and Tourette’s syndrome have been mixed [Chappell et al., 1995; Horrigan and Barnhill, 1995]. Results of more recent studies have been more promising [Scahill et al., 2001].
Pharmacology Clonidine and guanfacine are well absorbed from the gastrointestinal tract and reach peak plasma levels 1 to 3 hours after oral administration. The half-life of clonidine is 6 to 12 hours, and the half-life of guanfacine is 10 to 30 hours. Clonidine is also available in a transdermal patch. Clonidine and guanfacine exert agonist effects on presynaptic α2-adrenergic receptors in the sympathetic nuclei of the brain, resulting in decreased release of norepinephrine from presynaptic nerve terminals. In the central nervous system (CNS), clonidine and guanfacine are thought to regulate noradrenergic activity in the locus ceruleus [Catapres, 2004].
Clinical Management Before the initiation of clonidine or guanfacine, baseline ECG, heart rate, and blood pressure should be obtained. A history of syncope or cardiovascular disease is a relative contraindication. Heart rate and blood pressure should be monitored regularly during therapy for hypotension and bradycardia.
Lee and Walkup / Neuropsychopharmacology
Clonidine is initiated at 0.05-mg dose taken at bedtime, gradually titrating the dose over several weeks to 0.15 to 0.3 mg/day in divided doses. Clonidine is also available in a transdermal patch, which may have the advantage of increased medication compliance and more stable blood levels. After a therapeutic dose of oral clonidine is achieved, the equivalent patch can be substituted. The patch lasts 5 days in children and 7 days in adults [Catapres, 2004]. Guanfacine offers the advantage of a longer half-life and therefore less frequent dosing, and it may cause less sedation than clonidine [Hunt et al., 1995]. It is initiated at 0.5 mg at bedtime and is titrated up to a maximum of 3 mg/day.
Adverse Effects The most common side effects of clonidine and guanfacine include sedation, dizziness, fatigue, dry mouth and eyes, nausea, hypotension, and constipation [Catapres, 2004]. Catapres-TTS may be associated with contact dermatitis, which may be reduced by rotating its location on the body. Because of the risk of rebound hypertension with abrupt discontinuation, these medications should be prescribed only to patients with reliable medication compliance. Likewise, the dose should be tapered gradually when discontinuing the medication [Catapres, 2004]. One study retrospectively examined the effects of clonidine and clonidine plus stimulants on the ECGs of children and adolescents treated for ADHD or tic disorder. ECGs were examined before and after treatment, and no systematic electrocardiographic effect of clonidine was found [Kofoed et al., 1999].
Drug Interactions Clonidine may potentiate the CNS-depressant effects of alcohol and sedating medications. The manufacturer advises caution in combining clonidine with medications that affect cardiac conduction and sinus node function because of potential additive effects such as bradycardia and atrioventricular block [Catapres, 2004].
945
ANTIDEPRESSANTS Tricyclic Antidepressants Clinical Applications Tricyclic antidepressants are approved for the treatment of depression in adults and adolescents (Table 39-3). Placebocontrolled studies have demonstrated the efficacy of tricyclic antidepressants in the treatment of depression in adults, but studies enrolling children and adolescents have yielded inconsistent results. Some open studies show no significant response to tricyclic antidepressants [Kashani et al., 1984; Kramer and Feiguine, 1981]. Others suggest efficacy of desipramine, imipramine, and nortriptyline [Boulos et al., 1991; Geller et al., 1986; Ryan et al., 1986]. Placebo-controlled studies, however, do not support efficacy [Geller et al., 1989, 1990; Puig-Antich et al., 1987]. The lack of efficacy in placebo-controlled trials may be related to methodologic problems, such as a small number of subjects, types of subjects enrolled (with depression that too mild or too severe), and the high placebo response rates in many studies. The use of tricyclic antidepressants for the treatment of depression in children and adolescents has declined because of their equivocal efficacy in this population and the availability of antidepressants with a more favorable side effect profile (e.g., selective serotonin re-uptake inhibitors). Clomipramine has been approved for use in children 10 years old or older for obsessive-compulsive disorder. A number of randomized, controlled trials have demonstrated short-term efficacy [DeVeaugh-Geiss et al., 1992] and efficacy in maintenance treatment [Leonard et al., 1991]. Clomipramine is less commonly used for obsessive-compulsive disorder than selective serotonin re-uptake inhibitors, in part because of the worse side-effect profile, but the drug should be considered for patients who do not tolerate selective serotonin re-uptake inhibitors for the treatment of obsessivecompulsive disorder. It is best to choose an antidepressant for which there is established efficacy for the primary or most impairing
TABLE 39-3 Representative Tricyclic Antidepressants Used in the Clinical Practice of Child Neuropsychopharmacology DRUG
PREPARATIONS
PHARMACOKINETICS
DOSING
Imipramine
Tofranil (imipramine hydrochloride) (10-, 25-, and 50-mg tablets) Tofranil-PM (imipramine pamoate) (75-, 100-, 125-, and 150-mg capsules)
Time to peak plasma conc = 1-2 hr Half-life = 8-16 hr
Nortriptyline hydrochloride
Pamelor (10-, 25-, 50-, and 75-mg capsules) Pamelor (10 mg/5 mL solution)
Time to peak plasma conc = 7-8.5 hr Half-life = 16-90 hr
Clomipramine hydrochloride
Anafranil (25-, 50-, and 75-mg capsules)
Time to peak plasma conc = 2-6 hr Half-life = 19-37 hr Time to steady state = 2-3 wk
Initiate at 25 mg/day and increase by 25 mg/day every 4-6 days while monitoring serum conc and electrocardiograms Therapeutic serum conc = combined serum concentration of imipramine and desipramine, 125 to 250 ng/mL Initiate at 10 mg/day and increase by 10 mg/day every 4-6 days while monitoring serum conc and electrocardiogram Therapeutic serum conc = 60-100 ng/mL Initiate at 25 mg/day and increase gradually while monitoring serum conc and electrocardiogram to a maximum dose of 3 mg/kg or 200 mg/day, whichever is lower
946
Neurobehavioral Disorders / 39
condition. However, in patients with co-occurring conditions, it is not unusual for the prescriber to consider use of a single agent to treat both conditions. In the rare circumstance when there is proven efficacy of one medication for two conditions—the selective serotonin re-uptake inhibitors fluoxetine or sertraline for obsessive-compulsive disorder and depression—such a strategy is reasonable. Clinicians commonly use bupropion for depression and ADHD based on bupropion’s proven efficacy for depression in adults and its activity on norepinephrine or dopamine. This approach may ultimately be useful for an individual child, but is not likely to be as consistently effective as using an appropriate medication combination for two conditions (i.e., selective serotonin re-uptake inhibitor and a stimulant). Although amitriptyline is commonly used in neurologic settings, its side-effect profile in doses effective for the treatment of anxiety and depression is often prohibitive—sedation and weight gain. The primary metabolite of amitriptyline, nortriptyline, is often better tolerated at treatment doses. Because clinical trials do not support the efficacy of amitriptyline or nortriptyline for anxiety or depression, they should not be considered first-line treatments. For children who cannot tolerate the selective serotonin re-uptake inhibitors or atypical antidepressants, tricyclic antidepressants should be considered, and of the tricyclic antidepressants, nortriptyline likely has a better side-effect profile at treatment doses. Nortriptyline also has the benefit of a target blood level for efficacy that is unique among the tricyclic antidepressants. Tricyclic antidepressants have been prescribed as third-line treatments for patients with ADHD who have failed adequate trials of stimulants, who could not tolerate the adverse effects of stimulants, and who had co-occurring conditions such as depression, anxiety, tic disorders [Wilens et al., 1993], or enuresis. Studies have demonstrated significant improvement in ADHD symptoms with imipramine, nortriptyline [Saul, 1985; Wilens et al., 1993], and desipramine [Biederman et al., 1986, 1989; Gastfriend et al., 1984]. However, tricyclic antidepressants appear to be less efficacious than methylphenidate [Rapoport et al., 1974], and they have been associated with a large dropout rate over time due to loss of efficacy or side effects [Quinn and Rapoport, 1975]. Studies of imipramine in the treatment of separation anxiety disorder and school refusal have yielded inconsistent findings [Bernstein et al., 2000; Gittelman-Klein, 1971; Klein et al., 1992]. Imipramine plus a psychologic intervention increased school attendance significantly more than the psychologic intervention plus placebo. Case reports describe usefulness of tricyclic antidepressants in the treatment of panic disorder [Ballenger et al., 1989; Black and Robbins, 1990; Garland and Smith, 1990], but no placebo-controlled trials have been done. Imipramine appears to be effective in treating enuresis as an initial agent [Fritz et al., 1994; Poussaint and Ditman, 1965; Rapoport et al., 1980] and in children who have failed nonpharmacologic interventions and desmopressin [Gepertz and Neveus, 2004]. Efficacy appears to be correlated with serum concentration [Fritz et al., 1994]. Clomipramine is approved for the treatment of obsessivecompulsive disorder in adults and children older than 10 years. In short-term clinical trials, clomipramine has
demonstrated superiority over placebo [DeVeaugh-Geiss et al., 1992; Leonard et al., 1989] in reducing symptoms of obsessive-compulsive disorder and preventing relapse [Leonard et al., 1991]. Improvement in clomipramine-treated subjects was sustained during 1-year open treatment [DeVeaugh-Geiss et al., 1992].
Pharmacology Tricyclic antidepressants are divided into two groups based on the number of methyl groups bonded to the nitrogen atom of the side chain. Tertiary amines (i.e., imipramine, amitriptyline, clomipramine, trimipramine, and doxepin), which have two methyl groups, are metabolized into secondary amines. Several secondary amines, which have one methyl group, are marketed as independent entities, including desipramine (imipramine), nortriptyline (amitriptyline), and protriptyline (trimipramine). Tricyclic antidepressants differ from each other in their ability to block the re-uptake of norepinephrine and serotonin (5HT) and act as competitive antagonists at muscarinic, histaminic (H1), and adrenergic (α1, α2) receptors. Their therapeutic mechanism of action is thought to result from their effect on norepinephrine and serotonin systems in the CNS. Clomipramine distinguishes itself from other tricyclic antidepressants in its relatively potent inhibition of serotonin re-uptake in addition to its noradrenergic activity. Their central and peripheral activity at muscarinic, histaminic, and adrenergic receptors is not thought to be involved in the clinical response but rather is associated with side effects. Tricyclic antidepressants are well absorbed in the gastrointestinal tract. Tricyclic antidepressants are metabolized in the liver by the cytochrome P-450 system. Although multiple isoenzymes are involved in their metabolism (i.e., CYP1A2, CYP2D6, CYP3A4, and CYP2C), the CYP2D6 isoenzyme is of particular importance. About 7% of the population are poor metabolizers, with reduced activity of CYP2D6. This results in increased plasma concentrations of tricyclic antidepressants and other medications metabolized by CYP2D6 compared with most of the population. Several medications can inhibit or induce the activity of the cytochrome P-450 isoenzymes. Co-administration of the tricyclic antidepressants with medications that inhibit cytochrome P-450 can result in clinically significant interactions. These drug interactions may result in discernible changes in efficacy or exacerbation of common tricyclic antidepressant side effects, but coadministration of tricyclic antidepressants with medications that specifically inhibit the respective cytochrome P-450 pathway may result in elevated blood levels leading to silent but potentially significant impact on cardiac conduction (i.e., prolonged QTc interval). Electrocardiographic monitoring is required for patients taking such drug combinations.
Clinical Management ASSESSMENT As with ADHD, the assessment for anxiety disorders and depression requires gathering information from multiple
Lee and Walkup / Neuropsychopharmacology
sources, including the child, parents, school, therapist, and others involved with the child. Information can be gathered through clinical interview, other informants, self-reports, and medical evaluation, including laboratory screening [AACAP, 1997c]. Diagnostic criteria for anxiety disorders and depressive disorders are detailed in the DSM-IV [APA, 1994]. The diagnostic evaluation of children with depression and anxiety should also determine whether other coexisting conditions are present. Risk factors for adverse effects with tricyclic antidepressants should be identified: family and personal history of bipolar disorder; nonvasovagal syncope, history of cardiac disease (especially arrhythmias, conduction abnormalities, and sudden death); use of concomitant medications; hepatic disease; pregnancy; and narrow-angle glaucoma. A medical evaluation is required before initiating tricyclic antidepressants. A physical examination should have been completed within the past 1 year. A baseline ECG, orthostatic blood pressure and heart rate, complete blood cell count, electrolyte determination, renal and hepatic functions, thyroid function tests, and urinalysis should be performed [Green, 1995]. Other laboratory screening measures may be indicated based on findings in the history or physical examination.
INITIATION AND TITRATION OF TRICYCLICS Because there is large variability in plasma drug concentration with a given dose of imipramine among individuals, monitoring of serum concentration has been recommended [Biederman et al., 1989]. A combined serum concentration of imipramine and desipramine in the range of 125 to 250 ng/mL is considered therapeutic. Higher serum concentrations in this range have correlated with higher response rates compared with placebo in the treatment of pediatric depression. Serum concentrations greater than 250 ng/mL have not improved response rates and were associated with increased side effects [Preskorn et al., 1989]. Because of the risk of adverse cardiac effects, serial ECGs are recommended with the use of all tricyclic antidepressants. They should be obtained at baseline, at the middle point in titration, and at the final dose [Elliot and Popper, 1990/1991]. The following parameters have been suggested as safety parameters for cardiovascular monitoring: PR interval: no greater than 210 milliseconds QRS interval: widening no greater than 30% above baseline QTc interval: less than 450 milliseconds Heart rate: maximum of 130 beats per minute Systolic blood pressure: maximum of 130 mm Hg Diastolic blood pressure: maximum of 85 mm Hg Imipramine may be initiated at 25 mg and increased by 25 mg every 4 to 6 days while monitoring serum concentration and ECGs. Nortriptyline is not approved for use for any indication in children, but its use in limited studies did not appear to result in serious adverse effects [Geller et al., 1989, 1992]. Nortriptyline may be initiated at 10 mg/day and increased by 10 mg/day every 4 to 6 days. In adolescents, a total dose of 30 to 50 mg/day is recommended; however, there may
947
be value in monitoring serum concentrations [Geller et al., 1986]. The therapeutic range for nortriptyline is 60 to 100 ng/mL [Geller and Carr, 1988; Geller et al., 1987]. ECGs should be obtained at baseline and after steady-state plasma levels are achieved [Geller et al., 1987]. Clomipramine may be initiated at 25 mg/day and increased gradually over the course of 2 weeks to a maximum dose of 100 mg/day or 3 mg/kg/day, whichever is less. After 2 weeks, the dose may be gradually increased to 200 mg/day or 3 mg/ kg/day, whichever is less. To allow tolerance to side effects and to avoid toxicity, slow titration is recommended after the first 2 weeks, because steady-state plasma concentrations may not be reached for 2 to 3 weeks. Total daily dosing above 3 mg/kg/day should be avoided because of the increased risk of seizures. ECGs should be obtained at baseline and when steady-state plasma levels are obtained.
Adverse Effects Side effects of tricyclic antidepressants include sedation, weight gain, orthostatic hypotension, and anticholinergic side effects (i.e., dry mouth, constipation, blurred vision, and urinary retention). Serious anticholinergic effects may occur, including paralytic ileus, exacerbation of narrowangle glaucoma, and the anticholinergic syndrome (“mad as a hatter, dry as a bone, blind as a bat, hotter than a hare”) [Sadock and Sadock, 2003]. Six sudden deaths have been reported for children taking antidepressant medications [Riddle et al., 1993; Zimnitzky, 1994]. Five were taking desipramine, and one was taking imipramine. Although the role of the tricyclic antidepressants in these tragic deaths is unclear, it has been speculated that the cause of death was cardiac in nature, most likely due to malignant arrhythmias. After the reports, child psychiatrists have become more cautious about prescribing tricyclics in general, carefully screening patients at risk for adverse effects and monitoring cardiac status with serial ECGs [Elliot and Popper, 1990/1991]. It is not clear whether the vulnerability to such medication effects can be determined from routine monitoring of cardiac function. Those who experience increased QTc above that which is considered safe while on tricyclic antidepressants should be monitored closely, and the dose should be adjusted downward until resolution of QTc prolongation. Behavioral side effects include early and acute increases in anxiety or depression. Tricyclic antidepressants may also induce manic episodes or rapid cycling in patients with a history of bipolar disorder. A family history of bipolar disorder may be a risk factor for this effect, but such a history is not a contraindication for the use of antidepressants. A discontinuation syndrome (e.g., flulike syndrome with nausea, headache, and malaise), hypomania, or mania may result from abrupt cessation of tricyclic antidepressants [Sadock and Sadock, 2003]. The Food and Drug Administration mandated a black box warning regarding increases in suicidal ideation for all antidepressants (see “Selective Serotonin Re-uptake Inhibitors”).
Drug Interactions Tricyclic antidepressants have multiple drug interactions. The product information for each of the tricyclic anti-
948
Neurobehavioral Disorders / 39
depressants provides detailed information regarding specific drug interactions. A combination of tricyclic antidepressants and monoamine oxidase inhibitors can precipitate a hypertensive crisis requiring immediate medical treatment. Early signs and symptoms include headache, stiff neck, palpitations, sweating, nausea, and vomiting [Sadock and Sadock, 2003]. Medications that inhibit CYP2D6 activity such as fluoxetine, paroxetine, and haloperidol (refer to prescribing information for other inhibitors) result in increased serum concentrations of tricyclic antidepressants and increased risk for tricyclic antidepressant side effects. Decreased serum concentrations may be caused by cigarette smoking, lithium (Eskalith), ascorbic acid, ammonium chloride, barbiturates, and primidone. Oral contraceptives may induce hepatic enzymes and decrease tricyclic antidepressant serum concentrations. Tricyclic antidepressants may block the activity of antihypertensives (e.g., guanethidine, propranolol, clonidine). Tricyclic antidepressants may increase the sedative effects of other drugs such as over-the-counter cold medications, alcohol, opioids, anxiolytics, and hypnotics [Sadock and Sadock, 2003].
Selective Serotonin Re-uptake Inhibitors Clinical Applications The selective serotonin re-uptake inhibitors, including citalopram, escitalopram, fluvoxamine, fluoxetine, paroxetine, and sertraline, have Food and Drug Administration indications for a number of mood, anxiety, and eating disorders in adults (Table 39-4). In children, fluoxetine, fluvoxamine, and sertraline have a Food and Drug Administration indica-
tion for obsessive-compulsive disorder; fluoxetine also has a Food and Drug Administration indication for major depression. These indications are based on large-scale, randomized, controlled trials for obsessive-compulsive disorder [Geller et al., 2001; March et al., 1998; Riddle et al., 2001] and major depression [Emslie et al., 1997, 2002]. Other large, randomized, controlled trials of the agents have been completed, but not all have been published. Published trials demonstrating efficacy include citalopram for depression [Wagner et al., 2004]; fluoxetine [Birmaher et al., 2003] and fluvoxamine for separation, social, and generalized anxiety [RUPP, 2001]; sertraline for depression [Wagner et al., 2003] and generalized anxiety [Rynn et al., 2001]; and fluoxetine for stereotypies in children with autistic spectrum disorder [Hollander et al., 2001]. The use of the selective serotonin re-uptake inhibitors for depression and anxiety disorder has increased significantly over the past 10 years, with upward of 1% to 2% of teens currently taking these medications for all indications [Olfson et al., 2002]. Despite the marked increase in use, the prevalence of disorders in children and adolescents that are potentially responsive to the selective serotonin re-uptake inhibitors (e.g., depression and anxiety disorders) is much greater (minimum prevalence of 3% to 5%) than the number of children who are taking these medications (1% to 2%), suggesting overall undertreatment. However, this upward trend may be short lived. In response to finding an increased incidence of suicidal thoughts and behaviors in the large, controlled trails of antidepressants (including selective serotonin re-uptake inhibitors), the Food and Drug Administration began requiring a black box warning in the product information for
TABLE 39-4 Selective Serotonin Re-uptake Inhibitors DRUG
PREPARATIONS
PHARMACOKINETICS
DOSING
Citalopram
Celexa (20- and 40-mg scored tablets)
Initiate at 10 or 20 mg/day; titrate to maximum of 40 mg/day
Escitalopram
Lexapro (5-mg tablet; 10- and 20-mg scored tablets)
Fluoxetine
Prozac (10-mg scored tablet; 10-, 20-, and 40-mg pulvules; 20 mg/5 mL liquid)
Fluvoxamine
Luvox (50- and 100-mg scored tablets)
Paroxetine
Paxil (10- and 20-mg scored tablets; 30- and 40-mg tablets; 10 mg/5 mL suspension)
Time to peak conc = 4 hr Half-life = 35 hr Time to steady state = 1 wk Linear kinetics with dosage ↑ Time to peak conc = 5 hr Half-life = 27-32 hr Time to steady state = 1 wk Linear kinetics with dosage ↑ Time to peak conc = 6-8 hr Half-life (chronic administration) = 7 days (fluoxetine), = 16 days (norfluoxetine) Time to steady state = 4-6 wk Nonlinear kinetics with dosage ↑ Time to peak conc = 8 hr Half-life = 15 hr Time to steady state = 10-14 days Linear kinetics at low dose Nonlinear kinetics at high dose Time to peak conc = 5 hr Half-life = 21 hr Time to steady state = 10 days Nonlinear kinetics with dosage ↑
Sertraline
Zoloft (25-, 50-, and 100-mg scored tablets; 20 mg/mL concentrate)
Time to peak conc = 4-8 hr Half-life = 26 hr Time to steady state = 1 wk Linear kinetics with dosage ↑
No clinical trials in pediatric population Adult dosing: 10-20 mg/day, up to 30 mg/day in partial responders Initiate at 10 mg/day; after 1-2 wk, increase to 20 mg/day; increase to 30 mg or 40 mg/day at week 4-6 if indicated Initiate at 25 or 50 mg/day; increase by 50 mg weekly to maximum of 200 mg/day Average treatment dose in clinical trials = 150-200 mg/day Initiate at 5 mg/day Adult dosing: initiate at 20 mg/day; increase by 10 mg/day every 7-10 days; maximum dose = 50 mg/day Initiate at 25 or 50 mg/day; maximum dose = 200 mg/day
Lee and Walkup / Neuropsychopharmacology
all antidepressants as of January 28, 2005. They also mandated a change in how antidepressants are delivered from the pharmacy to the patient and required a medication guide to be delivered to consumers every time a prescription is picked up at the pharmacy. The black box warning describes the potential increased risk for suicidal ideation and behavior and the need for careful monitoring early in the course of treatment. No longer supplied in bulk to pharmacies, antidepressants instead are provided in unit packaging that contains a predetermined amount of medication. Inside each unit, a medication guide provides consumers with information regarding depression, suicide, the risk for suicidality early in the course of treatment, and strategies for monitoring worsening of depression or suicidal thoughts or behaviors.
Pharmacology PHARMACODYNAMICS The pharmacodynamic profiles of the selective serotonin reuptake inhibitors are very similar. Their beneficial effects are purported to be associated with their ability to block neuronal re-uptake of serotonin and the low side-effect profile is associated with their low affinity for other receptors. Although some individuals may do better on one selective serotonin re-uptake inhibitor than another, comparative treatment trials suggest similarity in efficacy across all agents in this class. The selective serotonin re-uptake inhibitors may demonstrate benefit in as little as 1 week, with substantial benefit occurring in 8 to 12 weeks. Improvement may continue at a more gradual rate for up to 6 to 12 months. Despite the similarity in pharmacodynamics, the selective serotonin re-uptake inhibitors are very different in chemical structure and pharmacokinetics in ways that may impact their use. Very little is known about the pharmacodynamics or pharmacokinetics of the selective serotonin re-uptake inhibitors in children. The following information pertains to adults unless stated otherwise.
PHARMACOKINETICS Citalopram Peak blood levels of citalopram (Celexa) occur at about 4 hours, with a half-life of about 35 hours. Single- and multiple-dose pharmacokinetics of citalopram are linear throughout the standard dose range (10 to 60 mg/day). Steadystate plasma concentrations are reached in approximately 1 week. Citalopram is metabolized in the liver to a number of mostly inactive metabolites. Citalopram appears to have limited ability to inhibit cytochrome P-450 isoenzymes; inhibition of these isoenzymes is primarily responsible for the demethylation of citalopram. CYP3A4 and CYP2C19 do not appear to significantly affect citalopram blood levels or halflife. The (S)-enantiomer of citalopram is mostly responsible for the serotonin re-uptake [Celexa, 2004].
Escitalopram Escitalopram (Lexapro) is the (S)-enantiomer of a 50:50 racemic mixture of (R)- and (S)-enantiomers of citalopram. The (S)-enantiomer in escitalopram is approximately 100 times more potent at serotonin re-uptake inhibition than the (R)-enantiomer. The peak blood level of escitalopram is
949
reached at about 5 hours; the half-life is 27 to 32 hours. Steady state is achieved in about 1 week. The pharmacokinetic profiles of escitalopram for single and multiple doses are linear in the range of doses used clinically (10 to 30 mg/day). Escitalopram is metabolized primarily in the liver by CYP3A4, CYP2C19, and other enzymes. The primary metabolites are found in lesser concentrations in the plasma than escitalopram and are not thought to be clinically active. Similar to citalopram, it is not anticipated that escitalopram will inhibit cytochrome P-450 or be inhibited by medication that inhibits the cytochrome P-450 system [Lexapro, 2004].
Fluoxetine Fluoxetine (Prozac) [Simeon et al., 1986] reaches peak plasma levels approximately 6 to 8 hours after oral administration and is almost completely protein bound. Fluoxetine is extensively metabolized in the liver to norfluoxetine (active metabolite) through a variety of isoenzymes of the cytochrome P-450 system. The kinetic profiles are generally nonlinear, with chronic plasma levels not directly linked to dose. With chronic administration, the half-life of fluoxetine and norfluoxetine increases to 7 days and up to 16 days, respectively. Steadystate concentrations are therefore delayed for up to 4 to 6 weeks. This long duration of activity can have potential benefits (e.g., ongoing medication exposure with occasional missed doses and single-dose weekly administration for the sustained-release fluoxetine) and some risks—side effects may emerge as the plasma level increases 4 to 6 weeks after initiation of treatment, and newly prescribed medications may interact with fluoxetine or norfluoxetine for up to 4 weeks after fluoxetine discontinuation. The prolonged half-life may be problematic for patients who do not tolerate the medication, develop manic reactions, or have other problematic behavioral side effects [Hoehn-Saric et al., 1990, 1991] when the need to discontinue and clear the medication from the body is critical.
Fluvoxamine Fluvoxamine (Luvox) reaches peak plasma levels in up to 8 hours after oral administration and up to 12 hours with the extended-release preparation. Pharmacokinetic profiles are nearly linear in the lower range of treatment doses, with a loss of linearity with higher doses. The half-life of fluvoxamine increases slightly from 15 hours to between 17 and 22 hours after single and multiple doses, respectively. Steady-state plasma levels are usually achieved within 10 to 14 days. Fluvoxamine undergoes extensive metabolism in the liver to a number of clinically inactive metabolites, but the specific cytochrome P-450 isoenzymes involved are unknown. Fluvoxamine does inhibit CYP1A2 and, to a lesser extent, CYP3A4 and CYP2D6, resulting in potentially significant drug interactions, including tertiary amine tricyclic antidepressants (e.g., imipramine, clomipramine), some benzodiazepines, propranolol, warfarin, and theophylline [van Harten, 1995]. Pharmacokinetic studies suggest that children, especially young girls, metabolize fluvoxamine more slowly and that they therefore may require lower treatment doses [Labellarte et al., 2004].
Paroxetine Paroxetine (Paxil) reaches peak plasma concentrations at approximately 5 hours, and the average terminal half-life is about 21 hours after chronic administration of 30 mg/day.
950
Neurobehavioral Disorders / 39
Steady-state paroxetine plasma levels are reached after about 10 days. Pharmacokinetics were nonlinear for multiple dosing and approximately eight times what would be expected based on single-dose kinetics. A nonlinear kinetic profile results from the saturation of CYP2D6, which is primarily responsible for paroxetine metabolism. Paroxetine undergoes extensive first-pass metabolism to a number of metabolites, none of which appears to have any significant clinical activity. Paroxetine appears to be a strong inhibitor of cytochrome P-450, which suggests the potential for clinically meaningful drug-drug interactions. Pediatric data suggest that children metabolize paroxetine more quickly than adults but that oncedaily dosing is likely adequate [Findling et al., 1999].
Sertraline Sertraline (Zoloft) reaches peak plasma concentrations at approximately 4 to 8 hours after a 2-week period of oral administration, with an average terminal half-life of about 26 hours. Steady-state sertraline plasma levels are reached after about 1 week. Pharmacokinetic profiles were linear for single doses in the treatment range of 50 to 200 mg/day. Sertraline undergoes extensive first-pass metabolism by multiple cytochrome P-450 isoenzymes to N-desmethylsertraline, which is substantially less clinically active than sertraline. Sertraline appears not to be a strong inducer or inhibitor of cytochrome P-450; coupled with the fact that sertraline is metabolized by multiple isoenzymes, this suggests that few clinically meaningful drug-drug interactions should occur. Pediatric data suggest that although children metabolize sertraline more quickly than adults, they may require lower doses because of their lower body weight to avoid excessive plasma levels.
Clinical Management ASSESSMENT The assessment of mood and anxiety disorders before initiation of a selective serotonin re-uptake inhibitor is similar to that described earlier for the tricyclic antidepressants. Assessment requires gathering information from multiple sources, including the child, parents, school, therapist, or others involved with the child. Information can be gathered through clinical interview, other informants, self-reports, and medical evaluation, including laboratory screening [AACAP, 1997a]. Diagnostic criteria for anxiety disorders and depressive disorders are detailed in the DSM-IV [APA, 1994]. The diagnostic evaluation should pay particular attention to conditions that may coexist with depression, such as anxiety disorders and ADHD. Risk factors for adverse effects of selective serotonin re-uptake inhibitors should be identified and include a family and personal history of bipolar disorder, history of suicidal ideation or behavior, sensitivity to other selective serotonin re-uptake inhibitors, concurrent medications that could inhibit or could be inhibited by the selective serotonin re-uptake inhibitor, pregnancy, and hepatic or renal disease. No medical evaluation is required before initiating selective serotonin re-uptake inhibitor treatment, but it may be prudent to medically clear a child by means of a medical history and physical examination, including baseline height and weight and targeted laboratory examination as indicated by the history or physical examination findings.
INITIATION AND TITRATION OF DOSE For all of the selective serotonin re-uptake inhibitors, treatment usually is initiated with a low dose that is adjusted upward slowly at weekly intervals. Because the time-response pattern for the selective serotonin re-uptake inhibitors occurs over a minimum of weeks, aggressive titration often leads to early side effects and may result in early discontinuation of the medication and the need to start again with another medication. Starting low and slowly titrating may allow the patient time to develop some tolerance to some of the side effects. However, the risk of starting with low doses and proceeding slowly is going too slowly and leaving patients undertreated. Dosing of selective serotonin reuptake inhibitors is usually recommended in the morning because of activating side effects and in the evening for individuals who feel sedated on the medication.
Citalopram Citalopram comes in 20- and 40-mg scored tablets. Treatment doses range from 10 to 60 mg/day in adults. In industry-sponsored clinical trials of citalopram in children, patients were started on 20 mg/day, with the option for going up to 40 mg/day at week 6. Citalopram 20-mg tablets are scored, allowing beginning doses of 10 mg/day.
Escitalopram Escitalopram comes in 5-, 10-, and 20-mg tablets. The 10and 20-mg tablets are scored. There are no published controlled trials to guide dosing in children. Standard adult dosing is 10 to 20 mg/day, with higher doses (30 mg/day) used only in those who have had a partial response.
Fluoxetine Fluoxetine comes in 10-, 20-, and 40-mg pulvules; 10-mg scored tablets; and Prozac Weekly, which contains approximately 90 mg of fluoxetine in a time-released preparation. Fluoxetine is also available in a liquid (20 mg/5 mL). In most clinical trials of fluoxetine in children and adolescents, dosing began at 10 mg/day for 1 to 2 weeks, with a subsequent increase to 20 mg. The dose is often held at this level up to 4 to 6 weeks before going to 30 or 40 mg/day [TADS, 2004]. Doses as high as 60 mg/day have been used in clinical trials, but maximum doses are used only if this dose is reached after a patient has demonstrated partial benefit after 10 to 12 weeks of treatment [TADS, 2004].
Fluvoxamine Fluvoxamine comes in 25-, 50-, and 100-mg scored tablets. In clinical trials of fluvoxamine in children, dosing began at 25 or 50 mg/day and increased by 50 mg on a weekly basis to a maximum dose of up to 200 mg/day. Average therapeutic doses at the end of treatment were between 150 and 200 mg/day [Riddle et al., 2001]. This method of titration often leads to the highest safe dose rather than least effective dose. Aggressive titration may lead to increased side effects early in treatment. With slower dosage adjustment, it may be possible to establish benefit at lower doses. This is particularly true for prepubertal children (especially girls) who may metabolize fluvoxamine more slowly and have higher blood levels than teens and adults [Labellarte et al., 2004].
Lee and Walkup / Neuropsychopharmacology
Paroxetine Paroxetine comes in 10-, 20-, 30-, and 40-mg tablets. The 10- and 20-mg tablets are scored. Paroxetine is also available in a suspension of 10 mg/5 mL. In adults, initial treatment can begin with 20 mg, given once daily in the morning or evening. Doses are increased by 10 mg/day every 7 to 10 days to a maximum dose of 50 mg. In clinical trials, final doses for adults ranged from 20 to 50 mg/day. For children, dosing can start as low as 5 mg/day.
Sertraline Sertraline comes in 25-, 50-, and 100-mg scored pills or tablets and in a concentrate of 20 mg/mL. Generally, 50 mg/day given as a single dose appears to be as effective as other doses for most conditions. Dosing can begin at 25 or 50 mg/day. For those who do not respond or only partially respond, higher doses may be necessary. Clinical trials enrolling adults and children using sertraline have usually used doses up to 200 mg/day as tolerated. One clinical trial of sertraline in children demonstrated efficacy on a fixed dose of 50 mg/day [Rynn et al., 2001].
Adverse Effects COMMON EFFECTS The product information for each medication should be consulted for a comprehensive review of adverse events and warnings. Given the similar pharmacodynamic properties of the selective serotonin re-uptake inhibitors, it is not surprising that their side-effect profiles are also very similar. Although many side effects are reported to have occurred in placebocontrolled trials of the selective serotonin re-uptake inhibitors, a few side effects occurred significantly more often on active medication than on placebo. These include nausea or other gastrointestinal symptoms, insomnia, and anxiety or agitation. Other side effects that occur more often on active medication but are less common overall include apathy or somnolence, tremor, sweating, sexual dysfunction, and allergic reactions, including rash. The most common causes of medication discontinuation other than lack of efficacy are the behavioral or psychiatric side effects such as anxiety or agitation. Although clinicians usually think of side effects as physical changes such as dry mouth, constipation, and sedation, for selective serotonin re-uptake inhibitors, the behavioral and psychiatric side effects and their impact on growth and development are a greater concern and require review with the patient and parent before starting treatment [Walkup and Labellarte, 2001]. Perhaps the most important of these side effects is activation, which occurs in about 10% to 20% of patients [March et al., 1998; RUPP, 2001]. This activation syndrome (distinct from the mood improvement effects of the antidepressants) can result in a number of complaints, including anxiety, increased activity level or akathisia, increased impulsivity, and disinhibition. This activation is very similar to what some children experience when they take diphenhydramine. Activation effects usually appear very early in treatment or after a dose change. When mildmannered children present with an increased activity level, the reaction can be clinically significant and debilitating. Patients do not appear to develop tolerance to these symp-
951
toms, but they resolve with dose reduction or discontinuation, which is consistent with the pharmacokinetics of the medication. Much less common but also serious are manic and hypomanic reactions. Manic reactions (1% to 2%) are much less common than activation, occur later in treatment after a period of improvement, do not always go away with dose reduction or discontinuation, and may require medical intervention to control. Core symptoms of mania include decreased need for sleep, euphoria, and grandiosity. It is critical to differentiate activation effects from manic reactions as activation effects likely have little prognostic significance beyond potential sensitivity to other selective serotonin reuptake inhibitors, whereas manic reaction may have prognostic significance for the later development of mania. Children with anxiety and mood disorders who benefit from selective serotonin re-uptake inhibitor treatment do not always have uniform outcomes. For most, symptom relief is associated with return to normal and appropriate function. However, some children, especially those with behavioral problems or those at risk for other behavioral problems (i.e., poor parental discipline and monitoring), may present with increasing behavior problems after successful treatment of anxiety and depression. For example, a child with severe oppositional behavior may have a reduction of such behavior during a depressive episode due to psychomotor slowing or social withdrawal but may actually have more behavioral difficulties with normalization of mood or decreased anxiety. Parents of youngsters at risk for or with a history of behavior problems need to be more active about structure and to limit settings to manage the behavioral difficulties that can complicate recovery. Children with anxiety and mood disorders also experience an evolution of symptoms over time. Children first presenting with separation anxiety at age 8 years may evolve into a generalized anxiety disorder or have periods of recurrent depression in their middle to late teens. Because this can occur during the course of treatment, parents may be confused about whether medication treatment actually causes these changes in the progression of symptoms. Educating the patient and family regarding the progression of symptoms and the course of illness and treatment is helpful so that changes in the clinical course are to some degree anticipated and can be dealt with more easily. The selective serotonin re-uptake inhibitors have also been reported to induce an apathy syndrome. Although it may manifest early in treatment, those with anxiety and depression may not be sensitive to this subtle medication effect until after a period of recovery. Awareness of the potential for apathy improves the likelihood that it will be recognized. Even though patients who have experienced apathy can readily differentiate it from depression or sedation, careful interviewing may be required to make these differentiations. Apathy responds to dose reduction; however, dose reductions required to eliminate apathy may lead to loss of symptom control. Patients who report loss of response, not feeling like themselves, or feeling better but numb or who appear to have lost interest in living without significant depressive symptoms should be interviewed closely to assess for apathy [Hoehn-Saric et al., 1990]. Sexual side effects are not commonly documented in clinical trials with children and adolescents, but in clinical
952
Neurobehavioral Disorders / 39
practice, it is not uncommon for physicians to find that teens begin to spontaneously complain about sexual side effects when they become sexually active in high school or college. Awareness of sexual side effects can make it more likely that these effects are identified and managed and that that they will not lead to discontinuation and loss of treatment response. Dose reduction, changing to antidepressants with a lower risk for sexual side effects, or the addition of medication that may improve sexual function (i.e., bupropion or Viagra) have all been reported to be effective [Woodrum and Brown, 1998]. Although epistaxis is common in children and adolescents, some children experience increased rate or severity of epistaxis and increased bruising. Such changes appear to be an effect of the selective serotonin re-uptake inhibitors on platelet functions, not on coagulation factors [Lake et al., 2000]. Selective serotonin re-uptake inhibitors, specifically fluoxetine, have been associated with change in the rate of linear growth. This was first reported in a small case series and confirmed in a review of the large fluoxetine database. It appears that the deceleration of growth stopped with medication discontinuation and recurred in one case when the medication was restarted. It is not clear whether this is an effect of all the selective serotonin re-uptake inhibitors or specific to fluoxetine. It also appears that this effect is mediated by suppression of growth hormone and is not mediated by reduction in appetite, as can occur with the stimulants. It does not appear to uniformly affect all children. Because the follow-up period is relatively short, it is unclear whether children can catch up while on medication or whether medication discontinuation is required for children to obtain their optimal height [Weintrob et al., 2002]. Although there are no data to suggest that selective serotonin re-uptake inhibitor treatment leads to drug-seeking behavior (i.e., addictive), some individuals do appear to have a discontinuation syndrome with abrupt discontinuation [Ditto, 2003]. There are three complications to abrupt discontinuation. The first complication is a withdrawal reaction that includes flulike symptoms, such as malaise and gastrointestinal symptoms, but it may also include unusual symptoms such as sensory or psychologic disturbances. Some patients with abrupt discontinuation also experience an abrupt return of symptoms, including suicidal risk. Ironically, case reports suggest that abrupt discontinuation of antidepressants can be associated with hypomanic reactions. Such a patient may initially report feeling much better off of medication and be reluctant to resume medication treatment. Antidepressants with shorter half-lives appear to be more commonly associated with discontinuation syndromes than selective serotonin re-uptake inhibitors with longer halflives.
ANTIDEPRESSANTS AND SUICIDE RISK Antidepressants have long carried warnings in their product labeling regarding the increased risk for suicidal ideation and behavior (i.e., suicidality) early in the course of treatment. The mechanism of this effect has never been clear, but it is commonly attributed to the positive energizing effects of antidepressants outpacing the improvement in
mood and suicidality. For example, a patient with depression, psychomotor retardation, and suicidality when treated with antidepressants may experience increased energy and be capable of acting on suicidal impulses. After approximately 10 years of market exposure, concerns about the development of suicidality on antidepressants, especially the selective serotonin re-uptake inhibitors, prompted a complete review by the British Medical and Healthcare Product Regulatory Agency and the U.S. Food and Drug Administration and ultimately led to stronger warnings within the product information. In the United States, this means that all antidepressants must carry a black box warning regarding the risk for suicidality while on antidepressants early in the course of treatment and the need for close monitoring. In the United States, antidepressants are packaged in unit doses (i.e., month-supply bottles), and each unit includes a medication guide for the patient. The data on which these new warnings are based include more than 24 randomized, controlled clinical trials (>4000 subjects) of the newer non-tricyclic antidepressants completed for the purpose of extended exclusivity under the Food and Drug Administration Modernization Act [FDAMA, 1997]. Although a number of methodologic limitations plague the analysis of these studies, it appears that there is a small but significant increased risk for more suicidality adverse events on active medication (about four events per 100 patients) versus placebo (about two events per 100 patients). There does not appear to be a groupwise risk for emergence or worsening of suicidal behavior for the medications, but the data do support an association with activation syndrome. Although the risk appears to be small (number needed to harm is about 50), the fact that in these same studies there is marginal antidepressant efficacy suggests that more caution is required when considering the use of these medications. In contrast to the industrysponsored studies completed for exclusivity, NIH-funded studies of the treatment of depression and anxiety in children suggest significant benefit for the selective serotonin re-uptake inhibitors [Birmaher et al., 2003; Emslie et al., 1997; RUPP, 2001; TADS, 2004]. The big difference between industry-sponsored and NIH-sponsored clinical trials is the large placebo response rate in industrysponsored trials, with resulting smaller sizes of effect than those observed in NIH-funded trials. The increased risk for suicidality previously observed was principally seen in depressed patients, and its use for other indications such as anxiety or for the treatment of children with autism may not share this increased risk. This may be an important consideration for child neurologists, because they are more likely to use selective serotonin re-uptake inhibitors for such purposes. The risk for suicide is higher overall among teenagers and less so in younger children.
Drug Interactions The product information for each of the selective serotonin re-uptake inhibitors provides detailed information regarding specific drug interactions. Because the number of individual interactions is too high to describe here, general principles are discussed. Adverse drug-drug interactions occur most commonly with highly protein-bound medications and with medications that significantly inhibit or induce cytochrome
Lee and Walkup / Neuropsychopharmacology
P-450 isoenzymes. Drug-drug interactions can result in loss (e.g., anticonvulsant combinations) or increase in benefit (e.g., cyclosporine and ketoconazole), increase in noticeable side effects (e.g., sedation), and an increase in side effects that can only be identified with careful monitoring (e.g., QTc prolongation). As a class, the selective serotonin reuptake inhibitors have more and more frequent drug-drug interactions because most of the selective serotonin reuptake inhibitors inhibit cytochrome P-450 isoenzymes. Most result in increased benefit of the co-administered agent or increase in noticeable side effects. The caution with using the selective serotonin re-uptake inhibitors is when they are combined with medications that have silent side effects such as QTc prolongation effects. Ironically, medications used in neuropsychiatry such as the antipsychotics (e.g., pimozide) and tricyclic antidepressants (e.g., desipramine) have a potential for producing cardiac conduction effects. Caution is warranted and monitoring is indicated when using selective serotonin re-uptake inhibitors in combination with medication that may affect the QTc interval.
Other Antidepressants Bupropion CLINICAL APPLICATIONS Bupropion (Wellbutrin, Zyban) is approved for the treatment of depression, nicotine dependence, and smoking cessation in adults [Wellbutrin, 2002]. Off-label uses of bupropion include monotherapy in the treatment of depression in children and adolescents, augmentation of selective serotonin reuptake inhibitor therapy in the treatment of depression [Lam et al., 2004], management of selective serotonin re-uptake
953
inhibitor–induced sexual side effects [Masand et al., 2001], and as a second-line agent in the treatment of ADHD. Bupropion appears to improve symptoms of ADHD in prepubertal children [Casat et al., 1989; Simeon et al., 1986]. Effect sizes of bupropion and placebo differences were smaller than for standard stimulant medications [Casat et al., 1989]. However, bupropion appeared to have comparable efficacy compared with methylphenidate in a double-blind, crossoverdesign study [Barrickman, 1995]. Adolescents with depression [Glod et al., 2003] and those with co-occurring ADHD with depression [Daviss et al., 2001] demonstrated improvement with bupropion.
PHARMACOLOGY Bupropion is available in immediate-release tablets (Wellbutrin, Zyban) and extended-release tablets (Wellbutrin SR, Wellbutrin XL). The mechanism of action in ameliorating depression is unknown. In animals, bupropion selectively inhibits noradrenergic neurons in the locus ceruleus and inhibits the re-uptake of dopamine, but it does not have significant activity at α-adrenergic, cholinergic, or histaminic receptors. Bupropion is well absorbed through the gastrointestinal tract, with a peak serum concentration attained in 2 to 3 hours and with a half-life of 14 to 21 hours. Steady-state concentrations are achieved in 8 days. Steady-state plasma levels achieved with the extended-release form were about 85% of the immediate-release preparation. Bupropion is 80% bound to serum albumin. It is metabolized by the liver (primarily by CYP2B6) and excreted in urine and feces. Although bupropion has been found to induce its own metabolism in animals, this has not been specifically studied in humans (Table 39-5) [Wellbutrin, 2002].
TABLE 39-5 Other Antidepressants Used in Clinical Practice of Child Neuropsychopharmacology DRUG
PREPARATION
PHARMACODYNAMIC ACTIONS
PHARMACOKINETIC PROPERTIES
Bupropion
Wellbutrin (75- and 100-mg tablets) Wellbutrin XR (100-, 150-, and 200-mg tablets) Wellbutrin XL (150- and 300-mg tablets)
Unclear effects on NE systems
Time to peak = 2-3 hr Half-life = 14-21 hr
Venlafaxine
Effexor (25-, 37.5-, 50-, 75-, and 100-mg tablets) Effexor XR (37.5-, 75-, and 150-mg extended-release capsules)
Mirtazapine
Remeron (15- and 30-mg scored tablets; 45-mg tablet) Remeron SolTab (15-, 30-, and 45-mg orally disintegrating tablets)
DA, dopamine; 5HT, serotonin; NE, norepinephrine
DOSING
Immediate release: initiate at 50 mg/day; increase by 50 mg/day weekly Optimum dose: 100-250 mg/day or 3-6 mg/kg/day, given bid at least 8 hr apart Maximum dose of 400 mg/day and 200 mg/dose (extended release); 450 mg/day and 150 mg/dose (immediate release) At low doses, inhibits 5HT Time to peak = 5.5 hr 1-3 mg/kg/day given in re-uptake (immediate release), = 9 hr divided doses bid or tid At high doses, inhibits 5HT (extended release) and NE uptake Half-life = 3.5 hr (immediate release), = 9 hr (extended release) Time to peak = 2 hr Initiate at 7.5 mg/day at Antagonism of 5HT2 and 5HT3 receptors Half-life = 20-40 hr bedtime; increase by Antagonism of α2-adrenergic 7.5 mg/day every 1-2 wk receptors, ↑ synaptic NE Maximum dose = 45 mg/day and 5HT levels
954
Neurobehavioral Disorders / 39
CLINICAL MANAGEMENT In addition to the standard assessment for ADHD or depression, possible risk factors for adverse effects should be identified. The risk of seizures increases with conditions that lower the seizure threshold, such as preexisting seizure disorder, anorexia and bulimia, head trauma, CNS tumor, concomitant use of medications that lower seizure threshold, excessive use of alcohol, abrupt withdrawal of alcohol or sedatives. Conditions that could raise bupropion levels, such as hepatic cirrhosis, increase the risk of seizures. No specific laboratory tests are recommended by the manufacturer before initiation. To minimize the risk of seizures, the manufacturer recommends that clinicians titrate bupropion slowly and divide the dose three times per day (immediate release), with each single dose no greater than 150 mg to avoid large peak serum concentrations. The dose should not exceed 450 mg/day for immediate-release preparations and 400 mg/day for extended-release preparations [Wellbutrin, 2002]. Bupropion has not been approved for use in children or adolescents. Bupropion may be initiated at 50 mg/day and increased by 50 mg/day at weekly intervals [Simeon et al., 1986]. Optimal doses in studies have ranged from 100 mg to 250 mg/day in prepubertal children [Clay et al., 1988; Simeon et al., 1986] or 3 to 6 mg/kg/day [Conners et al., 1996]. No incidence of seizure was reported in these studies. Short-term studies of 6 to 8 weeks have observed improvement of ADHD and depressive symptoms [Conners et al., 1996; Daviss et al., 2001; Glod et al., 2003]. If symptoms fail to respond to therapeutic doses of bupropion over this period, the medication should be tapered slowly to avoid adverse effects.
ADVERSE EFFECTS Common adverse effects include agitation, dry mouth, insomnia, headache, nausea, vomiting, constipation, and tremor [Wellbutrin, 2002]. Neuropsychiatric side effects have been observed in some patients, including psychotic symptoms and confusion. In general, antidepressants carry a risk of inducing manic symptoms in patients with bipolar affective disorder. The risk of inducing mania with bupropion is thought to be less than with tricyclic antidepressants and selective serotonin re-uptake inhibitors [Sadock and Sadock, 2003]. Bupropion has been reported to exacerbate tics in children with co-occurring ADHD and Tourette’s syndrome [Spencer et al., 1993]. Bupropion has been associated with seizures in approximately 0.4% of patients treated at doses up to 450 mg/day. The risk of seizures appears to be strongly associated with peak serum concentrations and dose. The incidence of seizures appears to increase significantly above daily doses of 450 mg and with rapid dose titration [Wellbutrin, 2002].
DRUG INTERACTIONS Because bupropion is metabolized by CYP2B6, plasma concentrations may increase if it is given concomitantly with inhibitors of this enzyme (e.g., orphenadrine, cyclophosphamide). Bupropion inhibits CYP2D6 and potentially
increases the plasma concentrations of other medications metabolized by this isoenzyme. The combination of bupropion with monoamine oxidase inhibitors may precipitate a hypertensive crisis. Both Wellbutrin and Zyban contain bupropion, and this combination is contraindicated because of an increased risk of seizure. Concurrent use of L-dopa and bupropion has been associated with an increased rate of adverse effects [Wellbutrin, 2002].
Venlafaxine CLINICAL APPLICATIONS Venlafaxine (Effexor) is approved for the treatment of major depressive disorder, generalized anxiety disorder, and social phobia in adults. Venlafaxine has also shown promise in the treatment of ADHD in adults [Findling et al., 1996] and cooccurring major depressive disorder and ADHD in adults [Hornig-Rohan and Amsterdam, 2002]. Studies of venlafaxine in children and adolescents are limited, and results have not been as promising as for adults. Children and adolescents treated with venlafaxine for major depressive disorder did not appear to benefit from medication compared with placebo [Mandoki et al., 1997]. In a group of children and adolescents with ADHD, venlafaxine was associated with improvements of behavioral (7 of 16 subjects) but not cognitive symptoms of ADHD; however, 3 of 16 patients had worsening of hyperactivity that precipitated drug discontinuation [Olvera et al., 1996].
PHARMACOLOGY Venlafaxine is available in immediate-release tablets (Effexor) and extended-release capsules (Effexor XR). At doses less than 150 mg/day, it selectively inhibits serotonin re-uptake. At higher dose, it inhibits serotonin and norepinephrine re-uptake. Venlafaxine does not have significant activity at muscarinic, histaminic, or α-adrenergic receptors. Venlafaxine is well absorbed through the gastrointestinal tract and is metabolized by the liver and excreted in the urine. The serum half-lives of venlafaxine and its active metabolite are about 5 and 11 hours, respectively (see Table 39-5) [Effexor, 2003].
ADVERSE EFFECTS Common side effects associated with venlafaxine include asthenia, sweating, nausea, constipation, anorexia, vomiting, somnolence, dry mouth, dizziness, nervousness, anxiety, tremor, blurred vision, and sexual dysfunction. Venlafaxine has been associated with a mean increase in diastolic blood pressure of 7.2 mm Hg, an effect that is dose dependent [Effexor, 2003].
DRUG INTERACTIONS Venlafaxine may increase plasma levels of haloperidol. Although venlafaxine is metabolized by CYP2D6, the serum concentration of venlafaxine and its active metabolite was not altered by imipramine, a CYP2D6 inhibitor, or in poor metabolizers [Effexor, 2003].
Lee and Walkup / Neuropsychopharmacology
Mirtazapine CLINICAL APPLICATIONS Mirtazapine (Remeron) is available in tablets and orally disintegrating tablets. It is approved for the treatment of major depressive disorder in adults. In short-term studies, it appears to be more effective than placebo and comparable to amitriptyline in improving depressive symptoms [Bremner, 1995; Claghorn and Lesem, 1995]. No placebocontrolled studies support the use of this medication in children.
PHARMACOLOGY Mirtazapine increases synaptic levels of norepinephrine and serotonin through antagonism of α2-adrenergic receptors in the CNS. It is an antagonist at 5HT2 and 5HT3 receptors, increasing relative 5HT1 activity. Mirtazapine has antagonist activity at H1 histaminic, α1-adrenergic, and muscarinic receptors. Mirtazapine is well absorbed from the gastrointestinal tract. It reaches peak concentration in 2 hours, and its elimination half-life is in the range of 20 to 40 hours. Mirtazapine is metabolized by the liver and excreted in the urine. The isoenzymes CYP2D6, CYP1A2, and CYP3A4 are involved in its metabolism (see Table 39-5) [Remeron, 2002].
CLINICAL MANAGEMENT In clinical practice, the sedating and appetite-stimulating effects of mirtazapine may be useful for patients who suffer from insomnia, agitation, decreased appetite, or anxiety as part of their depressive syndrome. Patients may be started at 7.5 mg (orally disintegrating tablets cannot be split) to 15 mg at bedtime. The dose may be increased up to a maximum of 45 mg daily at intervals of 1 to 2 weeks [Remeron, 2002]. More rapid dose escalation may actually be associated with fewer side effects, especially sedation and increased appetite.
955
ANXIOLYTICS Anxiety disorders are one of the most prevalent categories of childhood and adolescent psychopathology. Approximately 8.9% of prepubertal children [Costello, 1989] in a general pediatric sample and approximately 8.7% of an adolescent sample [Kashani and Orvaschel, 1988] met criteria for at least one anxiety disorder. Anxiety disorders in children tend to have a chronic course with low remission rates [Keller et al., 1992]. Co-occurring conditions, such as other anxiety disorders [Kashani and Orvaschel, 1990; Strauss and Last, 1993], depression [Bernstein, 1991; Kashani and Orvaschel, 1988; Strauss et al., 1988], and ADHD [Anderson et al., 1987; Last et al., 1987] are common. Treatment of anxiety disorders in children and adolescents is multimodal, including psychoeducation, cognitivebehavioral therapy, family therapy, school interventions, and pharmacotherapy [AACAP, 1997a]. Psychopharmacologic intervention may be used if warranted by the severity of anxiety symptoms and level of impairment [AACAP, 1997a]. Choices include tricyclic antidepressants, selective serotonin re-uptake inhibitors, benzodiazepines, and α2-agonists and β-blockers. Tricyclic antidepressants may be a reasonable choice for patients with co-occurring depression, ADHD, or enuresis. Selective serotonin re-uptake inhibitors may be the preferred choice for patients with co-occurring depression or obsessive-compulsive disorder, and they have a more favorable side-effect profile than alternatives. The role of benzodiazepines is limited to the short-term management of anxiety symptoms. In cases of severe anxiety, they may be added to tricyclic antidepressants or selective serotonin re-uptake inhibitors for acute management of anxiety symptoms until the therapeutic effects of the antidepressants emerge. In clinical practice, the use of benzodiazepines is limited by concerns about possible abuse or dependence, drug diversion, and adverse cognitive effects.
Benzodiazepines ADVERSE EFFECTS
Clinical Applications
Common side effects of mirtazapine include sedation, dizziness, nausea, increased appetite, weight gain, and increased serum levels of cholesterol. Effects on sedation and appetite decrease at higher doses of mirtazapine. Less common side effects include liver enzyme elevations (i.e., aspartate transaminase) greater than three times the upper limit of the normal range and induction of mania or hypomania. Mirtazapine has been associated with rare cases of neutropenia or agranulocytosis in premarketing clinical trials [Remeron, 2002].
Benzodiazepines are classified as sedative-hypnotic medications. They act as sedatives or anxiolytics at low doses and sleep-inducing hypnotics at high doses. Although rapidly effective in relieving symptoms, they carry a risk of tolerance, dependence, and withdrawal with long-term use. These effects may be avoided by using only moderate doses for short-term therapy (1 to 2 weeks) [Sadock and Sadock, 2003]. Benzodiazepines differ from each other with regard to relative potency and half-life. In contrast to long-half-life benzodiazepines, short-half-life benzodiazepines are associated with less daytime sedation, more frequent dosing, earlier and more severe withdrawal syndromes, rebound insomnia, and anterograde amnesia. Long-half-life benzodiazepines require less frequent dosing and have a less severe withdrawal syndrome, but high plasma concentrations of the drug may accumulate and cause signs of toxicity over time [Sadock and Sadock, 2003]. Case reports and small open trials indicate that clonazepam and alprazolam may be helpful in treating anxiety
DRUG INTERACTIONS Mirtazapine may have additive effects if combined with alcohol or other CNS depressants. Mirtazapine is not a potent inhibitor of CYP2D6, CYP1A2, or CYP3A4. Combination of mirtazapine and monoamine oxidase inhibitors may induce a hypertensive crisis [Remeron, 2002].
956
Neurobehavioral Disorders / 39
disorders in children and adolescents [Biederman, 1987; Kutcher and MacKenzie, 1988; Simeon and Ferguson, 1987]. However, placebo-controlled studies have not supported their use [Graae et al., 1994; Simeon et al., 1992]. With the availability of more effective anxiolytics (e.g., selective serotonin re-uptake inhibitors, tricyclic antidepressants, buspirone), benzodiazepines are not considered first-line treatment for anxiety disorders in children and adolescents. However, benzodiazepines can be useful for the short-term management of specific anxiety-provoking situations, such as medical procedures, or as short-term adjunctive treatment with selective serotonin re-uptake inhibitors in the initial treatment of severe anxiety disorders. Chronic administration of benzodiazepines for anxiety should be undertaken only after patients have failed more effective treatments for anxiety, including other medications and behaviorally oriented psychotherapy.
Pharmacology Benzodiazepines are well absorbed from the gastrointestinal tract. They are extensively metabolized in the liver and excreted in urine. Benzodiazepine plasma concentrations are sensitive to medications that inhibit or induce cytochrome P-450 isoenzymes (see “Drug Interactions”). Benzodiazepines activate γ-aminobutyric acid (GABA)–benzodiazepine binding sites, which open chloride channels, resulting in a reduced rate of neuronal firing and muscle activity (Table 39-6) [Klonipin, 2004].
Clinical Management In considering benzodiazepine therapy for a patient, the clinician should inquire about any possible history of substance abuse, because this is a relative contraindication [DuPont and Saylor, 1992]. Family history of substance abuse may identify patients who are at risk for drug abuse or dependence, and household members with substance use histories may indicate a risk for drug diversion. Concomitant use of medications and co-occurring medical conditions that may affect the metabolism of benzodiazepines should be identified. The patient and family should be informed about the risks of tolerance, dependence, and withdrawal effects, as well as possible effects on cognitive and motor functioning. During treatment, the clinician must ensure that medications are not overused, abused, or diverted and monitor for possible adverse cognitive or behavioral side effects. After the treatment trial is complete, the medication should be tapered slowly because of the potential for withdrawal and rebound anxiety [Coffey, 1993; Kutcher et al., 1992].
Adverse Effects The most frequent adverse effects in children and adolescents are sedation, drowsiness, and decreased mental acuity [Biederman, 1991]. Benzodiazepines may cause paradoxic behavioral disinhibition, which manifests as increased agitation, aggression, and hyperactivity. This has been described with clonazepam in children [Graae et al., 1994]
TABLE 39-6 Benzodiazepines: Pharmacokinetic Properties, Dosing, and Drug Interactions DRUG
PREPARATIONS
DOSE EQUIV.
HALF-LIFE
DOSING
DRUG INTERACTIONS
Alprazolam
Xanax (0.25-, 0.5-, 1.0-, and 2.0-mg tablets) Xanax XR (0.5-, 1.0-, 2.0-, and 3.0-mg tablets)
0.25
6-20 hr
Initial dose (immediate release) of 0.25 mg/day if < 40 kg, or 0.5 mg/day if > 40 kg Maximum daily dose of 0.04 mg /kg/day in divided doses bid to qid [Simeon et al., 1992]
Clonazepam
Klonopin (0.5-, 1.0-, and 2.0-mg tablets)
0.5
>20 hr
Initial dose of 0.25 mg/day; increase by 0.25 mg every 3-4 days Maximum dose of 2 mg/day [Graae et al., 1994]
Diazepam
Valium (2-, 5-, and 10-mg tablets) Diazepam injection (5 mg/mL)
5
>20 hr
Initial oral dose of 1 to 2.5 mg tid or qid; increase gradually as needed and tolerated [PDR, 2004]
Lorazepam
Ativan (0.5-, 1.0-, and 2.0-mg tablets) Ativan injectable (2 mg/mL, 4 mg/mL)
1
6-20 hr
Usual daily dose of 1 to 6 mg/day [Green, 1995]
CNS depressants (additive effects) Inhibitors of cytochrome P-450 3A4 (↑ plasma concentration) Fluoxetine (↑ plasma concentration) Propoxyphene (↑ plasma conc) Oral contraceptives (↓ clearance) CNS depressants (additive effects) Inhibitors of cytochrome P-450 3A4 (↑ plasma concentration) Inducers of cytochrome P-450 (↓ plasma concentration) CNS depressants (additive effects) Inhibitors of cytochrome P-450 3A4 (↑ plasma concentration) CNS depressants (additive effects) Inhibitors of cytochrome P-450 3A4 (↑ plasma concentration)
Lee and Walkup / Neuropsychopharmacology
and adolescents [Reiter and Kutcher, 1991]. Anterograde amnesia also has been associated with benzodiazepines, particularly high-potency benzodiazepines [Sadock and Sadock, 2003]. Benzodiazepine therapy carries a risk of tolerance, dependence, and withdrawal effects. Abrupt discontinuation or rapid dose reduction has been associated with seizures, delirium, and withdrawal symptoms [Xanax, 2004].
Drug Interactions Additive CNS depression may occur when benzodiazepines are administered concomitantly with other CNS depressants, such as alcohol. Disulfiram may decrease the clearance of diazepam and chlordiazepoxide. Because benzodiazepines are metabolized by cytochrome P-450 isoenzymes, inhibitors and inducers of these isoenzymes can significantly alter the plasma concentration of benzodiazepines. Clonazepam and phenytoin decrease each other’s plasma concentrations. Valproate may increase plasma concentrations of lorazepam [Sadock and Sadock, 2003].
957
antagonist at 5HT1A receptors, as an agonist at postsynaptic dopamine receptors, and as an antagonist at presynaptic autoreceptor and postsynaptic sites in the CNS. Buspirone is rapidly absorbed from the gastrointestinal tract. Only 4% of the dose reaches systemic circulation because of extensive first-pass metabolism. The onset of clinical response may appear within the first 2 weeks of therapy, but optimal therapeutic effect is usually delayed [Kutcher et al., 1992]. The elimination half-life is about 2 to 4 hours; it is prolonged by renal or hepatic impairment. Buspirone is metabolized in the liver, primarily by the CYP3A4 isoenzyme, and it is excreted in the urine and feces [BuSpar, 2002].
Clinical Management Laboratory screening is not required before prescribing buspirone. The typical starting dose is 5 mg taken three times daily, with gradual increases to 15 mg taken three times daily. Younger children may be started at 2.5 to 5 mg/day and gradually increased to a total dose of 20 to 30 mg/day, administered in divided doses three times daily [Scahill and Martin, 2002].
Buspirone
Adverse Effects
Clinical Applications
The most common adverse effects of buspirone are dizziness, headache, drowsiness, and lightheadedness [BuSpar, 2002]. Side effects appear to be dose related and to decrease over time [Feighner and Cohn, 1989]. CNS depression is less common than in benzodiazepines.
Buspirone (BuSpar) is approved for use in the treatment of anxiety disorders and for short-term relief of symptoms of anxiety [BuSpar, 2002]. It is typically used in the treatment of generalized anxiety disorder. Buspirone does not appear to be effective as monotherapy in other anxiety disorders, such as post-traumatic stress disorder, panic disorder [Sheehan et al., 1988], or social phobia [van Vliet et al., 1997]. Although randomized, controlled trials do not support the use of buspirone to augment selective serotonin re-uptake inhibitors in partial responders, some patients with depression [Dimitriou and Dimitriou, 1998] and obsessivecompulsive disorder [Jenike et al., 1991] may benefit. Adolescents with generalized anxiety disorder appeared to benefit from buspirone in an open trial [Kutcher et al., 1992]. Another open trial showed improvement in anxiety symptoms in a group of children and adolescents with varied anxiety disorders [Simeon, 1991]. Buspirone appeared to improve anxiety and irritability in children with pervasive developmental disorders [Buitelaar et al., 1998]. A very large industry-sponsored, randomized, controlled trial did not demonstrate benefit (http://www.fda.gov). Buspirone offers several benefits over benzodiazepines, including lack of euphoric effects, performance impairment, abuse potential, and withdrawal symptoms with discontinuation. Although buspirone appears to be as effective as benzodiazepines in decreasing psychic symptoms of anxiety, it appears to be less effective for somatic symptoms of anxiety, and the onset of therapeutic effect may be delayed 2 to 4 weeks [Kutcher et al., 1992].
Pharmacology Buspirone differs from benzodiazepines in that it has no activity at the GABA-benzodiazepine receptor complex. Buspirone acts as a partial agonist or mixed agonist/
Drug Interactions Combination of buspirone and monoamine oxidase inhibitors may result in a hypertensive crisis, requiring emergency medical attention. Because of reports of liver transaminase elevations with the concomitant use of buspirone and trazodone, the manufacturer recommends monitoring liver function when prescribing this combination. Because buspirone is highly protein bound, it may displace other medications, which are protein bound and increase their free plasma level. Inducers of CYP3A4 may decrease plasma levels of buspirone. Alternatively, inhibitors of CYP3A4 (e.g., erythromycin, itraconazole, grapefruit juice) may increase the serum concentration of buspirone. Increased serum concentrations of haloperidol have been reported when combined with buspirone [BuSpar, 2002].
MOOD STABILIZERS The term mood stabilizers refers to a group of medications used to treat bipolar affective disorder, which in adults is characterized by alternating episodes of depression, mania, and euthymia [APA, 2002]. The diagnosis of bipolar disorder in children has been controversial because it does not resemble bipolar disorder in adults, and its symptoms often overlap with other syndromes. Studies have indicated that juvenile bipolar disorder has been under-recognized, misdiagnosed as schizophrenia or disruptive behavior disorders [Carlson et al., 1994], and sometimes overdiagnosed [Carlson, 1990]. Bipolar children are not likely to exhibit classic symptoms of adult
958
Neurobehavioral Disorders / 39
bipolar disorder; rather, they are more likely to exhibit atypical manic or mixed-mood symptoms [Bowring and Kovacs, 1992]. Adding to the complexity of making the diagnosis is the broad differential diagnosis and co-occurrence of other neuropsychiatric disorders [AACAP, 2002]. Mood stabilizers are used to treat the acute episodes of mood disturbances and are used prophylactically during the maintenance phase of the disorder [APA, 2002]. Mood stabilizers used in clinical practice can be grouped into four categories: 1. Lithium 2. Anticonvulsants approved for use in adults with bipolar disorder (e.g., valproic acid, lamotrigine) 3. Neuroleptics approved for use in adults with bipolar disorder (e.g., risperidone, olanzapine, quetiapine) 4. Anticonvulsants prescribed off-label (e.g., gabapentin, carbamazepine) Case series and open trials using the newer anticonvulsants show promise, but large, placebo-controlled trials are lacking. Each mood stabilizer is not equally effective for all phases of the disorder or as prophylaxis. Lithium, valproate, risperidone, olanzapine, ziprasidone, and quetiapine are approved for treating manic symptoms. Lamotrigine is the only mood stabilizer labeled for use during the depressive phase [Calabrese et al., 1999; Evins, 2003]. Lamotrigine, lithium, and olanzapine are approved for use during the maintenance phase of treatment to delay the occurrence of acute mood episodes [Lamictal, 2003; Zyprexa, 2004]. Polypharmacy in the treatment of bipolar affective disorder in adults is common. Typical treatment consists of long-term maintenance with a mood stabilizer as prophylaxis. A neuroleptic or an additional mood stabilizer may be added to stabilize the acute symptoms of a manic episode. During a depressive episode, an antidepressant or lamotrigine may be added while cautiously monitoring for the possible emergence of antidepressant-induced manic or rapid-cycling symptoms. The pediatric literature is less well developed than that for adults, and all pharmacologic treatments used in clinical practice for the treatment of childhood bipolar disorder are off-label. As with childhood depression, children with bipolar affective disorder are thought to be less responsive to medication compared with adults [AACAP, 2002]. Combination of mood stabilizers [Findling et al., 2003] or a mood stabilizer with a neuroleptic [Kafantaris, 1995] is sometimes required to stabilize acute manic symptoms. Given the complexity of making an accurate diagnosis, the treatment-resistant nature of pediatric bipolar illness, and the complicated regimens of off-label medication sometimes required, the average pediatric neurologist may wish to request a consultation from a child psychiatrist if faced with a patient with possible bipolar disorder.
Lithium Clinical Applications Lithium is approved for use in the treatment of bipolar affective disorder. It is effective in managing acute manic
and depressive episodes, preventing or diminishing the intensity of subsequent episodes in maintenance treatment and decreasing mood instability between episodes [Goodwin and Jamison, 1990]. Data in children and adolescents with bipolar disorder are sparse and mixed. Several studies have shown good response rates. However, one study [Carlson et al., 1992] did not demonstrate superiority over placebo [DeLong and Aldershof, 1987; Geller and Fetner, 1989; Strober et al., 1990; Varanka et al., 1988]. Lithium also has been used with positive results in the treatment of severe aggression in adults [Sheard, 1975] and children [Campbell et al., 1984; Malone et al., 2000].
Pharmacology Lithium is an alkali metal, similar to sodium and potassium, and it is available in salt form as lithium carbonate or lithium citrate. Lithium has effects at the cellular level (i.e., cell membrane ion channels and cyclic adenosine monophosphate second-messenger cellular processes) and in neurotransmitter systems [Alessi and Bos, 1991]. The specific mechanism of action in the CNS is unclear [Viesselman et al., 1993]. Lithium is available in immediate-release and sustainedrelease preparations. Ninety percent of immediate-release lithium is absorbed by the gastrointestinal tract; 60% to 90% of extended-release lithium is absorbed. Immediate-release lithium reaches peak serum levels in 1 to 1.5 hours (4 to 12 hours for the extended-release form), and it is almost completely excreted in urine, with the remainder excreted in the feces and breast milk. Lithium has a half-life of about 20 hours and reaches steady-state levels after 1 week of administration [Eskalith-CR, 2002].
Clinical Management Before starting lithium therapy, the patient should be screened for conditions that may contraindicate or complicate lithium therapy, such as pregnancy, renal disease, or diabetes mellitus. A medical evaluation should be completed, including an ECG, laboratory screen for electrolytes, kidney and thyroid function tests, complete blood cell count, urinalysis, and urine pregnancy screen. Lithium is started at dosages ranging from 300 to 600 mg/day. Formulas [Weller et al., 1986] and nomograms [Alessi and Bos, 1991; Geller and Fetner, 1989] have been developed to guide lithium dosing. Trough lithium levels are drawn when steady state is achieved, at least 5 days after initiating lithium or changing the dose. The recommended therapeutic serum levels range from 0.6 to 1.2 mEq/L [Viesselman et al., 1993]. Patients maintained at serum levels between 0.8 and 1.0 mEq/L were less likely to relapse compared with patients with lower serum levels. Lithium levels above the therapeutic range increase the risk of toxicity. Early therapeutic effects may be detected at 10 to 14 days after achieving a therapeutic level; however, there is often a significant lag of 4 to 6 weeks [Kowatch et al., 2000]. Between 4 and 6 weeks of lithium at therapeutic serum concentrations constitutes an adequate trial. Because several days are required to achieve therapeutic plasma concentrations, neuroleptic medications may be necessary
Lee and Walkup / Neuropsychopharmacology
to acutely stabilize severe mania, especially if psychotic symptoms are present. After target mood symptoms are stabilized, lithium levels should be routinely checked every 3 to 6 months. Other
959
indications to obtain a lithium level include symptoms of toxicity, worsening side effects, and breakthrough mood symptoms. Urinalysis, renal evaluation, and thyroid function tests should be repeated every 3 to 6 months to
TABLE 39-7 Mood Stabilizers: Baseline Assessment, Monitoring, and Adverse Effects DRUG
PREPARATIONS
BASELINE ASSESSMENTS
MONITORING
ADVERSE EFFECTS
Lithium, immediate release
Lithium carbonate (150-, 300-, and 600-mg tablets) Lithium citrate syrup (8 mEq/mL)
Laboratory screening: thyroid function tests, electrolytes, renal function tests, complete blood cell count, urinalysis, pregnancy test Electrocardiogram
Sedation, tremor, acne, weight gain, polydipsia, polyuria, renal effects, electrocardiographic changes, leukocytosis, hypothyroidism
Lithium, sustained release Valproic acid
Litho bid (300-mg tablets) Eskalith CR (450-mg tablets) Depakote, divalproex (125-, 250-, and 500-mg delayed-release tablets) Depakene syrup (250 mg of valproic acid/5 mL) Depakote Sprinkle, divalproex (125-mg capsules with coated particles) Depakote ER, divalproex extended release (250and 500-mg tablets) Tegretol (200-mg scored tablets) Tegretol XR (100-, 200-, and 400-mg extendedrelease tablets) Carbatrol (200- and 300-mg extended-release capsules) Tegretol (100 mg/5 mL suspension) Tegretol (100-mg chewable tablets) Lamictal (25-, 100-, 150-, and 200-mg tablets) Lamictal (2-, 5-, and 25-mg chewable/dispersible tablets)
Same as for immediate-release form Laboratory screening: liver function tests, pancreatic enzymes, complete blood cell count, pregnancy test
Lithium level (target of 0.8-1.0 ng/mL) during dose titration, every 3-6 months or with signs of toxicity or breakthrough symptoms Urinalysis, thyroid-stimulating hormone test, and renal function tests every 3-6 months or with signs and symptoms of toxicity Same as for immediate-release form Valproic acid level (target of 80-100 ng/mL) during dose titration, every 3-6 months, or with signs of toxicity or breakthrough symptoms Liver function tests, complete blood cell count, and pancreatic enzymes every 3-6 months or with signs and symptoms of toxicity
Topiramate
Gabapentin
Carbamazepine
Lamotrigine
Same as for immediaterelease form Sedation, weight gain, elevated liver function test results, nausea, liver failure, pancreatitis, polycystic ovary syndrome
Laboratory screening: liver function tests, complete blood cell count, electrolytes, pregnancy test
Carbamazepine level (target of Nausea, vomiting, anorexia, 4-12 μg/mL) during dose ataxia, sedation, tremor, titration, every 3-6 months, aplastic anemia, or with signs of toxicity or agranulocytosis, elevated breakthrough symptoms liver function test results, Liver function tests, complete acute hepatitis, blood cell count, and cholestasis, lifeelectrolytes every 3-6 months threatening skin or with signs and symptoms conditions of toxicity
None
Laboratory screening: None Monitor for rash
Topamax (15- and 25-mg capsules) Topamax (25-, 50-, 100-, and 200-mg film-coated tablets)
Baseline electrolytes
Laboratory screening: none Electrolytes for metabolic acidosis Routine clinical monitoring
Neurontin (100-, 300-, and 400-mg capsules) Neurontin (250 mg/5 mL solution) Neurontin (600- and 800-mg film-coated tablets)
None
Laboratory screening: none Routine clinical monitoring
Dizziness, ataxia, somnolence, headache, diplopia, blurred vision, nausea, vomiting, rash Serious rashes requiring hospitalization and discontinuation of treatment, StevensJohnson syndrome (1% of pediatric population); rare cases of toxic epidermal necrolysis and rash-related death have been reported Fatigue, ataxia, confusion, impaired concentration and memory, sedation, agitation, anorexia with weight loss, kidney stones and diplopia, metabolic acidosis Dizziness, ataxia, sedation, fatigue, nystagmus, dyspepsia, peripheral edema, diplopia and amblyopia.
960
Neurobehavioral Disorders / 39
monitor for the emergence of subclinical renal and thyroid dysfunction (Table 39-7). Stabilization of manic symptoms may be prolonged up to several years [Biederman et al., 1998]. Lithium should be continued for at least 18 months after manic symptoms have been stabilized [APA, 2002], because discontinuation of lithium therapy, especially abrupt discontinuation, is associated with increased relapse rates [Strober et al., 1990].
Adverse Effects Side effects of lithium are polydipsia, polyuria or enuresis, gastric distress (i.e., nausea, vomiting, and diarrhea), weight gain, tremor, fatigue, leukocytosis, acne, and mild cognitive impairment [Alessis et al., 1999; Silva et al., 1992; Viesselman et al., 1993]. Serious renal side effects are rare and include nephrotic syndrome, features of distal renal tubular acidosis, nonspecific interstitial fibrosis, and renal failure [Alessis et al., 1999; Gelenberg and Schoonover, 1991]. Lithium therapy can induce alterations in thyroid function tests and produce hypothyroidism [Alessis et al., 1999]. Lithium can have rare cardiac side effects, including first-degree atrioventricular block, irregular sinus rhythm, and increased premature ventricular contractions [Gelenberg and Schoonover, 1991]. Reversible conduction abnormalities in children have been demonstrated on their ECGs [Campbell et al., 1972]. Studies examining the longterm effects of lithium treatment of children are lacking. Intrauterine exposure to lithium during the first trimester has been associated with teratogenic effects, most commonly Ebstein’s anomaly of the tricuspid valve [Eskalith-CR, 2002].
Drug Interactions Lithium levels are affected by medications or conditions that can alter the body’s fluid and electrolyte status. Dehydration and extremely low salt intake can result in elevated lithium levels. Likewise, an extremely high salt intake can result in lowered lithium levels. Many medications, such as diuretics and nonsteroidal anti-inflammatory drugs, can cause an increase or decrease in lithium level by influencing renal clearance [Green, 1995]. Lithium is commonly used in combination with other psychotropic medications in the treatment of bipolar disorder. However, case reports have described interactions with neuroleptic medications (i.e., encephalopathic syndrome and neuroleptic malignant syndrome), and carbamazepine may increase lithium serum concentration by decreasing lithium renal clearance [Green, 1995].
studies of valproic acid in children and adolescents with bipolar mania have yielded mixed results. In one study, 61% of patients with mania, hypomania, or mixed symptoms were rated responders to valproic acid; however, there was a high dropout rate (23 of 40) [Wagner et al., 2002]. In a retrospective chart review of pediatric bipolar patients, 53% appeared to respond to divalproex; approximately one third of the patients discontinued the medication, mostly because of side effects [Henry et al., 2003]. In a small, double-blind, placebocontrolled, crossover-design study, children and adolescents with explosive temper and mood lability had superior response to divalproex sodium compared with placebo [Donovan et al., 2000]. In a retrospective examination of divalproex sodium treatment of autistic children, 71% were rated improved in the core symptoms of autism and associated symptoms of affective instability, aggression, and impulsivity [Hollander et al., 2001].
Pharmacology The mechanism of action of valproic acid is unidentified, although it is known to increase brain concentrations of the inhibitory neurotransmitter GABA [Viesselman et al., 1993]. Valproic acid is available in several preparations: valproic acid (Depakene capsules); valproate (Depakene syrup); divalproex (Depakote); divalproex capsules with coated particles (Depakote Sprinkle); divalproex, delayedrelease tablets (Depakote), which are released from particles in the small intestine; and divalproic acid in extendedrelease tablets (Depakote ER). Valproate rapidly converts to the acid form in the stomach. Divalproex dissociates into valproic acid in the gastrointestinal tract. Valproic acid is rapidly and almost entirely absorbed from the gastrointestinal tract. Peak plasma concentrations are achieved 1 to 4 hours, 3 to 5 hours, and 7 to 14 hours after oral administration of valproate, divalproex, and extended-release tablets, respectively. Valproic acid binds plasma proteins; therefore, protein binding can be altered by the presence of other protein-bound drugs and by renal or hepatic disease. Plasma protein binding of valproic acid is concentration dependent. Peak and trough concentrations with delayed-release tablets and capsules containing coated particles may differ from the equivalent dose valproic acid. Concentrations of therapeutically effective free valproic acid increase at serum concentrations (total) above 50 to 100 μg/mL. Valproic acid is metabolized in the liver and excreted predominantly in the urine [Depakote, 2003]. No therapeutic serum concentrations for the treatment of behavioral or psychiatric disorders have been determined.
Clinical Management
Valproic Acid Clinical Applications Valproic acid is approved for the treatment of seizures, migraine prophylaxis, and the manic phase of bipolar affective disorder in adults. In adults, valproic acid appears to be more helpful than lithium in treating rapid cycling and dysphoric or mixed mania [McElroy et al., 1992]. Support for use of valproic acid in child psychiatric practice is primarily based on the adult literature. The few
In addition to the routine psychiatric or neurologic history, patients should be asked about risk factors affecting treatment with valproate, including pregnancy, disorders of metabolism, hepatic or renal disease, concomitant medications, and coagulation disorders. Laboratory screening should include liver function tests, a complete blood cell count, coagulation studies, and determinations of pancreatic enzyme levels [Davanzo and McCracken, 2000]. Parents should be educated about potential signs of hepatic or pancreatic toxicity and polycystic ovary disease.
Lee and Walkup / Neuropsychopharmacology
961
Recommended initial dosing of valproic acid is 10 to 15 mg/kg/day, given in divided doses two or three times per day. Dosage may be increased by 5 to 10 mg/kg/day at weekly intervals [Depakote, 2003]. The manufacturer’s maximum recommended dosage is 60 mg/kg/day. However, starting at lower doses and using slower upward adjustments of dose may be required for tolerability. Although therapeutic levels for treating mania have not been established, achieving a plasma concentration of 85 to 110 μg/L [Kowatch et al., 2000] is needed to consider a trial adequate for determining outcome in an individual patient. In adult psychiatry, an oral loading dose of valproate is sometimes used to achieve a therapeutic plasma concentration and to gain rapid control over mania. The tolerability of an oral loading dose of divalproex sodium was examined in children and adolescents [Good et al., 2001]. A loading dose of 15 mg/kg/day resulted in therapeutic plasma levels by day 5 of treatment, and it was well tolerated. Dosage adjustment was required for overweight children to avoid supratherapeutic drug levels [Good et al., 2001]. Total valproic acid levels should be checked when steady state is reached, after any dosage change, after conversion to a different preparation of valproate, for signs of toxicity, or for a change in clinical status. Maintenance involves monitoring of the therapeutic response and side effects, and it requires laboratory screening. Liver and pancreatic enzymes, complete blood cell count, and serum valproic acid levels should be periodically monitored, although the exact frequency of testing has not been ascertained. Initially, monitoring may be done every 3 to 6 months for the first year and semiannually thereafter (see Table 39-7).
unclear. Other reports suggest that oral carnitine can be useful in reducing ammonia levels [Bohan et al., 2001]. Rare cases of pancreatitis have been reported [Depakote, 2003]. Cases of polycystic ovary disease have been reported in some women treated with valproate for seizure disorder [Isojarvi et al., 1993]. It is unclear whether this is related to the medication or an endocrine abnormality related to the seizure disorder [Davis et al., 2000]. Intrauterine exposure to valproic acid during the first trimester is associated with neural tube defects [Depakote, 2003].
Adverse Effects
Clinical Applications
Side effects include sedation, nausea, vomiting, gastrointestinal upset, increased appetite, weight gain, and hair loss. Rare side effects include thrombocytopenia, platelet dysfunction, prolonged bleeding time, elevation in liver transaminase levels, and lactate dehydrogenase without clinical symptoms. Children younger than 2 years appear to have an increased risk of hepatotoxicity and extreme caution should be used in this population. This heightened risk may result from an undiagnosed metabolic or mitochondrial disorder. In particular, children with urea cycle defects such as ornithine transcarbamylase deficiency should not receive this medication. Carnitine supplementation should be considered when prescribing this medication as this may facilitate the processing of valproate in the mitochondrial βoxidation pathway. Valproate has also been associated with rare cases of hyperammonemic encephalopathy [Barrueto, 2001; Elgudin et al., 2003; Verrotti et al., 1999, 2002], which occurs more commonly with polypharmacy and with associated liver dysfunction [Verrotti et al., 1999]. One case reported in the child psychiatry literature manifested as increased aggression and confusion, an electroencephalogram with symmetric 5- to 6-Hz waves, elevated serum ammonia levels, and normal levels of serum liver transaminases [Yehya et al., 2004]; the situation resolved with valproic acid discontinuation. Elevated ammonia levels have also been observed in the absence of encephalopathy, but the clinical relevance of such laboratory abnormalities is
Few data are available on the use of carbamazepine for the treatment of bipolar disorder in children and adolescents. Case reports describe its effectiveness in stabilizing symptoms of juvenile bipolar disorder [Hsu, 1986; Woolston, 1999]. Justification for its use in clinical practice has rested on the adult literature, which is difficult to interpret. Studies have shown carbamazepine to be superior to placebo and comparable to lithium [Lerer et al., 1987; Small et al., 1991] in improving manic symptoms. However, another study indicated that it was not as effective as valproate, and patients on carbamazepine required adjunctive medication to achieve stabilization [Vasudev et al., 2000]. Carbamazepine may be helpful in the depressive phase of bipolar disorder [Ballenger and Post, 1980; Dilsaver et al., 1996]. Carbamazepine can have multiple drug interactions resulting from hepatic enzyme induction that complicates the management of bipolar disorder, because polypharmacy is often required. Clinicians and patients may prefer carbamazepine to the other mood stabilizers because of its reduced tendency to cause weight gain.
Drug Interactions Valproic acid, alone or in combination with lamotrigine, may cause potentially fatal Stevens-Johnson syndrome. When valproic acid is combined with neuroleptics, CNS depressant effects and extrapyramidal side effects may increase. Valproic acid may increase lithium-associated tremor. Carbamazepine can induce metabolism of valproic acid and decrease plasma levels. Aspirin has been shown to decrease the metabolism of valproic acid and decrease valproic acid protein binding. Valproic acid may displace warfarin from protein binding sites and prolong coagulation time. Increases in valproic acid levels have been reported when combined with guanfacine, amitriptyline, and fluoxetine. Valproic acid can cause increases in plasma concentrations of carbamazepine, lamotrigine, diazepam, amitriptyline, nortriptyline, and phenobarbital. Valproic acid can decrease plasma concentrations of phenytoin and desipramine [Depakote, 2003].
Carbamazepine
Pharmacology Carbamazepine is structurally related to tricyclic antidepressants. It reduces activity at sodium and calcium channels resulting in reduced synaptic transmission. It is
962
Neurobehavioral Disorders / 39
available in immediate-release forms (e.g., Tegretol tablets, chewable tablets, suspension) and extended-release capsules (i.e., Tegretol XR). It is slowly absorbed from the gastrointestinal tract. The plasma half-life gradually decreases over 3 to 5 weeks from 25 to 65 hours to approximately 12 to 17 hours due to autoinduction. Steady-state concentrations are achieved in 2 to 4 days. Between 75% and 90% of the drug is bound to plasma proteins. It is metabolized in the liver and excreted in the urine [Tegretol, 2002].
Clinical Management Patients should be evaluated for medical conditions that may contraindicate use of carbamazepine, including liver disease, hematologic disorders, immune disorders, cardiac disease, and pregnancy. Laboratory screening should include a urine pregnancy screen, liver function tests, and a complete blood cell count. Because laboratory screening can fail to predict impending hepatic and hematologic complications, parents should be aware of signs and symptoms indicating serious adverse effects, such as rash, symptoms of aplastic anemia or agranulocytosis, and hepatitis or cholestasis. Sexually active patients should be informed of its teratogenic effects and the possible decrease in effectiveness of oral contraceptives [Tegretol, 2002]. Dosage is initiated at 100 to 300 mg/day, increasing as tolerated while monitoring blood levels. Therapeutic blood levels in the treatment of mania have not been established. Recommended levels are the same as those for seizure disorder, 4 to12 μg/mL [Rosenberg et al., 1994]. Blood levels should be checked 5 days after initiating or changing doses and again in 4 weeks because of an anticipated reduction in plasma levels due to autoinduction. Although it is recommended that liver function tests, bilirubin levels, and complete blood cell counts be routinely checked every 3 months, the utility of such testing in predicting serious hepatic or hematologic complications is questionable (see Table 39-7). Hyponatremia resulting from carbamazepine use is rare in children, and if it is clinically suspected, sodium levels should be obtained.
Adverse Effects The most common side effects are nausea, vomiting, sedation, and ataxia [Tegretol, 2002]. Carbamazepine can cause benign elevations in liver transaminases; hepatitis, indicated by elevated liver transaminase levels greater than three times normal; and cholestasis, indicated by elevations in bilirubin and alkaline phosphatase. Carbamazepine therapy has been associated with leukopenia in 1% to 2% of patients and agranulocytosis or aplastic anemia in 1 of 250,000 patients. Although blood dyscrasias are not always predicted by leukopenia, complete blood cell counts are recommended at 3- to 6-month intervals. Other adverse effects observed with carbamazepine include cognitive or behavioral disturbance [Carpenter and Vining, 1993], CNS toxicity, altered cardiac conduction, and lifethreatening dermatologic conditions (i.e., exfoliative dermatitis, toxic epidermal necrolysis, and Stevens-Johnson syndrome). Intrauterine exposure has been associated with neural tube defects and other fetal malformations [Rosa, 1991].
Drug Interactions Carbamazepine is an inducer of CYP3A4, leading to decreased plasma concentrations of medications metabolized by that isoenzyme. Several medications that are commonly combined with carbamazepine in psychiatric practice may be affected, including anticonvulsants (e.g., lamotrigine, clonazepam, valproic acid), antidepressants (e.g., bupropion, clomipramine, desipramine, imipramine), and neuroleptics (e.g., clozapine, fluphenazine, haloperidol). Carbamazepine levels can be increased by fluoxetine, lamotrigine, and valproate. Carbamazepine levels can be reduced by valproate and carbamazepine itself (i.e., autoinduction). Combination with lithium or neuroleptics may increase the risk of adverse neurologic effects (e.g., drowsiness, dizziness, ataxia) [Tegretol, 2002].
Novel Anticonvulsants Although lithium and valproate are first-line pharmacologic treatments for bipolar disorder in adults [APA, 2002], many children and adolescents do not respond adequately to these medications and cannot tolerate the side effects or the requirement of laboratory monitoring. In clinical practice, newer anticonvulsants are beginning to be used for the treatment of bipolar disorder. Many of the novel anticonvulsants have a more favorable side-effect profile and do not require blood tests. Support for their use in clinical practice, however, has been primarily based on case reports and open trials. Use of these medications is more appropriate for patients with bipolar disorder who are unresponsive to traditional therapies or cannot tolerate traditional agents.
Lamotrigine CLINICAL APPLICATIONS Lamotrigine (Lamictal) is approved for use in the treatment of seizure disorders and for prophylaxis of mania during maintenance therapy for type 1 bipolar disorder [Lamictal, 2003]. In adults, lamotrigine appears to be helpful in the treatment of patients with bipolar depression [Calabrese et al., 1999; Evins, 2003], some patients with rapid-cycling bipolar disorder [Bowden et al., 1999; Frye et al., 2000], and as a prophylactic agent to prevent or attenuate recurrences of bipolar episodes [Bowden et al., 2003; Calabrese et al., 2000, 2003; McElroy et al., 2004]. It was reported to be an effective add-on agent to valproate in adolescents with bipolar depression [Kusumakar and Yatham, 1997].
PHARMACOLOGY Lamotrigine has weak inhibitor effects on the 5HT3 receptor. Its mechanism of action is unknown. Lamotrigine is available in tablets and chewable dispersible tablets, which should not be divided. Lamotrigine is rapidly absorbed through the gastrointestinal tract, metabolized in the liver, and excreted in urine [Lamictal, 2003].
Lee and Walkup / Neuropsychopharmacology
963
CLINICAL MANAGEMENT
DRUG INTERACTIONS
Because supporting data are lacking for the pediatric population, the use of lamotrigine in children for the treatment of bipolar disorder should be reserved for extreme cases, in which patients have failed alternative treatments [Scahill and Martin, 2002]. Before initiating treatment, a urine pregnancy test should be obtained. The patient and family should be educated about the risk of serious rash or hypersensitivity reaction and instructed about how to recognize the signs and symptoms requiring immediate medical attention. These dosage recommendations are based on those for patients who are being treated for seizure disorder and who are not taking valproate concomitantly; physicians should refer to the product package insert for dosage recommendations for lamotrigine added to valproate. Therapeutic doses for the treatment of bipolar disorder have not been determined. For children between the ages of 2 and 12 years, 0.6 mg/kg/day of lamotrigine is administered in one or two divided doses (rounded down to the nearest 5 mg) during the first 2 weeks. During the third and fourth week, 1.2 mg/kg/day is administered in two divided doses (rounded down to the nearest 5 mg). The dose may be titrated up in increments of 1.2 mg/kg/day (rounded down to the nearest 5 mg) every 2 weeks. The usual maintenance dose of seizures is 15 mg/kg/day. For pediatric patients older than 12 years, 50 mg of lamotrigine is administered daily during the first 2 weeks of treatment. During the third week, the dose is increased to 100 mg/day and given in two divided doses. The dose may be increased by increments of 100 mg/day every 1 to 2 weeks (see Table 39-7). Maintenance dosage ranges from 300 to 500 mg daily given in two divided doses [Lamictal, 2003].
Carbamazepine, phenytoin, phenobarbital, and primidone increase clearance of lamotrigine. Valproate decreases clearance of lamotrigine and may increase the risk of potentially life-threatening rashes [Lamictal, 2003].
ADVERSE EFFECTS Common side effects observed in clinical studies include dizziness, ataxia, somnolence, headache, diplopia, blurred vision, nausea, vomiting, and rash [Lamictal, 2003]. Lamotrigine has been associated with serious rashes requiring hospitalization and discontinuation of treatment. The manufacturer reports the incidence of Stevens-Johnson syndrome as 1% in the pediatric population. Rare cases of toxic epidermal necrolysis and rash-related death have been reported. Potential risk factors for serious rash are concomitant use of valproate, rapid dose escalation, and use of exceedingly high doses [Lamictal, 2003]. Rashes have been reported in 10% of patients in clinical trials. Because it is difficult to distinguish a benign rash from the early stages of a more serious rash, the manufacturer recommends discontinuation of treatment at the first sign of a rash, unless it is clearly not medication related. Rare but potentially life-threatening hypersensitivity reactions have occurred with lamotrigine. Symptoms such as fever and lymphadenopathy, with or without a rash, should prompt immediate evaluation and possible discontinuation of treatment. Lamotrigine accumulates in melanin-rich tissues, such as skin and the eye. Clinical trials did not detect ophthalmologic adverse effects; however, no long-term data are available. Lamotrigine inhibits dihydrofolate reductase; administration of lamotrigine to rats reduced serum folate levels. Low folate levels have been associated with teratogenic effects [Lamictal, 2003].
Gabapentin CLINICAL APPLICATIONS Gabapentin is indicated as a treatment for post-herpetic neuralgia, adjunctive therapy in the treatment of partial seizures in adults and children 12 years or older, and partial seizures in children 3 years or older [Gabapentin, 2002]. Case reports and open studies of gabapentin as adjuvant therapy in bipolar patients were promising; however, double-blind trials have not confirmed efficacy in mania as monotherapy [Frye et al., 2000] or adjunctive treatment [Pande, 2000] or treatment of resistant rapid-cycling bipolar disorder [Evins, 2003; Yatham et al., 2002].
PHARMACOLOGY Gabapentin (Neurontin) is available in capsules, tablets, and solution. Plasma half-life is 5 to 7 hours. It is not metabolized in the liver, and it is excreted in the urine unchanged. No clinically significant drug interactions have been described [Gabapentin, 2002].
CLINICAL MANAGEMENT The dose can be started at 300 mg, given two or three times daily, and titrated gradually up to 1800 mg/day, given in divided doses three times daily. Clinical trial data do not indicate any routine monitoring of laboratory screens. No therapeutic plasma concentrations have been established (see Table 39-7).
ADVERSE EFFECTS Gabapentin is generally well tolerated. Common side effects include dizziness, ataxia, sedation, fatigue, and nystagmus [Gabapentin, 2002]. Less common side effects include dyspepsia, peripheral edema, diplopia, and amblyopia. Behavioral adverse effects are possible, including agitation and emotional lability. Gabapentin has been associated with teratogenic effects in animal studies [Gabapentin, 2002].
Topiramate CLINICAL APPLICATIONS Topiramate (Topamax) has an indication as adjuvant therapy for partial seizures and primary generalized tonic-clonic seizures in adults and children ages 2 and older [Topamax, 2003]. In adults, topiramate appears to be effective as adjuvant therapy in treatment-resistant bipolar disorder [Ghaemi et al., 2001; Vieta et al., 2002]. It may be more effective in managing the manic phase or in rapid-cycling bipolar disorder [Chengappa et al., 1999; McElroy et al., 2000]. A retrospective chart review of children and adolescents with bipolar disorder
964
Neurobehavioral Disorders / 39
treated with topiramate as an adjuvant mood stabilizer indicated response rates of 73% for mania [DelBello et al., 2002a]. Potential advantages of topiramate over other mood stabilizers are its weight-neutral and appetite-suppressive effects [Chengappa et al., 1999; McElroy et al., 2000].
PHARMACOLOGY Topiramate is available in tablets or sprinkle capsules, which are bioequivalent. Its absorption is rapid, reaching peak plasma concentrations at 2 hours. Antacids can decrease absorption of topiramate. Plasma elimination half-life is 21 hours, and steady state is reached in about 4 days. About 70% of topiramate is excreted unchanged in the urine. The remainder is metabolized in the liver [Topamax, 2003].
CLINICAL MANAGEMENT Topiramate should be initiated at 25 to 50 mg daily (1 to 3 mg/kg/day), with small weekly increases of 1 to 3 mg/kg/day to minimize adverse effects. The recommended total daily dose in the treatment of seizures is 5 to 9 mg/kg/day [Topamax, 2003]. Monitoring the plasma concentration is unnecessary unless it is concomitantly used with phenytoin or carbamazepine (see Table 39-7).
ADVERSE EFFECTS AND DRUG INTERACTIONS Adverse effects include fatigue, ataxia, confusion, impaired concentration and memory, sedation, agitation, anorexia with weight loss, kidney stones, and diplopia. Topiramate may decrease systemic levels of bicarbonate, leading to a metabolic acidosis. Consequently, slow titration, clinical observation, and laboratory monitoring are advised. Carbamazepine, valproic acid, and phenytoin can lower the plasma concentration of topiramate. Topiramate may increase the concentration of phenytoin and decrease that of valproic acid [Topamax, 2003].
DOPAMINE RECEPTOR ANTAGONISTS: TYPICAL NEUROLEPTICS Dopamine receptor antagonist is a term used to refer to a medication that is a high-affinity antagonist of dopamine receptors. Other terms used to refer to these drugs include typical neuroleptics, typical antipsychotics, and major tranquilizers. The first neuroleptic, chlorpromazine, was initially used in the early 1950s in France to manage preoperative anxiety and postoperative shock [Sadock and Sadock, 2003]. When it was found to have a calming effect on patients with schizophrenia and mania, it gained widespread use in psychiatry. Unfortunately, these patients developed neurologic side effects, including extrapyramidal symptoms, associated with short- and long-term use of chlorpromazine. Other antipsychotic agents were developed that were effective in treating a variety of psychiatric conditions, but they could not escape the risk of producing extrapyramidal symptoms. Uncovering their pharmacodynamic properties led to more sophisticated drug development. The antipsychotic effects of these medications are thought to be
mediated through the inhibition of dopamine binding at dopamine D2 receptors, resulting in the reduction of dopaminergic neurotransmission in the mesocortical region. The neurologic side effects appear to be mediated by dopamine antagonism in the nigrostriatal pathway. Other side effects associated with neuroleptics were found to be associated with its activity at adrenergic, cholinergic, and histaminic receptors. Dopamine receptor antagonists are distinguished from serotonin-dopamine antagonists, also called novel or atypical antipsychotics or neuroleptics. In contrast to typical neuroleptics, the serotonin-dopamine antagonists are antagonists at dopaminergic and serotonergic receptors. They also differ in their ability to reduce negative symptoms of schizophrenia and their reduced risk of short- and longterm neurologic side effects. Unfortunately, as patients and clinicians gained experience with serotonin-dopamine antagonists, other adverse effects, such as hyperglycemia and hyperlipidemia, were recognized. Serotonin-dopamine antagonists have become first-line medications in the treatment of psychotic disorders in adults [APA, 1997], and their apparently lower risk of extrapyramidal symptoms makes them more appealing in the clinical practice of child psychiatry. Nonetheless, haloperidol and pimozide continue to be used, especially in the treatment of Tourette’s syndrome.
Common Characteristics of Typical Neuroleptics The common characteristic among typical neuroleptics is their ability to antagonize dopamine receptors in the CNS. Activity in the mesocortical region is presumed to result in their therapeutic effects, and their neurologic side-effect profile is attributed to activity in the nigrostriatal region. Dopamine antagonism in the tuberoinfundibular tract results in endocrine effects, such has hyperprolactinemia [Sadock and Sadock, 2003]. Typical neuroleptics can be classified by their chemical structure. In clinical practice, classification according to dopamine receptor binding potency is more practical. Highpotency neuroleptics (e.g., haloperidol, fluphenazine, pimozide) are more likely to cause extrapyramidal symptoms, whereas low-potency neuroleptics (e.g., chlorpromazine, thioridazine) are more likely to cause side effects mediated by cholinergic (e.g., dry mouth, constipation), α1adrenergic (e.g., vasodilation and orthostatic hypotension), and histaminic receptor activity (e.g., sedation, weight gain) (Table 39-8) [Sadock and Sadock, 2003]. Non–dopamine-mediated side effects include orthostatic hypotension, peripheral anticholinergic effects (i.e., dry mouth, blurred vision, constipation, urinary retention, and mydriasis), central anticholinergic effects (i.e., agitation, delirium, hallucinations, seizures, and coma), hyperprolactinemia, leukopenia, agranulocytosis, jaundice, photosensitivity, decreased seizure threshold, and weight gain. Thioridazine has been associated with irreversible retinal pigmentation. Chlorpromazine has been associated with skin pigmentation and deposits in the lens and cornea, which usually do not affect vision. Cardiotoxicity and sudden death have been associated with some typical neuroleptics, especially low-potency neuroleptics. Dose-related prolongation of the QTc interval,
Lee and Walkup / Neuropsychopharmacology
965
TABLE 39-8 Representative Dopamine Antagonists: Comparison of Potency, Side-Effect Profile, and Dosing DRUG
PREPARATIONS
POTENCY
SEDATIVE EFFECT
ANTICHOLINERGIC EFFECT
EXTRAPYRAMIDAL EFFECT
DOSING
Chlorpromazine
Thorazine (10-, 25-, 50-, 100-, and 200-mg tablets) Syrup (10 mg/5 mL) Concentrate (30 mg/mL, 100 mg/mL) Haldol (0.5-, 1-, 2-, 5-, 10-, and 20-mg)
Low
High
High
Low
High
Low
Low
High
Orap (1- and 2-mg tablets)
High
Low
Low
High
Age ≤ 12 yr: 0.25 mg/kg every 4 to 6 hr as needed Age >12 yr: 10 mg tid to 25 mg qid; titrate with increases of 20 to 50 mg once or twice per week. Initial dose of 0.5 mg/day; increase gradually by 0.5 mg every 5-7 days until therapeutic effect is achieved or increase is prohibited by side effects Initial dose of 0.05 mg/kg; increase gradually by 0.5 mg once or twice per week until therapeutic effect is achieved or increase is prohibited by side effects; maximum dose of 10 mg/day or 0.2 mg/kg/day
Haloperidol
Pimozide
arrhythmias, torsade de pointes, and sudden death have been reported with thioridazine. Chlorpromazine may cause nonspecific, reversible Q- and T-wave abnormalities, and sudden death has been reported. Pimozide, especially when combined with CYP3A4 inhibitors, has been associated with cardiotoxicity. Neurologic adverse effects are seen more commonly with high-potency neuroleptics (Table 39-9). Parkinsonism has been observed in children and adolescents treated with typical neuroleptics [Campbell et al., 1985; Richardson
et al., 1991]. Symptoms include cogwheel rigidity, shuffling gait, bradykinesia, masklike facies, stooped posture, coarse tremor, perioral tremor (i.e., rabbit syndrome), and akinesia (i.e., lack of initiative). Symptoms may be managed by reducing the dose of the neuroleptic or addition of anticholinergic medications such as benztropine (Cogentin) or antihistamines such as diphenhydramine (Benadryl). Acute dystonic reactions, which are slow, sustained muscular contractions, may occur within hours to days of initiation of neuroleptics. They may be painful and
TABLE 39-9 Extrapyramidal Symptoms Associated with Neuroleptic Medications NEUROLOGIC SIDE EFFECTS
TIME COURSE
SYMPTOMS
INTERVENTION
Parkinsonism
Within 5 to 90 days of initiation
Anticholinergic medications: benztropine (Cogentin) and diphenhydramine (Benadryl)
Acute dystonia
Within hours to days of initiation
Akathisia
Any time during treatment
Cogwheel rigidity, shuffling gait, bradykinesia, masklike facies, stooped posture, coarse tremor, perioral tremor (rabbit syndrome), akinesia (lack of initiative), ataraxia (indifference toward the environment) Slow, sustained muscular contractions involving any part of the body, which may be painful: eyes (oculogyric crisis), neck (torticollis or retrocollis), tongue, jaw, whole body (opisthotonos) Motor restlessness and muscular discomfort.
Tardive dyskinesia
Any time during treatment; risk increases with duration of treatment
Neuroleptic malignant syndrome
Any time during treatment
Involuntary choreoathetoid movements in muscles of the head (perioral movements, lip smacking, grimacing, tongue protrusion, lateral jaw movements), trunk (trunk twisting and pelvic thrusting), and extremities Muscle rigidity, fever, autonomic instability, delirium, elevated levels of creatine phosphokinase, leukocytosis, rhabdomyolysis, myoglobinuria, renal failure
Intramuscular anticholinergic medication
Decreased dose of neuroleptic; anticholinergic medications; propranolol Monitor severity of movements with objective ratings; decreased dose of typical neuroleptic; discontinue typical neuroleptic; switch to atypical neuroleptic Emergency medical treatment and immediate discontinuation of neuroleptic
966
Neurobehavioral Disorders / 39
frightening to patients and families who are not forewarned of this possible side effect. Dystonias may involve the eyes (i.e., oculogyric crisis), neck (i.e., torticollis or retrocollis), tongue, jaw, or entire body (i.e., opisthotonos). Use of 1 to 2 mg of intramuscular benztropine or 25 to 50 mg of oral or intramuscular diphenhydramine can relieve the dystonia within several minutes. Akathisia is a persistent, uncomfortable restlessness. Patients may constantly rock or pace around the room and secondarily feel depressed and dysphoric. Extreme cases have been described of patients developing suicidal ideation and behavior [Van Putten and Marder, 1987]. Dosage reduction or propranolol sometimes brings relief [Adler et al., 1986]. Tardive dyskinesia is a syndrome of involuntary movements, characterized by choreoathetoid movements of the muscle in the head, trunk, extremities, or the entire body. Tardive dyskinesia may occur any time during treatment with neuroleptics, or it may be associated with neuroleptic withdrawal (i.e., withdrawal dyskinesia). The prevalence of neuroleptic-induced and withdrawal dyskinesia in children and adolescents has ranged from 0% to 51%. The risk of developing withdrawal dyskinesias increases with the duration of neuroleptic treatment. The risk is higher in females, children, the elderly, and patients with brain damage or mood disorders. Withdrawal dyskinesias may resolve over the course of weeks to months [Baldessarini, 1990]; however, irreversible tardive dyskinesia has been reported. The presence of preexisting involuntary movements should be assessed with objective rating scales, such as the Abnormal Involuntary Movement Scale (AIMS). Serial assessments should be completed every 3 months during neuroleptic therapy. An increase in involuntary movements should prompt a discussion with the patient and family about treatment options. There are no consistently useful treatments for tardive dyskinesia, although symptom reduction has occurred with many medications from different classes. The most consistently effective medications are neuroleptics, but continued exposure may make tardive dyskinesia symptoms worse over time. Neuroleptic malignant syndrome is a rare and potentially fatal adverse effect, which may occur any time during treatment with neuroleptics, but it may be more likely to occur in the first 2 weeks [Addonizio et al., 1987]. The frequency of occurrence has been 0.02% to 2.44% with typical neuroleptics [Khan and Farver, 2000]. It is characterized by symptoms in four major areas: autonomic instability, extrapyramidal symptoms, hyperpyrexia, and altered mental status. Specific symptoms include muscle rigidity, hyperpyrexia (mean temperature of 103 ± 1.9° F [Rosebush and Stewart, 1989]), sweating, increased blood pressure and heart rate, confusion, agitation, and possible renal failure. Laboratory findings include leukocytosis; elevated levels of serum creatine phosphokinase, liver transaminases, and myoglobin; and myoglobinuria. In a review of 49 cases of neuroleptic malignant syndrome, the mortality rate among children was 27%, and the mortality rate among adolescents was 13% [Latz and McCracken, 1992]. Treatment involves immediate hospitalization for supportive treatment and discontinuation of the neuroleptic drug.
Haloperidol Clinical Applications Haloperidol is approved for the treatment of psychotic disorders and for Tourette’s syndrome. It is approved for use in treating children with severe behavioral disorders that have not responded to nonpharmacologic interventions or non-antipsychotic medications [Haloperidol, 2001]. In clinical practice, it is sometimes administered intramuscularly as a chemical restraint to acutely stabilize agitated and aggressive patients who pose an immediate threat to themselves or others when alternative measures have failed. Haloperidol appears to be effective in children with schizophrenia [Green et al., 1992; Spencer et al., 1992]. It appears to be effective in improving behavior in children with autism [Anderson et al., 1984; Joshi et al., 1988] and in reducing tics in Tourette’s syndrome [Sallee et al., 1997; Shapiro and Shapiro, 1989].
Pharmacology Haloperidol is a high-potency dopamine receptor antagonist. It is available in oral tablets, an oral concentrate, parenteral preparations (intramuscular or intravenous), and depot intramuscular injections (Haldol decanoate). Oral haloperidol is well absorbed from the gastrointestinal tract and undergoes first-pass metabolism in the liver. Peak plasma concentrations are reached within 2 to 6 hours. Peak plasma haloperidol concentration occurs 10 to 20 minutes after intramuscular injection. Peak pharmacologic action occurs within 30 to 45 minutes in agitated patients. In psychotic patients, improvement may be seen within 30 to 60 minutes, and the effects increase over the next 2 hours. Haldol decanoate is released slowly, with peak concentrations occurring 6 to 7 days after injection. Steady-state concentrations are achieved in approximately 3 months with monthly injections. Haloperidol is metabolized by the liver and excreted in urine and feces [Haldol, 2001].
Dosing For children between the ages of 3 and 12 years, haloperidol may be initiated at 0.5 mg/day. The dose may be increased by increments of 0.5 mg at 5- to 7-day intervals to a clinically therapeutic dose. Dosing recommendations for psychotic disorders is 0.05 to 0.15 mg/kg/day. For nonpsychotic behavior disorders and Tourette’s syndrome, the therapeutic range is 0.05 to 0.075 mg/kg/day [Haldol, 2001].
Adverse Effects Adverse effects of haloperidol are characteristic of highpotency typical neuroleptics (see “Common Characteristics of Typical Neuroleptics”). Rates of acute dystonic reaction with haloperidol have been observed to be 16.7% and 25% in children treated for schizophrenia [Green et al., 1992; Spencer et al., 1992]. The rate of withdrawal tardive dyskinesia observed in a long-term study in autistic children was 33.9%. Higher cumulative dose, female gender, and perinatal complications appeared to increase risk [Campbell et al., 1997].
Lee and Walkup / Neuropsychopharmacology
967
Drug Interactions
Clinical Management
Medications that inhibit the cytochrome P-450 isoenzyme system can increase serum concentrations of haloperidol. The combination of such medications with haloperidol has been associated with neurotoxicity and cases of irreversible brain damage.
Before beginning pimozide, the patient should undergo a thorough psychiatric and medical evaluation. Potential drug interactions and co-occurring psychiatric or medical conditions that may contraindicate pimozide (e.g., history of arrhythmias, congenital long QT, pregnancy, conditions that alter potassium levels) require adjustment in medication management or independent intervention (e.g., ADHD, obsessive-compulsive disorder). Baseline measurements that may be helpful include laboratory screening (i.e., complete blood cell count, electrolyte determinations, tests of renal function and thyroid function, prolactin level, glucose concentration, and urine drug screen), height, weight, and baseline assessment of the extrapyramidal system [Bryden et al., 2001]. Because pimozide can prolong the QT interval, serial ECGs should be obtained at baseline and during dose titration. When monitoring ECGs, the QTc interval should remain less than 0.47 seconds or less than 25% above baseline [Green, 1995]. A pediatric cardiologist should be consulted if the ECG is equivocal. In addition to the baseline ECG, electrolyte levels should be obtained, because serum potassium levels can affect cardiac conduction. Pimozide may be initiated at 0.05 mg/kg and gradually increased by 0.5 mg once or twice weekly. Doses greater than 0.2 mg/kg/day or 10 mg/day are not recommended [Orap, 2004]. Efficacy (i.e., severity and frequency of tics) and safety (i.e., serial ECGs and serum electrolytes) of pimozide should be actively monitored over time.
Pimozide Clinical Applications Pimozide (Orap) is labeled for use in the treatment of Tourette’s syndrome in patients who have failed to respond to standard treatment and experience severe impairment from tics. Pimozide has been shown to be effective in decreasing tics [Sallee et al., 1997; Shapiro and Shapiro, 1984; Shapiro et al., 1983]. However, the atypical neuroleptic risperidone appears to be more efficacious in decreasing tics when directly compared with pimozide [Bruggeman et al., 2001; Gilbert et al., 2004], and it has a more favorable side-effect profile.
Pharmacology Pimozide is a high-potency dopamine receptor antagonist. It is metabolized by the liver, primarily by CYP3A4 and to a lesser extent by CYP1A2, and it is excreted in urine. Mean serum half-life is about 55 hours [Orap, 2004].
TABLE 39-10 Serotonin-Dopamine Antagonists: Comparison of Receptor Activity and Dosing DRUG
PREPARATIONS
DOPAMINE RECEPTOR ACTIVITY
SEROTONIN RECEPTOR ACTIVITY
Risperidone
Risperdal (0.25-, 0.5-, 1-, 2-, 3-, and 4-mg tablets) Risperdal M-TAB (0.5-, 1-, and 2-mg tablets) Risperdal Elixir (1 mg/mL) Zyprexa (2.5-, 5-, 7.5-, 10-, 15-, and 20-mg tablets) Zyprexa Zydis (5-, 10-, 15-, and 20-mg tablets) Seroquel (25-, 100-, 200-, and 300-mg tablets) Geodon (20-, 40-, 60-, and 80-mg tablets)
D2
5HT2A
D1, D2, D4
5HT2A
D1, D2
Olanzapine
Quetiapine Ziprasidone
Aripiprazole
Abilify (5-, 10-, 15-, 20-, and 30-mg tablets)
ANTICHOLINERGIC RECEPTOR ACTIVITY
ADRENERGIC RECEPTOR ACTIVITY
HISTAMINE RECEPTOR ACTIVITY
DOSING
α1, α2
H1
Initial dose of 0.25 to 0.5 mg; increase by 0.25 to 0.5 mg/week
α1
H1
Initial dose of 2.5 to 5 mg; increase by 2.5 to 5 mg/week; maximum dose of 20 mg/day
5HT2, 5HT6
α1, α2
H1
D2, D3, D4
5HT1D, 5HT2A, 5HT2C
α1
H1
Partial D2 agonist
5HT1A, 5HT2A
α1
H1
Initial dose of 12.5 to 25 mg/day; increase by 25 to 50 mg/day Initial dose of 20 mg/day; increase gradually; maximum of 160 mg/day Initial dose 5 mg to 10 mg per day; gradually increase by 5 mg to 10 mg every 2 wk; maximum 30 mg/day
M1-M5
968
Neurobehavioral Disorders / 39
Adverse Effects Adverse effects of pimozide are those typical of highpotency neuroleptics (see “Common Characteristics of Typical Neuroleptics”). Pimozide has been associated with QT prolongation, serious cardiac arrhythmias, and sudden death. Use of pimozide with clarithromycin (Biaxin), erythromycin, azithromycin (Zithromax), and dirithromycin (Dynabac) is contraindicated by the Food and Drug Administration because of the risk of cardiotoxicity with these combinations [Orap, 2004].
SEROTONIN-DOPAMINE ANTAGONISTS: ATYPICAL NEUROLEPTICS Common Characteristics Serotonin-dopamine antagonists, or atypical neuroleptics, differ from conventional or typical neuroleptics in that they block serotonin receptors in addition to dopamine receptors. Each atypical neuroleptic possesses different affinities at dopamine, serotonin, adrenergic, cholinergic, and histaminic receptors, which result in different side-effect profiles and clinical effects (Table 39-10). Atypical neuroleptics offer advantages over typical neuroleptics in their ability to improve the negative and positive symptoms of schizophrenia and their lower risk of producing extrapyramidal symptoms. However, they may pose other health risks with regard to weight gain, insulin resistance, and hyperlipidemia. Compared with adults, children appear to carry a greater risk of developing extrapyramidal symptoms [Lewis, 1998]. Development of tardive dyskinesia was more likely in children and adolescents treated with typical neuroleptics compared with atypical agents [Connor et al., 2001]. Among the atypical neuroleptics, extrapyramidal symptoms appear to occur more frequently with risperidone than with quetiapine or olanzapine [Findling et al., 2000; Grcevich et al., 1996]. As experience with atypical neuroleptics in the pediatric population has increased, greater attention has been paid to their weight gain effects. In children and adolescents, weight gain has been associated with risperidone [Hellings et al., 2001; Martin et al., 2000; Zuddas et al., 2000], olanzapine [Findling et al., 2000], and quetiapine therapy [Findling et al., 2000]. Olanzapine appears to have the greatest tendency to produce weight gain, followed by risperidone and then quetiapine [Findling et al., 2000]. Aripiprazole and ziprasidone do not appear to cause significant weight gain in adults [Keck and McElroy, 2003; Marder et al., 2003; Nasrallah, 2003]. Clinicians need to be sensitive to the weight gain effects of these medications, because significant weight gain is likely to affect a child or adolescent’s selfesteem and may lead to noncompliance with the medication and reduced efficacy. Recommendations to increase exercise and to make healthier food choices may be effective with motivated patients and families. Studies have indicated that atypical antipsychotic medications are associated with metabolic disturbances such as increased insulin resistance [Haupt and Newcomer, 2001], metabolic syndrome [L’Italien, 2003], and dys-
lipidemia [Lindenmayer et al., 2003]. Patients treated with olanzapine and clozapine appear to have higher insulin resistance compared with those treated with risperidone, typical antipsychotics, and control subjects [Newcomer et al., 2002]. Clozapine, olanzapine, and quetiapine treatment were more frequently associated with elevations of serum lipids (i.e., triglycerides, total cholesterol, and lowdensity lipoprotein cholesterol) compared with risperidone, ziprasidone, and aripiprazole [Casey, 2004]. New-onset cases of type 2 diabetes mellitus have been associated with atypical neuroleptics, 25% of which occur in the absence of substantial weight gain or obesity [Haupt and Newcomer, 2001]. These patients are at risk for diabetic ketoacidosis, which has a mortality rate of 6% to 10% if not recognized and treated promptly [Gomez Diaz et al., 1996; Lebovitz, 1995; Malone et al., 1992]. Typical antipsychotics, risperidone, and olanzapine increase serum prolactin levels [Tandon and Halbreich, 2003]. These elevations have not been observed with clozapine and quetiapine [Stigler et al., 2001]. Given the possible adverse effects of neuroleptics and the increasing use of neuroleptics for off-label use, careful monitoring of pediatric patients is necessary. A comprehensive psychiatric evaluation should include an assessment for the risk of adverse effects. Recommended baseline measurements include laboratory screening (e.g., complete blood cell count, electrolytes, liver and renal function tests, thyroid function test, prolactin and glucose levels, urine drug screen), height, weight [Bryden et al., 2001], and baseline assessment of extrapyramidal symptoms using clinician ratings (e.g., AIMS). A baseline ECG is recommended before initiating risperidone, olanzapine, quetiapine, or ziprasidone.
Risperidone Clinical Applications Risperidone (Risperdal) is labeled for use in the treatment of psychotic disorders and the manic phase of bipolar disorder in adults. In children and adolescents, it has been found to be effective for psychotic disorders [Armentaros et al., 1997; Grcevich et al., 1996; Quintana and Keshavan, 1995], bipolar disorder [Frazier et al., 1999; Schreier, 1998], conduct disorder [Findling et al., 2000], aggressive behavior in children with subaverage IQ [Aman et al., 2002; Buitelaar et al., 2001; Snyder et al., 2002], autism [Fisman and Steele, 1996; Hellings et al., 2001; Masi et al., 2001; McCracken et al., 2002; McDougle et al., 1997; Zuddas et al., 2000], tic disorders [Bruggeman et al., 2001; Dion et al., 2002; Gaffney et al., 2002; Lombroso et al., 1995; Scahill et al., 2003], and co-occurring tic disorders and obsessive-compulsive disorder [Bruggeman et al., 2001; Gaffney et al., 2002].
Pharmacology Risperidone is a serotonin-dopamine antagonist with activity at serotonin 5HT2A, dopamine D2, α1- and α2adrenergic, and histaminic H1 receptors. It is available in tablets, solution, orally disintegrating tablets, and injectable preparations. It is well absorbed in the gastrointestinal tract, and it undergoes extensive first-pass metabolism by
Lee and Walkup / Neuropsychopharmacology
CYP2D6 to its active metabolite, 9-hydroxyrisperidone. The mean half-life of both forms is about 20 hours [Risperdal, 2004].
Clinical Management Given the risks of serious adverse effects and the lack of knowledge regarding possible long-term adverse effects in the pediatric population, consideration of alternative nonpharmacologic and pharmacologic interventions is advised. A thorough risk-benefit analysis should be part of the informed consent discussion with the parent or guardian. Baseline assessment includes evaluation of potential risk factors (i.e., cardiovascular disease, hepatic or renal impairment, pregnancy, and diabetes), preexisting movement disorders, and fasting glucose levels. Risperidone can be initiated at 0.25 to 0.5 mg/day, increasing the dose by small increments weekly.
Adverse Effects Risperidone may be associated with sedation, orthostatic hypotension [Toren et al., 1998], gastrointestinal side effects, elevations in hepatic transaminase levels, fatty liver infiltrates [Kumra et al., 1997], and increased appetite with weight gain [Toren et al., 1998]. Neurologic side effects include extrapyramidal symptoms [Mandoki, 1995], which are dose dependent, and tardive dyskinesia, whose risk increases with duration of treatment [Leucht et al., 1999]. The most serious adverse effect is neuroleptic malignant syndrome [Feeney and Klykylo, 1996; Toren et al., 1998]. This potentially fatal condition is characterized by hyperpyrexia, muscle rigidity, altered mental status, autonomic instability, elevated creatine phosphokinase level, myoglobinuria, and acute renal failure. Risperidone or its metabolite can prolong the QT interval in some patients, which can lead to cardiac arrhythmia if combined with medications with similar effects. Risperidone has been associated with hyperprolactinemia. In 2003, the labeling of risperidone was revised to include warnings of cerebrovascular adverse events in elderly patients with dementia [Risperdal, 2004].
Drug Interactions Risperidone may potentiate sedative and hypotensive effects of other medications. Risperidone can increase plasma concentrations of clozapine. Combination with phenytoin or selective serotonin re-uptake inhibitors may cause increased extrapyramidal symptoms [Sadock and Sadock, 2003]. Inhibitors of CYP2D6 decrease the metabolism of risperidone to 9-hydroxyrisperidone, which does not appear to cause adverse effects. Risperidone is a weak inhibitor of CYP2D6 and has little effect on the metabolism of other medications.
Olanzapine
969
prophylaxis in bipolar disorder. In adults with schizophrenia, olanzapine was found to be comparable to haloperidol in treating positive symptoms and superior in treating negative symptoms [Tollefson and Kuntz, 1999]. It has been shown to be beneficial in the treatment of schizophrenia in children and adolescents [Findling et al., 2003; Kumra et al., 1998; Mozes et al., 2003]. It has also been used in the treatment of juvenile bipolar disorder [Chang and Ketter, 2000; Frazier et al., 2001], autism [Heimann, 1999; Malone et al., 2001; Potenza et al., 1999; Rubin, 1997], and Tourette’s syndrome [Stamenkovic et al., 2000].
Pharmacology Olanzapine is a serotonin-dopamine antagonist with activity at serotonin 5HT2A/2C; dopamine D1, D2, and D4; α1adrenergic; muscarinic M1-5; and histaminic H1 receptors (Zyprexa, 2004]. Olanzapine is available in a tablet, oral disintegrating tablet (Zyprexa-Zydis), and injectable form. It is well absorbed from the gastrointestinal tract. Approximately 40% of the dose is metabolized by first-pass metabolism. It reaches peak concentration in about 6 hours; its mean half-life is 30 hours [Zyprexa, 2004].
Clinical Management Before initiation of olanzapine, patients should be assessed for risk factors complicating or contraindicating treatment (e.g., diabetes, pregnancy, liver disease, cardiovascular disease). Baseline weight, assessment for preexisting involuntary movements, and laboratory screening, including a fasting blood glucose determination and liver panel, should be completed. Dosing is started at 2.5 to 5.0 mg/day and may be increased by small increments weekly, not to exceed 20 mg/day. Weight, serum glucose concentration, and levels of liver transaminases should be monitored during ongoing therapy.
Adverse Effects Side effects include sedation, orthostatic hypotension, and sialorrhea. The risk of weight gain may be higher than with most atypical neuroleptics [Allison and Casey, 2001; Allison et al., 1999; Wirshing et al., 1999]. Olanzapine has been associated with elevations in liver transaminases, γ-glutamyltransferase, and serum prolactin [Risperdal, 2004]. As with other neuroleptics, patients may experience extrapyramidal symptoms, tardive dyskinesia, and neuroleptic malignant syndrome. In 2004, the labeling of olanzapine was revised to include warnings of possible hyperglycemia, ketoacidosis, hyperosmolar coma, or death resulting from atypical neuroleptics [Zyprexa, 2004]. Patients with diabetes mellitus or those at risk for the disorder are advised to undergo fasting blood glucose testing at baseline. The fasting blood glucose level and clinical symptoms of hyperglycemia should be monitored routinely.
Clinical Applications
Drug Interactions
Olanzapine (Zyprexa) is labeled for use as a treatment for psychotic disorders, manic phase of bipolar disorder, and
Fluvoxamine can increase serum concentrations of olanzapine [Zyprexa, 2004].
970
Neurobehavioral Disorders / 39
Quetiapine Clinical Applications Quetiapine (Seroquel) is labeled for use in the treatment of psychotic disorders, schizophrenia, and the manic phase of bipolar disorder. In adolescents, quetiapine has shown efficacy in the treatment of psychotic disorders [McConville et al., 2000, 2003; Shaw et al., 2001] and bipolar mania [DelBello et al., 2002b]. Two case reports and one small study describe usefulness of quetiapine in Tourette’s syndrome [Mukaddes and Abali, 2003; Parraga et al., 2001]. In one small study of patients with autism and mental retardation, quetiapine was ineffective [Martin et al., 1999].
Pharmacology Quetiapine is a serotonin-dopamine antagonist similar to clozapine in its neurochemical profile. It has activity at serotonin 5HT2A and 5HT6; dopamine D1, D2, and D4; α1and α2-adrenergic; and histaminic H1 receptors. It has been associated with minimal or transient elevations of prolactin. Quetiapine is rapidly absorbed through the gastrointestinal tract, reaching peak plasma levels in 1 to 2 hours. The steady-state half-life is about 6 hours [Seroquel, 2004].
Clinical Management Quetiapine may be initiated at 12.5 to 25 mg/day and increased by increments of 25 to 50 mg/day. The drug is usually given in divided doses two or three times daily. Mean dose in studies of adolescents with psychotic disorders was 467 mg/day [Shaw et al., 2001]. The mean dose in a study of adolescents with bipolar mania was 450 mg/day [DelBello et al., 2002b].
Adverse Effects Side effects of quetiapine include dizziness, postural hypotension, dry mouth, and dyspepsia. Quetiapine is thought to have less risk of weight gain [Findling et al., 2000] and serum prolactin elevation [Stigler et al., 2001]. Development of cataracts in dogs has been observed during animal testing. Lens changes have been observed in patients with long-term use of quetiapine. The manufacturer recommends a baseline ophthalmologic examination and serial examinations every 6 months during treatment [Seroquel, 2004].
Drug Interactions Phenytoin and thioridazine increase clearance of quetiapine. Inhibitors of CYP3A4 decrease clearance of quetiapine, significantly increasing serum concentrations [Seroquel, 2004].
Ziprasidone Pharmacology Ziprasidone (Geodon) is a serotonin-dopamine antagonist with activity at serotonin 5HT1D, 5HT2A, 5HT-2C; dopamine D2, D3, and D4; α1-adrenergic; and histaminic H1 receptors. It is an agonist at 5HT1A and inhibits uptake of serotonin and norepinephrine [Geodon, 2004].
Clinical Applications Ziprasidone is labeled for use in the treatment of psychotic disorders in adults. In clinical practice, its main advantage over other atypical antipsychotics is its weight-neutral effects [Keck and McElroy, 2003; Marder et al., 2003; Nasrallah, 2003]. Clinicians may be hesitant to use it because of its effects on the QT interval and the lack of data on safety and efficacy in the pediatric population. In a study of 12 patients with autism spectrum disorder, 6 were responders, and 2 patients with co-occurring bipolar disorder were rated much worse [McDougle et al., 2002]. In a study of children and adolescents with Tourette’s syndrome, reduction of tics was significant in patients treated with ziprasidone versus placebo (35% versus 7%) [Sallee et al., 2000b].
Pharmacology Ziprasidone is extensively metabolized in the liver. About one third of ziprasidone’s metabolic clearance is mediated by the CYP3A4 isoenzyme [Geodon, 2004].
Clinical Management Before initiating ziprasidone, a careful history must be obtained to identify possible contraindications, including concomitant use of drugs known to prolong the QTc interval, history of congenitally long QT syndromes, history of cardiovascular disease or cardiac arrhythmia, and conditions that place the patient at risk for electrolyte disturbances. Baseline ECG, serum electrolytes, renal and hepatic screens, and complete blood cell count should be obtained. Ziprasidone is available in oral (ziprasidone hydrochloride) and injectable (ziprasidone mesylate) forms. Initial adult dosage of ziprasidone hydrochloride is 20 mg taken twice daily, which may be incrementally increased after a minimum of 2 days. Maximum dosage recommended by the manufacturer is 80 mg taken twice daily [Geodon, 2004]. The mean dosage used by Sallee and colleagues [2000b] in a study of ziprasidone in 28 children and adolescents with tic disorders was 28 mg/day. Ziprasidone was initiated at 5 mg/day and flexibly titrated to a maximum dose of 40 mg/day. Within this dosage range, ziprasidone was well tolerated with no cardiac adverse effects. In adults, intramuscular ziprasidone can be used to control acute agitation in patients with schizophrenia; 10 to 20 mg is given as a single dose. Use in patients who are already receiving oral ziprasidone should be avoided because the safety of concomitant use has not been established [Geodon, 2004]. No data are available on the safety or efficacy of intramuscular ziprasidone in children or adolescents.
Adverse Effects The most common side effects of ziprasidone are somnolence, extrapyramidal symptoms, and respiratory disorder. Other side effects of ziprasidone include rash, orthostatic hypotension, decreased seizure threshold, and hyperprolactinemia. Ziprasidone has been associated with prolongation of the QT interval, which may increase the risk of
Lee and Walkup / Neuropsychopharmacology
fatal arrhythmias, such as torsades de pointes, or sudden death [Geodon, 2004].
Drug Interactions Use of ziprasidone is contraindicated in patients who are taking medications that are known to prolong the QTc interval. Psychiatric medications in this category include thioridazine, chlorpromazine, droperidol, pimozide, and tricyclic antidepressants. Ziprasidone may potentially interact with inducers or inhibitors of CYP3A4. It potentially has additive hypotensive effects when combined with hypotensive agents and potential additive sedative effects when combined with CNS agents [Geodon, 2004].
Aripiprazole Clinical Applications Aripiprazole (Abilify) is labeled for use in the treatment of schizophrenia in adults. It has been shown to be superior to placebo in managing positive and negative symptoms of schizophrenia [Kane et al., 2002; McGavin and Goa, 2002].
Pharmacology Aripiprazole differs from other atypical neuroleptics in its pharmacodynamic properties. It is a partial agonist at the dopamine D2 receptor. It has serotonin antagonist activity at 5HT2A receptors and partial agonist activity at 5HT1A receptors. It has moderate affinity for α1-adrenergic and histaminic H1 receptors, but it has no activity at cholinergic muscarinic receptors. Aripiprazole is well absorbed, with peak plasma concentrations attained in 3 to 5 hours. It is highly bound to plasma proteins, and it is metabolized by the liver. The isoenzymes CYP3A4 and CYP2D6 are involved in its metabolism [Abilify, 2004].
Clinical Management Initial evaluations should incorporate an assessment of risk factors, including a history of cardiovascular disease, seizure disorder, pregnancy, and use of medications that potentially interact with aripiprazole. In adults, the recommended initial and target dosages of aripiprazole are 10 or 15 mg/day. Dosage adjustments should not be made at intervals less than 2 weeks because of the slow rate at which steady-state concentrations are achieved [Abilify, 2004].
Adverse Effects Side effects include headache, fatigue, hypotension, gastrointestinal side effects, anorexia, insomnia, somnolence, and blurred vision. In short-term and long-term placebocontrolled trials there were no differences in the extrapyramidal symptoms, lipid profile, or electrocardiographic parameters between active drug and placebo [Abilify, 2004].
Drug Interactions Because aripiprazole is metabolized by CYP3A4 and CYP2D6, serum concentrations may be affected by medica-
971
tions that induce or inhibit these isoenzymes. In vivo studies revealed that aripiprazole had no significant effect on metabolism through CYP2D6, CYP2C9, CYP2C19, or CYP3A4. In vitro studies demonstrated that it had no effect on CYP1A2 activity [Abilify, 2004].
CONCLUSIONS Many factors have led to an increased use of psychotropic medications in children and adolescents. Newer data suggest more opportunities for children to benefit but also raise more concerns about safety and monitoring. To support this increased use of psychotropic medications, more studies are needed to assess the acute efficacy of newer medications and the long-term safety and efficacy of most psychotropic agents. Developing standards for active monitoring of children on psychotropic medications may result in changes in physician practice, increasing problems with access to physicians and perhaps worsening outcomes. Despite these many challenges, children can and do benefit from medications when treatment is provided in the context of a thorough diagnostic assessment that integrates information from multiple sources; knowledge of the available data for adults and children in the literature; knowledge of standards of community care, especially when prescribing medications off-label; an analysis of the risks and benefits of treatment options; appropriate involvement of the parent or guardian in the informed consent process; and close monitoring for adverse effects during therapy. REFERENCES AACAP. American Academy of Child and Adolescent Psychiatry practice parameters for the assessment and treatment of children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 1997a;10 (Suppl):69S. AACAP. American Academy of Child and Adolescent Psychiatry practice parameter for assessment of children and adolescents. J Am Acad Child Adolesc Psychiatry 1997b;10 (Suppl):49S. AACAP. American Academy of Child and Adolescent Psychiatry practice parameters for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1997c;10 (Suppl):177S. AACAP. American Academy of Child and Adolescent Psychiatry practice parameter for the assessment and treatment of children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;10 (Suppl):157S. Abilify. Abilify product information. Princeton, NJ: Bristol-Myers Squibb, 2004. Adderall. Adderall product information. Newport, KY: Shire Pharmaceuticals, 2004. Addonizio G, Susman VL, Roth SD. Neuroleptic malignant syndrome: Review and analysis of 115 cases. Biol Psychiatry 1987;22:1004. Adler L, Angrist B, Peselow E, et al. A controlled assessment of propranolol in the treatment of neuroleptic-induced akathisia. Br J Psychiatry 1986;149:42. Alessi N, Bos T. A controlled assessment of propranolol in the t reatment of neuroleptic-induced akathisia. Am J Psychiatry 1991;11:1605. Alessis N, Naylor MW, Ghaziuddin M, et al. Update on lithium carbonate therapy in children and adolescents. J Am Acad Child Adolesc Psychiatry 1999;33:291. Allison DB, Casey DE. Antipsychotic-induced weight gain: A review of the literature. J Clin Psychiatry 2001;62 (Suppl 7):22. Allison DB, Mentore JL, Heo M, et al. Antipsychotic-induced weight gain: A comprehensive research synthesis. Am J Psychiatry 1999;156:1686.
972
Neurobehavioral Disorders / 39
Aman MG, De Smedt G, Derivan A. Double-blind, placebo-controlled study of risperidone for the treatment of disruptive behaviors in children with subaverage intelligence. Am J Psychiatry 2002;159:1337. Anderson JC, Campbell M, Grega DM, et al. Haloperidol in the treatment of infantile autism: Effects on learning and behavioral symptoms. Am J Psychiatry 1984;141:1195. Anderson JC, Williams S, McGee R. DSM-III disorders in preadolescent children: Prevalence in a large sample from the general population. Arch Gen Psychiatry 1987;44:69. APA. Diagnostic and statistical manual of mental disorders, 4th ed. DSM-IV. Washington, DC: American Psychiatric Association, 1994. APA. American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. 1997;154 (Suppl):1. APA. American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159(Suppl):1. Armenteros JL, Whitaker AH, Welikson M, et al. Risperidone in adolescents with schizophrenia: An open pilot-study. J Am Acad Child Adolesc Psychiatry 1997;36:694. Baldessarini RJ. Drugs and the treatment of psychiatric disorders. New York: Pergamon Press, 1990. Ballenger JC, Carek DJ, Steele JJ, et al. Three cases of panic disorder with agoraphobia in children. Am J Psychiatry 1989;146:922. Ballenger JC, Post RM. Carbamazepine in manic-depressive illness: A new treatment. Am J Psychiatry 1980;137:782. Barkley R. Attention-deficit/hyperactivity disorder. New York: Guilford, 1996. Barrickman LL, Perry PJ, Allen AJ, et al. Bupropion versus methylphenidate in the treatment of attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1995;5:649. Barrueto F, Hack JB. Hyperammonemia and coma without hepatic dysfunction induced by valproate therapy. Acad Emerg Med 2001;8:999. Bernstein GA. Comorbidity and severity of anxiety and depressive disorders in a clinic sample. J Am Acad Child Adolesc Psychiatry 1991;1:43. Bernstein GA, Borchardt CM, Perwien AR, et al. Imipramine plus cognitive-behavioral therapy in the treatment of school refusal. J Am Acad Child Adolesc Psychiatry 2000;3:276. Biederman J. Clonazepam in the treatment of prepubertal children with panic-like symptoms. J Clin Psychiatry 1987;48 (Suppl):38. Biederman J. Psychopharmacology. Washington DC: American Psychiatric Press, 1991. Biederman J. Pharmacotherapy for attention-deficit/hyperactivity disorder (ADHD) decreases the risk for substance abuse: Findings from a longitudinal follow-up of youths with and without ADHD. J Clin Psychiatry 2003;64 (Suppl 11):3. Biederman J, Baldessarini RJ, Wright V, et al. A double-blind placebo controlled study of desipramine in the treatment ADD. II. Serum drug levels and cardiovascular findings. J Am Acad Child Adolesc Psychiatry 1989;6:903. Biederman J, Gastfriend DR, Jellinek MS. Desipramine in the treatment of children with attention deficit disorder. J Clin Psychopharmacol 1986;6:359. Biederman J, Mick E, Bostic JQ, et al. The naturalistic course of pharmacologic treatment of children with maniclike symptoms: A systematic chart review. J Clin Psychiatry 1998;11:628. Birmaher B, Axelson DA, Monk K, et al. Fluoxetine for the treatment of childhood anxiety disorders. J Am Acad Child Adolesc Psychiatry 2003;4:415. Birmaher B, Greenhill LL, Cooper TB, et al. Sustained release methylphenidate: Pharmacokinetic studies in ADDH males. J Am Acad Child Adolesc Psychiatry 1989;5:768. Black B, Robbins DR. Panic disorder in children and adolescents. J Am Acad Child Adolesc Psychiatry 1990;1:36. Bohan TP, Helton E, McDonald I, et al. Effect of L-carnitine treatment for valproate-induced hepatotoxicity. Neurology 2001;10:1405. Borcherding BG, Keysor CS, Rapoport JL, et al. Motor/vocal tics and compulsive behaviors on stimulant drugs: Is there a common vulnerability? Psychiatry Res 1990;1:83. Boulos C, Kutcher S, Marton P, et al. Response to desipramine treatment in adolescent major depression. Psychopharmacol Bull 1991;1:59. Bowden CL, Calabrese JR, McElroy SL, et al. The efficacy of lamotrigine in rapid cycling and non-rapid cycling patients with bipolar disorder. Biol Psychiatry 1999;8:953.
Bowden CL, Calabrese JR, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently manic or hypomanic patients with bipolar I disorder. Arch Gen Psychiatry 2003;4:392. Bowring MA, Kovacs M. Difficulties in diagnosing manic disorders among children and adolescents. J Am Acad Child Adolesc Psychiatry 1992;4:611. Bremner JD. A double-blind comparison of Org 3770, amitriptyline, and placebo in major depression. J Clin Psychiatry 1995;11:519. Brown RT, Sexson SB. Effects of methylphenidate on cardiovascular responses in attention deficit hyperactivity disordered adolescents. J Adolesc Health Care 1989;3:179. Brown TE. Atomoxetine and stimulants in combination for treatment of attention deficit hyperactivity disorder: Four case reports. J Child Adolesc Psychopharmacol 2004;1:129. Brown TE, Gammon GD. ADHD-associated difficulties falling asleep and awakening: Clonidine and methylphenidate treatments. Proceedings of the Annual Meeting of the American Academy of Child and Adolescent Psychiatry, Washington DC, 1992. Bruggeman R, van der Linden C, Buitelaar JK, et al. Risperidone versus pimozide in Tourette’s disorder: A comparative double-blind parallelgroup study. J Clin Psychiatry 2001;1:50. Bryden KE, Carrey NJ, Kutcher SP. Update and recommendations for the use of antipsychotics in early-onset psychoses. J Child Adolesc Psychopharmacol 2001;2:113. Buitelaar JK, van der Gaag RJ, Cohen-Kettenis P, et al. A randomized controlled trial of risperidone in the treatment of aggression in hospitalized adolescents with subaverage cognitive abilities. J Clin Psychiatry 2001;4:239. Buitelaar JK, van der Gaag RJ, van der Hoeven J. Buspirone in the management of anxiety and irritability in children with pervasive developmental disorders: Results of an open-label study. J Clin Psychiatry 1998;2:56. BuSpar. BuSpar product information. Princeton, NJ: Bristol-Myers Squibb, 2002. Calabrese JR, Bowden CL, Sachs G, et al. A placebo-controlled 18-month trial of lamotrigine and lithium maintenance treatment in recently depressed patients with bipolar I disorder. J Clin Psychiatry 2003;9:1013. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebocontrolled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;2:79. Calabrese JR, Suppes T, Bowden CL, et al. A double-blind, placebocontrolled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. Lamictal 614 Study Group. J Clin Psychiatry 2000;11:841. Campbell M, Armenteros JL, Malone RP, et al. Neuroleptic-related dyskinesias in autistic children: A prospective, longitudinal study. J Am Acad Child Adolesc Psychiatry 1997;6:835. Campbell M, Fish B, Korein J, et al. Lithium and chlorpromazine: A controlled crossover study of hyperactive severely disturbed young children. J Autism Child Schizophr 1972;3:234. Campbell M, Green WH, Deutsch SI. Child and adolescent psychopharmacology. Beverly Hills: Sage, 1985. Campbell M, Small AM, Green WH, et al. Behavioral efficacy of haloperidol and lithium carbonate. A comparison in hospitalized aggressive children with conduct disorder. Arch Gen Psychiatry 1984;7:650. Carlson GA. Child and adolescent mania—diagnostic considerations. J Child Psychol Psychiatry 1990;3:331. Carlson GA, Fennig S, Bromet EJ. The confusion between bipolar disorder and schizophrenia in youth: Where does it stand in the 1990s? J Am Acad Child Adolesc Psychiatry 1994;4:453. Carlson GA, Rapport MD, Pataki CS, et al. Lithium in hospitalized children at 4 and 8 weeks: Mood, behavior and cognitive effects. J Child Psychol Psychiatry 1992;2:411. Carpenter RO, Vining EPG. Antiepileptics (anticonvulsants). New York: Plenum, 1993. Casat CD, Pleasants DZ, Schroeder DH, et al. Bupropion in children with attention deficit disorder. Psychopharmacol Bull 1989;2:198. Casey DE. Dyslipidemia and atypical antipsychotic drugs. J Clin Psychiatry 2004; 65 (Suppl 18):27. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant treatment of ADHD and comorbid Tourette’s syndrome: Effects of stimulant and dose. J Am Acad Child Adolesc Psychiatry 1997;5:589. Catapres. Catapres product information. Ingelheim, Germany: Boehringer-Ingelheim, 2004.
Lee and Walkup / Neuropsychopharmacology Celexa. Celexa product information. St Louis: Forest Pharmaceuticals, 2004. Chang KD, Ketter TA. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;1:45. Chappell PB, Riddle MA, Scahill L, et al. Guanfacine treatment of comorbid attention-deficit hyperactivity disorder and Tourette’s syndrome: Preliminary clinical experience. J Am Acad Child Adolesc Psychiatry 1995;9:1140. Chengappa KN, Rathore D, Levine J, et al. Topiramate as add-on treatment for patients with bipolar mania. Bipolar Disord 1999;1:42. Claghorn JL, Lesem MD. A double-blind placebo-controlled study of Org 3770 in depressed outpatients. J Affect Disord 1995;3:165. Clay TH, Gualtieri CT, Evans RW, et al. Clinical and neuropsychological effects of the novel antidepressant bupropion. Psychopharmacol Bull 1988;1:143. Coffey B. Review and update: Benzodiazepines in childhood and adolescence. Psychiatr Ann 1993;3:332. Cohen DJ, Detlor J, Young JG, et al. Clonidine ameliorates Gilles de la Tourette syndrome. Arch Gen Psychiatry 1980;12:1350. Comings D. Tourette syndrome and human behavior. Duarte: Hope Press, 1990. Conners CK, Casat CD, Gualtieri CT, et al. Bupropion hydrochloride in attention deficit disorder with hyperactivity. J Am Acad Child Adolesc Psychiatry 1996;10:1314. Connor DF, Fletcher KE, Swanson JM. A meta-analysis of clonidine for symptoms of attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1999;12:1551. Connor DF, Fletcher KE, Wood JS. Neuroleptic-related dyskinesias in children and adolescents. J Clin Psychiatry 2001;12:967. Costello EJ. Child psychiatric disorders and their correlates: A primary care pediatric sample. J Am Acad Child Adolesc Psychiatry 1989;6:851. Cylert. Cylert product information. North Chicago, IL: Abbott Laboratories, 2004. Davanzo PA, McCracken JT. Mood stabilizers in the treatment of juvenile bipolar disorder. Advances and controversies. Child Adolesc Psychiatr Clin N Am 2000;1:159. Davis LL, Ryan W, Adinoff B, et al. Comprehensive review of the psychiatric uses of valproate. J Clin Psychopharmacol 2000;1 (Suppl 1):1S. Daviss WB, Bentivoglio P, Racusin R, et al. Bupropion sustained release in adolescents with comorbid attention-deficit/hyperactivity disorder and depression. J Am Acad Child Adolesc Psychiatry 2001;3:307. DelBello MP, Kowatch RA, Warner J, et al. Adjunctive topiramate treatment for pediatric bipolar disorder: A retrospective chart review. J Child Adolesc Psychopharmacol 2002a;4:323. DelBello MP, Schwiers ML, Rosenberg HL, et al. A double-blind, randomized, placebo-controlled study of quetiapine as adjunctive treatment for adolescent mania. J Am Acad Child Adolesc Psychiatry 2002b;10:1216. DeLong GR, Aldershof AL. Long-term experience with lithium treatment in childhood: Correlation with clinical diagnosis. J Am Acad Child Adolesc Psychiatry 1987;3:389. Depakote. Depakote product information. N. Chicago: Abbott Laboratories, 2003. DeVeaugh-Geiss J, Moroz G, Biederman J, et al. Clomipramine hydrochloride in childhood and adolescent obsessive-compulsive disorder—a multicenter trial. J Am Acad Child Adolesc Psychiatry 1992;1:45. Dexedrine. Dexedrine product information. N. Chicago: Abbott Laboratories, 2002. Dilsaver SC, Swann SC, Chen YW, et al. Treatment of bipolar depression with carbamazepine: Results of an open study. Biol Psychiatry 1996;9:935. Di Martino A, Melis G, Cianchetti C, et al. Methylphenidate for pervasive developmental disorders: Safety and efficacy of acute single dose test and ongoing therapy: An open-pilot study. J Child Adolesc Psychopharmacol. 2004;14:207. Dimitriou EC, Dimitriou CE. Buspirone augmentation of antidepressant therapy. J Clin Psychopharmacol 1998;6:465. Dion Y, Annable L, Sandor P, et al. Risperidone in the treatment of Tourette syndrome: A double-blind, placebo-controlled trial. J Clin Psychopharmacol 2002;1:31. Ditto KE. SSRI discontinuation syndrome. Awareness as an approach to prevention. Postgrad Med 2003;2:79. Donovan SJ, Stewart JW, Nunes EV, et al. Divalproex treatment for youth with explosive temper and mood lability: A double-blind, placebo-controlled crossover design. Am J Psychiatry 2000;5:818.
973
Duncan M. Using psychostimulants to treat behavioral disorders of children and adolescents. J Child Adolesc Psychopharmacol 1990;1:7–20. DuPont RL, Saylor KE. Depressant substances in adolescent medicine. Pediatr Rev 1992;10:381. Effexor. Effexor product information. Philadelphia: Wyeth Laboratories, 2003. Elgudin L, Hall Y, Schubert D. Ammonia induced encephalopathy from valproic acid in a bipolar patient: Case report. Int J Psychiatry Med 2003;1:91. Elliot GR, Popper CW. Tricyclic antidepressants: The QT interval and other cardiovascular parameters [Editorial]. J Child Adolesc Psychopharmacol 1990/1991;1:187. Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: A placebocontrolled, randomized clinical trial. J Am Acad Child Adolesc Psychiatry 2002;10:1205. Emslie GJ, Rush AJ, Weinberg WA, et al. A double-blind, randomized, placebo-controlled trial of fluoxetine in children and adolescents with depression. Arch Gen Psychiatry 1997;11:1031. Eskalith-CR. Eskalith-CR product information. Research Triangle Park, NC: GlaxoSmithKline, 2002. Evins AE. Efficacy of newer anticonvulsant medications in bipolar spectrum mood disorders. J Clin Psychiatry 2003;64 (Suppl 8):9. Faraone SV, Wilens T. Does stimulant treatment lead to substance use disorders? J Clin Psychiatry 2003;64 (Suppl 11):9. FDAMA. Food and Drug Administration Modernization Act of 1997. Public Law 105–115, 105th Congress, Sec. III. Pediatric studies of drugs. Feeney DJ, Klykylo W. Risperidone and tardive dyskinesia. J Am Acad Child Adolesc Psychiatry 1996;11:1421. Feighner JP, Cohn JB. Analysis of individual symptoms in generalized anxiety—a pooled, multistudy, double-blind evaluation of buspirone. Neuropsychobiology 1989;3:124. Feldman H, Crumrine P, Handen BL, et al. Methylphenidate in children with seizures and attention-deficit disorder. Am J Dis Child 1989;143:1081. Fenichel RR. Combining methylphenidate and clonidine: The role of post-marketing surveillance. J Child Adolesc Psychopharmacol 1995;155:117. Findling RL, McNamara NK, Gracious BL. Paediatric uses of atypical antipsychotics. Expert Opin Pharmacother 2000;5:935. Findling RL, McNamara NK, Gracious BL, et al. Combination lithium and divalproex sodium in pediatric bipolarity. J Am Acad Child Adolesc Psychiatry 2003;8:895. Findling RL, Reed MD, Myers C, et al. Paroxetine pharmacokinetics in depressed children and adolescents. J Am Acad Child Adolesc Psychiatry 1999;8:952. Findling RL, Schwartz MA, Flannery DJ, et al. Venlafaxine in adults with attention-deficit/hyperactivity disorder: An open clinical trial. J Clin Psychiatry 1996;5:184. Fisman S, Steele M. Use of risperidone in pervasive developmental disorders: A case series. J Child Adolesc Psychopharmacol 1996;3:177. Fitzpatrick PA, Klorman R, Brumaghim JT, et al. Effects of sustainedrelease and standard preparations of methylphenidate on attention deficit disorder. J Am Acad Child Adolesc Psychiatry 1992;2:226. Frazier JA, Biederman J, Tohen M, et al. A prospective open-label treatment trial of olanzapine monotherapy in children and adolescents with bipolar disorder. J Child Adolesc Psychopharmacol 2001;3:239. Frazier JA, Meyer MC, Biederman J, et al. Risperidone treatment for juvenile bipolar disorder: A retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;8:960. Fritz GK, Rockney RM, Yeung AS. Plasma levels and efficacy of imipramine treatment for enuresis. J Am Acad Child Adolesc Psychiatry 1994;1:60. Frye MA, Ketter TA, Kimbrell TA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;6:607. Gabapentin. Gabapentin product information. Vega Baja, PR: Parke Davis Pharmaceuticals, 2002. Gadow KD, Nolan EE, Sverd J. Methylphenidate in hyperactive boys with comorbid tic disorder. II. Short-term behavioral effects in school settings. J Am Acad Child Adolesc Psychiatry 1992;3:462. Gadow KD, Sverd J, Sprafkin J, et al. Efficacy of methylphenidate for attention-deficit hyperactivity disorder in children with tic disorder. Arch Gen Psychiatry 1995;6:444.
974
Neurobehavioral Disorders / 39
Gadow KD, Sverd J, Sprafkin J, et al. Long-term methylphenidate therapy in children with comorbid attention-deficit hyperactivity disorder and chronic multiple tic disorder. Arch Gen Psychiatry 1999;4:330. Gaffney GR, Perry PJ, Lund BC, et al. Risperidone versus clonidine in the treatment of children and adolescents with Tourette’s syndrome. J Am Acad Child Adolesc Psychiatry 2002;3:330. Garland EJ, Smith DH. Panic disorder on a child psychiatric consultation service. J Am Acad Child Adolesc Psychiatry 1990;5:785. Gastfriend DR, Biederman J, Jellinek MS. Desipramine in the treatment of adolescents with attention deficit disorder. Am J Psychiatry 1984;7:906. Gelenberg AJ, Schoonover SC. Bipolar disorder. New York: Plenum, 1991. Geller B, Carr LG. Similarities and differences between adult and pediatric major depressive disorders. New York: Elsevier, 1988. Geller B, Cooper TB, Chestnut EC, et al. Preliminary data on the relationship between nortriptyline plasma level and response in depressed children. Am J Psychiatry 1986;10:1283. Geller B, Cooper TB, Graham DL, et al. Pharmacokinetically designed double-blind placebo-controlled study of nortriptyline in 6- to 12-year-olds with major depressive disorder. J Am Acad Child Adolesc Psychiatry 1992;1:34. Geller B, Cooper TB, McCombs HG, et al. Double-blind, placebocontrolled study of nortriptyline in depressed children using a “fixed plasma level” design. Psychopharmacol Bull 1989a;1:101. Geller B, Cooper TB, Schluchter MD, et al. Child and adolescent nortriptyline single dose pharmacokinetic parameters: Final report. J Clin Psychopharmacol 1987;5:321. Geller B, Cooper TB, Graham DL, et al. Double-blind placebo-controlled study of nortriptyline in depressed adolescents using a “fixed plasma level” design. Psychopharmacol Bull 1990;1:85. Geller B, Fetner HH. Children’s 24-hour serum lithium level after a single dose predicts initial dose and steady-state plasma level. J Clin Psychopharmacol 1989b;2:155. Geller DA, Hoog SL, Heiligenstein JH, et al. Fluoxetine treatment for obsessive-compulsive disorder in children and adolescents: A placebo-controlled clinical trial. J Am Acad Child Adolesc Psychiatry 2001;7:773. Geodon. Geodon product information. New York: Pfizer, 2004. Gepertz S, Neveus T. Imipramine for therapy resistant enuresis: A retrospective evaluation. J Urol 2004;6 (Pt 2):2607. Ghaemi SN, Manwani SG, Katzow JJ, et al. Topiramate treatment of bipolar spectrum disorders: A retrospective chart review. Ann Clin Psychiatry 2001;4:185. Gilbert DL, Batterson JR, Sethuraman G, et al. Tic reduction with risperidone versus pimozide in a randomized, double-blind, crossover trial. J Am Acad Child Adolesc Psychiatry 2004;2:206. Gittelman-Klein RKD. Controlled imipramine treatment of school phobia. Arch Gen Psychiatry 1971;25:204. Gittelman R, Mannuzza S, Shenker R, et al. Hyperactive boys almost grown up. I. Psychiatric status. Arch Gen Psychiatry 1985;10:937. Glod CA, Lynch A, Flynn E, et al. Open trial of bupropion SR in adolescent major depression. J Child Adolesc Psychiatr Nurs 2003;3:123. Gomez Diaz RA, Rivera Moscoso R, Ramos Rodriguez R, et al. Diabetic ketoacidosis in adults: Clinical and laboratory features. Arch Med Res 1996;2:177. Good CR, Feaster CS, Krecko VF. Tolerability of oral loading of divalproex sodium in child psychiatry inpatients. J Child Adolesc Psychopharmacol 2001;1:53. Goodwin FK, Jamison KR. Manic depressive illness. New York: Oxford, 1990. Graae F, Milner J, Rizzotto L, et al. Clonazepam in childhood anxiety disorders. J Am Acad Child Adolesc Psychiatry 1994;3:372. Grcevich SJ, Findling RL, Rowane WA, et al. Risperidone in the treatment of children and adolescents with schizophrenia: A retrospective study. J Child Adolesc Psychopharmacol 1996;4:251. Green W. Child and adolescent clinical psychopharmacology, 2nd ed. Baltimore: Williams & Wilkins, 1995. Green WH, Padron-Gayol M, Hardesty AS, et al. Schizophrenia with childhood onset: A phenomenological study of 38 cases. J Am Acad Child Adolesc Psychiatry 1992;5:968. Haldol. Haldol product information. Raritan, NJ: Ortho-McNeil Pharmaceutical, 2001. Haloperidol. Haloperidol product information. Raritan, NJ: Ortho-McNeil Pharmaceutical, 2001.
Hammad T. Review and evaluation of clinical data: Relationship between psychotropic drugs and pediatric suicidality. http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004-4065b110-TAB08-Hammads-Review.pdf, 2004. Haupt DW, Newcomer JW. Hyperglycemia and antipsychotic medications. J Clin Psychiatry 2001;62 (Suppl 27):15. Hechtman L. Adolescent outcome of hyperactive children treated with stimulants in childhood: A review. Psychopharmacol Bull 1985;2:178. Heimann SW. High-dose olanzapine in an adolescent. J Am Acad Child Adolesc Psychiatry 1999;5:496. Hellings JA, Zarcone JR, Crandall K, et al. Weight gain in a controlled study of risperidone in children, adolescents and adults with mental retardation and autism. J Child Adolesc Psychopharmacol 2001;3:229. Henry CA, Zamvil LS, Lam C, et al. Long-term outcome with divalproex in children and adolescents with bipolar disorder. J Child Adolesc Psychopharmacol 2003;4:523. Hoehn-Saric R, Harris GJ, Pearlson GD, et al. A fluoxetine-induced frontal lobe syndrome in an obsessive compulsive patient. J Clin Psychiatry 1991;3:131. Hoehn-Saric R, Lipsey JR, McLeod DR. Apathy and indifference in patients on fluvoxamine and fluoxetine. J Clin Psychopharmacol 1990;5:343. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry 2001;7:530. Hornig-Rohan M, Amsterdam JD. Venlafaxine versus stimulant therapy in patients with dual diagnosis ADD and depression. Prog Neuropsychopharmacol Biol Psychiatry 2002;3:585. Horrigan JP, Barnhill LJ. Guanfacine and treatment-resistant attentiondeficit hyperactivity disorder in boys. J Child Adolesc Psychopharmacol 1995;5:215. Hsu LK. Lithium-resistant adolescent mania. J Am Acad Child Psychiatry 1986;2:280. Hunt RD. Treatment effects of oral and transdermal clonidine in relation to methylphenidate: An open pilot study in ADD-H. Psychopharmacol Bull 1987;1:111. Hunt RD, Arnsten AF, Asbell MD. An open trial of guanfacine in the treatment of attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1995;1:50. Hunt RD, Capper S, O’Connell P. Clonidine in child and adolescent psychiatry. J Child Adolesc Psychopharmacol 1990;1:87. Hunt RD, Cohen DJ, Shaywitz SE, et al. Strategies for study of the neurochemistry of attention deficit disorder in children. Schizophr Bull 1982;2:236. Hunt RD, Lau S, Ryu J. Alternative therapies for ADHD. New York: Mary Ann Liebert, 1991. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, et al. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;19:1383. Jenike MA, Baer L, Buttolph L. Buspirone augmentation of fluoxetine in patients with obsessive compulsive disorder. J Clin Psychiatry 1991;1:13. Jensen PS, Bhatara VS, Vitiello B, et al. Psychoactive medication prescribing practices for U.S. children: Gaps between research and clinical practice. J Am Acad Child Adolesc Psychiatry 1999;5:557. Jensen PS, Hinshaw SP, Swanson JM, et al. Findings from the NIMH Multimodal Treatment Study of ADHD (MTA): Implications and applications for primary care providers. J Dev Behav Pediatr 2001;1:60. Joshi PT, Capozzoli JA, Coyle JT. Low-dose neuroleptic therapy for children with childhood-onset pervasive developmental disorder. Am J Psychiatry 1988;3:335. Kafantaris V. Treatment of bipolar disorder in children and adolescents. J Am Acad Child Adolesc Psychiatry 1995;6:732. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;9:763. Kashani JH, Orvaschel H. Anxiety disorders in mid-adolescence: A community sample. Am J Psychiatry 1988;8:960. Kashani JH, Orvaschel H. A community study of anxiety in children and adolescents. Am J Psychiatry 1990;3:313. Kashani JH, Shekim WO, Reid JC. Amitriptyline in children with major depressive disorder: A double-blind crossover pilot study. J Am Acad Child Psychiatry 1984;3:348. Katusic SK, Barbaresi WJ, Colligan RC. Substance abuse among ADHD cases: A population-based birth cohort study. Paper presented at the Pediatric Academic Society annual meeting, 2003.
Lee and Walkup / Neuropsychopharmacology Keck PE Jr, McElroy SL. Aripiprazole: A partial dopamine D2 receptor agonist antipsychotic. Expert Opin Invest Drugs 2003;4:655. Keller MB, Lavori PW, Wunder J, et al. Chronic course of anxiety disorders in children and adolescents. J Am Acad Child Adolesc Psychiatry 1992;4:595. Kelsey DK, Sumner CR, Casat CD, et al. Once-daily atomoxetine treatment for children with attention-deficit/hyperactivity disorder, including an assessment of evening and morning behavior: A double-blind, placebo-controlled trial. Pediatrics 2004;1:e1. Kemph JP, DeVane CL, Levin GM, et al. Treatment of aggressive children with clonidine: Results of an open pilot study. J Am Acad Child Adolesc Psychiatry 1993;3:577. Kent JD, Blader JC, Koplewicz HS, et al. Effects of late-afternoon methylphenidate administration on behavior and sleep in attention-deficit hyperactivity disorder. Pediatrics 1995;2 (Pt 1):320. Khan M, Farver D. Recognition, assessment and management of neuroleptic malignant syndrome. S D J Med 2000;9:395. Klein RG, Koplewicz HS, Kanner A. Imipramine treatment of children with separation anxiety disorder. J Am Acad Child Adolesc Psychiatry 1992;1:21. Klein RG, Mannuzza S. Hyperactive boys almost grown up. III. Methylphenidate effects on ultimate height. Arch Gen Psychiatry 1988;12:1131. Klonopin. Klonopin product information. Nutley, NJ: Roche, 2004. Kofoed L, Tadepalli G, Oesterheld JR, et al. Case series: Clonidine has no systematic effects on PR or QTc intervals in children. J Am Acad Child Adolesc Psychiatry 1999;9:1193. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium, and carbamazepine in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2000;6:713. Kramer AD, Feiguine RJ. Clinical effects of amitriptyline in adolescent depression. A pilot study. J Am Acad Child Psychiatry 1981;3:636. Kratochvil CJ, Heiligenstein JH, Dittmann R, et al. Atomoxetine and methylphenidate treatment in children with ADHD: A prospective, randomized, open-label trial. J Am Acad Child Adolesc Psychiatry 2002;7:776. Kumra S, Herion D, Jacobsen LK, et al. Case study: Risperidone-induced hepatotoxicity in pediatric patients. J Am Acad Child Adolesc Psychiatry 1997;5:701. Kumra S, Jacobsen LK, Lenane M, et al. Childhood-onset schizophrenia: An open-label study of olanzapine in adolescents. J Am Acad Child Adolesc Psychiatry 1998;4:377. Kusumakar V, Yatham LN. An open study of lamotrigine in refractory bipolar depression. Psychiatry Res 1997;2:145. Kutcher SP, MacKenzie S. Successful clonazepam treatment of adolescents with panic disorder. J Clin Psychopharmacol 1988;4:299. Kutcher SP, Reiter S, Gardner DM, et al. The pharmacotherapy of anxiety disorders in children and adolescents. Psychiatr Clin North Am 1992;1:41. Labellarte M, Biederman J, Emslie G, et al. Multiple-dose pharmacokinetics of fluvoxamine in children and adolescents. J Am Acad Child Adolesc Psychiatry 2004;12:1497. Lake MB, Birmaher B, Wassick S, et al. Bleeding and selective serotonin reuptake inhibitors in childhood and adolescence. J Child Adolesc Psychopharmacol 2000;1:35. Lam RW, Hossie H, Solomons K, et al. Citalopram and bupropion-SR: Combining versus switching in patients with treatment-resistant depression. J Clin Psychiatry 2004;3:337. Lamictal. Lamictal product information. Research Triangle Park, NC: GlaxoSmithKline, 2003. Last CG, Hersen M, Kazdin AE, et al. Comparison of DSM-III separation anxiety and overanxious disorders: Demographic characteristics and patterns of comorbidity. J Am Acad Child Adolesc Psychiatry 1987;4:527. Latz SR, McCracken JT. Neuroleptic malignant syndrome in children and adolescents: Two case reports and a warning. J Child Adolesc Psychopharmacol 1992;2:123. Law SF, Schachar RJ. Do typical clinical doses of methylphenidate cause tics in children treated for attention-deficit hyperactivity disorder? J Am Acad Child Adolesc Psychiatry 1999;8:944. Lebovitz HE. Diabetic ketoacidosis. Lancet 1995;345:767. Leckman JF, Cohen DJ, Detlor J, et al. Clonidine in the treatment of Tourette syndrome: A review of data. New York: Raven Press, 1982. Leckman JF, Hardin MT, Riddle MA, et al. Clonidine treatment of Gilles de la Tourette’s syndrome. Arch Gen Psychiatry 1991;4:324. Leonard HL, Swedo SE, Lenane MC, et al. A double-blind desipramine substitution during long-term clomipramine treatment in children and
975
adolescents with obsessive-compulsive disorder. Arch Gen Psychiatry 1991;10:922. Leonard HL, Swedo SE, Rapoport JL, et al. Treatment of obsessive-compulsive disorder with clomipramine and desipramine in children and adolescents. A double-blind crossover comparison. Arch Gen Psychiatry 1989;12:1088. Lerer B, Moore N, Meyendorff E, et al. Carbamazepine versus lithium in mania: A double-blind study. J Clin Psychiatry 1987;3:89. Leucht S, Pitschel-Walz G, Abraham D, et al. Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res 1999;1:51. Lewis R. Typical and atypical antipsychotics in adolescent schizophrenia: Efficacy, tolerability, and differential sensitivity to extrapyramidal symptoms. Can J Psychiatry 1998;6:596. Lexapro. Lexapro product information. St Louis: Forest Laboratories, 2004. Lindenmayer JP, Czobor P, Volavka J, et al. Changes in glucose and cholesterol levels in patients with schizophrenia treated with typical or atypical antipsychotics. Am J Psychiatry 2003;2:290. L’Italien G. Pharmacoeconomic impact of antipsychotic-induced metabolic events. Preventative Medicine in Managed Care 2003:S38. Lombroso PJ, Scahill L, King RA, et al. Risperidone treatment of children and adolescents with chronic tic disorders: A preliminary report. J Am Acad Child Adolesc Psychiatry 1995;9:1147. Malone ML, Gennis V, Goodwin JS. Characteristics of diabetic ketoacidosis in older versus younger adults. J Am Geriatr Soc 1992;11:1100. Malone RP, Cater J, Sheikh RM, et al. Olanzapine versus haloperidol in children with autistic disorder: An open pilot study. J Am Acad Child Adolesc Psychiatry 2001;8:887. Malone RP, Delaney MA, Luebbert JF, et al. A double-blind placebo-controlled study of lithium in hospitalized aggressive children and adolescents with conduct disorder. Arch Gen Psychiatry 2000;7:649. Mandoki MW. Risperidone treatment of children and adolescents: Increased risk of extrapyramidal side-effects. J Child Adolesc Psychopharmacol 1995;5:49. Mandoki MW, Tapia MR, Tapia MA, et al. Venlafaxine in the treatment of children and adolescents with major depression. Psychopharmacol Bull 1997;1:149. March JS, Biederman J, Wolkow R, et al. Sertraline in children and adolescents with obsessive-compulsive disorder: A multicenter randomized controlled trial. JAMA 1998;20:1752. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: Safety and tolerability in short-term, placebo-controlled trials. Schizophr Res 2003;61:123. Martin A, Koenig K, Scahill L, et al. Open-label quetiapine in the treatment of children and adolescents with autistic disorder. J Child Adolesc Psychopharmacol 1999;2:99. Martin A, Landau J, Leebens P, et al. Risperidone-associated weight gain in children and adolescents: A retrospective chart review. J Child Adolesc Psychopharmacol 2000;4:259. Masand PS, Ashton AK, Gupta S, et al. Sustained-release bupropion for selective serotonin reuptake inhibitor-induced sexual dysfunction: A randomized, double-blind, placebo-controlled, parallel-group study. Am J Psychiatry 2001;5:805. Masi G, Cosenza A, Mucci M, et al. Risperidone monotherapy in preschool children with pervasive developmental disorders. J Child Neurol 2001;6:395. McConville B, Carrero L, Sweitzer D, et al. Long-term safety, tolerability, and clinical efficacy of quetiapine in adolescents: An open-label extension trial. J Child Adolesc Psychopharmacol 2003;1:75. McConville BJ, Arvanitis LA, Thyrum PT, et al. Pharmacokinetics, tolerability, and clinical effectiveness of quetiapine fumarate: An open-label trial in adolescents with psychotic disorders. J Clin Psychiatry 2000;4:252. McCracken JT, McGough J, Shah B, et al. Risperidone in children with autism and serious behavioral problems. N Engl J Med 2002;5:314. McDougle CJ, Holmes JP, Bronson MR, et al. Risperidone treatment of children and adolescents with pervasive developmental disorders: A prospective open-label study. J Am Acad Child Adolesc Psychiatry 1997;5:685. McDougle CJ, Kem DL, Posey DJ. Case series: Use of ziprasidone for maladaptive symptoms in youths with autism. J Am Acad Child Adolesc Psychiatry 2002;8:921.
976
Neurobehavioral Disorders / 39
McElroy SL, Keck PE Jr, Pope HG Jr, et al. Valproate in the treatment of bipolar disorder: Literature review and clinical guidelines. J Clin Psychopharmacol 1992;1 (Suppl):42S. McElroy SL, Suppes T, Keck PE, et al. Open-label adjunctive topiramate in the treatment of bipolar disorders. Biol Psychiatry 2000;12:1025. McElroy SL, Zarate CA, Cookson J, et al. A 52-week, open-label continuation study of lamotrigine in the treatment of bipolar depression. J Clin Psychiatry 2004;2:204. McGavin JK, Goa KL. Aripiprazole. CNS Drugs 2002;11:779. Michelson D, Adler L, Spencer T, et al. Atomoxetine in adults with ADHD: Two randomized, placebo-controlled studies. Biol Psychiatry 2003;2:112. Michelson D, Buitelaar JK, Danckaerts M, et al. Relapse prevention in pediatric patients with ADHD treated with atomoxetine: A randomized, double-blind, placebo-controlled study. J Am Acad Child Adolesc Psychiatry 2004;7:896. Mozes T, Greenberg Y, Spivak B, et al. Olanzapine treatment in chronic drug-resistant childhood-onset schizophrenia: An open-label study. J Child Adolesc Psychopharmacol 2003;3:311. MTA. National Institute of Mental Health Multimodal Treatment Study of ADHD follow-up: Changes in effectiveness and growth after the end of treatment. Pediatrics 2004;4:762. Mukaddes NM, Abali O. Quetiapine treatment of children and adolescents with Tourette’s disorder. J Child Adolesc Psychopharmacol 2003;3:295. Nasrallah H. A review of the effect of atypical antipsychotics on weight. Psychoneuroendocrinology 2003;8 (Suppl 2):83. Newcomer JW, Haupt DW, Fucetola R, et al. Abnormalities in glucose regulation during antipsychotic treatment of schizophrenia. Arch Gen Psychiatry 2002;4:337. Nilsson M, Joliat MJ, Miner CM, et al. Safety of subchronic treatment with fluoxetine for major depressive disorder in children and adolescents. J Child Adolesc Psychopharmacol 2004;3:412. Olfson M, Marcus SC, Weissman MM, et al. National trends in the use of psychotropic medications by children. J Am Acad Child Adolesc Psychiatry 2002;5:514. Olvera RL, Pliszka SR, Luh J, et al. An open trial of venlafaxine in the treatment of attention-deficit/hyperactivity disorder in children and adolescents. J Child Adolesc Psychopharmacol 1996;4:241. Orap. Orap product information. Sellersville, PA: Gate Pharmaceuticals, 2004. Pande AC, Crockatt JG, Janney CA, et al. Gabapentin in bipolar disorder: A placebo-controlled trial of adjunctive therapy. Gabapentin Bipolar Disorder Study Group. Bipolar Disord 2000;3 (Pt 2):249. Parraga HC, Parraga MI, Woodward RL, et al. Quetiapine treatment of children with Tourette’s syndrome: Report of two cases. J Child Adolesc Psychopharmacol 2001;2:187. Pelham WE, Greenslade KE, Vodde-Hamilton M, et al. Relative efficacy of long-acting stimulants on children with attention deficithyperactivity disorder: A comparison of standard methylphenidate, sustained-release methylphenidate, sustained-release dextroamphetamine, and pemoline. Pediatrics 1990;2:226. Pelham WE, Sturges J, Hoza J, et al. Sustained release and standard methylphenidate effects on cognitive and social behavior in children with attention deficit disorder. Pediatrics 1987;4:491. Physicians’ Desk Reference, 58th ed. Montvale, NJ: Medical Economics Co, Inc, 2004. Potenza MN, Holmes JP, Kanes SJ, et al. Olanzapine treatment of children, adolescents, and adults with pervasive developmental disorders: An open-label pilot study. J Clin Psychopharmacol 1999;1:37. Poussaint AF, Ditman KS. A controlled study of imipramine (Tofranil) in the treatment of childhood enuresis. J Pediatr 1965;67:283. Preskorn SH, Bupp SJ, Weller EB, et al. Plasma levels of imipramine and metabolites in 68 hospitalized children. J Am Acad Child Adolesc Psychiatry 1989;3:373. Prince JB, Wilens TE, Biederman J, et al. Clonidine for sleep disturbances associated with attention-deficit hyperactivity disorder: A systematic chart review of 62 cases. J Am Acad Child Adolesc Psychiatry 1996;5:599. Puig-Antich J, Perel JM, Lupatkin W, et al. Imipramine in prepubertal major depressive disorders. Arch Gen Psychiatry 1987;1:81. Quinn PO, Rapoport JL. One-year follow-up of hyperactive boys treated with imipramine or methylphenidate. Am J Psychiatry 1975;3:241. Quintana H, Keshavan M. Case study: Risperidone in children and adolescents with schizophrenia. J Am Acad Child Adolesc Psychiatry 1995;10:1292.
Rapoport JL, Buchsbaum MS, Zahn TP, et al. Dextroamphetamine: Cognitive and behavioral effects in normal prepubertal boys. Science 1978;199:560. Rapoport JL, Mikkelsen EJ, Zavadil A, et al. Childhood enuresis. II. Psychopathology, tricyclic concentration in plasma, and antienuretic effect. Arch Gen Psychiatry 1980;10:1146. Rapoport JL, Quinn PO, Bradbard G, et al. Imipramine and methylphenidate treatments of hyperactive boys. A double-blind comparison. Arch Gen Psychiatry 1974;6:789. Reiter S, Kutcher SP. Disinhibition and anger outbursts in adolescents treated with clonazepam. J Clin Psychopharmacol 1991;4:268. Remeron. Remeron product information. West Orange, NJ: Organon, 2002. Richardson MA, Haugland G, Craig TJ. Neuroleptic use, parkinsonian symptoms, tardive dyskinesia, and associated factors in child and adolescent psychiatric patients. Am J Psychiatry 1991;10:1322. Riddle MA, Geller B, Ryan N. Another sudden death in a child treated with desipramine. J Am Acad Child Adolesc Psychiatry 1993;4:792. Riddle MA, Reeve EA, Yaryura-Tobias JA, et al. Fluvoxamine for children and adolescents with obsessive-compulsive disorder: A randomized, controlled, multicenter trial. J Am Acad Child Adolesc Psychiatry 2001;2:222. Risperdal. Risperdal product information. Titusville, NJ: Janssen Pharmaceuticals, 2004. Ritalin. Ritalin hydrochloride (methylphenidate hydrochloride) tablets: Product information. East Hanover, NJ: Novartis, 2004. Rosa FW. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;10:674. Rosebush P, Stewart T. A prospective analysis of 24 episodes of neuroleptic malignant syndrome. Am J Psychiatry 1989;6:717. Rosenberg DR, Holttum J, Gershon S. Textbook of pharmacotherapy for child and adolescent psychiatric disorders. New York: Brunner/Mazel, 1994. Rubin M. Use of typical antipsychotics in children with mental retardation, autism, and other developmental disabilities. Psychiatr Ann 1997;27:219. RUPP. Fluvoxamine for the treatment of anxiety disorders in children and adolescents. The Research Unit on Pediatric Psychopharmacology Anxiety Study Group. N Engl J Med 2001;17:1279. Ryan ND, Puig-Antich J, Cooper T, et al. Imipramine in adolescent major depression: Plasma level and clinical response. Acta Psychiatr Scand 1986;3:275. Rynn MA, Siqueland L, Rickels K. Placebo-controlled trial of sertraline in the treatment of children with generalized anxiety disorder. Am J Psychiatry 2001;12:2008. Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: Behavioral sciences/clinical psychiatry, 9th ed. Philadelphia: Lippincott Williams & Wilkins, 2003. Sallee FR, DeVane CL, Ferrell RE. Fluoxetine-related death in a child with cytochrome P-450 2D6 genetic deficiency. J Child Adolesc Psychopharmacol 2000a;1:27. Sallee FR, Kurlan R, Goetz CG, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: A pilot study. J Am Acad Child Adolesc Psychiatry 2000b;3:292. Sallee FR, Nesbitt L, Jackson C, et al. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry 1997;8:1057. Satcher D. US Public Health Service Report of the Surgeon General’s Conference on Children’s Mental Health: A national action agenda. Washington, DC: Department of Health and Human Services, 2000. Saul RC. Nortriptyline in attention deficit disorder. Clin Neuropharmacol 1985;4:382. Sawant S, Daviss SR. Seizures and prolonged QTc with atomoxetine overdose. Am J Psychiatry 2004;4:757. Scahill L, Chappell PB, Kim YS, et al. A placebo-controlled study of guanfacine in the treatment of children with tic disorders and attention deficit hyperactivity disorder. Am J Psychiatry 2001;7:1067. Scahill L, Leckman JF, Schultz RT, et al. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology 2003;7:1130. Scahill L, Martin A. Pediatric Psychopharmacology II: General principles, specific drug treatments, and clinical practice. Philadelphia: Lippincott Williams & Wilkins, 2002. Schreier HA. Risperidone for young children with mood disorders and aggressive behavior. J Child Adolesc Psychopharmacol 1998;1:49. Seroquel. Seroquel product information. Wilmington, DE: AstraZeneca Pharmaceuticals, 2004.
Lee and Walkup / Neuropsychopharmacology Shapiro AK, Shapiro E. Tic disorders. Baltimore: Williams & Wilkins, 1989. Shapiro AK, Shapiro E. Controlled study of pimozide vs. placebo in Tourette’s syndrome. J Am Acad Child Psychiatry 1984;2:161. Shapiro AK, Shapiro E, Eisenkraft GJ. Treatment of Gilles de la Tourette syndrome with pimozide. Am J Psychiatry 1983;9:1183. Shaw JA, Lewis JE, Pascal S, et al. A study of quetiapine: Efficacy and tolerability in psychotic adolescents. J Child Adolesc Psychopharmacol 2001;4:415. Sheard MH. Lithium in the treatment of aggression. J Nerv Ment Dis 1975;2-1:108. Sheehan DV, Raj AB, Sheehan KH, et al. The relative efficacy of buspirone, imipramine and placebo in panic disorder: A preliminary report. Pharmacol Biochem Behav 1988;4:815. Silva RR, Campbell M, Golden RR, et al. Side effects associated with lithium and placebo administration in aggressive children. Psychopharmacol Bull 1992;3:319. Simeon J. Buspirone effects in adolescent psychiatric disorders. Eur Neuropsychopharmacol 1991;1:421. Simeon JG, Ferguson HB. Alprazolam effects in children with anxiety disorders. Can J Psychiatry 1987;7:570. Simeon JG, Ferguson HB, Knott V, et al. Clinical, cognitive, and neurophysiological effects of alprazolam in children and adolescents with overanxious and avoidant disorders. J Am Acad Child Adolesc Psychiatry 1992;1:29. Simeon JG, Ferguson HB, Van Wyck Fleet J. Bupropion effects in attention deficit and conduct disorders. Can J Psychiatry 1986;6:581. Small JG, Klapper MH, Milstein V, et al. Carbamazepine compared with lithium in the treatment of mania. Arch Gen Psychiatry 1991;10:915. Snyder R, Turgay A, Aman M, et al. Effects of risperidone on conduct and disruptive behavior disorders in children with subaverage IQs. J Am Acad Child Adolesc Psychiatry 2002;9:1026. Spencer EK, Kafantaris V, Padron-Gayol MV, et al. Haloperidol in schizophrenic children: Early findings from a study in progress. Psychopharmacol Bull 1992;2:183. Spencer T, Biederman J, Steingard R, et al. Bupropion exacerbates tics in children with attention-deficit hyperactivity disorder and Tourette’s syndrome. J Am Acad Child Adolesc Psychiatry 1993;1:211. Spencer T, Biederman J, Wilens T. Growth deficits in children with attention deficit hyperactivity disorder. Pediatrics 1998;2 (Pt 3):501. Spencer T, Biederman J, Wilens T, et al. Pharmacotherapy of attentiondeficit hyperactivity disorder across the life cycle. J Am Acad Child Adolesc Psychiatry 1996;4:409. Spencer T, Heiligenstein JH, Biederman J, et al. Results from 2 proof-of-concept, placebo-controlled studies of atomoxetine in children with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2002;12:1140. Stamenkovic M, Schindler SD, Aschauer HN, et al. Effective open-label treatment of Tourette’s disorder with olanzapine. Int Clin Psychopharmacol 2000;1:23. Stein MA, Blondis TA, Schnitzler ER, et al. Methylphenidate dosing: Twice daily versus three times daily. Pediatrics 1996;4 (Pt 1):748. Steingard R, Biederman J, Spencer T, et al. Comparison of clonidine response in the treatment of attention-deficit hyperactivity disorder with and without comorbid tic disorders. J Am Acad Child Adolesc Psychiatry 1993;2:350. Stigler KA, Potenza MN, McDougle CJ. Tolerability profile of atypical antipsychotics in children and adolescents. Paediatr Drugs 2001;12:927. Strattera. Strattera product information. Indianapolis, IN: Eli Lilly, 2003. Strauss CC, Last CG. Social and simple phobias in children. J Anxiety Dis 1993;7:141. Strauss CC, Last CG, Hersen M, et al. Association between anxiety and depression in children and adolescents with anxiety disorders. J Abnorm Child Psychol 1988;1:57. Strober M, Morrell W, Lampert C, et al. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: A naturalistic study. Am J Psychiatry 1990;4:457. Swanson JM, Sandman CA, Deutsch C, et al. Methylphenidate hydrochloride given with or before breakfast: I. Behavioral, cognitive, and electrophysiologic effects. Pediatrics 1983;1:49. TADS. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents with Depression Study (TADS) randomized controlled trial. JAMA 2004;7:807.
977
Tandon R, Halbreich U. The second-generation ‘atypical’ antipsychotics: Similar improved efficacy but different neuroendocrine side effects. Psychoneuroendocrinology 2003; 28 (Suppl 1):1. Tannock R, Ickowicz A, Schachar R. Differential effects of methylphenidate on working memory in ADHD children with and without comorbid anxiety. J Am Acad Child Adolesc Psychiatry 1995;7:886. Tegretol. Tegretol product information. East Hanover, NJ: Novartis, 2002. Tollefson GD, Kuntz AJ. Review of recent clinical studies with olanzapine. Br J Psychiatry Suppl 1999;37:30. Topamax. Topamax product information. Raritan, NJ: Ortho-McNeil Pharmaceutical, 2003. Toren P, Laor N, Weizman A. Use of atypical neuroleptics in child and adolescent psychiatry. J Clin Psychiatry 1998;12:644. TSSG. Tourette Syndrome Study Group treatment of ADHD in children with tics: A randomized controlled trial. Neurology 2002;4:527. van Harten J. Overview of the pharmacokinetics of fluvoxamine. Clin Pharmacokinet 1995;29 (Suppl 1):1. Van Putten T, Marder SR. Behavioral toxicity of antipsychotic drugs. J Clin Psychiatry 1987;48 (Suppl):13. van Vliet IM, den Boer JA, Westenberg HG, et al. Clinical effects of buspirone in social phobia: A double-blind placebo-controlled study. J Clin Psychiatry 1997;4:164. Varanka TM, Weller RA, Weller EB, et al. Lithium treatment of manic episodes with psychotic features in prepubertal children. Am J Psychiatry 1988;12:1557. Vasudev K, Goswami U, Kohli K. Carbamazepine and valproate monotherapy: Feasibility, relative safety and efficacy, and therapeutic drug monitoring in manic disorder. Psychopharmacology (Berl) 2000;1:15. Verrotti A, Trotta D, Morgese G, et al. Valproate-induced hyperammonemic encephalopathy. Rev Metab Brain Dis 2002;17:367. Verrotti A, Greco R, Morgese G, et al. Carnitine deficiency and hyperammonemia in children receiving valproic acid with and without other anticonvulsant drugs. Int J Clin Lab Res 1999;1:36. Viesselman JO, Yaylayan S, Weller EB. Antidysthymic drugs (antidepressants and antimanics). New York: Plenum, 1993. Vieta E, Torrent C, Garcia-Ribas G, et al. Use of topiramate in treatment-resistant bipolar spectrum disorders. J Clin Psychopharmacol 2002;4:431. Wagner KD, Ambrosini P, Rynn M, et al. Efficacy of sertraline in the treatment of children and adolescents with major depressive disorder: Two randomized controlled trials. JAMA 2003;8:1033. Wagner KD, Robb AS, Findling RL, et al. A randomized, placebocontrolled trial of citalopram for the treatment of major depression in children and adolescents. Am J Psychiatry 2004;6:1079. Wagner KD, Weller EB, Carlson GA, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;10:1224. Walkup J, Labellarte M. Complications of SSRI treatment. J Child Adolesc Psychopharmacol 2001;1:1. Weintrob N, Cohen D, Klipper-Aurbach Y, et al. Decreased growth during therapy with selective serotonin reuptake inhibitors. Arch Pediatr Adolesc Med 2002;7:696. Weiss G, Hechtmann LT. Hyperactive Children Grow Up: ADHD in children, adolescents, and adults, 2nd ed. New York: Guilford, 1993. Weiss M, Weiss G. Attention deficit hyperactivity disorder. Philadelphia: Lippincott Williams & Wilkins, 2002. Wellbutrin. Wellbutrin product information. Research Triangle Park, NC: GlaxoSmithKline, 2002. Weller EB, Weller RA, Fristad MA. Lithium dosage guide for prepubertal children: A preliminary report. J Am Acad Child Psychiatry 1986;1:92. Wernicke JF, Faries D, Girod D, et al. Cardiovascular effects of atomoxetine in children, adolescents, and adults. Drug Saf 2003;10:729. Wilens TE, Biederman J, Geist DE, et al. Nortriptyline in the treatment of ADHD: A chart review of 58 cases. J Am Acad Child Adolesc Psychiatry 1993;2:343. Wilens TE, Biederman J, Spencer T. Clonidine for sleep disturbances associated with attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 1994;3:424. Wilens TE, Faraone SV, Biederman J, Gunawardene S. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics 2003;111:179–185.
978
Neurobehavioral Disorders / 39
Wilens TE, Spencer TJ, Swanson JM, et al. Combining methylphenidate and clonidine: A clinically sound medication option. J Am Acad Child Adolesc Psychiatry 1999;5:614. Wirshing DA, Wirshing WC, Kysar L, et al. Novel antipsychotics: Comparison of weight gain liabilities. J Clin Psychiatry 1999;6:358. Woodrum ST, Brown CS. Management of SSRI-induced sexual dysfunction. Ann Pharmacother 1998;32:1209. Woolston JL. Case study: Carbamazepine treatment of juvenile-onset bipolar disorder. J Am Acad Child Adolesc Psychiatry 1999;3:335. Wroblewski BA, Leary JM, Phelan AM, et al. Methylphenidate and seizure frequency in brain injured patients with seizure disorders. J Clin Psychiatry 1992;3:86. Xanax. Xanax product information. Kalamazoo, MI: Pharmacia & Upjohn, 2004. Yatham LN, Kusumakar V, Calabrese JR, et al. Third generation anticonvulsants in bipolar disorder: A review of efficacy and summary of clinical recommendations. J Clin Psychiatry 2002;4:275.
Yehya N, Saldarini CT, Koski ME, et al. Valproate-induced hyperammonemic encephalopathy. J Am Acad Child Adolesc Psychiatry 2004;8:926. Zahn TP, Rapoport JL, Thompson CL. Autonomic and behavioral effects of dextroamphetamine and placebo in normal and hyperactive prepubertal boys. J Abnorm Child Psychol 1980;2:145. Zeiner P. Body growth and cardiovascular function after extended treatment (1.75 years) with methylphenidate in boys with attention-deficit hyperactivity disorder. J Child Adolesc Psychopharmacol 1995;5:129. Zimnitzky B. A fifth case of sudden death in a child taking desipramine. New Research Poster (NR478-A). Washington, DC: American Psychiatric Association, 1994;181. Zito JM, Safer DJ, dosReis S, et al. Psychotropic practice patterns for youth: A 10-year perspective. Arch Pediatr Adolesc Med 2003;1:17. Zuddas A, Di Martino A, Muglia P, et al. Long-term risperidone for pervasive developmental disorder: Efficacy, tolerability, and discontinuation. J Child Adolesc Psychopharmacol 2000;2:79. Zyprexa. Zyprexa product information. Indianapolis, IN: Eli Lilly, 2004.
CHAPTER 40
Pediatric Epilepsy: An Overview Peter R. Camfield and Carol S. Camfield
Epilepsy may be diagnosed after a child has had two or more unprovoked seizures [Camfield et al., 1985a; Shinnar et al., 2000]. The term unprovoked implies that there has been no closely associated concurrent illness, fever, or acute brain injury. Recurrent seizures immediately after a head injury or associated with drug intoxication do not qualify for the diagnosis of epilepsy. Some specific provoking factors leading to reflex seizures are permitted, such as seizures provoked by patterns and flashes from video terminals for children with photosensitive epilepsy. Seizures are still viewed as unprovoked if they occur with stresses related to personal activity, such as sleep deprivation or severe emotional distress, unless these stresses are extreme.
SEIZURE TYPE AND EPILEPSY SYNDROME The definition of epilepsy allows for a tremendous variety of disorders. The seizure types, age of onset, cause, severity, comorbid conditions, response to medication, and clinical course vary widely. There are two main ways of grouping patients to bring an ordered approach to classification, treatment, and prognosis: seizure type and epilepsy syndrome. Both concepts continue to evolve. The International League against Epilepsy defined the seizure types listed in Box 40-1 [Commission on Classification and Terminology of the International League against Epilepsy, 1981]. There is a basic distinction between seizures with a generalized onset that seem to arise everywhere in the cortex at once and seizures with a partial or focal onset that begin in a defined area of cortex. A proposed update in the classification of epileptic seizures suggested that the distinction between simple partial and complex partial seizures is often difficult to assess and not needed [Engel, 2001]. A given seizure type may occur with many different associations. For example, a 2-year-old child with severe mental handicap may have generalized tonic-clonic seizures that are completely resistant to medication, or a normal teenager may have the same seizure type that is completely suppressed by medication. Factors beyond seizure type allow a more comprehensive diagnosis—an epilepsy syndrome diagnosis. Epileptic syndromes may have one or more seizure types, often with a characteristic interictal electroencephalogram. Each syndrome has a defined group of causes, sometimes a clear response to specific treatments, and sometimes a defined clinical course and prognosis. As with seizure types, syndromes have been classified as localizationrelated (focal) or generalized and then subdivided into idiopathic (when a genetic cause is likely), symptomatic (when a diffuse or localized brain abnormality is known), and
cryptogenic (when a diffuse or localized brain abnormality is suspected but unproven) (Table 40-1). In adults, localization-related epilepsy syndromes are most common, are usually symptomatic, and caused by a localized, structural abnormality. Children have similar disorders, but there are many other important syndromes. The idiopathic partial and generalized syndromes all begin in childhood, and genetic influences are significant. The generalized symptomatic syndromes of childhood account for most intractable epilepsy in children [Arzimanogolou et al., 2004; Camfield and Camfield, 2003]. The International League against Epilepsy classified febrile seizures as a special syndrome. Febrile seizures are the most common convulsive event in the human species. Because these seizures are provoked by fever, febrile seizures do not fit well with the usual definition of epilepsy, and few children with febrile seizures later develop unprovoked seizures. The disorder merits special consideration, as reviewed in Chapter 46. The 1989 International League against Epilepsy syndrome classification scheme is still in wide use, and most patients can be “forced” into one of the broad categories, but many children, especially those with symptomatic generalized epilepsy, do not meet the criteria for a more specific syndrome [Commission on Classification and Terminology of the International League Against Epilepsy, 1989]. There are many recently described epilepsy syndromes, but a newer, comprehensive syndrome classification system has been elusive. Advances in genetics have revealed that the same mutation may cause a variety of epilepsy syndromes, including partial and generalized epilepsies, even within the same family (see Chapter 41). The term cryptogenic has been troublesome because it depends on the sophistication of imaging techniques. A new proposal for syndrome classification in 2001 is based on a five-axis system [Engel, 2001]. Axis 1 concerns ictal phenomenology (i.e., what the seizure looks like). Axis 2 is the specific seizure type. Axis 3 is the specific epilepsy syndrome, when it can be defined; axis 4 is the cause; and axis 5 describes the degree of impairment associated with epilepsy. This proposal comes with a more comprehensive list of epilepsy syndromes, although the system is less categorical than the 1989 classification [Commission on Classification and Terminology of the International League against Epilepsy, 1989]. The validity of this proposal remains to be established, but it does serve well to alert the clinician to the many aspects of epilepsy in an individual patient. Table 40-1 summarizes some of the differences in accepted syndromes in the two classification schemes. A physician interested in epilepsy should be conversant with the 1989 and 2001 classification schemes and must anticipate additional revisions.
982
Epilepsy / 40
TABLE 40-1 International Classification of Epilepsies and Epileptic Syndromes and Related Seizure Disorders of 1989 and Epilepsy Syndromes Recognized in the Proposed 2001 International League against Epilepsy Classification Scheme 1989 ILAE CLASSIFICATION* Localization-Related (Local, Focal, Partial) Epilepsies and Syndromes Idiopathic (with age-related onset) Benign childhood epilepsy with centrotemporal spikes Childhood epilepsy with occipital paroxysms
2001 ILAE PROPOSAL†
Primary reading epilepsy
Benign childhood epilepsy with centrotemporal spikes Early-onset benign childhood occipital epilepsy (Panayiotopoulos type) (new) Late-onset childhood occipital epilepsy (Gastaut type) (new) Idiopathic photosensitive occipital lobe epilepsy (new) Primary reading epilepsy Now called reflex epilepsies, which also include: Other visual sensitive epilepsies Primary reading epilepsy Startle epilepsy
Symptomatic or cryptogenic Chronic progressive epilepsia partialis continua Syndromes characterized by seizures with specific modes of precipitation Temporal lobe epilepsies
No longer listed; see Rasmussen’s syndrome Now a reflex epilepsy
Frontal lobe epilepsies Parietal lobe epilepsies Occipital lobe epilepsies Generalized Epilepsies and Syndromes Idiopathic (with age-related onset) Benign familial neonatal seizures Benign neonatal convulsions Benign myoclonic epilepsy in infancy Childhood absence epilepsy Juvenile myoclonic epilepsy Epilepsy with grand mal seizures on awakening Childhood absence epilepsy Other generalized idiopathic epilepsies Juvenile myoclonic epilepsy
Epilepsies with seizures precipitated by specific modes of activation Cryptogenic or symptomatic West’s syndrome Lennox-Gastaut syndrome Epilepsy with myoclonic-astatic seizures Epilepsy with myoclonic seizures Epilepsy with myoclonic absences Early infantile epileptic encephalopathy with suppression burst Early myoclonic encephalopathy Other symptomatic generalized epilepsies
Limbic epilepsies (expanded) Mesial temporal lobe epilepsy with hippocampal sclerosis Mesial temporal lobe epilepsy defined by specific causes Other types defined by location and cause Neocortical epilepsies (new) Rasmussen’s syndrome (new) Hemiconvulsion-hemiplegia syndrome Migrating partial seizures of infancy (new) Other types defined by location and cause (new) Familial temporal lobe epilepsies (new) Familial focal epilepsy with variable foci (new) No longer listed, because location or onset of seizures is insufficient for classification of a syndrome No longer listed, because location or onset of seizures is insufficient for classification of a syndrome No longer listed, because location or onset of seizures is insufficient for classification of a syndrome
Benign familial neonatal seizures Benign neonatal convulsions (diagnosis of epilepsy not required) Benign myoclonic epilepsy in infancy Benign familial infantile seizures Benign infantile seizures (nonfamilial) Childhood absence epilepsy Juvenile absence epilepsy (new) Juvenile myoclonic epilepsy Epilepsy with generalized tonic-clonic seizures only (renamed) Childhood absence epilepsy Other undetermined epilepsies not defined above Juvenile absence epilepsy (new) Juvenile myoclonic epilepsy Landau-Kleffner syndrome (LKS) (new) Epilepsy with continuous spike and waves during slow-wave sleep (other than LKS) (new) Progressive myoclonus epilepsies (new) Now called reflex epilepsies
West’s syndrome Lennox-Gastaut syndrome Epilepsy with myoclonic-astatic seizures No longer listed Epilepsy with myoclonic absences Ohtahara’s syndrome (renamed) Early myoclonic encephalopathy Myoclonic status in progressive encephalopathies (new)
Camfield and Camfield / Pediatric Epilepsy: An Overview
983
TABLE 40-1, cont’d International Classification of Epilepsies and Epileptic Syndromes and Related Seizure Disorders of 1989 and Epilepsy Syndromes Recognized in the Proposed 2001 International League against Epilepsy Classification Scheme 1989 ILAE CLASSIFICATION* Specific Syndromes Epileptic seizures complicating other disease states Epilepsies and syndromes undetermined whether focal or generalized with generalized and focal seizures Neonatal seizures Severe myoclonic epilepsy of infancy Epilepsy with continuous spike waves during slow-wave sleep Acquired epileptic epilepsies (Landau-Kleffner syndrome)
2001 ILAE PROPOSAL†
No longer listed Dravet’s syndrome (renamed) Epilepsy with continuous spike waves during slow-wave sleep (not LKS) Acquired epileptic epilepsies (renamed) (Landau-Kleffner syndrome) Generalized epilepsies with febrile seizures plus (new) Autosomal dominant nocturnal frontal lobe epilepsy
Other undetermined epilepsies without unequivocal generalized or focal features Special Syndromes Situation-related seizures Febrile convulsions Isolated seizures of isolated status epilepticus Seizures occurring only with acute metabolic or toxic events
Febrile seizures (renamed) No longer listed Drug or other chemically induced seizures (expanded) Alcohol-withdrawal seizures Single seizures or isolated clusters of seizures Rarely repeated seizures (oligoepilepsy) Immediate and early post-traumatic seizures
*Modified from the 1989 International League against Epilepsy (ILAE) Proposal. † Modified from the 2001 ILAE Proposal. In this proposal, there are no headings or subheadings, only a listing of epilepsy syndromes by specific syndrome name. This presentation indicates where syndromes are removed or renamed from the 1989 ILAE proposal or are newly recognized in the 2001 proposal. Each syndrome was “forced” into the 1989 proposed schema. Adapted from Engel J. A proposed diagnostic scheme for people with epileptic seizures and epilepsy: Report of the ILAE task force on classification and terminology. Epilepsia 2001;42:796, and from Commission on Classification and Terminology of the International League against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989;30:389.
INCIDENCE The overall incidence of childhood epilepsy from birth to 16 years is approximately 40 cases in 100,000 children per year [Camfield et al., 1996b; Hauser et al., 1993]. The incidence in the first year of life is about 120 in 100,000. Between 1 and 10 years of age, the incidence plateaus at 40 to 50 cases in 100,000 children and then drops further in the teenage years to about 20 in 100,000. The details of
FIGURE 40-1. Incidence of epilepsy by age of onset. (From Camfield CS, Camfield PR, Wirrell E, et al. Incidence of epilepsy in childhood and adolescents: A population based study in Nova Scotia from 1977-1985. Epilepsia 1996b;37:19.)
incidence by year of life from the Nova Scotia childhood epilepsy study are illustrated in Figure 40-1. Hauser estimates that about 1% of all children will have at least one afebrile seizure by age 14 years and that 0.4% to 0.8% will have epilepsy by age 11 years [Hauser and Hesdorffer, 1990]. Epilepsy types vary in incidence. Syndromes dominated by generalized tonic-clonic or partial seizures account for 75% of childhood epilepsy. Syndromes dominated by absence seizures account for approximately 15%, and the secondary generalized epilepsies account for 10%. The latter group includes most of the “catastrophic” epilepsy syndromes, such as West and Lennox-Gastaut syndromes [Camfield et al., 1996b]. Prevalence data for seizure type or epilepsy syndrome are not easily collated because of various definitions of active epilepsy. When active epilepsy was defined as receiving daily antiepileptic drugs or a seizure within the past 5 years, the prevalence of epilepsy in children was 4.3 to 9.3 in 1000 [Hauser and Hesdorffer, 1990]. Because some epileptic syndromes rarely remit, they contribute more to prevalence of epilepsy than its incidence. The relative prevalence of symptomatic generalized epilepsies is higher than their relative incidence. This finding means that physicians who focus on newly diagnosed children will encounter a predominance of benign epilepsy syndromes. Those primarily treating chronic cases will observe a higher proportion of more malignant seizure disorders. A population-based prevalence study from Finland
984
Epilepsy / 40
found that the main seizure types for each patient were focal in 43%, with complex partial and partial with secondary generalization most common. For 44%, generalized seizures were dominant, with generalized tonic-clonic seizures most common. Overall, 45% had localization-related epilepsy syndromes, and 48% had generalized syndromes [Eriksson and Koivikko, 1997].
DIFFERENTIAL DIAGNOSIS The diagnosis of epilepsy is based almost exclusively on a clinical history of two or more unprovoked seizures [Van Donselaar et al., 1989]. Parents vary in their capacity to describe these frightening events, and physicians vary in their ability to ask good questions. Some children are misdiagnosed. A Dutch group of neurologists shared case descriptions of childhood seizure disorders and were able to agree about most diagnoses of epilepsy. However, even experts sometimes disagree. Studies of interobserver reliability have demonstrated important differences in
BOX 40-1 INTERNATIONAL CLASSIFICATION OF SEIZURE TYPE Partial Seizures Simple partial seizures With motor signs With somatosensory or special sensory hallucinations With autonomic symptoms With psychic symptoms Complex partial seizures Simple partial followed by impairment of consciousness With impaired consciousness at onset Partial seizures evolving to secondary generalized seizures Simple partial seizures evolving to generalized Complex partial seizures evolving to generalized Simple partial seizures evolving to complex partial seizures Generalized Seizures Absence seizures Atypical absence seizures Myoclonic seizures Clonic seizures Tonic seizures Tonic-clonic seizures Atonic seizures Unclassifiable Epileptic Seizures Adapted from the Commission on Classification and Terminology of the International League against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981;22:489.
BOX 40-2 DISORDERS THAT MAY MIMIC CHILDHOOD EPILEPSY Confused with Generalized Tonic-Clonic Seizures Pallid syncope (reflex anoxic seizure) Vasodepressor syncope (reflex anoxic seizure) Cyanotic breath-holding attacks Collapsing attacks with cardiac dysrhythmias Cataplexy Confused with Generalized Absence Seizures Behavioral staring attacks Complex partial seizures Tic disorder Confused with Complex Partial Seizures Self-stimulatory behavior, especially in children with autistic spectrum disorders Sleep walking Night terrors Temper tantrums with amnesia for the rage event Benign paroxysmal vertigo Migraine-related disorders [Dooley, 1990] Confused with Epileptic Myoclonus Physiologic hypnagogic myoclonus Benign infantile sleep myoclonus Startle disease
observations when families and neurologists have reviewed the same video seizures, and neurologists often disagree with each other. Neurology residents and faculty often classify seizures differently based on written histories [Camfield and Camfield, 2003]. When the history is not clear-cut, it is better to wait for additional attacks before diagnosing epilepsy. A list of disorders in children that are frequently confused with epilepsy is found in Box 40-2. Reflex anoxic seizures associated with pallid or vasodepressor syncope or with cyanotic breath-holding are particularly likely to be misinterpreted [Stephenson, 1991] (see Chapter 53). The electroencephalogram can be used to make the diagnosis of epilepsy only if a seizure is recorded—a rare event on routine electroencephalographic (EEG) acquisition because most children with epilepsy have infrequent seizures. A small percentage of normal children have epileptiform activity on electroencephalograms but never have a seizure [Petersen and Eeg-Olofsson, 1968], and up to 40% of children with chronic epilepsy never demonstrate epileptiform discharges on interictal electroencephalograms [Camfield et al., 1995]. EEG findings may change significantly over time and reveal conflicting findings [Camfield et al., 1995; Trojaborg, 1968]. An interictal electroencephalogram is often useful for syndrome clarification but must be interpreted in the clinical context. Likewise, the diagnosis of epilepsy cannot be based on brain-imaging studies. The presence of an anomaly on magnetic resonance imaging increases the possibility of epilepsy and, depending on the nature of the abnormality, increases the likelihood of a specific syndrome. For example, lesions typical of tuberous sclerosis in the first year of life increase the risk that a child will have West’s syndrome.
Camfield and Camfield / Pediatric Epilepsy: An Overview
NATURAL HISTORY OF CHILDHOOD EPILEPSY Recurrence after a First Seizure Many children are seen by a physician after a first unprovoked generalized tonic-clonic seizure, a few after a first complex partial seizure, but almost none after a single absence or myoclonic seizure. For children presenting after a single unprovoked seizure, there is an immediate question: Will it happen again? Berg and Shinnar’s meta-analysis of the recurrence risk after a first seizure concluded that, overall, about 40% will have a second seizure [Berg and Shinnar, 1991; Shinnar et al., 1996]. There is much less information about the further recurrence risk after a second seizure, especially if medication is withheld. Current data suggest that the risk of a third seizure after a second is at least 80% [Camfield et al., 1985b; Shinnar et al., 2000]. These observations validate the restriction of the diagnosis of epilepsy to those with two or more unprovoked seizures, because the concept of epilepsy implies a chronic, recurring disorder. If a child has a single seizure, a small number of clinical features are helpful to predict the risk of a second seizure. These include remote symptomatic cause, partial seizures, presence of intellectual or mental handicap, and possibly EEG spike discharge [Berg and Shinnar, 1991]. A normal child with a first generalized tonic-clonic seizure and a normal electroencephalogram has a recurrence risk of 20% to 30%, whereas a child with mental handicap, a partial seizure, and spike discharge on the electroencephalogram has a recurrence risk of 80% to 90% [Berg and Shinnar, 1991; Camfield et al., 1985b]. If a second seizure is to occur, it usually happens shortly after the first. At least 75% of recurrences happen within 6 months of the first, and most occur within a few weeks. Few recurrences are observed after 2 years. Very few children presenting with a first seizure develop severe epilepsy. Of 407 children with a first seizure identified by Shinnar and colleagues [2000], only 13% went on to have more than 10 seizures over the next 10 years. However, 28% of those with two seizures had more than 10 subsequent seizures.
Starting Medication Treatment There is little justification for beginning daily medication after a child’s first unprovoked seizure because 60% of these children will never have another attack [Van Donselaar et al., 1989.] Population-based studies have found that medication prescription after the first seizure does not alter the recurrence rate, probably because of poor compliance in taking the medication [Camfield et al., 1985b; Hauser et al., 1982; Hirtz et al., 1984]. An open-label, randomized trial of medication versus no medication after a first seizure in 397 children and adults demonstrated a significant reduction in recurrences for those on medication over a 2-year treatment period [First Seizure Trial Group, 1993]. The risk of recurrence without treatment was 51% by 24 months, but there were still relapses in 25% of those randomized to medication (i.e., 2.8 times higher; 95% confidence interval [CI ], 1.9 to 4.2). When this cohort was followed for several more years, the eventual remission rate was the same for those treated or untreated after the first seizure [Musicco et al., 1997].
985
It has become common practice to prescribe medication after a second seizure. There is no evidence that the prescription of medication alters the long-term outlook of childhood epilepsy. There is convincing information that delaying antiepileptic drug treatment until the child has had up to 10 seizures does not alter the ease of seizure control or the long-term remission rate [Camfield et al., 1996a]. In other words, if a child has few seizures, there is no evidence that each seizure facilitates the next. The main reasons to treat children with antiepileptic drugs are the avoidance of bodily injury from seizures and improvement in psychosocial function. Results from several studies indicate that injury is uncommon with most seizure types in children. Peters and associates [2001] described 79 children with benign rolandic epilepsy who together had more than 900 seizures over an 8.5-year period. There were no significant injuries. In a group of 59 children with generalized absence seizures followed over 15 years, Wirrell and colleagues [1997] observed that 16 had a serious physical injury as the result of a seizure. Kirsch and colleagues [2001] compared 31 cognitively normal children with epilepsy with bestfriend controls and found no significant differences in injury number or severity. Hodgman and co-workers [1979] described 25 adolescents with generalized tonic-clonic epilepsy and observed that those with poorer seizure control were better able to communicate about seizures and had a better self-image. The “hidden handicap” for children with controlled seizures may have important effects on social adjustment. When medication is started, most children still have more seizures. Only about 20% have “smooth-sailing epilepsy,” meaning that they start medication, become immediately seizure free, and later are able to successfully discontinue medication without ever having another seizure [Camfield et al., 1993]. Only 50% of children continue to receive the same medication 1 year after initiating treatment [Camfield et al., 1985b; Canadian Childhood Epilepsy Study Group, 1996; Verity et al., 1995]. The decision to start medication is often not the end of the seizure problem.
Long-Term Remission For many children, epilepsy is transient, and with maturation, the problem seems to vanish. At the time of diagnosis, it is possible to predict that at least 50% of children will outgrow their disorder and be able to discontinue medication [Camfield et al., 1993]. The Dutch Study of Epilepsy in Childhood followed 453 newly diagnosed children and found that 64% were no longer receiving medication 5 years later [Arts et al., 2004]. The longer the follow-up, the higher the proportion with remission of symptoms. In Rochester, Minnesota, 115 children with epilepsy beginning before age 10 years were followed through the Mayo Clinic record linkage system. Ten years later, 75% had been seizure free for at least 5 years, and 51% no longer received medication [Hauser et al., 1993]. At the end of a remarkable 30-year follow-up study of children with epilepsy from a population-based sample in Turku, Finland, Sillanpaa [1993] found that 76% of survivors had been seizure free for at least 3 years. Across most studies, factors that predict which children will outgrow their epilepsy have included normal intel-
986
Epilepsy / 40
TABLE 40-2 Scoring System for Remission of Childhood Epilepsy at the Time of Diagnosis VARIABLE Age of first seizure (months) 144 Intelligence Normal Retardation Previous neonatal seizures No Yes Number of seizures before starting medication 1 or 2 3 to 20 >20
SCORE* 99 142 0 111 0 218 0 72 123 0
*Add the scores from this column. If the total score is greater than 495, the child is predicted to have remission of epilepsy. Adapted from Sillanpaa M, Camfield PR, Camfield CS. Predicting long term outcome of childhood epilepsy in Nova Scotia, Canada, and Turku: Validation of a simple scoring system. Arch Neurol 1995;52:589.
ligence, normal neurologic examination findings, relatively small numbers of seizures at diagnosis (possibly a proxy measure for complex partial seizures), age of the first seizure younger than about 12 years, and absence of a remote symptomatic cause (an identified brain problem that preceded the onset of epilepsy). In an 8-year follow-up study of a population-based study of 504 children with epilepsy from Nova Scotia, a predictive scoring system was developed; it is outlined in Table 40-2 [Sillanpaa et al., 1995]. Those with a good prognosis had an 80% chance of remission (i.e., seizure free and no longer receiving medication). For those with one or more of these adverse factors, the chance of remission was less but still about 40%. The Dutch Study of Epilepsy in Childhood found comparable predictive variables and supplemented these with the clinical course in the first 6 months of treatment. Rates of correct prediction were similar. Based on clinical features present at the time of diagnosis, it is possible to predict the long-term outcome with moderate accuracy. Surprisingly, most epilepsy syndromes do not have a definite outcome; however, a few specific syndromes allow an accurate prognosis [Camfield et al., 2003]. Epilepsy is always outgrown in cases of benign rolandic epilepsy, benign myoclonic epilepsy of infancy, and benign occipital epilepsy, early-onset type. Epilepsy is never outgrown by children with Rasmussen’s syndrome, Lennox Gastaut syndrome, or Dravet’s syndrome.
Stopping Medication About 70% of children with epilepsy who have become seizure free for 1 to 2 years can successfully stop medication treatment [Berg and Shinnar, 1991; Dooley et al., 1996]. The rate of success is no greater if medication is continued for up to 5 years seizure free [Hollowach-Thurston et al., 1982]. Factors that predict successful discontinuation of medication include generalized seizures, age of onset before 10 to 12 years, normal neurologic examination, and in some studies, resolution of interictal EEG spike discharges. Chil-
dren with no adverse factors may have an 80% to 90% success rate. Each factor has an additive effect and those with all of the adverse factors may have only a 10% to 20% success rate. If an initial discontinuation trial is unsuccessful, medication is usually restarted. About 50% of children again become seizure free for sufficient time to try to discontinue medication a second time, with a 70% success rate [Camfield et al., 1993]. The remission rate for juvenile myoclonic epilepsy is so low that further attempts to discontinue medication after an initial failure are probably not warranted [Delgado-Escueta and Enrile-Bacsal, 1984]. A Scandinavian study randomized 207 children at the time of diagnosis of epilepsy to receive 1 or 3 years of treatment [Braathen and Melander, 1997]. If the child was seizure free for the last 6 months of study, medication was discontinued. This practice meant that some of the children in the 1-year treatment group had been seizure free for only 6 months before medication was stopped. The success rate for those in the short-treatment group was significantly less than for the 3-year group (53% versus 71%). A Dutch study randomized 161 children with epilepsy that was controlled within 2 months of starting treatment to 6 months or 1 year of treatment. The 6-month group had a higher relapse rate when medication was stopped; however, by 2 years later, the rates of remission were identical [Peters et al., 1998]. Nonetheless, for a substantial number of children, epilepsy was a short-lived disorder requiring only short-term medication use. Medication treatment for benign rolandic epilepsy often is not needed [Peters et al., 2001], and further studies will likely identify other children who do not require drug treatment.
Intractability Defining intractable epilepsy is difficult, and many definitions have been suggested. For a study of 613 children with epilepsy from Connecticut, Berg and Shinnar [2001] defined intractability as a “failure, for lack of seizure control, of more than 2 first-line antiepileptic drugs with an average of more than one seizure per month for 18 months and no more than 3 consecutive months seizure free during that interval.” There were 60 intractable cases in the first 24 months after diagnosis. The proportions of intractable patients in each major syndrome grouping were as follows: cryptogenic/symptomatic generalized, 34.6%; idiopathic generalized, 2.7%; other localization-related, 10.7%; and unclassified, 8.2%. Sillanpaa’s [1993] follow-up study from Turku, Finland, defined intractability as one or more seizures per year in the past 10 years of follow-up. After 20 years of follow-up, 22% of the subjects met these criteria. Predictors of intractability included poor initial response to medication, remote symptomatic cause, and status epilepticus. The Dutch Study of Childhood Epilepsy (using Berg and Shinnar’s definition of intractability), with 453 children followed for 5 years, found that 6% were intractable [Arts et al., 2004]. Camfield and colleagues [1993] defined intractability as “at least one seizure each three months for the last year of follow-up, with failure of at least 3 antiepileptic drugs.” For those with partial and generalized tonic-clonic epilepsies, 8% of 511 children became intractable during an average of 8 years of follow-up. After 20 years of follow-up,
Camfield and Camfield / Pediatric Epilepsy: An Overview
51% of 75 patients with childhood-onset symptomatic generalized epilepsy had intractable seizures. In this study, the major predictor was severe neurologic deficit at the time of diagnosis. An important issue in the definition of intractability is the length of follow-up. In the clinical setting, many children with intractable epilepsy eventually become well controlled. In a series of 145 children with intractable seizures (i.e., less than one per month for at least 2 years) followed over 18 years, Huttenlocker and Hapke observed that 75% of normally intelligent children and 30% with mental handicap had complete or nearly complete seizure remission (i.e., less than one seizure per year). In the Nova Scotia cohort, 39 patients with partial and generalized tonic-clonic epilepsies had intractable epilepsy after 7 years’ follow-up. After 12.5 years of followup, 7 (18%) of 39 became seizure free [Camfield et al., 1996a]. There is controversy about how many drug failures are required before intractability can be declared. In a Scottish study of 470 newly treated adults, 47% became seizure free with their first antiepileptic drug [Kwan and Brodie, 2000]. Only 11% gained control with subsequent medications. In children, the failure of a first drug is important but far less ominous [Camfield et al., 1997]. Of 417 eligible patients with partial and generalized tonic-clonic epilepsies with at least 4 years of follow-up, 83% were successfully treated with a single antiepileptic drug during the first year of treatment. Of these, 61% eventually had remission of epilepsy, and 4% had intractable seizures. Among the 17% who failed treatment with their first antiepileptic drug, 42% eventually had complete remission of epilepsy, although 29% developed intractable seizures. Children with absence epilepsies had nearly identical findings [Wirrell et al., 2001]. In summary, intractability for an individual child is difficult to predict before several years of antiepileptic drug treatment. Intractability appears to decrease with prolonged follow-up, although the burden of this wait-and-see approach may be substantial. Failure of a first antiepileptic drug is a risk factor for intractability but nonetheless many remit. As a general rule, consideration for epilepsy surgery should await failure of three appropriate drug treatments. Other factors influence this decision, including seizure severity, frequency, and duration of epilepsy.
Psychosocial Outcome for Children with Epilepsy Children with epilepsy have high rates of behavior and cognitive problems that contribute to social dysfunction in childhood and in later adulthood even if the epilepsy resolves. These issues are reviewed in more detail in Chapter 51. Austin and colleagues [2002] reported that at the time of diagnosis, 40% of children were at significant risk of behavior problems, as judged by scores on the Child Behavior Checklist. Those with multiple recurrent seizures were at even higher risk. The Isle of Wight study found that children with epilepsy had high rates of behavioral disorders [Rutter et al., 1970], which might have had their origins in social stigmatization, comorbid cognitive disorders, or medication effects. Oostrom and colleagues [2003] demonstrated greater cognitive and behavioral problems and the need for special educational assistance among 51 outpatient children with idiopathic or cryptogenic epilepsy compared with their classmate controls. Trostle [1988] reported that
987
parents indicate a reluctance to have their normal children play with a child with epilepsy. Less than one third of 20,000 U.S. high school students indicated that they would date a person with epilepsy [Austin et al., 2002]. These behavioral, cognitive, and social stigma problems in childhood all point to grave concerns for the social adjustment and success of children with epilepsy after they reach adulthood. Kokkonen and colleagues [1997] described the social outcome (by interview or questionnaire) of 81 young, “noninstitutionalized” adults from the catchment area of Oulu, Finland, compared with 211 randomly selected controls from the same birth cohort. At least 20% of this sample were unable to complete 9 years of education and presumably had severe learning disorders or mental retardation. They accounted for most of the poor social outcome, including a high rate of educational failure, failure to marry, and unemployment. In Nova Scotia and Finland, children with epilepsy only were followed into young adulthood [Camfield et al., 1993; Jalava et al., 1997]. Epilepsy only meant having normal intelligence and no other neurologic handicaps. About 30% of each cohort had significant social adjustment problems with decreased rates of stable relationships, marriage, social contacts, job satisfaction, and work achievement. Rates of unemployment or underemployment were high. Social outcome was not clearly related to epilepsy remission, and in the Nova Scotia study, variables related directly to epilepsy, such as age of onset, type of medication treatment, presence or absence of seizure remission, and frequency and severity of seizures, did not appear to predict social outcome in young adulthood [Camfield et al., 1993]. The strongest predictor of poor social outcome was the presence of a learning disorder, although predictive models were inaccurate; the main reasons for the unsatisfactory outcomes were unclear. Wakamoto and colleagues [2000] studied 148 normally intelligent young adults (>20 years old) living in a rural district of Japan who had childhood-onset epilepsy. This population-based study found that 72% attended regular classes (versus 99% of those without epilepsy), 66% (versus 97%) entered high school, 67% (versus 95%) had employment, and 23% (versus 33%) married. There were 49 patients with mental handicap having a less satisfactory outcome: 14% attended regular class, 6% entered high school, 20% were employed, and 2% married. Few studies have addressed the social outcome of children with specific epilepsy syndromes. Several studies have indicated a favorable outcome for adults with previous benign rolandic epilepsy (Loiseau et al., 1983; Peters et al., 2001]. In the Nova Scotia study, 56 children with typical Childhood absence epilepsy were followed to young adulthood [Wirrell et al., 1997] and compared with a similar cohort with mild juvenile rheumatoid arthritis. Those with absence had significantly greater problems with impulsive behavior, including a 34% risk of an unplanned pregnancy. Educational and work achievement, family and other social relationships, and alcohol abuse were more often unsatisfactory. Those with ongoing seizures despite medication had greater problems; however, most of the poor social outcome was unrelated to epilepsy-specific factors. Childhood epilepsy may have a life-long, serious effect on social function, an effect that is greater than some other
988
Epilepsy / 40
chronic disorders of childhood. Intervention studies have not been undertaken; however, the role of learning disorders and inadequate education is clear. If the long-term social outcome is to be rectified, physicians must address these areas with equal enthusiasm to the drug treatment of childhood epilepsy. Early referral to an epilepsy support group may be of benefit. REFERENCES Arzimanogolou A, Guerrini R, Aicardi J. Epilepsy in children, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2004. Arts WF, Brouwer OF, Peters AC, et al. Course and prognosis of childhood epilepsy: 5-year follow-up of the Dutch study of epilepsy in childhood. Brain 2004;127:1774. Austin JK, Shafer PO, Deering JB. Epilepsy familiarity, knowledge, and perceptions of stigma: Report from a survey of adolescents in the general population. Epilepsy Behav 2002;3:368. Berg AT, Shinnar S. The risk of seizure recurrence following a first unprovoked seizure: A meta-analysis. Neurology 1991;41:965. Braathen G, Melander H. Early discontinuation of treatment in children with uncomplicated epilepsy: A prospective study with a model for prediction of outcome. Epilepsia 1997;38:561. Camfield PR, Camfield CS. Nova Scotia Pediatric Epilepsy Study. In: Jallon P, ed. Prognosis of childhood epilepsy. London: John Libby Publishers, 2003. Camfield CS, Camfield PR, Gordon K, et al. Does the number of seizures before treatment influence ease of control or remission of childhood epilepsy? Not if the number is 10 or less. Neurology 1996a;46:41. Camfield CS, Camfield PR, Gordon K, et al. Outcome of childhood epilepsy: A population-based study with a simple predictive scoring system for those treated with medication. J Pediatr 1993;122:861. Camfield CS, Camfield PR, Wirrell E, et al. Incidence of epilepsy in childhood and adolescents: A population based study in Nova Scotia from 1977-1985. Epilepsia 1996b;37:19. Camfield PR, Camfield CS, Dooley JM, et al. Epilepsy after a first unprovoked seizure in childhood. Neurology 1985a;35:1657. Camfield PR, Camfield CS, Smith E, et al. Newly treated childhood epilepsy: A prospective study of recurrences and side effects. Neurology 1985b;35:722. Camfield PR, Camfield CS, Gordon K, Dooley JM. If a first antiepileptic drug fails to control a child’s epilepsy, what are the chances of success with the next drug? J Pediatr 1997;131;821–824. Camfield PR, Gordon K, Camfield CS, et al. EEG results are rarely the same if repeated within six months in childhood epilepsy. Can J Neurol Sci 1995;22:297. Canadian Childhood Epilepsy Study Group. Monotherapy clobazam has equivalent efficacy to carbamazepine and phenytoin in childhood epilepsy. Epilepsia 1996;37:117. Commission on Classification and Terminology of the International League against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981;22:489. Commission on Classification and Terminology of the International League against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989;30:389. Delgado-Escueta AV, Enrile-Bacsal F. Juvenile myoclonic epilepsy of Janz. Neurology 1984;34:285. Dooley J, Gordon K, Camfield P. “The rushes.” A migraine variant with hallucinations of time. Clin Pediatr 1990;29:536. Dooley JM, Gordon K, Camfield PR, et al. Discontinuation of anticonvulsant therapy in children free of seizures for 1 year. Neurology 1996;46:969. Engle J. International League against Epilepsy (ILAE). A proposed diagnostic scheme for people with epileptic seizures and with epilepsy. Report of the ILAE Taskforce on Classification and Terminology. Epilepsia 2001;42:796–803. Eriksson KJ, Koivikko MJ. Prevalence, classification, and severity of epilepsy and epileptic syndromes in children. Epilepsia 1997;38:1275. First Seizure Trial Group. Randomized clinical trial on the efficacy of antiepileptic drugs in reducing the risk of relapse after a first unprovoked tonic-clonic seizure. Neurology 1993;43:478.
Hauser WA, Anderson VE, Loewneson RB, et al. Seizure recurrence after a first unprovoked seizure. N Engl J Med 1982;307:522. Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935-84. Epilepsia 1993;34:453. Hauser WA, Hesdorffer DC. Epilepsy, frequency, causes, and consequences. New York: Demos Publications, 1990. Hirtz DG, Ellenberg JH, Nelson KB. The risk of recurrence of non-febrile seizures in children. Neurology 1984;34:637. Hirtz D, Berg A, Bettis D, et al. Practice parameter: Treatment of the child with a first unprovoked seizure: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2003;60:166–175. Hodgman CH, McAnarney ER, Myers GJ, et al. Emotional complications of adolescent grand mal epilepsy. J Pediatr 1979;95:309. Hollowach-Thurston J, Thurston DL, Hixton BB, et al. Prognosis of childhood epilepsy: Additional follow-up study of 148 children 15–23 years after withdrawal of anticonvulsant therapy. N Engl J Med 1982;306:831. Huttenlocker PR, Hapke RJ. A follow-up study of intractable seizures in childhood. Ann Neurol 1990;28;699–705. Jalava M, Sillanpaa M, Camfield CS, et al. Social adjustment and competence 35 years after onset of childhood epilepsy: A prospective controlled study. Epilepsia 1997;38:708. Kirsch R, Wirrell E. Do cognitively normal children with epilepsy have a higher rate of injury than their nonepileptic peers? Child Neurol 2001;16:100–104. Kokkonen J, Kokkonen ER, Saukkonen AL, Pennanen P. Psychosocial outcome of young adults with epilepsy in childhood. J Neurol Neurosurg Psychiatry 1997;62:265–268. Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med 2000;342:314–319. Loiseau P, Pestre M, Dartigues JF, et al. Long term prognosis in two forms of childhood epilepsy. Typical absence seizures and epilepsy with rolandic (centrotemporal) EEG foci. Ann Neurol 1983;13:642–648. Musicco M, Beghi E, Solari A, Viani F. Treatment of first tonic-clonic seizure does not improve the prognosis of epilepsy. First Seizure Trial Group (FIRST Group). Neurology 1997;49:991. Oostrom KJ, Smeets-Schouten A, Kruitwagen CL, et al. Not only a matter of epilepsy: early problems of cognition and behavior in children with “epilepsy only”—a prospective, longitudinal, controlled study starting at diagnosis. Pediatrics 2003;112(Pt 1):1338. Peters AC, Brouer OF, Geerts AT, et al. Randomized prospective study of early discontinuation of AEDs in children with epilepsy Neurology 1998;50:724–730. Peters J, Camfield CS, Camfield PR. Benign rolandic epilepsy can be safely managed without medication: A population-based study. Neurology 2001;57:537. Petersen O, Eeg-Olofsson O. Paroxysmal activity in EEG of normal children. In: Kelleway P, Peterson I, eds. Clinical electroencephalography of children. New York: Grune & Stratton, 1968. Rutter M, Graham P, Yule W. A neuropsychiatric study in childhood. Clin Dev Med 1970;35/36:175. Shinnar S, Berg AT, Moshe SL, et al. The risk of seizure recurrence after a first unprovoked afebrile seizure in childhood: An extended follow-up. Pediatrics 1996;98:216. Shinnar S, Shinnar S, Berg AT, et al. Predictors of multiple seizures in a cohort of children prospectively followed from the time of their first unprovoked seizure. Ann Neurol 2000;48:140–147. Sillanpaa M. Remission of seizures and predictors of intractability in long-term follow-up. Epilepsia 1993;34:930. Sillanpaa M, Camfield PR, Camfield CS. Predicting long term outcome of childhood epilepsy in Nova Scotia, Canada, and Turku, Finland: Validation of a simple scoring system. Arch Neurol 1995;52:589. Stephenson JB. Fits and faints. Philadelphia: JB Lippincott, 1991. Trojaborg W. Changes in spike foci in children. In: Kelleway P, Peterson I, eds. Clinical electroencephalography of children. New York: Grune & Stratton, 1968. Trostle JA. Social aspects of epilepsy. In: Hauser WA, ed. Current trends in epilepsy, Unit 1. Landover, MD: Epilepsy Foundation of America, 1988. Van Donselaar CA, Geerts AT, Meulstee J, et al. Reliability of the diagnosis of a first seizure.Neurology 1989;39:267–271.
Camfield and Camfield / Pediatric Epilepsy: An Overview Verity CM, Hosking G, Easter DJ. A multicentre comparative trial of sodium valproate and carbamazepine in paediatric epilepsy. The Paediatric EPITEG Collaborative Group. Dev Med Child Neurol 1995;37:97–108. Wakamoto H, Nagao H, Hayashi M, et al. Long-term medical, educational, and social prognoses of childhood-onset epilepsy: A population-based study in a rural district of Japan. Brain Dev 2000;22:246. Wirrell E, Camfield CS, Camfield PR, et al. Long-term psychosocial outcome in typical absence epilepsy: Sometimes a wolf in sheep’s clothing. Arch Pediatr Adolesc Med 1997;151:152. Wirrell E, Camfield C, Camfield P, Dooley J. Prognostic significance of failure of the initial antiepileptic drug in children with absence epilepsy. Epilepsia 2001;42:760–763.
989
SUGGESTED READING Arzimanogolou A, Guerrini R, Aicardi J. Epilepsy in children, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2004. Freeman JM, Vining EPG, Pillas DJ. Seizures and epilepsy in childhood: A guide, 3rd ed. Baltimore: Johns Hopkins University Press, 2003. Devinsky O. Epilepsy patient and family guide, 2nd ed. Philadelphia: FA Davis, 2002. Devinsky O, Westbrook LE. Epilepsy and developmental disabilities. Woburn, MA: Butterworth-Heinemann, 2002. Jallon P. Prognosis of epilepsies. London: John Libby, 2003. Roger J, Bureau M, Dravet C, et al. Epileptic syndromes in infancy, childhood and adolescence, 3rd ed. London: John Libby, 2003. Wyllie E. The treatment of epilepsy: Principles and practice, 3rd ed. Philadelphia: Lea & Febiger, 2001.
CHAPTER 41
Neurophysiology of Epilepsy Jong M. Rho and Carl E. Stafstrom
Epilepsy is defined by the occurrence of recurrent spontaneous seizures arising from aberrant electrical activity within the brain. Such electrical activity is the net product of biochemical processes at the cellular level occurring in the context of large neuronal networks, and it likely involves cortical and several key subcortical structures. The output of this activity is reflected on the surface electroencephalogram (EEG), which is the primary clinical tool with which normal and abnormal electrical activities in the brain are measured. At the cellular level, the two hallmark features of epileptiform activity are neuronal hyperexcitability and neuronal hypersynchrony. However, a single neuron discharging abnormally is insufficient to produce a temporary disruption of brain function; generally, a focal interictal discharge on an EEG cannot be seen unless a minimum of 1 to 2 cm2 of cortex exhibits increased excitability and synchrony [Niedermeyer and Lopes da Silva, 1999]. The cellular mechanisms of seizure genesis should always be viewed in this larger context. In many ways, clinical neurophysiologists and cellular electrophysiologists study the same phenomenon at macroscopic and microscopic levels. Although an extensive discussion of electricity and field theory is beyond the scope of the present discussion, it is helpful to understand the basic mechanisms that regulate neuronal activity. This chapter reviews the cellular basis for focal and generalized seizure activity (with specific attention to ion channels, the essential currency of neuronal excitability) and the factors that influence the enhanced susceptibility of the immature brain to seizures. The actions of antiepileptics that target the same ion channels that are required for normal brain function are summarized.
Generalized seizures begin with abnormal electrical discharges in both hemispheres and critically involve reciprocal thalamocortical connections (see Fig. 41-1). The electroencephalographic signature of a primary generalized seizure is bilaterally synchronous spike-wave discharges seen across all scalp electrodes. The manifestations of such widespread epileptiform activity can range from brief impairment of consciousness (e.g., an absence seizure) to rhythmic jerking movements of all extremities accompanied by loss of posture and consciousness. Although there are differences in the mechanisms that underlie partial and generalized seizure activity, it is still useful to view any seizure activity as a perturbation in the normal balance between inhibition and excitation in a localized region, in multiple areas (but linked in a multinodal network), or throughout the whole brain [McCormick and Contreras, 2001; Faingold, 2004]. This imbalance is likely a combination of increased excitation and decreased inhibition and, perhaps somewhat paradoxically, in some instances increased inhibition impinging on individual cells. However, it is important to recognize that epilepsy is not a singular disease. It is heterogeneous in terms of clinical expression, underlying causes, and pathophysiology (Table 41-1). As such, specific mechanisms and pathways underlying specific seizure phenotypes may vary when perturbations at a given hierarchical level lead to structural and functional changes at higher (e.g., network) or lower (e.g., molecular) levels of analysis.
CELLULAR ELECTROPHYSIOLOGY The Hippocampus
CLASSIFICATION OF SEIZURES Epileptic seizures are broadly divided into two groups, depending on their site of origin and pattern of spread (Fig. 41-1). Partial seizures arise from a localized region of the brain, and the associated clinical manifestations are related to the function ordinarily served by that area. Focal discharges can spread locally through synaptic and nonsynaptic mechanisms, distally to subcortical structures, and through commissural pathways to eventually involve the entire cortex. Such is the evolution believed to occur when focal seizures secondarily generalize. For example, a seizure arising from the left motor cortex may cause jerking movements of the right upper extremity. If the epileptiform discharges subsequently spread to adjacent areas and eventually encompass the entire brain, a secondarily generalized tonicclonic seizure may ensue.
The hippocampus has been a preferred brain region for many basic and epilepsy-related electrophysiologic studies, and hippocampal pyramidal cells have become one of the most intensively studied cell types in the central nervous system. Moreover, the orderly and relatively simple organization of hippocampal circuits have made them favorites among cellular electrophysiologists interested in studying synaptic and nonsynaptic mechanisms relevant to seizure genesis. Much of the following discussion focuses on studies conducted in the hippocampus. More details regarding the electrophysiology of the hippocampal formation have been provided by Schwartzkroin and Mueller [1987] and by Lopes da Silva and colleagues [1990]. The hippocampal formation consists of the dentate gyrus, the hippocampus proper (i.e., Ammon’s horn, with subregions CA1, CA2, and CA3), the subiculum, and the entorhinal cortex (Fig. 41-2). These four regions are linked
992
Epilepsy / 41 FIGURE 41-1. Coronal brain sections depicting seizure types and potential routes of seizure spread. A, Focal area of hyperexcitability (star under electrode 3) and spread to adjacent neocortex (solid arrow under electrode 4) by the corpus callosum (dotted arrow) or other commissural pathways to the contralateral cerebral hemisphere or by subcortical pathways (e.g., thalamus, upward dashed arrows). Accompanying electroencephalographic (EEG) patterns show brain electrical activity under electrodes 1 to 4. Focal epileptiform activity is maximal at electrode 3 and is seen at electrode 4 (left traces). If a seizure secondarily generalizes, activity may be seen synchronously at all electrodes after a delay (right traces). B, A primarily generalized seizure begins simultaneously in both hemispheres. The characteristic bilateral synchronous spike-wave EEG pattern is generated by reciprocal interactions between the cortex and thalamus, with rapid spread by means of the corpus callosum (CC) contributing to the rapid bilateral synchrony. One type of thalamic neuron (dark neuron) is a GABAergic inhibitory cell that displays intrinsic pacemaker activity. Cortical neurons (triangles) send impulses to thalamic relay neurons (diamond) and to inhibitory neurons, setting up oscillations of excitatory and inhibitory activity, which gives rise to the rhythmic spike-wave EEG pattern. (From Stafstrom CE. An introduction to seizures and epilepsy: Cellular mechanisms underlying classification and treatment. In: Stafstrom CE, Rho JM, eds. Epilepsy and the ketogenic diet. Totowa, NJ: Humana Press, 2004;6.)
TABLE 41-1 Pathophysiologic Defects Leading to Epilepsy LEVEL OF BRAIN FUNCTION
CONDITION
PATHOPHYSIOLOGIC MECHANISM
Neuronal network
Cerebral dysgenesis, post-traumatic scar, mesial temporal sclerosis (in TLE) Down syndrome and possibly other syndromes with mental retardation and seizures Pyridoxine (vitamin B6) dependency
Altered neuronal circuits; formation of aberrant excitatory connections (i.e., sprouting) Abnormal structure of dendrites and dendritic spines; altered current flow in neuron Decreased GABA synthesis; B6, a cofactor for GAD Abnormal GABA receptor subunits
Neuron structure Neurotransmitter synthesis Neurotransmitter receptors, inhibitory Neurotransmitter receptors, excitatory Synapse development
Angelman’s syndrome, juvenile myoclonic epilepsy
Neonatal seizures
Ion channels (i.e., channelopathies)
Benign familial neonatal convulsions
Nonketotic hyperglycinemia
Excess glycine leads to activation of NMDA receptors Many possible mechanisms, including the depolarizing action of GABA early in development Potassium channel mutations; impaired repolarization
GABA, γ-aminobutyric acid; GAD, glutamic acid decarboxylase; NMDA, N-methyl-D-aspartate; TLE, temporal lobe epilepsy.
by prominent excitatory, largely unidirectional feed-forward connections. There are, however, some “backward” projections, most prominently from the entorhinal cortex to Ammon’s horn and from the CA3 field to the dentate gyrus. The predominant forward-projecting trisynaptic circuit begins with neurons in layer II of the entorhinal cortex that project axons to the dentate gyrus along the perforant pathway, where they synapse on granule cell and interneuron dendrites. Granule cells, the principal cell type of the dentate gyrus, send their axons, called mossy fibers, to synapse on cells in the hilus and in the CA3 field of Ammon’s horn. CA3 pyramidal cells project to other CA3 pyramidal cells through local collaterals, to the CA1 field of Ammon’s horn through Schaffer collaterals, and to the contralateral hippocampus. CA1 pyramidal cells send their axons into the subicular complex, and neurons of the subicular complex project to the entorhinal cortex and other cortical and subcortical targets.
Overview of Ion Channels To understand abnormal electrical activity in the brain, it is essential to review the elements of normal synaptic functioning and neuronal firing (Fig. 41-3). The key channels and receptors involved in normal and epileptic firing are summarized in Table 41-2. Two major types of ion channels are responsible for inhibitory and excitatory activity. The first are voltage-gated sodium and calcium channels, whose function is to depolarize the cell membrane toward the action potential threshold, and voltage-gated potassium channels, which largely function to dampen excitation in the nervous system. These voltage-gated channels are activated by membrane potential changes that subsequently alter the conformational state of the channel and allow selective passage of charged ions through a pore. Ligand-gated receptors, such as glutamate and γ-aminobutyric acid (GABA) receptors, constitute the second type. In this group, a neurotransmitter
Rho and Stafstrom / Neurophysiology of Epilepsy rn
n’s
ho
o
m
Am
CA3
3
Fornix Schaffer collaterals 2 Mossy fibers
CA1 Granule cell
Hilus
yrus
ate g
Dent
Su
bic
ulu
m
1
Perforant path
inal orh ex o c rt
993
FIGURE 41-2. Schematic of major pathways of excitatory synaptic transmission in the hippocampal formation. The hippocampal trisynaptic pathway begins with neurons in layer II of the entorhinal cortex that project axons to the dentate gyrus along the perforant path (1), where they synapse on granule cell dendrites. Dentate granule cells send their axons (called mossy fibers) to synapse on cells in the hilus and in the CA3 field of Ammon’s horn (2). CA3 pyramidal cells project to the CA1 field of Ammon’s horn by means of Schaffer collaterals (3). CA1 neurons send projections outward through the fornix to other brain regions and back to the subiculum. For simplicity, only the classic feed-forward projections of the trisynaptic pathway are shown. Omitted are the known backward projections and local circuit interactions.
Ent
I
FIGURE 41-3. Normal neuronal firing is illustrated by the schematic of a neuron with one excitatory (E) and one inhibitory (I) input. Right trace shows membrane potential (in millivolts [mV]), beginning at a typical resting potential (–70 mV). Activation of E leads to graded excitatory postsynaptic potentials (EPSPs), the larger of which reaches threshold (approximately –40 mV) for an action potential. The action potential is followed by an after-hyperpolarization (AHP), the magnitude and duration of which determine when the next action potential can occur. Activation of I causes an inhibitory postsynaptic potential (IPSP). The inset shows a magnified portion of the neuronal membrane as a lipid bilayer with interposed voltage-gated Na+ and K+ channels; the direction of ion fluxes during excitatory activation is indicated. After firing, the membrane-bound Na+-K+ pump and star-shaped astroglial cells restore ionic balance. (From Stafstrom CE. An introduction to seizures and epilepsy: Cellular mechanisms underlying classification and treatment. In: Stafstrom CE, Rho JM, eds. Epilepsy and the ketogenic diet. Totowa, NJ: Humana Press, 2004;11.)
(prepackaged in vesicles) is released from a presynaptic terminal (after presynaptic calcium influx) into the synaptic cleft and then binds with selective affinity to a membranebound receptor on the postsynaptic membrane. Binding of neurotransmitter to its receptor recognition site activates a
cascade of events, including a conformational shift to reveal an ion-permeant pore. Passage of ions across these channels results in depolarization (i.e., inward flux of cations) or hyperpolarization (i.e., inward flux of anions or outward flux of cations).
994
Epilepsy / 41
TABLE 41-2 Roles of Channels and Receptors in Normal and Epileptic Firing CHANNEL OR RECEPTOR
ROLE IN NORMAL NEURONAL FUNCTION
POSSIBLE ROLE IN EPILEPSY
Voltage-gated Na+ channel Voltage-gated K+ channel Ca2+-dependent K+ channel Voltage-gated Ca2+ channel Non-NMDA receptor (i.e., AMPA) NMDA receptor
Subthreshold EPSP; action potential up-stroke Action potential down-stroke AHP after action potential; sets refractory period Transmitter release; carries depolarizing charge from dendrites to soma Fast EPSP Prolonged, slow EPSP
GABAA receptor GABAB receptor Electrical synapses Na+-K+ pump
IPSP Prolonged IPSP Ultrafast excitatory transmission Restores ionic balance
Repetitive action potential firing Abnormal action potential repolarization Limits repetitive firing Excess transmitter release; activates pathophysiologic intracellular processes Initiates PDS Maintains PDS; Ca2+ activates pathophysiologic intracellular processes Limits excitation Limits excitation Synchronization of neuronal firing Prevents K+-induced depolarization
AHP, after-hyperpolarization; AMPA, α-amino-3-hydroxy-5-methyl-4-isoxazoleproprionic acid; EPSP, excitatory postsynaptic potential; GABA, γ-aminobutyric acid; IPSP, inhibitory postsynaptic potential; NMDA, N-methyl-D-aspartate; PDS, paroxysmal depolarization shift.
Voltage-Dependent Membrane Conductances Depolarizing Conductances A rapidly inactivating inward sodium conductance underlies the depolarizing (excitatory) phase of the action potential, and a non-inactivating, persistent sodium current can augment cell depolarization (e.g., produced by excitatory synaptic input) in the range immediately subthreshold for spike initiation. Most antiepileptics are thought to act in part through interactions with voltage-dependent sodium channels [Rogawski and Löscher, 2004]. Each sodium channel exists as a complex of three polypeptide subunits; there is a major α subunit and two smaller β subunits that influence the kinetic properties of the α subunit. The shape of action potentials is determined by the types of α and β subunits present in an individual neuron [Catterall et al., 2003a]. Neurons also display voltage-gated inward calcium conductances. In the hippocampus, the most significant calcium currents occur in CA3 pyramidal cells and underlie burst discharges in these cells [Wong and Prince, 1978]. Activation of voltage-dependent calcium channels contributes to the depolarizing phase of the action potential, and it can affect neurotransmitter release, gene expression, and neuronal firing patterns. Several distinct subtypes of calcium channels are distinguished on the basis of electrophysiologic properties, pharmacologic profile, molecular structure, and cellular localization [Catterall et al., 2003b]. The molecular structure of voltage-gated calcium channels is similar to that of sodium channels. Voltage-dependent calcium channels are hetero-oligomeric complexes containing a principal pore-forming α1 subunit and one or more smaller subunits (α2, β, γ, and δ) that are not obligatory for normal activity but can modulate the kinetic properties of the channel.
Hyperpolarizing Conductances Depolarizing sodium and calcium currents are counterbalanced by an array of voltage-dependent hyperpolarizing (inhibitory) currents, primarily by potassium channels. Potassium channels represent the largest and most diverse family
of voltage-gated ionic channels, and they function to inhibit or decrease excitation in the nervous system. The prototypic voltage-gated potassium channel is composed of four membrane-spanning α subunits and four regulatory β subunits that are assembled in an octameric complex to form an ion selective pore. In hippocampal neurons, potassium conductances include a leak conductance, which is a major determinant of the resting membrane potential; an inward rectifier (involving the flux of other ions), which is activated by hyperpolarization; a large set of delayed rectifiers, which are involved in the termination of action potentials and repolarization of the neuron’s membrane potential; an A-current, which helps determine interspike interval and affects the rate of cell firing; an M-current, which is sensitive to cholinergic muscarinic agonists and affects resting membrane potential and rate of cell firing; and a set of calcium-activated potassium conductances, which are sensitive to intracellular calcium concentration and affect cell firing rate and interburst interval. Rectification is a term that comes from circuit theory, and it refers to a situation when the conductance of ions through an ion channel changes according to voltage in such a way that they flow better in one direction than another; rectification can also result from blocking of the pore by other ions. Modulation or facilitation of these hyperpolarizing conductances can be viewed as potentially antiepileptic. However, none of the traditional antiepileptics in clinical use today is thought to act directly and principally on voltagegated potassium channels. Newer antiepileptics appear to act in part by affecting potassium channel function. For example, topiramate induces a steady membrane hyperpolarization mediated by a potassium conductance [Herrero et al., 2002], and levetiracetam blocks sustained repetitive firing by paradoxically decreasing voltage-gated potassium currents [Madeja et al., 2003]. Retigabine, an investigational compound with broad efficacy in animal seizure models, appears to enhance activation of KCNQ2 and KCNQ3 potassium channels [Rogawski, 2000; Wickenden et al., 2000]. This finding is particularly intriguing, given that mutations in genes encoding these proteins have been linked to a rare form of inherited epilepsy, benign familial neonatal seizures [Biervert et al., 1998; Singh et al., 1998].
Rho and Stafstrom / Neurophysiology of Epilepsy
Synaptic Physiology Inhibitory Synaptic Transmission Synaptic inhibition in the hippocampus is mediated by two basic circuit configurations. First, feedback or recurrent inhibition occurs when excitatory principal neurons synapse with and excite inhibitory interneurons, which project back to the principal neurons and inhibit them (i.e., a negativefeedback loop). Second, feed-forward inhibition occurs when axons projecting into the region synapse with and directly activate inhibitory interneurons, which then inhibit principal neurons. Both feed-forward and feedback inhibitory circuits abound in the hippocampal formation [Lacaille et al., 1987], and in both circuit configurations, the major inhibitory neurotransmitter is GABA. GABA, the principal inhibitory neurotransmitter in the mammalian central nervous system, is a neutral amino acid synthesized from glutamic acid by the rate-limiting enzyme glutamic acid decarboxylase. GABA, released from axon terminals, binds to at least two classes of receptors, GABAA and GABAB, which are found on almost all cortical neurons [Martin and Olsen, 2000]. GABAA receptors also are found on glial cells, although their functional significance on these cells is unclear. The GABAA receptor is a macromolecular receptor complex consisting of an ion pore and binding sites for agonists and a variety of allosteric modulators, such as benzodiazepines and barbiturates, each differentially affecting the kinetic properties of the receptor [MacDonald and Olsen, 1994]. The GABAA receptor is a heteropentameric complex composed of combinations of several polypeptide subunits arranged in topographic fashion to form an ion channel. This channel is selectively permeable to chloride and bicarbonate ions. Seven subunits (α, β, γ, δ, ε, π, ρ) have been described, each with one or more subtypes. Although several thousand receptor isoforms are possible from differential expression and assembly of these various subtypes, there is likely to be only a limited number of functional combinations, but the precise subunit composition of native GABAA receptors has yet to be identified. However, it is thought that most functional GABAA receptors follow the general motif of containing either α and β or α, β, and γ subunits with uncertain stoichiometry. Because individual subunits may be differentially sensitive to pharmacologic agents, GABA receptor subunits represent potentially useful molecular targets for new antiepileptics. Activation of GABAA receptors on the somata of mature cortical neurons generally results in the influx of chloride ions (Cl–) and consequent membrane hyperpolarization, inhibiting cell discharge. In hippocampal cell dendrites and in the immature brain, however, GABAA receptor activation causes depolarization of the postsynaptic membrane. This reversal of the conventional GABAA effect is thought to reflect a reversed Cl– electrochemical gradient, a consequence of the immature expression of the K+-Cl– cotransporter, KCC2, which ordinarily renders GABA hyperpolarizing [Rivera et al., 1999]. Outward flux of bicarbonate through GABAA channels may further contribute to depolarization [Staley et al., 1995]. In addition to GABAA receptors, there are metabotropic GABAB receptors located on postsynaptic membrane and on presynaptic terminals. GABAB
995
receptors act through guanosine triphosphate (GTP)–binding proteins to control calcium or potassium conductances. Whereas GABAA receptors generate fast, high-conductance, inhibitory postsynaptic potentials close to the cell body, GABAB receptors on the postsynaptic membrane mediate slow, long-lasting, low-conductance inhibitory postsynaptic potentials, primarily in hippocampal pyramidal cell dendrites. Perhaps of more functional significance, activation of GABAB receptors on axon terminals blocks synaptic release of neurotransmitter. It is thought that GABAB receptors are associated with terminals that release GABA onto postsynaptic GABAA receptors. In such cases, activation of GABAB receptors reduces the amount of GABA released, resulting in disinhibition [Mott and Lewis, 1994; Simeone et al., 2003].
Excitatory Synaptic Transmission Glutamate, an excitatory amino acid, is the principal excitatory neurotransmitter of the mammalian central nervous system, including the hippocampal formation. Glutamatergic pathways are widespread throughout the brain, and excitatory amino acid activity is critical to normal brain development and activity-dependent synaptic plasticity [Simeone et al., 2004]. Ionotropic glutamate receptors are broadly divided into N-methyl-D-aspartate (NMDA) and non-NMDA receptors, based on biophysical properties and pharmacologic profiles [Dingledine et al., 1999]. Each subtype of glutamate receptor consists of a multimeric assembly of subunits that determine its distinct functional properties. Glutamate receptor channel subunits are classified into six subfamilies based on amino acid sequence homology [Hollmann and Heinemann, 1994]. The NMDA receptor contains a binding site for glutamate (or NMDA) and a recognition site for a variety of modulators (e.g., glycine, polyamines, MK-801, zinc). NMDA receptors also demonstrate voltage-dependent block by magnesium ions [Mori and Mishina, 1995]. When the membrane is depolarized and the magnesium block of the NMDA receptor is alleviated, activation of the NMDA receptor results in an influx of calcium (Ca2+) and sodium (Na+) ions. Calcium entry is central to the initiation of a number of second messenger pathways, such as stimulation of a variety of kinases that subsequently activate signal transduction cascades leading to changes in transcriptional regulation. Activation of the NMDA receptor leads to generation of relatively slow and long-lasting excitatory postsynaptic potentials. These synaptic events contribute to epileptiform burst discharges, and NMDA receptor blockade results in the attenuation of bursting activity in many models of epileptiform activity. Non-NMDA ionotropic receptors are divided into αamino-3-hydroxy-5-methyl-4-isoxazoleproprionic acid (AMPA) and kainate receptors [Dingledine et al., 1999]. The AMPA receptor in particular is responsible for the major part of the excitatory postsynaptic potential—fast rising and brief in duration—generated by release of glutamate onto postsynaptic neurons. The depolarization generated by AMPA receptors is necessary for effective activation of NMDA receptors. Consequently, AMPA receptor antagonists block most excitatory synaptic activity in pyramidal neurons. Metabotropic glutamate receptors represent a large, heterogeneous family of G-protein–coupled receptors that
996
Epilepsy / 41
subsequently activate various transduction pathways—phosphoinositide hydrolysis and activation of adenylate cyclase and phospholipases C and D [Conn, 2003]. These metabotropic receptors are important modulators of voltagedependent potassium and calcium channels, nonselective cation currents, ligand-gated receptors (i.e., GABA and glutamate receptors), and they can regulate glutamate release. It is not surprising that they have been invoked in the description of a wide variety of neurologic processes (e.g., long-term potentiation) and disease states (e.g., epilepsy). A detailed discussion of these receptors is beyond the scope of this chapter, but it is clear that different metabotropic glutamate receptor subtypes are specific for different intracellular processes. Although ubiquitous within the central nervous system, subtypes of metabotropic receptors appear to be differentially localized.
Abnormal Neuronal Firing What happens at the neuronal network level when neurons transition from their normal firing pattern to interictal epileptiform bursts and then to an ictal state in which there is an evolution of electrophysiologic changes that is sustained, evolving, and with a terminal event, followed by postictal changes? Much of our understanding of epilepsy mechanisms comes from electrophysiologic studies in which
microelectrodes are placed inside individual neurons to record intracellular potential changes. Figure 41-4 depicts electroencephalographic and intracellular changes that can be seen in normal, interictal, and ictal states. In the normal situation, action potentials (which represent all-or-none events) are generated in neuron 1 when the membrane potential reaches threshold for firing (approximately –40 mV). These discharges may influence the activity of an adjacent neuron (neuron 2) through electrical field (i.e., ephaptic) or synaptic mechanisms, resulting in an excitatory postsynaptic potential. An adjacent interneuron (neuron 3, which is inhibitory) may also be activated by a discharge from neuron 1 after a brief delay, giving rise to an inhibitory postsynaptic potential. The activity recorded in neuron 2 reflects the temporal and spatial summation of excitatory postsynaptic potential and inhibitory postsynaptic potential inputs. If this integrative concept is extrapolated to thousands of interconnections (i.e., synaptic contacts), it is easy to envision the “sculpting” or grading of individual cellular responses modulated by degrees of inhibition. If we consider that a single inhibitory interneuron, such as in the hippocampus, can connect with hundreds to several thousand pyramidal neurons, it is straightforward to see how hypersynchronous behavior can be influenced by even a single cell. For a localized collection of hyperexcitable neurons
FIGURE 41-4. Abnormal neuronal firing at the levels of the brain (A) and a simplified neuronal network (B), consisting of two excitatory neurons (1 and 2) and an inhibitory interneuron (solid circle, 3). Electroencephalographic (EEG) (top set of traces) and intracellular recordings (bottom set of traces) are shown for normal (left column), interictal (middle column), and ictal (right column)conditions. Numbered traces refer to like-numbered recording sites. Notice the time scale differences in different traces. A, Three EEG electrodes record activity from superficial neocortical neurons. In the normal case, activity is low voltage and desynchronized (i.e., neurons are not firing together in synchrony). In the interictal condition, large spikes are seen focally at electrode 2 (and to a lesser extent at electrode 1, where they may be called sharp waves), representing synchronized firing of a large population of hyperexcitable neurons (expanded in time below). The ictal state is characterized by a long run of spikes. B, At the neuronal network level, the intracellular correlate of the interictal EEG spike is called the paroxysmal depolarization shift (PDS). The PDS is initiated by a non–NMDA-mediated, fast excitatory postsynaptic potential (EPSP) (shaded area), but it is maintained by a longer, larger, NMDA-mediated EPSP. The post-PDS hyperpolarization (asterisk) temporarily stabilizes the neuron. If this post-PDS hyperpolarization fails (right column, arrow), ictal discharge can occur. The lowest traces, recordings from neuron 2, show activity similar to that recorded in neuron 1, with some delay (double-headed arrow). Activation of inhibitory neuron 3 by firing of neuron 1 prevents neuron 2 from generating an action potential (i.e., the inhibitory postsynaptic potential [IPSP] counters the depolarization caused by the EPSP). If neuron 2 does reach firing threshold, additional neurons will be recruited, leading to an entire network firing in synchrony (i.e., a seizure). NMDA, N-methyl-D-aspartate. (From Stafstrom CE. An introduction to seizures and epilepsy: Cellular mechanisms underlying classification and treatment. In: Stafstrom CE, Rho JM, eds. Epilepsy and the ketogenic diet. Totowa, NJ: Humana Press, 2004;18).
Rho and Stafstrom / Neurophysiology of Epilepsy EEG
Spike
Slow-wave
+20 0
2
–20 –40
receptors (i.e., AMPA receptors), whereas the sustained depolarization is a consequence of NMDA receptor activation. Afterward, the paroxysmal depolarization shift terminates with a repolarization phase, primarily as a consequence of inhibitory potassium and chloride conductances carried by voltage-gated potassium channels and GABA receptors. The prolonged period of hyperpolarization after the paroxysmal depolarization shift is mediated by inhibitory conductances and constitutes a refractory period.
Synchronizing Mechanisms
INTRACELLULAR RECORDING
Vm
997
Paroxysmal depolarization shift
1
–60 –80
ION CHANNELS
3
AMPA receptor activation NMDA receptor activation Sodium conductance Calcium conductance
Potassium conductance GABA inhibition Chloride conductance FIGURE 41-5. The paroxysmal depolarization shift (PDS) is the intracellular correlate of an interictal spike on the surface electroencephalogram. The temporal correlations are illustrated for an interictal epileptiform discharge (top, spike and slow-wave complex), intracellular recording (middle), and sequence of ionic conductance changes. The PDS is initiated by excitatory conductances (dark bars) and terminated by inhibitory conductances (light bars). The initial depolarization (phase 1), which is an excitatory postsynaptic potential (EPSP), is mediated by α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA) receptors and sustained by N-methyl-D-aspartate (NMDA) receptors, whereas the overriding action potentials (phase 2) are generated by voltage-gated sodium channels and calcium channels. Repolarization and after-hyperpolarization (phase 3) are mediated by inhibitory conductances (i.e., multiple voltage-gated potassium channels and chloride flux such as through γ-aminobutyric acid [GABA] receptors).
to spread to adjacent areas, the epileptic firing must overcome the powerful inhibitory influences that normally keep aberrant excitability in check (i.e., concept of the inhibitory surround).
Paroxysmal Depolarization Shift The intracellular correlate of the focal interictal epileptiform discharge on the EEG is known as the paroxysmal depolarization shift. It is seen when recording changes in membrane potential of a single neuron with a microelectrode while simultaneously recording a focal spike on the EEG (Fig. 41-5). Initially, there is a rapid shift in the membrane potential in a depolarizing direction, followed by a burst of repetitive action potentials lasting several hundred milliseconds. The initial depolarization is mediated by non-NMDA glutamate
The hippocampal formation (see Fig. 41-2) normally displays robust neuronal synchronization. Sharp waves, dentate spikes, theta activity, 40-Hz oscillations, and 200-Hz oscillations are all forms of neuronal synchronization that can be recorded in various regions of the hippocampal formation [Buzsáki et al., 1994]. Synchronization of neuronal activity appears to be intrinsic to the mechanism by which the hippocampus performs its normal functions. However, neuronal synchronization also is a hallmark of epilepsy. Exaggerated synchrony among hippocampal neurons may directly generate “seizures,” because seizures are defined by hypersynchronous neuronal activity. Normal forms of synchronized activity that do not trigger seizures in a normal hippocampus may trigger epileptiform discharges in a hippocampus that has undergone selective neuronal loss, synaptic reorganization, or changes in receptor expression. For example, electroencephalographic spikes have been recorded from the dentate gyrus of normal rats. They reflect the synchronized discharges of entorhinal cortical neurons, which synapse on granule cells to initiate inward currents in dentate granule cell dendrites [Bragin et al., 1995]. In the hippocampal formation, synchronizing mechanisms include inputs from subcortical nuclei and intrinsic interneuron-mediated synchronization. For example, highamplitude theta activity is a salient feature of the hippocampus. The theta rhythm represents synchronized activity of hippocampal neurons and largely depends on input from the septum [Buzsáki et al., 1983]. Subcortical nuclei such as the septum have divergent inputs that target hippocampal interneurons. The divergent axon projections of interneurons and the powerful effect of the GABAA receptor–mediated conductances that they produce enable interneurons to entrain the activity of large populations of principal cells [Cobb et al., 1995]. These characteristics make interneurons a very effective target for subcortical modulation of hippocampal principal cell activity. Mutual inhibitory interactions among hippocampal interneurons also can produce synchronized discharges [Jefferys et al., 1996]. Recurrent excitatory circuits are another basis for neuronal synchronization in the hippocampus. Recurrent excitatory collaterals are a normal feature of the CA3 region; CA3 pyramidal cells form direct, monosynaptic connections with other CA3 pyramidal cells. These recurrent excitatory interactions contribute to the synchronized burst discharges that characterize this region of Ammon’s horn [Traub and Miles, 1991]. The epileptic temporal lobe, synaptic reorganization, and axonal sprouting may lead to aberrant recurrent excitation, providing a synchronizing mechanism in other parts of the hippocampal formation, including the CA1 region, subicular complex, entorhinal cortex, and dentate
998
Epilepsy / 41
(+)
FIGURE 41-6. Granule cells (GC) receive their major input by the perforant path. The perforant path also stimulates hilar interneurons (e.g., mossy cells, basket cells) to provide feed-forward inhibition of the granule cells. Granule cell axons, the mossy fibers (MFs), make synaptic contact with CA3 pyramidal cells. Mossy fiber collaterals innervate the hilar interneurons such as the mossy cell shown in the diagram. Mossy cells are excitatory to GABAergic basket cells that provide feedback inhibition to the granule cell. Sprouting of mossy fibers (in response to seizure-induced loss of CA3 pyramidal cells and hilar mossy cells) can result in enhanced excitation by forming autapses (i.e., an axon sprout synapsing with the dendrites of the same cell) and can augment synchronization by stimulating neighboring granule cells (not shown), contributing to epileptogenicity. It has been suggested that the sprouted mossy fibers may restore inhibition lost after seizure-induced death of hilar mossy cells by direct stimulation of deafferented (dormant) basket cells. (From Menkes JH, Sankar R. Paroxysmal disorders. In: Menkes JH, Sarnat HB, eds. Child neurology, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2000;919.)
Perforant path from entorhinal cortex
(–)
(+)
(–)
(+) GC
Sprouted MFs
(+)
Basket cell (+)
(+)
Mossy cell
(+)
MFs to hilar and CA3 pyramidal cells
(+)
CA3 pyramidal cell To fornix via alveus and CA1 via Schaffer collaterals
gyrus. In the dentate gyrus of the normal hippocampus, for example, granule cells form few or no monosynaptic contacts with neighboring granule cells. However, in the epileptic hippocampus, mossy fiber sprouting results in direct excitatory interactions among granule cells (Fig. 41-6). Mechanisms independent of chemical synaptic transmission may synchronize hippocampal neuronal firing under some circumstances. Such mechanisms include gap junctions, electrical field effects, and changes in extracellular ion concentrations. Gap junctions allow electrical signals to pass directly between cells. Studies suggest that gap junctions are upregulated in epileptic brain tissue [Li et al., 2001] and that blockade of gap junctions significantly affects the duration of seizure activity [Kohling et al., 2001]. Electrical field effects are generated by current flow through the extracellular space. Earlier studies demonstrated the potential synchronizing effect of “ephaptic” interactions, and later experiments suggest that manipulations that alter the extracellular space volume (i.e., affecting current flow through this compartment) can impact the epileptogenic synchronization neurons [Hochman et al., 1995]. Increases in extracellular potassium concentration have long been thought to affect epileptogenic excitability and synchronization, and experiments have demonstrated clear epileptogenic effects of blocking potassium regulation (e.g., through inwardly rectifying potassium channels) [Emmi et al., 2000].
Glial Mechanisms for Modulating Epileptogenicity The role of glial cells in epileptiform discharge received considerable attention in the past, but glial contributions have been significantly neglected in studies of epileptogenic mechanisms. Because the ionic balance between the intracellular and extracellular compartments is altered after
CA1
neuronal activity (especially after sustained, repetitive discharges seen with seizures), there must exist mechanisms to restore ion homeostasis. Otherwise, even normal neuronal activity would cease. Astrocytes are perhaps most closely associated with regulation of extracellular potassium levels (i.e., potassium buffering) because glial cell membranes are preferentially permeable to potassium. A variety of inwardly rectifying potassium ion (K+) channels provide an appropriate means for potassium uptake, and the association of glial end-feet with brain microvasculature provides a convenient “sink” for potassium release. Glial cell membrane potential changes are directly correlated with changes in extracellular potassium, and blockade of potassium channels that is selective for glial cells results in neuronal hyperexcitability. It seems certain that glial cells help to modulate neuronal discharge through their regulation of extracellular potassium. Despite the circumstantial evidence for glial potassium regulation, some investigators think that the glial cells play an even more important role in the maintenance of neuronal excitability—transporting glutamate (released from neuronal terminals to excite other neurons) out of the extracellular space. Glia cells are uniquely equipped for this role, having at least two powerful glutamate transport molecules in their membranes [Gegelashvili and Schousboe, 1998]. Rapid and efficient removal of extracellular glutamate characterizes normal, healthy brain tissue, and it is essential because residual glutamate would continue to excite surrounding neurons. Blockade of glutamate transporters (or knockout of the genes for these transport proteins) results in epileptic or excitotoxic activities, or both [Meldrum et al., 1999; Rothstein et al., 1996]. Glial cells contribute to modulation of excitability in a number of other ways. First, they play a critical role of regulating extracellular pH by a proton exchanger [Deitmer
Rho and Stafstrom / Neurophysiology of Epilepsy
999
jections to thalamic relay neurons and inhibitory GABAergic neurons comprising the nucleus reticularis thalami. Excitatory outputs of the thalamic relay neurons impinge on the apical dendrites of layer VI pyramidal neurons in the neocortex. This so-called thalamocortical relay is a critical substrate for the generation of cortical rhythms, and it is influenced by sensory inputs (e.g., from the retina) and by several brainstem nuclei that constitute the origin of cholinergic, noradrenergic, serotonergic, and other projections. This reciprocal circuitry, which is responsible in large part for normal electroencephalographic oscillations during wake and sleep states, can become hyperactive to generate generalized spike-wave discharges or can be dampened to reduce or eliminate spontaneous cortical rhythms. The anatomy implies that spike-wave discharges can be interrupted at cortical or thalamic levels. Although multiple ionic conductances are involved in rhythmic pacemaking activity, two specific channels are believed to play a key role in regulating such thalamocortical activity. The first is a subtype of voltage-gated calcium channel known as the low-threshold calcium channel (T-type channel). These channels can be activated by small depolarizations of the plasma membrane. In many neurons, calcium influx through these channels triggers lowthreshold spikes and activates a burst of action potentials [McCormick and Contreras, 2001; Perez-Reyes, 2003]. Such an excitatory burst is thought to underlie the spike portion of a generalized spike-wave oscillation. Antiepileptics known to be clinically effective against absence seizures (e.g., ethosuximide, valproic acid) can block T-type calcium currents. Whether augmentation of T-type calcium currents is essential in the genesis of absence seizures remains controversial [Leresche et al., 1998; Song et al., 2004]. The second important ion channel involved in the regulation of thalamocortical rhythmicity is the hyperpolarization-activated cation channel, responsible for the
and Rose, 1996] and by bicarbonate transporter mechanisms [Newman, 1999]. Even low levels of neuronal activity create significant pH transients. The pH modulates receptor function, particularly the NMDA receptor that appears to play such an important role in epileptic discharges [Traynelis and Cull-Candy, 1990]. Second, glial cells are thought to release powerful neuroactive agents into the extracellular space. Studies have indicated that glial glutamate release can excite neighboring neurons, and some investigations have suggested that other glia-related factors—such as the cytokine interleukin-1—can have profound antiepileptic efficacy [Vezzani et al., 2000].
Physiology of Absence Epilepsy Absence seizures represent a subtype of generalized-onset seizures with distinct pathophysiologic substrates. As the term implies, an absence seizure is characterized by a temporary loss of consciousness with total amnesia for the event—usually, a sudden cessation of motor activity without falling. These seizures usually are short lived ( tablets > extended-release formulations [Garnett and Cloyd, 1993]. Formulation-related differences in absorption characteristics can also be determined by the composition of the inactive ingredients (e.g., filler, particle size of drug, nature of the capsule or tablet, coating).
Distribution Volume and Protein Binding Volume of distribution in its simplest form is the ratio of the amount of drug in the body to blood concentration and is expressed in terms of liters or liters per kilogram. Mathematically, the ratio is expressed as the following: Volume of distribution = intravenous dose (mg)/plasma concentration (mg/L) attained immediately after injection Because calculation of distribution volume is based on plasma concentration, volume usually does not directly relate to a physiologic space. For example, drugs that concentrate in certain tissues and have relatively low plasma concentrations may have distribution volumes measured in hundreds of liters. Changes in body composition such as increases or decreases in fat, muscle, or water can alter volume.
Distribution volume in drug therapy is useful in calculating loading doses. The purpose of a loading dose is to rapidly fill body compartments to reach a targeted plasma concentration and thus a targeted concentration at the site of action. The equation for calculating a loading dose is the following: Loading dose = volume of distribution (L/kg) × body weight (kg) × desired change in plasma concentration The change in plasma concentration denotes the desired increase after administration of the loading dose. For example, if a patient has a plasma concentration of 5 mg/L and the target concentration is 20 mg/L, the desired change in concentration is 15 mg/L. When loading doses are administered intramuscularly, orally, or rectally, resultant maximum plasma concentrations are usually less than after intravenous administration, owing to slower and incomplete absorption and the elimination of some drug during the absorption phase. Table 49-4 presents loading dose information for five major antiepileptic drugs. Several antiepileptic drugs are highly bound to one or more plasma proteins, most commonly albumin or α1-acid glycoprotein. Drug assays usually measure the total concentration of drug, which is a combination of the bound and
TABLE 49-4 Loading Doses of Antiepileptic Drugs DRUG
Vd (L/kg)
LOADING DOSE (mg/kg)
ROUTE, FORMULATION
Cmax (mg/L)
Tmax (hr)
Carbamazepine Fosphenytoin Phenobarbital Phenytoin (PHT)
0.8 0.04 0.8 0.75 0.75 0.75 0.15-0.25 0.15-0.25
10 10-20 20 20 20 20 20 15-25
PO, suspension IV, intramuscular IV IV PO, prompt-release capsule PO, ER capsule PO, syrup IV
6-9 PHT 15-25 15-25 20-30 15-25 10-20 60-100 90-100
2-6 200 ng/mL Nordiazepam reached in 15 min accumulates with repeated doses Well tolerated Peak concentration 0.5-2 hr Effect in 20 min; peak concentration 2.5 hr Peak concentration 4-5 hr 90% absorbed Same as for acute Peak concentration 0.5-1.5 hr Peak concentration 2-3 hr, 95% absorbed
Well tolerated Moderate cathartic effect; use glass syringe Onset may be too slow for acute use Well tolerated
Peak concentration 1-3 hr
Definite cathartic effect
Peak concentration 2-4 hr 80% absorbed
Well tolerated
*Extemporaneously prepared using commercial product; all other preparations are commercial products given rectally. Adapted from Graves NM, Kriel RL. Rectal administration of AEDs in children. Pediatric Neurol 1987;3:321 ; and Garnett, WR, Cloyd JC. Dosage from considerations in the treatment of epilepsy. In: Dodson WE, Pellock JM, eds. Pediatric epilepsy: Diagnosis and therapy. New York: Demos, 1993;373–385. Additional data from Birnbaum et al, 2000, 2001; and Conway et al., 2003.
training; and, under the right circumstances, allows rapid drug absorption. Although the absorptive area of the nasal cavity is approximately the same as that of the rectum, the volume of solution that can be instilled is 0.5 mL or less [Romeo et al., 1998]. Several studies comparing intranasal midazolam with intravenous diazepam have been done in children. In summary, both drugs had similar onset of effect and seizure control, although intranasal midazolam has been used for preoperative sedation. Several disadvantages are associated with intranasal midazolam administration: (1) many patients complain of significant nasal discomfort, presumably owing to the acidic pH of the solution, (2) the volume of a clinically relevant dose is too large for many patients, (3) bioavailability after intranasal administration is intermediate and variable, and (4) its elimination half-life in children is short [Burstein et al., 1997]. The rapid elimination half-life may explain the reports of seizure breakthrough within a few hours after intranasal delivery of midazolam [Scheepers et al., 2000]. Intranasal administration of midazolam has been used for preoperative sedation. Absorption of diazepam has been demonstrated after intranasal delivery [Lindhardt et al., 2001]. There are currently no commercial intranasal formulations available.
Other Routes of Administration Lorazepam is absorbed after sublingual administration and can be useful in treatment of serial and prolonged seizures [Yager and Seshia, 1988]. Delivery of antiepileptic agents directly into the cerebral subarachnoid or intraventricular space should be possible. Spinal intrathecal administration of baclofen for control of spasticity is currently used for persons with spinal cord disease and cerebral palsy and can be administered by a programmable continuous pump surgically placed in the abdomen [Albright et al., 1993; Penn et al., 1989]. Transdermal administration of antiepileptic medications is under experimental investigation.
MONITORING OF PATIENTS ON ANTIEPILEPTIC DRUG THERAPY Clinical Monitoring of Efficacy Clinical assessment of patients is of paramount importance in the assessment of the effectiveness of therapy. The ideal response would be the total elimination of seizures without
Conway, Kriel, and Birnbaum / Antiepileptic Drug Therapy in Children
any adverse effects of therapy. A satisfactory clinical response for many patients, however, might be substantial reduction of seizures with elimination of or decrease in adverse effects. One of the most common clinical errors is the premature interpretation of the clinical response. Assessment of seizure control requires an accurate record of seizure frequency and severity before and during therapy. Seizures may be eliminated, reduced or increased in frequency, and more or less severe during therapy. Patients with epilepsy have varying seizure frequency rates before therapy. The length of time required to assess clinical response varies with the frequency of seizures observed before beginning therapy. Patients with infrequent seizures need a longer period of observation on therapy to permit assessment of clinical response. Statistical interpretation of the change in seizure frequency based on modified sequential analysis has been proposed [Leppik et al., 1989]. In addition, achievement of steady state with the new drug regimen is necessary to determine if a medication has been given an adequate trial at any specific dose. The time to achieve a steady state varies considerably from drug to drug, depending on the drug’s half-life. In every case, 5 half-lives must elapse before a steady state is reached. Interpretation of clinical response in patients in whom polypharmacy is necessary is especially difficult. Clinical improvement or deterioration after the addition of a second antiepileptic drug could be due to numerous factors. Such factors include the additive or synergistic effect of the two medications, the effect of the second drug alone, and the effect of the second drug on the metabolism and/or displacement of the initial drug. It is important to make clinical conclusions only after a steady state is reached with the new drug regimen. If improvement is obtained after the addition of the second medication, the clinician should attempt to discontinue the first medication, to determine whether the clinical improvement is an effect of synergistic therapy or that of the second medication itself. Finally, it is necessary to remember that withdrawal of co-medication might have an effect on the disposition of the remaining drug(s), which could influence clinical response (see Fig. 49-5).
Clinical Monitoring of Adverse Effects The clinical state of the patient is more important than laboratory testing for the assessment of adverse effects. It is possible to continuously monitor clinical states, whereas laboratory tests generally are obtained at arbitrary times; therefore, impending organ dysfunction often may be detected earlier by clinical changes, rather than by laboratory tests. The most frequent adverse effects are dose related and often involve the nervous system. Common manifestations of adverse effects are cognitive changes and drowsiness, impaired attention, incoordination, ataxia, and diplopia. In addition to CNS adverse reactions, the liver also may produce signs of toxicity. Early signs of liver failure include anorexia, nausea, vomiting, lethargy, and abdominal pain.
Monitoring of Drug Concentrations The ability to measure blood levels of antiepileptic drugs has been a major advance in the understanding of drug metabolism and disposition and has led to more rational drug
1121
therapy. The influence of periodic monitoring of blood levels may reduce the number of therapeutic failures by 50% [Kutt and Penry, 1974]. As expected, drug concentrations generally are related to the dose administered; however, unexpected results may occur, especially in cases of patient noncompliance or with drugs that follow nonlinear kinetics.
Interpretation of “Optimal Drug Concentrations” Numerous factors should be considered in the interpretation of drug concentrations. Medications that have rapid absorption and clearance have wide fluctuation between dosing intervals. For example, the liquid formulation of valproic acid, especially when given to a child also receiving enzyme-inducing co-medications, is rapidly absorbed and eliminated; therefore, a twofold fluctuation during dosing intervals is possible. Recording the time of the blood sample in relation to the last dose is needed to properly interpret laboratory results. Unexpectedly low concentrations are most frequently the result of poor compliance; however, they might be seen after the addition of an enzyme-inducing co-medication. Very high drug concentrations are seen with administration of high doses, in persons with genetically low clearance or some disease states, or with use of enzyme-inhibiting comedications such as valproate [Perucca et al., 2001]. The terms optimal drug concentration and target range are preferred over therapeutic range, for several reasons. First, these newer terms express the concept that the optimal dose and drug concentration need to be determined for each individual patient. The ideal or optimal dose and drug concentration would be those associated with complete control of seizures with no adverse effects. Clinical effects and toxicity of antiepileptic drugs correlate better with drug concentrations than with total daily dosage [Glauser and Pippenger, 2000]. Published “optimal drug concentrations” are attempts to report ranges of concentrations at which most patients have improved seizure control without significant adverse effects. These ranges generally have not been determined by controlled studies in large populations. Obviously, more clinical experience correlating clinical response with drug concentrations is available for the older antiepileptic drugs. Although measurement of drug concentrations has contributed greatly to the development of rational drug management, such management is performed less frequently in current clinical practice. In a randomized controlled trial of the impact of drug monitoring, no benefit with regard to improved seizure control or reduced adverse effects was observed in the study group in which levels were routinely sampled [Jannuzzi et al., 2000]. A retrospective study of antiepileptic drug monitoring in a pediatric emergency room setting failed to find a correlation between drug concentrations and clinical decisions [Kozer et al., 2003].
When to Obtain Drug Concentrations Although enthusiasm for routine monitoring of drug concentrations has moderated, this assistance from the laboratory often is helpful in clinical management. Laboratory results are easiest to interpret when the specimen is obtained before a dose once the drug is at steady state. We agree with the published guidelines with regard to specific clinical situations in which determination of drug concentration is useful (Box 49-1) [Glauser and Pippenger, 2000].
1122
Epilepsy / 49
BOX 49-1 CLINICAL INDICATIONS FOR OBTAINING ANTIEPILEPTIC DRUG (AED) CONCENTRATIONS • • • •
Establishing baseline effective concentration Change in dosage Addition or elimination of another AED Evaluation of lack of efficacy (noncompliance or fast metabolizer) • Evaluation of toxicity (excessive dose, drug interaction, slow metabolizer, renal or liver failure) • Evaluation of loss of efficacy (compliance, drug interaction, change in formulation, pregnancy) • Estimation of the “room to move” Modified from Glauser TA, Pippenger CE. Controversies in blood-level monitoring: Reexamining its role in the treatment of epilepsy. Epilepsia 2000;41 (Suppl 8):S6.
It is useful to determine the optimal drug concentration at steady state for the individual patient when seizure control is obtained. Likewise, it can be helpful to demonstrate concentrations associated with adverse effects for a specific patient. Generally, levels should be measured after changes in dosage or changes in co-medication. Obviously, measurement of drug concentrations is essential in most cases to determine if poor seizure control is the result of lack of compliance.
What to Measure Total drug concentrations generally are measured; however, it also is possible to determine levels of free or unbound drug, as well as of metabolites of the administered drug. Free drug concentrations correlate best with clinical effect and toxicity; however, they are more expensive and difficult to obtain. In most cases, the ratio of free to bound drug is relatively constant for a particular patient; therefore, total drug concentrations usually are adequate. In certain instances, however, particularly with critically ill patients under intensive care, determination of free drug levels, especially for phenytoin and valproate, is essential. In such patients, typically many drugs are administered, increasing the likelihood that antiepileptic drugs will be displaced from protein-binding sites. The percentage of unbound valproate increases with higher drug concentrations and with comedication [Cloyd et al., 1992] or when valproic acid is rapidly administered [Birnbaum et al., 2003]. When the bound fraction is doubled, the valproic acid free fraction may be eight times higher [Fenichel, 1986]. Occasionally, measurement of antiepileptic drug metabolites is useful. With several antiepileptic drugs, metabolites are clinically active and contribute to both response and toxicity. Phenobarbital is an active metabolite present during primidone therapy. Carbamazepine-10,11-epoxide is a derivative of carbamazepine and contributes to toxicity [Schoeman et al., 1984]. Oxcarbazepine is therapeutically monitored by measuring its primary metabolite, MHD [Lloyd et al., 1994].
Laboratory Tests Other than Determination of Drug Concentrations In an effort to identify patients in whom serious or potentially life-threatening adverse effects may develop, obtain-
ing complete blood counts and chemistry profiles at routine intervals has become common practice. The cost for this routine monitoring can exceed the costs of medication [Hart and Easton, 1982]. Moreover, controversy is ongoing regarding whether routine laboratory monitoring can actually identify patients as risk for serious reactions or can identify significant adverse events better than clinical monitoring. Identification of life-threatening reactions is rarely made by routine laboratory screening of asymptomatic children [Camfield et al., 1986]. Fulminate or irreversible hepatic failure during valproate therapy is not reliably predicted by laboratory monitoring [Willmore et al., 1991]. Many clinicians, therefore, believe that routine laboratory screening of asymptomatic patients is of little value [Camfield et al., 1989; Pellock and Willmore, 1991]. Perhaps a reasonable compromise would be to obtain complete blood counts and chemistry profiles before, and once after, initiation of antiepileptic drug therapy [Harden, 2000]. Testing for inborn errors of metabolism is often performed before administering valproic acid in very young children.
ADVERSE DRUG REACTIONS TO ANTIEPILEPTICS Adverse drug reactions are defined by the World Health Organization as “any response to a drug that is noxious or unintended, and which occurs at doses used in man for prophylaxis, diagnosis, or therapy” [Venulet and ten Ham, 1996]. The most frequent adverse drug reactions are dose related, mild, and reversible. Less frequently observed but potentially more serious are the idiosyncratic adverse reactions, which generally are not related to dosage.
Central Nervous System Adverse Reactions The CNS adverse reaction profile for children is similar to that for adults. Most of the older antiepileptic drugs— phenytoin, phenobarbital, primidone, carbamazepine, and valproate—and their active metabolites have similar side effect profiles, comprising cognitive impairment, sedation, dizziness, diplopia, ataxia, headaches, and effects on somnolence. The effects of antiepileptic drugs on cognitive function generally are concentration (and dose) dependent. Drug therapy is known to contribute to cognitive deficits, especially treatment with multiple drugs [Thompson and Trimble, 1982]. Removal of antiepileptic drugs frequently results in improved cognitive function and motor skills [Duncan et al., 1990]. It is important to recognize that reaction times, disordered attention, and impulsivity differ even in untreated children with epilepsy from those in control subjects. The differences in attention and reaction time, however, are small between children with mild versus severe seizure disorders [Mitchell et al., 1992]. Side effects frequently occur in children who are given phenobarbital. Phenobarbital has been associated with a significant depression of cognitive function when it is used for treatment of febrile seizures in children. In a randomized, placebo-controlled prospective study, children had lower mean intelligence quotient (IQ) scores both during and 6 months after stopping therapy with phenobarbital [Farwell et al., 1990]. Clinical tolerance does develop to some degree; however, an unacceptably high frequency of adverse effects from phenobarbital commonly is observed in children
Conway, Kriel, and Birnbaum / Antiepileptic Drug Therapy in Children
[Farwell et al., 1990; Wolf and Forsythe, 1978]. The adverse effects are reminiscent of complaints present in attention deficit disorders and include overactivity, aggressiveness, inattention, and irritability. The behavioral disorders are observed in 20% to 50% of children receiving phenobarbital for febrile seizures and result in discontinuation of therapy in 20% to 30% of children [Herranz et al., 1984]. The existence of preexisting behavior problems, especially hyperactivity, is strongly predictive of adverse reactions during phenobarbital therapy. In a study of children receiving phenobarbital for febrile seizures, 80% of those with abnormal behavior before drug therapy reported aggravation of preexisting hyperactive behavior with phenobarbital versus only 20% for children with normal preseizure behavior [Wolf and Forsythe, 1978]. In some cases, these adverse effects may resolve with continuation or with a lower dose of phenobarbital; however, discontinuation of therapy or alternative medication should be considered. The newer antiepileptic drugs—gabapentin, felbamate, topiramate, lamotrigine, tiagabine, oxcarbazepine, levetiracetam, vigabatrin, and zonisamide—are thought to have fewer and less severe adverse effects; however, their adverse CNS effects are similar to those of the older antiepileptic drugs. Although gabapentin has a good safety profile and seems well tolerated in adults, significant behavioral side effects are observed in some children. In a nonblinded, uncontrolled series, adverse behavioral effects were reported in 47% of children given gabapentin for add-on therapy; however, only 12% of children were withdrawn from gabapentin because of these problems [Khurana et al., 1996]. In other reports, aggression, hyperactivity, temper tantrums, and increased oppositional behavior developed in 12 children taking the drug [Lee et al., 1996; Tallian et al., 1996; Wolf et al., 1996]. Most, but not all, of these children had preexisting cognitive dysfunction such as mental retardation, autistic features, or behavioral difficulties. The adverse cognitive changes resolved with discontinuation of gabapentin; if administration of the drug was resumed, the adverse cognitive changes tended to recur. In one 6-year-old female, the drug was clinically effective in controlling seizures as monotherapy and was well tolerated for 6 months before the aggressiveness developed [Tallian et al., 1996]. In limited pediatric trials, 36% of children taking tiagabine have experienced treatment-emergent adverse effects, most commonly somnolence [Gustavson et al., 1997]. In approximately 15% of children, decreased functioning in school, aggression, and other cognitive changes occurred within the first 4 months of initiation of topiramate therapy [Gerber et al., 2000]. A previous history of behavioral changes and concurrent lamotrigine therapy were associated factors. CNS-related adverse effects from topiramate tend to decrease over time [Ritter et al., 2000]. Of greater concern are reports of the development of major depression, schizophrenic-like reactions, and organic psychoses in adults taking vigabatrin (Ferrie et al., 1996; Ring et al., 1993]. A reversible acute psychosis has been reported in a child taking vigabatrin [Martinez et al., 1995]. Development of hyperkinesia, somnolence, and insomnia in children taking vigabatrin has been reported by a number of investigators [Aicardi et al., 1996; Bernardina et al., 1995; Dulac et al., 1991]. Generally, these effects have not led to
1123
discontinuation of the drug. Although placebo-controlled trials have been conducted in children, statistical analysis of adverse effects was not done.
Gastrointestinal Effects Weight Gain A survey in children and adolescents taking valproic acid found the most common side effects to be weight gain; however, for many patients, the weight gain was “beneficial.” The incidence of unwanted weight gain was 26% in adults and 15% in children and adolescents. An increase in weight was observed more than twice as frequently in females [Clark et al., 1980; Wirrell, 2003]. Weight increase was independent of dose [Covanis et al., 1982]. Weight gain also was reported in children during carbamazepine [Herranz et al., 1988; Hogan et al., 2000] and vigabatrin [Bernardina et al., 1995; Dulac et al., 1991] therapy. Weight gain has been reported in adults taking gabapentin [DeToledo et al., 1997].
Weight Loss Sustained weight loss was reported in children on maintenance topiramate therapy [Reiter et al., 2004]. Seventyfive percent of children and adults during clinical research trials reported a loss of appetite and decrease in body weight while taking felbamate [Bergen et al., 1995]. Zonisamide is being studied as a possible medication to decrease weight in obese adult patients in whom a mean weight loss of 10% has been reported [Gadde et al., 2003].
Gastric Irritation Signs of gastric irritation with heartburn and indigestion are seen with use of some antiepileptic drugs. Gastric irritation during valproic acid therapy can be reduced with administration of lower doses or by taking medication with food [Dean and Penry, 1992]. Use of enteric-coated preparations of valproic acid will enable most patients who did not tolerate valproic acid because of gastrointestinal symptoms (nausea/vomiting, eructation, heartburn) to resume valproic acid therapy [Clark et al., 1980; Wilder et al., 1983]. Aggressive medical intervention with antacids and H2 receptor antagonists (other than cimetidine) has been helpful for some children with clinical signs of gastritis, allowing valproic acid therapy to continue [Marks et al., 1988]. Approximately 20% of patients receiving ethosuximide will demonstrate dose-related adverse effects, primarily gastric distress, vomiting, hiccups, and anorexia [Sherwin, 1983]. Gastrointestinal disturbances also are encountered in 14% of patients taking carbamazepine, with symptoms of nausea, vomiting, anorexia, and constipation [Herranz et al., 1988]. Nausea and vomiting commonly are observed with felbamate [Dodson, 1984; Theodore et al., 1991].
Gingival Hyperplasia Gingival hyperplasia occurs in 10% to 20% of persons treated with phenytoin and is somewhat more frequent in
1124
Epilepsy / 49
young persons. It is observed more frequently in persons with higher dosages, often appears 2 to 3 months after beginning therapy, and reaches its maximum severity in 12 to 18 months [Babcock, 1965; Little et al., 1975]. Gingival hyperplasia generally resolves within 2 to 5 months after discontinuation or a reduction in medication [Little et al., 1975]. A vigorous program of good oral hygiene started before and continued during phenytoin therapy can be effective in minimizing gingival enlargement [Angelopoulos, 1975; Modeer and Dahloff, 1987; Pihlstrom et al., 1980]. Drugs other than antiepileptic drugs, including nifedipine and cyclosporine, have been associated with the development of gingival hyperplasia [Butler et al., 1987].
Increased Seizures Some patients, especially those with generalized or absence seizures, may experience an increase in seizure activity when carbamazepine is added [Horn et al., 1986; Perucca et al., 1998; Snead and Hosey, 1985]. Vigabatrin also has been reported to increase seizure activity and even lead to status epilepticus [DeKrom et al., 1995]. Aggravation of seizures occurred in 3% of children with generalized seizures, most often in those with nonprogressive myoclonic epilepsy, and was extremely unusual in children with partial epilepsies and infantile spasms [Lortie et al., 1997]. Oxcarbazepine has been reported to increase myoclonic jerks and absence seizures [Gelisse et al., 2004].
Osteomalacia Osteomalacia (rickets) occasionally is seen in patients taking antiepileptic drugs. In a survey of institutionalized patients, 52 of 144 mentally retarded patients ranging in age from 3 to 26 years who were on antiepileptic drug therapy for at least 2 years had elevations of serum alkaline phosphatase levels greater than 2 standard deviations above normal. Most patients were taking phenytoin or phenobarbital [Hunt et al., 1986]. The cause of osteomalacia during antiepileptic drug therapy appears to be multifactorial [Farhat et al., 2002]. Many antiepileptic drugs presumably enhance hepatic conversion of 25-hydroxyvitamin D to biologically inactive metabolites. Clinically significant rickets seldom develops in ambulatory children on antiepileptic drug therapy, or in institutionalized children who are not taking medication. On the other hand, clinically overt rickets was observed in 10% of institutionalized children on phenobarbital and/or phenytoin. In these patients, sunlight was more important for the maintenance of serum 25-hydroxyvitamin D than were supplements of vitamin D [Morijiri and Sato, 1981]. Current evidence indicates that antiepileptic drugs decrease bone mineral density in adults. In adults, correlation with 25-hydroxyvitamin D levels was poor [Farhat et al., 2002]. In children, no correlation was observed between duration of antiepileptic drug therapy and 25-hydroxyvitamin D levels. Bone mineral density measurements tended to be lower in patients on older antiepileptic drugs than in patients on newer antiepileptic drugs but were lower in all patients on any antiepileptic drug than in the control population. It was previously thought that older antiepileptic drugs resulted in induction of vitamin D metabolism, resulting in
decreased bone mineral density; however, the lack of correlation between vitamin D levels and bone mineral density suggests that other mechanisms are operative. Some authors recommend routine bone mineral density monitoring for patients on chronic antiepileptic drug therapy [Farhat et al., 2002]. Consensus is lacking on treatment of patients who have low bone mineral density secondary to antiepileptic drug therapy.
Tremor and Movement Disorders A benign essential type of tremor has been observed with use of valproic acid, beginning within 1 month of initiating therapy. It is dose dependent, occurring in some patients with blood valproic acid levels greater than 40 μg/mL. Reduction of tremor may occur with reduction of dose [Karas et al., 1982]. Tremor also has been seen with use of lamotrigine and gabapentin [Schmidt and Kramer, 1994]. Oculogyric crises and choreoathetotic movements have developed in several adults while taking gabapentin [Buetefisch et al., 1996; Reeves et al., 1996].
Other Effects Hair changes have been associated with antiepileptic drug treatment. Hair changes (thinning or wavy hair) are seen in 12% of children during valproic acid therapy [Clark et al., 1980]. Additional dose-related adverse effects of phenytoin include hirsutism, coarse facial features, and acne, especially in children and teenagers. Pancreatitis has been associated with valproate therapy [Coulter and Allen, 1980; Grauso-Eby et al., 2003; Wyllie et al., 1984]. Visual field changes, which may be irreversible, may occur with vigabatrin treatment [Krauss et al., 1998]. Topiramate has been reported to cause acute myopia and secondary angle closure glaucoma. Patients present with decreased visual acuity and ocular pain. In a majority of cases, immediate discontinuation of topiramate results in a resolution of symptoms [Sankar et al., 2001; Thambi et al., 2002]. Hyponatremia occasionally is encountered in patients taking carbamazepine and oxcarbazepine [Borusiak et al., 1998; Holtmann et al., 2002; Koivikko and Valikangas, 1983]. Hyperthermia and oligohydrosis has been reported in several children taking topiramate and zonisamide. Clinical signs included fever, decreased sweating, and exercise intolerance, which resolved in a majority of cases when topiramate or zonisamide was discontinued [Arcas et al., 2001; Knudsen et al., 2003]. Topiramate and zonisamide may cause nephrolithiasis. The risk is increased with topiramate or zonisamide treatment and the ketogenic diet [Kossoff et al., 2002].
Anticonvulsant Hypersensitivity Syndrome in Children Clinical Features The hypersensitivity syndrome is characterized by rash, fever, and malaise, generally occurring within the first several months of therapy. Certain types of rash may be particularly alarming, such as those of Stevens-Johnson syndrome or toxic epidermal necrolysis. Often hepatic involvement is part of the syndrome, and the liver is the most frequently involved inter-
Conway, Kriel, and Birnbaum / Antiepileptic Drug Therapy in Children
nal organ. Affected children may present with hepatomegaly and elevations in serum transaminase levels. The involvement may progress to hepatic necrosis. Other systems may be involved, including kidney, lungs, bone marrow, and the lymphatic system [Handfield-Jones et al., 1993].
Pathogenesis Although the mechanism of the hypersensitivity syndrome is not completely understood, current evidence implicates toxic metabolites [Glauser, 2000; Verrotti et al., 2002]. The aromatic antiepileptic drugs (phenobarbital, phenytoin, carbamazepine, oxcarbazepine), lamotrigine, and felbamate have been more frequently implicated in causing this syndrome. Presumably, accumulation of toxic metabolites, such as reactive aromatic epoxide intermediates, precipitate the syndrome [Glauser, 2000].
Prevention Routine laboratory monitoring (i.e., with complete blood counts or liver function tests) will not prospectively identify which patients are at high risk for the development of an acute hypersensitivity reaction. Nevertheless, research has allowed practitioners to identify factors that place some patients at high risk. Clinical profiles that identify patients at high risk for hypersensitivity reactions differ for specific antiepileptic drugs (valproic acid, felbamate, and lamotrigine) (Table 49-10). When one of these drugs is being considered for a patient at high risk, the clinician should proceed with caution. Alternative therapy, if possible, should be considered. Additional laboratory tests to screen for inborn errors of metabolism may be indicated when use of valproic acid is under consideration in children younger than 2 years of age. Families need to be advised that the child is in a high-risk category and counseled on the early recognition of the syndrome. Although the identification of a high-risk clinical profile is the most inexpensive practical way available to reduce the TABLE 49-10 Clinical Profiles for Patients at High Risk for Idiosyncratic Reactions to Valproic Acid, Lamotrigine, and Felbamate
1125
risk of hypersensitivity syndrome, various biomarkers also have been identified [Glauser, 2000]. These biomarkers may indicate that some patients have genetic susceptibility to the accumulation of toxic metabolites due to deficient detoxification pathways. The biomarkers that have been investigated include deficient epoxide hydrolase activity and deficiencies in free radical-scavenging enzyme activity. Unfortunately, assays for these markers are not routinely available at this time.
Managing Adverse Effects The clinician and the patient are faced with adverse effects approximately 30% of the time when antiepileptic medication is used, especially during initiation of therapy. In many instances, this rate is acceptable, especially when the patient and the physician mutually agree on which problems are most important to avoid. When no urgency exists, many adverse effects can be avoided during initiation of therapy by gradually increasing doses. In general, management of adverse effects depends on the problem. Most adverse effects are concentration dependent and are less prominent at lower doses and blood concentrations. Seizure control may or may not be maintained at the lower dose; if not, the clinician and the patient need to consider whether a compromise is acceptable with regard to either increased seizures or increased adverse effects, or if alternative medication should be considered. At times, toxicity is encountered only with high drug concentrations and is seen only at peak times; for these patients, it may be possible to avoid toxicity by more frequent and lower doses or by the use of extended release formulations. Gastric irritation generally is dose dependent and may be managed in several ways: The amount of drug can be reduced, the effective dose to the gastric mucosa can be lowered by use of enteric-coated formulations, or the patient can be protected by use of H2 receptor antagonists. Idiosyncratic reactions pose another problem. Asymptomatic elevations of liver enzymes in general do not mandate discontinuation of therapy if not in excess of two to three times normal values. On the other hand, StevensJohnson syndrome and toxic epidermal necrolysis, clinically symptomatic hepatotoxicity, pancreatitis, and most rashes are indications for immediate cessation of the responsible medication. If the rash was mild, however, and especially if the patient had an otherwise favorable clinical response to the drug, a cautious rechallenge might be considered. Successful resumption of therapy has been reported in a number of patients, especially with valproic acid after that drug was discontinued, when a more gradual dose escalation was used [Schlumberger et al., 1994; Tavernor et al., 1995].
SELECTION OF DRUGS FOR INITIATION OF ANTIEPILEPTIC DRUG THERAPY
From Glauser TA. Idiosyncratic reactions: New methods of identifying high-risk patients. Epilepsia 2000;41 (Suppl 8):S16.
The selection of a specific drug for the treatment of epilepsy is based primarily on the criteria of therapeutic efficacy expected for the patient and seizure type. Certain epileptic syndromes require specific therapy. For most patients and seizure types, however, efficacy differences are minimal, and the selection of the initial drug for antiepileptic therapy is guided equally by a consideration of potential adverse
1126
Epilepsy / 49
effects. Although highly effective, phenytoin is rarely a drug of first choice in children because of a higher incidence of dysmorphic effects. In children, especially those with preexisting tendencies for attention deficit disorders, an unacceptable incidence of behavioral problems, as well as of cognitive dysfunction, has been noted with barbiturate therapy. The principles to be used during initiation and selection of antiepileptic drug therapy in children have been summarized in the literature [Crumrine, 2002; Fenichel, 1986].
DISCONTINUATION OF ANTIEPILEPTIC DRUG THERAPY The decision to discontinue antiepileptic drug therapy often is as challenging as the decision to initiate and continue long-term drug therapy. Most commonly, the question arises after a patient has done well and has become seizure free for some substantial period. At other times, the question arises because of chronic noncompliance, or because no therapy has had a measurable effect on seizure control. Many factors are considered in making these decisions, including the length of the seizure-free interval, drug history, presence of adverse effects, and the neurologic and epilepsy syndrome diagnosis of the patient. Numerous retrospective and prospective investigations are available for review by the clinician who is facing this difficult decision. Ultimately, the decision to withdraw or to continue antiepileptic drug therapy is that of the patient and family, and their perception of acceptable risk of recurrence often differs from that of the treating physician [Gordon et al., 1996].
Benefits of Drug Discontinuation The potential benefits of drug discontinuation are numerous. Most obvious is the immediate reduction in cost to the family and third-party payer with elimination of drug therapy and usually in associated expenses of laboratory tests and physician and clinic charges. In addition, in many patients, the adverse, sometimes previously unrecognized effects of antiepileptic drug therapy are reversed. Patients who have been on phenobarbital, phenytoin, valproate, and topiramate have subtle improvement in various psychometric tasks such as memory, vigilance attention, and visual motor performance [Gallassi et al., 1992; Lee et al., 2003], and in psychomotor speed [Aldenkamp et al., 1993], when therapy was discontinued.
A guideline has been published to assist the physician and the family considering discontinuation of antiepileptic drug therapy. The conclusions were based on a MEDLINE search [Practice Parameter, 1996]. Children who were seizure free for 2 or more years while on antiepileptic drugs, who had a single type of partial or generalized seizure, who had a normal IQ and normal findings on neurologic examination, and a normalized EEG on therapy had a 69% chance of discontinuing antiepileptic drug therapy without seizure recurrence. A similar conclusion was reached by another meta-analysis, in which 75% of “relatively unselected” patients were seizure free 1 year after discontinuation and 71% 2 years after discontinuation of antiepileptic drug therapy [Berg and Shinnar, 1994]. Children with remote symptomatic seizures and those with seizure onset in adolescence (rather than earlier) were at greatest risk of recurrence. Although relapse was observed in every study, in one prospective series, relapse rates were slightly higher in children who had epileptiform activity on the last EEG before antiepileptic drug discontinuation [Andersson et al., 1997]. The authors concluded that the persistence of 3-Hz spikewave activity during therapy also was an unfavorable prognostic sign. Children more frequently had recurrences of seizures when antiepileptic drugs were stopped after 1 year versus 3 years of therapy. In another randomized, prospective study of 6 versus 12 months of antiepileptic drug therapy in children who became seizure free on antiepileptic drug therapy, no difference between relapse rates was observed [Peters et al., 1998]. That report again presented the predictive variables for relapse, which were partial epilepsy, a remote symptomatic etiology, an older age at onset (12 years and older), and an epileptiform EEG during therapy. Families should be encouraged to consider withdrawing antiepileptic drugs once children have become free of seizures for 1 year or longer while on antiepileptic drug therapy. Children whose EEGs have become normal have a somewhat better chance of successful withdrawal of therapy. We particularly encourage an attempt to stop therapy when appropriate in teenagers before they leave home or go to college. Finally, for some patients, withdrawal of antiepileptic drugs is rarely successful—for example, those with abnormalities on neurologic examination or with certain seizure syndromes as juvenile myoclonic epilepsy, LennoxGastaut syndrome, or infantile spasms [Peters et al., 1998; Shinnar et al., 1994]. REFERENCES
Risks of Drug Discontinuation The obvious risk of stopping antiepileptic drug therapy is the recurrence of seizures. In most cases, seizure control can be regained with resumption of the previous drug therapy. We agree with other investigators who have found that the response to therapy after a relapse generally is rapid and satisfactory [Arts et al., 1988]. Chadwick and colleagues observed that approximately 90% of patients who experience seizures after antiepileptic drug discontinuation have a 2-year remission after therapy is resumed [Chadwick et al., 1996]. This finding is in agreement with our experience that control was usually but not always regained despite increasing doses of a previously successful drug regimen.
Aicardi J, Mumford JP, Dumas C, et al. Vigabatrin as initial therapy for infantile spasms: A European retrospective survey. Epilepsia 1996;37:638. Albright AL, Barron WB, Fasick P, et al. Continuous intrathecal baclofen infusion for spasticity of cerebral origin. JAMA 1993;270:2475. Aldenkamp AP, Alpherts WCJ, Blennow G, et al. Withdrawal of antiepileptic medication in children—effects on cognitive function: The Multicenter Holmfrid Study. Neurology 1993;43:41. Andersson T, Braathen G, Persson A, et al. A comparison between one and three years of treatment in uncomplicated childhood epilepsy: A prospective study. II. The EEG as predictor of outcome after withdrawal of treatment. Epilepsia 1997;38:225. Angelopoulos A. A clinicopathological review: Diphenylhydantoin gingival hyperplasia: Etiology, pathogenesis, differential diagnosis and treatment. J Can Dent Assoc 1975;41: 275-277.
Conway, Kriel, and Birnbaum / Antiepileptic Drug Therapy in Children Arcas J, Ferrer T, Roche MC, et al. Hypohidrosis related to the administration of topiramate to children. Epilepsia 2001;42:1363. Arts WFM, Visser LH, Loonen MCB, et al. Follow-up of 146 children with epilepsy after withdrawal of antiepileptic therapy. Epilepsia 1988;29:244. Babcock JR. Incidence of gingival hyperplasia associated with dilantin therapy in a hospital population. J Am Dent Assoc 1965;71:1447. Banfield CR, Zhu GR, Jen JF, et al. The effect of age on the apparent clearance of felbamate: A retrospective analysis using nonlinear mixed-effects modeling. Ther Drug Monit 1996;18:19. Battino D, Buti D, Croci D, et al. Lamotrigine in resistant childhood epilepsy. Neuropediatrics 1993;24:332. Battino D, Croci D, Granata T, et al. Single-dose pharmacokinetics of lamotrigine in children: Influence of age and antiepileptic comedication. Ther Drug Monit 2001;23:217. Battino D, Estienne M, Avanzini G, et al. Clinical pharmacokinetics of antiepileptic drugs in paediatric patients. Part II. Phenytoin, carbamazepine, sulthiame, lamotrigine, vigabatrin, oxcarbazepine, and felbamate. Clin Pharmacokinet 1995;29:341. Ben-Menachem E. Potential antiepileptic drugs: Topiramate. In: Levy RH, Mattson RH, Meldrum BS, eds. Antiepileptic drugs. New York: Raven Press, 1995a;1063. Ben-Menachem E. Vigabatrin: Chemistry, absorption, distribution, and elimination. In: Levy RH, Mattson RH, Meldrum BS, eds. Antiepileptic drugs. New York: Raven Press, 1995b;915. Ben-Menachem E. Pregabalin pharmacology and its relevance to clinical practice. Epilepsia 2004;45 (Suppl 60):13. Berg AT, Shinnar S. Relapse following discontinuation of antiepileptic drugs: A meta-analysis. Neurology 1994;44:601. Bergen DC, Ristanovic RK, Waicosky K, et al. Weight loss in patients taking felbamate. Clin Neuropharmacol 1995;18:23. Bernardina BD, Fontana E, Vigevano F, et al. Efficacy and tolerability of vigabatrin in children with refractory partial seizures: A single-blind dose-increasing study. Epilepsia 1995;36:687. Birnbaum AK, Kriel RL, Burkhardt RT, et al. Rectal absorption of lamotrigine compressed tablets. Epilepsia 2000;41:850. Birnbaum AK, Kriel RL, Im Y, et al. Relative bioavailability of lamotrigine chewable dispersible tablets administered rectally. Pharmacotherapy 2001;21:158. Birnbaum AK, Kriel RL, Norberg SK, et al. Rapid infusion of sodium valproate in acutely ill children. Pediatr Neurol 2003;28:300. Borusiak P, Korn-Merker E, Holert N, et al. Hyponatremia induced by oxcarbazepine in children. Epilepsy Res 1998;30:241. Brockbrader H, Hunt T, Strand J, et al. Pregabalin pharmacokinetics and safety in healthy volunteers: Results from two phase I studies. Neurology 2000;54 (Suppl 3):421. Buetefisch CM, Gutierrez A, Gutmann L. Choreoathetotic movements: A possible side effect of gabapentin. Neurology 1996;46:851. Burstein AH, Modica R, Hatton M, et al. Pharmacokinetics and pharmacodynamics of midazolam after intranasal administration. J Clin Pharmacol 1997;37:711. Butler RT, Kalkwarf KL, Kaldahl WB, et al. Drug-induced gingival hyperplasia: Phenytoin, cyclosporine, and nifedipine. J Am Can Assoc 1987;114:56. Cacek AT. Review of alterations in oral phenytoin bioavailability associated with formulation, antacids, and food. Ther Drug Monit 1986;8:166. Camfield C, Camfield P, Smith E, Tibbles JA. Asymptomatic children with epilepsy: Little benefit from screening for anticonvulsant-induced liver, blood, or renal damage. Neurology 1986;36:838. Camfield P, Camfield C, Dooley J, et al. Routine screening of blood and urine for severe anticonvulsant reactions in asymptomatic patients is of doubtful value. Can J Neurol Sci 1989;16:361. Capparelli EV. Pharmacokinetic considerations in the adolescent: non-cytochrome P450 metabolic pathways. J Adolesc Health 1994;15:641. Chadwick D, Taylor J, Johnson R, et al. Outcomes after seizure recurrence in people with well-controlled epilepsy and the factors that influence it. Epilepsia 1996;37:1043. Challier JC, Rey E, Binten T, et al. Passage of S(+) and R(-) g-vinylGABA across the human isolated perfused placenta. Br J Clin Pharmacol 1992;34:139. Chen C, Casale EJ, Duncan B, et al. Pharmacokinetics of lamotrigine in children in the absence of other antiepileptic drugs. Pharmacotherapy 1999;19:437. Clark JE, Covanis A, Gupta AK, et al. Unwanted effects of sodium valproate in children and adolescents. In: Parsonage MJ, Caldwell
1127
ADS, eds.The place of sodium valproate in the treatment of epilepsy. London: Academic Press, 1980;30. Cloyd JC. Pharmacokinetic pitfalls of present antiepileptic medications. Epilepsia 1991;32 (Suppl 5):S53. Cloyd JC, Fischer JH, Kriel RL, et al. Valproic acid pharmacokinetics in children IV. Effects of age and antiepileptic drugs on protein binding and intrinsic clearance. Clin Pharmacol Ther 1993;53:22. Cloyd JC, Kriel RL, Fischer JH, et al. Pharmacokinetics of valproic acid in children. I. Multiple antiepileptic drug therapy. Neurology 1983;33:185. Cloyd JC, Kriel RL, Fischer JH, et al. Valproic acid pharmacokinetics in children. II. Discontinuation of concomitant antiepileptic drug therapy. Neurology 1985;35:1623. Cloyd JC, Kriel RL, Jones-Saete CM, et al. Comparison of sprinkle versus syrup formulations of valproate for bioavailability, tolerance, and preference. J Pediatr 1992;120:634. Conway JM, Birnbaum AK, Kriel RL, et al. Relative bioavailability of topiramate administered rectally. Epilepsy Res 2003;54:91. Coulter DL, Allen RJ. Pancreatitis associated with valproic acid therapy for epilepsy. Ann Neurol 1980;7:92. Covanis A, Gupta AK, Jeavons PM, et al. Sodium valproate: Monotherapy and polytherapy. Epilepsia 1982;23: 693-720. Crumrine PK. Antiepileptic drug selection in pediatric epilepsy. J Child Neurol 2002;17 (Suppl 2):S2–S8. Curatolo P, Bruni O, Cusmai R, et al. Use of erythromycin to inhibit carbamazepine metabolism in children with partial complex seizures. Brain Dev 1988;10:206. Dean JC, Penry JK. Valproate. New York: Marcel Dekker, 1992. Degen PH, Flesch G, Cardot JM, et al. The influence of food on the disposition of the antiepileptic oxcarbazepine and its major metabolites in healthy volunteers. Biopharm Drug Dispos 1994;15:519. de Krom MC, Verduin N, Visser E, et al. Status epilepticus during vigabatrin treatment: A report of three cases. Seizure 1995;4:159. DeToledo JC, Toledo C, DeCerce J, Ramsay RE. Changes in body weight with chronic, high-dose gabapentin therapy. Ther Drug Monit 1997;19:394. Devinsky O, Vazquez B, Luciano D, et al. New antiepileptic drugs for children: Felbamate, gabapentin, lamotrigine, and vigabatrin. J Child Neurol 1994;9 (Suppl 1):S33. Dodson WE. Antiepileptic drug utilization in pediatric patients. Epilepsia 1984;25 (Suppl 2):S132. Donn KH, Drissel DA, Quon CY, et al. Systemic availability and pharmacokinetics of phenytoin after intramuscular ACC-9653, a phenytoin prodrug. Epilepsia 1987;28:S87 (abstract). Doose DR, Gisclon LG, Stellar SM, et al. The effect of food on the bioavailability of topiramate from 100- and 400-mg tablets in healthy male subjects. Epilepsia 1992;33 (Suppl 3):105. Dulac O, Chiron C, Luna D, et al. Vigabatrin in childhood epilepsy. J Child Neurology 1991;6 (Suppl 2):S30. Duncan JS, Shorvon SD, Trimble MR, et al. Effects of removal of phenytoin, carbamazepine, and valproate on cognitive function. Epilepsia 1990;31:584. Dutta S, Reed RC, Cavanaugh JH, et al. Absolute bioavailability and absorption characteristics of divalproex sodium extended-release tablets in healthy volunteers. J Clin Pharmacol 2004;44:737. Dutta S, Zhang Y. Bioavailability of divalproex extended-release formulation relative to the divalproex delayed-release formulation. Biopharm Drug Dispos 2004;25:345. Easterling DE, Zakzewshi T, Moyer MD, et al. Plasma pharmacokinetics of topiramate, a new anticonvulsant in humans. Epilepsia 1988;29: 662. Eichelbaum M, Ekbom K, Bertilsson L, let al. Plasma kinetics of carbamazepine and its epoxide metabolite in man after single and multiple doses. Eur J Clin Pharmacol 1975;8:337. Elwes RD, Binnie CD. Clinical pharmacokinetics of newer antiepileptic drugs. Drug Dispos 1996;30:403. Faigle JW, Feldmann KF. Pharmacokinetic data of carbamazepine and its major metabolites in man. In: Schneider H, Janz D, Gardner-Thorpe C, et al, eds. Clinical pharmacology of antiepileptic drugs. Berlin: Springer-Verlag, 1975;159. Farhat G, Yamout B, Mikati MA, et al. Effect of antiepileptic drugs on bone density in ambulatory patients. Neurology 2002;58:1348. Farwell JR, Lee YJ, Hirtz DG, et al. Phenobarbital for febrile seizures— effects on intelligence and seizure recurrence. N Engl J Med 1990;322:364–369. Feldmann KF, Brechbuhler S, Faigle JS, et al. Pharmacokinetics and metabolism of GP 47 680, a compound related to CBZ in animals and
1128
Epilepsy / 49
man. In: Meinardi H, Rowan AJ, eds. Advances in epileptology. Amsterdam/Lisse: Swets and Zeitlinger, 1977;290. Feldmann KF, Dorhofer G, Faigle JW, et al. Pharmacokinetics and metabolism of GP 47 799, the main human metabolite of oxcarbazepine (GP 47 680) in animals and healthy volunteers. In: Dam M, Gram L, Penry JK, eds. Advances in epileptology: XIIth Epilepsy International Symposium. New York: Raven Press, 1981;89. Fenichel GM. Anticonvulsant therapy in children. Int Pediatr 1986;1:231. Ferrie CD, Robinson RO, Panayiotopoulos CP, et al. Psychotic and severe behavioral reactions with vigabatrin: A review. Acta Neurol Scand 1996;93:1. Finkelstein JW. The effect of developmental changes in adolescence on drug disposition. J Adolesc Health 1994;15:612. Fischer JH, Barr AN, Paloucek FP, et al. The effect of food on the serum concentration profile of enteric coated VPA. Neurology 1988;38:1319. Frisk-Holmberg M, Kerth P, Meyer PH, et al. Effect of food on the absorption of vigabatrin. Br J Clin Pharmacol 1989;27:S23. Froscher W, Engels HG. Tolerance to the anticonvulsant effect of clonazepam: Tolerance to beneficial adverse effects of antiepileptic drugs. New York: Raven Press, 1986. Fuerst RH, Graves NM, Kriel RL, et al. Absorption and safety of rectally administered phenytoin. Eur J Drug Metabol Pharmacokin 1988;13:257. Gadde KM, Franciscy DM, Wagner HR, et al. Zonisamide for weight loss in obese adults: A randomized controlled trial. JAMA 2003;289:1820. Gallassi R, Morreale A, DiSarro R, et al. Cognitive effects of antiepileptic drug discontinuation. Epilepsia 1992;33 (Suppl 6):S41. Garnett WR. Lamotrigine: Pharmacokinetics. J Child Neurol 1997;12 (Suppl 1):S10. Garnett WR, Cloyd JC. Dosage form considerations in the treatment of pediatric epilepsy. In: Dotson WE, Pellock JM, eds. Pediatric epilepsy: Diagnosis and therapy. New York: Demos, 1993:241. Gelisse P, Genton P, Kuate C, et al. Worsening of seizures by oxcarbazepine in juvenile idiopathic generalized epilepsies. Epilepsia 2004;45:1282. Gerber N, Mays DC, Dohn KH, et al. Safety, tolerance and pharmacokinetics of intravenous doses of the phosphate ester of 3-hydroxymethyl-5,5-diphenylhydantoin, a new prodrug of phenytoin. J Clin Pharmacol 1988;28:1023. Gerber PE, Hamiwka L, Connolly MB, et al. Factors associated with behavioral and cognitive abnormalities in children receiving topiramate. Pediatr Neurol 2000;22:200. Glauser TA. Preliminary observations on topiramate in pediatric epilepsies. Epilepsia 1997;38 (Suppl 1):S37. Glauser TA. Idiosyncratic reactions: New methods of identifying high-risk patients. Epilepsia 2000;41 (Suppl 8):S16. Glauser TA, Pippenger CE. Controversies in blood-level monitoring: Reexamining its role in the treatment of epilepsy. Epilepsia 2000;41 (Suppl 8):S6. Goff DA, Spunt AL, Jung D, et al. Absorption characteristics of three phenytoin sodium products after administration of oral loading doses. Clin Pharmacol 1984;3:634. Gordon K, MacSween J, Dooley J, et al. Families are content to discontinue antiepileptic drugs at different risks than their physicians. Epilepsia 1996;37:557. Grauso-Eby NL, Goldfarb O, Feldman-Winter LB, et al. Acute pancreatitis in children from valproic acid: Case series and review. Pediatr Neurol 2003;28:145. Graves NM, Kriel RL. Rectal administration of AEDs in children. Pediatric Neurol 1987;3:321. Graves NM, Kriel RL, Jones-Saete C, et al. Bioavailability of rectally administered lorazepam. Clin Neuropharmacol 1987;6:555. Greenblatt DJ, Ehrenberg BL, Gunderman J, et al. Kinetic and dynamic study of intravenous lorazepam: Comparison with intravenous diazepam. J Pharmacol Exp Ther 1989;250:134. Gustavson LE, Boellner SW, Granneman GR, et al. A single-dose study to define tiagabine pharmacokinetics in pediatric patients with complex partial seizures. Neurology 1997;48:1032. Gustavson LE, Mengel HB. Pharmacokinetics of tiagabine, a gamma-aminobutyric acid-uptake inhibitor, in healthy subjects after single and multiple doses. Epilepsia 1995;36:605. Haegele KD, Schoun J, Alken RG, et al. Determination of the R(-) and S(+)- enantiomers of γ-vinyl-γ-aminobutyric acid in human body fluids by gas chromatography–mass spectrometry. J Chromatogr 1983;274:103. Haig GM, Brockbrader HN, Wesche DL, et al. Single-dose gabapentin pharmacokinetics and safety in healthy infants and children. J Clin Pharmacol 2001;41:507.
Handfield-Jones SE, Jenkins RE, Whittaker SJ, et al. The anticonvulsant hypersensitivity syndrome. Br J Dermatol 1993;129:175. Harden CL. Therapeutic safety monitoring: What to look for and when to look for it. Epilepsia 2000;41 (Suppl 8):S37. Hart RG, Easton JD. Carbamazepine and hematological monitoring. Ann Neurol 1982;11:309. Henriksen O. Specific problems of children with epilepsy. Epilepsia 1988;29 (Suppl):S6. Herranz JL, Armijo JA, Arteaga R. Effectiveness and toxicity of phenobarbital, primidone, and sodium valproate in the prevention of febrile convulsions, controlled by plasma levels. Epilepsia 1984;25 89. Herranz JL, Armijo JA, Arteaga R, et al. Clinical side effects of phenobarbital, primidone, phenytoin, carbamazepine, and valproate during monotherapy in children. Epilepsia 1988;29:794. Hogan RE, Bertrand ME, Deaton RL, et al. Total percentage body weight changes during add-on therapy with tiagabine, carbamazepine and phenytoin. Epilepsy Res 2000;41:23. Hoke, KD, Chi EM, Antony KK, et al. Bioequivalence and relative bioavailability of vigabatrin. Epilepsia 1991;32 (Suppl 3):7. Holtmann M, Krause M, Opp J, et al. Oxcarbazepine-induced hyponatremia and the regulation of serum sodium after replacing carbamazepine with oxcarbazepine in children. Neuropediatrics 2002;33:298. Horn CS, Ater SB, Hurst DL, et al. Carbamazepine-exacerbated epilepsy in children and adolescents. Neurology 1986;2:340. Hunt PA, Wu-Chen ML, Handal NJ, et al. Bone disease induced by anticonvulsant therapy and treatment with calcitriol (1,25-dihydroxyvitamin D3). Am J Dis Child 1986;140:715. Hussey EK, Dukes GE, Messenheimer JA, et al. Evaluation of the pharmacokinetic interaction between diazepam and ACC-9653 (a phenytoin prodrug) in healthy male volunteers. Pharm Res 1990;7:1172. Jamerson BD, Donn KH, Dukes GE, et al. Absolute bioavailability of phenytoin after 3-phosphoryloxymethyl phenytoin disodium (ACC-9653) administration to humans. Epilepsia 1990;31:592. Jannuzzi G, Cian P, Fattore C, et al. A multicenter randomized controlled trial on the clinical impact of therapeutic drug monitoring in patients with newly diagnosed epilepsy. The Italian TDM Study Group in Epilepsy. Epilepsia 2000;41:222. Johannessen SI. Pharmacokinetics and interaction profile of topiramate: Review and comparison with other newer antiepileptic drugs. Epilepsia 1997;38 (Suppl 1):S18. Jung D, Powell JR, Walson P, et al. Effect of dose on phenytoin absorption. Clin Pharmacol Ther 1980;28:479. Jung MF, Lippert B, Metcalf BW, et al. Gamma-vinyl GABA (4-amino-hex-5-enoic acid), a new selective irreversible inhibitor of GABA-T: Effects on brain GABA metabolism in mice. J Neurochem 1977;29:797. Karas BJ, Wilder BJ, Hammond EJ, et al. Valproate tremors. Neurology 1982;32:428. Kauko K, Tammisto P. Comparison of two generically equivalent carbamazepine preparations. Ann Clin Res 1974;11:21. Keppra. Levetiracetam; product information. UCB Pharma, Inc., Smyrna, Ga, 2004. Kerr BM, Levy RH. Carbamazepine-carbamazepine epoxide. In: Levy RH, Mattson R, Meldrum B, eds. Antiepileptic drugs. New York: Raven Press, 1989;505. Khurana DS, Riviello J, Helmers S, et al. Efficacy of gabapentin therapy in children with refractory seizures. J Pediatr 1996;128:829. Klitgaard NA, Kristensen O. Use of saliva for monitoring oxcarbazepine therapy in epileptic patients. Eur J Clin Pharmacol 1986;31:91. Knudsen JF, Thambi LR, Kapcala LP, et al. Oligohydrosis and fever in pediatric patients treated with zonisamide. Pediatr Neurol 2003;28:184. Koella WP. Tolerance: Its various forms and their nature. In: Frey HH, Froscher W, Koella WP, et al, eds. Tolerance to beneficial and adverse effects of antiepileptic drugs. New York: Raven Press, 1986;1. Koivikko MJ, Valikangas SL. Hyponatraemia during carbamazepine therapy in children. Neuropediatrics 1983;14:93. Koren G, Brand N, MacLeod SM, et al. Influence of bioavailability on the calculated Michaelis-Menten parameters of phenytoin in children. Ther Drug Monit 1984;6:11. Kossoff EH, Pyzik PL, Furth SL, et al. Kidney stones, carbonic anhydrase inhibitors, and the ketogenic diet. Epilepsia 2002;43:1168. Kostenbauder HB, Rapp RP, McGovern JP, et al. Bioavailability in single-dose pharmacokinetics of intramuscular phenytoin. Clin Pharmacol Ther 1975;18:449.
Conway, Kriel, and Birnbaum / Antiepileptic Drug Therapy in Children Koudriakova TB, Sirota LA, Rozova GI, et al. Autoinduction and steady-state pharmacokinetics of carbamazepine and its major metabolites. Br J Clin Pharmacol 1992;33:611. Kozer E, Scolnik D, Agamata WM, et al. Utility of antiepileptic drug monitoring in the pediatric emergency department. Ther Drug Monit 2003;25:17. Krauss GL, Johnson MA, Miller NR, et al. Vigabatrin-associated retinal cone system dysfunction: Electroretinogram and ophthalmologic findings. Neurology 1998;50:614. Kriel RL, Birnbaum AK, Cloyd JC, et al. Failure of absorption of gabapentin after rectal administration. Epilepsia 1997;38:1242. Kutt H. Effects of acute and chronic diseases on the disposition of antiepileptic drugs. In: Morselli PL, Pippenger CE, Penry JK, eds. Antiepileptic drug therapy in pediatrics. New York: Raven Press, 1983;293. Kutt H, Penry JK. Usefulness of blood levels of antiepileptic drugs. Arch Neurol 1974;31:283. Kvan L, Johannessen S. Lack of efficacy of phenytoin suppositories in antiepileptic treatment. Acta Neurol Scand 1975;54:103. Lamictal. Lamotrigine: Product information. GlaxoSmithKline, Research Triangle Park, NC, 2004. Larkin JG, Mckee PJW, Forrest G, et al. Lack of enzyme induction with oxcarbazepine (600 mg daily) in healthy subjects. Br J Clin Pharmacol 1991;31:65. Lee DO, Steingard RJ, Cesena M, et al. Behavioral side effects of gabapentin in children. Epilepsia 1996;37:87. Lee S, Sziklas V, Andermann F, et al. The effects of adjunctive topiramate on cognitive function in patients with epilepsy. Epilepsia 2003;44: 339. Leppik IE, Boucher BA, Wilder BJ, et al. Pharmacokinetics and safety of a phenytoin prodrug given IV and IM in patients. Neurology 1990;40:456. Leppik IE, Boucher R, Wilder BJ, et al. Phenytoin prodrug: Preclinical and clinical studies. Epilepsia 1989;30 (Suppl 2):S22. Leppik IE, Cloyd JC, Miller K, et al. Development of tolerance to side effects of primidone. Ther Drug Monit 1984;6:189. Leppik IE, Derivan AT, Homan RW, et al. Double-blind study of lorazepam and diazepam in status epilepticus. JAMA 1983;249:1452. Leppik IE, Fischer JH, Kriel RL, et al. Altered phenytoin clearance with febrile illness. Neurology 1986;36:1367. Linday LA. Developmental changes in renal tubular function. J Adolesc Health 1994;15:648. Lindhardt K, Gizurarson S, Stefansson SB, et al. Electroencephalographic effects and serum concentrations after intranasal and intravenous administration of diazepam to healthy volunteers. Br J Clin Pharmacol 2001;52:521. Little TM, Girgis SS, Masotti RE, et al. Diphenyhydantoin-induced gingival hyperplasia: Its response to changes in drug dosage. Dev Med Child Neurol 1975;17:421. Lloyd P, Flesch G, Dieterle W, et al. Clinical pharmacology and pharmacokinetics of oxcarbazepine. Epilepsia 1994;35 (Suppl 3):S10. Lockard JS, Levy RH. Valproate and paroxysmal cyclicity compared to other anticonvulsants in the monkey model. New York: Raven Press, 1990. Lombroso CT. Intermittent home treatment of status and clusters of seizures. Epilepsia 1989;30 (Suppl 2):S11. Lortie A, Chiron C, Cumas C, et al. Optimizing the indication of vigabatrin in children with refractory epilepsy. J Child Neurol 1997;12:253. Luer MS, Hamani C, Dujovny M, et al. Saturable transport of gabapentin at the blood-brain barrier. Neurol Res 1999;21:559. MacKichan JJ. Influence of protein binding and use of unbound (free) drug concentrations. In: Evans We, Schentag JJ, Jusko WJ, eds. Applied pharmacokinetics: Principles of therapeutic drug monitoring, 3rd ed. Vancouver, WA: Applied Therapeutics, 1992;S1–S48. Marks WA, Morris MP, Bodensteiner JB, et al. Gastritis with valproate therapy. Arch Neurol 1988;45:903. Martinez AC, Baines JPO, Marques MB, et al. Vigabatrin-associated reversible acute psychosis in a child. Ann Pharmacother 1995;29:1115. Mass B, Garnett WR, Pellock JM, et al. A comparative bioavailability study of carbamazepine tablets in a chewable tablet formulation. Ther Drug Monit 1987;9:28. Matsumoto K, Miyazaki H, Fujii T, et al. Binding of sulfonamides to erythrocytes and their components. Chem Pharm Bull (Tokyo) 1989;37:1913. Matsumoto K, Miyazaki H, Fujii T, et al. Absorption, distribution and excretion of 3-(sulfamoyl[14C]methyl)-1,2-benzisoxazole (AD-810) in
1129
rats, dogs and monkeys and of AD-810 in men. Arzneimittelforschung 1983;33:961. Maynard GA, Jones KM, Guidry JR, et al. Phenytoin absorption from tube feedings. Arch Intern Med 1987;147:1821. Mengel H, Gustavson LE, Sørensen HJ, et al. Bioavailability and tolerability of a tiagabine HCl tablet formulation versus capsules and oral solution in normal subjects. Epilepsia 1991;32 (Suppl 3):6. Mengel H, Gustavson LE, Sørensen HJ, et al. Effect of food on the bioavailability of tiagabine HCl. Epilepsia 1991;32 (Suppl 3):6. Meyer MC, Straughn AB. Biopharmaceutical factors that could affect seizure control and toxicity. Am J Hosp Pharm 1993;50(12 Suppl 5):S17. Meyer MC, Straughn AB, Jarvi EJ, et al. The bioequivalence of carbamazepine tablets with a history of clinical failures. Pharm Res 1992;9:1612. Mikati M, Bassett N, Schachter S, et al. Double-blind randomized study comparing brand-name and generic phenytoin monotherapy. Epilepsia 1992;33:359. Mikati MA, Fayad M, Koleilat M, et al. Efficacy, tolerability, and kinetics of lamotrigine in infants. J Pediatr 2002;141:31. Mitchell WG, Zhou Y, Chavez JM, et al. Reaction time, attention, and impulsivity in epilepsy. Pediatr Neurol 1992;8:19. Modeer T, Dahloff G. Development of phenytoin-induced gingival overgrowth in non-institutionalized epileptic children subjected to different plaque control programs. Acta Odontol Scand 1987;45:81. Moolenaar F, Jelsma BH, Wisser J, et al. Manipulation of rectal absorption rate of phenytoin in man. Pharm Weekbl 1981;3:175. Morijiri Y, Sato T. Factors causing rickets in institutionalized handicapped children on anticonvulsant therapy. Arch Dis Child 1981;56:446. Morrow JI, Richens A. Disposition of anticonvulsants in childhood. Clin Pharmacokin 1989;17 (Suppl 1):89. Morselli PL. Development of physiological variables important for drug kinetics. New York: Raven Press, 1983. Nuwer MR, Drowne TR, Dodson WE, et al. Generic substitutions for AEDs. Neurology 1990;40:1647. Østergaard LH, Gram L, Mogens D. Potential antiepileptic drugs: Tiagabine. In: Levy RH, Mattson RH, Meldrum BS, eds. Antiepileptic drugs. New York: Raven Press, 1995;1058. Ouellet D, Brockbrader HN, Wesche DL, et al. Population pharmacokinetics of gabapentin in infants and children. Epilepsy Res 2001;47:229. Painter MJ, Pippenger CE, McDonald H, et al. Phenobarbital and diphenylhydantoin levels in neonates with seizures. J Pediatr 1978;92:315. Patsalos PN. Pharmacokinetic profile of levetiracetam: Toward ideal characteristics. Pharmacol Ther 2000;85:77. Patsalos PN, Elyas AA, Zakrzewska JM, et al. Protein binding of oxcarbazepine and its primary active metabolite, 10-hydroxycarbazepine, in patients with trigeminal neuralgia. Eur J Clin Pharmacol 1990;39:413. Pellock JM. The clinical efficacy of lamotrigine as an antiepileptic drug. Neurology 1994;44 (Suppl 8):S29. Pellock JM, Glauser TA, Bebin EM, et al. Pharmacokinetic study of levetiracetam in children. Epilepsia 2001;42:1574. Pellock JM, Willmore LJ. A rational guide to routine blood monitoring in patients receiving antiepileptic drugs. Neurology 1991;41:961. Penn RD, Savoy SM, Corcos D, et al. Intrathecal baclofen for severe spinal spasticity. N Engl J Med 1989;320:1517. Perhach JL, Shumaker RC. Felbamate: Absorption, distribution, and excretion. In: Levy RH, Mattson RH, Meldrum BS, eds. Antiepileptic drugs. New York: Raven Press, 1995;810. Perucca E, Bialer M. The clinical pharmacokinetics of the newer antiepileptic drugs. Focus on topiramate, zonisamide and tiagabine. Clin Pharmacokinetics 1996;31:29. Perucca E, Dulac O, Shorvon S, et al. Harnessing the clinical potential of antiepileptic drug therapy: Dosage optimization. CNS Drugs 2001;15:609. Perucca E, Gram L, Avanzini G, et al. Antiepileptic drugs as a cause of worsening seizures. Epilepsia 1998;39:5. Peters AC, Brouwer OF, Geerts AT, et al. Randomized prospective study of early discontinuation of antiepileptic drugs in children with epilepsy. Neurology 1998;50:724. Pihlstrom BL, Carlson JF, Smith QT, et al. Prevention of phenytoin associated gingival enlargement—a 15 month longitudinal study. J Peridontol 1980;51:311. Pisani F, Oteri G, Caputo M, et al. Diurnal fluctuations in plasma drug levels at steady-state: Studies with valproic acid and carbamazepine. New York: Raven Press, 1990.
1130
Epilepsy / 49
Porter RJ. General principles—how to use antiepileptic drugs. In: Levy RH, Mattson R, Meldrom B, et al, eds. Antiepileptic drugs. New York: Raven Press, 1989. Practice parameter: A guideline for discontinuing antiepileptic drugs in seizure-free patients—summary statement. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1996;47:600. Pynnonen S, Mantyla R, Iisalo E, et al. Bioavailability of four different pharmaceutical preparations of carbamazepine. Acta Pharmacol Toxicol 1978;43:306. Rane A, Wilson JT. Clinical pharmacokinetics in infants and children. Clin Pharmacokin 1976;1:2. Rawlins MD, Collste P, Bertilsson L, et al. Distribution and elimination kinetics of carbamazepine in man. Eur J Clin Pharmacol 1975;8:91. Reeves AL, So EL, Sharbrough FW, et al. Movement disorders associated with the use of gabapentin. Epilepsia 1996;37:988. Reiter E, Feucht M, Hauser E, et al. Changes in body mass index during long-term topiramate therapy in paediatric epilepsy patients—a retrospective analysis. Seizure 2004;13:491. Rey E, Pons G, Olive G, et al. Vigabatrin: Clinical pharmacokinetics. Clin Pharmacokinet 1992;23:267. Rey E, Pons G, Olive G, et al. Pharmacokinetics of vigabatrin (GVC) in children with measurement of R(-) and S(+) enantiomers. Proceedings of the 18th International Epilepsy Congress, Oct. 17-22, 1989, New Dehli (abstract No. 559). Rey E, Pons G, Richard MO, et al. Pharmacokinetics of the individual enantiomers of vigabatrin (gamma-vinyl GABA) in epileptic children. Br J Clin Pharmacol 1990;30:253. Richens A. Clinical pharmacokinetics of gabapentin. In: Chadwick D, ed. New trends in epilepsy management: The role of gabapentin. London: Royal Society of Medicine Services, 1993;41. Ring HA, Crellin R, Kirker S, et al. Vigabatrin and depression. J Neurol Neurosurg Psychiatry 1993;56:925. Ritter F, Glauser TA, Elterman RD, et al. Effectiveness, tolerability, and safety of topiramate in children with partial-onset seizures. Topiramate YP Study Group. Epilepsia 2000;41 (Suppl 1):S82. Riva R, Albani F, Franzoni E, et al. Valproic acid free fraction in epileptic children under chronic monotherapy. Ther Drug Monit 1983;5:197. Romeo VD, deMeireles J, Sileno AP, et al. Effects of physicochemical properties and other factors on systemic nasal drug delivery. Adv Drug Deliv Rev 1998;29:89. Sankar PS, Pasquale LR, Grosskreutz CL, et al. Uveal effusion and secondary angle-closure glaucoma associated with topiramate use. Arch Ophthalmol 2001;119:1210. Sarkar MA, Garnett WR, Karnes HT, et al. The effect of storage and shaking on the settling properties of phenytoin suspension. Neurology 1989;39:207. Scheepers M, Scheepers B, Clarke M, et al. Is intranasal midazolam an effective rescue medication in adolescents and adults with severe epilepsy? Seizure 2000;9:417. Scheyer RD, Cramer JA. Pharmacokinetics of AEDs. Semin Neurol 1990;10:414. Schlumberger E, Chavez F, Palacios L, et al. Lamotrigine in treatment of 120 children with epilepsy. Epilepsia 1994;35:359. Schmidt D, Haenel F. Therapeutic plasma levels of phenytoin, phenobarbital, and carbamazepine: Individual variation in relation to seizure frequency and type. Neurology 1984;34:1252. Schmidt D, Kramer G. The new anticonvulsant drugs: Implications for avoidance of adverse effects. Drug Safety 1994;11:422. Schoeman JF, Elyas AA, Brett EM, et al. Correlation between plasma carbamazepine-10,11-epoxide concentration and drug side-effects in children with epilepsy. Dev Med Child Neurol 1984;26:756. Schutz H, Feldmann KF, Faigle JW, et al. The metabolism of 14 C-oxcarbazepine in man. Xenobiotica 1986;16:769. Serrano WE, Wilder BJ. Intramuscular administration of diphenylhydantoin: Histologic follow-up. Arch Neurol 1974;31:276. Sherwin AL. How to use ethosuximide. New York: Raven Press, 1983. Shinnar S, Berg AT, Moshe SL, et al. Discontinuing antiepileptic drugs in children with epilepsy: A prospective study. Ann Neurol 1994;35:534. Shumaker RC, Fantel C, Kelton E, et al. Evaluation of the elimination of (14C) felbamate in healthy men. Epilepsia 1990;31:642.
Siegel S. Environmental modulation of tolerance: Evidence from benzodiazepine research: Tolerance to beneficial and adverse effects of antiepileptic drugs. New York: Raven Press, 1986;89. Silanpaa M. Carbamazepine: Pharmacology and clinical uses. Acta Neurol Scand 1981;64 (Suppl):88. Snead OC, Hosey LC. Exacerbation of seizures in children by carbamazepine. N Engl J Med 1985;313:916. Stefan H, Burr W, Fichsel H, et al. Intensive follow-up monitoring in patients with once daily and evening administration of sodium valproate. Epilepsia 1984;25:152. Stewart BH, Kugler AR, Thompson PR, et al. A saturable transport mechanism in the intestinal absorption of gabapentin is the underlying cause of the lack of proportionality between increasing dose and drug levels in plasma. Pharmaceut Res 1993;10:276. Tallian KB, Nahata MC, Lo W, et al. Gabapentin associated with aggressive behavior in pediatric patients with seizures. Epilepsia 1996;37:501. Tavernor SJ, Wong ICK, Newton R, et al. Rechallenge with lamotrigine after initial rash. Seizure 1995;4:67. Thambi L, Kapcala LP, Chambers W, et al. Topiramate-associated secondary angle-closure glaucoma: A case series. Arch Ophthalmol 2002;120:1108. Theisohn M, Heinmann G. Disposition of the antiepileptic oxcarbazepine and its metabolites in healthy volunteers. Eur J Clin Pharmacol 1982;22:545. Theodore WH, Raubertas RF, Porter RJ, et al. Felbamate: A clinical trial for complex partial seizures. Epilepsia 1991;32: 392-397. Thompson PJ, Trimble MR. Anticonvulsant drugs and cognitive functions. Epilepsia 1982;23:531. Troupin AS, Ojemann LM. Paradoxical intoxication: A complication of anticonvulsive administration. Epilepsia 1975;16:753. Venulet J, ten Ham M. Methods for monitoring and documenting adverse drug reactions. Int J Clin Pharmacol Ther 1996;34:112. Verrotti A, Trotta D, Salladini C, et al. Anticonvulsant hypersensitivity syndrome in children: Incidence, prevention and management. CNS Drugs 2002;16:197-205. Vollmer KO, Anhut H, Thomann P, et al. Pharmacokinetic model and absolute bioavailability of the new anticonvulsant gabapentin. Adv Epileptol 1987;17:209. Vollmer KO, von Hodenberg A, Kolle EU, et al. Pharmacokinetics and metabolism of gabapentin in rat, dog and man. Arzneim Forsch Drug Res 1986;36:830. Wagner ML, Graves NM, Leppik IE, et al. The effect of felbamate on valproate disposition. Epilepsia 1991;32:15. Wang JT, Shiu GK, Worsley W, et al. The effect of humidity and temperature on in vitro performance of carbamazepine tablets. Pharm Res 1990;7 (Suppl):S143. Ward DL, Shumaker RC. Comparative bioavailability of felbamate in healthy men. Epilepsia 1990;31 (Suppl 5):642. Wilder BJ, Karas BJ, Penry JK, et al. Gastrointestinal tolerance of divalproex sodium. Neurology 1983;33:808. Wilensky AJ, Firel PN, Ojemann LM, et al. Pharmacokinetics of W-554 (ADD 03055) in epileptic patients. Epilepsia 1985;26:602. Willmore LJ, Triggs WJ, Pellock JM, et al. Valproate toxicity: Risk screening strategies. Child Neurol 1991;6:3. Wilson EA, Brodie MJ. New antiepileptic drugs. Baillieres Clin Neurol 1996;5:723. Wirrell EC. Valproic acid–associated weight gain in older children and teens with epilepsy. Pediatr Neurol 2003;28:126. Wolf SM, Forsythe A. Behavior disturbance, phenobarbital and febrile seizures. Pediatrics 1978;61:728. Wolf SM, Shinner S, Kang H, et al. Gabapentin toxicity in children manifesting as behavioral changes. Epilepsia 1996;36:1203. Wyllie E, Wyllie R, Cruse RP, et al. Pancreatitis associated with valproic acid therapy. Am J Dis Child 1984;138:912. Yager JY, Seshia SS. Sublingual lorazepam in childhood serial seizures. Am J Dis Child 1988;142:931. Yuen WC, Peck AW. Lamotrigine pharmacokinetics: Oral and I.V. infusion in man. Epilepsia 1987;28:528. Zonegran. Zonisamide: Product information. Eisai, Inc., Teaneck, NJ, 2004.
CHAPTER 50
The Ketogenic Diet James W. Wheless
Seizure disorders in childhood represent a frequently occurring neurologic problem. The incidence of epilepsy in children and adolescents ranges from 50 to 100 cases per 100,000 [Hauser, 1994; Hauser and Hesdorffer, 1980]. Antiepileptic drugs are the primary treatment modality and provide good seizure control in most children. However, more than 25% of children with seizure disorders have intractable seizures or uncontrolled seizures, or they suffer significant adverse effects secondary to medication [Heller et al., 1993; Pellock, 1993, 1995, 1996]. Standard antiepileptic drugs produce side effects in 50% or more patients and are associated with a number of chronic toxicity syndromes [Patsalos and Duncan, 1993; Pellock and Pippenger, 1993]. Only a limited number of children benefit from surgical therapy. Uncontrolled seizures pose a variety of risks to children, including higher rates of mortality, accidents, and injuries; a greater incidence of cognitive and psychiatric impairment; poorer self-esteem; higher levels of anxiety and depression; and social stigmatization or isolation [Fisher et al., 1996]. Effective treatment to control seizures is fundamental to improving overall outcome in childhood epilepsy. The shortcomings of antiepileptic drug therapy and epilepsy surgery have allowed alternative treatments to emerge. The ketogenic diet has proved to be an effective alternative treatment for many children with epilepsy [Levy et al., 2003; Wheless, 1995a, 1995b]. An independent review of the role of the efficacy of the ketogenic diet by the Blue Cross and Blue Shield Technology Assessment Center [LeFever et al., 2000] concluded that “… the ketogenic diet appears efficacious in reducing the frequency of seizures in children with refractory epilepsy … this improvement is in the range of, or greater than that reported with the addition of newer antiepileptic drugs.” This evaluation verifies the efficacy and the utility of the ketogenic diet even in the modern era with many more medication treatment options available. In this
chapter, the history of the development of the diet, current understanding of the biochemistry of ketone body formation and its relation to the anticonvulsant effect of the diet, considerations related to patient selection, and diet efficacy, complications, advantages, and disadvantages are reviewed.
HISTORY For centuries, fasting has been used to treat many diseases, including seizures, and it might have been used since Biblical times [Bible, 1982; Livingston, 1972]. Contemporary accounts of fasting were also reported earlier in the 20th century (Table 50-1); the first was the patient of an osteopathic physician Hugh Conklin [Freeman et al., 1994; Hendricks, 1995]. This child did not respond to the conventional treatment of the day, which was a combination of bromides and phenobarbital [Lennox and Lennox, 1960]. Conklin managed the child’s seizures with prayer and fasting, producing dramatic improvement in seizure control during the period of starvation. However, when the period of starvation was terminated, the seizures returned [Bridge, 1949; Conklin, 1922; Freeman et al., 1994]. The child’s uncle, a pediatrician, enlisted the aid of John Howland at Johns Hopkins Hospital to understand how starvation and fasting controlled seizures and discover how to maintain the beneficial effects of fasting [Lennox and Lennox, 1960]. Concurrently, Wilder [1921] at the Mayo Clinic suggested that a diet high in fat and low in carbohydrates could maintain ketosis and its accompanying acidosis longer than fasting [Freeman et al., 1994; Schwartz et al., 1989a, 1989b]. Wilder also coined the term ketogenic diet. Wheless [2004] reviews the history of the ketogenic diet. The beneficial effects of this diet were initially recorded by investigators from Johns Hopkins University, the Mayo
TABLE 50-1 Efficacy of Fasting (1921-1928) PATIENTS STUDY
N
Age (yr)
SEIZURE TYPE
DIET
SUCCESS RATE
COMMENTS
Geyelin, 1921
30
3.5-35
PM, GTC
Fasting
87% seizure free
Weeks et al., 1923
64
7-61
PM, GTC
Fasting
Talbot et al., 1926 Lennox, 1928
23 27
Children 13-42
UN UN
Fasting Fasting
47% seizure free during fast Seizure free during fast 50% had marked reduction in seizures during fast
Results based on 20-day fast; no long-term follow-up Patients fasted for 3 weeks; all had seizures after return to regular diet Seizures returned in all after fast PB stopped on admission; fast lasted 4 to 21 days
GTC, generalized tonic-clonic; PB, phenobarbital; PM, petit mal; UN, unknown.
1132
Epilepsy / 50
Clinic, and Harvard University. Use of the ketogenic diet was included in almost every comprehensive textbook on epilepsy in childhood that appeared between 1941 and 1980 [Bower, 1980; Bridge, 1949; Keith, 1963; Lennox, 1941; Lennox and Lennox, 1960; Livingston, 1954, 1963, 1972; Livingston et al., 1977; Penfield and Erickson, 1941; Withrow, 1980]. Until 1938, the ketogenic diet was one of the few available therapies for epilepsy. The ketogenic diet fell into disfavor when researchers turned their attention to antiepileptic drug development [Livingston and Pauli, 1975]. After the introduction of sodium valproate, it was believed that this branched-chain fatty acid could treat those children previously placed on the ketogenic diet and that the diet could no longer be justified [Aicardi, 1994]. Use of the ketogenic diet decreased greatly until it received national media attention in October 1994, when NBC Dateline aired a program on the ketogenic diet [Charlie Foundation to Help Cure Pediatric Epilepsy, 1994a, 1994b; Freeman et al., 1990, 1994, 1996; Hendricks, 1995; NBC Dateline, 1994; Schneider and Wagner, 1995]. After an almost 2-decade hiatus, the renewed public and scientific interest led to a better understanding of the use of the ketogenic diet, its inclusion in the American Academy of Pediatrics textbook on pediatric nutrition [Kleinman, 2004], and the publication of a textbook devoted to the ketogenic diet [Stafstrom et al., 2004].
EFFICACY As presented in Table 50-2, reports began to appear in the 1920s and 1930s that documented the efficacy of the ketogenic diet [Barborka, 1928a, 1928b, 1929; Fischer, 1935; Geyelin, 1921; Helmholz, 1927; Helmholz and Keith, 1930; Helmholz and Goldstein, 1937; Lennox and Cobb, 1928; McQuarrie and Keith, 1927; Peterman, 1925; Pulford, 1932; Wilder, 1921; Wilder and Pollack, 1935; Wilkins, 1937]. These were all retrospective reports; some described a small number of patients, and many provided few clinical details or specification of epilepsy syndrome type. The studies clearly demonstrated that some patients had improved seizure control on the diet. Over the next 60 to 70 years, many more clinical reports appeared (Table 50-3) [Keith, 1942; Prasad et al., 1996]. Meta-analysis of the published data is not possible given the differences in study design, sparse clinical details, and the lack of any standardized definitions of what is meant by a good or partial response to the diet [Prasad et al., 1996]. Despite these limitations in some of the older studies, the literature supports the view that the diet improved seizure control in selected children. About one third to one half of children appeared to have had an excellent response to the diet, defined by cessation or marked reduction in seizure activity. When the diet was discontinued, it was usually because of a lack of efficacy. It appeared that younger children were
TABLE 50-2 Efficacy of the Ketogenic Diet (1921-1976) PATIENTS STUDY
N
Age (yr)
SEIZURE TYPE
Peterman, 1925
37
2.25-14.5
PM, GTC
Talbot et al., 1926
12
Children
Cooder, 1933
38
≤12
Helmholz and Goldstein, 1937
501
Children
Wilkins, 1937
30
3-14
Keith, 1963
729
UN
Hopkins and Lynch, 1970
34
1-13
Livingston, 1972
1001 UN
Dodson et al., 1976
50
0.5-38
DIET SUCCESS RATE
COMMENTS
KD 60% seizure free All idiopathic causes; follow-up 0.33 to 2.5 years; 34.5% improved only 2 on PB 5.5% not improved PM, GTC KD 50% seizure free Follow-up for 3-6 months; all idiopathic causes 33% improved 17% no change. GTC, SP, PM KD 50% seizure free >3-month follow-up 34% improved 16% not improved UN KD Idiopathic causes: 92 had symptomatic epilepsy; 142 could not 31% seizure free maintain diet. All children had > 1 year follow-up. 16% definite improvement Results from children treated between 1922 and 53% not improved 1936; 1 child developed pellagra Symptomatic causes: 11% seizure free GTC, PM, MM KD 27% seizure free Idiopathic causes; follow-up > 1.5 years; all 50% no benefit seizure-free patients resumed normal diet UN KD For 530 patients with Patients treated between 1922 and 1944; follow-up idiopathic causes: for 1-30+ years (some included in Helmholz, 1937); 31% seizure free excluded 84 with symptomatic epilepsy; 115 unable 24% improved to follow diet; no deaths due to diet 39% no benefit. GTC, MM KD 29% successful (seizure 1 renal calculus free or much reduced) 32% unsuccessful 26% inadequate trial. UN KD 52% seizures controlled 27% seizures marked improvement 21% no improvement UN KD 50% seizure free 20-30% seizures improved considerably
GTC, generalized tonic-clonic; KD, classic ketogenic diet; MM, minor motor; PB, phenobarbital; PM, petit mal; SP, simple partial; UN, unknown.
Wheless / The Ketogenic Diet
1133
TABLE 50-3 Efficacy of the Ketogenic Diet (1989-2002) PATIENTS STUDY
N
Age (yr)
SEIZURE TYPE
Schwartz et al., 1989b
59
50% reduction of MCT-22 seizures Mod. MCT-13 80% multiple KD 29% seizure controlled seizure type 38% had ≥50% seizure reduction 29% no improvement 230 seizures/mo KD At 1 year: average (IS, 53% off diet (one half with SP, GTC, AB, poor seizure control, one CP, A, M) half with poor tolerance) 40% of original group with ≥50% decrease in seizure frequency 10% seizure free 934 seizures/mo KD At 6 months: average 50% seizure free 42% have ≥50% seizure reductions only 1 discontinued diet 410 seizures/mo KD At 1 year: average (AB, M, 55% remained on diet A, IS, GTC) 43% of original group had ≥50% decrease in seizure frequency 7% seizure free 81% mixed KD-49 MCT-3 Only 13.5% continued diet seizure types >12 months. LGS – M, A KD 100% had >50% decrease in seizure frequency by fifth day. Multiple seizure KD 46% remained on >1 year. types Of those on at least 45 days, 38% had >90% seizure reduction, 33% had 50-90% reduction. Multiple seizure KD 83 on at 1 year types 58 on at >24 months 30 on at >3 years Of original 150: 13% seizure free 14% had 90-99% seizure decrease Many off or on fewer AEDs Multiple types: KD 68% on at 1 year: 34 focal 16% seizure free onset, 100 10% had 90-99% seizure decrease generalized 47% on fewer AEDs Average: 23.8 seizures/day Partial, IS, KD 19% seizure free generalized 35.5% had improvement KD
DiMario and 24 Holland, 2002
1-15 Not given (mean, 6.5)
KD
Coppola, 2002
1-23 CP, GTC, (mean, LGS, M, 10.4) GT, SMEI, AA
KD
56
SUCCESS RATE
At 6 months: 18 on diet 3 seizure free 4 >90% improved 6 >50%, 50% seizure reduction Mean duration, 5 months At 12 months: 5 patients (8.9%) on diet and all had a >50% to 45 days on diet (mean, 350 days)
Prosepective; 3- to 6- year follow-up of Freeman, 1998
Retrospective; 83 patients had mental retardation
Retrospective; IS responder better than other seizure types Retrospective; age younger than 1 year and exposure to ≤ 3 AEDs predicted improvement Retrospective
Prospective. multicenter; 96.4% had MR, 67% had cerebral palsy, and 16% had microcephaly
*Hyphenated numbers indicate the number of patients on the diet. A, atonic; AA, atypical absence; AB, absence; AEDs, antiepileptic drugs; CP, complex partial; DQ, development quotient; GT, generalized tonic; GTC, generalized tonic-clonic; IQ, intelligence quotient; IS, infantile spasms; KD, classic ketogenic diet; LGS, Lennox-Gastaut syndrome; M, myoclonic; MCT, medium-chain triglyceride diet; Mod MCT, modified medium-chain triglyceride diet; MR, mental retardation; SMEI, severe myoclonic epilepsy of infancy (Dravet’s syndrome); SP, simple partial.
1134
Epilepsy / 50
more likely to have a more favorable response than older children, because younger children were able to produce more elevated levels of serum ketones and to adhere to the diet’s regimen [Freeman et al., 1998a]. There is a striking lack of data regarding its efficacy in infants from these prior studies. Many studies attest to the efficacy and safety of the ketogenic diet in infants [Klepper et al., 2002; Kossoff et al., 2002; Nordli et al., 2001]. Nordli and colleagues [2001] retrospectively reviewed their experience with 32 infants who had been treated with the ketogenic diet, 17 of whom had infantile spasms. Most infants (71%) were able to maintain strong ketosis. The overall effectiveness of the diet in infants was similar to that reported for older children; 19.4% became seizure free, and an additional 35.5% had a more than 50% reduction in seizure frequency. The diet was particularly effective for children with infantile spasms. Kossoff and colleagues [2002] retrospectively reviewed their experience with the ketogenic diet as a treatment for infantile spasms during a 4-year period. Twenty-three children (5 months to 2 years old), 39% of whom had symptomatic infantile spasms and 70% of whom had hypsarrhythmia, were started on the ketogenic diet. The children had been previously exposed to an average of 3.3 (range, 0 to 7) antiepileptic drugs, and 74% had previously failed or relapsed after adrenocorticotropic hormone or steroids. The average time on the diet was 1.6 years, with 56% remaining on the diet at 12 months, 46% of whom were more than 90% improved (three were seizure free) and 100% of whom were more than 50% improved. Factors that predicted more than 90% improve-
ment at 12 months were age younger than 1 year (P = 0.02) and exposure to more than three antiepileptic drugs (P = 0.03). Improvement in development was related to seizure control. A few early studies evaluated use of the ketogenic diet in adults (Table 50-4). Some revealed improved seizure control [Barborka, 1928a, 1928b, 1930], but subsequent reports concluded that the diet was not particularly beneficial in adolescents and adults with epilepsy [Bridge, 1949; Lennox, 1941; Livingston, 1954, 1963, 1972; Notkin, 1934; Withrow, 1980]. Reasons cited for this finding were poor dietary compliance, types of seizures seen in these age groups, and the developmental differences in the ability of the brain to use ketone bodies. As a result, past studies suggested that the optimum age of response to the diet might be in young children before the onset of adolescence. Some studies have challenged the belief that older patients could not maintain therapeutic ketosis or could not comply with the rigors of the diet and that the ketogenic diet was less efficacious in this age group. Sirven and colleagues [1999] reviewed the tolerability, efficacy, and adverse events in 11 adult patients prospectively begun on the classic ketogenic diet for refractory symptomatic epilepsy. All were on stable medication and had not achieved seizure control with two or more medications, and four had prior surgery. At 8 months of follow-up, one patient was seizure free, five patients had a more than 50% decrease in seizure frequency, one patient had a less than 50% seizure decrease, and four patients discontinued the diet. Common adverse events included gastrointestinal complaints (100%), menstrual irregularities
TABLE 50-4 Efficacy of the Ketogenic Diet in Adolescents and Adults PATIENTS STUDY
N
Age (yr)
SEIZURE TYPE
DIET
SUCCESS RATE
COMMENTS
Barborka, 1928b
49
17-42
GTC, PM
KD
No patients with symptomatic epilepsy; only 5 on an AED (PB); 3-36 month follow-up
Baborka, 1930
100
16-51
GTC, PM
KD
Bastilble, 1931
45
19-57
GTC, PM
KD
Notkin, 1934
20
22-47
GTC
KD
Sirven et al., 1999
11
19-45
PE, GE
KD
Mady et al., 2003
45
12-19
MT, LGS, CP, GTC, M, AT, SP
KD
16% seizure free 22% improved 27% not benefited 35% did not cooperate and stay on diet 12% seizure free 44% improved 44% not benefited Of those staying on diet: 7% seizure free 72% improved 21% seizures increased 16 of 45 unable to maintain diet No improvement in any 90% had increased number of seizures 9% seizure free 46% had >50% decrease in seizure number 9% slight decrease in seizure number 36% discontinued diet Of 20 who remained on diet at 1 year: 6 had >90% efficacy 7 had 50-90% efficacy
No patients with symptomatic epilepsy; 3-60 month follow-up All institutionalized females diagnosed with “epileptic insanity” without known cause; 6-month follow-up; best response seen in those with least “mental disorder” All institutionalized patients and off AEDs; no known cause; average time on the diet 11 months All symptomatic epilepsy; 8-month follow-up
Average duration 1.2 years
AED, antiepileptic drug; AT, atonic; CP, complex partial; GE, generalized epilepsy; GTC, generalized tonic-clonic; KD, classic ketogenic diet; LGS, Lennox-Gastaut syndrome; M, myoclonic; MT, myoclonic-tonic; PB, phenobarbital; PE, partial epilepsy; PM, petit mal; SP, simple partial.
Wheless / The Ketogenic Diet
in all women, and increased serum cholesterol and highdensity lipoprotein (HDL) cholesterol ratios. Subjective improvements in thinking and mood, without a decrease in antiepileptic drugs, were reported in seven patients, one without improved seizure control. Mady and colleagues [2003] reviewed their experience with 45 adolescents who had been on the ketogenic diet for an average duration of 1.2 years. They found no evidence to support the beliefs that the diet was not efficacious and too restrictive in this age group. Adolescents with multiple seizure types did best, and simple and complex partial seizures had the poorest response. The retention rate for motivated adolescents on the diet was not significantly different than reports in younger children. Studies have critically reexamined the benefits of the diet in selected groups of patients (see Table 50-3). Schwartz and colleagues [1989a, 1989b] reported the results of metabolic profiles and seizure control in 59 epileptic children receiving a normal diet or one of three forms of the ketogenic diet: a classic diet (4:1 ratio of fat to protein and carbohydrate), a medium-chain triglyceride (MCT) diet, and a modified MCT diet. Patients fasted for 18 hours and then were placed on one of the diets and monitored for 6 weeks. All three diets produced a significant increase in total ketone body (e.g., acetoacetate, 3-hydroxybutyrate) levels that was most marked using the classic ketogenic diet as described in the Johns Hopkins protocol [Freeman et al., 2000]. Ketone body concentrations reached a maximum in the afternoon and were frequently lower in the morning. Urinary ketones were measured and reflected changes found in the serum. All three diets improved seizure control, and none were superior to the others during the 6 weeks of observation. Overall, these investigators found that 81% of patients had greater than a 45% reduction in seizures. Drowsiness, occurring in 25% of patients during initiation of the diet, usually resolved. The MCT diet was considered less palatable and associated with more side effects, including diarrhea and vomiting. Data for 59 patients have been reported from the group at Johns Hopkins [Kinsman et al., 1992]. All had severe intractable epilepsy, 80% had multiple seizure types, and 88% were on multiple antiepileptic drugs. Improved seizure control occurred in 67% of patients, 64% were able to reduce the amount of antiepileptic drugs they were taking, 36% became more alert, and 23% had better behavior. Comorbid neurologic conditions in this group of patients with refractory epilepsy included mental retardation (84%), microcephaly (15%), and cerebral palsy (45%). Seizure type did not predict success with the diet. Moreover, 75% of the improved patients continued the diet for at least 18 months, confirming the efficacy and palatability of the diet and the willingness to continue administration of the diet by patients and their families. This study confirmed the earlier work by Livingston [1972] on a large number of patients at the same institution demonstrating that 52% had complete control and an additional 27% had improved control. The first multicenter prospective study of the efficacy of the ketogenic diet was based on data collected on 51 children at seven comprehensive epilepsy centers [Vining et al., 1998]. All children had intractable epilepsy, averaging 230 seizures per month. It was found that 10% of treated patients were seizure free at 1 year. A greater than 50% decrease in seizure frequency was observed at 3 months in
1135
54% of patients. This improvement was maintained at 6 (53% controlled) and 12 months (49% controlled) after initiation of the diet. Patient age, seizure type, and electroencephalographic (EEG) abnormalities were not related to outcome. Approximately 47% remained on the diet for at least 1 year. Reasons for discontinuation included insufficient seizure control, inability to medically tolerate the diet, concurrent medical illnesses, or inability to tolerate the restrictive nature of the dietary regimen. Although the number of patients was small, the study demonstrated that the diet could be effectively used in different epilepsy centers with different support staff and that children and their families were able to comply with the diet when it was effective. The study also confirmed results similar to those reported over the past 5 decades. The first large, prospective evaluation of the ketogenic diet was conducted in 150 consecutive children who were 1 to 16 years old (mean age, 5.3 years) [Freeman, 1998a]. The children were followed for a minimum of 1 year, had previously been on an average of 6.24 medications, and were on a mean of 1.97 medications at the diet’s initiation. Seventy percent of children had an intelligence or a developmental quotient of less than 69. The children averaged 410 seizures per month before the ketogenic diet. At 6 months, 71% remained on the diet, and 32% had a more than 90% decrease in seizure frequency. At 1 year, 55% remained on the diet, 7% were seizure free, and 27% had a more than 90% decrease in seizure frequency. There was no statistically significant difference in seizure control based on age, gender, or seizure type, although none had purely partial seizures. Most of those discontinuing the diet did so because it was insufficiently effective or too restrictive. All of the prior reports of efficacy for the ketogenic diet were open-label trials (retrospective or prospective). The first blinded, crossover study of the diet evaluated its efficacy for atonic or myoclonic seizures in patients with Lennox-Gastaut syndrome [Freeman, 1999]. This attempt documented that it was feasible to perform a larger, blinded, placebo-controlled, crossover trial enrolling a population with frequent seizures. The Atkins diet is less restrictive than the ketogenic diet and induces a metabolic ketosis. A small pilot study revealed three of six patients had a more than 50% seizure reduction, with two becoming seizure free [Kossoff et al., 2003]. This report raises important questions about the level of restrictions on protein and calories imposed by the ketogenic diet, and there may be a subgroup of patients who benefit from a less restrictive diet. Dietary therapies may become even more valuable in the therapy of epilepsy when the mechanisms underlying their success are understood.
MECHANISM OF ACTION Clinical reports detailed the efficacy of the ketogenic diet, and several theories emerged to explain the diet’s mechanism of action [Schwartzkroin, 1999]. Four major areas have been investigated: cerebral acidosis, water balance, the direct effect of ketones or lipids, and alteration in brain energy substrates. The importance of ketone body formation was recognized early in the search for a mechanism of the ketogenic diet [McQuarrie and Keith,
1136
Epilepsy / 50
1927]. Initially, acidosis and partial dehydration were considered likely factors contributing to its success [Bridge and Lob, 1931; Lennox, 1928]. Even later, the diet’s effects on water and electrolyte metabolism were thought responsible for its efficacy [Millichap et al., 1964]. Animal studies have found no change in intracellular pH of the cerebral cortex on the ketogenic diet [Al-Mudallal et al., 1996; Harrik et al., 1997]. Preliminary studies using magnetic resonance spectroscopy (MRS) have demonstrated that children on the diet do not develop alteration of brain water and electrolyte distribution [Seymour et al., 1999] or cerebral acidosis [Marks et al., 1997; Seymour et al., 1999]. This finding suggests that although ketoacidosis occurs in these children, changes in brain pH may not be a critical factor. Animal models and human evidence suggest a prominent role for ketonemia [Al-Mudallal et al., 1995; Appleton and DeVivo, 1973, 1974; DeVivo et al., 1975; Stafstrom, 1999; Uhlemann and Neims, 1972]. One study considered elevated levels of plasma lipids a good index in predicting the extent of seizure control in children [Dekaban, 1966]. Subsequent analysis of blood metabolites in nine children on the ketogenic diet revealed a rise in the total serum arachidonate concentration correlated with improved seizure control, suggesting elevated polyunsaturated fatty acids may represent an anticonvulsant mechanism of the ketogenic diet [Fraser et al., 2003]. Despite its prolonged use and proven value, the exact mechanism of action of the diet remains unknown [Nordli and DeVivo, 1997].
Oxidation of Fatty Acids: Ketogenesis Ketonemia is essential for the ketogenic diet to work. Ketonemia occurs because of fatty acid oxidation during fasting or while on the ketogenic diet [Cahill, 1982; DeVivo, 1980; Hawkins and Biebuyck, 1980; Mayes, 1996a, 1996b]. Fatty acids are oxidized to and synthesized from acetylcoenzyme A (acetyl-CoA) [Roe and Coates, 1995]. However, these are not reverse processes. Fatty acid biosynthesis (i.e., lipogenesis) takes place in the cytosol, whereas fatty acid oxidation occurs in mitochondria and generates adenosine triphosphate (ATP). The oxidizable substrate may come from dietary sources (e.g., ketogenic diet) or from mobilization of peripheral adipose stores (e.g., starvation) (Fig. 50-1). The brain does not directly use fatty acids but readily oxidizes ketone bodies [Hawkins and Biebuyck, 1979, 1980]. Increased fatty acid oxidation leading to ketone body (i.e., acetoacetate and β-hydroxybutyrate
Triglycerol
Adipose tissue
Hormone-sensitive lipase
FFA
FFA
BLOOD
FFA
LIVER
FIGURE 50-1. Initial steps in ketogenesis: lipolysis. FFA, fatty acids.
[BHB]) formation by the liver is characteristic of starvation or the ketogenic diet (Fig. 50-2) [Mayes, 1996]. Glucose, present in small concentrations, is necessary to facilitate ketone body metabolism. This condition is referred to as the permissive effect of glucose and is explained metabolically by the conversion of glucose-derived pyruvate to oxaloacetate. Oxaloacetate is the key rate-limiting metabolite of the tricarboxylic acid (TCA) cycle and is necessary for the condensation reaction with acetyl-CoA to form citrate. Acetoacetate continually undergoes spontaneous decarboxylation to yield acetone, which is volatilized in the lungs and gives the breath its characteristic odor. The ratio of BHB to acetoacetate in blood varies between 1:1 and 10:1; the concentration of total ketone bodies in the blood does not normally exceed 0.2 mmol/L. The liver is the only organ capable of synthesizing significant quantities of ketone bodies that are released into the blood (see Fig. 50-2). The liver is equipped with an active enzymatic mechanism for the production of acetoacetate. Once formed, acetoacetate cannot be significantly metabolized back to fatty acids in the liver because it lacks the enzyme 3-oxoacid-CoA transferase. This accounts for the net production of ketone bodies by the liver. Ketone bodies are then transported to and oxidized in extrahepatic tissues in proportion to their concentration in the blood. Oxidation and brain influx rates of ketone bodies are proportional to their blood concentration up to approximately 12 mmol/L. At this level, the oxidative machinery and uptake mechanisms of the cell are saturated [Mayes, 1996]. Glucose is the principal source for brain metabolism. Until 1967, glucose was thought to be the obligate fuel source. Under certain conditions (e.g., fasting, ketogenic diet), the human brain uses ketone bodies for fuel [Owen et al., 1967], with the movement of ketone bodies into the brain depending on a monocarboxylic transport system [DeVivo, 1980]. Acetoacetate and BHB are metabolized primarily in the mitochondrial compartment. In the brain, the main pathway for the conversion of acetoacetate to acetoacetyl-CoA involves succinyl-CoA (Fig. 50-3). Acetoacetyl-CoA is split to acetyl-CoA and oxidized in the TCA cycle. The enzymes that break down BHB and acetoacetate into acetyl-CoA are regulated developmentally, with maximal expression early in life [Dahlquist et al., 1972; Hawkins et al., 1971; Nehlig, 1999]. This finding is consistent with the higher use of ketones by the brain in children compared with adults [Kraus et al., 1974]. The oxidation of ketone bodies serves as a source of energy and contributes to certain cerebral metabolic pathways that normally depend on glucose metabolism (i.e., glutamate, γ-aminobutyric acid (GABA)) [Cooper et al., 1996; Cremer, 1971; DeLorey and Olsen, 1994; Rodwell, 1996; Sokoloff, 1973]. TCA cycle activity is governed by the availability of oxaloacetate and the rate-limiting enzyme, α-ketoglutarate dehydrogenase, which is regulated by the concentration of succinyl-CoA. Increased α-ketoglutarate and decreased succinyl-CoA levels imply maximal TCA cycle activity. Fatty acid oxidation increases brain ATP concentration [Mayes, 1996a, 1996b]. Elevation of brain ATP concentration has been verified in an animal model of the ketogenic diet [DeVivo et al., 1978; Nakazawa et al., 1983] and suggests that the ketogenic diet improves cerebral energetics. Increased cerebral energy reserves are hypothesized to be important
Wheless / The Ketogenic Diet
1137
FFA
Blood
Cytosol
Blood
Mitochondrion Carnitine -Oxidation
Thiolase Acetoacetyl-CoA
Acetyl-CoA Tricarboxylic acid cycle (TCA)
HMG-CoA synthetase -OH--methylglutaryl-CoA HMG-CoA lyase CO2 Acetone
ATP Acetyl-CoA + Acetoacetate -OH-butyrate NADH+H+ dehydrogenase NAD+ -Hydroxybutyrate
Acetoacetate
-Hydroxybutyrate
FIGURE 50-2. Ketogenesis in the liver. Fatty acids (FFA) from the circulation enter the hepatocyte and then cross the mitochondrial membrane by carnitine transport (long-chain FA) or diffusion (short- and medium-chain FA).
Blood
Brain
-Hydroxybutyrate
-Hydroxybutyrate (1)
Acetoacetate
NAD+ NADH + H+
Acetoacetate Succinyl CoA (2) succinate Acetoacetyl CoA (3) Acetyl-CoA + OAA
TCA CYCLE
Succinate
Citrate
Succinyl CoA ␣-Ketoglutarate Succinic semialdehyde (5) GABA shunt
GABA
(4)
Glutamate
FIGURE 50-3. Ketone body use and oxidation in the brain. 1, β-hydroxybutyrate dehydrogenase; 2, 3-oxoacid coenzyme A (CoA) transferase; 3, acetoacetyl-CoA thiolase; 4, glutamic acid decarboxylase (GAD); 5, γ-aminobutyric acid (GABA); OOA, oxaloacetate; TCA, tricarboxylic acid cycle.
1138
Epilepsy / 50
for the anticonvulsant effect. Another mechanism may be alteration of the synthesis or function of GABA. Increases in α-ketoglutarate levels when on the diet may increase input into the GABAA shunt [DeVivo, 1980; McGeer and McGeer, 1989; Peng et al., 1993]. Although entire-brain GABA levels are not changed in an animal model of chronic ketosis [Al-Mudallal et al., 1996; Harik et al., 1997], local differences may occur [Rho et al., 1999b; Yudkoff et al., 2001a]. Two children studied with two-dimensional., double-quantum MRS had low initial GABA levels that increased over time on the ketogenic diet [Wang et al., 2003]. The addition of acetoacetate or BHB to rat synaptosomes increased the rate of GABA formation by 35% and 43%, respectively [Erecinska et al., 1996]. At the same time, the conversion of glutamate to aspartate, which has excitatory properties in the brain, is reduced [Erecinska et al., 1996; Yudkoff et al., 1997, 2001b]. Human studies correlate GABA receptor stimulation with increased energy demand, likely at the synaptic or glial cell level [Peyron et al., 1994]. Activation of GABA pathways, although inhibitory, requires increased energetic demand. The ketogenic diet increases cerebral energetics, potentially helping to meet this demand, and increases the overall GABA inhibitory effects by activating certain GABA receptor subtypes. Many types of epilepsy may involve disruptions of brain energy homeostasis, facilitating potential management through dietary elevations of ketone bodies and reduction of glucose [Greene et al., 2003].
Evidence from Clinical Studies Although the exact mechanism of action of the ketogenic diet is unknown, it is generally accepted that for the diet to be successful, the child must remain in ketosis and generate ketone bodies. Ketonemia is necessary but not sufficient for ketogenic diet-induced seizure control [Stafstrom and Spencer, 2000; Vining, 1999b]. Urine ketones are the only readily available inexpensive approach to ketone assessment, and the desired range is typically 80 to 160 mmol/L. Seizure control correlates significantly (P = 0.03) with serum BHB levels greater than 4 mmol/L, although urinary ketone levels of 160 mmol/L can be found when blood BHB levels exceed 2 mmol/L [Gilbert et al., 2000]. Although serum ketones, particularly BHB, are believed to more accurately reflect the immediate state of ketosis, it is not certain whether it is the presence of these ketone bodies that produces the antiseizure effect. Brown and colleagues [1998] measured serum BHB levels in 12 children during routine clinic visits and during illness. Eight experienced an increase in seizures and decrease in BHB during illness, and four had no seizure increase and no lowering of BHB levels. This finding suggests BHB levels are important for the antiseizure effect. Subsequently, Freeman and associates [1998b] evaluated BHB levels of 35 children 3 months after diet initiation. There was a significant correlation between higher levels of BHB and seizure control. The mean BHB concentration in patients with more than 90% seizure control was greater than 6 mM. The classic ketogenic diet is thought to produce the greatest amount of ketone bodies [Schwartz et al., 1989a]. Despite the fact that ketone bodies partially replace glucose for cerebral metabolism [DeVivo, 1980; Haymond et al., 1983], cerebral glucose levels are unaltered [Al-Mudallel et al., 1995; DeVivo et al., 1978]. Ketones from the circulation
are transported across the blood-brain barrier by facilitated diffusion, using a monocarboxylate transport system [Moore et al., 1976; Pellerin et al., 1998]. The efficacy of the diet in childhood and the apparent slightly lower efficacy in older children and adults may reflect maturational changes in this transport system [Dahlquist et al., 1976; DeVivo, 1980; Dodson et al., 1976; Kraus et al., 1974; Persson et al., 1972; Williamson, 1985]. A child’s ability to extract ketones from the blood into the brain is four to five times greater than that seen in adults [DeVivo, 1983]. This developmentally based ability to extract ketones from the blood may in part explain why the diet is more successful in children. However, even adult animals placed on the ketogenic diet can upregulate brain monocarboxylate transporter levels [Leino et al., 2001]. MRS has documented that fasting and intravenous BHB infusion in humans increase brain BHB levels [Pan et al., 2000, 2001]. Proton magnetic resonance spectroscopy (1H-MRS) carried out on occipital gray matter in five children on the ketogenic diet demonstrated a single resonance identified as acetone [Seymour et al., 1999]. No resonance for BHB or acetoacetate was detected, despite their presence in the blood, indicating the principal intracellular ketone accumulated in response to the ketogenic diet is acetone. Subsequent experiments in rats and mice found that acetone is an antiepileptic agent and that chronic administration may enhance its action [Likhodii et al., 2002; Rho et al., 2002]. MRS has also been used to study changes in cerebral energetics induced by the ketogenic diet. Alteration of the TCA cycle activity by ketosis, resulting in an increased ATP/ADP ratio or greater cerebral energy is thought to have an anticonvulsant effect. This hypothesis is supported by experiments in patients with Lennox-Gastaut syndrome that used phosphorus magnetic resonance spectroscopy (31P-MRS) to document improvement in cerebral energy metabolism on the ketogenic diet [Pan et al., 1999]. During chronic ketosis, adaptive mechanisms occur that increase the cerebral extraction of ketone bodies [Gjedde and Crone, 1975]. These mechanisms may be why ketosis develops promptly within several days after initiation of the diet, although the anticonvulsant effect may be delayed for 1 to 2 weeks [Appleton and DeVivo, 1973, 1974]. This observation suggests that ketosis per se is insufficient to explain the anticonvulsant effect. After ketone bodies are extracted, it is postulated that there is a secondary biochemical change or a cascade of biochemical effects that have some form of anticonvulsant effect [Prasad et al., 1996]. The importance of ketosis was demonstrated by Huttenlocher in 1976. He studied two children with a prior history of myoclonic seizures who were seizure free on the ketogenic diet. After a 50-minute infusion of glucose, the first patient’s serum ketones decreased 67%, with no change in serum pH, and a seizure occurred. The second child’s EEG pattern changed from normal to diffuse polyspike and slow-wave complexes accompanied by myoclonic jerks after 90 minutes of intravenous glucose. Another study, involving nine children with intractable atypical absence seizures treated with the MCT diet, found a significant decrease in the mean number of epileptiform discharges in treated patients [Ross et al., 1985]. A rise in serum ketone levels was the only prominent early biochemical change. DeVivo and associates [1991] also reported two children
Wheless / The Ketogenic Diet
suffering from seizures resulting from a glucose transporter type I defect who were treated with the ketogenic diet, resulting in complete control of seizures and improvement in neurologic development. These observations and others suggest a pivotal role for ketone bodies in providing an alternative energy source and in achieving a still unknown role in seizure control [Aicardi, 1992; DeVivo, 1983; DeVivo et al., 1978; Huttenlocher, 1976; Lamers et al., 1995; Livingston, 1954; Millichap et al., 1964; Schwartz et al., 1989b; Withrow, 1980].
Evidence from Experimental Studies In the past decade, the results of basic research have shed light on the ketogenic diet and its effect on brain chemistry. Several animal models have been used to study the effects of the ketogenic diet [Bough et al., 2002, 2004; Stafstrom, 1999; Stafstrom, 2003]. In general these animal models demonstrate that the ketogenic diet provides protection for partial-onset seizures with secondary generalization and generalized myoclonic, tonic, and tonic-clonic seizures, providing laboratory evidence that the diet is effective against a variety of seizure types. However, some studies have failed to demonstrate a protective effect for the ketogenic diet in models when animals were acutely challenged with a convulsant stimulus (i.e., kainic acid, strychnine, or maximal electroconvulsive shock) [Bough et al., 2000a, 2002; Thavendiranathan et al., 2000]. The discrepancy is likely explained by the fact that the later studies did not test the diet in animals with spontaneous seizures. The relative efficacy of the ketogenic diet in different animal models suggests that different areas of the brain may be affected more than others, and this pattern may be related to localized differences in the function of GABA, other neurotransmitters (e.g., norepinephrine) [Szot et al., 2001], or protein phosphorylation [Ziegler et al., 2002]. A direct effect by acetoacetate or BHB on the primary voltage- and ligandgated ion channels mediating excitatory or inhibitory neurotransmission in the hippocampus could not be demonstrated [Thio et al., 2000]. Despite differences in ketogenic diet protocols and laboratory models, they collectively document improvement in control of multiple seizure types by increasing seizure threshold [Thavendiranathan et al., 2003]. The response of most seizure types to the ketogenic diet implies that the diet exerts a general suppressant effect on neuronal excitability. A limited number of animal studies have investigated the effect of age at diet onset versus efficacy. These studies used different diet types and durations and different seizure models. However, all conclude that the diet provides a greater level of seizure protection for younger animals than for older animals [Bough et al., 1999c; Rho et al., 1999a]. However, adult animal models also demonstrate an elevated seizure threshold [Appleton et al., 1974; Bough et al., 1999b; Hori et al., 1997]. The relation between the degree of seizure control and extent of ketonemia has only recently been explored. Although it would seem intuitive that increasing ketonemia would correlate with efficacy of the ketogenic diet, experimental studies have not revealed a positive correlation [Bough et al., 1999a, 2000b; Likhodii et al., 2000]. However, rats that developed higher levels of ketosis also
1139
had higher thresholds for seizure induction [Bough et al., 1999b]. A threshold level of ketosis may be required that must be maintained for the ketogenic diet to be effective; whether seizure control is improved by further degrees of ketosis is not clear. These same investigators and others have suggested that caloric restriction can significantly influence seizure threshold and augment the effects of the ketogenic diet on seizure control [Bough et al., 2000a, 2002, 2003; Cheng et al., 2004; Greene et al., 2001]. The classic ketogenic diet is composed primarily of long-chain saturated fatty acids. Experimental studies in rats have found no difference in the level of seizure protection or brain fatty acid profiles when they were fed a variety of qualitatively different types of diets [Dell et al., 2001; Likhodii et al., 2000]. In addition to an anticonvulsant effect, several animal models (i.e., kainic acid, knockout mice, EL mice) provide evidence that the ketogenic diet can prevent epileptogenesis, the process by which the brain develops an epileptic condition [Bough et al., 2003; Muller-Schwarze et al., 1999; Rho et al., 1999c, 2000; Stafstrom et al., 1999; Su et al., 2000; Todorova et al., 2000]. These studies support the clinical observation that children can be gradually weaned off the ketogenic diet, resume a normal diet, and not experience loss of seizure control. These animal models help explain the mechanism of action of the ketogenic diet, ultimately aiding in the development of novel antiepileptic drugs or treatments.
SELECTION OF CANDIDATES FOR THE DIET Indications Indications for the use of the ketogenic diet have unfortunately grown out of experience, not from understanding its physiologic action. Despite the fact that several thousand patients have been treated, there are no consensus criteria describing which patients are candidates for the diet [Maria et al., 1997] (see Tables 50-1 to 50-4). Many seizure types appear to respond to the ketogenic diet. In general, several groups of children are potential candidates for treatment. These include children with the following conditions: 1. Medically intractable seizures 2. Poor tolerance or significant side effects from antiepileptic drugs 3. Intractable seizures in persons who are being considered for epilepsy surgery (i.e., callosotomy, nonlesional resection, or extratemporal resection) 4. Specific neurometabolic disorders or neurologic syndromes (Box 50-1) The physician must also consider age for patients with medically intractable epilepsy or those who have serious side effects from medication. Children 1 to 12 years old have had successful outcomes. It is often more difficult for older children to maintain ketosis. Seizure type appears to be less important. Almost all seizure types respond to the ketogenic diet. The success of the diet for children is determined far more by circumstances within the home than by the epilepsy itself. The ketogenic diet is a strictly regulated medical diet. Its success depends on the detailed
1140
Epilepsy / 50
Box 50-1 SPECIFIC CONDITIONS TREATED WITH THE KETOGENIC DIET • Glucose transporter deficiency syndrome (GLUT1-DS, McKusick 138140) • Pyruvate dehydrogenase complex deficiency (McKusick 312170) • Associated with Leigh’s syndrome • Associated with lactic acidosis and cerebral dysgenesis • Phosphofructokinase deficiency • Ketotic hypoglycemia • Acquired epileptiform opercular syndrome • Rett’s syndrome
accuracy and consistency with which the regimen is carried out within the home. Continued support, monitoring, and education by a team of professionals, including physicians, dietitians, nurses, and social workers, are necessary. Little is known about whether the ketogenic diet should be considered for patients who are being evaluated for epilepsy surgery. The diet could be used preferentially in selected candidates who are being considered for corpus callosotomy, nonlesional resection, or extratemporal resection. For patients in whom a malignancy or vascular malformation is detected, surgery is preferable. Additional research is needed in this area.
Brain
Blood
Glucose
A
Glucose
1
Pyruvate Acetoacetyl-CoA
2
Acetyl-CoA
B
Citric acid cycle
Respiratory chain
ATP
BBB
Ketones (acetoacetate, -hydroxybutyrate)
The ketogenic diet may be the preferred initial therapy for children with seizures and specific metabolic defects or seizures associated with specific neurologic syndromes (Fig. 50-4 and see Box 50-1) [DeVivo, 1991; DeVivo et al., 1973; Haas et al., 1986; Klepper et al., 2002, 2004; Liebhaber et al., 2003; Melvin et al., 1996; Shafrir and Prensky, 1995; Weber et al., 2001; Wexler et al., 1997; Wijburg et al., 1991]. These specific metabolic disorders are reviewed in other sections of this textbook, as is the use of the ketogenic diet for their treatment. For some patients, the ketogenic diet is contraindicated (Box 50-2). Children with acute intermittent porphyria and seizures should not be treated with the ketogenic diet because carbohydrate restriction can be harmful in this condition. The ketogenic diet may also worsen some mitochondrial diseases, pyruvate carboxylase deficiency, or organic acidurias [Demeritte et al., 1996b; Kleinman, 2004; Nordli, 2001]. When indicated, obtaining a metabolic screen, including urine amino and organic acids, serum amino acids, lactate, pyruvate, and carnitine profile should be done before starting the ketogenic diet [Wheless, 2001]. The combination of the use of the ketogenic diet with topiramate or zonisamide appears to be associated with an increased risk of acidosis.
Candidate Selection and Encephalography The predictive value of an electroencephalogram obtained before, during, or after initiation of the ketogenic diet is
FIGURE 50-4. Metabolic defects and the ketogenic diet. Glucose enters the brain by the glucose transporter, GLUT1 (A); ketones penetrate the blood-brain barrier (BBB) by the medium-chain triglyceride transporter (MCT1) (B). GLUT1 deficiency syndrome is caused by a defect in glucose transport into the brain (1). Pyruvate dehydrogenase deficiency impairs acetyl-CoA production (2). The ketogenic diet bypasses these two defects and provides acetyl-CoA for brain energy production.
Wheless / The Ketogenic Diet
Box 50-2 SPECIFIC CONTRAINDICATIONS TO THE KETOGENIC DIET • • • • • • • •
Pyruvate carboxylase deficiency Organic acidurias Mitochondrial disease Porphyria Defects in fatty acid oxidation Carnitine deficiency Glutaric aciduria, type II Pyruvate dehydrogenase phosphate deficiency
unknown. In 1933, Eley described 29 children with epilepsy studied before institution of the ketogenic diet. Approximately 90% of children with normal EEG results responded favorably to the diet, compared with only 12% with abnormal EEG patterns [Eley, 1933]. Penfield and Erickson [1941] mentioned that patients with abnormal hyperventilation study results were more likely to respond to the diet. Livingston [1954] reported on the EEG findings for 102 patients and found that those patients who did best on the diet had petit mal variants (i.e., spike-and-wave forms). Surprisingly, carefully done studies examining the relation of the EEG results and response to dietary treatment have not been reported. The multicenter study was unable to correlate any baseline EEG pattern with outcome, except for children with multifocal spikes, who did less well at 3 months but had no differences at 6 or 12 months [Vining et al., 1998]. Many studies, including the original works of Bridge [1949], Livingston [1954], and Keith [1963], have suggested improvement or normalization of the EEG pattern after the diet has been implemented. Nellhaus [1971] correlated normalization of the EEG pattern with the onset of ketosis, clinical improvement, and prognosis. Others have observed that EEG improvement might be seen with clinical improvement in patients with minor motor and petit mal seizures but not in those with focal or generalized tonic-clonic seizures [Janaki et al., 1976]. Children with atypical absence seizures demonstrated a significant decrease in the number of epileptiform discharges at initiation of MCT therapy. However, their EEG patterns were unchanged from baseline at the end of a 10-week treatment period, despite two thirds having a greater than 50% decrease in seizure frequency [Ross et al., 1985]. Demeritte [1996a] stated that there was no correlation between epileptiform activity and seizure improvement. However, background EEG improvements did correlate with a significant reduction in seizures. Ambulatory 24-hour electroencephalograms used to document the extent of ictal abnormalities in patients with frequent astatic events have shown sensitivity in documenting the rapid impact of the ketogenic diet in decreasing electroclinical seizures [Freeman et al., 1999].
INITIATION AND MAINTENANCE A comprehensive monograph on the evaluation and management of patients being considered for placement on the ketogenic diet was published and then revised by Freeman and colleagues at Johns Hopkins University [Freeman et al., 1994, 2000]. A videotape, “The Ketogenic
1141
Diet for Families, Dietitians, Nurses and Physicians,” and other resource materials are available from the Charlie Foundation (see “Resources” at the end of this chapter). The following sections offer an overview of how the diet can be implemented.
Prehospital Evaluation After a child is considered a candidate for the diet, a screening evaluation by selected members of the team responsible for implementing the diet is initiated. Screening usually includes a comprehensive evaluation by the dietitians and nursing staff. The purpose of this evaluation is to educate the family and to assess their ability on many levels to carry out the rigorous and exacting program necessary to maximize the diet’s success. At the same time, the different types of meal plans and foods that the child can eat and their preparation are discussed. Issues involved in this evaluation are carefully considered and reviewed by Casey and colleagues [1999] and by Freeman and associates [2000].
Hospitalization The child is scheduled for elective admission to the hospital for initiation of the ketogenic diet (Box 50-3). Parents are told to view this treatment as a 4-week trial. During this time, they must adhere strictly to the diet, with proof of persistent ketosis. The frequency of seizures usually decreases gradually, but reversal of the effect can occur rapidly. Weeks of hard work can be undone if a child eats a cookie or a piece of candy. If the seizures are improved, this usually is sufficient motivation for the parents to continue.
Box 50-3 INITIATION OF THE KETOGENIC DIET Hospitalization for 3 to 5 days Day 1 Initial fast Fluids, 75% of maintenance Check urine ketones each void Check fingerstick blood glucose every 6 hours Initial electroencephalogram, laboratory tests Simplify antiepileptic drug (AED) regimen; change to low or carbohydrate-free formulation Dietitian consultation Education Days 2 to 3 When urine ketone level is 160 mg/dL, start ketogenic diet, 4:1 ratio, with one third of total calories using eggnog for 2 or 3 meals, then two thirds of total calories for 2 or 3 meals Stop fingerstick blood glucose checks. Days 3 to 4 First regular meal on 4:1 ratio Discharge—AED regimen B vitamins, sugar-free multivitamin Calcium supplements
1142
Epilepsy / 50
If there are any questions that the child may have an underlying metabolic disease that could be exacerbated by the initial fast, an appropriate evaluation should be done before initiating the diet. Valproate has been proved experimentally to reduce fasting ketonemia [Thurston et al., 1983; Turnbull et al., 1986]. Clinically, valproate has not impaired the ability to initiate the ketogenic diet and achieve adequate ketosis. The day before hospital admission, the parents are asked to eliminate carbohydrates from the child’s diet. The child eats foods that contain only protein or fat. After dinner, the child begins fasting with only noncaloric, noncaffeinated beverages given. On the first hospital day, a wake-and-sleep electroencephalogram may be obtained. Laboratory studies (i.e., complete blood cell count, platelet count, chemistry panel, and antiepileptic drug levels) are carried out before or at the time of admission. During this time, the child receives 75% of maintenance fluids and may have one caffeine-free diet drink per day. Blood glucose levels are checked every 4 hours. The dietitian uses this time to further review meal plans and the child’s food preferences and eating habits with the parents [Lasser and Brush, 1973]. When the concentration of urinary ketones reaches 60 to 80 mg/dL, the child is started on the ketogenic diet, using a 3:1 or 4:1 ratio (fat to protein plus carbohydrate), depending on the child’s age. Ketogenic eggnog is used for the initial feedings. The child receives three meals at one third of the total calories, is advanced as tolerated to two thirds of the total calories for three meals, and then eats his or her first full meal. If the child does not achieve maximum urinary ketone levels by 48 hours of fasting, the diet is begun. More prolonged fasting has not been considered helpful. Before discharge, the parents prepare their first ketogenic meal for their child under the supervision of the dietitian. At discharge, the parents have several meal plans for their child and are instructed to monitor the urinary ketone levels on a daily basis and record all seizures. Individual decisions are made during the hospital stay about whether the antiepileptic drug regimen will be simplified. The child is given a prescription for sugar-free multivitamin, mineral, and calcium supplementation and instructed to begin these at home. Vitamin B supplement is given to prevent optic nerve dysfunction [Hoyt and Billson, 1979]. Vitamin D and calcium supplementation prevents osteomalacia and decreased bone mass while on the ketogenic diet [Hahn et al., 1979]. Inadvertent administration of carbohydrates may occur when intercurrent illnesses are treated. Parents and pediatricians must appreciate that decongestants, antipyretics, and antibiotics are often formulated in carbohydrate-containing vehicles [Feldstein, 1996; Freeman et al., 2000; Lebel et al., 2001; McGhee et al., 2001]. The child is seen regularly for follow-up evaluations (Box 50-4). Special attention should be given to the serum albumin and total protein concentrations to make sure that the diet is providing enough protein. Cholesterol and triglyceride levels typically rise when the diet is started, but the diet may be continued unless the cholesterol level rises above 1000 mg/dL and consistently stays there. It is not known whether cholesterol-reducing drugs can be safely given while the child is maintained on the diet. It is not unusual to see minor elevations in the direct bilirubin level. Decisions regarding withdrawal of antiepileptic drugs
Box 50-4 KETOGENIC DIET MAINTENANCE One Month Neurologist, dietitian, nurse Adjust diet as needed Laboratory tests: complete blood cell count (CBC), platelets; SMA20; antiepileptic drug (AED) levels Urine calcium, creatinine Three, 6, and 12 Months Neurologist, dietitian, nurse Labs, CBC, platelets, SMA20 AED levels, if needed, and urine calcium, creatinine New meals Maintain for 2 years, seizure free Wean over 1 year 3.5-3 months → 3:1-3 months → 3.5-3 months → 2:1-3 months → Off
depend on the child’s response to the diet. At follow-up, the dietitian reviews parental concerns about implementing the diet and makes adjustments in the meal plan as necessary to maintain the child in maximum ketosis. If the child is in apparent maximum ketosis (i.e., urinary ketone levels are more than 160 mg/dL) and seizures recur, the problem may be an excess amount of calories, which may manifest as an excessive gain in weight. Lowering the total caloric intake (and carbohydrates) may help reduce the number of seizure recurrences. If the child is not in maximum ketosis, seizures may be caused by a break in the diet (e.g., “cheating,” medicine with sugar) or perhaps a lower than 4:1 ratio of fat to protein and carbohydrate. For children who can be successfully withdrawn from antiepileptic drug therapy and are seizure free for 2 years on the ketogenic diet (about 10% of treated children), an electroencephalogram is repeated, and the ketogenic diet is slowly withdrawn over 1 year. Many of these families elect to continue a low-carbohydrate diet, concerned that seizures may recur.
COMPLICATIONS Physicians should stress to parents that the diet is a form of medical therapy, and as such, although it is relatively safe, it is not without side effects [Ballaban-Gil et al., 1996; Wheless, 2001]. However, only 6% to 12% of patients discontinued the diet for medical reasons [Thompson et al., 1998; Vining et al., 1998]. Like antiepileptic drugs, the ketogenic diet has an adverse event profile, consisting of possible complications seen during initiation or maintenance (Boxes 50-5 and 50-6) [Wheless, 2001]. If the child has an unrecognized metabolic defect, a catastrophic event could occur during the fasting phase (see Box 50-2). Other adverse events can occur during the initial hospital stay, and if recognized, they are usually easily treated (see Box 50-5). A number of adverse events can occur during the maintenance phase. Many can be prevented with close monitoring,
Wheless / The Ketogenic Diet
Box 50-5 POSSIBLE ADVERSE EVENTS DURING INITIATION OF THE KETOGENIC DIET Adverse Events Dehydration Hypoglycemia Vomiting Monitoring and Treatment Strategy Encourage fluids (do not limit fluids to less than 75% of maintenance); use intravenous fluids if necessary (without dextrose). Check blood glucose levels every 6 hours until the diet is initiated. If the patient is symptomatic or blood glucose < 30 mg/dL, give orange juice. Screen for metabolic errors in advance. Use intravenous fluids; give orange juice.
Box 50-6 POSSIBLE ADVERSE EVENTS DURING MAINTENANCE OF THE KETOGENIC DIET Adverse Events Constipation, exacerbation of gastroesophageal reflux disease Poor growth Kidney stones Dyslipidemia, hyperlipidemia Prolonged QT interval, cardiomyopathy; excessive bruising; optic neuropathy; elevated levels of very-long-chain fatty acids Vitamin D deficiency, osteomalacia Trace mineral deficiencies Monitoring and Treatment Strategy Medical management may include the use of mineral oil and suppositories. Check albumin and total protein levels. Ensure adequate protein in diet. Monitor height and weight. Assess with renal ultrasonography. Analyze stone (specific treatment). Increase fluids and alkalinize urine. Check liver function test results and lipid profile; for sustained elevations of cholesterol or triglycerides, adjust diet or treat, or both. Assess with electrocardiography or echocardiography. Check selenium levels. Obtain complete blood cell and platelet counts. Supplement B vitamins. Check patient before ketogenic diet starts if problems clinically suspected. Supplement vitamin D, calcium, copper, selenium, and zinc. vitamin supplementation, and anticipatory treatment. The most common side effect encountered is constipation, which can be reduced if a calcium supplement with magnesium is given. Many of the children who begin the diet are already prone to this problem because of limited mobility, hypotonia, or spasticity. Constipation can be treated with regular doses of mineral oil, intermittent pediatric Fleet
1143
enemas, or milk of magnesia. Renal stones have occurred in less than 5% to 10% of patients and can usually be easily managed [Casey et al., 1999; Chesney et al., 1999; Freeman et al., 1994, 1996; Furth et al., 2000; Herzberg et al., 1990; Kaytal et al., 2000; Kielb et al., 2000; Kossoff et al., 2002; Maydell et al., 2001; Nordli et al., 2001]. The risk of stone formation is increased in younger patients (2 years of treatment) on the ketogenic diet.
ADVANTAGES AND DISADVANTAGES Advantages The ketogenic diet has several advantages compared with other medical therapies. Anecdotal reports have indicated that many of the children who are maintained on the diet are able to have their antiepileptic drugs decreased or withdrawn. This typically results in the child being more alert and exhibiting better behavior [Maydell et al., 2001; Nordli et al., 2001]. However, even children whose antiepileptic drugs cannot be substantially decreased or withdrawn may have marked behavioral or cognitive improvements [Katyal et al., 2000]. These improvements have occurred in children who have become seizure free on the diet and had antiepileptic drugs withdrawn and in those whose seizures are only minimally improved and have not had dramatic changes in their antiepileptic drug regimen. Parents are concerned about cognitive side effects, and although the newer antiepileptic drugs tend to have fewer such effects, there are no cognitive effects with the diet. A prospective, pilot study assessed the effects of the ketogenic diet on development and behavior in 65 children with intractable epilepsy [Pulsifer et al., 2001]. Formal evaluation of development, behavior, and parental stress using parental report measures was utilized before diet initiation and 1 year later. At follow-up, the mean developmental quotient indicated statistically significant improvement (P < 0.05), with significant behavioral improvements (P < 0.05) in attention and social functioning. The observed developmental and behavioral improvements were not statistically related to reductions in seizure frequency or antiepileptic medications. Parental stress was essentially unchanged. This preliminary report supports the prior anecdotal observations of the beneficial effects of the diet on cognition and behavior. Experiments in rats have discovered no adverse effect of the ketogenic diet on spatial learning and memory, the animal’s response to a novel environment, or a battery of behavioral tests [Bough et al., 2000b; Hori et al., 1997]. These reports of a positive cognitive effect of the diet in children and experimental models are in contrast to a single study of cognition in rats [Zhao et al., 2004] and one weight loss study in adults [Wing et al., 1995]. Twenty-three rats were fed a ketogenic diet for 1 month. These animals had a severe impairment in visual-spatial memory and decreased brain growth. Adults on the ketogenic diet for weight loss fared worse on some neurocognitive tasks than untreated control subjects [Wing et al., 1995]. These concerns have not been raised by any study of human beings but should be pursued in experimental and clinical research arenas [Snead, 2004]. With the ketogenic diet, there appear to be no concerns about organ failure or toxicity. For many families, the ketogenic diet provides a dramatic change in their role in the treatment of their children’s epilepsy. This form of therapy requires preparation by the parents and monitoring of urinary ketone levels. This requirement gives the parents an active role in the treatment of their children and a sense that what they are doing is influencing their children’s epilepsy and has a positive
Wheless / The Ketogenic Diet
psychosocial effect. Only occasionally can this become a disadvantage when children on the diet do not improve. Because the diet is totally provided by the parents, they may feel guilty, take the failure personally, and wonder if it is not something they have done wrong with the preparation of the diet that has kept it from working. In such instances, it is important to assure the parents that they have carried out the diet correctly, that the diet does not work in all children, and that they are not responsible for its failure. Rarely, even if the ketogenic diet is not working, parents may not want to stop it. The diet is the first therapy for their children’s seizures they are in charge of, and the parents may not want to lose this empowerment.
Disadvantages The most common reasons cited for discontinuation of the ketogenic diet are lack of efficacy, complications, noncompliance (more common in older children), and caregiver concerns [Lightstone et al., 2001]. The ketogenic diet is a strictly regulated medical diet that requires an epilepsy team for success. The team typically consists of a pediatric neurologist, dietitian, nurse, and social worker. The ketogenic diet requires active participation by the parents and children, if possible. The work required to initiate and maintain this rigorous diet by the parents may be considered a disadvantage. In the 1930s and 1940s the cost of the diet was considered a major disadvantage. However, at that time, the diet was compared with the cost of bromides or phenobarbital. Currently, the child with intractable epilepsy can incur costs of up to or more than $1000 per year for new antiepileptic drugs. A retrospective study of medical costs for 15 children with intractable epilepsy who were placed on the ketogenic diet found savings of more than $10,000 per child for the 1to 2-year period after initiation of the diet, compared with the same period before the diet [Mandel et al., 2002]. Successful maintenance on the ketogenic diet can provide a substantial financial benefit. Many physicians perceive the diet as unpalatable and difficult to initiate and maintain. However, modern nutritional labeling requirements and the use of computers allow the dietitian to construct a palatable diet with the patient’s food preferences in mind that permits a much more varied meal plan [Brake and Brake, 1997].
KETOGENIC DIET IN THE 21ST CENTURY More than 75 years have passed since the ketogenic diet was initially used, and many more therapies are now available for children with epilepsy. The ketogenic diet compares favorably with other new treatments that have been introduced to treat epilepsy in children [Felbamate Study Group, 1993; George, 1994; LeFever et al., 2000; Vagus Nerve Stimulation Study Group, 1995]. Studies on the newer antiepileptic drugs such as zonisamide, lamotrigine, tiagabine, gabapentin, topiramate, oxcarbazepine, and levetiracetam typically indicate that only 3% to 10% of all intractable patients achieve complete relief of seizures. One question remains unanswered: When in the course of therapy for a child with intractable epilepsy should
1145
the ketogenic diet be used? Currently, it is not used until children have failed multiple medications and are not considered surgical candidates. However, for some epilepsy syndromes, the diet should be offered as a treatment strategy after failure of one or two drugs. If the child has an epilepsy syndrome that is often resistant to current therapy, the ketogenic diet should be mentioned at the time of the initial therapeutic discussions as an alternative therapy if the seizures are not controlled on medication. This recommendation is especially appropriate for children who are not good candidates for epilepsy surgery or whose parents do not wish to have epilepsy surgery. Renewed interest in the ketogenic diet has again raised several research questions that, if answered, have the potential to improve our understanding of the neurochemistry of epilepsy and to allow better treatment of all patients with epilepsy [Nordli and DeVivo, 1997; Prasad et al., 1996]. In addition needing a better understanding of the underlying neurochemical changes induced with the ketogenic diet, other clinical questions remain. For example, for what seizure types or epilepsy syndromes does this diet have a greater chance of successful short- or long-term treatment? It would be helpful to have more long-term (i.e., 10 to 20 years) follow-up data on patients who appear not to have a return of seizures after the diet is stopped [Keith, 1963]. Issues that require investigation include the duration of treatment with the diet, the risk of late seizure recurrence after the diet is terminated, long-term effects of the diet on growth and development, and whether the response to treatment is because the patient has a specific subset of known seizure type or epilepsy syndrome. Feasibility of prolonged treatment also needs to be determined. Many children who are not seizure free or who are not able to discontinue all antiepileptic drugs are improved on the ketogenic diet. The improvement in seizure control or behavior and cognitive abilities is such that parents wish to continue the ketogenic diet. How long can we safely maintain these children on the ketogenic diet without encountering new side effects because of micronutrient deficiency? What is the feasibility of prolonged therapy? If no other therapy works better, how do we counsel parents about remaining on the diet when there is no apparent chance of withdrawing it? This same set of questions could be raised for a child who is seizure free on the diet for 2 years but then does not tolerate withdrawal without recurrence of seizures. The effects of the ketogenic diet on family dynamics are unknown. Are there different psychosocial effects on the siblings of the child with epilepsy who depends on this form of therapy? There are additional questions about the role of the ketogenic diet in treating less affected or normal children with epilepsy. How does the risk-benefit ratio of the ketogenic diet compare with other therapies? Many adults with intractable epilepsy wish to know if any of them could benefit from the ketogenic diet. The ketogenic diet also may be useful in other childhood neurologic disorders such as alternating hemiplegia of childhood or tumors of the nervous system [Nebeling et al., 1995]. The ketogenic diet is a therapy that started at the beginning of the 20th century and still appears to have a definitive role in the treatment of childhood epilepsy in the 21st century. The preferred sequence of treatments for
1146
Epilepsy / 50
children with epilepsy will continue to be reassessed and redefined. It will likely be several years before the exact roles for all current therapies are characterized. Until then, it is critical that those taking care of children with seizures be aware of all the treatment options and refer children whose seizures are not controlled to medical centers specializing in the care of such children [National Association of Epilepsy Centers, 1990]. For many of these children, the ketogenic diet continues to represent a therapeutic alternative. REFERENCES Aicardi J. Clinics in developmental medicine 115/118: Diseases of the nervous system in childhood. New York: MacKeith, 1992. Aicardi J. The international review of child neurology. In: Epilepsy in children, 2nd ed. New York: Raven Press, 1994. Al-Mudallal AS, LaManna JC, Lust WD, et al. Diet-induced ketosis does not cause cerebral acidosis. Epilepsia 1996;37:258. Al-Mudallal AS, Levin BE, Lust WD, et al. Effects of unbalanced diets on cerebral glucose metabolism in the adult rat. Neurology 1995;45:2261. Appleton DB, DeVivo DC. An experimental model for the effect of ketogenic diet on epilepsy. Proc Aust Assoc Neurologists 1973;10:75. Appleton DB, DeVivo DC. An animal model for the ketogenic diet. Epilepsia 1974;15:211. Ballaban-Gil K, Callahan C, O’Dell C, et al. Complications of the ketogenic diet. Ann Neurol 1996;40:307. Ballaban-Gil K, Callahan C, O’Dell C, et al. Complications of the ketogenic diet. Epilepsia 1998;39:744. Ballaban-Gil KR. Cardiomyopathy associated with the ketogenic diet. Epilepsia 1999;40 (Suppl 7):129. Barborka CJ. The ketogenic diet. Proc Meet Mayo Clin 1928a;3:273. Barborka CJ. Ketogenic diet treatment of epilepsy in adults. JAMA 1928b;91:73. Barborka CJ. The ketogenic diet and its use. Med Clin North Am 1929;12:1639. Barborka CJ. Epilepsy in adults: Results of treatment by ketogenic diet in one hundred cases. Arch Neurol Psychiatry 1930;23:904. Bastible C. The ketogenic treatment of epilepsy. Irish J Med Sci 1931;2:506. Bergqvist AGC, Chee C, Fink L, et al. Serial measurements of serum cholesterol and triglycerides in the ketogenic diet. Ann Neurol 1998;44:565. Bergqvist AGC, Chee CM, Bettler JE, et al. Zinc deficiency resulting from the ketogenic diet. Epilepsia 1999;40 (Suppl 7):133. Bergqvist AGC, Chee CM, Lutchka L, et al. Selenium deficiency associated with cardiomyopathy: A complication of the ketogenic diet. Epilepsia 2003;44:618. Berry-Kravis E, Booth G, Sanchez C, et al. The ketogenic diet: Need for carnitine supplementation. Ann Neurol 1998;44:566. Berry-Kravis E, Booth G, Taylor A, et al. Bruising and the ketogenic diet: Evidence for diet-induced changes in platelet function. Ann Neurol 2001a;49:98. Berry-Kravis E, Booth G, Sanchez, AC, et al. Carnitine levels and the ketogenic diet. Epilepsia 2001b;42:1445. Best TH, Franz DN, Gilbert DL, et al. Cardiac complications in pediatric patients on the ketogenic diet. Neurology 2000;54:2328. Bible, The New King James Version, Mark 9:14-29. Carmel, NY: Guideposts, 1982. Bough K, Chen R, Eagles D. Path analysis shows that increasing ketogenic diet ratio but not beta-hydroxybutyrate, elevates seizure threshold in the rat. Dev Neurosci 1999a;21:400. Bough KJ, Eagles DA. A ketogenic diet increases the resistance to pentylenetetrazole-induced seizures in the rat. Epilepsia 1999b;40:138. Bough KJ, Valiyil R, Han FT, et al. Seizure resistance is dependent upon age and caloric restriction in rats fed a ketogenic diet. Epilepsy Res 1999c;35:21. Bough KJ, Matthews PJ, Eagles DA. A ketogenic diet has different effects upon seizures induced by maximal electroshock and by pentylenetetrazole infusion. Epilepsy Res 2000a;38:105. Bough KJ, Yao SG, Eagles DA. Higher ketogenic diet ratios confer protection from seizures without neurotoxicity. Epilepsy Res 2000b;38:15. Bough KJ, Gudi K, Han FT, et al. An anticonvulsant profile of the ketogenic diet in the rat. Epilepsy Res 2002;50:313.
Bough KJ, Schwartzkroin PA, Rho JM. Calorie restriction and ketogenic diet diminish neuronal excitability in rat dentate gyrus in vivo. Epilepsia 2003;44:752. Bough KJ, Stafstrom CE. The ketogenic diet: Scientific principles underlying its use. In: Rho JM, Sankar R, Cavazos JE, eds. Epilepsy: Scientific foundations of clinical practice. New York: Marcel Dekker, 2004:263. Bower BD. Epilepsy in childhood and adolescence. In: Tyrer JG, ed. Current status of modern therapy: The treatment of epilepsy, Vol. 5. Philadelphia: JB Lippincott, 1980. Brake D, Brake C. The ketogenic cookbook. Gilman, Conn: Pennycorner Press, 1997. Bridge EM. Epilepsy and convulsive disorders in children. New York: McGraw-Hill, 1949. Bridge EM, Lob LV. The mechanism of the ketogenic diet in epilepsy. Bull Johns Hopkins Hosp 1931;48:373. Brown L, Lutchka LM, Bergqvist C, et al. Monitoring betahydroxybutyrate as an anti-convulsant level in the ketogenic diet. Epilepsia 1998;39 (Suppl 6):168. Cahill GF. Starvation. Trans Am Clin Climatol Assoc 1982;94:1. Casey JC, McGrogan J, Pillas D. The implementation and maintenance of the ketogenic diet in children. J Neurosci Nurs 1999;31:294. Charlie Foundation to Help Cure Pediatric Epilepsy. An Introduction to the ketogenic diet—a treatment for pediatric epilepsy. Videotape. Santa Monica, Calif: Charlie Foundation, 1994a. Charlie Foundation to Cure Epilepsy. The ketogenic diet—doctor’s version. Videotape. Santa Monica, Calif: Charlie Foundation, 1994b. Chee CM, Lutchka L, Brown L, et al. Ketogenic diet: Unrecognized selenium deficiency. Epilepsia 1998;39 (Suppl 6):228. Cheng CM, Hicks K, Wang J, et al. Caloric restriction augments brain glutamic acid decarboxylase-65 and -67 expression. J Neurosci Res 2004;77:270. Chesney D, Brouhard BH, Wyllie E, et al. Biochemical abnormalities of the ketogenic diet in children. Clin Pediatr 1999;38:107. Conklin HW. Cause and treatment of epilepsy. J Am Osteopath Assoc 1922;22:11. Cooder HR. Epilepsy in children with particular reference to the ketogenic diet. Calif West Med 1933;39:169. Cooper JR, Bloom FE, Roth RH. Amino acid transmitters. In: The biochemical basis of neuropharmacology. New York: Oxford Press, 1996. Couch SC, Schwarzman F, Carroll J, et al. Growth and nutritional outcomes of children treated with the ketogenic diet. J Am Diet Assoc 1999;99:1573. Cremer JE. Incorporation of label from D-beta-hydroxy(14C) butyrate and [3-14C) acetoacetate into amino acids in rat brain in vivo. Biochem J 1971;122:135. Dahlquist G, Persson U, Persson B. The activity of D-betahydroxybutyrate dehydrogenase in fetal, infant, and adult rat brain and the influence of starvation. Biol Neonate 1972;20:40. Dahlquist G, Persson B. The rate of cerebral utilization of glucose, ketone bodies, and oxygen: A comparative in vivo study of infant and adult rats. Pediatr Res 1976;10:910. Dekaban AS. Plasma lipids in epileptic children treated with the high fat diet. Arch Neurol 1966;15:177. Dell CA, Likhodii SS, Musa K, et al. Lipid and fatty acid profiles in rats consuming different high-fat ketogenic diets. Lipids 2001;36:373. DeLorey TM, Olsen RW. GABA and glycine. In: Siegel GJ, Agranoff BW, Albers RW, et al., eds. Basic neurochemistry. New York: Raven Press, 1994. Demeritte EL, Coyne M, Ventimiglia J, et al. Electroencephalographic analysis in the ketogenic diet. Ann Neurol 1996a;40:305. Demeritte EL, Ventimiglia J, Coyne M, et al. Organic acid disorders and the ketogenic diet. Ann Neurol 1996b;40:305. DeVivo DC. The effects of ketone bodies on glucose utilization. In: Passoneau JV, Lust WD, Hawkins JR, et al., eds. Cerebral metabolism and neural function. Baltimore: Williams and Wilkins, 1980:243. DeVivo DC. How to use other drugs (steroids) and the ketogenic diet. In: Morselli PL, Pippenger CE, Penry JK, eds. Antiepileptic drug therapy in pediatrics. New York: Raven Press, 1983. DeVivo DC, Leckie MP, Ferrendelli JS, et al. Chronic ketosis and cerebral metabolism. Ann Neurol 1978;3:331. DeVivo DC, Malas KL, Leckie MP. Starvation and seizures: Observations on the electroconvulsive threshold and cerebral metabolism of the starved adult rat. Arch Neurol 1975;32:755.
Wheless / The Ketogenic Diet DeVivo DC, Pagliara AS, Prensky AL. Ketotic hypoglycemia and the ketogenic diet. Neurology 1973;23:640. DeVivo DC, Trifiletti RR, Jacobson RI, et al. Glucose transport across the blood-brain barrier as a cause of persistent hypoglycorrhachia, seizures and developmental delay. N Engl J Med 1991;325:703. DiMario FJ, Holland J. The ketogenic diet: A review of the experience at Connecticut Children’s Medical Center. Pediatr Neurol 2002;26:288. Dodson WE, Prensky AL, DeVivo DC, et al. Management of seizure disorders. Selected aspects, part II. J Pediatr 1976;89:695. Eley RC. Epilepsy. The value of encephalography in the selection of patients for treatment by the ketogenic diet. J Pediatr 1933;3:359. Erecinska M, Nelson D, Daikhin Y, et al. Regulation of GABA level in rat brain synaptosomes: Fluxes through enzymes of the GABA shunt and effects of glutamate, calcium, and ketone bodies. J Neurochem 1996;67:2325. Erickson JC, Jabbari B, Difazio MP. Basal ganglia injury as a complication of the ketogenic diet. Mov Disord 2003;18:448. Felbamate Study Group in Lennox-Gastaut Syndrome. Efficacy of felbamate in childhood epileptic encephalopathy (Lennox-Gastaut syndrome). N Engl J Med 1993;328:29. Feldstein TJ. Carbohydrate and alcohol content of 200 oral liquid medications for use in patients receiving ketogenic diets. Pediatrics 1996;97:506. Fischer L. Epilepsy: Its treatment by the use of the ketogenic diet versus drugs. Arch Pediatr 1935;52:131. Fisher RS, Parks-Trusz SL, Lehman C. Social issues in epilepsy. In: Shorvon S, Dreifuss F, Fish D, et al., eds. The treatment of epilepsy. Woburn, Mass: Blackwell Science, 1996. Fraser DD, Witing S, Andrew RD, et al. Elevated polyunsaturated fatty acids in blood obtained from children on the ketogenic diet. Neurology 2003;60:1026. Freeman JM, Freeman JB, Kelly MT. The ketogenic diet, 3rd ed. New York: Demos, 2000. Freeman JM, Kelly MT, Freeman JB. The epilepsy diet treatment: An introduction to the ketogenic diet. New York: Demos, 1994. Freeman JM, Vining EPG. Seizures decrease rapidly after fasting: Preliminary studies of the ketogenic diet. Arch Pediatr Adolesc Med 1999;153:946. Freeman JM, Vining EPG, Pillas DJ. Seizures and epilepsy in childhood: A guide for parents. Baltimore: Johns Hopkins University Press, 1990. Freeman JM, Vining EPG, Pillas DJ, et al. The efficacy of the ketogenic diet—1998: A prospective evaluation of intervention in 150 children. Pediatrics 1998a;102:1358. Freeman JM, Vining EPG, Pyzik PL, et al. Beta-hydroxybutyrate levels in blood correlate with seizure control in children on the ketogenic diet. Epilepsia 1998b;39 (Suppl 6):167. Freeman JM, Kelly MT, Freeman JB. The epilepsy diet treatment. New York: Demos, 1996. Furth SL, Casey JC, Pyzik PL, et al. Risk factors for urolithiasis in children on the ketogenic diet. Pediatr Nephrol 2000;15:125. George R, Salinsky M, Kuzniecky R, et al. Vagus nerve stimulation for treatment of partial seizures. 3. Long-term follow-up on the first 67 patients exiting a controlled study. Epilepsia 1994;35:637. Geyelin HR. Fasting as a method for treating epilepsy. Med Rec 1921;99:1037. Gilbert DL, Pyzik PL, Freeman JM. The ketogenic diet: Seizure control correlates better with serum beta-hydroxybutyrate than with urine ketones. J Child Neurol 2000;15:787. Gjedde A, Crone C. Induction processes in blood-brain transfer of ketone bodies during starvation. Am J Physiol 1975;229:1165. Goodwell W, Chez MG, Buchana CP, et al. Bone marrow suppression from copper deficiency in 2 patients on the ketogenic diet. Ann Neurol 1998;44:568. Goyens P, DeLaet C, Ranguelov N, et al. Pitfalls of the ketogenic diet in a neonate. Pediatrics 2002;109:1185. Greene AE, Todorova MT, McGowan R, et al. Caloric restriction inhibits seizure susceptibility in epileptic EL mice by reducing blood glucose. Epilepsia 2001;42:1371. Greene AE, Todorova MT, Seyfried TN. Perspectives on the metabolic management of epilepsy through dietary reduction of glucose and elevation of ketone bodies. J Neurochem 2003;86:529. Haas RE, Rice MA, Trauner DA, et al. Therapeutic effects of a ketogenic diet in Rett syndrome. Am J Med Genet 1986;1:225. Hahn TJ, Halstead LR, DeVivo DC. Disordered mineral metabolism produced by ketogenic diet therapy. Calcif Tissue Int 1979;28:17.
1147
Harik SI, Al-Mudallal AS, LaManna JC, et al. Ketogenic diet and the brain. Ann N Y Acad Sci 1997;835:218. Hassan AM, Keene DL, Whiting SE, et al. Ketogenic diet in the treatment of refractory epilepsy in childhood. Pediatr Neurol 1999;21:548. Hauser WA. The prevalence and incidence of convulsive disorders in children. Epilepsia 1994;35:S1. Hauser WA, Hesdorffer DH. Epilepsy: Frequency, causes and consequences. New York: Demos Press, 1980. Hawkins RA, Biebuyck JF. Ketone bodies are selectively used by individual brain regions. Science 1979;205:325. Hawkins RA, Biebuyck JF. Regional brain utilization of ketone bodies. In: Passoneau JV, Lust WD, Hawkins JR, et al., eds. Cerebral metabolism and neural function. Baltimore: Williams and Wilkins, 1980: 255. Hawkins RA, Williamson DH, Krebs HA. Ketone-body utilization by adult and suckling rat brain in vivo. Biochem J 1971;122:13. Haymond MW, Howard C, Ben-Galim E, et al. Effects of ketosis on glucose flux in children and adults. Am J Physiol 1983;245:E373. Heller AJ, Stewart J, Hughes E, et al. Comparative efficacy and toxicity of phenobarbital, phenytoin, carbamazepine, and valproate in adults and children with newly diagnosed previously untreated epilepsy: A randomized long-term trial. Epilepsia 1993;34:66. Helmholz HF. The treatment of epilepsy in childhood: Five years experience with the ketogenic diet. JAMA 1927;88:2028. Helmholz HF, Goldstein M. Results of 15 years’ experience with the ketogenic diet in the treatment of epilepsy in children. Proc Staff Meet Mayo Clinic 1937;12:433. Helmholz HF, Keith HM. Eight years’ experience with the ketogenic diet in the treatment of epilepsy. JAMA 1930;95:707. Helmholz HF, Keith HM. Ten years’ experience in the treatment of epilepsy with the ketogenic diet. Arch Neurol Psychiatry 1932;29:808. Hemingway C, Freeman JM, Pillas DJ, et al. The ketogenic diet: A 3- to 6-year follow-up of 150 children enrolled prospectively. Pediatrics 2001;108:898. Hendricks M. High fat and seizure free. Johns Hopkins Magazine 1995;April:14. Herzberg GZ, Fivush BA, Kinsman SL, et al. Urolithiasis associated with the ketogenic diet. J Pediatr 1990;117:743. Hopkins IJ, Lynch BC. Use of ketogenic diet in epilepsy in childhood. Aust Pediatr J 1970;6:25. Hori A, Tandon P, Holmes GL, et al. Ketogenic diet: Effects on expression of kindled seizures and behavior in adult rats. Epilepsia 1997;38:750. Hoyt CS, Billson FA. Optic neuropathy in ketogenic diet. Br J Ophthalmol 1979;63:191. Huttenlocher PR. Ketonemia and seizures: Metabolic and anticonvulsant effects of two ketogenic diets in childhood epilepsy. Pediatr Res 1976;10:536. Janaki S, Rashid MD, Gulati MS, et al. A clinical electroencephalographic correlation of seizures on a ketogenic diet. Indian J Med Res 1976;64:1057. Kaytal NG, Koehler AN, McGhee B, et al. The ketogenic diet in refractory epilepsy: The experience of Children’s Hospital of Pittsburgh. Clin Pediatr 2000;39:153. Keith HM. Results of treatment of recurring convulsive attacks of epilepsy. Am J Dis Child 1942;74:140. Keith HM. Convulsive disorders in children: With reference to treatment with ketogenic diet. Boston: Little, Brown, 1963. Kielb S, Koo HP, Bloom DA, et al. Nephrolithiasis associated with the ketogenic diet. J Urol 2000;164:464. Kinsman SL, Vining EPG, Quaskey SA, et al. Efficacy of the ketogenic diet for intractable seizure disorders: Review of 58 cases. Epilepsia 1992;33:1132. Kleinman RE, ed. The ketogenic diet. Pediatric nutrition handbook, 5th ed. Chicago: American Academy of Pediatrics, 2004:773. Klepper J, Diefenbach S, Kohlschutter A, et al. Effects of the ketogenic diet in the glucose transporter 1 deficiency syndrome. Prostaglandins Leukot Essent Fatty Acids 2004;70:321. Klepper J, Leiendecker B, Bredahl R, et al. Introduction of a ketogenic diet in young infants. J Inherit Metab Dis 2002;25:449. Kossoff EH, Krauss GL, McGrogan JR, et al. Efficacy of the Atkins diet as therapy for intractable epilepsy. Neurology 2003;61:1789. Kossoff EH, Pyzik PL, McGrogan JR, et al. Efficacy of the ketogenic diet for infantile spasms. Pediatrics 2002;109:780. Kraus H, Schlenker S, Schwedesky D. Developmental changes of cerebral ketone body utilization in human infants. Hoppe Seylers Z Physiol Chem 1974;355:164.
1148
Epilepsy / 50
Lamers KJB, Gabreels FJM, Renier WO, et al. Fasting studies in cerebrospinal fluid and blood in children with epilepsy of unknown origin. Epilepsy Res 1995;21:59. Lasser JL, Brush MK. An improved ketogenic diet for treatment of epilepsy. J Am Diet Assoc 1973;62:281. Lebel D, Morin C, Laberge M, et al. The carbohydrate and caloric content of concomitant medications for children with epilepsy on the ketogenic diet. Can J Neurol Sci 2001;28:232. Lefevre F, Aronson N. Ketogenic diet for the treatment of refractory epilepsy in children: A systematic review of efficacy. Pediatrics 2000;105. Available at http://www.pediatrics.org/cgi/content/full/ 105/4/e46. Leino RL, Gerhart DZ, Duelli R, et al. Diet-induced ketosis increases monocarboxylate transporter (MCT1) levels in rat brain. Neurochem Int 2001;38:519. Lennox WG. Ketogenic diet in the treatment of epilepsy. N Engl J Med 1928;199:74. Lennox WG. Science and seizures: New light on epilepsy and migraine. New York: Harper, 1941. Lennox WG, Cobb S. Studies in epilepsy. VIII. The clinical effect of fasting. Arch Neurol Psychiatry 1928;20:771. Lennox WG, Lennox MA. Epilepsy and related disorders, Vol. 2. Boston: Little, Brown, 1960. Levy R, Cooper P. Ketogenic diet for epilepsy. Cochrane Database Syst Rev 2003;3:CD001903. Liebhaber GM, Riemann E, Baumeister FA. Ketogenic diet in Rett syndrome. J Child Neurol 2003;18:74. Lightstone L, Shinnar S, Callahan CM, et al. Reasons for failure of the ketogenic diet. J Neurosci Nurs 2001;36:292. Likhodii SS, Musa K, Mendonca A, et al. Dietary fat, ketosis, and seizure resistance in rats on the ketogenic diet. Epilepsia 2000;41:1400. Likhodii SS, Burnham WM. Ketogenic diet: Does acetone stop seizures? Med Sci Monit 2002;8:HY19. Lin M, Mitchell WG, Chen LS, et al. Symptomatic carnitine depletion is uncommon in children on ketogenic diet. Epilepsia 1998; 39 (Suppl 6):168. Liu YM, William S, Basualdo-Hammond C, et al. A prospective study: Growth and nutritional status of children treated with the ketogenic diet. J Am Diet Assoc 2003;103:707. Livingston S. The diagnosis and treatment of convulsive disorders in children. Springfield, Ill: Charles C Thomas, 1954. Livingston S. Living with epileptic seizures. Springfield, Ill: Charles C Thomas, 1963. Livingston S. Comprehensive management of epilepsy in infancy, childhood and adolescence. Springfield, Ill: Charles C Thomas, 1972. Livingston S, Pauli LL. Ketogenic diet and epilepsy. Dev Med Child Neurol 1975;17:818. Livingston S, Pauli LL, Pruce I. Ketogenic diet in the treatment of childhood epilepsy. Dev Med Child Neurol 1977;19:833. Mady MA, Kossoff EH, McGregor AL, et al. The ketogenic diet: Adolescents can do it, too. Epilepsia 2003;44:847. Mandel A, Ballew M, Pina-Garza JE, et al. Medical costs are reduced when children with intractable epilepsy are successfully treated with the ketogenic diet. J Am Diet Assoc 2002;102:396. Maria BL, Borum PR, Friedman T, et al. The ketogenic diet. In: Maria BL, ed. Consensus in child neurology. Hamilton, Ontario: Decker Periodicals, 1997. Marks WJ, Vermathen P, Sum JM, et al. Brain pH in humans treated with the ketogenic diet. Neurology 1997;48:A111. Maydell BV, Wyllie E, Akhtar N, et al. Efficacy of the ketogenic diet in focal versus generalized seizures. Pediatr Neurol 2001;25:208. Mayes PA. Integration of metabolism and the provision of tissue fuels. In: Murray RK, Granner DK, Mayes PA, et al., eds. Harper’s biochemistry, 24th ed. Stamford, Conn: Appleton and Lange, 1996a. Mayes PA. Oxidation of fatty acids: Ketogenesis. In: Murray RK, Granner DK, Mayes PA, et al., eds. Harper’s biochemistry, 24th ed. Stamford, Conn: Appleton & Lange, 1996b. McGeer PL, McGeer EG. Amino acid neurotransmitters. In: Siegel GJ, Agranoff BW, Albers RW, et al., eds. Basic neurochemistry. New York: Raven Press, 1989. McGhee B, Katyal N. Avoid unnecessary drug-related carbohydrates for patients consuming the ketogenic diet. J Am Diet Assoc 2001;101:87. McQuarrie I, Keith HM. Epilepsy in children. Am J Dis Child 1927;34:1013.
Melvin JJ, Legido A, Faerber EN, et al. Pyruvate dehydrogenase complex deficiency associated with brain dysgenesis: Response of lactic acidemia to a ketogenic diet. Neurology 1996;46:A114. Millichap, JG, Jones JD, Rudis BP. Mechanism of anticonvulsant action of ketogenic diet. Am J Dis Child 1964;107:593. Moore T, Lione A, Sugden M, Regen D. Hydroxybutyrate transport in rat brain: Developmental and dietary modification. Am J Physiol 1976;230:619. Muller-Schwarze AB, Tandon P, Liu Z, et al. Ketogenic diet reduces spontaneous seizures and mossy fiber sprouting in the kainic acid model. Neuroreport 1999;10:1517. National Association of Epilepsy Centers. The National Association of Epilepsy Centers Guidelines for diagnosis and treatment in specialized epilepsy centers. Epilepsia 1990;31:1. Nakazawa M, Kodama S, Matsuo T. Effects of ketogenic diet on electroconvulsive threshold and brain contents of adenosine nucleotides. Brain Dev 1983;5:375. NBC Dateline. The ketogenic diet. October 26, 1994. Nebeling LC, Miraldi F, Shurin SB, et al. Effects of a ketogenic diet on tumor metabolism and nutritional status in pediatric oncology patients: Two case reports. J Am Coll Nutr 1995;14:202. Nehlig A. Age-dependent pathways of brain energy metabolism: The suckling rat, a natural model of the ketogenic diet. Epilepsy Res 1999;37:211. Nellhaus G. The ketogenic diet reconsidered: Correlation with EEG. Neurology 1971;21:424. Nordli DR. The ketogenic diet: Uses and abuses. Neurology 2000; 58 (Suppl 7):S21. Nordli DR Jr, DeVivo DC. The ketogenic diet revisited: Back to the future. Epilepsia 1997;38:743. Nordli DR, Kuroda MM, Carroll J, et al. Experience with the ketogenic diet in infants. Pediatrics, 2001;108:129. Notkin J. Epilepsy: Treatment of institutionalized adult patients with a ketogenic diet. Arch Neurol Psychiatry 1934;31:787. Owen OE, Morgan AP, Kemp HG, et al. Brain metabolism during fasting. J Clin Invest 1967;46:1589. Pan J, Bebin E, Chu W, et al. Ketosis and epilepsy: 31P spectroscopic imaging at 4.1 T. Epilepsia 1999;40:703. Pan JW, Rothman DL, Behar KL, et al. Human brain betahydroxybutyrate and lactate increase in fasting-induced ketosis. J Cereb Blood Flow Metab 2000;20:1502. Pan JW, Telang FW, Lee JH, et al. Measurement of beta-hydroxybutyrate in acute hyperketonemia in human brain. J Neurochem 2001;79:539. Patsalos PN, Duncan JS. Antiepileptic drugs: A review of clinically significant drug interactions. Drug Safety 1993;9:156. Pellerin L, Pellegri G, Martin J-L, et al. Expression of monocarboxylate transporter mRNAs in mouse brain: Support for a distinct role of lactate as an energy substrate for the neonatal vs. adult brain. Proc Natl Acad Sci U S A 1998;95:3990. Pellock JM. Seizures and epilepsy in infancy and childhood. Neurol Clin 1993;3:755. Pellock JM. Antiepileptic drug therapy in the United States: A review of clinical studies and unmet needs. Neurology 1995;45:S17. Pellock JM. Utilization of new antiepileptic drugs in children. Epilepsia 1996;37:S66. Pellock JM, Pippenger CE. Adverse effects of antiepileptic drugs. In: Dodson WE, Pellock JM, eds. Pediatric epilepsy: Diagnosis and therapy. New York: Demos, 1993. Penfield W, Erickson TC. Epilepsy and cerebral localization. A study of the mechanism, treatment and prevention of epileptic seizures. Baltimore: Charles C Thomas, 1941. Peng L, Hertz L, Huang R, et al. Utilization of glutamine and of TCA cycle constituents as precursors for transmitter glutamate and GABA. Dev Neurosci 1993;15:367. Persson B, Settergress G, Dahlquist G. Cerebral arterio-venous difference of acetoacetate and D-beta-hydroxybutyrate in children. Acta Paediatr Scand 1972;61:273. Peterman MG. The ketogenic diet in epilepsy. JAMA 1925;84:1979. Peyron R, LeBars D, Cinotti L, et al. Effects of GABAA receptor activation on brain glucose metabolism in normal subjects and temporal lobe epilepsy (TLE) patients. A positron emission tomography (PET) study. Part I. Brain glucose metabolism is increased after GABAA receptor activation. Epilepsy Res 1994;19:45. Prasad AN, Stafstrom CF, Holmes GL. Alternative epilepsy therapies: The ketogenic diet, immunoglobulins, and steroids. Epilepsia 1996;37:S81.
Wheless / The Ketogenic Diet Pulford DS. The present status of the ketogenic diet. Ann Intern Med 1932;6:795. Pulsifer MB, Gordon JM, Brandt J, et al. Effects of ketogenic diet on development and behavior: Preliminary report of a prospective study. Dev Med Child Neurol 2001;43:301. Rho J, Kim D, Robbins C, et al. Age-dependent differences in flurothyl seizure sensitivity in mice treated with a ketogenic diet. Epilepsy Res 1999a;37:233. Rho JM, Shin DH, Robbins CA, et al. GABA levels are increased in the hippocampus of mature mice fed a ketogenic diet. Epilepsia 1999b;40 (Suppl 7):161. Rho JM, Szot P, Tempel BL, et al. Developmental seizure susceptibility of Kv1.1 potassium channel knockout mice. Dev Neurosci 1999c;21:320. Rho JM, Robbins CA, Wenzel J, et al. An experimental ketogenic diet promotes long-term survival and reduces synaptic reorganization in the hippocampus of epileptic Kv1.1 null mutant mice. Epilepsia 2000;41 (Suppl 7):34. Rho JM, Anderson GD, Donevan SD, et al. Acetoacetate, acetone, and dibenzylamine (a contaminant in L-(+)-beta-hydroxybutyrate) exhibit direct anticonvulsant actions in vivo. Epilepsia 2002;43:358. Rodwell VW. Conversion of amino acids to specialized product. In: Murray RK, Granner DK, Mayes PA, et al., eds, Harper’s biochemistry, 24th ed. Stamford, Conn: Appleton & Lange, 1996. Roe CR, Coates PM. Mitochondrial fatty acid oxidation disorders. In: Scriver CR, Beaudet AL, Sly WS, et al., eds. The metabolic and molecular basis of inherited disease. New York: McGraw-Hill, 1995:1501. Ross DL, Swaiman KF, Torres F, et al. Early biochemical and EEG correlates of the ketogenic diet in children with atypical absence epilepsy. Pediatr Neurol 1985;1:104. Schneider KS, Wagner J. Recipe for hope. People Magazine 1995; April 17:54. Schwartz RM, Boyes S, Aynsley-Green A. Metabolic effects of three ketogenic diets in the treatment of severe epilepsy. Dev Med Child Neurol 1989a;31:152. Schwartz RH, Eaton J, Bower BD, et al. Ketogenic diets in the treatment of epilepsy: Short term clinical effects. Dev Med Child Neurol 1989b;31:145. Schwartzkroin PA. Mechanisms underlying the anti-epileptic efficacy of the ketogenic diet. Epilepsy Res 1999;37:171. Seymour KJ, Bluml S, Sutherling J, et al. Identification of cerebral acetone by 1H-MRS in patients with epilepsy controlled by ketogenic diet. MAGMA 1999;8:33. Shafrir Y, Prensky AL. Acquired epileptiform opercular syndrome: A second case report, review of the literature, and comparison to the Landau-Kleffner syndrome. Epilepsia 1995;36:1050. Sirven J, Whedon B, Caplan D, et al. The ketogenic diet for intractable epilepsy in adults: Preliminary results. Epilepsia 1999;40:1721. Snead OC III. The ketogenic diet: A cautionary note. Pediatr Res 2004;55:368. Sokoloff L. Metabolism of ketone bodies by the brain. Annu Rev Med 1973;24:271. Stafstrom CE. Animal models of the ketogenic diet: What have we learned, what can we learn? Epilepsy Res 1999;37:241. Stafstrom CE, Spencer S. The ketogenic diet: A therapy in search of an explanation. Neurol 2000;54:282. Stafstrom CE, Bough KJ. The ketogenic diet for the treatment of epilepsy: A challenge for nutritional neuroscientists. Nutr Neurosci 2003;6:67. Stafstrom CE, Rho JM, eds. Epilepsy and the ketogenic diet. Totowa, NJ: Humana Press, 2004. Stafstrom CE, Wang C, Jensen FE. Electrophysiological observations in hippocampal slices from rats treated with the ketogenic diet. Dev Neurosci 1999;21:393. Stewart WA, Gordon K, Camfield P. Acute pancreatitis causing death in a child on the ketogenic diet. J Child Neurol 2001;16:682. Su SW, Cilio MR, Sogawa Y, et al. Timing of the ketogenic diet initiation in an experimental epilepsy model. Dev Brain Res 2000;125:131. Swink T, Vining E, Casey, et al. Efficacy of the ketogenic diet in children under 2 years of age. Epilepsia 1997a;38:26. Swink TD, Vining EPG, Freeman JM. The ketogenic diet: 1997. Adv Pediatr 1997b;44:297. Szot P, Weinshenker D, Rho JM, et al. Norepinephrine is required for the anticonvulsant effect of the ketogenic diet. Dev Brain Res 2001;129:211. Takeoka M, Riviello JJ, Pfeifer H, et al. Concomitant treatment with topiramate and ketogenic diet in pediatric epilepsy. Epilepsia 2002;43:1072.
1149
Talbot FB, Metcalf K, Moriarty M. The ketogenic diet in the treatment of idiopathic epilepsy. Am J Dis Child 1926;32:316. Thavendiranathan P, Mendonca A, Dell C, et al. The MCT ketogenic diet: Effects on animal seizure models. Exp Neurol 2000;161:696. Thavendiranathan P, Chow C, Cunnane S, et al. The effect of the ‘classic’ ketogenic diet on animal seizure models. Brain Research 2003;959:206. Theda C, Woody RC, Naidu S, et al. Increased very long chain fatty acids in patients on a ketogenic diet: A cause of diagnostic confusion. J Pediatr 1993;122:724. Thio LL, Wang M, Yamada KA. Ketone bodies do not directly alter excitatory or inhibitory hippocampal synaptic transmission. Neurology 2000;54:325. Thompson JA, Van Orman CB, Peterson P. Ketogenic diet: Long-term efficacy and patient tolerance in the treatment of efficacy and patient tolerance in the treatment of intractable pediatric epilepsy. Epilepsia 1998;39 (Suppl 6):167. Thurston JH, Carroll JE, Dodson WE, et al. Chronic valproate administration reduces fasting ketonemia in children. Neurology 1983;33:1348. Todorova MT, Tandon P, Madore RA, et al. The ketogenic diet inhibits epileptogenesis in EL mice: A genetic model for idiopathic epilepsy. Epilepsia 2000;41:933. Turnbull DM, Dick DJ, Wilson L, et al. Valproate causes metabolic disturbance in normal man. J Neurol Neurosurg Psychiatry 1986;49:405. Uhlemann ER, Neims AH. Anticonvulsant properties of the ketogenic diet in mice. J Pharmacol Exp Ther 1972;180:231. Vagus Nerve Stimulation Study Group. A randomized controlled trial of chronic vagus nerve stimulation for treatment of medically intractable seizures. Neurology 1995;45:224. Vining EPG, Freeman JM, Ballaban-Gil K, et al. Multi-center study of the efficacy of the ketogenic diet. Arch Neurol 1998;55:1433. Vining EPG, Freeman JM, Kwiterovich P, et al. The ketogenic diet induces dyslipidemia. Epilepsia 1999a;40 (Suppl 7):122. Vining EPG. Clinical efficacy of the ketogenic diet. Epilepsy Res 1999b;37:181. Vininig EPG, Pyzik P, McGrogan J, et al. Growth of children on the ketogenic diet. Dev Med Child Neurol 2002;44:796. Wang ZJ, Bergqvist C, Hunter JV, et al. In vivo measurement of brain metabolites using two-dimensional double-quantum MR spectroscopyexploration of GABA levels in a ketogenic diet. Magn Reson Med 2003;49:615. Weber TA, Antognetti R, Stacpoole PW. Caveats when considering ketogenic diets for the treatment of pyruvate dehydrogenase complex deficiency. J Pediatr 2001 138:390. Weeks DF, Renner DS, Allen FM, et al. Observations on fasting and diets in the treatment of epilepsy. J Metab Res 1923;3:317. Wexler ID, Hemalatha SG, McConnell J, et al. Outcome of pyruvate dehydrogenase deficiency treated with ketogenic diet. Neurology 1997;49:1655. Wheless JW. The epilepsy diet treatment: An introduction to the ketogenic diet, book review. J Child Neurol 1995a;10:489. Wheless JW. The ketogenic diet: Fa(c)t or fiction. J Child Neurol 1995b;10:419. Wheless JW. The ketogenic diet: An effective medical therapy with side-effects. J Child Neurol 2001;16:633. Wheless JW. History and origin of the ketogenic diet. In: Stafstrom CE, Rho JM, eds. Epilepsy and the ketogenic diet. Totowa, NJ: Humana Press, 2004:31. Wijburg FA, Barth PG, Bindoff LA, et al. Leigh syndrome associated with a deficiency of the pyruvate dehydrogenase complex: Results of treatment with a ketogenic diet. Neuropediatrics 1992;23:147. Wilder RM. The effects of ketonuria on the course of epilepsy. Bull Mayo Clin 1921;2:307. Wilder RM, Pollack H. Ketosis and the ketogenic diet: Their application to treatment of epilepsy and infections of the urinary tract. Int Clin 1935;1:1. Wilkins L. Epilepsy in childhood. III. Results with the ketogenic diet. J Pediatr 1937;10:341. Williams S, Basualdo-Hammond C, Curtis R, et al. Growth retardation in children with epilepsy on the ketogenic diet: A retrospective chart review. J Am Diet Assoc 2002;102:405. Williamson DH. Ketone body metabolism during development. Fed Proc 1985;44:2342. Wing R, Vazquez J, Ryan C. Cognitive effects of ketogenic weight-reducing diets. Int J Obes Relat Metab Disord 1995;19:811.
1150
Epilepsy / 50
Withrow CD. Antiepileptic drugs, the ketogenic diet: Mechanism of anticonvulsant action. In: Glaser GH, Penry JK, Woodbury DM, eds. Antiepileptic drugs: Mechanism of action. New York: Raven, 1980. Woody, RC, Steele RW, Knapple W, et al. Impaired neutrophil function in children with seizures treated with the ketogenic diet. J Pediatr 1989;115:427. Yudkoff M, Daikhin Y, Nissim I, et al. Effects of ketone bodies on astrocyte amino acid metabolism. J Neurochem 1997;69:682. Yudkoff M, Daikhin Y, Nissim I, et al. Brain amino acid metabolism and ketosis. J Neurosci Res 2001a;66:272. Yudkoff M, Daikhin Y, Nissim I, et al. Ketogenic diet, amino acid metabolism, and seizure control. J Neurosci Res 2001b;66:931. Zhao Q, Stafstrom CE, Fu DD, et al. Detrimental effects of the ketogenic diet on cognitive function in rats. Pediatr Res 2004;55:498. Ziegler DR, Araujo E, Rotta L, et al. A ketogenic diet increases protein phosphorylation in brain slices of rats. J Nutr 2002;132: 483.
RESOURCES Brake D, Brake C. The ketogenic cookbook. Gilman, Conn: Greider Pennycorner Press, 1996. Both authors are culinary arts graduate chefs whose children were on the ketogenic diet treatment program. George M. Greider, Pennycorner Press, P.O. Box 8, Gilman, CT 06336; phone: (860) 873-3545; fax: (860) 873-1311. Freeman JM, Freeman JB, Kelly MT. The epilepsy diet treatment, 3rd ed. New York: 2000. Demos Vermande, 386 Park Avenue South, Suite 210, New York City, NY 10016; phone: (800) 532-8663. The Keto Klub, a quarterly newsletter devoted to the ketogenic diet. Elaine Huffman, Editor, 61557 Miami Meadows Court, South Bend, IN 46614; fax: (210) 299-8602. Video tapes on the ketogenic diet for families, dietitians, nurses, and physicians. The Charlie Foundation to Help Cure Pediatric Epilepsy, 501 10th Street, Santa Monica, CA 90402; fax: (310) 393-2347.
CHAPTER 51
Epilepsy Surgery in the Pediatric Population Mary L. Zupanc
Epilepsy is one of the most common chronic problems facing children and adolescents. The overall prevalence of epilepsy has been estimated to be 5 to 8 per 1000 [Bharucha et al., 1988; Hauser et al., 1975, 1994, 1996, 1998; Olafsson et al., 1996; Osuntokun et al., 1987; Zielinski, 1974]. Extrapolating the Hauser data from Rochester, Minnesota, of 6.66 per 1000 to the total population in 2004, approximately 2.3 million persons in the United States will have epilepsy [Hauser et al., 1991]. In developed countries, the incidence of epilepsy is 50 to 100 cases per 100,000 population per year, and the prevalence is approximately 5 to 8 per 1000 [Hauser et al., 1991, 1994, 1996, 1998]. The cumulative risk of developing epilepsy from birth through adolescence is 1% [Hauser et al., 1991, 1994]. What are the best ways to determine the prognosis of epilepsy, and who may be a candidate for epilepsy surgery? Several studies have addressed these questions. The identification of a specific epilepsy syndrome is one of the best determinants of prognosis. Some epilepsy syndromes are genetically determined “channelopathies” and are selflimited in their time course. Other epilepsy syndromes, particularly the lesional epilepsies, are life-long conditions. As an example, benign rolandic epilepsy is characterized by nocturnal focal motor seizures, age at onset between 3 and 8 years, normal findings on neurologic examination, and sleep-activated central-temporal epileptiform discharges on the electroencephalogram (EEG). In this case, the parents can be reassured that their child’s epilepsy will remit by puberty. On the other hand, predictors for the low probability of epilepsy remission include (1) the presence of a symptomatic localization-related epilepsy secondary to a remote central nervous system injury; (2) abnormalities on neurologic examination or cognitive/motor delays; (3) persistent epileptiform abnormalities on EEG; and (4) older age at onset [Arts et al., 1988; Berg et al., 2001; Camfield and Camfield, 2003; Emerson et al., 1981; Hauser et al., 1975, 1996, 1998; Juul-Jensen and Foldsprang, 1983; Schmidt et al., 1983; Shafer et al., 1988; Sillanpaa et al., 1998; Sofijanov, 1982; Todt, 1984]. In addition, the longer epilepsy persists without control, the smaller the chance of its going into remission. Specifically, if seizures remain under inadequate control for longer than 4 years, the chance of remission decreases to approximately 10% [Annegers et al., 1979]. The presence of multiple seizure types and frequent generalized tonic-clonic seizures also lessens the chance for complete remission. It is estimated that in 20% to 25% of all persons with epilepsy, accounting for approximately 20,000 cases annually, the seizures eventually will become intractable. Approximately 60% of these patients will have partial seizures. Estimates by several investigators suggest that approximately 3000 patients with newly diagnosed
epilepsy will ultimately be epilepsy surgery candidates [Hauser, 1993]. This figure may increase as new technologies enable more precise identification of an underlying epileptogenic focus. Additionally, as medical intractability for children with epilepsy is further defined, the number of pediatric epilepsy surgical procedures likely will increase. An increasing number of pediatric comprehensive epilepsy centers are equipped to handle the complexities of the preoperative evaluation in children and infants. Many issues must be addressed before a child becomes a candidate for epilepsy surgery. The number of children undergoing epilepsy surgery in the United States is rising, with greater than 200 pediatric epilepsy surgical procedures performed annually. Costs for a temporal lobectomy are estimated at $20,000 to $30,000 [King et al., 1997]. Costs for an extratemporal resection can be twice as high, especially if invasive subdural EEG monitoring and newer neuroimaging techniques are used. The developing brain is highly susceptible to recurrent seizures. Until recently, the brain was believed to be relatively resistant to brain injury. A growing body of evidence in animal models, however, suggests that early seizures, even if brief and recurrent, can result in demonstrable structural and physiologic changes in the developing brain’s circuitry, resulting in aberrant excitation and inhibition. Clinically, this defect produces spontaneous seizures (epilepsy) and cognitive impairments [Holmes and Ben-Ari, 1998; Holmes et al., 1998; Stafstrom et al., 2000], with the possibility of missed windows of developmental opportunity. Thus, plasticity of the brain in a young infant and child is a “double-edged sword”: It protects the brain from the neurologic consequences of destructive lesions and status epilepticus; however, recurrent seizures in this age group can produce permanent abnormal neuronal circuitry, resulting in long-term developmental delays and continued, intractable seizures. In addition, chronic uncontrolled epilepsy in infants and children poses a significant risk for emotional, behavioral, social, cognitive, and family dysfunction. Population studies have demonstrated that epilepsy reduces life expectancy, and poorly controlled seizures further increase the risk of death in adults and children [Nashef et al., 1995]. The estimated risk of sudden unexpected death in epilepsy may be as high as 1 in 500 in the adolescent population (the incidence in young children remains undetermined) [Harvey et al., 1993c; Hauser, et al., 1980]. What are the outcomes of epilepsy surgery in the pediatric population? A majority of the outcome studies have been performed in older adolescents and adults. In these outcome studies, the focus has been primarily on the improvement of seizure control, with 64% to 69% of patients having seizurefree outcomes [Engel, 1996; Wyllie, 1998; Wyllie et al., 1998]. These studies have placed less emphasis on
1152
Epilepsy / 51
improvement in quality of life—for example, enhancement of self-image, improvement in academic performance and psychosocial functioning, and increased independence in activities of daily living [Spencer, 1996; Taylor et al., 1997]. A growing number of long-term follow-up studies have infants and young children as their major focus. Malformations of cortical development are the most frequently cited pathologic abnormalities in pediatric surgical patients [Duchowny et al., 1996; Wyllie et al., 1998]. The overall outcome of pediatric epilepsy surgery in young infants and children is roughly comparable to that in the older adolescent and adult population. In infants, 61% to 65% have seizure-free outcomes following epilepsy surgery [Chugani et al., 1993; Duchowny et al., 1998; Sinclair et al., 2003; Wyllie et al., 1996, 1998a]. In young children, the rate of seizure-free outcomes varies, ranging from 59% to 67% [Paolicchi et al., 2000; Sinclair et al., 2003; Wyllie et al., 1998]. The etiology of the epilepsy appears to play the major role in the prognosis in young infants and children, regardless of location (temporal versus extratemporal). Specifically, in the series of patients from Miami Children’s Hospital, 62% of children (13 of 21) with malformations of cortical development had a seizure-free outcome, as opposed to patients with low-grade tumors; 100% of them were seizure free after epilepsy surgery [Duchowny et al., 1998]. Several studies have reported on cognitive function after surgery in children who have undergone temporal lobectomy (predominantly older children and adolescents) [Gillam et al., 1997; Gleissner et al., 2002; Mabbott and Smith, 2004; Meyer et al., 1986; Szabo et al., 1998; Westerveld et al., 2000]. These studies generally have found that memory and intelligence are unchanged, although some reports note a decline in verbal memory and improvements in language, attention, and memory. Reports on the cognitive effects of extratemporal resections have been relatively few, in part because of the young age of the patients. In patients who have undergone successful frontal lobe resection, outcomes include apparent improvements in attention and concentration but no change in executive functions, manual coordination, and language [Blanchette and Smith, 2002; Lendt et al., 2002]. Studies on postoperative psychosocial functioning in children have been relatively rare, almost exclusively retrospective, and based on subjective measures. In children who have undergone temporal lobectomies, studies indicate improvement in behavior, mood, and selfesteem, with the changes linked to improvement in seizure control [Danielsson et al., 2002; Davidson and Falconer, 1975; Duchowny et al., 1992; Meyer et al., 1986]. Of children who have undergone extratemporal resections, improved social behavior was found in about 50% [Adler et al., 1991]. Other retrospective studies that combine temporal and extratemporal cases suggest that reduction of seizure frequency, although not necessarily complete elimination of seizures, results in improved family life, socialization and behavior, and quality of life [Adler et al., 1991; Keene et al., 1998; Mihara et al., 1994; Whittle et al., 1981]. Other reports indicate that a reduction in seizures may result in a favorable and significant improvement in the quality of life with behavioral and developmental “catch-up” progress [Asarnow et al., 1997; Bourgeois et al., 1999; Chugani et al., 1990; Duchowny et al., 1990, 1992; Wyllie et al.,
1996; Zupanc, 1996]. A recent study looking at patients 1 year after surgery, however, challenges the assumptions that the elimination of seizures results in improved cognitive, psychosocial, and family functioning [Smith et al., 2004]. Fifty-seven percent of these patients were seizure free. Cognitive and psychosocial status did not change over time. The differences between this study and other studies may be due to the relatively short duration between epilepsy surgery and follow-up evaluation. Nonetheless, this study had a nonsurgical comparison group, was prospective in nature, and used well-known standardized outcome measures. Further data on epilepsy surgery outcome are needed.
HISTORICAL BACKGROUND Epilepsy has always been a part of human existence. A generalized tonic-clonic seizure was first described in Akkadian, the oldest written language, more than 3000 years ago [Goldensohn et al., 1997]. Since that time, many descriptions of epilepsy appear in the literature, including the Bible. In On the Sacred Disease, written in the fifth century, Hippocrates wrote that epilepsy was a brain disease caused by an excess of phlegm that resulted in an abnormal brain consistency. He proposed diet and drugs as therapy [Scott, 1993]. Until the late 19th century, the treatment of epilepsy was surrounded by superstition, exorcism, magic, and alchemy. Caton’s (1842 to 1926) discovery in 1875 of spontaneous electrical activity of the brain and evoked potentials suggested that seizures might be the result of aberrant electrical activity in the brain [Caton, 1875]. The first effective treatment for epilepsy was potassium bromide, introduced in 1857 [Locock, 1857]. A few years later, in 1886, Horsley performed the first epilepsy surgery on a patient with intractable post-traumatic epilepsy. Several decades later, the antiepileptic drug phenobarbital was introduced in 1912, followed by phenytoin in 1937. Similarly, epilepsy surgery did not advance until 1950, when Penfield published his article on 70 cases of temporal lobectomy [Flanigin et al., 1991; Penfield and Flanigin, 1950]. His neurosurgical career was devoted to the study of seizure semiology (i.e., clinical description) and its correlation with the brain cortex. He used cortical mapping and stimulation in much the same way in which it is used today. He also recognized the substrates of epilepsy, particularly trauma and infection. His seminal clinical research has been instrumental in guiding the hands of contemporary epileptologists and neurosurgeons interested in the surgical approach to epilepsy. Epilepsy surgery was not regarded as a conventional treatment for intractable epilepsy until recently. In the past 25 years, dramatic improvements in brain imaging that identify specific anatomic substrates of epilepsy have sparked renewed interest in this modality. Temporal lobectomy with amygdalohippocampectomy has become the standard of care in adult patients with intractable epilepsy emanating from the temporal lobe. The surgical success rate for a seizure-free outcome in these carefully selected patients approaches 80% to 90% [Duchowny et al., 1992; King et al., 1986; Penfield and Flanigin, 1950]. Unfortunately, surgical success does not necessarily translate to an improvement in quality of life. The accumulation of years of low selfesteem, loss of independence, poor peer relations, and
Zupanc / Epilepsy Surgery in the Pediatric Population
academic failure, coupled with high financial costs, often without benefit of full insurance coverage, translates to continued lack of employment and depression [Reeves et al., 1997]. The lifetime cost of epilepsy for an estimated 181,000 people with onset in 1995 is projected at $11.1 billion dollars, and the annual cost for the estimated 2.3 million people with epilepsy estimated at 12.5 billion dollars [Bazil, 2004; Begley et al., 1994, 2000; Hathaway et al., 1995]. Indirect costs account for 80% to 85% of the total costs and include delayed or missed educational opportunities, psychiatric and social service needs, and lost employment. The direct costs of epilepsy are concentrated in the patients with intractable epilepsy. The growing recognition of the real costs of epilepsy—medical, psychological, educational—have led to increased interest in the early identification of children who might benefit from epilepsy surgery [Jalava et al., 1997]. Attempts have been made to calculate the cost-benefit ratio for anterior temporal lobectomy. Even with the most conservative estimates, the benefit to society outweighs the costs when projected over an affected person’s life span. In the older child and adolescent, temporal lobectomies are common epilepsy surgical procedures. In younger children and infants, however, extratemporal resections, including multilobar resections and hemispherectomies, are the more typical procedures. Demonstration of seizure control and long-term developmental improvement should be the goals for any pediatric epilepsy surgery [Nordli, 2000].
INDICATIONS FOR EPILEPSY SURGERY In determining whether a child is a candidate for epilepsy surgery, several key issues must be considered. The decision-making task must take into account the following: • Seizure recurrence despite appropriate antiepileptic drug management • Natural history of the epilepsy syndrome (likelihood of continued intractability usually can be determined on the basis of the identification of symptomatic lesional epilepsy) • Identification of a known epileptogenic substrate • Impact of epilepsy on the quality of life as defined by cognitive and developmental parameters—now and in the future The proper classification of seizure type and epilepsy syndrome is crucial in the determination of whether or not a patient is an appropriate epilepsy surgery candidate [Aicardi, 1994; Holmes, 1993]. The benign seizure disorders, such as benign rolandic epilepsy or benign epilepsy with central centrotemporal spikes, must be recognized. With rare exceptions, these syndromes usually are easily treated, and affected patients do not present to tertiary epilepsy centers. The catastrophic epilepsies of infancy and childhood are recognizable early, and affected patients should be referred to a tertiary epilepsy center for consideration for epilepsy surgery. These epilepsy syndromes are characterized by the triad of (1) multiple daily seizures, (2) medical intractability to the standard antiepileptic drug therapies, (3) cognitive/ developmental stagnation or decline, and (4) presumed or known epileptogenic pathology. The patients should be
1153
surgically treated at an early age as soon as these catastrophic epilepsies are recognized and the preoperative evaluation can be completed with confidence. The catastrophic epilepsies of infancy and childhood include (1) SturgeWeber syndrome; (2) large unilateral or focal malformations of cortical development such as hemimegalencephaly or unilateral schizencephaly; (3) symptomatic infantile spasms with focal malformations of cortical development, typically temporal-parietal-occipital dysplasias; and (4) Rasmussen’s syndrome. Children with Sturge-Weber syndrome who have frequent, medically refractory seizures accompanied by progressive hemiparesis and cognitive impairment should be evaluated promptly for hemispherectomy [Thomas-Sohl et al., 2004; Vining et al., 1997]. Clinical outcome studies indicate that early surgical resection can result in the elimination of seizures, improvement in cognitive abilities, and overall improvement in quality of life despite hemiparesis and visual field defect as residual neurologic deficits [Erba and Cavazzuti, 1990; Hoffman et al., 1979; Ogunmekan et al., 1991]. Another category of patients with catastrophic epilepsy comprises those with unilateral or focal malformations of cortical development. Children with hemimegalencephaly can present in infancy with multiple daily seizures, developmental stagnation or decline, and hemiparesis. Again, hemispherectomy provides relief from seizures (especially in those patients with unilateral epileptiform abnormalities) and improved developmental outcome [Andermann et al., 1993; Vigevano and DiRocco, 1990; Vigevano et al., 1989]. Another subset of patients with symptomatic infantile spasms who have underlying focal cortical dysplasias, usually temporal-parietal-occipital, should be considered for focal cortical resection. University of California at Los Angeles investigators have provided the seminal clinical research in this area and have documented a significant improvement in seizure control and enhanced developmental gains, greater than would have been predicted using the natural history of infantile spasms as a comparison [Asarnow et al., 1997; Chugani et al., 1990, 1993; Duchowny et al., 1990]. Rasmussen’s encephalitis is characterized by intractable focal motor seizures, often evolving into epilepsia partialis continua, cognitive decline, and progressive hemiparesis. Recent findings of glutamate receptor antibodies in some patients with Rasmussen’s encephalitis implicate an autoimmune pathophysiology [Antel and Rasmussen, 1996; Pardo et al., 2004; Rogers et al., 1994]. Although initial trials of intravenous immunoglobulin and plasmapheresis have been encouraging, long-term studies have not confirmed efficacy [Andrews et al., 1996; Hart et al., 1994; Krauss et al., 1996]. Therefore, the only definitive treatment for Rasmussen’s encephalitis remains hemispherectomy. In addition to those with the catastrophic epilepsies of infancy and childhood, all children with tumors and concomitant localization-related epilepsy should be considered for early surgical intervention. Compelling reasons for such intervention exist. Most tumors need to be biopsied or excised. Additionally, although the tumors associated with epilepsy usually are slow growing, cortical, and well circumscribed, some tumors, especially astrocytomas, are not necessarily benign and can undergo malignant change over
1154
Epilepsy / 51
A
B
FIGURE 51-1. MRI scans from a patient with a ganglioglioma of the right temporal lobe. A, T1-weighted imaging without gadolinium (TR 500 msec/TE 16 msec). B, T1-weighted imaging with gadolinium (TR 500 msec/TE 16 msec). MRI, magnetic resonance imaging; TE, echo time; TR, recovery time.
time [Jack, 1995]. Without resection, the natural history of these tumor-associated epileptic syndromes is one of continued seizures with little hope of remission. Antiepileptic drugs produce side effects; subtle and overt side effects can affect cognitive function and behaviors, with concomitant impact on psychosocial development [Vining et al., 1987]. Examples of tumors that usually are easily resectable are the gangliogliomas and dysembryonic neuroectodermal tumors, which have a predilection for the temporal lobe (Fig. 51-1) [Duchowny et al., 1992; Tice et al., 1993; Vali et al., 1993]. Children with other types of lesional symptomatic localization-related epilepsy also should be considered epilepsy surgery candidates. Common substrates of epilepsy include encephalomalacias, vascular malformations, tubers, and malformations of cortical development. Sometimes these patients present with generalized epileptiform discharges on surface EEG monitoring. In the presence of a lesion on magnetic resonance imaging (MRI) scan of the brain, the epilepsy syndrome is most likely to be due to a symptomatic localization-related epilepsy with rapid secondary bisynchrony. With the improvement in neuroimaging, source localization on EEG, and magnetoencephalography (MEG), our ability to identify the epileptogenic zone is greatly enhanced, making a surgical resection a possibility. Patients with tuberous sclerosis and medically refractory symptomatic localization-related epilepsy also should be considered for epilepsy surgery. In patients with multiple tubers, emerging neuroimaging techniques, particularly interictal α-[11C]methyl-L-tryptophan (AMT) positron emission tomography (PET) scans, offer promise in identifying the most highly epileptogenic tuber [Asano et al., 2000; Chugani et al., 1998; Juhasz et al., 2003]. If the presurgical evaluation points to a specific tuber, studies have shown that it can be successfully removed, with a significant improvement in seizure control [Bebin et al., 1993; Koh et al., 2000; Romanelli et al., 2004].
Factors that favor early intervention with epilepsy surgery include the following: (1) seizure recurrence despite an adequate trial of two or three antiepileptic drugs; (2) seizures severe enough to interfere with progression in development or overall quality of life; (3) location of the lesion in the temporal lobe; and (4) epilepsy caused by identifiable malformations of cortical development. Even if the lesion is outside the temporal lobe, in carefully selected patients, lesionectomies generally can be performed with little risk of neurologic sequelae [Britton et al., 1994; Cascino et al., 1990, 1992, 1993, 1994; Montes et al., 1995; Paolicchi et al., 2000]. Data from our own retrospective study and from the work of Palmini and co-workers suggest that malformations of cortical development, no matter where the cortical location, carry a greater than 35% risk for status epilepticus [Laoprosert et al., 1997; Palmini et al., 1997]. Focal cortical dysplasias, as opposed to unilateral or bilateral polymicrogyria and schizencephaly, are almost universally refractory to antiepileptic drugs [Palmini et al., 1997]. Histopathologic examination, therefore, may play a large role in identifying the natural history of these epileptic syndromes. If the epilepsy is temporal in onset and pathologic features include associated hippocampal formation atrophy or mesial temporal sclerosis, the surgical success rate approaches 80% to 90% [Cascino et al., 1993; Sinclair et al., 2001] (Fig. 51-2). Epilepsy surgery should be considered early in these patients. Those children with intractable nonlesional extratemporal localization-related epilepsy represent the biggest challenge to the epileptologist but should still be considered for epilepsy surgery if their seizures remain intractable. The benefits of surgery must be weighed against the risks, especially the risk of neurologic deficits. As an example, localization-related epilepsy emanating from the sensorimotor cortex demands a more conservative approach. Several antiepileptic drugs and suitable investigational anti-
Zupanc / Epilepsy Surgery in the Pediatric Population
FIGURE 51-2. MRI scan from a patient with left temporal hippocampal atrophy. The scan shows a coronal cut obtained with T1-weighted imaging (TR 24 msec/TE 9 msec). MRI, magnetic resonance imaging; TE, echo time; TR, recovery time.
epileptic drugs should be tried before embarking on a surgical approach with its attendant risks of hemiparesis. On the other hand, if a child has severe, frequent seizures with developmental stagnation and the preoperative evaluation demonstrates congruence of data from seizure semiology, electroencephalography, MRI, single-proton emission computed tomography (SPECT), PET, MEG, and MR spectroscopy (MRS), epilepsy surgery can be performed. Children with generalized or multifocal epilepsy also may be considered for epilepsy surgery if data suggest an underlying focal generator for the epileptic condition [Wyllie, 1995]. Approximately 10% to 15% of children with LennoxGastaut syndrome, one of the most common symptomatic “generalized” epilepsy syndromes, have underlying focal malformations of cortical development and should be evaluated carefully for epilepsy surgery. Children with intractable epilepsy who have tonic-atonic seizures associated with generalized spikes/polyspikes (usually Lennox-Gastaut syndrome) and no identifiable lesion on neuroimaging may respond to a corpus callosotomy, a palliative treatment that can have a significant impact on quality of life [Wyllie et al., 1993].
PREOPERATIVE EVALUATION Once a child has been selected as a possible epilepsy surgery candidate, further questions need to be addressed before epilepsy surgery can take place: (1) Can the epileptogenic zone be identified using video EEG, neuroimaging, and other modalities? Is there congruence of the data? (2) Can
1155
the epileptogenic focus be removed without causing unacceptable neurologic deficits? (3) Will a delay in epilepsy surgery cause loss of developmental plasticity? A multidisciplinary team is required to address the many issues surrounding the prospect of surgery in a child with chronic epilepsy. Epilepsy surgery itself may cure the seizures but will not necessarily address other needs of the family. A child with medically intractable epilepsy and the child’s family have complex and diverse problems—not just medical but also developmental, educational, psychosocial, economic, and relational. The coordinated services of a pediatric neurologist or epileptologist, child psychiatrist, pediatric neurosurgeon, pediatric neuropsychologist, speech and language pathologist, and pediatric neuroradiologist, along with diagnostic studies including electroencephalography, neuroimaging, and nuclear isotopic scanning, are required to evaluate the medical aspects before surgery is considered. Clinical nurse specialists are integral, often acting as the case managers and coordinators of the care designed to meet patient and family needs. The social worker is a critical part of the team, providing families with avenues for financial assistance, counseling families, and assisting with transitional services from hospital and clinic to the home environment. In addition, networking with other families who have undergone similar evaluations and treatment also is a critical aspect of the multidisciplinary evaluation, which cannot be effectively carried out without the integration of these services.
Concept of Congruence Under ideal conditions, identification of the epileptogenic focus is made by the congruence of data obtained during the preoperative evaluation, with the precise localization based on seizure semiology, physical examination, surface ictal and interictal EEG monitoring (and, if necessary, invasivedepth electrodes or subdural electrode strips or grid), MRI scan of the brain, ictal and interictal SPECT scans, interictal PET scan, MEG, functional MRI scan, and/or MR spectroscopy. Each case must be individualized, with some cases requiring the acquisition of data from all of these studies. Others may be resolved with a less complicated approach. At a minimum, seizure semiology, surface ictal EEG monitoring, and MRI scan of the brain should be congruent. With lesional localization-related epilepsy, the use of invasive EEG monitoring generally is not necessary. Electrocorticography at the time of surgery usually can assist with identifying the dimensions of the epileptogenic zone. The sensorimotor cortex can be identified intraoperatively using motor-evoked potentials, somatosensory-evoked potentials, or direct electrical cortical stimulation mapping. If the surgical excision is near functional speech and language cortex, older children and adolescents usually can be cooperative enough to tolerate an awake surgical procedure. In younger children (before the age of 5 to 6 years), plasticity of the brain is sufficient that removal of the primary speech and language centers will result in transition to the other hemisphere [Peacock, 1995; Shields, 2000]. The most complex cases are those of nonlesional extratemporal epilepsy. The patients usually require an interictal PET scan, subtraction SPECT scan, MR spectroscopy, or MEG, to look for evidence of a localized abnormality. In
1156
Epilepsy / 51
these patients, placement of invasive subdural strips or grids may be needed for precise localization of the epileptogenic focus.
Techniques and Technologies Seizure Semiology Seizure semiology can provide insightful clues to the lateralization and localization of the underlying epileptogenic focus. The presence of adversive head movements, unilateral motor clonic activity, and eye deviation may constitute critical lateralizing information. In similar fashion, seizures consisting of olfactory or gustatory hallucinations followed by complex motor automatisms and staring unresponsively are virtually diagnostic of involvement of the temporal lobe. These seizures generally are seen in older children or adolescents but also may occur in younger children. It should be noted, however, that seizures emanating from the temporal lobe in infants and young children commonly are associated with behavioral arrest, motor dystonic posturing, and fewer automatisms [Brockhaus and Elger, 1995; Jayakar and Duchowny, 1990; Wyllie et al., 1993]. Additionally, young children usually are incapable of describing the premonitory symptoms before the onset of the more overt clinical seizure. Video EEG monitoring has been helpful in fully elucidating the seizure semiology in these patients. Children with infantile spasms may have partial seizures before, during, or after the onset of the infantile spasms [Kobayashi et al., 2001; Watanabe et al., 2001]. Partial seizures can be a helpful clue that informs the epileptologist to screen carefully for an underlying focal abnormality, such as a tuber or focal cortical dysplasia.
Physical Examination The physical examination also can provide very valuable lateralizing information. As with seizure onset or its evolution, a focal abnormality on physical examination may point to an underlying focal structural lesion. For example, a child with schizencephaly and partial seizures may have a subtle hemiparesis, effectively demonstrating the affected hemisphere.
Electroencephalography The surface EEG is a critical element in the evaluation of children with epilepsy. The advent of computerized prolonged video EEG monitoring has ushered in a new era in the evaluation and management of epilepsy. This technique is used for many purposes, including (1) differentiation of epileptic versus nonepileptic events; (2) seizure classification; (3) recognition of specific epileptic syndromes; (4) preoperative evaluation with identification of the epileptogenic zone; (5) determination of seizure frequency; and (6) management of status epilepticus. In the adult preoperative evaluation, prolonged video EEG monitoring provides the baseline data with which all of the other data are compared. In children, however, it is becoming increasingly clear that the surface EEG data may be poorly localized and at times misleading in the preoperative evaluation [Wyllie, 1995]. Therefore, this modal-
ity may be less important in localizing the epileptogenic focus. In these children, other modalities, particularly neuroimaging studies (MRI, MRS, PET, and SPECT), may provide the pivotal information that determines the location of the epileptogenic zone and the need for invasive subdural EEG monitoring. Indeed, in the near future, the improvement of noninvasive functional brain imaging techniques may obviate the need for invasive EEG monitoring. Even now, invasive EEG monitoring may be deferred if surface EEG monitoring and MRI data are congruent [Wyllie et al., 1998].
Magnetic Resonance Imaging MRI scans have greatly enhanced the ability to visualize intraparenchymal brain structures. The linkage between intracranial abnormalities and epilepsy is well accepted [Zupanc, 1997a]. The mechanism(s) involved in the production of epilepsy is an area of intense research and involves structural changes, synaptic reorganization, stimulation of mossy fibers, astroglial proliferation with neuronal cell loss, and neurotransmitter or corresponding receptor changes. With the recent advances in MRI technology, the ability to identify these substrates of epilepsy has been greatly enhanced. This modality provides some of the most sensitive and specific neuroimaging data for localization of the epileptogenic zone [Brooks et al., 1990; Cascino, 1994; Cascino et al., 1989, 1991; Kuzniecky et al., 1993a, 1993c]. The following new technologies are exciting and innovative [Jack, 1995]: • Use of thin contiguous cuts of 1.5 to 1.6 mm in multiple sections of the cortex in combination with a three-dimensional volumetric pulse sequence provides the necessary resolution to detect small lesions that would be missed with conventional MRI scans. Specific areas can be targeted, and images can be reformatted to correct for head rotation and other perturbations in data collection. This technique has allowed detection of even small amounts of unilateral hippocampal atrophy (see Fig. 51-2), as well as identification of small areas of focal cortical dysplasia. • The ability to conduct quantitative volumetric analysis of the hippocampus has resulted in the determination of unilateral or bilateral hippocampal atrophy. In patients with epilepsy emanating from the temporal lobe, the identification of unilateral hippocampal atrophy combined with concordant surface ictal EEG data is sufficient to allow a temporal lobectomy with amygdalohippocampectomy to proceed without invasive EEG monitoring. • The fluid-attenuated inversion recovery imaging (FLAIR) technique highlights lesions such as mesial temporal sclerosis and malformations of cortical development and allows detection of previously unidentifiable small lesions. This sequence produces a T2-weighted image that subtracts out the cerebrospinal fluid signal (white and bright on T2) but keeps the T2 signal for intraparenchymal structures (Figs. 51-3 and 51-4). • Diffusion tensor imaging is an MRI imaging technique that can identify white matter tracts [Rugg-Gunn et al., 2001] that may be disrupted in areas of cortical
Zupanc / Epilepsy Surgery in the Pediatric Population
A
1157
B
FIGURE 51-3. MRI scans from a patient with focal cortical dysplasia of the posterior left parasagittal region. A, With T1-weighted imaging (TR 24 msec/TE 9 msec), thickening of the cortex and blurring of the white/gray matter are evident. B, The dysplasia is seen more clearly with fluid-attenuated inversion recovery imaging (FLAIR) sequencing (TR 1100 msec/TE 142 msec/TI 2600 msec) (see text). MRI, magnetic resonance imaging; TE, echo time; TI, inversion time; TR, recovery time.
dysplasia. With use of these techniques, MRI scans can identify many substrates of epilepsy, including malformations of cortical development, tumors, vascular malformations, and encephalomalacias secondary to trauma, infection, and infarction. Malformations of cortical development are increasingly recognized as being highly epileptogenic [Kuzniecky and Ruben, 1995; Kuzniecky and Barkovich, 2001; Palmini et al., 1995; Raymond et al., 1995]. Advances in MRI technology have greatly improved the ability to identify these abnormalities. They may account for greater than 60% of the intractable localization-related epilepsies of childhood [Kuzniecky et al., 1993c]. These malformations can be small and difficult to detect even with sophisticated MRI scans of the brain or can be widespread and diffuse, as with lissencephaly [Dobyns and Truwit, 1995; Dobyns et al., 1996] (Figs. 51-5 and 51-6). The unilateral and focal malformations of cortical development are most often targeted for surgical excision. Clinically, information on the natural history of the malformations of cortical development is emerging. Status epilepticus is a common initial presentation, usually in the latter half of the first decade of life [Laoprasert and Zupanc, 1997]. Many of the malformations of cortical development produce an epileptic syndrome that is intractable to medical management [Palmini et al., 1997]. Finally, although mesial temporal sclerosis and hippocampal atrophy are not commonly found in children with intractable epilepsy younger than 10 years of age, identification of these abnormalities is a powerful indicator of the zone of epileptogenesis [Cascino, 1994; Cascino et al.,
1991; Jack, 1995; Swartz et al., 1992]. The pathophysiology of mesial temporal sclerosis and hippocampal formation atrophy is poorly understood. Do the seizures themselves cause mesial temporal sclerosis and hippocampal formation atrophy? Does an underlying malformation of cortical development cause the initial seizures, ultimately resulting in mesial temporal sclerosis and hippocampal formation atrophy? [Cendes et al., 1993; Kuks et al., 1993; Trenerry et al., 1993]. These questions have not yet been clearly answered. We do know, however, that the degree of volume loss correlates with the amount of cellular loss as measured in pathologic specimens [Cascino et al., 1991]. The neuronal cell loss, coupled with the presence of aberrant mossy fibers and synaptic reorganization, probably accounts for the recurrent, recalcitrant seizures [Fuerst et al., 2003; Holmes and Ben-Ari, 1998; Jokeit et al., 1999; Kalviainen et al., 1998; Kotloski et al., 2002; Sutula et al., 1988, 1989; Tasch et al., 1999]
Single-Photon Emission Computed Tomography SPECT also has enhanced the ability to identify the epileptogenic zone. Penfield and colleagues observed relative hyperperfusion in the epileptogenic zone during a seizure [Penfield, 1958]. Interictally, blood flow and metabolism decrease. SPECT scan technology enables quantification of cerebral blood flow and identification of areas of relative blood flow change. SPECT images are reconstructed from data obtained by recording photon emissions from radiotracers injected intravenously. These radiotracers rapidly
1158
Epilepsy / 51
FIGURE 51-4. MRI scans showing coronal cuts through the temporal lobes, from a patient with left temporal hippocampal atrophy. The atrophy is seen best with T1-weighted imaging (top panel) (TR 24 msec/TE 9 msec). Concomitant left temporal mesial temporal sclerosis is seen best with FLAIR sequencing (bottom panel) (TR 1100 msec/TE 142 msec/TI 2600 msec). Middle panel represents the picture created on T2-weighted imaging (TR 2000 msec/TE 80 msec). FLAIR, fluid-attenuated inversion recovery imaging; MRI, magnetic resonance imaging; TE, echo time; TR, recovery time.
FIGURE 51-6. MRI scan from a patient with unilateral perisylvian dysplasia with polymicrogyria (left hemisphere). T1-weighted imaging (TR 24 msec/TE 9 msec) was used. MRI, magnetic resonance imaging; TE, echo time; TR, recovery time.
FIGURE 51-5. MRI scan from a patient with focal cortical dysplasia of the left frontal region. With T1-weighted imaging (TR 24 msec/TE 9 msec), thickening of the cortex and blurring of the white/gray matter are seen. MRI, magnetic resonance imaging; TE, echo time; TR, recovery time.
cross the blood-brain barrier because of their lipophilic nature and bind within minutes to the brain, producing an instantaneous picture of cerebral blood flow [English and Brown, 1990]. Clinical research has focused on both interictal and ictal SPECT scans, with a substantial portion of the clinical research using the radioisotope 99mtechnetiumhexamethylpropyleneamine oxime (99mTc-HMPAO). More recently, 99mTc ethyl cysteinate dimer (ECD) (i.e., 99mTcN,N′(1,2-ethylenediyl)bis-L-cysteine diethyl ester), prepared as technetium Tc-99m bicisate (Neurolite), has been introduced [Lanceman et al., 1997]. Logistically, Neurolite provides distinct advantages for ictal SPECT scans because it is a stable isotope tracer that can be mixed well ahead of the time of injection, as opposed to 99mTc-HMPAO, which decomposes quickly in vitro and must be used less than 30 minutes after it is reconstituted. For ictal SPECT scans, a technologist or nurse trained in the delivery of these radioisotopes can sit at the bedside and deliver the Neurolite within seconds after the onset of a seizure. Spatial resolution with SPECT scans also has improved because of the development of gamma cameras with multiple detectors that provide more data points, with subsequent enhanced sensitivity. Interictal SPECT scans have been used for longer than 10 years as a method for identifying the epileptogenic focus in patients with medically intractable localization-related epilepsy who are candidates for epilepsy surgery. With interictal SPECT scans, the epileptogenic zone can be identified by a regional area of reduced cerebral blood flow [Adams et al., 1992; Berkovic et al., 1992, 1993; Cordes et al., 1990; Coubes et al., 1993; Denays et al., 1988; Dietrich et al., 1991; Grunwald et al., 1991; Hajek et al., 1991; Kuzniecky
Zupanc / Epilepsy Surgery in the Pediatric Population
et al., 1993b; Lamanna et al., 1989; Launes et al., 1992; Lee et al., 1988; Rowe et al., 1989, 1991; Ryding et al., 1988; Ryvlin et al., 1992; Shen et al., 1990; Verhoeff et al., 1992]. Clinical research clearly indicates that interictal studies alone have a relatively low sensitivity for identification of the epileptogenic focus in adults with temporal lobe epilepsy and even lower sensitivity with extratemporal epilepsy. Data pooled from several studies yield estimates of interictal SPECT sensitivity of 66% for temporal lobe epilepsy and 60% for extratemporal epilepsy localized by EEG [Spencer, 1994]. Interictal SPECT scans do demonstrate regional hypoperfusion, most prominent in those persons who have frequent seizures, but the hypoperfusion generally is over a larger region of cortical tissue than found with ictal recordings. Other studies suggest that the sensitivity of interictal SPECT studies in children may be higher than in adults, but the studies are still not as reliable as the ictal studies [Cross et al., 1995; Harvey et al., 1993a, 1993b]. Ictal SPECT scan data, however, have proved valuable with respect to localization of the epileptogenic focus. Ictal SPECT scans typically reveal an area of regional hyperperfusion that corresponds to the underlying epileptogenic focus as verified by surgical pathology and surface EEG localization [Bauer et al., 1989; Grunwald et al., 1991; Ho et al., 1994; Hwang et al., 1990; Katz et al., 1990; Lee et al., 1988; Marks et al., 1992; Newton et al., 1992b; Rowe et al., 1989, 1991; Shen et al., 1990; Stefan et al., 1990]. Using data pooled from several centers, the sensitivity of ictal SPECT (as judged by EEG correlation) has been estimated at 90% for temporal and 81% for extratemporal epilepsy, with specificity at 77% and 93%, respectively [Spencer, 1994]. Critical to the efficacy of the ictal SPECT scan is the timing of the injection. If the injection can be given within
1159
30 seconds of the seizure onset, the isotope remains localized and can “capture” the epileptogenic focus or generator before the epileptogenic discharge spreads [ Newton et al., 1995]. When the injection cannot be given immediately or if it is recognized that seizure propagation is rapid, observation at the time of injection for comparison with known patterns of propagation enables determination of the epileptogenic focus. Specifically, in temporal lobe epilepsy, ipsilateral basal ganglia hyperperfusion may be observed in some instances, usually correlated with contralateral arm dystonia in seizures emanating from the temporal lobe [Newton et al., 1992a]. In addition, if clonic motor activity is seen during an ictal event and before the isotope injection, contralateral hyperperfusion involving the motor cortex, basal ganglia, and thalamus may be present regardless of the location of the epileptogenic focus. Comparison of ictal and interictal scans also is important in determining whether any abnormality in blood flow is significant. With the assistance of computerized technology and surface matching techniques, co-registration of the ictal SPECT scan to the volumetric MRI scan has demonstrated a close relationship between the region of ictal hyperperfusion and MRI structural lesions [Hogan et al., 1995; Mountz et al., 1994]. A technique has been developed whereby the ictal and interictal SPECT scan data are co-registered with one another and the interictal image is subtracted from the ictal image, producing the area of true ictal hyperperfusion [Zubal et al., 1995]. This difference image, called a subtraction SPECT scan, then is co-registered with a three-dimensional representation of the MRI scan. In nonlesional extratemporal epilepsy, this information may prove to be especially helpful in either guiding placement for subdural invasive EEG monitoring or obviating the need for invasive monitoring altogether. Several studies have
A
B
FIGURE 51-7. SPECT scans. A, Ictal (upper left) and interictal (upper middle) scans, along with subtraction SPECT scan (upper right). B, Using SISCOM software (see text), subtraction scans coregistered to the MRI study (left) and with volumetric MRI (right) were obtained. MRI, magnetic resonance imaging; SPECT, single-photon emission computed tomography.
1160
Epilepsy / 51
demonstrated that periictal subtraction SPECT provides useful information for seizure localization in patients with focal malformations of cortical development, even when the MRI study is nonlocalizing (i.e., “nonlesional”) [O’Brien et al., 1998, 2000, 2004]. In a large series involving pediatric and adult epilepsy patients, if the site of the surgical resection was concordant with the subtraction SPECT localization (using SISCOM technology, a Mayo Clinic– patented computer program that performs subtraction SPECT and then co-registers the results to a volumetric MRI scan of the brain), postoperative seizure frequency scores were significantly lower and postoperative improvement was greater [O’Brien et al., 1998] (See Fig. 51-7). In summary, SPECT scan technology holds great merit and promise for the future. It is widely available and is reasonable in cost. Additionally, the new stable tracers have simplified the procedure and improved the ability to obtain accurate ictal scans. These facts, coupled with increasing resolution of the image scanners, ensure that SPECT scan technology will gain increasing prominence.
Positron Emission Tomography PET is another technique used for localization of the epileptogenic focus [Mohan et al., 1999]. It uses radiotracers
A
labeled with specific positron-emitting isotopes (11C, 15O, and 18F) to measure a variety of biochemical functions in the brain. With the aid of computerized technology and mathematical modeling, the source and concentration of the emission are either qualitatively or quantitatively plotted on a three-dimensional representation of the brain. Cerebral glucose metabolism is the most commonly measured parameter, using 18F-fluorodeoxyglucose (FDG) (Fig. 51-8). Other tracers also can be used to measure cerebral blood flow, benzodiazepine and opiate receptors, pH, serotonin metabolism, and amino acid transport [Henry et al., 1993; Mohan et al., 1999; Shah et al., 1995]. FDG PET images are averaged over a 40-minute time interval, suggesting the limited value of this technique for ictal studies. The interictal images, on the other hand, are highly sensitive in complex partial seizures emanating from the temporal lobe. In several studies in adult patients with medically refractory epilepsy of temporal lobe origin, glucose hypometabolism in the temporal lobe correlated highly with localized ictal EEGs and MRI abnormalities in this region [Abou-Khalli et al., 1987; Chugani et al., 1990; Coubes et al., 1993; Debets et al., 1990; Engel et al., 1982; Hajek et al., 1993; Henry et al., 1993; Liederman et al., 1992; Radtke et al., 1993; Sackellares et al., 1990; Stefan et al., 1987, 1990; Swartz et al., 1992; Theodore et al., 1986,
B
FIGURE 51-8. FDG PET scan from a 12-year-old girl with complex partial seizures, showing a focal decrease in glucose metabolism in the left parietal and, to a lesser extent, the left occipital cortex. The images in A and B were obtained at two different horizontal levels of the brain. EEG obtained during the scan demonstrated occasional sharp-wave discharges over the left parietal and central regions. EEG, electroencephalogram; FDG PET, fluorodeoxyglucose positron emission tomography. (Courtesy of Dr. HG Chugani and Children’s Hospital of Michigan PET Center, Wayne State University, Detroit, Michigan.)
Zupanc / Epilepsy Surgery in the Pediatric Population
1990; Valk et al., 1993]. Glucose hypometabolism in the temporal lobe, as obtained on interictal FDG PET scan, has been found to have an overall sensitivity of 84% and a specificity of 86% [Spencer, 1994]. In a study by Theodore and co-workers [1997], the presence of glucose hypometabolism on PET scan in the temporal lobe in the presence of a nonlocalizing surface ictal EEG predicted successful outcome with temporal lobectomy. Localization to the temporal lobe was confirmed with invasive EEG monitoring in these patients, but the authors make the point that invasive EEG monitoring may be unnecessary and may even provide false localizing information in some patients being evaluated for epilepsy surgery. As technology improves, concordance of noninvasive neuroimaging techniques may be all that is necessary before proceeding with the surgery. Analysis of nonlesional extratemporal epilepsy in adult patients with PET scans has provided data that have been less conflicting or less definitive. [Chugani et al., 1990; Sackellares et al., 1990; Stefan et al., 1990]. In children with refractory epilepsy, however, despite poor localization on surface EEG and negative findings on MRI scans of the brain, FDG PET scans have been useful in identifying an underlying epileptogenic focus. Specifically, University of California at Los Angeles investigators were the first to recognize a small subset of children with intractable infantile spasms and underlying deficits of focal glucose metabolism on PET scan [Chugani et al., 1988, 1990; Olson et al., 1990]. These deficits usually were temporal-parietaloccipital in origin. Many of these patients had partial seizures before, during, or after the onset of their infantile spasms, often providing a clue to localization. Additionally, interictal surface EEG examined retrospectively often disclosed focal delta slowing or an asymmetry in beta activity. Large cortical resections of the underlying epileptogenic zone were performed, guided by PET scan data and electrocorticography. After surgery, the seizures (infantile spasms and/or partial seizures) disappeared. Results indicate that not only did seizure control improve but also that these patients’ development improved at a faster rate and to a greater degree than would have been predicted without surgery [Asarnow et al., 1997; Chugani et al., 1988]. Newer ligands also have been developed. In flumazenil PET scans, the flumazenil binds to benzodiazepine receptors [Juhasz et al., 1999; Mohan et al., 1999]. In the area of the epileptogenic zone, benzodiazepine binding appears to be decreased. In one clinical study, the flumazenil PET scan demonstrated a more restricted area of decreased binding than was apparent on the FDG PET scan; the resection of this cortical region was associated with good surgical outcome [Juhasz et al., 2000]. In addition, diffuse cortical abnormalities on flumazenil PET scans predict poor seizure control following epilepsy surgery [Juhasz et al., 2001]. AMT PET scans also have been studied. AMT is a precursor for serotonin synthesis [Chugani et al., 1998; Juhasz et al., 2003]. Data suggest that the AMT PET scans can identify the most epileptogenic tuber in patients with tuberous sclerosis, multiple tubers, and medically intractable epilepsy. Concordance of the epileptogenic tuber with increased AMT uptake has been observed on PET scans [Asano et al., 2000; Chugani et al., 1998, Chugani and Muzik, 2000]. In addition, AMT PET scans also appear to be very helpful in
1161
reevaluating patients in whom epilepsy surgery has failed to effect improvement. In the patients studied with AMT PET, the area of increased AMT binding correlated closely with the epileptogenic zone [Juhasz et al., 2004].
Magnetic Resonance Spectroscopy MRS has been used in the study of patients with intractable epilepsy. Specifically, phosphorus MRS measures phospholipid metabolism. In the region of the epileptogenic focus, investigators have found abnormal phosphocreatine– to–inorganic phosphate ratios. Phosphocreatine (Pcr), intracellular pH, and inorganic phosphorus (Pi) increase during a seizure. Adenosine triphosphate concentration, however, only decreases slightly [Duncan, 1997; Prichard, 1994]. Proton MRS also can measure regional abnormalities in lactate, N-acetyl-aspartate (NAA), creatine (Cr), and choline (Cho). Lactate levels increase during a seizure and remain elevated for several hours. Data also indicate reductions in the NAA/Cho and NAA/Cr ratios in the region of the epileptogenic zone, presumed to reflect neuronal loss and reactive astrocytosis [Petroff et al., 1984, 1986; Prichard, 1994]. Therefore, abnormal NAA/Cr and NAA/ Cho ratios may serve as indices of regional cellular pathology. MRS is being applied in clinical research as an additional tool in assisting with the localization of nonlesional epilepsy [Connelly et al., 1994; Kuzniecky et al., 1992; Laxer et al., 1992; Matthews et al., 1990; Ng et al., 1993, 1994; Novotny, 1995]. In a study of children with temporal lobe epilepsy and mesial temporal sclerosis on MRI of the brain, low NAA/Cho and NAA/Cr ratios were found ipsilateral to the abnormal MRI; none demonstrated false localization [Cross et al., 1997]. Interictal SPECT scans using 99mTc-HMPAO also were performed in these children. About 71% of the children (10 of 14) had regional hypometabolism in the MRI-identified abnormal temporal lobe, and 81% demonstrated abnormal NAA/Cho + Cr ratios. The excellent correlation among interictal SPECT, MRS, and mesial temporal sclerosis on brain MRI studies suggests that neuronal cell loss is the physiologic change reflected in these noninvasive technologies. MRS holds promise as an important adjunctive noninvasive technique for assisting with the identification of the underlying epileptogenic zone.
Magnetoencephalography MEG is another technology that has been developed to improve the ability to identify epileptogenic foci. It measures tiny magnetic fields in the brain that are created by the electrical activity of the brain. Most institutions are using 128-channel MEG technology to enhance resolution. MEG offers several advantages over EEG. First, the magnetic fields are not attenuated by the skull, scalp, and skin, as are electrical potentials; therefore, the MEG signal contains fewer distortions or changes [Barth, 1993]. Second, the MEG is a monopolar measure and does not require a dipolar montage, eliminating the possibility of artifact associated with an “active reference.” Finally, and of greatest importance, MEG measures postsynaptic intracellular currents in the dendrites of neurons situated tangentially to the skull, whereas the EEG measures the extracellular postsynaptic ionic currents [Barth, 1993; Barth et al., 1984].
1162
Epilepsy / 51
Clinical research suggests that although surface interictal EEG spike recordings may indicate multifocal activity, MEG can more precisely localize the underlying epileptogenic focus [Barth, 1993; Stefan et al., 2003; Sutherling et al., 1988; Wheless et al., 1999]. MEG has provided pivotal information and may become the most precise way of identifying the size, location, and dipole orientation of the epileptogenic zone [Minassian et al., 1999; Stefan et al., 2003; Wheless et al., 1999, 2004]. In addition, MEG may be a very useful tool in children with respect to functional imaging, particularly imaging language cortex [Papanicolaou et al., 2004; Simos et al., 1999].
Functional Mapping If an underlying epileptogenic focus is identified, the next question to consider is whether the epileptogenic zone can be removed without causing unacceptable neurologic deficits. In infants and young children, this proves to be less problematic because of brain plasticity. Classically, in the older child and adolescent, the sodium amytal test (Wada test) is used in the preoperative evaluation for the localization of speech and language and to determine whether memory can be supported in the contralateral hemisphere [Loring, 1997; Wyllie et al., 1990]. This test involves injecting sodium amytal into either the left or the right internal carotid artery, in an attempt to chemically ameliorate ipsilateral hemispheric function and determine which hemisphere is “dominant” (i.e., responsible for speech and language function and, to a lesser extent, memory). It is a time-consuming test that is invasive and provides a broad but nonspecific overview of hemispheric function. Additionally, controversy is ongoing over its interpretation and its ability to predict postoperative function, particularly with respect to memory [Loring et al., 1992; Perrine, 1994]. As an example, language is a complex function. Although speech arrest after sodium amytal injection usually is in the dominant hemisphere, this is not always the case [Loring et al., 1992]. Language involves spontaneous speech, repetition, comprehension, reading, and counting. These aspects of language are all interactive, but their correponding cortical areas may be located in different areas of the brain, making it difficult
to relegate language to one specific hemisphere or region. In younger children, the Wada test can be even more challenging and technically difficult. Obtaining full cooperation from a child requires preparation, time, and patience. If the child becomes frightened during the test, test validity becomes questionable. Two other techniques also used frequently to identify eloquent cortex (i.e., cortex controlling vital motor, language, or memory functions) are somatosensory-evoked potentials and stimulation mapping. The measurement of somatosensory evoked potentials has the advantage of being able to be applied successfully regardless of the state of the patient. This modality can be used in the operating room in the anesthetized patient or in an awake and cooperative patient. Somatosensory-evoked potentials are used primarily to identify the sensorimotor cortex. Stimulation mapping is another useful technique in the identification of eloquent cortex. This technique involves the application of subdural electrodes followed by sequential electrical stimuli at various intensities and durations. Penfield pioneered this technique during the 1930s through the 1950s to localize language and motor functions intraoperatively, to avoid postoperative neurologic deficits. Subsequent investigators have used cortical stimulation preoperatively (using implanted grid electrodes) and intraoperatively to map out functional cortex, such as the sensorimotor cortex or expressive language cortex [Ojemann, 1978, 1979, 1993; Ojemann and Dodrill, 1987]. Although cortical stimulation mapping has yielded a tremendous amount of information about the localization of functions, several other emerging techniques are providing valid, noninvasive methods for mapping out functional areas of the brain. These techniques include functional MRI scans, MEG and magnetic source imaging, and transcranial magnetic stimulation [Binder, 1997; Detre, 2004; Knowlton and Shih, 2004; Peresson et al., 1998; Perrine, 1994; Powell et al., 2004; Sabsevitz et al., 2003; Wheless et al., 2004]. In view of the limitations of the previously described techniques for functional mapping, other noninvasive techniques that might provide more specific and salient information are being developed. Functional MRI scans are being used experimentally in a number of epilepsy centers to define eloquent cortex [Kwong et al., 1992; Lee et al., 1996;
FIGURE 51-9. Functional MRI scan. Identification of left hemisphere motor cortex was achived by asking the patient to open and close his right hand repetitively. Functional activity (in white) is superimposed on gray scan multishot echo planar images. MRI, magnetic resonance imaging.
Zupanc / Epilepsy Surgery in the Pediatric Population
Ogawa et al., 1992]. Functional MRI is based on the fact that performance of a specific act will activate the anatomically appropriate cortex in the brain. With activation, a concomitant increase in blood flow occurs, resulting in a change in the paramagnetic properties of the affected cortex. This produces a signal that can then be detected by the MRI scanner. Functional MRI is a technique that will be increasingly used in the future to map out eloquent functions, such as sensorimotor cortex and speech and language centers [Logan et al., 1995, 1997, 1998]. It is still unsuitable for the young, uncooperative infant or child, but for older children and adolescents, clinical research is yielding increasing proof that functional MRI can provide important localization data. In the young infant and child, functional studies are less likely to alter surgical resection because the enhanced plasticity of the brain in these age groups makes localization less criticial [Shields, 2000; Stafstrom et al., 2000; Wyllie, 1998]. An example of a functional MRI scan is illustrated in Figure 51-9.
TYPES OF SURGERY Several types of epilepsy surgery are performed in children and adults, depending on the identification of the epileptogenic focus and its location and extent [Zupanc, 1997b]. The most common surgical procedures are (1) temporal lobectomy; (2) cortical resection; (3) stereotactic lesionectomy; (4) hemispherectomy—either functional, modified hemispherectomy or anatomic hemispherectomy; (5) multiple subpial transection; and (6) corpus callosotomy. Temporal lobectomy is the most common epilepsy surgery performed in adolescents and adults. This procedure is almost exclusively a temporal lobectomy with amygdalohippocampectomy, because the removal of the mesial temporal structures is correlated with good surgical outcome. Often an associated abnormality or lesion, such as a tumor (DNET or ganglioglioma), mesial temporal sclerosis, hippocampal formation atrophy, or malformation of cortical development, is found to be present. The new technologies currently available in MRI have been helpful in identification of these substrates of epilepsy. Those patients with mesial temporal sclerosis or hippocampal atrophy concordant with ictal surface EEG abnormalities have an excellent prognosis for successful epilepsy surgery, with a 90% chance of becoming seizure free [Duchowny et al., 1992; Falconer, 1970; Mizrahi et al., 1990]. Younger children do not commonly have mesial temporal sclerosis or hippocampal atrophy [Ng et al., 2004]. Many of the intractable epilepsies in childhood are extratemporal and nonlesional. Extratemporal cortical resection commonly is performed in children, often involving extensive lobar or multilobar resections. The extent of the resection is dictated primarily by the extent of the lesion. For example, a simple tuberectomy in a patient with tuberous sclerosis or a multilobar resection in a child with infantile spasms and an underlying focal cortical dysplasia involving the temporal-parietaloccipital lobes might be performed. As the ability to identify focal cortical dysplasias and the concomitant epileptogenic zone improves, epilepsy surgical outcomes also will improve. Focal cortical dysplasias are a common cause of intractable partial epilepsy in children, accounting for 60%
1163
of the cases [Kuzniecky and Barkovich, 2001; Kuzniecky et al., 1993c]. The best predictive factor in successful surgical outcome is completeness of the resection. Stereotactic lesionectomy is performed in highly selected cases in children and adults, with a reported 50% to 60% chance of rendering the patient seizure free [Britton et al., 1994; Cascino et al., 1990, 1992, 1993, 1994]. Outcome is improved if intraoperative electrocorticography is used to remove not only the lesion but also the surrounding “epileptogenic zone” [Jooma et al., 1995; Montes et al., 1995; Palmini et al., 1995; Pilcher et al., 1993]. To date, no prospective, controlled studies of statistically significant numbers of patients have critically compared the different operative strategies with respect to outcome [Shields, 2000; Tonini et al., 2004; Wyllie, 1998]. The surgical outcome in these patients may vary, depending on the age of the patient, location of lesion, and most important, the type of lesion. In a review of 47 published articles about epilepsy surgery outcome, the best predictors for seizure-free outcome were found to include history of febrile seizures as a child, mesial temporal sclerosis, tumors, EEG and MRI data concordance, and an extensive surgical resection [Tonini et al., 2004]. Hemispherectomy also is performed in young children [Vining et al., 1997]. The indications for this type of surgery are catastrophic epilepsies in which the substrate of epilepsy is limited to one hemisphere. Epileptic syndromes that frequently meet these criteria include the following: (1) Sturge-Weber syndrome, (2) hemimegalencephaly, and (3) Rasmussen’s encephalitis. In Sturge-Weber syndrome, the pathologic features consist of unilateral leptomeningeal angiomatosis, frequently resulting in changes in the involved hemisphere with concomitant focal seizures, progressive hemiparesis, and cognitive decline [Roach et al., 1994]. Hemimegalencephaly, by definition, is a malformation of cortical development involving one hemisphere and is characterized by general disorganization and overgrowth of the neuronal tissue. Early hemispherectomy, particularly if the EEG reveals unilateral discharges, can significantly alter the prognosis in affected children [Andermann et al., 1993; Vivegano et al., 1989; Vivegano and DiRocco, 1990]. With Rasmussen’s encephalitis, children have intractable focal seizures, often progressing to epilepsia partialis continua, accompanied by progressive hemiparesis and cognitive decline. Although debate is ongoing about the pathophysiology (autoimmune versus infectious), the only long-term successful treatment has been hemispherectomy [Antel and Rasmussen, 1996]. Multiple subpial transection is a newer surgical technique that is used when the epileptogenic zone overlies an area of functional cortex. Multiple subpial transection involves the disruption of connecting horizontal fibers, rather than resection of actual tissue [Blount et al., 2004; Devinsky et al., 2003; Schramm et al., 2002; Spencer et al., 2002]. This technique has been used in the treatment of LandauKleffner syndrome [Morrell et al., 1995]. Children with this syndrome have an acquired epileptic aphasia, often intractable to medication. The multiple subpial transection technique has been used over the area deemed to be the epileptogenic zone on electrocorticography. Although good surgical results have been reported, the technique remains controversial. Multiple subpial transection also is being used in areas involving functional cortex. Data indicate that although multiple sub-
1164
Epilepsy / 51
pial transection may be an appropriate adjunctive surgical technique, it will not eliminate seizures if the primary epileptogenic focus is not completely removed [Hufnagel et al., 1997; Spencer et al., 2002]. Corpus callosotomy is a palliative surgery that can reduce the seizure burden in carefully selected patients. It most commonly is used in children with Lennox-Gastaut syndrome, with the goal being reduction of tonic and atonic seizures. It can be highly effective [Carson, 2000; Maehara and Shimizu, 2001; McInerney et al., 1999; Sassower et al., 2001; Sorenson et al., 1997]. Most often, callosotomy of the anterior two thirds of the corpus callosum initially is performed, to minimize postoperative side effects. If seizures return or persist, the corpus callosotomy can be completed [Geoffroy et al., 1983; Wyler, 1993].
GOALS OF SURGERY With use of innovative, noninvasive technologies, the ability of the clinician to identify the underlying epileptogenic zone has improved. In patients with medically intractable epilepsy, this ability allows one of the principal goals of epilepsy surgery to be achieved—that is, the elimination of seizures. The goals of epilepsy surgery, however, may vary, depending on the epileptic syndrome, the underlying pathophysiology, the cognitive and developmental status of the child or adolescent, and the identification and location of an epileptogenic zone [Taylor et al., 1997]. Specifically, if a cognitively normal patient has temporal lobe epilepsy as documented by congruence of seizure semiology and EEG and MRI data, the goals of epilepsy surgery are clear: elimination of seizures and improvement in psychosocial, behavioral, emotional, and family functioning without significant loss of cognitive abilities. On the other hand, a cognitively impaired patient with an extensive bilateral malformation of cortical development might be considered for a corpus callosotomy. In this case, the primary goals of epilepsy surgery would be the reduction of seizures and possible improvement in cognitive and behavioral functions. Although improvement in cognition, development, and behavior usually is achieved by virtue of decreased seizure frequency and reduction of antiepileptic drug doses, such results are not always obtained, and outcomes will vary with each patient, depending on the epilepsy syndrome and the identified etiology for the epilepsy. The goals of epilepsy surgery and potential limitations of the results of surgery need to be discussed openly with the family before any decision is made. In patients with malformations of cortical development (in children, typically extratemporal), epilepsy surgery usually has involved lobar or multilobar resections, as well as hemispherectomies. Approximately 60% to 65% of these patients are seizure free after surgery, and a majority achieve a significant reduction in seizure burden [Shields, 2000; Wyllie, 1998]. At critical stages of development, this reduction in seizure burden is associated with an improvement in development that appears to be sustained. In patients with malformations of cortical development and medically refractory epilepsy who undergo surgical resection, withdrawal of antiepileptic medication is rarely successful. The cortical dysplasia often is very extensive,
involving multiple lobes. On the other hand, children with lesions such as mesial temporal sclerosis, low-grade tumors, or middle cerebral artery infarctions can achieve seizurefree status, with eventual discontinuation of antiepileptic medication.
RESEARCH ISSUES: TRENDS FOR THE FUTURE The following are some of many unanswered questions to be addressed in the pursuit of helping children with intractable epilepsy: • What are the age-specific developmental mechanisms in childhood epilepsy? Can they be targeted for the development of new and more effective antiepileptic drugs or surgical therapy? • In children with similar electrographic findings and seizure semiology, why do some respond to antiepileptic drugs whereas others do not? What clues might this information provide about the mechanisms of epilepsy and possible treatments? • What is the definition of seizure intractability in children? This concept is in evolution and likely depends on multiple factors, including the natural history of the epileptic syndrome, etiology of the seizures, seizure frequency, and the degree to which the seizures and antiepileptic drug therapy impact the quality of life. • Does a time frame exist during which specific epileptic syndromes mandate intervention, because of either (1) windows of developmental opportunity or (2) diminishing capabilities of neural plasticity? What can we learn about the dimensions of neural plasticity? • Do seizures contribute to the development of cognitive impairments and to what degree? Can prompt surgery in patients with catastrophic epilepsy ameliorate cognitive impairments? • Can early successful intervention, with either antiepileptic drugs or epilepsy surgery, result in an improvement in the quality of life for patients with epilepsy? Future trends for exploration will involve several avenues of research: source localization and predictive EEG patterns for identification of the epileptogenic zone [Smart et al., 2004; Worrell, 2004]; implantable devices that can detect predictive EEG patterns before a clinical seizure and deliver either an abortive dose of antiepileptic medication or an abortive electrical stimulus; deep brain cortical-thalamic stimulation to diminish seizure frequency in those patients with subcortical-cortical epileptogenic networks (intractable nonlesional, generalized epilepsy syndromes); and, finally, “designer” antiepileptic drugs targeting specific mechanisms of epilepsy—most likely sodium, potassium, calcium, and γ-aminobutyric acid channels—to be delivered locally or systemically. REFERENCES Abou-Khalil BW, Siegel GJ, Sackellares JC, et al. Positron emission tomography studies of cerebral glucose metabolism in chronic partial epilepsy. Ann Neurol 1987;22:480.
Zupanc / Epilepsy Surgery in the Pediatric Population Adams C, Hwang PA, Gilday DL, et al. Comparison of SPECT, EEG, CT, MRI, and pathology in partial epilepsy. Pediatr Neurol 1992;8:97. Adler J, Erba G, Winston KR, et al. Results of surgery for extratemporal partial epilepsy that began in childhood. Arch Neurol 1991;48:133. Aicardi J. Benign partial epilepsies. In: Epilepsy in children, 2nd ed. New York: Raven Press, 1994. Andermann FA, Freeman JM, Vivegano F, et al. Surgically remediable diffuse hemispheric syndromes. In: Engel JJ, ed. Surgical treatment of the epilepsies, 2nd ed. New York: Raven Press, 1993. Andrews PI, Dichter MA, Berkovic SF, et al. Plasmapheresis in Rasmussen’s encephalitis. Neurology 1996;46:242. Annegers JF, Hauser WA, Elveback LR. Remission of seizures and relapse in patients with epilepsy. Epilepsia 1979;20:729. Antel JP, Rasmussen T. Rasmussen’s encephalitis and the new hat. Neurology 1996;46:9. Arts WFM, Visser LH, Loonen MCB, et al. Follow-up of 146 children with epilepsy after withdrawal of antiepileptic therapy. Epilepsia 1988;29:244. Asano E, Chugani DC, Muzik O, et al. Multimodality imaging for improved detection of epileptogenic foci in tuberous sclerosis complex. Neurology 2000;54:1976. Asarnow RF, LoPresti C, Elliott T. Developmental outcomes in children receiving resection surgery for medically intractable infantile spasms. Dev Med Child Neurol 1997;39:430. Barth DS, Sutherling WW, Engel J, et al. Neuromagnetic evidence of spatially distributed sources underlying epileptiform spikes in the human brain. Science 1984;223:293. Barth DS. Magnetoencephalography. In: Wyllie E, ed. The treatment of epilepsy: Principles and practice. Philadelphia: Lea and Febiger, 1993. Bauer J, Stefan H, Huk WJ, et al. CT, MRI and SPECT neuroimaging in status epilepticus with simple partial and complex partial seizures: Case report. J Neurol 1989;236:296. Bazil CW. Comprehensive care of the epilepsy patient—control, comorbidity, and cost. Epilepsia 2004;45 (Suppl 6):3. Bebin EM, Kelly PJ, Gomez MR. Surgical treatment for epilepsy in cerebral tuberous sclerosis. Epilepsia 1993;34:651. Begley CE, Annegers JF, Lairson DR, et al. Cost of epilepsy in the United States: A model based on incidence and prognosis. Epilepsia 1994;35:1230. Begley CE, Famulari M, Annegers JF, et al. The cost of epilepsy in the US: An estimate from population-based clinical and survey data. Epilepsia 2000;41:342. Berg AT, Shinnar S, Levy SR, et al. Two year remission and subsequent relapse in children with newly diagnosed epilepsy. Epilepsia 2001;42:1553. Berkovic SF, Newton MR, Chiron C, et al. Single photon emission tomography. In: Engel J Jr, ed. Surgical treatment of the epilepsies, 2nd ed. New York: Raven Press, 1993. Berkovic SF, Rowe CC. The use of SPECT in focal epilepsy. In: Luders HO, ed. Epilepsy surgery. New York: Raven Press, 1992. Bharucha NE, Bharucha AE, Bharucha EP. Prevalence of epilepsy in the Parsi community of Bombay. Epilepsia 1988;29:111. Binder J. Functional magnetic resonance imaging language mapping. Neurosurg Clin N Am 1997;8:383. Blanchette N, Smith ML. Language after temporal or frontal lobe surgery in children with epilepsy. Brain Cogn 2002;3:51. Blount JP, Langburt W, Otsubo H, et al. Multiple subpial transactions in the treatment of pediatric epilepsy. J Neurosurg Spine 2004;100:118. Bourgeois M, Sainte-Rose C, Lellouch-Tubiana A, et al. Surgery of epilepsy associated with focal lesions in childhood. J Neurosurg 1999;90:833. Britton JW, Cascino GD, Sharbrough FW, et al. Low-grade glial neoplasms and intractable partial epilepsy: Efficacy of surgical treatment. Epilepsia 1994;35:1130. Brockhaus A, Elger CE. Complex partial seizures of temporal lobe origin in children of different age groups. Epilepsia 1995;36:1173. Brooks B, King D, El Gammal T, et al. MRI in patients with intractable complex partial seizures. AJNR Am J Neuroradiol 1990;11:93. Camfield P, Camfield C. Childhood epilepsy: What is the evidence for what we think and what we do? J Child Neurol 2003;18:272. Carson BS. Indications and outcomes for lobectomy, corpus callosotomy, and hemispherectomy in pediatric neurosurgical patients. Clin Neurosurg 2000;47:385. Cascino GD, Hirschorn KA, Jack CR, et al. Gadolinium-DTPA enhanced MRI in intractable partial epilepsy. Neurology 1989;39:1115.
1165
Cascino GD, Hulihan JF, Sharbrough FW, et al. Parietal lobe lesional epilepsy: Electroclinical correlation and operative outcome. Epilepsia 1993;34:52. Cascino GD, Jack CR Jr, Parisi JE, et al. MRI-based volume studies in temporal lobe epilepsy: Pathologic correlations. Ann Neurol 1991;30:31. Cascino GD, Kelly PJ, Hirschorn KA, et al. Stereotactic resection of intra-axial cerebral lesions in partial epilepsy. Mayo Clinic Proc 1990;65:1053. Cascino GD, Kelly PJ, Sharbrough FW, et al. Long-term follow-up of stereotactic lesionectomy in partial epilepsy: Predictive factors and electroencephalographic results. Epilepsia 1992;33:639. Cascino GD, Sharbrough FW, Trenerry MR, et al. Extratemporal cortical resections and lesionectomies for partial epilepsy: Complications of surgical treatment. Epilepsia 1994;35:1085. Cascino GD. Commentary: How has neuroimaging improved patient care? Epilepsia 1994;35:S103. Caton R. The electrical currents of the brain. BMJ 1875;2:278. Cendes F, Andermann F, Gloor P, et al. Atrophy of mesial structures in patients with temporal lobe epilepsy: Causes or consequence of repeated seizures? Ann Neurol 1993;34:795. Chugani DC, Chugani HT, Muzik O, et al. Imaging epileptogenic tubers in children with tuberous sclerosis complex using alpha 11 C-methyl-L-tryptophan positron emission tomography. Ann Neurol 1998;44:858. Chugani DC, Muzik O. Alpha (C-11) methyl-L-tryptophan PET maps brain serotonin synthesis and kynurenine pathway metabolism. J Cereb Blood Flow Metab 2000;20:2. Chugani HT, Shewmon A, Shields WD, et al. Pediatric epilepsy surgery: Pre-and postoperative evaluation with PET. J Epilepsy 1990;3:75. Chugani HT, Shewmon DA, Peacock WJ, et al. Surgical treatment of intractable neonatal onset seizures: The role of positron emission tomography. Neurology 1988;38:1178. Chugani HT, Shewmon DA, Shields WD, et al. Surgery for intractable infantile spasms. Neuroimaging perspectives. Epilepsia 1993;34:764. Chugani HT, Shields WD, Shewmon DA, et al. Infantile spasms: I. PET identified focal cortical dysgenesis in cryptogenic cases for surgical treatment. Ann Neurol 1990;24:405. Connelly A, Jackson GD, Duncan JS, et al. Magnetic resonance spectroscopy in temporal lobe epilepsy. Neurology 1994;44:1411. Cordes M, Christie W, Henkes H, et al. Focal epilepsies: HMPAO SPECT compared with CT, MR, and EEG. J Comput Assist Tomogr 1990;14:402. Coubes P, Awad IA, Antar M, et al. Comparison and spatial correlation of interictal HMPAO-SPECT and FDG-PET in intractable temporal lobe epilepsy. Neurol Res 1993;15:160. Cross JH, Gordon I, Connelly A, et al. Interictal 99mTc HMPAO SPECT and 1H MRS in children with temporal lobe epilepsy. Epilepsia 1997;38:338. Cross JH, Gordon I, Jackson GD, et al. Children with intractable focal epilepsy: Ictal and interictal 99mTc HMPAO single photon emission computed tomography. Dev Med Child Neurol 1995;37:673. Danielsson S, Rydenhag B, Uvebrant P, et al. Temporal lobe resection in children with epilepsy: Neuropsychiatric status in relation to neuropathology and seizure outcome. Epilepsy Behav 2002;3:76. Davidson S, Falconer MA. Outcome of surgery in 40 children with temporal-lobe epilepsy. Lancet 1975;1:1260. Debets RMC, van Veelen CWM, Maquet P, et al. Quantitative analysis of 18 FDG-PET in the presurgical evaluation of patients suffering from refractory partial epilepsy: Comparison with CT, MRI, and combined subdural and depth EEG. Acta Neurochir Suppl (Wien) 1990;50:88. Denays R, Rubinstein M, Ham H, et al. Single photon emission computed tomography in seizure disorders. Arch Dis Child 1988;63:1184. Detre JA. Functional MRI: Applications in epilepsy. Epilepsia 2004;45 (Suppl 4):26. Devinsky O, Romanelli P, Orbach D, et al. Surgical treatment of multifocal epilepsy involving eloquent cortex. Epilepsia 2003;44:718. Dietrich ME, Bergen D, Smith MC, et al. Correlation of abnormalities of interictal N-isopropyl-p-iodoamphetamine single-photon emission tomography with focus of seizure onset in complex partial seizure disorders. Epilepsia 1991;32:187. Dobyns WB, Andermann E, Andermann F, et al. X-linked malformations of neuronal migration. Neurology 1996;47:331. Dobyns WB, Truwit CL. Lissencephaly and other malformations of cortical development: 1995 update. Neuropediatrics 1995;26:132.
1166
Epilepsy / 51
Duchowny M, Jayakar P, Resnick T, et al. Epilepsy surgery in patients under age 3 years. Ann Neurol 1996;40:286. Duchowny M, Jayakar P, Resnick T, et al. Epilepsy surgery in the first three years of life. Epilepsia 1998;39:737. Duchowny M, Lewin B, Jayakar P, et al. Temporal lobectomy in children. Epilepsia 1992;33:298. Duchowny MS, Resnick TK, Alvarez LA, et al. Focal resection for malignant partial seizures in children. Neurology 1990;40:980. Duncan JS. Magnetic resonance spectroscopy. Epilepsia 1997;37:598. Emerson R, D’Souza BJ, Vining EP, et al. Stopping medication in children and epilepsy predictors of outcome. N Engl J Med 1981;304:1125. Engel J Jr, Kuhl DE, Phelps ME, et al. Interictal cerebral glucose metabolism in partial epilepsy and its relation to EEG changes. Ann Neurol 1982;12:510. Engel J Jr. Surgery for seizures. N Engl J Med 1996;334:647. English RJ, Brown SE. Single photon emission computed tomography—a primer. New York: Society of Nuclear Medicine, 1990. Erba G, Cavazzuti V. Sturge-Weber syndrome: Natural history and indications for surgery. J Epilepsy 1990;3 (Suppl 1):287. Falconer MA. Significance of surgery for temporal lobe epilepsy in childhood and adolescence. J Neurosurg 1970;33:233. Flanigin HF, Hermann BP, King DW, et al. The history of surgical treatment of epilepsy in North America prior to 1975. In: Luders H, ed. Epilepsy surgery. New York: Raven Press, 1991. Fuerst D, Shah J, Shah A, et al. Hippocampal sclerosis is a progressive disorder: A longitudinal volumetric MRI study. Ann Neurol 2003;53:413. Gillam F, Wyllie E, Kashden J, et al. Epilepsy surgery outcome: Comprehensive assessment in children. Neurology 1997;48:1368. Gleissner U, Sassen R, Lendt M, et al. Pre- and postoperative verbal memory in pediatric patients with temporal lobe epilepsy. Epilepsy Res 2002;51:287. Geoffroy G, Lassonde M, Delisle F, et al. Corpus callosotomy for control of intractable epilepsy in children. Neurology 1983;33:891. Goldensohn ES, Porter RJ, Schwartzkroin PA. The American Epilepsy Society: An historic perspective on 50 years of advances in research. Epilepsia 1997;38:124. Grunwald F, Durwen HF, Bockisch A, et al. Technetium-99m-HMPAO brain SPECT in medically intractable temporal lobe epilepsy: A postoperative evaluation. J Nucl Med 1991;32:388. Haerer AF, Anderson DW, Schoenber BS. Prevalence and clinical features of epilepsy in a biracial United States population. Epilepsia 1986;27:66. Hajek M, Antonini A, Leenders KL, et al. Mesiobasal versus lateral temporal lobe epilepsy: Metabolic differences in the temporal lobe shown by interictal 18F-FDG positron emission tomography. Neurology 1993;43:79. Hajek M, Siegel A, Haldemann R, et al. Value of HMPAO-SPECT in selective temporal lobe surgery for epilepsy. J Epilepsy 1991;4:43. Hart YM, Cortez M, Andermann F, et al. Medical treatment of Rasmussen’s syndrome (chronic encephalitis and epilepsy): Effect of high-dose steroids or immunoglobulin in 19 patients. Neurology 1994;44:1030. Harvey AS, Bowe JM, Hopkins IJ, et al. Ictal 99Tc HMPAO single photon emission computed tomography in children with temporal lobe epilepsy. Epilepsia 1993a;34:869. Harvey AS, Hopkins IJ, Bowe JM, et al. Frontal lobe epilepsy: Clinical seizure characteristics and localization with ictal 99mTc-HMPAO SPECT. Neurology 1993b;43:1966. Harvey AS, Nolan T, Carlin JB. Community-based study of mortality in children with epilepsy. Epilepsia 1993c;34:597. Hathaway S, Kasnic K, Barkley G, et al. Comparison of medical and surgical costs for the treatment of intractable epilepsy. Epilepsia 1995;36:95 (abstract). Hauser WA. The natural history of seizures. In: Wyllie E, ed. The treatment of epilepsy: Principles and practice. Philadelphia: Lea and Febiger, 1993. Hauser WA. The prevalence and incidence of convulsive disorders in children. Epilepsia 1994;35 (Suppl 2):S1. Hauser WA, Annegers JF, Brodie MJ, et al. Mortality in patients with epilepsy. Epilepsia 1980;21:399. Hauser WA, Annegers JF, Kurland LT. The prevalence of epilepsy in Rochester, Minnesota, 1940-1980. Epilepsia 1991;32:429. Hauser WA, Annegers JF, Rocca WA. Descriptive epidemiology of epilepsy: Contributions of population-based studies from Rochester, Minnesota. Mayo Clin Proc 1996;71:576.
Hauser WA, Kurland LT. The epidemiology of epilepsy in Rochester, Minnesota, 1935 through 1967. Epilepsia 1975;16:1. Hauser WA, Rich SS, Lee JR, et al. Risk of recurrent seizures after two unprovoked seizures. N Engl J Med 1998;338:429. Henry TR, Chugani HT, Abou-Khalil BW, et al. Positron emission tomography. In: Engel J Jr, ed. Surgical treatment of the epilepsies, 2nd ed. New York: Raven Press, 1993. Ho SS, Berkovic SF, Newton MR, et al. Parietal lobe epilepsy: Clinical features and seizure localization by ictal SPECT. Neurology 1994;44:2277. Hoffman HH, Hendrick EG, Dennis M, et al. Hemispherectomy for Sturge-Weber syndrome. Child Brain 1979;5:233. Hogan RE, Cook MJ, Kilpatrick CJ, et al. Accuracy of coregistration of single photon emission tomography with MR images using a brain surface matching technique. AJNR Am J Neuroradiol 1996;17:793. Holmes GL. Benign focal epilepsies of childhood. Epilepsia 1993;34:S49. Holmes GL, Ben-Ari Y. Seizures in the developing brain: Perhaps not so benign after all. Neuron 1998;21:1231. Holmes GL, Gaiarsa J-L, Chevassus-Au-Louis N, et al. Consequences of neonatal seizures in the rat: Morphological and behavioral effects. Ann Neurol 1998;44:845. Hufnagel A, Zentner J, Fernandez G, et al. Multiple subpial transection for control of epileptic seizures: Effectiveness and safety. Epilepsia 1997;38:678. Hwang PA, Gilday DL, Adams C, et al. SPECT studies in epilepsy: Application to epilepsy surgery in children. J Epilepsy 1990;3:83. Jack CR. Neuroimaging and anatomy: Magnetic resonance imaging. Neuroimag Clin North Am 1995;5:1. Jalava M, Sillanpaa M, Camfield C, et al. Social adjustment and competence 35 years after onset of childhood epilepsy: A prospective study. Epilepsia 1997;38:708. Jayakar P, Duchowny MS. Complex partial seizures of temporal lobe origin in early childhood. J Epilepsy 1990;3 (Suppl):41. Jokeit H, Ebner A, Arnold S, et al. Bilateral reductions of hippocampal volume, glucose metabolism, and Wada hemispheric memory performance are related to the duration of mesial temporal lobe epilepsy. J Neurol 1999;246:926. Jooma R, Yeh HS, Privitera MD, et al. Lesionectomy versus electrophysiologically guided resection for temporal lobe tumors manifesting with complex partial seizures. J Neurosurg 1995;83:231. Juhasz C, Chugani DC, Muzik O, et al. Electroclinical correlates of flumazenil and fluorodeoxyglucose PET abnormalities in lesional epilepsy. Neurology 2000;55:825. Juhasz C, Chugani DC, Muzik O, et al. Relationship of flumazenil and glucose PET abnormalities to neocortical epilepsy surgery outcome. Neurology 2001;56:1650. Juhasz C, Chugani DC, Muzik O, et al. Alpha-methyl-L-tryptophan PET detects epileptogenic cortex in children with intractable epilepsy. Neurology 2003;60:960. Juhasz C, Chugani DC, Padhye UN, et al. Evaluation with alpha(11C)methyl-L-tryptophan positron emission tomography for reoperation after failed epilepsy surgery. Epilepsia 2004;45:124. Juhasz C, Nagy F, Muzik O, et al. [11C]flumazenil PET in patients with epilepsy with dual pathology. Epilepsia 1999;40:566. Juul-Jensen P, Foldsprang A. Natural history of epileptic seizures. Epilepsia 1983;24:297. Kalviainen R, Salmenpera T, Partanen K, et al. Recurrent seizures may cause hippocampal damage in temporal lobe epilepsy. Neurology 1998;50:1377. Katz A, Bose A, Lind SJ, et al. SPECT in patients with epilepsia partialis continua. Neurology 1990;40:1848. Keene DL, Loy-English I, Ventureya EC. Long-term socioeconomic outcome following surgical intervention in the treatment of refractory epilepsy in childhood and adolescence. Childs Nerv Syst 1998;14:362. King DW, Flanigin HF, Gallagher BB, et al. Temporal lobectomy for partial complex seizures: Evaluation, results and 1-year follow-up. Neurology 1986;36:334. King JT, Sperling MR, Justice AC, et al. A cost-effectiveness analysis of anterior temporal lobectomy for intractable temporal lobe epilepsy. J Neurosurg 1997;87:20. Knowlton RC, Shih J. Magnetoencephalography in epilepsy. Epilepsia 2004;45 (Suppl 4):61. Kobayashi K, Ohtsuka Y, Ohno S, et al. Clinical spectrum of epileptic spasms associated with cortical malformation. Neuropediatrics 2001;32:236.
Zupanc / Epilepsy Surgery in the Pediatric Population Koh S, Jayakar P, Dunoyer C, et al. Epilepsy surgery in children with tuberous sclerosis complex: Presurgical evaluation and outcome. Epilepsia 2000;41:1206. Koh S, Jayakar P, Resnick T, et al. The localizing value of ictal SPECT in children with tuberous sclerosis complex and refractory partial epilepsy. Epileptic Disord 1999;1:41. Kotloski R, Lynch M, Lauersdorf S, et al. Repeated brief seizures induce progressive hippocampal neuron loss and memory deficits. Prog Brain Res 2002;135:95. Krauss GL, Campbell ML, Roche KW, et al. Chronic steroid-responsive encephalitis without autoantibodies to glutamate receptor GluR3. Neurology 1996;46:247. Kuks JBM, Cook KJ, Fish DR, et al. Hippocampal sclerosis in epilepsy and childhood febrile seizures. Lancet 1993;342:1391. Kuzniecky RI, Barkovich AJ. Malformations of cortical development and epilepsy. Brain Dev 2001;23:2. Kuzniecky R, Cascino G, Palmini A, et al. Structural neuroimaging. In: Engel JE, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1993a. Kuzniecky R, Elgavish GA, Hetherington HP, et al. In vivo 31P nuclear magnetic resonance spectroscopy of human temporal lobe epilepsy. Neurology 1992;42:1586. Kuzniecky R, Mountz JM, Wheatley G, et al. Ictal single photon emission computed tomography demonstrates localized epileptogenesis in cortical dysplasia. Ann Neurol 1993b;34:627. Kuzniecky R, Murro A, King D, et al. Magnetic resonance imaging in childhood intractable partial epilepsies: Pathologic correlations. Neurology 1993c;43:681. Kuzniecky, Ruben I. MRI in cerebral developmental malformations and epilepsy. Magn Reson Imag 1995;13:1137. Kwong KK, Belliveau JW, Chesler DA, et al. Dynamic magnetic resonance imaging of human brain activity during primary sensory stimulation. Proc Natl Acad Sci U S A 1992;89:5675. Lamanna MM, Sussman NM, Harner RN, et al. Initial experience with SPECT imaging of the brain using I-123 p-iodoamphetamine in focal epilepsy. Clin Nucl Med 1989;14:428. Lanceman ME, Morris HH, Raja S, et al. Usefulness of ictal and interictal 99m Tc ethyl cysteinate dimer single photon emission computed tomography in patients with refractory partial epilepsy. Epilepsia 1997;38:472. Laoprasert P, Zupanc ML. Malformations of cortical development and epilepsy surgery outcome in children and adults. Epilepsia 1997;38:78. Launes J, Iivanainen M, Salmi T, et al. Interictal brain 99m-Tc-HMPAO SPECT hypoperfusion in patients with unstable partial epilepsy and normal CT. Acta Neurol Scand 1992;86:558. Laxer KD, Hubesch B, Sappey MD, et al. Increased pH and inorganic phosphate in temporal seizure foci demonstrated by 31P MRS. Epilepsia 1992;33:178. Lee BI, Markand ON, Wellman HN, et al. HIPDM-SPECT in patients with medically intractable complex partial seizures: Ictal study. Arch Neurol 1988;46:397. Lee CC, Riederer SJ, Jack CR. The specificity of sensorimotor mapping using functional MRI. Epilepsia 1996;37:206. Leiderman OB, Balish M, Sato S, et al. Comparison of PET measurements of cerebral blood flow and glucose metabolism for the localization of human epileptic foci. Epilepsy Res 1992;13:153. Lendt M, Gleissner U, Helmstaedter C, et al. Neuropsychological outcome in children after frontal lobe epilepsy surgery. Epilepsy Behav 2002;3:51. Lendt M, Helmstaedter C, Kuczaty S, et al. Behavioural disorders in children with epilepsy: Early improvement after surgery. J Neurol Neurosurg Psychiatry 2000;69:739. Locock C. Discussion of a paper by EH Sievking: Meeting of the Royal Medical and Chirurgical Society of London. Lancet 1857;1:527. Logan WJ, Benson RR, Cosgrove GR, et al. Functional MRI (fMRI) localization of language in children. Can J Neurol Sci 1995;22:24. Logan WJ, Crawley AP, Mikulis DJ. Functional MRI: An imaging technique particularly suited for children. Ann Neurol 1997;42:530. Logan WJ, McAndrews MP, Crawley A, et al. Functional MRI (fMRI) language localization and lateralization in children using object naming and word generation tasks. Ann Neurol 1998;44:551. Loring DW. Neuropsychological evaluation in epilepsy surgery. Epilepsia 1997;38 (Suppl 4):S18. Loring D, Meador K, Lee G, et al. Amobarbital effects and lateralized brain function. New York: Springer-Verlag, 1992. Mabbott DM, Smith ML. Material-specific memory in children with
1167
temporal and extratemporal lobectomies. Neuropsychologia 2004;41:995. Maehara T, Shimizu H. Surgical outcome of corpus callostomy in patients with drop attacks. Epilepsia 2001;42:67. Marks DA, Katz A, Hoffer P, et al. Localization of extra-temporal epileptic foci during ictal single photon emission computed tomography. Ann Neurol 1992;31:250. Matthews PM, Andermann F, Arnold DL. A proton magnetic resonance spectroscopy study of focal epilepsy in humans. Neurology 1990;40:985. McInerney J, Siegel AM, Nordgren RE, et al. Long-term seizure outcome following corpus callosotomy in children. Stereotact Funct Neurosurg 1999;73:79. Meyer FB, Marsh WR, Lawa ER, et al. Temporal lobectomy in children with epilepsy. J Neurosurg 1986;64:371. Mihara T, Inoue Y, Watanabe Y, et al. Improvement in quality-of-life following resective surgery for temporal lobe epilepsy: Results of patient and family assessments. Jpn J Psychiatry Neurol 1994;48:221. Minassian BA, Otsubo H, Weiss S, et al. Magnetoencephalographic localization in pediatric epilepsy surgery: Comparison with invasive intracranial electroencephalography. Ann Neurol 1999;46:627. Mizrahi EM, Kellaway P, Grossman RG, et al. Anterior temporal lobectomy and medically refractory temporal lobe epilepsy of childhood. Epilepsia 1990;31:302. Mohan KK, Chugani DC, Chugani HT. Positron emission tomography in pediatric neurology. Semin Ped Neurol 1999;6:111. Montes JL, Rosenblatt B, Farmer JP, et al. Lesionectomy of MRI detected lesions in children with epilepsy. Pediatr Neurosurg 1995;22:167. Morrell F, Whisler WW, Smith MC, et al. Landau Kleffner syndrome: Treatment with subpial intracortical transection. Brain 1995;118:1529. Mountz JM, Zhang B, Liu HG, et al. A reference method for correlation of anatomic and functional brain images: Validation and clinical applications. Semin Nucl Med 1994;4:256. Nashef L, Fish DR, Sander JW, et al. Incidence of sudden unexpected death in adult outpatient cohort with epilepsy at a tertiary referral centre. J Neurol Neurosurg Psychiatry 1995;58:462. Newton MR, Berkovic SF, Austin MC, et al. Dystonia, clinical lateralization and regional cerebral blood flow in temporal lobe seizures. Neurology 1992a;42:371. Newton MR, Berkovic SF, Austin MC, et al. A postictal switch in blood flow distribution characterizes human temporal lobe seizures. J Neurol Neurosurg Psychiatry 1992b;55:891. Newton MR, Berkovic SF, Austin MC, et al. SPECT in the localization of extratemporal and temporal epilepsy. J Neurol Neurosurg Psychiatry 1995;59:26. Ng TC, Comair Y, Xue M, et al. Proton chemical shift imaging for the presurgical localization of temporal lobe epilepsy. Soc Magn Reson Med Abst 1993;12:428 Ng TC, Comair YG, Xue M, et al. Temporal lobe epilepsy; presurgical localization with proton chemical shift imaging. Radiology 1994;193:465. Ng YT, McGregor AL, Wheless JW. Magnetic resonance imaging detection of mesial temporal sclerosis in children. Pediatr Neurol 2004;30:81. Nordli DR Jr. Epilepsy surgery in children, with special attention to focal cortical resections. Semin Pediatr Neurol 2000;7:204. Novotny, EJ. Overview—the role of NMR spectroscopy. Magn Reson Imaging 1995;13:1171. O’Brien TJ, So EL, Cascino GD, et al. Subtraction SPECT coregistered to MRI in focal malformations of cortical development: Localization of epileptogenic zone in epilepsy surgery candidates. Epilepsia 2004;45:367. O’Brien TJ, So EL, Mullan BP, et al. Subtraction ictal SPECT coregistered to MRI improves clinical usefulness of SPECT in localizing the surgical seizure focus. Neurology 1998;50:445. O’Brien TJ, So EL, Mullan BP, et al. Subtraction peri-ictal SPECT is predictive of extratemporal epilepsy surgery outcome. Neurology 2000;55:1668. Ogawa S, Tank D, Menon R, et al. Intrinsic signal changes accompanying sensory stimulation: Functional brain mapping with magnetic resonance imaging. Proc Natl Acad Sci U S A 1992;89:5951. Ogunmekan AO, Hwang PA, Hoffman HJ. Sturge-Weber-Dimitri disease: Role of hemispherectomy in prognosis. Can J Neurol Sci 1991;78:80. Ojemann GA. Organization of short-term verbal memory in language areas of the human cortex: Evidence from electrical stimulation. Brain Lang 1978;5:331.
1168
Epilepsy / 51
Ojemann GA. Individual variability in cortical localization of language. J Neurosurg 1979;50:164. Ojemann GA. Cortical stimulation. In: Engel J Jr, ed. Surgical treatment of the epilepsies, 2nd ed. New York: Raven Press, 1993. Ojemann G, Dodrill CB. Intraoperative techniques for reducing language and memory deficits with left temporal lobectomy. In: Wolf P, Dam M, Janz D, et al, eds. Advances in epileptology. XVIth Epilepsy International Symposium. New York: Raven Press, 1987. Olafsson E, Hauser WA, Ludvigsson P, et al. Incidence of epilepsy in rural Iceland: A population based study. Epilepsia 1996;37:951. Olson DM, Chugani H, Shewmon A, et al. Electrocorticographic confirmation of focal positron emission tomographic abnormalities in children with intractable epilepsy. Epilepsia 1990;31:731. Osuntokun BO, Adeuja AOG, Nottidge VA, et al. Prevalence of the epilepsies in Nigerian Africans: A community-based study. Epilepsia 1987;28:272. Palmini A, da Costa JC, Calcogrotto ME, et al. Patients with specific histopathological types of cortical dysplasia have specific degrees of severity of the epileptic condition—a study of 78 patients. Epilepsia 1997;38:5. Palmini A, Gambardella A, Andermann F, et al. Intrinsic epileptogenicity of human dysplastic cortex as suggested by corticography and surgical results. Ann Neurol 1995;37:476. Paolicchi JM, Jayakar P, Dean P, et al. Predictors of outcome in pediatric epilepsy surgery. Epilepsia 1996;37:210. Paolicchi JM, Jayakar P, Dean P, et al. The outcome of focal resection in preadolescent children with intractable partial epilepsy. Neurology 2000;54:642. Papanicolaou AC, Simos PG, Castillo EM, et al. Magnetocephalography: A noninvasive alternative to the Wada procedure. J Neurosurg 2004;100:867. Pardo CA, Vining EPG, Guo L, et al. The pathology of Rasmussen syndrome: Stages of cortical involvement and neuropathological studies in 45 hemispherectomies. Epilepsia 2004;45:516. Peacock WJ. Hemispherectomy for the treatment of intractable seizures in childhood. Neurosurg Clin N Am 1995;6:549. Penfield W, Flanigin H. Surgical therapy of temporal lobe seizures. Arch Neurol Psychiatry 1950;64:491. Penfield W. Pitfalls and success in surgical treatment of focal epilepsy. BMJ 1958;45:669. Peresson M, Lopez L, Narici L, et al. Magnetic source imaging and reactivity to rhythmical stimulation in tuberous sclerosis. Brain Dev 1998;20:512. Perrine K. Future directions for functional mapping. Epilepsia 1994;35:S90. Petroff OAC, Prichard JW, Behar KL, et al. In vivo phosphorus nuclear magnetic resonance spectroscopy in status epilepticus. Ann Neurol 1984;16:169. Petroff OAC, Prichard JW, Ogino T, et al. Combined 1H and 31P nuclear magnetic resonance studies of bicuculline-induced seizures in vivo. Ann Neurol 1986;20:185. Pilcher WH, Silbergeld DL, Berger MS, et al. Intraoperative electrocorticography during tumor resection: Impact on seizure outcome in patients with gangliogliomas. J Neurosurg 1993;78:891. Powell NW, Koepp MJ, Richardson MP, et al. The application of fMRI of memory in temporal lobe epilepsy: A clinical review. Epilepsia 2004;45:855. Prichard JW. Nuclear magnetic resonance spectroscopy of seizure states. Epilepsia 1994;35:514. Radtke RA, Hanson MW, Hoffman JM, et al. Temporal lobe hypometabolism on PET: Predictor of seizure control after temporal lobectomy. Neurology 1993;43:1088. Raymond AA, Fish DR, Sisdiya SM, et al. Abnormalities of gyration, heterotopias, tuberous sclerosis, focal cortical dysplasia, microdysgenesis, dysembryoplastic neuroepithelial tumor and dysgenesis of the archiocortex in epilepsy—clinical, EEG and neuroimaging features in 100 adult patients. Brain 1995;118:629. Reeves AL, So EL, Evans RW, et al. Factors associated with work outcome after anterior temporal lobectomy for intractable epilepsy. Epilepsia 1997;38:689 Roach ES, Ricla AR, Chugani HT, et al. Sturge-Weber syndrome: Recommendations for surgery. J Child Neurol 1994;9:190. Rogers SW, Andrews PI, Gahring LC, et al. Autoantibodies to glutamate receptor 3 in Rasmussen’s encephalitis. Science 1994;265:648. Romanelli P, Verdecchia M, Rodas R, et al. Epilepsy surgery for tuberous sclerosis. Pediatr Neurol 2004;31:239.
Rowe CC, Berkovic SF, Austin M, et al. Patterns of postictal cerebral blood flow in temporal lobe epilepsy: Qualitative and quantitative analysis. Neurology 1991;41:1096. Rowe CC, Berkovic SF, Sia STB, et al. Localization of epileptic foci with postictal single photon emission computed tomography. Ann Neurol 1989;26:660. Rugg-Gunn FJ, Eriksson SH, Symms MR, et al. Diffusion tensor imaging of cryptogenic and acquired partial epilepsies. Brain 2001;124:627. Ryding E, Rosen I, Elmqvist D, et al. SPECT measurements with 99m Tc-HM-PAO in focal epilepsy. J Cereb Blood Flow Metab 1988;8 (Suppl 1):S95. Ryvlin P, Garcia-Larrea L, Philippon B, et al. High signal intensity on T2-weighted MRI correlates with hypoperfusion in temporal lobe epilepsy. Epilepsia 1992;33:28. Sabsevitz DS, Swanson SJ, Hammeke TA, et al. Use of pre-operative functional neuroimaging to predict language deficits from epilepsy surgery. Neurology 2003;60:1788. Sackellares JC, Siegel GJ, Abou-Khalil BW, et al. Differences between lateral and mesial temporal metabolism interictally in epilepsy of mesial temporal origin. Neurology 1990;40:1420. Sassower KC, Rollinson DC, Duchowny M. Outcome of corpus callosotomy and other pediatric epilepsy surgery: Parental perceptions. Epileptic Disord 2001;3:197. Schmidt D, Tsai JJ, Janz D. Generalized tonic-clonic seizures in patients with complex partial seizures: Natural history and prognostic relevance. Epilepsia 1983;24:43. Schramm J, Aliashkevich AF, Grunwald T. Multiple subpial transactions: Outcome and complications in 20 patients who did not undergo resection. J Neurosurg 2002;97:39. Scott DF. The history of epileptic therapy: Account of how medication was published. Pearl River, NY: Parthenon Publishing, 1993. Shafer SQ, Hauser WA, Annegers JF, et al. EEG and other early predictors of epilepsy remission: A community study. Epilepsia 1988;29:590. Shah A, Watson C, Chugani HT, et al. Comparison between (C-11) flumazenil (FMZ) and (F-18) fluorodeoxyglucose (FDG PET) scanning in temporal lobe epilepsy. American Epilepsy Society Meeting, December 1995. Epilepsia 1995;36:165 (abstract). Shen W, Lee BI, Park HM, et al. HIPDM-SPECT brain imaging in the presurgical evaluation of patients with intractable seizures. J Nucl Med 1990;31:1280. Shields WD. Catastrophic epilepsy of childhood. Epilepsia 2000;41 (Suppl 2):S2. Sillanpaa M, Jalva M, Kaleva O, et al. Long-term prognosis of seizures with onset in childhood. N Engl J Med 1998;338:1916. Simos PG, Papanicolaou AC, Breier JI, et al. Localization of languagespecific cortex by using magnetic source imaging and electrical stimulation mapping. J Neurosurg 1999;91:787. Sinclair BD, Aronyk KE, Snyder TJ, et al. Pediatric epilepsy surgery at the University of Alberta: 1988-2000. Pediatr Neurol 2003;29:302. Sinclair DB, Wheatley M, Aronyk K, et al. Pathology and neuroimaging in pediatric temporal lobectomy in intractable epilepsy. Pediatr Neurosurg 2001;35:239. Smart O, Worrell G, Litt B, et al. Automatic detection of HFEO from focal intracranial EEG using fuzzy c-means clustering [Abstract]. British Mechanical Engineering Science, 2004. Smith ML, Elliott IM, Lach L. Cognitive, psychosocial, and family function one year after pediatric epilepsy surgery. Epilepsia 2004;45:650. Sofijanov NG. Clinical evolution and prognosis of childhood epilepsies. Epilepsia 1982;21:61. Sorenson JM, Wheless JW, Baumgartner JE, et al. Corpus callosotomy for medically intractable seizures. Pediatr Neurosurg 1997;27:260. Spencer SS, Schramm J, Wyler A, et al. Multiple subpial transaction for intractable partial epilepsy: An international meta-analysis. Epilepsia 2002;43:141. Spencer SS. Long-term outcome after epilepsy surgery. Epilepsia 1996;37:807. Spencer SS. The relative contributions of MRI, SPECT, and PET imaging in epilepsy. Epilepsia 1994;35:572. Stafstrom C, Lynch M, Sutula T. Consequences of epilepsy in the developing brain: Implications for surgical management. Semin Pediatr Neurol 2000;7:147. Stefan H, Bauer J, Feistel H, et al. Regional cerebral blood flow during focal seizures of temporal and frontocentral onset. Ann Neurol 1990;27:162.
Zupanc / Epilepsy Surgery in the Pediatric Population Stefan H, Hummel C, Scheler G, et al. Magnetic brain source imaging of focal epileptic activity: A synopsis of 455 cases. Brain 2003;126:2396. Stefan H, Pawlik G, Bocher-Schwarz HG, et al. Functional and morphological abnormalities in temporal lobe epilepsy: A comparison of interictal and ictal EEG, CT, SPECT, and PET. J Neurol 1987;234:377. Sutherling WW, Crandall P, Cahan LD, et al. The magnetic field of epileptic spikes agrees with intracranial localizations in complex partial epilepsy. Neurology 1988;38:778. Sutula T, Cascino G, Cavazos F, et al. Mossy fiber synaptic reorganization in the epileptic human temporal lobe. Ann Neurol 1989;26:321. Sutula T, He XX, Davazoa J, et al. Synaptic reorganization in the hippocampus induced by abnormal functional activity. Science 1988;26:321. Swartz BE, Tomiyasu U, Delgado-Escueta AV, et al. Neuroimaging in temporal lobe epilepsy: Test sensitivity and relationship in pathology and post-surgical outcome. Epilepsia 1992;33:624. Szabo CA, Wyllie E, Stanford LD, et al. Neuropsychological effect of temporal lobe resection in preadolescent children with epilepsy. Epilepsia 1998;39:814. Tasch E, Cendes F, Li LM, et al. Neuroimaging evidence of progressive neuronal loss and dysfunction in temporal lobe epilepsy. Ann Neurol 1999;45:568. Taylor DC, Neville BGR, Cross JH. New measures of outcome needed for surgical treatment of epilepsy. Epilepsia 1997;38:625. Theodore WH, Dorwart R, Holmes M, et al. Neuroimaging in refractory partial seizures: Comparison of PET, CT, and MRI. Neurology 1986;36:750. Theodore WH, Katz D, Kufta C, et al. Pathology of temporal lobe foci: Correlation with CT, MRI and PET. Neurology 1990;40:797. Theodore WH, Sato S, Kufta CV, et al. FDG positron emission tomography and invasive EEG: Seizure focus detection and surgical outcome. Epilepsia 1997;38:81. Thomas-Sohl KA, Vaslow DF, Maria BL. Sturge-Weber syndrome: A review. Pediatr Neurol 2004;30:303. Tice H, Barnes PD, Goumnerova L, et al. Pediatric and adolescent oligodendrogliomas. Am J Neuroradiol 1993;14:1293. Todt H. The late prognosis of epilepsy in childhood: Results of a prospective follow-up study. Epilepsia 1984;25:137. Tonini C, Beghi E, Berg AT, et al. Predictors of epilepsy surgery outcome: A meta-analysis. Epilepsy Res 2004;62:75. Trenerry MR, Jack CR, Sharbrough FW, et al. Quantitative MRI hippocampal volumes: Association with onset and duration of epilepsy and febrile convulsions in temporal lobectomy patients. Epilepsy Res 1993;15:247. Vali AM, Clarke MA, Kelsey A. Dysembryoplastic neuroepithelial tumors as a potentially treatable cause of intractable epilepsy in children. Clin Radiol 1993;47:255. Valk PE, Laxer KD, Barbaro NM, et al. High-resolution (2.6 mm) PET in partial complex epilepsy associated with mesial temporal sclerosis. Radiology 1993;186:55. Verhoeff NPLG, Weinstein HC, Aldenkamp AP, et al. Focus localization in patients with partial epilepsy with 99mTc HMPAO SPECT under continuous surface EEG monitoring. Nucl Med Commun 1 992;13:127.
1169
Vigevano F, Bertini E, Boldrini R, et al. Hemimegalencephaly and intractable epilepsy: Benefits of hemispherectomy. Epilepsia 1989;30:833. Vigevano F, DiRocco C. Effectiveness of hemispherectomy in hemimegalencephaly with intractable seizures. Neuropediatrics 1990;21:222. Vining EPG, Freeman JM, Pillas DJ, et al. Why would you remove half a brain? The outcome of 58 children after hemispherectomy—the Johns Hopkins experience: 1968 to 1996. Pediatrics 1997;100:163. Vining EPG, Mellits ED, Dorwen MM, et al. Psychologic and behavioral effects of antiepileptic drugs in children: A double-blind comparison between phenobarbital and valproic acid. Pediatrics 1987;80:165. Watanabe K, Negoro T, Okumura A. Symptomatology of infantile spasms. Brain Dev 2001;23:453. Westerveld M, Sass KJ, Chelune GL, et al. Temporal lobectomy in children: Cognitive outcome. J Neurosurg 2000;92:24. Wheless JW, Castillo E, Maggio V, et al. Magnetoencephalography (MEG) and magnetic source imaging (MSI). Neurologist 2004;10:138. Wheless JW, Willmore LJ, Breier JI, et al. A comparison of magnetoencephalography, MRI and V-EEG in patients evaluated for epilepsy surgery. Epilepsia 1999;40:931. Whittle IR, Ellis HJ, Simpson DA. The surgical treatment of intractable childhood and adolescent epilepsy. Aust N Z J Surg 1981;51:190. Worrell, GA, Parish L, Craunstoun SD, et al. High frequency oscillations and seizure generalization in neocortical epilepsy. Brain 2004;127:1496. Wyler AR. Corpus callosotomy: The treatment of epilepsy. In: Wyllie E, ed. Principles and practice. Philadelphia, Lea and Febiger, 1993. Wyllie E. Developmental aspects of seizure semiology: Problems in identifying localized onset seizures in infants and children. Epilepsia 1995;36:1170. Wyllie E. Surgical treatment of epilepsy in children. Pediatr Neurol 1998;19:179. Wyllie E, Chee M, Granström ML, et al. Temporal lobe epilepsy in early childhood. Epilepsia 1993;34:859. Wyllie E, Comair YG, Kotagal P, et al. Epilepsy surgery in infants. Epilepsia 1996;37:625. Wyllie E, Comair YG, Kotagal P, et al. Seizure outcome after epilepsy surgery in children and adolescents. Ann Neurol 1998;44:740. Wyllie E, Luders H, Murphy D, et al. Intracranial amobarbital (Wada) test for language dominance: Correlation with results of cortical stimulation. Epilepsia 1990;31:156. Zielinski JJ. Epidemiology and medical-social problems of epilepsy in Warsaw. Warsaw, Poland: Psychoneurological Institute, 1974. Zubal IG, Spencer SS, Imam K, et al. Difference images calculated from ictal and interictal technetium-99m-HMPAO SPECT scans of epilepsy. J Nucl Med 1995;36:684. Zupanc ML. Neuroimaging in the evaluation of children and adolescents with intractable epilepsy: I. Magnetic resonance imaging and the substrates of epilepsy. Pediatr Neurol 1997a;17:19. Zupanc ML. Neuroimaging in the evaluation of children and adolescents with intractable epilepsy: II. Neuroimaging and pediatric epilepsy surgery. Pediatr Neurol 1997b;17:111. Zupanc ML, Abrahamson KD, Cascino GD, et al. Efficacy of surgery on seizure control and resultant quality of life in pediatric patients—Mayo Clinic experience, 1988-1994. Epilepsia 1996;37:105.
CHAPTER 52
Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy Wendy G. Mitchell and Michèle Van Hirtum-Das
Children and adolescents with epilepsy and adults with childhood-onset epilepsy often are reported to have social maladjustment, including poor educational attainment, lower-than-expected occupational status, poorer perceived health and fitness, more frequently reported behavior problems, lower rates of marriage as adults, and higher rates of social isolation at all ages [Camfield et al., 1993; Clement and Wallace, 1990; Hoare, 1984; Jalava and Sillanpaa, 1997; Mitchell, 1995; Rutter et al., 1970; Sillanpaa, 1990]. These poor outcomes have multiple causes. In any particular patient, one or more causes of poor functioning may be identified and, at times, remedied. In general, neither epilepsy nor the seizures themselves are the most important cause of cognitive or behavioral disability. The underlying causes of cognitive and behavioral dysfunction may be subtle or obvious but generally are complex and multifactorial. In some instances, underlying neurologic structural lesions cause both epilepsy and other disabilities, including cognitive dysfunction. In others, such as benign focal epilepsy of childhood, learning and behavioral disorders are more difficult to explain, and the relationship with epilepsy is almost certainly not causal.
in populations surveyed for both mental retardation and epilepsy. Again, definitions of both epilepsy and mental retardation are not uniform. Prevalence of epilepsy is highest in cohorts of mentally retarded children with associated cerebral palsy [Curatolo et al., 1995; Sussova et al., 1990]. More subtle cognitive dysfunction has been found by many researchers, even when study groups are restricted to children with epilepsy syndromes thought to be independent of structural brain disease, such as benign focal epilepsy of childhood, childhood-onset absence epilepsy, or idiopathic generalized epilepsy [Chen et al., 1996; D’Allessandro et al., 1990; Dieterich et al., 1985; Olsson and Campenhausen, 1993; Piccirilli et al., 1994; Singhi et al., 1992]. Conflicting evidence exists regarding the role of interictal epileptiform discharges on cognitive function. Research using sophisticated computerized cognitive test batteries time-locked to EEG discharges has noted transient cognitive impairment, primarily slowing of reaction times, during epileptiform discharges [Aldenkamp et al., 1996; Binnie, 1993; Shewmon and Erwin, 1989]. The clinical significance of such findings is uncertain.
Learning Disabilities and Academic Underachievement COGNITIVE AND BEHAVIORAL DISORDERS Cognitive Function in Children with Epilepsy Although not all children with epilepsy have cognitive deficits, epilepsy is more frequent in mentally retarded children than in the general population [Britten et al., 1986; Forsgren et al., 1990; Sillanpaa, 1992]. Various populationbased prospective studies and cohort studies of mentally retarded children have documented the prevalence of epilepsy to be 15% to 35%. Children with severe mental retardation and cerebral palsy have the highest rates of epilepsy. Table 52-1 contains information from selected population-based or cohort studies that estimate the prevalence of epilepsy in mentally retarded populations. Caution must be used in interpreting this information, since definitions of both epilepsy and mental retardation vary. Several studies divide mentally retarded groups into mild (intelligence quotient [IQ] of 50 to 70) and moderate to severe mental retardation (IQ is under 50). Epilepsy is substantially more prevalent in more severely retarded cohorts. Even excluding children with major structural brain disease causing epilepsy and associated disabilities, mental retardation is more common in children with epilepsy than in children without epilepsy, with or without other chronic illnesses. Table 52-2 lists selected studies of the prevalence of mental retardation in cohorts of children with epilepsy or
Learning disability is diagnosed when one or more areas of learning are significantly below expectations, not explained by overall cognitive level (mental retardation), sensory abnormalities, or lack of opportunity or teaching (see Chapter 34). Learning disabilities are reported to be more frequent in children with epilepsy. Educational underachievement, particularly in reading, has been reported in a variety of settings, with comparisons of children with epilepsy both with their normal peers and with other children with chronic illnesses, such as asthma [Bagley, 1970; Holdsworth and Whitmore, 1974; Mitchell et al., 1991; Seidenberg et al., 1986; Stores, 1981; Stores and Hart, 1976; Sturniolo and Galletti, 1994]. It is unclear, however, whether the relationship is a direct one (in which the epilepsy, seizures, or medications themselves cause learning disability) or an indirect one (in which an underlying neurologic condition causes both seizures and abnormalities in perception, memory, visual-motor skills, and so on, which contribute to learning disabilities). In addition, many studies of children with epilepsy draw subjects from teaching hospitals with excessive representation of inner-city, immigrant, poor, minority, or non–English-speaking families. Educational underachievement may be excessive in subjects drawn from such teaching hospitals because of social factors entirely unrelated to medical conditions [Mitchell et al., 1991]. Parental expectations for their child with epilepsy are often lowered, at times inappropriately [Chavez, 1985; Hartlage and Green,
1172
Epilepsy / 52
TABLE 52-1 Rates of Epilepsy in Mentally Retarded Children and Adolescents: Population and Cohort Studies STUDY LOCALE [author(s), year] Sweden [Blomquist et al., 1981] Sweden [Hagberg et al., 1981] United States (Atlanta) [Trevathan et al., 1986] Same as preceding study Sweden [Steffenberg et al., 1996] Same as above Australia [Wellesley et al., 1992] Same as preceding study Sweden [Gustavson et al., 1977] United States (New York) [Jacobson and Janicki, 1983] United States (Oakland) [van den Berg and Yerushalmy, 1969] Scotland [Goulden et al., 1991] United States (Atlanta) [Murphy et al., 1995]
AGE (years)
% WITH EPILEPSY
8 to 19 8 to 12 10
18 12 8 32 15 44 11 15 36 23 29 15 30
6 to 13 6 to 16 5 to 16 0 to 21 0 to 7 0 to 22 10
SEVERITY OF MENTAL RETARDATION Mild Mild-moderate Mild Moderate-severe Mild Severe Mild Moderate Severe Undefined Undefined Undefined Two or more unprovoked seizures on separate days
Adapted from Steffenburg S, Gillberg C, Steffenburg U. Psychiatric disorders in children and adolescents with mental retardation and active epilepsy. Arch Neurol 1996;53:904; and Hauser WA, Hesdorffer DC. Seizures and the developmental disabilities. In: Hauser WA, Hesdoffer DC, eds. Epilepsy: Frequency, causes and consequences. New York: Demos Publications, 1990.
TABLE 52-2 Frequency of Mental Retardation in Children with Epilepsy: Population and Cohort Studies STUDY LOCALE [Author(s), Year]
AGE (years)
% MENTALLY RETARDED
EPILEPSY DEFINITION
Sweden [Brorson, 1970] England [Ross et al., 1980] Finland [Sillanpaa, 1992] Sweden [Sidenvall et al., 1996] Sweden [Steffenburg et al., 1996]
6 to 13 11 4 to 15 0 to 16 6 to 13
35 33 31 40 38
Active epilepsy with one or more seizures in previous 3 years Two or more unprovoked seizures Two or more unprovoked seizures Active epilepsy with one or more seizures in previous 5 years Active epilepsy with one or more seizures in previous 5 years
Adapted from Steffenburg S, Gillberg C, Steffenburg U. Psychiatric disorders in children and adolescents with mental retardation and active epilepsy. Arch Neurol 1996;53:904.
1972; Hoare and Kerley, 1991; Long and Moore, 1979]. Even after the effects of sociocultural variability have been accounted for, at least some children with epilepsy manifest learning disabilities. In one study comparing children with newly diagnosed epilepsy to children with recently diagnosed moderate asthma, academic underachievement was significantly more common in children with epilepsy, particularly boys with severe epilepsy [Austin et al., 1998]. Testing of groups of children with epilepsy using detailed neurocognitive batteries has demonstrated higher-thanexpected rates of dyslexia, visuospatial difficulties, nonverbal learning difficulties, and slowed reaction times [Farwell et al., 1985; Mitchell et al., 1992]. Some of these findings may be related to subtle or overt underlying structural lesions causing both the epilepsy and the learning disability, but not all can be explained on the basis of abnormalities detectable on neuroimaging.
Attention Deficit, Impulsivity, and Overactivity Attention, impulsivity, and activity level can be measured in various ways, ranging from parent and teacher questionnaires to psychometric testing to computerized continuous performance tasks. Regardless of method, most studies of children and adults with epilepsy demonstrate an excess incidence of inattention, impulsivity, and slowed reaction time [Kinney et al., 1990; Mitchell et al., 1992; Stores, 1978]. This finding should not imply that clinical attention-
deficit–hyperactivity disorder is extremely common in children with epilepsy, although the prevalence is probably somewhat increased. As with overall cognitive function in children with epilepsy, simple cause-and-effect relationships are uncommon. Underlying neurologic conditions may cause both symptoms of attention-deficit–hyperactivity disorder and epilepsy [Kinney et al., 1990]. Antiepileptic medications may affect attention and impulsivity, both positively and negatively, at least in some persons [Mitchell et al., 1993; Riva and Devoti, 1996]. Generally measured effects on attention are small, however, and may not be clinically significant. In rare instances, frequent seizures may affect attention, and seizure control may eliminate an apparent attention deficit. There is some evidence that frequent epileptiform discharges may disrupt attention, which may improve with antiepileptic treatment [Gordon et al., 1996]. Children with epilepsy and low IQ have a higher rate of significant behavior problems and mood disorders than those with normal IQ [Buelow et al., 2003]. It is unlikely that the relationship is a simple one of cause and effect. More likely, underlying neurologic abnormalities explain the coexistence of low IQ, epilepsy, and psychiatric abnormalities.
Psychiatric Disorders in Childhood Epilepsy Major “psychiatric” disorders of young childhood, such as autistic spectrum disorders, are associated with an increased incidence of epilepsy, but evidence that one causes the other
Mitchell and Van Hirtum-Das / Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy
is lacking [Carlton Ford et al., 1995; Cavazzuti and Nalin, 1990; Olsson et al., 1988; Steffenburg et al., 1996; Wong, 1993]. Child neurologists and psychiatrists recognize that these disorders are neurobiologic in origin. A number of syndromes are associated with a high incidence of both autistic behavior and seizures (e.g., Angelman’s syndrome, tuberous sclerosis), but the coincidence of seizures and behavior disorder is due to the underlying neurobiologic condition. A possible rare exception is the child in whom autistic behavior develops along with language regression, accompanied by an epileptiform electroencephalogram (continuous spike-and-wave pattern during sleep) [Hirsch et al., 1990; Kyllerman et al., 1996; Perez et al., 1993; Roulet et al., 1991]. This condition has been considered to be a variant of Landau-Kleffner syndrome. Behavior and language may improve with treatment with antiepileptics (rarely), corticosteroids, or corticotropin, or after subpial transection of epileptogenic cortex [Hirsch et al., 1990]. Little evidence exists to support the notion that severe psychiatric disorders are more common in children with epilepsy. Although major psychiatric illnesses, such as schizophrenia, obsessive-compulsive disorder, or affective disorders, may coexist with childhood epilepsy, the prevalence is not higher than in the general population. Treatment of coexisting severe psychiatric disorder and epilepsy may be complex. Some antiepileptics (carbamazepine, valproic acid) are reported to be beneficial in treatment of certain psychiatric disorders, most notably bipolar affective disorder [Fenn et al., 1996]. In general, however, treatment of epilepsy does not relieve symptoms of major psychiatric illness. Occasionally, “paradoxical normalization,” or “forced normalization,” is reported in children who experience a decrease in psychiatric symptoms when seizures are uncontrolled, with worsening of symptoms when seizures are in good control [Amir and Gross-Tsur, 1994]. Depressive disorders and mood disturbances have been reported more frequently in adolescents and adults with epilepsy than in healthy peers. The etiology of depressive symptoms may be complex; social stigmas, lack of employment opportunities, and lack of social contacts may contribute to depression. Phenobarbital occasionally may contribute to depressed mood in some adolescents with epilepsy [Brent et al., 1987]. Self-reported lower quality of life is lower in adolescents with epilepsy than in adolescents with asthma. Although this difference was more striking for young persons with active epilepsy, quality of life measures were low even when seizures were fully controlled or inactive [Austin et al., 1996].
Behavioral Problems, Conduct Disorders, and Delinquency Behavioral disturbances in children and adolescents with epilepsy may be due to family factors and parental anxiety about epilepsy, rather than a primary result of epilepsy or of the underlying neurologic disorder [Austin et al., 1992; Carlton Ford et al., 1995; Gortmaker et al., 1990; Hoare and Kerley, 1991; Lothman and Pianta, 1993; Mitchell et al., 1994; Pianta and Lothman, 1994]. Self-esteem is reported to be lower and behavioral problems are more frequent in children and adolescents with epilepsy than in peers without chronic illness or with other chronic illnesses, such as asthma or diabetes [Apter et al., 1991; Austin, 1989; Hoare
1173
and Mann, 1994; Matthews et al., 1982; Westbrook et al., 1991]. Increasing evidence, however, suggests that epilepsy may be frequently associated with behavior problems, perhaps if both are the result of an underlying neurologic disturbance. When children with epilepsy are assessed at the time of first seizure diagnosis, behavior problems are frequently reported by parents and teachers, particularly in children who had previously unrecognized seizures [Austin et al., 2001, 2002]. Adolescents and young adults with childhood-onset epilepsy have slightly higher-than-expected rates of delinquency in some studies [Camfield et al., 1993]. It is uncertain whether this propensity is due to underlying brain disease with poor impulse control, stigma, and lack of opportunity or to other sociocultural factors. A populationbased study in Finland, however, failed to find a relationship between delinquency and epilepsy in males up to age 22 years, although delinquency was associated with a history of central nervous system trauma [Rantakallio et al., 1992].
Epilepsies Specifically Associated with Poor Cognitive and Behavioral Outcome Certain pediatric epilepsy syndromes have been associated with particular, sometimes devastating, cognitive or behavioral declines, or both. Perhaps the most well studied of the catastrophic childhood epilepsies is infantile spasms. Mental retardation has been reported in up to 80% of children with infantile spasms and is described as severe in more than half of the cases [Jambaqué, 1994]. Although many patients exhibit arrest of global learning, specific cognitive deficits such as speech difficulties and impaired visuospatial abilities have been noted in others [Besag, 2004]. Thirteen percent of those with cryptogenic infantile spasms were reported to exhibit persistent autistic features; this number is higher (58%) if the child was diagnosed with tuberous sclerosis, with some further association with temporal lobe tubers in particular [Bolton et al., 2002; Hunt and Dennis, 1987; Riikonen and Amnell, 1981]. What has become clear is that effective early treatment of both cryptogenic and symptomatic spasms improves cognition and behavior [Caplan et al., 2002; Jambaqué et al., 2000; Kivity et al., 2004]. Many of the epileptic encephalopathies with onset in the neonatal or early infancy period are associated with frequent seizures that are notoriously refractory to treatment with both conventional and newer antiepileptic medication. Included in this group are severe myoclonic epilepsy in infancy (Dravet’s syndrome), early infantile epileptic encephalopathy (Ohtahara’s syndrome), neonatal myoclonic encephalopathy (or early infantile myoclonic encephalopathy), and migrating partial seizures of infancy. Delayed development usually is seen by the second year, and interpersonal relationships rarely progress past a level expected for that of a 2 year old [Besag, 2004]. Behavior in the affected child typically is hyperactive with autistic features. It is difficult to fully attribute the abnormalities in cognition and behavior to the frequent seizures and paroxysmal findings on EEG when an undiagnosed metabolic or genetic etiology may play a causative or contributory role. On the other hand, control of seizures in the context of tuberous sclerosis or Sturge-Weber syndrome plays a role in the favorable outcome of neurodevelopment and behavior [Jambaqué et al., 2000; Kramer et al., 2000].
1174
Epilepsy / 52
Lennox-Gastaut syndrome frequently has been associated with autistic features and cognitive deficits, although published literature specific to this topic is sparse [Besag, 2004]. Long-term follow-up evaluation of these patients commonly reveals slowness of intellectual ability and motor speed, apathy (possibly better described as an inability to engage with the environment secondary to frequent epileptiform discharges) and perseverative behavior [Kieffer-Renaux et al., 2001]. Electrical status epilepticus in sleep is an EEG pattern detected in some cases of pediatric epilepsy that often is associated with specific cognitive and language dysfunction. It frequently is encountered in those syndromes described as continuous spikes and waves (continuous spike-and-wave sleep syndrome) during slow-wave sleep and Landau-Kleffner syndrome. With continuous spike-and-wave activity in sleep, a typical decrease in the IQ or developmental quotient is noted by most investigators [Boel and Casaer, 1989; Roulet-Perez et al., 1993]. Approximately 50% to 100% of affected children exhibit impaired temporospatial orientation, and two thirds are noted to have attention deficits and exhibit hyperactivity. Of interest, some 40% to 60% of children with continuous spike-wave sleep exhibit an expressive aphasia, which is in contrast with children with Landau-Kleffner syndrome, who tend to present with a verbal or auditory agnosia [Galanopoulou et al., 2000]. In patients with Landau-Kleffner syndrome, language may recover spontaneously, partially improve with therapy, or unfortunately remain permanently affected despite improvement of the EEG abnormality [Besag, 2004]. Of specific note is the syndrome termed benign childhood epilepsy with centrotemporal spikes. Although this disorder was once thought of as a universally benign syndrome, increasing evidence suggests that a subpopulation of children may present with recently impaired IQ, visual perception, concentration, and short-term memory [Weglage et al., 1997].
FAMILY, COMMUNITY, AND CULTURAL PERCEPTIONS OF EPILEPSY Social acceptance and inclusion of children and adolescents with epilepsy are far from complete, even when seizures are infrequent or fully controlled. In some cultural settings, it is not generally disclosed to friends or extended family that a child has epilepsy [Ju et al., 1990]. Some children are not sent to school if seizures are uncontrolled. Despite laws guaranteeing disabled and medically impaired children access to schools, some schools discourage attendance by children with active seizure disorders. All of these prejudices and stigmas may further impair social and academic function in children with epilepsy. Fear of stigma may contribute to the high frequency of nondisclosure of epilepsy among adolescents [MacLeod and Austin, 2003].
SOCIAL ADJUSTMENT OF ADULTS WITH CHILDHOOD-ONSET EPILEPSY Population-based studies from several countries document that social functioning is impaired in adults who had childhood-onset epilepsy, compared with their healthy peers
[Farmer et al., 1992; Sillanpaa, 1990]. Marriage is less frequent, employment is less frequent and at less skilled occupations, and social isolation is more frequent. Differences are more striking when adults have ongoing seizures but are present even when complete remission or control has been obtained. Even when studies were restricted to adults with childhood-onset absence epilepsy, a disorder thought to be benign and likely to remit, social functioning continued to be impaired in comparison with that in nonepileptic peers [Dieterich et al., 1985]. In a long-term follow-up (30 years) of a population-based cohort of children with epilepsy in Finland, about 60% of subjects were independent in activities of daily living, and 57% were employed, most in manual labor or semiskilled positions [Sillanpaa and Helenius, 1993]. Several studies are notable for including only adults with childhood-onset absence [Olsson and Campenhausen, 1993] or mixed generalized seizures (absence plus generalized tonic-clonic) [Dieterich et al., 1985]. Young adults with persisting absence seizures since childhood or adolescence, who were originally identified during a population-based study of absence epilepsy diagnosed from 1973 to 1982, were compared with a Swedish reference sample of young adults, using a questionnaire to assess the impact of epilepsy on schooling, occupation, leisure-time activities, friends, daily routines, and housing. Although the overall employment rate did not differ from that in the reference subjects, persons with epilepsy were more likely to be employed in an unskilled job or employed in an occupation below that expected for educational level. Social isolation, defined by the reply of “no close friend,” was reported in 34.5%, compared with 7.9% of the reference group. A high percentage of subjects (74%) reported that epilepsy had affected at least one area of their social functioning [Olsson and Campenhausen, 1993]. In a Finnish study of adults who had uncomplicated childhoodonset epilepsy, quality of life of adults with epilepsy in remission on medication was lower, and rates of unemployment were higher, than in comparison subjects or in adults whose epilepsy was in remission after withdrawal of medication [Sillanpaa et al., 2004]. Other studies of outcome in adults with childhood-onset epilepsy find substantial maladaptation as well, particularly in social and vocational function. Social functioning is generally much more impaired in the subgroup of adults with ongoing seizures than in those who attain complete remission.
EFFECTS OF ANTIEPILEPTIC DRUGS ON BEHAVIOR, ATTENTION, AND MOOD General Effects of Antiepileptic Drugs Cognitive, psychiatric, and behavioral abnormalities in children with epilepsy often are attributed to antiepileptic medications. Most of these effects are unsupported by wellcontrolled clinical research. It is clear, however, that idiosyncratic adverse behavioral and cognitive responses can occur with any antiepileptic drug (see Chapter 49). In addressing issues of abnormal cognition and behavior in the management of pediatric epilepsy, several factors need to be recognized. Epilepsy occurring in the developing brain is
Mitchell and Van Hirtum-Das / Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy
likely to be substantially different from that in an adult in both its qualities and response to treatment. In addition, the most refractory epilepsies are likely to begin in childhood. The management of severe childhood epilepsy may prove challenging in that the choice of antiepileptic medication depends on the type of syndrome in which the seizures often occur, as well as the cognitive and behavioral abnormalities that may occur with these syndromes. Finally, treating a combination of several seizure types in one patient may be difficult, because many drugs that are effective in treating one type of seizure may exacerbate another type. In well-designed controlled studies, evidence of longterm adverse cognitive effects of antiepileptic medications is generally slight or difficult to document objectively. A few studies have randomized subjects at the onset of seizures to receive one of several antiepileptic drugs [Forsythe et al., 1991; Mitchell and Chavez, 1987]. Most studies, however, examine patients assigned nonrandomly to receive various antiepileptic drugs when medication is started, changed, or withdrawn [Aldenkamp et al., 1993; Aman et al., 1994; Chen et al., 1996; Mitchell et al., 1993; Sabers et al., 1995; Stores et al., 1992]. Only a few double-blind, placebocontrolled studies of the behavioral effects of antiepileptic drugs are available and are limited to studies of phenobarbital for febrile seizures in infants and toddlers [Farwell et al., 1990; Camfield et al., 1979]. In older children and adults, the major effect of antiepileptic medications on cognitive function appears to be a slowing of motor speed. Early reports that phenytoin caused generalized declines in cognitive function were later disputed when further data analysis and research found that the major effect of phenytoin was on motor speed [Aldenkamp et al., 1994; Dodrill and Tempkin, 1989; Duncan et al., 1990]. Other cognitive functions are relatively spared, if analyzed independent of response speed. Many standardized cognitive tests are at least partly dependent on timed performance. Thus, IQ may appear to be lowered by medications, whereas the sole effect is on motor speed. Nevertheless, some patients perceive that their responses are slower and are bothered by this, despite otherwise normal functioning by most other measures. Conversely, improvement in cognitive function, impulsivity, and behavior has been reported with several antiepileptic drugs. This improvement may occasionally be dramatic, resulting from control of frequent seizures, such as when a child with frequent petit mal seizures is started on ethosuximide or valproic acid. Improved behavior and cognitive function as a direct result of antiepileptic medication also has been documented for some antiepileptic drugs, most consistently carbamazepine [Aman et al., 1994; Mitchell et al., 1993]. Effects are slight, however, and probably not clinically significant in most instances and may even be disputed (Seidel and Mitchell, 1999). Most sedative drugs have the potential for causing excitement and agitation when they are first initiated, but this effect dissipates in most children over a few weeks. Phenobarbital causes sustained behavioral difficulties, primarily overactivity, in some children and can cause irritability and disturbed sleep in infants and toddlers [Camfield et al., 1979; Wolf et al., 1977]. Estimates of the number of children who do not tolerate phenobarbital because of resulting overactivity range from 5% to 25%. This effect is more frequent in toddlers and preschoolaged children but may occur at any age.
1175
Published case reports document a variety of idiosyncratic behavioral adverse reactions to virtually all antiepileptic drugs. Valproic acid occasionally causes a confused state or psychosis [Papazian et al., 1995]. Felbamate also has been reported to cause agitation and significant behavioral effects early in treatment, although overall this drug tends to improve behavior with prolonged treatment [Gay et al., 1995].
BEHAVIORAL AND COGNITIVE EFFECTS OF THE NEWER ANTIEPILEPTIC AGENTS Over the last decade, several new medications have been formulated for use as antiepileptic drugs—namely, levetiracetam, lamotrigine, tiagabine, topiramate, zonisamide, gabapentin, and oxcarbazepine. The newer antiepileptic drugs also have been reported to cause behavior change, both positive and negative. Virtually none have been studied in properly designed, blinded studies, either in comparison with placebo or in comparison to another antiepileptic drug. Nearly all published information regarding neurocognitive effects of the newer medications is anecdotal and from uncontrolled studies. Comparison across studies of antiepileptic drugs is further hampered by varying criteria for selection of participants for studies, and use of differing neuropsychologic tests and study designs [Brunbech and Sabers, 2002]. In addition, most published studies use either overall IQ or developmental quotient as the outcome measure, which may be insufficiently sensitive to medication effects, particularly subtle ones. A recent review of the literature regarding anticonvulsant effects in children summarizes published studies, nearly all of which examined phenobarbital, carbamazepine, or valproic acid (Loring and Meador, 2004).
Specific Medications Topiramate Topiramate is a sulfamate-substituted monosaccharide that blocks sodium and calcium channels and DL-α-amino3-hydroxy-5-methyl-4-isoxazole-propionic acid (AMPA)/ kainate-gated ion channels, positively modulates γ-aminobutyric acid type A (GABAA) receptors, and weakly inhibits carbonic anhydrase [Ketter et al., 1999]. It generally is well tolerated, although it has been reported in adult epileptic and nonepileptic persons to cause significant cognitive difficulties, primarily involving word-finding and verbal memory, particularly during initial treatment and titration [Fisher and Blum, 1995; Lee et al., 2003; Martin et al., 1999]. These adverse effects apparently dissipate over time, particularly if the dosage is increased slowly, although they may persist [Aldenkamp et al., 2003; Tatum et al., 2001]. Behavioral and cognitive abnormalities reported in pediatric epilepsy patients appear to be unrelated to either rate of dosage titration or maximal dose. However, prior behavioral or cognitive deficits may be predisposing factors [Gerber et al., 2000]. As yet, no controlled studies have evaluated the cognitive impairment induced by topiramate. In one double-blind, randomized, placebo-controlled trial of topiramate for add-on therapy in 86 children with partial epilepsy, children receiving topiramate had an increased frequency of
1176
Epilepsy / 52
emotional lability, difficulties with concentration, and fatigue, but the changes were not severe enough to cause any subject to discontinue treatment [Elterman et al., 1999].
Lamotrigine Lamotrigine is an agent that blocks voltage-dependent sodium channels, thereby preventing glutamate release, a phenomenon known to occur with the mood-stabilizing antiepileptics carbamazepine and oxcarbamazepine [Ketter et al., 1999]. Since its introduction in the United States in 1994, lamotrigine has received much attention with respect to its potential positive psychotropic effects. Significant improvements in behavior, cognition, and motor skills (unrelated to seizure control) are noted in pediatric patients, although these effects have not yet been formally studied [Culy and Goa, 2000; Meador and Baker, 1997]. Lamotrigine has been reported to have fewer cognitive effects in adults with newly diagnosed epilepsy than those described for carbamazepine and phenytoin [Brodie et al., 1995; Meador et al., 2001; Steiner et al., 1999]. A short-term treatment study performed on healthy volunteers using low-dose lamotrigine revealed improvement in cognitive activation and mood and reported subjective positive effects on quality of life relative to that achieved with use of valproate [Aldenkamp et al., 2002]. In addition, lamotrigine reportedly exhibits a positive effect on age-associated memory difficulties and social functioning in the mentally retarded [Earl et al., 2000; Mervaala et al., 1995]. In a trial of lamotrigine for add-on therapy in children with Lennox-Gastaut syndrome, responders with improved seizure control were noted to be more alert and attentive, whereas nonresponders were more likely to experience agitation. Further controlled trials are necessary to evaluate whether a positive effect on cognition and behavior occurs in children [Ericksson et al., 1998].
Gabapentin Gabapentin is similar in structure to GABA but does not seem to have effects at the GABA receptors. Rather, it potentiates GABA-mediated inhibition by increasing GABA release from glia and possibly inactivates sodium channels as well [Aldenkamp et al., 2003; Ketter et al., 1999]. Double-blind, placebo-controlled trials suggest efficacy of gabapentin in treatment of social phobia and in severe panic disorder in adults [Crockatt et al., 1998; Pande et al., 1997]. In both adult volunteer studies and studies with double-blind, randomized, crossover designs, gabapentin produced no significant alteration of psychomotor or memory abilities when used for either monotherapy or add-on treatment (Leach et al., 1997; Martin et al., 1999; Meador et al., 1999). Gabapentin occasionally has been reported to cause aggressive or agitated behavior, however [Lee et al., 1996; Tallian et al., 1996]. Children in whom significant adverse behavioral changes occur with use of gabapentin tend to have some degree of documented mental retardation [Khurana et al., 1996]. No published controlled studies have evaluated the cognitive and behavioral effects of gabapentin in children who have epilepsy.
Levetiracetam Levetiracetam, a structurally and mechanistically novel antiepileptic drug, has a favorable pharmacokinetic profile and is effective in treating partial seizures in adults, although pediatric studies are not yet published. [Dooley and Plosker, 2000]. Among adult patients with epilepsy who received
levatiracetam, behavioral abnormality was reported in a significant proportion relative to those patients with anxiety or cognitive disorders but without epilepsy. However, the behavioral events cited were less common than those reported with other antiepileptic agents [Cramer et al., 2003]. A prospective open-label, add-on trial using levetiracetam to treat refractory partial and generalized seizures in children younger than 16 years of age revealed adverse events in 51% of subjects. Most of these events were behavioral in nature, although most children did not require discontinuation of the medication. As with the gabapentin study, a majority of the children were developmentally delayed or mentally retarded. In this same study, however, improvement in behavior and/or cognition after the addition of levetiracetam was reported in 25.6% [Wheless and Ng, 2002]. A few anecdotal reports have described improved behavior in children with autism treated with levetiracetam, but in the same population, some children experienced an increase in aggressive behavior [Rugino and Samsock, 2002].
Oxcarbazepine Oxcarbazepine is a keto homolog of carbamazepine, although it has a very distinct metabolic profile. It is labeled for use for monotherapy or adjunctive therapy for partial seizures with or without secondarily generalized seizures in children 6 years of age and older. Although no deterioration in cognitive function test results were reported in one crossover and several comparative monotherapy studies in adult epilepsy patients, cognitive function has not been systematically studied in children and adolescents.
Tiagabine Tiagabine acts as a GABA uptake inhibitor in neurons and glial cells and is effective for add-on therapy in the treatment of refractory partial epilepsy. Very few data are currently published regarding the psychotropic effects of this medication, and no information is available for the pediatric population.
Zonisamide No published trials have included cognitive or behavioral observations in pediatric patients with either partial or generalized seizures treated with zonisamide. Reports from Japan, where the medication has been in use for longer than 15 years, suggest that psychotic episodes and behavior changes may occur in children given zonisamide, despite improved seizure control [Hirai et al., 2002; Kimura, 1994].
Fear of Side Effects and Effective Antiepileptic Drug Use Despite the relative paucity of documentation of sustained adverse cognitive effects of antiepileptics, sophisticated parents and teachers often are well versed in the possible adverse effects of medications, exaggerated, to some degree, by frightening stories in the lay media and, increasingly, on the Internet. Parents may be under the erroneous impression that a particular antiepileptic drug will “make the child retarded” and may blame developmental problems that subsequently emerge on previous administration of antiepileptic drugs or may avoid administration of these medications because of fear of disturbing the child’s behavior or development.
Mitchell and Van Hirtum-Das / Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy
TREATMENT As with all medical treatment, care of the child with epilepsy must be individualized. Nevertheless, several general principles apply. The developmental, cognitive, academic, and behavioral status of the child and the social functioning of the family must be integral and ongoing concerns in the management of a child with epilepsy. Brief developmental, cognitive, or academic testing is appropriate on initial evaluation and at follow-up visits. Although treatment generally will not alter the underlying cognitive capacity of the child, early intervention and referral to appropriate community and school resources will maximize function. Appropriate counseling of the family may minimize later behavioral and adjustment difficulties. Group programs to help families with their children with epilepsy may be effective in altering parental attitudes, reducing fears, and improving the children’s participation in family and community activities [Lewis et al., 1990].
School Issues At times, parents report that a child with epilepsy is being excluded from school programs, sent home repeatedly, or placed in a more restrictive class setting than is appropriate for their abilities. It may be essential that the treating neurologist or pediatrician intervene with appropriate authorities if a child is being denied appropriate educational experiences because school personnel are concerned about the possibility of seizures occurring at the school. Local branches of voluntary organizations, such as the Epilepsy Foundation of America, may be helpful in providing informational programs to schools. At least in the United States, federal law mandates inclusion of children with disabilities and medical conditions in educational programs in the least restrictive environment appropriate for the child’s needs.
Behavior Problems and Discipline Behavioral problems and parent-child interaction should be addressed regularly in the management of children with epilepsy. Parents may avoid disciplining a child with epilepsy in an age-appropriate manner out of fear that the child’s becoming angry or upset may trigger seizures. Parents must be reassured that this is not the case. Significant abnormalities in behavior, activity, or attention warrant a more detailed evaluation, including comprehensive psychometric testing. Psychometric testing, along with clinical history gathered from parents, teachers, and patients, may be necessary to differentiate behavioral difficulties associated with coexisting attention-deficit–hyperactivity disorder from those due to family dysfunction, oppositional disorders, inappropriate parental expectations, and other factors.
Attention-Deficit Disorders: Treatment in Children with Epilepsy Alteration in antiepileptic treatment may improve behavior and attention if the original treatment has substantially affected behavior. Nevertheless, attention-deficit–hyperactivity dis-
1177
order may coexist with epilepsy, independent of antiepileptic treatment. Treatment of attention-deficit–hyperactivity disorder with stimulants (e.g., methylphenidate, pemoline, dextroamphetamine) or with tricyclic antidepressants (e.g., imipramine, desipramine) generally does not compromise seizure control [Gross-Tsur et al., 1997]. A newer medication for attention-deficit disorder, atomoxetine (a nonamphetamine selective norepinephrine reuptake inhibitor with stimulant properties), does not significantly affect seizure control, nor does it have significant pharmacokinetic interactions with antiepileptic medications. Bupropion, an anti-depressant drug occasionally useful for attention deficit disorder, particularly when associated with mood disorder, may increase tendency toward seizures, particularly at high doses. Most pediatric neurologists avoid its use at doses greater than 100 mg per day in children with epilepsy.
Peer Relationships, Teasing, and Social Isolation Social isolation and poor peer relationships are a particular problem in school-aged and adolescent children with epilepsy and are difficult to address therapeutically. Nonverbal learning disabilities may make the child socially maladroit and target them for teasing by peers. Children may be particularly at risk for teasing and exclusion by peers if they also have had seizures at school or are singled out by the need to leave the classroom to take medication during the school day. Therapeutic or educational programs that emphasize social skills and assertiveness training may be helpful in some children and adolescents [Henriksen, 1990; Lewis et al., 1990; Strang, 1990].
Occupational Planning and Adjustment Occupational adjustment may be poor in adults with childhood-onset epilepsy. Vocational plans and postsecondary education should be discussed with adolescents who have epilepsy, with appropriate goal-setting. Adolescents with well-controlled epilepsy may be assured that their epilepsy will not interfere with career goals, with a few notable exceptions; military service, airlines, and public safety professions (police and fire) generally will exclude applicants with epilepsy, regardless of control. Some states will restrict commercial driver’s licenses, even with good seizure control. Appropriate resources for assessment, training, and placement should be identified in the community. In addition to school-based programs, local epilepsy foundations may be a good resource, as may departments of vocational rehabilitation in many states. REFERENCES Aldenkamp AP, Alpherts WC, Blennow G, et al. Withdrawal of antiepileptic medication in children—effects on cognitive function: The Multicenter Holmfrid Study. Neurology 1993;43:41. Aldenkamp AP, Alpherts WC, Diepman L, et al. Cognitive side effects of phenytoin compared with carbamazepine in patients with localization related epilepsy. Epilepsy Res 1994;19:37. Aldenkamp AP, Arends J, Bootsma HPR, et al. Randomized double-blind parallel-group study comparing cognitive effects of a low-dose lamotrigine with valproate and placebo in healthy volunteers. Epilepsia 2002;43:19. Aldenkamp AP, De Krom M, Reijs R. Newer antiepileptic drugs and cognitive issues. Epilepsia 2003;44 (Suppl 4):21.
1178
Epilepsy / 52
Aldenkamp AP, Overweg J, Gutter T, et al. Effect of epilepsy, seizures and epileptiform EEG discharges on cognitive function. Acta Neurol Scand 1996;93:253. Aman MG, Werry JS, Paxton JW, et al. Effects of phenytoin on cognitive motor performance in children as a function of drug concentration, seizure type, and time of medication. Epilepsia 1994;35:172. Amir N, Gross-Tsur V. Paradoxical normalization in childhood epilepsy. Epilepsia 1994;35:1060. Apter A, Aviv A, Kaminer Y, et al. Behavioral profile and social competence in temporal lobe epilepsy of adolescence. J Am Acad Child Adolesc Psychiatry 1991;30:887. Austin JK. Comparison of child adaptation to epilepsy and asthma. J Child Adolesc Psychiatr Ment Health Nurs 1989;2:139. Austin JK, Dunn DW, Caffrey HM et al. Recurrent seizures and behavior problems in children with first recognized seizures: A prospective study. Epilepsia 2002;43:564. Austin JK, Harezlak J, Dunn DW et al. Behavior problems in children before first recognized seizures. Pediatrics 2001;107:115. Austin JK, Huberty TJ, Huster GA et al. Academic achievement in children with epilepsy or asthma. Dev Med Child Neurol 1998;40:248. Austin JK, Huster GA, Dunn GW et al. Adolescents with active or inactive epilepsy or asthma: A comparison of quality of life. Epilepsia 1996;37:1228. Austin JK, Risinger MW, Beckett LA. Correlates of behavior problems in children with epilepsy. Epilepsia 1992;33:1115. Bagley CR. Educational performance of children with epilepsy. Br J Educ Psychol 1970;40:82. Besag FM. Behavioral aspects of pediatric epilepsy syndromes. Epilepsy Behav 2004;5;S3. Binnie CD. Significance and management of transitory cognitive impairment due to subclinical EEG discharges in children. Brain Dev 1993;15:23. Blomquist HK, Gustavson K-H, Holmgren G. Mild mental retardation in children in a northern Swedish county. J Ment Defic Res 1981;25:169. Boel M, Casaer P. Continuous spikes and waves during slow sleep: A 30 months follow-up study of neuropsychological recovery and EEG findings. Neuropediatrics 1989;20:176. Bolton PF, Park RJ, Higgins JN, et al. Neuroepileptic determinants of autism spectrum disorders in tuberous sclerosis complex. Brain 2002;125:1247. Brent BA, Crumrine PK, Varma RR, et al. Phenobarbital treatment and major depressive disorder in children with epilepsy. Pediatrics 1987;80:909. Britten N, Morgan K, Fenwick PBC, et al. Epilepsy and handicap from birth to age 36. Dev Med Child Neurol 1986;28:719. Brodie MJ, Richens A, Yuen AWC. Double-blind comparison of lamotrigine and carbamazepine in newly diagnosed epilepsy. Lancet 1995;345:476. Brorson LO. Epilepsi hos barn och ungdom. In: Social Department ed Epileptikervarden. Stockholm: Allmanna Forlaget, 1970. Brunbech L, Sabers A. Effect of antiepileptic drugs on cognitive function in individuals with epilepsy. A comparative review of newer versus older agents. Drugs 2002;62:595. Buelow JM, Austin JK, Perkins SM, et al. Behavior and mental health problems in children with epilepsy and low IQ. Dev Med Child Neurol 2003;45:683. Camfield CS, Camfield PR, Smith B, et al. Biologic factors as predictors of social outcome of epilepsy in intellectually normal children: A population-based study. J Pediatr 1993;122:869. Camfield CS, Chaplin S, Doyle AV, et al. Side effects of phenobarbital in toddlers; behavior and cognitive aspects. J Pediatr 1979;95:361. Caplan R, Siddarth P, Mathern G, et al. Developmental outcome with and without successful intervention. Int Rev Neurobiol 2002;49:269. Carlton Ford S, Miller R, Brown M, et al. Epilepsy and children’s social and psychological adjustment. J Health Soc Behav 1995;36:285. Cavazzuti GB, Nalin A. Psychobehavioral disturbance in epileptic children. Childs Nerv Syst 1990;6:430. Chavez JM. The impact of epilepsy on mother-child interaction in Mexican-American families at different levels of acculturation. Diss Abst Int 1985;46:1741. Chen YJ, Kang WM, So WC. Comparison of antiepileptic drugs on cognitive function in newly diagnosed epileptic children: A psychometric and neurophysiological study. Epilepsia 1996;37:81. Clement MJ, Wallace SJ. A survey of adolescents with epilepsy. Dev Med Child Neurol 1990;32:849.
Cramer JA, De Rue K, Devinsky O, et al. A systematic review of the behavioral effects of levetiracetam in adults with epilepsy, cognitive disorders, or an anxiety disorder during clinical trials. Epilepsy Behav 2003;4:124. Crockatt JG, Greiner M, Clift LL, et al. Treatment of panic disorder with gabapentin. Proceedings of the 38th Annual Meeting of New Clinical Drug Evaluation Unit Progress, 1998;154 (abstract). Culy CR, Goa KL. Lamotrigine: A review of its use in childhood epilepsy. Paediatr Drugs 2000;2:299. Curatolo P, Arpino C, Stazi MA, et al. Risk factors for the co-occurrence of partial epilepsy, cerebral palsy and mental retardation. Dev Med Child Neurol 1995;37:776. D’Alessandro P, Piccirilli M, Tiacci C, et al. Neuropsychological features of benign partial epilepsy in children. Ital J Neurol Sci 1990;11:265. Dieterich E, Doose H, Baier WK, et al. Long-term follow-up of childhood epilepsy with absences. II. Absence-epilepsy with initial grand mal. Neuropediatrics 1985;16:155. Dodrill CB, Tempkin NR. Motor speed is a contaminating factor in evaluating the “cognitive” effects of phenytoin. Epilepsia 1989;30:453. Dooley M, Plosker GL. Levetiracetam: A review of its adjunctive use in the management of partial onset seizures. Drugs 2000;60:871. Duncan JS, Shorvon SD, Trimble MR. Effects of removal of phenytoin, carbamazepine, and valproate on cognitive function. Epilepsia 1990;31:584. Earl N, McKee JR, Sunder TR, et al. Lamotrigine adjunctive therapy in patients with refractory epilepsy and mental retardation. Epilepsia 2000;41:72. Elterman RD, Glauser TA, Wyllie E, et al. A double-blind, randomized trial of topiramate as adjunctive therapy for partial-onset seizures in children. Topiramate YP Study Group. Neurology 1999; 52:1338. Eriksson AS, Nergardh A, Hoppu K. The efficacy of lamotrigine in children and adolescents with refractory generalized epilepsy: A randomized, double-blind, crossover study. Epilepsia 1998;39:495. Farmer PJ, Placencia M, Junbo L, et al. Effects of epilepsy on daily functioning in Northern Ecuador: Summary of findings of a population-based research project. Neuroepidemiology 1992;11:180. Farwell JR, Lee YJ, Hirtz DG, et al. Phenobarbital for febrile seizures: Effects on intelligence and on seizure recurrence. N Engl J Med 1990;322:364. Farwell JR, Dodrill CB, Batzel LW. Neuropsychological abilities of children with epilepsy. Epilepsia 1985;26:395. Fenn HH, Robinson D, Luby V, et al. Trends in pharmacotherapy of schizoaffective and bipolar affective disorders: A 5-year naturalistic study. Am J Psychiatry 1996;153:711. Fisher R, Blum D. Clobazam, oxcarbazepine, tiagabine, topiramate, and other new antiepileptic drugs. Epilepsia 1995;36 (Suppl 2):S105. Forsgren L, Edvinsson SO, Blomquist HK, et al. Epilepsy in a population of mentally retarded children and adults. Epilepsy Res 1990;6:234. Forsythe I, Butler R, Berg I, et al. Cognitive impairment in new cases of epilepsy randomly assigned to carbamazepine, phenytoin and sodium valproate. Dev Med Child Neurol 1991;33:524. Galanopoulou AS, Bojko A, Lado F, et al. The spectrum of neuropsychiatric abnormalities associated with electrical status epilepticus in sleep. Brain Dev 2000;22:279. Gay PE, Mecham GF, Coskey JS, et al. Behavioral effects of felbamate in childhood epileptic encephalopathy (Lennox-Gastaut syndrome). Psychol Rep 1995;77:1208. Gerber PE, Hamiwka L, Connolly MB, et al. Factors associated with behavioral and cognitive abnormalities in children receiving topiramate. Pediatr Neurol 2000;22:200. Gordon K, Bawden H, Camfield P, et al. Valproic acid treatment of learning disorder and severely epileptiform EEG without clinical seizures. J Child Neurol 1996;11:41. Gortmaker SL, Walker DK, Weitzman M, et al. Chronic conditions, socioeconomic risks, and behavioral problems in children and adolescents. Pediatrics 1990;85:267. Goulden KJ, Shinnar S, Koller H, et al. Epilepsy in children with mental retardation. A cohort study. Epilepsia 1991;32:690. Gross-Tsur V, Manor O, van der Meere J, et al. Epilepsy and attention deficit hyperactivity disorder: Is methylphenidate safe and effective? J Pediatr 1997;130:40. Gustavson K-H, Holmgren G, Jonsell R, et al. Severe mental retardation in children in a northern Swedish county. J Ment Defic Res 1977;21:161. Hagberg B, Hagberg G, Lewerth A, et al. Mild mental retardation in Swedish school children. I. Prevalence. Acta Paediatr Scand 1981;70:441.
Mitchell and Van Hirtum-Das / Behavioral, Cognitive, and Social Aspects of Childhood Epilepsy Hartlage LA, Green JB. The relation of parental attitudes to academic and social achievement in epileptic children. Epilepsia 1972;13:21. Hauser WA, Hesdorffer DC. Seizures and the developmental disabilities. In: Epilepsy: Frequency, causes and consequences. New York: Demos Publications, 1990. Henriksen O. Education and epilepsy: Assessment and remediation. Epilepsia 1990;31 (Suppl 4):S21. Hirai K, Kimiya S, Tabata K, et al. Selective mutism and obsessive compulsive disorders associated with zonisamide. Seizure 2002;11:468. Hirsch E, Marescaux C, Maquet P, et al. Landau-Kleffner syndrome: A clinical and EEG study of five cases. Epilepsia 1990;31:756. Hirsch E, Schmitz B, Carreno M. Epilepsy, antiepileptic drugs (AEDs) and cognition. Acta Neurol Scand 2003;108 (Suppl 180):23. Hoare P. The development of psychiatric disorder among schoolchildren with epilepsy. Dev Med Child Neurol 1984;26:3. Hoare P, Kerley S. Psychosocial adjustment of children with chronic epilepsy and their families. Dev Med Child Neurol 1991;33:201. Hoare P, Mann H. Self esteem and behavioural adjustment in children with epilepsy and children with diabetes. J Psychosom Res 1994;38:859. Holdsworth L, Whitmore K. A study of children with epilepsy attending ordinary schools;I. Seizure patterns, progress and behavior in school. Dev Med Child Neurol 1974;16:746. Hunt A, Dennis J. Psychiatric disorder among children with tuberous sclerosis. Dev Med Child Neurol 1987;29:190. Jacobson JW, Janicki MP. Observed prevalence of multiple developmental disabilities. Ment Retard 1983;21:87. Jalava M, Sillanpaa M. Physical activity, health related fitness, and health experience in adults with childhood onset epilepsy: A controlled study. Epilepsia 1997;38:424. Jambaqué I. Neuropsychological aspects. In: Dulac O, Chugani HT, Dalla Bernadina B, eds. Infantile spasms and West syndrome. London: Saunders, 1994;82. Jambaqué I, Chiron C, Dumas C, et al. Mental and behavioral outcome of infantile epilepsy treated by vigabatrin in tuberous sclerosis patients. Epilepsy Res 2000;38:151. Ju SH, Chang PF, Chen YJ, et al. Parental attitude and adjustment to childhood epilepsy. Acta Paediatr Sin 1990;31:103. Ketter TA, Post RM, Theodore WH. Positive and negative psychiatric effects of antiepileptic drugs in patients with seizure disorders. Neurology 1999;53 (Suppl 2):S53. Khurana DS, Riviello J, Helmers S, et al. Efficacy of gabapentin therapy in children with refractory partial seizures. J Pediatr 1996;128:829. Kieffer-Renaux V, Kaminska A, Dulac O. Cognitive deterioration in Lennox-Gastaut and Doose epilepsy. In: Jambaqué I, Lasonde M, Dulac O, eds. Neuropsychology of childhood epilepsy. New York: Kluwer Academic/Plenum, 2001;185. Kimura S, Zonisamide-induced behavior disorder in two children. Epilepsia 1994;35:403. Kinney RO, Shaywitz BA, Shaywitz SE, et al. Epilepsy in children with attention deficit disorder: Cognitive, behavioral, and neuroanatomic indices. Pediatr Neurol 1990;6:31. Kivity S, Lerman P, Ariel R, et al. Long-term cognitive outcomes of a cohort of children with cryptogenic infantile spasms treated with high-dose adrenocorticotropic hormone. Epilepsia 2004;45:255. Kramer U, Kahana E, Shorer Z, et al. Outcome of infants with unilateral Sturge-Weber syndrome and early onset seizures. Dev Med Child Neurol 2000;42:756. Kyllerman M, Nyden A, Praquin N, et al. Transient psychosis in a girl with epilepsy and continuous spikes and waves during slow sleep (CSWS). Eur Child Adolesc Psychiatry 1996;5:216. Leach JP, Girvan J, Paul A, et al. Gabapentin and cognition: A double blind, dose ranging, placebo controlled study in refractory epilepsy. J Neurol Neurosurg Psychiatry 1997;62:372. Lee DO, Steingard RJ, Cesena M, et al. Behavioral side effects of gabapentin in children. Epilepsia 1996;37:87. Lee S, Sziklas V, Andermann F, et al. The effects of topiramate on cognitive function in patients with epilepsy. Epilepsia 2003;44:339. Lewis MA, Salas I, de la Sota A, et al. Randomized trial of a program to enhance the competencies of children with epilepsy. Epilepsia 1990;31:101. Long CG, Moore JR. Parental expectations for their epileptic children. J Child Psychol Psychiatry 1979;20:299. Loring DW, Meador KJ. Cognitive side effects of antiepileptic drugs in children. Neurology 2004;62:872.
1179
Lothman DJ, Pianta RC. Role of child-mother interaction in predicting competence of children with epilepsy. Epilepsia 1993;34:658. MacLeod JS, Austin JK. Stigma in the lives of adolescents with epilepsy: A review of the literature. Epilepsy Behav 2003;4:112. Martin R, Kuzniecky R, Ho S, et al. Cognitive effects of topiramate, gabapentin, and lamotrigine in healthy young adults. Neurology 1999;52:321. Matthews WS, Barabas G, Ferrari M. Emotional concomitants of childhood epilepsy. Epilepsia 1982;23:671. Meador KJ, Baker GA. Behavioral and cognitive effects of lamotrigine. J Child Neurol 1997;12 (Suppl 1):S44. Meador KJ, Loring DW, Ray PG, et al. Differential cognitive and behavioral effects of carbamazepine and gabapentin. Epilepsia 1999;40:1279. Meador KJ, Loring DW, Ray PG, et al. Differential cognitive and behavioral effects of carbamazepine and lamotrigine. Neurology 2001;56:1177. Mervaala E, Koivista K, Hanninen T, et al. Electrophysiological and neuropsychological profiles of lamotrigine in young and age-associated memory impairment (AAMI) subjects. Neurology 1995;45 (Suppl 4):A259. Mitchell WG. Long term prognosis for children with epilepsy. Curr Probl Pediatr 1995;25:113. Mitchell WG, Chavez JM. Carbamazepine versus phenobarbital for partial onset seizures in children. Epilepsia 1987;28:56. Mitchell WG, Chavez JM, Lee H, et al. Academic underachievement in children with epilepsy. J Child Neurol 1991;6:65. Mitchell WG, Scheier LM, Baker SA. Psychosocial, behavioral, and medical outcomes in children with epilepsy: A developmental risk factor model using longitudinal data. Pediatrics 1994;94:471. Mitchell WG, Zhou Y, Chavez JM, et al. Reaction time, attention, and impulsivity in epilepsy. Pediatr Neurol 1992;8:19. Mitchell WG, Zhou Y, Chavez JM, et al. Effects of antiepileptic drugs on reaction time, attention, and impulsivity in children. Pediatrics 1993;91:101. Murphy CC, Trevathan E, Yeargin-Allsopp M. Prevalence of epilepsy and epileptic seizures in 10-year-old children: Results from the Metropolitan Atlanta Developmental Disabilities Study. Epilepsia 1995;36:866. Olsson I, Campenhausen G. Social adjustment in young adults with absence epilepsies. Epilepsia 1993;34:846. Olsson I, Steffenburg S, Gillberg C. Epilepsy in autism and autistic-like conditions. Arch Neurol 1988;45:666. Papazian O, Canizales E, Alfonso I, et al. Reversible dementia and apparent brain atrophy during valproate therapy. Ann Neurol 1995;38:687. Perez ER, Davidoff V, Despland PA, et al. Mental and behavioral deterioration of children with epilepsy and CSWS: Acquired epileptic frontal syndrome. Dev Med Child Neurol 1993;35:661. Pianta RC, Lothman DJ. Predicting behavior problems in children with epilepsy: Child factors, disease factors, family stress, and child-mother interaction. Child Dev 1994;65:1415. Piccirilli M, D’Alessandro P, Sciarma T, et al. Attention problems in epilepsy: Possible significance of the epileptogenic focus. Epilepsia 1994;35:1091. Rantakallio P, Koiranen M, Motteonen J. Association of perinatal events, epilepsy, and central nervous system trauma with juvenile delinquency. Arch Dis Child 1992;67:1459. Riikonen R, Amnell G. Psychiatric disorders in children with earlier infantile spasms. Dev Med Child Neurol 1981;23:747. Riva D, Devoti M. Discontinuation of phenobarbital in children: Effects on neurocognitive behavior. Pediatr Neurol 1996;14:36. Ross EM, Peckham CS, West PB, et al. Epilepsy in childhood: Findings from the National Child Development Study. BMJ 1980;280:207. Roulet E, Deonna T, Gaillard F, et al. Acquired aphasia, dementia, and behavior disorder with epilepsy and continuous spike and waves during sleep in a child. Epilepsia 1991;32:495. Roulet-Perez E, Davidoff V, Despland PA, et al. Mental and behavioural deterioration of children with epilepsy and CSWS: Acquired epileptic frontal syndrome. Dev Med Child Neurol 1993;35:661. Rugino TA, Samsock TC. Levetiracetam in autistic children: An openlabel study. J Dev Behav Pediatr 2002;23:225. Rutter M, Graham P, Yule W. A neuropsychiatric study in childhood. Philadelphia: JB Lippincott, 1970. Sabers A, Moller A, Dam M, et al. Cognitive function and anticonvulsant therapy: Effect of monotherapy in epilepsy. Acta Neurol Scand 1995;92:19.
1180
Epilepsy / 52
Seidel WT, Mitchell WG. Cognitive and behavioral effects of carbamazepine in children: Data from benign rolandic epilepsy. J Child Neurol 1999;14:716. Seidenberg M, Beck N, Geisser M, et al. Academic achievement in children with epilepsy. Epilepsia 1986;27:753. Sidenvall R, Forsgren L, Heijbel J. Prevalence and characteristics of epilepsy in children in Northern Sweden. Seizure 1996;5:139. Shewmon DA, Erwin RJ. Transient impairment of visual perception induced by single interictal occipital spikes. J Clin Exp Neuropsychol 1989;11:675. Sillanpaa M. Epilepsy in children: Prevalence, disability, and handicap. Epilepsia 1992;33:444. Sillanpaa M. Children with epilepsy as adults: Outcome after 30 years of follow up. Acta Paediatr Scand 1990;368 (Suppl):1. Sillanpaa M, Haataja L, Shinnar S. Perceived impact of childhood-onset epilepsy on quality of life as an adult. Epilepsia 2004;45:971. Sillanpaa M, Helenius H. Social competence of people with epilepsy: A new methodologic approach. Acta Neurol Scand 1993;87:335. Singhi PD, Bansal U, Singhi S, et al. Determinants of IQ profile in children with idiopathic generalized epilepsy. Epilepsia 1992;33:1106. Steffenburg S, Gillberg C, Steffenburg U. Psychiatric disorders in children and adolescents with mental retardation and active epilepsy. Arch Neurol 1996;53:904. Steiner TJ, Dellaportas CI, Findley LJ, et al. Lamotrigine monotherapy in newly diagnosed untreated epilepsy: A double-blind comparison with phenytoin. Epilepsia 1999;40:601. Stores G. Problems of learning and behavior in children with epilepsy. In: Reynolds EH, Trimble MJ, eds. Epilepsy and psychiatry. Edinburgh: Churchill Livingstone, 1981. Stores G. School-children with epilepsy at risk for learning and behavior problems. Dev Med Child Neurol 1978;20:502. Stores G, Hart J. Reading skills of children with generalized or focal epilepsy attending ordinary schools. Dev Med Child Neurol 1976;18:705.
Stores G, Williams PL, Styles E, et al. Psychological effects of sodium valproate and carbamazepine in epilepsy. Arch Dis Child 1992;67:1330. Strang JD. Cognitive deficits in children: Adaptive behavior and treatment techniques. Epilepsia 1990;31 (Suppl 4):S54. Sturniolo MG, Galletti F. Idiopathic epilepsy and school achievement. Arch Dis Child 1994;70:424. Sussova J, Seidl Z, Farber J. Hemiparetic forms of cerebral palsy in relation to epilepsy and mental retardation. Dev Med Child Neurol 1990;32:972. Tallian KB, Nahata MC, Lo W, et al. Gabapentin associated with aggressive behavior in pediatric patients with seizures. Epilepsia 1996;37:501. Tatum WO, French JA, Faught E. Postmarketing experience with topiramate and cognition. Epilepsia 2001;42:1134. Trevathan E, Yeargin-Allsopp M, Murphy CC, et al. Epilepsy among children with mental retardation. Ann Neurol 1988;24:321. van den Berg BJ, Yerushalmy J. Studies on convulsive disorders in young children. I. Incidence of febrile and nonfebrile convulsions by age and other factors. Pediatr Res 1969;3:298. Weglage J, Demsky A, Pietsch M, et al. Neuropsychological, intellectual, and behavioral findings in patients with centrotemporal spikes with and without seizures. Dev Med Child Neurol 1997;39:646. Wellesley DG, Hockey KA, Montgomery PD, et al. Prevalence of intellectual handicap in Western Australia. A community study. Med J Aust 1992;156:94. Westbrook LE, Silver EJ, Coupey SM, et al. Social characteristics of adolescents with idiopathic epilepsy: A comparison to chronically ill and nonchronically ill peers. J Epilepsy 1991;4:87. Wheless JW, Ng YT. Levetiracetam in refractory pediatric epilepsy. J Child Neurol 2002;17:413. Wolf SM, Carr A, Davis DC, et al. The value of phenobarbital in the child who has had a single febrile seizure: A controlled prospective study. Pediatrics 1977;59:378. Wong V. Epilepsy in children with autistic spectrum disorder. J Child Neurol 1993;8:316.
CHAPTER 53
Headaches in Infants and Children Donald W. Lewis
Headache is a universal affliction of humankind from which children are not spared. Headache is the most common reason that children are referred to child neurology practices. It is therefore essential for clinicians to have a thorough, systematic approach to the evaluation and management of the child or adolescent with the complaint of headache. Headaches are classified into two categories, primary and secondary (Box 53-1). Migraine and tension-type are examples of primary headache in which there is no underlying pathology and the pain arises from intrinsic processes. Alternatively, the headache pain may result from secondary causes such as brain tumors, increased intracranial pressure, drug intoxications, paranasal sinus disease, or acute febrile illnesses such as influenza. The evaluation of a child presenting with headache follows the traditional medical model with extraction of necessary history and performance of a thorough physical and neurologic examination. In most instances, this initial process will yield a diagnosis or indicate the need for further ancillary testing. Once the diagnosis is established, a comprehensive treatment program can be put into place, blending pharmacologic and biobehavioral measures and being mindful of both physical and emotional factors. The purpose of this chapter is to explore the symptom of headache, reviewing the epidemiology, current classification system, appropriate evaluation, and differential diagnosis.
EPIDEMIOLOGY Headaches are common during childhood and become increasingly more frequent during adolescence. The prevalence of headache ranges from 37% to 51% in 7 year olds, gradually rising to 57% to 82% by age 15. Recurring or frequent headaches occurred in 2.5% of 7 year olds and 15% of 15 year olds [Bille, 1962]. Before puberty, boys are affected more frequently than girls, but after puberty, headaches occur more frequently in girls [Dalsgaard-Nielsen, 1970; Deubner, 1977; Laurell et al., 2004; Sillanpaa, 1983]. The prevalence of migraine headache steadily increases throughout childhood, and the male-to-female ratio shifts during adolescence. The prevalence rises from 3% at ages 3 to 7 years, to 4% to 11% by ages 7 through 11, and up to 8% to 23% during adolescence (Table 53-1). The mean age of onset of migraine is 7.2 years for boys and 10.9 years for girls [Dalsgaard-Nielsen, 1970; Lipton et al., 1994; Mortimer et al., 1992; Sillanpaa, 1976; Small and Waters, 1974; Stewart et al., 1991; Stewart et al., 1992; Valquist, 1955]. Data regarding tension-type headache are limited. Two recent studies including school children, ages 7 to 19 years, using the International Headache Society criteria found a 1year prevalence of tension-type headache to be 10% to 23%.
The prevalence of tension-type headache increased with age in both boys and girls, up to age 11 years, and thereafter increased only in girls [Laurell et al., 2004; Zwart et al., 2004].
CLASSIFICATION The International Headache Society has recently published an updated classification system for headache disorders (see Box 53-1) that is available online at www.ihs.org. Each headache category is further subclassified. The classification for the most common primary headache disorder, migraine, has been modified based on current views of the pathophysiology of migraine, in that the focal, comTABLE 53-1 The Prevalence of Migraine Headache through Childhood By age Prevalence Gender ratio
3–7 years 1.2%–3.2% boys > girls
7–11 years 4%–11% boys = girls
15 years 8%–23% girls > boys
Box 53-1 THE INTERNATIONAL CLASSIFICATION OF HEADACHE DISORDERS Primary Headache Disorders 1. Migraine 2. Tension-type 3. Cluster headache 4. Other primary headache disorders Secondary Headaches 5. Headache attributed to head or neck trauma 6. Headache attributed to cranial or cervical vascular disorder 7. Headache attributed to nonvascular intracranial disorder 8. Headache attributed to substance or withdrawal from substances 9. Headache attributed to infection 10. Headache attributed to disorders of homeostasis 11. Headache attributed to disorders of the cranium, neck, eyes, ears, nose, sinuses, teeth, or other facial or cranial structures 12. Headache attributed to psychiatric disorders 13. Cranial neuralgia and central causes of facial pain 14. Other headache, cranial neuralgia, central or primary facial pain
1184
Nonepileptiform Paroxysmal Disorders and Disorders of Sleep / 53 HEADACHE TYPES
BOX 53-2 2003 INTERNATIONAL CLASSIFICATION OF HEADACHE DISORDERS CRITERIA FOR MIGRAINE
Acute ? Symptoms
Migraine Migraine without aura Migraine with aura Typical aura with migraine headache Typical aura with nonmigraine headache Typical aura without headache Familial hemiplegic migraine Sporadic hemiplegic migraine Basilar-type migraine Childhood periodic syndromes that are commonly precursors of migraine Cyclical vomiting Abdominal migraine Benign paroxysmal vertigo of childhood Retinal migraine Complications of migraine Chronic migraine Status migraine Persistent aura without infarction Migrainous infarction Probable migraine
Acute recurrent Chronic progressive Chronic nonprogressive Mixed
0
30 Time (d)
60
FIGURE 53-1. Five temporal patterns of pediatric headache.
plicated, or variants of migraine are all included under migraine with aura (Box 53-2). For example, a migraine with hemiparesis (e.g., familial or sporadic hemiplegic migraine) falls in the category of migraine with aura. Another change in the new classification system is the inclusion of cyclic vomiting and abdominal migraine within the category of “Childhood periodic syndromes that are commonly precursors of migraine.” The new classification system also recognizes that many patients experience frequent or near daily migraine (more than 15 headaches per month) in a category of “chronic migraine” (see “Chronic Daily Headache”). Omitted from the 2004 classification are “Alternating hemiparesis of childhood” and the “Alice in Wonderland” syndrome. The rare and bizarre entity of alternating hemiparesis of childhood, once thought to be a migrainous phenomenon, is viewed as a metabolic disorder, probably
because of a mitochondrial disorder or a channelopathy. Recently, however, a novel ATP1A2 mutation in a kindred with features that bridge the phenotypic spectrum between alternating hemiparesis of childhood and familial hemiplegic migraine has been reported, which may draw alternating hemiparesis of childhood back into the migraine spectrum [Swoboda et al., 2004]. The Alice in Wonderland syndrome represents transient visual or perceptual disturbances with micropsia or macropsia and, when heralding an otherwise typical migraine headache, is appropriately viewed as migraine with aura. Anatomically, the aura is arising from the occipital, parietal, or posterior temporal lobes to produce these distorted visual symptoms. Another modification in the new classification is to remove “Ophthalmoplegic migraine” from the category of migraine to the group of cranial neuralgias. Although paradoxically still labeled as “migraine,” this clinical entity is characterized by transient disturbances of cranial nerves III, IV, or VI coupled with intense peri- or retro-orbital pain. A separate, clinically useful classification system was proposed by Rothner that divides headache into five temporal patterns (Fig. 53-1): acute, acute-recurrent, chronic-progressive, chronic-nonprogressive, and mixed. Each of these temporal patterns suggests differing pathophysiologic processes and has distinctive differential diagnoses (Table 53-2).
TABLE 53-2 Examples of Syndromes That Cause Headaches ACUTE GENERALIZED
ACUTE LOCALIZED
ACUTE RECURRENT
CHRONIC PROGRESSIVE
CHRONIC NONPROGRESSIVE
Fever Systemic infection Central nervous system infection Toxins: lead CO2 After seizure Electrolyte imbalance Hypertension Hypoglycemia After lumbar puncture Trauma Embolic Vascular thrombosis Hemorrhage Collagen disease Exertional
Sinusitis Otitis Ocular abnormality Dental disease Trauma Occipital neuralgia Temporomandibular joint dysfunction
Migraine Complex migraine Migraine variants Cluster Paroxysmal hemicrania After seizure Tic douloureux Exertional
Tumor Pseudotumor Brain abscess Subdural hematoma Hydrocephalus Hemorrhage Hypertension Vasculitis
Muscle contraction Conversion Malingering After concussion Depression Anxiety Adjustment reaction Hemicrania continua
Lewis / Headaches in Infants and Children
The acute, sudden onset of headache in an otherwise healthy child is usually due to intercurrent viral infection (e.g., upper respiratory infection or pharyngitis). The acute headache with focal neurologic signs must raise concerns for intracranial hemorrhage from aneurysm, vascular malformation, or coagulopathy. Sudden headache with fever warrants consideration of cerebrospinal fluid analysis for the possibility of meningitis. Acute-recurrent pattern implies attacks of headache, separated by symptom-free intervals. The primary headache disorders—migraine and tension-type—are the most common causes of this pattern, although, infrequently, complex partial seizures, substance abuse, cluster headache, and recurrent trauma can produce recurring headache syndromes. Chronic-progressive headaches implies a gradually increasing frequency and severity of headache and is the most ominous of the five temporal patterns. The pathologic correlate is increasing intracranial pressure. Causes of this pattern include brain tumor, hydrocephalus, pseudotumor cerebri, chronic meningitis, brain abscess, or subdural collections. Chronic-nonprogressive or chronic daily headache represents a pattern of frequent or near-constant headache. The definition of CDH requires a period longer than 4 months during which the patient experiences more than 15 headaches per month and the headaches last more than 4 hours per day. Many adolescents will have continual, unremitting, disabling daily headache. Affected patients generally have normal neurologic examinations, and there are usually interwoven psychologic factors and heightened anxiety about unrecognized, underlying organic causes. “Mixed” headache pattern represents the superimposition of acute-recurrent headache (usually migraine) upon a chronic daily background pattern; therefore, it represents a variant of chronic-nonprogressive headache (see later sections).
DIAGNOSTIC CRITERIA The 2004 International Classification of Headache Disorders also establishes the diagnostic criteria for the primary headache disorders (Box 53-3). Beginning in the 1950s, efforts were made to define migraine in children. Valquist, Bille, and later, Prensky and Sommer all proposed the criteria for pediatric migraine, which included the following features: 1. Paroxysmal headache separated by pain-free intervals 2. Accompanied by a variable number of associated features including: Visual aura Nausea Abdominal pain Throbbing quality Unilateral pain Family history of migraine [Bille, 1962; Prensky and Sommer, 1979; Valquist, 1955] In 1988, the International Headache Society established the gold standard for the definition of migraine [Olesen, 1988]. Although these criteria provided a solid framework for adult migraine, their sensitivity for the pediatric population was less than satisfactory. Therefore, in 2003, the International Headache Society revised the diagnostic criteria, incorporating many developmentally sensitive changes that
1185
BOX 53-3 2003 INTERNATIONAL HEADACHE SOCIETY DIAGNOSTIC CRITERIA FOR THE PRIMARY HEADACHE DISORDERS: MIGRAINE AND TENSION-TYPE Pediatric Migraine without Aura A. At least five attacks fulfilling criteria B through D B. Headache attacks lasting 1 to 72 hours C. Headache has at least two of the following characteristics: 1. Unilateral location, may be bilateral, frontotemporal (not occipital) 2. Pulsing quality 3. Moderate or severe pain intensity 4. Aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs) D. During the headache, at least one of the following: 1. Nausea and/or vomiting 2. Photophobia and phonophobia, which may be inferred from behavior E. Not attributed to another disorder Episodic Tension-Type Headache A. At least 10 episodes occurring on more than 1, but fewer than 15 days per month for at least 3 months and fulfilling criteria B through D. B. Headache lasting 30 minutes to 7 days. C. Headache has at least two of the following characteristics: 1. Bilateral location 2. Pressing or tightening (nonpulsing) quality 3. Mild or moderate intensity 4. Not aggravated by routine physical activity such as walking or climbing stairs. D. Both of the following: 5. No nausea or vomiting (anorexia may occur) 6. Photophobia or phonophobia (but not both) F. Not attributed to another structural or metabolic disorder permit a broader applicability for children and adolescents, maintaining specificity and improving sensitivity [Olesen, 2004]. These new criteria accept the clinical observations that pediatric migraine may be brief (≈1 hour) and bifrontal, and that the associated symptoms of photophobia and phonophobia may be inferred by the child’s behavior, such as withdrawing to a dark, quiet room to rest during the headache attack. The diagnostic criteria also include cyclic vomiting and abdominal migraine (Boxes 53-4 and 53-5).
EVALUATION OF THE CHILD WITH HEADACHE The evaluation of a child with headaches follows the traditional medical model and begins with a thorough medical history and complete physical and neurologic examination. A brief series of questions shown in Box 53-6 provides a logical framework for evaluating headaches and generally yields sufficient information to diagnose most primary headaches and reveal clues to the presence of secondary headache disorders.
1186
Nonepileptiform Paroxysmal Disorders and Disorders of Sleep / 53
Box 53-4 INTERNATIONAL CLASSIFICATION OF HEADACHE DISORDERS CRITERIA FOR CYCLIC VOMITING Description Recurrent episodic attacks, usually stereotypical in the individual patient, of vomiting and intense nausea. Attacks are associated with pallor and lethargy. There is complete resolution of symptoms between attacks. Diagnostic Criteria A. At least five attacks fulfilling criteria B and C B. Episodic attacks, stereotypical in the individual patient, of intense nausea and vomiting lasting 1 to 5 days C. Vomiting during attacks occurs at least 5 times/hour for at least 1 hour D. Symptom-free between attacks E. Not attributed to another disorder. History and physical examination do not reveal signs of gastrointestinal disease.
Box 53-5 INTERNATIONAL CLASSIFICATION OF HEADACHE DISORDERS CRITERIA FOR ABDOMINAL MIGRAINE Description An idiopathic recurrent disorder seen mainly in children and characterized by episodic midline abdominal pain manifesting in attacks lasting 1 to 72 hours with normality between episodes. The pain is of moderate-to-severe intensity and associated with vasomotor symptoms, nausea, and vomiting. Diagnostic Criteria A. At least five attacks fulfilling criteria B through D B. Attacks of abdominal pain lasting 1 to 72 hours C. Abdominal pain has all of the following characteristics: 1. Midline location, periumbilical or poorly localized 2. Dull or “just sore” quality 3. Moderate or severe intensity D. During abdominal pain, at least two of the following: 1. Anorexia 2. Nausea 3. Vomiting 4. Pallor Not attributed to another disorder. History and physical examination do not indicate signs of gastrointestinal or renal disease, or such disease has been ruled out by appropriate investigations. The role of further ancillary diagnostic studies such as laboratory testing, electroencephalography (EEG), and neuroimaging has been extensively reviewed in a practice parameter of the American Academy of Neurology [Lewis et al., 2002]. The practice parameter determined that there is inadequate documentation in the literature to support any recommendation as to the appropriateness of routine laboratory studies (e.g., hematology or chemistry panels) or
Box 53-6 KEY QUESTIONS TO ASK IN THE EVALUATION OF CHILDREN WITH HEADACHES Headache Database 1. How and when did your headache(s) begin? 2. What is the time pattern of your headache: sudden first headache, episodes of headache, an everyday headache, gradually worsening, or a mixture? 3. Do you have one type of headache or more than one type? 4. How often does the headache occur and how long does it last? 5. Can you tell that a headache is coming? 6. Where is the pain located and what is the quality of the pain: pounding, squeezing, stabbing, or other? 7. Are there any other symptoms that accompany your headache: nausea, vomiting, dizziness, numbness, weakness, or other? 8. What makes the headache better or worse? Do any activities, medications, or foods tend to cause or aggravate your headaches? 9. Do you have to stop your activities when you get a headache? 10. Do the headaches occur under any special circumstances or at any particular time? 11. Do you have other symptoms between headaches? 12. Are you taking or are you being treated with any medications (for the headache or other purposes)? 13. Do you have any other medical problems? 14. Does anyone in your family suffer from headaches? 15. What do you think might be causing your headache? Adapted from Rothner, 1995.
performance of lumbar puncture. Routine EEG is not recommended as part of the headache evaluation. Data compiled from eight studies demonstrated that the EEG was not necessary for differentiation of primary headache (e.g., migraine, tension-type) from secondary headache due to structural disease involving the head and neck or from headaches due to a psychogenic etiology. EEG is unlikely to define or determine an etiology of the headache or distinguish migraine from other types of headaches. Furthermore, in those children undergoing evaluation for recurrent headache who were found to have paroxysmal EEGs, the risk of future seizures is negligible. The role of neuroimaging is better defined. Data compiled from six pediatric studies permitted the following recommendations: 1. Obtaining a neuroimaging study on a routine basis is not indicated in children with recurrent headaches and a normal neurologic examination. 2. Neuroimaging should be considered in children in whom there are historical features to suggest the following: a. Recent onset of severe headache b. Change in the type of headache c. Neurologic dysfunction
Lewis / Headaches in Infants and Children
3. Neuroimaging should be considered in children with an abnormal neurologic examination (e.g., focal findings, signs of increased intracranial pressure, significant alteration of consciousness) and the coexistence of seizures. Care must be taken not to over- or underinterpret these recommendations. Neuroimaging may be considered in children with recurrent headache based on clues extracted from the medical history or on the findings of neurologic examination. Since publication of this parameter, feedback from clinicians and personal experience has demonstrated that many in the “managed care industry” have focused only on recommendation number one and not recognized numbers two and three, which clearly places the responsibility in the hands of the clinician to make the decision to perform ancillary testing, including neuroimaging, based on good clinical judgment. The findings of the American Academy of Neurology support the medical decision to perform scans or to withhold scans, based on clinical determinants for the individual patient.
PRIMARY HEADACHE SYNDROMES Migraine Migraine is the most common acute-recurrent headache syndrome. The classifications of migraine are shown in Box 53-2 and the cardinal diagnostic features are shown in Box 53-3.
Pathophysiology Migraine is considered to be a primary neuronal process (Fig. 53-2) [Pietrobon and Striessnig, 2003; Silberstein,
Abnormal cortical hyperexcitability
?
CORTICAL SPREADING DEPRESSION Brainstem nuclei Activation of trigeminovascular system
Sterile neurogenic inflammation
Central and peripheral sensitization
MIGRAINE ATTACK
FIGURE 53-2. Migraine pathophysiology. (Adapted from Pietrobon D, Striessnig J. Neurobiology of migraine. Nat Rev 2003;4:386.)
1187
2004]. The principal underlying phenomenon of migraine is a hyperexcitable cerebral cortex. Polygenic influences produce disturbances of neuronal ion channels (e.g., calcium channels), leading to a lowered threshold for external and/or internal factors that trigger episodes of cortical spreading depression. Cortical spreading depression represents a slowly propagating wave (≈2 to 6 mm/minute) of neuronal depolarization and is now viewed as the key initial phase that is responsible for (1) migraine aura and (2) activation of the “trigeminovascular system.” The aura of migraine represents transient, focal somatosensory phenomena such as visual scotomata or distortions, dysesthesias, hemiparesis, or aphasia. The aura is viewed to be caused by the regional neuronal depolarization and/or the accompanying regional oligemia observed with cortical spreading depression. In addition to sustained cortical oligemia, cortical spreading depression is accompanied by extravasation of plasma proteins from dural vessels and activation of meningeal afferents. The sum of these effects is to increase FOS expression in the trigeminal nucleus within the brainstem [Prensky and Sommer, 1979]. Cortical spreading depression, then, is the key event for episodic activation of the trigeminal vascular system that culminates in the migraine attack. The role played by the brainstem nuclei is controversial. Some investigators believe the locus ceruleus and dorsal raphe nuclei act as the “migraine generator,” initiating noradrenergic and serotonergic signals to the cortex and dural vessels in a parallel fashion. Other investigators favor the view that cortical spreading depression is the initiating phenomenon and believe that the brainstem nuclei provide a “permissive” role, favoring “central trigeminal hyperexcitability.” Although cortical spreading depression nicely explains the somatosensory aura, only about 30% of children and adolescents experience aura. Clearly, the processes leading to pain may occur in the absence of a perceived aura. Two mechanisms are thought to be responsible for the generation of the pain of migraine: (1) neurogenic inflammation of the meningeal vessels and (2) “sensitization” of peripheral and central trigeminal afferents. Cortical spreading depression initiates vascular dilation with extravasation of plasma proteins from dural vessels and activates trigeminal meningeal afferents. These processes set the stage for “neurogenic” inflammation of the dural and pial vessels, mediated principally by neuropeptides and calcitonin gene-related protein. The inflammatory cascade stimulates nociceptive afferents, leading to pain. Many authors question whether neurogenic inflammation alone is sufficient to produce the pain of migraine. One of the striking features noted during an attack of migraine is that seemingly innocuous activities, such as coughing, walking up stairs, or bending over greatly intensify the pain. In fact, the International Classification of Headache Disorders criteria include “aggravation” by activities as one of the diagnostic features of migraine. This observation coupled with elegant research has led to the concepts of “sensitization” of trigeminal vascular afferents, whereby both peripheral and central afferent circuits become exceptionally sensitive to mechanical, thermal, and chemical stimuli. These circuits become so sensitive that
1188
Nonepileptiform Paroxysmal Disorders and Disorders of Sleep / 53
virtually any stimulation is perceived as painful, the concept of allodynia [Burstein et al., 2000; Burstein et al., 2004; Burstein and Jakubowski, 2004]. Therefore, the current view of the pathophysiology of migraine begins with an inherited vulnerability with a hyperexcitable cerebral cortex. A variety of stimuli may trigger episodes of cortical spreading depression, which, in turn, initiates the processes of localized, neurogenic inflammation and of sensitization of both peripheral and central afferent circuitry.
Clinical Manifestations MIGRAINE WITHOUT AURA The diagnostic criteria for migraine without aura are shown in Box 53-3. Migraine without aura is the most frequent form, accounting for 60% to 85% of all migraine in children and adolescents. Patients often recognize prodromal features: mood changes (euphoria to depression), irritability, lethargy, yawning, food cravings, or increased thirst. Perhaps the most frequent heralding feature is a change in behavioral patterns or withdrawal from activities. A migraine headache begins gradually and is usually localized to the frontal or temporal region. The pain may be unilateral. The quality is generally described as pounding, pulsing, or throbbing, but the key feature is its intensity. Routine activities will be interrupted. Photophobia and phonophobia are common and may be inferred by the child’s desire to seek a quiet, dark place to rest or even to sleep because sleep often produces significant relief. Nausea, vomiting, and abdominal pain may be the most disabling feature because a student with headache may be able to stay in the classroom with pain, but the onset of nausea or vomiting necessitates a visit to the school nurse. A migraine headache typically last for hours, even days (1 to 72 hours) but does not generally occur more fre-
TABLE 53-3 Migraine Aura Visual:
Sensory: Motor: Aphasia Psychic:
Negative scotoma “Fortification” scotoma Field deficits: Hemianopsia Quadrantanopsia Photopsia Visual distortions: Teichopsia Metamorphopsia Prosopagnosia “Alice in Wonderland” Parasthesias Dysesthesias Perioral and/or hand numbness (chiro-oral) Hemiparesis Monoparesis Confusion Dysphasia Amnesia Disequilibrium
quently than 6 to 8 times per month. More than 8 to 10 attacks per month must warrant consideration of alternative diagnoses such as organic conditions (i.e., pseudotumor cerebri) or the chronic daily headache syndromes [American College of Emergency Physicians, 1996; Gladstein et al., 1997]. The time of day when the headache occurs tends to shift through childhood. Younger children often complain in the afternoon, after school. Younger teenagers frequently begin to report their headaches about lunchtime, often precipitated by the chaos of the school cafeteria with its combination of bright lights, loud noise, and peer pressure. Older teens acquire the more adult patterns of morning headache, often a concern because morning occurrence frequently raises suspicion of space-occupying lesions. Although most verbal children can readily relate to these symptoms, the developmentally challenged child may be unable to express these complaints. Caregivers report repeated cycling events of quiet, withdrawn behavior with pallor, regurgitation, vomiting, and desire to rest. These stereotyped episodes may prompt investigation for epilepsy, gastroesophageal reflux, or hydrocephalus, when in fact they may represent migraine.
MIGRAINE WITH AURA Approximately 14% to 30% of children report visual disturbances, distortions, or obscuration before or as the headache begins (Table 53-3) [Lewis, 1995]. The aura (“cool breeze”) is, however, an inconsistent feature in childhood and adolescents. The presence of an aura must be elicited with very specific questions: “Do you have spots, colors, lights, or dots in your eyes before or as you are getting a headache?” Typically, the aura is a visual phenomenon, but, as discussed in the pathophysiology section previously, the cortical spreading depression responsible for the aura may disturb virtually any cortical region including language, motor, or sensory areas. The classic visual symptomatology during migraine include three dominant visual phenomena: 1. Binocular visual impairment with scotoma (77%) 2. Distortion or hallucinations (16%) 3. Monocular visual impairment or scotoma (7%) [Hachinshi et al., 1973] The onset of the visual aura is gradual and lasts minutes. Sudden images and complicated visual perceptions should prompt consideration of complex partial seizures, even if followed by headache. Young adolescents may experience strange visual effects (distortions, illusions, micropsia, and macropsia) within the spectrum of the Alice in Wonderland syndrome. Transient visual obscurations, brief episodes of near-complete blindness, are also features of pseudotumor cerebri. The aura has long been thought to be an extremely useful feature therapeutically, with early warning of an impending headache permitting the institution of abortive measures such as ergotamine or the “triptan” agents. Unfortunately, the therapeutic utility of treating the headache at the onset of the aura in adolescent migraine is not reliable or effective.
Lewis / Headaches in Infants and Children
Alice in Wonderland Syndrome Bizarre visual illusions and spatial distortions occasionally precede migraine headaches. Similar to Alice’s visual distortions after eating mushrooms in Through the Looking Glass, affected children describe visual distortions before or as the headache is beginning. The children may describe bizarre or vivid visual illusions, such as the following: Macropsia: objects appear larger Micropsia: objects appear smaller Metamorphopsia: objects (such as faces) appear distorted Teleopsia: objects appear far away These patients are often not confused or frightened by these illusions and are able to relate the experience in enthusiastic detail. This unusual visual symptomatology is best considered as migraine with aura, though historically, Alice-in-Wonderland syndrome is included as a distinct variant. This type of visuoperceptual abnormality has been reported with infectious mononucleosis, complex partial seizures, and hallucinogenic drug ingestion.
Retinal Migraine Also referred to as ocular, ophthalmic, or anterior visual pathway migraine, retinal migraine is uncommon in young children but occurs during adolescence. Affected patients will report brief (seconds to